FDA’s last word on the safety of hydroxychloroquine and chloroquine was issued last year/ FDA
By Meryl Nass, MD | May 16, 2021
FDA managed to find 385 adverse event reports for either HCQ or CQ in its FDA adverse event reporting system database, as justification for withdrawing its EUA for the chloroquine drugs.
But there wa something strange about these reports. Only 102 of the 385 reports, or 26%, came from the United States. Why would foreigners be submitting reports of adverse events associated with a chloroquine drug to the FDA, instead of to their own pharmacovigilance system?
According to FDA, “FAERS is a database that contains information on adverse event and medication error reports submitted to FDA.” It is not an international database.
Might FDA have requested that foreign entities submit reports? Might some of those foreign entities have been sites where the HCQ overdose trials were conducted? The big three multicenter overdose trials were Recovery, Solidarity and REMAP-Covid. Page 8 of the FDA report does indicate that some of those patients, for whom adverse event reports were filed, had received excessive HCQ doses. Of a total of 256 reports for which FDA had dosing data, depending where you place the excessive dose cut-off, between 23 and 95 had received high doses.
FDA did a number of different things to suppress the use of hydroxychloroquine. This just happens to be one thing I had not previously reported on.
What else is interesting is that this report was compiled in May 2020. It is attached to a website dated July 2020, ten months ago.
In the intervening 10 months, well over 100 papers have been published on HCQ’s use in Covid. FDA claims, “The FDA’s job is to carefully evaluate the scientific data on a drug to be sure that it is both safe and effective for a particular use…” Yet FDA has ignored this massive amount of accumulating literature on hydroxychloroquine, during which 400,000 Americans died of/with Covid. Why? Willful misconduct?
THE NEW ABNORMAL AND THE CONFLICTED MIND OF JOE NORMIE
Computing Forever | May 13, 2021
Reality Bites Sort Of… | Thomas Sheridan | https://www.youtube.com/watch?v=qFUsPz2b3jo
Watch: Reality Bites Sort Of… | Thomas Sheridan | https://www.youtube.com/watch?v=qFUsPz2b3jo
Support my work here: https://computingforever.com/donate/
Support my work on Subscribe Star: https://www.subscribestar.com/dave-cullen
Follow me on Bitchute: https://www.bitchute.com/channel/hybM74uIHJKf/
Buy How is This a Thing Mugs here: https://teespring.com/stores/computing-forever-store
http://www.computingforever.com
KEEP UP ON SOCIAL MEDIA:
Gab: https://gab.ai/DaveCullen
Subscribe on Gab TV: https://tv.gab.com/channel/DaveCullen
Minds.com: https://www.minds.com/davecullen
Subscribe on Odysee: https://odysee.com/@ComputingForever
EPA Updates Its “Climate Change Indicators”
By Francis Menton | Manhattan Contrarian | May 13, 2021
It appears that some time last month the EPA provided a major update of what it calls its “climate change indicators.” The EPA’s web page for this is headed “Climate Change Indicators in the United States,” with the sub-heading “Climate Change Is Happening Now.” The update is an initiative of the Biden administration, now eager to invest a few trillion dollars of your money in new “green” infrastructure, after several years in which the Trump EPA paid no attention to keeping these data up to date. The New York Times reports on the big update on today’s front page, under the headline “Climate Change Is getting Worse, E.P.A. Says. Just Look Around.”
The basic technique here is to propagandize you with every sort of essentially irrelevant anecdotal information, while diverting your attention away from the only indicator of “climate change” that actually counts, which is temperature. After all, if temperatures aren’t going up, it isn’t “global warming.” Here, we have some 54 supposed climate “indicators” — everything from rain to drought to ice to sea level — out of which the things relating to actual temperature are only a handful, and then are buried deep in the midst of all the others, probably in the hope that you will miss them. And moreover, the temperature data are then grossly misrepresented in what has to be an intentional effort at deception.
But let’s start with the official line from the new Biden EPA.
The Earth’s climate is changing. Temperatures are rising, snow and rainfall patterns are shifting, and more extreme climate events – like heavy rainstorms and record high temperatures – are already happening. Many of these observed changes are linked to the rising levels of carbon dioxide and other greenhouse gases in our atmosphere, caused by human activities.
The Times then picks up on the theme by its headline calling for you to “just look around” to determine that “climate change” is happening. The idea is that you can determine that there is “climate change” by observing ice on ponds, or something, without having to bother with those complicated thermometers, let alone sophisticated satellite measurements:
Wildfires are bigger, and starting earlier in the year. Heat waves are more frequent. Seas are warmer, and flooding is more common. The air is getting hotter. Even ragweed pollen season is beginning sooner. . . . [EPA’s indicators] map everything from Lyme disease, which is growing more prevalent in some states as a warming climate expands the regions where deer ticks can survive, to the growing drought in the Southwest that threatens the availability of drinking water, increases the likelihood of wildfires but also reduces the ability to generate electricity from hydropower.
So how about the temperature guys? As you can see, the Times does throw in a couple of references to “heat waves” and “hotter air” in the midst of all the stuff about flooding, ragweed pollen, ticks, and whatever else. What’s missing is any citation or link to any source to support the assertion about actual temperatures. But over at the EPA page, under the heading “U.S. and Global Temperature,” we find the following graph, which is said to have been updated to April 2021:
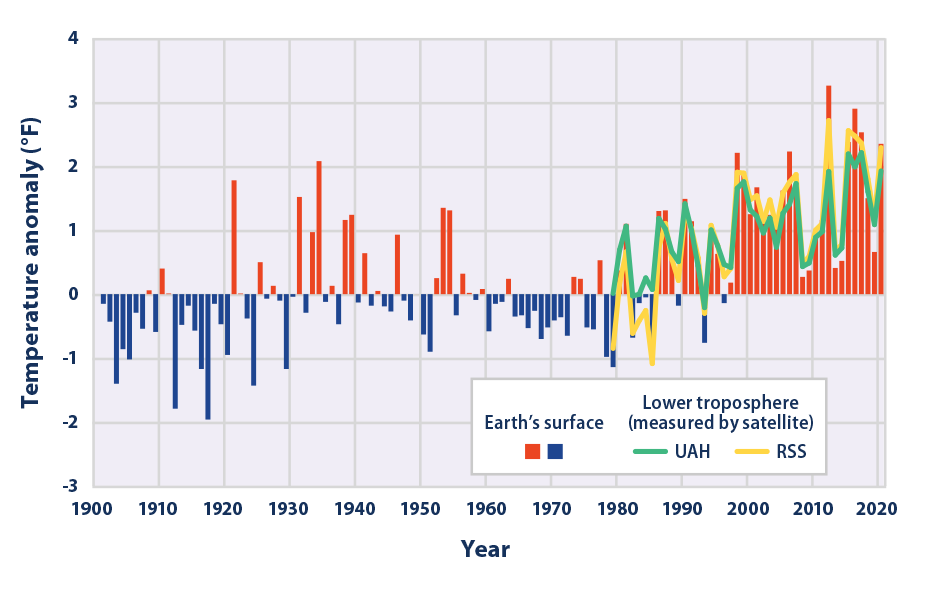
That appears rather scary! Everything looks like it is going up sharply with passing time. Check out especially the green line, which is identified as the “lower troposphere [temperatures] (measured by satellite) of UAH.” The green line ends with a steep uptick, leaving it with the latest data point just below a record reached in 2016, and a full 2 deg F above the 1901-2000 average.
Oh, but here is the actual lower troposphere temperature record from UAH, available at the website of Roy Spencer, who is the guy who compiles the UAH record:
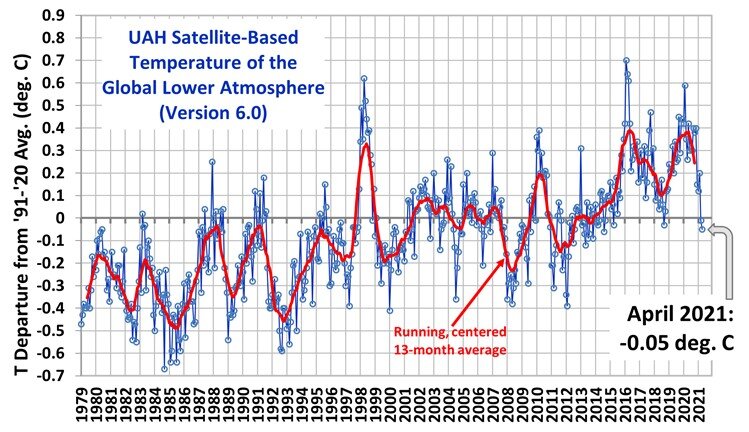
There are a few differences in the presentation that require a little interpretation, like the EPA graph is in deg F and has anomalies from a 1901-2000 mean, while the UAH graph is in deg C and shows anomalies from a 1991-2020 mean. But still, it leaps out that the green line on EPA’s web page, said to be the UAH record, ends with a sharp uptick and with the last point a full 2 deg F above the mean line; while this record, from UAH itself, ends with a sharp downtick and the last point actually below the mean line. Although EPA explicitly says on its web page that it updated the information in April 2021, this downtick in the UAH record began in January 2020 — a year and 4 plus months ago — and reflects a decline in lower troposphere temperatures of some 0.65 deg C, which is almost 1.2 deg F.
In other words, well more than half of the seemingly scary increase in temperature since 1901 shown in the EPA graph has just gone away in the last 16 months. So the Biden EPA, not wanting to complicate the official story of “climate change is happening now,” simply truncated the data in its graph at January 2020 to shut out the last year plus of big temperature declines. There is no way to characterize the EPA graph as other than intentionally deceptive.
I guess it’s OK because it’s in the noble cause of convincing the American people to allow the government to spend a few trillion dollars on windmills and electric car charging stations for the rich.
Government insider says UK Gov. plans to continue Lockdown and the Mainstream Media are in on it
THE DAILY EXPOSE • MAY 15, 2021
A Whitehall source directly linked to the Covid Response has said that the UK Government have already structured a detailed plan designed to neutralise each stage of lockdown easing, including the compliance of media outlets to help spread fear.
The Whitehall source has said that he has been “increasingly concerned” with how the Government are behaving, and that their “relationship with the truth” is now not even on nodding terms. The latest plan will involve a series of ‘crisis’ around drug supply; mutant strains; and third waves, specifically choreographed to condition the public for further lockdowns and vaccine passports.
The plan, that according to the source is designed to take us to September 27th 2021 is to be released in stages over the summer months and, according to the Whitehall source, is already ‘well underway’.
On March the 8th, the first milestone of the roadmap was implemented, with school children finally returning to class. The following day Chris Whitty gave a pre-written speech to the Commons that said schools reopening would cause another surge in the virus and ended it with “Let me be clear, many, many more people will die before this is over” the soundbite obligingly repeated on every news outlet, with BBC news having it on-loop all day.
On March the 29th, the second milestone of the roadmap was implemented. The Government said – “The evidence shows that it is safer for people to meet outdoors rather than indoors,”. This is why from the 29th March, when most schools start to break up for the Easter holidays, outdoor gatherings (including in private gardens) of either 6 people (the Rule of 6) or 2 households will also be allowed, making it easier for friends and families to meet outside.
The next day (March 30th) the AstraZeneca Vaccine was again stopped due to blood clots fears, despite the medicine’s regulator clearing it only the previous week. Whilst Boris Johnson repeated what he’d said the previous week that the mutated virus on the continent would inevitably “wash up on our shores”.
On April 19th, the third milestone saw pub gardens, and non-essential shops reopen. Followed immediately by news of a second vaccine being halted for fear it was causing blood clots and the discovery of the South African mutation said to be able to avoid them anyway.
The next milestone is due on May 17th with the Government relaxing social contact rules further and the opening of indoor venues. This will be followed by a story that the mutation is ‘more deadly than first thought’ and that young people are now also vulnerable to it, accompanied by the result of the vaccine passport trials have shown that they have a ‘positive effect on virus reduction’.
The final milestone is due on June 21st where ALL restrictions were promised to be lifted. This will not be allowed to happen. Vaccine passports / Track and Trace will be mandatory, as will masks and social distancing. The entire week of the 21st will be taken up by a third wave, which will suddenly be ‘rampant’, and this will be attributed to a new variant which they will declare is more deadly than the previous strains of Covid allegedly doing the rounds. This will be accompanied with yet more issues with vaccine supplies. Authorities will declare that one of the vaccines is effective against the deadlier strain, but a ‘problem’ with its manufacture will emerge.
The Whitehall source went on to say –
“All the measures are aimed at two things, vaccine passports and lockdowns starting next winter,
“The ultimate goal is to have the public, back in their box.
“Note that Boris is now talking down vaccine’s and bigging-up lockdowns, that wasn’t a mistake, that was all part of the plan”.
The plan also includes an ad campaign like the one seen at Christmas, the message this time will be that the pandemic isn’t over and vaccine passports are the ‘solution’.
Seeing Through the COVID-19 Spin

By Barbara Loe Fisher | The National Vaccine Information Center | April 26, 2021
Seeing through the COVID-19 spin is a challenge even for those who have been writing and talking for years about the need to limit Big Pharma’s influence on health policy and law. Perhaps the greatest change I have seen in vaccine regulation, policymaking and law over the past four decades has been the development of public-private business partnerships between Big Pharma and the government.1 2 3 4 5 That seismic change has affected how new vaccines are developed, licensed and regulated and is influencing what we see happening today.6 7
Since the coronavirus pandemic was declared by government officials in early 2020, lawmakers have been persuaded to build the entire global pandemic response around a single experimental biological product.8 9 10 That single product is generating billions of dollars in profits for liability free drug companies and their partners.11 12 The COVID-19 spin is reaching dizzying new heights every day,13 14 with fundamental facts about the experimental product’s risks and failures getting lost in the hard sell.
At dinner time, if you turn on any major television network in the U.S., you will see that the evening news has turned into one long COVID vaccine commercial infused with a heavy dose of fear mongering. Before the pandemic declaration, we had learned to ignore prescription drug advertising in-between getting news of the day. Now newscasters and TV docs are Pharma’s new COVID “vaccine” sales reps and the only way to get away from the 24/7 sales pitch is to turn off the TV.
Billions of Dollars Paid to TV Networks for DTC Pharma Ads
We should not be surprised. The U.S. and New Zealand are the only two countries in the world that allow direct to consumer pharmaceutical product advertising.15 16 17 In this country. Big Pharma pays US television networks five billion dollars per year to push use of drugs and vaccines.18
Taking a page out of Big Tobacco’s old book and upping the ante, Big Pharma has become a business partner of government.19 The COVID business deal is perhaps the single biggest one in the history of public health programs.20 21 22
Already wealthy drug companies were given at least nine billion dollars from the. government to develop experimental COVID vaccines in record breaking time,23 shaving five to 10 years off the normal vaccine development, testing and licensing process.24 25 But that wasn’t enough. Congress also handed companies a liability shield from lawsuits whenever the product government paid them to produce fails to work as advertised or a person is hurt by using it.26
If you or a loved one dies or is permanently injured by an experimental or soon-to-be FDA licensed COVID vaccine, you cannot sue the drug company who made it, even if there is evidence the company could have made it less reactive or more effective.
Big Pharma Pays Big Tech Billions of Dollars for Ads, Censorship Campaigns
If you are searching for relief from the hype by turning off the TV and turning on your computer, you will be disappointed. The COVID vaccine ad campaign is in high gear online, especially on social media platforms. The Thought Police hired by Big Tech to censor information that does not conform with pre-approved pandemic narratives are making sure you do not have an opportunity to carefully weigh the vaccine’s benefits and risks.27 28 29
Rational thinking on the World Wide Web is no longer tolerated and neither is freedom of speech. The Internet has become a drug company stockholder’s dream and a consumer’s worst nightmare.
Big Pharma and its business partners have paid a lot of money to Big Tech to eliminate freedom of thought and speech online. Right now the weapon of choice is a social media censorship campaign to de-platform dissenters, including reputable charitable organizations like the National Vaccine Information Center publishing well referenced information.30 31 32 The Internet Thought Police are especially upset when anyone talks about reports of serious vaccine complications and deaths, but reports about COVID-19 disease complications and deaths are allowed without restrictions.33
As COVID social distancing regulations have kept more people at home and on their electronic devices, the healthcare and pharma industry has poured more money into direct to consumer digital ads.34 In 2020, drug and vaccine manufacturers funneled about 10 billion dollars into digital advertising that we view on our computers, tablets and cell phones.35 36
How much of Big Tech’s decision to ghost dissenters from search engine results and de-platform social media accounts is influenced by an infusion of direct to consumer advertising dollars from Big Pharma?37
American Taxpayer Pays for COVID-19 Vaccine Ads
This year, the American taxpayer is also paying for TV and digital advertising to promote the use of the COVID-19 vaccine.38 On April 1, 2021, the government announced a three billion dollar COVID vaccine ad campaign39 to get make sure that every American gets vaccinated, a national ad campaign that is using community and religious leaders, as well as celebrities,40 41 to reach into every community to boost vaccine uptake in stores,42 sports arenas,43 schools44 and churches.45
Right now, Pfizer and Moderna, the two U.S. corporations manufacturing experimental messenger RNA (mRNA) COVID-19 vaccines are leading beneficiaries of the free advertising paid for by tax dollars. The first to secure an Emergency Use Authorization (EUA) from the FDA, Moderna counts the federal National Institutes for Health as a business partner,46 while Pfizer partnered with the German company BioNTech.47 Together, Moderna and Pfizer have captured market share and, by the end of 2020, Pfizer had achieved a 180 percent increase in revenue48 49 and Moderna had scored an eye watering 3,900 percent increase. 50 51
So what has the COVID vaccine advertising blitz done so far, other than convincing half of all adults to get at least one dose of the vaccine by mid-April 2021?52
The most notable achievement of the COVID vaccine campaign has been to keep everyone in a constant state of fear and confusion about what is true and what is false.53 There are so many misunderstandings and false impressions out there about the biological product manufactured by Moderna and Pfizer, a product that most people call a vaccine and other call a therapeutic drug but I call a cell disrupter biological.
No Long Term Safety Studies of Experimental mRNA Vaccines
Whatever you want to call it, the experimental mRNA technology that Moderna and Pfizer employed to create the product has not yet been licensed by the FDA to prevent infections in humans. 54 It is a genetic engineering technology that radically departs from the production methods used for two centuries to make live attenuated and inactivated viral and bacterial vaccines.55 It is an experimental technology that injects synthetic RNA directly into cells and, in effect, attempts to turn the human body into a vaccine manufacturing machine.56 57
There are no long-term studies58 evaluating the range of effects at the cellular and molecular level on the biological and genetic integrity of humans who receive the product. Nobody knows if it will, over time, negatively affect normal immune function and cause autoimmune and other chronic inflammatory conditions in the body,59 60 61 or provoke enhanced disease in vaccinated persons encountering mutated versions of the coronavirus in the future.62
Myth: Pfizer and Moderna mRNA Vaccines Have Been Proven to Prevent Infection and Transmission of SARS-CoV-2
What are the two biggest myths that have been generated by the advertising campaign being conducted with Pharma and taxpayer dollars?
The first big myth is that if you get two doses of the mRNA COVID vaccine, you will get artificial immunity and cannot be asymptomatically or symptomatically infected with the SARS-CoV-2 virus and you will not be able to infect others who come in physical contact with you: you dutifully got vaccinated and now you are immune.63 That is a normal assumption because that is what vaccines are supposed to do, but it is a false assumption.
The Emergency Use Authorization the FDA gave to Pfizer and Moderna was not granted based on scientific evidence that the product prevented infection and transmission of SARS-Cov-2.64 65 In fact, the FDA directed manufacturers in the summer of 2020 to make a product that had at least a 50 percent efficacy rate in either preventing or reducing severity of COVID-19 disease.66
The companies chose to apply for an EUA based on nine months of clinical trial data that the product prevents people from developing severe symptoms of COVID-19 disease 67 and reduces the likelihood they will have serious complications leading to hospitalization and death – not that it prevents infection and transmission. There is a difference.
TAKE HOME FACT: COVID-19 vaccines were not designed and have not yet been proven to prevent infection and transmission of the new coronavirus in the majority of recipients. Apparently, that is why public health officials are telling vaccinated people they have to continue wearing masks and social distancing just like unvaccinated people.68 69
Myth: It is “Good” to Feel Bad After mRNA Covid-19 Shots Because It Means the Vaccine is “Working”
The second big myth being perpetuated by COVID spin is that when you have strong reactions to a COVID-19 shot, it is “good” because it means the vaccine is “working.”70 71
The companies and public health officials admit that the mRNA vaccines are reactive and that the majority of people, especially younger people, who get vaccinated will experience reactions strong enough to require a day or two of recovery and even time off work.72 73 But there is not one credible scientific study published in the medical literature demonstrating that high fevers, chills, headache, joint and muscle aching, disabling fatigue and other symptoms are “good” for the body and indicate the body is successfully producing artificial immunity.
In fact, strong reactions to pharmaceutical products like drugs and vaccines are usually something to be concerned about and a reason to exercise caution, especially with repeat doses. 74 75 76
More concerning are the 68,000 adverse event reports following COVID-19 vaccinations, including over 2600 deaths, 77 that have been reported as of April 8, 2021 to the federal Vaccine Adverse Event Reporting System (VAERS) created under the 1986 National Childhood Vaccine Injury Act.78 79 80 81 More than 70 percent of the reaction reports occurred in people between 17 and 65 years old. And that may be just the tip of the iceberg because one government funded study found that less than one percent of vaccine reactions are ever reported to the vaccine reaction reporting system82 created under the 1986 National Childhood Vaccine Injury Act.
Although Pfizer, Moderna and the government admit that messenger RNA COVID vaccines can cause a lot of reaction symptoms like fever, body pain and disabling fatigue,83 84 85 they adamantly deny that the shots cause sudden death86 87 88 or blood clots89 90 91 92 and bleeding disorders like immune thrombocytopenic purpura,93 cardiac and respiratory arrest,94 95 and other very serious health problems.96
Where is the biological mechanism science that proves it is only a coincidence when people suddenly die within minutes, 97 days or weeks of being given a COVID shot98 and that none of the tens of thousands of bad health outcomes being reported to the Vaccine Adverse Event Reporting System are causally related?99
Where is science backing up the claim that feeling so bad you can’t get out of bed or go to work after getting vaccinated is “good” because being in pain is evidence that the product is effective?
TAKE HOME FACT: COVID-19 shots cause reactions in the majority of people.100 101 There is no scientific evidence that having strong reactions to a drug or biological means that the product is effective.102
Government health officials have said that COVID-19 vaccines will be approved for use in children of any age by early 2022.103 With the majority of adults suffering very strong COVID vaccine reactions, especially younger adults,104 105 why are there plans to give the messenger RNA cell disrupter biological to infants and young children when the CDC says the majority of chilren with COVID-19 disease either have mild symptoms or no symptoms at all? 106
The enormous sums of money that Big Pharma and government is spending on television and digital ad campaigns to make sure that every child and adult in America gets a COVID-19 vaccine is creating false impressions and assumptions. When public policy precedes the science and aggressive advertising campaign blur the lines between facts and myths, truth gets lost in the spin and nobody is safe.
Go to NVIC.org and learn more about SARS-Cov-2 and the biological product being referred to as the COVID-19 vaccine on our new coronavirus information pages.
Go to NVICAdvocacy.org, where you can learn how to help defend informed consent rights in your state so you can make voluntary decisions about vaccination for yourself and your minor children.
References
1 Fisher BL. Here Comes the 21st Century Cures Act: Say Goodbye to Vaccine Safety Science. NVIC Newsletter July 21, 2015.
2 Ramsey L, Friedman LF. The government agency in charge of approving drugs gets a surprising amount of money from the companies that make them. Business Insider Aug. 17, 2016.
3 Fisher BL. End Pharma Liability Shield Endangering Public Health and Human Rights. NVIC Newsletter Nov. 8, 2016.
4 The Vaccine Reaction. Drug Companies Pay FDA and NIH to Fast Track and Market Vaccines. Sept 28, 2018.
5 Fisher BL. WHO, Government, Gates & Government: Who’s Calling the Shots? NVIC Newsletter Jan. 27, 2019.
6 National Academies of Sciences, Engineering, and Medicine. Public–private partnership responses to COVID-19 and future pandemics: Proceedings of a workshop—in brief. Washington, DC: The National Academies Press 2020.
7 U.S. Government Accountability Office (GAO). COVID-19: Federal Efforts to Accelerate Vaccine and Therapeutic Development But More Transparency Needed on Emergency Use Authorization. Nov. 17, 2020.
8 National Institutes of Health. NIH clinical trial of investigational vaccine for COVID-19 begins. NIH Press Release Mar. 16, 2020.
9 Lurie N, Saville M et al. Developing Covid-19 Vaccines at Pandemic Speed. NEJM Mar. 31, 2020
10 Fisher BL. COVID-19 Meltdown and Pharma’s Big Money Win. NVIC Newsletter Apr. 1, 2020.
11 Kollewe J. From Pfizer to Moderna: Who’s making billions from Covid-19 vaccines? The Guardian Mar. 6, 2021.
12 Egan M. Pfizer and Moderna could score $32 billion in Covid-19 vaccine sales – in 2021 alone. CNN Dec. 11, 2020.
13 Megan Garnett Coyle. Ad Tech Leaders Unite to Measure the Ad Council & COVID Collaborative’s COVID-19 Vaccine Education Initiative – the Largest PSA Campaign in US History. Businesswire Mar. 30. 2021.
History
14 Medical Xpress. US launches major COVI vaccination ad campaign. Apr. 1, 2021.
15 Lee B. How is Consumer Drug Advertising Regulated in the United States? June 17, 2019.
16 Harvard Health Publishing. Do not get sold on drug advertising. February 2017.
17 Rapaport L. U.S. health care industry spends $30 billion a year on marketing. Reuters Jan. 8, 2019.
18 Kanski A. Nielsen: Pfizer tops list of biggest pharma advertisers in 2018. Medical Marketing & Media Apr. 2, 2019.
19 Johnson B. Up in Smoke: Documents from the Annals of Tobacco Marketing. Ad Age Mar. 29, 2010.
20 Meyer R. Profiteering off a Covid vaccine. World of DTC Marketing Mar. 25, 2021.
21 Kollewe J. From Pfizer to Moderna: Who’s making billions from Covid-19 vaccines? The Guardian Mar. 6, 2021.
22 Dunleavy BP. Pfizer CEO says need for third dose of COVID-19 vaccine ‘likely.’ UPI Apr. 16, 2021.
23 Weintraub EW. Federal spending on COVID-19 vaccine candidates tops $9 billion, spread among 7 companies. USA Today Aug. 10, 2020.
24 The College of Physicians of Philadelphia. Vaccine Development, Testing and Regulation. The History of Vaccines Jan. 17, 2018.
25 Broom D. 5 charts that tell the story of vaccines today. World Economic Forum June 2, 2020.
26 Fisher BL, Parpia R. 2005 PREP Act and 1986 Act Shield Vaccine Manufacturer’s from Liability. The Vaccine Reaction Aug. 10, 2020.
27 Fisher BL. The New Internet Police Protecting You from Freedom of Thought and Speech. NVIC Newsletter Dec. 3, 2018.
28 Caceres M. When Even the New York Times Doesn’t Pass Facebook Muster. The Vaccine Reaction Dec. 28, 2020.
29 Mercola J. New Thought Police NewsGuard Is Owned by Big Pharma. Jan. 24, 2020.
30 Fisher BL. Vaccination and Censorship: The Truth Will Set Us Free. NVIC Newsletter Jan. 26, 2021.
31 O’Neill J. White House working with social media giants to silence anti-vaxxers. New York Post Feb. 19, 2021.
32 Attkisson S. CENSORED: The National Vaccine Information Center. Mar. 8, 2021.
33 Presson J. Questions linger about COVID-19 vaccine. The Mountaineer Feb. 12, 2021.
34 Droesch B. US Healthcare and Pharma Is Among the Fastest-Growing Digital Ad Spenders. EMarketer Oct. 9, 2020.
35 Droesch B. US Healthcare and Pharma Is Among the Fastest-Growing Digital Ad Spenders. EMarketer Oct. 9, 2020.
36 Silk B. Why Digital Is the Future for Pharma Advertising. Ethoseo Oct. 15, 2019.
37 Robbins R. Get ready for more drug ads: Facebook is making a bid for pharma dollars. STAT News Nov. 1, 2016.
38 Holmes K, Kaufman E. HHS begins national vaccine ad campaign with You Tube ads. CNN Dec. 4, 2020.
39 DHHS. U.S. Department of Health and Human Services Launches Nationwide Network of Trusted Voices to Encourage Vaccination in Next Phase of Public Education Campaign. HHS Press Office Apr. 1, 2021.
40 Facher L. The White House is set to unveil a wide-reaching billion-dollar campaign aimed at convincing every American to get vaccinated. STAT News Mar. 15, 2021.
41 Associated Press. Celebrities Make a Stand for COVID-19 Vaccines on TV Special. Voice of America Apr. 16, 2021.
42 Walmart. Administering COVID-19 Vaccines. Apr. 21, 2021.
43 Hoffman DC. Mass COVID-19 Vaccination Site Set to Open at PPG Paints Arena. KDKA2 Mar. 15, 2021.
44 Archie A. This Indiana school district is helping high schoolers get a COBID-19 vaccine before prom. Louisville Courier Journal Apr. 13, 2021.
45 AdventHealth News. AdventHealth Partners with Churches to Provide COVID-19 Vaccines. Apr. 20, 2021.
46 Collins FS. Statement from NIH and BARDA on the FDA Emergency Use Authorization of the Moderna COVID-19 Vaccine. NIAID Dec. 18, 2020.
47 Pfizer Inc. Pfizer and BioNTech Announce Further Details on Collaboration to Accelerate Global GOVIC-19 Vaccine Development. Businesswire Apr. 9, 2020.
48 Macrotrends. Pfizer Revenue 2006-2020. January 2021.
49 NASDAQ. Pfizer sees about $15 billion in 2021 sales from COVID-19 vaccine. Feb. 2, 2021.
50 NASDAQ. Moderna Earnings Date, Estimates & History. MarketBeat Apr. 16, 2021.
51 CBS News. Moderna forecasts $18.4 billion in COVID-19 vaccine sales. Feb. 28, 2021.
52 Yen H, Mattise J. Half of US adults have received at least one COVID-19 shot. Associated Press Apr. 18, 2021.
53 Syal A. Is It Safe to Visit Grandparents After Getting COVID Vaccine? NBC Feb. 14, 2021.
54 Pfizer Inc. The Facts About Pfizer and BioNTech’s COVID-19 Vaccine. Jan 6, 2021.
55 Banks MA. What Are mRNA Vaccines, and Could They Work Against COVID-19? Smithsonian Magazine Nov. 16, 2020.
56 Trafton A. Explained: Why RNA vaccines for Covid-19 raced to the front of the pack. MIT News Office Dec. 11, 2020.
57 Langreth R, Krege N. Moderna Wants to Transform the Body Into a Vaccine-Making Machine. Bloomberg News Aug. 11, 2020.
58 Harris R. Long-Term Studies of COVID-19 Vaccines Hurt by Placebo Recipients Getting Immunized. NPR Feb. 19, 2021.
59 Pardi N, Hogan MJ et al. mRNA vaccines – a new era in vaccinology. Nature Reviews Drug Discovery 2018; 17: 261-279.
60 Jaffe-Hoffman M. Could mRNA COVID-19 vaccines be dangerous in the long- term? Jerusalem Post Nov. 17, 2020.
61 Odell J. Messenger RNA (nRNA) SARS Coronavirus ‘Vaccines’ and their Potential Autoimmunity Part 2. Bioregulatory Medicine Institute Feb. 24, 2021.
62 Arvin AM, Fink K et al. A perspective on potent antibody-dependent enhancement of SARA-Cov-2. Nature 2020; 584: 352-363.
63 Healthline. How Long Does Immunity Last After COVID-19?: How vaccine-induced immunity after receiving immunization works. Feb. 24, 2021.
64 FDA. Pfizer-BioNTech COVID-19 Vaccine. Dec. 11, 2020.
65 FDA. Moderna COVID-19 Vaccine. Dec. 18, 2020.
66 Heidt A. FDA to Require 50 Percent Efficacy for COVID-19 Vaccines. The Scientist July 1, 2020.
67 Crist C. Early Vaccines Will Prevent Symptoms, Not Virus. WebMD Oct. 28, 2020.
68 Syal A. Is It Safe to Visit Grandparents After Getting COVID Vaccine? NBC Feb. 14, 2021.
69 Rouan R. Fact Check: CDC recommends masks in most cases even after COVID-19 vaccines. USA Today Apr. 22, 2021.
70 Crow S. The CDC Says These 3 Side Effects Mean Your Vaccine Is Working. Yahoo Feb. 15, 2021.
71 Finberg R. No, vaccine side effects don’t tell you how well your immune system will protect you from COVID-19. Yahoo News Apr. 19, 2021.
72 Hendler C. Severe Reactions to COVID-19 Vaccine Close Schools in Michigan, Ohio and New York. The Vaccine Reaction Mar. 8, 2021.
73 Farber M. Is the COVID-19 vaccine effective if you don’t have a reaction to it? Fox News Feb. 9, 2021.
74 Bircher AJ. Symptoms and danger signs in acute drug hypersensitivity. Toxicology 2005; 209(2): 201-207.
75 Davidovici BB, Wolf R. The challenge of drug-rechallenge: Facts and controversies. Clin Dermatol 2010; 281(3): 249-253.
76 GlaxoSmithKline Biologicals. Highlights of Prescribing Information for INFANRIX – diphtheria and tetanus toxoids and acellular pertussis vaccine adsorbed suspension: Contraindications, Warnings and Precautions. Nov. 20, 2019.
77 MedAlerts. Search the VAERS Database.
78 FDA. VAERS Overview. Mar. 29, 2019.
79 CDC. Vaccine Safety: Vaccine Adverse Event Reporting System (VAERS).
80 LaVigne P. The Story Behind MedAlerts. NVIC Newsletter Aug. 20, 2013.
81 The College of Physicians of Philadelphia. Vaccine Injury Compensation Programs: National Childhood Vaccine Injury Act (NCVIA)/National Childhood Vaccine Injury Program (NCVIP). The History of Vaccines Jan. 17, 2018.
82 Harvard Pilgrim Health Care, Inc. Electronic System for Public Health Vaccine Adverse Event Reporting System. AHRQ 2011.
83 The Vaccine Reaction. Moderna’s COVID-19 Vaccine Provokes COVID-Like Symptoms in Phase 3 Trial. Oct. 19, 2020.
84 Fisher BL. Over 3,000 “Health Impact Events” After COVID-19 mRNA Vaccinations. The Vaccine Reaction Dec. 22, 2020.
85 Gale J. COVID-19 vaccine side effects hit some recipients hard; that’s not all bad. Here’s what to do about them. Seattle Times Mar. 11, 2021.
86 Sforza T. Health care worker dies after second dose of COVID vaccine, investigation underway. Orange County Register Feb. 4, 2021.
87 Percy N. Kaiser says Pfizer vaccine likely not cause of Calfornia woman’s death. Mercury News Feb. 15, 2021
88 Brown E. Fact Check: Have 966 People Died After Receiving the COVID vaccine? Newsweek Mar. 8, 2021.
89 Goldstein S. Blood clots prevalent with Pfizer and Moderna Vaccine as with Astra Zeneca’s study. Dow Jones/Market Watch Apr. 16, 2021.
90 Ma A. Schuster-Bruce C. Johnson & Johnson asked other drugmakers to help it study blood-clot risks, and Moderna and Pfizer decline, report says. Business Insider Apr. 16, 2021.
91 Scribner H. Recent vaccine news should improve further confidence, doctor says. Deseret News Apr. 15, 2021.
92 Beusekom MV. Study: COVID much more likely than vaccines to cause blood clot. CIDRAP Apr. 15, 2021.
93 Fisher BL. Miami Obstetrician Develops Bleeding Disorder, Dies After Getting COVID-19 Vaccine. The Vaccine Reaction Jan. 11, 2021.
94 Israel National News. Mexican doctor hospitalized after receiving COVID-19 vaccine. Jan. 2, 2021.
95 Microsoft News. 72-year old man sent to ICU following COVID-19 vaccination; MOH confirms cardiac arrest wasn’t caused by vaccine. Feb. 19, 2021.
96 Fisher BL. Healthy Mom, 39, in Utah Dies of Organ Failure Days After Moderna COVID Vaccination. The Vaccine Reaction Mar. 15. 2021.
97 The Vaccine Reaction. Woman Dies Immediately After Getting COVID-9 Vaccine in Virginia. Feb. 21, 2021.
98 Haglage A. No evidence COVID-19 vaccines cause death epidemiologists say: ‘Coincidences are going to happen.’ Yahoo Feb. 4, 2021.
99 Rouan R. Fact check: CDC data on adverse effects of vaccine cannot determine cause. USA Today Apr. 8, 2021.
100 CDC. Local Reactions, Systemic Reactions, Adverse Events and Serious Adverse Events: Pfizer COVID-19 Vaccine. Dec. 13, 2020.
101 FDA. Moderna COVID-19 Vaccine. Dec. 18, 2020.
102 Finberg R. No, vaccine side effects don’t tell you how well your immune system will protect you from COVID-19. Yahoo News Apr. 19, 2021.
103 Thomas N. Fauci expects almost all children to be eligible for Covid-19 vaccines by first quarter 2022 at the latest. CNN Apr 18, 2021.
104 Koweek M. Younger adults are having harsher Covid vaccine side effects. WHIO TV Mar. 5, 2021.
105 Bendix A. Why you can expect more severe vaccine side effects if you’re younger or a woman. Business Insider Apr. 6, 2021.
106 CDC. COVID-19 in Children and Teens: What You Need to Know. Mar. 17, 2021.
When Will the Evidence From Florida and Texas Break Through the SAGE Groupthink?

By Will Jones • Lockdown Sceptics • May 16, 2021
The latest model of doom from Government advisory group SAGE appeared yesterday, predicting a ludicrous 10,000 hospital admissions a day in mid-July in a vaccinated population (nearly three times the January peak) because of the Indian variant – and that’s the central scenario. Furthermore, the researchers don’t even think the Indian variant is more deadly or particularly good at evading vaccines. So how do they conclude it will precipitate such a calamity?
Professor Adam Kucharski, a SAGE modeller from the London School of Hygiene and Tropical Medicine (LSHTM), explains their reasoning:
The issue is that many people have a mental image that we’ve [already] had the biggest possible epidemic waves, whereas we’ve actually had ones that are relatively small compared to what could have happened without control measures in place. Because of these controls, only a fraction of the people who could have got infected in the past year or so have been infected, so they’re still out there. Of course, for many of these people vaccines have now decreased their risk substantially. But a very large number of infections that come with a very small individual level of risk can produce a similar outcome to a smaller epidemic that carries a larger individual level of risk.
Maths whizz Glen Bishop, writing for Lockdown Sceptics, has shown why SAGE’s assumptions are so unrealistic as to produce these highly implausible scenarios. In their central scenario, for example, they assume that around half of the UK will be simultaneously infected in one week in mid-July. This is despite the January peak only having around 2% of the population infected at one time, according to the ONS.
Another of the models’ big assumptions, prominent in what Prof Kucharski says above, is that lockdowns and social distancing have successfully suppressed the virus and that it is only because they continue in some form that the flood of infections, hospitalisations and deaths is held back. The latest modelling starkly shows how, even with a high vaccination coverage as in the UK, such an assumption can produce predictions so dire they send twitchy Governments reaching for the lockdown order.
As the SAGE briefing says:
At this point in the vaccine rollout, there are still too few adults vaccinated to prevent a significant resurgence that ultimately could put unsustainable pressure on the NHS, without non-pharmaceutical interventions. … It is a realistic possibility that this new variant of concern could be 50% more transmissible. If [the Indian variant] does have such a large transmission advantage, it is a realistic possibility that progressing with all roadmap steps would lead to a substantial resurgence of hospitalisations.
In fact, there is no evidence (outside models, which are not evidence) that lockdown measures or social distancing have any significant impact on reducing Covid infections or deaths. This is why the states in America which removed their restrictions in March (Texas) or last autumn (Florida) or never imposed them (South Dakota) are doing no worse, and often better, than many states which maintained strict restrictions throughout the winter (see the graph above). Sweden demonstrates a similar point in Europe.
The depressing truth, though, is that sceptics have largely failed to get this basic point across to those in charge and their scientific advisers. It’s not as though the evidence is not there. There are numerous peer-reviewed articles in leading journals that set out the evidence on this, and more keep appearing. Leading scientists have raised their heads to make the evidence-based case.
Graphs like the above, which should by themselves undermine the entire lockdown edifice, are easy to produce. Leading journalists such as Fraser Nelson, writing in one of the leading Tory newspapers, the Telegraph, has pointed repeatedly to the evidence on this. The data is plain for all to see and the voices highlighting it are not marginal or lacking in credibility.
Yet here we are again, with another model built on dubious assumptions and a presumption of lockdown efficacy once more imperilling our liberty. Freedom has never felt so fragile as in these past 14 months, when access to basic liberties has rested on the evidence-free assumptions made by a small group of mathematical modellers whose word seems to be taken as holy writ by those in charge.
Adam Kucharski is on Twitter. So why not ask him (politely!) why, if so many people remain so susceptible to this virus and its variants as to produce such dire predictions, Florida, Texas and South Dakota have fared no worse than places which have imposed or maintained restrictions? I’ve put the graph as the featured image to make it easy to share – just put a link to this article in the tweet and the graph should appear. If you get any answers from him, why not email them to us here.
REVIEW: COVID-19 Vaccines May Lead To Prion-Linked Brain Degeneration Similar To Mad Cow Disease
Researchers published a review that sounds the alarm about potential unintended COVID-19 vaccine side effects
By Tom Pappert | National File | May 12, 2021
A new review of possible unintended consequences of COVID-19 vaccines suggests that the controversial mRNA vaccines – Moderna and Pfizer – may lead to unexpected neurological conditions similar to Mad Cow Disease.
The review by Stephanie Seneff, who works at the Computer Science and Artificial Intelligence Laboratory at MIT, and Dr. Nigh, who specializes in Naturopathic Oncologogy at Immerson Health in Portland, Oregon, was released this week in the International Journal of Vaccine Theory, Practice, and Research, and devotes a considerable space to discussing the research of Dr. J. Bart Classen, who first published a research paper on the possibility of prion-linked brain degeneration caused by the COVID-19 vaccine last month, and expands on his research.
The researchers explain that “researchers have identified a signature motif linked to susceptibility to misfolding into toxic oligomers, called the glycine zipper motif. It is characterized by a pattern of two glycine residues spaced by three intervening amino acids, represented as GxxxG. The bovine prion linked to MADCOW has a spectacular sequence of ten GxxxGs in a row,” and notes that “the SARS-CoV-2 spike protein is a transmembrane protein, and that it contains five GxxxG motifs in its sequence” and, thus, “it becomes extremely plausible that it could behave as a prion”.
“Recall that the mRNA vaccines are designed with an altered sequence that replaces two adjacent amino acids in the fusion domain with a pair of prolines,” the authors continue. “This is done intentionally in order to force the protein to remain in its open state and make it harder for it to fuse with the membrane. This seems to us like a dangerous step towards misfolding potentially leading to prion disease.”
Prions were first described as the method by which Mad Cow Disease causes brain degeneration due to misfolding proteins in the body. The CDC notes that “prion diseases are usually rapidly progressive and always fatal.” Mad Cow Disease “progressively attacks the brain but can remain dormant for decades,” per the BBC.
“Pfizer claims the RNA fragments ‘likely… will not result in expressed proteins’ due to their assumed rapid degradation in the cell,” the researchers note. They add, “While we are not asserting that non-spike proteins generated from fragmented RNA would be misfolded or otherwise pathological, we believe they would at least contribute to cellular stress that promotes prion-associated conformational changes in the spike protein that is present.”
When Classen previously published his research, fact checkers were quick to point to public statements from Pfizer that dismissed concerns of brain prions as a result of their vaccine. It may be worth noting that “the most expensive settlement that Pfizer has paid was over $2.3 billion paid as a fine to resolve civil and criminal penalties for illegal marketing of four medications including Bextra, Geodon, Zyvox, and Lyrics.”
The End of The Mask
By Kip Hansen | Watts Up With That? | May 15, 2021
If there was ever a surer example of the perversion of the Power of Experts than the Covid Mask Mania, I am unaware of it. I doubt that there is a single self-aware person in the world that does not know what the Covid Mask Mania means, even most of those who have been stanch supporters and promoters of The Mask are aware that it is, in fact, a product of a world-wide Mass Hysteria that grew out of the unknowns surrounding the outbreak of a novel coronavirus in Wuhan, China in late 2019.
Those of you who still have the ability to remember the recent past, despite endless propaganda aimed at making you forget, the original CDC Guidance on Face Masks for Covid-19 was this:
Wear a facemask if you are sick
If you are sick: You should wear a facemask when you are around other people (e.g., sharing a room or vehicle) and before you enter a healthcare provider’s office. If you are not able to wear a facemask (for example, because it causes trouble breathing), then you should do your best to cover your coughs and sneezes, and people who are caring for you should wear a facemask if they enter your room. Learn what to do if you are sick.
If you are NOT sick: You do not need to wear a facemask unless you are caring for someone who is sick (and they are not able to wear a facemask). Facemasks may be in short supply and they should be saved for caregivers.[ source CDC website dated 28 March 2020 via WayBack Machine ]
The Famous Fauci, back when he was just Director of the National Institute of Allergy and Infectious Diseases and not yet a global media star – let me be clear, we are talking about when Dr. Anthony Fauci was the nation’s leading expert on infectious diseases of all kinds – he said the following in a televised interview on March 8, 2020:
[ Quoting the opinion checking website, FactCheck.org which found that history requires a revision in order to comply with “latest guidelines” in its current coverage here. ]
Here’s what Fauci told Dr. Jon LaPook, chief medical correspondent for CBS News, in the clip circulating on social media:
LaPook, March 8: There’s a lot of confusion among people, and misinformation, surrounding face masks. Can you discuss that?
Fauci: The masks are important for someone who’s infected to prevent them from infecting someone else… Right now in the United States, people should not be walking around with masks.
LaPook: You’re sure of it? Because people are listening really closely to this.
Fauci: … There’s no reason to be walking around with a mask. When you’re in the middle of an outbreak, wearing a mask might make people feel a little bit better and it might even block a droplet, but it’s not providing the perfect protection that people think that it is. And, often, there are unintended consequences — people keep fiddling with the mask and they keep touching their face.
LaPook: And can you get some schmutz, sort of staying inside there?
Fauci: Of course, of course. But, when you think masks, you should think of health care providers needing them and people who are ill. The people who, when you look at the films of foreign countries and you see 85% of the people wearing masks — that’s fine, that’s fine. I’m not against it. If you want to do it, that’s fine.
LaPook: But it can lead to a shortage of masks?
Fauci: Exactly, that’s the point. It could lead to a shortage of masks for the people who really need it.”
Other than adding a link to the definition of schmutz – I have not highlighted any of Faucci’s statement. I don’t need to catch Fauci out in anything because Fauci was absolutely scientifically correct in everything he said. In this, he totally depended on the existing science on the prevention of the transmission of coronavirus illnesses. And the science on the topic has not changed – if anything, it has been reinforced over and over throughout the Covid-19 pandemic.
Yet, FactOpinionCheck.org decided that Fauci, the USA’s leading expert on Infectious Diseases and their transmission, was not expert enough – so they check his knowledge against the opinion of the Director of the CDC? No…. against the opinion of Dr. Dean Winslow, a well-known infectious disease physician at Stanford (University) Health Care who told FactOpinionCheck.org:
“In early March, so few patients had been tested that public health officials didn’t yet know that people could spread the virus without showing symptoms, said Winslow.
“That was just not known at that point.”
There was no new science that suddenly made masks effective for the general public but something maybe about Covid-19.
And what does that science really say? “… there’s little scientific evidence that the various face coverings we call ‘masks’ do much if anything to stop the spread of the coronavirus.” [ source ] There are just too many peer-reviewed, high-powered, definitive studies and meta-analyses to list here. The Big List of such studies is in the book: “The Price of Panic. . . .” by Jay W. Richards, Douglas Axe, and William Briggs.
It is, of course, as in all things that deal with the political interference in things that should depend on strict empirical science, worse than that.
In April 2020, the Famous Fauci said
“So, we want to make sure that this issue of having a broader community approach towards putting on a facial covering doesn’t, in fact, get in the way of the primary purpose of masks.
[ which was, he had just explained: “masks that are most appropriately used and necessary for the front-line health care workers, who do need it for the clear and present danger that they find themselves in when they are taking care of people who are actually sick with coronavirus disease.” ]
And in that regard, that’s why what we’re talking about are things that may not necessarily need to be a classical mask, but could be some sort of facial covering.
You know, we’re pretty good in making things in a way that spontaneously becomes effective just because of your own creativity.”
[ source – PBS interview here. ]
Once the CDC changed it’s tune on masks, demanding that The Mask be worn at all times under almost all circumstances, the rhetoric ramped up not only demanding that everyone everywhere wear masks, but accusing those who fail or refuse to wear masks of “killing their grandmothers” (Andrew Cuomo – Governor of New York – a charge he repeats in the present about those who don’t get vaccinated).
In a mass-hysteria-type reaction, everyone who could find a public megaphone jumped on the bandwagon, making wilder and wilder public statements about the deadly-serious importance of wearing masks:
“Everyone should wear a mask,” Blumberg said. “People who say ‘I don’t believe masks work’ are ignoring scientific evidence. It’s not a belief system. It’s like saying, ‘I don’t believe in gravity.’
“People who don’t wear a mask increase the risk of transmission to everyone, not just the people they come into contact with,” he said. “It’s all the people those people will have contact with. You’re being an irresponsible member of the community if you’re not wearing a mask.” [ source ]
Wearing a mask became a virtue signaling bellweather: “I’m a good person, a patriot, a saint….” Because I wear a mask, even in my own home or when alone in my car.
And now?
In an unexpected change of heart (must have been as there has been no new science or breakthrough understanding), the CDC has said:
Vaccinated Americans May Go Without Masks in Most Places, Federal Officials Say
Fully vaccinated people do not have to wear masks or maintain social distance indoors or outdoors, with some exceptions, the C.D.C. advised. [ source ]
Directly from the CDC:
“Update that fully vaccinated people no longer need to wear a mask or physically distance in any setting, except where required by federal, state, local, tribal, or territorial laws, rules, and regulations, including local business and workplace guidance
Update that fully vaccinated people can refrain from testing following a known exposure unless they are residents or employees of a correctional or detention facility or a homeless shelter”
[ source: CDC here 13 May 2021 ]
End BQ
What does this mean for the real world?
Up to 13 May 2021, US News and World Report list the following U.S. states as having NO Mask Mandate previous-to-CDC-announcement:
Alabama | Alaska | Arizona | Arkansas | Florida | Georgia | Idaho | Indiana | Iowa | Kansas | Louisiana | Minnesota | Mississippi | Missouri | Montana | Nebraska | New Hampshire | North Dakota | Oklahoma | South Carolina | South Dakota | Tennessee | Texas | Utah | Wisconsin | Wyoming | Northern Mariana Islands (an unincorporated territory and commonwealth of the U.S.)
That’s 26 out of 50 states with no mandate before the new CDC guidelines.
So far today:
Kentucky Governor Andy Beshear says the state’s mask mandate will end June 11, 2021. On that date, the Bluegrass State will also return to 100% capacity at venues and events. [ source ]
Minnesota — Following New CDC Guidance, Governor Walz Announces End to Statewide Face Covering Requirement — Minnesota will align with CDC guidance and recommend unvaccinated Minnesotans continue to wear face coverings indoors [ source ]
North Carolina has removed its indoor mask mandate for most settings and lifted all mass gathering and social distancing limits. This step forward is effective immediately and follows yesterday’s guidance from the CDC. [ source ]
Rhode Island — paraphrasing “fully vaccinated people, as of this coming Tuesday, will no longer need to wear masks or social distance”. [ source ]
Michigan – paraphrasing “everyone who is two weeks out from their second vaccine dose can go without a mask”. [ source ]
Oregon – “Starting today, Oregon will be following this guidance, which only applies to fully-vaccinated individuals. That means Oregonians who are fully-vaccinated no longer need to wear masks or social distance in most public spaces.” [ source ]
Florida — “Floridians should not be penalized for rejecting the overreach of local authorities through unnecessary mask mandates,” [Governor] DeSantis wrote on Twitter Thursday about his decision to pardon the Carnevales. [ who had been arrested for failing to require masks and social distancing at their business, a gym.]” “The governor confirmed his intentions to pardon people at a press conference Thursday in Ormond Beach, Florida, saying he would “remit” the remaining outstanding fines that have been issued against people at the state’s next clemency meeting.” [ source ]
Connecticut — Masks Not Required Indoors For Fully Vaccinated People in Connecticut Starting May 19: Governor [ source ]
Illinois – “Gov. J.B. Pritzker says that he will revise executive orders to sync up with new CDC guidelines on mask wearing by vaccinated individuals in indoor and outdoor spaces.” [ source ]
Nevada – “On May 3, Gov. Steve Sisolak signed an emergency directive updating mask and face covering requirements for the state to align with the CDC’s recommendations, including any subsequent guidance. As a result, the new guidance from the federal agency became effective immediately, according to a news release from the state.” [ source ]
Pennsylvania – “In short, the Health Department says it is following the CDC’s lead. That means Pennsylvanians who are fully vaccinated no longer have to wear masks outdoors or indoors except in certain situations.“ [ source ]
Washington – “Masks off: Fully vaccinated people can shed masks in Washington, [Washington Governor] Inslee announces following new CDC rules” [ source ]
New York – “Governor Andrew M. Cuomo today announced that New York State will adopt the Centers for Disease Control and Prevention’s new guidance on mask use for fully vaccinated people. The guidelines state that fully vaccinated people, defined as two or more weeks after receiving the second dose of the Pfizer or Moderna vaccine or the single-dose Johnson & Johnson vaccine, no longer need to wear masks outdoors, except in certain crowded settings and venues.” [ source ]
Virginia – “Governor Ralph Northam today lifted Virginia’s universal indoor mask mandate to align with new guidance from the Centers for Disease Control and Prevention (CDC). Governor Northam also announced that Virginia will ease all distancing and capacity restrictions on Friday, May 28, two weeks earlier than planned. The updates to Virginia’s mask policy …. will become effective at midnight tonight along with previously announced changes to mitigation measures.” [ source ]
Colorado – “Coloradans who are fully vaccinated are no longer required to wear masks, and people who aren’t vaccinated are only required to wear them in limited settings, Gov. Jared Polis said Friday.” [ source ]
Delaware – “Governor John Carney on Friday announced that – effective May 21 – the State of Delaware will lift its requirement that Delawareans and visitors must wear face coverings anytime they are indoors with others outside their household. Delawareans should instead follow masking guidance issued on Thursday by the Centers for Disease Control and Prevention (CDC) for all indoor and outdoor activities.” [ source ]
West Virginia – “West Virginia Governor Jim Justice announced that he is signing an executive order to modify the face covering requirement during a press conference on Friday. The governor says West Virginia will immediately begin following the updated CDC guidance for those who are fully vaccinated. The facial covering requirement will still apply to those who have not been vaccinated until June 20.” [ source ]
The Governors of the states (in the United States) are announcing allegiance to the CDC so quickly that I literally cannot keep up with adding them in above as I write this column.
How long do you think the other governors, who have not yet fallen into line with the new (and very welcome) diktat from the CDC, can delay? Does anyone think that citizens of one state seeing freedom restored in the neighboring state will not demand the same freedom?
I think that reasonable people will realize that the mask mandate was unnecessary from the beginning — especially as The Science from The Epidemiologists has been telling them all to expect to have to wear masks for at least another six months, a year longer, two years, or maybe forever. In a poll conducted by the NY Timesthat was completed just 4 days ago, 81% of professional epidemiologists expected mask mandates to continue for at least 1 more year. 52% expected masking to last for more than a year. The minimum expected was “a few more months”. Up until yesterday, Epidemiologists represented The Science…. no longer, they have been kicked to the curb.
In my opinion, this new CDC Guideline breaks the back of the oppressive Covid-19 Panic Power Grab by presidents, governors, city councils and mayors who have reveled in their free pass to rule by executive order under emergency powers without oversight by elected law makers.
There will be no going back, I don’t think the people will stand for it, at least not in the United States.
‘Inconvenient’ U.S. Wildfire Data Has Been ‘Disappeared’ by National Interagency Fire Center
By Anthony Watts | Watts Up With That? | May 13, 2021
It’s been an open secret, ever since Dr. Michael Mann used “Mike’s Nature Trick” to “hide the decline” by covering up some inconvenient tree ring data in the hockey stick climate graph, that climate alarmists will go to almost any length to only show the public the “crisis side” of climate data.
The National Interagency Fire Center (NIFC) has been the keeper of U.S. wildfire data for decades, tracking both the number of wildfires and acreage burned all the way back to 1926. However, after making that entire dataset public for decades, now, in a blatant act of cherry picking, NIFC “disappeared” a portion of it, and only show data from 1983. You can see it here.
Fortunately, the Internet never forgets, and the entire dataset is preserved on the Internet Wayback machine and other places, despite NIFC’s ham-handed attempt to disappear the data.
Why would they do this you ask? The answer is simple; data prior to 1983 shows that U.S. wildfires were far worse both in frequency and total acreage burned. By disappearing all data prior to 1983, which just happens to be the lowest point in the dataset, now all of the sudden we get a positive slope of worsening wildfire aligning with increased global temperature, which is perfect for claiming “climate change is making wildfire worse.” See figure 1 below for a before and after comparison of what the data looks like when you plot it.

Figure 1: Comparison of the before and after erasure NIFC dataset showing acres burned. The blue trend line goes from a negative trend to a positive one when cherry picked data is used.
Clearly, wildfires were far worse in the past, and clearly, now the data tells an entirely different story when showing only data post-1983. The new story told by the sanitized data is in alignment with the irrational screeching of climate alarmists that “wildfires are driven by climate change”.
This wholesale erasure of important public data stinks, but in today’s narrative control culture that wants to rid us of anything that might be inconvenient or doesn’t fit the “woke” narrative, it isn’t surprising.
Interestingly, the history on the Internet Wayback Machine shows how NIFC rationalized this erasure of important public data.
Back in June 2011 when this data was first presented by NIFC publicly, it was simply presented “as-is”. They say only this:
Figures prior to 1983 may be revised as NICC verifies historical data.
In 2018, they added a new caveat, saying this:
The National Interagency Coordination Center at NIFC compiles annual wildland fire statistics for federal and state agencies. This information is provided through Situation Reports, which have been in use for several decades. Prior to 1983, sources of these figures are not known, or cannot be confirmed, and were not derived from the current situation reporting process. As a result the figures prior to 1983 should not be compared to later data.
According to the Internet Wayback Machine, that caveat first appeared on the NIFC data page somewhere between January 14 and March 7 of 2018.
Curiously, that caveat appeared just a few weeks after I first drew wide attention to the issue in December 2017, with an article citing NIFC fire data titled Is climate change REALLY the culprit causing California’s wildfires?
It seems they received some blowback from the idea that their data, when plotted, clearly showed wildfires to be far worse in the past, completely blowing the global-warming-climate-change-wildfire connection out of the water.
Here is what NIFC says now:
Prior to 1983, the federal wildland fire agencies did not track official wildfire data using current reporting processes. As a result, there is no official data prior to 1983 posted on this site.
Not only is that a lie of omission, it is ridiculous. Their agenda seems very clear. When the data was first published, they only advised the public that some data prior to 1983 might be “… revised as NICC verifies historical data”.
There was no published concern that the data might be invalid, or that we shouldn’t use it. Besides, the data is very simple; a count of the number of fires and the number of acres burned. How hard is that to compile and verify as accurate?
What’s worse is that this data has been trusted for decades in almost every news story about any wildfire that ever occurred in the U.S. In virtually every news story about a wildfire, the number of acres burned it THE NUMBER the press uses in the story, without it, there is no scale of the severity of the fire. Similarly, for every story about “what a bad wildfire season we’ve had”, the press cites the number of fires as well as the acreage burned.
And now, after decades of that data being provided to the press and the public, and nearly a decade of NIFC making it publicly available on their website, they want us to believe that it is now unreliable data?
Seriously, just how hard is it to count the number of fires that have happened and the number of acres burned?
What NIFC is doing is essentially labeling every firefighter, every fire captain, every forester, and every smoke jumper who has fought wildfires for decades as being untrustworthy in their assessment and measurement of this critical, yet very simple fire data. I’ll take data from people on the fire scene over government bureaucratic doublespeak every day of the week and twice on Sundays.
This whole affair is outrageous. But what is even more outrageous is that NIFC isn’t at all transparent as to the reason for the change. They essentially say “The data prior to 1983 is no good, trust us”. There is no citation of a study, no methodology given, no rationale for the removal. That’s not science, that’s not statistics, that’s not even sensible, but that is what is happening.
Plotting the entire NIFC dataset (before it was partially disappeared) gives us some hints as to why this has been done, and how wildfire and weather patterns have been inextricably linked for decades. Note figure 2 below, combining the number of fires and number of acres burned. See the annotations that I have added.

Figure 2: Plot of the entire NIFC wildfire dataset, with acreage burned in amber, and total number of fires in a given year in blue. Annotations show major weather events in the U.S.
Clearly, what NIFC has done by saying data prior to 1983 is “unreliable” and disappearing it is not just hiding important fire history, but cherry picking a data starting point that is the lowest in the entire record to ensure that an upwards trend exists from that point.
The definition of cherry picking is:
Cherry picking, suppressing evidence, or the fallacy of incomplete evidence is the act of pointing to individual cases or data that seem to confirm a particular position while ignoring a significant portion of related and similar cases or data that may contradict that position.
And by choosing the lowest point in the record for total fires, 1983, and making all data prior to that unavailable, NIFC ensures that any comparison between fires and climate change over the last 38 years always shows an upward trend and correlation with rising temperature.
It seems to me that NIFC very likely caved to pressure from climate activists to disappear this inconvenient data. By erasing the past data, NIFC has become untrustworthy. This erasure is not just unscientific, it’s dishonest and possibly fraudulent.
For posterity, the entire dataset from NIFC (including pre-1983) is available here in an Excel (.xlsx) file:
NIFC-Wildfires-1926-2020Download
UPDATE: Here is an analysis paper from 2015 using the same data that is on the U.S. Forest Service website:
Featured Video
Trump Announces Operation To Escort Ships – Fmr. CIA Analyst Larry Johnson
or go to
Aletho News Archives – Video-Images
From the Archives
Who Runs Our World?

Netanyahu addresses US Congress
By Richard Hugus | January 4, 2019
Our world is run by oligarchs, the holders of vast wealth from monopolies in banking, resource extraction, manufacturing, and technology. Oligarchs have such power that most of the world doesn’t even know of their influence over our lives. Their overall agenda is global power — a world government, run by them — to be achieved through planned steps of social engineering. The oligarchs remain in the background and have heads of state and entire governments acting in their service. Presidents and prime ministers are their puppets. Bureaucrats and politicians are their factotums.
Who are politicians? Politicians are people who work for the powerful while pretending to represent the people who voted for them. This double-dealing involves a lot of lying, so successful politicians must be good at it. It’s not an easy job to make the insane agenda of the powerful seem reasonable. Politicians can’t reveal this agenda because it almost always goes against the interests of their constituents, so they become adept at sophistry, mystification, and the appearance of authority. For example, wars for Israel have been part of the agenda of the powerful for years. Since 2001, wars for Israel have been sold as “the war on terror” and lots of lies had to be made up as to why the war on terror was a real thing. The visible faces promoting the war on terror were neoconservatives in the US, almost all of whom were advocates for Israel, or Zionists. Zionists are not the only members of the oligarchy, but they seem to be its lead actors. ... continue
Blog Roll
 Aletho News
Aletho News- Government Kills the Spirit
- How ‘Israel’s’ Iran regime change plot failed – again
- 1977 Influenza Pandemic Sequence Shows Signs of Laboratory Creation: Journal ‘Cell’
- China issues first prohibition order to safeguard international trade order under rule of law
- Iran rejects Trump’s ‘Project Freedom,’ warns US over Hormuz role
- TRUMP ANNOUNCES OPERATION TO ESCORT SHIPS – Fmr. CIA Analyst Larry Johnson
- A few observations on Iran’s latest proposal to Trump
- ‘I urged that our objective be regime change… so did Netanyahu’ – ex-Trump adviser on Iran
- “STAGED”: Conspiracy Theories Are Everywhere!
- NATO courts screenwriters to embed alliance messaging in film, TV
- If Americans Knew
- One Gaza is not enough: Israel is turning southern Lebanon into another Gaza – Daily Update
- As Palestinians die, Ben-Gvir celebrates birthday with golden noose cake – Daily Update
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- No Tricks Zone
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
