Could Bird Flu Be the October Surprise?
By Clayton J. Baker, MD | Brownstone Institute | September 21, 2024
Bird flu was the hot topic in pandemic fear-mongering until very recently. Just a few months ago, former CDC director Robert Redfield publicly described Bird flu (also known as H5N1 Influenza A or Avian Influenza virus) as the likely next pandemic – predicting a laboratory-leaked virus as the cause. Meanwhile, Deborah Birx, aka the “Scarf Lady” of Covid infamy, was making the TV news, promoting an unrealistic and excessive program of testing farm animals and humans for Bird flu.
At present, bird flu seems to have been put on the back burner by the authorities. Monkeypox has since taken center stage, with the World Health Organization declaring a state of emergency over that virus. Furthermore, the “experts” have trotted out numerous other viruses with which to terrify the public. Examples include West Nile virus – who no less than Anthony Fauci himself supposedly contracted – and even the exotic “Sloth virus” (also known as Oropouche virus).
The first step in dealing with these continual reports of horrific pathogens is recognizing the vital importance of living in knowledge rather than in fear. “Fear porn” is a real psychological weapon and one that is being used against us on a daily basis. As we painfully learned during Covid, a terrified population is easily manipulated, controlled, and exploited. As free citizens, we must remain mindful and knowledgeable, rather than fearful, about the flood of information and propaganda that is hurled at us.
Regarding bird flu, we should remain mindful of the following. In its current iteration, bird flu has caused no widespread human illness, no human deaths, and sporadic outbreaks in farm animal populations. However, there is much evidence that bird flu could be used as a bioweapon. Furthermore, it could also be applied to disrupt the November 5 US Presidential election.
Here are 3 reasons why bird flu may still be weaponized to alter the election:
- Multiple bio labs in the United States and abroad – such as the lab run by Yoshihiro Kawaoka, PhD at the University of Wisconsin – perform alarming Gain-of-Function research on the H5N1 virus, making variants of the virus that are much more dangerous to humans than variants that occur in nature. These labs have had leaks with alarming frequency. The current strains of bird flu in the US show strong genetic evidence of having originated in a laboratory. A laboratory leak of a new strain of the virus, manipulated to be highly transmissible and/or pathogenic in humans, remains a real possibility.
- The “International Bird Flu Summit” will be held on October 2-4, 2024 at the Hilton Fairfax in Fairfax, VA – just outside Washington, DC – exactly one month prior to the election. Listed topics include “Command, Control and Management,” “Emergency Response Management,” and “Surveillance and Data Management.” If this sounds eerily reminiscent to you of the Covid lockdowns – which were also closely preceded by government-based planning exercises – your memory serves you well.
- The infrastructure is already in place for a “pandemic” of bird flu, much more than it is for other potential pathogens. Already, widespread testing of farms is underway. The development of bird flu vaccines has increased dramatically. The FDA has already approved vaccines made by Sanofi, GSK subsidiary ID Biomedical Corporation of Quebec, and CSL Seqirus, while Moderna recently received a $176 million government grant for its mRNA-based bird flu injection, which is in development.
In the bigger picture, a number of viruses could potentially be employed as an “October Surprise” to disrupt the election. Bird flu appears to be a leading candidate (pun intended), but it is not the only one.
We, as citizens, must remain vigilant to this threat to our electoral process. We should contact our local and state officials now, before anything is attempted, and express our absolute insistence on fair, legal, and regular elections. We should share this information widely with others so that all are aware of what might be attempted. Over the longer term, we must work to end Gain-of-Function research.
With Covid, we experienced first-hand what can be done to our civil rights and to our Constitutionally guaranteed electoral and governmental processes when a fear-driven, emergency-based takeover of society occurs. As free citizens, we must never allow this to happen again. From now on, we must live in knowledge, not in fear.
C.J. Baker, M.D. is an internal medicine physician with a quarter century in clinical practice. He has held numerous academic medical appointments, and his work has appeared in many journals, including the Journal of the American Medical Association and the New England Journal of Medicine. From 2012 to 2018 he was Clinical Associate Professor of Medical Humanities and Bioethics at the University of Rochester.
They Think We Are Stupid, Volume 11
Everything you need to know about our ruling class’s opinion of you
By Aaron Kheriaty, MD | Human Flourishing | September 19, 2024




New Report: State Department Funded Fact-checkers to Censor ‘Lawful Speech’
By Michael Nevradakis, Ph.D. | The Defender | September 18, 2024
The U.S. Department of State-funded domestic and international fact-checking entities that censored American independent media outlets and social media users who questioned the Biden administration’s COVID-19 and other policies, according to a congressional report.
The report by the U.S. House of Representatives Committee on Small Business stated:
“The Federal government has funded, developed, and promoted entities that aim to demonetize news and information outlets because of their lawful speech.”
The government’s actions fueled “a censorship ecosystem” that suppressed “individuals’ First Amendment rights” and “the ability of certain small businesses to compete online.”
The report focused on the State Department’s Global Engagement Center (GEC), which promoted and funded “tech start-ups and other small businesses in the disinformation detection space … with domestic censorship capabilities.”
The “fact-checking” firms named in the report include the International Fact-Checking Network — owned by the Poynter Institute — and NewsGuard.
The International Fact-Checking Network, established in 2015, has received funding from another State Department-affiliated group, the National Endowment for Democracy — and from Google, the Open Society Foundations and the Bill & Melinda Gates Foundation.
According to the House report, the federal government “assisted the private sector in detecting alleged MDM [misinformation-disinformation-malinformation] for moderation” and “worked with foreign governments with strict internet speech laws,” including European Union member states and the United Kingdom, to censor speech.
The report determined that the GEC and the National Endowment for Democracy violated international restrictions by “collaborating with fact-checking entities” to assess the content of domestic media outlets.
The “fact-checking” operations targeted independent media outlets, and as a result, “the scales are tipped in favor of outlets which express certain partisan narratives rather than holding the government accountable.”
Whether the State Department’s actions rise to “unconstitutional violations of the First Amendment is currently before the courts,” the report stated.
The State Department and several GEC officials are defendants in Murthy v. Missouri, a lawsuit alleging the Biden administration colluded with social media to censor free speech.
Children’s Health Defense (CHD) and its chairman on leave, Robert F. Kennedy Jr., are plaintiffs in Kennedy v. Biden, a similar lawsuit that last year was consolidated with Murthy v. Missouri.
The Poynter Institute is a defendant in another censorship lawsuit, CHD v. Meta, that CHD filed against Facebook’s parent company.
NewsGuard partnered with CDC, WHO to censor online content
According to the report, NewsGuard used money it received from the GEC and the U.S. Department of Defense to fund efforts to lower the advertising revenue “of businesses purported to spread MDM.”
“A system that rates the credibility of press is fatally flawed as it is subject to the partisan lens of the assessor, making the ratings unreliable,” the report states.
NewsGuard leveraged taxpayer dollars to develop Misinformation Fingerprints, a product that “catalogues what it determines to be the most prominent falsehoods and ‘misinformation narratives’” circulating online, “essentially outsourcing the U.S. government’s perception of fact to NewsGuard,” the report states.
NewsGuard later partnered with dozens of companies, organizations, universities and media outlets, including the Centers for Disease Control and Prevention, the Office of the Surgeon General and the World Health Organization (WHO).
“During the pandemic, the WHO enlisted NewsGuard for its input, including regular reports, on which COVID-19 narratives it determined to be misinformation were prevalent online,” the report states. “The WHO then contacted social media companies and search engines asking them to remove this content.”
‘Nobody wanted’ fact-checkers until ‘actual truths started getting out’
Tim Hinchliffe, publisher of The Sociable, told The Defender, “These so-called ‘fact-checkers’ are not in the business of actually checking facts. They are in the business of controlling narratives … Nobody wanted or needed these organizations until actual truths started getting out.”
Catherine Austin Fitts, founder and publisher of the Solari Report and former U.S. assistant secretary of Housing and Urban Development, told The Defender the government increasingly relies on censorship to promote its favored narratives.
“They need to institute more and more censorship,” Fitts said. “It’s hard to refute the gaslighting that flows from this imagination factory.”
Francis Boyle, J.D., Ph.D., professor of international law at the University of Illinois, told The Defender he wasn’t surprised that the State Department is “working to censor those who disagree with U.S. government policies and their globalist agenda.”
The report recommends that no federal funds “should be used to grow companies whose operations are designed to demonetize and interfere with the domestic press” and that federal agencies “should not be outsourcing their perception of fact to speech-police organizations subject to partisan bias.”
GEC also faces the loss of its government funding. According to the Washington Examiner, “A provision through the annual State Department appropriations bill, which passed the House this summer and will be negotiated in the Senate, aims to ban future checks to the GEC.”
But for Boyle, this is not enough. He said the State Department has, “at a minimum,” committed “the federal crime of conspiracy to defraud the U.S. government.”
Censorship ‘a pendulum that swings both ways’
The Gateway Pundit last week reported on additional links between the International Fact-Checking Network, other “fact-checking” firms and Big Tech.
In 2015, Poynter partnered with Google News Lab, which earlier that year, helped establish First Draft News. Active until 2022, First Draft was a consortium of social media verification groups that shared methods for combating “fake news.”
Another First Draft founder, fact-checking firm Bellingcat, also received funding from the National Endowment for Democracy.
First Draft was previously led by Claire Wardle, Ph.D., a Brown University professor who, according to “Twitter Files” released last year, advised the Biden administration on COVID-19 “misinformation” — despite having no science or medical credentials.
In 2016, Poynter and the International Fact-Checking Network partnered with First Draft “to tackle common issues, including ways to streamline the [news] verification process.” Other partners included Facebook, Twitter, YouTube, The New York Times, The Washington Post, CNN, ABC News, NBC News and BBC News.
In 2017, Google News Lab partnered with the International Fact-Checking Network “to dramatically increase the searchable output of fact-checkers worldwide, expand fact-checking to new markets and support fact-checking beyond politics, such as in sports, health and science.” The following year, Poynter acquired PolitiFact.com.
Google was also one of the original funders of The Trust Project, a consortium of news organizations that developed eight “trust indicators” to help the public “easily assess the integrity of news.”
These “trust indicators” later became “one of the sources being used by NewsGuard Technologies for a new product to improve news literacy,” and formed “a foundation for NewsGuard review development.”
Hinchliffe warned that the beneficiaries of censorship based on today’s “fact-checking” may become its targets in the future.
“One of the problems of censorship that operates under the guise of misinformation and disinformation, apart from stifling free speech and suppressing actual truths, is that it’s a pendulum that swings both ways,” he said. “The people calling for censorship now may be in a greater position of power to do so, but it will one day swing back at them.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Bill Gates Defends Free Speech — Unless It Hurts His Investments
By Michael Nevradakis, Ph.D. | The Defender | September 16, 2024
Bill Gates took a shot at free speech, the First Amendment, and everyone who questions vaccines and vaccine safety in a CNBC interview earlier this month.
“We should have free speech, but if you’re inciting violence, if you’re causing people not to take vaccines, where are those boundaries that even the U.S. should have rules? And then if you have rules, what is it?” Gates asked on CNBC’s “Make It.”
Gates made similar remarks this month in an interview with CNET, during which he directly targeted the First Amendment:
“The US is a tough one because we have the notion of the First Amendment and what are the exceptions like yelling ‘fire’ in a theater. … I do think over time, with things like deepfakes, most of the time you’re online you’re going to want to be in an environment where the people are truly identified, that is they’re connected to a real-world identity that you trust, instead of just people saying whatever they want.”
Gates, described by CNBC as “the subject of numerous conspiracy theories,” said he does not have a solution for how to stop the spread of “misinformation.” He lamented his “naivete, that when we made information available, that people would want correct information.”
According to CNBC, Gates, who “spends a lot of his time and money trying to help solve some of the world’s biggest problems,” said that unlike tackling diseases or promoting clean energy, there is no clear path forward for solving what he views as the problem of “misinformation.”
Gates told CNBC any “solution” would involve “rules” for online speech, but he said he isn’t sure what form those rules would take or who would enforce them. Similarly, he told CNET “systems and behaviors” should be in place to target “misinformation.”
“Is there some AI [artificial intelligence] that encodes those rules because you have billions of activity [sic] and if you catch it a day later, the harm is done,” Gates told CNBC. However, he acknowledged that he is sensitive to the argument that restricting online information would be detrimental to free speech.
Gates’ remarks a ‘blatant affront to the First Amendment’
Experts who spoke with The Defender said Gates’ remarks belie a disregard for the principles of free speech and the First Amendment.
Author Naomi Wolf, Ph.D., co-founder and CEO of DailyClout, told The Defender Gates “should re-read the Constitution,” adding:
“No individual, and certainly not the state, has the authority in our system to be the arbiter of what can be read or said. Our First Amendment has very few and limited exceptions, such as threats of violence. ‘Misinformation’ is not one of them. History shows that censorship never works ultimately to repress the truth.”
Other experts cited Gates’ questionable track record on free speech and issues such as vaccines. Epidemiologist M. Nathaniel Mead told The Defender Gates’ “post-2020 track record on this issue is well-documented.”
Mead said:
“He tried to sell us on the ‘vaccine-only’ solution to COVID by falsely claiming that the modified mRNA injections would avert infection and transmission, thereby ending the pandemic. He also openly urged media to disparage as ‘conspiracy theorists’ or anyone who questioned mandates for masking, social distancing, lockdowns, PCR testing and, of course, the so-called vaccines.”
Mead called this “a rather blatant affront” to the First Amendment. “Given his track record with public health communications, Gates is being grotesquely disingenuous when he speaks about wanting to protect free speech.”
Mead suggested Gates relies on control over narratives in the media to further his promotion of — and investments in — vaccines. He said:
“Bill Gates has a vested interest in ensuring that counternarrative information, or what he calls ‘misinformation,’ is eliminated. That’s because it interferes with his Bio-Pharma agenda and what appear to be authoritarian aspirations as well, given his efforts to impose vaccine passport requirements internationally and to restrict free speech through his control of many news media channels, having given over $300 million of his own funds in recent years to support ‘independent’ media platforms such as NPR, PBS and The Guardian.
“Since the mass media relies heavily on Big Pharma advertising to maintain operations, it has largely abandoned the traditional skepticism of government directives, instead aiding in the suppression of dissenting viewpoints. Anyone posing counter-establishment narratives is a ‘problem’ from Gates’ perspective.”
‘Afraid that when their plans are exposed, people will resist’
Others argued that Gates’ reputation was hurt as a result of his outspoken support for and investments in COVID-19 vaccines and mRNA technology — and can only be restored through censorship of online speech.
“To restore his reputation from mad scientist back to computer guy, Gates has one hope: censorship. Indeed, the vast amount of censorship needed for that job is basically to wipe the internet,” attorney Greg Glaser told The Defender.
Catherine Austin Fitts, founder and publisher of the Solari Report and former U.S. assistant secretary of Housing and Urban Development, cited a recent survey showing that a significant percentage of the population believes COVID-19 vaccines are deadly.
“A recent Rassmussen survey published in June 2024 reported that 33% of American adults agree with the statement: ‘The [COVID-19] vaccine is killing people, and is killing large numbers of people,’” Fitts said.
“If Mr. Gates wants to stop misinformation, his first step should be to stop financing, speaking or republishing misinformation that results in the poisoning of our children,” Fitts added.
For Seamus Bruner, author of “Controligarchs: Exposing the Billionaire Class, their Secret Deals, and the Globalist Plot to Dominate Your Life,” Gates’ support for stopping “misinformation” is tied to his support for vaccines and digital ID.
Bruner, director of research at the Government Accountability Institute, argued that the “systems and behaviors” Gates advocated include “a de facto digital ID system” that would “track and trace our precise digital footprint — what we say and do online.”
Bruner said:
“Gates and the other controligarchs are pouring billions of dollars into digital ID efforts, and they plan to use misinformation — particularly related to vaccines — to do it.
“He wants to control what we put in our bodies. Now, he wants to control what we’re allowed to put into our minds — what we think — by controlling what we are allowed to say. The reason ‘misinformation’ is a ‘problem’ for controligarchs like Gates is simple: They are afraid that when their plans are exposed, people will resist.”
Gates making an ‘emotional appeal to manipulate public opinion’
CNBC’s interview with Gates came just days before the release of a five-part Netflix docuseries, “What’s Next? The Future With Bill Gates.”
The series will premiere on Sept. 18 — the same day as the documentary “Vaxxed 3: Authorized to Kill” will be released. “Vaxxed 3” features excerpts from thousands of interviews with people about vaccine injuries and deaths people allege were caused by hospital COVID-19 treatment protocols.
According to CNBC, in one episode of “What’s Next?” Gates tells his daughter Phoebe he feels bad for failing to stem the spread of “misinformation.”
“Hearing my daughter talk about how she’d been harassed online … brought that into focus in a way that I hadn’t thought about before,” Gates told CNBC.
According to CNBC, “Phoebe Gates spoke out about what she called ‘the misconceptions and conspiracy theories’” — “including racist online commentary about one of her ex-boyfriends, who is Black” — and about her family in an interview with The Information.
Gates told CNBC, “We’ve handed this problem to the younger generation,” referring to “misinformation.”
Mead accused Gates of trying to conceal his support for censorship by eliciting an emotional response.
“Calling attention to the cyber harassment of his daughter has less to do with misinformation than with predatory and abusive online behaviors,” Mead said. “But Gates seems to be getting desperate, and his attempt to make this kind of illogical linkage is an emotional appeal to manipulate public opinion.”
Mead said Gates used similar emotional tactics to equate questioning vaccines with “inciting violence.” He said:
“In the video clip teaser, we hear Gates say we should have free speech and then attempt to obliquely link ‘inciting violence’ with ‘causing people not to take vaccines.’
“When he juxtaposes the incitement of violence with causing people not to take vaccines, he’s resorting to the most basic propaganda tactic, that of emotional manipulation.”
Such plays on emotion also represent a concerted effort to target young people in particular, according to Glaser:
“One of the most surprising things I’ve learned from interviewing young people is they generally don’t like to fact check. Scrolling is way more fun. They want verification processes done for them, and they are content to rely on their peer group’s perception of the information. That’s the phenomenon that people like Gates are trying to exploit.”
Instead of censorship, a focus on allowing free speech to thrive?
“Misinformation is becoming more common,” CNBC reported, citing developments such as AI chatbots that “make it easier to generate and spread falsehoods quickly,” and a January World Economic Forum report that said “misinformation” is the top global risk for the next two years.
While citing AI as a prime driver of “misinformation,” CNBC cited a 2023 interview with Beth Goldberg, head of research and development at Jigsaw, a Google unit, who said researchers are attempting to develop AI tools to identify what CNBC described as “misinformation and toxic speech online.”
But in a blog post last year, Gates argued that AI’s ability to fight “misinformation” would be imperfect.
“Someone finds a way to detect fakery, someone else figures out how to counter it, someone else develops counter-countermeasures, and so on. It won’t be a perfect success, but we won’t be helpless either,” Gates wrote.
But Glaser said society should focus on creating the conditions for free speech to flourish.
“Free speech does not exist in a vacuum, but rather its quality is a measure of the character of people speaking and listening. This is the root of the issue that censorship cannot address. Only as we improve the character and morality of our societies will free speech truly thrive,” Glaser said.
“The largest danger to an organic human system — like a free market — is inorganic authoritarianism,” Glaser added. “Bill Gates teaming up with the United Nations to impose a global order is the picture of inorganic authoritarianism.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Lawsuit Takes on Federal Campaign to Silence Vaccine Injury Claims
By Cindy Harper | Reclaim The Net | September 15, 2024
The New Civil Liberties Alliance (NCLA) has taken significant legal action by amending its complaint in the ongoing Dressen, et al. v. Flaherty, et al. case. This action challenges the alleged collusion between various federal entities and social media platforms aimed at stifling the voices of individuals claiming injuries from Covid vaccines. The complaint underscores a pervasive campaign spearheaded by agencies including the White House, the CDC, and the Surgeon General’s Office. These bodies are accused of pressuring social media giants to dismiss and discredit as “misinformation” the personal accounts and communications within private online groups of those affected by vaccine side effects.
We obtained a copy of the lawsuit for you here.
Central to the lawsuit are the stories of Brianne Dressen, Shaun Barcavage, Kristi Dobbs, Nikki Holland, Suzanna Newell, and Ernest Ramirez, all of whom reported severe adverse reactions to Covid vaccines—ramifications severe enough, in the tragic case of Mr. Ramirez, to include the vaccine-related death of his son five days post-vaccination. Despite experiencing firsthand the vaccines’ potential risks, these plaintiffs are not opposed to vaccination per se. For instance, Ms. Dressen herself participated in the AstraZeneca vaccine trials before reportedly suffering complications.
These individuals united in their distress, have faced relentless censorship on social media platforms where they sought solidarity and exchanged treatment ideas. Their attempts to share their personal stories and support one another were met with content flags, removals, and the outright shutdown of their support groups—actions directly influenced by what the NCLA terms an unconstitutional campaign by the Biden-Harris Administration.
This legal battle, which aims to secure an injunction against this alleged state-sponsored censorship, asserts that such actions violate the First Amendment’s protections of free speech and association. The ongoing suppression efforts not only undermine the plaintiffs’ rights but also silence an important dialogue about vaccine safety and personal health sovereignty.
Statements from NCLA’s legal team encapsulate the gravity of the case and its broader implications for civil liberties. Litigation Counsel Casey Norman emphasized, “If there is any case that exemplifies why the First Amendment exists—as well as the abominable and Orwellian consequences that take place when the government evades its restraint—it is this one. The time has come for the federal government and its private partners in this cruel censorship scheme to be held to account for the ongoing harm that they have caused our clients, along with so many other Americans across the country who were simply trying to do their part by getting vaccinated—and who were then silenced and made to be pariahs by their own government.”
Echoing this sentiment, Jenin Younes, another Litigation Counsel at NCLA, pointed out the stark contradiction in the government’s narrative versus the plaintiffs’ harsh realities. “The plaintiffs in this case posed a threat to the Biden Administration because their personal experiences conflicted with the government’s heavy-handed approach to Covid-19 vaccination, which was predicated on the false claim that vaccine injuries were virtually nonexistent. The response of the government defendants here—to wield their authority to get social media companies to silence these individuals, who had suffered serious injuries and in the case of Mr. Ramirez lost his own son—should shock the conscience of all Americans. Through this lawsuit, we will hold the Administration and these wayward officials accountable for their flagrantly unconstitutional conduct.”
The Witch Hunt continues
Another Questioning Voice is removed from the Medical Register
Health Advisory & Recovery Team | September 13, 2024
A chill wind passed through the dissident medical profession this week when Dr Sam White was permanently erased from the medical register. But it will not cause us to stop speaking truth to power or more importantly being open and honest with our patients about the potential harms of mRNA vaccines.
For those who don’t know of Dr White, he was an experienced General Practitioner who, like many others, found himself conflicted between his NHS practice expecting him to promote Covid-19 vaccines to his patients, while in his clinical practice seeing increasing numbers of people with vaccine injuries. After much soul-searching he resigned from his post in February 2021. A few months later, in June 2021, he recorded a short face to camera video explaining why he had decided to quit, which he then posted on a social media site. Perhaps to his surprise, it was viewed by millions and within a few days had come to the attention of his employer, namely NHS England, who blocked him from any NHS work, which he legally challenged. A GMC investigation then followed and his NHS suspension was reversed, but an Interim Orders Tribunal put conditions on his registration, namely that he must not use social media to express any medical opinion about the pandemic. Dr White challenged this in the High Court on the grounds that it breached his right to freedom of speech. The court upheld his challenge, as described in the BMJ here, though oddly enough the link to the actual judgement is no longer available, except via Wayback machine. Mr Justice Dove ruled that there had been “an error of law and a clear misdirection in the interim orders tribunal’s decision making process.” Its decision was “clearly wrong and cannot stand,” he added. He stressed that he was expressing no views on the merits of Dr White’s claims on social media. But he said the tribunal had failed to consider a provision in the Human Rights Act 1998. This states that a court or tribunal should not restrain somebody’s freedom of expression before a full hearing unless it was satisfied that after a full hearing the application to restrict publication was more likely than not to succeed.
At the time, the GMC clearly didn’t think that Dr White was a danger to his patients (there had been no clinical complaints against him) nor even sufficient danger to public health for them to suspend him and for the next 3 years he was entitled to work and to speak freely, and many of his supporters had thought this was the end of it. But the wheels of ‘justice’ (ironically in this case more like the wheels of ‘injustice’) grind slowly and in August 2024, the GMC set up a full hearing by the Medical Practitioners Tribunal Service (MPTS). By this stage, Dr White had moved entirely to a practice of naturopathic medicine and decided that he would not engage with the process – he neither attended nor was he legally represented. No-one who has experienced a GMC investigation will blame him at all for this decision – it is time-consuming, emotionally draining and very costly. But his absence may have enabled a serious miscarriage of justice.
The charge against Dr White concerned 5 video interviews about the pandemic which he had recorded between June 2021 and July 2022, and the hearing hinged around details of the Human Rights Act 1998.
Article 10, paragraph 1 states:
“Everyone has the right to freedom of expression. This right shall include freedom to hold opinions and to receive and impart information and ideas without interference by public authority and regardless of frontiers. This Article shall not prevent States from requiring the licensing of broadcasting, television or cinema enterprises.”
However in certain circumstances, the law allows for these rights to be restricted, as in Article 10, paragraph 2:
“The exercise of these freedoms, since it carries with it duties and responsibilities, may be subject to such formalities, conditions, restrictions or penalties as are prescribed by law and are necessary in a democratic society, in the interests of national security, territorial integrity or public safety, for the prevention of disorder or crime, for the protection of health or morals, for the protection of the reputation or rights of others, for preventing the disclosure of information received in confidence, or for maintaining the authority and impartiality of the judiciary.”
The Tribunal chairman quoted from the case of Adil v GMC [2023] EWCA Civ 126. Mohammad Adil is a surgeon who was suspended by the GMC in 2020, again for a face to camera video which went viral. He also took the GMC to court but in his case he lost. In that case, “the Court held that the fact that a doctor expresses a minority view, even a view shared by a small minority is not sufficient of itself to render his conduct improper. Medical progress depends upon such debate and is littered with examples of what were thought to be heretical views becoming accepted wisdom, and vice-versa. Article 10 and the common law protect the right to express views with which most people disagree. Views contrary to widely accepted medical opinion are not sufficient to establish misconduct.” However, the judgement went on to say that this does not apply to views so far removed from any concept of legitimate medical debate and must be considered on the facts of each individual case. “There is an important qualitative difference between a doctor’s views which have some supporting scientific basis, even if not widely accepted, and views whose validity or accuracy is unconnected to any supporting evidential basis, in other words baseless.”
With Dr White absent from the proceedings, the Tribunal seem to have assumed that his views on the safety of the Covid-19 mRNA vaccines were ‘baseless’, whereas of course they are shared by a significant minority of doctors who have assembled a huge amount of scientific literature on vaccine harms. However, the judgement in quoting from his interviews has barely mentioned Dr White’s criticisms of the vaccine, for all of which he had provided many references to the GMC in 2021. It has instead focussed almost entirely on discussions about the ‘why’ of the vaccine rollout and the censorship, quoting Dr White speaking of: ‘evil’, ‘planned’, ‘globalists’, ‘tyranny’, ‘totalitarianism’, et cetera. These, of course, are all issues which are widely discussed but are not subject to testing and writing up in peer-reviewed journals. They are a matter of opinion. The question of whether Dr White’s opinions in any way harmed public health has not been demonstrated by the GMC, yet the Tribunal “determined that, it was more likely than not, such comments undermined public confidence in the medical profession.”
Another aspect of Dr White’s absence was that, whereas the GMC were actually asking for a suspension rather than for his name to be permanently erased from the register, the Tribunal interpreted his absence as showing a lack of insight into the seriousness of his actions and a lack of any effort at mitigation or remediation. For a surgeon who has cut off the wrong limb or a physician who has missed a potentially treatable fatal condition, remorse and a desperate wish to ensure you never make the same mistake again, would be the universal reaction, even without censure from the GMC. But for a doctor who is in effect a whistleblower, it is hard to show remorse, whilst still hoping that your actions have indeed saved lives.
The irony is that if the GMC really believed that Dr White was a danger to public health, they would have suspended him in 2021, at a time when the vaccine rollout was in full swing and we were heading towards a second winter of masks and lockdowns. Yet they appear to have made no effort to bring forward a full hearing, and have instead waited a full 3 years after his initial video before bringing this case. The rules for deciding on a penalty are that the Tribunal must consider whether the doctor poses a risk to future patients rather than only past. Given the government messaging with which Dr White disagreed all came to an end during 2022, it is hard to see what harm he is thought to be causing in 2024.
It was, however, made very clear that the penalty was not only intended for Dr White but also to send a clear message to other doctors considering speaking out. “Sanctioning doctors for comments likely to undermine public health and confidence in the medical profession so as to deter such behaviour engages the aim of the protection of public health and safety.” Indeed, coming close in the heels of Dr White, is a consultant psychiatrist, Dr Daniel Armstrong, also facing the possibility of being struck off for a single online video, “Navigating the Truth-deception duality”. And there are others with hearings in the near future. This is not about clinical complaints of patient safety. This is about doctors questioning the government about the management of the pandemic, especially the poor safety record of the vaccines.
In May of this year, Professor Dame Carrie McEwen, chair of the GMC, published a statement in response to the contaminated blood scandal. She commented robustly on the importance of protecting whistleblowers. “There is extensive commentary within the report about the importance of speaking up about both mistakes and near misses and a cautionary note about the need to protect those who do so from detriment to their career.” She said, “We are of course aware that referrals to us are sometimes used to intimidate. This is completely unacceptable, has significant consequences for doctors’ wellbeing and puts the safety of patients at risk….We’ve put a number of safeguards in place” and she committed to assessing “whether further interventions are needed to prevent retaliatory or weaponised referrals.” “also seen investigative media reports alleging that a number of NHS managers have taken actions to silence whistleblowers, including threatening referral to the GMC.” The Telegraph (15th May 2024), published one such report under the title “The four-step ‘playbook’ the NHS uses to break whistleblowers”.
A large group of doctors and other health professionals wrote to the GMC in June, highlighting their concerns over what appeared to be a witch hunt of doctors speaking out about covid-vaccine harms. The ongoing correspondence is published here. Several of the signatories to that letter had previously signed a fully referenced scientific letter to the Chief Medical Officer in June 2021 calling on him not to recommend covid vaccines for children, and found themselves referred by the DoHSC to the Counter Disinformation Unit.
A recent BMA survey showed that the proportion of doctors being discouraged from or even afraid of speaking out has risen significantly between 2018 and 2024, to the point where 61% of those polled in 2024 said they may not raise concerns because they were “afraid” they or colleagues could be “unfairly blamed or suffer adverse consequences”.
The UK is not alone in its efforts to stifle free speech with eminent doctors being similarly sanctioned in Canada, Australia, and most recently the USA. Whistleblowing in academia is no easier.
If public confidence in the medical profession has fallen, rather than blaming dissenters for speaking out against the prevailing message, perhaps doctors need to take a hard look at their unquestioning acceptance of the ‘Safe and Effective’ message and ask themselves why is covid continuing, why are their vulnerable patients being recommended for another booster every 6 months, and yet why are they apparently busier than ever?
Many of the doctors currently being hounded for speaking out on social media, are the same doctors who are repeatedly thanked by members of the public for their honesty and integrity and especially for their efforts to support the vaccine injured, often ignored and disbelieved by others. Comments beneath an article in the Mail about Dr White’s erasure, suggest that many members of the public have rather more faith in Dr White than they have in the GMC.
The current situation of self-censorship amongst doctors combined with GMC overreach, risks serious ongoing harms to patients and must not continue.
No, New York Times, Climate Change Isn’t Destroying Bridges
By Anthony Watts | Climate Realism | September 6, 2024
The New York Times (NYT) recently published an article titled “Climate Change Can Cause Bridges to ‘Fall Apart Like Tinkertoys,’ Experts Say,” written by Coral Davenport. Multiple lines of evidence and examples not only refute this claim as false but expose the sheer absurdity of the claim.
These sorts of absurdly false claims have been tried before, for instance, when the I-35W bridge collapsed in Minneapolis, MN in 2007. An article in 2007 by Noel Sheppard at NewsBusters exposed the claim as false:
A former member of the Clinton administration, and current Senior Fellow at the virtual Clinton think tank the Center for American Progress, claimed Monday that global warming might have played a factor in the collapse of the I-35W bridge in Minneapolis last week.
I kid you not.
Writing at Climate Progress, the global warming blog of CAP, Joseph Romm – who served as Acting Assistant Secretary of the U.S. Department of Energy in 1997 and as Principal Deputy Assistant Secretary from 1995 though 1998 – stated in a piece amazingly entitled “Did Climate Change Contribute To The Minneapolis Bridge Collapse?“
Unsurprisingly, the actual cause had nothing to do with climate change at all but rather an engineering failure that used undersized gusset plates that were too thin for the load of the bridge:
The investigation revealed that photos from a June 2003 inspection of the bridge showed gusset-plate bowing. On November 13, 2008, the NTSB released the findings of its investigation. The primary cause of the collapse was the undersized gusset plates, at 0.5 inches (13 mm) thick. Contributing to that design or construction error was the fact that 2 inches (51 mm) of concrete had been added to the road surface over the years, increasing the static load by 20%. Another factor was the extraordinary weight of construction equipment and material resting on the bridge just above its weakest point at the time of the collapse. That load was estimated at 578,000 pounds (262 tonnes), consisting of sand, water, and vehicles.
So, human error and extra weight, not climate change, was determined to be the cause of the bridge’s failure.
Fast forward to the present. The NYT’s article makes similar claims:
Bridges designed and built decades ago with materials not intended to withstand sharp temperature swings are now rapidly swelling and contracting, leaving them weakened.
“It’s getting so hot that the pieces that hold the concrete and steel, those bridges can literally fall apart like Tinkertoys,” Dr. Chinowsky said.
As temperatures reached the hottest in recorded history this year, much of the nation’s infrastructure, from highways to runways, has suffered. But bridges face particular risks.
Really? The bridges in question weren’t engineered to handle daily temperature swings? A natural event that happens daily across seasons? That sounds like poor planning. Besides the absurdity of that claim, there are two further contradictory points to consider.
First, in the United States, we’ve seen far worse sustained heatwaves before, such as in the 1930s when the July 1936 heatwave hit America’s Midwest, where some places experienced up to 14 days of above 100°F temperatures. This is evidenced by the graph in Figure 1, provided by the U.S. Environmental Protection Agency.

Figure 1. This figure shows the annual values of the U.S. Heat Wave Index, from 1895 to 2020 contiguous 48 states. Environmental Protection Agency.
In the many reports of the heatwaves in the 1930’s, there is no mention of bridge collapse, which suggests that the linkage to “extreme heat aided by climate change” claim is false. Otherwise, such temperatures in the 1930s would have resulted in collapsed bridges. However, there simply are none from that period reportedly linked to heat.
Secondly, the article says “As temperatures reached the hottest in recorded history this year, much of the nation’s infrastructure, from highways to runways, has suffered.” But this isn’t true either. The claim NYT uses is about the global temperature, not the U.S. temperature. As seen in Figure 2 below showing data from the National Oceanic and Atmospheric Administration (NOAA), from the U.S. Climate Reference Network (USCRN), widely considered to be the most accurate source of surface temperature data, July 2024 was not “the hottest in recorded history.” For example, maximum U.S. temperature was higher in 2012 and 2005 than in July 2024.
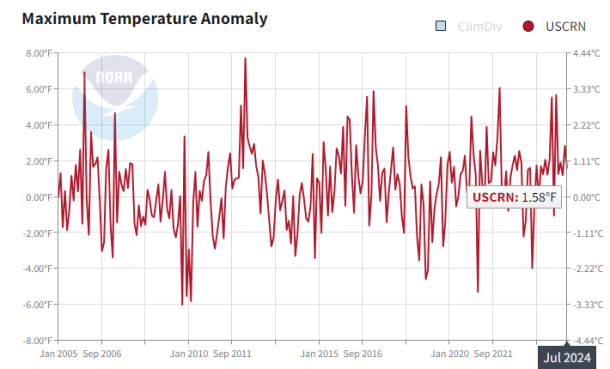
Figure 2: NOAA – USCRN Maximum Temperature
Diving deeper into the NYT article, the Times attributes the failure of a railroad bridge connecting Iowa and South Dakota during floods to climate change. Flooding in the rivers and streams across and bordering Iowa and South Dakota have been common for as long as records of such event have been kept back into the mid-1800s. And railroad bridge collapses have happened repeatedly in the United States and around the world, well before climate change ever became an issue. Since data show no increase in the number or severity of flood events across the United States, in general, or in Iowa and South Dakota, in particular, there is no evidence climate change played any role in that particular railroad bridge collapse.
The next claim is that the concrete buckled and broke on a bridge in Lewiston, Maine which NYT blamed on “recent fluctuation in temperature and rain.”
Looking at the weather in Lewiston, ME when the event occurred shows that although high and low temperatures were higher than the normal average for late June, the fluctuations the NYT was so concerned about were less extreme than normal, about a 15 degree change from high to low in June 2024 rather than the historic daily average of about 20 degrees. (See figure 3, below).
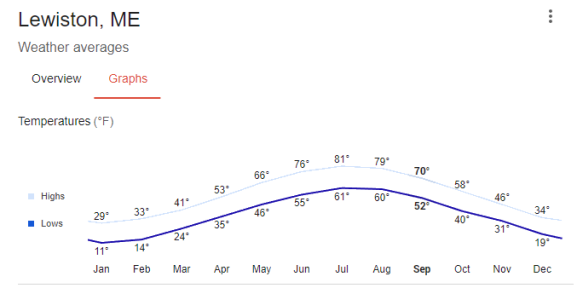
Figure 3: Normal average daily fluctuations in temperatures throughout the year for Lewiston Maine. Source: Google
The high temperature for the third week of June was 95℉, above the normal maximum for the date, but it was well below the historic high temperature for the city of 99℉ recorded in 1911, 113 years of global warming ago. Lewiston’s 2024 June high was also 10 degrees lower than the high temperature record for the state as a whole of 105℉ set in North Bridgton, ME, just thirty miles away from Lewiston, also from 1911, when that temperature was hit twice.
Because temperatures in Lewiston didn’t fluctuate wildly and were also not record setting, it is implausible for the bridge’s concrete cracking and buckling to have anything at all to do with climate change. It was likely a result of poor construction or, even more likely, poor maintenance, a problem for many bridges and overpasses in Maine and the U.S. as a whole, combined with increased traffic and load, due to significant population growth in the city and the region, using the bridge.
Literally, it takes two minutes of work on Google search to find this data. Apparently, NYT reporter Coral Davenport couldn’t be troubled to seek out the facts. Or perhaps, she just doesn’t know how. This sort of slapdash reporting containing speculative claims rather than simple facts seems like something out of the old TV series The Twilight Zone.
If such an episode aired today, my suggested title would be “Bogus Maximus.” This story was pure science fiction.
The Bird Flu Vaccine Clinical Trials
What the safety data tells us
Injecting Freedom by Aaron Siri | September 11, 2024
Bird flu is all the rage. As this issue heats up, here is a bit of information about each of the three bird flu (H5N1) vaccines licensed by the FDA.
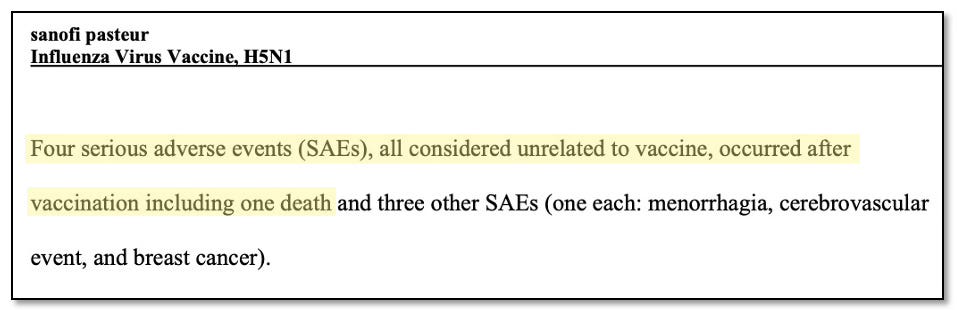
First is Sanofi (National Stockpile), which was licensed for adults based on a clinical trial in which only 103 adults were vaccinated and 48 received the placebo. Worse, there were four serious adverse events in the vaccine group.
Next up is ID Biomedical, which was licensed for adults in a clinical trial in which the vaccine group had four times the rate of new immune-mediated diseases. The trial for ages 6 months to 17 years had only 838 children, making it underpowered and unable to adequately measure safety.

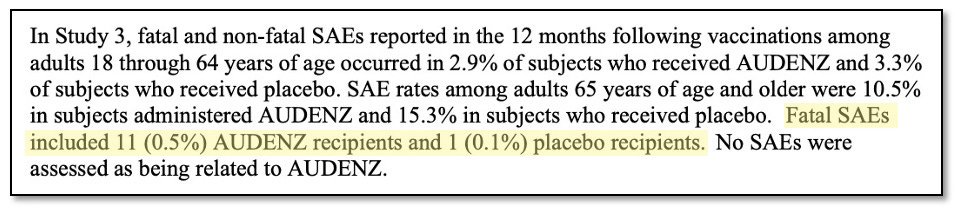
And last but not least is Seqirus, which was licensed for adults in a clinical trial in which 0.5% of the vaccinated group died but only 0.1% of the placebo group died. The trial for ages 6 months to 17 years had only 329 children, making it significantly underpowered and unable to adequately measure safety.
And that is a wrap. Needless to say, if you plan to get pricked, be informed!
Featured Video

Language is a Weapon
or go to
Aletho News Archives – Video-Images
From the Archives
Aaron Siri’s Book: Vaccines, Amen
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
Aaron Siri makes it clear in Vaccines, Amen: The Religion of Vaccines that the story we’ve been told about vaccine science rests far more on belief than proof.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
And he does. … continue
Blog Roll
 Aletho News
Aletho News- The UK Joins the Pirates
- Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report
- Press TV reporter wounded in Israeli drone strike on southern Lebanon
- Time for Trump to Tell Benjamin Netanyahu to Go Away!
- Israeli officials: ‘Security zones’ to remain in Lebanon, Syria, Gaza
- Israel Fails to Sabotage Islamabad Accord… At Least for Now
- Araghchi: US Responsible for Implementing MoU with Iran
- US must cut military, intelligence assistance to Israel to protect Iran deal: Ex-Trump official
- The 12 Screenings That Manufacture the Patients They Claim to Find
- Iran deputy FM says MoU with US finalized, to be signed in Geneva on Friday
- If Americans Knew
- They Weren’t Convicted of Terrorism, But These Palestine Activists Got Sentenced as Terrorists Anyway
- “Ceasefire” is not in Israel’s vocabulary – Daily Update
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- Oxfam: More Palestinians killed by Israel across West Bank in last 3 years than previous 17 years combined
- US-Iran ceasefire may be imminent, but will Israel blow it up? – Daily Update
- The Issue of Israel Is Ending Democracy In Michigan
- Israel is stealing homes, livelihoods, and lives in West Bank
- Gaza is not an aberration – Israel planned this genocide decades ago
- No Tricks Zone
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
