New study reveals Antarctic ice shelf area has grown by 5305 km2 from 2009-2019

Global Warming Policy Foundation | June 3, 2023
A new study by a team of climate scientists and published by the European Geosciences Union reveals that the Antarctic ice shelf area has grown by 5305 km2 from 2009-2019, gaining 661 Gt of ice mass over the past decade.

The new observations confirm the findings of eminent meteorologist Professor J. Ray Bates whose research has shown that trends in polar sea-ice levels give little cause for alarm.
In a paper published just over a year ago by the Global Warming Policy Foundation, Professor Bates contrasted climate model simulations – which predict significantly decreasing sea ice levels in both hemispheres – with empirical data and observed trends in Arctic and Antarctic sea ice.
Professor Bates said:
“In 2007, Al Gore told us that Arctic sea ice levels were ‘falling off a cliff’. It’s clear now that he was completely wrong. In fact, the trends in sea-ice are an antidote to climate alarm.”
Professor Bates also says that little reliance should be placed on model simulations of future sea-ice decline:
“Climate models failed to predict the growth in Antarctic sea ice, and they missed the recent marked slowdown of sea-ice decline in the Arctic. It would be unwarranted to think they are going to get things right over the next 30 years.”
Professor Bates’ paper can be downloaded here (pdf)
Vaccinated Veterans MORE Likely to Die from COVID, VA Study Proves
It’s Even Worse to Be Boosted
BY IGOR CHUDOV | JUNE 2, 2023
The U.S. Veterans Administration oversees the medical care of the United States Armed Forces veterans. It has complete medical records of every veteran, including their hospitalizations, vaccinations, deaths, and more.
Therefore, studies of veterans that include sub-populations broken down by vaccination status provide accurate data about the effectiveness of COVID vaccines. I already reported on two such studies: one shows that COVID and flu vaccines are useless at preventing hospitalization due to COVID or flu, and another (posted on Feb 2022) proves that Covid vaccines cause myocarditis in veterans.
A new study was published in the Journal of Infectious Diseases and is worth a look.

The study is very straightforward: it looked at 1,459 veterans receiving Merck’s Molnupiravir and compared them with 63,281 veterans NOT receiving it. Its objective was to see if Molnupiravir was helpful (drumroll, it was not). The period covered was from Jan 1 to August 21, 2022.
The study has the breakdown of the Molnupiravir group and the standard-treatment group by vaccination status.
Such a breakdown allows us to check which veterans did better: the COVID-vaccinated or the unvaccinated.
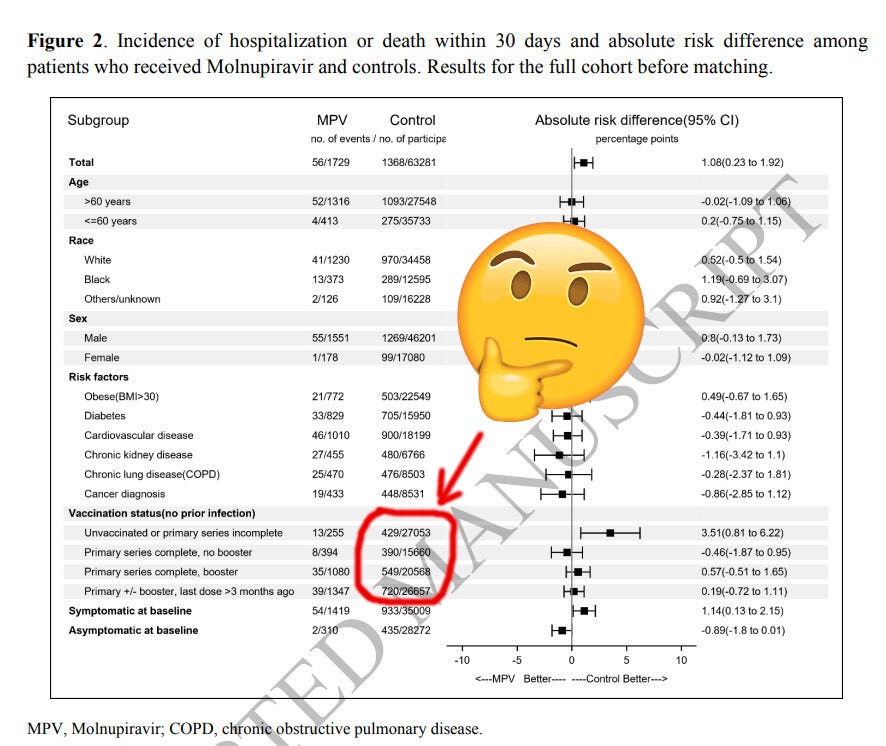
Look at the “control group”: veterans who did NOT receive Molnupiravir and received standard care instead (circled above). Let’s make a nice table out of that:

Each category above contains only US veterans, mostly older males, so they are roughly the same age category. Therefore, age confounding can change the picture somewhat but should not change too much. They all have access to the same VA medical resources, so no medical disparities exist. The only difference between them is their vaccination status.
You would think that right in the midst of the deadly COVID pandemic, many lives of those older persons would be saved by safe, effective, science-backed COVID vaccines, right? Every TV program told us this last year, so it must be true! (note my sarcasm)
Guess what? It was the opposite! The category in the above table with the least hospitalizations and deaths is the veterans who refused COVID vaccines and remained unvaccinated. Those had only 15.86 veterans per 1,000 hospitalized or dead. The more vaccines the veterans received, the worse their outcome: double-dosed veterans had 24.90 hospitalizations/deaths per thousand and boosted veterans had 27 hospitalizations per thousand.
These ratios are derived from a population with precisely known vaccination status of each participant. They show that the Covid vaccine does not work – when vaccination statuses are known, and when outcomes are counted properly.
This finding is based on a plain reading of numbers provided (but not discussed) by the study authors. They only looked at the effectiveness of Molnupiravir. By the way, they found Monupiravir ineffective and harmful.
Had they looked, or were allowed to look at, the effectiveness of the COVID vaccines, based on their own data, their findings would be much more explosive.
If I may guess, had they tried to bring our attention to the ineffectiveness of COVID vaccines, the article would not have been published to maintain “scientific consensus,” nicely described by El Gato Malo. Despite all that, I am thankful to the authors who gave us the numbers we can properly interpret ourselves.
So, to recap, the unvaccinated veterans had the LOWEST rate of hospitalizations and deaths.
Occurrence of Convulsions and Death After DTP Childhood Vaccination
Data Published Over 20 Years Ago Signaled Concern
By Peter A. McCullough, MD, MPH | Courageous Discourse | May 27, 2023
When the CDC ACIP Panel added the unsafe, ineffective, mRNA COVID-19 vaccines to the routine pediatric childhood schedule without full FDA licensure and with no assurances on long-term safety, the entire schedule was called into question from the perspectives of clinical indication, medical necessity, safety, and efficacy. Is it possible since the release of older vaccines that the medical community and CDC ACIP panel ignored solid data and safety concerns with established vaccines? I was participating in the Novel Coronavirus Southwestern Intergovernmental Committee deliberations in the Arizona Senate building, when a paper published over 20 years ago was presented on the diphtheria, tetanus, and pertussis vaccines. The results were astonishing.
Geier and Geier published a massive study and one of the first of its kind at the time using the CDC Vaccine Adverse Events Reporting System. The hypothesis was that febrile convulsions were more likely to occur with combined vaccine products that in some cases it would lead to death. Here is what they did: “The incidence rates calculated in this study are based on the estimates by the CDC of the number of doses administered during the study period: 121,954,137 doses of whole-cell DTP; 54,611,651 doses of acellular DTP (DTaP); and 9,335,142 doses of DT were administered. The background rate of development of convulsions by children is based on the estimates of the 1991 report by the Institute of Medicine of 0.2 per million children per day.”

Geier DA, Geier MR. An analysis of the occurrence of convulsions and death after childhood vaccination. Toxicol Mech Methods. 2002;12(1):71-8. doi: 10.1080/15376510209167937. PMID: 20597817.
They found more cases (occurrence/million) of febrile seizures and death after whole-cell DTP, DTaP, DT alone, in a descending, nonlinear graded fashion, and the risks were in a tight temporal relationship. This is concerning because of the associations between post-vaccine febrile seizures and childhood/adult epilepsy requiring medications and with the development of neuropsychiatric conditions including autism.
In summary, no vaccine is perfectly safe. Combining multiple products into single shots increases the reactogenicity and the risk of a catastrophic outcome. As parents and doctors begin to make more discerning choices they may consider going to less complex products, spreading them out, and giving them at later ages.
Alternatively, some parents and doctors may choose for a child to “go natural” or completely unvaccinated, which has the best overall outcomes in contemporary studies at this time. Diphtheria and pertussis are easily treated with antibiotics, so prompt recognition and treatment if such a rare infection occurs is always an option for parents. Tetanus is avoided with good wound care and antibiotics for deep tissue lacerations and puncture wounds.
The bureaucrats & science retards responsible for the last three years of destruction and mass medical experimentation are unrepentant and eager to do the same thing all over again
eugyppius: a plague chronicle | June 3, 2023
While I travel and work on a longer piece, I thought you might enjoy some outtakes from this recent article in Welt, about the complete lack of self-reflection exhibited by German pandemic Science-Followers even after the failure of their policies:
Helge Braun … the former head of Angela Merkel’s Chancellery, was invited to Berlin’s Futurium to discuss science and politics. Behind the scenes, Braun was a key figure in the German Corona response. Time for a few awkward questions? The CDU politician need not fear them – despite his vehement advocacy of school closures and lockdowns …
He was joined by three members of the Leopoldina [that is, the German National Academy of Sciences] – climate researcher Gerald Haug, its president; paediatrician and adolescent physician Jutta Gärtner and sociologist Armin Nassehi. The Academy became known during the pandemic not for its balanced scientific advice, but primarily for its politicised demands for tougher measures. And as often as its members emphasised institutional independence from the government that evening, you could tell their intellectual independence was notably lacking.
“Team Caution,” as members of the Leopoldina members still like to call themselves, was full of praise for their own work … “The pandemic was a good example of science-based policy advice,” Haug explains – and by “good” he really does mean that the Academy advised well … “Team Caution” always did everything right … The sensible majority followed the recommendations of the government, the Leopoldina and the RKI. Everything else is nasty fake news from the internet.
Yet Haug himself is a good example of the Leopoldina’s convoluted self-perception. On the one hand, he insisted repeatedly that science only represents “the facts”; that is, he claims objectivity for his profession. On the other hand, Haug freely admits that the Leopoldina aimed to “really hit it out of the park” and “make a splash” with their recommendations. “We’re often too soft…”
A real problem with the technocrats, is that they only have relevance in one direction. As soon as the National Academy of Sciences issues an opinion that the virus isn’t much to worry about and people should continue to live their lives as before, their political relevance is finished. For this reason alone, technocratic systems will be biased towards intervention, even in harmless situations, and nothing they tell you to do can ever be trusted.
The damage inflicted by lockdowns, the vaccines, social exclusion and attendant social conflicts – nobody wanted to talk about that. Nor did anyone want to discuss Braun’s role as one of the main instigators of the German pandemic response, distinguished internationally especially by the long school closures. As is well known, Braun’s promise that all measures would end “as soon as we have made an offer of vaccination to everyone in Germany” turned out to be empty talk. His threat that the vaccinated should receive “more freedom” than the unvaccinated, on the other hand, became brutal reality. No matter. For Braun, the Corona era represents a positive interaction between politics and science, which serves as an important example for the future.
Braun claimed that “Citizens don’t like arguments in politics. The strange democratic understandings of this unassuming Merkel confident could be summed up as “Dare to demand more expertocracy …
At the end, they moved on from Corona to discuss climate change. A scientist in the audience suggested that the Leopoldina should … take to the streets. The opinionated moderator suggested that, when it comes to climate, fear is rational; and that, in consequence, the rational mandate of science would be to spread fear …
Apparently, the politicians and academics who set the tone in the Corona crisis now feel encouraged to extend the Corona model to future grand programmes …
Mark my words: Should they ever be allowed to get the public panic juggernaut up and running again, what they do next will make Corona seem like a mildly rough case of cultural and political indigestion. They’ve learned that the hard limits on their power are far weaker than they ever imagined. Their dark ambitions will hang over us like a Sword of Damocles for decades now.
The UK’s “Chilling” Secret Unit That Monitored Lockdown Dissent
More revelations about the secretive Counter Disinformation Unit
By Cindy Harper | Reclaim The Net | June 3, 2023
A clandestine UK Government unit dubbed the Counter-Disinformation Unit (CDU) has been implicated in a troubling endeavor to curb and control online discussions about the controversial Covid-19 lockdown policies. The covert operation allegedly involved the collaboration of social media companies in a strategic bid to quell supposed domestic “threats.”
According to revelations from Freedom of Information requests and data protection requests from The Telegraph, posts critical of Covid-19 restrictions, including those questioning mass vaccination of children, were systematically removed.
Social media companies are now under scrutiny following allegations that their technologies were deployed to thwart the wide circulation or promotion of posts tagged as potentially problematic by the CDU or its Cabinet Office equivalent.
The files revealed the surreptitious monitoring of critics of the Government’s Covid plans. Artificial intelligence firms were reportedly enlisted by the government to search social media platforms, flagging any discussions opposing vaccine passports.
In a startling revelation, the BBC was implicated in clandestine government policy discussions regarding this alleged misinformation.
The CDU, hosted by the Department for Culture, Media, and Sport (DCMS), operated a “trusted flagger” system with major social media companies. This mechanism expedited requests for content removal. The CDU, still operational, was formed in 2019, initially focusing on the European elections, later shifting its attention to the pandemic.
Critics, including MPs and freedom of speech campaigners, have labeled the revelations as “truly chilling” and a strategy tantamount to “censoring British citizens” — a tactic likened to those of the Chinese Communist Party.
“Any attempt by governments to shut down legitimate debate is hugely concerning, but to discover that DCMS actively sought to censor the views of those who were speaking up for children’s welfare is truly chilling,” said Miriam Cates, a Conservative MP to The Telegraph.
A government spokesman refuted the allegations, stating that the unit was designed to track narratives and trends using publicly available information to safeguard public health and national security. The spokesman insisted that the unit never monitored individuals and had a strict policy against referring journalists and MPs to social media platforms.
Like the Curious Bride in “Bluebeard”
By John Leake | Courageous Discourse | May 31, 2023
Recently I’ve been thinking about the old French folktale, Bluebeard. For readers who are unfamiliar with the story, Bluebeard is a nobleman who has been married six previous times to young women who have all mysteriously vanished. Wikipedia provides a succinct account of what happens when he marries a seventh time.
[A neighbor’s youngest daughter who decides to marry him] goes to live with him in his rich and luxurious palace in the countryside, away from her family.
Bluebeard announces that he must leave for the country and gives the palace keys to his wife. She is able to open any room with them, each of which contain some of his riches, except for an underground chamber that he strictly forbids her to enter lest she suffer his wrath. He then goes away, leaves the palace, and the keys in her hands. She invites her sister, Anne, and her friends and cousins over for a party. However, she is eventually overcome with the desire to see what the secret room holds, and she sneaks away from the party and ventures into it.
She immediately discovers that the room is flooded with blood and the murdered corpses of Bluebeard’s previous six wives hanging on hooks from the walls. Horrified, she drops the key in the blood and flees the room.
I’ve long been intrigued by Bluebeard as an archetypal expression of the horror we may experience when we become curious to know what is going on behind the closed doors of power. Bluebeard is a powerful nobleman who is apparently beyond the law. His young bride is an ordinary girl who becomes implacably curious to see all of the rooms of his castle, which seem to symbolize the rooms of his soul.
I spent this evening carefully reviewing declassified e-mails authored by the eminent Scripps Institute virologist, Kristian Andersen. The first one was dated January 31, 2020 and addressed to Anthony Fauci:

The most noteworthy sentences in the email are:
The unusual features of the virus make up a really small part of the genome [0.1%] so one has to look really closely at all the sequences to see that some of the features (potentially look engineered. … I should mention that after discussions earlier today, Eddie, Bob, Mike [Edward Holmes, Robert Garry, Michael Farzan] and myself all find the genome [of SARS-CoV-2] inconsistent with expectations from evolutionary theory.
3.5 days later—shortly after a phone conference with Dr. Fauci and others—Dr. Andersen completely changed his tune. By then, the decision had been to submit a letter to the National Academies of Sciences, Engineering and Medicine regarding the origin of SARS-CoV-2.

Please note the final sentence:
If one of the main purposes of this document is to counter those fringe theories [about the virus being engineered] I think it’s very important that we do so strongly and in plain language (“consistent with” [natural evolution] is a favorite of mine when talking to scientists, but not when talking to the public—especially conspiracy theorists).
After these e-mails were released to the public in response to a FOIA request, Dr. Andersen claimed that he learned revelatory things about the novel virus in the 3.5 days following his initial e-mail to Fauci, and that these revelations caused his perfect volte-face. However, it seems to me that his explanation doesn’t really account for his strident, unequivocal assertions in his second e-mail.
Many of the recipients’ names in his February 4, 2020 have been redacted, but there [are] many apart from the two men who received his January 31 e-mail (Dr. Fauci and Jeremy Farrar). His first e-mail was a matter of strictly confidential counsel. His second pertains to an open letter—about to be sent to a large institution with many members—declaring that anyone who even suspects the novel virus to have emerged from a lab is a crackpot conspiracy theorist.
What on earth could inspire a virologist to adopt a posture of such Machiavellian duplicity about an infectious agent that—as he well knew—was about to inflict a catastrophe on all of mankind? He had to have known that such pronouncements—coming from a virologist of his eminence—would likely retard a thorough and impartial investigation of the virus’s origin.
Contemplating this question this evening, I thought Bluebeard’s young bride when she discovers the chamber of horrors in her husband’s castle. I suspect that Tess Lawrie felt the same way in her encounter with Dr. Andrew Hill, which she recounted in the short documentary film Dear Andy.
The EU Plans To Test Twitter To See How Fast It Responds To Censorship Demands
By Cindy Harper | Reclaim The Net | June 3, 2023
The European Union will stress test Twitter and other platforms to see how well they comply with the upcoming censorship law, the Digital Services Act (DSA), whose enforcement will begin in August. In a similar style program to that created by the Chinese Communist Party, where government enforcers visit tech companies directly, a team of 10 digital specialists will visit the companies later this month, said Thierry Breton, the EU Commissioner for Internal Market.
The test will help companies learn how the DSA will be enforced. Breton, who will also visit the companies, said the team will review how platforms respond to what is problematic content under the law including content that has been flagged by the EU and content that has not been flagged.
The team will also review why some content is not flagged, citing an example of “fake news that caused disturbances but was promoted because it generated virality and advertising.”
“Did you have enough moderators beforehand? Was it promoted by the algorithm?” Breton said. “We want to do this for real, in the real world, so they see how it happens, and above all so they prepare,” Breton said.
Some of the findings from the test will be made public while some will only be communicated to the companies.
In an interview where he talked about the visits to the social media companies, Breton said: “I’m not threatening anyone. We are here to help companies comply with our new law.”
Last week, after Twitter withdrew from the voluntary Code of Conduct on Disinformation, Breton warned: “You can run but you can’t hide,” adding that “fighting disinformation will be legal obligation under #DSA as of August 25.”
Exposed: The UK Company Subjecting Your Social Media Posts To State Surveillance
By Ken Macon | Reclaim The Net | June 3, 2023
A UK government-funded artificial intelligence (AI) firm based in an unassuming industrial estate in Yorkshire, England, has been engaged in state surveillance, monitoring the social media posts of citizens, a recent revelation suggests.
Logically, the firm in question, has earned over £1.2 million (1.49 million USD) from government contracts to identify and analyze “disinformation” and “misinformation” spread across social media.
The AI company was started by Lyric Jain, a 27-year-old Cambridge engineering graduate, who launched the technology first during Indian elections. With one of the largest dedicated fact-checking teams globally, the company sifts through material from hundreds of thousands of media sources and all public posts on major social media platforms.
Logically has bagged lucrative deals, including a £1.2 million (1.49 million USD) contract with the Department for Culture, Media and Sport (DCMS) and another worth up to £1.4 million (1.7 million uSD) with the Department of Health and Social Care to monitor threats to high-profile vaccine service individuals, The Telegraph reported. Its client list includes US federal agencies, the Indian electoral commission, TikTok, and Facebook.
While Logically asserts that it does not share evidence collected for the UK Government with Facebook, this partnership has ignited concerns among freedom of speech campaigners.
The company’s responsibilities grew over time, aiding in building a comprehensive picture of potentially harmful misinformation and disinformation. Documents revealed that it produced regular “Covid-19 Mis/Disinformation Platform Terms of Service Reports” for the Counter-disinformation Unit – a secretive operation within the DCMS.
A public document titled “Covid-19 Disinformation in the UK” disclosed Logically’s perspective, referring to “anti-lockdown” and “anti-Covid-19 vaccine sentiment”, along with hashtags “#sackvallance” and “#sackwhitty” as evidence of “a strong disdain for expert advice.”
Logically defended its actions, stating that it is possible for content not specifically mis- or disinformation to be included in a report if there is a potential for a narrative to be weaponized.
The firm denied limiting freedom of speech, stating: “We do not specifically monitor individuals and their behavior, nor do we make any recommendations that limit their right to free speech… We monitor content, including narratives and trends across public information environments online, to help tackle the proliferation of online harms, mis- and disinformation, and prevent real-world harms.”
The company’s practices have raised questions about freedom of speech and privacy rights. Critics argue that this case illuminates the ethical and regulatory challenges posed by the powerful convergence of artificial intelligence and big data.
Featured Video

Rewriting the risk? Inside the government’s vaccine safety messaging
or go to
Aletho News Archives – Video-Images
Book Review
“Davos Can Really Replace the UN”
Inside the book that maps the architecture behind global governance — from the Epstein files to the Pact for the Future
Lies are Unbekoming | April 1, 2026
On June 13, 2019, the United Nations and the World Economic Forum signed a partnership deal to “accelerate the implementation of the 2030 Agenda for Sustainable Development.” That same evening, WEF president Börge Brende — Norway’s former Foreign Minister — had dinner with Jeffrey Epstein at Epstein’s Manhattan townhouse. The Epstein files, released January 2026, contain an exchange between the two from the previous year. Epstein to Brende: “Davos can really replace the UN. C21, cyber, crypto . genetics… intl coordination.” Brende back to Epstein: “Exactly — we need a new global architecture. World Economic Forum (Davos) is uniquely positioned — public private.”
The next day, the UN General Assembly adopted the framework for restructuring global governance.
That sequence — the partnership signing, the Epstein dinner, the candid admission about replacing the UN with a public-private architecture, and then the formal adoption — opens Jacob Nordangård’s The Digital World Brain. Pages two and three. Footnoted to the UN resolution number, the Epstein files, and the General Assembly record.
I keep coming back to it because it captures what this book does that almost nothing else in the independent research space manages. I’ve followed Jacob’s work for years now and interviewed him about his research. Each book peels back another layer of the same institutional architecture, and each time I think he’s reached the limit of what can be documented, the next one goes further. Nordangård doesn’t speculate. He doesn’t editorialize much. He lays institutional actions next to each other in chronological order and lets the pattern announce itself. … continue
Blog Roll
 Aletho News
Aletho News- How I fell foul of the BBC thought police
- The End of NATO
- 37 days of war on Iran cost US staggering $42bln, tracker shows
- Baghdad tells Asian refiners, traders to begin loading Iraqi crude amid Iranian exemption
- Under fire, Moscow and Tehran close ranks
- Iran, US receive Pakistan-mediated plan for ceasefire then final deal
- Iran submits demands for end to war as mediators scramble ahead of Trump deadline
- Iran Threatens Retaliatory Strike on Stargate AI Project in UAE
- US sent ‘a lot’ of arms to Iranian protesters – Trump
- Barak Ravid Launders Deception To Allow Trump To Back Off Of His Power Plant Threat – Again
- If Americans Knew
- Israel’s Latest Genocide Is Against the Shias of Lebanon. Why Is the World Silent?
- How Eliot Cohen’s influence over U.S. war-making paved the way for Trump’s war crimes in Iran
- Israelis don’t pay for the weapons we ‘sell’ to them — US taxpayers do
- While Distancing from AIPAC, Most 2028 Democratic Hopefuls Are Still Embracing Israel
- A brief history of the Israeli nuclear program, the open secret at the heart of the Iran war
- Israeli Settlers Killed a Palestinian Farmer on His Own Land, in Front of His Father. Yes, Again
- The US-Israeli War on Science is an Assault on our Future
- 100+ International Law Experts Say US Strikes on Iran Violate UN Charter, Could Be War Crimes
- ‘Vile, Horrifying, Evil’: Trump Threatens to Bomb Nation of 90 Million People ‘Back to the Stone Ages’
- The Axis of Resistance: Islamic Liberation Theology and the Struggle for Freedom
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
