Dr. Peter McCullough: COVID Shots for Kids ‘the Last Straw’
By Brenda Baletti, Ph.D. | The Defender | August 19, 2024
“A child today faces well over a hundred shots,” cardiologist Dr. Peter McCullough told host Mat Staver on a recent episode of “Freedom Alive.” Many of those shots are for infectious diseases of the past or contemporary illnesses that don’t pose a risk to infants.
McCullough said the “inflection point” was the 1986 National Childhood Vaccine Injury Act, which freed vaccine manufacturers from liability for vaccine injuries. “We saw essentially a vaccine bonanza develop,” he said, and “excessive, unnecessary” vaccination could be leading to serious side effects.
Those vaccines start just after a baby is born, he said, when they are given the hepatitis B vaccine.
As a cardiologist, dealing with blood and body fluids, McCullough said the vaccine is appropriate for him, but babies are not at risk for it unless their mother has the illness or is an active IV drug user. For most babies, he said, it is a “completely unnecessary shot on the first day of life.”
The Centers for Disease Control and Prevention (CDC) in October 2023 recommended newborns receive Beyfortus, the monoclonal antibody shot meant to protect babies from RSV-related illness.
“This has no safety track record,” he said. “We’ve never given a synthetic antibody to a baby ever in the history of medicine, and now it’s being given uniformly with no idea of what is going to happen to the baby’s immune system over the next several weeks or months.”
The clinical trials were inconclusive as to whether Beyfortus is safe, and evidence from France shows increased mortality among infants after the shot was introduced, he said.
McCullough said the broader safety concerns stem largely from the fact that so many are given in combination. “For some babies, it’s too much,” he said.
Excessive vaccination, he explained, sends the immune system into overdrive, which can lead a baby to develop a fever and a febrile seizure (convulsion).
Research shows febrile seizures have about a 40% chance of causing permanent neurologic injury, ranging from epilepsy to attention-deficit/hyperactivity disorder to autism spectrum disorder.
Staver said many parents who saw their children develop autism post-vaccination are told either that it isn’t true or it’s just a coincidence because there is no evidence of such a link.
“The direct observation by a mother and father of their child is the strongest evidence,” McCullough said, citing Dr. Andy Wakefield’s controversial 1998 study.
McCullough also cited a recent study by the Children’s Health Defense science team, which showed that combining multiple vaccines is dangerous. Spacing them out and giving them individually — rather than combining three vaccines into one shot, like the measles-mumps-rubella, or MMR, vaccine — is safer, he said.
And, he said, all children do not need all vaccines. Which vaccines a child gets should be determined on a risk basis. For example, a child with cystic fibrosis might need the respiratory illness vaccines, but healthy kids probably don’t.
Yet these vaccines are given to all children in part, he said, because the people who advise the CDC on which vaccines should be recommended for children have serious conflicts of interest — most take money from Big Pharma. Then schools enact mandates based on those recommendations, leaving parents feeling as if they have no choice.
Vaccine makers lobby state legislators to continually increase the list of mandatory vaccines.
McCullough said:
“Can you imagine if you had a product that treats an illness? You would have to treat a small number of people in a population. But if you have a vaccine, that means the whole entire population has to receive the product.
“A product that must be purchased by the entire population with no liability is an absolute boon to any purveyor of that product.”
McCullough said the CDC has turned a blind eye to vaccine safety. For example, none of the childhood vaccines have been studied for safety when given in combination.
He added that Dr. Paul Thomas reported in The Defender that pediatricians receive substantial incentives from insurance companies to vaccinate certain high percentages of their patients.
For lower-income kids, there is also government financial support to ensure that the vast majority of the population is vaccinated against legacy diseases like diphtheria, tetanus, polio and other diseases that are either no longer commonly circulating or for which good treatments exist.
For many, McCullough said, the recommendation that children take the COVID-19 vaccine, given its alarming safety data, was “the last straw.”
“That act was irresponsible. It triggered the World Council for Health, which is an evidence-based, consensus-driven body to recommend waiting on all the childhood vaccines,” he said.
Vaccines are not safe or effective enough to mandate, McCullough said. “Every parent and child unit should be able to make their own decisions free of any pressure, coercion, or threat of reprisal.”
Watch the interview here.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
COVID-19 Vaccines Cause far More Myocarditis than Infection, Overall Risks Greatly Outweigh Theoretical Benefits
BREAKING PUBLICATION
By Peter A. McCullough, MD, MPH | Courageous Discourse™ | August 19, 2024
When the Springer Nature CUREUS Journal of Biomedical Sciences retracted one of the most comprehensive and valid risk-benefit analyses of the COVID-19 vaccines, they probably had no idea the message would be greatly amplified and now fully published in a pair of papers in the International Journal of Vaccine Theory, Practice, and Research.
This manuscript evaluated all of the published data and has completely overturned a false narrative held by government agencies and the American College of Cardiology who erroneously assert that SARS-CoV-2 infection poses a greater risk of heart damage than vaccination. Mead et al importantly conclude the vaccines cause actual adjudicated and oftentimes fatal myocarditis while the infection remains a theoretical risk without adjudicated, autopsy proven cases.
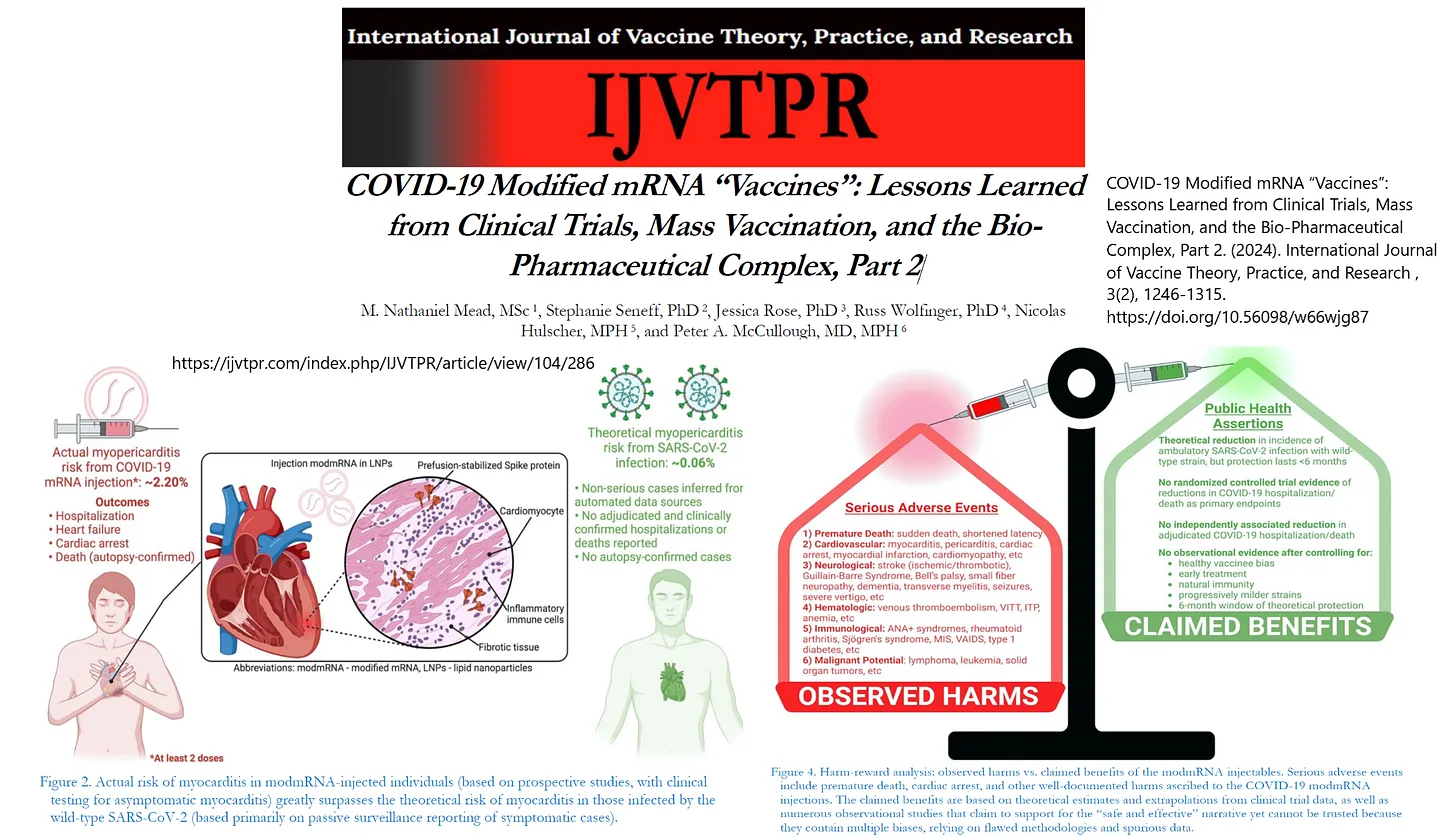
COVID-19 Modified mRNA “Vaccines”: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex, Part 2. (2024). International Journal of Vaccine Theory, Practice, and Research , 3(2), 1246-1315. https://doi.org/10.56098/w66wjg87
The paper goes into great depth to enumerate harms from the shot along the lines of six domains where observed adverse events greatly outweigh claimed, theoretical benefits:
“We then categorize the principal adverse events associated with the modmRNA products with a brief systems-based synopsis of each of the six domains of potential harms: (1) cardiovascular, (2) neurological, (3) hematologic; (4) immunological, (5) oncological, and (6) reproductive. We conclude with a discussion of the primary public health and regulatory issues arising from this evidence-informed synthesis of the literature and reiterate the urgency of imposing a global moratorium on the modmRNA-LNP-based platform.”
The final call is clear, the COVID-19 mass, indiscriminate vaccination campaign should come to an end and with it, the four-year long false “safe and effective” narrative from the Bio-Pharmaceutical Complex.
What’s Really Happening with Mpox
The Mpox Emergency
By David Bell | Brownstone Institute | August 18, 2024
The World Health Organization (WHO) acted as expected this week and declared Mpox a Public Health Emergency of International Concern (PHEIC). So, a problem in a small number of African countries that has killed about the same number of people this year as die every four hours from tuberculosis has come to dominate international headlines. This is raising a lot of angst from some circles against the WHO.
While angst is warranted, it is mostly misdirected. The WHO and the IHR emergency committee they convened had little real power – they are simply following a script written by their sponsors. The African CDC, which declared an emergency a day earlier, is in a similar position. Mpox is a real disease and needs local and proportionate solutions. But the problem it is highlighting is much bigger than Mpox or the WHO, and understanding this is essential if we are to fix it.
Mpox, previously called Monkeypox, is caused by a virus thought to normally infect African rodents such as rats and squirrels. It fairly frequently passes to, and between, humans. In humans, its effects range from very mild illness to fever and muscle pains to severe illness with its characteristic skin rash, and sometimes death. Different variants, called ‘clades,’ produce slightly different symptoms. It is passed by close body contact including sexual activity, and the WHO declared a PHEIC two years ago for a clade that was mostly passed by men having sex with men.
The current outbreaks involve sexual transmission but also other close contact such as within households, expanding its potential for harm. Children are affected and suffer the most severe outcomes, perhaps due to issues of lower prior immunity and the effects of malnutrition and other illnesses.
Reality in DRC
The current PHEIC was mainly precipitated by the ongoing outbreak in the Democratic Republic of Congo (DRC), though there are known outbreaks in nearby countries covering a number of clades. About 500 people have died from Mpox in DRC this year, over 80% of them under 15 years of age. In that same period, about 40,000 people in DRC, mostly children under 5 years, died from malaria. The malaria deaths were mainly due to lack of access to very basic commodities like diagnostic tests, antimalarial drugs, and insecticidal bed nets, as malaria control is chronically underfunded globally. Malaria is nearly always preventable or treatable if sufficiently resourced.
During this same period in which 500 people died from Mpox in DRC, hundreds of thousands also died in DRC and surrounding African countries from tuberculosis, HIV/AIDS, and the impacts of malnutrition and unsafe water. Tuberculosis alone kills about 1.3 million people globally each year, which is a rate about 1,500 times higher than Mpox in 2024.
The population of DRC is also facing increasing instability characterized by mass rape and massacres, in part due to a scramble by warlords to service the appetite of richer countries for the components of batteries. These in turn are needed to support the Green Agenda of Europe and North America. This is the context in which the people of DRC and nearby populations, which obviously should be the primary decision-makers regarding the Mpox outbreak, currently live.
An Industry Produces What It Is Paid for
For the WHO and the international public health industry, Mpox presents a very different picture. They now work for a pandemic industrial complex, built by private and political interests on the ashes of international public health. Forty years ago, Mpox would have been viewed in context, proportional to the diseases that are shortening overall life expectancy and the poverty and civil disorder that allows them to continue. The media would barely have mentioned the disease, as they were basing much of their coverage on impact and attempting to offer independent analysis.
Now the public health industry is dependent on emergencies. They have spent the past 20 years building agencies such as CEPI, inaugurated at the 2017 World Economic Forum meeting and solely focused on developing vaccines for pandemic, and on expanding capacity to detect and distinguish ever more viruses and variants. This is supported by the recently passed amendments to the International Health Regulations (IHR).
While improving nutrition, sanitation, and living conditions provided the path to longer lifespans in Western countries, such measures sit poorly with a colonial approach to world affairs in which the wealth and dominance of some countries are seen as being dependent on the continued poverty of others. This requires a paradigm in which decision-making is in the hands of distant bureaucratic and corporate masters. Public health has an unfortunate history of supporting this, with restriction of local decision-making and the pushing of commodities as key interventions.
Thus, we now have thousands of public health functionaries, from the WHO to research institutes to non-government organizations, commercial companies, and private foundations, primarily dedicated to finding targets for Pharma, purloining public funding, and then developing and selling the cure. The entire newly minted pandemic agenda, demonstrated successfully through the Covid-19 response, is based on this approach. Justification for the salaries involved requires detection of outbreaks, an exaggeration of their likely impact, and the institution of a commodity-heavy and usually vaccine-based response.
The sponsors of this entire process – countries with large Pharma industries, Pharma investors, and Pharma companies themselves – have established power through media and political sponsorship to ensure the approach works. Evidence of the intent of the model and the harms it is wreaking can be effectively hidden from public view by a subservient media and publishing industry. But in DRC, people who have long suffered the exploitation of war and the mineral extractors, who replaced a particularly brutal colonial regime, must now also deal with the wealth extractors of Pharma.
Dealing with the Cause
While Mpox is concentrated in Africa, the effects of corrupted public health are global. Bird flu will likely follow the same course as Mpox in the near future. The army of researchers paid to find more outbreaks will do so. While the risk from pandemics is not significantly different than decades ago, there is an industry dependent on making you think otherwise.
As the Covid-19 playbook showed, this is about money and power on a scale only matched by similar fascist regimes of the past. Current efforts across Western countries to denigrate the concept of free speech, to criminalize dissent, and to institute health passports to control movement are not new and are in no way disconnected from the inevitability of the WHO declaring the Mpox PHEIC. We are not in the world we knew twenty years ago.
Poverty and the external forces that benefit from war, and the diseases these enable, will continue to hammer the people of DRC. If a mass vaccination campaign is instituted, which is highly likely, financial and human resources will be diverted from far greater threats. This is why decision-making must now be centralized far from the communities affected. Local priorities will never match those that expansion of the pandemic industry depends on.
In the West, we must move on from blaming the WHO and address the reality unfolding around us. Censorship is being promoted by journalists, courts are serving political agendas, and the very concept of nationhood, on which democracy depends, is being demonized. A fascist agenda is openly promoted by corporate clubs such as the World Economic Forum and echoed by the international institutions set up after the Second World War specifically to oppose it. If we cannot see this and if we do not refuse to participate, then we will have only ourselves to blame. We are voting for these governments and accepting obvious fraud, and we can choose not to do so.
For the people of DRC, children will continue to tragically die from Mpox, from malaria, and from all the diseases that ensure return on investment for distant companies making pharmaceuticals and batteries. They can ignore the pleading of the servants of the White Men of Davos who will wish to inject them, but they cannot ignore their poverty or the disinterest in their opinions. As with Covid-19, they will now become poorer because Google, the Guardian, and the WHO were bought a long time back, and now serve others.
The one real hope is that we ignore lies and empty pronouncements, refusing to bow to unfounded fear. In public health and in society, censorship protects falsehoods and dictates reflect greed for power. Once we refuse to accept either, we can begin to address the problems at the WHO and the inequity it is promoting. Until that time, we will live in this increasingly vicious circus.
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. He is a former medical officer and scientist at the World Health Organization (WHO), Programme Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland, and Director of Global Health Technologies at Intellectual Ventures Global Good Fund in Bellevue, WA, USA.
Dear Elon, 1,000ppm of carbon dioxide is safe, we breathe it every day
Elon is scratching for a reason to keep worrying about CO2
By Jo Nova | August 16, 2024
In the interview with Donald Trump, Elon Musk tried to argue that we ought be limiting carbon dioxide because we are too close to 1,000ppm where people get headaches. Not to put too fine a point on it, but we breath out air at 40,000 ppm fifteen times a minute for our entire lives. If 1,000 ppm gave us a headache or made us nauseous, we’d have to hold our breath every time we kissed someone.
@ElonMusk: The point I was making is that, even if CO2 did not cause global warming, it is uncomfortable to breathe air with >1000 ppm of CO2. Given that the outdoor ppm away from cities is now ~420 (lol), it is already getting close to 1000 ppm indoors in cities at times. You can buy a cheap CO2 monitor and measure this for yourself.
As the global base level of CO2 keeps increasing, it will cause air quality in cities to feel stuffy and unpleasant, resulting in drowsiness, poor concentration and eventually headaches and nausea. That would not be a good future.
And then he quotes CO2meter.com which, ahem, sells CO2 meters, and has an incentive to wildly overstate the problems with CO2, which they do.
CO2 is not the problem, the stale air and other pollutants cause headaches and sleepiness.
The point of CO2 meters is not so much to warn us about excessive CO2 levels, but to indicate how well the room is ventilated. CO2 levels are just an indicator for air quality. Air with higher CO2 levels usually also has higher levels of organic compounds, humidity, body odour, mold, chemicals from furniture and paint (like formaldehyde) and potentially viruses too. When people report headaches and nausea, the high CO2 levels are not the issue, it’s the bioeffluence that causes problems. When researchers do cognitive tests with pure CO2 added to clean air, performances don’t suffer. The stale air is the problem, not the CO2. (See Zhang, and Misra where they compared the cognitive effects from badly ventilated air and clean air with high CO2 levels up to 3,000ppm. Problems disappear when they use fresh air plus higher CO2.) Well ventilated rooms may also be cooler rooms, which might explain why results so often contradict each other.
Classrooms are at 1,000ppm “typically”
While outdoor air is 420ppm, indoor levels of CO2 are commonly 1,000ppm in classrooms every day, and can rise as high as 3,000ppm if all the windows are shut. The recognized occupational health and safety levels for long term working exposure are 5,000 ppm for 8 hours straight, five days a week. It’s no big deal.
The National Collaborative Centre for Environmental Health (Canada) measured school and buildings and advises that “Typically, in an occupied classroom situation, the recommended level of ventilation would correspond to a CO2 level of approximately 1000-1100 ppm“. Furthermore, they said the “lowest level at which a human health effect (i.e. acidosis) has been observed in humans is 7,000 ppm, and that only after several weeks of continuous exposure in a submarine environment”.
The occupational limits for CO2recommended by the American Conference of Governmental Industrial Hygienists (ACGIH) are 5000 ppm (TLV-TWA) and 30,000 ppm (TLV-STEL), based on the direct effects on acidification of the blood. — via Marc Morano and Climate Depot

At NASA The Office of the Chief Health and Medicial Officer reports that a typical spacecraft works at around 3,000-7,000 ppm (or o.3-0.7% CO2). The recommended exposure is 5,000, and the permissible exposure limit is 10,000 ppm. Although the flight surgeons found levels of nearly 7,000 were safe and “didn’t affect performance”. On Apollo 13, CO2 levels rose to 20,000ppm. Sweating and shortness of breath became a problem above 30,000 ppm.
Submariners typically live with CO2 levels of 2,000- 5,000 ppm, and when a small sample of sailors was tested at 600, 2500 or 15,000 ppm, the researchers couldn’t find any difference in results from an 80 minute test on decision making. (Rodeheffer at al) Likewise another study at the Johnson Space Centre, people did cognition tests at 600, 1,200, 2,500 and 5,000ppm and there was no dose response effect. Results look rather random.
Lowther et al looked at 51 studies in 2021, and found nothing conclusive in terms of harms from CO2 below 5,000ppm. Most studies were confounded, results were conflicting. Teams of researchers are hunting to find another problem “due to CO2”. If there was a strong negative effect of CO2 it would have shown up by now. Instead CO2 is only associated with occasional headaches and nausea — probably because it is high in crowded rooms with little ventilation.
One large review in 2019 was described as showing CO2 affected people at levels as low as 1,000ppm, but the paper itself points at the confounding data and uses the words “possible” and “potential effects” and concludes “we need more studies.”
UPDATE: Commenters Alan Klein and Mr Farnham points out the safety limits for Australian coal miners (NSW) is 1.25% CO2 which is 12,500ppm, and that is for 8 hour shifts. Brief excursions up to 3% (30,000ppm) are acceptable. See comment #17 for more details.
REFERENCES
Lowther, Scott D., Sani Dimitroulopoulou, Kerry Foxall, Clive Shrubsole, Emily Cheek, Britta Gadeberg, and Ovnair Sepai. 2021. “Low Level Carbon Dioxide Indoors—A Pollution Indicator or a Pollutant? A Health-Based Perspective” Environments 8, no. 11: 125. https://doi.org/10.3390/environments8110125
Mishra AK, Schiavon S, Wargocki P, Tham KW. Respiratory performance of humans exposed to moderate levels of carbon dioxide. Indoor Air. 2021 Sep;31(5):1540-1552. doi: 10.1111/ina.12823. Epub 2021 May 15. PMID: 33991134.
Rodeheffer CD, Chabal S, Clarke JM, Fothergill DM. Acute Exposure to Low-to-Moderate Carbon Dioxide Levels and Submariner Decision Making. Aerosp
Zhang X, Wargocki P, Lian Z, Thyregod C. Effects of exposure to carbon dioxide and bioeffluents on perceived air quality, self-assessed acute health symptoms, and cognitive performance. Indoor Air. 2017 Jan;27(1):47-64. doi: 10.1111/ina.12284. Epub 2016 Mar 7. PMID: 26825447.
h/t to Willie Soon, Marc Morano and Climate Depot.
Chinese Scientists Propose Magnetic Launcher on Moon to Send Resources to Earth – Reports
Sputnik – 18.08.2024
BEIJING – Chinese scientists proposed building a magnetic launcher on the Moon, which could become an cost-effective way to deliver resources mined on the lunar surface to Earth, and, in addition, part of the Russian-Chinese lunar station project, Chinese media reported on Sunday.
According to the publication, scientists from the Shanghai Institute of Satellite Engineering suggest that the magnetic levitation installation will work on the same principle as the hammer throw in athletics, but the rotation at increasing speed will be carried out before a cargo capsule is sent to Earth.
Scientists are convinced that, due to the unique environmental conditions on the Moon, such as high vacuum and low gravity, payloads can be sent twice a day, and the cost of such transportation will be about 10% of the cost of existing methods.
“The system’s technical readiness is relatively high. Since it consumes only electricity and does not require any propellant, it will be relatively small in scale and straightforward to implement,” the scientists said in their paper.
They also noted that the main task will be the extraction of helium-3 to help solve the problem of the energy crisis on Earth. The project, in their opinion, will also contribute to the development of space mining technologies, heavy launch vehicles and artificial intelligence.
The proposed launch system will use a 50-meter-long rotating arm and a high-temperature superconducting engine to launch capsules with mined resources. Ten minutes after launch, the rotation speed of the arm will reach the second cosmic velocity of the Moon of 2.4 kilometers per second and about one-sixth of the second cosmic velocity of Earth — and put it on the correct trajectory for returning to Earth.
The system is designed to last at least 20 years, but it will weigh about 80 tonnes, so before it can be delivered to the Moon, it will be necessary to wait for the start of operation of the Chinese super-heavy launch vehicle, the publication said.
The team working on the project suggested that it could be part of a proposed joint Russian-Chinese project to build a research station at the south pole of the Moon by 2035.
The intergovernmental Russian-Chinese agreement on the joint creation of the International Scientific Lunar Station (ISLS) was signed on November 25, 2022. Russian President Vladimir Putin signed a law ratifying the agreement on June 12, 2024, and it entered into force on July 18. The document was published on July 25. It indicates that the station will be created in three phases and will receive modules both on the surface of the Earth’s natural satellite and in its orbit. During the third phase, it is planned not only to study and develop the Moon, but also to assist other countries in landing on the Moon. The implementation dates for each of the phases are not yet mentioned.
UK rejects payment to Covid-19 jab victims for not being ‘disabled enough’ – Telegraph
RT | August 18, 2024
Almost 14,000 people in Britain have applied for payments from the government for disabilities they claim were caused by Covid-19 vaccines, The Telegraph has reported.
Only 175 people, or less than 2% of those seeking compensation, have so far received a one-off money transfer of £120,000 ($155,300), the paper said in an article on Saturday.
Data obtained by The Telegraph through Freedom of Information requests indicates that those who were eventually reimbursed suffered from conditions such as stroke, heart attack, dangerous blood clots, inflammation of the spinal cord, excessive swelling of the vaccinated limb, and facial paralysis.
Around 97% of the satisfied applications were related to the Oxford-AstraZeneca Covid-19 vaccine, developed by Oxford University and British-Swedish company AstraZeneca, and the rest to the US-made vaccines from Pfizer and Moderna, it said.
The outlet noted that the UK government continued to recommend the AstraZeneca vaccine, despite its use being halted in Germany, Italy, France, and other European countries by March 2021, amid reports of a growing number of blood clotting cases.
Thousands of people have been refused payment due to the government’s medical assessors arguing that there is no concrete proof that their health problems are a result of the vaccines, the report read.
Hundreds of others were turned down due to being “not disabled enough,” it added. Under the rules of the Vaccine Damage Payment Scheme (VDPS), an applicant has to be at least 60% disabled to qualify.
A spokesman for AstraZeneca told The Telegraph that its vaccine “has continuously been shown to have an acceptable safety profile and regulators around the world consistently state that the benefits of vaccination outweigh the risks of extremely rare potential side effects.”
As for the health complications caused by the vaccine, the spokesman said, “our sympathy goes out to anyone who has lost loved ones or reported health problems.”
In May, AstraZeneca, which officially admitted that its vaccines could cause blood clots in certain cases, began the withdrawal of its product worldwide, saying that newer vaccines adapted to the latest coronavirus variants were more effective.
Around 16,000 people have sought payments since the introduction of the VDPS in 1979, with most of the claims related to Covid-19 vaccines. The growing workload resulted in an increase of the staff responsible for handling applications from four people to 80 last year. “We continually review our processes to further develop the way in which we manage claims, and to provide a better service for claimants,” a National Health Service spokesperson said.
Health Officials Push Whooping Cough Vaccine Amid Uptick in Cases, But Scientists Say Shots Don’t Prevent Transmission
By Suzanne Burdick, Ph.D.John-Michael Dumais | The Defender | August 14, 2024
Public health officials are urging families to get vaccinated against whooping cough, citing an uptick in cases, particularly among adolescents. However, critics say the vaccine doesn’t prevent transmission and contains dangerous toxins that may harm human health.
Connecticut Department of Public Health Commissioner Manisha Juthani said that there were 111 confirmed cases of pertussis in the state so far in 2024 — nearly a 10-fold increase compared to 2023, NBC Connecticut reported this week.
Juthani told The Hour that public health officials are concerned the spread will increase when school begins in just a few weeks.
“We are raising attention to this, both to providers and to families,” she said, “so that theoretically, people can get back up to date on their vaccines before children potentially are going back to day care, are going back to school.”
Other states, including New York and Pennsylvania, have also seen an uptick in whooping cough cases this year, Newsweek reported in early June. Outside the U.S., the United Kingdom and Australia have also reported increases.
Whooping cough, also known as pertussis, is a highly infectious respiratory tract infection, according to the Mayo Clinic. Deaths from it are rare and typically occur in infants.
It’s caused by a bacteria called Bordetella pertussis, according to the Centers for Disease Control and Prevention (CDC).
The CDC recommends that “everyone” — from babies as young as 2 months old to adults, particularly pregnant women — vaccinate against the illness by getting either a DTaP or Tdap vaccine, which also ostensibly protect against tetanus and diphtheria.
According to the CDC, the vaccine is “the best way to prevent whooping cough.”
Pertussis can be treated with antibiotics
However, Karl Jablonowski, Ph.D., senior research scientist at Children’s Health Defense (CHD) told The Defender the pertussis vaccine may contribute to the spread of the infection — because it doesn’t prevent transmission.
“The pertussis vaccine is one of those that breaks the mold of what we think a vaccine is,” Jablonowski said. “Pertussis is probably the best case I can think of for a vaccine that does not prevent transmission.”
He added, “Every time there is a case of it, health officials will get on TV urging people to get vaccinated — wrongfully believing it will stop transmission.”
As The Defender recently reported, the CDC has been tracking changes in the prevalence of bacteria causing whooping cough for years.
Although the CDC’s whooping cough website still says the illness is caused by Bordetella pertussis, the most recent CDC data found that the Bordetella parapertussis type of whooping cough has significantly overtaken Bordetella pertussis in prevalence — and according to research published in Vaccines in March, the existing vaccines “scarcely provide protection” against this strain.
Brian Hooker, Ph.D., CHD chief scientific officer, told The Defender pertussis can be treated with antibiotics — “erythromycin and azithromycin are standard,” he said — and high doses of vitamin C.
The CDC’s website acknowledges whooping cough can be treated with antibiotics and fails to explain why the agency favors vaccination over antibiotics.
Pertussis vaccine may prevent herd immunity
Earlier this year, Jablonowski spoke on the poor efficacy and high-risk profile of the pertussis vaccine before Tennessee lawmakers as they weighed a bill to prohibit the state’s Department of Children Services from “requiring an immunization as a condition of adopting or overseeing a child in foster care if an individual or member of an individual’s household objects to immunization on the basis of religious or moral convictions.”
During March testimony before the Tennessee General Assembly Civil Justice Committee, Jablonowski cited scientific studies that debunk the notion that the vaccine is the best way to prevent whooping cough.
For instance, a 2016 review published in JAMA that reviewed more than 10,000 whooping cough cases found that more than half the cases in the five largest statewide outbreaks occurred in individuals who were partially or fully vaccinated against pertussis.
A 2019 review published in the Journal of the Pediatric Infectious Disease Society concluded that “all children who were primed by DTaP vaccines will be more susceptible to pertussis throughout their lifetimes, and there is no easy way to decrease this increased lifetime susceptibility.”
Another review, also published in 2019, concluded that pertussis vaccines “do not reduce the circulation of B. pertussis and do not exert any herd immunity effect.”
Jablonowski told lawmakers that not only does the pertussis vaccine not “exert” a herd immunity effect, but the vaccine “has a negative effective on herd immunity.”
He explained:
“A vaccinated person can asymptomatically carry and transmit the disease, and cannot then learn how to fight it naturally.
“If you accept that in order to achieve herd immunity 90% of the population needs to not retransmit the bacteria once exposed to it, then once you have vaccinated more than 10% of the population herd immunity becomes impossible, as the vaccinated citizens will be contracting and transmitting the disease.”
Jablonowski told The Defender the only two scenarios in which getting the vaccine might protect someone else is when it’s given during pregnancy or to a nursing mother.
According to the CDC, pregnant women should get the Tdap vaccine to provide their babies with the “best protection” from whooping cough, ideally between 27 and 36 weeks gestation. Protective antibodies pass from the pregnant woman’s body to the fetus, the agency said.
Researchers funded by the pharmaceutical company Sanofi — which sells pertussis vaccines — in 2022 published a statement saying that vaccination against pertussis during the second or early third trimester of pregnancy is “highly protective” against pertussis in young infants.
Both the CDC and Jablonowski said that vaccinating nursing mothers doesn’t appear to be effective in protecting babies from whooping cough.
A 2012 study conducted in a Houston area hospital found that giving postpartum moms the Tdap vaccine didn’t reduce the number of infections in babies when compared to prior years in which the hospital didn’t readily give the vaccine postpartum.
The hospital implemented a standing order that all new mothers get Tdap, Jablonowski said.
The researchers looked at health data from moms and babies 7.5 years before and almost 1.5 years after this standing order, he said. “Cases of infant pertussis practically doubled and the mortality rate practically tripled” after the standing order.
Vaccine contains aluminum and formaldehyde
Both of the two current formulations of the pertussis vaccine contain toxins known to harm human health, including aluminum and formaldehyde, Jablonowski told the lawmakers.
Aluminum is a known neurotoxin that can affect more than “200 important biological reactions” and cause “negative effects on [the] central nervous system,” according to a 2018 paper published in the Journal of Research in Medical Sciences.
Formaldehyde is a known carcinogen that is toxic to the respiratory system, central nervous system, optic nerve, kidney, liver, testicles and other body systems.
The pertussis vaccine, typically administered as part of combination vaccines like DTaP or Tdap, contains several other potentially harmful ingredients. These typically include inactivated B. pertussis toxin and several of its components, polysorbate 80, gluteraldehyde, 2-phenoxoyethanol and in some cases, trace amounts of mercury, according to the National Vaccine Information Center (NVIC).
Some researchers suggest the chemically inactivated pertussis toxin in DTaP may retain some bioactivity, potentially inducing brain inflammation in certain individuals.
CDC didn’t follow up on 2012 report on adverse events following DTaP/Tdap vaccines
For the past 70 years, researchers have used the pertussis toxin in animal studies to purposefully trigger various physiological responses. Responses include heightened sensitivity to histamine, serotonin and endotoxins. Researchers also used the pertussis toxin to induce experimental autoimmune encephalomyelitis.
The toxin’s ability to penetrate the blood-brain barrier under certain conditions has long been a concern. This property makes brain inflammation, or encephalitis, and its potential for lasting neurological damage a particularly severe complication associated with both whooping cough infection and pertussis vaccination.
According to the Vaccine Adverse Event Reporting System (VAERS), from 1990 to 2024, there were 190,994 injury reports following pertussis-containing vaccines, including 3,377 deaths, according to NVIC. Over 85% of these deaths occurred in children under age 3.
While this data includes pre-1996 reports, when the whole-cell pertussis portion of the DTP vaccine formulation was changed due to its serious side effects, it’s important to note that a significant portion would be related to the DTaP vaccine given its widespread use since 1996.
Over 6,000 claims for injuries from pertussis-containing vaccines were submitted to the federal Vaccine Injury Compensation Program (VICP) as of Aug. 1, 2024. The cases include 872 deaths and over 5,000 serious injuries. Pertussis-containing vaccines comprise the highest number of VICP death claims and the second most compensated vaccine injury claims.
A 2012 study published in JAMA found an increased risk of febrile seizures in children 3-5 months old on the day of or day after receiving the first two doses of DTaP-containing vaccines.
The Institute of Medicine’s (IOM) 2012 report, “Adverse Effects of Vaccines: Evidence and Causality,” evaluated 26 reported adverse events following DTaP/Tdap vaccination. They included encephalopathy, encephalitis, chronic hives, autism, sudden infant death syndrome, arthritis, Guillain-Barré syndrome, diabetes mellitus, immune thrombocytopenic purpura, transverse myelitis and others.
For 24 of the 26 adverse events, the committee said there was not enough data either to support or reject vaccine-related causality, primarily due to a lack of adequate studies.
To date, the CDC has not conducted any additional studies in response to IOM’s recommendations, according to the authors of “Vax-Unvax: Let the Science Speak,” Hooker and Robert F. Kennedy Jr., CHD’s chairman on leave.
A 2017 study led by Dr. Anthony Mawson published in the Journal of Translational Science, compared the health outcomes of vaccinated and unvaccinated children ages 6-12. The study found that while vaccinated children had fewer cases of chicken pox and pertussis, they had significantly higher rates of other health issues.
According to the study, vaccinated children were more likely to be diagnosed with allergic rhinitis, eczema and neurodevelopmental disorders. The vaccinated group also showed higher rates of attention-deficit/hyperactivity disorder, autism, learning disabilities and chronic health problems.
Additionally, the study reported that vaccinated children had a higher incidence of pneumonia and ear infections compared to unvaccinated children.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The American Board of Internal Medicine Revoked All 3 Of My Board Certifications
Although I can still practice medicine, the ABIM’s actions against me and Paul Marik threaten the sanctity and autonomy of the physician-patient relationship.
Pierre Kory’s Medical Musings | August 17, 2024
I will just start by saying that I believe that the ABIM’s decision was 100% predetermined even before we first received their accusation in June 2022. There was no way they were going to declare us innocent of misinformation, even though a good portion of this country knows how effective and accurate our deeply evidence-based Covid treatment guidance was (and still is).
One of the reasons why they were never gonna let us off is that, if they declared us “innocent,” (i.e. accurate) that action would have immediately imperiled the decisions by medical boards across the country who persecuted hundreds of doctors for using ivermectin or hydroxychloroquine or for recommending against Covid-19 mRNA gene therapy products. More importantly, it could potentially launch hundreds of thousands of lawsuits by the families of patients who died due to lack of early treatments offerred by clinics and hospitals or filled by pharmacies.
The above examples which led to the deaths of so many shows the sheer power of mega-corporations that put their financial interests ahead of our health and our lives. Through their overwhelming influence over nearly every institution of society and Science (media, journals, health agencies, politicians, medical schools, physicians etc), they literally succeeded in depriving a whole country (and world) of the most effective, inexpensive, safe, and widely available treatments for Covid. My biggest worry is that this crime against humanity may never enter the history books and thus will be eventually erased from memory. Which is looking probable.
The massive financial opportunities that Covid immediately presented to Big Pharma were threatened by the “inconvenient truths” Paul and I put out there. This ABIM action is one way in which Big Pharma punishes those who are foolish enough to do so. Foolish is not quite the right word in our case as I would argue we were simply naive to the consequences of advocating publicly for the use of off-patent medicines for an immensely profitable disease. It wasn’t heroism as some think, but rather extreme naivete.
I really never thought I would have to lose/leave three jobs and now three Board certifications for speaking truths. Recall that I was very well known in my specialty prior to Covid and was about to become Full Professor when I resigned as Chief of the Critical Care Service at the University of Wisconsin (where I was also the Medical Director of the Trauma and Life Support Center). Reading the Washington Post article “Doctors Accused of Spreading Misinformation Lose Certification” was a pretty sobering reminder of how far I have supposedly “fallen” (Not so fun fact: they completely overstated my salary as the money I received in 2022 included retroactive pay for 2021).
But I am still standing folks. I am happily practicing medicine at my Leading Edge Clinic with my amazing partner Scott Marsland. As many know, we specialize in treating vaccine injury syndromes and Long Covid, and I believe we are soon closing in on having treated our 1,400th patient.
Thank God I managed to build a private, fee-based practice two and half years ago. At the time I suspected this was coming while also already aware that I was “unemployable” by the system. I got fired by my last hospital for a 100% made up complaint, despite the fact they desperately needed me. I was an independent contractor at the time and my ICU partners and all the nurses really liked me. But my partners were telling me that they were under increasing pressure by the Chief Medical Officer to “get rid of Kory.” Although they initially resisted, my stance on vaccines started to cause even more problems for them. When the ICU Director, who was both a friend and a colleague, called to fire me, his last words were, “Pierre, I know there is a war going on and unfortunately you are a casualty.” Truer words were never spoken.
Just know that Board certification is not a license to practice medicine (that comes from state medical licensing Boards of which I have more than a few still). But this ABIM action now puts a definitive end to any hope of me returning to an academic or “system” position (not that I have that hope anymore). Why is that? Well, because Board Certification was originally just a badge of distinction that doctors could use to impress each other and their patients. But they have since weaponized and monetized Board Certification in that currently you cannot obtain a faculty appointment at an academic medical center without one. Nor can you work for most hospitals without one. Even worse, insurance plans will not put you on their provider panels without it. So, although I have been fully excommunicated from “the system,” I cannot be happier about it.
Understand that what happened to me this week was a devastating censorship action, plain and simple. It was done for two reasons; the first was to destroy my reputation and credibility so that my voice will no longer carry (essentially silencing me) and the other was to send a message to doctors that if they stray from consensus, no matter how scientifically absurd (e.g. mRNA vaccines for a coronavirus), dangerous (e.g. remdesivir, mRNA jabs), or ineffective (Paxlovid), they will be punished.
The damage that will result to patients again, is incalculable. No longer will “system” doctors be able to practice medicine with the autonomy they require to arrive at the best decision for each individual patient. Nearly everything they do will be protocolized with society guideline recommended treatments (i.e. consensus manufactured by Pharma). No longer will they be able to “think out of the box” or use treatments which although known effective, do not have the blessing of those in control of that system. I am as terrified as ever of needing a hospital.
Not to overstate the importance of their actions, but Medicine as I knew it, or thought I knew it, is even more dead if that is possible. If you can’t have a differing scientific opinion without losing your career over it, then how is that Medicine or Science? In fact, in our repeated written defenses, we challenged the ABIM, asking them where “the line” is between legitimate scientific debate driven by a differing emphasis on or interpretation of data and outright misinformation.
Misnformation, as I understand it, is defined as “incorrect or misleading” information. For us to be misinformationists, in my mind, would mean that all the data from trials and studies that exist for therapeutics in Covid;
- the overwhelming preponderance of data for the efficacy and safety of ivermectin in Covid shows it to be ineffective and dangerous
- the overwhelming preponderance of data for the vaccines show they are safe and effective
Basically, it comes down to how you interpret the body of evidence which currently exists. Paul and I adhered rigidly to a “totality of the evidence” approach, drawing from in-vitro, in-vivo, clinical and epidemiologic data. All of it lined up in a truly magnificent, inspiring, and unprecedented way. Well, except for the “Big 7 RCT’s” which manipulated the design, conduct and analyses to conclude ivermectin was ineffective. I spent literally hundreds of hours (along with others like Alexandros Marinos), publishing critiques which exposed the most absurd scientific misconduct I had ever witnessed. If interested, here are just some of those critiques, e.g. Oxfords’ PRINCIPLE trial, the TOGETHER trial (three parts, here, here, and here, and the NIH ACTIV-6 trial )
We also evolved with the data, unlike the agencies who had quickly determined in December of 2020 that the vaccines were safe and effective and never, ever veered from that stance up until this day. In contrast, the founding members of the FLCCC, for quite a long time, differed in respect to the efficacy, safety, and need for the mRNA vaccines. I was the first and most vocal against the mRNA vaccines (starting in April 2021) which actually almost led to the breakup of the FLCCC or at least the membership of the original 5.
Prior to April 2021 I was simply neutral/skeptical. That skepticisim was due to what I thought might be folly in trying to vaccinate against a coronavirus (I knew that historically coronavirus vaccines had failed because the vaccinated animals developed antibody dependent enhancement and also that coronaviruses mutate rapidly). Then I did my first deep dive on VAERS and the epidemiologic data showing massive spikes in mortality and hospitalizations timed with the rollout of the jabs across dozens of countries. Voila, I was now “anti-vaxx.”
I continued to track and analyze the ever-emerging data and the horrors they revealed. This work ultimately led the FLCCC to reach an internal “consensus” that the vaccines should be avoided at all costs (literally at all costs as none of the costs incurred by taking the jab were worth someones life). Anyway, I just wanted to show that we evolved with the data, always questioning and reviewing as new data emerged.
I will end by reminding all of how dangerous the ABIM’s actions will be to all of our lives because it will further erode and/or literally destroy the patient-physician relationship. As I wrote in a previous Op-ED in the Daily Caller on January 31, 2023, “A War Is Still Being Waged Against Doctors Who Question Covid Orthodoxy:”
By virtue of their professional training, doctors must advise patients on available treatments and known risks of any treatment or procedure. By threatening doctors who might provide information different than their preferred worldview, ABIM is disrupting the doctor-patient relationship.
When allowed to practice their craft freely, physicians can prevent societal disaster by focusing on individual patients, informed by clinical experience.
Groups like the ABIM, and public medical officials like Fauci, should support and encourage evidence-based debate and patient-centered care.
Instead, they have suppressed both that debate and treatment approach by persecuting its proponents. This campaign must be stopped, its origins and evolution must be thoroughly documented, and it must never be allowed to recur. Physician autonomy must be restored lest all patients suffer.
‘Medical Warfare’: Doctors Who Questioned COVID Shots, Promoted Ivermectin Lose Certification
By Michael Nevradakis, Ph.D. | The Defender | August 14, 2024
Two doctors who spoke out about vaccines and alternative treatments for COVID-19 received notice that their medical certifications were revoked, while another doctor said her certification was revoked without her knowledge.
The American Board of Internal Medicine (ABIM) last week revoked the certifications of Drs. Pierre Kory and Paul Marik, following a two-year investigation into their promotion of ivermectin and hydroxychloroquine as treatments for COVID-19 and their statements questioning the safety and efficacy of COVID-19 vaccines.
According to The Washington Post, the two physicians continued “to promote ivermectin, an anti-parasitic medication, as a treatment for COVID long after the medical community found it to be ineffective.”
Kory and Marik are co-founders of the Front Line COVID-19 Critical Care Alliance (FLCCC), which promotes alternative treatments for COVID-19.
Citing unnamed experts, the Post claimed the FLCCC “spread misinformation about the coronavirus pandemic.”
MedPageToday quoted an ABIM spokesperson, who said the organization “does not comment publicly on the reasons for the revocation of certification.”
However, in a summary of the ABIM’s decision reviewed by The Defender, the organization stated that the doctors’ “conduct poses serious concerns for patient safety and undermines the trust that the public and the medical profession place in the meaning of ABIM board certification.”
In a press release, the FLCCC Alliance said it “categorically disagrees” with ABIM’s decision.
“We believe this decision represents a dangerous shift away from the foundational principles of medical discourse and scientific debate that have historically been the bedrock of medical education associations,” the press release states.
Marik told The Defender :
“The bottom line is we’re disappointed because we stand up for the truth. To censor science is to censor progress. Science is based on dialogue and people can have different points of view. That is the principle of science: it’s people having different points of view.
“We’ve never been in a situation before where physicians who have opposing points of view are silenced … It sets a really bad precedent that you can’t really challenge the status quo, and as we know, in medicine, there have been very dramatic changes based on changing understandings of science.”
In the FLCCC Alliance press release, Kory said, “This fight is about more than just our right to speak — it’s about protecting the future of healthcare. When doctors are silenced for questioning the prevailing narrative, we all lose.”
Kory and Marik participated in an ABIM hearing in May, but internist Dr. Meryl Nass, founder of Door to Freedom, told The Defender that ABIM revoked her certification without her knowledge.
Nass said she was blindsided by ABIM’s decision to revoke her license, which she said she found out about only when she searched for herself in the organization’s database of certified physicians.
Nass told The Defender :
“After the Maine Medical Board suspended my license illegally — even though none of my alleged transgressions met the statutory requirement for an immediate suspension — the board later found me guilty of things I had not done and continued the suspension … All of this with never a single patient complaint.
“Now I learn, by chance, that the ABIM has suspended me without ever informing me I was even under an investigation, which is illegal according to the ABIM’s process.”
Dr. Peter McCullough also faced similar difficulties with the ABIM over his positions on COVID-19 vaccines and treatments. According to MedPageToday, ABIM revoked his certifications in 2022 — although, as of today, ABIM lists him as certified.
McCullough told The Defender, “The ABIM is violating principles of equal protection, due process, rules of evidence and has gone ex post facto to find reasons to attack qualified ABIM-certified doctors who innovated and saved lives early in the pandemic.”
Science based on ‘different points of view’
Kory and Marik held ABIM certifications in internal and critical care medicine, while Kory was also certified in pulmonary disease, according to MedPageToday.
They were initially notified about the risk of losing their certification in May 2022. Last year, ABIM’s Credentials and Certification Committee recommended the revocation of their certification for disseminating “false or inaccurate medical information.” A hearing followed in May.
According to the FLCCC Alliance’s press release, Kory and Marik “tirelessly defended their positions.” However, despite “presenting over 170 references in a detailed 60-page response submitted in January 2023, the ABIM has chosen to dismiss these robust scientific contributions in favor of a narrow, ‘consensus-driven’ narrative.”
According to the summary of ABIM’s decision, Kory and Marik’s “statements about the safety and efficacy of ivermectin and hydroxychloroquine” as treatments for COVID-19 “are false and inaccurate because they are unsupported by factual, scientifically grounded, and consensus-driven medical information.”
The ABIM also addressed the doctors’ positions on the COVID-19 vaccines:
“[The doctors’] statements about the purported ineffectiveness and dangers of COVID-19 vaccines are false and inaccurate because they are unsupported by factual, scientifically grounded, and consensus-driven medical information. …
“There is extensive factual, scientifically grounded, and consensus-driven medical information demonstrating that the COVID-19 vaccines are safe and effective, and lead to better health outcomes.”
Marik questioned the board’s assertions regarding ivermectin, hydroxychloroquine and the vaccines.
“What they do is, they cherry-pick articles which support their point of view and then they go on to say the vaccine is safe and effective. We know that’s completely not true. There’s overwhelming data to question both the safety and efficacy of the vaccine,” Marik added.
McCullough said:
“ABIM never updated its members on important risks such as fatal vaccine adverse events, including myocarditis, nor failing theoretical efficacy necessitating boosters that skipped human testing altogether.
“Setting a new dark milestone, ABIM is decertifying highly qualified physicians for nonclinical reasons and ignoring the evidence for early therapeutics and COVID-19 vaccine safety.”
ABIM engaging in ‘medical lawfare’
According to the Post, Kory maintains a license to practice medicine in California, New York and Wisconsin, where “there are no disciplinary actions listed against him.” Marik has retired and his medical license expired in 2022.
Revocation of their ABIM certification “effectively prevents them from practicing at large hospitals and academic institutions,” the Post reported.
Marik and Nass outlined the difficulties of practicing medicine without certification.
“It doesn’t affect us directly, but it affects us indirectly because we’re being accused of committing offenses that are just not true,” Marik said. “The indirect impact to our reputation … it’s a slap in the face, basically, for all the hard work we’ve done.”
Accusing the ABIM of being part of the “medical-industrial complex,” Marik said, “They seem more interested in making money than in protecting physicians. There have been a number of lawsuits against ABIM, so they don’t have the best of reputations. But unfortunately, they are the main certifying organization in the U.S., so they have enormous power and leverage.”
“If I get my license back — a big if, without board certification, I would have great difficulty getting hospital privileges and collecting insurance reimbursements. In other words, I would be unemployable, though I could potentially work on my own if patients paid me directly,” Nass said.
In 2021, ABIM and the Federation of State Medical Boards collaborated to draft the statement used to discipline Nass.
Nass said organizations like ABIM are engaging in “medical lawfare.” She said they are:
“Creating crimes that do not exist, using procedures that do not exist, to try and silence people like me. What did I do wrong? I read the literature and told the truth about what it said, publicly. The COVID vaccines are very dangerous. They don’t prevent COVID. Drugs can effectively treat COVID. And I prescribed those drugs and helped hundreds of Maine citizens. That was my crime.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Whistleblower Will Appeal After Federal Court Dismisses Lawsuit Alleging Fraud in Pfizer COVID Vaccine Trials
By Michael Nevradakis, Ph.D. | The Defender | August 13, 2024
For the second time, a federal court in Texas has dismissed a whistleblower lawsuit alleging Pfizer and two of its contractors manipulated data and committed other acts of fraud during clinical trials for the Pfizer-BioNTech COVID-19 vaccine in 2020.
In his Aug. 9 ruling, District Judge Michael J. Truncale sided with the U.S. government, ruling the government had demonstrated “good cause” to intervene and dismiss the case. He wrote:
“The Government’s desire to dismiss the case — because of its doubt as to the case’s merits, differing assessment of the Pfizer vaccine data, desire to avoid discovery and litigation obligations, and belief that it should not have to expend resources in a case that is contrary to its public health policy — constitutes good cause to intervene.”
Whistleblower Brook Jackson filed the lawsuit against Pfizer, Ventavia Research Group — which conducted some of the clinical trials for Pfizer’s COVID-19 vaccine — and Pfizer contractor ICON PLC in January 2021. Jackson’s complaint was most recently amended in October 2023.
Jackson, a former Ventavia employee, alleged the companies committed numerous violations of the False Claims Act (FCA) during the clinical trials.
According to the lawsuit, the three companies “deliberately withheld crucial information from the United States that calls the safety and efficacy of their vaccine into question,” thus defrauding the federal government, which purchased the vaccines.
The FCA allows the government or a party suing on its behalf to attempt to recover money for false claims made by parties to secure payment from the government.
The FCA also allows whistleblowers to be rewarded for confidentially disclosing fraud that results in a financial loss to the government.
While whistleblowers have the right to sue under the FCA, the federal government can choose to intervene in the case at a later date. In Jackson’s lawsuit, the U.S. government initially declined to intervene in February 2022. However, in March, the government filed a motion to intervene and to dismiss the case.
Attorney Warner Mendenhall, one of the lawyers representing Jackson, questioned whether the U.S. government’s “public health policy” is tolerant toward allegations of fraud during clinical trials for vaccines.
In an interview Monday with Sasha Latypova, a former pharmaceutical industry executive with 25 years of experience in pharmaceutical research and development, Mendenhall said:
“What’s the public health policy of the United States? To kill people and damage people and injure people and make them sick? If that’s the public health policy, well then yes, we’re inconsistent with that.”
Latypova told The Defender she was “not really surprised” by the ruling, noting that drugmakers enjoy legal immunity afforded by emergency use authorization granted by the U.S. Food and Drug Administration (FDA). Latypova described this immunity as a “legal cage.”
She said “The court took as evidence an unsubstantiated opinion of two government bureaucrats … published in an editorial article of a medical journal,” but did not consider the extensive evidence of wrongdoing Jackson provided.
The government’s motion to dismiss cited a Jan. 5 JAMA editorial authored by FDA Commissioner Robert Califf and the FDA’s Center for Biologics Evaluation and Research Director Peter Marks, claiming that “data from various studies” show that “tens of millions of lives were saved by vaccination.”
During his interview with Latypova, Mendenhall argued the government failed to demonstrate good cause and that last week’s ruling did not name any specific examples of this. He said:
“If you read the actual document, there’s no cause listed at all. In fact, the judge has a footnote saying, ‘There is no cause here, but I’m going to look at this other motion I think I can find’ … that’s not how courts are supposed to proceed. You look at the motion first to intervene for good cause. If it’s not there, you’re done. You don’t get to go on and look at the motion to dismiss for hints that maybe there is good cause.”
The ruling also stated that Jackson “failed to allege that she complained to Ventavia or the FDA about fraud against the government.” Accordingly, her claims don’t “rise to the level of protected activity” as a whistleblower.
Mendenhall told Latypova this poses “constitutional concerns” and may have “a chilling effect on other whistleblowers.”
Jackson has 30 days to appeal the ruling, and plans to, Mendenhall said.
“I am very confident we’re going to win that case and get, at least, the retaliation [claim] vindicated, and vindicate what she did as a conscientious citizen of the United States,” Mendenhall said.
Jackson fired within six hours of submitting claims to the FDA
Ventavia, which operated several sites where it conducted clinical trials on behalf of Pfizer, hired Jackson in September 2020.
That same month, Jackson reported problems she observed with the Pfizer vaccine trial to the company’s management. When management didn’t respond, she took her claims to the FDA on Sept. 25, 2020. Ventavia fired her later that day.
Jackson, who had over 15 years of experience working with clinical trials, claimed she “repeatedly informed her superiors of poor laboratory management, patient safety concerns and data integrity issues.”
She also gave The BMJ a cache of internal company documents, photos and recordings highlighting alleged wrongdoing by Ventavia.
“Her job was to fix things. They wouldn’t fix them. She reported it to the FDA, and six hours later was fired from her job,” Mendenhall said.
He added:
“There was not informed consent. They were making up records. I mean, it was just endless. They were violating patient privacy, which is critical in a clinical trial because you have to not know who’s getting the shot in order to determine any effectiveness.
“Basically, the allegations that she brought forward show that the clinical trial that she saw, what she saw of it, was essentially worthless. It wasn’t valuable or useful data.”
Jackson filed her qui tam lawsuit under the FCA in January 2021. A qui tam action refers to any legal case where a private citizen initiates legal action on behalf of a state.
Documents released in November 2021 supported Jackson’s claims that she was directly involved in the Phase 3 trials for the Pfizer-BioNTech COVID-19 vaccine.
‘Level of ignorance’ of scientific facts by government officials ‘astounding’
In February 2022, the federal government declined to intervene in the lawsuit on Jackson’s behalf but reserved the right to intervene at a later date.
Later that month, Jackson filed her first amended complaint, while the court unsealed 400 pages of exhibits.
In July 2022, Pfizer asked the court to dismiss Jackson’s lawsuit on the basis that the U.S. government was aware of wrongdoings in the clinical trials but continued to do business with the vaccine maker. In March 2023, Truncale granted the motion to dismiss, ruling that Jackson had not proved the companies violated the FCA.
Jackson appealed the dismissal in April 2023, and in August 2023 submitted a motion to file a second amended complaint, which was granted in September. Jackson filed her second amended complaint in October 2023.
Pfizer and Ventavia filed motions to dismiss the second amended complaint later in October 2023, while the U.S. government filed its motion to intervene and dismiss in March 2024. Oral arguments discussing the motions to dismiss took place on May 1.
“What happened in the interim here while we’re fighting the case and moving forward, apparently the government itself decided that what we were doing in exposing Pfizer and Ventavia and ICON, the three companies involved here, was contrary to the public health policy in the United States,” Mendenhall said.
In ruling in favor of the government, the court cited a 2023 U.S. Supreme Court decision that gave the government significant leeway concerning when it could intervene in an FCA case and on what basis.
According to Mendenhall, this occurred despite meetings Jackson and her legal team had last year with representatives of the U.S. Department of Justice (DOJ), during which he said they “were completely unaware” of evidence questioning the safety of the COVID shots, including SV40 DNA contamination and vaccine injuries.
Mendenhall said:
“The level of ignorance about the scientific facts that we have uncovered was astounding to me, for someone who is supposed to be in charge of a major decision on behalf of the United States’ people, whether these shots need to be pulled from the market, whether Pfizer needs to be prosecuted or at least held civilly liable along with the other companies.
“I think that, certainly for some in the government, they just don’t want to face what they’ve actually done … they have hurt, damaged the health of millions of Americans and tens of millions, at least, around the world.”
According to Mendenhall, government attorneys were “actually sitting on the side of the courtroom with Pfizer” attorneys during the May 1 hearing.
“How strange that was to have the defendants sitting with the government who’s supposed to be going after them,” Mendenhall said.
In April, Pfizer submitted a statement to the court in support of the U.S. government’s motion to intervene and dismiss.
Pfizer previously was fined in connection with the FCA. As part of a 2009 settlement, the company paid $2.3 billion in fines — the largest healthcare fraud settlement in the history of the DOJ — stemming from allegations of illegal marketing of off-label products not approved by the FDA.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Featured Video

Did the 9/11 Hijackers Really Fly the Planes?
or go to
Aletho News Archives – Video-Images
Book Excerpt
Biden’s Closed Circle on Russia
An excerpt from ‘The Great Betrayal’
By James W. Carden | The Realist Review | June 14, 2026
Joe Biden’s presidency may ultimately come to be seen as a cautionary tale. Here was a president who showed little interest in entertaining arguments that might have contradicted his most deeply held assumptions.[1] And there were precious few within the upper ranks of the administration who might have attempted to do so, after all, only policy hands and political operatives who had come up through the ranks of the Clinton and Obama administrations or had longstanding ties to the citadels of the foreign policy community were invited into the fold. … continue
Blog Roll
 Aletho News
Aletho News- UN: Israel continues to violate Lebanon airspace in defiance of Iran-US MoU
- Araghchi: Israeli occupation of Lebanese land a violation of MoU
- Hezbollah fighters confront intruding Israeli forces in southern Lebanon
- The Straight of Hormuz is Open for Iranian Business… Oil is Moving and Iran is Getting Paid
- Biden’s Closed Circle on Russia
- Lebanon Accuses Israel Of Violating The Chemical Weapons Convention By Spraying Toxic Herbicide Over Farmland
- Did the 9/11 Hijackers Really Fly the Planes?
- ‘Jewish lobby’ deceived Putin – Lukashenko
- The UK Joins the Pirates
- Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report
- If Americans Knew
- The Forward’s Hit Piece on Thomas Massie and USS Liberty Veterans
- Israel’s former defense minister compares settler ideology to Nazism
- The Pro-Israel Lobby’s Quiet Cash Shuffle
- Trinity Broadcasting Network (TBN) Propagandizes for Israel’s Wars
- A grim milestone: Gaza’s death toll surpasses 73,000 – Daily Update
- Jared Kushner’s Israel-linked island, and other dubious projects
- Why Are Crypto Billionaires and AIPAC Spending $8+ Million to Elect Adrian Boafo?
- Why the Mainstream Media Should Stop Using the ADL as Their Go-To Antisemitism Source
- Censorship and Thuggery Won’t Save Israel’s Reputation
- Israel Searches for a Red Sea Foothold in Somaliland
- No Tricks Zone
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
