‘If We Get Away With It, It’s Legal’: Documents Reveal New Details on U.S. Government’s ‘Censorship-Industrial Complex’
By Michael Nevradakis, Ph.D. | The Defender | November 29, 2023
Government agencies, private-sector firms, academia and nonprofits were collaborating to combat alleged “misinformation” and “disinformation” as far back as 2017, according to new documents released Tuesday.
The “CTIL Files” — which refer to the Cyber Threat Intelligence League, or CTI League, a key player in the so-called “Censorship-Industrial Complex” — are based on documents received from an unnamed but “highly credible” whistleblower, according to investigative journalists Michael Shellenberger, Alex Gutentag and Matt Taibbi, who released the files.
The new documents rival or exceed the “Twitter Files” and “Facebook Files” in “scale and importance,” according to the journalists, two of whom — Shellenberger and Taibbi — were instrumental in releasing many of the “Twitter Files” that first called attention to the “Censorship-Industrial Complex.”
A comprehensive picture of the birth of the ‘anti-disinformation’ sector
The documents, which the journalists detailed on Substack, center around the activities of the CTI League, which “officially began as the volunteer project of data scientists and defense and intelligence veterans but whose tactics over time appear to have been absorbed into multiple official projects, including those of the Department of Homeland Security (DHS).”
According to the journalists, the CTI League documents “offer the missing link … to key questions not addressed in the Twitter Files and Facebook Files” and “offer a comprehensive picture of the birth of the ‘anti-disinformation’ sector.”
“The whistleblower’s documents describe everything from the genesis of modern digital censorship programs to the role of the military and intelligence agencies, partnerships with civil society organizations and commercial media, and the use of sock puppet accounts and other offensive techniques,” the journalists wrote.
Documents in the “CTIL Files” show members of the CTI League, DHS officials and key figures from social media companies “all working closely together in the censorship process.”
This “public-private model” laid the groundwork for “anti-misinformation” and “anti-disinformation” campaigns launched by the U.S. and U.K. governments in 2020 and 2021, the journalists wrote, including attempts to circumvent First Amendment protections against government censorship of speech in the U.S.
Such tactics included “masking censorship within cybersecurity institutions and counter-disinformation agendas; a heavy focus on stopping disfavored narratives, not just wrong facts; and pressuring social media platforms to take down information or take other actions to prevent content from going viral,” they added.
The CTI League went still further though, the journalists wrote, engaging “in offensive operations to influence public opinion, discussing ways to promote ‘counter-messaging,’ co-opt hashtags, dilute disfavored messaging, create sock puppet accounts, and infiltrate private invite-only groups.”
Such censorship lies at the heart of Missouri et al. v. Biden et al., a First Amendment censorship case where injunctions were issued against several federal agencies and government officials, barring them from communicating with social media companies regarding user content. The injunctions are now under review by the U.S. Supreme Court.
Former British intelligence analyst charged with creating counter-disinformation project
The journalists wrote that while previous releases of the “Twitter Files” and “Facebook Files” revealed “overwhelming evidence of government-sponsored censorship,” they had not revealed “where the idea for such mass censorship came from.”
The whistleblower alleged that a key figure in the CTI League, “a ‘former’ British intelligence analyst, was ‘in the room’ at the Obama White House in 2017 when she received the instructions to create a counter-disinformation project to stop a ‘repeat of 2016.’”
By 2019, this analyst, Sara-Jayne “SJ” Terp, had “developed the sweeping censorship framework,” leading a team of U.S. and U.K. “military and intelligence contractors” who “co-led CTIL.” Previously, in 2018, Terp attended a 10-day military exercise organized by the U.S. Army Special Operations Command, according to the journalists.
It was there that Terp met Pablo Breuer, a former U.S. Navy commander, who became a key figure in the CTI League. According to Wired, the two realized that misinformation “could be treated … as a cybersecurity problem.” This led to the development of CogSec, which soon housed the “MisinfoSec Working Group.”
“Terp’s plan, which she shared in presentations to information security and cybersecurity groups in 2019, was to create ‘Misinfosec communities’ that would include government,” the journalists wrote.
By spring 2020, it appears Terp achieved this plan, as the CTI League partnered with the Cybersecurity and Infrastructure Security Agency (CISA), which has been implicated in prior releases of the “Twitter Files” for its role in the “Censorship-Industrial Complex.”
The MisinfoSec Working Group included Renee DiResta, a former CIA operative who worked for the Election Integrity Partnership (EIP) — later renamed the Virality Project (VP). This group “created a censorship, influence, and anti-disinformation strategy called Adversarial Misinformation and Influence Tactics and Techniques (AMITT).”
According to the journalists, AMITT adapted “a cybersecurity framework developed by MITRE, a major defense and intelligence contractor that has an annual budget of $1 to $2 billion in government funding.” MITRE is a backer of the Vaccination Credential Initiative and the SMART Health Card — a digital “vaccine passport.”
Terp used AMITT to develop the DISARM framework, which the World Health Organization (WHO) applied in “countering anti-vaccination campaigns across Europe.”
The same framework “has been formally adopted by the European Union and the United States as part of a ‘common standard for exchanging structured threat information on Foreign Information Manipulation and Interference’” according to the journalists.
‘Can we get a troll on their bums?’
According to the journalists, MisinfoSec’s motivation for counter-misinformation was the “twin political earthquakes of 2016: Brexit and the election of Trump.”
“There’s something off kilter with our information landscape,” Terp and other CTI League members wrote, according to documents.
“The usual useful idiots and fifth columnists — now augmented by automated bots, cyborgs and human trolls — are busily engineering public opinion, stoking up outrage, sowing doubt and chipping away at trust in our institutions. And now it’s our brains that are being hacked,” they added.
In spring 2020, the CTI League set its sights on COVID-19-related narratives, targeting users who engaged in messaging that ran contrary to official policy.
“CTIL began tracking and reporting disfavored content on social media, such as anti-lockdown narratives like ‘all jobs are essential,’ ‘we won’t stay home,’ and ‘open America now,’” the journalists wrote.
“CTIL created a law enforcement channel for reporting content as part of these efforts. The organization also did research on individuals posting anti-lockdown hashtags … and kept a spreadsheet with details from their Twitter bios. The group also discussed requesting ‘takedowns’ and reporting website domains to registrars,” they added.
Regarding the “we won’t stay home” narrative, internal documents revealed by the whistleblower showed that CTI League members wrote, “Do we have enough to ask for the groups and/or accounts to be taken down or at a minimum reported and checked?” and “Can we get all troll on their bums if not?”
They also called posters circulating online promoting anti-lockdown posters “disinformation artifacts,” saying, “We should have seen this one coming” and asking “can we stop the spread, do we have enough evidence to stop superspreaders, and are there other things we can do (are there countermessagers we can ping etc).”
During CTI League brainstorming sessions to develop strategies for “counter-messaging for things like encouraging people to wear masks,” statements such as “Repetition is truth” were uttered by CTI League staff, the journalists noted.
The CTI League also sought to go “beyond simply urging Twitter to slap a warning label on Tweets, or to put individuals on blacklists.”
According to the journalists, “The AMITT framework calls for discrediting individuals as a necessary prerequisite of demanding censorship against them” and “trying to get banks to cut off financial services to individuals who organize rallies or events.”
As part of these efforts, even truthful information was targeted. In a 2019 podcast on “Disinformation, Cognitive Security, and Influence,” Terp admitted, “Most information is actually true … but set in the wrong context.”
“You’re not trying to get people to believe lies most of the time,” she said. “Most of the time, you’re trying to change their belief sets. And in fact, really deeper than that, you’re trying to change, to shift their internal narratives … the set of stories that are your baseline for your culture.”
Previous “Twitter Files” releases have revealed that true information was targeted for censorship by the U.S. government and social media platforms like Twitter if the information contradicted official policy regarding COVID-19 vaccines and restrictions.
‘Cognitive security’ a euphemism for censorship
In the same podcast, according to the journalists, Terp said, “Cognitive security is the thing you want to have. You want to protect that cognitive layer. It basically, it’s about pollution. Misinformation, disinformation is a form of pollution across the Internet.”
The journalists wrote, “A key component of Terp’s work through CTIL, MisinfoSec, and AMITT was to insert the concept of ‘cognitive security’ into the fields of cybersecurity and information security.”
Such “cognitive security” was seen as being threatened by the erosion of the mass media’s control on information and influence over public opinion.
Documents revealed by the whistleblower included a MisinfoSec report stating “For a long time, the ability to reach mass audiences belonged to the nation-state (e.g. in the USA via broadcast licensing through ABC, CBS and NBC).”
“Now, however, control of informational instruments has been allowed to devolve to large technology companies who have been blissfully complacent and complicit in facilitating access to the public for information operators at a fraction of what it would have cost them by other means,” the report said.
The same report also called for a form of “pre-bunking,” to “preemptively inoculate a vulnerable population against messaging,” suggesting that DHS-funded Information Sharing and Analysis Centers could be used to promote such pre-bunking.
‘If we get away with it, it’s legal’
Public-private partnerships were specifically sought out in an attempt to circumvent First Amendment free speech protections in the U.S., the documents revealed, even while Bloomberg, The Washington Post and Wired wrote glowing articles portraying the CTI League as a mere group of “volunteer” cybersecurity experts.
Yet, according to the journalists, “In just one month, from mid-March to mid-April [2020], the supposedly all-volunteer CTIL had grown to ‘1,400 vetted members in 76 countries’” and had “helped to take down 2,833 cybercriminal assets on the internet” including some which impersonated government organizations, the United Nations and WHO.
On the same 2019 podcast, according to the journalists, Breuer explained how the CTI League was getting around the First Amendment, by working to get “nontraditional partners into one room,” including “maybe somebody from one of the social media companies, maybe a few special forces operators, and some folks from Department of Homeland Security.”
Together, they would “talk in a non-attribution, open environment in an unclassified way so that we can collaborate better, more freely and really start to change the way that we address some of these issues,” Breuer said.
Breuer even likened these tactics to those employed by the Chinese government, saying “If you talk to the average Chinese citizen, they absolutely believe that the Great Firewall of China is not there for censorship. They believe that it’s there because the Chinese Communist Party wants to protect the citizenry and they absolutely believe that’s a good thing.”
“If the US government tried to sell that narrative, we would absolutely lose our minds and say, ‘No, no, this is a violation of our First Amendment rights.’ So, the in-group and out-group messaging have to be often different,” he said.
The whistleblower told the journalists that CTI League leaders did not discuss their potential violation of the First Amendment.
“The ethos was that if we get away with it, it’s legal, and there were no First Amendment concerns because we have a ‘public-private partnership’ — that’s the word they used to disguise those concerns. ‘Private people can do things public servants can’t do, and public servants can provide the leadership and coordination,’” the whistleblower said.
According to the journalists, the authors of the MisinfoSec report also “advocated for police, military, and intelligence involvement in censorship, across Five Eyes nations, and even suggested that Interpol should be involved.”
The CTI League documents also suggest that the organization was involved in a form of domestic spying, with one document noting that while censorship activities abroad are “typically” performed by “the CIA and NSA and the Department of Defense,” such efforts “against Americans” necessitate the use of private partners because the government lacks the “legal authority” to do so.
According to the whistleblower, CTI League members also went to great lengths to conceal their activities, with a CTI League handbook recommending the use of burner phones, online pseudonyms and the generation of fake AI faces. One document advised, “Lock your s**t down … your spy disguise.”
One suggested list of questions to be posed to prospective CTI League members proposed asking whether those individuals had ever “worked with influence operations (e.g. disinformation, hate speech, other digital harms etc) previously” and whether those efforts included “active measures” and “psyops” (psychological operations).
Indeed, according to the documents, several CTI League members had worked for the military or intelligence agencies, while according to the whistleblower, “roughly 12-20 active people involved in CTIL worked at the FBI or CISA” — even, for a time, displaying their agency seals alongside their names on the CTI League’s internal Slack channel.
Terp, for instance, previously designed machine learning algorithms and unmanned vehicle systems for the U.K.’s Ministry of Defence.
According to the whistleblower, the CTI League sought “to become part of the federal government.”
Shellenberger, Taibbi to testify before Congress this week
According to the journalists, the FBI declined to comment, while CISA, Terp and other CTI League figures did not respond to requests for comment.
However, one CTI League member, Bonnie Smalley, did respond to the journalists’ request. She wrote, verbatim, “all i can comment on is that i joined cti league which is unaffiliated with any govt orgs because i wanted to combat the inject bleach nonsense online during covid. … i can assure you that we had nothing to do with the govt though.”
“CTIL appears to have generated publicity about itself in the Spring and Fall of 2020 for the same reason EIP did: to claim later that its work was all out in the open and that anybody who suggested it was secretive was engaging in a conspiracy theory,” the journalists wrote.
“But as internal messages have revealed, much of what EIP did was secret, as well as partisan, and demanding of censorship by social media platforms, contrary to its claims,” they said, adding that “EIP and VP, ostensibly, ended, but CTIL is apparently still active, based on the LinkedIn pages of its members.”
The journalists said the documents will be presented to Congressional investigators and made public, while protecting the identity of the whistleblower.
Shellenberger and Taibbi will testify at Thursday’s hearing of the U.S. House of Representatives’ Select Subcommittee on the Weaponization of the Federal Government. They previously testified before the same committee in March.
On Tuesday, Taibbi appeared in a live YouTube webcast presenting some of the key revelations from the first release of the “CTIL Files.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Meet The “Medically Kidnapped” Teenager Who Brought A Tyrannical Healthcare System To Its Knees
The story of Maya Kowalski and how it might help Covid treatment victims

BY JJ STARKY | NOVEMBER 19, 2023
Days ago, a Floridian jury ruled in favour of the surviving family members of a wife and mother who took her own life after her daughter, Maya, was “medically kidnapped” for nearly 90 days.
The six-person jury in Sarasota County unanimously determined Johns Hopkins All Children’s Hospital in St. Petersburg was liable for the incidents leading up to the January 2017 death of Beata Kowalski, 43.
They also ruled that the hospital should pay the Kowalski family well over $210 million for the losses they endured, which included punitive damages.
The Kowalski’s story is one of torment, heartache, and anguish.
In fact, it is the sort of story that would make the most limp-wristed of us metamorphose into an angry cage fighter that looks like they’ve snorted a cubic tonne of cocaine before stepping into the octagon. You want blood after hearing it.
Netflix made a near two-hour documentary on their case, ‘Taking Care of Maya’, which I highly recommend watching.
To recap the bare bones, in 2015, 10-year-Maya began experiencing some nasty symptoms. These included breathing problems, headaches, blurred vision, skin lesions, lower limb dystonia, and debilitating chronic pain. And they would come on arbitrarily. So her parents, Jack and Beata, naturally sought medical advice.
But it was to no avail. They saw dozens of medical experts and they still didn’t know what was wrong with their daughter. That was until they visited one Dr. Anthony Kirkpatrick in September 2015, who diagnosed Maya with advanced complex regional pain syndrome (CRPS).
CRPS is a form of amplified musculoskeletal pain syndrome in which pain from a physical interaction outlasts the expected recovery time. For example, a gentle touch can mimic a slap – a flick, a punch.
Fortunately for Jack and Beata, Dr Kirkpatrick encountered the syndrome before in past patients. He had a treatment protocol in mind using ketamine, but – and herein lies the beginning of the problem – it was not conventional or well-known. Nor was the prescribed treatment available in Florida, where the Kowalski family lived.
Low doses of ketamine kept proving ineffective and so the family travelled to Mexico so Maya could undergo a ketamine coma, fearing her symptoms would worsen and become fatal. Thankfully, the procedure was successful. Her symptoms dissipated.
Except, one random night in October 2016, they returned – with vengeance. Her father rushes her to the local hospital, Johns Hopkins All Children’s, admits her, and tries to explain the rare syndrome to the staff. But they were mystified. They hadn’t come across the condition and even became suspicious of its existence. Beata told the hospital staff what treatment was required, but as soon as they learnt of the amount of Ketamine she had been taking, it was too late.
The next thing they know, a child abuse paediatrician, Dr Sally Smith, turns up unidentified to Maya’s bedside for an assessment. Within ten minutes, Smith concludes Beata has been abusing Maya, and that CRPS is not present. A nurse then informs Jack that his daughter is now in state custody and orders him to leave. Maya has been diagnosed with Munchausen syndrome by proxy, the fancy phrase for “medical child abuse”.

Sally Smith
What transpires over the next 3 months is nothing short of parental hell. Maya was still separated from her family. Her father was allowed to see her now and again because he adopted the role of pacifier, but her mother, Beata, who’d actively argued with hospital staff, was not.
Beata descended into a pit of depression. During rare scheduled calls with Maya, she discovered her symptoms were deteriorating and that the hospital had changed her treatment without her consent. Allegations also surfaced that a contracted social worker had stripped her daughter down to a sports bra against her will in order to take pictures of her body. This, again, occurred without Beata and Jack’s consent.
The same social worker, Catherine Bedy, Maya accused of telling her she was “going to go into a foster home”, her mother “was in a mental institution”, and she was “going to end up adopting” her.
Catherine Bedy
On January 8, 2017, after 87 days without her daughter, believing she is the primary reason for Maya’s separation, Beata commits suicide. She hangs herself in the garage at home while Jack and her son Kyle attend a party. Jack didn’t discover her body until her brother had read Beata’s suicide note and rushed over to the home. When Jack woke up to Beata’s brother’s piercing screams, he knew his wife had taken her own life.

10-year-old Maya with her mother, Beata
In the fallout of Maya’s medical kidnapping, the Kowalski’s lawyer, Debra Salisbury, discovered Dr Smith works for the Suncoast Center, which provides child welfare services to Pinellas County. Salisbury also finds out that children in Pinellas County, where the hospital is based, are almost two and a half times as likely to be removed from their families when compared to the Florida average. Suspicions arise Suncoast has incentivised its employees to misdiagnose children so their customer base could increase.
Retrospective analysis of Maya’s diagnosis would support this theory. After Beata’s suicide, Dr Kirkpatrick, the doctor who initially prescribed the Ketamine, testifies that he informed Dr Smith of Maya’s rare condition and offered to send her all the documented evidence to support his prescription when she contacted him to file her original report. The only thing is, she didn’t include any details of their discussion in that report. The medical expertise of the doctor who’d provided the most materially effective treatment was totally excluded.
Weeks later, local investigative reporter Daphne Chen hears of Beata’s passing. Like any good journalist seeking truth, she refuses to accept the “official story” – “official narrative” connotations intended – and digs in. In January 2019, when her fingertip presses publish on a write up about the Kowlaski’s, something unexpected occurs. Calls start flying in.
Chen becomes inundated with calls and emails from local parents, alleging the misdiagnosis of Munchausen syndrome by proxy. Instances where parents called 911 because their child was experiencing a life-threatening emergency – seizures, breathing difficulty, excess vomiting – were resulting in the same outcome. After their child underwent a series of tests and scans, hospital staff would question parents over the injuries and symptoms and issue a case review. And curiously, the one thing they all had in common – you guessed it – was an assessment from Dr. Smith. Post-Smith assessment, these parents found themselves legally segregated from their child, with some being arrested. They did what the system told them to do, sought help, but were instead, punished.
Upon further investigation, Salisbury, the Kowalski’s lawyer, found that the root cause was less to do with a rogue clinician than it was a deep fault in the system. In the 1970s, child protective services in the U.S. diagnosed child abuse via excess corporeal punishment. We’re talking overt physical abuse – beatings, cigarette burns, etc. But overtime, they redefined the criteria. Fast forward to the 2020s, parents with children suffering from rare conditions that consult with over 3 or 4 doctors can find themselves accused of “doctor-shopping”, exposing a child to unnecessary medical procedures and thus, being guilty of medical child abuse.
In a recent interview with The Epoch Times, investigative journalist Stellar Paul explained how similar circumstances led to the mistreatment of hospitalised Covid patients. Like Maya, these patients were attacked by a system that continually found itself departing from traditional medical ethics and toward a form of blanket-style healthcare. In turn, personalised treatment and attention were subverted. The medical complex treated them en masse, rather than as individuals with unique health needs.
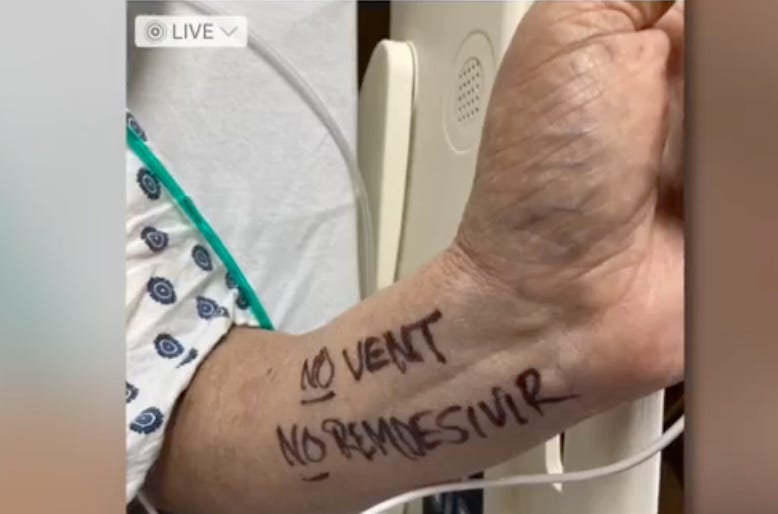
Take the story of Ray Lamar, who, when hospitalised with Covid, specifically requested he not receive certain treatments. He even wrote on his inner forearm, “no vent. (ventilator) no Remdesivir”. So what did his “carers” do? They gave him Remdesivir, without informing him of dangers, without receiving his consent. He later died.
Then, there is Christine Johnson. Christine’s daughter was a nurse, so she was aware of Remdesivir’s questionable benefit-to-risk ratio and the detrimental impact it could have on her kidneys. She also said she didn’t want the drug. So hospital staff gave it to her while she slept. She also died.
These stories go on and on.

Why did hospitals treat patients in this way? Well, again, as Stellar explains, it is because, whether by policy or practice, external forces adulterated the structure of the system. For Ray and Christine, it was the 2020 Coronavirus Aid, Relief, and Economic Security Act (CARES) and the Public Readiness and Emergency Preparedeness Act (PREP). One financially incentivised the use of dangerous treatments while the other legally shielded hospitals that administered them. For Maya, it was the empowerment of Dr Sally Smith and the dilution of the definition of “child abuse”.
The court proceedings for the Kowalski’s were not straightforward. There were various lengthy delays, and they wondered if they would ever see justice. To give you an idea of how vicious the hospital’s lawyers were, when Maya missed just one hearing, they combed through her social media and presented photos to the jury of her attending her homecoming. This, they argued, was proof that Maya could live a “normal teenager’s life”. Talk about vipers.

However, thanks to Beata’s meticulous note-taking of events without which the family’s lawyer said prosecution would have not been possible, the Kowlaski family successfully sued the hospital on multiple claims of false imprisonment, battery, intentional infliction of emotional distress, medical negligence, negligent infliction of emotional distress, negligent training of doctors and healthcare providers, and fraud.
There are numerous parallels we could draw from Maya’s story and 2020 Covid treatment victims but if there is one overarching precedent set, it is how the mutated structure of the medical complex has facilitated anti-healthcare. And it is one that could help dozens upon dozens of Covid treatment victims currently fighting their battles in court as well as other victims of the misdiagnosis of medical child abuse.
Perhaps the saddest realisation after researching this case is that had Beata not taken her own life, it is unlikely we would have heard about Maya’s ordeal. May she rest in peace.
Elon Musk’s Comments On Mechanical Ventilation Betrayed A Stunning Amount of Ignorance – Part 1
BY PIERRE KORY, MD, MPA | NOVEMBER 15, 2023
Recently, Elon Musk was interviewed by Joe Rogan where he shared that, early in Covid, he had access to front-line data in China and “talked to doctors from Wuhan,” implying that if we had known what he knew, our use of mechanical ventilation would have been different. That is almost certainly true but he then went on to make several inaccurate statements which I think further fuel widespread misunderstanding and overestimation of the actual negative impacts of mechanical ventilation use during Covid in the U.S.
Now, I find it shocking that I might be putting myself in a position to defend the U.S. Covid response as that would be an outrageous endeavor, however, I take issue with his subsequent statements on mechanical ventilation use as they were almost completely wrong (almost).
I hate misinformation (inaccurate /false information) about Covid and I believe Elon trafficked in the same. I do not believe he did so out of willful, malevolent intent as that would be disinformation (what the now corporate controlled U.S. government regime does to us). His comments were instead borne of a stunning amount of ignorance regarding the real risks of mechanical ventilation and exactly how mechanical ventilation was misused (and not misused) both in China and in the U.S. during that first wave. So, here is my attempt to “set the record straight.”
ELON: “We had 20,000 employees in China and during the first wave we had nobody die and nobody get ill.”
This is both interesting and unsurprising and almost certainly accurate. It brings back harsh memories of all the fear porn that was being blasted out by the world’s media with cherry-picked images of scenes from the hardest hit areas like Wuhan, Lombardy, New York, Seattle etc. They did this while the vast majority of urban areas in the country and around the world did not experience such tidal waves of people in acute respiratory failure.
Although news media trying to get as many eyeballs glued to their shows is not new (i.e. “if it bleeds it leads”) in early Covid, it soon became apparent to many (in my world at least) that they also did so to instill widespread fear to increase compliance with what were soon to be draconian violations of civil liberty, bodily autonomy, informed consent, and free speech. Those violations were deemed necessary in their plight to coerce the entire U.S. population to be vaccinated. This is probably a good time to re-read the anonymous poem I posted last year titled “Message to the Unvaccinated.” Link here:
However, on this point of instilling the greatest amount of fear possible, a recent post by A Midwestern Doctor quoted Scott Atlas, a completely sane member of the White House’s insane Coronavirus Task Force:
As often happened, Fauci spoke up to support Dr. Birx’s concerns, saying people need to be warned even more strongly about the dangers of the virus spreading, about wearing masks and distancing. He claimed Americans didn’t think the virus was serious, and that was the reason cases spread. I was honestly surprised. I thought people were already panic-stricken. Normal life had virtually ceased to exist, even eliminating serious medical care or last visits with dying family. Meanwhile the media were on-message 24/7, instructing the public about masks and social distancing; there were signs and announcements demanding masks and diagrams about distancing everywhere; healthy young people were outside riding bicycles or driving their cars alone, wearing masks. Indeed, surveys showed that most adults perceived grossly exaggerated risks, particularly but not only younger people; and yes, a high percentage were obeying the edicts, distancing and wearing masks, according to virtually every published survey.
I challenged him to clarify his point, because I couldn’t believe my ears. “So you think people aren’t frightened enough?”
He [Fauci] said, “Yes, they need to be more afraid.”
To me, this was another moment of Kafkaesque absurdity. I replied, “I totally disagree. People are paralyzed with fear. Fear is one of the main problems at this point.” Inside, I was also shocked at his thought process, as such an influential face of the pandemic. Instilling fear in the public is absolutely counter to what a leader in public health should do. To me, it is frankly immoral, although I kept that to myself.”
Note: Fauci also fear-mongered for his own benefit throughout the AIDS crisis (which amongst other things created significant stigmatization towards the gay community as Fauci asserted without evidence that HIV might be transmitted without physical contact).
ELON: I called doctors in Wuhan and asked “what are some of the biggest mistakes you made in the first wave” and they said “we put far too many people on mechanical ventilators.”
My motivation for writing this post is to try to correct (but not completely refute) the now widespread, strong belief that it was the “ventilators” that killed people and that if we did not use mechanical ventilators, many lives would have been saved. Or, similarly, “if they hadn’t put my (wife/mother/father etc) on a ventilator, they would be alive today.”
I largely and strongly disagree with the latter assessment (but not completely). The reason for my disagreement is that, based on my experiences running Covid ICU’s at the University of Wisconsin in Madison, Beth Israel Medical Center in New York City, Greenville Memorial Hospital in South Carolina, St. Lukes Medical Center in Milwaukee, and Aspirus Wausau in Central Wisconsin, it wasn’t the vents that killed people. It was the lack of effective treatments being adopted.
Initially, it was the lack of any treatment (i.e. “supportive care only” approaches, particularly at UW) that led to widespread death after what was often weeks on a ventilator and later it morphed into sub-optimal, insufficiently aggressive, sometimes harmful, monolithic treatments like Remdesivir and a modest dose of corticosteroids instead of a broad, multi-component, safe, synergistic combination of therapies such as the MATH+ protocol that FLCCC members were using and recommending for hospital patients (forgive me for I am biased). However, Elon then said the following regarding mechanical ventilation:
“This is what is exactly damaging the lungs it is not Covid. The treatment, the cure is worse than the disease.”
“People yelled at me saying I am not a doctor but I said yeah but I do make spaceships with life support systems, what do you do?”
Well, Elon, although I don’t build spaceships, I actually used and taught mechanical ventilation to keep people alive for a living and did so throughout most of Covid. Further, mechanical ventilation was a deep interest if not passion of mine for almost 20 years prior.
The act of of sedating and paralyzing someone to place an endotracheal tube through their vocal cords and into their trachea is called “intubation” and is required to transition someone to support by an invasive mechanical ventilator. What I witnessed in the first wave (but not later waves) was doctors favoring “early intubation/mechanical ventilation” out of fear that the patient would suddenly crash (intubating a “crashing” patient is a higher risk procedure). And yes, another subtle, but not overt motivation, very early on, was to “protect” staff from exhaled breath due to fear of heated high flow nasal cannulas (this is an intermediate support device often used to avoid intubation) – more on this issue/aspect in Part 3 which is already available here).
Now, although it is true that each extra day on a ventilator can worsen prognosis, the harms are much more from prolonged, poorly responsive illness requiring prolonged sedation and immobility which then cause confusion/delirium and disuse atrophy of the muscles. So for him to say it is the ventilators which damage the lungs more than Covid is completely off – know that patients with neurological injuries affecting respiration can be kept alive safely on ventilators for weeks to months to years to decades without significant “damage” accumulating to the lungs.
Admittedly, the situation of someone with a lung injury is different in that inappropriate ventilator settings can certainly further damage the lungs, but with modern ventilator techniques such as low tidal volumes, daily spontaneous breathing trials, use of appropriate positive-end expiratory pressure, highly responsive inhalation triggers etc, the harms of mechanical ventilation to the lungs are generally minimal.
To wit, I have successfully extubated thousands of patients in my career despite devastating injuries to their lungs requiring prolonged periods on the ventilator, even in situations where the ventilator was particularly difficult to set in order to achieve the holy grail of mechanical ventilation, that of “patient-ventilator synchrony.” All I am saying is that his comment on the harms of mechanical ventilation was grossly overstated to an un-credible degree. He then went further:
“The treatment is worse than the disease.”
Ugh. Mechanical ventilation is not and has never been a treatment, it is simply a means to support a patient’s breathing to keep them alive while you administer therapies (more on this below) to reverse the underlying insult or infection that landed them on the ventilator in the first place – no-one, and I mean no-one in medicine has ever viewed the ventilator as a treatment or cure for anything.
However, the initial practice of “early intubation” caused unmanageable and chaotic situations in many hospitals by increasing demand for ICU rooms and ventilators, but I will argue below that this situation was almost completely fueled by the lack of effective treatments being adopted.
This is a key distinction, i.e the harm of ineffectively or not treating the disease far, far outweighed the harms of intubating too early. Further, “early” intubations largely occurred during the first wave, and as physicians became more familiar with the disease they began to defer intubation to much more advanced degrees of respiratory failure and hypoxemia (obviously there were exceptions to this, but, as I mentioned above, I travelled and worked fairly widely, and in each center I found that the ICU docs quickly learned to defer intubation to as late as possible in Covid induced hypoxemic respiratory failure. This issue is what I will explore in further detail in Part 2.
I instead maintain that the absurdly high death rates in many hospitals in the U.S and across the world in the early waves of Covid was due to an over-reliance on “supportive care only” approaches (i.e. limiting interventions to just supplemental oxygen, fluids, nutrition, fever suppressants, mechanical ventilation). Rarely were effective treatments targeting the underlying pathophysiology being offerred at most academic medical centers based on the widespread belief that patients were dying of a viral pneumonia and that no effective anti-viral therapies existed.
What was not being sufficiently taught or disseminated at that time is that Covid-19 disease had multiple phases, i.e. an early “viral replicative phase” marked by typical viral syndrome symptoms such as cough, fever, congestion, sore throat, fatigue etc with a minority of those patients then going on to develop the later “hyper-inflammatory phase” involving the lungs. The FLCCC tried very hard to alert “the system” to the fact that early studies found no live, culturable virus in patient secretions beyond Day 6 (cue the folks who state there is no virus and/or they don’t exist. To those, all I can offer is this excellent post addressing the issue by A Midwestern Doctor).
Thus, after about Day 6, a minority of Covid-19 patients began to develop morphed a hyper-inflammatory, pulmonary phase due largely to activated macrophages (an immune cell) as well as micro-clumping or clotting of blood cells and proteins. In this latter phase, anti-inflammatory or immunosuppressive therapies combined with anti-coagulants were required (this is why the FLCCC recommended corticosteroids and blood thinners in hospital patients from the outset and were observing excellent results with early use).
To wit, my first paper on Covid (and the one I am most proud of) was initially drafted in April of 2020. I argued then that Covid-19 pulmonary disease was not a viral pneumonia but instead an “organizing pneumonia” (a form of lung injury with many causes (viruses are only one of them) but whose mainstay of therapy is corticosteroids).
From the abstract:
I arrived at that hypothesis after a couple of weeks of being mystified by the repeated presentations of Covid patients with what was called at the time, “happy hypoxia”, i.e. the state of requiring high amounts of supplemental oxygen yet without exhibiting a significant increase in the work of breathing.
I knew I had seen “happy hypoxia” on a couple of occasions in my career but could not remember what was wrong with those patients until one morning during a shower before an ICU shift in New York City it hit me – “these patients remind me of patients with organizing pneumonia!” As soon as I got to work, before my shift, I called Dr. Jeff Kanne at the University of Wisconsin, one of the top chest radiologists in the world and an expert on organizing pneumonia.
“Jeff, what would you say if I told you that I think that all of these Covid patients are suffering from organizing pneumonia?” I asked. His answer? “Of course they are. We wrote this up in March in the journal Radiology after an expert panel that I chaired completed our review of all the CT scans from Wuhan.” They had actually written in their expert report that “the most common reported CT findings in Covid-19 patients are typical of an organizing pneumonia pattern of lung injury.”
“Clinicians don’t read radiology journals,” I shouted into the phone. “We need to publish this in a clinical medical journal! Like NOW!” We quickly agreed that we would write it up together.
I went home after my ICU shift and started working furiously. The paper included radiographic, pathologic, and clinical evidence to try to prove that the pulmonary phase of Covid-19 was an organizing pneumonia and that the first line of therapy for this condition was (wait for it)… corticosteroids.
Note that my paper above was not published until September 2020 due to 5 journals rejecting it, with one journal rejecting it because a peer-reviewer said “this cannot be published until a randomized controlled trial of corticosteroids is conducted.” Welcome to my life.
The problem we in the FLCCC had with getting the world to use corticosteroids in the hospital phase were many and will be explored in Part 2 (already available).
Mayo Clinic is Sued For Suspending Doctor Over Online Posts on Covid and Transgenderism
By Ben Squires | Reclaim The Net | November 15, 2023
Dr. Michael Joyner, backed by the Academic Freedom Alliance (AFA), has initiated a lawsuit against the Mayo Clinic College, including its president and board chair. The suit arises from disciplinary actions taken against Joyner following his public comments on topics within his field of expertise. Specifically, the controversy revolves around statements he made to the New York Times about gender differences in athletic performance and to CNN regarding the use of convalescent plasma in COVID-19 treatment. The Mayo Clinic’s response, which involved suspension, salary review implications, and strict media interview oversight, is at the heart of this legal challenge.
We obtained a copy of the complaint for you here.
Lucas Morel, chair of the AFA’s academic committee, emphasized the lawsuit’s significance, asserting that “academic freedom is a key guarantor of scientific integrity.”
Morel expects the case to establish a precedent for the freedom of scientists and academics to express their professional opinions without undue influence from financial or political interests. The AFA, which previously supported Joyner during his disciplinary hearings, is now financing this lawsuit, highlighting the organization’s commitment to protecting academic freedom.
Joyner’s legal action, filed with the State of Minnesota’s Third Judicial District, seeks compensation for the damages incurred from the disciplinary measures. These included a week-long unpaid suspension, denial of salary increase, and a potential termination threat, all of which have reportedly harmed Joyner’s finances and professional reputation. The lawsuit, handled by Allen Harris Law, was filed after allowing the defendants to review and respond, which they declined.
What does the WHO say about its power to enforce the Pandemic Treaty (and International Health Regulations)?
By MERYL NASS | NOVEMBER 12, 2023
Many people have insisted that the WHO could not make the US do anything. Let me remind those people that the US government under Biden is instrumental in pushing forward the WHO proposals, and so it will comply. Here is what the WHO says:

What is meant by a ‘convention, agreement or other international instrument’?
Conventions, framework agreements and treaties are all examples of international instruments, which are legal agreements made between countries that are binding.
Why did WHO’s Member States decide to create an accord for pandemic preparedness and response?
In light of the impact of the COVID-19 pandemic, WHO’s 194 Member States established a process to draft and negotiate a new convention, agreement, or other international instrument (referred to in the rest of this FAQ, generally, as an “accord”) on pandemic preparedness and response. This was driven by the need to ensure communities, governments, and all sectors of society – within countries and globally – are better prepared and protected, in order to prevent and respond to future pandemics. The great loss of human life, disruption to households and societies at large, and impact on development are among the factors cited by governments to support the need for lasting action to prevent a repeat of such crises.
[Ho ho ho—Nass]
At the heart of the proposed accord is the need to ensure equity in both access to the tools needed to prevent pandemics (including technologies like vaccines, personal protective equipment, information and expertise) and access to health care for all people.
[If this were true, why do the treaty and amendments only discuss health “coverage” which means health insurance, rather than health care? The WHO knows the difference, but only demands “coverage”—a sop to the insurance industry.
Furthermore, the WHO demands censorship of information not in agreement with the WHO’s narratives, not free sharing of information—so much for information equity—and its so-called expertise was used to overdose hospitalized patients with HCQ without informed consent, when these unfortunates were enrolled in the WHO’s “SOLIDARITY” trial. Its expertise led to demanding that nations stop the use of HCQ and ivermectin for COVID and administer more shots. Who needs this expertise? —Nass]
Who else is involved in the process for the accord?
Besides WHO Member States, the process for developing a possible new accord is providing extensive opportunities for engagement with relevant stakeholders, including other United Nations system bodies, and a wide range of other non-State actors in official relations with the WHO, to ensure robust and inclusive participation in the proceedings of the Intergovernmental Negotiating Body. Furthermore, WHO is seeking complementary inputs through public hearings with stakeholders including: international organizations; civil society; the private sector; philanthropic organizations; scientific, medical, public policy and academic institutions and other entities with relevant knowledge, experience and/or expertise.
[In other words, Bill Gates, who was the largest funder of the WHO the year Trump defunded the organization, gets the lion’s share of input, while we peons get none. Trump then turned around and funded Gate’s’ charity GAVI with the money, and GAVI turned around and gave it back to the WHO. That was our money, by the way.—Nass]
—There is more of this nonsense on this webpage, but you can go look it up yourself if you have the stomach for it.—Meryl
CPSO Pronounces Judgment Over Dr Trozzi
But the shots are still toxic, Pfizer committed fraud, everyone has been assaulted, and we must act now to save lives.
Dr Mark Trozzi | November 6, 2023
Health Canada recognizes that Pfizer committed fraud. The shots turn out to be even worse than I thought. They contain large quantities of DNA, and multiple genetic sequences including a very dangerous SV40 promoter sequence which promotes permanent genetic modification, disease, and cancer. Sadly, innocent people are uninformed and lining up for injections that they would never agree to if they knew what was in them and what it can do to them.
Here is my ten minute video to update you, with a focus on current priorities and strategies. Crisis is a combination of danger and opportunity. The SV40 revelation marks severe danger, but it is also an opportunity to finally set things right. This video includes genuinely kind and honest advice for the CPSO administrators and staff; and a small request for you to please share your judgement of me as a doctor with the CPSO.
Please Share Your Judgment of Dr Trozzi with the CPSO here:
- CPSO Compliment a physician https://www.cpso.on.ca/en/Public/Public-Information/Compliment-a-physician
- or by email direct to feedback@cpso.on.ca

CPSO v. Trozzi – Case Update – November 1, 2023
COLLEGE DENIES DR. TROZZI’S RIGHT TO FREEDOM OF EXPRESSION
We are the Administrative State and You are Not
The Ontario Physicians and Surgeons Discipline Tribunal has ruled that Dr. Mark Trozzi is guilty of professional misconduct and dishonourable conduct and is incompetent in the practice of medicine for questioning the government’s Covid-19 narrative. He was also found guilty of professional misconduct and was deemed incompetent for writing medical exemptions for Covid-19 injections in support of a patient’s right to refuse coerced medical treatment under Ontario’s Health Care Consent Act and section 7 of the Canadian Charter of Rights and Freedoms.
In 2021, the College of Physicians and Surgeons of Ontario established three Covid-19 restrictions through website statements — doctors were forbidden from: (i) making any statements that discourage anyone from following Covid-19 public policies and recommendations; (ii) prescribing alternative Health Canada approved medications for the treatment of Covid-19; and (iii) writing medical exemptions for Covid-19 injections, unless a patient had suffered a severe allergic reaction or developed myocarditis after a first shot. Based on the restrictions relating to freedom of expression and medical exemptions, the College issued investigation orders against Dr. Trozzi in 2021.
This eventually led to a five-day hearing in July of 2023 during which the College Tribunal focused its prosecution on Dr. Trozzi’s daily newsletter at drtrozzi.org, where he had supposedly caused harm by spreading “misinformation” about Covid-19 science. The College was particularly concerned with Dr. Trozzi’s view that neither Big Pharma nor Health Canada had done the due diligence required to prove the Covid-19 injections were safe and effective. The Tribunal concluded that his views were inflammatory, unprofessional and worthy of censure. On November 10th, the Tribunal will hold a penalty hearing to determine whether to revoke the licence of the 25-year ER veteran and former university professor.
Trozzi’s lawyer, Michael Alexander, commented: “The Tribunal wrote up the prosecution’s position on almost every issue. The one saving grace was the College’s acknowledgement that the right to free expression includes the right to make statements that may be wrong or mistaken. However, that position is difficult to reconcile with the Tribunal’s view that Dr. Trozzi can be punished for spreading misinformation.“
He added: “The Tribunal did not address our argument that the College lacked the authority to investigate and prosecute Dr. Trozzi since its Covid-19 restrictions were merely recommendations rather than binding rules or regulations, even though we cited the Ontario Divisional Court and the Ontario Court of Appeal in support of our position.”
Further, he stated: “The Tribunal totally ignored our cross-examination of the College’s expert witnesses, which makes the entire decision a complete travesty. On cross, the College’s main expert witness on Covid science, Dr. Andrew Gardam, admitted that he had never responded to the 41-page expert report provided by Dr. Trozzi in which he rebutted Gardam’s own 8-page expert report with 29 scientific citations. As a result, in closing submissions, we argued that Dr. Trozzi was unrefuted on Covid science; yet, the Tribunal made no mention of this fact.”
Finally, he added: “The Tribunal also paid no attention to the fact that the Supreme Court recognized an expansive right to freedom of expression as an inherent feature of parliamentary government as early as 1939, which gives the right a higher status than it enjoys under the Charter. In matters of law, we will appeal the decision to the Divisional Court on the standard of correctness.”
For media inquiries, please contact Michael Alexander by cell at 416-318-4512 and by e-mail at malexanderjd@protonmail.com.
Please support the fight to restore ethical medicine and the rule of law in Ontario and Canada.
Please sign this petition to defend my license to practice medicine in Ontario and ultimately restore Canadians’ access to many honest doctors who have been persecuted for resisting the unethical and unscientific covid agenda.
Reports about Dr Trozzi and the CPSO from others:
- Life site News: Dr. Mark Trozzi may lose medical license for defying COVID narrative
- Epoch Times Tribunal Finds Ontario Doctor Critical of COVID Measures Committed Professional Misconduct
- Derek Sloan Funding the Fight: Dr. Trozzi Latest Update – May Lose Licence Next Week
- Denis Rancourt, “In Canada, Dr Mark Trozzi has opposed the toxic death-causing vaccine in every way he can, so the CPSO @cpso has decided that he is incompetent! ( And “disgraceful, dishonourable or unprofessional”)”
Here’s a history to be proud of, and “accused” of:
- To follow Dr Trozzi’s public covid truth mission beginning January 2021 and right up until the present start here
- Or to begin with the most recent and work your way back start here
DNA Contamination/ SV40 promoter sequence/ Pfizer’s Fraud/ Health Canada
- Dr Trozzi Alert | There’s DNA in the RNA Shots. Lots! April 2023
- World Council For Health Urgent Panel of Global Experts Confirm Dangerous Criminal Undeclared DNA In Pfizer And Moderna Covid-19 “Vaccines”
- Epoch Times regarding plasmid DNA contamination and Health Canada
Cancer:
Canadian doctor sounds alarm over ‘turbo cancers’ in young people due to COVID jabs. ‘I’ve never seen anything like this,’ said Dr. William Makis regarding ‘stage four’ cancers presenting in young people and uncharacteristically aggressive leukemias.
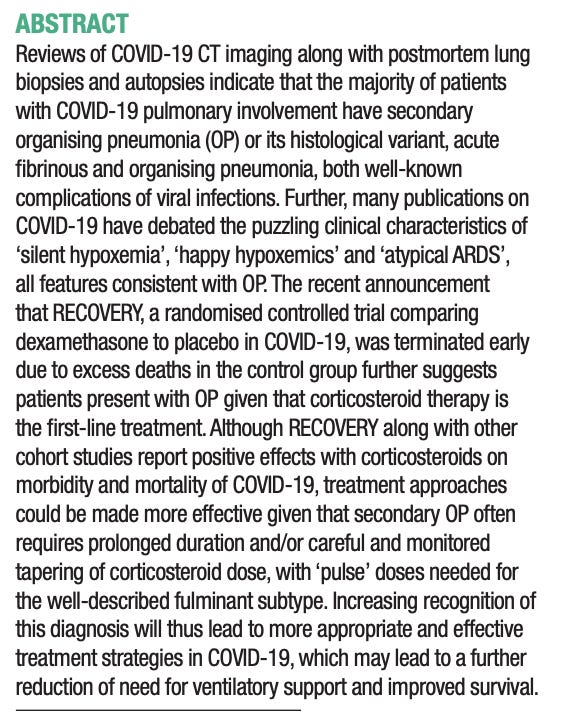
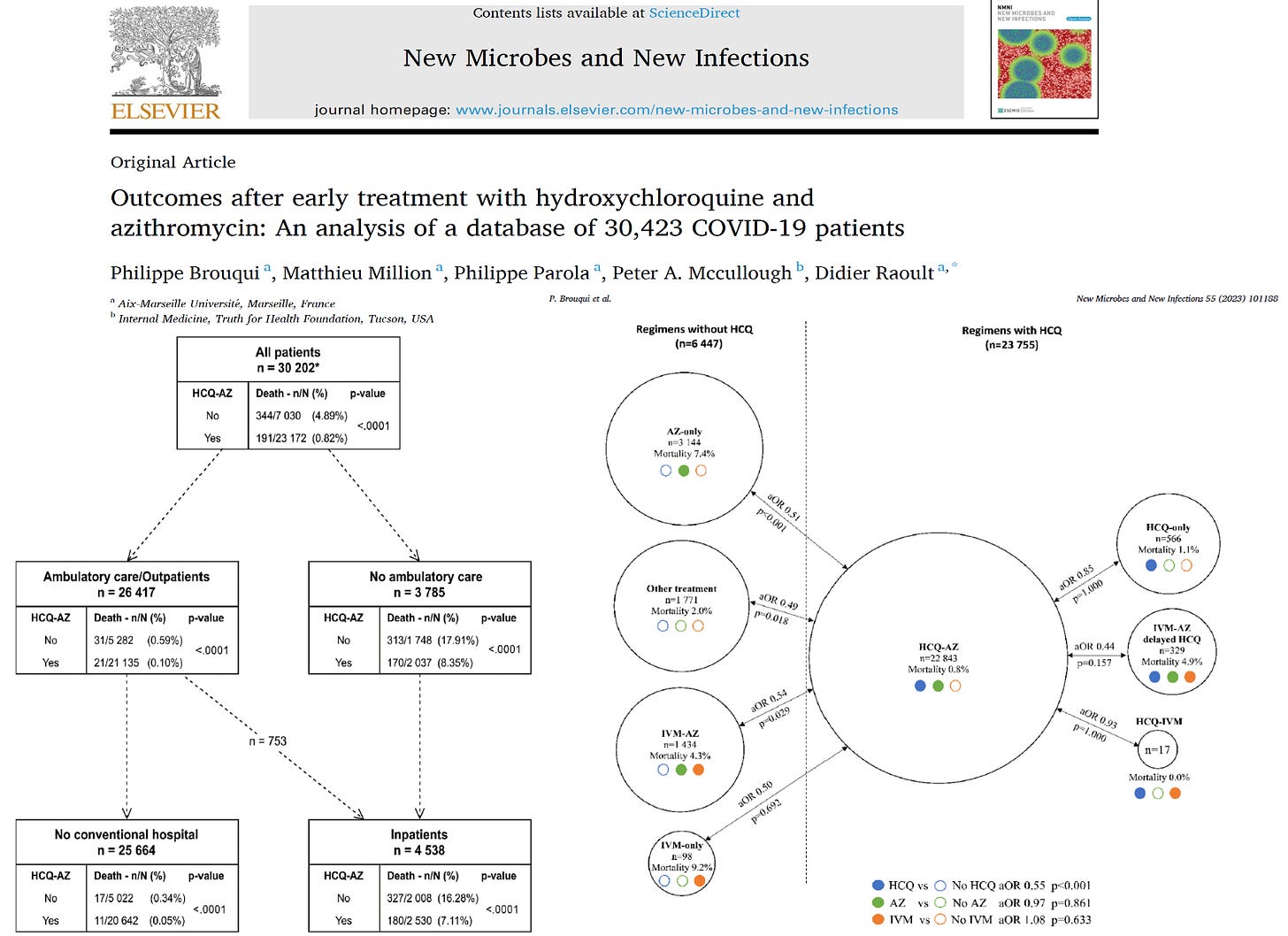
Outcomes after Early Treatment with Hydroxychloroquine and Azithromycin: An Analysis of 30,423 COVID-19 patients
By Peter A. McCullough, MD, MPH | Courageous Discourse | November 6, 2023
We perform prospective, randomized, double-blind, placebo-controlled trials to test drugs, vaccines, devices, and other products for safety and efficacy. Randomization is important since it handles: 1) selection bias, 2) all known and unknown confounders. Despite the hundreds of billions of dollars spent during the pandemic, we did not have an investment in large, multidrug prospective, randomized, placebo controlled trials or comparative studies to test the best drug regimens.
In the end, what patients care about is how they feel, function, and survive. When it came to COVID-19, whether randomized or not, if patients survived if they were in the optimally treated group. The only way to assess how a high-risk population fared in the pandemic is to report on a large sample of patients sick with COVID-19 with a large number of the outcome of of interest—death.
Brouqui et al reported from a French database of 30,423 COVID-19 patients of whom 535 succumbed to the illness. In great detail, the investigators report mortality according to ambulatory treatment received, hospitalization, and the course over the following six weeks.
An explosive discussion with ex-CDC scientist Norman Pieniazek
BY MARTIN NEIL, JONATHAN ENGLER, AND JESSICA HOCKETT | OCTOBER 30, 2023
Dr Norman Pieniazek is a molecular biologist, geneticist, epidemiologist with 147 publications in virology and parasitology. Before he retired, he spent 24 years working at the Center for Disease Control (CDC) in the USA. He has also spent time abroad including time working in Spain and Poland.
We met up with Norman for what was planned to be a short meeting to introduce ourselves and informally discuss common interests around covid. However, this turned into a two-hour long, wide-ranging and fascinating discussion that touched on a huge number of topics.
Early on in the meeting Norman made the wise suggestion that we record and share the discussion. So, he hit the record button on Skype and we started again. The video, accessible below, is approximately two hours long. Be aware that, given it wasn’t planned as an ‘interview’ or for broadcast, it is largely unstructured. However, for those short of time here is a synopsis of the discussion with a focus on what Norman said1:
- The bacterial pneumonia hypothesis suggests that early treatment – hydroxychloroquine, ivermectin and antibiotics address bacterial infection. Norman confirmed bacteria are everywhere in our bodies including in the lungs, creating an ever-present potentially hazardous predisposition that, given the right circumstances, might cause a deadly bacterial pneumonia infection.
- Well-understood remedies such as the stockpile of antibiotics, as recommended by Fauci, were cast aside in 2020. Bacterial infection can cause sepsis hence we need antibiotics. A Cytokine storm is caused by bacterial infection in the lungs, filling them with fluid; this lowers the oxygen level in the blood because of poor lung function.
- In-person diagnosis by a physician based on physical symptoms was largely replaced by the PCR test, and with the rise in tele-health visits, social distancing etc physicians stopped using stethoscopes to listen to a patient’s chest. This is an essential diagnostic tool to enable a doctor to audibly tell whether a patient has crossed the line into a bacterial infection which will then require antibiotics.
- Norman knew Donald Henderson who co-authored a classic work on how to best respond to a flu epidemic. Henderson and colleagues did not recommend any of the NPIs that were followed during covid because of the obvious severe health, social and economic costs. (As an aside this work was co-authored by Prof. Thomas Inglesby at John Hopkins who attended Event 201 and, oddly, recommended NPIs be used for covid – the very same ones he had rejected previously).
- Orthodox immunology was ignored – herd immunity is a fiction given there is a ‘soup’ of constantly mutating coronaviruses.
- Why didn’t scientists at the CDC question things early in 2020? Work from home restrictions meant that people at CDC couldn’t communicate and coordinate to overturn the madness being imposed from the ‘sixth floor’ top brass. You could not isolate CDC from the HHS (Health and Human Services) and it was HHS that were calling the shots.
- The Wuhan scientists were on a routine ‘fishing expedition’ for coronaviruses and unusual pneumonias. Why was this work being done in Wuhan? It is easier to do in China because it is legal and because there are lots of hospitals, in a concentrated area, where the population is in relatively poor health. Also, it is easier to get permission to perform a painful bronchial lavage procedure on patients to obtain pathogens in China; this is much harder to do in the USA. This procedure is done in the lower respiratory tract and guarantees higher quality samples than can be obtained using swabs, which really just measure the quality of the air that has entered your upper respiratory tract.
- To determine what pathogen is causing lower respiratory tract symptoms you should not use swabs and PCR. Why not? CDC acknowledges the inability of swabs to collect causative agents as reported by the EPIC study in these 2015 NEJM articles (one done on adults and one on children). Hence a positive result gained from a sample taken from the upper throat or the nose does not mean an infection is caused by the detected pathogen.


- In 2002-2004 SARS-COV was not subject to mass PCR testing, yet SARS-COV-2 was. PCR was used for SARS-COV but only on samples taken using bronchial lavage, but NOT from swab samples taken from the nose or upper throat.2
- Wu et al discovered WH-Human-1 using samples collected by bronchial lavage, and next generation sequencing of the collected genetic samples, and ultimately reported it in GenBank.
- Before reporting on GenBank they published a preprint identifying the genetic sequences3, which was appropriated and found its way into the hands of Corman and Drosten, who then decided to exploit it for personal gain (via commercial PCR testing), fabricating a story about validating it against SARS-1. It was subsequently renamed SARS-COV-2. (For a proposed timeline of events see here).
- Norman thinks SARS-COV-2 is simply a beta coronavirus (a cold), one of the many thousands of cold viruses that had remained undiscovered until 2020, but which have always been ever present in nature.
- SARS-COV-2 cannot be a novel virus created in a lab or by natural zoonotic mutation. It is simply novel to detection4. As soon as the EUA approved PCR tests started to be used the virus was simultaneously discovered in a number of disparate geographical regions. There was no evidence of sudden spread.
- In effect the results of any test are as much determined by the choice of test to apply as by the presence/absence of viruses. Norman says, “you will find whatever you want to find”. Hence people will be symptomless yet will have a lot of, whatever viruses happen to be around in their nose or throat.
- The established taxonomy of viruses is unusable simply because there are so many unknown viruses circulating in the wild.
- The mRNA vaccine technology ended in a ‘garbage heap’, because it is extremely toxic, and was rendered obsolete by protein subunit vaccines by 2019. So, the mRNA vaccines were doomed from the start. Subunit (protein-based) vaccines have been known since the late 1970s, but Moderna, Pfizer and BioNTech needed a way to realise a return on their vast investments in mRNA. Hence the pandemic.
- Novavax is a protein subunit vaccine, based on the spike protein, which was available in August 2020 but did not get approval from the FDA. Although it is protein based it will stay in the deltoid muscle injection site. It was however approved in Canada. It may not be very good for you (and ineffective against coronaviruses), but it is less dangerous than the mRNA vaccines.
- mRNA vaccines were found to be too dangerous for animals. Also, arguments that they are a safe basis for cancer drugs are based on lies. There is a competing technology called humanised monoclonal antibodies that cured President Carter from a melanoma that had migrated to his brain and there are now 500 versions of these drugs currently available.
- Norman was told that the patent on the flu vaccines, grown in eggs, expired in 2020. Hence there was little ROI in continuing with this technology.
- Viruses are in your respiratory tract and antibodies, responding to vaccines, are in your blood. These two things do not match well because the antibodies in the blood do not get into the lungs. The immune system ‘stays away’ from the complex respiratory system that deals with the thousands of pathogens we breathe in with every breath.
- Are serology studies a pointless exercise? Because of wide variation between individual’s antibody measurement only makes sense by studying change in any single individual over time.
- Testing for antibodies means nothing because antibodies in the blood cannot travel to the lungs to react.
- Testing for antigens is a cheaper and less sensitive version of the PCR test with the same limitation.
- Norman is very sceptical of a number of covid virus theories including those by Walter Chesnut and JJCoey’s infectious clone theory, though they weren’t discussed in any great detail and were probably not characterised fully (or maybe even fairly).
- The issue with ‘infectious clones’ is that ‘you do not know what to create’ because there are millions of sequences of coronavirus so there is no ‘clonality’ and each one has 30 thousand nucleotides and there are combinatorically infinite changes you could potentially need to consider when creating a coronavirus5. It therefore isn’t possible to know what to change, via Gain of Function (GoF), to make the virus behave in more dangerous ways.
- As part of the ‘partnership for peace’ programme in 1994 Norman hired two ex-Soviet bioweapons scientists and asked them ‘how come you worked for 20 years and didn’t create any new deadly viruses?’
- They can create thousands of virus combinations, but the problem is how to test these creations. There is no way to test the billions and billions of possible changes to a virus and identify which changes to the sequence are ‘bad’. You need the phenotype, and you cannot deduce the phenotype from the genotype. So how would GoF researchers – E.g., EcoHealth alliance – know exactly what to create?
- The claim that Saddam Hussian had biological weapons was groundless and this was confirmed to Norman by Donald Henderson who was involved at the time and who said it was not possible.
- Thus, GoF claims that changes to spike protein and furin cleavage sites make a virus more deadly are fiction. It isn’t possible and there is no proof they can produce deadly bioweapons. Those advocating this position and making these claims – EcoHealth alliance (Fauci, Baric and Duszak) should get fired by their bosses for producing “not a tiger but a kitty”.
- We discussed Gulf War syndrome. Norman said people imagine anthrax is dangerous, but the ex-Soviet bioweapons researchers said to attack New York with anthrax would need 20,000 Boeing 747s flying over the city, dropping millions of tons of anthrax spores from a low height then people spreading it with shovels. The only way to infect people with anthrax is by direct means via an oxygen line or a direct injection.
- Norman said the Tokyo gas attack was successful in Japan because the terrorist used sarin, a nerve agent. The biological agents used, botulinum and anthrax, fortunately failed.
- Within the CDC Fauci was called the ‘mean midget’ and during the AIDS epidemic he sunk Robert Gallo by inventing the story that Gallo had stolen the HIV virus from Luc Montagnier, thus destroying Gallo’s chances of being awarded the Nobel prize (he was also denied a patent).
- Fauci is “not stupid, he is mean”. Fauci wanted to get a Nobel prize, but he didn’t get a Nobel prize for AIDS, so he wanted it for the Wuhan virus. In January 2023 knowing that he wasn’t going to get the Nobel prize he “pulled the plug” and published this paper saying new types of vaccines are needed for respiratory infections, as an act of spite.
We learned a lot from Norman and are very grateful to him for giving us his valuable time. You will notice that we briefly discussed the vaccines, but you will be very pleased to hear that Norman has agreed to follow up with another meeting in early December to share his thoughts on this important topic (see here for a sneak peek)
You can access Norman’s other material on YouTube and Facebook (much of his material is in Polish and Norman speaks six languages!) His twitter handle is @normanpie.
1 Note that this synopsis is not a verbatim and true transcription of the conversation.
2 This document presents evidence PCR was used to collect samples, but no mass testing was undertaken.
3 Submitted (05-JAN-2020) Department of Zoonoses, National Institute of Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention. The first submission to GenBank had two subsequent revisions.
4 The supposed ‘novel and deadly’ attributes of the virus are discussed extensively here.
5 See this paper. “Mammals are the reservoir hosts of the majority of emerging zoonoses (2, 3, 18). If we assume that all 5,486 described mammalian species (19) harbor an average of 58 viruses in the nine families of interest (as estimated here in P. giganteus) and that these viruses exhibit 100% host specificity, the total richness of mammalian viruses awaiting discovery exceeds ~320,000.”
Critics of Biden’s ‘Censorship Regime’ Say Government Dragging Its Feet on Lawsuit
By Aaron Kheriaty, MD | Human Flourishing | November 3, 2023
M.J. Koch over at the New York Sun has published a very good article on Missouri v. Biden and the Supreme Court’s decision to place a temporary stay on the injunction until they can rule on the case:
Next year’s presidential election may have something to do with the slow pace of Missouri v. Biden.
The Biden administration is said to be dragging its feet on an explosive free speech case against its alleged “Orwellian” censorship of social media platforms. Those leading the lawsuit say it’s because the government wants to continue its censorship regime as long as possible before the presidential election.
The Supreme Court has agreed to hear the case, Missouri v. Biden. In certifying it, the high court last week also approved the government’s request for a stay on a preliminary injunction from the Fifth Circuit. The injunction would’ve enjoined the government from continuing what two lower courts called a “coordinated campaign” by top federal officials and agencies to suppress undesirable opinions on public issues such as Covid lockdowns and election integrity.
The suspension of that injunction “is a green light for future censorship,” the founder of the civil rights group representing four of the plaintiffs in the case, Philip Hamburger, of the New Civil Liberties Alliance, tells the Sun. The high court appears to be siding with the executive branch in its latest legal action…. “Undoubtedly,” Mr. Hamburger says, “there’s deference, in the sense of political deference, to the government.”
Next year’s presidential election might have something to do with this “deference.” Oral arguments in Murthy will be heard in January or February, but the court won’t complete its review until late in the spring. Even if the ruling requires the government to immediately desist its behavior, several more months of the status quo will have passed as the contest for the U.S. presidency intensifies.
You can read the rest of the article, which includes my comments on this issue, here.
How (not) to Relativize the Holocaust

By CJ Hopkins | Consent Factory | November 1, 2023
OK, I owe everyone an apology. I get it now. I’ve seen the light. I finally understand the true nature of my thoughtcrimes, and I take responsibility for them, and I stand ready to pay my debt to society.
I have to thank the State of Israel for bringing about this sudden epiphany. How it happened was, Gilad Erdan, Israel’s Ambassador to the United Nations, and his delegation wore yellow Stars of David, i.e., the ones the Nazis forced the Jews to wear in public, at a Security Council session to make a statement. According to The Jerusalem Post, Ambassador Erdan then made remarks comparing the October 7 Hamas attack on Israel to the Holocaust.
“When Jewish babies were burned in Auschwitz, the world was silent, and today Jewish babies were burned in Be’eri and the towns of the South by the Nazi Hamas – and the world is silent again. I will make you remember the shame of your silence every time you look at me,” Arden said. “I will wear the yellow patch until the Nazi Hamas is eliminated and until the Security Council stops being silent and condemns the October 7 massacre. Some of you have learned nothing in the last eighty years! Some of you have forgotten why the United Nations was founded. So I will remind you. From today on, every time you look at me you will remember. When my grandfather and his children were sent to Auschwitz, the world was silent. When his wife and their seven children were sent to the gas chambers, the world was silent. When their bodies were burned alongside millions of other Jewish children, the world was silent,” Erdan said, comparing the silence of the UN about the Hamas massacre on October 7 to the silence of the international community regarding the horrors of the Holocaust.
Now, I’ll be honest, the first thought that went through my head when I read that Jerusalem Post piece was, “Great! Here’s an Israeli diplomat doing exactly what I’m being prosecuted for doing, and no one’s going to prosecute him! All I need to do is bring this to the attention of the Berlin District Court, and they’ll dismiss my case!”
But then I had my epiphany.
Basically, my epiphany was, I realized the two things are completely different, i.e., Israel’s use of a Nazi symbol to make a political statement and me doing the same thing … well, almost the same thing. I’ve never actually relativized or minimized or trivialized or compared anything to the Holocaust, as Gilad Erdan did at the UN. Actually, I’ve advised against doing that. But that doesn’t let me off the hook for my thoughtcrimes! No, I did what I did, and I will have to answer for it in January at the District Court of Berlin!
For readers unfamiliar with my case, what I did was, I tweeted these two Tweets featuring the the cover art of my book, The Rise of the New Normal Reich, which is banned in Germany, and referring to the medical-looking masks that everyone was forced to wear during 2020-2022 as “ideological conformity symbols.”

You can read the background on my case here, or here, or here, or listen to me talk about it here, or here, or here, so I won’t go on about it here.
The important thing is, I understand now how totally wrong (and criminal) it was to do that, and how what I did is completely different from what UN Ambassador Erdan just did!
For starters, it wasn’t just those two Tweets. No, on Twitter, Facebook, and in my essays, and interviews, and, basically, every chance I got, for two years, I compared the rise of the “New Normal” to the rise of Nazi Germany in the 1930s. I noted the similarities between these two forms of totalitarianism: the declaration of a “state of emergency” as a pretext to justify the cancellation of constitutional rights and rule by decree; the propaganda; the censorship; the criminalization of dissent; the mandatory displays of ideological conformity; the invasion of bodily autonomy; the segregation, demonization, and persecution of a scapegoat underclass; and so on … all the classic hallmarks of totalitarian systems.
I understand now how wrong (and criminal) that was.
Watching the Israelis whip out their yellow Stars of David at the Security Council clarified for me when it is and isn’t appropriate to compare things to the Nazis.
Check me, but I think I’ve got it straight now.
When governments and non-governmental entities roll out a “New Normal” on account of a completely fictional “apocalyptic pandemic,” lock people down in their homes for months, terrorize them with official propaganda, force everybody to wear medical-looking masks to display their conformity to the new official “reality” and create the appearance of a deadly plague, outlaw political protests, censor dissent, segregate and demonize anyone refusing to conform to the new official ideology, and otherwise transform societies into pathologized de facto police states, those governments and global non-governmental entities are absolutely nothing like the Nazis.
On the other hand, Hamas, the Islamist political and military organization that governs the Gaza Strip, is definitely exactly like the Nazis … except that there are only around 25,000 of them, and their “Reich” is a tiny stretch of land that has been totally blockaded by Israel for years, and is completely surrounded by an “Israel-Gaza barrier,” and has been under Israeli military occupation since 1967. But, otherwise, Hamas is exactly like the Nazis!
See, the thing I didn’t quite understand when I tweeted my thoughtcrimes in 2022 was that being “exactly like the Nazis” has nothing to do with the actual history of Nazi Germany or totalitarianism per se. I was operating under the assumption that it did. That’s no excuse. I should have known better. Obviously, no one should ever be allowed to compare the rise of Nazism in Germany to any other totalitarian system or movement, no matter how blatantly similar it may be. In fact, the history of the rise of Nazism in Germany is irrelevant to, well, basically everything, unless your discussion is strictly limited to the Holocaust, or if you’re relativizing the Holocaust in defense of Israel’s right to defend itself … in which case, sure, break out those yellow stars and go nuts with the Holocaust comparisons.
Seriously, check my reasoning on this, because I don’t want to get it wrong again and end up facing yet another prosecution. Based on my new post-epiphany understanding, questioning the details of the official account of the October 7 attack is “Holocaust denial.” Hundreds of thousands of people peacefully demonstrating in support of Palestinians is a “hate march.” “Hamas Holocaust denial is dragging us into a new Dark Age.” The October 7 massacre was “barbarism as consequential as the Holocaust,” or at least as barbaric as the Babyn Yar massacre!
How am I doing? Am I good so far? I haven’t relativized the Holocaust, have I?
OK, one more test, just to make sure I’ve got my mind right around this stuff. If I, or anyone, were to compare what the State of Israel is doing to the Palestinians in Gaza to, I don’t know, let’s say, just hypothetically, the liquidation of the Warsaw ghetto, that would be completely inappropriate, and anti-Semitic, and a hate crime, right? I mean, the IDF isn’t liquidating the strip. They’re defending Israel against Hamas, and are doing their best to protect civilians as they bomb whole neighborhoods into heaps of rubble, wiping out thousands of men, women, and children, entire extended families, who are trapped inside the “Israel-Gaza barrier,” and have nowhere to run or hide from the slaughter.
If anyone were to make that comparison, that would definitely be relativizing the Holocaust, right? That would be like calling for “the extermination of the Jews,” or literally dressing up like Hitler and walking around barking Nazi slogans in public. In fact, anyone comparing the Israeli-occupied Gaza Strip to the Warsaw Ghetto, or to any other enclave of any other Nazi-occupied territory, is relativizing, minimizing, and trivializing the Holocaust, and should be fired from their job, blacklisted, and publicly condemned as “a Hamas-loving anti-Semite.”
Help me out. Am I getting the hang of this?
I hope so. All I can do at this point is apologize for leading people astray with all that stuff I wrote about “The New Normal Reich” and “pathologized totalitarianism” during 2020-2022. That, and try to make amends by humiliating myself on social media …

… which seems to be going pretty well so far.
Anyway, I am terribly sorry. No more “Holocaust relativizing” for me! I have seen how it is wrong, and terribly wrong, to compare anything to Nazi Germany, ever. I have learned my lesson. I’m cured! Praise god!
Featured Video

9/11 Suspects: General Ralph Eberhart
or go to
Aletho News Archives – Video-Images
From the Archives
From glorious millennia to death and destruction: Zionists rewrite Palestine’s story

By Miko Peled | MintPress News | September 20, 2021
One of the great tragedies of Palestine is that almost every day there is a commemoration of one massacre or another, the death of a child or destruction of a home or village, leading one to think that the Palestinian narrative is one of death and destruction, which is what Israel wants people to think. But the truth is that this is not the case. The Palestinian narrative is one of a glorious history with periods of great sadness and tragedy. It is the Zionist story that is full of killing, stealing and destruction and not, as they try to sell it, one of creation and growth.
September 16, 2021, marked 39 years since the massacres at Sabra and Shatila refugee camps in Lebanon. As people remember and mourn the thousands of unarmed civilians who were butchered and the countless who survived suffering terrible injuries and emotional scars, we must also remember the man that stood behind this bloodbath.
This was a man whose complicity even the Israeli authorities could not ignore, the former general and renowned war criminal Ariel Sharon. And although he was momentarily penalized and banished from politics, he very quickly returned, and for a quarter of a century, he was the most powerful and influential man in Israeli politics. … continue
Blog Roll
 Aletho News
Aletho News- Iran to deepen ties with ‘principal strategic partner’ China: Ghalibaf
- House Votes to Terminate Iran War, While Preparing to Vote to Ramp Up the Ukraine War
- IRGC: No peace without Israel’s withdrawal from occupied Lebanese territories
- Israeli war chief vows continued strikes on Lebanon as part of ‘conditional’ truce
- UNIFIL peacekeeper killed after shells strike position near Marjayoun
- Hours after reiterating ‘ceasefire’, ‘Israel’ targets car in S.Lebanon
- US says Lebanon, Israel reach new ceasefire deal, Hezbollah vows resistance, rejects disarmament
- Trump’s call to Bibi probably didn’t happen
- Iran moved to change the US-Iran equation yesterday
- Former Israeli soldier: I left the Gaza war with shame and regret
- If Americans Knew
- The battle for Al-Aqsa: How Israel is reshaping the status quo
- Israeli study finds starvation in Gaza was result of deliberate policy
- US-Israel integration in NDAA is far from ‘America First’ – Joe Kent
- Now will the world believe? Israeli study finds starvation in Gaza was deliberate policy – Daily Update
- The Faustian Bargain of Journalists Embedding with the Israeli Military in Gaza
- AIPAC: Defending the Indefensible
- “You Either Leave Right Now or You Die”—Israel’s Ethnic Cleansing of a Village in Lebanon
- Selling American dead bodies to the US Navy for Israeli military training?
- AIPAC affiliate has funded lavish trips to Israel for dozens of Congress members since 7 October, filings reveal
- Trump called Netanyahu crazy, stopped Israel attack on Beirut: three articles
- No Tricks Zone
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
