The Latest Paper From Neil Ferguson et al. Defending the Lockdown Policy is Out of Date, Inaccurate and Misleading

By Mike Hearn • The Daily Sceptic • August 24, 2021
Neil Ferguson’s team at Imperial College London (ICL) has released a new paper, published in Nature, claiming that if Sweden had adopted U.K. or Danish lockdown policies its Covid mortality would have halved. Although we have reviewed many epidemiological papers on this site, and especially from this particular team, let us go unto the breach once more and see what we find. The primary author on this new paper is Swapnil Mishra.
The paper’s first sentence is this:
The U.K. and Sweden have among the worst per-capita Covid mortality in Europe.
No citation is provided for this claim. The paper was submitted to Nature on March 31st, 2021. If we review a map of cumulative deaths per million on the received date then this opening statement looks very odd indeed:
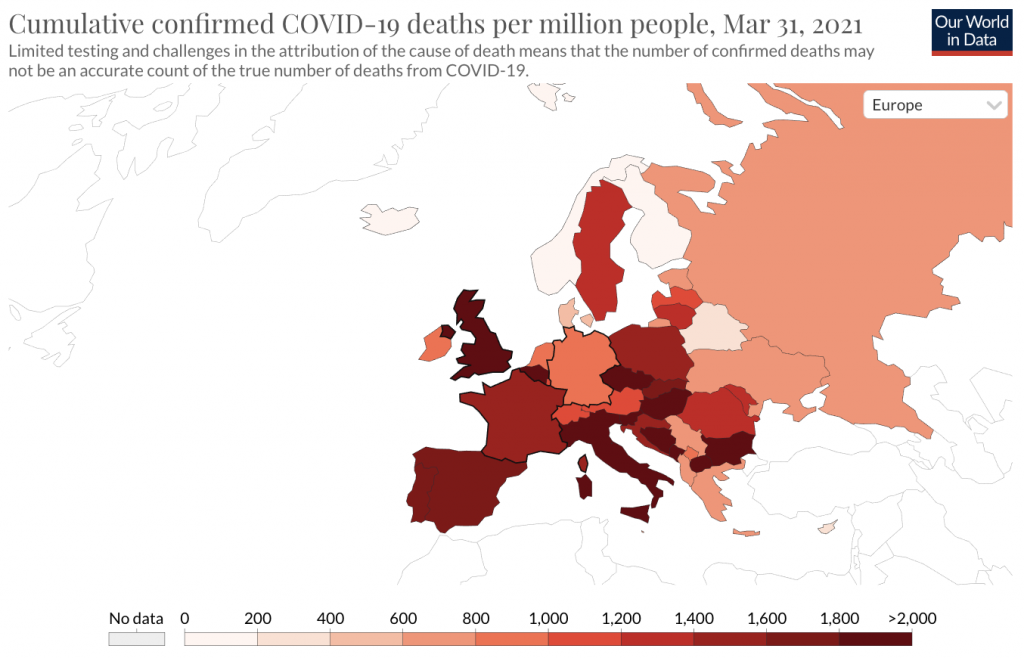
Sweden (with a cumulative total of 1,333 deaths/million) is by no means “among the worst in Europe” and indeed many European countries have higher totals. This is easier to see using a graph of cumulative results:
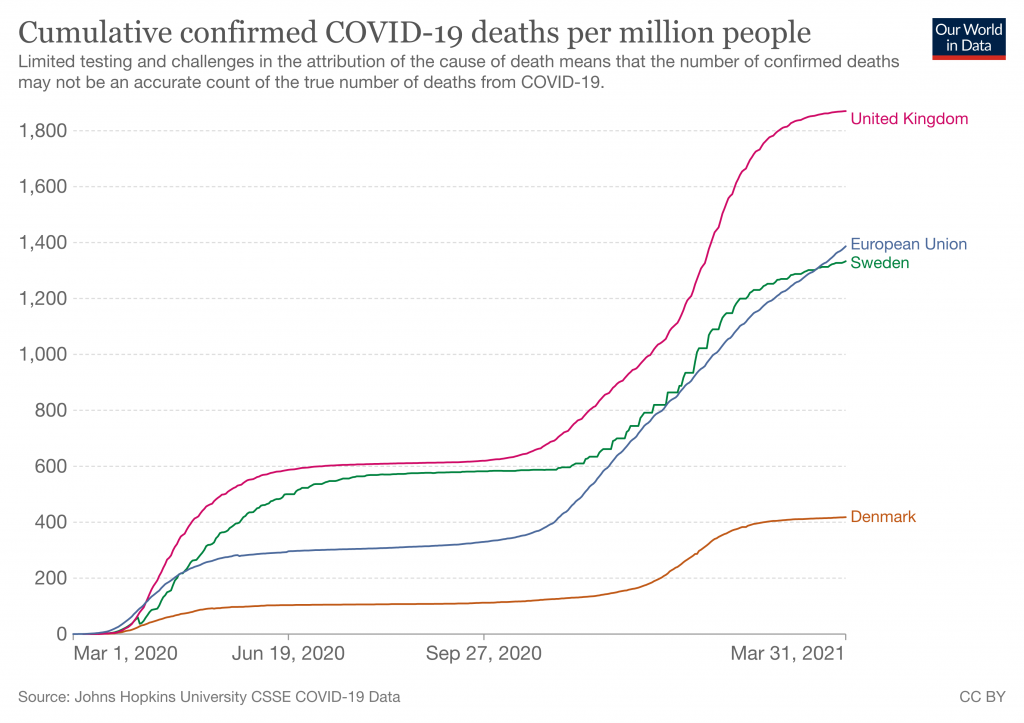
But that was in March, when the paper was submitted. We’re reviewing it in August because that’s when it was published. Over the duration of the journal’s review period this statement – already wrong at the start – became progressively more and more incorrect:
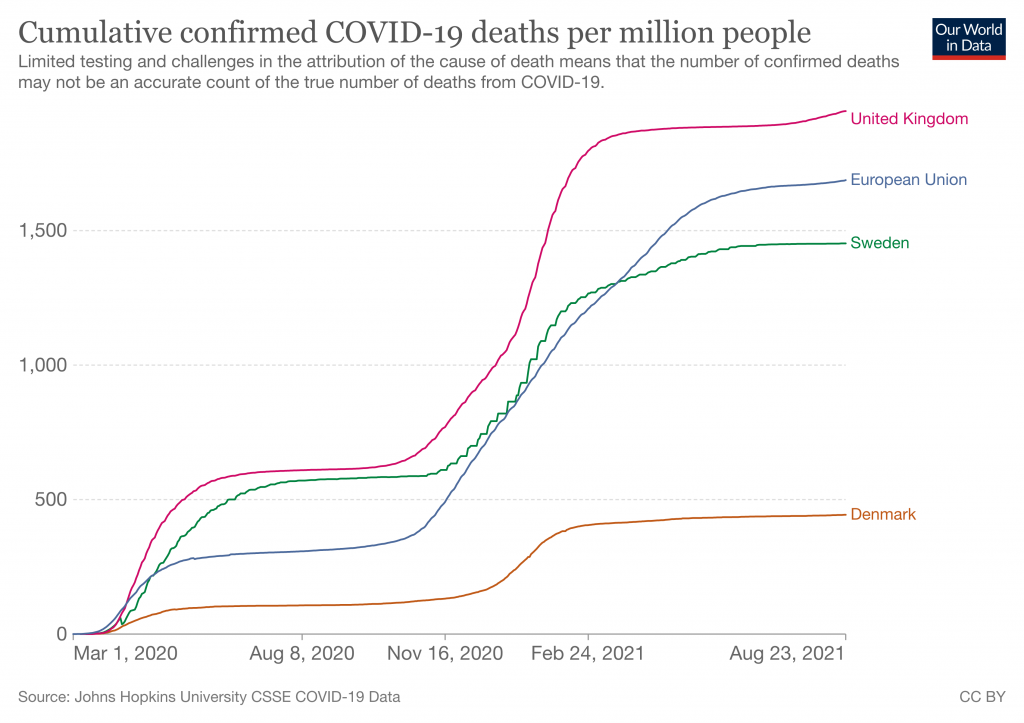
As always, we must note that these ‘death’ graphs can be heavily affected by testing levels, because Covid deaths are defined as any death within 28 days of a positive test. The U.K. tests much more than Sweden does. But putting that to one side, Sweden by now has significantly better results than the rest of the E.U. What’s going on here? A likely explanation is that although the paper was submitted in March it was actually written some time last year, probably starting around the end of the summer and finishing up in August. There then followed a strange many month gap before they submitted it, and then many more months were added by the glacial peer review process journals use. We can see evidence of this timeline in the abstract, where they say:
We use two approaches to evaluate counterfactuals which transpose the transmission profile from one country onto another, in each country’s first wave from March 13th (when stringent interventions began) until July 1st, 2020.
More evidence comes from the upload dates on the released code, which is from 10 months ago. In other words, Nature is publishing a paper about the fast-moving coronavirus situation that builds its entire case on obsolete data more than a year old, without explicitly noting that anywhere. In July 2020, Sweden and the U.K. did indeed have worse results than the rest of the E.U. However as we now know, this meant nothing and a year on the data looked very different.
Why did ICL wait so long before submitting this paper to Nature? No obvious explanation occurs. And why didn’t anyone notice that the claims were no longer true? Not for the first time, it appears nobody can actually be reading these papers adversarially before publication. Time and again we see that at major scientific journals the lights are on, but nobody’s home.
Seeing this made me wonder if they were once more engaging in a favourite trick of this team, by using Verity et al.‘s obsolete infection:fatality ratio estimates from January 2020. And indeed they are:
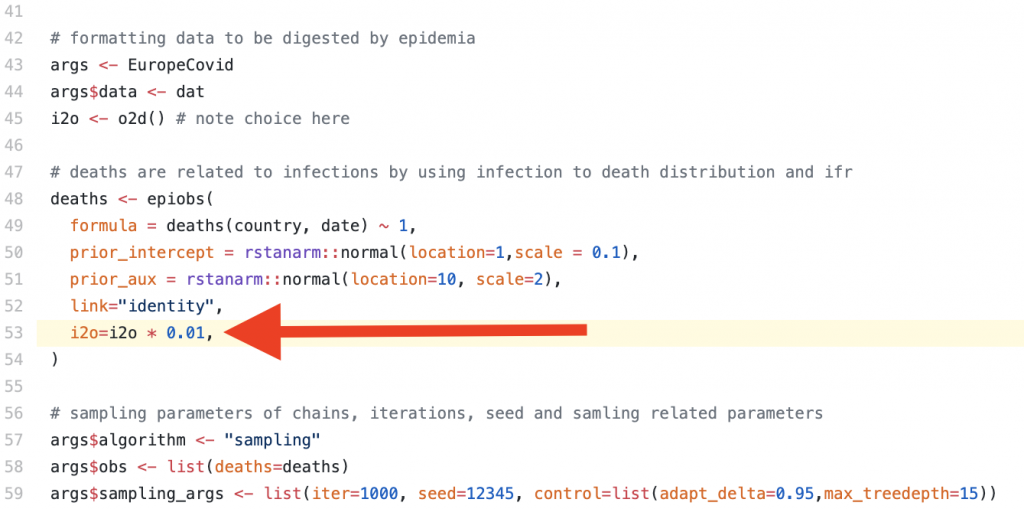
The idea that 1% of all SARS-CoV-2 infections would lead to death was later disputed as being ~4x too high by a meta-study of seroprevalence data published by the WHO. This newer estimate was based on far larger sample sizes, and serosurveys give an ability to detect people who recently had mild disease without getting tested or reporting it at the time. It’s thus a much more scientifically robust method of IFR estimation than Verity’s paper, which being written very early on had to rely on media reports and questionably reliable information coming out of China. As the authors discuss in the supplementary material, using a lower IFR (they try 0.5) means that the U.K.’s predicted mortality from adopting the Swedish strategy drops significantly due to the changed impact of herd immunity.
Who is responsible for this situation? Nature appears to be knowingly publishing a paper on Covid that makes claims in the present tense, but which is in reality so out of date that the very first sentence is factually false. This is not merely useless but actively damaging because non-academic readers (i.e., politicians and public health officials) will reasonably assume that claims published by scientists about Covid in August 2021 were actually written in August and have some relevance to the current situation. Nowhere is it explicitly stated at what time the analysis was believed to be accurate: it must instead be inferred from the choice of datasets and audit trails left on the source code hosting site they use.
Overall approach
Moving on. What does the model actually do?
The core concept is to try and calculate the changing infectiousness of SARS-CoV-2 for each of the U.K., Sweden and Denmark over time, then ‘graft’ the generated timeseries for R(t) onto the other countries. As is typical for this team, the authors assume that changes in Rt are driven only by government interventions or voluntary behavioural changes, and thus by transposing Rt onto other countries they claim to be calculating what would have happened if different countries had adopted each other’s policies. They try two different approaches to this, an ‘absolute’ and a ‘relative’ approach.
There are many problems with this methodology.
The study of only the U.K., Sweden and Denmark has no scientific basis. Why Denmark and not, say, France? This selection is very obviously politically motivated. In fact, the entire paper is basically a policy paper designed to influence politicians, not answer any question about viruses that a real scientist might ask.
With the benefit of 2021 hindsight we can argue persuasively that lockdowns had no real impact on Covid. The most recent and effective demonstration of that was the U.K.’s ‘Freedom Day’ in which cases dropped off a cliff just days after restrictions were relaxed, in defiance of the warnings of “international health leaders” that this would be “foolish” and “unethical”, a “threat to the world”, etc. There have been many other such events and analyses of global datasets show no correlation between lockdowns and health outcomes. Thus their underlying assumption that social policy is responsible for different outcomes is wrong. In fact, although they are well aware that there must be many factors influencing mortality outcomes, they explicitly disregard all of them: “While we cannot fully encompass the myriad of differences between each country, our analysis is nonetheless informative on best practice for control of future waves of the Covid pandemic.”
Despite asserting that their analysis can tell lawmakers what to do in future epidemics, they later admit that “our counterfactual scenarios should be interpreted as a exchange of both population behaviour and government policy between donor and recipient countries“. This is important for them to admit because they tried to explain why Covid has varying infectiousness in different countries by reference to “cultural differences“, which they boil down to a single statistic about the proportion of single person households in each country. But this is illogical nonsense. Even if we (wrongly) assume that all differences in observed outcomes are to do with policy and culture, governments cannot magically make the U.K. population become Danish or vice-versa. Any analysis that assumes this and claims to be “informative on best practice” is wrong and should have been dropped during peer review.
The paper has another difficulty with being “informative“. Although the authors propose two different approaches to try and answer the same underlying question, the two approaches give totally different answers. For example: “If Denmark followed U.K. policies, our relative approach estimates that mortality would not have been markedly different, although our absolute approach implies that mortality would have been more than twice that observed.” Their calculations aren’t even consistent with each other, yet the paper provides no specific recommendation on which approach is supposed to yield the best answer.
Other problems include an inability to actually calculate Rt from death data (“the high variance of this distribution leads to high uncertainty in Rt estimates“), even though their entire analysis is based on the presumed integrity of that calculation, and an implausibly high sensitivity to the exact starting date of policy changes (“a three-day difference in the introduction of measures can lead to twofold differences in mortality“). The strength of this connection in their model is absurd and would appear to be strongly motivated by ICL’s attempted rewriting of history to one of: “If only the Government had listened to us sooner everything would have been far better.”
Conclusion
Given the history of this department, it’s no surprise that ICL is still churning out delusional and misleading epidemiology papers. They will continue doing so for as long as they’re funded. Analysing each and every one is a futile effort due to the sheer scale at which academia operates (e.g. this paper alone has 19 authors). But we can nonetheless learn some more about bad science by reading them. This paper shows all the usual hallmarks of an academic sector that’s gone off the rails:
- A grotesque level of data cherry picking.
- A publishing process so slow that the claims are entirely wrong on the date of publication, and wrong from literally the first sentence.
- A delusional belief that their work is “informative” to policy makers, despite implicitly arguing that entire societies can be transplanted from one country to another.
Who is ultimately responsible for stopping this? It must be the funders, who for this paper include:
- The National Institute for Health Research
- The Bill and Melinda Gates Foundation
- The U.K. Medical Research Council
- Community Jameel (a Saudi family foundation)
- Microsoft, who donated free compute time on Azure
- And finally, universities and other institutions who subscribe to Nature despite its history of publishing misleading papers
The theme here is that none of these organisations is paying close attention to what’s actually being written, apparently including the journals and peer reviewers. For funders, giving away money is not the means but the end. Until research is funded by people who actually care about the utility of the results our society will continue to be flooded with highly evolved scientism, of which the output of the ICL Epidemiology Department is a textbook example.
Mike Hearn is a former Google software engineer. You can read his blog here.
With a “left press” like this, who needs fascist media?
“Progressive” stars and outlets manage not to say a word about the gravest crisis in the history
By Mark Crispin Miller | OffGuardian | August 27, 2021
It pains me to say it, but Caitlin Johnstone—whose work I used to champion ardently, defending her against the crypto-Stalinists at Counterpunch—is one of many “leftists” who keep partying like it’s 2019.
Same with the interminable Noam Chomsky, The Nation, Consortium News, MoveOn, Popular Resistance, Nation of Change, Covert Action Bulletin, Naomi Klein, Tom Engelhardt and others that I used to champion, and (in some cases) see as friends, as well as outlets that I used to write for.
So Caitlin loves her boomer Dad for his irrepressible outrage over the bombing of Afghanistan, and loves ALL boomers for their fiery dissidence—on issues that don’t matter much at this apocalyptic moment.
From her, and all those other “progressive” voices/outlets, you’d never know that World War III has been raging (openly) since January 2020—a global war against humanity itself.
Someone should tell Caitlin—an Australian!—that those feisty boomers, with some very few exceptions, have turned rigidly authoritarian, and often downright hateful toward the bravest and most necessary dissidents today, standing firm against the bio-fascist mandates of the New World Order, and the looming portents of the Great Reset: dangers that those “leftist” sages never even mention, much less question or confront.
While Caitlin, resident of Melbourne, riffs indignantly about the bombing of Afghanistan back in 19 B.C. (Before COVID), the staunchest dissidents Down Under are the truck drivers threatening to shut that country down, if its cops don’t take their boots off everybody’s necks.
In the midst of this vast slo-mo Holocaust, conducted in the name of “public health” (much as the last one was), we find no reference to it, nor any reference to the unprecedented global wave of censorship on which that Holocaust depends, or to the naked violence of the police throughout the “democratic” West, or to the financial purposes of this whole global nightmare, in any of the “leftist” outlets named above.
Instead, we get “Ban Killer Drones,” “Why US Policy in Nicaragua Isn’t Working,” “America’s Merchants of Death Then and Now” (with no mention of Big Pharma), “Hidden costs of militarism: Climate change, pollution and biodiversity loss,” and (my personal favorite) “Is a Cold War Still Possible in an Overheating World?”
My point is not that such well-worn concerns don’t matter anymore (though some of them were overblown before the COVID crisis), but that they’re now being used by our “left” press to give the misimpression that they’re really on the left — working for peace, freedom, civil rights and economic fairness, always in the interests of the people over all — instead of blinding us to this unprecedented global drive to make those things impossible, and snuff the people out.
Mark Crispin Miller is Professor of Media, Culture and Communication at New York University and the author of several books, including Boxed In: The Culture of TV; Seeing Through Movies; Mad Scientists: The Secret History of Modern Propaganda; Spectacle: Operation Desert Storm and the Triumph of Illusion; and The Bush Dyslexicon. You can read more of his work through his newsletter, News from the Underground
ALERT: All Parents In U.K. With Children Aged 12 – 15 years
By Dr. Mike Yeadon | August 26, 2021
I’ve just been informed via someone senior in the vaccination authorities that they will begin VACCINATING ALL SCHOOL CHILDREN AGED 12 – 15 years old STARTING SEPTEMBER 6th 2021.
WITH OR WITHOUT YOUR CONSENT.
Children are at no measurable risk from SARS-CoV-2 & no previously healthy child has died in U.K. after infection. Not one.
The vaccines are NOT SAFE. The USA reporting system VAERS is showing around 13,000 deaths in days to a few weeks after administration. A high % occur in the first 3 days. Around 70% of serious adverse events are thromboembolic in nature (blood clotting- or bleeding-related).
We know why this is: all of the gene-based vaccines cause our bodies to manufacture the virus spike protein & that spike protein triggers blood coagulation.
The next most common type of adverse events are neurological.
Death rates per million vaccinations are running everywhere at around 60X more than any previous vaccine.
Worse, thromboembolic events such as pulmonary embolisms, appear at over 400X the typical low rate after vaccination.
These events are serious, occur at a hideously elevated level & are at least as common in young people as in elderly people. The tendency is that younger people are having MORE SEVERE adverse events than older people.
There is literally no benefit whatsoever from this intervention. As stated, the children are unquestionably NOT AT RISK & vaccinating them WILL ONLY RESULT IN PAIN, SUFFERING, LASTING INJURIES AND DEATH.
Children rarely even become symptomatic & are very poor transmitters of the virus. This isn’t theory. It’s been studied & it pretty much doesn’t happen that children bring the virus into the home. In a large study, on not one occasion was a child the ‘index case’ – the first infected person in a household.
So if you’re told “it’s to protect vulnerable family members”, THAT IS A LIE.
The information emerging over time from U.K. & Israel is now showing clearly that the vaccines DO NOT EVEN WORK WELL. If there’s any benefit, it wanes.
Finally, the vaccines ARE NOT EVEN NECESSARY. There are good, safe & effective treatments.
IF YOU PERMIT THIS TO GO AHEAD I GUARANTEE THIS: THERE WILL BE AVOIDABLE DEATHS OF PERFECTLY HEALTHY CHILDREN, and severe illnesses in ten times as many.
And for no possible benefit.
KNOWING WHAT I KNOW FROM 40 years TRAINING & PRACTISE IN TOXICOLOGY, BIOCHEMISTRY & PHARMACOLOGY, to participate in this extraordinary abuse of innocent children in our care can be classified in no other way than MURDER.
It’s up to you. If I had a secondary school age child in U.K., I would not be returning them to school next month, no matter what.
The state is going to vaccinate everyone. The gloves are off. This has never been about a virus or public health. It’s wholly about control, totalitarian & irreversible control at that, and they’re nearly there.
PLEASE SHARE THIS INFORMATION WIDELY.
With somber best wishes,
Mike
Dr Mike Yeadon
The Dubious Ethics of ‘Nudging’ the Public to Comply With Covid Restrictions

By Dr. Gary Sidley | The Daily Sceptic | August 22, 2021
A middle-aged woman, walking along a pavement in the afternoon sunshine, sees a young family approaching and instantly becomes stricken with terror at the prospect of contracting a deadly infection. A man in a queue in a garage kiosk leans into the face of another and screams, “You selfish idiot! Hundreds of people will die because you don’t wear a mask.” The aggressor is oblivious to the fact that his victim suffers a history of asthma and anxiety problems. A neighbour puts on a face covering and plastic gloves before wheeling her dustbin to the end of her drive. These are three recent examples of many similar events I’ve observed or read. What could be the main reason for such extraordinary behaviour? Has the emergence of the SARS-COV-2 virus magically re-wired our brains, transforming many of us into vindictive germaphobes?
No, of course not. These extreme human reactions are, I believe, primarily the result of the Government’s deployment of covert psychological ‘nudges’, introduced as a means of increasing people’s compliance with the Covid restrictions.
In an article in the Critic, I discussed the remit of the Government’s behavioural scientists in the Scientific Pandemic Insights Group on Behaviours (SPI-B), a subgroup of SAGE which offers advice to the Government about how to maximise the impact of its Covid communications strategy. The methods of influence recommended by the SPI-B are drawn from a range of ‘nudges’ described in the Institute of Government document, MINDSPACE: Influencing behaviour through public policy, several of which primarily act on the subconscious of their targets – the British people – achieving a covert influence on their behaviour. The three ‘nudges’ to have evoked the most controversy, among both psychological practitioners and the general public, are: the strategic use of fear (inflating perceived threat levels); shame (conflating compliance with virtue); and peer pressure (portraying non-compliers as a deviant minority) – or ‘affect’, ‘ego’ and ‘norms’, to use the language of behavioural science. (Specific examples of how each of these covert strategies have been used throughout the Covid crisis are described here).
The British Psychological Society (BPS) is the leading professional body for psychologists in the U.K. According to their website, a central role of the BPS is: “To promote excellence and ethical practice in the science, education and application of the discipline.” In light of this remit, I – together with 46 other psychologists and therapists – wrote a letter to the BPS on January 6th, 2021, expressing our ethical concerns about the use of covert psychological strategies as a means of securing compliance with Covid restrictions. In particular, our alarm centred on three areas: the recommendation of ‘nudges’ that exploit heightened emotional discomfort as a means of securing compliance; implementing potent covert psychological strategies without any effort to gain the informed consent of the British public; and harnessing these interventions for the purpose of achieving adherence to contentious and unevidenced restrictions that infringe basic human rights.
Responses from the BPS to our initial letter were slow and circuitous. However, on July 1st we received an email from Dr. Roger Paxton, the Chair of the Ethics Committee, which clarified the BPS’s position: in the Committee’s view, there is nothing ethically questionable about deploying covert psychological strategies on the British people as a means of increasing compliance with public health restrictions.
An in-depth inspection of Dr. Paxton’s defence of the BPS reveals that it is evasive, disingenuous and wholly unconvincing.
First, he quibbles about the use of the word “covert”, arguing that the compliance techniques under scrutiny are more appropriately described as “indirect”. Behavioural-science documents routinely refer to the psychological strategies underpinning Government communication campaigns as evoking responses from people that are “unconscious”, “subconscious” or “automatic”. The crucial point is that the human targets of these ‘nudges’ are often unaware that the intention of the SPI-B psychologists is to scare, shame them and socially pressure them to conform. The MINDSPACE publication – co-authored by Professor David Halpern, an SPI-B and SAGE member – seems to concur: “Citizens may not fully realise that their behaviour is being changed… Clearly, this opens Government up to charges of manipulation… [as] it may offer little opportunity for citizens to opt-out.” (p. 66)
Second, Dr. Paxton rejects the idea that it would be ethical to offer citizens an opportunity to opt-out by asserting that the application of covert psychological strategies to shape people’s behaviour falls outside the realm of individual consent. The BPS appears to be claiming that an appeal to some nebulous, ideologically-driven concept of social decision-making exempts psychologists from the fundamental requirement to seek a person’s informed agreement before delivering an intervention. So according to the BPS – the formal guardians of ethical practice in the U.K. – the Covid communications strategy, aimed at achieving mass behavioural change, was intended to influence some anonymous collective rather than the actions of as many individuals as possible.
Again, the BPS stance is at odds with Professor Halpern’s position. In his 2019 book, Inside the Nudge Unit, he states: “If Governments… wish to use behavioural insights, they must seek and maintain the permission of the public. Ultimately, you – the public, the citizen – need to decide what the objectives, and limits, of nudging and empirical testing should be.” (p. 375)
Third, Dr. Paxton’s claim that the levels of fear throughout the Covid pandemic were proportionate to the viral threat is ill-informed and does not stand up to scrutiny. The minutes of the SPI-B meeting of March 22nd, 2020, demonstrate that its endorsement of a covert psychological strategy was a calculated decision to scare the British people, recommending that: “The perceived level of personal threat needs to be increased among those who are complacent… using hard-hitting emotional messaging.” In her book, A State of Fear, Laura Dodsworth interviewed members of SPI-B who confirmed that there had been a concerted effort to elevate the fear levels of the general public. One committee member, Educational Psychologist Dr. Gavin Morgan, admitted: “They went overboard with the scary message to get compliance.” Another SPI-B member – who wished to remain anonymous – was even more forthright: “The way we have used fear is dystopian… The use of fear has definitely been ethically questionable. It’s been like a weird experiment. Ultimately, it backfired because people became too scared.”
The mission to indiscriminately instil fear in the British public has been highly effective. An opinion poll prior to ‘Freedom Day’ suggested most people were worried about the prospect of lifting the remaining Covid restrictions. Even now, when all the vulnerable groups have been offered vaccination, many of our citizens remain tormented by ‘Covid Anxiety Syndrome’ – a disabling combination of fear and maladaptive coping strategies – with 20% of the population ‘markedly affected’. And this psychology-assisted fear inflation will be responsible for a substantial proportion of the extensive collateral damage associated with the restrictions, including excess non-Covid deaths and mental health problems.
Fourth, Dr. Paxton’s response makes no reference to the use of shame and scapegoating, and whether these are acceptable strategies for a civilised society to use. One can only assume that the BPS either views these tactics as acceptable, or that they seek to avoid acknowledging that psychologists have recommended practices that, in some respects, resemble the methods used by totalitarian regimes such as China, where the state inflicts pain on a subset of its population in an attempt to eliminate beliefs and behaviour they perceive to be deviant.
The dismissal of our ethical concerns by the BPS was predictable: a cursory glance at the scientists comprising the SPI-B shows that several of its members are also influential figures in the BPS; a major conflict of interest that renders the impartiality of their views highly questionable. What was surprising was the strident tone of Dr. Paxton’s rejoinder, as exemplified by his assertion that the psychologists’ role in the pandemic response demonstrated “social responsibility and the competent and responsible employment of psychological expertise”. I suspect the lady trembling on the pavement, the young man being verbally abused in the garage, and the neighbour donning mask and gloves to wheel out her dustbin – along with the many others in similar positions – might all beg to differ.
Dr. Gary Sidley is a retired NHS Consultant Clinical Psychologist.
Fury over Covid rules is FINALLY helping Aussies lose their long-held, unhealthy respect for authority
By Damian Wilson | RT | August 26, 2021
Having been forced to endure months of harsh lockdowns, my often-malleable compatriots Down Under are starting to fight back as they realise their government is clueless and they’ve been nuts to swallow the ‘zero Covid’ strategy.
By any measure, Australia has not enjoyed the coronavirus pandemic – and that has nothing to do with the number of deaths, because at less than 1,000 for a population of 25 million, it has, in the main, escaped lightly.
Where it has really suffered is in identifying exactly what level of threat Covid-19 poses to the population and then acting accordingly. Instead of being bold, brave, and positive in its handling of the situation, Australia has shown all the spine of a bluebottle jellyfish.
The collywobbles set in at the slightest whiff of Covid. Not deaths. Not hospitalisations. But simple cases of the virus send public health officials into a spin, locking down millions, deploying the military onto the streets, and imposing needless and draconian curfews. Blind panic best sums up the Australian government’s approach.
Then there are the stern warnings from state leaders that would be hilarious if they weren’t so serious – about enjoying sunset on the beach, removing a mask to drink beer, dodging errant footballs while watching a game, and most recently, a local council deciding to shoot 15 rescue dogs rather than allow volunteers from an animal shelter to travel for their collection in case they spread the virus.
That’s the level of insanity we’re looking at.
Meanwhile, it was humans on the receiving end at a so-called ‘freedom rally’ in Melbourne, where violence between protesters and police led to officers firing rounds of pepper balls – the most powerful non-lethal force at their disposal – into the anti-lockdown crowd.
It was one sign that patience with being treated like sheep might finally have snapped among parts of the Australian public. And it’s about time. I had begun to wonder what happened to the rebellious larrikins, the famed Aussie battlers, the brave Diggers, the pioneering ‘new Australians’ who just a generation or so ago left homes and family in Italy, Greece, Vietnam and beyond to pursue their dreams in the Lucky Country.
It seemed that a subservience to the ruling class, an unhealthy respect for authority, had overwhelmed my homeland.
The whole penal colony fable is a bit exaggerated, and of course there have been generations of intermingling since the 18th century, when Australia’s first white arrivals were drawn from the ranks of Great Britain’s sheep thieves and petty criminals. The violence and harsh conditions that welcomed those newcomers to the shores of Botany Bay, however, instilled a deep loathing and mistrust of their governing class, and it is often argued that Australia’s success was built on that resentment, driving its people to prove themselves to the authorities at home – and back in Mother England – that they could more than hold their own on the world stage. That inferiority complex was the driving force that has seen us excel in literature, in music, and particularly in sport.
But it also makes the Aussies a malleable bunch at times. Authority can make us go all weak at the knees. Public awareness campaigns that might struggle for lift-off elsewhere prove wildly successful in obedient Oz.
There’s no doubt this has been employed effectively in the past. There were the anti-litter ‘Keep Australia Beautiful’, keep-fit ‘Life. Be in it’, and skin cancer prevention ‘Slip! Slop! Slap!’ campaigns of my childhood. There was the mandatory wearing of bike helmets that came into force in the early 1990s, the plain packaging for cigarettes that appeared in 2012, and even the strict limits on gun ownership under the National Firearms Agreement that followed the Port Arthur massacre which left 35 people dead in 1996.
We have long been suckers for any message whose central premise is: follow this prescriptive guidance and you will be totally free to enjoy the great outdoors (without dying from cancer, obesity, bike accident or gunshot). That explains why the heavy-handed Covid rules have faced such little resistance.
The problem public health officials are facing now, however, is that the message is no longer working. Aussies were told the ‘zero Covid’ strategy that their government was pursuing was the envy of the world. That closing all international borders and keeping everyone at home was the pathway to freedom. Just do as we say and everything will be bonzer.
But they lied. With the Delta variant on the loose, lockdowns, curfews, restrictions on movement and the rest of the usual draconian measures are coming into play once more. But the government has overplayed its hand, and a sceptical public is starting to think, “These galahs haven’t got a bloody clue!” And they’re right.
So we see unrest on the streets of Brisbane, Sydney, Perth, and Melbourne because patience has finally snapped. I say let it rip! I look forward to continuing protests, rule-breaking, tough questions, and political accountability. I look forward to heads rolling, humiliating inquiries, and heartfelt apologies from the bungling clowns in charge.
I might have to wait a few months, but hey, that’s okay… because like my fellow compatriots, I’m not going anywhere.
Damian Wilson is a UK journalist, ex-Fleet Street editor, financial industry consultant and political communications special advisor in the UK and EU.
Silenced and smeared – the hounding of Dr Sam
By Sally Beck | TCW Defending Freedom | August 25, 2021
As I reported in TCW Defending Freedom here, Dr Sam White, a former partner in a Hampshire GPs’ practice, was suspended by NHS England after tweeting a resignation video in February explaining his concerns around Covid vaccination and what he felt about the government and NHS’s over-zealous response to the pandemic.
Now the independent Medical Practitioners Tribunal Service (MPTS) has ruled that there were no grounds for suspending Dr White – but he must still be gagged.
For the next 18 months, Dr White ‘must not use social media to put forward or share any views about the Covid-19 pandemic and its associated aspects’.
Dr White’s lawyers will appeal under Article 10 of the Human Rights Act 1998, which states that everyone has the right to freedom of expression, although the law may be subject to conditions or restrictions necessary in a democratic society. Surely doctors should never be silenced in a democratic society? Dr White said: ‘If I lose my ability to speak freely so will other doctors.
‘I have been forced to agree that I will erase the video and any other Covid criticism from my Twitter and Instagram accounts.
‘In the wake of the Jane Barton issue [Jane Barton was dubbed “Dr Opiate” after 650 patients in her care died after she prescribed powerful painkillers] the Royal College of General Practitioners commented that doctors should feel able to report promptly systemic failings and that is what I did. So to be punished for that is confusing to say the least.’
The RCGP guide for whistleblowers states: ‘When a professional working in the NHS is aware that care is threatened, sub-standard or dangerous for whatever reason, they have a duty to make these concerns known and for those in charge to assess and, if necessary, act.’
Last Tuesday (August 17) the MPTS, which is independent from medical personnel regulators the General Medical Council (GMC) who are investigating Dr White over alleged fitness to practise issues, said they had received 18 complaints connected with his social media output but did not name any complainants.
They are also relying on the evidence of the manager at his former practice who had not complained about him to bosses while he worked with her, only since she was contacted by NHS England. She is alleged to have stated that the practice had ‘significant concerns’ about Dr White, and that he had expressed ‘strange ideas’ and used inappropriate language whilst at work. Dr White strenuously denies the allegations.
Francis Hoar QC, who defended Dr White, told the tribunal: ‘The NHS and GMC had relied on hearsay with no signed statements being available, no validation of the identity of the complainants, no investigation as to whether his [Dr White’s] remarks were supported by science or clinical practice and no investigation by the NHS of the complaints he has made.’
In fact, Dr White, 41, talked through his concerns about the Covid response to a local GP during his annual appraisal and spoke again to a responsible officer acting on behalf of the GMC and NHS England during his five-year revalidation (relicensing) procedure, but received no meaningful response. He says he turned to social media as a last resort.
His main bones of contention were that the vaccination programme had been rolled out in breach of legal requirements in relation to free and informed consent. As we have reported, informed consent is not being taken seriously at vaccine hubs with people receiving details about potential serious adverse events only after receiving the jab. Dr White also voiced concerns about face masks. He felt elderly patients should not have to wear them and that he should not have to wear one in an NHS setting unless consulting with patients, which he did willingly.
Without investigating any of Dr White’s concerns, which included worries about inaccurate PCR tests that are being abandoned in America by the Centers for Disease Control in December; or vaccination harms, with reports to the Medical Healthcare products Regulatory Agency of 1,596 fatalities post vaccination up to August 11, the tribunal concluded that they had serious concerns about his conduct.
They said: ‘Dr White posted misinformation on social media platforms’, but did not go into detail.
A popular method of silencing doctors wanting to challenge the narrative is to question their mental health. In April, Swiss cardiologist Thomas Binder, 58, based in Baden, an open critic of coronavirus measures and treatment, was taken away from his practice by a SWAT team and locked in a psychiatric ward. He managed to fire off a tweet, minutes before his arrest and before his Twitter account was suspended for criticising the Swiss government, which said: ‘In front of my practice there is a SWAT team from Aargau. They are here to arrest me. Help!’
Dr White’s mental health has been questioned too by a senior NHS England clinical adviser. After a phone conversation with him she urged NHS England in June to ‘consider an emergency suspension given the suspicion that he was suffering from paranoid beliefs and mental ill health’. She concluded this without meeting Dr White and without any kind of formal mental health assessment. Dr White taped the conversation, and the tape reveals that at no time does she ask any direct question about his mental health, so it is hard to know how she came to that conclusion.
The tribunal ruled that Dr White should inform the GMC of any new job he takes so that his behaviour can be monitored, but the ruling will not prevent him from practising as an integrative doctor, a locum or as a GP in any NHS practice.
Dr White maintains: ‘Everything I have said or written is substantiated by peer-reviewed papers or by expert witness testimony, all of which has been discussed by professionals with the lawyer Dr Reiner Fuellmich at his International Corona Committee. [Weekly interviews with respected doctors, scientists, academics, journalists, concerned with the global pandemic response.]
‘I knew that there were problems with the way medicine had become protocol driven and not patient focused but had no idea of the scale.’
Dr White is crowdfunding to pay for his legal expenses.
July’s Age-Standardised Mortality Rate Was Equal to the Five-Year Average
By Noah Carl • The Daily Sceptic • August 24, 2021
The ONS announced on Monday that there were 40,467 deaths registered in England in July, which is 4.8% more than in June, and 7.6% more than the five-year average. In fact, the number of deaths registered in England was above the five-year average in all four weeks of last month.
These increases make sense, given that there has been a small uptick in COVID-19 deaths associated with the ‘Delta wave’. Although COVID-19 was only the ninth leading cause of death in July, deaths from the first eight causes were all below their five-year averages.
However, because the English population is ageing, the absolute number of people at risk of dying each year is going up. You’d therefore expect to see a greater number of deaths each year, even without a pandemic. What’s more, people who die from COVID-19 tend to be slightly older than those dying of other causes, so the average COVID-19 death is associated with fewer life-years lost.
For these reasons, it’s more informative to track age-adjusted measures of mortality. In July, the age-standardised mortality rate was only 1.3% higher than in May, and was approximately equal to the five-year average. (The exact figure was marginally higher, but the percentage difference was only 0.4%.)
This chart from the ONS shows the age-standardised mortality rate for the first seven months of the year, each year, going back to 2001:

Although 2021’s figure was higher than the figure for 2019, it was 3.6% lower than the figure for 2015 and 2.0% lower than the figure for 2018. This means that – despite higher-than-expected mortality in the winter – the overall level of mortality in the first seven months of 2021 was still lower than three years before.
As a matter of fact, the age-standardised rate from January through July was only 0.8% higher than the five-year average. Another month without many excess deaths and 2021 will officially be an ‘average year’ for English mortality.
FDA admits: Neither VAERS nor its many other pharmacovigilance systems are functional, nor will VAERS be in the future
By Dr. Meryl Nass, MD | August 24, 2021
FDA made an extraordinary admission in its letter to BioNTech yesterday, to justify failing to find safety “signals” better know as serious, common vaccine-induced injuries and deaths. So it asked the fox to please guard the henhouse instead. Pretty please Mr. Pfizer, would you look into myocarditis and other serious problems for us? We are not capable…
Guess FDA thought few would be able to parse its bureaucratize, discussed here and in the prior 5 posts. See page 6 of the document linked above:
“We have determined that an analysis of spontaneous postmarketing adverse events [VAERS reports] reported under section 505(k)(1) of the FDCA [Federal Food, Drug and Cosmetic Act] will not be sufficient to assess known serious risks of myocarditis and pericarditis and identify an unexpected serious risk of subclinical myocarditis.
Furthermore, the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA is not sufficient to assess these serious risks.”
Let’s parse this some more. VAERS, with about 13,000 deaths reported this year, and about 500,000 adverse events reported this year, is somehow unable to be analyzed to discover what it was established by Congress to discover: serious vaccine-induced adverse events. Reporting to VAERS since the vaccines became available is unprecedented. For example, about 8,000 cumulative deaths were reported to the system during its entire 30 year existence. Yet in 2021, over 12,000 deaths have reported following Covid vaccinations alone.
We already know from Israeli data, and US data presented to CDC’s advisory committee on June 23, that the rate of reported cases of myocarditis in vaccinated teenage boys aged 12-17 is at least 25 times greater than expected, and is 50 times greater than the reported rate in vaccinated males over 65.
But analysis of VAERS by CDC and FDA, who jointly manage it, cannot properly assess this risk? Even though Congress requires them to do so?
Equally as shocking, FDA can apparently see into the future, and any hopes that it will soon fix its analytic conundrum have been dashed. FDA can already state that VAERS analysis will not be sufficient to assess known myocarditis risks.
What about all the other databases that Steve Anderson, PhD, head of the Office of Biostatistics and Epidemiology, told us in October he would be using to evaluate vaccine safety? I posted screenshots showing databases encompassing over 300 million people that Anderson said FDA would access to evaluate the safety of Covid vaccines. After all, this system is required by Congress to function, and if it doesn’t, FDA is breaking the law:
“the pharmacovigilance system that FDA is required to maintain under section 505(k)(3) of the FDCA is not sufficient to assess these serious risks.”
So there you have it. FDA is required by law to properly use and maintain massive databases for the evaluation of vaccine safety. Yet it says neither is working. But no matter, FDA issued a license for the Comirnaty vaccine anyway yesterday.
Who Is ‘The Real Anthony Fauci’?
By Robert F. Kennedy, Jr. | Children’s Health Defense | August 25, 2021
 Today, Dr. Anthony Fauci is a household hero to half of America. Drug companies, government officials and the pharma-funded corporate media invoke his name to justify lockdowns, masks and experimental vaccines. The other half do not look on him favourably.
Today, Dr. Anthony Fauci is a household hero to half of America. Drug companies, government officials and the pharma-funded corporate media invoke his name to justify lockdowns, masks and experimental vaccines. The other half do not look on him favourably.
A recent editorial in a leading medical journal urged Congress to make it a felony to publicly criticize Dr. Fauci.
Encouraging his own deification, Dr. Fauci has declared that all those who questioned his pronouncements are “anti-science.”
But who is Dr. Fauci really?
In my new book, I show that Dr. Fauci has done little to earn the sobriquet “America’s Doctor.”
Instead, he has survived 50 years as the J. Edgar Hoover of public health by consistently prioritizing Big Pharma profits over the welfare of his countrymen, and through mercenary homage to the chemical and agricultural industry, the military industrial complex, the intelligence apparatus and all the other pushers of pills, potions, powders, poisons, pricks and the police state.
During more than a year of painstaking and meticulous research, I unearthed a shocking story that obliterates the obsequious media’s spin on Dr. Fauci … and that will alarm every American — Democrat or Republican — who cares about democracy, our Constitution and the future of our children’s health.
In my book I reveal how Fauci:
- has been the principal architect of “agency capture” — the subversion of democracy by a drug industry that manipulates regulators like sock puppets.
- failed dismally over his 50-year career with the National Institute for Allergy and Infectious Diseases (NIAID) to address the cause, to prevent or cure the exploding epidemics of allergies and chronic disease that Congress charged him with curtailing. The chronic disease pandemic is his enduring legacy. Those ailments now debilitate 54 percent of American children compared to 6 percent when he joined NIAD.
- repeatedly used fraud, bullying, intimidation, dissembling and falsified science to win approval for worthless and deadly drugs and vaccines.
- sabotaged safe and effective off-patent therapeutic treatments for AIDS while promoting deadly chemotherapy drugs that almost certainly caused more deaths than HIV.
- transformed NIAD from a public health regulator into an incubator for pharmaceutical drugs for which he and his trusted deputies often file patents and collect royalties. Dr. Fauci has claimed Moderna vaccine patent rights worth billions of dollars for NIAD and hand-picked at least four of his NIAD underlings to receive $150,000 annually from royalties.
- exercises dictatorial control over the army of “knowledge-and-innovation” leaders who appear nightly on TV to parrot his orthodoxies and “debunk” his opponents who run his crooked clinical trials globally and who populate the “independent” federal panels that approve and mandate drugs and vaccines — including the committees that allowed the Emergency Use Authorization of COVID-19 vaccines.
- violated federal law to allow his pharma partners to sacrifice and kill hundreds of impoverished and dark-skinned children and orphans in the U.S and Africa as lab rats in deadly experiments with toxic AIDS and cancer chemotherapies.
- repeatedly concocted and weaponized fraudulent pandemics, including bird flu (2005), swine flu (2009) and Zika (2015-2016), in order to sell novel vaccines.
- partnered with the Pentagon and intelligence agencies to conduct “gain-of-function” experiments to breed pandemic superbugs in poorly regulated labs in Wuhan, China and elsewhere, under conditions that virtually guaranteed the escape of weaponized microbes like SARS-CoV-2.
That’s just the short list.
Dr. Fauci and his band of pharma and Silicon Valley profiteers — working with corrupted politicians, captured federal agencies and the bought and brain-dead mainstream media — have used the COVID pandemic to mint billions from vaccines and other profitable medicines.
His disastrous mismanagement ran up one of the biggest COVID death counts among all nations.
Dr. Fauci has led the crusade to suppress functional remedies like Ivermectin and hydroxychloroquine which could have avoided 80 percent of the deaths and hospitalizations from COVID and ended the pandemic overnight.
We need to stop Dr. Fauci and the coup d’état against the Constitution, human rights and liberal democracy globally.
Because this book threatens their trillion-dollar vaccine enterprise, Dr. Fauci and his allies in the medical cartel, the media and military will hurl fierce criticism and use censorship — to debunk and silence “The Real Anthony Fauci.”
With your help, this book can play a transformational role in exposing Dr. Fauci as a charlatan and quack and in showing the world that Dr. Fauci, far from being a healer, is one the most noteworthy mass murderers in human history.
It is my hope that this book will motivate — and mobilize — millions more advocates for truth, health and democracy.
“The Real Anthony Fauci” publication date is Nov. 9. By pre-ordering your copy today, you’ll help push the book to bestseller status, diminishing the powers of the censors to silence me. Thank you.
The Face Mask Folly in Retrospect
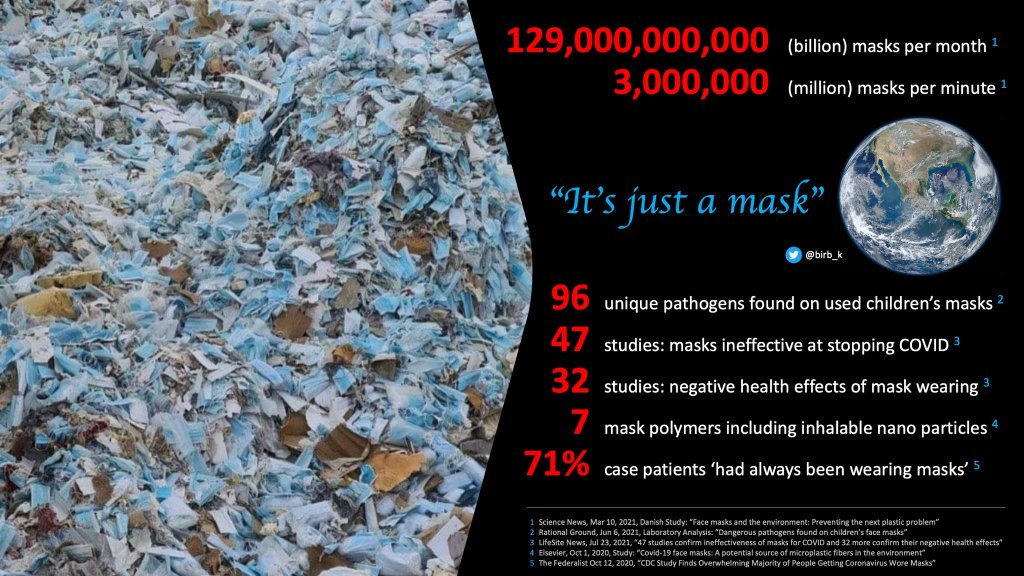
“It’s just a mask”: Global impact of the face mask folly (K. Birb)
Swiss Policy Research | August 22, 2021
It has been known for decades that face masks don’t work against respiratory virus epidemics. Why has much of the world nonetheless fallen for the face mask folly? Ten reasons.
1) The droplet model
Many ‘health authorities’ have relied on the obsolete ‘droplet model’ of virus transmission. If this model were correct, face masks would indeed work. But in reality, respiratory droplets – which by definition cannot be inhaled – play almost no role in virus transmission. Instead, respiratory viruses are transmitted via much smaller aerosols, as well as, possibly, some object surfaces. Face masks don’t work against either of these transmission routes.
2) The Asian paradox
During the first year of the pandemic, several East Asian countries had a very low coronavirus infection rate, and many ‘health experts’ falsely assumed that this was due to face masks. In reality, it was due to very rapid border controls in some countries neighboring China as well as a combination of metabolic and immunologic factors reducing transmission rates. Nevertheless, many East Asian countries eventually got overwhelmed by the coronavirus, too (see charts below).
3) The Czech mirage
In the spring of 2020, the Czech Republic was one of the first European countries that introduced face masks. Because the Czech infection rate initially stayed low, many ‘health experts’ falsely concluded that this was due to the masks. In reality, most of Eastern Europe simply missed the first wave of the epidemic. A few months later, the Czech Republic had the highest infection rate in the world, but by then, much of the world had already introduced face mask mandates.
4) Fake science
For decades, studies have shown that face masks don’t work against respiratory virus epidemics. But with the onset of the coronavirus pandemic and increasing political pressure (see below), suddenly studies appeared claiming the opposite. In reality, these studies were a mixture of confounded observational data, unrealistic modelling and lab results, and outright fraud. The most influential fraudulent study certainly was the WHO-commissioned meta-study published in The Lancet.
5) Asymptomatic transmission
Another factor contributing to the implementation of mask mandates was the notion of ‘asymptomatic transmission’. The idea was that everybody should be wearing a mask because even people without symptoms might spread the virus. The importance of asymptomatic and pre-symptomatic transmission is still a matter of debate – up to half of all transmission might occur prior to symptom onset –, but either way, face masks simply don’t work against aerosol transmission.
6) Political pressure
Several political factors contributed to the implementation of mask mandates. First, some politicians simply wanted to “do something” against the pandemic; second, some politicians thought face masks might have a “psychological effect” and might “remind” citizens to stay cautious (if anything, it had the opposite effect: creating a ‘false sense of security’); third, some politicians used mask mandates to enforce compliance and pressure the population into accepting mass vaccination.
In addition, there was a vicious circle involving science and politics: politicians claimed to “follow the science”, but scientists followed politics. For instance, the WHO famously admitted that their updated mask guidelines were in response to “political lobbying”, not new evidence. The most influential lobby group was “masks4all”, founded by a “Young Leader” of the World Economic Forum (WEF).
7) The media
Perhaps unsurprisingly, most of the ‘mass media’ amplified the fraudulent science and the political pressure driving mask mandates. Only some independent media outlets and some truly independent experts questioned the validity of the underlying evidence. However, their voices got suppressed as dubious “fact checking” organizations eagerly enforced official guidelines and throttled or censored many articles and videos critical of face masks.
8) “Surgeons wear masks”
Surgeons wear masks, so they must be effective, right? This was another notion contributing to the face mask misunderstanding. In reality, surgeons wear masks not against viruses, but against much larger bacteria, but more importantly, studies have long shown that even surgeons’ masks make no difference in terms of bacterial wound infections.
9) Misleading memes
To convince low-IQ social media users of the effectiveness of face masks, several unscientific memes were created. The most notorious one probably was the “peeing into your pants” meme, shared by many ‘health experts’ (really). Many of these memes exploited the fact that most people simply don’t realize how small and ubiquitous viral aerosols really are.
10) Doubling down
After mask mandates had been implemented globally and hundreds of billions of dollars had been spent on masks, it soon became obvious – once more – that masks simply don’t work against respiratory virus epidemics (see charts below). But at that point, neither politicians, nor ‘health experts’, nor duped citizens who had to wear them for months wanted to admit this anymore.
Instead, some ‘health authorities’ doubled down and enforced outdoor masking (even on beaches), double-masking, or N95/FFP2 masking, to no avail. The one novel scientific insight produced during the coronavirus pandemic was that even N95/FFP2 mask mandates have made no difference at all.
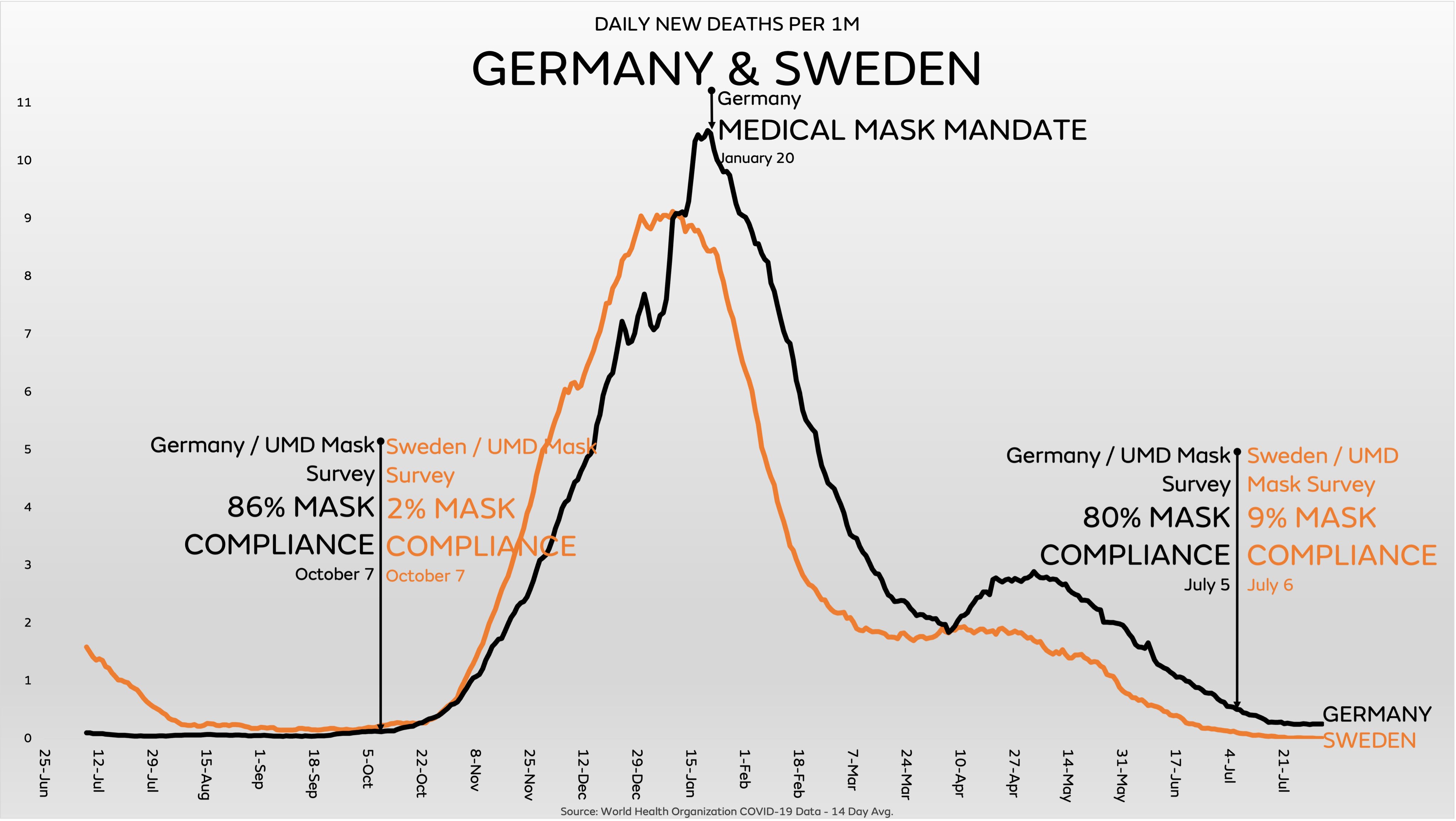
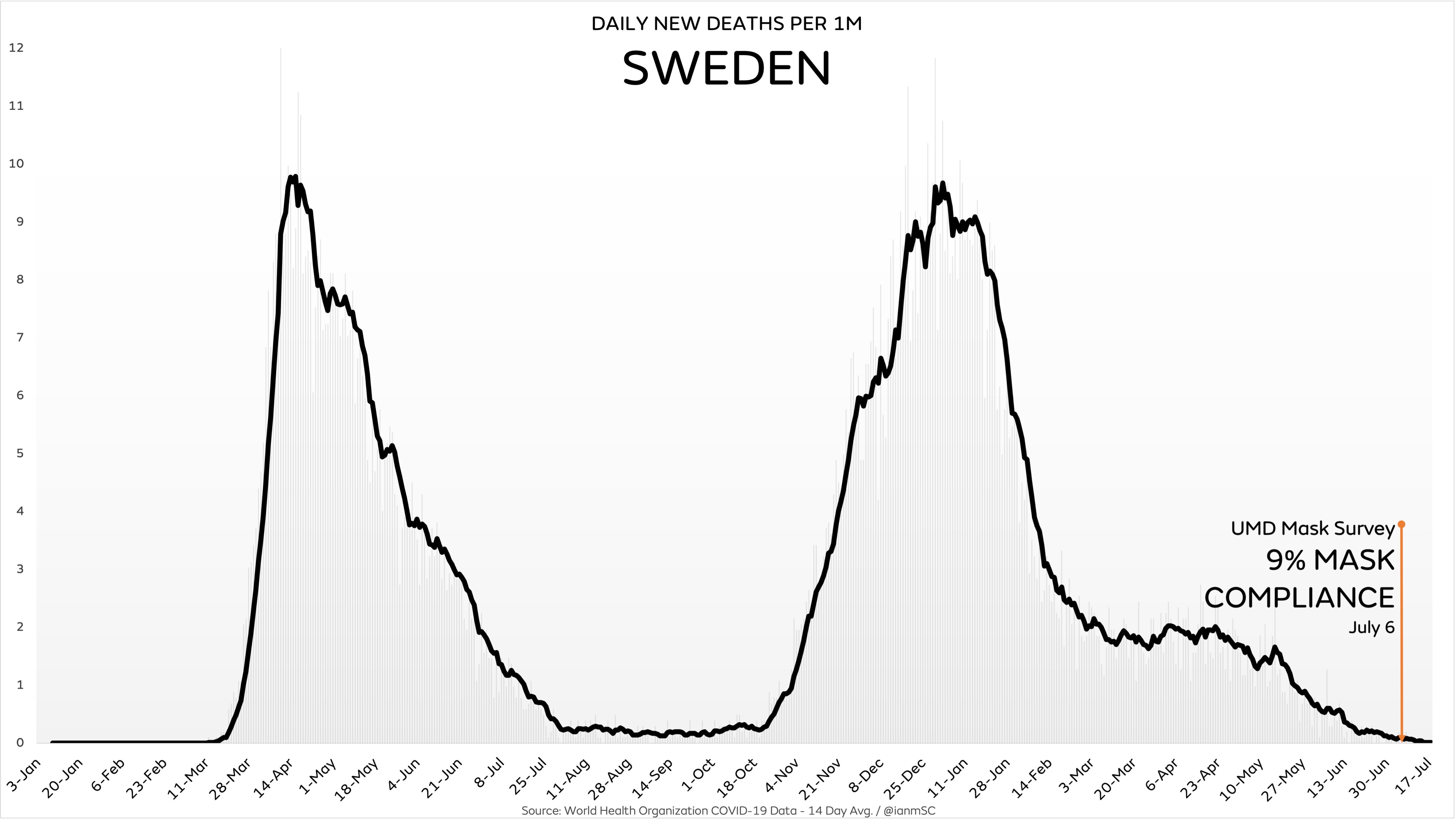
Sweden: The exception that proved the rule
Only very few countries in the world have resisted the face mask folly. The most famous example certainly is Sweden (see charts below), which has also resisted the lockdown experiment. Naturally, Swedish coronavirus mortality has remained below the European average. But the many vicious attacks against Sweden by much of the international media showed just how difficult it has been to escape the global madness and follow the real science during this bizarre pandemic.

A child wearing a mask at school (more)
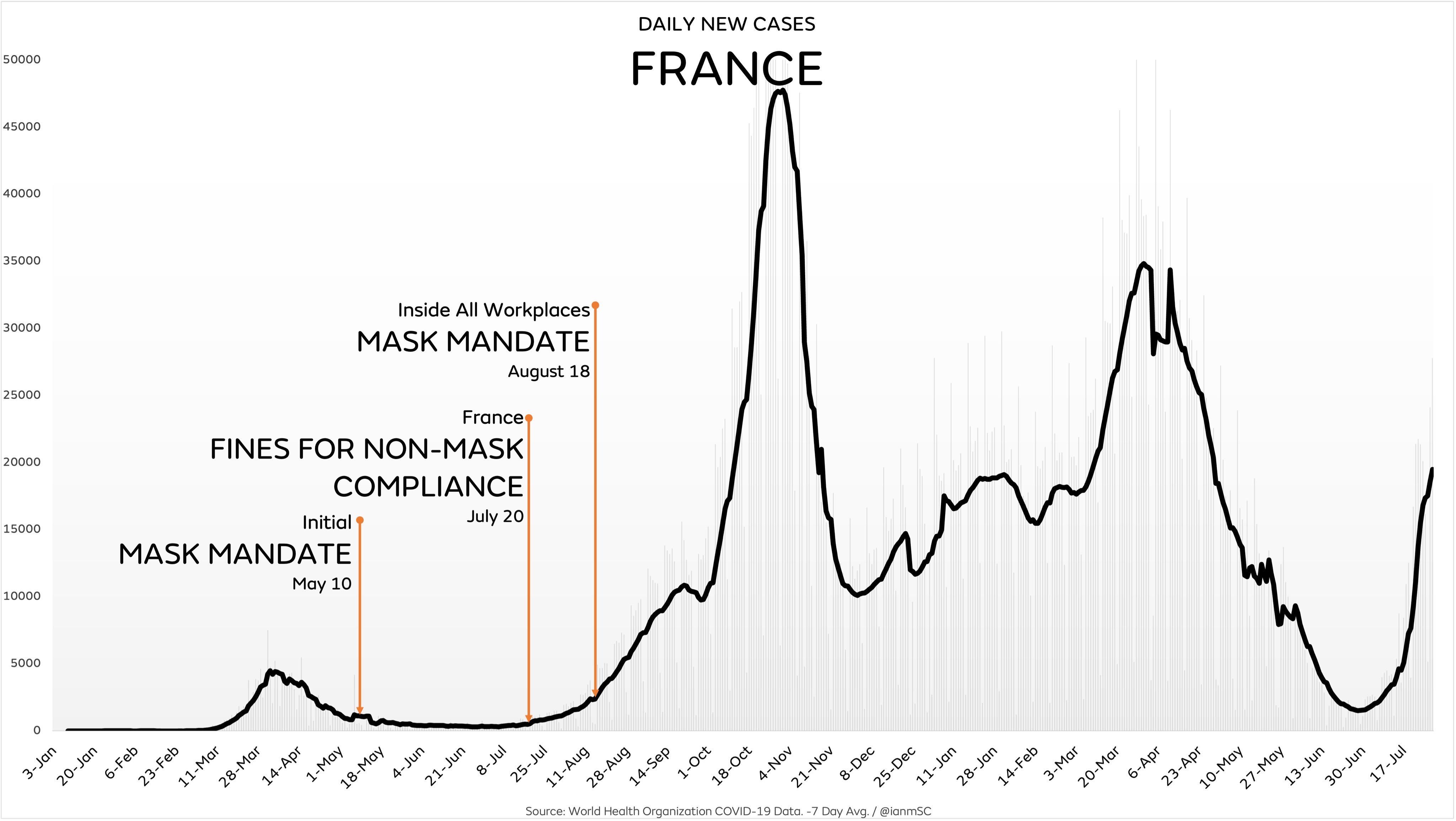
How face masks and lockdowns failed
The following charts show that infections have been driven primarily by seasonal and endemic factors, whereas mask mandates and lockdowns have had no discernible impact (charts: IanMSC).







Comments in response to FDA’s license of Pfizer vax today for 16 years and up
By Meryl Nass, MD | August 23, 2021
The vaccine-induced protection provided by Covid vaccines starts fading within months. In late July, Israel’s Minister of Health said vaccine protection had dropped to 39%. It is not preventing severe illness in Israel and the UK either, though the US CDC changed its collecting methods for breakthrough cases on May 1 to disguise this fact.
While the US government has said it will begin booster doses of mRNA vaccines the week of September 20, there is actually NO evidence that Covid-19 boosters will provide increased protection against infection, or that they are effective against the delta variant or other new variants.
For other vaccines, such as mumps and pertussis, there is no evidence that booster doses after the initial course add measurable protection.
Boosters do raise antibody levels, briefly, which increases the risk of autoimmune adverse effects, immune overactivity and the dire possibility of antibody-enhanced disease (AED), a.k.a. vaccine-enhanced disease (VED), in which those who are vaccinated have a much more severe illness when exposed to Covid than do the unvaccinated.
Since the UK’s top vaccine expert Sir Andrew Pollard told Parliament 2 weeks ago that herd immunity cannot be obtained—in fact it is a “myth”– because the vaccine is not halting transmission, and since the CDC director confirmed this, there is no logical reason to mandate vaccinations for anyone, since the vaccines are not protecting the community.
Mandating vaccinations for the young and healthy, who are at minimal risk from Covid, but at increased risk from Covid vaccinations, is a travesty. The risk of myocarditis after vaccination in a male teenager is 50 times higher than the risk to a 65 year old, according to CDC data. The teenager has many years ahead of him, while the long-term side effects from Covid vaccines have yet to be identified.
Reported deaths following Covid vaccinations are at least 10 times higher than for any vaccine ever approved in the US. Yet FDA and CDC have never explained the causes of these deaths, and they pretend they do not exist.
This fact alone should have been sufficient to stop FDA granting a license to the Pfizer vaccine.
Here is the convoluted license-plus-authorization letter from FDA. This could be a bait and switch–see the next post.
Featured Video
House Resolution Calls for Tech Companies to Censor Speech
or go to
Aletho News Archives – Video-Images
Book Review
Alarmist climate science as a textbook example of groupthink
By Paul MacRae | May 1, 2012
… Groupthink was extensively studied by Yale psychologist Irving L. Janis and described in his 1982 book Groupthink: Psychological Studies of Policy Decisions and Fiascoes.
Janis was curious about how teams of highly intelligent and motivated people—the “best and the brightest” as David Halberstam called them in his 1972 book of the same name—could have come up with political policy disasters like the Vietnam War, Watergate, Pearl Harbor and the Bay of Pigs. Similarly, in 2008 and 2009, we saw the best and brightest in the world’s financial sphere crash thanks to some incredibly stupid decisions, such as allowing sub-prime mortgages to people on the verge of bankruptcy.
In other words, Janis studied why and how groups of highly intelligent professional bureaucrats and, yes, even scientists, screw up, sometimes disastrously and almost always unnecessarily. The reason, Janis believed, was “groupthink.” He quotes Nietzsche’s observation that “madness is the exception in individuals but the rule in groups,” and notes that groupthink occurs when “subtle constraints … prevent a [group] member from fully exercising his critical powers and from openly expressing doubts when most others in the group appear to have reached a consensus.”[2]
Janis found that even if the group leader expresses an openness to new ideas, group members value consensus more than critical thinking; groups are thus led astray by excessive “concurrence-seeking behavior.”[3] Therefore, Janis wrote, groupthink is “a model of thinking that people engage in when they are deeply involved in a cohesive in-group, when the members’ strivings for unanimity override their motivation to realistically appraise alternative courses of action.”[4]
The groupthink syndrome
The result is what Janis calls “the groupthink syndrome.” This consists of three main categories of symptoms:
1. Overestimate of the group’s power and morality, including “an unquestioned belief in the group’s inherent morality, inclining the members to ignore the ethical or moral consequences of their actions.” [emphasis added]
2. Closed-mindedness, including a refusal to consider alternative explanations and stereotyped negative views of those who aren’t part of the group’s consensus. The group takes on a “win-lose fighting stance” toward alternative views.[5]
3. Pressure toward uniformity, including “a shared illusion of unanimity concerning judgments conforming to the majority view”; “direct pressure on any member who expresses strong arguments against any of the group’s stereotypes”; and “the emergence of self-appointed mind-guards … who protect the group from adverse information that might shatter their shared complacency about the effectiveness and morality of their decisions.”[6]
It’s obvious that alarmist climate science—as explicitly and extensively revealed in the Climatic Research Unit’s “Climategate” emails—shares all of these defects of groupthink, including a huge emphasis on maintaining consensus, a sense that because they are saving the world, alarmist climate scientists are beyond the normal moral constraints of scientific honesty (“overestimation of the group’s power and morality”), and vilification of those (“deniers”) who don’t share the consensus. … Read full article
Blog Roll
 Aletho News
Aletho News- Iran unveils new control measures over Strait of Hormuz transit
- House Resolution Calls for Tech Companies to Censor Speech
- Ceasefire no longer viable after 200 days of Israeli violations: Hamas
- Israeli strikes intensify across southern Lebanon, casualties reported
- Left in Disbelief: Israel in Panic over Hezbollah FPV Drone Nightmare
- Trump Taps Israel Lobbyist From Mossad Cutout FDD To Join Iran Negotiations
- Trump’s Blockade Snatches Defeat from the Jaws of Victory
- Geopolitics and Geoeconomics of the Strait of Hormuz
- Mali: a new front in the Western war on multipolarism
- CHD Scientist: CDC, FDA COVID Vaccine Safety Monitoring ‘Insulting, and Many People Are Injured’
- If Americans Knew
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- Israel’s top Jewish religious body ‘refuses to condemn’ smashing of Jesus statue
- No Tricks Zone
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
