California Hospital Concealed Evidence Linking ‘Catastrophic Surge’ in Stillbirths to COVID Vaccine, Lawsuit Alleges
By Brenda Baletti, Ph.D. | The Defender | August 4, 2025
A California hospital concealed data linking a “catastrophic surge” in stillbirths among women who received COVID-19 vaccines, according to a lawsuit filed last week in the Superior Court of California, Fresno County.
Michelle Spencer, a nurse at Community Medical Centers’ (CMC) Community Regional Medical Center, said the hospital “deliberately and selectively” concealed from staff, patients and regulators a spike in unborn baby deaths that began in spring 2021, and retaliated against her when she publicized the information.
The lawsuit also says the hospital concealed medical data related to the fetal deaths that showed a link to COVID-19 vaccination of pregnant mothers.
The data include hospital-wide medical records documenting the number of stillbirths and the vaccination histories of those babies’ mothers. One managing nurse at the hospital told a staff member that nearly all of the stillbirths occurred among vaccinated mothers.
According to the complaint, Spencer “witnessed firsthand the exponential increase in unborn baby deaths directly correlating with pregnant women who received a Covid vaccine and then would deliver a dead baby a close number of days or weeks following their injection.”
Spencer’s attorney, Greg Glaser, said:
“The essence of this case is that the truth shall set you free. The hospital possessed vaccinated versus unvaccinated comparison data. The numbers proved the vaccines were causing miscarriages and more in the vaccinated group.
“We know hospital management analyzed the data because they said so, and we see they concealed it from regulators because that file [requested by regulators] is empty.”
Children’s Health Defense is funding the lawsuit, which accuses the hospital of fraud, retaliation and unethical business practices.
Graphic email describes spike in ‘demise patients,’ or stillbirths
Spencer, who has been employed with the hospital since 2017, works in the antepartum, postpartum and labor and delivery units, all located on the hospital’s third floor. Before the COVID-19 vaccination rollouts, the hospital averaged one fetal death per month, she said in the lawsuit.
However, beginning in spring 2021, the number of stillbirths skyrocketed to about 20 per month, and remains at that level today, Spencer said. The number is an estimate because Spencer can’t access the hospital’s full medical records.
In September 2022, Julie Christopherson, a nurse manager specializing in perinatal care and bereavement, sent an email to the nursing and technical staff at the hospital describing the ongoing spike in stillborn babies, which she called “demise patients.”
“Well, it seems as though the increase of demise patients that we are seeing is going to continue,” Christopherson wrote. “There were 22 demises in August, which ties the record number of demises in July 2021, and so far in September there have been 7 and it’s only the 8th day of the month.”
She said the nurses hadn’t seen all of the deaths because the statistics included other units within the hospital, “but there have still been so many in our department.”
Christopherson said:
“It’s a lot of work for you as the bedside RN’s and it’s also a lot of work for me. Demises have taken a lot of my time away from the other groups of patients that I serve, so I hope this trend doesn’t continue indefinitely.
“I know of a few more that are scheduled to deliver in the week ahead, so unfortunately the process is going to be very familiar with all of you.”
According to the email, many parents requested autopsies of their babies. It also provided graphic details of the mishandling of a dead fetus, and reminded the staff of proper procedures for handling the babies’ remains and other associated biological material.
Hospital ‘aggressively’ promoted vaccines despite signs of risk, lawsuit alleges
The lawsuit alleges the spike in baby deaths began in spring 2021, as the hospital “was aggressively promoting Covid-19 vaccines to pregnant women, including requiring OBGYNs with hospital privileges (and their staff) to administer vaccines without knowing or disclosing risks or benefits.”
According to the lawsuit, Christopherson “expressed bias against unvaccinated children and their parents” and helped the hospital conceal data linking vaccines to the record-high number of stillbirths.
Nearly all of the deceased babies were born to mothers who received the COVID-19 vaccine, while the number of fetal deaths in mothers who didn’t get the vaccine remained at the pre-vaccine rollout level, averaging one per month, according to the lawsuit.
The hospital management ignored “multiple safety signals” for COVID-19 vaccine injuries among mothers and babies, according to the complaint, which states:
“Not only did the increase in unborn baby deaths occur, but mothers suddenly … began having more frequent and more significant health problems (i.e., vascular, clotting, hemorrhaging) that did not occur prior to Spring 2021 based on Plaintiff’s direct observations and conversations with colleagues. ….
“ … At the same time … the neonatal intensive care unit (NICU) on the fourth floor also experienced such dramatic spikes in injuries that the patient population nearly doubled. … From direct observation and conversations with colleagues after March 2021, Plaintiff learned of increasing numbers of babies being born at CMC with conditions such as missing fingers and toes, heart murmurs, and jaundice.”
The hospital benefited financially from promoting the vaccines, the lawsuit says, while pushing the cost of that policy on patients and healthcare professionals by refusing to investigate the COVID-19 shot as the possible cause of its increasing injury and death rates.
Hospital retaliated by withholding her bonus, Spencer said
Spencer kept a copy of Christopherson’s email, which she shared with multiple independent news sources. She also appealed to clinical supervisors to investigate whether the vaccines were linked to fetal deaths.
In response, Spencer “was gaslit by management who continued to make unsubstantiated excuses such as ‘pesticides’ as a more likely cause of the record high dead babies at CMC,” according to the lawsuit.
Spencer said she followed the standards of ethical whistleblowing and did not violate hospital rules. However, when the hospital learned she had shared the email with the media, it opened what Spencer called a “biased investigation” into her, in an attempt to silence her and other concerned colleagues.
Spencer said the hospital wasted its resources investigating her, instead of investigating the cause of the stillbirths.
She appealed to the California Department of Public Health to investigate the deaths. However, the hospital used its influence to prevent any investigation, provided false medical information to the agency regarding the number of fetal deaths, and stated COVID-19 vaccines played no role in the stillbirths, according to the lawsuit.
In December 2022, the hospital declined to pay Spencer a $5,000 retention bonus, claiming she was no longer in good standing because she was under investigation.
This sent a message to staff that “whistleblowers will be punished,” she said.
By intentionally concealing the vaccine-correlated data regarding baby deaths, the hospital prevented her from fulfilling her responsibility as a nurse to properly inform her patients of their health risks, Spencer said.
She continues working at the hospital and informs patients of the risks associated with vaccines, including the Hep B vaccine. However, she has been reprimanded for those actions.
Spencer is asking the court to compel the hospital to have a qualified third party investigate the deaths. She also seeks lost wages and punitive damages.
Spencer said she hopes her lawsuit will “expose the evil that’s going on in the hospital system,” and will “wake up parents and educate nurses.”
Glaser said:
“The hospital chose financial gain over people’s lives, and the hospital retaliated against Ms. Spencer as the nurse who blew the whistle on all of this. Our goal with the case is to give the evidence to a jury to set the truth free. Only then can we really begin to heal. And God knows we need it.”
Related articles in The Defender
- Study of 1.3 Million Women Links COVID Vaccines to Pregnancy Risk
- Study Finds 37 Safety Signals for COVID Vaccines During Pregnancy, CDC Still Urges Women to Get the Shots
- COVID Shots During Pregnancy Linked With Rise in Fetal Deaths, Leaked Emails Suggest
- Hep B Vaccines Come With High Risk, Little Benefit — Why Does CDC Recommend Them for Every Newborn?
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
HHS Cancels mRNA Vaccine Development – ‘poses more risk than benefit’ says RFK Jr
By Jefferey Jaxen | August 5, 2025
A stunning announcement from HHS Secretary RFK Jr. has set the media ablaze.
“After reviewing the science and consulting top experts at NIH and FDA, HHS has determined that mRNA technology poses more risk than benefits than these respiratory viruses.”
The official HHS press release states:
“BARDA is terminating 22 mRNA vaccine development investments because the data show these vaccines fail to protect effectively against upper respiratory infections like COVID and flu. We’re shifting that funding toward safer, broader vaccine platforms that remain effective even as viruses mutate.”
The announcement wipes out nearly $500 million worth of Covid mRNA vaccine development projects, “we’re moving beyond the limitations of mRNA and investing in better solutions” stated Kennedy in the HHS press release.
Kennedy’s announcement comes after months of outside pressure to wind down the Covid mRNA vaccine platform in the U.S.
In May 2025, RFK Jr. removed COVID-19 vaccines from the list of routine immunizations for healthy pregnant women and children.
HHS and America now have pressing work at hand to undue the damage of the rushed and forced mRNA vaccine platform.
World-leading cancer researcher Dr. Patrick Soon-Shiong recently stated in an interview: “This non-infectious pandemic of cancer is sadly upon us” referring to how both the virus and the vaccine can awaken sleeping cancer cells in the body. A topic mainstream science is just now, after years of alternative researchers and journalists banging the drum, beginning to admit and study. The new study in the journal Nature chronicles how it is actually the immune system’s response to the lab created gain-of-function bioweapon (and the mRNA shot as we have pointed out) that down-regulates and allows for accelerated cancer progression.
Kennedy has signaled over the last month that he is now taking aim at the broken vaccine injury compensation in the United States.
America, and other countries that align with our mission, must now develop a Manhattan Project-level effort to reverse the many harms brought about by the lab-constructed virus and the shot we were falsely told would save us from it.
FDA stalls decision on petition to suspend mRNA injections, citing ‘other priorities’
US regulator quietly delays action despite evidence of regulatory failure, DNA contamination, and a surge in cancers among young people.
By Maryanne Demasi, PhD | July 19, 2025
The U.S. Food and Drug Administration (FDA) has delayed its response to a formal petition demanding the suspension of the mRNA Covid-19 injections, citing “the existence of other FDA priorities.”
In a letter dated 17 July 2025, Dr Vinay Prasad—recently appointed Director of the FDA’s Center for Biologics Evaluation and Research (CBER)—acknowledged that the agency had “not yet reached resolution of the issues raised” in the petition.
Filed on 20 January 2025, the petition alleges that Pfizer’s Comirnaty and Moderna’s Spikevax were “unlawfully approved” in violation of federal regulatory requirements.
It calls for an immediate halt to the injections, independent testing of retained vials, and a full investigation into the approval process.
Fatal flaws in licensing mRNA products
Submitted by lawyer Katie Ashby-Koppens of PJ O’Brien & Associates, and spearheaded by former barrister Julian Gillespie, the petition argues that the mRNA injections were misclassified from the outset.
Although the products meet the FDA’s own definition of gene therapy, they were not regulated as such—sidestepping the heightened oversight normally required for gene-based interventions.
Under U.S. law, gene therapies must undergo ‘Environmental Assessments,’ be reviewed by specialised advisory committees, and face a more rigorous public transparency process.
But by labelling the mRNA injections as conventional ‘vaccines,’ regulators were able to fast-track their approval through a separate, less stringent pathway—bypassing critical safeguards.
The petition also raises alarm over synthetic DNA fragments found in the final products. Independent testing by multiple laboratories—including the FDA’s own facility—revealed DNA contamination far exceeding the safety limits.
Because the DNA is encapsulated in lipid nanoparticles, it can bypass normal immune defences, enter human cells, and in some cases integrate into the genome. The potential consequences, the petition warns, include genomic instability, cancer, and heritable genetic damage.
One of the most serious findings is the presence of SV40 promoter sequences in Pfizer’s injection—elements known to interfere with tumour-suppressing pathways such as p53.
The petition accuses Pfizer of withholding this information from the FDA in breach of disclosure laws.
Interim letter, no timeline
Under federal law, the FDA was required to respond to the petition within 180 days.
Just before the deadline, it issued a standard interim letter—acknowledging the petitioners’ main concerns but offering no timeline for a final decision.
Nor did the agency indicate that any investigation had begun. “We will respond to your petition as soon as we have reached a decision on your request,” wrote Prasad.
The agency’s delay is not uncommon—but critics say it reflects a deeper reluctance to confront the scientific and regulatory implications head-on.
Fully addressing the petition would require a sweeping and uncomfortable re-evaluation of how mRNA technologies were developed, approved, and marketed under the guise of conventional ‘vaccines.’
If the products were unlawfully licensed—mislabelled as vaccines to circumvent gene therapy regulations—the fallout would be unprecedented.
The admission alone could expose governments to extraordinary legal and financial liability—including product withdrawals, class actions, long-term health monitoring, injury compensation, and potential criminal investigations.
Petitioners speak out
Gillespie said the FDA is caught “between a rock and a hard place”—but that doesn’t excuse inaction. He believes the recent surge in cancers among young people demands urgent scrutiny.
“There’s been a tremendous and continuing rise in cancers across the United States commensurate with the rollout of these products,” he said. “Government officials have seen the data… and are refusing to address the elephant in the room.”
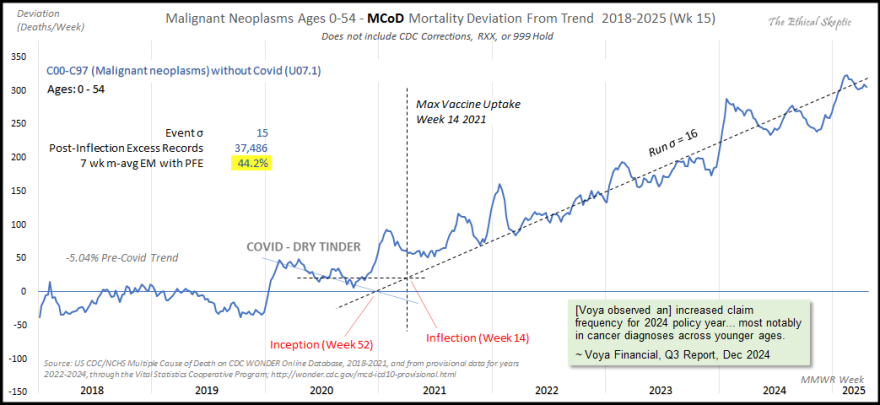
Analysis by Ethical Skeptic shows young cancers are up by 44%
Dr Jessica Rose, a computational biologist and co-author of the petition, said the public was never given accurate information about the nature of the products.
“The public was not told what they were being injected with,” she said. “And still to this day, they are not.”
She described the failure to distinguish gene-based therapies from traditional vaccines as “an existential crisis,” warning that “more and more people—including children and infants—are being exposed to the harms of foreign DNA.”
Dr David Speicher, a virologist and co-signatory on the petition, said the FDA’s letter amounts to bureaucratic minimisation.
“The number of vaccine-injured people continues to grow, and we do not all know the long-term harms caused by these genetic products,” he said. “Yet the FDA states that ‘other priorities’ are more important.”
He called for “an independent scientific team to examine the regulatory process, as well as to provide funding to researchers to explore biological mechanisms such as genomic integration.”
Pharmacy consultant and petitioner Maria Gutschi said the mRNA products represent a new therapeutic category “with no previous knowledge to leverage in assessing safety and efficacy.”
She argued that, given the novelty and risks, “the bar to suspend and/or mandate ‘black box’ warnings must be higher than for any previous therapeutic agent.” Gutschi urged the FDA to treat this as “THE priority” going forward.
A tale of two gene therapies
Critics say the FDA’s handling of mRNA harms stands in stark contrast to its swift response to safety concerns involving other gene therapies.
Yesterday, the agency announced a halt to clinical trials for Sarepta Therapeutics’ investigational gene therapy after the company reported another patient death—bringing the total to three deaths across two separate gene therapy products.
The treatment, developed for limb girdle muscular dystrophy, prompted immediate regulatory action.
“Today, we’ve shown that this FDA takes swift action when patient safety is at risk,” said FDA Commissioner Marty Makary, declaring the agency is “not afraid to take immediate action when a serious safety signal emerges.”
In contrast, the FDA has remained inert on mRNA injections—which also deliver genetic material into human cells but were classified as “vaccines”—despite thousands of reported deaths and serious adverse events following administration.
According to the petitioners, the public was led to believe they were receiving a conventional vaccine—when in fact, they were being administered gene therapy.
By failing to recognise and regulate the products accordingly, the FDA violated public trust—bypassing transparency laws, concealing critical risks, and depriving individuals of the opportunity to make informed medical decisions.
Next steps
People don’t want agencies to stall. They don’t want bureaucratic evasions. They want answers—and they want accountability.
The FDA’s next move won’t simply test regulatory process.
It will test courage—whether anyone inside the system is willing to confront the fallout in what may be the most consequential medical misclassification in modern history.
Massie Proposes to Make COVID Vaccine Makers Liable for Injuries, Opening Door for Thousands of Lawsuits
By Michael Nevradakis, Ph.D. | The Defender | July 16, 2025
Rep. Thomas Massie (R-Ky.) on Tuesday introduced legislation to repeal the “sweeping” liability shield that exempts COVID-19 vaccine manufacturers from responsibility for serious injuries or death caused by their products.
The liability protection amounts to “medical malpractice martial law,” Massie said in a press release.
The PREP Repeal Act (H.R.4388) would revoke the Public Readiness and Emergency Preparedness (PREP) Act of 2005, a law that provides legal immunity to “covered persons” who manufacture or administer countermeasures during a public health emergency.
“Covered persons” under the PREP Act include vaccine makers, manufacturers of masks and other personal protective equipment, and physicians, nurses and pharmacists who administer vaccines.
The Biden administration ended the COVID-19 public health emergency in May 2023. However, the public health emergency, declared in January 2020 by the U.S. Department of Health and Human Services (HHS) under the PREP Act, remains in effect.
In December 2024, HHS extended the liability protections through 2029. It was the 12th extension since 2020.
Massie’s bill would strip away these protections, repealing the PREP Act’s liability shield and restoring civil remedy rights for people harmed by products covered under the act.
“Τhe ability of citizens to seek redress for injury or harm is a fundamental principle of justice and due process,” the bill states, adding that the PREP Act’s liability shield has “undermined public trust and accountability” and “enabled regulatory capture.”
“The 2005 PREP Act prevents people from holding corporations accountable for the pain and suffering they cause during Presidentially declared emergencies. Americans deserve the right to seek justice when injured by government-mandated products. The PREP Repeal Act will restore that right,” Massie said in the press release.
In an interview today on the “Brian Thomas Morning Show,” Massie said the bill would apply to all COVID-19-related countermeasures, not just vaccines.
“If somebody made a mask that had cancer particles on it, and you inhaled those … too bad, they’re covered by the PREP Act,” Massie said. “I don’t like lawsuits, but they do keep corporations sort of in check. There’s this incentive not to harm people if you’re going to have to pay for it, if it becomes unprofitable.”
Attorney Ray Flores, senior outside counsel for Children’s Health Defense and an expert on the PREP Act, said:
“The ‘sweeping liability protections’ extend far beyond manufacturer shields to condone every conceivable medical atrocity. If Massie’s bill passes, the pandemic assembly line would be dismantled. It would be goodbye liability protections, goodbye mandates and goodbye mass-human experimentation.”
According to Flores, repeal of the PREP Act would also end other current public health emergencies, including mpox (monkeypox), pandemic influenza, anthrax and Zika.
Dr. Meryl Nass, founder of Door to Freedom, said the bill “will stop another COVID vaccine fiasco and also stop the widespread use of unproven tests such as the COVID-19 PCR tests, which were also issued under emergency use authorizations (EUA).”
Wayne Rohde, author of “The Vaccine Court: The Dark Truth of America’s Vaccine Injury Compensation Program” and “The Vaccine Court 2.0,” said the bill contains “nonspecific language” and gaps that require attention. Rohde said this includes:
“How to wind down the Act, address all of the amendments added to the Act over the last 4 years, covered persons, how to handle the covered countermeasures such as medical devices, medications, drugs and personal protective equipment, and, of course, the elephant in the room, the vaccines used and their future legal liability.”
Legislation would open the door to thousands of lawsuits previously blocked by PREP Act
Massie’s proposed legislation would apply to all current and future lawsuits challenging the PREP Act, including pending appeals.
Attorney Rick Jaffe said the proposed legislation is retroactive to March 10, 2020, “reopening the courthouse doors to thousands of injured individuals whose claims were previously blocked by PREP’s sweeping liability shield.”
The legislation would allow claimants to sue COVID-19 vaccine makers directly, Jaffe said:
“The bill, if passed, allows people injured by the COVID shots to sue, presumably, the manufacturers as well as those who administered the shots, and that would be a big and much unwanted thing from the perspective of the manufacturers and pharmacy chains which administered the shots.”
Massie told Brian Thomas he believes the PREP Act is unconstitutional, as it preempts state medical malpractice laws.
“Here’s why I call the PREP Act medical malpractice martial law,” Massie said. “It’s a federal law that says none of the state laws apply, and I think it’s a violation of the 10th Amendment. There’s nowhere in the Constitution that lets the federal government say that all state laws dealing with liability are null and void.”
Most, but not all, courts have so far sided against vaccine injury lawsuits challenging the PREP Act’s liability shield.
In March, the Maine Supreme Judicial Court upheld a lower court ruling that school medical staff who gave a COVID-19 vaccine to a minor without obtaining parental consent cannot be held liable under the PREP Act.
The Maine ruling came one week after the U.S. Supreme Court refused to review a lower court’s ruling in a similar lawsuit in Vermont. In that case, a school administered a COVID-19 vaccine to a 6-year-old boy despite his and his parents’ objections. Last year, the Vermont Supreme Court ruled that the PREP Act shielded school officials from liability.
At least two recent lawsuits challenging the PREP Act have cleared initial judicial hurdles but remain pending.
In March, the Supreme Court of North Carolina ruled that a lawsuit filed by the mother of a 14-year-old boy given a COVID-19 vaccine at school without consent can proceed. The court ruled the PREP Act does not preempt state law requiring parental consent for vaccination.
In November 2024, a federal court ruled that a lawsuit filed by a woman injured by AstraZeneca’s COVID-19 vaccine during a U.S. clinical trial can continue.
According to the complaint, AstraZeneca’s consent form for trial participants promised enrollees medical treatment in the event of illness or injury suffered during the study. The court rejected the drugmaker’s claim that a federal liability shield protects it from breach-of-contract claims.
Bill would end ‘dismal’ PREP Act vaccine injury compensation program
Massie’s proposed bill also rescinds unused federal funds earmarked for injury claims under the PREP Act.
Such claims are heard by the Countermeasures Injury Compensation Program (CICP), a government-run COVID-19 vaccine injury compensation program established under the PREP Act.
CICP has faced criticism for its slow pace of resolving claims and the limited compensation it offers.
Jaffe said:
“The PREP Act created a legal black hole where traditional tort rights and due process protections disappeared, replaced by a virtually unreviewable administrative compensation program — the CICP — that has denied nearly every COVID-related claim. In effect, Americans injured by federally endorsed products were stripped of their constitutional right to seek redress. This bill restores that right.”
According to the most recent CICP data, of the 13,836 claims related to COVID-19 countermeasures filed to date, 75 were found eligible for compensation. As of June 1, 39 of those have been compensated. The overwhelming majority of claims were denied (4,338) or are “pending review or in review” (9,423).
Dr. Joel Wallskog, an orthopedic surgeon injured by COVID-19 vaccines and co-chair of React19, an organization advocating on behalf of vaccine-injury victims, said CICP strips claimants of their constitutional rights to due process and a jury trial.
“The CICP program was intended to be the safety net for those Americans injured by the emergency countermeasures, such as the COVID-19 shots. However, the program is a dismal failure with over a 98% denial rate,” Wallskog said.
If the proposed legislation passes, Flores said, the most likely outcome would be attempting to move COVID-19 injuries into the National Vaccine Injury Compensation Program (VICP), which covers injuries from vaccines routinely administered to children and pregnant women.
However, such a move may face obstacles, including complications regarding how to handle claims pending before the CICP.
Rohde said:
“Money obligated for current operations would not be affected [but] how do you determine the monetary need for pending CICP petitions? How to handle the CICP petitions already received and what about the future claims? Do you move all the CICP vaccine petitions into the VICP? That creates all sorts of new problems.”
In May, the Centers for Disease Control and Prevention (CDC) changed its recommendations on COVID-19 vaccines for healthy children. The CDC now recommends that parents of healthy children consult their pediatricians and together make decide whether to vaccinate against the virus.
According to Flores, “Now that these injections are not on the routine recommended schedule for healthy children and pregnant women, they wouldn’t qualify” for compensation from the VICP.
‘It will probably only pass if Americans get behind it in a big way’
Massie’s proposed legislation is similar to a bill introduced last year that would allow Americans to sue the manufacturers of COVID-19 vaccines for vaccine-related adverse events, including deaths, by removing the vaccine makers’ liability shield.
The Let Injured Americans Be Legally Empowered Act, or the LIABLE Act (H.R.7551), has since languished in the U.S. House of Representatives.
Wallskog said Massie’s bill faces “an uphill battle to make it to the Congressional floor and get to a vote.”
Flores was less optimistic about the bill’s future because it would allow claimants to sue COVID-19 vaccine manufacturers directly.
“The bill, in theory, is just what we need. However, implementing it would cause utter chaos,” Flores said. “Absent a miracle, the prospects [of passage] are slim to none.”
Nass said public awareness and support are crucial for the bill’s success.
“It will probably only pass if Americans get behind it in a big way,” Nass said.
Wallskog said if the legislation is passed, it would be more far-reaching than a declaration by Health Secretary Robert F. Kennedy Jr. removing COVID-19 countermeasures from the PREP Act.
“Executive orders can simply be reversed by the next HHS secretary. Legislative change is much more powerful with more staying power,” Wallskog said.
This has not occurred to date, which Flores said is “the greatest indication of the forces that Kennedy and Rep. Massie are up against.”
Related articles in The Defender
- COVID Vaccine Makers Get Another Free Pass as Biden Administration Extends Liability Shield Through 2029
- Exclusive: Public Health Emergency in U.S. Set to Expire May 11 — But EUA Vaccines, Liability Shields Aren’t Going Away Anytime Soon
- Nearly 10,000 Claims Pending as COVID Vaccine Injury Compensation Program Faces Possible Budget Cut
- New Law Would Make COVID Vaccine Makers Liable for Injuries, Deaths
- Liability-Free COVID Vaccine Makers Seek Additional ‘Free Pass’ From FDA
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Net Zero: The Mystery of the Falling Fertility
By Tomas Furst | Brownstone Institute | July 8, 2025
In January 2022, the number of children born in the Czech Republic suddenly decreased by about 10%. By the end of 2022, it had become clear that this was a signal: All the monthly numbers of newborns were mysteriously low.
In April 2023, I wrote a piece for a Czech investigative platform InFakta and suggested that this unexpected phenomenon might be connected to the aggressive vaccination campaign that had started approximately 9 months before the drop in natality. Denik N – a Czech equivalent of the New York Times – immediately came forward with a “devastating takedown” of my article, labeled me a liar and claimed that the pattern can be explained by demographics: There were fewer women in the population and they were getting older.
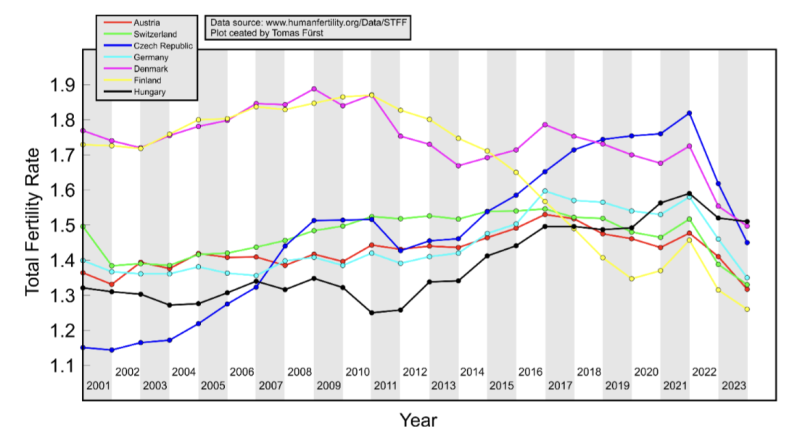
To compare fertility across countries (and time), the so-called Total Fertility Rate (TFR) is used. Roughly speaking, it is the average number of children that are born to a woman over her lifetime. TFR is independent of the number of women and of their age structure. Figure 1 below shows the evolution of TFR in several European countries between 2001 and 2023. I selected countries that experienced a similar drop in TFR in 2022 as the Czech Republic.
So, by the end of 2023, the following two points were clear:
- The drop in natality in the Czech Republic in 2022 could not be explained by demographic factors. Total fertility rate – which is independent of the number of women and their age structure – dropped sharply in 2022 and has been decreasing ever since. The data for 2024 show that the Czech TFR has decreased further to 1.37.
- Many other European countries experienced the same dramatic and unexpected decrease in fertility that started at the beginning of 2022. I have selected some of them for Figure 1 but there are more: The Netherlands, Norway, Slovakia, Slovenia, and Sweden. On the other hand, there are some countries that do not show a sudden drop in TFR, but rather a steady decline over a longer period (e.g. Belgium, France, UK, Greece, or Italy). Notable exceptions are Bulgaria, Spain, and Portugal where fertility has increased (albeit from very low numbers). The Human Fertility Project database has all the numbers.
This data pattern is so amazing and unexpected that even the mainstream media in Europe cannot avoid the problem completely. From time to time, talking heads with many academic titles appear and push one of the politically correct narratives: It’s Putin! (Spoiler alert: The war started in February 2022; however, children not born in 2022 were not conceived in 2021). It’s the inflation caused by Putin! (Sorry, that was even later). It’s the demographics! (Nope, see above, TFR is independent of the demographics).
Thus, the “v” word keeps creeping back into people’s minds and the Web’s Wild West is ripe with speculation. We decided not to speculate but to wrestle some more data from the Czech government. For many months, we were trying to acquire the number of newborns in each month, broken down by age and vaccination status of the mother. The post-socialist health-care system of our country is a double-edged sword: On one hand, the state collects much more data about citizens than an American would believe. On the other hand, we have an equivalent of the FOIA, and we are not afraid to use it. After many months of fruitless correspondence with the authorities, we turned to Jitka Chalankova – a Czech Ron Johnson in skirts – who finally managed to obtain an invaluable data sheet.
To my knowledge, the datasheet (now publicly available with an English translation here) is the only officially released dataset containing a breakdown of newborns by the Covid-19 vaccination status of the mother. We requested much more detailed data, but this is all we got. The data contains the number of births per month between January 2021 and December 2023 given by women (aged 18-39) who were vaccinated, i.e., had received at least one Covid vaccine dose by the date of delivery, and by women who were unvaccinated, i.e., had not received any dose of any Covid vaccine by the date of delivery.
Furthermore, the numbers of births per month by women vaccinated by one or more doses during pregnancy were provided. This enabled us to estimate the number of women who were vaccinated before conception. Then, we used open data on the Czech population structure by age, and open data on Covid vaccination by day, sex, and age.
Combining these three datasets, we were able to estimate the rates of successful conceptions (i.e., conceptions that led to births nine months later) by preconception vaccination status of the mother. Those interested in the technical details of the procedure may read Methods in the newly released paper. It is worth mentioning that the paper had been rejected without review in six high-ranking scientific journals. In Figure 2, we reprint the main finding of our analysis.
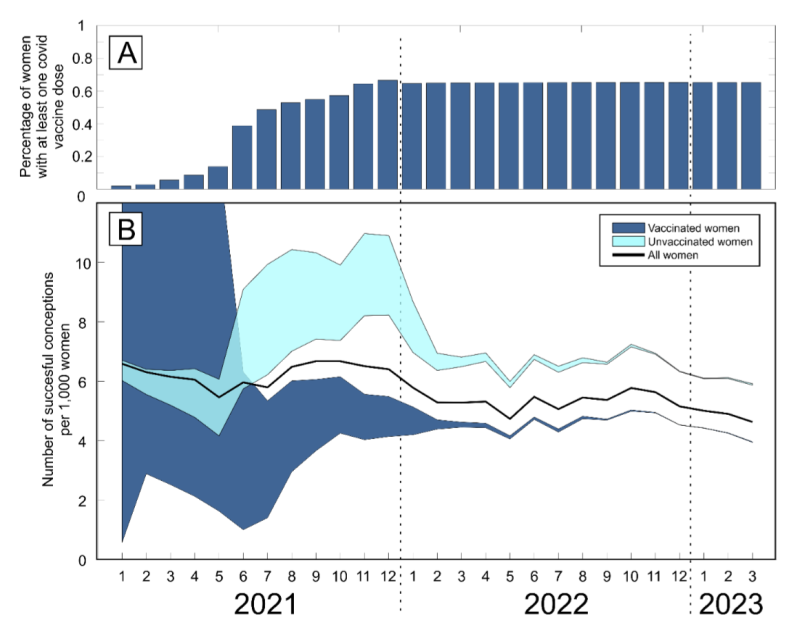
Figure 2 reveals several interesting patterns that I list here in order of importance:
- Vaccinated women conceived about a third fewer children than would be expected from their share of the population. Unvaccinated women conceived at about the same rate as all women before the pandemic. Thus, a strong association between Covid vaccination status and successful conceptions has been established.
- In the second half of 2021, there was a peak in the rate of conceptions of the unvaccinated (and a corresponding trough in the vaccinated). This points to rather intelligent behavior of Czech women, who – contrary to the official advice – probably avoided vaccination if they wanted to get pregnant. This concentrated the pregnancies in the unvaccinated group and produced the peak.
- In the first half of 2021, there was significant uncertainty in the estimates of the conception rates. The lower estimate of the conception rate in the vaccinated was produced by assuming that all women vaccinated (by at least one dose) during pregnancy were unvaccinated before conception. This was almost certainly true in the first half of 2021 because the vaccines were not available prior to 2021. The upper estimate was produced by assuming that all women vaccinated (by at least one dose) during pregnancy also received at least one dose before conception. This was probably closer to the truth in the second part of 2021. Thus, we think that the true conception rates for the vaccinated start close to the lower bound in early 2021 and end close to the upper bound in early 2022. Once again, we would like to be much more precise, but we have to work with what we have got.
Now that the association between Covid-19 vaccination and lower rates of conception has been established, the one important question looms: Is this association causal? In other words, did the Covid-19 vaccines really prevent women from getting pregnant?
The guardians of the official narrative brush off our findings and say that the difference is easily explained by confounding: The vaccinated tend to be older, more educated, city-dwelling, more climate change aware…you name it. That all may well be true, but in early 2022, the TFR of the whole population dropped sharply and has been decreasing ever since.
So, something must have happened in the spring of 2021. Had the population of women just spontaneously separated into two groups – rednecks who wanted kids and didn’t want the jab, and city slickers who didn’t want kids and wanted the jab – the fertility rate of the unvaccinated would indeed be much higher than that of the vaccinated. In that respect, such a selection bias could explain the observed pattern. However, had this been true, the total TFR of the whole population would have remained constant.
But this is not what happened. For some reason, the TFR of the whole population jumped down in January 2022 and has been decreasing ever since. And we have just shown that, for some reason, this decrease in fertility affected only the vaccinated. So, if you want to argue that a mysterious factor X is responsible for the drop in fertility, you will have to explain (1) why the factor affected only the vaccinated, and (2) why it started affecting them at about the time of vaccination. That is a tall order. Mr. Occam and I both think that X = the vaccine is the simplest explanation.
What really puzzles me is the continuation of the trend. If the vaccines really prevented conception, shouldn’t the effect have been transient? It’s been more than three years since the mass vaccination event, but fertility rates still keep falling. If this trend continues for another five years, we may as well stop arguing about pensions, defense spending, healthcare reform, and education – because we are done.
We are in the middle of what may be the biggest fertility crisis in the history of mankind. The reason for the collapse in fertility is not known. The governments of many European countries have the data that would unlock the mystery. Yet, it seems that no one wants to know.
Court Orders Bank Freezing Records in Freedom Convoy Case
By Cindy Harper | Reclaim The Net | July 9, 2025
A Canadian court has ordered the release of documents that could shed light on how federal authorities and law enforcement worked together to freeze the bank accounts of a protester involved in the Freedom Convoy.
Both the RCMP and TD Bank are now required to provide records related to Evan Blackman, who took part in the 2022 demonstrations and had his accounts frozen despite not being convicted of any crime at the time.
The Justice Centre for Constitutional Freedoms (JCCF) announced the Ontario Court of Justice ruling. The organization is representing Blackman, whose legal team argues that the actions taken against him amounted to a serious abuse of power.
“The freezing of Mr. Blackman’s bank accounts was an extreme overreach on the part of the police and the federal government,” said his lawyer, Chris Fleury. “These records will hopefully reveal exactly how and why Mr. Blackman’s accounts [were] frozen.”
Blackman was arrested during the mass protests in Ottawa, which drew thousands of Canadians opposed to vaccine mandates and other pandemic-era restrictions.
Although he faced charges of mischief and obstructing police, those charges were dismissed in October due to a lack of evidence. Despite this, prosecutors have appealed, and a trial is set to begin on August 14.
At the height of the protests, TD Bank froze three of Blackman’s accounts following government orders issued under the Emergencies Act. Then-Prime Minister Justin Trudeau had invoked the act to grant his government broad powers to disrupt the protest movement, including the unprecedented use of financial institutions to penalize individuals for their support or participation.
In 2024, a Federal Court Justice ruled that Trudeau’s decision to invoke the act had not been justified.
Blackman’s legal team plans to use the newly released records to demonstrate the extent of government intrusion into personal freedoms. According to the JCCF, this case may be the first in Canada where a criminal trial includes a Charter challenge over the freezing of personal bank accounts under emergency legislation.
Von der Leyen blames Russia for no-confidence motion

RT | July 8, 2025
European Commission President Ursula von der Leyen has dismissed efforts by members of the European Parliament to oust her, branding her critics “conspiracy theorists” and accusing them of acting on behalf of Russian President Vladimir Putin.
Von der Leyen is facing a parliamentary motion of no-confidence in her presidency, which is scheduled for a vote on Thursday after being tabled by Romanian MEP Gheorghe Piperea. Addressing the parliament during a debate on Monday, von der Leyen said those backing the proposal were following “the oldest playbook of extremists” and were attempting to undermine public confidence in the EU with “false claims.”
“There is no proof that they have any answers, but there is ample proof that many are supported by our enemies and by their puppet masters in Russia or elsewhere.”
“These are movements fueled by conspiracies, from anti-vaxxers to Putin apologists. And you only have to look at some of the signatories of this motion to understand what I mean.”
In his remarks to parliament, Piperea accused the Commission of centralizing decision-making in a non-democratic fashion and of interfering in the internal affairs of member states.
Russian officials have claimed that EU leaders are using fear tactics to shield themselves from criticism. Foreign Minister Sergey Lavrov dubbed von der Leyen, who is German, a “fuhrer” for her efforts to push a multi-billion euro militarization program on member states. Russia maintains that unlike Western states it does not interfere with other nations’ domestic affairs.
Von der Leyen urged “all the pro-Europeans, pro-democracy forces” in the chamber to support her agenda, arguing that unity was essential to uphold the EU’s foreign policy strength.
Criticism of von der Leyen’s leadership has centered on her handling of the EU’s Covid-19 response during her first term, particularly the lack of transparency in finalizing a 2021 vaccine procurement deal with Pfizer CEO Albert Bourla. Earlier this year, the European Court of Justice found her office at fault for failing to retain text messages exchanged with Bourla and for refusing to release them to journalists with adequate justification.
Piperea is a member of Romania’s AUR party, led by George Simion, who narrowly lost a presidential runoff this year to a pro-EU candidate. The election followed a scrapped first-round vote earlier in 2024, in which outsider Calin Georgescu emerged as the frontrunner. The country’s Constitutional Court annulled the results, citing government allegations of Russian interference. Critics of the EU claim the episode reflects a broader anti-democratic trend allegedly enabled by Brussels.
“Why Can’t We Talk About This?”
Rainey Media TV | June 4, 2025
Please Support Our Film via: E-Transfer: dean_rainey@yahoo.ca
PAYPAL: deanrainey@raineymedia.com
Buy My A Coffee: https://buymeacoffee.com/raineymedia
SNAIL MAIL: Rainey Media, PO Box 5, Delhi PO Main, ON, N4B 2W8 Canada
To book your own screening: deanrainey@raineymedia.com
“Why Can’t We Talk About This?” delves into the life of a man grappling with the aftermath of a COVID-19 vaccine injury, weaving his personal struggle into a broader examination of why such experiences are rarely discussed.
To help Michael via support: https://www.gofundme.com/f/benefit-fo…
We’ve made this film easily accessible for everyone because the information it contains and the discussion it starts is just too important. This film had no funding and was made without sponsorship. All costs were paid out of my own pocket. My team and I spent over a year and a half making this film. Any support you give will go towards expenses incurred making and marketing the movie. (Even sending the price of a movie ticket would help.) Once we cover those costs, we will be providing Michael with a share of the proceeds.
To order DVDs of this film, visit: https://raineymedia.com/video-store/
Also available on Rumble.
After Years of Silence, New CDC Vaccine Panel to Vote on Mercury in Flu Shots
By Suzanne Burdick, Ph.D. | The Defender | June 18, 2025
The CDC’s vaccine advisory committee will vote next week on the mercury-based flu vaccine, according to an Advisory Committee on Immunization Practices (ACIP) meeting agenda draft posted today on the ACIP website
The committee will also vote on RSV vaccines for pregnant mothers, babies and young children.
This will be the first meeting since U.S. Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. tapped eight new ACIP members — just days after removing all 17 former members in what he called a “clean sweep … needed to re-establish public confidence in vaccine science.”
Before they vote, ACIP members will hear presentations on respiratory syncytial virus, or RSV vaccines, including Merck’s new RSV shot for newborns. Last week, the U.S. Food and Drug Administration (FDA) approved the new shot, even though clinical trials showed an 11.71% rate of serious adverse events, including death.
Discussions, but no votes, are slated for other vaccines, including COVID-19, Chikungunya, Anthrax and MMRV (Measles, Mumps, Rubella, Varicella).
ACIP decides which vaccines should be recommended to the public, who should take them and how often — recommendations the Centers for Disease Control and Prevention (CDC) typically rubber stamps and publishes on its immunization schedules.
The committee will meet June 25-26 in Atlanta, Georgia.
ACIP to discuss thimerosal after years of silence
Thimerosal is a mercury-based preservative used in multi-dose vials of the flu vaccine, according to the CDC. Most single-dose vials and pre-filled syringes of the flu shot don’t contain the preservative, as they’re intended for single use.
Over 25 years ago, vaccine industry leaders and public health officials concealed evidence from the CDC’s own database that linked thimerosal to neurodevelopmental disorders in children, including autism, according to transcripts from a meeting in Norcross, Georgia.
The U.S. government has long said thimerosal poses no harm to children. However, in 2001, out of what the agency said was an abundance of caution, the CDC said the ingredient would no longer be used in childhood vaccines.
A recent investigation by journalist Sharyl Attkisson proved both statements untrue.
Thimerosal’s potential to harm kids has been on Kennedy’s radar for over a decade. In 2014, he edited a book on the topic: “Thimerosal: Let the Science Speak: The Evidence Supporting the Immediate Removal of Mercury — a Known Neurotoxin — from Vaccines.”
The CDC webpage for flu shot safety considerations during pregnancy makes no mention of thimerosal, nor does it encourage pregnant women to be sure they get a flu shot from a single-dose vial or prefilled syringe to avoid mercury exposure.
Next week, ACIP members will hear a presentation on thimerosal in vaccines and a presentation on proposed recommendations for flu vaccines that contain thimerosal. The names of the presenters were not listed on the agenda at press time.
The committee will also vote on flu vaccines that don’t contain thimerosal.
Dr. Meryl Nass, who has attended many past ACIP meetings, said, “There is no need for thimerosal, a known neurotoxin, as it is not used in single-dose vials. Its use should be ended.”
Critics weigh in on ACIP agenda
Reactions to the ACIP meeting agenda were mixed. Some said it signaled that the CDC is veering off course, while others called for even more change.
Brian Hooker, Ph.D., Children’s Health Defense’s (CHD) chief scientific officer, said that although he was encouraged by Kennedy’s selections for the new ACIP members, he was disappointed in the slate of meeting presenters and moderators.
“It is the same old cast of CDC characters (from the National Center for Infectious and Respiratory Diseases) who present a very biased viewpoint,” Hooker said. “CDC’s culture is vaccinology as a religion, straight up. ACIP committee members desperately need an alternative view that is based on the very stark reality of vaccine ineffectiveness and the extremely high prevalence of vaccine adverse events.”
Dr. Jeremy Faust, editor of Medpage, said in a Substack post critiquing the ACIP meeting agenda that the planned vote on thimerosal “revives and elevates a longstanding anti-vaccine conspiracy theory.”
“Removing the compound will do nothing to improve vaccine safety,” Faust wrote, “but it certainly will undermine confidence in other existing vaccines.”
Faust also criticized the CDC for failing to put a COVID-19 vaccine vote on the meeting agenda, writing that the move will leave “fall policies unclear.”
HHS officials last month removed the COVID-19 shot from the CDC’s recommended list of immunizations for healthy children and pregnant women after the FDA limited its COVID-19 vaccine approvals to high-risk groups and the elderly.
‘This could mark a turning point’
James Lyons-Weiler, Ph.D. is president and CEO of the Institute for Pure and Applied Knowledge, an advocacy group that pushes for accuracy and integrity in science and for biomedical researchers to put people’s health before profits. He said the ACIP meeting agenda suggested that the CDC was making progress in “structure, balance, and transparency.”
“If public comment is taken seriously and if safety data are rigorously and honestly evaluated — then this could mark a turning point,” Lyons-Weiler said.
Lyons-Weiler said it’s also important that the CDC be “fully open” about its Evidence to Recommendations framework.
When ACIP makes a vaccine recommendation, it’s accompanied by what’s called an Evidence to Recommendations framework that describes the information the committee used in making its decision.
In the past, the CDC took shortcuts in showing this evidence, Lyons-Weiler said. He said he hopes the next ACIP meeting shows that the CDC is moving forward “with the full light of science, skepticism, and civic trust.”
ACIP guidelines don’t address full scope of possible vaccine injuries
Historically, states use ACIP recommendations to help shape vaccine policy and doctors use them in making decisions.
Some states consider the ACIP’s “General Best Practice Guidelines for Immunization,” which lists examples of contraindications and precautions for each vaccine, as the only acceptable authority when deciding whether to grant a child’s medical exemption request to a school-required vaccine.
However, ACIP’s list of contraindications isn’t exhaustive, according to attorney Sujata Gibson, who said:
“Right now, states like New York and California are overruling treating physicians and rejecting medical exemptions when they don’t see the condition listed in the ACIP best practices guideline as a contraindication or a precaution.
“But the guideline doesn’t provide an exhaustive list of all the reasons a child may be at risk of serious harm… The way that New York, California and other states are treating these guidelines is reckless and dangerous, and children are being severely harmed as a result.”
In other words, it doesn’t matter how many doctors confirm that a particular child will likely be harmed by a certain vaccine, states like New York and California give medical exemptions only for conditions specified in ACIP’s guidelines.
The Defender reached out to the CDC to ask if the new ACIP committee will clarify that its guidance is not a substitute for clinical decision-making and should not be used as a standard for clinicians or schools in deciding whether to grant medical exemptions. The CDC did not respond by the deadline.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Did Covid Vaccines Really Save Millions?
By Yaakov Ophir | Brownstone Institute | June 21, 2025
Two years have passed since the official end of the Covid-19 pandemic, yet the topic of vaccination remains highly sensitive in both public and scientific discourse. Attempts to question the legitimacy of the mass vaccination campaign or to raise concerns about potential harms are often met with a moral red line: the widely repeated claim that “Covid-19 vaccines have saved millions and millions of lives.”
Remarkably, this assertion was treated as established fact even during the recent U.S. Senate PSI hearing on May 21, 2025, which focused on vaccine-related adverse outcomes.1 Ranking Member Richard Blumenthal opened the hearing with the following statement:
“As we talk about the side effects of COVID vaccines, I think we need to be clear about the most important fact. For all Americans, COVID-19 vaccines have saved millions and millions of lives. There is no scientific question about that fact… One study found that 3 million American deaths were averted…in the United States… I would like this study entered into the record.1
This confident assertion raises a fundamental question: Is there truly solid and conclusive scientific evidence to support the powerful claim that the Covid-19 mass vaccination campaign resulted in a net benefit of millions of lives saved?
Faced with this fundamental question, our research team undertook a structured, step-by-step evaluation of the empirical foundations of the “millions saved” narrative. Building on our prior work,2, 3 we critically examined the hypothetical statistical models that produced this extraordinary figure, as well as multiple randomized controlled trials and large-scale observational studies that served as the empirical basis for the vaccine efficacy estimates fed into these models.
We have now uploaded our full-length article with what we believe to be urgently important findings to a preprint server,4 in order to allow scientists, physicians, and policymakers to independently evaluate the evidence. Because meaningful scientific discourse requires careful scrutiny of the data, we strongly urge readers not to rely solely on the current brief article, but to engage directly with the full analysis presented in our preprint.4
Our goal here is to highlight several central findings that, in our view, demand serious attention, given their direct relevance to one of the most significant public health interventions in modern history: a global, government-backed mass vaccination campaign that, in many countries, was accompanied by mandates and unprecedented restrictions on individual freedoms.
What follows is a concise overview of key insights from our structured analysis that, in our view, every health professional, policymaker, and citizen deserves to consider:
- The widely cited claim that “millions of lives were saved” by Covid-19 vaccines is based on hypothetical models that rest on a long sequence of assumptions—many of which are either weak, unvalidated, or demonstrably false (see below). As a result, the outputs of these models are of questionable value and cannot be taken as reliable evidence.
- A central assumption underlying these models was that Covid-19 vaccines provided strong and durable protection against infection and transmission. Consider the original statement by Dr. Anthony Fauci, then Chief Medical Advisor to the US President: “When you get vaccinated you not only protect your own health… but also you contribute to the community health by preventing the spread of the virus throughout the community…you become a dead end to the virus” (bold added).5 This assumption—serving as the cornerstone of the mass vaccination campaign—turned out to be false. Real-world data quickly revealed that vaccine efficacy against infection was fragile and short-lived, and efficacy against transmission was never directly studied.
- Strikingly, despite the collapse of this original narrative (point 2), the vaccination campaign continued under a revised justification: that the vaccines provide lasting protection against severe illness and death, even after their short-term effect against infection diminishes. It is important to recognize that this updated claim hinges on a conceptual separation between these two types of efficacy—a separation that, as we demonstrate repeatedly in our preprint article, was never empirically validated.
- In fact, available data suggest that protection against infection and protection against severe illness or death are closely linked, following a similar trajectory of waning over time. The difference lies primarily in timing, with a natural delay between initial infection and the development of severe outcomes.
- To directly assess the validity of this supposed distinction between protection against infection and protection against severe illness, we examined the conditional probability of severe illness among individuals who became infected across several key studies. The results were clear: the apparent protection against severe outcomes was most likely a byproduct of the short-term protection against infection. None of the influential studies we analyzed demonstrated independent or durable protection against severe illness or death.
- Notably, some studies stopped tracking severe outcomes precisely at the point when vaccine protection would be expected to wane—paralleling the well-documented decline in protection against infection and the typical delay between infection and the onset of severe illness or death mentioned above. This pattern raises serious concerns about potential misrepresentation or selective reporting of research findings.
- Finally, the pivotal randomized controlled trial that led to the Emergency Use Authorization (EUA) of the Pfizer vaccine showed no meaningful difference between the vaccine and placebo groups in preventing: (1) flu-like symptoms, (2) severe Covid-19, or (3) all-cause mortality. The only significant difference was observed in a non-clinical outcome—laboratory-confirmed Covid-19 infection—and even this result was based on data from no more than 8.24% of participants, collected in a potentially biased manner, as detailed in our preprint.
- Notably, no Covid-19-related deaths were recorded in Pfizer’s pivotal trial. This absence raises serious questions about whether the legal and medical criteria for issuing an emergency use authorization were truly met.
- Even more importantly, the six-month follow-up trial by Pfizer reported 15 deaths in the vaccine group (n = 21,720), compared to 14 in the placebo group (n = 21,728). Given the large sample size, this lack of mortality benefit should have served as a critical anchor for any hypothetical model or evidence-based discussion regarding the overall benefit of the vaccine.
These findings seriously challenge the notion that Covid-19 vaccines saved millions of lives. Moreover, our in-depth investigation uncovered a broader range of methodological flaws that cast doubt on the overall reliability of the existing evidence base. These include: (a) followup periods that were exceedingly short and inconsistently applied across groups; (b) implausible efficacy signals appearing almost immediately after vaccination—well before full immunization could have occurred biologically; and (c) heavy reliance on observational data vulnerable to Healthy Vaccinee Bias, differential testing rates, and numerous other confounding factors.
Taken together, these methodological and empirical concerns not only undermine the foundation of the “millions saved” narrative, but also raise a deeper question: If the evidence is so limited and flawed, how did this narrative gain such dominance in scientific and public discourse?
The issue is not whether some degree of vaccine efficacy was observed at specific moments (e.g., see the fascinating example in our preprint of the Bar-On et al. study on the second booster), but rather how such fleeting observations came to shape the broader public narrative. Isolated data points were elevated and decontextualized, while critical considerations—such as (a) waning immunity, (b) the lack of demonstrated mortality benefit, (c) vaccine breakthrough infections leading to hospitalization or death, and (d) an increasingly robust body of evidence on adverse effects—were systematically sidelined (Figure 1).
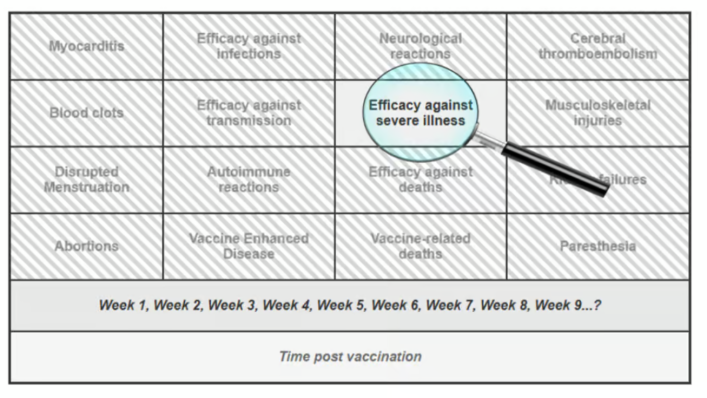
Figure 1. Illustrating a Selective Focus on a Transiently Favorable Outcome While Ignoring Concerning Data
This narrowing of focus — peering through the keyhole of one transient success — has allowed a fragile claim to solidify into a powerful myth, reinforced by institutional authority, social conformity, and the systematic suppression of dissenting voices (including our own experience of censorship, as detailed in our preprint).
We therefore call on the scientific and medical communities to take a step back, widen the lens, and return to a foundational principle of medicine: every intervention, no matter how promising, must undergo continuous, evidence-based evaluation of both its benefits and its potential harms. To the best of our knowledge, such a balanced and rigorous appraisal has yet to be applied to the Covid-19 vaccines.
Based on the evidence reviewed in our preprint, we conclude that the claim that “Covid-19 vaccines saved millions and millions of lives”1 is not supported by empirical evidence. While these vaccines were widely promoted as safe and effective, accumulating reports of serious adverse events—such as myocarditis, pericarditis, thrombosis, and neurological symptoms—have been extensively documented across pharmacovigilance systems and in multiple peer-reviewed studies (e.g., 6-16), many co-authored by the last author of the current article.
Notably, this biologically active intervention was administered repeatedly in the form of boosters, thereby compounding potential risks—often in populations with near-zero risk of Covid-related mortality, such as children. Taken together with the lack of demonstrable long-term efficacy presented in our preprint,4 the available evidence suggests that the risk–benefit balance of the Covid-19 vaccines may, in fact, tilt toward the negative end of this fundamental medical equation.17, 18
References
1. Homeland Security. The Corruption of Science and Federal Health Agencies: How Health Officials Downplayed and Hid Myocarditis and Other Adverse Events Associated with the COVID-19 Vaccines.
2. Ophir Y, Shir-Raz Y, Zakov S, McCullough PA. The Efficacy of COVID-19 Vaccine Boosters against Severe Illness and Deaths: Scientific Fact or Wishful Myth?. Journal of American Physicians and Surgeons. 2023;28(1). doi: https://www.jpands.org/vol28no1/ophir.pdf.
3. Ophir Y. The Final Brick in the Vaccine Efficacy Narrative ⋆ Brownstone Institute. 2023.
4. Ophir Y, Shir-Raz Y, Zakov S, McCullough PA. A Step-by-Step Evaluation of the Claim That COVID-19 Vaccines Saved Millions of Lives. Researchgate (preprint). 2025. doi: 10.13140/RG.2.2.12897.42085.
5. NEWS C. Transcript: Dr. Anthony Fauci on “Face the Nation,” May 16, 2021. 2021.
6. Rose J. A Report on the US Vaccine Adverse Events Reporting System (VAERS) of the COVID-1 9 Messenger Ribonucleic Acid (mRNA) Biologicals. Science, Public Health Policy, and The Law. 2021;2:59–80.
7. Fraiman J, Erviti J, Jones M, et al. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine. 2022;40(40):5798–5805. doi: 10.1016/j.vaccine.2022.08.036.
8. Shir-Raz Y. Breaking: Leaked Video Reveals Serious Side-Effects Related to the Pfizer COVID-19 Vaccine Covered Up by the Israeli MOH. 2022.
9. Witberg G, Barda N, Hoss S, et al. Myocarditis after Covid-19 Vaccination in a Large Health Care Organization. N Engl J Med. 2021;385(23):2132–2139. doi: 10.1056/NEJMoa2110737.
10. Chua GT, Kwan MYW, Chui CSL, et al. Epidemiology of Acute Myocarditis/Pericarditis in Hong Kong Adolescents Following Comirnaty Vaccination. Clinical Infectious Diseases. 2021:ciab989. doi: 10.1093/cid/ciab989.
11. Hulscher N, Alexander PE, Amerling R, et al. A Systematic REVIEW of Autopsy findings in deaths after covid-19 vaccination. Forensic Sci Int. 2024:112115. doi: 10.1016/j.forsciint.2024.112115.
12. Oster ME, Shay DK, Su JR, et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA. 2022;327(4):331–340. doi: 10.1001/jama.2021.24110.
13. Takada K, Taguchi K, Samura M, et al. SARS-CoV-2 mRNA vaccine-related myocarditis and pericarditis: An analysis of the Japanese Adverse Drug Event Report database. Journal of Infection and Chemotherapy. 2024.
14. McCullough P, Rogers C, Cosgrove K, et al. Association between COVID-19 Vaccination and Neuropsychiatric Conditions. 2025.
15. McCullough PA, Hulscher N. Risk stratification for future cardiac arrest after COVID-19 vaccination. World J Cardiol. 2025;17(2):103909. doi: 10.4330/wjc.v17.i2.103909.
16. Hulscher N, Hodkinson R, Makis W, McCullough PA. Autopsy findings in cases of fatal COVID-19 vaccine-induced myocarditis. ESC Heart Failure. 2024;n/a. doi: 10.1002/ehf2.14680.
17. Mead MN, Seneff S, Wolfinger R, et al. COVID-19 Modified mRNA “Vaccines”: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex, Part 1. International Journal of Vaccine Theory, Practice, and Research. 2024;3(2):1112–1178. doi: 10.56098/fdrasy50.
18. Mead MN, Seneff S, Rose J, Wolfinger R, Hulscher N, McCullough PA. COVID-19 Modified mRNA “Vaccines”: Lessons Learned from Clinical Trials, Mass Vaccination, and the Bio-Pharmaceutical Complex, Part 2. International Journal of Vaccine Theory, Practice, and Research. 2024;3(2):1275–1344. doi: 10.56098/w66wjg87.
This article was co-authored by Yaffa Shir-Raz, Shay Zakov, and Peter A. McCullough.
Dr. Yaakov Ophir is Head of the Mental Health Innovation and Ethics Lab at Ariel University and a member of the Steering Committee for the Centre for Human-Inspired Artificial Intelligence (CHIA) at the University of Cambridge. His research explores digital-age psychopathology, AI and VR screening and interventions, and critical psychiatry. His recent book, ADHD Is Not an Illness and Ritalin Is Not a Cure, challenges the dominant biomedical paradigm in psychiatry. As part of his broader commitment to responsible innovation and scientific integrity, Dr. Ophir critically assesses scientific studies related to mental health and medical practice, with particular attention to ethical concerns and the influence of industrial interests. He is also a licensed clinical psychologist specializing in child and family therapy.
Featured Video

Trita Parsi: Iran War Ends Today? Threats of Deporting Trita Parsi
or go to
Aletho News Archives – Video-Images
From the Archives
Iran UN ambassador calls for destruction of all nuclear weapons

Iran’s ambassador to the UN Gholamali Khoshroo
Press TV – March 29, 2017
Iran’s ambassador to the UN Gholamali Khoshroo has called for the total eradication of nuclear weapons.
Khoshroo reiterated Iran’s call during a UN conference aimed at creating a nuclear weapons ban treaty in New York on Tuesday.
“Iran, as a victim of chemical weapons, strongly feels the danger posed by the existence of weapons of mass destruction and is determined to engage actively in international diplomatic efforts to save humanity from the menace of nuclear weapons,” he said.
Khoshroo stressed that Iran is committed to its Non-Proliferation Treaty (NPT) obligations, which include negotiations based on effective nuclear disarmament measures.
He added that several countries continue to ignore international calls and treaties for nuclear disarmament and even continue to increase their nuclear stockpiles. “They do not have political determination to abandon doctrines of nuclear deterrence and nuclear terror,” he went on to say.
Iran’s UN ambassador noted that boycotting the talks by many countries, including the US, shows that the world’s nuclear powers are by no means committed to the eradication of nuclear arms. Britain and France were also among the some 40 countries that did not join the talks.
“We note that prohibition of nuclear weapons must be accompanied by the elimination of such weapons. There can be no doubt that without complete abolition of nuclear weapons, there will be no absolute guarantee against the danger of nuclear war and the use of such weapons,” Khoshroo added.
Blog Roll
 Aletho News
Aletho News- The Crusades – colliding narratives
- Trita Parsi: Iran War Ends Today? Threats of Deporting Trita Parsi
- What Is SIDS?
- DHS docs: Govt bracing for nationwide anti-AI riots, preparing to crack down on dissent
- India signals rethink over West Asia
- Israeli Ex-Navy Chief admits massive damage from Iran missiles
- The strategic arsenal US lost in war against Iran – and why replenishment will take years
- Documents Suggest Fauci Knew COVID Was Created in Wuhan Lab, and mRNA Vaccines Wouldn’t Work
- No return to pre-war status for Strait of Hormuz – Iran’s top diplomat
- Ex-South Korean President sentenced for trying to provoke conflict with Pyongyang
- If Americans Knew
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- Oxfam: More Palestinians killed by Israel across West Bank in last 3 years than previous 17 years combined
- US-Iran ceasefire may be imminent, but will Israel blow it up? – Daily Update
- The Issue of Israel Is Ending Democracy In Michigan
- Israel is stealing homes, livelihoods, and lives in West Bank
- Gaza is not an aberration – Israel planned this genocide decades ago
- Israel is changing the face of Lebanon, mainstream media is normalizing it – 3 articles
- Genocide lobby benefits from EU anti-racist fund
- No Tricks Zone
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
