THE RUSSIAN HYDRA
By Paul Robinson | IRRUSSIANALITY | March 16, 2021
If you want to understand international affairs but only have time to read one academic article, the one I’d recommend would be Robert Jervis’ “Hypotheses on Misperception,” published in World Politics in 1968. It contains 14 hypotheses about how states misperceive one another, creating many of the problems which endanger international security. None of it is exactly rocket science, but it’s the kind of obvious truth that needs to be said, and then repeated over and over again, because people seem to be unable to take it in.
I give the article to students in my defence policy course so we can discuss things such as “Hypothesis 8 is that there is an overall tendency for decision-makers to see other states as more hostile than they are,” and “Hypothesis 9 states that actors tend to see the behavior of others as more centralized, disciplined, and coordinated than it is.” Obvious stuff, as I said, but it comes in useful when we move on to discuss other matters such as this week’s class topic, which was hybrid warfare.
Long-term readers of this blog will know that I’m not a fan of the concept of hybrid warfare, but as it’s something students of defence policy will hear a lot about I kind of have to discuss it, for which purpose I googled around looking for suitable diagrams to use to explain the idea. In the process, I came across this one that accompanied an interview a couple of years ago with a guy called Mark Voyger who was at one time a special advisor to Lieutenant General Ben Hodges, the former Commanding General of US Army Europe.

I thought this depiction of the Russian ‘hydra’ with multiple tentacles emanating from a central core to attack the ‘target nation’ was great because it so clearly demonstrates hypotheses 8 & 9 mentioned above, as well as highlighting the absurdity of the hybrid warfare concept.
For what it does is label absolutely everything ‘war’. Intelligence, diplomacy, law, social-cultural activities, cyber, information, energy, economic relations, infrastructure, crime, and conventional military forces are not just intelligence, diplomacy, law etc. They’re WAR!! Which if you think about it is kind of odd. Isn’t diplomacy meant to be kind of the opposite of war? Why are social-cultural activities (e.g. cultural exchanges) war? Why are information or economic relations war? It’s an extraordinarily paranoid view of the world, in which everything another state, or its citizens do, is part and parcel of a campaign to destroy us from within. They don’t trade with us to get rich. No, they trade with us to subvert us! And so on.
In short, the hybrid warfare concept is pretty much an embodiment of hypothesis 8, allowing those who propagate it to exaggerate threats, and make just about everything a matter of security. That, if you think about it, is more than a little scary. Trade, diplomacy, culture, etc. shouldn’t be securitized. But it’s also conceptual dodgy – after all, when everything is war, then the term war loses any meaning as something distinct.
Beyond that, the Russian hydra model in the diagram above perfectly illustrates hypothesis 9 – i.e. the tendency, “to see the behavior of others as more centralized, disciplined, and coordinated than it is.” For in the diagram, all the tentacles come out of a single core, suggesting that the Russian political leadership is coordinating everything everybody in Russia does and directing it towards a single common purpose – destroying the “target nation.” Which is of course absurd – not only does it exaggerate the Russian state’s power and abilities, but it also ignores the fact that many of those engaged in activities such as cultural exchanges, trade, the media, etc., etc., are following their own agendas not those of the state.
Unfortunately, the hydra model seems quite well entrenched in Western thinkers’ minds. I was looking today at the British government’s new review of foreign and defence policy, and it had the following to say:
A more integrated approach supports faster decision-making, more effective policy-making and more coherent implementation by bringing together defence, diplomacy, development, intelligence and security, trade and aspects of domestic policy in pursuit of cross-government, national objectives. The logic of integration is to make more of finite resources within a more competitive world in which speed of adaptation can provide decisive advantage. It is a response to the fact that adversaries and competitors are already acting in a more integrated way – fusing military and civilian technology and increasingly blurring the boundaries between war and peace, prosperity and security, trade and development, and domestic and foreign policy.
You get it – foreign, “malign” states have fully integrated policies, “blurring the boundaries between war and peace” by coordinating defence, diplomacy, trade, etc., etc, in a seamless strategy of aggression.
And here we run into another danger of the hybrid warfare theory. On the basis of the myth of the hybrid ‘hydra’, Western states are now arguing that they need to become the hydra themselves. I can’t see it ending well.
How Do Big Media Outlets So Often “Independently Confirm” Each Other’s Falsehoods?

NBC News’ national security reporter and long-time de facto CIA spokesman Ken Dilanian purporting to “independently confirm” a false CNN story, Dec. 8, 2017
By Glenn Greenwald | March 16, 2021
There were so many false reports circulated by the dominant corporate wing of the U.S. media as part of the five-year-long Russiagate hysteria that in January, 2019, I compiled what I called “The 10 Worst, Most Embarrassing U.S. Media Failures on the Trump-Russia Story.” The only difficult part of that article was choosing which among the many dozens of retractions, corrections and still-uncorrected factual falsehoods merited inclusion in the worst-ten list. So stiff was the competition that I was forced to omit many huge media Russiagate humiliations, and thus, to be fair to those who missed the cut, had to append a large “Dishonorable Mention” category at the end (note: the Intercept’s site seems to be down for the moment, rendering that first link inoperable).
That the entire Russiagate storyline itself was a fraud and a farce is conclusively demonstrated by one decisive fact that can never be memory-holed: namely, the impetus for the scandal and subsequent investigation was the conspiracy theory that the Trump campaign had secretly and criminally conspired with the Russian government to interfere in the 2016 election, primarily hacking into the email inboxes of the DNC and Clinton campaign chief John Podesta. And a grand total of zero Americans were accused (let alone convicted) of participating in that animating conspiracy.
The New York Times’ May, 2017 announcement of Robert Mueller as special counsel stated explicitly that his task was “to oversee the investigation into ties between President Trump’s campaign and Russian officials” and specifically “investigate ‘any links and/or coordination between the Russian government and individuals associated with the campaign of President Donald Trump.’”
The related secondary media-created conspiracy theory was that the Kremlin clandestinely controlled U.S. political institutions by virtue of sexual and financial blackmail held over President Trump, which they used to compel him to obediently obey their dictates. “I don’t know what the Russians have on the president, politically, personally, or financially” was the dark innuendo which House Speaker Nancy Pelosi and her media allies most loved to spout. “Prestige news” outlets created their own Q-Anon-level series of art designed to implant in Americans’ minds a slew of McCarthyite imagery showing the Kremlin (or an iconic Moscow cathedral they mistook for the Kremlin) having fully infiltrated Washington’s key institutions.

Cover story of The New Yorker, Feb. 24, 2017
But that all came crashing down on their heads in April, 2019, when Mueller announced that he was closing his investigation without charging even a single American with the criminal conspiracy that launched the entire spectacle: criminally conspiring with the Russian government to interfere in the election. Again: while Mueller — like so many Washington special counsels before him — ended up snaring some operatives in alleged process crimes committed after the investigation commenced (lying to the FBI and obstruction of justice) or unrelated crimes (Manafort’s financial sleaze), the 18-month aggressive, sprawling investigation resulted in exactly zero criminal charges on the core claim that Trump officials had criminally conspired with Russia.
If that were not sufficient to make every person who drowned the country in this crazed conspiracy theory feel enormous shame (and it should have been), the former FBI Director’s final Report explicitly stated that “the investigation did not establish that members of the Trump campaign conspired or coordinated with the Russian government in its election.” In many cases, the Report went even further than this “did not establish” formulation to state that there was no evidence of any kind found for many of the key media conspiracies (“The investigation did not identify evidence that any U.S. persons knowingly or intentionally coordinated with the IRA’s interference operation”; the “evidence does not establish that one campaign official’s efforts to dilute a portion of the Republican platform was undertaken at the behest of candidate Trump or Russia”; “the investigation did not establish that [Carter] Page coordinated with the Russian government in its efforts to interfere in the 2016 presidential election”). The Report also barely even dignified let alone confirmed the long-standing, utterly deranged Democratic/media conspiracy theory that the Kremlin had taken over U.S. policy through blackmail.

The Advocate, Mar. 10, 2017
For a few weeks following the issuance of the Mueller report, Democrats and media figures gamely attempted to deny that it obliterated the conspiracy theories to which they had relentlessly subjected the country for the prior four years. How could they do otherwise? They staked their entire reputations and the trust of their audience on having this be true. To avoid their day of reckoning, they would hype ancillary events such as Paul Manafort’s conviction on unrelated financial crimes or Michael Flynn’s guilty plea for a minor and dubious charge (for which even Mueller recommended no prison time) or Roger Stone’s various process charges to insist that there was still a grain of truth to their multifaceted geopolitical fairy tale seemingly lifted straight from a Tom Clancy Cold War thriller about the world’s two largest nuclear powers.
But even they knew this was just a temporary survival strategy and that it was unsustainable for the long term. That the crux of the scandal all along was that key Trump allies if not the President himself would be indicted and imprisoned for having conspired with the Russians was too glaring to make people forget about it.
That was why former CIA Director John Brennan assured the MSNBC audience in March — just weeks before Mueller closed his investigation with no conspiracy crimes alleged — that it was impossible that the investigation could close without first indicting Trump’s children and other key White House aides on what Brennan correctly said was the whole point of the scandal from the start: “criminal conspiracy involving the Russians . . . . whether or not U.S. persons were actively collaborating, colluding, cooperating, involved in a conspiracy with them or not.” Brennan strongly insinuated that among those likely to be indicted for criminally conspiring with the Russians were those “from the Trump family.”
As we all know, literally none of that happened. Not only were Trump family members not indicted by Mueller on charges of “criminal conspiracy involving the Russians,” no Americans were. Brennan believed there was no way that the Mueller investigation could end without that happening because that was the whole point of the scandal from the start. To explain why it had not happened up to that point after eighteen months of investigation by Mueller’s subpoena-armed and very zealous team of prosecutors, Brennan invented a theory that they were waiting to do that as the final act because they knew they would be fired by Trump once it happened. But it never happened because Mueller found no evidence to prove that it did.
In other words, the conspiracy theory that the media pushed on Americans since before Trump’s inauguration — to the point where it drowned out most of U.S. politics and policy for years — proved to have no evidentiary foundation. And that is one reason I say that the sectors of the media pretending to be most distraught at the spread of “disinformation” by anonymous citizens on Facebook and 4Chan are, in fact, the most aggressive, prolific and destructive disseminators of that disinformation by far (nor was it uncredentialed YouTube hosts, Patreon podcasters or Substack writers who convinced Americans to believe that Saddam Hussein possessed nuclear weapons and was in an alliance with Al Qaeda but rather the editor-heavy prestige outlets such as The New York Times, The New Yorker, NBC News and The Atlantic).
With the crux of the Russiagate conspiracy theory collapsed, U.S. media outlets began acknowledging — because they had to — that none of it was vindicated by Mueller’s report. To do so, they abruptly nullified a rule that had been in place since Mueller’s appointment: one may not speak ill of the former FBI Director because he is a patriotic man of the highest integrity and to malign him is to undermine the Brave Men and Women of the FBI Who Keep Us Safe. The only self-preservation tactic they could find to salvage their credibility was to turn on Mueller, quite viciously. Overnight, the storyline emerged: the conspiracy theory we pushed on you was correct all along, but Mueller was a coward and failed in his patriotic duty to say so.

While the hypocrisy of watching a media that for months demanded reverence for Mueller turn on a dime to accuse him of being a borderline-senile, unpatriotic coward was quite amazing, it was at least some progress toward acknowledging the undeniable reality that the media had collectively failed. Their dark conspiracies and predictions of doom were pipe dreams. They flooded the country with disinformation for years about all of this. And while they characteristically engaged in exactly zero self-reflection or self-critique — preferring to heap all the blame on Mueller instead for failing to find the evidence that is still out there of their cognitive derangements — it at least consecrated the fact that this scandal ended in humiliation for them.
When I created my top ten list of media Russiagate debacles, choosing the top ten was difficult but choosing the top spot was not. It is worth briefly revisiting that particular journalistic humiliation because of what it reveals about ongoing media behavior.
On the morning of December 8, 2017, CNN went on the air with one of the most cataclysmic and breathless scoops of the entire Russiagate saga. The network hauled out all of its most melodramatic graphics, music and host voice-tones to signify that this was it : the smoking gun, the ultimate bombshell, the final nail in the coffin, inescapable proof for their conspiracy theory. The big huge scoop notably came from its Congressional reporter Manu Raju (one of the favorite dumping grounds for false leaks by leading House Democrat Russiagate fanatics such as Rep. Adam Schiff and Eric Swalwell (D-CA)).
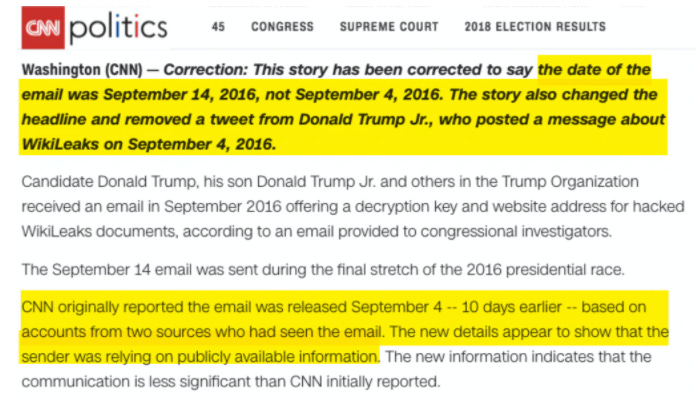
According to this historic CNN revelation, a stunning and incriminating email had been obtained by “congressional investigators,” and “multiple sources” conveyed its contents to CNN. This email proved, said CNN, that Donald Trump Jr. was given advanced access to the archive of DNC and Podesta emails ultimately published by WikiLeaks on September 14, 2016. This earth-shattering email to Trump, Jr. was dated September 4 — ten days before WikiLeaks began publishing — and this, in the minds of CNN, proved somehow that the Trump campaign was in on the plot from the start.
Now, even if Trump had been shown the archive in advance by WikiLeaks or someone else, it would not have remotely proven that the Trump campaign was a participant in the plot, but let us not get detained on that hypothetical. The CNN story was treated by the entire liberal sector of the press as the most devastating and incriminating evidence yet produced to prove the truth of the Russiagate conspiracy theory, with one particularly loyal Democratic partisan-writer using an image of a nuclear explosion to convey its significance:

Talking Points Memo editor Josh Marshall, Dec. 8, 2017
As it turns out, there was one small problem with the CNN story: it was completely and utterly false. The email to Trump, Jr. on which the entire bombshell was based was sent after WikiLeaks began publishing the archive, not before. And it was sent not by some super-secret inside source with the Kremlin or WikiLeaks, but by a random member of the public who, having read about the WikiLeaks publications in the newspaper, emailed Trump, Jr. to encourage him to take a look.
How “multiple sources” all got the date on the email wrong — mis-reading it as September 4 rather than the real date of the email: September 14 — was never explained by CNN. That is because corporate media outlets believe they owe the public no explanation or accountability for the massive errors they commit.
But what was most notable about this episode is that it was not just CNN which reported this fraudulent story. An hour or so after the network shook the political world with its graphics-and-music-shaped bombshell, other news networks — including MSNBC and CBS News — claimed that they had obtained what they called “independent confirmation” that the story was true.
All of these media outlets, reading Orwell as if it is an instruction manual, have now scrubbed most of the humiliating videos where they did this from the internet. But one can still watch here as NBC News’ national security reporter and long-time de facto CIA spokesman Ken Dilanian breathlessly tells an MSNBC host, who herself can barely maintain her composure, that he has spoken with “sources” who have provided independent confirmation of the CNN story, thus adding NBC News’ imprimatur to it. Shortly thereafter, CBS News did the same.
All of this prompted the obvious question: how could MSNBC and CBS News have both purported to “independently confirm” a CNN bombshell that was completely false? The reason this matters is because the term “independently confirm” significantly bolsters the credibility of the initial report because it makes it appear that other credible-to-some news organizations have conducted their own investigation and found more evidence that proves it is true. That is the purpose of the exercise: to bolster the credibility of the story in the minds of the public.
But what actually happens is as deceitful as it is obvious. When a news outlet such as NBC News claims to have “independently corroborated” a report from another corporate outlet, they often do not mean that they searched for and acquired corroborating evidence for it. What they mean is much more tawdry: they called, or were called by, the same anonymous sources that fed CNN the false story in the first place, and were fed the same false story. And just as CNN did — repeated what they were told (almost certainly by Democratic Congressional members and/or their staff) without independently investigating it, because they knew any anti-Trump story would please their partisan audience — NBC News pretended they had obtained “independent confirmation” when all they had done was speak to the same sources that fed CNN.
This episode is so worth recalling not only because it is one of the most stunning and pathetic media humiliations of the Trump era — though it is that — but also because the shoddy tactic that drove it is still in full use by the same media outlets. We just saw proof of that again with a major Washington Post “correction” — which should be called a retraction — of one of the most-discussed news stories of the last six months: the Post’s claims about what Trump said when he called a Georgia election official while he was still contesting the 2020 election results.
On January 9, The Washington Post published a story reporting that an anonymous source claimed that on December 23, Trump spoke by phone with Frances Watson, the chief investigator of the Georgia Secretary of State’s office, and directed her that she must “find the fraud” and promised her she would be “a national hero” if she did so. The paper insisted that those were actual quotes of what Trump said. This time, it was CNN purporting to independently confirm the Post’s reporting, affirming that Trump said these words “according to a source with knowledge of the call.”
But late last week, The Wall Street Journal obtained a recording of that call, and those quotes attributed to Trump do not appear. As a result, The Washington Post — two months after its original story that predictably spread like wildfire throughout the entire media ecosystem — has appended a correction at the top of its original story. Politico’s Alex Thompson correctly pronounced these errors “real bad” because of how widely they spread and were endorsed by other major media outlets.

This is a different species of journalistic malpractice than mere journalistic falsehoods. As I detailed in February and again two weeks ago, the U.S. public was inundated for weeks with an utterly false yet horrifying story — that a barbaric pro-Trump mob had savagely murdered Capitol Police Officer Brian Sicknick by bashing his skull in with a fire extinguisher. That false tale about the only person said to have been killed at the January 6 riot other than pro-Trump supporters emanated from a New York Times report based on the claims of “two anonymous law enforcement officials.”
As it turns out, Sicknick’s autopsy revealed that he suffered no blunt trauma, and two men arrested this week were charged not with murder but assault and conspiracy to injure an officer: for using an unidentified gas. In reporting those arrests, even The New York Times acknowledged that “prosecutors stopped short of linking the attack to Officer Sicknick’s death the next day” because “both officers and rioters deployed spray, mace and other irritants during the attack” and “it remains unclear whether Officer Sicknick died because of his exposure to the spray.”
Many liberals defenders of these corporate media outlets insist that these major factual errors do not matter because the basic narrative — Trump and his supporters at the Capitol are bad people who did bad things — is still true. But these errors are enormous. That Trump, Jr. received that email from a random member of the public after WikiLeaks began publicly publishing documents transforms the story from smoking gun to irrelevant. That Trump did not utter the extremely incriminating quotes attributed to him in that call at least permits debate about whether he did anything wrong there and what his intent was (encouraging the official to find the fraud he genuinely believed was there or pressuring her to manufacture claims with threats and promises of reward). And there is, manifestly, a fundamental difference in both intent and morality between deliberately murdering someone by repeatedly bashing their skull in with a fire extinguisher and using a non-lethal crowd-control spray frequently used at protests even if it is ultimately proven that the spray is what caused Officer Sicknick’s death (which is why those two acts would carry vastly different punishments under the law).
But all of this highlights the real crisis in journalism, the reason public faith and trust in media institutions is in free fall. With liberal media outlets deliberately embracing a profit model of speaking overwhelmingly to partisan Democrats who use them as their primary source of news, there is zero cost to publishing false claims about people and groups hated by that liberal audience.
That audience does not care if these media outlets publish false stories as long as it is done for the Greater Good of harming their political enemies, and this ethos has contaminated newsrooms as well. Given human fallibility, reporting errors are normal and inevitable, but when they are all geared toward advancing one political agenda or faction and undermining the other, they cease to be errors and become a deliberate strategy or, at best, systemic recklessness.
But whatever else is true, it is vital to understand what news outlets mean when they claim they have “independently verified” the uncorroborated reports of other similar outlets. It means nothing of consequence. In many if not most cases — enough to make this formulation totally unreliable — it signifies nothing more than their willingness to serve as stenographers for the same anonymous political operatives who fed their competitors similar propaganda.
New York Times: Most East Coast Beaches Gone By 2020
BY Tony Heller | Real Climate Science | March 11, 2021
In 1995, the New York Times predicted “most of the beaches on the East Coast of the United States would be gone in 25 years”

Scientists Say Earth’s Warming Could Set Off Wide Disruptions – The New York Times
Barack Obama believes in the science, and just bought a $15 million home on an East Coast beach.
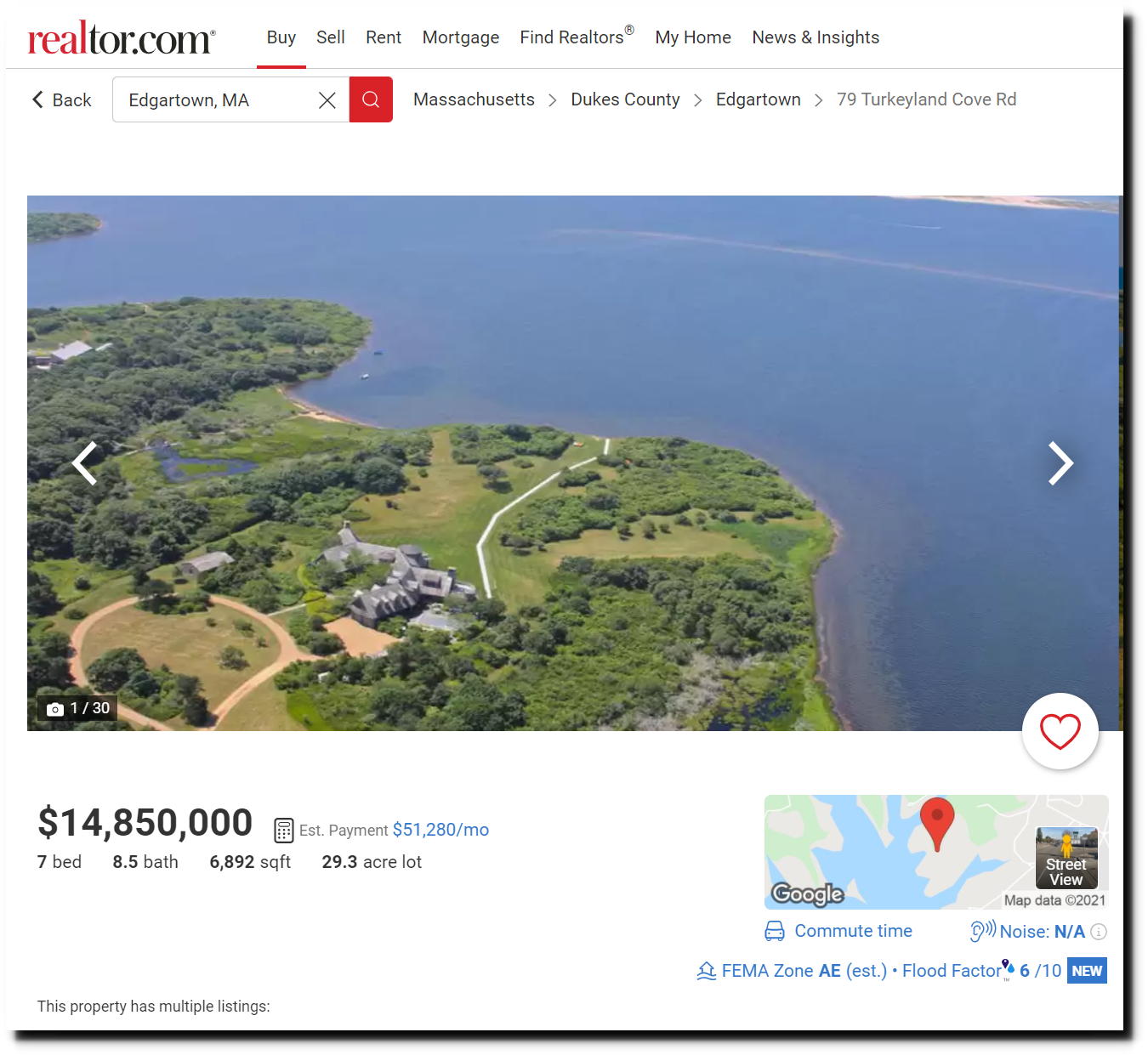
Barack and Michelle Obama buying $14.85M Martha’s Vineyard estate
The article also said:
The intergovernmental panel forecasts an increase in droughts like the current one in the Northeastern United States, heat waves like the one in Chicago this summer, and more fires and floods in some regions.
*A “striking” retreat of mountain glaciers around the world, accompanied in the Northern Hemisphere by a shrinking snow cover in winter.“
Since then, winter snow cover has increased to near record highs.
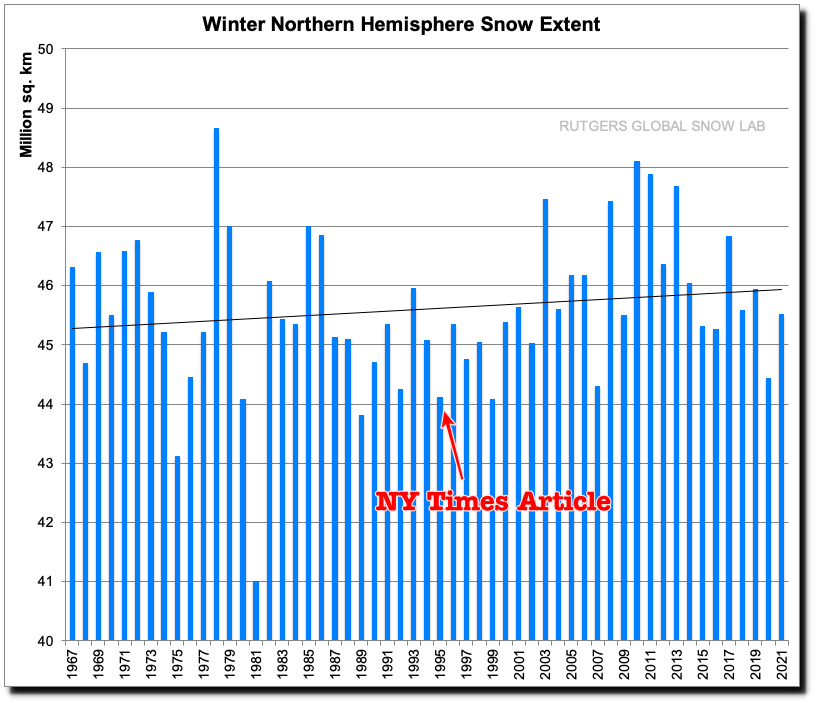
Rutgers University Climate Lab :: Global Snow Lab
Droughts have become less common and severe in the US since the 19th century.

Climate at a Glance | National Centers for Environmental Information (NCEI)
And the likelihood of hot weather has plummeted in the US.

Video evidence of ‘massacre’ by UK special forces in Afghanistan mysteriously VANISHES

RT | March 14, 2021
Video allegedly showing a “rogue” SAS unit committing war crimes in Afghanistan has supposedly disappeared, as an investigation into the squad’s alleged “massacres” has been plagued by missing evidence and silence from witnesses.
Saifullah Yar was just 19 when his family were shot dead in an SAS raid on their Afghan village in 2011. When British military investigators flew to Kabul in 2017 to investigate the raid, he told them he was handcuffed and led away from his father, brother and two male cousins. He heard two sustained bursts of gunfire, and when the Brits departed, his relatives were dead, their bodies riddled with bullets.
Video footage of the raid was apparently captured by US air support overhead, but according to a new Sunday Times report, American authorities mysteriously lost the footage, and were unable to provide it to a British court, where Saifullah has brought a judicial review into the fatal raid.
The mysterious disappearance isn’t the first time that key evidence from the raid has gone missing, or been intentionally hidden. The Royal MIlitary Police (RMP) investigators’ 2017 visit to Kabul was one of their last tasks in a three-and-a-half year probe into allegations of war crimes against the SAS unit, during which they found that the British operators doctored mission reports to implicate Afghan special forces in similar killings, dozens of which took place between 2011 and 2013.
The investigators interviewed 42 soldiers who said they were unable to remember the mission. Court documents reported on by the Times stated that a judge termed this a case of “collective amnesia.” The weapons used in the raid on Saifullah’s village were destroyed the same year the RMP opened its investigation.
However, evidence against the SAS troops has piled up. Investigators found that British 5.56mm bullets, rather than the 7.62mm rounds used by the Afghan commandos, were used to kill the victims. Additionally, they examined reports that weapons were planted on the bodies of these victims, in order to justify the killings later.
The reports that followed the 2011 raid on Saifullah’s village stated that his family were killed when they reached for weapons as the SAS searched their property. These reports were met with skepticism by senior commanders, who in a chain of emails seen by the British court, described the raid as “the latest massacre,” and expressed disbelief at the idea of four overpowered prisoners reaching for hidden grenades and rifles during the raid.
“And finally they shot a guy who was hiding in a bush who had a grenade in his hands. You couldn’t MAKE IT UP!,” one senior noncommissioned officer wrote.
The British government closed down the investigation in late 2017 without prosecuting a single case. The same year, another wide-ranging investigation into alleged war crimes, the Iraq Historic Allegations Team (IHAT), was shut down, also without prosecuting a case.
With the SAS typically exempt from parliamentary oversight, the courts are now Saifullah’s best hope of finding justice. “Our client is seeking a fresh investigation into the deaths of his loved ones and he wants to find out whether their deaths were part of a pattern of unlawful killings of Afghan civilians,” his lawyer, Tessa Gregory, told the Sunday Times.
Featured Video

Tales of American POWs in Vietnam
or go to
Aletho News Archives – Video-Images
From the Archives
US Also Destroyed Iraqi Water Supply During First Gulf War
International Humanitarian Law prohibits the attack, destruction, or rendering useless of objects indispensable to civilian survival.
By Kurt Nimmo | Another Day in the Empire | June 10, 2026
… During the first Gulf War, the United States “deliberately bombed Iraq’s water system,” Thomas J. Nagy, a professor at George Washington University, wrote in September, 2001. The Bush administration, “with malice aforethought,” “destroyed, removed, or rendered useless” Iraq’s ‘drinking water installations and supplies’… They amount to a systematic effort to, in the DIA’s own words, ‘fully degrade’ Iraq’s water sources.”
Nagy found declassified documents at the website of the Office of the Special Assistant for Gulf War Illnesses that detailed the effort to degrade Iraq’s water supply and commit a serious violation of humanitarian law. The documents included “Iraq Water Treatment Vulnerability,” “Disease Information,” “Disease Outbreaks in Iraq,” “Medical Problems in Iraq,” “Status of Disease at Refugee Camps,” “Health Conditions in Iraq,” and “Iraq: Assessment of Current Health Threats and Capabilities.”
Then Representative Cynthia McKinney, a Democrat from Georgia (subsequently removed from Congress), referred to the Iraq Water Treatment Vulnerabilities document, and said, “Attacking the Iraqi public drinking water supply flagrantly targets civilians and is a violation of the Geneva Convention and of the fundamental laws of civilized nations.” … Read full article
Blog Roll
 Aletho News
Aletho News- EU court adviser delivers another ‘Pfizergate’ blow to von der Leyen
- 88 attacks against Palestinian Christians recorded since start of year
- Secretary of War Crimes
- Palestinian factions submit response to mediators, reject disarmament proposal
- US ‘limited war’ strategy against Iran deepens its strategic quagmire as Tehran’s deterrence grows
- Arab Powers Mull Regional Security Alliance – Jordan’s Ex-Minister
- A New Economic Front: Yemen’s Entrance to Regional War against US-Israeli Alliance
- Will Trump Break JFK’s Agreement on Cuba?
- Settlers, sanctions and impunity
- Christian village in occupied West Bank goes up in flames after large-scale attack by Israeli settlers
- If Americans Knew
- Senate wants to force US to share sensitive intel with Israel
- ‘They used dogs’: New Al Jazeera film exposes Israel’s use of rape in jails
- Israel is abducting ordinary Syrians and seizing their land in Quneitra
- Piro Inc Promotes Israel Government Ad Agency’s push to sway US Public Opinion: 2 Articles
- Israel has US on the brink of war with Iran, stirs up chaos around the world – Daily Update
- Welcome to the 60th Year of Israel’s Occupation of the West Bank
- In south Lebanon, as in Gaza, Israeli drones use the sound of crying children to lure civilians
- Israel’s ethnic cleansing of West Bank Bedouin and herding communities
- Israel has no mercy on Christian communities in West Bank, Lebanon: 2 Articles
- “No Exit”: Israel is killing Gaza patients with delays – Daily Update
- No Tricks Zone
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
