Whistleblower Will Appeal After Federal Court Dismisses Lawsuit Alleging Fraud in Pfizer COVID Vaccine Trials
By Michael Nevradakis, Ph.D. | The Defender | August 13, 2024
For the second time, a federal court in Texas has dismissed a whistleblower lawsuit alleging Pfizer and two of its contractors manipulated data and committed other acts of fraud during clinical trials for the Pfizer-BioNTech COVID-19 vaccine in 2020.
In his Aug. 9 ruling, District Judge Michael J. Truncale sided with the U.S. government, ruling the government had demonstrated “good cause” to intervene and dismiss the case. He wrote:
“The Government’s desire to dismiss the case — because of its doubt as to the case’s merits, differing assessment of the Pfizer vaccine data, desire to avoid discovery and litigation obligations, and belief that it should not have to expend resources in a case that is contrary to its public health policy — constitutes good cause to intervene.”
Whistleblower Brook Jackson filed the lawsuit against Pfizer, Ventavia Research Group — which conducted some of the clinical trials for Pfizer’s COVID-19 vaccine — and Pfizer contractor ICON PLC in January 2021. Jackson’s complaint was most recently amended in October 2023.
Jackson, a former Ventavia employee, alleged the companies committed numerous violations of the False Claims Act (FCA) during the clinical trials.
According to the lawsuit, the three companies “deliberately withheld crucial information from the United States that calls the safety and efficacy of their vaccine into question,” thus defrauding the federal government, which purchased the vaccines.
The FCA allows the government or a party suing on its behalf to attempt to recover money for false claims made by parties to secure payment from the government.
The FCA also allows whistleblowers to be rewarded for confidentially disclosing fraud that results in a financial loss to the government.
While whistleblowers have the right to sue under the FCA, the federal government can choose to intervene in the case at a later date. In Jackson’s lawsuit, the U.S. government initially declined to intervene in February 2022. However, in March, the government filed a motion to intervene and to dismiss the case.
Attorney Warner Mendenhall, one of the lawyers representing Jackson, questioned whether the U.S. government’s “public health policy” is tolerant toward allegations of fraud during clinical trials for vaccines.
In an interview Monday with Sasha Latypova, a former pharmaceutical industry executive with 25 years of experience in pharmaceutical research and development, Mendenhall said:
“What’s the public health policy of the United States? To kill people and damage people and injure people and make them sick? If that’s the public health policy, well then yes, we’re inconsistent with that.”
Latypova told The Defender she was “not really surprised” by the ruling, noting that drugmakers enjoy legal immunity afforded by emergency use authorization granted by the U.S. Food and Drug Administration (FDA). Latypova described this immunity as a “legal cage.”
She said “The court took as evidence an unsubstantiated opinion of two government bureaucrats … published in an editorial article of a medical journal,” but did not consider the extensive evidence of wrongdoing Jackson provided.
The government’s motion to dismiss cited a Jan. 5 JAMA editorial authored by FDA Commissioner Robert Califf and the FDA’s Center for Biologics Evaluation and Research Director Peter Marks, claiming that “data from various studies” show that “tens of millions of lives were saved by vaccination.”
During his interview with Latypova, Mendenhall argued the government failed to demonstrate good cause and that last week’s ruling did not name any specific examples of this. He said:
“If you read the actual document, there’s no cause listed at all. In fact, the judge has a footnote saying, ‘There is no cause here, but I’m going to look at this other motion I think I can find’ … that’s not how courts are supposed to proceed. You look at the motion first to intervene for good cause. If it’s not there, you’re done. You don’t get to go on and look at the motion to dismiss for hints that maybe there is good cause.”
The ruling also stated that Jackson “failed to allege that she complained to Ventavia or the FDA about fraud against the government.” Accordingly, her claims don’t “rise to the level of protected activity” as a whistleblower.
Mendenhall told Latypova this poses “constitutional concerns” and may have “a chilling effect on other whistleblowers.”
Jackson has 30 days to appeal the ruling, and plans to, Mendenhall said.
“I am very confident we’re going to win that case and get, at least, the retaliation [claim] vindicated, and vindicate what she did as a conscientious citizen of the United States,” Mendenhall said.
Jackson fired within six hours of submitting claims to the FDA
Ventavia, which operated several sites where it conducted clinical trials on behalf of Pfizer, hired Jackson in September 2020.
That same month, Jackson reported problems she observed with the Pfizer vaccine trial to the company’s management. When management didn’t respond, she took her claims to the FDA on Sept. 25, 2020. Ventavia fired her later that day.
Jackson, who had over 15 years of experience working with clinical trials, claimed she “repeatedly informed her superiors of poor laboratory management, patient safety concerns and data integrity issues.”
She also gave The BMJ a cache of internal company documents, photos and recordings highlighting alleged wrongdoing by Ventavia.
“Her job was to fix things. They wouldn’t fix them. She reported it to the FDA, and six hours later was fired from her job,” Mendenhall said.
He added:
“There was not informed consent. They were making up records. I mean, it was just endless. They were violating patient privacy, which is critical in a clinical trial because you have to not know who’s getting the shot in order to determine any effectiveness.
“Basically, the allegations that she brought forward show that the clinical trial that she saw, what she saw of it, was essentially worthless. It wasn’t valuable or useful data.”
Jackson filed her qui tam lawsuit under the FCA in January 2021. A qui tam action refers to any legal case where a private citizen initiates legal action on behalf of a state.
Documents released in November 2021 supported Jackson’s claims that she was directly involved in the Phase 3 trials for the Pfizer-BioNTech COVID-19 vaccine.
‘Level of ignorance’ of scientific facts by government officials ‘astounding’
In February 2022, the federal government declined to intervene in the lawsuit on Jackson’s behalf but reserved the right to intervene at a later date.
Later that month, Jackson filed her first amended complaint, while the court unsealed 400 pages of exhibits.
In July 2022, Pfizer asked the court to dismiss Jackson’s lawsuit on the basis that the U.S. government was aware of wrongdoings in the clinical trials but continued to do business with the vaccine maker. In March 2023, Truncale granted the motion to dismiss, ruling that Jackson had not proved the companies violated the FCA.
Jackson appealed the dismissal in April 2023, and in August 2023 submitted a motion to file a second amended complaint, which was granted in September. Jackson filed her second amended complaint in October 2023.
Pfizer and Ventavia filed motions to dismiss the second amended complaint later in October 2023, while the U.S. government filed its motion to intervene and dismiss in March 2024. Oral arguments discussing the motions to dismiss took place on May 1.
“What happened in the interim here while we’re fighting the case and moving forward, apparently the government itself decided that what we were doing in exposing Pfizer and Ventavia and ICON, the three companies involved here, was contrary to the public health policy in the United States,” Mendenhall said.
In ruling in favor of the government, the court cited a 2023 U.S. Supreme Court decision that gave the government significant leeway concerning when it could intervene in an FCA case and on what basis.
According to Mendenhall, this occurred despite meetings Jackson and her legal team had last year with representatives of the U.S. Department of Justice (DOJ), during which he said they “were completely unaware” of evidence questioning the safety of the COVID shots, including SV40 DNA contamination and vaccine injuries.
Mendenhall said:
“The level of ignorance about the scientific facts that we have uncovered was astounding to me, for someone who is supposed to be in charge of a major decision on behalf of the United States’ people, whether these shots need to be pulled from the market, whether Pfizer needs to be prosecuted or at least held civilly liable along with the other companies.
“I think that, certainly for some in the government, they just don’t want to face what they’ve actually done … they have hurt, damaged the health of millions of Americans and tens of millions, at least, around the world.”
According to Mendenhall, government attorneys were “actually sitting on the side of the courtroom with Pfizer” attorneys during the May 1 hearing.
“How strange that was to have the defendants sitting with the government who’s supposed to be going after them,” Mendenhall said.
In April, Pfizer submitted a statement to the court in support of the U.S. government’s motion to intervene and dismiss.
Pfizer previously was fined in connection with the FCA. As part of a 2009 settlement, the company paid $2.3 billion in fines — the largest healthcare fraud settlement in the history of the DOJ — stemming from allegations of illegal marketing of off-label products not approved by the FDA.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Court Denies Jordan Peterson’s Appeal as Free Speech Fight Heats Up in Canada
By Didi Rankovic | Reclaim The Net | August 15, 2024
Psychologist and author Jordan Peterson has announced that Canada’s Supreme Court refused his appeal against undergoing social media re-education (“remedial”) training.
The case stems from the demand of the Ontario College of Psychologists (which licenses practicing clinical psychologists) for Peterson to be subjected to media training. The ruling now means he is to pay court costs to the organization seeking to impose this measure on him.
According to Peterson, the demand was spurred by his negative stance regarding what’s known as “gender-affirming care,” the doomsday climate change narrative (that he spoke about on Joe Rogan’s podcast), and criticism of Canadian Prime Minister Justin Trudeau.
In a video posted on YouTube, Peterson said the court’s “terrible decision” not to consider his appeal was yet another “blow to free speech” in his country – and could well result in the revoking of his license to practice, while the ultimate goal of the social media re-education would be to get “something approximating a public apology” for his opinions and for expressing them.
Peterson previously mentioned his criticism of social service workers and police “threatening to apprehend the children of the Trucker Convoy protestors” as another reason for the Ontario College of Psychologists wanting to get him “reeducated” – though he did not speak about this in the YouTube video.
In a post on X, Peterson said that the Supreme Court ruling amounted to admitting that “mid-level bureaucrats who rule the professional colleges and regulatory boards” have more power than the Canadian Charter of Rights and Freedoms.
In another post, he criticized Ontario Premier Doug Ford’s government which he said was “overseeing the commissars” standing in the way of conservatives’ free expression, including “perhaps” Ford himself.
Peterson is also critical of the way Canada’s CBC covers the case (including his remarks on the Rogan podcast), referring to the broadcaster as “paid lackeys.”
But Peterson has received support from other corners, including Alliance Defending Freedom (ADF) International, who said they were willing to work with him “to see if he wants to take the case international” – which he seems to be open to.
And Canadian Conservative Party leader Pierre Poilievre lambasted the decision as an attempt to impose forced political reeducation, noting that this came after “another government bureaucracy threatened to ban a Canadian from practicing his profession because he expressed political opinions the state doesn’t like.”
How Antidepressants Are Numbing More Than Depression
The devastating effects on empathy, love, intimacy & sex
By Dr. Roger McFillin | Radically Genuine | August 15, 2024
In our relentless pursuit to transcend the human suffering, we’ve stumbled into a dangerous oversimplification: an improved mental state reflects the absence or decrease in negative emotional states. This reductionist view has not only cheapened our understanding of the human emotional spectrum but has also paved the way for a troubling linguistic shift.
The word “sad” has all but vanished from our lexicon, replaced by the catch-all term “depression” – a linguistic sleight of hand that medicalizes every shade of human sorrow, from loneliness to anxiety, from fear to disappointment. This semantic broadening has opened the floodgates for indiscriminate prescribing of “antidepressant” drugs, extending far beyond their original purpose to treat clinical depression.
Today, these powerful drugs are doled out for an alarming array of off-label conditions: gastrointestinal issues, fibromyalgia, grief, chronic pain, and eating disorders, to name but a few. This prescription epidemic is built not on scientific evidence, but on a dangerous myth – the allure of a quick fix for life’s complexities. The medical profession and mental health communities, seemingly hypnotized by the promise of “antidepressant” effects, have unwittingly become complicit in a grand experiment on human neurochemistry.
At the heart of this phenomenon lies a disturbing paradox: the very mechanism that gives these drugs their “antidepressant” label – emotional blunting – is causing more harm than good. By dampening our ability to feel, these “medications” offer a Faustian bargain: potential short-term relief from suffering at the cost of our full range of human experiences.
For those battling severe clinical depression, the trade-off of emotional blunting might seem a necessary evil. Yet paradoxically, these individuals often struggle most acutely with the very emptiness that antidepressants can exacerbate. More alarmingly, the vast majority caught up in the widening net of antidepressant prescriptions aren’t facing such severe depressive episodes. For them, the potential for permanent emotional deadening was never a consideration, let alone a risk they knowingly accepted.
Emotional Blunting is Not Mental Healthcare
In our misguided quest to eradicate pain, we’ve stumbled upon a chemical lobotomy that threatens the very essence of what makes us human. Emotional blunting, the insidious “side effect of antidepressants”, doesn’t just dull our sorrows – it extinguishes the vibrant flames of joy, love, and connection that give life its meaning.
Imagine a world painted in shades of gray, where the highs of ecstasy and the lows of despair are replaced by a monotonous, tepid middle ground. This is the reality for countless individuals trapped in the purgatory of SSRI-induced emotional blunting. They walk through life as spectators, unable to fully participate in the rich tapestry of human experience.
The medical establishment, in its haste to silence the symptoms, has forgotten a fundamental truth: pain, in all its forms, is not just an inconvenience to be eliminated. It’s a vital signal, a call to action, a catalyst for growth and change. By indiscriminately muting this signal, we’re not just treating depression – we’re risking the very essence of what makes us human.
But the consequences of this chemical flattening extend far beyond personal discomfort. Recent research has unveiled a chilling truth: SSRIs decrease affective empathy, our ability to emotionally resonate with others’ experiences. Neuroimaging reveals a reduction in activity across three crucial brain regions associated with empathy for pain. In our attempt to shield ourselves from suffering, we’ve created a generation of emotional zombies, incapable of truly connecting with the joys and sorrows of those around them.
Consider the implications for love and attachment – the very foundations of human society. How can one form deep, meaningful bonds when the heart’s strings have been chemically severed? The butterflies of new love, the warmth of familial affection, the bittersweet ache of nostalgia – all reduced to mere concepts, intellectually understood but never truly felt. In this emotional wasteland, how can we expect individuals to develop a robust sense of gender and sexual identity, both of which are intimately tied to our capacity for emotional and physical intimacy?
The cruel irony is that in our desperate bid to numb pain, we’ve numbed everything that makes life worth living. Joy becomes a faded memory, a concept understood but no longer experienced. The exhilaration of achievement, the quiet satisfaction of a beautiful sunset, the overwhelming surge of love for a newborn child – all diluted into pale imitations of their former glory.
This emotional castration strikes at the very heart of the human spirit. Our ability to feel deeply – to be moved by music, stirred by art, inspired by acts of kindness – is what separates us from machines. It’s the wellspring of creativity, the driving force behind innovation, the fuel for compassion and altruism. By chemically muting these essential aspects of our humanity, we risk creating a society of hollow individuals, going through the motions of life without ever truly living.
The consequences ripple out far beyond the individual. A populace incapable of deep emotional resonance is a populace ripe for manipulation, apathy, and moral decay. How can we expect people to fight injustice, to stand up for the oppressed, to sacrifice for the greater good, when they can no longer feel the burning indignation or overwhelming compassion that drives such actions?
In our shortsighted attempt to eliminate suffering, we’ve stumbled upon a cure far worse than the disease. The price of emotional blunting is nothing less than our humanity itself. As we continue down this perilous path, we must ask ourselves: in our quest for painlessness, are we willing to sacrifice everything that makes us human? What impact does this emotional blunting have on sexual desire and intimacy?
Post SSRI Sexual Dysfunction (PSSD)
Imagine a world where the very essence of your being – your capacity for intimacy, pleasure, and connection – is suddenly and inexplicably stripped away. This isn’t the plot of a dystopian novel; it’s the harsh reality for countless individuals suffering with Post-SSRI Sexual Dysfunction (PSSD), a hidden epidemic born from our society’s pill-popping approach to mental health.
A vibrant libido isn’t just about carnal pleasure; it’s the body’s barometer of vitality, a complex symphony of physical, hormonal, and psychological factors humming in harmony. But for those struck by PSSD, this life-affirming melody is replaced by a deafening silence.
PSSD is the pharmaceutical industry’s dirty little secret, a Pandora’s box of sexual side effects that persist long after the last antidepressant pill is swallowed. We’re talking about a cruel trifecta of desire destroyed, genitals numbed, and an inability to orgasm.
The numbers are staggering – up to 73% of patients dancing with these serotonin-enhancing devils report one or more of these bedroom-killing effects. That’s not a side effect; that’s a full-blown assault on human sexuality.
But here’s where it gets truly Kafkaesque: PSSD doesn’t play by the rules. It doesn’t fade away when you kick the meds to the curb. No, it sets up shop in your nervous system, potentially rewiring your sexual circuitry for years – or even indefinitely. Imagine trying to rebuild your life post-depression, only to find that your capacity for one of life’s most fundamental joys has been carpet-bombed into oblivion.
The medical community, in its infinite wisdom, largely turns a blind eye to this sexual holocaust. PSSD sufferers are left adrift in a sea of misdiagnoses and dismissals, their anguish compounded by the very professionals sworn to help them.
As for the root cause of this sexual sabotage? The jury’s still out. Some point to a chemical lobotomy of the brain’s pleasure centers, others to a genetic vandalism that silences the body’s sexual whispers. But while the white coats scratch their heads, real people are left struggling with shattered relationships, crippled self-esteem, and a quality of life that’s been gutted like a fish.
We stand at a critical juncture in mental health care, facing a silent epidemic that threatens the very essence of human experience. Post-SSRI Sexual Dysfunction (PSSD) is not just a side effect – it’s a life sentence of emotional and sexual numbness that demands immediate recognition and action.
To the medical community, pharmaceutical industry, and mental health advocates: I implore you to acknowledge PSSD as a real and devastating condition. To researchers and funding bodies: We desperately need your support to unravel the mechanisms behind PSSD and develop effective treatments. Donations could be the lifeline that restores hope to countless sufferers.
But recognition and research are not enough. We must revolutionize the informed consent process for antidepressant prescription. To every potential patient, we pose this grave question:
Would you willingly sacrifice your ability to feel emotions deeply, to experience sexual desire, and to forge intimate connections, all for the possibility of short-term relief?
This is not a hypothetical – it’s the reality faced by PSSD sufferers worldwide. We demand transparency about these risks before a single pill is prescribed. The human cost of our current approach is too high, the potential for lifelong suffering too great. It’s time to prioritize true informed consent and explore alternative treatments that don’t gamble with the core of our humanity. The stakes couldn’t be higher – it’s not just about saving lives, but preserving what makes those lives worth living.
I encourage everyone to visit the PSSD Network to learn more about this debilitating condition.
Routine Infant Hepatitis B Vaccination Fails to Protect Into Young Adulthood
Parents Should Not Expect a Long-Term Benefit
By Peter A. McCullough, MD, MPH | Courageous Discourse™ | August 12, 2024
In 1991, the Advisory Committee on Immunization Practices (ACIP) first recommended that all infants in the United States receive the hepatitis B vaccine at birth or within 1–2 months of age. The goal was to prevent maternal transmission of the hepatitis B virus (HBV) and reduce the incidence of infections in babies. Many healthy mothers without hepatitis B or risk factors such as IV drug abuse with normal infants ask what is the benefit in their babies?
The CDC recommends that children receive three doses of the hepatitis B vaccine as part of their routine childhood vaccine schedule:
- First dose: Within 24 hours of birth
- Second dose: Between 1–2 months of age
- Third dose: Between 6–18 months of age
What happens later in life when young people go into the medical field and are potentially exposed to hepatitis B in sick patients? Posuwan et al evaluated a prospective cohort of young people (mean age 18 years) going into medicine and evaluated their antibody titers as a proxy of enduring immunity to hepatitis B.

Posuwan N, Vorayingyong A, Jaroonvanichkul V, Wasitthankasem R, Wanlapakorn N, Vongpunsawad S, Poovorawan Y. Implementation of hepatitis B vaccine in high-risk young adults with waning immunity. PLoS One. 2018 Aug 20;13(8):e0202637. doi: 10.1371/journal.pone.0202637. PMID: 30125298; PMCID: PMC6101408.
The investigators were disappointed to find that only 6.9% had long-lasting immunity to hepatitis B, and thus underwent booster doses upon entering medical school. It is unclear when immunity is lost in this cohort. The results are important for parents to understand that the hepatitis B shots given at birth are only applicable if the mother has hepatitis B or serious risks for carrying it including active IV drug abuse. Otherwise the vaccine schedule for this illness has little value at that age.
Mpox Vaccine Maker’s Stock Price Soars After WHO Declares Global Public Health Emergency
By Brenda Baletti, Ph.D. | The Defender | August 15, 2024
Stock prices for mpox vaccine maker Bavarian Nordic surged after the World Health Organization (WHO) on Thursday declared mpox a global public health emergency.
The company’s share prices jumped 17% in early trading in Copenhagen today, Forbes reported, after climbing 12% yesterday when the WHO made its announcement. In the U.S., shares were up 33% this morning.
The WHO cited recent outbreaks in the Democratic Republic of Congo (DRC) and neighboring nations in its declaration.
In the first known infection of its kind outside Africa, Sweden today confirmed a case of the highly contagious strain of mpox, according to NBC News. The WHO’s European regional office in Copenhagen said it was discussing with Sweden how best to manage the newly detected case, according to Medical Xpress.
This is the second time in two years the WHO has declared mpox a “public health emergency of international concern” PHEIC — pronounced “fake” — which is its highest form of an alert.
The announcement follows a declaration Tuesday by the Africa Centres for Disease Control and Prevention that mpox is a continent-wide public health emergency.
Last week, the WHO triggered the process to grant Emergency Use Listing to two mpox vaccines, although it didn’t name which ones it would list. The agency also invited manufacturers of mpox vaccines to submit an “expression of interest” for Emergency Use Listing.
The DRC, where the outbreak is concentrated and most severe, has approved two vaccines — Japan’s LC16 and Bavarian Nordic’s Jynneos, which is also marketed as Imvamune and Imvanex.
Bavarian Nordic is one of the few companies in the world with an already-approved mpox vaccine that is also available in large quantities. Other contenders, such as Emergent BioSolutions’ ACAM2000 have been available under special investigational protocols. Others, like Tonix Pharmaceuticals, have experimental shots that are in earlier stages of development.
LC16 is a smallpox vaccine licensed in 1980 in Japan and approved in July 2022 for mpox. It isn’t commercially available, but there are large supplies in Japan’s national stockpile, the Center for Infectious Disease Research and Policy reported. Like Jynneos, it is a third-generation mpox vaccine that uses attenuated virus strains.
Jynneos and ACAM2000 can cause myocarditis, pericarditis and other serious side effects at high rates, Dr. Meryl Nass told The Defender last week, as the labels for both drugs indicate.
The Japanese LC16 vaccine also has been linked to encephalitis, Nass reported on her Substack today.
“The WHO is using the monkeypox outbreak in Africa to fast-track, under emergency use, two monkeypox vaccines,” Dr. Kat Lindley, a senior fellow at FLCCC Family Medicine and president of the Global Health Project told The Defender.
“We need to use discernment and evaluate risks and benefits before recommending any experimental new product to a vulnerable population,” she said.
The African CDC in a LinkedIn post said it needed 10 million doses to control the outbreak and called for global support for its vaccination efforts.
Bavarian Nordic’s CEO Paul Chaplin told Bloomberg the company can provide 10 million doses of its vaccine to African countries over the next year and a half.
In an interview Wednesday — before today’s stock price surge — Chaplin said, “We have inventory and we have the capabilities. What we’re missing are the orders.”
In May 2022, the WHO announced it would phase out the name “monkeypox” and rename the disease “mpox” to avoid the stigma generated by associating the disease with monkeys.
WHO process for issuing PHEIC declarations ‘non-transparent and contradictory’
WHO Director-General Tedros Adhanom Ghebreyesus said in his press announcement that the agency decided to declare a PHEIC because:
“The detection and rapid spread of a new clade of mpox in eastern DRC [Democratic Republic of Congo], its detection in neighboring countries that had not previously reported mpox, and the potential for further spread within Africa and beyond is very worrying.”
The WHO declaration signals a public health risk requiring an international coordinated response. It can lead to WHO member countries and private investors pouring substantial resources into countries with outbreaks to facilitate sharing of vaccines, treatments and testing.
The declaration also grants the WHO authority to issue travel warnings or restrictions, to review and critique the validity of public health measures by member countries and to help persuade people that they ought to follow public health recommendations.
This is the eighth public health emergency the WHO has declared since 2007, when it substantially revised its International Health Regulations (IHR). Critics have called the process for designating such an emergency “non-transparent and contradictory.”
In July 2022, the WHO declared mpox a global emergency after reporting the disease had spread to more than 70 countries, mostly affecting gay and bisexual men. At the time, Tedros made the declaration unilaterally, in direct contradiction to independent review panel advice.
At that time, the Jynneos vaccine was licensed in the U.S. and ACAM2000 was “made available for use against mpox in the current outbreak [2022] under an Expanded Access Investigational New Drug (EA-IND) protocol.” Jynneos received emergency use authorization in the U.S. for children under 18 considered to be at high risk.
Although in the U.S. monkeypox has appeared to be a mild illness, several lucrative government contracts in 2022 paid the vaccine makers hundreds of millions to stockpile the vaccines.
The 2022 outbreak reportedly affected nearly 100,000 people, primarily gay and bisexual men, in 116 countries and about 200 people died.
Despite media hype and hundreds of millions of dollars spent to stockpile mpox vaccines in the U.S., the designation was quietly withdrawn in May 2023, “given the sustained decline in cases.”
On Aug. 8, the Biomedical Advanced Research and Development Authority renewed its contract with Bavarian Nordic, committing $156.8 million to manufacture and store Jynneos doses to partly replenish the inventory used to manufacture vaccines in response to the mpox outbreak in 2022.
Critics suggest ‘common sense mitigation measures’
Mpox was first detected in humans in 1970 in the DRC, according to the WHO, and is considered endemic to countries in central and west Africa, with the number of cases rising and falling periodically.
The disease causes flu-like symptoms and pus-filled lesions. It is usually mild but can be serious, particularly in people with weakened immune systems, Reuters reported.
In its announcement Wednesday, the WHO said the DRC is experiencing a severe outbreak of mpox, with 15,600 cases and 537 deaths. It said the current outbreak is caused by a virus strain, or “clade” — clade 1b — that is more severe than clade 2, which was responsible for the global outbreak in 2022.
It “appears to be spreading mainly through sexual networks,” and it has been detected in neighboring countries of Burundi, Kenya, Rwanda and Uganda, with 100 “laboratory-confirmed cases of clade 1b” in total in those countries.
Lindley said health officials are most likely using PCR tests, which were shown during the COVID-19 pandemic to generate false positive results.
“We really have no idea,” she said, if the alleged deaths are “complications of people who have depressed immune systems and are dying of other things.”
“Why would we start mass vaccination with a new product for which we know nothing about the safety profile when common sense mitigation measures can work?” she asked. “If it is sexually transmitted, use a condom or abstain from sex. If it can be transmitted through secretions, wash your hands and don’t touch people with clinical presentation.”
Nass expressed similar skepticism on her Substack:
“If this generally mild viral illness is killing people, what is the cause of death? Does it only cause death in severely immune suppressed patients? Are babies dying due to dehydration? Do we need to treat babies with fluids rather than give them a vaccine that was never tested in babies? Lots of unanswered questions.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Injecting Babies: 1986 v Today
Important reminder regarding the explosive growth in the vaccine schedule since 1986
Injecting Freedom by Aaron Siri | August 7, 2024
If you have not seen this before, please take a moment to really let this image we created sink in—and keep in mind that this only reflects the vaccines given during pregnancy and the first year of life (there are far more thereafter on the current schedule):
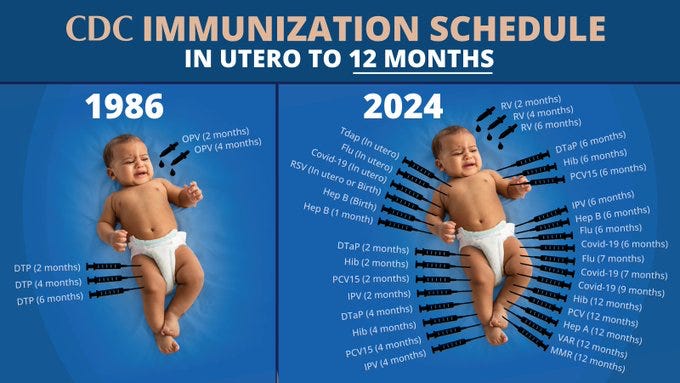
Also keep in mind that virtually every single one of today’s vaccines was developed by a pharma company knowing it would not face liability for injuries caused by these products. This is because, as most of you know, the National Childhood Vaccine Injury Act of 1986 gave them immunity from having to pay for harms.
And chronic childhood diseases, many of which are autoimmune or immune-mediated, have exploded from 12.4% in the early 1980s to over 50 percent of children today. CDC and public “health” authorities cannot figure out the cause despite desperately searching (though they haven’t studied vaccines, even though smaller independent studies have indicated vaccines are a major contributor).
With that in mind, let this chart also sink in, comparing the clinical trials relied upon to license Pfizer’s top five selling products (excluding the COVID-19 vaccine) with vaccines given in the first six months of life:
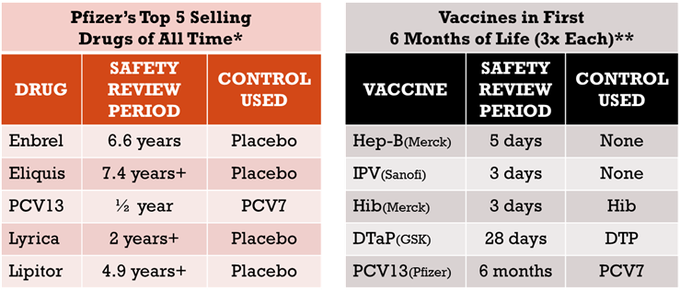
For a more in-depth treatment, read my written testimony to Congress.
Judges Back Meta in Vaccine “Misinformation” Battle, Free Speech Advocates Vow to Fight On
By Dan Frieth | Reclaim The Net | August 10, 2024
The 9th Circuit US Court of Appeals ruled this week in favor of Meta, Facebook’s parent company. The case was brought forward by the Children’s Health Defense (CHD) over allegations that the social media giant violated free speech rights.
The lawsuit, initiated in August 2020 and later updated in December, claimed that Facebook, along with its CEO Mark Zuckerberg and two fact-checking entities, Science Feedback, and the Poynter Institute’s PolitiFact site, was complicit in an unconstitutional act of privately exercising governmental censorship. CHD alleges that Facebook, in collaboration with the Centers for Disease Control and Prevention (CDC) and other federal institutions, is censoring content and discussions that the government is barred from suppressing under the First Amendment.
We obtained a copy of the opinion for you here.
The plaintiff specifically accused these sides of working in tandem to unfairly stifle valid attempts to discuss vaccine safety on Facebook, often through indirect yet sensorial measures like the use of warning labels. According to CHD, this type of arrangement between public entities and private corporations represents a breach of the First Amendment due to its perceived status as “state action.”
Despite these arguments, the 9th Circuit court concluded that CHD was not successful in meeting the initial requirement for state action, as the censorship inflicted was more a result of Meta’s content moderation policies and not any directive under federal law. Further, the court also asserted that CHD did not present any evidence of a binding agreement requiring Facebook to execute any particular action in response to misinformation about vaccines.
Although all judges did not share the same opinion, Circuit Judge Daniel P. Collins presented a partially dissenting viewpoint. He opined that the interactions between Meta and the Government involving the suppression of specific types of vaccine-related speech were substantial enough to evoke First Amendment considerations.
Expressing disappointment and worry, CHD CEO Mary Holland stated, “If we cannot stop the government’s joint action with Big Tech to censor unwanted information, our First Amendment is a pyrrhic victory — it means almost nothing in our real world of social media.” While she was pleased with the non-unanimous nature of the decision, Holland hinted at the possibility of appealing to the US Supreme Court after further review.
At the heart of the court battle, ongoing for almost four years, were claims, primarily leveled by CHD’s then-Chairman and Chief Executive Counsel, Robert F. Kennedy Jr., that tactics employed by the US Government to pressure Facebook into censoring vaccine “misinformation” were existential threats.
Be Careful What You Say
How honesty leads to the trauma of unnecessary psychiatric hospitalization

By Dr. Roger McFillin | Radically Genuine | August 8, 2024
Picture a soul in turmoil, wrapped in the suffocating embrace of despair. In the sanctuary of a therapist’s office, they finally find the courage to voice the unspeakable:
“Sometimes, I think about not being here anymore.”
The words hang heavy in the air, a testament to the crushing weight of their pain, loneliness, and emptiness. This confession, born from a place of vulnerability and trust, should be the beginning of a deeper healing journey.
During these intense emotional struggles, it’s important to understand that thoughts of escape, including suicide, are a common human response to overwhelming pain. There’s a vast chasm between contemplating an end to suffering and actively planning to end one’s life.
Context is everything.
The mind, overwhelmed by anguish, may grasp at any perceived exit, including the idea of nonexistence. But voicing these thoughts doesn’t signal imminent danger. Rather, it’s often a cry for understanding, a desperate reach for connection in the depths of isolation.
Skilled and experienced therapists understand this.
The very act of sharing these dark musings with a trusted professional can be profoundly cathartic. It’s in these raw, unfiltered moments that true therapy has the potential to work its magic. A skilled therapist, one who can navigate these turbulent waters without succumbing to panic, becomes a lifeline. They offer not just a listening ear, but a steady hand to guide the patient through the storm, helping them to contextualize their pain and find hope in the midst of despair. This is the essence of healing – not in avoiding the darkness, but in facing it together, unafraid.
Fast forward to mental healthcare in 2024.
As the demand for mental health services skyrockets, we’re witnessing a disturbing trend: the proliferation of ill-equipped therapists flooding the market. What was once a skilled profession has, in many cases, devolved into little more than paid listening.
The rise of virtual therapy platforms, while increasing accessibility, has created a cohort of isolated practitioners. Lured by the promise of higher profits without the overhead of a physical office, many therapists now find themselves cut off from the vital support networks of supervisors and mentors. Without this crucial guidance, they’re left to navigate treacherous emotional waters alone, often defaulting to a “cover your ass” mentality when confronted with challenging situations.
Simultaneously, as large hospital networks muscle into the mental health arena, therapy is increasingly reduced to an appendage of psychiatry. The nuanced art of healing is replaced by a simplistic “take your pills and manage your mental illness” approach. This medicalization of human suffering is fundamentally dehumanizing, reducing complex emotional states to mere chemical imbalances.
The consequences of this shift are stark. Individuals brave enough to voice thoughts of death are no longer met with understanding, but with fear. Their pain is hastily labeled as emerging “mental illness,” triggering a rigid psychiatric protocol that leads to overmedicalization and unnecessary hospitalization.
“I want you to go to the emergency room”
The knee-jerk mantra of risk-averse therapists and doctors who’ve been brainwashed to treat every fleeting suicidal thought like a ticking time bomb.
They herd the emotionally vulnerable into sterile, overpriced hospital rooms, mistaking cold fluorescent lights and paper gowns for actual care. It’s a convenient way to abdicate responsibility, slap a band-aid on deep-seated pain, and pad the pockets of our broken healthcare system – all while patting themselves on the back for “saving lives.”
A Rise In Psychiatric Hospitalizations
The U.S. mental health care system is at a breaking point, buckling under the weight of an insatiable demand for inpatient care. Recent federal data, as reported by CBS News, reveals a system in crisis: hospitals and clinics are operating at a staggering 144% capacity for inpatient psychiatric beds. This alarming statistic, courtesy of the Substance Abuse and Mental Health Services Administration (SAMHSA), exposes the raw nerve of a long-festering problem – a dire shortage of psychiatric inpatient facilities.
Yet, this begs a crucial question: Is this surge in demand a genuine need, or merely a symptom of a more insidious systemic failure?
The COVID-19 pandemic has cast a long shadow over youth mental health, with alarming consequences. A recent study comparing mental health emergency admissions among young people before and after the outbreak reveals a disturbing trend. In the two years following March 2020, youth psychiatric emergencies surged by an astonishing 116.7% compared to the same period in 2018-2020. Even more concerning, this new wave of patients skewed younger and were less likely to have prior psychiatric histories.
These findings suggest a troubling shift: the pandemic appears to have triggered new, earlier onset psychiatric manifestations in previously unaffected youth. Moreover, these emergencies lead to psychiatric drugs as a matter of course.
Which leads to worsening outcomes.
Primary Care Driving Hospitalizations
The mental health crisis among youth has been sensationalized to a dangerous degree, leading to misguided interventions that may do more harm than good. In pediatric offices across the country the use of quick, invalid screening measures that reduce complex emotional states to simple checkboxes is the primary assessment approach. These cursory assessments, administered by primary care doctors ill-equipped to handle nuanced mental health concerns, are causing undue panic.
A single checked box on these questionable screening measures can set off a chain reaction of fear-mongering, with parents being urgently directed to emergency rooms for what may be nothing more than typical teenage angst or temporary emotional struggles. This knee-jerk approach not only overwhelms emergency services unnecessarily but also risks pathologizing normal developmental experiences.
The media’s portrayal of primary care doctors drowning in a youth mental health crisis obscures a more insidious reality: these physicians, despite their best intentions, are conducting mental health evaluations in alarmingly short timeframes without the proper training to contextualize their findings.
The result is a perfect storm of misunderstanding, where the vulnerability and complex emotions inherent to adolescence are stripped of their context and hastily labeled as mental health emergencies. This approach not only fails to address the real needs of struggling youth but also potentially traumatizes families and clogs a healthcare system already stretched to its limits.
Even if these youth are not hospitalized they are going to placed on a drug that will at least double the risk of suicide, if not more. Lexapro is often prescribed despite the 6-fold increase in suicide risk!
The Trauma of Psychiatric Detention
When desperate parents drag a sullen teenager to the ER, or a vulnerable adult finds themselves cornered by an ER social worker, a grim dance begins. The fluorescent-lit stage is set for a performance of “crisis management theater,” where real human suffering collides with bureaucratic checklists and liability concerns.
Parents, gripped by fear that their child might take their own life, often feel coerced into consenting to psychiatric hospitalization and medication. This fear becomes a potent weapon wielded by hospital staff, despite the lack of evidence that such interventions actually prevent suicide.
Ironically, within academic circles, it’s widely acknowledged that these very interventions may increase the likelihood of suicide. This grim reality makes a perverse kind of sense: patients are prescribed powerful, mood-altering drugs and then discharged back into the very circumstances that initially drove them to contemplate suicide.
The experience of psychiatric detention is frequently described as traumatizing. Patients are stripped of their dignity – quite literally during invasive searches – and their autonomy, as their phones and personal belongings are confiscated. Many report being treated like cattle by burned-out, unprofessional staff.
Young women often feel unsafe, surrounded by men who are also experiencing mental health crises. For women struggling with the aftermath of sexual violence – a common precursor to psychiatric hospitalization – the hospital stay itself can be profoundly re-traumatizing.
This system, designed ostensibly to help, often inflicts further harm. It substitutes genuine care and understanding with a one-size-fits-all approach that prioritizes risk management over true healing. In our rush to “do something,” we’ve created a revolving door of trauma, where those seeking help often emerge more damaged than when they entered.
When parents, armed with knowledge and a desire to protect their children from potentially harmful interventions, attempt to resist the pressure to medicate, they’re often met with a dismissive and exasperated “What do you want us to do then?”
It exposes a mental health apparatus that has become reliant on the false promise of quick-fix pharmaceutical solutions, lacking the resources, training, or willingness to explore alternative approaches. This attitude effectively holds families hostage: either accept potentially harmful psychiatric drugs or be left with no support at all.
This false dichotomy – drugs or nothing – is a damning indictment of a system that has lost sight of its purpose. It reveals a profound lack of creativity and compassion in addressing mental health crises. Instead of working collaboratively with families to develop comprehensive, individualized care plans, hospital staff often default to a one-size-fits-all approach that prioritizes expediency over efficacy.
Moreover, this response subtly shifts blame onto the parents, implying that by refusing medication, they’re somehow obstructing their child’s care. It’s a manipulative tactic that exploits parental fear and guilt, further eroding trust between families and mental health providers.
Fear Based Therapy
The mental health industry has a dirty secret: it’s terrified of the patients it claims to help. Therapists, those supposed bastions of understanding and support, turn into protocol-driven robots at the mere whisper of suicide. Gone is the empathy, replaced by a checklist of CYA questions designed more to protect their licenses than to save lives.
This is how they are trained.
This fear-based charade masquerading as care has created a toxic environment where honesty is punished. Patients learn quickly: bare your soul at your own risk. Admit to dark thoughts, and watch your therapist’s eyes glaze over with panic as they mentally rehearse their mandatory reporting script.
In my years of specializing in treating chronically suicidal clients, I’ve witnessed firsthand the deep-seated trauma inflicted not just by their original experiences, but by the very system purporting to help them.
A disturbing pattern emerges, particularly among women survivors of sexual violence. Their acute trauma reactions are frequently misunderstood and hastily misdiagnosed as bipolar disorder or other psychiatric illnesses, leading to a cascade of inappropriate treatments and interventions. The psychiatric hospitalizations that often follow are not just ineffective; they’re actively traumatizing.
When these survivors finally find their way to my office, the damage is palpable. Trust, the very foundation of effective therapy, has been shattered by their previous encounters with mental health professionals. It can take months of patient, careful work to rebuild that trust, to convince them that it’s safe to be open and honest in therapy. This process is painstaking, requiring us to undo layers of iatrogenic harm – harm caused by the very institutions and individuals tasked with healing.
The tragedy here is twofold: not only are these women denied proper care for their actual traumas, but they’re also subjected to a secondary trauma at the hands of a mental health system that fails to recognize the complexities of their experiences. This cycle of misdiagnosis, inappropriate treatment, and subsequent re-traumatization doesn’t just delay healing – it actively impedes it, sometimes for years. Many never recover.
What Genuine Help Looks Like
True healing begins with the compassionate ear of a skilled, experienced therapist who can create a safe space for emotional expression and validation. This approach recognizes a fundamental truth: everything, including emotional pain and suicidal thinking, is temporary. By understanding struggles in their proper context, therapists can help clients navigate their darkest moments without resorting to extreme measures.
A competent therapist knows that most expressions of suicidal thoughts are not declarations of intent, but rather desperate attempts to communicate profound suffering. This nuance, while seemingly obvious, often eludes less experienced or inadequately trained professionals who are paralyzed by fear and uncertainty. Instead of reacting with panic, skilled therapists help clients explore their pain and envision a life worth living, even in the midst of emotional turmoil and trauma.
When someone is in emotional turmoil and suicidal risk is present, truly skilled therapists know that a gentle, personalized approach can make all the difference. Instead of rushing to hospitalization, these compassionate professionals take the time to really listen and understand. They work hand-in-hand with the person in crisis, crafting a safety plan that feels right and makes sense for their unique situation. It’s not about imposing rules, but about finding inner strength and support.
Effective therapy often involves teaching clients how to regulate intense emotions and tolerate distress. This might include techniques drawn from dialectical behavior therapy (DBT) or other evidence-based approaches. For many, additional support such as telephone coaching and family-based therapies can create a plan to weather crisis periods. These interventions recognize that suicidal crises tend to be episodic and often resolve when the underlying problems are addressed.
Primary care doctors should not be administering mental health screening measures or prescribing psychiatric drugs for complex emotional issues. Their well-intentioned but misguided interventions often exacerbate the situation, medicalizing normal human experiences and setting patients on a path of unnecessary and harmful treatments.
Working in “mental health” requires patience, understanding, and a willingness to sit with discomfort – both from the client and the therapist. By moving away from a fear-based, reactionary model of care towards one that embraces complexity and prioritizes genuine human connection, we can create a mental health system that truly serves those in need.
When the storm of the mind rages, feel-good therapy buzzwords and empty reassurances are as useful as a paper umbrella in a hurricane. What’s needed isn’t another degree or certification, but something far rarer: the guts to stare unflinchingly into the abyss of another’s pain without flinching. In the end, perhaps the most radical act in modern mental health care is simply having the backbone to shut up, sit down, and bear witness to suffering without trying to sanitize it.
Featured Video

The Sordid History of the CIA – Part 2
or go to
Aletho News Archives – Video-Images
Book Review
Jeffrey Epstein: A Jewish Individual?
The Occidental Observer | February 5, 2023
One Nation Under Blackmail: The Sordid Union between Intelligence and Organized Crime that Gave Rise to Jeffrey Epstein (Volume 1 & 2) by Whitney Webb
“Far from being an anomaly, Epstein was one of several men who, over the past century, have engaged in sexual blackmail activities designed to obtain damaging information (i.e., “intelligence”) on powerful individuals with the goal of controlling their activities and securing their compliance.”[1]
Jeffrey Epstein is dead and Ghislaine Maxwell is locked away in prison, and the thought-makers of our world seem keen to let the more explosive parts of the scandal dissipate from the public consciousness. As far as the mainstream media is concerned, Epstein and Maxwell were little more than well-connected socialites who ran a sex-trafficking ring for the rich and the powerful, and the focus has shifted instead to the criminal and civil cases seeking to achieve redress for the victims of sexual abuse.
On occasion some newspaper articles will mention the hidden cameras littered across Epstein’s properties, others the reams of CDs and hard drives found within them during the FBI raids. Altogether missing from the Netflix documentaries (Jeffrey Epstein: Filthy Rich [2020] and Ghislaine Maxwell: Filthy Rich [2022]) or the articles that spend their time narrowly focusing on the links between Epstein and Bill Gates, is the acknowledgement of the true nature of Epstein himself and the ultimate purpose of this sex-trafficking of minors — a sexual blackmail operation.
Not everyone is cowardly enough to let these controversial aspects lie untouched, as the newly released two-volume book One Nation Under Blackmail by independent reporter Whitney Webb seeks to blow wide open this media-enforced blackout. Utilizing primarily open-source information (that is, publicly accessible information such as books, newspapers articles and government reports),[2] Webb’s book delves into the life and times of Jeffrey Epstein and his deep ties to Jewish billionaires and Israeli intelligence. … continue
Blog Roll
Recent Comments
 Aletho News
Aletho News- At The Munich Security Conference, AOC Gets It Wrong On Foreign Policy
- Europe Decided to Go to War With Russia by 2030, Already Preparing – Orban
- Russia and China Are Expanding Their Cooperation to Counter US Efforts to Bully Iran and Cuba
- NATO plotting maritime blockade of Russia – Moscow
- Jeffrey Epstein’s sinister shadow over West Asia
- The Sordid History of the CIA – Part 2
- French FM under fire over ‘false’ claims about UN rapporteur
- Israel Wants ISIS-Linked Militias To Control Rafah Crossing — The New Order in Gaza
- ISIS never left Syria, it just changed uniforms
- Why ARE the US and Israel Obsessed With Eliminating Iran’s Ballistic Missiles?
- If Americans Knew
- Israel battles Palestinian right of return, one Palestinian at a time – Not a ceasefire Day 127
- Noor’s short life of unimaginable suffering
- Israel Destroyed Gaza’s Hospitals. Now It’s Banning Doctors Without Borders.
- Is Spite of What Zionists Say, It’s a Good Thing to Criticize Governments
- Palestinian mother, daughter recount strip searches, harsh conditions in Israeli detention
- Israel used weapons in Gaza that made thousands of Palestinians evaporate
- ADL’s Stats Twist Israel’s Critics Into Antisemites
- Why Is the World Silent When the Gaza Genocide Is Not Over?
- In Gaza: 8,000 bodies under rubble, 3,000 missing – Not a ceasefire Day 126
- AZAPAC, the new PAC opposing Israeli domination of U.S policies
- No Tricks Zone
- Unfudging The Data: Dutch Meteorological Institute Reinstates Early 20th Centruy Heat Waves It Had Erased Earlier
- German Gas Crisis…Chancellor Merz Allegedly Bans Gas Debate Ahead of Elections!
- Pollen Reconstructions Show The Last Glacial’s Warming Events Were Global, 10x Greater Than Modern
- Germany’s Natural Gas Storage Level Dwindles To Just 28%… Increasingly Critical
- New Study Rebuts The Assumption That Anthropogenic CO2 Molecules Have ‘Special’ Properties
- Climate Scientist Who Predicted End Of “Heavy Frost And Snow” Now Refuses Media Inquiries
- Polar Bear Numbers Rising And Health Improving In Areas With The Most Rapid Sea Ice Decline
- One Reason Only For Germany’s Heating Gas Crisis: Its Hardcore-Dumbass Energy Policy
- 130 Years Later: The CO2 Greenhouse Effect Is Still Only An Imaginary-World Thought Experiment
- New Study Affirms Rising CO2’s Greening Impact Across India – A Region With No Net Warming In 75 Years
