Government Contracts With COVID Vaccine Makers Let Federal Agencies Bypass Normal Regulatory Process: FOIA Docs
By Brenda Baletti, Ph.D. | The Defender | June 30, 2023
A little-known federal agency called BARDA dedicated to countering “health security threats” was responsible for conducting the quality review of every COVID-19 vaccine dose administered in the U.S., Sasha Latypova reported on her Substack.
But BARDA, the Biomedical Advanced Research and Development Authority, which has a “militarized” purpose according to Latypova, is not subject to the same regulations as typical pharmaceutical manufacturers, distributors or regulatory agencies.
Distribution through BARDA was part of the “bait and switch” the federal government subjected the American people to with the COVID-19 vaccines, Latypova — a former pharmaceutical industry executive who now exposes fraud in COVID-19 countermeasures — told The Defender in an interview.
“The public was told these vaccines are made by Pfizer and Moderna and rigorously approved by the FDA.” That, she said, would mean that the “consumer protections we expect from pharmaceutical products, medical devices and even food — which are huge and extensive — we expect them to be in place.”
But in fact, countermeasures contracts made available through Freedom of Information Act (FOIA) requests by various parties and U.S. Securities and Exchange Commission disclosures show the U.S. Department of Defense (DOD) and BARDA contracts with the pharmaceutical companies were structured such that these protections weren’t required, according to Latypova.
The contracts also specified that manufacturers and federal agencies were protected by the Public Readiness and Emergency Preparedness (PREP) Act, which shields “covered persons” — such as pharmaceutical companies, or the DOD/BARDA — from liability for injuries sustained from “countermeasures,” such as vaccines and medications administered during a public health emergency.
Latypova posted a video of a November 2022 presentation during which BARDA’s then-director of Regulatory and Quality Affairs (RQA) Tremel Faison bragged that before the U.S. government could purchase and release any COVID-19 product, the RQA team had to perform a review and acceptance.
“I thought it was very strange, given that this is technically the FDA’s [U.S. Food and Drug Administration] job,” Latypova wrote, so she investigated BARDA.
BARDA is housed within the U.S. Department of Health and Human Services, but its purpose is “to develop medical countermeasures that address the public health and medical consequences of chemical, biological, radiological, and nuclear (CBRN) accidents, incidents and attacks, pandemic influenza, and emerging infectious diseases.”
BARDA now functions as part of the Office of the Assistant Secretary for Pandemic Preparedness and Response, elevated by the Biden administration in 2022 to coordinate the nation’s response to health emergencies.
BARDA reports that it has 77 products on the market.
This is concerning, Latypova said, because typically pharmaceutical products are subject to regulations that govern the clinical trial and manufacturing process and then the licensed pharmacy distribution system monitors for consumer safety.
They are subject to “cGxP” regulations, a suite of “current good practice” processes and procedures with the “x” standing in for a variety of life sciences areas, including manufacturing, laboratory, clinical and distribution.
Those regulations create tight control over pharmaceutical products ensuring, for example, that labeling is accurate, dosage is accurate, there are no impurities, and the active ingredients are active and present in the proper amounts.
The regulations also establish supply chain regulations so the products are tracked during transportation and distribution and are traceable, and they protect consumers from drugs being counterfeit, stolen, contaminated or otherwise harmful.
According to Latypova, the fact that BARDA receives and quality checks the vaccines means the vaccines and COVID-19 countermeasures are subject to different protocols than typical FDA-approved or FDA-authorized products.
According to BARDA’s Standard Operating Procedure (SOP) documents outlining its procedures for receiving and inspecting medical countermeasure products, which Children’s Health Defense obtained through a FOIA request, materials ordered by BARDA have their own process of approval.
Products are shipped from the manufacturer to BARDA. Prior to delivery, BARDA receives the lot number and a certification from the producer that says the product meets its established specifications and contains other technical information such as lot number, etc.
BARDA’s RQA team then receives sealed trucks, makes sure documentation is in order and temperature control is maintained, watches the unloading, and “conducts a cursory examination of obvious physical damage.”
BARDA does not test or verify the contents of the vials it receives. It simply accepts the claims in the manufacturers’ paperwork.
And the products from BARDA, according to the SOP, go into storage at a Strategic National Stockpile site, which, unlike typical pharmaceutical storage sites, is also not subject to regulations.
Pharmacy distribution is licensed on a state-by-state basis. Those regulations are typically extensive as seen, for example, in the Pharmacy Lawbook for the state of California that Latypova posted.
It was previously known that the FDA exempted COVID-19 countermeasures from many of these requirements, justifying that exemption based on the public health emergency.
In May, the FDA extended that exemption beyond the May 11 end of the COVID-19 public health emergency.
But the BARDA documents reveal how limited the oversight provided for the receipt and inspection of countermeasures is in practice.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Can this treatment bring hope to the abandoned vaccine victims?
By Sally Beck | TCW Defending Freedom | June 29, 2023
The unprecedented range and extent of Covid vaccine injury is not open to argument. Yellow Card reporting, which the Medicine and Healthcare products Regulatory Agency say represents just 10 per cent of the true number of reactions, reveals that medical staff and victims have reported half a million adverse events and nearly 2,600 fatalities.
The most common issues following vaccination are low blood platelets (immune thrombocytopenia), heart inflammation (myocarditis), blood clots in the body and brain, (thrombosis and cerebral venous thrombosis) and Guillain-Barré syndrome, where the body attacks its nerves and can cause paralysis.
More than one thousand peer-reviewed research papers have documented and explained the connection between injury and the novel Covid gene therapy; 228 of those papers involve myocarditis, 150 thrombosis, 116 thrombocytopenia, 61 cerebral venous thrombosis, and 43 Guillain-Barré syndrome.
According to the American Vaccine Adverse Events Reporting System (VAERS), who have received 35,302 reports of deaths, the Covid vaccine has led to more death reports than any other vaccine in history. The weight of evidence is startling but many doctors still deny Covid-19 vaccines can cause disability or death.

Despite such unprecedented numbers, our national medicines monitors continue to diminish vaccine injury. Last month the UK Health Security Agency (UKHSA) published this 51-page report on the Covid-19 vaccine programme for healthcare professionals which still describes vaccine injury as rare or of little significance. With no official recognition, there is no government investment into research to understand the pathology of vaccine injury, and no treatment trials to help the millions of vaccine injured.
Former scaffolder Alex Mitchell, 59, from Glasgow, nearly died of vaccine-induced thrombotic thrombocytopenia (VITT) officially caused by the AstraZeneca vaccine which he received on March 20, 2021. He developed blood clots so severe that his left leg was amputated above the knee. A range of medication controls his continuing clotting problems, but Alex, who has been called a liar, conspiracy theorist and anti-vaxxer, despite his official diagnosis and £120,000 compensation payment, has found more help to deal with his ongoing health issues through social media than he has through the NHS.
He said: ‘Supplements were recommended by someone who contacted me on Twitter who has a degree in chemistry and biology. My energy and the fatigue that us vaccine-injured suffer from has improved since I started taking them six months ago.
‘The other things that help are acupuncture and red light therapy. They reduce inflammation, and the severe muscle spasms I was experiencing, which felt like someone had taken a cattle prod to my heel bone, have almost stopped.’
A few dedicated doctors are listening and are raising funds for independent research. One is the US organisation Frontline Covid-19 Critical Care Alliance (FLCCC) founded by a number of doctors including Dr Pierre Kory, and Children’s Health Defence Europe, who held a conference with Dr Meryl Nass last month to discuss vaccine injury.
FLCCC is at the forefront of developing protocols to help the vaccine injured. It is spearheaded by Professor Paul E Marik, formerly chair of pulmonary and critical care at the Eastern Virginia Medical School. He talks regularly to practitioners from all over the world via phone or Zoom who share their clinical experiences. Nothing is added to the FLCCC protocols without a high degree of investigation and scientific reference. Their current vaccine injury protocol has more than 700 scientific references.
Their natural healing regime includes the enzyme nattokinase and aspirin to dissolve blood clots; the anti-inflammatory supplement resveratrol; the mineral magnesium which regulates blood pressure, blood sugar, and is needed for good muscle and nerve function; omega-3 fatty acids which regulate blood clotting; energy boosting co-enzyme Q (CoQ10); the sleep-regulating hormone melatonin; bromelain, the pain-reducing enzyme found in pineapple; the plant chemical berberine which helps strengthen heartbeat, and the brain-nourishing amino acid N-acetylcysteine (NAC).
It has had mixed results but one group called ZeroSpike hope they have made a major breakthrough. ZeroSpike was put together by Fabio Zoffi, a tech entrepreneur, who three years ago formed Federazione Rinascimento Italia (FRI), a civil society of Italian doctors, lawyers, scientists, professionals, and entrepreneurs, horrified by the draconian Covid response.
He contacted Dr Loretta Bolgan, a doctor of chemistry and pharmaceutical technology, and asked her to investigate the Sars-CoV-2 virus and the new mRNA vaccine technology. Once the team discovered that the Covid vaccines and the virus both contained the spike protein, Zoffi asked them to develop a way to get rid of it.
The spike contributes to cardiovascular, brain, and blood clotting problems, and can cause autoimmune conditions, cell deformation and cell fusion damage. It can cross the blood-brain barrier causing memory loss and brain fog, can trigger a stroke or cause other neurological issues.
Manufacturers said the injected spike would clear itself naturally but information from the respected pathologist Professor Arne Burkhardt in Germany, who died recently, and from a freedom of information request from Pfizer’s nonclinical evaluation report submitted to the Australian Department of Health, shows it does not and that it can damage major organs, including the ovaries, liver, spleen and adrenal glands.
The team of ten focused on the food supplement NAC which specifically helped the condition which the vaccine injured and those with long Covid describe as brain fog. Studies showed that NAC denaturated (removed) between 12 per cent and 15 per cent of the Covid spike protein.
NAC is derived from the amino acid L-cysteine and helps replenish glutathione levels in the body and can help to improve brain function. Glutathione is produced by the liver and helps with immune system function, as well as tissue building and repair, vital to help the injured recover. The team then used quantum physics to turbo charge – augment – the NAC molecule, which made a huge difference. In the lab (in vitro), they claim it removed 99.8 per cent of extracellular spike, although there are no traditional double-blind placebo-controlled trials to support the claim.
To prove it, the team developed a urine test which showed how much spike was being excreted. Women’s health specialist Dr Tina Peers told the audience at the Better Way conference in Bath this month: ‘If you check someone’s urine before they take augmented-NAC there aren’t the end products of the denaturation, but by day eight of taking it, they found that the urine was full of denatured spike protein.’
Health practitioners with no financial interest in the product are calling it a ‘game-changer’. Pulmonary and critical care specialist Dr Pierre Kory told the Better Way audience: ‘I integrated it into my practice two months ago. Not everybody responds but some testimonials are really earth-shattering.’
Scott Marsland, a registered nurse (RN) since 1997 and a family nurse practitioner (FRP-C) since 2014, is a partner with Dr Kory in a Covid treatment practice in Syracuse, New York. They have treated more than 2,000 Covid, long Covid or vaccine injured patients in the last 14 months.
Marsland is impressed with A-NAC. He said: ‘I have treated 72 patients with it and 75 per cent have noted benefit. Three had adverse responses of mild to severe rash, but that fully resolved quickly.
‘I had a patient with mental health issues, including anxiety and depression. After taking it, he said, “I’m sleeping like a baby. A cloud has lifted.” Another, who suffered spinal injury after a car crash, had very poor respiratory status preventing the operation. Within a week she reported her lungs were stronger than in the last three years. A young patient with 5/10 chest pain reported after three days the pain was measuring 2/10.’
Dr Peers was herself injured by two AstraZeneca vaccines. She said: ‘I had a tremor in my hand, I had dormant mast-cell activation syndrome (MCAS) which flared, my face was puffy, my eyes were swollen. It affected my immune system.’
She began taking augmented NAC more than two months ago and developed a rash, like Marsland’s patients. She said: ‘After a few days I had a detox reaction and developed eczema on my face. It lasted about 48 hours but now my tremor has gone, the rash has gone and my MCAS is under control again.’
In Italy, a country hit by some of the most brutal Covid measures including a ‘no jab, no job’ policy which lasted for 18 months, ZeroSpike have helped more than 10,000 patients. Internationally, they have treated a total of 20,000 patients and say that none has come back with any complaints. Patients will generally complain if they experience negative events.
Can this new treatment give people abandoned by their governments hope? Will the medical establishment engage with this research and its findings? With countries such as Canada already making a move to ban all natural supplements like A-NAC, there will be a huge battle for recognition. But as Alex Mitchell says, ‘They’ll stop us accessing successful treatments over my dead body.’
CISA Was Behind the Attempt to Control Your Thoughts, Speech, and Life
Brownstone Institute | June 30, 2023
Keeping up with the corruption of the Covid regime feels like drinking from a firehose. The volume of the fraud, the pace of new discoveries, and the breadth of the operations are overwhelming. This makes it imperative for groups like Brownstone Institute to digest the onslaught of information and communicate salient themes and dispositive facts, particularly given the dereliction of mainstream media.
On Monday, the House Judiciary Committee released a report on how the Cybersecurity and Infrastructure Security Agency (CISA) “colluded with Big Tech and ‘disinformation’ partners to censor Americans,” adding to the informational firehose we work to imbibe.
The 36-page report raises three familiar issues: first, government actors worked with third parties to overturn the First Amendment; second, censors prioritized political narratives over truthfulness; and third, an unaccountable bureaucracy hijacked American society.
- CISA’s Collusion to Overturn the First Amendment
The House Report reveals that CISA, a branch of the Department of Homeland Security, worked with social media platforms to censor posts it considered dis-, mis-, or malinformation. Brian Scully, the head of CISA’s censorship team, conceded that this process, known as “switchboarding,” would “trigger content moderation.”
Additionally, CISA funded the nonprofit EI-ISAC in 2020 to bolster its censorship operations. EI-ISAC worked to report and track “misinformation across all channels and platforms.” In launching the nonprofit, the government boasted that it “leverage[d] DHS CISA’s relationship with social media organizations to ensure priority treatment of misinformation reports.”
The switchboard programs directly contradict sworn testimony from CISA Director Jen Easterly. “We don’t censor anything… we don’t flag anything to social media organizations at all,” Esterly told Congress in March. “We don’t do any censorship.” Her statement was more than a lie; it omitted the institutionalization of the practice she denied. The agency’s initiatives relied on a collusive apparatus of private-public partnerships designed to suppress unapproved information.
This should sound familiar.
Alex Berenson gained access to thousands of Twitter communications that uncovered concrete evidence that government actors – including White House Covid Advisor Andy Slavitt – worked to censor him for criticizing Biden’s Covid policies.
White House Director of Digital Strategy Rob Flaherty privately lobbied social media groups to remove a video of Tucker Carlson reporting the link between Johnson & Johnson’s vaccine and blood clots.
Facebook worked with the CDC to censor posts related to the Covid “lab-leak” hypothesis. Company employees later met with the Department of Health and Human Services to de-platform the “disinformation dozen,” a group including Robert F. Kennedy, Jr.
These were not cherry-picked examples – they were part of an institutional collusion to strip Americans of their First Amendment rights. Journalists Michael Shellenberger and Matt Taibbi exposed the “Censorship Industrial Complex,” a collection of the world’s most powerful government agencies, NGOs, and private corporations that worked together to silence dissent.
The Supreme Court has held that it is “axiomatic” that the government cannot “induce, encourage, or promote private persons to accomplish what it is constitutionally forbidden to accomplish.” Yet, CISA has joined the disturbing tendency of public-private partnerships designed to impede Americans’ right to information and freedom of speech.
- Political Operatives
Second, these programs were not idealistic attempts to promote the truth; they were calculated programs designed to quash inconvenient but truthful narratives.
The report outlines how CISA censored “malinformation – truthful information that, according to the government, may carry the potential to mislead.” Journalist Lee Fang later wrote that the malinformation campaign “highlights not only the broad authority that the federal government has to shape the political content available to the public, but also the toolkit that it relies upon to limit scrutiny in the regulation of speech.”
In this system, uncensored information has a tacit government approval, amounting to a system of widespread propaganda.
“State and local election officials used the CISA-funded EI-ISAC in an effort to silence criticism and political dissent,” the report notes. “For example, in August 2022, a Loudon County, Virginia, government official reported a Tweet featuring an unedited video of a county official ‘because it was posted as part of a larger campaign to discredit the word of’ that official. The Loudon County official’s remark that the account she flagged ‘is connected to Parents Against Critical Race Theory’ reveals that her ‘misinformation report’ was nothing more than a politically motivated censorship attempt.”
The officials supporting the operation remained unrepentant in their aim to advance political agendas. Dr. Kate Starbird, a member of CISA’s “Misinformation & Disinformation” subcommittee, lamented that many Americans seem to “accept malinformation as ‘speech’ and within democratic norms.”
Of course, the program explicitly violated the Constitution. The First Amendment does not discriminate based on the veracity of a statement. “Some false statements are inevitable if there is to be an open and vigorous expression of views in public and private conversation,” the Supreme Court’s controlling opinion held in United States v. Alvarez. But CISA – led by zealots like Dr. Starbird – appointed themselves the arbiters of truth and worked with the most powerful information companies in the world to purge dissent.
This was part of a larger political campaign.
Hunter Biden’s laptop, natural immunity, the lab-leak theory, and side effects of the vaccine were all censored at the government’s behest. The truth of the reports were not at issue; instead, they presented inconvenient narratives for Washington’s political class, who then used the Orwellian label of “malinformation” to lend cover to eviscerating the First Amendment.
- The Terror of the Administrative State
Third, the report exposes the increasing power of the administrative state. Federal bureaucrats rely on anonymity and unaccountability. Private industry employees could never oversee a disaster like the Covid response and maintain their jobs. It’d be like if BP’s head of safety for the Gulf of Mexico received a promotion after the oil spill.
But unelected officilals like CISA officials enjoy ever-increasing power over Americans’ lives without having to answer for their calamities. Suzanne Spaulding, a member of the Misinformation & Disinformation Subcommittee, warned that it was “only a matter of time before someone realizes we exist and starts asking about our work.”
Spaulding’s comment reflects the power that CISA wields and the benefit it derives from its lack of public exposure. Most Americans have never heard of CISA despite its overwhelming influence over lockdowns.
In March 2020, CISA divided the American workforce into categories of “essential” and “nonessential.” Within hours, California became the first state to issue a “stay at home” edict. This began a previously unimaginable assault on Americans’ civil liberties.
The House Report indicates that CISA was a central actor in censoring criticism of the Covid regime in the ensuing months and years. The agency is representative of the cabal of censorial and unaccountable officials engaged in public-private partnerships designed to keep us in the dark.
Rogan’s RFK interview is full of vitally-important taboo info
BY BILL RICE, JR. | JUNE 26, 2023
Yesterday, I spent several hours reading the transcript of the 3-hour interview RFK, Jr. recently did with Joe Rogan. The conversation was fascinating. Any U.S. citizen interested in more detailed information on Kennedy’s thoughts can simply watch this interview (a link to the Rogan episode and a transcript are included in this article which summarizes the interview).
I particularly recommend the final paragraphs of the CHD article, where Kennedy talks about the mothers of autistic children who finally convinced him to look into a possible connection between vaccines and autism.
Here are highlights that jumped out to me after reading transcripts of the entire interview:
- Kennedy said (again) that he’s NOT running on the “vaccine issue” and only talks about vaccines when specifically asked a question about them by an interviewer.
- However, he did say he’s not going to dodge a legitimate question when asked. He also said that he didn’t plan on doing any more in-depth interviews like this in the future, suggesting this conversation with Rogan should provide sufficient answers on why and how he got so interested in the vaccine issue … an intellectual quest which later informed his conviction that the entire public health establishment has become brazenly and shockingly corrupt and captured.
- Kennedy said alarms went off when he had a phone conversation with Dr. Paul Offit about mercury in vaccines and caught this extremely-influential vaccine booster in an obvious lie. Kennedy also noted that this man said he would get back to him with specific scientific studies that backed up his vaccine autism point (that there was bad “mercury” and “safe” mercury). Kennedy said this revered scientist never did provide the promised study(ies).
- Kennedy also recounts a similar conversation with Dr. Fauci, who told Kennedy that he would provide germane studies on some topic Kennedy had challenged Fauci on …. and Fauci never followed through.
One of Kennedy’s main points is that whenever he wanted to see the published peer-reviewed scientific studies backing different conclusions of the Science Establishment … the members of the Scientific Establishment couldn’t and didn’t do this.
Kennedy also notes he personally knows and had spoken to many leading authorities in the public health bureaucracies and he always got the impression these leaders had not read any of the scientific studies that Kennedy had read. They weren’t even familiar with these studies.
- Rogan talked a good bit about censorship and how he (Rogan) had been maligned and intentionally discredited for comments he’d made. Almost as an aside, Kennedy noted that he had been censored for “18 years” (!)
- … Kennedy also said that nobody has ever debated him on these topics, and cited examples of “debates” or events that were supposed to happen and never did.
- One such “debate” was supposed to be Kennedy vs. one of these alleged science authorities at a hearing in the Connecticut Senate (if memory serves, on the autism question).
- According to Kennedy, a Connecticut elected official asked Kennedy to participate in a hearing with this other authority. Later, Kennedy was told it would be him vs. two executives, then three, then four.
- Kennedy, as it turns out, would only get six minutes to make his points. Still, Kennedy said (paraphrasing): “This is not fair, but okay. I’ll be there.” The debate/testimony was later cancelled – after Kennedy had flown “on the red-eye” to Connecticut on his own dime to participate. Nobody told him why this hearing with him was cancelled. Kennedy just assumes someone told these people to NOT debate RFK, Jr. This scenario should sound very familiar today. (Think the “Hotez debate.”)
- I found Kennedy’s points about the explosion of autism to be very convincing. His main point is that nobody his age (or my age) grew up with anyone who had the severe autism that is common with many children today.Kennedy does note that observations such as this do NOT equal scientific “causation” or “correlation” … but when so many mothers of autistic children keep reaching the same conclusion, this should be enough anecdotal evidence to launch serious and real scientific studies and genuine scientific investigations, Kennedy argues.
- Kennedy’s points about VAERS picking up only a tiny fraction of vaccine injuries and deaths are very persuasive and important. (This is the topic of one of my next articles, which will highlight the fact Ed Dowd’s work on “all-cause excess” deaths is STILL being ignored by the mainstream media – 18 months after Dowd, among others, began to highlight this.)
- Regarding his book The Real Anthony Fauci, Kennedy notes that the book sold more than one million copies in its “first three months.” Oddly (to me), Kennedy said he doesn’t know how many copies this book sold after this because he hasn’t looked at the numbers.
- I’ve been curious about the book’s cumulative sales figure as every story I can find on the book says only that it “sold more than one million copies.”
- This is certainly a true statement, but I wonder if the book might have sold at least two million copies by now. Kennedy also points out that nobody at mainstream “news” organizations reviewed the book and very few “independent” book-sellers ever stocked the book in their stores (a point I made in a recent column.) Also, for some reason, lists of “best-selling” books often omitted The Real Anthony Fauci from these sales rankings.
- The above anecdotes should tell the public that most owners of book stores (and the “free press”) believe in banning certain books (more specifically, they don’t stock or mention books that question the prevailing orthodoxy).
- Question: How many copies of The Real Anthony Fauci would have been sold if this book had been available in bookstores all over the world (like other big best-sellers)? Would this have made a difference and perhaps saved lives?
Note: Joe Rogan said his entire thinking about vaccines, public health and Kennedy changed dramatically after he did read this book. Question: Think if Rogan had not read this book. He probably would have never had Kennedy on his show and Rogan probably would never have become one of the leading contrarian voices on the “authorized narrative.” This shows the power of the written word or of one book … and why such a book had to be censored.
- According to Kennedy, the vast majority of the book’s sales came from just one source – Amazon. (Authors like Naomi Wolf and many other skeptics of the official narratives have also published “taboo” Covid books. This question also occurs to me: How many additional copies of these books would have been sold if readers interested in these topics had seen them and been able to buy them if they had been available in local bookstore? (I guess this is another “unknown unknowable.”)
* Rogan made interesting points about how other podcasters are seemingly being bullied with the threat of “de-platforming” or “de-monetization” if the hosts of these shows invite contrarian Covid speakers onto their shows as guests (including Rogan himself).
* Rogan mentioned that he knows several comedian friends who think like he does, which he suggests helped him maintain his sanity in these New Normal Covid times. Kennedy later asked Rogan (paraphrasing), “Who are these people? I haven’t heard any stand-up comedians doing gigs where they poke fun of this Covid madness.” The Kimmels and Colberts of the world were (and still are) all singing from the same “authorized narrative” hymnal.
- Kennedy provides a good bit of detail about his life as an environmental lawyer and how he and his allies in his cause helped clean up the Hudson River waterways. It was his belief that mercury was getting into fish that later led him to believe that the same toxic mercury (far more dangerous than lead, according to Kennedy) was being injected into children with their mandatory vaccines.
- According to Kennedy, this was a point that mothers kept making to him at Kennedy’s speaking engagements. Finally, one of these mothers showed up at his house, dropped an 18-inch pile of documents on his door step and told Kennedy she wasn’t leaving until he read these documents.
- Kennedy read them … and the rest is … history … History that also explains why Robert Kennedy, Jr. is now the No. 1 threat to the Big Pharma/Medicine/Science establishment. It also explains how a once popular liberal environmental lawyer almost instantly became a pariah to the Establishment and a conspiracy-spreading, wacko kook.
- Kennedy notes that he has filed “hundreds” of lawsuits and every one of them deal with “science.” Regarding the narrative that everyone should “trust the science and the experts,” Kennedy makes a great point in his conversation with Rogan:
- Every lawsuit he has ever been a part of includes “experts” … from both sides. Kennedy gives an example of one big environmental lawsuit where the defendants called experts from prestigious academic institutions like Harvard, Stanford and Yale as witnesses. But the plaintiffs also called “expert” witnesses who were professors at the same colleges. So the obvious question is: What “experts” are more credible? This, Kennedy says, is for a jury to decide (and plenty of juries sided with Kennedy’s experts).
Kennedy also pointed out that almost all of the “new” vaccines since the late ’80s allegedly “protect” children from diseases that do not pose a real health risk to them. He gave the example of the Hepatitis B vaccine newborns get at the hospital. Kennedy pointed out this is a “vaccine” to allegedly provide “protection” against a disease that might affect only a few of these children 16 to 30 years later – if they became a prostitute or a needle drug user.
I thought Kennedy was also very persuasive, making his point that advancements in nutrition, sanitation and “engineering” almost completely explain the disappearance of most childhood or adult diseases in the last century or so (for example, refrigeration.)
This leads people like me to conclude that the Mother of All medical scams might be the one that tells us that “vaccines” are the wonder-drug of our times and have saved millions of lives. This is almost certainly a “false” or at least “dubious” narrative. (But a profitable one for Big Pharma).
Yet another fascinating segment was when Kennedy explains the “95 percent effective” canard. He points out that the best metric flowing from Pfizer’s limited safety trials should have been the conclusion that it takes 22,000 doses of Covid vaccine to (maybe) prevent one “Covid” death.
If this is the case (and it apparently is), “You better be sure that vaccine isn’t causing any deaths,” Kennedy states. As Kennedy points out, in the Pfizer trials only three people died from Covid in the ensuing six months – one person in the “vaccinated” group, and two in the “unvaccinated” group.
However, four or five more people in the “vaccinated” group later died from “all causes.” But identifying deaths from “any cause” was not a goal of the study. (It took a Freedom of Information request and a judge’s ruling to release this key information to the public … something Pfizer didn’t want to do for 75 years).
So trial participants had a much greater chance of dying (from any cause) if they’d received the Covid vaccine than if they had not been vaccinated. Question asked by Kennedy: Shouldn’t this data point/finding have been the big headline and enough to stop the vaccines?
Regarding the “vaccines-cause autism” theory, Kennedy does not definitively or categorically blame just vaccines. He seems to be saying many factors probably explain this – including vaccines.
Kennedy notes that when he was a child he received three childhood vaccines. Today, children MUST get 72 shots (from 16 vaccines). Kennedy also noted that five of his children suffer from food allergies, something that also was almost unheard of when Kennedy was growing up.
Kennedy also did a great job explaining how Big Pharma got immunity from vaccine lawsuits, per hugely-significant legislation passed in the Reagan administration in 1986. This gave Big Pharma a license to make “billions of dollars,” Kennedy argues.
All Pharma companies had to do was come up with a new “vaccine” and make sure this vaccine got placed on the childhood immunization schedule (which apparently was a sure-thing).
I also found it interesting that RFK, Jr. acknowledges that his own uncle, Sen. Ted Kennedy – who was chairman of an important Senate Health Committee at the time – helped pass this world-changing legislation. That is, it wasn’t just President Reagan who made this possible; it was the Democrats in Congress too – including his own uncle.
Kennedy also debunks the accepted wisdom that vaccines are “safe” by pointing out the whole reason this legislation was passed into law was because vaccines are obviously not (always) safe. Vaccines are inherently unsafe – this is why the industry needed legal immunity from lawsuits to keep producing them, says Kennedy.
My main-take away from this in-depth interview is how well Kennedy knows this material. During this 3-hour interview, Kennedy didn’t refer to any notes. He cited study after study from memory. He had read these studies – critically – and quickly identified the holes and likely cover-ups in them.
I’m convinced this is the real reason no expert or authority will debate someone like Kennedy (or, for example, Steve Kirsch). They all know Kennedy knows this material better than they do. And they all know that they can’t answer Kennedy’s key questions.
Hopefully, more people will take the time to watch this 3-hour interview or read the transcripts. If they do, they’ll see that Kennedy is not some crazy “kook.” I also commend Joe Rogan for giving RFK, Jr. this 3-hour platform to express his views and more fully discuss these life-and-death public health issues.
Religious Exemption Form for Parents of School-Age Kids in D.C. ‘Intentionally Misleading and Unlawful’
The Defender | June 27, 2023
A form provided by the District of Columbia Department of Health for parents seeking a religious exemption for mandated vaccines on behalf of their minor children is “intentionally misleading and unlawful,” according to Children’s Health Defense (CHD) Senior Staff Attorney Rolf Hazlehurst.
A letter from Hazlehurst and CHD Acting President Laura Bono to D.C. Mayor Muriel Bowser and school and health department officials states there is “no legal basis or requirement” for parents to use the newly revised “2023 Religious Exemption Request Process for Families” posted on the DC Health website.
According to the health department, “In consideration of the COVID-19 vaccine mandate for eligible students, and the need to ensure all students in the District remain up to date with all necessary or required vaccinations to attend school,” health officials revised the religious exemption form “to include a section to document a strongly held religious belief opposing vaccination.”
Parents and guardians are instructed to request the form and return it directly to DC Health/Immunization Division after carefully reading and completing it in its entirety. “incomplete or non-compliant forms will be returned before being sent for review, the department said.
But the updated form contains at least two subsections that are “unlawful as written and applied,” Hazlehurst said.
In the first part of Section 2, parents and guardians are required to initial to acknowledge that “by not vaccinating their child for one or more of the listed vaccinations, they are placing their child at ‘increased risk,’ thus implying that they are unfit parents or guardians.”
And, according to the letter, the second part of Section 2 requires each parent or guardian to:
“Please provide a written statement on a) why you do not get vaccinations based on your sincerely held religious beliefs, b) the religious principles that guide your decision not to get vaccinated, and c) whether you are opposed to all vaccinations, and if not, d) the religious beliefs you follow that will not allow you to get the COVID-19 vaccination.”
In their letter, Bono and Hazlehurst said this language “intentionally misleads those parents or guardians seeking religious exemptions into believing they must comply with these instructions or their request will be denied.”
“Nothing could be further from the truth,” they wrote, adding that according to the law, Code of the District of Columbia §38-506, entitled “Exemption from Certification” states:
No certification of immunization shall be required for the admission to a school of a student:
(1) For whom the responsible person objects in good faith and in writing, to the chief official of the school, that immunization would violate his or her religious beliefs.
In other words, parents and guardians are not required to complete the updated form — they can simply write a letter to the chief official of the child’s school certifying that in accordance with the Code of the District of Columbia §38-506, they object in good faith that immunization(s) violate their sincerely held religious beliefs.
If DC Health officials wanted to create a new process in which parents and guardians must comply to receive a religious exemption, the agency is required by law to promulgate the new rule by complying with the administration process and allowing the public the opportunity to respond — neither of which were done, Hazlehurst and Bono wrote.
D.C. Council weighs bill to remove COVID vaccine mandate for schools
Hazlehurst and Dr. Elizabeth Mumper last week submitted written testimony to D.C. Council members in support of Bill 25-0278, the School Student Vaccination Amendment Act of 2023, which would remove the COVID-19 vaccine mandate for students attending D.C. schools.
Both commended the council members for introducing the amendment. In his written statement, Hazlehurst called on the council to expedite passage of the bill “to avoid parents unnecessarily getting their children the COVID-19 vaccine in order to attend school.”
He also outlined his legal objections to the health department’s newly revised religious exemption form.
Mumper, a pediatrician, also showed support for the bill. In a lengthy written statement, she said:
“As a pediatrician with 43 years of experience in pediatrics and 24 years of experience identifying and treating children with vaccine injuries, I oppose giving COVID-19 vaccines to infants and children.
“Having carefully studied the risks and benefits, I conclude unequivocally that the risk of harm outweighs any potential benefit. Multiple sources of scientifically sound data support my position.”
In July 2022, The Washington Post said the district’s COVID-19 vaccine mandate for schoolchildren was “among the strictest in the nation.”
CHD last year represented a group of parents challenging the D.C. Minor Consent for Vaccination Act, which would have allowed children as young as 11 to consent to vaccination without parental knowledge or consent.
CHD fought, and the court issued a preliminary injunction prohibiting enforcement of the law and the district was forced to repeal it.
In his ruling, Judge Trevor N. McFadden said:
“States and the District are free to encourage individuals, including children, to get vaccines. But they cannot transgress on the Program Congress created. And they cannot trample the Constitution.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Serious adverse events from Pfizer’s mRNA vaccine are not “rare”
Maryanne Demasi, reports | June 27, 2023
Drug regulators and public health agencies have saturated the airways with claims that serious harms following covid vaccination are “rare.”

But there has been very little scrutiny of that claim by the media, and I could not find an instance where international agencies actually quantified what they meant by the term “rare” or provided a scientific source.
The best evidence so far, has been a study published in one of vaccinology’s most prestigious journals, where independent researchers reanalysed the original trial data for the mRNA vaccines.
The authors, Fraiman et al, found that serious adverse events (SAEs) – i.e. adverse events that require hospitalisation – were elevated in the vaccine arm by an alarming rate – 1 additional SAE for every 556 people vaccinated with Pfizer’s mRNA vaccine.
According to a scale used by drug regulators, SAEs occurring at a rate of 1 in 556 is categorised as “uncommon,” but far more common than what the public has been told.

Therefore, I asked eight drug regulators and public health agencies to answer a simple question: what is the official calculated rate of SAEs believed to be caused by Pfizer’s mRNA vaccine, and what is the evidence?
The agencies were FDA, TGA, MHRA, HC, PEI, CDC, ECDC and EMA.
The outcome was startling.
Not a single agency could cite the SAE rate of Pfizer’s vaccine. Most directed me to pharmacovigilance data, which they all emphasised does not establish causation.
The Australian TGA, for example, referred me to the spontaneous reporting system but warned, “it is not possible to meaningfully use these data to calculate the true incidence of adverse events due to the limitations of spontaneous reporting systems.”
Both the German regulator (PEI) and European CDC referred me to the European Medicines Agency which, according to its own report, saw no increase at all in SAEs. “SAEs occurred at a low frequency in both vaccinated and the placebo group at 0.6%.”
The UK regulator MHRA went so far as to state it “does not make estimations of a serious adverse event (SAE) rate, or a rate for adverse reactions considered to be causally related for any medicinal product.”
The US FDA, on the other hand, did conceded that SAEs after mRNA vaccination have “indeed been higher than that of influenza vaccines,” but suggested it was justified because “the severity and impact of covid-19 on public health have been significantly higher than those of seasonal influenza.”
Despite analysing at the same dataset as Fraiman, the FDA said it “disagrees with the conclusions” of the Fraiman analysis. The agency did not give specifics on the areas of disagreement, nor did it provide its own rate of SAEs.
In response to the criticism, Joe Fraiman, emergency doctor and lead author on the reanalysis said, “To be honest, I’m not that surprised that agencies have not determined the rate of SAEs. Once these agencies approve a drug there’s no incentive for them to monitor harms.”
Fraiman said it’s hypocritical for health agencies to tell people that serious harms of the covid vaccines are rare, when they have not even determined the SAE rate themselves.
“It’s very dangerous not to be honest with the public,” said Fraiman, who recently called for the mRNA vaccines to be suspended.
“These noble lies may get people vaccinated in the short term but you’re creating decades or generations of distrust when it’s revealed that they have been misleading the public,” added Fraiman.
Dick Bijl, a physician and epidemiologist based in the Netherlands, agreed. “It goes to show how corrupted these agencies are. There is no transparency, especially since regulators are largely funded by the drug industry.”
Bijl said it’s vital to know the rate of SAEs for the vaccines. “You must be able to do a harm:benefit analysis, to allow people to give fully informed consent, especially in young people at low risk of serious covid or those who have natural immunity.”
Bijl said the mainstream media has allowed these agencies to make false claims about the safety of vaccines without interrogating the facts.
“The rise of alternative media is strongly related to the lies being told by the legacy media, which just repeats government narratives and industry marketing. In the Netherlands, there is a lot of discussion about the distrust in public messaging,” said Bijl.
mRNA: Vaccine or Gene Therapy? The Safety Regulatory Issues
Dr. Helene Banoun Elucidates the History of Misguided Use of Genetic Code for Vaccination
By Peter A. McCullough, MD, MPH | Courageous Discourse | June 26, 2023
I have been impressed with the quality of scholarship from independent academic researchers during the pandemic. During this time there has been a silence from academia in terms of any viewpoints that deviate from the mainstream scientific narrative. Dr. Helene Banoun is an independent researcher, former research fellow at INSERM (French Institute for Health and Medical Research), Marseille, France. She has published several very important review papers during the crisis.
Dr. Banoun has recently published an analysis on the mRNA vaccines in consideration of definitions and regulations that apply to gene therapy. For most people vaccinated, it was the first time they had been injected synthetic genetic code for a potentially lethal foreign protein (Wuhan Spike protein). A perfectly compliant American who started the COVID-19 vaccination program on time is on their seventh mRNA injection—an astonishing observation given the lack of any safety information concerning the cumulative effect of frequent, serial administrations. Banoun makes the case that they should be classified as gene therapy products. I have heard no counter arguments to the contrary.

Banoun, H. mRNA: Vaccine or Gene Therapy? The Safety Regulatory Issues. Int. J. Mol. Sci. 2023, 24, 10514. https://doi.org/10.3390/ijms241310514
Banoun goes on to state: “The wide and persistent biodistribution of mRNAs and their protein products, incompletely studied due to their classification as vaccines, raises safety issues. Post-marketing studies have shown that mRNA passes into breast milk and could have adverse effects on breast-fed babies. Long-term expression, integration into the genome, transmission to the germline, passage into sperm, embryo/fetal and perinatal toxicity, genotoxicity and tumorigenicity should be studied in light of the adverse events reported in pharmacovigilance databases.”
This is important for discussants and litigators to have this predicate. Genetic vaccines are gene therapy products, all the regulations, laws, and safety protections should be called for and pointed out when missing in the discussion on the next steps to be taken on mRNA genetic vaccines.
Featured Video
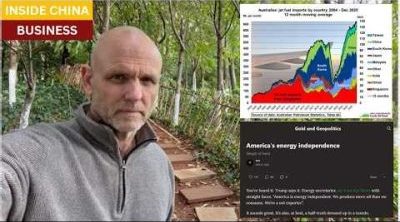
Chinese jet fuel and the myth of energy independence
or go to
Aletho News Archives – Video-Images
Book Review
Former Insiders Criticize Iran Policy as U.S. Hegemony
By GARETH PORTER | CounterPunch | February 27, 2013
“Going to Tehran” arguably represents the most important work on the subject of U.S.-Iran relations to be published thus far.
Flynt Leverett and Hillary Mann Leverett tackle not only U.S. policy toward Iran but the broader context of Middle East policy with a systematic analytical perspective informed by personal experience, as well as very extensive documentation.
More importantly, however, their exposé required a degree of courage that may be unparalleled in the writing of former U.S. national security officials about issues on which they worked. They have chosen not just to criticise U.S. policy toward Iran but to analyse that policy as a problem of U.S. hegemony. … continue
Blog Roll
 Aletho News
Aletho News- What is fueling unrest across the EU?
- Why no power can undermine Iran’s eternal dominance over the Strait of Hormuz
- Is The War Against Iran Over?
- Iran war will leave long-term ‘scar’ on Wall Street, investors warn
- How Iran decimated US power projection in West Asia: Military lessons of 40-day war
- Iran’s report details US-Israeli war crimes in targeting schools, hospitals, livelihoods
- NATO’s Slow Fracture: How Trump’s Iran War Exposed the Instrument of Hegemony
- Chinese jet fuel and the myth of energy independence
- Ukraine Sea Drone Fired From Libya Hit Russian Tanker in Mediterranean
- IRGC: Iranian forces launched no attacks during ceasefire hours
- If Americans Knew
- DNC Shoots Down Resolutions Calling Out AIPAC and Limiting Arms to Israel
- TCN: Is Israel Blackmailing President Trump?
- Israel killed at least 303 Lebanese yesterday – who were they? Daily Update
- Amnesty: Urgent – Protect Lebanese civilians from brutal escalation in Israeli attacks
- Is The War Against Iran Over?
- Inside the Israeli army’s propaganda wing
- Hundreds of Gaza Amputees Stranded in Legal Limbo
- The gallows law: Israel moves toward executing Palestinian children
- Tucker Carlson: The Path to Peace requires ending ‘special alliance’ with Israel
- This is ceasefire? Israel’s biggest massacre yet in Lebanon, another journalist killed in Gaza – Daily Update
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
