Most Variation in All-Cause Mortality Explained by Mass COVID-19 Vaccination
Australian Ecological Analysis Points to Vaccine Campaign Causing Rising Death Counts
By Peter A. McCullough, MD, MPH | Courageous Discourse | September 1, 2024
After a pandemic, all cause mortality should go down due to a culling effect of the frail and vulnerable. We saw acute COVID-19 become the proximate cause of death in many seniors who were in the final year of natural life.
Now an analysis from Allen indicates that all-cause mortality is up in heavily vaccinated Australia and that at least two thirds in the variation per region is explained by mass COVID-19 vaccination. There are numerous well-documented fatal vaccine serious adverse events which are piling up months and years after the shots. Cumulative toxicity is another factor as a single person is not vaccinated just with the primary series (first two injections), but continued dosing every six months.

Allen, DE. 2024. The correlation between Australian Excess Deaths by State and Booster Vaccinations. Medical Research Archives, [online] 12(7).https://doi.org/10.18103/mra.v1 2i7.5485
These data call for a direct data merge of the vaccine administration and death data in Australia to explore these very uncomfortable relationships. Because the Australian government pushed the vaccines so hard, officials have been stonewalling the public on this important next analysis.
Gaza and Polio
By Richard Hugus | August 27, 2024
On July 30, 2024 the Health Ministry of Gaza declared a polio epidemic in Gaza. The World Health Organization then said it would send more than a million polio vaccine doses to Gaza. On August 16, according to Al-Jazeera, the first case was reported and the UN’s Antonio Guterres called for a ceasefire to make a vaccination campaign possible. This call was supported by Hamas.
Health authorities rightly point out that the cause of the horrific health conditions in Gaza is the ongoing Israeli genocide – the bombing of homes and infrastructure, the shelling, the withholding of food and medical supplies, the sadistic evacuations — and the authorities of course call for all these things to end. But the involvement of globalist agencies like the UN and WHO raise suspicions that the polio declaration may be just another attack on the people of Gaza concealed under a cloak of humanitarianism.
According to Al-Jazeera, the announcement of the alleged outbreak came on August 7 from one Dr. Hamid Jafari, a World Health Organization polio specialist who claimed the polio virus was found in wastewater samples in Deir el-Balah and Khan Younis. Dr. Jafari is currently employed by the US Centers for Disease Control, a deeply corrupt organization which has spent the past three years pushing vaccines for another purported virus – covid 19 – in spite of clear proof from the very beginning of multiple harms caused by the vaccine. This harm is not limited to the US. Denis Rancourt and colleagues have recently offered statistical proof of almost 31 million excess deaths globally for the period 2020-2022, deaths which they attribute to the strangely universal worldwide public health response to covid 19, to include lockdowns, business closures, isolation, harmful hospital protocols, and particularly the mRNA vaccines.
Regarding Dr. Jafari in Gaza, The CDC website tell us that he “is a graduate of CDC’s Epidemic Intelligence Service (EIS) program, class of 1992. . . currently serving as the Principal Deputy Director, Center for Global Health, at the Centers for Disease Control and Prevention.The website goes on to say that “Dr. Jafari served as the project manager of World Health Organization’s (WHO’s) National Polio Surveillance Project in India from 2007-2012. As the project manager, he was the main technical advisor to the government of India in the implementation of the nation’s large scale polio eradication, measles control, and routine immunization activities, and he directed WHO’s extensive network of more than 2000 field staff.”
Thus Dr. Jafari was in in charge of a vaccination campaign in India where, in one study, researchers found that between 2000–2017 there were “an additional 491,000 paralyzed children” above normal. The ambitious “polio eradication” program in India was funded and led by the Gates Foundation and the WHO. The number of paralysis cases was found to be proportional to the number of vaccine doses administered. The Gates Foundation and WHO are not exactly separate entities – Gates is a major funder of the WHO. Dr. Jafari’s employment at the CDC, his authoritative declaration of a polio epidemic in Gaza, and WHO’s immediate announcement of the shipment of over a million vaccines should raise red flags.
Polio is a condition that is often confused with the catchall “acute flaccid paralysis.” Acute flaccid paralysis may even be the result of injection of polio “vaccines, but it is not polio. The polio vaccine can and does cause acute flaccid paralysis. From experience in the US since the 1950s it is known that what was often called polio was not the gut virus that humans have lived with more or less uneventfully throughout history, but a form of paralysis caused by human exposure to neurotoxins introduced in the 20th century — for example, mercury and aluminum adjuvants used in vaccines, leaded fuel, fluoridated water, pesticides and herbicides like arsenic, DDT, dioxin, and glyphosate. DDT was in widespread use in the 1950s. When it was banned, the high numbers of “polio” cases went down. The famous Salk and Sabin vaccines had little to do with it, though the medical establishment claimed victory. Indeed, as we know from what is called “the Cutter incident” in 1955, vaccines produced by Cutter Laboratories ended up causing 40,000 cases of polio, severely paralyzed 200 children, and killed 10. Later iterations of the vaccine were found to contain a cancer-causing agent called SV-40 (SV being short for ‘simian virus’). Bernice Eddy, the scientist who discovered this, was hounded out of her job at the US National Institute of Health. Lest one think that things are surely more advanced now than in the 1950s, as recently as April 2023 a well-known scientist named Kevin McKernan found SV-40 in samples of the Pfizer covid -19 vaccine. A new term was coined to describe a common effect of the covid injections — “turbo cancer” — perhaps attributable to the SV-40 and the normally forbidden DNA plasmids also found in the samples.
In an emergency involving a projected 2,700 aid workers delivering 1.6 million doses over a short period of time (between bombings), will the parents of the one million children in Gaza be given complete information about the contents of the polio vaccine their children are about to be given? Will there be a full explanation about risks and possible side-effects? Will the parents have any understanding of the negative history of polio vaccines or of vaccines in general? Will they have the informed consent required in any medical intervention? Will they be given redress for any injuries? No, not a chance. The instructions will be “here’s your dose, now move along.” To be fair, it’s the same all over the world.
Dr. Suzanne Humphries is a well-known kidney specialist who spent years of her professional life coming to grips with organized medicine’s ignorance of the fact that vaccines may cause rather than cure disease. She found that high numbers of polio cases mysteriously went away when polio came to be named other things, like poliomyelitis, transverse myelitis, Guillain-Barré syndrome, enteroviral encephalopathy, traumatic neuritis, and Reye’s syndrome. A similar trick was played when influenza suddenly disappeared between 2020 and 2023 and “covid” took its place. Incidentally, one of the common effects of the covid vaccine was facial paralysis, or Guillain-Barré syndrome. Vaccines contain neurotoxins. Neurotoxins cause paralysis and myriad other problems. When it comes to Gaza, we might ask: is the confirmed case there actually polio, or is it one of the many distinct diseases under the umbrella of acute flaccid paralysis? Does a vaccine designed for one strain of polio address some, all, or even any of the mimicking diseases? Is there documentation that the confirmed case was actually polio, or do we just have to take Dr. Jafari’s word for it?
According to Dr. Humphries, “no vaccines are safe. Having “efficacy” means an antibody response is generated, not that they keep you from getting sick. There are many other ways to keep children healthy other than injecting them with disease matter, chemicals, animal DNA, animal proteins, detergents and surfactants that inflame and weaken the blood brain barrier, potentially causing inflammation and other problems.” One way would be to stop bombing them.
The Gaza Health Ministry and Hamas are surely busy enough dealing with zionist genocide, but they need to know that in the last few years public health has been revealed as a very effective weapon of war. The US Department of Defense had a leading role in the worldwide biowarfare operation known as “covid 19 countermeasures.” The WHO and the UN were very much involved in this operation. They are not to be trusted. Like the US government, these supposed humanitarian organizations speak from both sides of their mouth – calling for ceasefire while doing nothing to stop the weapons that every day kill more Palestinians. They know that the best way to protect the children of Gaza is to bring good nutrition, clean water, clean air, housing, and an end to the trauma of psychopath Israel’s daily bombing, yet they do nothing meaningful to bring this about. They are not offering aid with their polio vaccines; they are offering more poison.
Court Finds Kennedy Has Standing in Our Consolidated Case
As I predicted, our new co-plaintiff Kennedy meets even the Supreme Court’s stringent standing requirements, the injunction against the government is back in play.

By Aaron Kheriaty, MD | Human Flourishing | August 26, 2024
As I explained in a previous post, Robert F. Kennedy Jr.’s companion lawsuit Kennedy v. Biden has been consolidated by the court into our Missouri v. Biden case. Based upon documents we obtained on discovery, the court recently found that Kennedy meets the Supreme Court’s stringent standing criteria. We only need one co-plaintiff with standing to bring the case and the petition for the injunction. So the injunction is back in play, and we will likely find ourselves at the Supreme Court again in a few months. Unless SCOTUS invents another technicality on which to temporize, they will be forced to rule on the merits of the evidence against the government, which we believe is overwhelming.
On the issue of Kennedy’s standing, U.S. District Court judge Terry Doughty last week ruled: “There is not much dispute that both Kennedy and CHD [Kennedy’s nonprofit Children’s Health Defense] were specifically targeted by the White House, the Office of Surgeon General, and CISA, and the content of Kennedy and CHD were suppressed. Therefore, Kennedy must now show a substantial risk that in the near future, at least one platform will restrict the speech of Kennedy in response to the actions of one Government Defendant.” Citing evidence we uncovered in Missouri v. Biden, Doughty explained: “The Court finds that Kennedy is likely to succeed on his claim that suppression of content posted was caused by actions of Government Defendants, and there is a substantial risk that he will suffer similar injury in the near future.”
As reported in The Kennedy Beacon Substack:
The latest ruling is not only significant for Kennedy but for the future of online speech. In June of this year, the Supreme Court ruled that the state attorneys general of Missouri and Louisiana did not have standing to bring their case on government directed mass censorship. Now that Kennedy and the CHD have been found to have standing in the matter, the Supreme Court will likely have an opportunity to judge the issue on its merits rather than on a technicality as it did when making its standing ruling on an injunction in June.
If Kennedy and his co-plaintiffs are able to demonstrate to judges that the Biden administration’s intrusion into the actions of major social media companies resulted in censorship, the country will be one step closer to a major legal ruling guaranteeing freedom to speak online without the censorious interference of the federal government.
In related news, Kennedy announced Friday that he is suspending his presidential campaign. While he has deep disagreements with Trump on several issues, he is endorsing Trump’s candidacy to advance the key issues on which they have substantial agreements—including stopping government censorship and propaganda. His 48-minute speech announcing this decision was an extraordinary moment in American politics and is worth watching. In addition to discussing the issue of government censorship, which seriously hamstrung his ability to campaign, Kennedy’s remarks focus also on the root causes of the current epidemic of chronic disease in the United States.
While there is online buzz that Trump may tap Kennedy as Attorney General, I anticipate if Trump is elected he will appoint Kennedy to his cabinet as Secretary of Health and Human Services, a department which includes the CDC, FDA, and NIH. This could prove a welcome opportunity for the reform of our public health agencies. I am currently working with a team of policy analysts and health freedom advocates on concrete policy proposals for just such reforms, and will keep you posted on our progress with that project.
What Does a Fraudulent Vaccine Safety Study Look Like?
By Dr. William H. Gaunt | The Defender | August 26, 2024
New vaccines should be proven safe before they are accepted onto the Centers for Disease Control and Prevention (CDC) vaccine schedule.
Here is what is actually happening: Vaccine companies are doing studies that claim to demonstrate the safety of new vaccines but are carefully designed and conducted to intentionally hide the toxicity of these vaccines.
To see how this is done, read on.
What does an honest vaccine safety study look like?
An honest safety study must have a test group that gets the vaccine and a control group that gets a harmless placebo. Injuries and deaths are compared in the two groups.
If the test group has many more adverse events than the placebo control group, the vaccine is not safe.
Most people would be shocked to learn that none of the vaccines on the CDC vaccine schedule have been safety tested in this way.
What does a fraudulent vaccine safety study look like?
Rule No. 1 for conducting a fraudulent study: Do not have a placebo control group. Here is where the fraud is happening: The “control group” is deliberately given something that is as toxic as the vaccine being tested. It can be an older vaccine or the vaccine ingredients minus the antigen.
The results will show that the injuries and deaths are similar in both groups. That is because they are both receiving toxic ingredients. The new vaccine is then illogically declared safe.
If there is no placebo control group, the toxicity of the vaccine is hidden. This is both clever and diabolical. Can you see it?
The public is unaware of this subterfuge
“Turtles All The Way Down: Vaccine Science and Myth” is the most thorough and brutally honest book ever written about vaccines.
The authors tell us on page 81:
“As we have seen in this chapter, vaccine trials are designed and performed in such a way as to ensure that the true extent of adverse events is hidden from the public. There is not a single vaccine in the US routine childhood vaccination schedule whose true rate of adverse events is known.”
Two examples of how unsafe toxic vaccines got on the CDC vaccine schedule
Prevnar-13 (a pneumococcal vaccine) was given to the test group of children and the “control group” was given the older Prevnar vaccine.
Severe adverse events occurred in 8.2% (one out of every 12 children) in the test group. Severe adverse events also occurred in 7.2% (one out of every 14 children) of the control group.
What percent of a placebo control group would have had severe adverse events? Probably 0% because they would have received something harmless. We can’t know because the authors of this study chose not to have a placebo control group.
The Prevnar-13 vaccine was declared “safe” and was approved for use by the U.S. Food and Drug Administration (FDA). You don’t have to be a doctor or scientist to suspect that both the Prevnar and the Prevnar-13 vaccines are unsafe. “Turtles All The Way Down” covers this fraudulent vaccine safety study on pages 60 and 61.
Here is the second example, which the authors describe on pages 77 and 78:
“In one of the DTaP vaccine trials, 1 in every 22 subjects in the trial group was admitted to the hospital. A similar hospitalization rate was also reported in the ‘control group’ (which received the older-generation DTP vaccine).”
Again, there was no placebo control group. Both vaccines appear to be decidedly unsafe yet the newer DTaP vaccine made it onto the CDC vaccine schedule. DTP and DTaP vaccines contain antigens for diphtheria, tetanus and pertussis.
Why is this happening?
Ultimately, the answer is greed. It is enormously profitable to get a vaccine on the CDC schedule. Vaccine companies will do whatever it takes to accomplish this. If it takes a little scientific fraud, so be it.
The vaccine companies are cheating on vaccine safety studies by omitting placebo control groups, thereby lying about the safety of vaccines. The FDA and CDC are complicit because they are doing nothing to stop this fraud.
Corporate capture or regulatory capture
The FDA and CDC are regulatory agencies. The original function of these agencies was to protect the public from dangerous drugs and vaccines.
Unfortunately, these agencies have been captured by Big Pharma. They no longer focus on protecting the public. They focus on protecting and promoting the interests of pharma companies.
Can we compare the health outcomes of vaccinated versus unvaccinated children?
Theoretically, yes but not if we expect our health authorities or pharma companies to do these types of studies. Chapter 6 of the “Turtles” book is titled “The Studies That Will Never Be Done.”
On page 207 the authors tell us:
“No study that compares the health of vaccinated children to that of unvaccinated children has ever been done by the medical establishment.”
If such a study showed that vaccinated children are healthier than unvaccinated children, it would have been published and been headlined in every newspaper and been the lead story on the nightly news. That hasn’t happened. We suspect that such a study has been done internally at the CDC.
The unwanted conclusion that they won’t allow to see the light of day is that unvaccinated children are far healthier than vaccinated children. This study has likely been done and buried instead of published. Such a study is verboten because it would be a disaster for the vaccine companies.
Private studies show that unvaccinated children are healthier
Here are two privately funded studies:
- “Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination” by Dr. Paul Thomas and James Lyons-Weiler, Ph.D.
- “Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders” by Brian S. Hooker, Ph.D., and Neil Z. Miller.
Another great resource is the book “Vax-Unvax: Let the Science Speak,” by Robert F. Kennedy Jr. and Hooker. They report on many studies where unvaccinated children have better health outcomes compared to vaccinated children.
Science is for sale
The book “Science for Sale: How the US Government Uses Powerful Corporations and Leading Universities to Support Government Policies, Silence Top Scientists, Jeopardize Our Health, and Protect Corporate Profits” by David L. Lewis, Ph.D., tells the story of how corporate profits can frequently trump true science.
This happens in many industries, not just in vaccines. It is not unusual for government agencies to take the side of the corporations. The author was fired from the EPA for revealing details of how this happens.
The health of the public is subverted by powerful corporations in these situations. Does that sound familiar? Lewis doesn’t cover vaccines in his book except in Chapter 7 where he describes how Dr. Andrew Wakefield was unjustly crushed for questioning the safety of the measles-mumps-rubella or MMR vaccine.
Are vaccines the main cause of autism?
If the answer is yes, that would be very bad for vaccine companies. The “Turtles” authors point out on page 209 how our health authorities are trying hard not to find the correct answer to this question:
“Over the past 15 years, dozens of epidemiological studies have been conducted examining the association between vaccines and autism, but not a single one compared the rate of autism in fully vaccinated and fully unvaccinated children.”
If they actually wanted to answer this question, they would do vax/unvax studies. Such studies are easy to do but our health authorities refuse to do them.
Why do health authorities favor epidemiological studies?
The “Turtles” authors provide the answer on page 198:
“Epidemiological studies are the tool of choice for health authorities and pharma companies to maintain a facade of vaccine safety science. They are cheap, relatively simple to conduct, and, above all, their results are easily manipulated.”
It is entirely possible to get an epidemiological study to conclude whatever its authors want it to conclude. These types of studies are not the gold standard.
What caused the drastic decline in infectious disease mortality?
We are supposed to believe that vaccines have been our saviors. Not true. The huge decline in infectious disease mortality was largely due to sanitation, hygiene and improved nutrition (the availability of fresh fruits and vegetables year-round).
The “Turtles” authors make this clear on page 293. They reference a report by the American Institute of Medicine, which states:
“The number of infections prevented by immunization is actually quite small compared with the total number of infections prevented by other hygienic interventions such as clean water, food, and living conditions.”
The claim that vaccines alone saved us is false and our health authorities know it is false.
Below is a simple graph that causes cognitive dissonance in those who believe that vaccines saved us from high rates of infectious disease mortality.

We can clearly see that deaths from measles were reduced to near zero by the interventions mentioned above BEFORE the measles vaccine was introduced.
Similar graphs for other infectious diseases are shown in the book “Dissolving Illusions: Disease, Vaccines, and the Forgotten History” by Dr. Suzanne Humphries and Roman Bystrianyk. The mortality rate for all infectious diseases was dropping rapidly before vaccines were introduced.
Do you smell a rat?
Yes. And it has been dead for quite a while. We have been bamboozled (deceived, cheated, swindled and defrauded).
Vaccines are now doing far more harm than good by causing a huge increase in chronic diseases like autism, asthma, attention-deficit/hyperactivity disorder or ADHD, Type 1 diabetes, learning disabilities, seizures and much more.
It is way past time to use honest unbiased science to sort it out. Imagine what will happen when honest science is applied to vaccine safety studies.
Here is how the ‘Turtles’ authors sum it up
On page 518:
“Science belongs to the people. It belongs to humanity, not to corrupt government agencies and pharmaceutical giants who collude to rewrite the principles of science in order to continue the decades-long cover-up of their crimes against humanity.
“The magnitude of these crimes is enormous — these entities are in way too deep to ever be able to admit any wrongdoing. They will do whatever is necessary to protect the great vaccine hoax. For them, it is a matter of life and death — literally. And so it is for us.”
The lie that vaccines are safe and effective and that serious adverse events are exceedingly rare is still believed by many people — yet trust in pharma and our coopted regulatory agencies is now rapidly eroding. For example, only a tiny percentage of people are continuing to take the COVID-19 vaccine boosters.
Also, the percentage of parents who are choosing to obtain an exemption to vaccines for their children is increasing. This can be done in almost all states.
It is becoming obvious to a growing number of people that we are being intentionally misled regarding vaccines and vaccine safety.
Debate: Is A Demonstration Project Really Necessary?
By Francis Menton | Manhattan Contrarian | August 17, 2024
My repeated calls for a Demonstration Project of a zero-emissions electrical grid have led to a spirited debate among knowledgeable commenters. While most back my position, some say that a Demonstration Project is really not necessary and would be a waste of effort.
The gist of the argument of those disputing the necessity of a Demonstration Project is that it is so obvious that a zero-emissions grid powered predominantly by wind and solar generation cannot be achieved that the expense and effort of building an actual physical facility cannot be justified. Before the building of a physical demonstration project there would inevitably be an engineering feasibility study, and such a feasibility study would not get through its first day before everybody involved realized that this could never work. All it would take would be a few back-of-the-envelope calculations using basic arithmetic and the whole endeavor would be sunk.
Regular commenter Richard Greene leads the forces arguing against a demonstration project. From a comment by Richard on my August 10 post:
A good demonstration project that included manufacturing and farming is very likely not needed. A real local utility Nut Zero grid engineering plan on paper would have grid engineers laughing hysterically. The money allocated for backup batteries would be nowhere close to paying for the battery GWh capacity needed. Backup natural gas power plants could do the job, but gas backup is not wanted. . . . 100% wind and solar can never work due to compound energy droughts, wind drought and solar droughts (batteries are far too expensive).
Representative of the pro-demonstration project side is a comment from “dm” on the August 13 post. Excerpt:
Because many people doubt paper analyses, lived experience is a necessary teacher. Thus, demonstration projects are NEEDED to prove the folly of “sustainable” electricity grids. Furthermore, the demonstration projects MUST be in regions heavily populated with nut zero enthusiasts, and ALL costs MUST be paid SOLELY by households, businesses, institutions … located within the demonstration areas.
My natural sympathies here would lie with Richard’s side of this debate. How can spending what would likely be billions of dollars of public money be justified when calculations that I have made or verified myself show that the project will never come close to success?
But then we must look at what is happening in large states and countries that are proceeding toward the stated goal of a zero-emissions grid without ever having had a working demonstration project. In some of these cases (Germany, UK) the wasted resources are now into the trillions, not billions. And at some point the whole effort will inevitably be ended with some kind of hard-to-predict catastrophe (long blackouts? multiplication of consumer costs by a factor of ten or more?). By then, many of the working resources that have made the grid function will have been destroyed and will have to be re-created, at a cost of further trillions.
Consider the case of Germany. Germany is a very substantial country (80+ million people, making it twice the size of California and four times the size of New York), with the world’s fourth largest GDP at over $4 trillion annually. Germany was one of the first to start down the road to a zero-emissions grid back in the 1990s, and formally adopted its “Energiewende” fourteen years ago in 2010. Germany has proceeded farther than any other large country in converting its electricity generation to wind and solar.
And yet, as I look around for information on Germany’s progress toward zero-emissions electricity, I can’t find any concern or recognition that this might not be doable in the end. Perhaps that exists in German language sources that I can’t read. But from anything I can find, it looks like Germany is forging ahead in the blind faith that if only they build enough wind turbines and solar panels at some point they will have the zero-emissions electricity that they crave.
Go to the website of the Umweltbundesamt (Federal Environmental Agency) for the latest information. At least on the electricity front, you will not find any indication that there may be problems in achieving the zero-emissions utopian future:
The “Energiewende” – Germany’s transition towards a secure, environmentally friendly, and economically successful energy future – includes a large-scale restructuring of the energy supply system towards the use of renewable energy in all sectors. . . . [T]he switch towards renewables in the electricity sector has been very successful so far. . . . While in the year 2000 renewables accounted for 6.3 percent of electricity demand only, its [sic] share has been growing significantly over the past years, exceeding 10 percent in the year 2005 and 25 per cent in the year 2013. In 2023 renewable energy sources provided 272 billion kilowatt-hours of electricity and account for 51.8 percent of German electricity demand. With wind power being by far the most important energy source in the German electricity mix.
Some 30+ years into this process, and they’re only up to barely over 50% of their electricity from “renewables.” And while they may claim that “wind power [is] by far the most important source in the German electricity mix,” in fact when you get a breakdown you find that wind and solar together provided well less than 50%. According to solar advocates Fraunhofer Institute here, in 2023 “biomass” provided some 42.3 TWh of Germany’s electricity (about 8%), hydro provided 19.5 TWh (about 4%), and “waste non-renewable” (I think that means burning garbage) provided 4.5 TWh (about 1%). That leaves under 40% for wind and solar.
If they keep building solar and wind facilities, and expect batteries to be the backup, has anybody calculated how much battery storage they will need? Not that I can find. Here is a website of a company called Fluence, which is an affiliate of German industrial giant Siemens. They excitedly predict a rapid expansion of grid storage in Germany:
Storage capacity will grow 40-fold to 57 GWh by 2030.
Wow, a 40-fold increase! It may sound like a lot. But Germany’s average electricity demand is about 50 GW, so the 57 GWh of battery storage in 2030 will come to about 1 hour’s worth. Competent calculations of the amount of energy storage needed to back up a predominantly wind/solar grid run in the range of around 500 to 1000 hours.
Here from another website is a chart of the growth of energy storage in Germany up to this year.

Look at that acceleration! But the 10 GWh of storage that they currently have will last no more than about 10 minutes when the wind and sun quit producing on a calm night.
In short, this large and seemingly sophisticated country is completely delusional, with no sane voices anywhere to be heard. A demonstration project that fails spectacularly is the only thing with any hope of saving them.
Australian Government blocks Covid inquiry ‘with teeth’
Once again, Labor characterised its foes as ‘conspiracy theorists’, ‘cranks,’ ‘kooks’ and ‘far right extremists’ rather than engaging in rational debate
By Rebekah Barnett | Dystopian Down Under | August 22, 2024
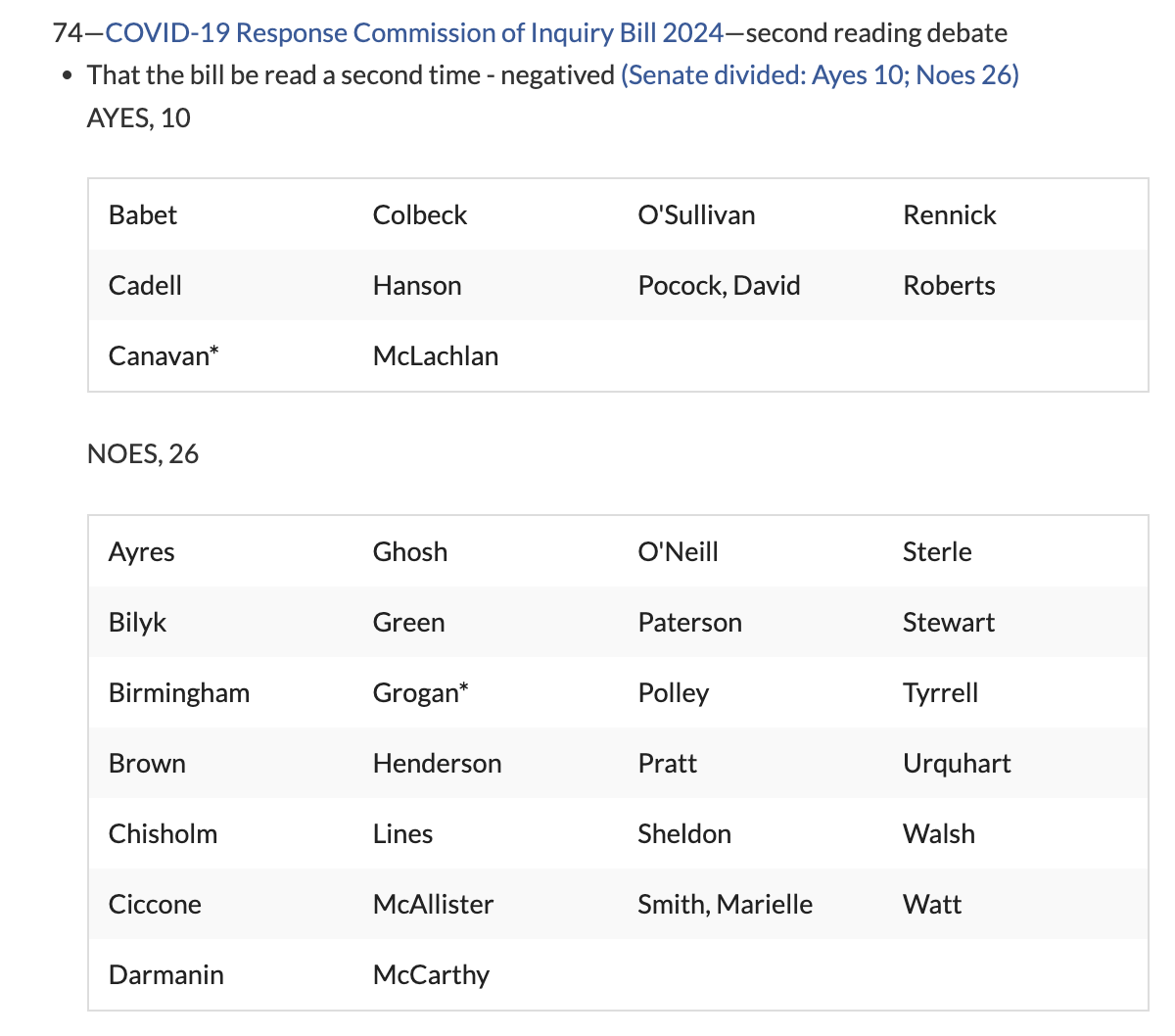
The Australian Government has voted down a bill to establish a Covid Commission of Inquiry, which would have essentially the same powers and independence as a Royal Commission.
The bill was supported by a small coalition of senators from minor parties and the Opposition (conservative), but was rejected by the Labor Party(left-wing) in a vote today.
To date, Australia has had plenty of Covid inquiries, but none with teeth.
The siloing of inquiries to deal only with states and territory and federal governments on an individual basis has allowed for a lot of finger pointing with very limited accountability.
The scope of the federal Covid Inquiry excludes the policies of state and territory governments, which enacted vaccine mandates, lockdowns and inter-state border restrictions, leading politicians and media to call it “toothless.”
In turn, states and territories have focused on how well they implemented policies heavily influenced by the Federal Government and national advisory bodies without actually considering whether the policies were any good.
The patchwork nature of these inquiries allows the Federal Government to blame states and territories for implementing the harshest measures, and the states and territory governments pass the buck to the federal agencies and departments for influencing them to do so.
More holistic independent reviews like the Fault Lines report have resulted in talk of ‘lessons learned’ about “ill-conceived policies, politically driven health orders and excessive use of lockdowns,” but no meaningful attempts to hold anyone to account or guarantees that the lessons will inform future pandemic policy making.
Another problem with inquiries to date is that federal, state and territory governments have played hide the ball with important documentation and data required to properly assess their performance. As yet, no Australian government has released the health advice that draconian measures were based upon.
A Royal Commission or similar, taking the entire Covid response – at federal, state and territory levels – and with aggressive powers to command access to information that governments don’t want to release, would be required for real accountability.
The only ways to bring this about are for the executive to call a Royal Commission, or for the Senate to call a Commission of Inquiry.
However, despite the recommendation of the Senate Select Committee on COVID-19 in 2022 that a Royal Commission into Australia’s Covid response be established, the Labor Government has resisted calls to do so.
The Committee, led by senior Labor Party member Katy Gallagher (now Minister for Finance, for Women and for the Public Service) criticised the then Liberal Government’s lack of transparency and accountability around pandemic decision making by the National Cabinet.
Emergency law making had “challenged the Australian Parliament’s capacity to provide meaningful scrutiny of proposed laws, particularly in identifying and addressing the impact of emergency powers on the rights of individuals,” the Committee stated in its recommendations.
Leader of the Opposition at the time, Anthony Albanese, sort of promised a Covid Royal Commission. But after being elected to government in May 2022, Prime Minister Albanese has resolutely dodged the issue, throwing his support behind the limited federal inquiry instead.
Hence, a group of concerned senators tabled the COVID-19 Response Commission of Inquiry Bill 2024 in a bid to open up option B, an inquiry initiated by the Senate.
The bill, prepared by Senator Matt Canavan (Liberal), was co-sponsored by Senators Malcolm Roberts (One Nation), Alex Antic (Liberal), Gerard Rennick (Liberal), Ralph Babet (United Australia Party) and Matt O’Sullivan (Liberal), all of whom have been vocal critics of Australia’s pandemic response.

Source: Senator Alex Antic on X
During speaking time, senators who sponsored the bill argued that a Covid Commission of Inquiry is needed so that Australia can finally move on from Covid with a good plan in place for future pandemics. A proper inquiry would get to the bottom of what went wrong (and what went right) to restore trust in public health, they said.
Senator Roberts also said that in light of the fact that multiple U.S. states are now suing Pfizer for misleading about its Covid vaccine, if an inquiry found that Pfizer was indeed guilty of fraudulent behaviour, this could shift the financial burden of injuries and deaths associated with Pfizer’s product from Australian tax payers to the pharmaceutical giant.
Australian tax payers have coughed up more than $20 million on compensation for Covid vaccine injuries, but they will have to pay a lot more if a Covid vaccine injury class action is successful. The action, which was filed in the Federal Court last year, has enrolled over 1,500 injured Australians (or families of the deceased).
However, only ten senators supported the bill when it went to a vote in Parliament today. The bill was supported by the above mentioned senators (with the exception of Senator Antic, who is on leave), some members of the Coalition, One Nation, and independent Senator David Pocock.
Despite Greens Senator Jordon Steele-John stating that his party supports the establishment of a “frank” and “transparent” inquiry with the powers of a Royal Commission, the Greens abstained from the vote. Labor voted against the bill.
Source: Dynamic Red, 22 August 2024
I am told by the office of one of the senators who sponsored this bill that they have no intention of dropping the matter.
Previously, Senator Babet brought five separate motions to establish the world’s first government Excess Mortality Inquiry, which is now in progress thanks to Senator Babet’s persistence.
An inquiry into proposed terms of reference for a Covid Royal Commission has already been conducted, which will prove helpful in the event that either a Royal Commission or a Commission of Inquiry into Australia’s Covid response are eventually established.
Nonetheless, such efforts will face stiff opposition from the Albanese Government, if Labor Senator Tim Ayres’ speech in Parliament today is representative of his party’s position.
In speaking time before the vote, Senator Ayres said that the Government did not support the bill because “there’s already a public inquiry,” before launching into an astonishing diatribe of ad hominem attacks on the senators who proposed the bill.
Senator Ayres used the term ‘conspiracy theories’ or ‘conspiracy theorist’ more than twenty times, likened the efforts of senators to bring about a thorough Covid inquiry to movements motivated by “anti-semitism,” and called these same senators “cranks,” and the “nastiest, extreme, kooky elements of politics.”

Senator Ayres referred to ‘conspiracy theorists/theories’ more than 20 times in Parliament, 22 August 2024. Source: Australian Parliament House Streaming Portal, YouTube.
Senator Rennick called Senator Ayres’ speech “disgusting,” stating, “all we’re recommending today and supporting is that we have a thorough inquiry.”
In a statement after the vote, Senator Canavan said that more disheartening than Australia’s damaging pandemic response was “the response to the response.”
“Those Australians hurt during Covid deserve to have the accountability of proper public hearings, the publication of all the health advice and an open, transparent attempt to recognise mistakes as well as put in processes to prevent such things ever happening again.
“Why can’t the Government accept that if it is given immense power to lock people in their homes and force people out of work, that there should be an equal and corresponding obligation for them to be accountable to the people hurt by their decisions?”
Senator Babet took to X to express his dissatisfaction with the outcome, calling the decision of the Senate “weak.”
“Is it too much for Australians to ask for governments and the bureaucrats advising them to be held to account for the advice and actions they took during the pandemic?”
Apparently, yes.
Categorizing The mRNA-Vaccinated… Most Can Be Forgiven, But Some Cannot

By P Gosselin | No Tricks Zone | August 24, 2024
When discussing the mRNA COVID vaccines, we need to be careful about dividing people into the two broad groups of the vaccinated and the unvaccinated.
The truth is that many vaccinated people didn’t want to be injected and now deeply regret it.
There are 6 categories of the vaccinated, ranging from the innocent victims to the wicked, unrepentant perpetrators.
1. Those vaccinated by force, against their will
These people were forced to get the jab against their will, and included babies and children who were unable to resist. By forced, we mean they were subjected to extreme duress through threats like job loss or being banned from performing their livelihoods. Many knew that the experimental mRNA shots were potentially dangerous, or didn’t work, and were just unnecessary, but were forced against their will to accept them. These people are victims serious human rights violations. – injured or not.
2. The harassed and coerced
These people were not convinced and many were distrustful of the shot, or even fearful of the drug’s side effects. Many understood that the novel gene-manipulative drug was untested and could be potentially dangerous. Many understood the risk,and never would have allowed themselves to be vaccinated. But they did because the harassment at work, home and in public was just too much to bear.
3. The restriction dodgers
Many were convinced the novel vaccine would work or at least wouldn’t do any harm. Many had felt they didn’t need it, but simply wanted to go back to normal living. Unfortunately these people didn’t do the necessary research to make an informed decision. They were duped into thinking they weren’t harmful. We can forgive this category because at least they didn’t run around lecturing, persecuting and excluding those who resisted taking the mRNA shots. Like in category 1 and 2 above, many deeply regret allowing the injection and promise not to ever take these shots again.
4. The dimwitted follower sheep
They were gullible beyond belief, blindly following everything they were told, and refused to listen to informed experts and hard data contradicting the bogus claims made by the vaccine makers and tyrants. Even today many continue to insist the vaccine works, some even willing to roll up their sleeves again whenever instructed. Too many of them are simply too brainwashed, hypnotized are just flat out too dimwitted to learn. For them, denying is better than confessing and admitting to having been a fool. Yet, we can forgive them to some extent, but we need not give them much sympathy if things go wrong for them.
5. The mRNA vaccine tyrants
We all know who these people are. They were in the media, institutes, governments and big corporations. They lied and hid the risks from us. These people will remain evil until they confess to their grave sins and change their malicious ways. Everyday we heard them ridicule, persecute, marginalize and coerce the unvaccinated. Many of these tyrants need to be punished, prosecuted for fraud, or forever fired from their positions. The late Dr. Vladimir Zelenko even called for the death penalty for the worst offenders. These people can be forgiven, but only through lots of repentance, remorse, apologies and making solemn pledges to redeem themselves.
6. The unrepentant mRNA tyrants
Those who don’t repent must know we will never forget and will not ever relent hauling you in to face legal justice. Your numbers are shrinking and your protection is crumbling. But it’s (still) not too late for you to redeem yourselves.
CDC USES ‘COVID SURGE’ TO STOKE FEAR
The HighWire with Del Bigtree | August 22, 2024
The CDC is using new, questionable techniques to declare a ‘COVID surge’ and stoke fears. Coincidentally, a new booster hits the market as students head back to school. Jefferey Jaxen reports.
Statement on proposed emergency roll-out of vaccine program in Africa for monkeypox
SAVIMS | August 23, 2024
We are deeply concerned about the recent announcements made by Africa Centres for Disease Control and Prevention (CDC) Director General Jean Kaseya on Aug. 13 and World Health Organization (WHO) Director-General Tedros Adhanom Ghebreyesus on Aug. 14. It is important to address these announcements openly to the public.
In his statements, Kaseya declared regarding monkeypox vaccines:
“We have a clear plan to secure more than 10 million doses in Africa, starting with 3 million doses in 2024.”
We at the South Africa Vaccine Injury Medico-Legal Study-Group (SAVIMS) would like to point out pertinent facts to both institutions and other relevant bodies of interest:
1. There is no prescribed vaccine with documented Level 1 scientific evidence for monkeypox. The current WHO-recommended live virus vaccines, Jynneos and ACAM2000, are:
(a) intended for smallpox and are thus experimental for monkeypox;
(b) have reported serious adverse effects, and;
(c) contain live viral strains which may instigate a resurgence of the eradicated smallpox virus.
2. The potential use of mRNA vaccines. There is no scientific evidence supporting the use of any mRNA vaccine to prevent or mitigate any infectious disease. The observed data of adverse reactions to experimental mRNA vaccines far outweighs any benefit.
3. Informed consent is an ethical concept that is codified in the law and is in daily practice at every healthcare institution. Three fundamental criteria are needed for clinical informed consent: the patient must be competent, adequately informed and not coerced.
It is not possible for any recipient of these vaccines to receive legitimate informed consent based on current research.
4. The article by Allan-Blitz et al., “A position statement on Mpox as a Sexually Transmitted Disease,” concluded that monkeypox is a “sexually transmitted disease.” Preventative measures for this scenario should necessitate and provoke relevant clinical and primary healthcare and education initiatives directed at the high-risk group.
There is no merit in the recommendation of experimental vaccines to the general population.
5. The statistics and analysis, regarding the collated monkeypox data in the Democratic Republic of Congo and other countries in Africa by the WHO, warrant further investigation and must be independently audited.
The areas in which the highest statistics were collated should detail the criteria for testing, the procedures for testing, equipment sensitivity and specificity, personnel skill, clinical scenarios, and provocation for testing these specific communities. What tests were done to investigate and exclude other diseases, including communicable diseases?
6. There have been no autopsy reports published on the deaths related to monkeypox. The lack of formal documented autopsy, lack of information regarding equipment test sensitivities and specificities, and lack of information on procedures validating random collation of data, further reduces and invalidates the authenticity of the statistics.
SAVIMS position statement regarding emergency monkeypox vaccine rollout in Africa
We have reviewed the literature and analyzed the data on monkeypox, as well as its etiopathogenesis. Based on our understanding of this disease:
1. We do not support the Africa CDC and WHO declaration of a global health emergency for monkeypox.
2. It is established that monkeypox is predominantly a self-limiting condition. This does not warrant vaccine intervention.
3. We strongly object, based on the scientific evidence, to the “emergency” rollout of repurposed smallpox vaccines or any other proposed monkeypox vaccine to the people of Africa.
4. We question the authenticity of the number of deaths associated with monkeypox, as reported by the Africa CDC unless it can be verified through autopsy.
5. We warn members of the public about the inherent risks of taking any vaccine, including those proposed for mpox, of which the effectiveness and safety have not been reliably determined by Level 1 clinical trials. There can be no justification for a vaccine with unknown adverse effects.
6. We urge the public to exercise their inherent human rights to refuse to give consent to any medical intervention that they do not feel comfortable taking.
We are open to dialogue and discussion with the Africa CDC on the issues raised above and on all matters of health and well-being concerning the African population.
SAVIMS is a voluntary multidisciplinary association under the Common Law governed by its members in accordance with the Constitution of the Republic of South Africa. The purpose of SAVIMS is to follow the evidence to gain and communicate knowledge about vaccine injuries. This knowledge is necessary for the treatment and counseling of patients with vaccine injuries; as well as for medico-legal report writing and provision of evidence in respect of victims of vaccine injury and in other vaccine-related disputes. The objectives of SAVIMS are to promote human health and human rights as enshrined in the Bill of Rights of South Africa’s Constitution.
Featured Video

Did the 9/11 Hijackers Really Fly the Planes?
or go to
Aletho News Archives – Video-Images
Book Excerpt
Biden’s Closed Circle on Russia
An excerpt from ‘The Great Betrayal’
By James W. Carden | The Realist Review | June 14, 2026
Joe Biden’s presidency may ultimately come to be seen as a cautionary tale. Here was a president who showed little interest in entertaining arguments that might have contradicted his most deeply held assumptions.[1] And there were precious few within the upper ranks of the administration who might have attempted to do so, after all, only policy hands and political operatives who had come up through the ranks of the Clinton and Obama administrations or had longstanding ties to the citadels of the foreign policy community were invited into the fold. … continue
Blog Roll
 Aletho News
Aletho News- UN: Israel continues to violate Lebanon airspace in defiance of Iran-US MoU
- Araghchi: Israeli occupation of Lebanese land a violation of MoU
- Hezbollah fighters confront intruding Israeli forces in southern Lebanon
- The Straight of Hormuz is Open for Iranian Business… Oil is Moving and Iran is Getting Paid
- Biden’s Closed Circle on Russia
- Lebanon Accuses Israel Of Violating The Chemical Weapons Convention By Spraying Toxic Herbicide Over Farmland
- Did the 9/11 Hijackers Really Fly the Planes?
- ‘Jewish lobby’ deceived Putin – Lukashenko
- The UK Joins the Pirates
- Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report
- If Americans Knew
- Israel’s former defense minister compares settler ideology to Nazism
- The Pro-Israel Lobby’s Quiet Cash Shuffle
- Trinity Broadcasting Network (TBN) Propagandizes for Israel’s Wars
- A grim milestone: Gaza’s death toll surpasses 73,000 – Daily Update
- Jared Kushner’s Israel-linked island, and other dubious projects
- Why Are Crypto Billionaires and AIPAC Spending $8+ Million to Elect Adrian Boafo?
- Why the Mainstream Media Should Stop Using the ADL as Their Go-To Antisemitism Source
- Censorship and Thuggery Won’t Save Israel’s Reputation
- Israel Searches for a Red Sea Foothold in Somaliland
- They Weren’t Convicted of Terrorism, But These Palestine Activists Got Sentenced as Terrorists Anyway
- No Tricks Zone
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
