COVID-19: Just the Facts

By Will Jones | Lockdown Sceptics | May 9, 2021
Twelve key questions about COVID-19 and lockdowns answered. All answers fully referenced from peer-reviewed research and leading authorities.
How deadly is COVID-19?
Stanford Professor of Medicine and Epidemiology John P. A. Ioannidis in the European Journal of Clinical Investigation has reviewed data from studies globally and estimated that the infection fatality rate (IFR) of COVID-19 is around 0.15%. It varies considerably by region (for reasons such as demographics and prior susceptibility) and between countries within regions. In Europe and the Americas it is around 0.3%-0.4%. In Africa and Asia it is around 0.05%.
It also varies considerably between ages and depending on the presence of underlying conditions. Cambridge Professor of Statistics David Spiegelhalter has used the mortality data from the spring 2020 epidemic in England and Wales to show that the risk of dying from a COVID-19 infection roughly increases by 12-13% for each year older, doubles every 5-6 years and is around 10,000 times higher for the oldest compared to the youngest. It is also roughly equivalent to the normal risk of dying in a given year (though is mostly in addition to that normal risk). Men have around double the risk of death of women of the same age.

The average age of death from Covid in England and Wales in the spring epidemic was 80.4 according to the ONS, splitting 78.7 for men and 82.5 for women. The average age of death in the UK is 79.3 for men and 82.9 for women (though note these are modelled estimates of life expectancy at birth based on life tables, not the actual average age of those who die each year). Public Health England has estimated that life expectancy was reduced by 1.3 years for men and 0.9 years for women in 2020 due to the Covid and lockdown death tolls, though these figures are also modelled.
Economist John Appleby writing in the BMJ has shown that every year prior to 2009 was more deadly than 2020 in England and Wales once the size and age of the population is taken into account. The same analysis also shows that previous pandemics have not resulted in continued elevated death rates for more than a year or two despite not having vaccines for the diseases, indicating how the human immune system and the diseases adapt into a less deadly relationship.

A Swedish review of Covid deaths outside hospitals (i.e., in care homes and private homes) in one county found 85% were from a different underlying cause. In Northern Ireland, 38% of Covid deaths in spring 2020 were determined to be not primarily due to COVID-19. However, the same figure in England and Wales was 8%, suggesting significant differences in how Covid deaths are registered between jurisdictions.
How is COVID-19 spread?
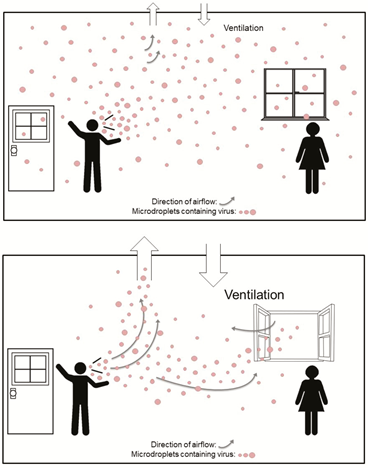
According to the most up-to-date data, COVID-19 primarily spreads via aerosols that build-up in the air of a room rather than via larger droplets or through contact with surfaces (fomites). This is why many of the measures taken to combat the spread of COVID-19, such as distancing, barriers, face masks (see below) and cleaning surfaces are ineffective. Outdoor transmission is very rare.
Public Health England has used data from the Government testing programme to show that the secondary attack rate (proportion of contacts who catch the virus from an infected person) in private homes is around 10.1%. An American study in JAMA found it was 16.6%.
The low secondary attack rate in the high-exposure context of private homes is indicative of high levels of pre-existing immunity to the disease, as discussed in the BMJ by Peter Doshi. Note that immunity is not binary – a person can be resistant on one occasion and not resistant on another, for a variety of reasons. Cross-reactive T-cells that provide a measure of immunity have been found in a number of studies in 20-50% of unexposed people. Exposure without detectable infection (detectable by a PCR test) has also been found to induce a degree of T-cell immunity.
Infection with COVID-19 has been shown in a number of studies, including one on U.S Marines published in the Lancet, to confer natural immunity that gives around 80% protection from re-infection and 90% protection from symptomatic re-infection, with ten times lower viral load (corresponding to infectiousness).
What about asymptomatic and pre-symptomatic transmission?
Asymptomatic infection is typically characterised by a much lower viral load and consequently much lower infectiousness. The study in JAMA on household secondary attack rate (SAR) cited above found that asymptomatic infections had a SAR of just 0.7% versus a SAR of 18% for symptomatic infection. The proportion of infections that are asymptomatic increases among those with immunity from previous infection or vaccination, showing that it is a characteristic of immunity.
People become infectious around two days prior to onset of symptoms as viral load peaks. This pre-symptomatic transmission is estimated to account for around 6.4% of spread, according to a study of actual transmission events from Singapore. Modelled estimates of the contribution of pre-symptomatic spread appear to go too high.
This means that people without symptoms, whether asymptomatic or pre-symptomatic, are not major drivers of the epidemic.
Do lockdowns work?
Restrictions on social contact, such as stay-at-home orders, business closures and gathering limits, have consistently been shown in peer-reviewed studies to have had no significant impact on outcomes such as Covid infections and deaths. Here is a sample, with a key quote from each.
- “Full lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality.” “A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes” by Rabail Chaudhry, George Dranitsaris, Talha Mubashir, Justyna Bartoszko, Sheila Riazi. EClinicalMedicine (Lancet) 25 (2020) 100464, July 21st, 2020.
- “We find that shelter-in-place orders had no detectable health benefits, only modest effects on behaviour, and small but adverse effects on the economy.” “Evaluating the effects of shelter-in-place policies during the COVID-19 pandemic” by Christopher R. Berry, Anthony Fowler, Tamara Glazer, Samantha Handel-Meyer, and Alec MacMillen, Proceedings of the National Academy of Science of the USA, April 13th, 2021.
- “Stringency of the measures settled to fight pandemia, including lockdown, did not appear to be linked with death rate.” “Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation” by Quentin De Larochelambert, Andy Marc, Juliana Antero, Eric Le Bourg, and Jean-François Toussaint. Frontiers in Public Health, November 19th, 2020.
- “Comparing weekly mortality in 24 European countries, the findings in this paper suggest that more severe lockdown policies have not been associated with lower mortality. In other words, the lockdowns have not worked as intended.” “Did Lockdown Work? An Economist’s Cross-Country Comparison” by Christian Bjørnskov. CESifo Economic Studies March 29th, 2021.
- “While small benefits cannot be excluded, we do not find significant benefits on case growth of more restrictive NPIs.” “Assessing Mandatory Stay‐at‐Home and Business Closure Effects on the Spread of COVID‐19” by Eran Bendavid, Christopher Oh, Jay Bhattacharya, John P.A. Ioannidis. European Journal of Clinical Investigation, January 5th, 2021.
Studies which conclude otherwise are invariably based on models rather than data.
Professor Simon Woods, a mathematician, has shown that infections were in decline prior to the start of all three lockdowns in England.

You can find a useful round-up of the studies showing lockdowns don’t work at AIER.
Does social distancing work?
Many studies (including some of those above) which conclude that lockdowns don’t work nonetheless add that voluntary social distancing practices do reduce infections or deaths by suppressing spread. However, this is typically stated without supporting evidence. In fact, the evidence on this is also quite weak.
An international comparison study in Nature by R.F. Savaris and colleagues found that actually staying at home (measured by mobile phone mobility data) made no significant difference to outcomes either. “We were not able to explain the variation of deaths per million in different regions in the world by social isolation, herein analysed as differences in staying at home, compared to baseline,” they wrote. “In the restrictive and global comparisons, only 3% and 1.6% of the comparisons were significantly different, respectively.”
The fact that transmission is mainly via aerosols that build-up in the air of a room means that keeping a physical distance from people makes little difference to risk. A study from MIT used a model of viral dynamics to show that physical distancing makes no significant difference to transmission risk in indoor spaces.
Social distancing doesn’t have a significant impact on infections or deaths for a number of reasons.
Firstly, much of the spread, especially which leads to serious infection and death, is nosocomial, i.e., it occurs in care homes and hospitals. According to data from the ONS, 39% of Covid deaths in England and Wales in spring 2020 were care home residents. According to Public Health Scotland, between half and two thirds of serious Covid infections during the winter were picked up in hospital.
Second, not everyone is staying at home, even when they’re unwell. ONS figures show that nearly half of people in the U.K. travelled to work during the January lockdown. A major survey from King’s College London found that less than half of those with symptomatic Covid fully self-isolated during their infectious period.
Because social distancing does not significantly suppress viral spread, there is no reason to expect a large new wave of infections when social distancing practices are eased or ended. This aligns with the experience of states in the U.S. such as Florida, Texas and South Dakota which ended restrictions or never imposed them and did not experience noticeably worse outcomes than states which maintained them.

Are lockdowns harmful?
Lockdowns are extremely harmful to human health and well-being, leading to large reductions in access to healthcare, education and sources of social support, and considerable reductions in economic activity resulting in large-scale losses of earnings and livelihoods.
A U.K. Government report estimated that the first lockdown would kill at least 63,000 people through missed medical care and worsened economic conditions. It argued this loss of life was justified because COVID-19 was predicted to kill directly up to 1.5 million people or around 2.2% of the population. However, this figure is many times higher than the death toll in any country on earth no matter how lax its response. The worst affected country as of May 8th 2021, Hungary, has lost less than 0.3% of its population with COVID-19 according to official data. Sweden, with looser restrictions, has lost less than 0.14%.
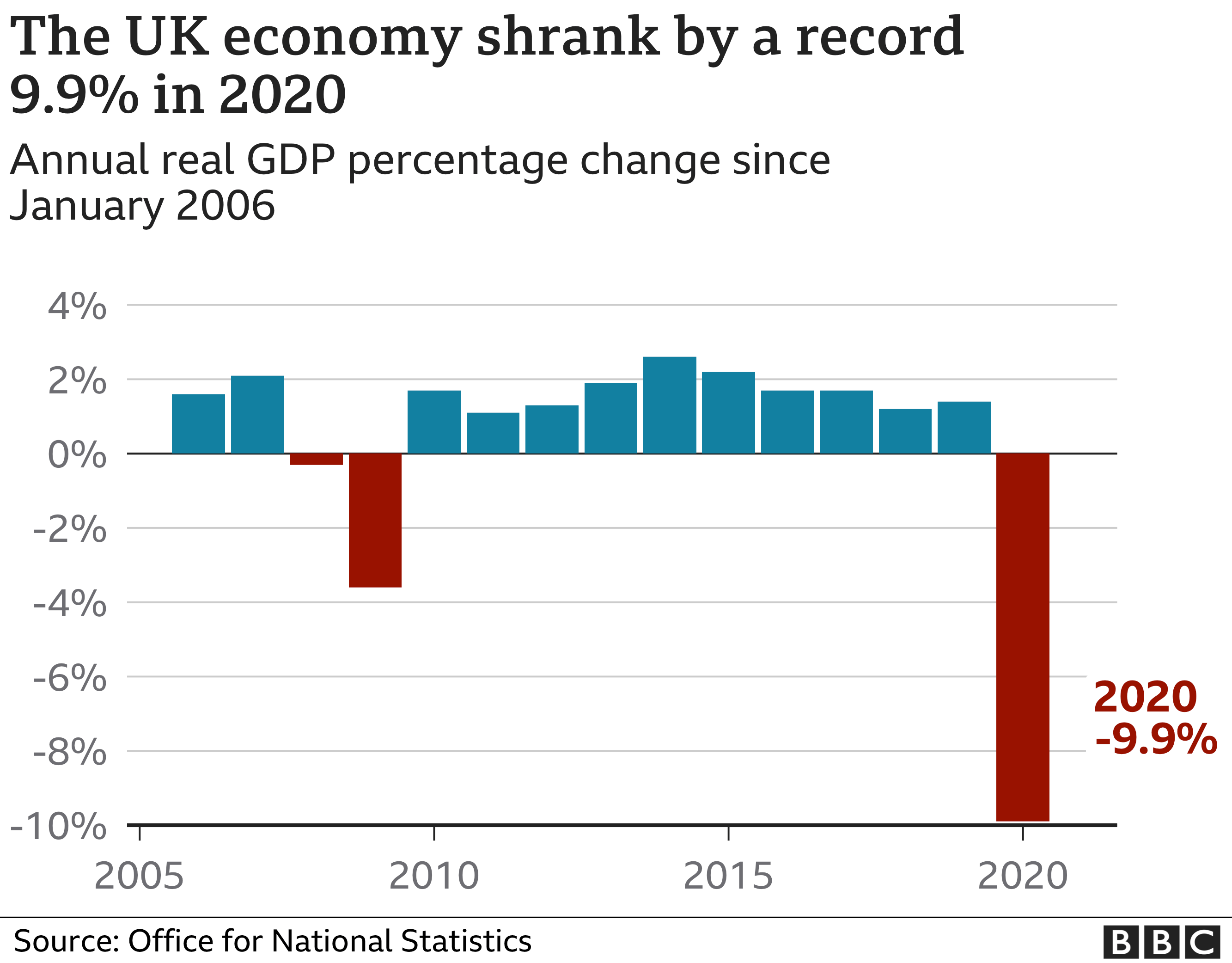
The UK economy shrank by almost 10% in 2020, the largest annual fall on record.
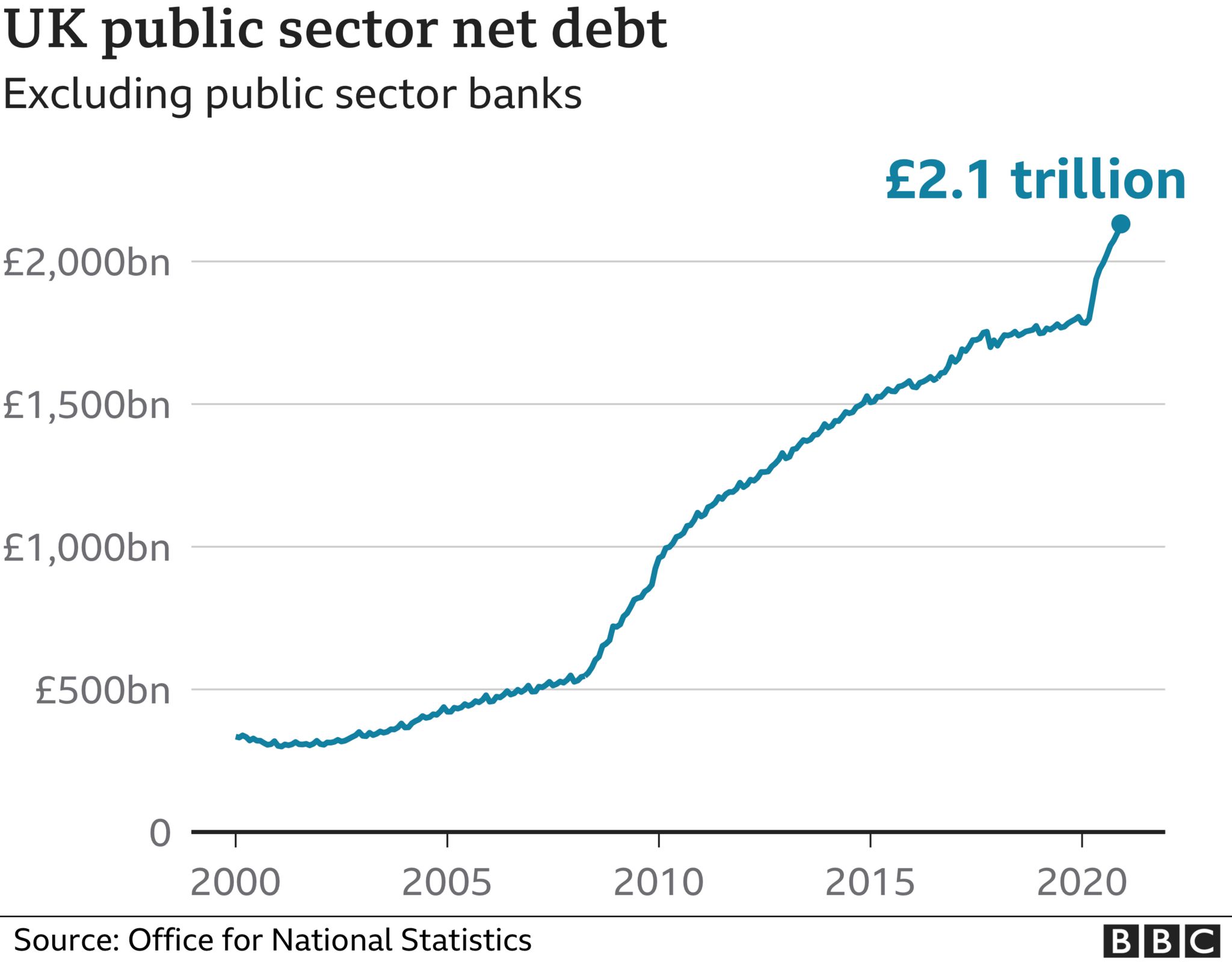
UK national debt has also jumped considerably during the pandemic to £2.1 trillion.
Lockdowns take a toll on mental health. The ONS estimates that the proportion of UK adults experiencing some form of depression is “more than double” what it was before the pandemic, increasing from 10% in 2019 to 21% in 2020.
The United Nations has estimated that disruption in healthcare services caused by government responses to COVID-19 in Afghanistan, Nepal, Bangladesh, India, Pakistan and Sri Lanka (home to some 1.8 billion people) may have led to 239,000 maternal and child deaths. Of these, an estimated 228,000 were children under five, who are at very low risk from the virus.
The United Nations has also estimated that an additional 207 million people could be pushed into extreme poverty over the next decade due to the long term impact of lockdowns.
A website has been created by the signatories of the Great Barrington Declaration to document some of the harms of lockdowns called Collateral Global.
Are the vaccines effective?
The vaccines, particularly the mRNA vaccines such as Pfizer’s, appear to be effective at preventing COVID-19 infection. They succeed in producing antibodies to SARS-CoV-2. They appear to give a level of protection comparable to that provided by infection (80-90%). A Public Health England study suggested they cut transmission rates in half after one dose.
However, among those groups who are most vulnerable to the virus they appear to be significantly less effective. A Danish study in nursing homes found that the Pfizer vaccine (often the best performing vaccine) was reduced to 64% effectiveness at preventing COVID-19 among fully vaccinated care home residents. A German study found a third of those over 80 fully vaccinated with the Pfizer jab did not generate antibodies.
Some coronavirus variants are showing signs of partial escape from vaccine-induced immunity. The AstraZeneca vaccine, for example, was found to be only 21.9% effective against the South African variant. The need for regular boosters tailored to new variants has been suggested.
Are the vaccines safe?
A number of safety concerns have been raised about the vaccines, some of which have led to some of the vaccines being restricted or removed in some countries.
The U.S. vaccine adverse effects reporting system (VAERS) has generated reports of deaths linked with Covid vaccinations at a rate 30 times greater than with flu vaccinations (although the number of deaths associated with flu vaccines is very low). Hundreds of serious adverse reactions have been reported in the UK.
A major study in the UK reported “an abundance of patients admitted to hospital within seven days of vaccination”.
The vaccines involve using genetic instructions to induce the body to produce the virus’s spike protein. However, there are concerns that the spike protein is itself pathogenic. One study reported that: ”The SARS-CoV-2 spike protein (without the rest of the viral components) triggers cell signalling events that may promote pulmonary vascular remodelling and pulmonary arterial hypertension as well as possibly other cardiovascular complications.” The spike protein by itself was shown to harm the lungs of mice.
There is also evidence that a Covid vaccination programme can cause a spike in infections. The association of vaccination programmes and Covid surges in a number of countries has been discussed in the pages of the BMJ. Dr. Clare Craig has argued against it being behaviour based (people letting their guard down) and pointed to the results from the vaccine trials which showed a reduction in white blood cells in the days following the jab that may indicate temporary immune suppression.

The risk-benefit calculation for Covid vaccination has been acknowledged by leading figures including Chief Medical Officer Chris Whitty to be different for those who are at lower risk from the disease, particularly the young. In the U.K., the AstraZeneca vaccine is no longer recommended for those under 40.
Do masks work?
Because transmission of COVID-19 is primarily via aerosols building up in the air of indoor spaces, face masks have little to no impact on risk of infection or transmission. This is because even surgical masks do not filter out enough infected aerosols to be considered respiratory protection devices. In addition, aerosols routinely escape with breath around the sides of the mask.
Accordingly, studies consistently find no significant benefit from wearing masks. The Danmask-19 randomised controlled trial (RCT) found that surgical masks provide no significant protection for the wearer from COVID-19 infection. This is in line with other RCTs for other similar viruses. One, published in autumn 2020, concluded face masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection”.
The Government’s scientific advisers admit masks are little use to the wearer, saying they “may provide a small amount of protection to an uninfected wearer; however, this is not their primary intended purpose”. Rather they are “predominantly a source control” (preventing transmission). The advisers cite the findings of a study by Brainard et al, which reviews a number of RCTs and concludes surgical masks provide the wearer with protection from just 6% of infections. The same study’s review of RCTs for masks as source control finds no evidence above low quality.
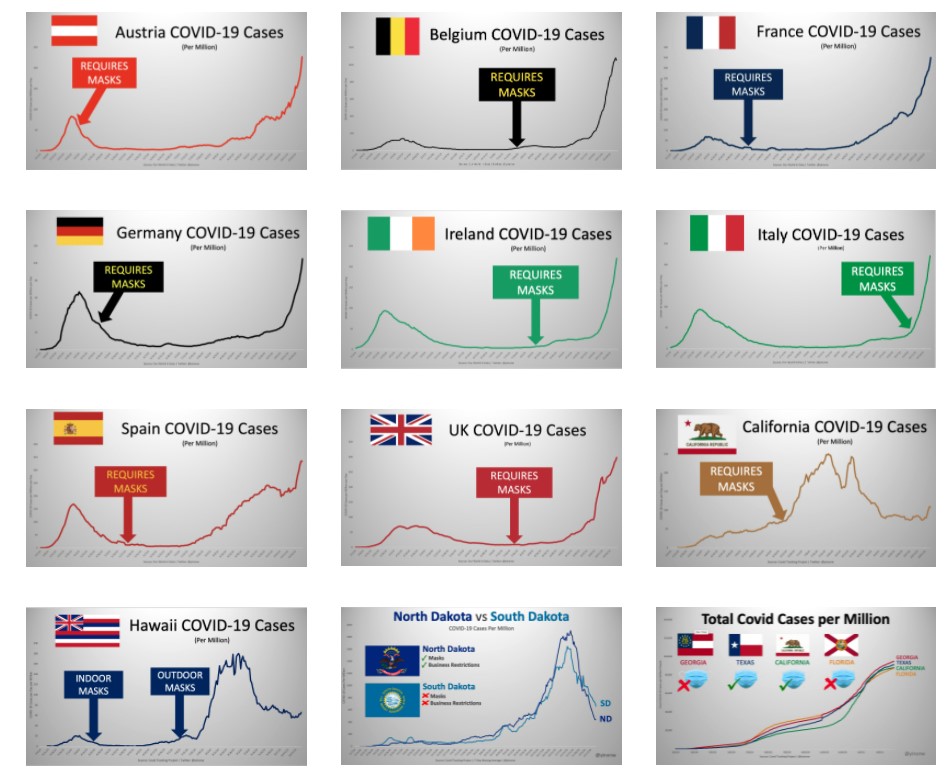
Yinon Weiss has plotted real-world data to show there is no sign of mask mandates altering the course or size of Covid epidemics in countries and states around the world.
Are masks safe?
A number of studies raise concerns about the safety of face masks used daily and for long periods.
A study in Water Research has called for a “full investigation” into the safety of face masks, after detecting easily detached particles of microplastics and heavy metals. “The toxicity of some of the chemicals found and the postulated risks of the rest of the present particles and molecules, raises the question of whether DPFs [disposable plastic face masks] are safe to be used on a daily basis.”

Professor Michael Braungart, head of the Hamburg Environmental Institute, has warned: “Many of them are made of polyester, so you have a microplastic problem. If I have the mask in front of my face, then of course I inhale the microplastic directly and these substances are much more toxic than if you swallow them, as they get directly into the nervous system,”
The World Health Organisation highlights a number of potential harms and risks of prolonged mask use in its guidance, including contamination, skin lesions and headaches.
A study in Clinical Research in Cardiology, “Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity“, finds significant impact on lung function from wearing a mask during exercise: “The pulmonary function parameters were significantly lower with mask… the ventilation was significantly reduced with both face masks… Peak blood lactate response was reduced with mask. … Participants reported consistent and marked discomfort wearing the masks.”
Face masks have been found to be a transmission risk, with infectious virus remaining on the mask for several days.
There are also important psychological consequences from frequent and widespread mask wearing.
Are effective treatments available?
A number of treatments have been used by clinicians around the world that appear to have some beneficial impact on treating COVID-19. Among the most promising are Ivermectin, as detailed in the American Journal of Therapeutics, and Budesonide, as detailed in the Lancet. The safety profile of these well-established drugs is well-known and not controversial.
What should governments have done?
The UK Government has a Pandemic Preparedness Strategy, drafted in 2011 in line with international ethical norms and scientific evidence. It is primarily for an influenza pandemic, but also envisages a SARS-like pandemic and anticipates up to 315,000 deaths, most in the space of a few weeks. It primarily recommends hand hygiene and self-isolation of the infected. It does not recommend school closures, border closures, business closures, face masks in the community or bans on large gatherings. It aims to encourage “business as usual”, stating:
During a pandemic, the Government will encourage those who are well to carry on with their normal daily lives for as long and as far as that is possible, whilst taking basic precautions to protect themselves from infection and lessen the risk of spreading influenza to others. The UK Government does not plan to close borders, stop mass gatherings or impose controls on public transport during any pandemic. …
Large public gatherings or crowded events where people may be in close proximity are an important indicator of ‘normality’ and may help maintain public morale during a pandemic. The social and economic consequences of advising cancellation or postponement of large gatherings are likely to be considerable for event organisers, contributors and participants.
The Government should have followed this strategy, as it was doing until around March 16th 2020, and not been pressured into deviating from it. It should have recognised that no pandemic has caused elevated mortality for more than a year or two and maintained a sense of proportion.
That said, the strategy is notably silent on the role of hospitals and care homes in spreading the virus (nosocomial spread). It includes no special provisions for protecting care home residents, hospital patients, or any other vulnerable category. It could therefore be improved by considering how focused protection, as advocated in the Great Barrington Declaration, could reduce deaths among the vulnerable. It could also give more consideration to how infected patients could be more effectively isolated from uninfected patients in hospitals.
It should also place more emphasis on quickly finding effective treatments besides vaccines, especially repurposed drugs which are readily available and whose safety profile is known.
Dr Mike Yeadon – “Please warn everyone not to go near top-up vaccines”
THE DAILY EXPOSE • MAY 9, 2021
We spoke to Dr Mike Yeadon about his views on the experimental Covid-19 vaccines, the medicine regulators approving them and his fears for the future.
From the outset, Dr. Yeadon said “I’m well aware of the global crimes against humanity being perpetrated against a large proportion of the worlds population.
“I feel great fear, but I’m not deterred from giving expert testimony to multiple groups of able lawyers like Rocco Galati in Canada and Reiner Fuellmich in Germany.
“I have absolutely no doubt that we are in the presence of evil (not a determination I’ve ever made before in a 40-year research career) and dangerous products.
“In the U.K., it’s abundantly clear that the authorities are bent on a course which will result in administering ‘vaccines’ to as many of the population as they can. This is madness, because even if these agents were legitimate, protection is needed only by those at notably elevated risk of death from the virus. In those people, there might even be an argument that the risks are worth bearing. And there definitely are risks which are what I call ‘mechanistic’: inbuilt in the way they work.
“But all the other people, those in good health and younger than 60 years, perhaps a little older, they don’t perish from the virus. In this large group, it’s wholly unethical to administer something novel and for which the potential for unwanted effects after a few months is completely uncharacterized.
“In no other era would it be wise to do what is stated as the intention.
“Since I know this with certainty, and I know those driving it know this too, we have to enquire: What is their motive?
“While I don’t know, I have strong theoretical answers, only one of which relates to money and that motive doesn’t work, because the same quantum can be arrived at by doubling the unit cost and giving the agent to half as many people. Dilemma solved. So it’s something else. Appreciating that, by entire population, it is also intended that minor children and eventually babies are to be included in the net, and that’s what I interpret to be an evil act.
“There is no medical rationale for it. Knowing as I do that the design of these ‘vaccines’ results, in the expression in the bodies of recipients, expression of the spike protein, which has adverse biological effects of its own which, in some people, are harmful (initiating blood coagulation and activating the immune ‘complement system’), I’m determined to point out that those not at risk from this virus should not be exposed to the risk of unwanted effects from these agents.”
The Israel Supreme Court decision last week cancelling COVID flight restrictions said: “In the future, any new restrictions on travel into or out of Israel need, in legal terms, a comprehensive, factual, data-based foundation.”
In a talk you gave four months ago, you said –
“The most likely duration of immunity to a respiratory virus like SARS CoV-2 is multiple years. Why do I say that? We actually have the data for a virus that swept through parts of the world seventeen years ago called SARS, and remember SARS CoV-2 is 80% similar to SARS, so I think that’s the best comparison that anyone can provide.
“The evidence is clear: These very clever cellular immunologists studied all the people they could get hold of who had survived SARS 17 years ago. They took a blood sample, and they tested whether they responded or not to the original SARS and they all did; they all had perfectly normal, robust T cell memory. They were actually also protected against SARS CoV-2, because they’re so similar; it’s cross immunity.
“So, I would say the best data that exists is that immunity should be robust for at least 17 years. I think it’s entirely possible that it is lifelong. The style of the responses of these people’s T cells were the same as if you’ve been vaccinated and then you come back years later to see if that immunity has been retained. So I think the evidence is really strong that the duration of immunity will be multiple years, and possibly lifelong.”
In other words, previous exposure to SARS – that is, a variant similar to SARS CoV-2 – bestowed SARS CoV-2 immunity.
The Israel government cites new variants to justify lockdowns, flight closures, restrictions, and Green Passport issuance. Given the Supreme Court verdict, do you think it may be possible to preempt future government measures with accurate information about variants, immunity, herd immunity, etc. that could be provided to the lawyers who will be challenging those future measures?
Yeadon: “What I outlined in relation to immunity to SARS is precisely what we’re seeing with SARS-CoV-2.The study is from one of the best labs in their field.” So, theoretically, people could test their T-cell immunity by measuring the responses of cells in a small sample of their blood. There are such tests, they are not “high throughput” and they are likely to cost a few hundred USD each on scale. But not thousands. The test I’m aware of is not yet commercially available, but research only in U.K.
“However, I expect the company could be induced to provide test kits “for research” on scale, subject to an agreement. If you were to arrange to test a few thousand non vaccinated Israelis, it may be a double edged sword. Based on other countries experiences, 30-50% of people had prior immunity & additionally around 25% have been infected & are now immune.
“Personally, I wouldn’t want to deal with the authorities on their own terms: that you’re suspected as a source of infection until proven otherwise. You shouldn’t need to be proving you’re not a health risk to others. Those without symptoms are never a health threat to others. And in any case, once those who are concerned about the virus are vaccinated, there is just no argument for anyone else needing to be vaccinated.”
My understanding of a “leaky vaccine” is that it only lessens symptoms in the vaccinated, but does not stop transmission; it therefore allows the spread of what then becomes a more deadly virus.
For example, in China they deliberately use leaky Avian Flu vaccines to quickly cull flocks of chicken, because the unvaccinated die within three days. In Marek’s Disease, from which they needed to save all the chickens, the only solution was to vaccinate 100% of the flock, because all unvaccinated were at high risk of death. So how a leaky vax is utilized is intention-driven, that is, it is possible that the intent can be to cause great harm to the unvaccinated.
Stronger strains usually would not propagate through a population because they kill the host too rapidly, but if the vaccinated experience only less-serious disease, then they spread these strains to the unvaccinated who contract serious disease and die.
Do you agree with this assessment? Furthermore, do you agree that if the unvaccinated become the susceptible ones, the only way forward is HCQ prophylaxis for those who haven’t already had COVID-19?
Would the Zelenko Protocol work against these stronger strains if this is the case? And if many already have the aforementioned previous “17-year SARS immunity”, would that then not protect from any super-variant?
“I think the Gerrt Vanden Bossche story is highly suspect. There is no evidence at all that vaccination is leading or will lead to ‘dangerous variants’. I am worried that it’s some kind of trick.
“As a general rule, variants form very often, routinely, and tend to become less dangerous & more infectious over time, as it comes into equilibrium with its human host. Variants generally don’t become more dangerous.
“No variant differs from the original sequence by more than 0.3%. In other words, all variants are at least 99.7% identical to the Wuhan sequence.
“It’s a fiction, and an evil one at that, that variants are likely to “escape immunity.”
“Not only is it intrinsically unlikely – because this degree of similarity of variants means zero chance that an immune person (whether from natural infection or from vaccination) will be made ill by a variant – but it’s empirically supported by high-quality research.
“The research I refer to shows that people recovering from infection or who have been vaccinated ALL have a wide range of immune cells which recognize ALL the variants.
“This paper shows WHY the extensive molecular recognition by the immune system makes the tiny changes in variants irrelevant.
“I cannot say strongly enough: The stories around variants and need for top up vaccines are FALSE. I am concerned there is a very malign reason behind all this. It is certainly not backed by the best ways to look at immunity. The claims always lack substance when examined, and utilize various tricks, like manipulating conditions for testing the effectiveness of antibodies. Antibodies are probably rather unimportant in host protection against this virus. There have been a few ‘natural experiments’, people who unfortunately cannot make antibodies, yet are able quite successfully to repel this virus. They definitely are better off with antibodies than without. I mention these rare patients because they show that antibodies are not essential to host immunity, so some contrived test in a lab of antibodies and engineered variant viruses do NOT justify need for top up vaccines.
“The only people who might remain vulnerable and need prophylaxis or treatment are those who are elderly and/or ill and do not wish to receive a vaccine (as is their right).
“The good news is that there are multiple choices available: hydroxychloroquine, ivermectin, budesonide (inhaled steroid used in asthmatics), and of course oral Vitamin D, zinc, azithromycin etc. These reduce the severity to such an extent that this virus did not need to become a public health crisis.”
Do you feel the MHRA does a good job regulating ‘big pharma’? In what ways does ‘big pharma’ get around the regulator? Do you feel they did so for the mRNA jab?
“Until recently, I had high regard for global medicines regulators. When I was in Pfizer, and later CEO of a biotech I founded (Ziarco, later acquired by Novartis), we interacted respectfully with FDA, EMA, and the MHRA.
Always good quality interactions.
“Recently, I noticed that the Bill & Melinda Gates Foundation (BMGF) had made a grant to the Medicines and Healthcare products Regulatory Agency (MHRA)! Can that ever be appropriate? They’re funded by public money. They should never accept money from a private body.
“So here is an example where the U.K. regulator has a conflict of interest.” The European Medicines Agency failed to require certain things as disclosed in the ‘hack’ of their files while reviewing the Pfizer vaccine.
“You can find examples on Reiner Fuellmich’s “Corona Committee” online.
“So I no longer believe the regulators are capable of protecting us. ‘Approval’ is therefore meaningless.
“Dr. Wolfgang Wodarg and I petitioned the EMA Dec 1, 2020 on the genetic vaccines. They ignored us.
“Recently, we wrote privately to them, warning of blood clots, they ignored us. When we went public with our letter, we were completely censored. Days later, more than ten countries paused use of a vaccine citing blood clots.
“I think the big money of pharma plus cash from BMGF creates the environment where saying no just isn’t an option for the regulator.
“I must return to the issue of ‘top up vaccines’ (booster shots) and it is this whole narrative which I fear will he exploited and used to gain unparalleled power over us.
“PLEASE warn every person not to go near top up vaccines. There is absolutely no need to them. As there’s no need for them, yet they’re being made in pharma, and regulators have stood aside (no safety testing), I can only deduce they will be used for nefarious purposes.
“For example, if someone wished to harm or kill a significant proportion of the worlds population over the next few years, the systems being put in place right now will enable it.
“It’s my considered view that it is entirely possible that this will be used for massive-scale depopulation.”
Update on ivermectin for covid-19
By Sebastian Rushworth, M.D. | May 9, 2021
Back in January I wrote an article about four randomized controlled trials of ivermectin as a treatment for covid-19 that had at that time released their results to the public. Each of those four trials had promising results, but each was also too small individually to show any meaningful impact on the hard outcomes we really care about, like death. When I meta-analyzed them together however, the results suddenly appeared very impressive. Here’s what that meta-analysis looked like:

It showed a massive 78% reduction in mortality in patients treated with covid-19. Mortality is the hardest of hard end points, which means it’s the hardest for researchers to manipulate and therefore the least open to bias. Either someone’s dead, or they’re alive. End of story.
You would have thought that this strong overall signal of benefit in the midst of a pandemic would have mobilized the powers that be to arrange multiple large randomized trials to confirm these results as quickly as possible, and that the major medical journals would be falling over each other to be the first to publish these studies.
That hasn’t happened.
Rather the opposite, in fact. South Africa has even gone so far as to ban doctors from using ivermectin on covid-19 patients. And as far as I can tell, most of the discussion about ivermectin in mainstream media (and in the medical press) has centred not around its relative merits, but more around how its proponents are clearly deluded tin foil hat wearing crazies who are using social media to manipulate the masses.
In spite of this, trial results have continued to appear. That means we should now be able to conclude with even greater certainty whether or not ivermectin is effective against covid-19. Since there are so many of these trials popping up now, I’ve decided to limit the discussion here only to the ones I’ve been able to find that had at least 150 participants, and that compared ivermectin to placebo (although I’ll add even the smaller trials I’ve found in to the updated meta-analysis at the end).
As before, it appears that rich western countries have very little interest in studying ivermectin as a treatment for covid. The three new trials that had at least 150 participants and compared ivermectin with placebo were conducted in Colombia, Iran, and Argentina. We’ll go through each in turn.
The Colombian trial (Lopez-Medina et al.) was published in JAMA (the Journal of the American Medical Association) in March. There is one thing that is rather odd with this study, and that is that the study authors were receiving payments from Sanofi-Pasteur, Glaxo-Smith-Kline, Janssen, Merck, and Gilead while conducting the study. Gilead makes remdesivir. Merck is developing two expensive new drugs to treat covid-19. Janssen, Glaxo-Smith-Kline, and Sanofi-Pasteur are all developers of covid vaccines. In other words, the authors of the study were receiving funding from companies that own drugs that are direct competitors to ivermectin. One might call this a conflict of interest, and wonder whether the goal of the study was to show a lack of benefit. It’s definitely a little bit suspicious.
Anyway, let’s get to what the researchers actually did. This was a double-blind randomized controlled trial that recruited patients with mildly symptomatic covid-19 who had experienced symptom onset less than 7 days earlier. Potential participants were identified through a statewide database of people with positive PCR-tests. By “mildly symptomatic” the researchers meant people who had at least one symptom but who did not require high-flow oxygen at the time of recruitment in to the trial.
Participants in the treatment group received 300 ug/kg body weight of ivermectin every day for five days, while participants in the placebo group received an identical placebo. 300 ug/kg works out to 21 mg for an average 70 kg adult, which is quite high, especially when you consider that the dose was given daily for five days. For an average person, this would work out to a total dose of 105 mg. The other ivermectin trials have mostly given around 12 mg per day for one or two days, for a total dose of 12 to 24 mg (which has been considered enough because ivermectin has a long half-life in the body). Why this study gave such a high dose is unclear. However, it shouldn’t be a problem. Ivermectin is a very safe drug, and studies have been done where people have been given ten times the recommended dose without any noticeable increase in adverse events.
The stated goal of the study was to see if ivermectin resulted in more rapid symptom resolution than placebo. So participants were contacted by telephone every three days after inclusion in the study, up to day 21, and asked about what symptoms they were experiencing.
398 patients were included in the study. The median age of the participants was 37 years, and they were overall very healthy. 79% had no known co-morbidities. This is a shame. It means that this study is yet another one of those many studies that will not be able to show a meaningful effect on hard end points like hospitalization and death. It is a bit strange that studies keep being done on young healthy people who are at virtually zero risk from covid-19, rather than on the multi-morbid elderly, who are the ones we actually need an effective treatment for.
Anyway, let’s get to the results.
In the group treated with ivermectin, the average time from inclusion in the study to becoming completely symptom free was 10 days. In the placebo group that number was 12 days. So, the ivermectin treated patients recovered on average two days faster. However, the difference was not statistically significant, so the result could easily be due to chance. At 21 days after inclusion in the study, 82% had recovered fully in the ivermectin group, as compared to 79% in the placebo group. Again, the small difference was not statistically significant.
In terms of the hard end points that matter more, there were zero deaths in the ivermectin group and there was one death in the placebo group. 2% of participants in the ivermectin group required “escalation of care” (hospitalization if they were outside the hospital at the start of the study, or oxygen therapy if they were in hospital at the start of the study) as compared with 5% in the placebo group. None of these differences was statistically significant. But that doesn’t mean they weren’t real. Like I wrote earlier, the fact that this was a study of healthy young people meant that, even if a meaningful difference does exist in risk of dying of covid, or of ending up in hospital, this study was never going to find it.
So, what can we conclude?
Ivermectin does not meaningfully shorten duration of symptoms in healthy young people. That’s about all we can say from this study. Considering the conflicts of interest of the authors, my guess is that this was the goal of the study all along: Gather together a number of young healthy people that is too small for there to be any chance of a statistically significant benefit, and then get the result you want. The media will sell the result as “study shows ivermectin doesn’t work” (which they dutifully did).
It is interesting that there were signals of benefit for all the parameters the researchers looked at (resolution of symptoms, escalation of care, death), but that the relatively small number and good health status of the participants meant that there was little chance of any of the results reaching statistical significance.
Let’s move on to the next study, which is currently available as a pre-print on Research Square (Niaee et al.). It was randomized, double-blind, and placebo-controlled, and carried out at five different hospitals in Iran. It was funded by an Iranian university.
In order to be included in the trial, participants had to be over the age of 18 and admitted to hospital because of a covid-19 infection (which was defined as symptoms suggestive of covid plus either a CT scan typical of covid infection or a positive PCR test).
150 participants were randomized to either placebo (30 people) or varying doses of ivermectin (120 people). The fact that they chose to make the placebo group so small is a problem, because it makes it very hard to detect any differences even if they do exist, by making the statistical certainty of the results in the placebo group very low.
The participants were on average 56 years old and the average oxygen saturation before initiation of treatment was 89% (normal is more than 95%), so this was a pretty sick group. Unfortunately no information is provided on how far along people were in the disease course when they started receiving ivermectin. It stands to reason that the drug is more likely to work if given ten days after symptom onset than when given twenty days after symptom onset, since death usually happens around day 21. If you, for example, wanted to design a trial to fail, you could start treating people at a time point when there is no time for the drug you’re testing to have a chance work, so it would have been nice to know at what time point treatment started in this trial.
So, what were the results?
20% of the participants in the placebo group died (6 out of 30 people). 3% of the participants in the various ivermectin groups died (4 out of 120 people). That is an 85% reduction in the relative risk of death, which is huge.
So, in spite of the fact that the placebo group was so small, it was still possible to see a big difference in mortality. Admittedly, this is a pre-print (i.e. it hasn’t been peer-reviewed yet), and the absolute numbers of deaths are small, so there is some scope for random chance to have created these results (maybe people in the placebo group were just very unlucky!). However, the study appears to have followed all the steps expected for a high quality trial. It was carried out at multiple different hospitals, it used randomization and a control group that received a placebo, and it was double-blinded. And death is a very hard end point that is not particularly open to bias. So unless the researchers have falsified their data, then this study constitutes reasonably good evidence that ivermectin is highly effective when given to patients hospitalized with covid-19. That’s great, because it would mean that the drug can be given quite late in the disease course and still show benefit.
Let’s move on to the third trial (Chahla et al.), which is currently available as a pre-print on MedRxiv. It was carried out in Argentina, and funded by the Argentinean government. Like the first trial we discussed, this was a study of people with mild disease. It literally boggles my mind that so many researchers choose to study people with mild disease instead of studying those with more severe disease. Especially when you consider that these studies are all so small. A study of people with mild disease needs to be very large to find a statistically significant effect, since most people with covid do well regardless. The risk of false negative results is thus enormous. If you’re going to do a small-ish study, and you want to have a reasonable chance of producing results that reach statistical significance, it would make much more sense to do it on sick hospitalized patients.
The study was randomized, but it wasn’t blinded, and there was no placebo. In other words, the intervention group received ivermectin (24 mg per day), while the control group didn’t receive anything. This is a bad bad thing. It means that any non-hard outcomes produced by the study are really quite worthless, since there is so much scope for the placebo effect and other confounding factors to mess up the results. For hard outcomes, in particular death, it should be less of a problem (although we wouldn’t expect any deaths in such a small study of mostly healthy people with mild disease anyway).
The study included people over the age of 18 with symptoms suggestive of covid-19 and a positive PCR test. The average age of the participants was 40 years, and most had no underlying health issues. A total of 172 people were recruited in to the study.
The researchers chose to look at how quickly people became free of symptoms as their primary endpoint. This is enormously problematic, since the study, as already mentioned, wasn’t blinded and there was no placebo. Any difference between the groups could easily be explained by the placebo effect and by biases towards treatment benefit among the researchers.
Anyway, the study found that 49% in the treatment group were free of symptoms at five to nine days after the beginning of treatment, compared with 81% in the control group. However, the lack of blinding means that this result is worthless. The methodology is just too flawed.
No data is provided on the number of people who died in each group. Since it isn’t reported, I think it’s safe to assume that there were no deaths in either group. Nor is any data provided on the number of hospitalizations in each group.
So, what does this study tell us?
Absolutely nothing at all. What a waste of time and money.
Let’s move on and update our meta-analysis. The reason we need to do a meta-analysis here is that none of the trials of ivermectin is large enough on its own to provide a definitive answer as to whether it is a useful treatment for covid-19 or not. For those who haven’t heard of meta-analyses before, basically what you do is just take the results from all different studies in existence that fulfill your pre-selected criteria, and then put them together, so as a to create a single large “meta”-study. This allows you to produce results that have a much higher level of statistical significance. It is particularly useful in a situation where all the individual trials you have to work with are statistically underpowered (have too few participants), as is the case here.
In this new meta-analysis, I’ve included every double-blind randomized placebo-controlled trial I could find of ivermectin as a treatment for covid. Using only double-blind placebo-controlled trials means that only the highest quality studies are included in this meta-analysis, which minimizes the risk of biases messing up the results as far as possible. In order to be included, a study also had to provide mortality data, since the goal of the meta-analysis is to see if there is any difference in mortality.
I was able to identify seven trials that fulfilled these criteria, with a total of 1,327 participants. Here’s what the meta-analysis shows:

What we see is a 62% reduction in the relative risk of dying among covid patients treated with ivermectin. That would mean that ivermectin prevents roughly three out of five covid deaths. The reduction is statistically significant (p-value 0,004). In other words, the weight of evidence supporting ivermectin continues to pile up. It is now far stronger than the evidence that led to widespred use of remdesivir earlier in the pandemic, and the effect is much larger and more important (remdesivir was only ever shown to marginally decrease length of hospital stay, it was never shown to have any effect on risk of dying).
I understand why pharmaceutical companies don’t like ivermectin. It’s a cheap generic drug. Even Merck, the company that invented ivermectin, is doing it’s best to destroy the drug’s reputation at the moment. This can only be explained by the fact that Merck is currently developing two expensive new covid drugs, and doesn’t want an off-patent drug, which it can no longer make any profit from, competing with them.
The only reason I can think to understand why the broader medical establishment, however, is still so anti-ivermectin is that these studies have all been done outside the rich west. Apparently doctors and scientists outside North America and Western Europe can’t be trusted, unless they’re saying things that are in line with our pre-conceived notions.
Researchers at McMaster university are currently organizing a large trial of ivermectin as a treatment for covid-19, funded by the Bill and Melinda Gates foundation. That trial is expected to enroll over 3,000 people, so it should be definitive. It’s going to be very interesting to see what it shows when the results finally get published.
Texas Medical Doctors Testify Before State Senate to Oppose Mandatory COVID Shots
By Brian Shilhavy | Health Impact News | May 8, 2021
This past week the Texas Senate Committee on State Affairs took testimony from Texas physicians regarding SB 1669: Stop Forced Vaccination and Vaccine Passports in Texas.
SB 1669 was sponsored by Senator Bob Hall.

You can learn more about this bill at the National Vaccine Information Center’s Advocacy Portal (registration required.)
Here is some of the text provided to the public regarding Senate Bill 1669:
Contact your Texas State Legislators and Demand No Forced Vaccination, No Vaccine Passports, No Exceptions – Support SB 1669
Mandated vaccination in Texas with COVID-19 vaccines will be the reality unless the legislature takes decisive action now. In fact, it has already started happening.
Houston Methodist Hospital has told its 26,000 employees to get vaccinated by June 7th or get fired. Atria Senior Living, which has 16 facilities in Texas, is requiring all employees to receive 2 COVID-19 vaccines by May 1, 2021 as a condition of employment or face termination.
The city of Farmer’s Branch, Texas is requiring COVID-19 vaccination to access the city run facility called The Branch Connection. Forget taking a cruise with Royal Caribbean from Texas unless you’ve been COVID-19 vaccinated. St. Edwards University in Austin became one of the first colleges to mandate COVID-19 vaccines.
This is just the beginning.
Governor Abbott’s Executive Order Prohibiting COVID-19 Vaccine Passports Falls Short at Protection
Texas Governor Greg Abbott has been quoted saying that in Texas, COVID-19 vaccines “are always voluntary and never forced.”
The truth is Executive Order GA 35 falls short at preserving the right of law-abiding Texas citizens to be able to function normally in society without having to show proof of a COVID-19 vaccination.
EO GA 35 only prohibits the government, or public or private entities funded by the government, from requiring documentation of an individual’s COVID-19 vaccination status. This does nothing to prohibit businesses not receiving government funding from banning customers who don’t have a COVID-19 vaccine. Also, this executive order fails to give any protection to employees whose employers are requiring COVID-19 vaccination as a condition of employment.
In addition, the limited protections offered in EO GA 35 will be short lived because the order only applies to “Emergency Use Authorization” (EUA) COVID-19 vaccines. Once a vaccine has received full FDA approval, the EUA designation no longer applies and therefore neither will any protection in this executive order including the ban on forced vaccination by the government. Full FDA approval will be soon. Moderna, the manufacture of one of the 3 available COVID-19 vaccines, is already seeking full FDA approval, and Pfizer, one of the other manufacturers, announced it would seek full approval in the first half of 2021.
Governor Abbott’s executive order also falls short when compared to Florida Governor Ron DeSantis’s executive order banning vaccines passports which additionally prohibits all business from requiring COVID-19 vaccination status or post infection recovery status to gain access to or service from the business, and it applies to all COVID-19 vaccines instead of expiring after full FDA approval is achieved. It also protects personal privacy rights by prohibiting the government from publishing or sharing a person’s COVID-19 vaccination status to third parties.
Texans Need a Law Passed to Protect them From Forced Vaccination and Vaccine Passports (If you want to immediately see what you can do to help pass SB 1669 into law in Texas scroll down to “Action Needed)”
We are grateful to announce that Texas history has been made with the filing of
SB 1669 in the Texas Legislature by Senator Bob Hall.SB 1669 prohibits discrimination or segregation based on vaccination or immune status and prohibits forced vaccination in all areas of your life.
We need your help getting SB 1669 moving as the bill is currently stalled awaiting a hearing in the Senate State Affairs Committee. Legislators need to be educated about the shortcomings in Governor Abbott’s executive order and the vulnerabilities for mandated vaccination in Texas based on current law so they can pass this bill or amend parts of it onto other bills.
This is by far the most comprehensive bill prohibiting mandated vaccination in all areas that could affect your life including government orders, employment, healthcare, education, access to businesses, access to events and venues like sports and concerts, long-term care, nursing homes, insurance, and childcare.
Read more at the National Vaccine Information Center’s Advocacy Portal.
Senator Bob Hall, in his opening statements at the Senate hearing this week stated:
The chief responsibility and Constitutional role of our government is to protect the rights of the individual. Employees can take off their helmets, masks, and uniforms at the end of the work day, but they cannot remove a vaccine.

Dr. Richard Bartlett was the first physician to testify in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas.
Dr. Bartlett has over 28 years of medical practice experience and is a veteran primary care and emergency room doctor in West Texas.
Dr. Bartlett is best known since the COVID crisis started as a doctor who has cured many patients using an older, already FDA approved drug, called budesonide, which is an inhaled corticosteroid. (Learn more here.)
During his testimony, Dr. Bartlett explained that there are existing treatments already available to treat COVID patients, making it unnecessary to mandate experimental new “vaccines.”
He pointed to a recent Oxford University study just published that showed 90% success rate in using inhaled budesonide with COVID patients in preventing long-term care or hospitalization.
From the Oxford study:
The STOIC study found that inhaled budesonide given to patients with COVID-19 within seven days of the onset of symptoms also reduced recovery time. Budesonide is a corticosteroid used in the long-term management of asthma and chronic obstructive pulmonary disease (COPD).
Findings from the phase 2 randomised study, which was supported by the NIHR Oxford Biomedical Research Centre (BRC), were published on the medRxiv pre-print server.
The findings from 146 people – of whom half took 800 micrograms of the medication twice a day and half were on usual care – suggests that inhaled budesonide reduced the relative risk of requiring urgent care or hospitalisation by 90% in the 28-day study period. Participants allocated the budesonide inhaler also had a quicker resolution of fever, symptoms and fewer persistent symptoms after 28 days. (Source.)
Dr. Bartlett works in the Emergency Room, and he stated that there are very few patients coming in now with COVID, but “I am now seeing more people come in (to the ER) who are having complications from the COVID shot.”
And Dr. Bartlett points out that these are mostly younger people who were in excellent health before the shot, since Dr. Bartlett works in Lubbock, Texas, which is a college town.

Dr. Ben Edwards of Veritas Medical in Lubbock, Texas, was the next physician to give testimony in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas.
Dr. Edwards received his degree from Baylor University, and later graduated from UT-Houston Medical School. He moved to Waco to complete his training at the Waco Family Practice Residency Program where he was Chief Resident. He now operates three clinics in West Texas.
Dr. Edwards stated his concern that “the forced and coerced COVID-19 vaccinations would, in my opinion, be a violation of the Nuremberg Code,” as well as several other international codes on bioethics and human rights.
He cited the fact that the CDC is now reporting 4,178 deaths reported to VAERS, while for the previous 20 years combined there were 4,182 deaths recorded from all vaccines.
He also pointed out that a Harvard Study has previously estimated that only about 1% of all adverse reactions to vaccines are ever reported to VAERS. Two other subsequent studies showed the same thing.
In his own practice, Dr. Edwards stated that he has received “numerous reports within hours of receiving the COVID vaccines that people have suffered strokes, heart attacks, pulmonary embolisms (blood clots), and sudden death.”
Dr. Edwards went on to cite research which shows that those with natural immunity to COVID (they already had it) will see a 2 to 3 fold increase risk of adverse reactions from the COVID shots.
Over half of Texans now have this natural immunity. He stated:
On a personal note, I believe that God gave us an amazingly robust immune system, and I don’t think you can improve on God.

The next physician to testify in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas was Dr. Amy Offutt from St. Marble Falls, TX.
Dr. Offutt is trained in Integrative Medicine. She was recently appointed by Governor Greg Abbott to the Pediatric Acute-Onset Neuropsychiatric Syndrome Advisory Council. In addition, she serves on the Board of Directors for ILADS (International Lyme and Associated Diseases Society).
Dr. Offutt is another physician who has been successfully treating COVID patients with existing early treatment protocols.
She testified:
As of last Friday, my practice has treated 579 acutely ill patients as old as 98 years of age, with only ten hospitalizations and one dead.
The man who died presented on the 12th day of illness was a transplant patient and had already been to the ER multiple times before seeking care from us. This was such an unnecessary tragedy.
Dr. Offutt believes that “informed consent is the core to shared decision making in medicine.”

The next physician to testify in favor of SB 1669 to Stop Forced Vaccination and Vaccine Passports in Texas was Dr. Angelina Farella from Webster, TX.
Dr. Farella is a pediatrician with over 25 years experience. She started out her testimony to the Senate Committee by stating:
I am here today to protect our children in Texas. This is a very scary situation that we are in right now.
Dr. Farella stated that as a pediatrician she has given out tens of thousands of vaccines, and that she is not “anti-vaccine,” but:
I am against this COVID vaccine, if we can even call it that (a vaccine.)
What we are doing to our children with this vaccine is actually criminal.
All of these physicians are “frontline physicians” who actually treat patients, but their clinical experiences in treating COVID patients is being censored by the corporate media, and ignored by the government and Big Pharma, in favor mass vaccination instead.
Here is their testimony. This is from our Rumble Channel, and it is also on our Bitchute Channel.
Why are people going blind after having the Covid Vaccine?
THE DAILY EXPOSE • MAY 8, 2021
Since the first Covid-19 vaccine was authorised for use in the United Kingdom, and administered on the 8th December 2020, there have been hundreds of thousands of adverse reactions reported to the MHRA Yellow Card scheme. But there is one particular adverse reaction which is both concerning and strange, and the number of people suffering from it is increasing by the week – Blindness.
The MHRA Yellow Card scheme analysis print for the Pfizer / BioNTech mRNA jab shows that since the first jab was administered on the 9th December and up to the 28th April, thirty-three people have reported suffering blindness due to the jab. Another two people have reported central vision loss, and a further two have reported sudden visual loss.
Five people have also reported an adverse reaction known as ‘blindness transient’ due to the Pfizer vaccine. This is where a person suffers visual disturbance or loss of sight in one eye for seconds or minutes at a time. And a further six people have reported an adverse reaction known as ‘unilateral blindness’. This is where a person is blind or has extremely poor vision in one eye.

However the MHRA Yellow Card scheme analysis print for the AstraZeneca viral vector vaccine shows that recipients are at a significantly higher risk of suffering loss of vision after having the jab compared to having the Pfizer jab. Since the first AstraZeneca jab was administered on the 4th January 2021 and up to the 28th April 2021 a total of one-hundred-forty-three people have reported suffering blindness due to the jab. Another four-hundred-seventeen people have reported visual impairment, and a further three have reported sudden visual loss.
Ten people have also reported suffering transient blindness as a result of having the AstraZeneca jab, and a further thirteen have reported suffering unilateral blindness as a result of the same jab.

In all there have been 11,279 eye disorders reported as adverse reactions to both jabs, with 2,438 reported due to the Pfizer jab, and a frightening 8,841 reported due to the AstraZeneca jab. The fact-checkers alongside authorities have recently been on the case to sweep this data under the carpet and have called it unreliable. Their reasoning is that “just because someone reports the event after having the vaccine, it doesn’t necessarily mean it is due to the vaccine”.
But what they’re not telling you is that it also doesn’t necessarily mean it is not due to the vaccine, and we imagine every single person who has reported an adverse reaction would disagree with the fact checkers and authorities attempts to play down these reports. For instance one person who goes by the name of Louis has been documenting the story of his wife on Twitter since she had the AstraZeneca Covid vaccine.
Unfortunately his wife has gone completely blind in her left eye and 30-60% blind in her right eye since she had the AstraZeneca jab and the neurologist treating her has categorically told her not have the second dose. Louis states that as of the 8th May 2021 it has been 59 days since his wife had the AstraZeneca vaccine, 55 days since she went blind, 19 days since she started steroid treatment and unfortunately has seen zero improvement. In that time she has had 2 CT scans and 1 MRI. She has also seen 3 ophthalmologists, 2 opticians and had dozens of blood tests.

As you can see the misery which the fact checkers are disregarding as “not necessarily the fault of the vaccine” is very real for the people who are reporting them. But why are the Covid vaccines causing people to go blind?
Well there is another extremely concerning adverse reaction that has been reported to the MHRA Yellow Card scheme, one which has seen an astronomical increase in the number of reports in the past few weeks – stroke.
As of the 28th April 2021 the MHRA has received two-hundred-ninety-seven reports of stroke due to the Pfizer vaccine. This includes twenty-one reports of cerebral haemorrhage, 16 reports of cerebral infarction, twenty-five reports of ischaemic stroke, and a frightening 192 reports of cerebrovascular accident. Sadly this has resulted in twenty-seven deaths.

But yet again the AstraZeneca jab has caused far more misery in terms of causing a stroke compared to the Pfizer jab. As of the 28th April 2021 the MHRA Yellow Card scheme has received one-thousand-eighty-eight reports of stroke, this is almost four times the amount of reports received due to the Pfizer jab. These include eleven cerebral haematomas, forty-six cerebral infarctions, one-hundred-seven cerebral haemorrhages, and a terrifying six-hundred-seven cerebrovascular accidents.

But it doesn’t end there. The AstraZeneca jab has also caused fifteen cases of lacunar stroke, fifty-nine cases of sbarachnoid haemorrhage, and seventy-four cases of ischaemic stroke. Sadly this has resulted in eighty-five deaths.

But what does this have to do with people going blind? Well this helpful fact sheet provided by the Stroke Foundation in Australia provides the answer as to why. According to the fact sheet around one-third of stroke survivors suffer visual loss, and most sadly never fully recover their vision.
The reason strokes cause blindness is that vision depends on a healthy eye to receive information and a healthy brain to process that information. The nerves in the eye travel from the eye through the brain to the occipital cortex at the back of the brain, allowing you to see.
Most strokes affect one side of the brain. Nerves from each eye travel together in the brain, so both eyes are affected. If the right side of your brain is damaged, the left side vision in each eye may be affected. It is rare for both sides of the brain to be affected by stroke. When it does happen, it can result in blindness.
So if you’ve been wondering how on earth the experimental Covid vaccines could cause a person to go blind, you now know why. It’s the vast amount of strokes the Covid jabs are causing that is contributing to this devastating and life-changing adverse event. Strokes will not be the only contributing factor of course, but the numbers shows us they are most likely the main adverse reaction at fault.
Halt Vaccine Passports! It’s illegal, medical apartheid
By Dr Mike Yeadon | OffGuardian | May 7, 2021
It is very important that people understand what is happening here. The intention is to introduce vaccine passports everywhere. But this is a disguise. It’s a world’s first digital common-format, globally-interoperable ID system with an editable health flag (vaccinated Y or N).
It makes no one safer. If you’re vaccinated, you’re protected & are not made safer by knowing others immune status.
As in Israel, you will be compelled to present a valid VaxPass in order to access defined facilities or access services. No VaxPass, you’re denied.
This system only needs 50%+ of the adult population to start up because of its huge, coercive power on the unvaccinated.
It’s illegal, medical apartheid.
If they succeed, it won’t help you to refuse. They’ll move on, leaving that minority behind.
A VaxPass System like this will give to those controlling the database & it’s algorithms TOTALITARIAN TYRANNY over us all.
The ONLY way to stop this biosecurity nightmare is to NOT GET VACCINATED FOR NON-MEDICAL REASONS!!!
I fear that, if our adversaries gain this absolute control, they will use it to harm the population. There’s no limit to the evil which will flow from this strategic goal.
DO NOT ALLOW THIS SYSTEM TO START UP, because it’s unstoppable afterwards.
One example: your VaxPass pings, instructing you to attend for your 3rd or 4th or 5th booster or variant vaccine. If you don’t, your VaxPass will expire & you’ll become an out-person, unable to access your own life.
How much choice do you have?
It’s none. You are controlled. Forever.
PLEASE share this widely, on every platform you use.
Thank you,
Dr Mike Yeadon
Acclaimed Swedish Hospital Stops Irreversible Hormone Treatment of Minors
By Igor Kuznetsov – Sputnik – 07.05.2021
Karolinska University Hospital in Stockholm, one of Sweden’s largest medical institutions, is now terminating its controversial irreversible hormone treatments for minors suffering from ‘gender dysphoria’, that is, being born into the ‘wrong sex’, national broadcaster SVT reported.
In its updated guidelines that came into force at the start of May, the acclaimed hospital called these treatments controversial and suggested that they involve risks.
Previously, Karolinska University Hospital became the first in Sweden to offer gender identity investigations for children and young people. The special department opened in 2000 and over 700 young people have since been investigated for gender dysphoria. The diagnosed patients were able to receive hormone treatment at Karolinska Hospital.
Previously, the practice of hormone treatment had fallen under scrutiny, not least from SVT’s team for investigative journalism that highlighted the risks associated with this practice, as well as its irreversible health effects. SVT also reported an “explosive” increase in adolescents undergoing gender reassignment amid other conditions such as depression and eating disorders.
Yet another problem associated with the so-called “regretters” who have second thoughts about the “gender-confirming” treatment afterwards.
“Healthcare does not know what they are doing. They have no science behind this. They are experimenting on a young generation that has their whole life ahead of them. I don’t know of any other area in medicine where a treatment is tried in this way,” one of patients who lives with irreversible consequences of hormone treatment told SVT.

Karolinska’s Per-Anders Rydelius previously defended the treatment by claiming that it follows investigation models and is by no means experimental.
However, Karolinska’s updated guidelines now describe a plethora of side effects: cardiovascular disease, osteoporosis, infertility, cancer and thrombosis. The hospital also emphasised the low evidence of achieving the desired effect and that there is very little knowledge about safety in the long term.
The new guidelines imply that no new minors will receive hormone treatment, other than within the framework of clinical studies. For patients already undergoing treatment, physicians should make a “careful individual assessment of whether treatment should be continued or discontinued”.
This step was welcomed by, among others, Emelie Köhler, the co-founder of detransinfo.se, a website for people who regret their gender correction. She called it a “super important step in the right direction”.
“Now it is important that the others follow Karolinska’s decision”, Emelie Köhler told SVT.
Wild Exaggeration and Egregious Lies
By Kip Hansen | Watts Up With That? | May 6, 2021
The Covering Climate Now propaganda effort was “co-founded by the Columbia Journalism Review and The Nation in association with The Guardian and WNYC in 2019, CCNow’s 460-plus partners include some of the biggest names in news” with the stated purpose “to produce more informed and urgent climate stories, to make climate a part of every beat in the newsroom”. Their basic document, the CCNow Climate Emergency Statement, claims, in part, “… to preserve a livable planet, humanity must take action immediately. Failure to slash the amount of carbon dioxide in the atmosphere will make the extraordinary heat, storms, wildfires, and ice melt of 2020 routine and could “render a significant portion of the Earth uninhabitable…”. To accomplish their goals, CCNow provides its partners with republishable stories from other partners (.pdf), editorial guidance, story writing ideas, a list of talking points labelled Climate Science 101 provided by Katharine Hayhoe.
Important Notice: Call 911 immediately if you are choking or experiencing chest pains as a result of reading that last sentence – in Europe, dial 112 – in the UK, dial 112 or 999 – in Australia, 000 or 112.
CCNow also supplies NPR’s Climate Guide of mis- and dis-information on climate and their own “fact sheet“ [ sic ] “Who says it’s a climate emergency?” in addition to their list of ten “Best Practices” for climate propagandists.
If this is your first time hearing about CCNow, please read my previous essays posted here at WUWT, most recently The Climate Propaganda Cabal and Turning Opinion into Science Fact. There are some earlier essays as well – here and here.
Last week, on April 27 2021, CCNow web site posted a list of Nine Pieces We Loved. One of those featured was:
How Warming Oceans Are Accelerating the Climate Crisis — Humans have locked in at least 20 feet of sea level rise—can we still fix it?” by Harold R. Wanless
On the upside, the article in The Nation is clearly and prominently marked:
![]()
Adapted from an article for the Florida Climate Reporting Network’s project “The Invading Sea,” this article is published as part of Covering Climate Now, a global journalism collaboration strengthening coverage of the climate story.
My quick check of web search results show this article, one week old now, being re-posted or linked 16 times, before I stopped counting.
This article represents the “Big Lie” aspect of professional propaganda. Big Lies sell better, persuade people better than little nit-picky lies.
Here’s the bottom line Big Lie from this CCNow propaganda piece:
The climate emergency is bigger than many experts, elected officials, and activists realize. Humanity’s greenhouse gas emissions have overheated Earth’s atmosphere, unleashing punishing heat waves, hurricanes, and other extreme weather—that much is widely understood. The larger problem is that the overheated atmosphere has in turn overheated the oceans, assuring a catastrophic amount of future sea level rise.
As oceans heat up, the water rises—in part because warm water expands, but also because the warmer waters have initiated a major melt of polar ice sheets. As a result, average sea levels around the world are now all but certain to rise by at least 20 to 30 feet. That’s enough to put large parts of many coastal cities, home to hundreds of millions of people, under water.
Let me point out, unnecessarily for many readers, that not a single phrase or sentence in the first paragraph is true. The second paragraph fares little better. But only because “warm water does rise” — just not in the odd way Wanless says. [Technically, warming the water in the ocean causes expansion of the ocean’s water — the fact the ‘warmer water rises’ is not involved in this – it is the expansion that can lead to rising sea levels.] Nothing else in the second paragraph is true.
I am loathe to exaggerate, as this is what I am accusing CCNow and Wanless of doing, so let’s take a close look:
“The climate emergency is bigger than many experts, elected officials, and activists realize.” There is no real physical climate emergency – there is only a shared opinion that there is a climate emergency. At best, the sentence is an unsupported opinion (being presented here as fact). It would be hard for the real climate situation to be bigger (worse) than some of the more bizarre activists and politicians (“we have nine years left” – John Kerry).
“Humanity’s greenhouse gas emissions have overheated Earth’s atmosphere, unleashing punishing heat waves, hurricanes, and other extreme weather—that much is widely understood.” There is no scientific consensus that the Earth’s atmosphere has been “overheated”. Increasing CO2 concentrations in the atmosphere are believed to have caused a small amount of warming – but only that since the mid-1900s. Many think that that small warming and the CO2 that may have caused it are beneficial, including some of the smartest people in America. The real data on global heat waves, hurricanes, and extreme weather do not support the claim that the small warming experienced has “unleash[ed] punishing heat waves, hurricanes, and other extreme weather” – that is the climate activist’s preferred meme, not fact. More on the facts are available from the specialized pages on this web site and here. [Readers: Please supply links in comments to reliable graphs showing that the CCNow/Wanless claims are false.] Since this point is broadly contested by experts in wildfires, heat waves, hurricanes and extreme weather, it cannot be said to be “widely understood”.
“The larger problem is that the overheated atmosphere has in turn overheated the oceans, assuring a catastrophic amount of future sea level rise.” The oceans have not overheated – that is simply not true in any sense – it is difficult to even scientifically support that the oceans have warmed in any substantial, climatically important way. Measuring ocean water temperature is an ongoing project and we have a very short time series of even moderately reliable data. It is madness to claim that the tiny amount (if any) of ocean water warming has “assur[ed] a catastrophic amount of future sea level rise.”
I will leave parsing the rest of second paragraph to readers. But let’s take a further look at the idea that sea levels are assured to rise “20 to 30 feet”.
Wanless states: “But if seas rise 20 feet or more over the next 100 to 200 years—which is our current trajectory—the outlook is grim. In that scenario, there could be two feet of sea level rise by 2040, three feet by 2050, and much more to come.”
That link in there leads to “NOAA Technical Report NOS CO-OPS 083 — GLOBAL AND REGIONAL SEA LEVEL RISE SCENARIOS FOR THE UNITED STATES” [ .pdf ] which you will not be surprised says no such thing. The NOAA document does not say that the most extreme (RCP8.5) scenario is our current trajectory at all. And it does not, under any of the scenarios, predict 2 feet of sea level rise by 2040 or three feet by 2050, not even under RCP8.5 (a scenario which is now widely considered highly improbable to impossible).

Even under impossible RCP8.5 conditions, NOAA predicts only 16 inches (2040) and 25 inches (2050) [yellow highlight] – but in the real world, we saw only the 0.03m (30 mm) predicted for 2010 to 2020 for the very lowest scenario [blue highlight]. Wanless apparently gets his claimed our current trajectory to 20-30 feet from the lower right corner, highlighted in red, RCP8.5 at 2200.
Adding insult to injury, Wanless goes on to claim in his article that “Today, oceans are rising six mm a year (over two inches a decade), and this pace will continue to dramatically accelerate.” The only thing correct in this sentence is that 60mm is over two inches. Wanless’s link to a CSIRO page is broken but current sea level rise, according to NOAA:

Not 6 mm/yr, but 3.3 mm/yr, and level for the last two or three years. [source: https://climate.nasa.gov/ to see this graph select Sea Level from right hand bottom section of the graphic at the top of the page.]
You may ask, “How can any article with so many obvious, egregious errors – wild exaggerations, inaccuracies and falsehoods — get published in The Nation?” That might be the wrong question. Better to ask, “How did it get published by the AGU in EOS in its science news section?”
The answer is: The Nation, AGU and EOS are all partners of CCNow.
# # # # #
Author’s Comment:
The American Geophysical Union (AGU) and its associated online magazine, EOS, have abandoned even the pretext of science and opted to join forces with the acknowledged propaganda effort, Covering Climate Now, with its anything-goes push to convince the world that there is a Climate Emergency so they will willingly give up fossil fuels. This example today shows that that effort extends to publishing wild exaggeration and egregious lies to forward The Message – propaganda’s Big Lie in play.
I honestly don’t know how it has come to this and am simultaneously saddened and outraged.
This has now gone far, far beyond the go-along-to-get-along mutual back-patting of climate alarmists at AGU meetings of the 1990’s. Where are the real scientists who are members of the AGU? How can they remain silent when EOS publishes such articles without even a disclaimer. Shame.
Promoting and Profiting from Mass-Toxification
By Stephen Lendman | May 6, 2021
Founded in 1823, the Lancet calls itself “an independent, international weekly general medical journal (that) strive(s) (for) medicine (to) transform society, and positively impact the lives of people.”
Instead of fulfilling its pledge on all things covid, it’s been going the other way by promoting toxic mass-jabbing to be shunned, never used as directed.
In late April, the Lancet proved it can’t be trusted for falsely claiming the following:
Pfizer and AstraZeneca covid inoculations “have shown excellent safety and efficacy in phase 3 trials (sic).”
One in four people experienced mild, short-lived side effects, usually lasting one or two days (sic), it added.
Inoculations “decrease the risk of (covid) infection after 12 days (sic).”
Pharma-connected epidemiologist Tim Spector was quoted, saying:
“The data should reassure many people that in the real world, after effects of the (jab) are usually mild and short-lived, especially in the over 50’s who are most at risk of the infection (sic).”
“Rates of new disease are at a new low in the UK (sic) due to a combination of social measures and (mass-jabbing), and we need to continue this successful strategy to cover the remaining population.”
“The results also show up to 70% protection after 3 weeks following a single dose (sic), which is fantastic news for the country, especially as more people have now had their second jabs.”
Mathematician — specializing in statistical genetics — Cristina Menni defied reality by claiming that “results support the aftereffects safety of both vaccines with fewer side effects in the general population than reported in the Pfizer and AstraZeneca experimental trials and should help allay safety concerns of people willing to get” jabbed (sic).
All the above rubbish reported by the Lancet is fake news.
It’s part of relentless US-led Western mind-manipulating propaganda to get maximum numbers of unwitting people to self-inflict harm.
The Lancet allied with Western governments, their public health handmaidens, Pharma, and media press agents to all of the above in promoting what’s harmful to health, not beneficial.
There’s nothing remotely safe and beneficial from use of experimental, unapproved Pfizer/Moderna mRNA drugs or AstraZeneca/J & J vaccines for covid.
When used as directed, they risk likely irreversible harm to health or death — sooner or later.
State-sponsored coverup in the West is concealing slow-motion genocide.
According to an unnamed UK National Health Service health professional whistleblower, what’s going on is “genocide… Your children are next.”
In the US, the Pharma-connected FDA is set to OK mass-jabbing emergency use authorization for children aged 12 – 15.
If contract seasonal flu-renamed covid, their risk of serious harm or death is virtually nil.
The survival rate for flu now called covid for individuals under age-70 is 99.95% — 95% for people over age-70.
Mass-jabbing for covid should be banned.
It’s well known that toxins in experimental covid inoculations risks serious harm, nothing beneficial.
Mass-jabbing children should be criminalized, not OK’d and promoted.
State-sponsored draconian social control and depopulation hugely benefit Pharma.
Since mass-jabbing for covid began last December, Pfizer, Moderna, AstraZeneca and J & J have been cashing in big on a bonanza of huge profits.
If things go as planned, the diabolical scheme will be a gift that keeps on giving.
One or two jabs aren’t enough. Plans are for perpetual mass-toxification of unwitting people annually or semi-annually worldwide.
In Q I 2021, about one-fourth of Pfizer’s pharmaceutical revenue came from jabbing with its hazardous mRNA covid drug.
For 2021, the company projects around $26 billion in revenue from covid mass-jabbing — an annual revenue stream it aims to be permanent.
Perhaps so if countless millions of mass deceived people continue to self-inflict harm — the more covid jabs taken, the greater the harm to health near-or-longer-term.
All of the above goes on while the myth of a nonexistent pandemic persists because of the power of establishment media promoted mass deception.
Followers of my writing and likeminded others on this cutting-edge issue of our time know what’s deceptively called covid is garden variety seasonal flu.
It shows up annually without perpetual mass deception fear-mongering.
Until last year, non-beneficial/potentially harmful flu shots were promoted annually.
When for the first time ever, flu disappeared last year — because it was renamed covid — draconian mandates and recommendations have effectively manipulated the public mind in the West and elsewhere to harm health instead of protecting what’s too precious to lose.
If what’s going on continues unchecked because of public ignorance, harm to health in the West and elsewhere is highly likely to be unprecedented and suppressed — so most people will remain unaware of state-sponsored genocide.
It’s unfolding in real time below the radar — Western dark forces and their media press agents convincing most people that what’s harmful and deadly is beneficial.
I’ve stressed before and it bears repeating.
No matter how many times people have been fooled before, they’re easy marks to be duped again and again and again ad infinitum.
It’s because of the power of state-sponsored/media promoted fake news, along with the failure of most people to do minimal due diligence fact-checking.
Every literate person connected online can learn the truth on most all issues that affect their rights, health, and well-being with minimal effort.
Yet most people are easily distracted by bread and circuses.
They’re putty in the hands of manipulative dark forces and their hostile to truth-telling press agents.
We’re consistently lied to and mass deceived about all important domestic and geopolitical issues.
Yet most people are too out-of-touch with reality to notice.
My personal interfacing with individuals intelligent enough to know better but fooled like most others bears out the above reality.
Featured Video
Trump Announces Operation To Escort Ships – Fmr. CIA Analyst Larry Johnson
or go to
Aletho News Archives – Video-Images
From the Archives
Who Runs Our World?

Netanyahu addresses US Congress
By Richard Hugus | January 4, 2019
Our world is run by oligarchs, the holders of vast wealth from monopolies in banking, resource extraction, manufacturing, and technology. Oligarchs have such power that most of the world doesn’t even know of their influence over our lives. Their overall agenda is global power — a world government, run by them — to be achieved through planned steps of social engineering. The oligarchs remain in the background and have heads of state and entire governments acting in their service. Presidents and prime ministers are their puppets. Bureaucrats and politicians are their factotums.
Who are politicians? Politicians are people who work for the powerful while pretending to represent the people who voted for them. This double-dealing involves a lot of lying, so successful politicians must be good at it. It’s not an easy job to make the insane agenda of the powerful seem reasonable. Politicians can’t reveal this agenda because it almost always goes against the interests of their constituents, so they become adept at sophistry, mystification, and the appearance of authority. For example, wars for Israel have been part of the agenda of the powerful for years. Since 2001, wars for Israel have been sold as “the war on terror” and lots of lies had to be made up as to why the war on terror was a real thing. The visible faces promoting the war on terror were neoconservatives in the US, almost all of whom were advocates for Israel, or Zionists. Zionists are not the only members of the oligarchy, but they seem to be its lead actors. ... continue
Blog Roll
 Aletho News
Aletho News- New KC-46 Supertankers Promise Israel Conventional Samson Option Strike Сapability
- No, New York Times, We Don’t Need to Dam the Bering Strait
- Gates-Funded ‘Big Catch-Up’ Delivers 100 Million Vaccine Doses — Including High-Risk DTP Vaccine Not Used in U.S.
- No commercial ship or oil tanker transited Strait of Hormuz in past hours: IRGC
- Russia warns of escalating NATO military activity in Baltic region
- Government Kills the Spirit
- How ‘Israel’s’ Iran regime change plot failed – again
- 1977 Influenza Pandemic Sequence Shows Signs of Laboratory Creation: Journal ‘Cell’
- China issues first prohibition order to safeguard international trade order under rule of law
- Iran rejects Trump’s ‘Project Freedom,’ warns US over Hormuz role
- If Americans Knew
- New Member of Trump’s Iran Negotiating Team Comes From Notoriously Pro-Israel Think Tank
- Israeli army demolishes Christian monastery, nuns’ school in southern Lebanon
- Tokenizing Christians In Israel
- One Gaza is not enough: Israel is turning southern Lebanon into another Gaza – Daily Update
- As Palestinians die, Ben-Gvir celebrates birthday with golden noose cake – Daily Update
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- No Tricks Zone
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
