https://www.bitchute.com/video/Yd5AuSxmyAln/
In this group interview facilitated by Sam Dubé, M.D., Ph.D., four physicians from across Canada – emergency physician Dr. Chris Milburn, rural family physician Dr. Charles Hoffe, general surgeon Dr. Francis Christian, and pathologist Dr. Roger Hodkinson – tell their stories of persecution at the hands of their governing bodies. Their only crime: practicing evidence-based medicine by questioning the safety of their patients and the public during the pandemic.
A legal representative for their cases, John Carpay, Esq., provides insights and legal commentary, invoking the Canadian Charter of Rights and Freedoms. These physicians, and others like them, are the living embodiment of the medical mantras of “do no harm” and “informed consent”.
July 14, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science, Timeless or most popular, Video | Canada, Covid-19, COVID-19 Vaccine, Human rights |
Leave a comment
One of the strangest things about the last few months on planet Earth has been the relentless drive to vaccinate everyone, regardless of what their individual risk from the virus is, and whether or not they’ve already had the disease. It was well known long before covid came along that people who have had an infection are usually at least as well protected as those who get vaccinated. The whole point of vaccination is, after all, to mimic infection so as to stimulate immunity. If you’ve had measles, you don’t need to take the measles vaccine. If you’ve had hepatitis A, you don’t need to take the hepatitis A vaccine. If you’ve had chickenpox, you don’t need to take the chickenpox vaccine. Yet if you’ve had covid, you should supposedly still take the covid vaccine. Strange.
The obsession with vaccinating everyone is particularly odd in a situation where access to vaccines is limited and the stated goal is to reach herd immunity as quickly as possible, since wasting time vaccinating people who have already had the infection will inevitably delay the time it takes for a population to reach herd immunity.
Yet many people who should know better have been happy to play along with the “everyone needs to be vaccinated” mantra, in spite of the fact that it runs counter to the stated goal of governments and public health agencies. Many doctors had covid during 2020, yet they were more than happy to stand at the front of the line and take the vaccine in late 2020 and early 2021, even though they knew (or should have known) that they were almost certainly already maximally protected from the virus, and that taking the vaccine would inevitably mean a delay in vaccination of those who had not yet had the infection.
A few months back I wrote about a study, published in The Lancet in April, that showed a 93% decreased risk of re-infection in people who had already had covid. That would make prior infection equivalent to the most effective vaccines, in terms of its ability to protect against covid (which is as we would expect).
For those who remain unconvinced that prior infection is at least equivalent to vaccination, however, a very interesting study was recently posted on MedRxiv. This was a retrospective cohort study of the 52,238 employees of the Cleveland Clinic, who were followed from December 16th 2020 (when the Cleveland Clinic started vaccinating its staff) until May 15th 2021. The objective of the study was to compare the relative rates of infection between four groups of employees: Thos who had had covid and been vaccinated, those who had had covid but not yet been vaccinated, those who had not had covid but had been vaccinated, and those who had neither had covid nor been vaccinated.
A PCR test was used to diagnose covid in the study. The Cleveland Clinic was not engaging in any screening of asymptomatic staff during the study period, so tests were in almost all cases carried out when participants developed symptoms suggestive of covid. In other words, the method used to diagnose covid in this study was equivalent to the method used in most other studies, and also the method that is used in the real world.
So, what were the results?
There were 2,139 new covid infections among the 52,238 participants. In other words, 4.1% of the participants in the study developed covid during the five month period. 99.3% of these infections were among participants who had neither had covid nor been vaccinated. The remaining 0,7% were among participants who hadn’t had covid but had been vaccinated.
2,579 participants had already had covid at the start of the study. Not a single one of them developed covid during the five month period. This includes both the 1,229 with prior infection who were vaccinated, and the 1,359 who weren’t. What that means is that prior infection was associated with a 100% reduction in the relative risk of infection. That was true regardless of whether the person with prior infection was vaccinated or not. Vaccination did not provide any additional benefit to those who had already had covid.
What can we conclude?
Prior infection is highly effective at protecting against covid. There is thus no need for people who have already had covid to get vaccinated. When governments do vaccinate people who have already had covid, they are wasting taxpayers money and putting people at risk of side effects for no good reason.
July 13, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine |
Leave a comment
Dr Charles Hoffe MD, in his latest update of July 6, 2021 is reporting on the disturbing findings in his patients. He says the mRNA vaccines are plugging up thousands of tiny capillaries in the blood of those who took the ‘vaccine.’ Most will die in a few short years from heart failure.
The spike proteins injected, which are designed to be mass produced in the bodies of the vaccinated, are the cause of the clotting, which is having adverse effects on no fewer than 60 percent of people injected.
Dr Hoffe, who practices medicine at Lytton BC Canada explains:
“We now know that only 25 percent of the ‘vaccine’ injected into a person’s arm actually stays in your arm. The other 75 percent is collected by your lymphatic system and literally fed into your circulation so these little packages of messenger RNA, and by the way in a single dose of Moderna ‘vaccine’ there are literally 40 trillion mRNA molecules. These packages are designed to be absorbed into your cells. But the only place they can be absorbed is around your blood vessels and the place where they are absorbed is the capillary networks – the tiniest blood vessels where the blood flow slows right down and where the genes are released. Your body then gets to work reading and then manufacturing trillions and trillions of these spike proteins. Each gene can produce many, many spike proteins. The body then recognises these are foreign bodies so it makes antibodies against it so your are then protected against COVID. That’s the idea.”
But here’s where the problem comes. In a coronavirus that spike protein becomes part of the viral capsule. In other words it becomes part of the cell wall around the virus. But it is not in a virus. It is in your cells. So it becomes part of the cell wall of your vascular endothelium.
This means that these cells which line your blood vessels, which are supposed to be smooth so that your blood flows smoothly now have these little spikey bits sticking out.
Dr Hoffe continues:
“So it is absolutely inevitable that blood clots will form because your blood platelets circulate round your blood vessels, and the purpose of blood platelets is to identify damaged vessels and stop bleeding. So, when the platelet comes through the capillary it suddenly hits all these COVID spikes and it becomes absolutely inevitable that blood clots will form to block that vessel.”
Therefore, these spike proteins can predictably cause blood clots. They are in your blood vessels (if mRNA ‘vaccinated’) so it is guaranteed. Dr Bahrdi then said to me that the way to prove this is to do a blood test called a D-dimer blood test.
“The blood clots we hear about which the media claim are very rare are the big blood clots which are the ones that cause strokes and show up on CT scans, MRI, etc. The clots I’m talking about are microscopic and too small to find on any scan. They can thus only be detected using the D-dimer test.”
Dr Hoffe explains he has been performing D-dimer tests on his mRNA ‘vaccinated’ patients and he has worryingly identified that 62 percent of them had these microscopic blood clots.
“These people have no idea they are even having these microscopic blood clots. The most alarming part of this is that there are some parts of the body like the brain, spinal cord, heart and lungs which cannot re-generate. When those tissues are damaged by blood clots they are permanently damaged.”
The result, says Dr Hoffe, is that these patients have what is termed Reduced Effort Tolerance (RET) which means they get out of breath much easily than they used to. It is because the blood vessels in their lungs are now blocked up. In turn, this causes the heart to need to work harder to try to keep up against a much greater resistance trying to get the blood through your lungs.
This is called pulmonary artery hypertension – high blood pressure in the lungs because the blood simply cannot get through effectively. People with this condition usually die of heart failure within a few short years.
In conclusion, Dr Hoffe lamented:
“These Shots Are Causing Huge Damage And The Worst Is Yet To Come.”
Source: www.bitchute.com
July 13, 2021
Posted by aletho |
Timeless or most popular, Video | COVID-19 Vaccine |
Leave a comment
Groups allied with the Biden administration are planning on working directly with cellphone network providers to ‘fact check’ private SMS messages if they contain “misinformation about vaccines.”
The revelation is made in a Politico article which explains how the White House is preparing to characterize “conservative opponents of its Covid-19 vaccine campaign as dangerous and extreme.”
The decision to ramp up the information war against vaccine skeptics was made after conservatives showed resistance to the Biden administration’s plan to go “door-to-door” to increase vaccination rates.
“Biden allied groups, including the Democratic National Committee, are also planning to engage fact-checkers more aggressively and work with SMS carriers to dispel misinformation about vaccines that is sent over social media and text messages,” states the report. “The goal is to ensure that people who may have difficulty getting a vaccination because of issues like transportation see those barriers lessened or removed entirely.”
https://twitter.com/disclosetv/status/1414655500344565764?ref_src=twsrc%5Etfw%7Ctwcamp%5Etweetembed%7Ctwterm%5E1414655500344565764%7Ctwgr%5E%7Ctwcon%5Es1_&ref_url=https%3A%2F%2Fsummit.news%2F2021%2F07%2F12%2Fdemocrat-groups-plan-to-fact-check-private-sms-messages%2F
The prospect of the DNC and other government-affiliated groups having access to Americans’ private text messages represents a chilling surveillance dystopia.
Interfering with and trying to ‘fact check’ people’s personal conversations is also utterly demented.
Recall that ‘fact-checkers’ infamously declared the Wuhan lab leak hypothesis to be a “debunked conspiracy theory” at the start of the pandemic, only to be forced into a humiliating reversal later on.
In doing so, they may have helped facilitate one of the biggest cover-ups in modern history, so what business such groups have in snooping on people’s private SMS messages is anyone’s guess.
July 12, 2021
Posted by aletho |
Civil Liberties, Full Spectrum Dominance | COVID-19 Vaccine, United States |
Leave a comment
The latest weekly US VAERS update added a shocking 2,083 post-vaccination deaths

USA: Reported post-vaccination deaths, 1990 to 2021 (OpenVAERS)
The latest weekly US VAERS update added a shocking 2,083 post-vaccination deaths – by far the largest weekly increase to date – raising the total of reported post-vaccination deaths to 9,048. Not all of these 2,083 deaths occurred within a week, as there is a very significant reporting backlog.
In total, close to 1,000 post-vaccination miscarriages, more than 3,000 heart attacks, about 7,500 disabilities, close to 20,000 severe allergic reactions, and close to 1,000 cases of heart muscle inflammation in people under 25 have already been reported to VAERS.
A recent analysis by researchers at Queen Mary University in London found that even in senior citizens, about 85% of deaths reported to VAERS were definitively, likely or possibly caused by the vaccine. Moreover, due to significant under-reporting, the true number of vaccine-related deaths may already be significantly higher, possibly in the range of 10,000 to 50,000 deaths in the US alone.
Indeed, despite very few covid deaths, there continues to be unexplained excess all-cause mortality in all US age groups below the age of 75, with all-cause mortality having reached record levels in age groups below 45 since the beginning of the vaccination campaign. In people over 75, potential vaccine-related mortality may be masked by post-winter wave negative excess mortality.
There has been much discussion recently about an ultimately retracted paper that claimed covid vaccines kill 2 people for every 3 people they save. The two major points of criticism were that the paper underestimated vaccine protection by considering only a three-week period, and that the paper overestimated vaccine-related deaths by counting all reported post-vaccination deaths.
The first point is valid: vaccine protection should be estimated based on a near-100% population infection rate, not just a three-week window. But the second point is misguided: due to under-reporting, reported deaths are a lower bound, not an upper bound, of vaccine-related deaths.
Yet there is an even more important point to be considered: age-based risk-stratification. Below a certain age, covid-related mortality is so low that covid vaccines are bound to kill or severely injure more healthy people than they save. In some western European countries, this age threshold may in fact be as high as 60 years (for healthy people).
It has been argued that vaccination against covid may at least prevent “long covid” or multi-system inflammatory syndrome (MIS) in children and young adults; however, new reports from Israel and the US indicate that, to the contrary, covid vaccines may themselves cause MIS as well as “long covid”-like conditions, often lasting for months or possibly even longer.
Going forward, three covid vaccine-related potential risks should be kept in mind:
- In addition to immediate adverse events (such as strokes and heart attacks), are covid vaccines causing cardiovascular damage that will become apparent only later?
- In the face of new immune-escape coronavirus variants, such as the Indian and Peruvian variants (delta and lambda), how long will vaccine protection last, especially in senior citizens?
- Once new coronavirus variants achieve full immune escape, will the very high levels of vaccine-induced, non-neutralizing antibodies cause antibody-dependent disease enhancement (ADE)?
As a potential alternative to current covid vaccines, three options could be considered:
- Natural infection, combined with early treatment to avoid disease progression
- Medically supervised, low-dose oral live virus challenge (using least virulent strain)
- Fast-tracking possibly safer nasal/oral covid vaccines currently being developed
July 11, 2021
Posted by aletho |
Aletho News | COVID-19 Vaccine |
Leave a comment

… This is what is called a “trial balloon.” The government is throwing this out there as a “trial” to see just how much the American public will tolerate in terms of government intervention.
Let them know that you will not tolerate it at all!
The Fourth Amendment of the Constitution protects you from unlawful searches and seizures in your home.
So here is my advice for what you should be prepared to do NOW, this week, if people come to your door to talk to you about the COVID-19 shots.
This advice is based on my years of experience in my working with attorneys all across the U.S. regarding the over-reach of local government agencies such as Child Protective Services who routinely come to people’s homes with the express purpose of looking for a reason to medically kidnap their children.
Most of those legal issues apply to this situation as well, regarding government agents coming to your home to discuss COVID-19 “vaccines.”
First, whether you are a renter or homeowner, the government has no right to enter your property without a warrant signed by a local judge. Absent that warrant, if you don’t want them there, they are trespassing.
And this includes any law enforcement agents. If they cannot produce a warrant signed by a judge, not only are they trespassing, if they are openly carrying a firearm (as most do), they are presenting a threat to you and your family.
Treat them as your enemy, not as your friend. Ask them to leave immediately.
Secondly, you are under no legal obligation to answer any questions – period! You have a 5th Amendment right to remain silent, and if that applies to criminals who are arrested based on an arrest warrant, how much more does that apply to you as a private citizen on your own property where you have not even been accused of a crime?
Do NOT answer any questions! Ask them to leave immediately. Put up as many “No Trespassing” signs as possible on your property, like the one I put as the featured image in this article.
No matter what they say to you, or ask you, the only words that should come out of your mouth should be: “You need to leave now. You are trespassing on private property.”
Third, RECORD EVERYTHING! The best way to record is to have a hidden camera pointed at your door, and then to also hold up a cell phone camera right in front of their face to let them know you are recording.
If they rip the cell phone out of your hand, hopefully you have a second camera somewhere also recording that. If you do, take that recording to your local District Attorney and ask them to press charges. Then send it to us also, and we will publish it to our international audience.
Expect FALSE FLAG events! To merely question the safety or efficacy of these injections is to be labeled a “domestic terrorist.” You can be sure that if these volunteers that are sent out door-to-door are not successful, that they will soon move on to the next stage of their plan, and at some point they are going to stage an event where some “domestic terrorists” allegedly decide to start killing people who are just “trying to do their jobs” and “provide a safe community” by “getting everyone vaccinated.”
Do your best to record everything that happens when unwelcome visitors decide to violate your 4th Amendment rights by coming on your property to discuss COVID-19 “vaccines” that you have no intention of discussing. … Full article
July 11, 2021
Posted by aletho |
Civil Liberties | COVID-19 Vaccine, Human rights, United States |
Leave a comment

Once a con man, always one — how Sanders operated throughout his public life as Burlington, VT mayor, congressman and senator.
Time and again saying one thing, then going another way, he nearly always supports destructive policies pursued by undemocratic Dems.
Notably he backs public health destroying flu/covid policies while pretending to want Americans protected.
“Does anyone deny that we have a major healthcare crisis,” he asked?
True enough because of increasing unaffordability, leaving most US households uninsured or way-underinsured.
His remark also relates to all things flu/covid he supports — notably the Biden regime’s diabolical scheme to mass-jab maximum numbers of Americans with unapproved, experimental drugs designed to destroy health, not the other way around.
Falsely calling them “safe and effective (sic),” he urged Americans to “continue wearing masks (that don’t protect and risk respiratory harm) and engage in social distancing” that’s all about destruction of normal interactions and social control.
Claiming the above “is how we will beat this virus and end this terrible pandemic” ignores that protecting and preserving health requires ignoring what’s mandated and recommended at a time when a so-called “pandemic” was invented, not real.
Complicit with state-sponsored fear-mongering, Sanders defied reality by falsely claiming that a non-crisis “crisis we face from (flu/covid) is on the scale of a major war (sic).”
He urged continued use of respiratory system-destroying ventilators and need for “increase(d) healthcare capacity to handle a (nonexistent) surge in (flu/covid) cases” during months when they normally increase with no fear-mongering created mass hysteria until last year.
He also falsely claimed that the US “healthcare system does not have the doctors and nurses we need (sic). We are understaffed (sic),” adding:
“We need to mobilize medical residents (sic), retired medical professionals (sic), and other medical personnel to help us deal with this crisis (sic).”
No shortage of providers exists. No crisis.
Because over one-fourth of working-age Americans are unemployed, most others way underemployed as healthcare costs rise, an affordability crisis exists, not availability of care in the world’s richest country.
The Economic Collapse Blog explained the following:
“(T)he vast majority of the available (US) ‘jobs’ pay so little that most Americans don’t want them.”
It’s at a time of “skyrocketing” costs of housing, health insurance premiums, food and other essentials.
“The cost of living is rising far faster than (incomes so) an increasing number of Americans are not even able to afford the basics.”
“(B)uy(ing) enough food to eat is becoming a challenge for a lot of people.”
The above are real issues facing most US households, not a flu/covid crisis that does not exist.
Yet Sanders called for increased PCR testing that nearly always produces false results when positive.
He urged increased “production of critical supplies (sic) such as masks, ventilators, and protective equipment for health care workers (sic)” when none of the above is needed.
He wants Pentagon forces used to “build mobile hospitals and testing facilities, assist providers, reopen hospitals that have been shut down and expand our health care capacity in at-risk areas (sic).”
He called for “emergency funding to dramatically expand access to community health centers.”
His prescription for dealing with garden variety flu now called covid ignores reality like the vast majority of other US/Western politicians, bureaucrats, and their press agent media.
Separately, Biden regime propaganda falsely called flu/covid “a global challenge” — that doesn’t exist so US/Western dark forces invented it to pursue their diabolical mass-extermination campaign.
According to Biden’s double, the “US is exercising diplomatic leadership to mobilize an international response to (a nonexistent) crisis and (invented) health-related threats” ahead.
Interventionist Blinken added that the Biden regime is “leading the global response to (a nonexistent) pandemic (with) an arsenal of (toxic health-destroying drugs) for the world.”
Con man Sanders supports the Biden regime’s diabolical agenda.
It includes transforming nations worldwide into ruler-serf societies, along with mass-extermination of unwanted people everywhere.
Resisting tyranny is a universal right.
Now is the time to challenge a diabolical US/Western agenda no one should tolerate before a rubicon of no return is crossed.
July 11, 2021
Posted by aletho |
Deception, Science and Pseudo-Science | Bernie Sanders, COVID-19 Vaccine, United States |
Leave a comment
Covid-19 vaccine propaganda is everywhere, and particularly shrill in the sanctified NHS. Reluctant care workers are given a chance to see the error of their thinking, through a teaching session attended with compliant colleagues. Take for example the webinar Vaccination Myth Busting Session for Care Staff, used for NHS and other health and social care staff in Hertfordshire.
The slides begin with results of an Ipsos MORI poll, which asked ‘how convincing are arguments for taking a coronavirus vaccine?’ Of the several items, ‘to protect other people from catching the coronavirus’ and ‘because it will reduce my risk of catching the coronavirus’ got 77% and 76% support respectively. This use of a public opinion poll is manipulative, enabling the educators to make a point without recourse to scientific evidence. In fact, the vaccines do not prevent infection or transmission. As Peter Doshi explained in the British Medical Journal, trials could only measure mild symptoms, because hospitalisations and deaths were too few for statistical significance.
Also scoring 77% was ‘because vaccines have been very successful against other diseases’. This may be true, but would you agree to take an experimental pill because drugs work for other diseases? Trust in medicine is being exploited. While 66% agreed with the statement ‘because I trust scientists and other medical experts if they say I should take it’, there was also 45% support for following the advice of pharmaceutical companies, and 39% on government recommendation. This is troublingly naïve.
The next slide is on the World Health Organisation’s steps in vaccine development. No mention is made of the need for long-term safety assessment in the trial stages, as would normally be required. Instead, this is left to post-marketing surveillance. Yet the danger of insufficient time for testing was shown by the thalidomide scandal.
The purpose of vaccines is herd immunity, a state that is only reached ‘when most people in a community are vaccinated against a disease’. Naturalistic herd immunity has been conveniently forgotten. According to the slides, ‘vaccines train your immune system using a harmless form of the virus’. Fact check: false. The mRNA type, described in the slides as ‘genetic vaccines’, instructs cells to produce spike proteins. The adenovirus vector type does not use SARS-CoV-2 either, as the virus has never been properly isolated.
‘Single dose is not single dose’ is the illogical title of the next slide. Although there is ‘high efficacy after first dose’, the second dose gives more lasting protection. However, there is clearly not much confidence in immunisation because the webinar instructs staff to ‘behave as if everyone you meet outside your home is infected and you are too’. The status of sick until proven healthy, apparently, persists for the double-jabbed.
Thus everyone should wear face coverings I guess that ‘2 layers min, preferably three’ means the thickness of cloth rather than the number of masks, although Tony Fauci was telling people earlier this year to wear two masks. As with the vaccines, masking is presented as part of a package. Amusingly, a block of Swiss cheese analogises the various interventions: all slices are riddled with holes, but no hole goes through the entire block. None of these are optional: ‘if you want to get out of lockdown, your only real option is compliance’.
The threatening tone continues with the assertion that unvaccinated people will cause new variants to arise, and ‘vaccine escape’. Reference is made to the ‘Green Book’, which makes almost no exceptions to the vaccine regime. Based on advice from the British School for Allergy and Clinical Immunology, anyone who had an anaphylactic shock after a previous jab should be given the Astra Zeneca vaccine rather than Pfizer, and should have half an hour of monitoring afterwards.
The slides were produced before the authorities gave the green light for jabbing pregnant women, but there is little caution: expectant mothers ‘should be reassured that the vaccine does not contain live SARS-CoV-2 virus, and therefore cannot cause COVID-19 infection in her or in her baby’. So that’s all right then. The impact on fertility cannot be known, but the webinar glibly states: ‘current guidance is that the vaccination is safe for women of childbearing age’.
Lastly, the session considers side effects. It is accepted that all drugs can cause adverse reactions in some people. However, the covid-19 vaccine is not a treatment but an experimental intervention on the healthy. Thus the risk-benefit ratio is different from a medicine used to treat illness. The teaching session describes the common side effects of ‘a painful arm, feeling tired, headache, general aches and mild flu-like symptoms’, which disappear over a few days.
Then comes a leap of faith: ‘these symptoms are a sign that your body is building immunity’. Such information may explain why people experiencing adverse reactions say ‘at least I know it’s working’. But the reality is that many vaccine recipients feel very poorly after the jab, as known to healthcare providers due to the high level of staff sickness.
It is unethical and against the principles of the Hippocratic Oath to tell people that adverse reactions are normal. But this seems to be the message of the vaccine regime. A Guardian article this week advised people who are suffering nasty side effects: ‘don’t think of this as a bad sign – it’s exactly what’s expected from an effective but imperfect jab’. In this Orwellian newspeak, harm is safe.
The most egregious economy of truth in this teaching session is on the most serious adverse reaction of all – death. By the time that the slides were produced (27th January), millions of Britons had been jabbed. But this bold claim is made:
‘Nobody has died following having the vaccine in the UK or anywhere else in the world’.
In January covid-19 mortality surged, a pattern seen in most other countries after vaccine rollout. The likely reason is weakened immunity for two or three weeks after the jab. In the frail elderly, recovery of the immune system takes longer, exposing them to infection in the winter peak. This correlation is not proven, but numerous care homes had a spate of covid deaths after all residents were jabbed.
The blood clotting problem was also well known, with several reports of people dying shortly after vaccination. Again, causation has not been fully determined (although belatedly the authorities have added cardiovascular risks to the vaccine marketing information). But why have a Yellow Card system if reported adverse reactions are simply ignored?
The producers and presenters of this misinformation should be held to account. As the ‘no jab, no job’ mandate looms, it is time for professional practitioners to speak out. Indeed, their code of conduct demands they do so.
July 11, 2021
Posted by aletho |
Mainstream Media, Warmongering, Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine, UK |
Leave a comment
I HAD the pleasure of interviewing Dr Robert Malone, an industrial scientist and the authoritative voice on mRNA (messenger ribonucleic acid) technology since he invented it when he was a graduate student at the Salk Institute in 1988.
US-based Dr Malone is not a conspiracy theorist and he’s not an anti-vaxxer. He’s spent the past three decades building vaccines and vaccine technology.
He has more than 20 years of management and leadership experience in academia, pharmaceutical and biotechnology industries, as well as in governmental and non-governmental organisations.
The fact that he is now being ‘ghosted’ for speaking about the adverse effects of the mRNA vaccines reflects the dark era of censorship that we’ve been experiencing for far too long.
Even my interview with him was pulled off YouTube in the space of just three hours. Fortunately, I posted it on alternative video-sharing platforms, such as Rumble and BitChute.
Here are some of the highlights he revealed in the interview. Firstly, Dr Malone stated: ‘In the Security and Exchange Commission filings for both Pfizer and Moderna, there’s explicit statements that acknowledge that these are gene therapy-based (vaccines) and the FDA (Food and Drug Administration) perceives them as such.’
He brilliantly explained the science behind the vaccines by using the metaphor of an industrial robot used to build cars. The RNA in this metaphor is the code that a hacker is inserting into the bit stream to make these robots (your cells) make something they would not have otherwise made. In this case, it’s the spike protein that’s recognised by the immune system triggering a response.
‘In a conventional vaccine you can precisely calculate how much protein goes into your shoulder because it’s fixed and predictable, but in the case of these genetic vaccines you can’t,’ he warned.
‘You can’t calculate how long it produces this protein and how much protein it makes and exactly what cells in your body the protein goes into. Conventional vaccines go around your cell, but for these gene therapy-based vaccines the target is your cell.’
When I asked whether he thought the UK (which was the first country in the world to approve the Pfizer vaccine on December 2, 2020) rushed through their approval of it, Dr Malone quickly responded: ‘I wouldn’t say maybe, I would say they did. You can’t take a process that normally takes a decade and push it down into nine months and not cut corners.’
He explained that regulatory agencies such as America’s FDA and Britain’s MHRA (Medicines and Healthcare products Regulatory Agency) have different safety check lists for vaccines and gene therapies. Typically, genotoxicity and reproductive toxicity studies are not done with vaccines, but are done with gene therapy products.
Dr Malone revealed that in the face of the crisis, apparently there was a global consensus with these regulatory agencies that they were going to suspend their gene therapy checklist, or if they were done, they were not done in a ‘vigorous’ way. He said this was the biggest mistake of the regulatory agencies.
Children are at very low risk of hospitalisation and death from Covid-19, Dr Malone confirmed. In their age group, the risks overwhelmingly outweigh the benefits from the vaccine.
The risks are the cardiotoxicity events (pericarditis and myocarditis) being recorded in the adverse event databases coming out of Israel, Norway and the Netherlands, to name but a few.
Given that the MHRA and FDA have approved the Pfizer vaccine for 12 to 15-year-olds and have been actively encouraging the use of it across multiple age groups, Dr Malone likened this application to the situation where ‘if you give a three-year-old a hammer, everything becomes a nail’.
He talked intently on bioethics and whether it’s ethical to encourage the young (including children) who are currently healthy to take on the responsibility of being exposed to the risks associated with the vaccines in order to protect the vulnerable (the elderly and those with a compromised immune status).
For him, the answer was a categorical, no – it’s not ethical. When I asked him why there’s such a push to get children vaccinated, he answered: ‘A cynic might mention the financial compensation at stake.’
He raised more alarm bells by suggesting there’s bias in the data stating there’s no effect of the vaccine on pregnant women, causing spontaneous abortion. In fact, many of the women in those studies were in the third trimester, where the risk of miscarriage is much lower.
Dr Malone said if you took out the third trimester data and reanalysed it, just looking at those women in the first and second trimester, then the risk of spontaneous abortion jumps to above 50 per cent.
The topic of censorship was raised, as at the time of the interview the doctor had been ‘erased’ from LinkedIn and his full interview with Brett Weinstein and Steve Kirsch had been removed from YouTube.
One of the reasons LinkedIn gave him was because he mentioned that a chairman on the board at Reuters had links to Pfizer.
Dr Malone stressed that Reuters is a member of the Trusted News Initiative, led by the BBC, which was first formed to combat the spread of misinformation during the US presidential election, but now its attention is on combating vaccine misinformation.
Its other members include AFP, CBC/Radio-Canada, the European Broadcasting Union (EBU), Facebook, the Financial Times, First Draft, Google/YouTube, The Hindu, Microsoft , Twitter, and the Wall Street Journal.
Dr Malone warned that ‘the only version of scientific truth that’s allowed to be discussed are those truths endorsed by large bureaucratic public health agencies’. He was very concerned about ‘this integration between Big Tech, government and biopharma’.
On a final note, he raised the insidious question of whether ‘there is a group of people that could be exploiting this window for their own purposes, whether it’s financial, political or power.’ That, he said, would be ‘a huge travesty’.
Here is a link to my full interview with Dr Malone.
July 11, 2021
Posted by aletho |
Full Spectrum Dominance, Science and Pseudo-Science, Timeless or most popular, Video | COVID-19 Vaccine |
Leave a comment
The U.S. CDC released more data today in their Vaccine Adverse Event Reporting System (VAERS), a U.S. Government funded database that tracks injuries and deaths caused by vaccines, and they added more than 2000 deaths following COVID-19 shots over what they reported last week.
Last week they were reporting 6,985 deaths, and this week that number jumped up to 9,048.
This is by far the largest increase of recorded deaths in one week since they started reporting deaths following COVID-19 shots.
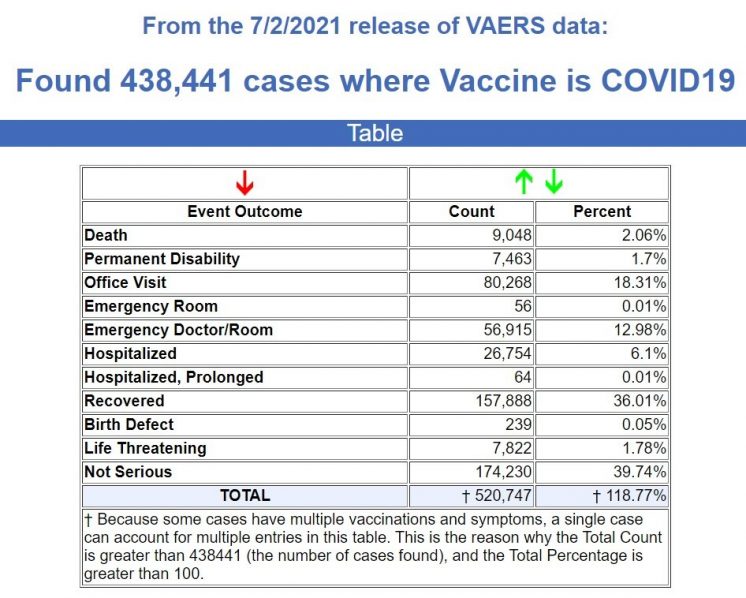
Besides the 9,048 deaths, there are 7,463 permanent disabilities, 56,971 Emergency Room visits, 26,818 Hospitalizations, and 7,822 Life Threatening injuries following the COVID-19 injections.
And yet, none of this government data will be reported in any corporate media news broadcast, and those who try to post it on the Big Tech social media sites will be flagged for “fake news” by the “fact checkers.”
These are not even the true numbers, as the CDC selectively chooses what to release to the public each week, and of course many deaths and injuries go unreported because the public is conditioned to believe that none of these deaths and injuries have anything to do with the COVID-19 shots.
To put this into perspective, there are now 30% more deaths recorded in 7 months since the launch of the COVID-19 shots in December of 2020, than during the entire 31-year history of VAERS recording deaths following vaccines since it started in 1990.
1990 to November 2020: 6,145 deaths following ALL VACCINES. (Source.)
December 2020 to July 2, 2021: 9,048 deaths from COVID-19 shots only. (Source.)
Deaths of Unborn Babies Much Higher than Originally Thought
Last week we reported 622 deaths of unborn children when the pregnant mother received a COVID-19 injection. Using the same search parameters, that number increased to 803 cases this week. (Source.)
However, deaths recorded in the age group of 12-15 have not really increased yet according to the data that the CDC is releasing, so I began to look at the deaths in the “unknown” age group to see if there were some there. I did find a couple, but what I also found was that there were other “symptoms” that the VAERS data uses that do NOT include the term “abortion” when reporting deaths of unborn children in pregnant mothers who took the shots.
So I noted those symptoms, such as “Foetal death, Premature baby death, Stillbirth,” etc., and the deaths increased from 803 to 917. (Source.) And it is very possible I am still missing some, not to mention the ones that never get reported, or if they are reported, are not released by the CDC.
Of the 9,048 deaths the CDC recorded, 3,073 of those deaths are listed as age “unknown.” (Source.)
Trying a few different searches among this “unknown” age group, I did find a 13-year-old boy who died, and a curious entry of an 11-year-old girl who died and where the “family who got vaccinated died along with their dog due to have been being exposed to the members who got vaccinated.”
VAERS ID: 1440065 – Write-up: died three days after Covid vaccination; Autopsy showed enlarged heart and fluid surrounding the heart; Autopsy showed enlarged heart and fluid surrounding the heart; This is a spontaneous report from a contactable consumer or other non-health care professional in response to mail sent regarding the confirmation of below mentioned query. A 13-year-old male patient received second dose of bnt162b2 (PFIZER-BIONTECH COVID-19 mRNA VACCINE, Formulation: Solution for injection, Batch/Lot number and Expiration date not reported) via an unspecified route of administration in an unspecified anatomical location on an unspecified date as single dose for COVID-19 immunisation. The patient medical history and concomitant medications were not reported. The patient previously received first dose of bnt162b2 (PFIZER-BIONTECH COVID-19 mRNA VACCINE, Formulation: Solution for injection, Batch/Lot number and Expiration date not reported) via an unspecified route of administration in an unspecified anatomical location on an unspecified date as single dose for COVID-19 immunisation. On an unspecified date, the patient after receiving his second Covid vaccine from Pfizer died three days later. The patient underwent lab tests and procedures which included autopsy: enlarged heart and fluid surrounding the heart caused by the Covid vaccination. The outcome of the events was fatal. No follow-up attempts are possible; information about lot/batch number cannot be obtained.; Reported Cause(s) of Death: enlarged heart and fluid surrounding the heart.
VAERS ID: 1320319 – Write-up: Girl”s family who got vaccinated died along with their dog due to have been being exposed to the members who got vaccinated; 11 year old, pre-period, girls family who got vaccinated; This is a spontaneous report from a contactable consumer. A 11-years-old patient of an unspecified gender received BNT162B2 (PFIZER-BIONTECH COVID-19 VACCINE), via an unspecified route of administration on an unspecified date (Batch/Lot number was not reported) as single dose for covid-19 immunisation. The patient medical history and concomitant medications were not reported. The reporter reported that 11 year old, pre-period, girls family who got vaccinated died along with their dog due to have been being exposed to the members who got vaccinated. The patient died on an unspecified date. It was not reported if an autopsy was performed. The lot/batch number has been requested; Reported Cause(s) of Death: Girl”s family who got vaccinated died along with their dog due to have been being exposed to the members who got vaccinated.

18-year-old Camilla Canepa died in Italy following the AstraZeneca COVID-19 shot
Neurosurgeon Who Operated on 18-year-old Girl: “I had never seen a brain reduced in those conditions by a thrombosis so extensive and so serious”.
On June 15th this year we published the story of Camilla Canepa, the 18-year-old Italian woman who developed blood clots and was dead two weeks after experimental AstraZeneca shot. The full story was originally published on The COVID Blog.
Her death shocked the community where she lived so much, that a criminal investigation was started, and Italy changed its policy on the AstraZeneca COVID-19 shot limiting it to only people over the age of 60.
The neurosurgeon who operated on her brain has since spoken out, and English translations of what he stated have been circulating through the alternative media this week.
I found an original source from Italy that reported this, and here is the translation, courtesy of DeepL.
The death of Camilla Canepa has shocked the whole of Italy, so much so that after the death of the 18-year-old girl from Sestri Levante as a result of thrombosis emerged a few days after the administration of the vaccine AstraZeneca the Ministry of Health has decided to ban the product against Covid to those under 60 years.
Waiting for the autopsy on the body of the young woman that will be carried out on Tuesday, to speak to La Stampa is Gianluigi Zona, director of the neurosurgical and neurotraumatology clinic of the San Martino Hospital in Genoa: “I had never seen a brain reduced in those conditions by a thrombosis so extensive and so serious”.
“Reasoning in retrospect – explains the doctor on the controversy for the lack of immediate intervention on Camilla – it’s all easy and everyone is a world champion, the last doctor who comes to see a patient is always the smartest.
I can’t judge what could have been picked up already in the first CT scan, it never arrived at San Martino. Normally, if there are no clues that lead to assume something serious is going on, no doctor in the emergency room prescribes a CT scan with contrast or other tests.”
The situation was immediately serious once the operation began: “All the venous sinuses were blocked by thrombi, a scenario that I had never seen in many years of this profession. You have to imagine the venous sinus as the river in the middle of a valley in which several streams converge.
If you build a dam in the middle of the river, the river swells and at that point the tributaries cannot discharge, with the result that the upstream pressure rises. In front of the picture I saw in the head of that girl, it is clear that – concludes the head physician – we are facing something not normal”. (Source.)
July 10, 2021
Posted by aletho |
War Crimes | COVID-19 Vaccine |
Leave a comment
1. COVID-19 vaccination is voluntary research. The COVID-19 public vaccination program operated by the CDC and the FDA is a clinical investigation and under no circumstance can any person receive pressure, coercion, or threat of reprisal on their free choice of participation. Violation of this principle of autonomy by any entity constitutes reckless endangerment with a reasonable expectation of causing personal injury resulting in damages.
2. COVID-19 vaccines do not work well enough. The current COVID-19 vaccines are not sufficiently protective against contracting COVID-19 to support its use beyond the current voluntary participation in the CDC sponsored program. A total of 10,262 SARS-CoV-2 vaccine breakthrough infections had been reported from 46 U.S. states and territories as of April 30, 2021. Among these cases, 6,446 (63%) occurred in females, and the median patient age was 58 years (interquartile range = 40–74 years). Based on preliminary data, 2,725 (27%) vaccine breakthrough infections were asymptomatic, 995 (10%) patients were known to be hospitalized, and 160 (2%) patients died. Among the 995 hospitalized patients, 289 (29%) were asymptomatic or hospitalized for a reason unrelated to COVID-19. The median age of patients who died was 82 years (interquartile range = 71–89 years); 28 (18%) decedents were asymptomatic or died from a cause unrelated to COVID-19. Sequence data were available from 555 (5%) reported cases, 356 (64%) of which were identified as SARS-CoV-2 variants of concern, including B.1.1.7 (199; 56%), B.1.429 (88; 25%), B.1.427 (28; 8%), P.1 (28; 8%), and B.1.351 (13; 4%). None of these variants are encoded in the RNA or DNA of the current COVID-19 vaccines. In response to these numerous reports, the CDC announced on May 1, 2021, that community breakthrough cases would no longer be reported to the public and only those vaccine failure cases requiring hospitalization will be reported, presumably on the CDC website.
3. COVID-19 vaccines have a dangerous mechanism of action. The Pfizer, Moderna, and JNJ vaccines are considered “genetic vaccines” or vaccines produced from gene therapy molecular platforms.[i] [ii] They have a injurious mechanism of action in that they all cause the body to make an uncontrolled quantity of the pathogenic spike protein from the SARS-CoV-2 virus. This is unlike all other vaccines where there is a set amount of antigen or live-attenuated virus. This means for the Pfizer, Moderna, and JNJ vaccines it is not predictable among patients who will produce more or less of the spike protein. The spike protein itself has been demonstrated to injure vital organs such as the brain, heart, lungs, as well as damage blood vessels and directly cause blood clots. Additionally, because these vaccines infect cells within these organs, the generation of spike protein within heart and brain cells in particular, causes the body’s own immune system to attack these organs.
4. There is a burgeoning number of cases of myocarditis or heart inflammation among individuals below age 30 years.[iii] The Centers for Disease Control has held emergency meetings on this issue and the medical community is responding to the crisis and the US FDA has issued a warning on the Pfizer and Moderna vaccines for myocarditis.[iv] It is known that myocarditis causes injury to heart muscle cells and may result in permanent heart damage leading to heart failure, arrhythmias, and cardiac death. Because this risk is not predictable and the early reports may represent just the tip of the iceberg, no individual under age 30 under any set of circumstances should feel any obliged to take this risk with the current genetic vaccines particular the Pfizer and Moderna products.
5. The US FDA has given an update on the JNJ vaccine concerning the risk of cerebral venous sinus thrombosis in women ages 18-48 associated with low platelet counts.[v] Because this risk is not predictable no woman under age 48 under any set of circumstances should feel at all obliged to take this risk with the JNJ vaccine.
6. COVID-19 vaccines are generating record safety reports. In 1990, the Vaccine Adverse Event Reporting Systems (“VAERS”) was established as a national early warning system to detect possible safety problems in U.S. licensed vaccines.[vi] VAERS is a passive reporting system, meaning it relies on individuals to voluntarily send in reports of their experiences to CDC and FDA. VAERS is useful in detecting unusual or unexpected patterns of adverse event reporting that might indicate a possible safety problem with a vaccine. The total safety reports in VAERS all vaccines per year up to 2019 was 16,320. The total safety reports in VAERS for COVID Vaccines alone through June 25, 2021 is 411,931.[vii]
7. People are dying and being hospitalized in record numbers in the days after COVID-19 vaccination. Based on VAERS as of June 25, 2021, there were 6,985 COVID-19 vaccine deaths reported and over 23,257 hospitalizations reported for the COVID-19 vaccines (Pfizer, Moderna, JNJ). By comparison, from 1999, until December 31, 2019, VAERS received 3167 death reports (158 per year) adult death reports for all vaccines combined. Thus, the COVID-19 mass vaccination is associated with at least 39-fold increase annualized vaccine deaths reported to VAERS. COVID-19 vaccine adverse events account for 98% of all vaccine-related AEs from Dec 2020 through present in VAERS.
8. The safety profile is unknown and there is a reasonable expectation for harm for the following groups at all age ranges: COVID-19 recovered, suspected COVID-19 recovered, women of childbearing potential, children, persons with one or more chronic diseases.
9. Any personal choice or protected health information concerning the COVID-19 vaccine and its complications is confidential and anonymous according to federal law, otherwise, you will be subject to additional federal fines and penalties for violation of protected health information laws and statutes.
In conclusion, the investigational, genetic COVID-19 vaccines are not safe for general use and cannot be deployed indiscriminately unless proven otherwise. Please cease and desist pressure/harassment/mandates for COVID-19 vaccination.
References
[i] To KKW, Cho WCS. An overview of rational design of mRNA-based therapeutics and vaccines. Expert Opin Drug Discov. 2021 May 31. doi: 10.1080/17460441.2021.1935859. Epub ahead of print. PMID: 34058918.
[ii] Doerfler W. Adenoviral Vector DNA- and SARS-CoV-2 mRNA-Based Covid-19 Vaccines: Possible Integration into the Human Genome – Are Adenoviral Genes Expressed in Vector-based Vaccines? Virus Res. 2021 Jun 1;302:198466. doi: 10.1016/j.virusres.2021.198466. Epub ahead of print. PMID: 34087261; PMCID: PMC8168329.
[iii] Abu Mouch S, Roguin A, Hellou E, Ishai A, Shoshan U, Mahamid L, Zoabi M, Aisman M, Goldschmid N, Berar Yanay N. Myocarditis following COVID-19 mRNA vaccination. Vaccine. 2021 Jun 29;39(29):3790-3793. doi: 10.1016/j.vaccine.2021.05.087. Epub 2021 May 28. PMID: 34092429; PMCID: PMC8162819.
[iv] https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-june-25-2021
[v] https://www.fda.gov/news-events/press-announcements/joint-cdc-and-fda-statement-johnson-johnson-covid-19-vaccine
[vi]VAERS may be publicly accessed at https://www.openvaers.com/covid-data.
[vii] VAERS may be publicly accessed at https://www.openvaers.com/covid-data (accessed June 25, 2021)
July 10, 2021
Posted by aletho |
Timeless or most popular | Covid-19, COVID-19 Vaccine |
Leave a comment


 Aletho News
Aletho News