COVID QUESTIONERS DEEMED ‘DOMESTIC TERRORISTS’
The Highwire with Del Bigtree | August 3, 2023
A trip down memory lane chronicling how Homeland Security labeled us all ‘domestic terrorists’ for trying to warn people about the harms of the COVID shots, masking kids, warnings and attacks meant to achieve COVID compliance. Will the same op be run during a climate emergency?
How the current version of the WHO’s Pandemic Treaty (aka Bureau Text) encourages rather than prevents pandemics
BY MERYL NASS | AUGUST 5, 2023
Weapons of Mass Destruction: Chem Bio
Traditionally, Weapons of Mass Destruction (WMD) were Chemical, Biological, Radiologic and Nuclear (CBRN).
The people of the world don’t want them used on us—they are cheap ways to kill and maim lots of people at once. And so international treaties were created to try to prevent their development (sometimes) and use. First was the Geneva Protocol of 1925, banning the use of biological and chemical weapons in war. The US and many nations signed it, but it took 50 years for the US to ratify it, so we believed we were not bound by it.
The US used chemical weapons subsequently. The US probably used biological weapons in the Korean War, and perhaps in Vietnam, which experienced an odd outbreak of plague during the war. The use of napalm, white phosphorus, agent orange (with its dioxin excipient causing massive numbers of birth defects and other tragedies) and possibly other chemical weapons led to much pushback, especially since we had signed the Geneva Protocol and we were supposed to be a civilized nation.
In 1968, a young Seymour Hersh wrote a book about the US chemical and biological warfare program. In 1969 Congressman Richard D. McCarthy wrote the book “Ultimate Folly” about the US production and use of chemical and biological weapons. Prof. Matthew Meselson’s review of the book noted,
Our operation, “Flying Ranch Hand, ” has sprayed anti-plant chemi-
cals over an area almost the size of the state of Massachusetts, over
10 per cent of it cropland. “Ranch Hand” no longer has much to do with
the official justification of preventing ambush. Rather, it has become
a kind of environmental warfare, devastating vast tracts of forest in
order to facilitate our aerial reconnaisance. Our use of “super tear
gas” (it is also a powerful lung irritant) has escalated from the originally
announced purpose of saving lives in “riot control-like situations” to the
full-scale combat use of gas artillery shells, gas rockets and gas bombs
to enhance the killing power of conventional high explosive and flame
weapons. Fourteen million pounds have been used thus far, enough
to cover all of Vietnam with a field effective concentration. Many
nations, including some of our own allies have expressed the opinion
that this kind of gas warfare violates the Geneva Protocol, a view
shared by M cCarthy.
A Biological Weapons Convention
Amid great pushback over US conduct in Vietnam, in November 1969 President Nixon announced to the world we were going to end the US biowarfare program (but not the chemical program). In February 1970 Nixon announced we would also get rid of our toxin weapons (snake, snail, frog, fish, bacterial and fungal toxins that could be used for assassinations, etc.). Furthermore, Nixon said the US would initiate an international treaty to prevent the use of these weapons ever again. And we did: the 1972 Convention on the prohibition of the development, production and stockpiling of bacteriological (biological) and toxin weapons and on their destruction, or Biological Weapons Convention (BWC) for short, which entered into force in 1975.
The BWC established conferences to be held every 5 years to strengthen the Convention. The expectation was that these would add a method to call for ‘challenge inspections’ to prevent cheating and would add sanctions (punishments) if nations did not comply with the treaty. However, the US has consistently blocked the addition of protocols that would have an impact on cheating. By now, everyone knows that cheating occurs and is likely widespread.
A leak in an anthrax production facility in Sverdlovsk, USSR in 1979 caused the deaths of about 60 people. A clear BWC violation. US experiments with anthrax production during the Clinton administration, detailed by Judith Miller et al. in the 2001 book Germs were also thought by experts to have transgressed the BWC.
In 1997 a Chemical Weapons Convention came into force. It took over 20 years, but all official stocks of chemical weapons have been destroyed by the USA and by Russia and the other 193 member nation signatories.
Pandemics or Biological Warfare?
So here we are. It is 2023 and the WHO Director General has declared 2 pandemics (the current terminology is ‘Public Health Emergency of International Concern’) over the past 3 and a half years: COVID-19 and monkeypox, which was renamed MPOX to “avoid stigma.” I am sure the monkeys were relieved by the name change.
I have previously (in my substack) described why I believe both SARS-CoV-2 and MPOX were bioengineered pathogens that came from labs. I do not know if they leaked or were deliberately released, but I am leaning toward deliberately released for both of them, based on where they appeared, how they spread, and in particular the official responses to each—neither of which was explained accurately to the public, and yet we never changed course, even when the lack of efficacy with masks, social distancing, EUA drugs and vaccines had become clear.
Vaccines: the Chicken or the Egg?
Both the monkeypox vaccines (there are two, Jynneos and ACAM2000) are known to cause myocarditis, as do the two COVID-19 mRNA vaccines and the Novavax vaccine. The Novavax vaccine was first associated with myocarditis during its clinical trial in Australia. I have written about all this previously on substack.
How frequently does myocarditis occur after these vaccines? If you use elevated cardiac enzymes as your marker, ACAM2000 caused this in one in thirty people receiving it for the first time. If you use other measures like abnormal cardiac MRI or echo, according to the CDC it occurs in one in 175 vaccinees. We do not know the number for Jynneos, but there was some degree of elevation of cardiac enzymes in 10% and 18% of recipients in two small prelicensure studies. My guess for the mRNA vaccines is that they are somewhere in this range. I don’t know about Novavax’ vaccine.
Why would our governments push 5 separate vaccines all known to cause myocarditis on young males who have been at extremely low risk from COVID, and who simply get a few pimples for 1-4 weeks from monkeypox unless they are immunocompromised? It’s an important question. It does not make medical sense. Especially when the vaccine probably does not work — Jynneos didn’t on the monkeys in whom it was tested. And CDC has clammed up about the 2,000 Congolese healthcare workers on whom CDC tested it for efficacy and safety in 2017. (I have detailed this too in earlier substacks.)
The health authorities could have just been ignorant—that could explain the first 8 months of the COVID vaccines’ rollout. But once they figured out, and even announced in August 2021 that the vaccines did not prevent catching COVID or transmitting it, why did they still push it on low risk populations who were clearly at greater risk from a vaccine side effect?
Once this is acknowledged, you realize that maybe the vaccines were not made for the pandemic, and instead the pandemic was made to roll out the vaccines. I’m not sure. But I’m suspicious. And the fact that multiple countries contracted for 10 doses per person makes me even more suspicious—for vaccines whose safety and efficacy had not been established. WHY would you want ten doses apiece? Three maybe. But ten?
Furthermore, you don’t need a vaccine passport aka digital ID aka justification to convert to all-electronic money unless you are giving out regular boosters. Were the vaccines conceived of as the pathway to getting our vaccinations, health records, official documents and financial transactions all online—as Ukraine has already done?
A Pandemic Treaty and Amendments: Brought to you by the same people who mismanaged the past 3 years, to save us from themselves?
The same US government and western governments that imposed draconian measures on their citizens to force us to be vaccinated and take dangerous, expensive, experimental drugs and withheld the good drugs, decided in 2021 we needed a pandemic treaty to prevent and ameliorate future pandemics or biological warfare events… so we would not suffer as we did with the COVID pandemic.
Except COVID was a disaster due to its mismanagement (or should I say dismanagement or malmanagement?) by our nations’ rulers, their bosses and the WHO. Hundreds of millions of our fellow human being were slammed into extreme poverty—by nations following guidelines issued by the WHO, whose main job it was to protect exactly those people. Tens of millions died from starvation as a result. Yet the WHO blathers on about equity, diversity and solidarity—having itself caused the worst (manmade) food crisis in our lifetimes. Have you heard any apology or explanation?
How can anyone with a brain believe the public health officials who messed up COVID so badly want to spare us from another medical and economic disaster, after they imposed the last one on us? And the fact that no governments or health officials will admit their mistakes — especially how they made it nearly impossible to obtain the cheap and safe drugs that effectively treat COVID — why would we let them plan anything, let alone an international treaty that will bind our governments to obey the WHO’s dictates? How thoughtful of these officials to want to spend a king’s ransom of our money to prevent the next government-caused disaster.
We are fed up with secret vaccine contracts, waivers of liability for junk medical products, and spikes in sudden deaths and chronic disabilities. No more secret negotiations. Please shove your pandemic planning where the sun…
The Gain of Function farce
Obviously, the best way to spare us from another pandemic is to immediately stop funding “Gain of Function”* research, and get rid of what has already been funded and created. Let all the nations make big bonfires and burn up their evil creations at the same time, while allowing other nations to inspect their biological facilities and records.
But the WHO in its Bureau Text of the draft Pandemic Treaty has a plan that is the exact opposite of this. In the WHO’s world, which almost all nations’ rulers have bought into, all the governments will share any and all viruses and bacteria they come up with that have “pandemic potential” — share them with all the other governments. They are supposed to sequence them and then put the sequence online. No kidding. Then the WHO and all the Faucis of the world would gain access to every Frankenstein virus, at once. Presumably a bunch of hackers would also gain access to the sequences. Does this make you feel more secure?
The WHO Treaty draft incentivizes Gain Of Function research
At least this plan makes clear whose side everyone is on. Fauci, Tedros and their ilk at the WHO, and those managing biodefense and biomedical research for nation states are on one side, the side that gains access to even more biological weapons, and the rest of us are on the other, at their mercy.
This crazy plan used to be called proliferation of weapons of mass destruction—and it is almost certainly illegal. But it is their plan. Governments will all share the weapons. And they are to put a lot more money into biolabs, and especially into genomic sequencing. Presumably so they can make even better weapons, and maybe they will even get around to cures or antidotes. But who will get the cures? It wasn’t us during the COVID-19 pandemic. Here is where you can read the current Treaty draft:
https://apps.who.int/gb/inb/pdf_files/inb5/A_INB5_6-en.pdf
Pages 10 and 11:




What else is in the Treaty? Gain of Function research (designed to make pathogens more transmissible or more virulent) is explicitly incentivized. Administrative hurdles to it must be minimized, while unintended consequences (pandemics) should be prevented: (page 14)

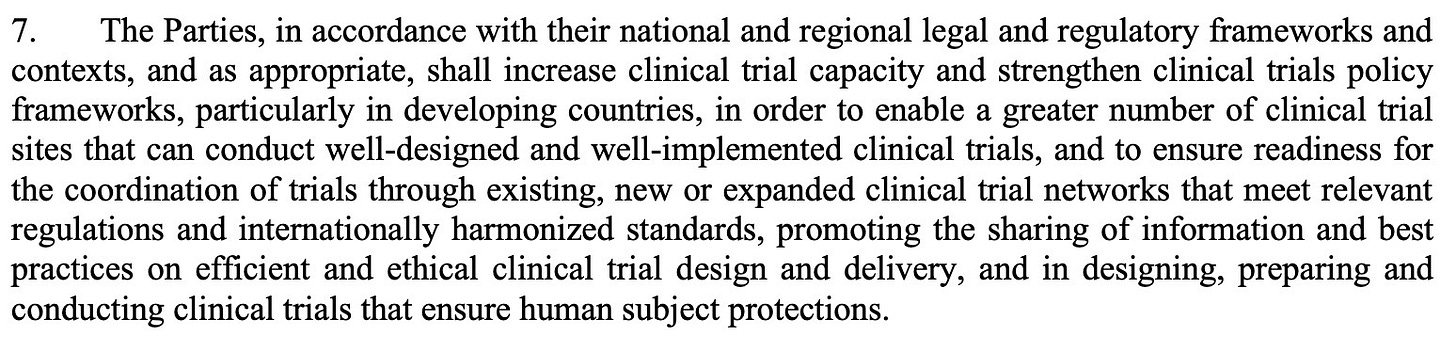
Vaccines will be rolled out speedily under future testing protocols
Just in case you thought the COVID vaccines took too long to be rolled out, the WHO has plans to shorten testing. There will be new clinical trial platforms. Nations must increase clinical trial capacity. (Might that mean mandating people to be human subjects in out-of-the-way Africa, for example?). And there will be new “mechanisms to facilitate the rapid interpretation of data from clinical trials” as well as “strategies for managing liability risks.” (page 14)
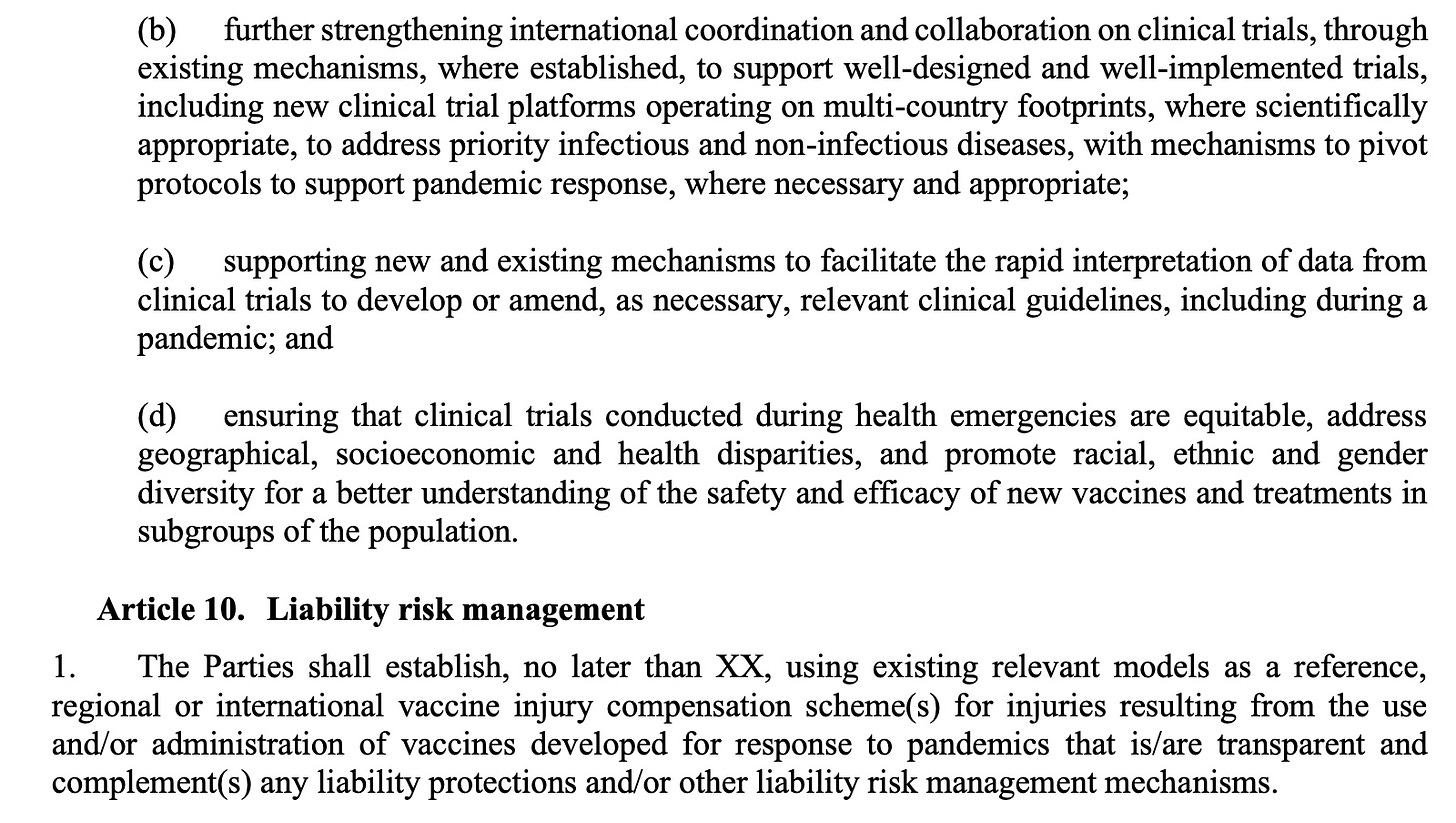
Manufacturer and government liability will be “managed”
Nations are supposed to use existing models as a reference for compensation of injuries due to pandemic vaccines. Of course, most countries do not have vaccine injury compensation schemes, and when they do the benefits are usually minimal. The US government scheme for injuries due to COVID pandemic products (the Countermeasures Injury Compensation Program or CICP) has compensated 4 (yes, FOUR) people as of July 1, 2023. All pandemic EUA drugs and vaccines fall into this program (monoclonal antibodies, early remdesivir, paxlovid, molnupiravir, some ventilators and all COVID vaccines). There have been nearly 12,000 claims made to the CICP related to a COVID product. Slightly over 1,000 have been adjudicated while 10,886 are pending review. Twenty claims were deemed eligible and are waiting to see whether they can collect. A total of 983 people, or 98% had their claims denied. About 90% of all claimants filed for a vaccine injury.

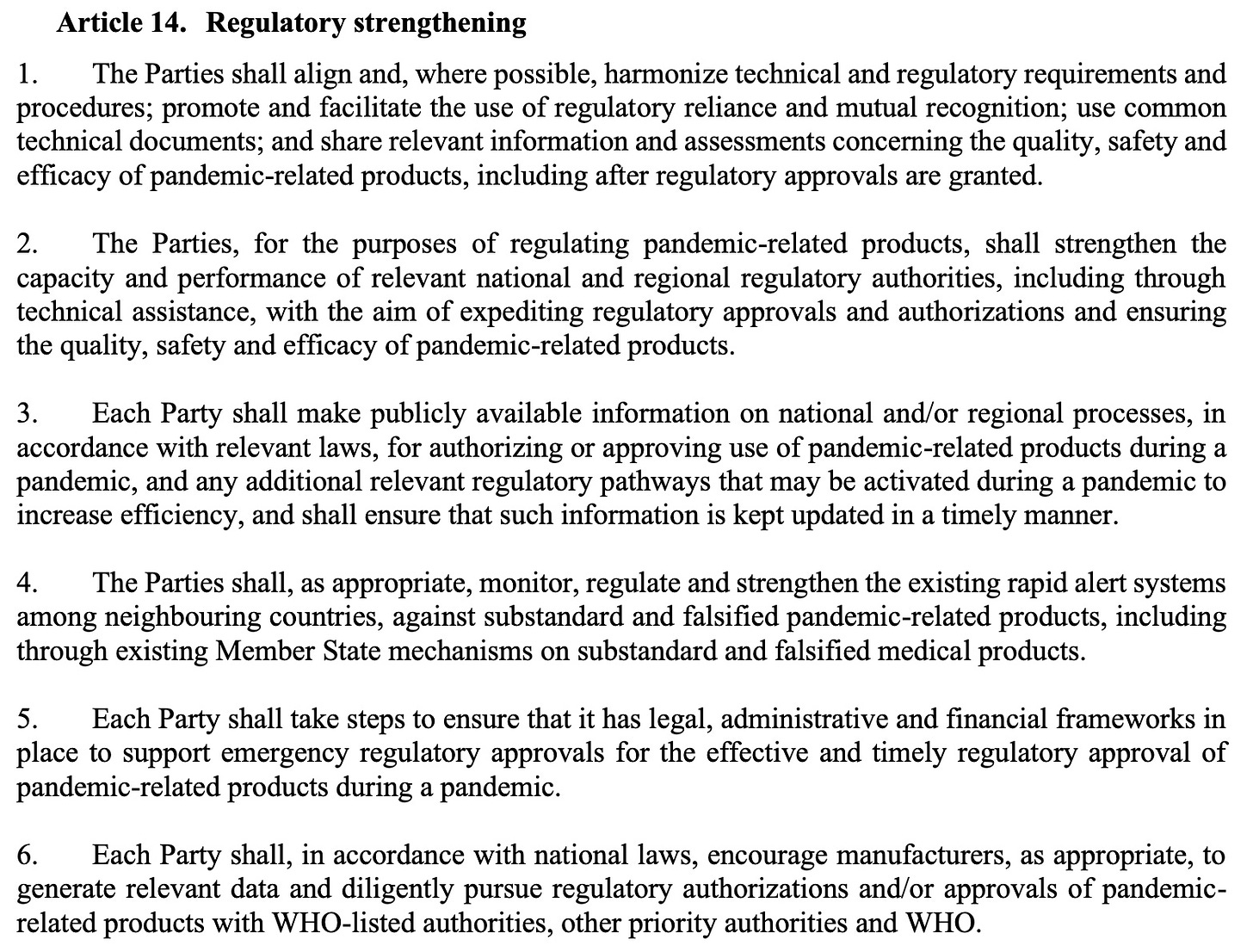
The treaty draft also demands weakening the regulation of medical drugs and vaccines during emergencies under the rubric of Regulatory Strengthening. As announced in the UK last week, where ‘trusted partner’ approvals will be used to speed licensure, this is moving toward a single regulatory agency approval or authorization, to be immediately adopted by other nations (p 25)
Why would any developed country sign up for this? Is this what we the people want?
The WHO did sweeten the pot, however. Remember how the need to respect “human rights, dignity, and freedom of persons” was removed in the WHO’s draft IHR Amendments that are being negotiated? Well, WHO apparently did not like us pointing that out—so the old human rights language that was removed from the International Health Regulations draft has been added to this newest version of the Treaty.
There is much more I could say about problems with this draft of the Treaty, but I will save them for another time.
Please share this brief analysis of the WHO’s Pandemic Treaty. We must EXIT the WHO.
*Gain of Function is a euphemism for biological warfare reserch or germ warfare research. It is so foolhardy that it was banned in the US for SARS coronaviruses and avian flu viruses from 2014-2017 due to public outcry by scientists. Then in 2017 Fauci and Collins lifted the moratorium, claimed they were putting safeguards in place, which were just a handwaving exercise, and off we were to the races: creating new bioweapons. Fauci and Collins had the nerve to publish their opinion that the risk was ‘worth it.’
PSYOP-19 UPDATE: New Variant Spreading Across UK – As Overall Cases Continue to Rise
2nd Smartest Guy in the World | August 5, 2023
The followup “pandemic” trial balloon intended to gauge the level of future societal “mandate” compliance has now been officially deployed.
According to the latest Mockingbird article by SKY NEWS entitled, COVID-19: New variant spreading across UK – as overall cases continue to rise:
A new COVID variant is spreading across the UK, according to the UK Health Security Agency (UKHSA) – and already makes up one in seven new cases.
Scientifically known as EG.5.1, it is descended from the Omicron variant of COVID.
The UKHSA has been monitoring its prevalence in the country due to increasing cases internationally, particularly in Asia, and it was classified as a variant here on 31 July.
Since viruses never mutate into more virulent strains, we must ask: is this another gain of function (GoF) release by the usual Intelligence Industrial Complex criminals, and their useful idiot “expert” apparatchiks ahead of the fall and winter flu season, or is this a consequence of the “vaccinated” genetically modified humans incubating and transmitting new viral mutations as a function of the Modified mRNA slow kill bioweapon injections?
In the week beginning 10 July, one in nine cases were down to the variant.
The latest data suggests it now accounts for 14.6% of cases – the second most prevalent in the UK.
It appears to be spreading quickly and could be one reason why there has been a recent rise in cases and hospitalisations.
COVID-19 rates have continued to increase – up from 3.7% of 4,403 respiratory cases last week to 5.4% of 4,396 this week.
The latest data also shows the COVID-19 hospital admission rate was 1.97 per 100,000 population, an increase from 1.17 per 100,000 in the previous UKHSA report.
Officials say they are “closely” monitoring the situation as COVID case rates continue to rise.
It is no surprise that the wholly fraudulent PCR tests are what these “officials” are yet again referencing; in other words, they are up to their same old junk science tricks.
“We have also seen a small rise in hospital admission rates in most age groups, particularly among the elderly,” said Dr Mary Ramsay, head of immunisation at the UKHSA.
“Overall levels of admission still remain extremely low and we are not currently seeing a similar increase in ICU admissions.
“We will continue to monitor these rates closely.”
Senicide is the gift that keeps on giving, as said “officials” happily discharge liabilities and assets of the elderly useless eaters. Any eugenics program worth it’s salt always commences with the oldsters, and then works it way across ever larger swaths of society.
The Arcturus XBB.1.16 variant – another descendant of Omicron – is the most dominant, UKHSA figures show. It makes up 39.4% of all cases.
Another variant with a menacing name and lots of decimals, another opportunity for the One World Government’s main eugenics node in the WHO to fear-monger:
The World Health Organisation (WHO) started tracking the EG.5.1 variant just over two weeks ago.
As this Substack has exposed on several occasions now, the WHO’s director-general is a Marxist war criminal deliberately selected for his extreme sociopathy by the Rockefeller Crime Syndicate’s most prominent puppet and genocidal frankenmosquito advocate Billy Boy Gates:
WHO director-general Tedros Adhanom Ghebreyesus said though people are better protected by vaccines and prior infection, countries should not let down their guard.
“WHO continues to advise people at high risk to wear a mask in crowded places, to get boosters when recommended, and to ensure adequate ventilation indoors,” he said.
They also just can’t let up on the absurdly useless MK Ultra masks, because ensuring that the genetically ruined slaves reinforce their mass induced fear slavery is an effective means of self-policing into ever more mindless compliance.
“And we urge governments to maintain and not dismantle the systems they built for COVID-19.”
Of course, the WHO urges that their unconstitutional and anti-human systems for PSYOP-19 not to be dismantled because they need their said systems for their followup PSYOP-23 “pandemic” this fall.
What the WHO certainly does not want you to know is that inexpensive repurposed drugs will act as prophylaxis against all of their “pandemics,” along with the associated plethora of their “vaccine” induced adverse events like turbo cancers, and prion-based diseases, all while also protecting the genetically unmodified refuseniks from “vaccine” shedding, and environmental damage.
Do NOT comply.
Belgian Defender is Second Brighton Player to Retire With Heart Problems in Last Year

BY ROBERT KOGON | THE DAILY SCEPTIC | AUGUST 3, 2023
The 22-year-old Belgian defender Lars Dendoncker announced last week that he was retiring from football due to a heart condition, thus making him the second Brighton player to retire because of heart problems in less than a year.
Dendoncker, the younger brother of Leander Dendoncker of Aston Villa and the Belgian national team, announced his retirement on Instagram, saying “this was and will be the hardest decision ever in my life” and that it “really hurts”. He was signed by Brighton & Hove Albion on a two-year contract in 2020 and played for the Scottish side St Johnstone for a year on loan.
Although Dendoncker has only now made his retirement official, he in fact already stopped playing football over a year ago after being diagnosed with myocarditis. In an Instagram post from last December, he wrote:
I have been through tough times the past few months. Six months ago I was about to make a transfer to a new club. I did my medical and something wasn’t right with my heart condition. I suffered from myocarditis.
Six months earlier will have been in May, not long before the unfortunate Dendoncker’s contract with Brighton was set to expire.
Last October, the Brighton midfielder Enock Mwepu was also forced into retirement by a heart condition. At the time, the condition was described as congenital. But when Mwepu first started feeling unwell and was rushed to the hospital just two weeks earlier while on a trip to Mali, the problem did not sound congenital. Thus, in his own September 26th Instagram post, he noted cryptically that doctors, and presumably he himself, were not at liberty to disclose the details of “what really happened”.
Mwepu’s words are reminiscent of remarks made by the American basketball player Brandon Goodwin. In mid-2021, while playing for the Atlanta Hawks of the NBA, Goodwin fell ill after being vaccinated against COVID-19 and was subsequently diagnosed with blood clots.
Goodwin himself attributed his condition “1000%” to the vaccine. But in a Twitch video, he described how while in the hospital a team official told him “Don’t say anything about it, don’t tell anyone” – to which he responded, “Bruh, what?” (The video appears to have been removed from Goodwin’s Twitch account, but relevant excerpts are still available on the Daily Caller here.)
Brighton is not the only major football club to have had multiple players stricken by cardiac problems in the last two years. So too did German powerhouse Bayern Munich, though the Bayern players have since returned to action: French winger Kinsley Coman after undergoing heart surgery in September 2021 and Canadian defender Alphonso Davies after being diagnosed with myocarditis in January 2022.
Robert Kogon is a pen name for a widely-published financial journalist, translator and researcher working in Europe. Subscribe to his Substack and follow him on Twitter.
Understanding Your Rights and Responsibilities in Childhood Vaccination: A Guide for Parents
Are vaccines required for your child to attend school?

Photo by Daiga Ellaby on Unsplash
BY PAUL THOMAS MD (RETIRED) | AUGUST 3, 2023
With summer winding down and schools about to open, parents around the country (USA) have received or will receive letters of exclusion from their child’s school. The letter will state that your child is required to be up to date on their childhood immunizations according to the CDC, or they will not be allowed to attend school.
You are not told that other than a handful of states that have eliminated both the religious and the philosophical exemptions, you are free to do whatever you believe is best for your child. You can do some, all, or none of the childhood vaccines. Each state may have a different form or process but rest assured; it is the law of your state that you have this right; the freedom to choose.
To learn more about the specifics for your state, NVIC (National Vaccine Information Center) https://www.nvic.org has all the information you need.
If you live in California, New York, West Virginia, Maine, and possibly Mississippi, the only exemption allowed is a medical exemption. All states allow medical exemptions, which is where a doctor writes a medical exemption.
The challenge for doctors is that the states only allow medical exemptions according to the CDC guidelines, which means you can only get exemptions for a vaccine that has caused death or a severe anaphylactic reaction. They essentially don’t allow exemptions for all vaccines. More importantly, doctors who write medical exemptions invite an investigation by their state medical board and risk losing their medical license. This has made medical exemptions something, in theory, one could hope to get, but in reality, and practically speaking, medical exemptions no longer exist.
So, what do you do if you live in one of the states that only allow medical exemptions?
Basically, you either must get your child up to date, home school, or leave the state for one that allows religious or philosophical exemptions. If you feel you have no choice but to get your child up to date, I highly recommend that you consult a medical provider to help you figure out the safest way to do this.
I am available for coaching at https://www.kidsfirst4ever.com. I don’t diagnose or treat as I am retired and relinquished my license.
Parents and guardians, there is nothing more important in your role to nurture and protect your children than how you handle the vaccine situation. There is no one size fits all that makes sense. Each vaccine should be looked at individually, and you should determine if it makes sense for your child, given the prevalence of the disease for which there is a vaccine and the risks and benefits of giving the vaccine or not giving the vaccine.
Number of Vaccine Doses During Neonatal Period and Infancy and Mortality in Children at 1 and 5 Years
Ecological Analysis Suggests Worldwide Mass Vaccination for Childhood Illnesses Could be Backfiring
By Peter A. McCullough, MD, MPH | Courageous Discourse | August 3, 2023
When ACIP panel added the experimental mRNA vaccines for infants age 6 months and older, it triggered concerns that ACIP may not have ever had adequate intent for risk mitigation or re-evaluation of the ever expanding vaccine schedule. Many have had reservations for a long time and have felt drowned out by the medical orthodoxy of “more vaccines are better.” Now an analysis by Miller, et al, suggests the entire program of hyper vaccination may be backfiring.
The two main independent variables in this analysis restricted to developed countries at two time points 2019 and 2021 (check for internal validity) were the number of vaccines given in the 28 day neonatal period (none, hepatitis B, Bacille Calmette-Guérin (BCG) for tuberculosis) and then the overall number of shots given before age 1 year. The outcome variable was all cause mortality at age 1 and 5 years.
As you can see this does not look good for vaccines. In every analysis the children who went “natural” with no shots did the best and there was a trend for the fewest number of injections to be associated with the lowest mortality. I was born in 1962, so I received zero shots in the neonatal period and a total of 6 doses for four diseases (diphtheria, tetanus, pertussis, polio) before the age of 1 years. As you can see the optimal number of infant doses in the vaccine schedule is <14. The current US ACIP schedule is ~23 doses by year one—a proxy for national intent for hyper vaccination.

This paper has all the limitations of an ecological analysis where individual child record information is not available. The exact configuration of specific vaccines and causes of death are not specified. Thus we can only conclude from this study that “less is more” and countries should consider a risk stratified approach. The two main neonatal vaccines, hepatitis B and BCG should be reconsidered altogether according to individual risk of hepatitis B and tuberculosis, respectively.
Do The COVID Vaccines Affect Your Ability to Think?
Examining some of the common neurological injuries caused by vaccination
A Midwestern Doctor | The Forgotten Side of Medicine | July 20, 2023
When the COVID-19 vaccines were brought to market, due to their design I expected them to have safety issues, and I expected over the long term, a variety of chronic issues would be linked to them. This was because there were a variety of reasons to suspect they would cause autoimmune disorders, fertility issues and cancers—but for some reason (as shown by the Pfizer EMA leaks), the vaccines had been exempted from being appropriately tested for any of these issues prior to being given to humans.
Since all new drugs are required to receive that testing, I interpreted it to be a tacit admission it was known major issues would emerge in these areas, and that a decision was made that it was better to just not officially test any of them so there would be no data to show Pfizer knew the problems would develop. Sadly, since the time the vaccines entered the market, those three issues (especially autoimmunity) have become some of the most common severe events associated with the vaccines.
At the start of the vaccine rollout, there were four red flags to me:
• The early advertising campaigns for the vaccines mentioned that you would feel awful when you got the vaccine, but that was fine and a sign the vaccine was working. Even with vaccines that had a very high rate of adverse events (e.g., the HPV vaccine), I had never seen this mentioned. This signified it was likely the adverse event rate with the spike protein vaccines would be much higher than normal.
• Many of my colleagues who got the vaccine (since they were healthcare workers they were able to get it first) posted on social media about just how awful they felt after getting the vaccine. This was also something I had never seen with a previous vaccine. After some digging, I noticed those with the worse vaccine reactions typically had already had COVID and their reaction was to the second shot rather than the first, signifying that some type of increased sensitization was occurring from repeated exposures to the spike protein. Likewise, the published clinical trial about Pfizer’s vaccine also showed adverse reactions were dramatically higher with the second rather than first shot.
• Once it became available to the general public, I immediately had patients start showing up with vaccine reactions, many of whom stated they received their flu shot each year and never had experienced something similar with a previous vaccination. One of the most concerning things were the pre-exacerbation of autoimmune diseases (e.g., spots in their body they previously would occasionally have arthritis and felt like they were on fire). After I started looking into this I realized people were seeing between a 15-25% rate of new autoimmune disorders or exacerbations of existing autoimmune disorders developing after the vaccine (later shown in an Israeli survey), a massive increase I had never seen any previous vaccine cause.
• About a month after the vaccines were available to the public, I started having friends and patients share that they’d known someone who had unexpectedly died suddenly after receiving the vaccine (typically from a heart attack, stroke, or a sudden aggressive case of COVID-19).
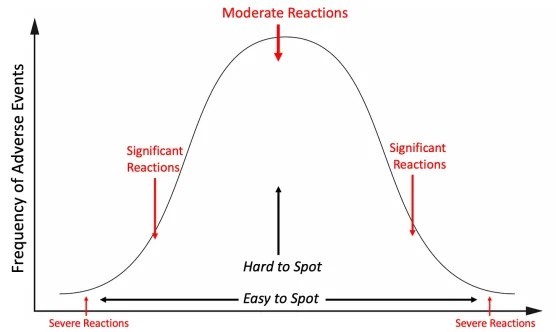
This was extremely concerning to me, because reactions to a toxin typically distribute on a bell curve, with the severe ones being much rarer than the moderate ones. This meant that if that many severe reactions were occurring, what I could already see was only the tip of the iceberg and far, far more less obvious reactions were going to be happening, to the point it was likely many people I knew would end up experiencing complications from the vaccine.
I tried to warn my colleagues about the dangers of this vaccine, but even when I pointed out Pfizer’s own trial admitted the vaccine was more likely to harm than help you, no one would listen to me. Not being sure what else to do, but not be willing to do nothing, I decided to start documenting all the severe reactions I came across so I could have some type of “proof” to show my colleagues.
This was something that was extremely important at the time since no one was willing to take on the personal risk of publishing something went against the narrative (that vaccines were killing people) in the peer reviewed literature. Shortly after Steve Kirsch kindly helped launch my Substack, I decided to post the log I’d put together, and since there was a critical need for that information, the post went viral and created much of the initial reader base that made my substack possible.
It was immensely time consuming to do the project (especially the verification of the story that was reported to me), so I ended the project after a year. During that time, I came across 45 cases of either a death (these comprised the majority of the 45 cases), something I expected to be fatal later on (e.g., a metastatic cancer) or a permanent and total disability. Additionally, in line with the previously described bell curve, I also came across many more serious but not quite as severe injuries.
I’ve had a long term interest in studying pharmaceutical injuries because many of my friends and relatives have had bad reactions to pharmaceuticals. In most of these cases, ample data existed to show that reaction could happen (often to the degree it strongly argued against the pharmaceutical remaining on the market) and yet almost no one in the medical field was aware of those dangers, hence leading to my injured friends never being warned before they took the pharmaceutical or even while the injury was occurring.
My bell curve theory originally came about from examining all of their cases. I thus was interested to know if the distribution of adverse events from the spike protein vaccines would match what I had observed with previous dangerous pharmaceuticals and if what I saw personally did or did not match what everyone was reporting online.
One of the things that immediately jumped out at me were the multiple cases of a friend’s parent in a nursing home receiving the vaccine, immediately undergoing a rapid cognitive decline which was “diagnosed” as Alzheimer’s disease and then dying not long after. At the time, I assumed these were most likely due to undiagnosed ischemic strokes as that was the most plausible mechanism to describe what I’d heard, but I was not certain as I could never examine any of these individuals for signs a stroke had indeed happened.
These cases were very concerning to me, as they signified (per the bell curve) that there was going to be a much larger portion of people who would develop less severe (but nonetheless impactful) cognitive decline following vaccination.
Note: one of the most common types of injuries from pharmaceuticals are neurological injuries which both impair cognitive function and create psychiatric symptoms. This places patients in a difficult situation of being gaslighted by the medical system. This is because their doctors assume the psychiatric symptoms the patients are experiencing are the cause of their illness rather than a symptom of it, leading to the patient being told the illness is all in their head and continually referred for psychiatric help. One of the best examples with this occurred as a result of the abnormal heart rhythms (e.g., rapid anxiety provoking palpitations) caused by the vaccine damaging the heart which were consistently diagnosed as being a result of anxiety, even when a subsequent workup I requested showed heart damage was present.
As I began seeing more and more signs of cognitive impairment following vaccination, I realized that what I observed mirrored what I had previously seen with chronic inflammatory conditions such as mold toxicity, HPV vaccine injuries, and lyme disease. Some of the examples included:
• Many people reported having a “COVID” brain where it was just harder for them to think and remember things. I sometimes saw this after more severe cases of COVID, more frequently after vaccination, and repeatedly in patients who per their timeline clearly developed it from the vaccine but believed it had come from COVID.
• These issues tended to be more likely to affect older adults, but younger ones were more likely to notice (and complain) about them. In the case of older adults, I typically learned about them from someone else who had observed the cognitive decline rather than directly from the individual.
• I saw cases of vaccine injured individuals who had trouble remembering or recalling the word they knew expressed what they were trying to communicate (this is also a common mold toxicity symptom).
• I had friends and patients who told me their brain just didn’t work the same since they’d received the vaccine. As an example, a few colleagues told me they started losing the ability to remember basic things they needed to practice medicine (e.g., medication dosages for prescriptions). They shared that they were very worried they would need to take an early retirement and that they thought it came from the vaccine but there was no one they could talk to about it (which understandably created a lot of doubt and anxiety).
• I saw cases of coworkers demonstrating noticeable (and permanent) cognitive impairment after I’d assumed they’d received the vaccine. Their impairment was never mentioned or addressed (rather the physician kept on working, did not perform as well, and in some cases retired).
• I met significantly injured vaccine injured patients who told me one of the primary symptoms was a loss of cognitive functioning they had taken for granted throughout their life. In many cases following treatment of their vaccine injury, their cognition also improved.
• Colleagues who treated vaccine injured patients told me cognitive impairment was one of the common symptoms they saw and was particularly noteworthy because they had never seen anything like that happen to young adults.
• One of my friends (a very smart immunologist) developed complications from the first two vaccines and based on their symptoms was able to describe exactly which parts of their immune systems were becoming dysregulated. Against my advice, they took a booster and reported they suffered a significant cognitive impairment never experienced before in their lifetime. I feel this case was important to share as it illustrates how an exacerbation of a vaccine injury can also cause an exacerbation of cognitive symptoms.
Note: I also saw significant cognitive impairment occur in individuals who were acutely ill with COVID-19. This was not as unusual since delirium is a well known complication in patients hospitalized with a systemic illness (e.g., sepsis), but it seemed to happen more frequently than ususual.
At the same time I was observing these effects, many rumors were also swirling around online that the vaccines would cause severe cognitive impairment and that we would witness a zombie apocalypse from the vaccine injuries.
This apocalypse of course never happened, but many observed a suspicion cognitive impairment was occurring. For example to quote Igor Chudov’s recent article:
I own a small business and deal with many people and other small businesses. Most provided reliable service, would remember appointments, followed up on issues, and so on. I noticed that lately, some people have become less capable cognitively. They forget essential appointments, cannot concentrate, make crazy-stupid mistakes, and so on.
In my own case, the most evident change I noticed was a worsening of drivers around me and had a few near misses from impaired driving.
The challenge with these situations is that it’s very hard to tell if something is actually happening or your perception is simply a product of confirmation bias. For this reason, while I was comfortable asserting my belief the COVID-19 vaccines were causing the severe injuries on either end of the bell curve, I avoided doing so for many of the less impactful injuries in the middle where it was much more ambiguous if what I was observing was “real” or simply my own biased perception of the events around me. Because of this, amongst other things, I never mentioned the changes in driving I observed.
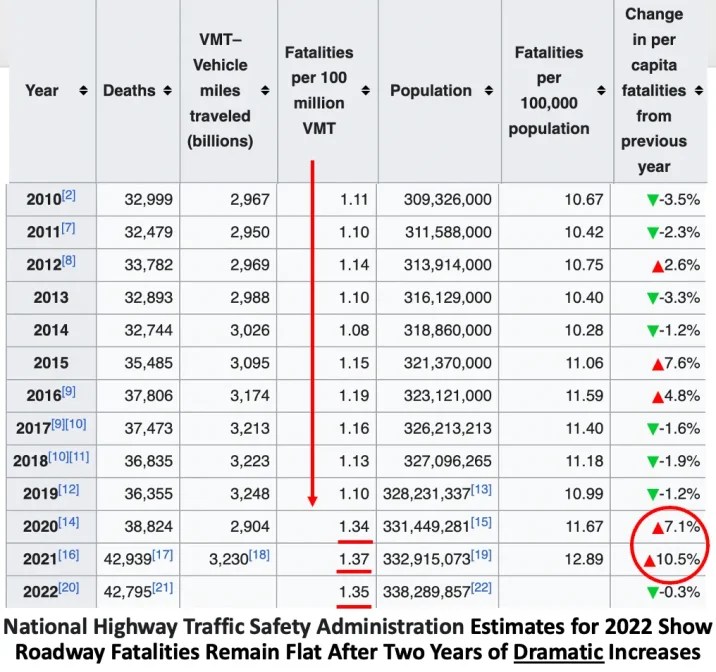
Note: after I posted the original article many of the readers stated they too had observed a significant worsening in the behavior of drivers around them. I was then pointed to this dataset, which suggests this issue was happening, but is difficult to properly assess because COVID-19 can also cause cognitive impairment and less people were driving in 2020.
Typically, when we have situations like this, large bodies of data or scientific studies are needed to tease out if a correlation is in fact occurring. Unfortunately, since there are political repercussions for dissenting from the dominant narrative, data which threatens tends not to be published. This creates the challenging situation where those who are looking for answers on a topic which challenges a vested interest have to look quite carefully for clues on the subject (e.g., by dissecting papers to see exactly what the data is actually showing).
Igor periodically finds those, and after I saw the most recent one he unearthed, I requested to write the original guest post. To quote his discovery from the Netherlands:
Primary care data for January to March 2023 showed that adults visited their GP more frequently for a number of symptoms compared to the same period in 2019. Memory and concentration problems were significantly more common than last year and in the period before COVID-19. Where these symptoms are concerned, the difference compared to 2019 is growing steadily in each quarter.
In the first quarter of 2023, there was a 24% increase in GP [general practioner] visits related to memory and concentration problems among adults (age 25 years and older) compared to the same period in 2020. This is evidenced by the latest quarterly research update from the GOR Network. The increase in memory and concentration problems of adults seems to be a longer-term effect of the coronavirus measures as well as SARS-CoV-2 infections.
More specifically they found:
• No increase was observed in adults under 25 years old.
• A 31% increase was observed in those 24-44 years old.
• A 40% increase was observed in those 45-74 years old.
• A 18% increase was observed in those over 75 years old.
Note: previous rounds of this survey, in addition to the cognitive issues described above, worsening mental health (e.g, anxiety, depression or suicidal thoughts), sleep problems, tiredness, and cardiovascular issues (e.g., shortness of breath, dizziness or heart palpitation) were also observed to have significantly increased since 2019.
Typically, patients, less than 75 years old are unlikely to visit their doctors for cognitive issues. Taken in context with this data, it means there is a stronger case that the (massive) increases in those under 75 were caused by something that happened after 2019. Additionally, since there were already a large number of visits for cognitive impairment in the elderly, the lower percentage increase is slightly misleading in quantifying the extent to which everyone was affected. For example to quote the previous report:
Primary care data showed that adults visited their GP somewhat more frequently for sleep problems in October–December 2022 than in the same period in 2019. This was particularly striking in the oldest age group (75 years and older).
All of this data put health officials in a bit of an awkward situation since publishing data demonstrating large scale cognitive impairment directly undermines the narrative they previously had committed themselves to. Nonetheless, the authors of the report were significantly more candid than many other before them:
The source of this increase in memory and concentration problems is unclear. A possible explanation could be that COVID-19 measures caused accelerated cognitive decline among people who were starting to have problems with memory and concentration (66 years on average).
COVID-19 was of course cited as a potential cause (which, as discussed above can sometimes cause long term cognitive impairment):
A supplementary explanation could be that some of these people have long-term symptoms after COVID-19. Various studies have shown that memory and concentration problems are common in post-COVID symptoms. Other infectious diseases, such as flu, can also cause these symptoms. However, recent studies have shown that long-term memory and concentration problems are much more common after COVID-19 than after flu. In addition, these symptoms are more common in older age groups. The figures provided by GPs are consistent with this expectation.
Fortunately, the authors acknowledged that long COVID could not be the primary explanation for what was occurring, and instead alluded to the elephant in the room—the vaccines.
Note: on VAERS, in the 23 years VAERS has operated, 2352 of the 3071 (76.6%) reports of memory impairment following vaccination came from the COVID-19 vaccines. Additionally, Ed Dowd has identified numerous government datasets demonstrating that widespread impairment and disability has occurred since the vaccine rollout.
My specific interest in studying spike protein vaccine toxicity arose because I suspected I would see many similarities to other pharmaceutical injuries I had observed previously and treatments that had developed for those injuries could be used to treat COVID-19 vaccine injuries. On Substack, I’ve tried to focus on explaining the areas that I believe are the most important to understanding this, zeta-potential, the cell danger response (CDR) and the treatments for Alzheimer’s disease. Note: Each of these is interrelated with and often causes the others.
Zeta Potential: Zeta potential (explained in detail here) governs if fluid in the body clumps together (e.g., forming a clot) or remains dispersed and capable of freely flowing. Additionally, it also influences if proteins will stay in their correct formation or misfold and clump together. Many different issues (discussed here) emerge when fluid circulation (be it blood, lymph, interstitial fluid or cerebrospinal fluid) becomes impaired. Since the spike protein is uniquely suited for impairing zeta potential, we have found restoring zeta potential (discussed here) often is immensely helpful during COVID-19 infections and for treating COVID-19 vaccine injuries. Many of those approaches were initially developed from working with other vaccine injuries and cognitive decline in the elderly.
Cell Danger Response (CDR): When cells are exposed to a threat, their mitochondria shift from producing energy for the cell to a protective mode where the cell’s metabolism and internal growth shuts down, the mitochondria release reactive oxygen species to kill potential invaders, the cell warns other cells to enter the CDR and the cell seals off and disconnects itself from the body. The CDR (explained further here) is an essential process for cellular survival, but frequently in chronic illness, cells become stuck in it rather than allowing the healing response to complete.
Understanding the CDR is extremely important when working with complex illnesses because it explains why triggers from long ago can cause an inexplicable illness, and why many treatments that seem appropriate (specifically those that treat a symptom of the CDR rather than the cause of it) either don’t help or worsen the patient’s conditions. Many of the most challenging patients seen by integrative practitioners are those trapped within the CDR, but unfortunately, there is still very little knowledge of this phenomena.
My interest was drawn back to the CDR after I realized that one of the most effective treatments for long COVID and COVID-19 vaccine injuries was one that directly treated the CDR. Since many of the therapies that have been developed to revive nonfunctional tissue was developed by the regenerative medical field, I wrote an article describing how these approaches are applied to restore localized regions of dysfunctional tissue (which is sometimes needed to treat vaccine injuries) and another on the regenerative treatments that treat systemic CDRs (and are more frequently needed for vaccine injuries).
Alzheimer’s Disease (AD): AD is one of the most devastating and costly conditions in existence (e.g., for the year of 2020 it was estimated to have cost America 305 billion dollars) and as a result, billions of dollars are spent each year in researching a cure for it. This research (which began in 1906) has gone nowhere and presently the FDA is working with the drug industry to push forward ineffective, quite dangerous but highly profitable treatments for AD.
However, effective treatments do exist for AD and my colleagues have developed a few different methods that have successfully treated the condition. Additionally, one neurologist, Dale Bresden developed a method for reversing AD that he proved worked in mulitiple publications (included a recent 2022 clinical trial).
All of these successful approaches utilize the following principles:
• Restore both the blood flow to the brain and the lymphatic drainage from it (which removes amyloid plaques). This often requires restoring the physiologic zeta potential and having a healthy sleep cycle.
• Treating the CDR (which causes chronic inflammation) and reactivating brain cells that became trapped in an unresolved CDR (which amongst other things requires reclaiming a healthy sleep cycle).
Note: Bresden’s approach also emphasizes the importance of addressing chronically elevated blood sugar or insulin levels.
One of the most important things to recognize about AD is that it is a slowly worsening disease which often progresses over decades. In the early stages of AD, minor cognitive changes occur, which (when possible to autopsy) correlate with tissue changes within the brain. In rare instances, individuals can instead have a rapidly progressing form of Alzheimer’s which strikes with a younger age and is often linked to the toxin exposure.
In the case of spike proteins illnesses, I have seen both the early signs of AD cognitive decline occurring in much younger patients, and exist in cases of AD rapidly progressing following COVID vaccination. Additionally, I have also seen cases of rapid cognitive decline in the elderly following the administration of other vaccinations—however they were far less frequent than those seen with the COVID-19 vaccines.
Anytime you attempt to perceive the world around you, you are always biased by the pre-existing filters you have which prevent you from seeing much of the world around you (discussed further here). To some extent, these filters are a necessary evil as without them, the world would be overwhelmingly complicated. However, if you cannot be open to the possibility a biased filter this is clouding your perception of reality, you become blind to a great deal of important things around you. Misleading filters for example, explain why many of those committed to the narrative cannot see the overwhelming evidence of COVID-19 vaccine injuries around them.
One of the most commonly used filters is “social proof,” which essentially says people will typically not act on something, believe it, or even see it unless their peers (the herd) already are. This creates a problem, because frequently when you need to know something, the herd does not yet believe it, forcing you to either make a decision no one else supports (which can be quite terrifying) or to wait until there is safety in doing it because the herd has now moved in that direction (which is often too late).
As I’ve gotten to know those who challenged the COVID-19 narrative, I’ve noticed they all had a tendency they’d learned through life experience to not follow the crowd and be willing to act on their initial impression of what preliminary data suggested before the rest of the crowd caught on. For example, Ed Dowd was a highly successful stock trader (e.g., he made Blackrock a lot of money) and his method boiled down to spotting early trends before anyone else and acting on them while they were still profitable to investors.
Like many, from the start of the vaccination campaign, based on the preliminary data points that were available, I suspected it was going to cause long-term cognitive issues. Now that the data which supports that trend is beginning to appear, and concerningly the issue appears to be gradually worsening, something commonly observed over time with factors that give rise to dementia. This is an important issue and I want to extend my thanks to Igor Chudov for drawing attention to this very important dataset.
Pfizer Ad Spreads Misinformation
BY DAVID ZWEIG | SILENT LUNCH | AUGUST 1, 2023
A Pfizer ad on Twitter claims that 3 out of 4 US adults are at “high risk” for severe Covid-19.
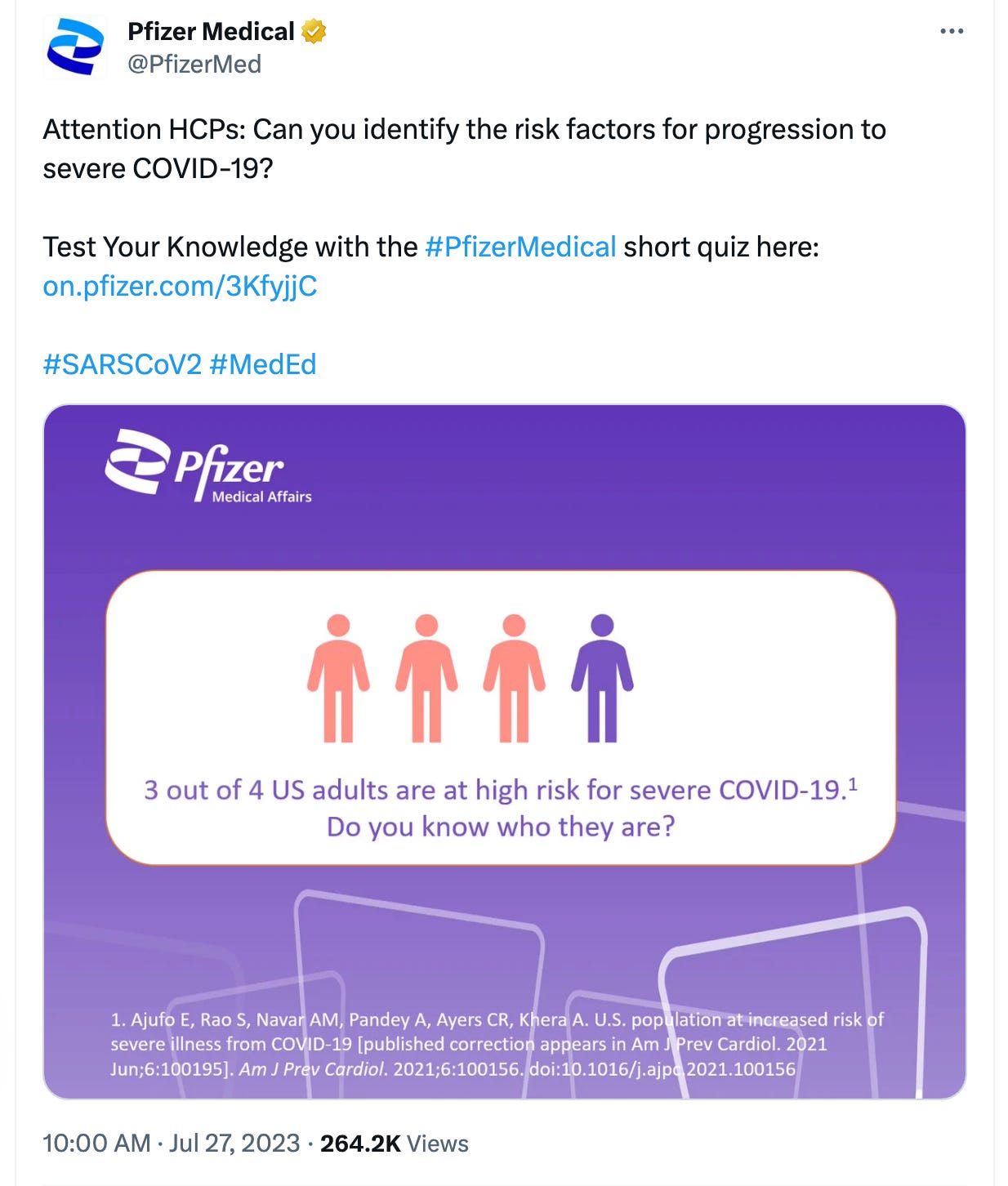
This ad is highly misleading or, arguably, outright false.
Problem 1: What is “high” risk?
We don’t know because Pfizer doesn’t define it.
The graphic in the ad cites a study as the source of its claim “3 out of 4 US adults are at high risk for severe Covid-19.” Except the study never uses the term “high risk.” Rather, the study is on people at “increased risk.”
“Increased risk,” of course is quite different from “high risk.” Obviously, high risk is worse than merely increased risk. I need not explain why Pfizer would choose language in its ad that exaggerates the risk of Covid.
Problem 2: The cited study itself doesn’t even define “increased risk.” Does that mean a 0.1% increase, a 1% increase, 20% increase, 1000% increase? On this point, the study includes the following caveat: “the effect size of each risk factor was not taken into account in our analysis, so this report does not address degree of risk. Effect estimates of severe COVID-19 risk factors are widely variable and ultimately unreliable.”
Digging a little deeper, the study links to a CDC webpage that gives a list of conditions for people who are “more likely to get very sick with COVID-19” and uses “higher risk,” “increased risk,” “greater risk” and “high risk” in its text, seemingly interchangeably. The page gives a long list of medical conditions—from cancer to diabetes to depression. Still, we don’t know what “more likely” or “increased risk” actually means. This webpage, in turn, links to another CDC webpage that describes “Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19.”
We’ve gone from the scary “high” risk (not defined), to “increased” risk (also not defined), to “higher risk.” How is “higher risk” defined? Here is what the page says:
Higher risk is defined as an underlying medical condition or risk factor that has a published meta-analysis or systematic review or underwent the CDC systematic review process. The meta-analysis or systematic review demonstrates a conclusive increase in risk for at least one severe COVID-19 outcome.
So we are now three layers deep and we still don’t have a quantifiable definition for what, exactly, “high,” “increased,” or “higher” even means, nor a clear differentiation of what the first study acknowledges is a wide variability in estimates of risk factors. I’m sure there is a quantifiable threshold defined somewhere, but I stopped digging because this isn’t even the main problem.
Problem 3 (the main problem): The data from the cited study in the Pfizer ad saying 3 out of 4 US adults are at high (aka increased) risk of severe Covid are from 2015-2018. But this ad is being run in July 2023—after nearly the entire population has either already been infected, vaccinated, or both, each circumstance, we have been told, decreases one’s risk of severe Covid. In other words, Pfizer’s own ad suggests that prior infection and vaccination have not reduced the number of people at high risk of severe Covid. Does Pfizer want us to believe that its product—the vaccine—did not lower the rate of people at high risk of severe Covid?
The fact is, 3 out of 4 US adults are not at “high” risk of severe Covid. This statement is based on data from before accounting for the protective effect of infection and vaccination. Moreover, “high risk” is not defined and appears to simply be a made up description.
We’ve heard a lot about “misinformation” in the past few years. Generally, the government and media have pointed the finger at so-called “anti-vaxxers” and “conspiracy theorists.” A critical spotlight from the government has rarely seemed to shine on claims made by Pfizer. Advertisements like this misinform and unnecessarily scare people, perhaps pushing some of them into taking additional doses of the vaccine, or therapeutics like Paxlovid (also made by Pfizer), that have potential harms, and for many people, especially now, without clear benefit.
‘Facebook Files’ Reveal Despicable Disregard for the Constitution
By Ron Paul | July 31, 2023
Last week’s revelation that Facebook took orders from the Biden Administration to censor even accurate information about Covid is the latest example of the US government’s disregard for our Constitution. Thanks to Rep. Jim Jordan, Chairman of the House Judiciary Committee, we now know the extent to which the Biden Administration went in its proxy war against the First Amendment.
Getting the information wasn’t easy. It was only after Facebook founder Mark Zuckerberg was threatened with being held in contempt of Congress that he relented and shared information with the Judiciary Committee about Biden Administration pressure to censor Americans on Facebook who disagreed with White House policy on Covid.
What we have discovered thus far is disgusting. For example, in April 2021, a Facebook employee sent a message to top executives in the company complaining that, “we are facing continued pressure from external stakeholders, including the [Biden] White House” to remove posts. In another example, senior executive Nick Clegg complained that Andy Slavitt, a Senior Advisor to President Biden, was “outraged… that [Facebook] did not remove” a particular post, according to Rep. Jordan’s report.
Rep. Jordan revealed that the “offending post” that the Biden Administration wanted removed was simply a joke making fun of possible vaccine injury down the road. The Biden Administration even wanted to “protect” us from jokes that it didn’t like.
The Administration did not stop at targeting what it called “misinformation.” As Constitutional Law Professor Jonathan Turley noted in a recent column, “the administration also demanded the removal of ‘malinformation’ that is ‘based on fact, but used out of context to mislead, harm, or manipulate.’” So the Biden Administration wanted to “cancel” even truthful information counter to its own preferred narrative.
This level of contempt for our Constitution is shocking. As Robert F. Kennedy, Jr. – who was himself censored at the behest of the Biden Administration – testified recently before Congress: “A government that can censor its critics has license for every atrocity. It is the beginning of totalitarianism.”
Who knows how many thousands of Facebook accounts were banned or restricted at the behest of the Biden White House. Early last year I received notice that my own Facebook Page was “restricted” for 90 days because I pointed out that the CEO of Pfizer once claimed that his Covid shot was “100 effective” but later changed his story. The post was completely accurate but still my page was targeted.
Although some are using this information for partisan gain against the Democrats in power, Americans should not delude themselves: left unchecked, there is little reason to believe a Republican Administration would show any more respect for the Constitution than the Biden Administration. Both parties have shown themselves to be selective in their pledged oath to uphold and defend the US Constitution.
It is just as unconstitutional – and thus illegal – for the US Government to violate the First Amendment by proxy – through so-called private companies – as if the government directly attacked our free speech. We must remember that the unprecedented US government censorship of Americans during Covid was just the test run. Be assured that when the next “crisis” comes – and it will – the authoritarians in charge will again ramp up the censorship machine unless we do something about it.
Copyright © 2023 by RonPaul Institute
One Pfizer jab, 20 months of battling to keep hope alive
By Brian Howard | TCW Defending Freedom | January 23, 2023
It has been a very long 20 months since my one and only Pfizer vaccine. I was hesitant but seeing friends and family seemingly OK I decided to ‘do the right thing’ as we were told. The regret still lives on, of course, although over time you do begin to forgive yourself and recognise the huge pressures we were all under.
Within ten days it started. Pins and needles in the hands at night. Then numbness down the whole right side of my body. Then the constant muscle twitches all over the legs. Within a month the tremors started. By this stage I’d already been fobbed off by my GP and a private neurologist. They didn’t want to know or simply didn’t have a clue how to help. I’ll never forget another neurologist suggesting I even take the second jab. Trust in the system had gone at that point. The symptoms continued. Random jolty movements of the body, intense dizziness, headaches and head pressure, brain-shaking sensations, adrenaline rushes, some elevated heart rate episodes. By the six-month point I was rapidly losing hope. You try to stay positive but it really can be a battle. I was fortunate enough to be self-employed and able to work from home but I had to let jobs go as it became far too much, and the money spent on finding alternative therapies and supplements to fix the problem wiped out any savings I had left.
Eventually I started to see some glimmers of improvement, finding certain things that seemed to at least provide relief. It was slow but bit by bit I could sense some progress. At the 20-month point many of the symptoms are still there and I still have a daily battle with them but generally they are at a far more manageable level. The relapses send you backwards, but you get used to them. It feels odd sometimes to say I’ve got used to any of this. I was perfectly healthy before. Never had any prior issues but when this happens you are forced to adapt pretty quickly. You start to forget what it felt like before all of this.
Beyond the physical, all of us have experienced the gaslighting from the medical profession, the online hatred of the vaccine-injured, the censorship by Big Tech. Whether you like it or not it forces you to see the world very differently.
There are positives. For me that comes from the amazing communities of vaccine-injured who have united to help each other, to listen to each other with an openness and compassion that gives me a great deal of hope for the future. To see what a group of people from all over the country and all over the world can do when they simply come together is quite something. The connections you make and communities you become a part of are like a beacon of light.
That’s why we must keep talking. We know there are more of us out there and they need to know that they are not alone.
Brian is a member of UK CV Family, a vaccine injured support group, that can be contacted here. https://www.ukcvfamily.org
Document Specials: Dr. Peter McCullough about mRNA-vaccine death
Dr. Peter McCullough | July 27, 2023
Death counts were very important for government and public institutions during the Covid-19 pandemic and yet again death is being used as fearporn to scare people into accepting climate change, whilst sudden death, an increase in hospitalizations and an increase in diseases somehow never seemed to interest governments nor the public institutions. Why? Because it’s all connected to the “safe and effective” mRNA-products.
Dr. Peter McCullough, cardiologist and president of the McCullough Foundation, has yet again experienced censorship as the medical journal The Lancet removed a study written by Dr. McCullough and his colleague, within the first 24 hours of it being published. Dr. McCullough and his colleagues found that 74 percent of 325 autopsies of people who died after covid vaccination, were caused by the vaccine.
In this interview Dr. McCullough fills us in on the study, why it was removed and also what was found in the Danish study, which shows that the Pfizer vaccine was an experiment with peoples lives.
Welcome to Document Specials.
Follow Dr. Peter McCullough:
Website, www.petermcculloughmd.com
President, McCullough Foundation, www.mcculloughfnd.org
Author, Courage to Face COVID-19, www.couragetofacecovid.com
Radio Show, www.americaoutloud.com/author/dr-peter-mccullough/
Substack, petermcculloughmd.substack.com/
Follow our Document News Rumble channel where all our international broadcasts are streamed and uploaded.
Featured Video
Chinese jet fuel and the myth of energy independence
or go to
Aletho News Archives – Video-Images
Book Review
Former Insiders Criticize Iran Policy as U.S. Hegemony
By GARETH PORTER | CounterPunch | February 27, 2013
“Going to Tehran” arguably represents the most important work on the subject of U.S.-Iran relations to be published thus far.
Flynt Leverett and Hillary Mann Leverett tackle not only U.S. policy toward Iran but the broader context of Middle East policy with a systematic analytical perspective informed by personal experience, as well as very extensive documentation.
More importantly, however, their exposé required a degree of courage that may be unparalleled in the writing of former U.S. national security officials about issues on which they worked. They have chosen not just to criticise U.S. policy toward Iran but to analyse that policy as a problem of U.S. hegemony. … continue
Blog Roll
 Aletho News
Aletho News- NATO’s Slow Fracture: How Trump’s Iran War Exposed the Instrument of Hegemony
- Chinese jet fuel and the myth of energy independence
- Ukraine Sea Drone Fired From Libya Hit Russian Tanker in Mediterranean
- IRGC: Iranian forces launched no attacks during ceasefire hours
- Trump Administration Moves To Automate U.S. Military Draft Registration
- Spain orders reopening of Tehran embassy, condemns Israel’s carpet bombing of Lebanon
- Israel faces ‘unsustainable’ strategic crisis following 40-day war against Iran: Analyst
- Iran restricts Hormuz access to 15 vessels per day under ceasefire terms: Report
- The ‘Opposition Party’ Has Done Nothing to Stop the Iran War and Much to Goad Trump Into Continuing It
- Moscow backs Tehran on status of Lebanon in US-Iran deal
- If Americans Knew
- Amnesty: Urgent – Protect Lebanese civilians from brutal escalation in Israeli attacks
- Is The War Against Iran Over?
- Inside the Israeli army’s propaganda wing
- Hundreds of Gaza Amputees Stranded in Legal Limbo
- The gallows law: Israel moves toward executing Palestinian children
- Tucker Carlson: The Path to Peace requires ending ‘special alliance’ with Israel
- This is ceasefire? Israel’s biggest massacre yet in Lebanon, another journalist killed in Gaza – Daily Update
- Tucker Carlson on Israel: This Is the Behavior of an Ally? Really?
- Gazans face a triple crisis: severe shortages of water and bread, healthcare in tatters
- NY Times reports how Netanyahu took the US into Iran War
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
