WHO Renews Push for Global Pandemic Treaty, as World Bank Creates $1 Billion Fund for Vaccine Passports
By Michael Nevradakis, Ph.D. | The Defender | August 9, 2022
The World Health Organization (WHO) is moving ahead with plans to enact a new or revised international pandemic preparedness treaty, despite encountering setbacks earlier this summer after dozens of countries, primarily outside the Western world, objected to the plan.
A majority of WHO member states on July 21, during a meeting of WHO’s Intergovernmental Negotiating Body (INB), agreed to pursue a legally binding pandemic instrument that will contain “both legally binding as well as non-legally binding elements.”
STAT News described the agreement, which would create a new global framework for responding to pandemics, as “the most transformative global health call to action since [the] WHO itself was formed as the first specialized United Nations agency in 1948.”
Meanwhile, the World Economic Forum, African Union and World Bank — which created a $1 billion fund for “disease surveillance” and “support against the current as well as future pandemics” — are developing their own pandemic response mechanisms, including new cross-country vaccine passport frameworks.
WHO’s ‘pandemic treaty’: what’s been proposed and what would it mean?
Ongoing talks to formulate a new or revised “pandemic treaty” are building on the existing international framework for global pandemic response, the WHO’s International Health Regulations (IHR), considered a binding instrument of international law.
On Dec. 1, 2021, in response to calls from various governments for a “strengthened global pandemic strategy” and signaling the urgency with which these entities are acting, the WHO formally launched the process of creating a new treaty or amending the IHR, during Special Session — only the second in the organization’s history.
During the meeting, held May 10-11, WHO’s 194 member countries unanimously agreed to launch the process, which previously had been discussed only informally.
The member countries agreed to:
“Kickstart a global process to draft and negotiate a convention, agreement or other international instrument under the Constitution of the World Health Organization to strengthen pandemic prevention, preparedness and response.”
The IHR, a relatively recent development, were first enacted in 2005, in the aftermath of SARS-CoV-1.
The IHR legal framework is one of only two binding treaties the WHO has achieved since its inception, the other being the Framework Convention on Tobacco Control.
The IHR framework already allows the WHO director-general to declare a public health emergency in any country, without the consent of that country’s government, though the framework requires the two sides to first attempt to reach an agreement.
The proposals for a new or revised pandemic treaty, put forth at the special ministerial session of the WHO in May, would “somewhat” strengthen the WHO’s pandemic-related powers, including establishing a “Compliance Committee” that would issue advisory recommendations for states.
However, according to the Daily Sceptic, while the IHR is already legally binding, the amendments proposed in May would not strengthen existing legal obligations or requirements:
“The existing treaty regulations, like all (or most) international law, do not actually compel states to do anything other than talk to the WHO and listen to it, and neither do they specify sanctions for non-compliance; almost all their output is advice.
“The proposed amendments don’t alter that. They don’t allow the WHO unilaterally to impose legally binding measures on or within countries.”
The Daily Sceptic noted one of the risks stemming from the negotiations for a new or updated treaty include the potential codification of “the new lockdown orthodoxy for future pandemics,” which would “replace the sound, science-based, pre-COVID recommendations” previously in place.
According to Dr. Joseph Mercola, such a treaty would grant the WHO “absolute power over global biosecurity, such as the power to implement digital identities/vaccine passports, mandatory vaccinations, travel restrictions, standardized medical care and more.”
Mercola also questioned a “one-size-fits-all approach to pandemic response,” pointing out that “pandemic threats are not identical in all parts of the world. In his view, he said, “the WHO is not qualified to make global health decisions.”
Similar concerns contributed at least in part to opposition against the proposals presented at the special ministerial session, during which a bloc of mostly non-Western countries, including China, India, Russia and 47 African nations, prevented an agreement from being finalized.
Will opposition fade away?
Although no final agreement was achieved at the May meeting, consensus was reached to organize a new special ministerial session of the WHO later this year, possibly after the WHO’s World Health Assembly, scheduled for Nov. 29 through Dec. 1, Reuters reported.
Mxolisi Nkosi, South Africa’s ambassador to the UN, told the WHO’s annual ministerial assembly the new special session would “consider the benefits for such a convention, agreement or other international instrument.”
Nkosi added:
“Probably the most important lesson COVID-19 has taught us is the need for stronger and more agile collective defences against health threats as well as for building resilience to address future potential pandemics.
“A new pandemic treaty is central to this.”
At the time, the U.K.’s ambassador to the UN, Simon Manley, addressing the lack of an immediate agreement and the consensus to hold a new meeting, tweeted “negotiations may take time, but this is a historic step towards global health security.”
The INB, at its meeting held in Geneva July 18-21, also agreed with this view, reaching a consensus that its members will work on finalizing a new legally binding international pandemic agreement by May 2024.
As part of this process, the INB will meet again in December and will deliver a progress report to the 76th World Health Assembly of the WHO in 2023.
According to the WHO, “Any new agreement, if any when agreed by Member States, is drafted and negotiated by governments themselves, [which] will take any action in line with their sovereignty.”
The WHO further claims that “governments themselves will determine actions under the accord while considering their own national laws and regulations.”
The Biden administration expressed broad support for a new or updated pandemic treaty, with the U.S. heading previous negotiations on this issue, along with the European Commission, via its president Ursula von der Leyen, who, as previously reported by The Defender, is also a strong proponent of vaccine passports and mandatory COVID-19 vaccination.
An analysis by the Alliance for Natural Health International speculated that any final agreement may simply strengthen the existing IHR or, alternatively, may involve an amendment to the WHO’s constitution — or both.
Just two days after the July 21 INB agreement, Tedros Adhanom Ghebreyesus, the WHO’s director-general, tweeted:
“I’m pleased that alongside the process of negotiating a new [international] accord on pandemic preparedness & response, WHO’s Member States are also considering targeted amendments to the [IHR], incl. ways to improve the process for declaring a [public health emergency of international concern, or PHEIC].”
In the same Twitter thread, he also declared the ongoing monkeypox outbreak “a public health emergency of international concern,” one “that is concentrated among men who have sex with men, especially those with multiple sexual partners.”
Notably, the WHO director-general overruled an expert panel that was divided over whether to classify the outbreak as a global public health emergency.
With this declaration, three “global health emergencies” are now in place, as determined by the WHO: COVID-19, monkeypox and polio.
Busy summer for vaccine passport proposals
While the WHO and global governments weigh plans for an updated or new pandemic treaty, other organizations are moving forward on vaccine passport technologies and partnerships.
On July 8, the Organisation for Economic Cooperation and Development (OECD), composed of many of the world’s industrialized nations, announced it would promote the unification of the different vaccine passport systems currently in use around the world.
Thirty-six countries and international organizations participated in a July meeting with the goal of “creating a multilateral framework for establishing a global vaccine passport regime,” according to Nick Corbishley of Naked Capitalism.
The development is a continuation of efforts involving the WHO to harmonize global vaccine passport regimes.
In February, the WHO selected Germany’s T-Systems as an “industry partner to develop the vaccination validation service,” which would enable “vaccination certificates to be checked across national borders.”
T-Systems, an arm of Deutsche Telekom, was previously instrumental in developing the interoperability of vaccine passport systems in Europe.
Also in July, 21 African governments “quietly embraced” a vaccine passport system, which in turn would also be interlinked with other such systems globally.
On July 8, which is also Africa Integration Day, the African Union and the Africa Centers for Disease Control launched a digital vaccine passport valid throughout the African Union, describing it as “the e-health backbone” of Africa’s “new health order.”
This follows the development in 2021, of the Trusted Travel platform, now required by several African countries, including Ethiopia, Kenya, Togo and Zimbabwe, and air carriers such as EgyptAir, Ethiopian Airlines and Kenya Airways, for both inbound and outbound travel.
Beyond Africa, Indonesia, which currently holds the rotating presidency of the G20, is conducting “pilot projects” that would bring about the interoperability of the various digital vaccine passport systems currently in use globally. The project is expected to be completed by November, in time for the G20 Leaders’ Summit.
Naked Capitalism highlighted the role of South African company Cassava Fintech in the efforts to develop an interoperable vaccine passport for all of Africa.
A subsidiary of African telecommunication company Econet, Cassava initially developed the “Sasail” app, which the company described as Africa’s first “global super app” that combines “social payments” with the ability to send and receive money and pay bills, chat with others and play games.
Cassava and Econet entered into a strategic partnership with Mastercard, “to advance digital inclusion across Africa and collaborate on a range of initiatives, including expansion of the Africa CDC TravelPass.”
As previously reported by The Defender, Mastercard supports the Good Health Pass vaccine passport initiative that is also backed by the ID2020 alliance and endorsed by embattled former U.K. prime minister Tony Blair.
Mastercard has also promoted technology that can be embedded into the DO Card, a credit/debit card that keeps track of one’s “personal carbon allowance.”
ID2020, founded in 2016, claims to support “ethical, privacy-protecting approaches to digital ID.” Its founding partners include Microsoft, the Rockefeller Foundation, Accenture, GAVI-The Vaccine Alliance (itself a core partner of the WHO), UNICEF, the Bill & Melinda Gates Foundation and the World Bank.
Mastercard’s top two stockholders are Vanguard and BlackRock, which hold significant stakes in dozens of companies that supported the development of vaccine passports or implemented vaccine mandates for their employees. The two investment firms also hold large stakes in vaccine manufacturers, including Pfizer, Moderna and Johnson & Johnson.
Mastercard provides funding for the World Bank’s Identity for Development (ID4D) Program, which “focuses on promoting digital identification systems to improve development outcomes while maintaining trust and privacy.”
The Center for Human Rights and Global Justice at the New York School of Law recently described the ID4D program, which touts its alignment with the UN’s Sustainable Development Goals (SDGs) , as one which could pave the way to a “digital road to hell.”
According to the center, this would occur through the prioritization of “economic identity” and the use of an infrastructure that has “been linked to severe and large-scale human rights violations” in several countries.
Mastercard is also active in Africa through its joint initiative with another fintech (financial technology) company, Paycode, to “increase access to financial services and government assistance for remote communities across Africa” via a biometric identity system containing the data of 30 million individuals.
World Bank, WHO promote ‘pandemic preparedness’ and vaccine passports
The World Bank in late June announced the creation of a fund that will “finance investments in strengthening the fight against pandemics” and “support prevention, preparedness and response … with a focus on low- and middle-income countries.”
The fund was developed under the lead of the U.S., Italy and current G20 president Indonesia, “with broad support from the G20,” and will be active later this year.
It will provide more than $1 billion in funding for areas such as “disease surveillance” and “support against the current as well as future pandemics.”
The WHO is also a “stakeholder” in the project and will provide “technical expertise,” according to WHO’s director-general.
The agreement follows a 2019 strategic partnership between the UN and the World Economic Forum, to “accelerate” the implementation of the UN’s 2030 Agenda for Sustainable Development and its SDGs.
Although the agreement has recently circulated on social media, it was announced in June 2019, prior to the COVID-19 pandemic. It encompasses six areas of focus, including “health” and “digital cooperation.”
In terms of health, the agreement purports that it will “support countries [sic] achieve good health and well-being for all, within the context of the 2030 Agenda, focusing on key emerging global health threats that require stronger multistakeholder partnership and action.”
In turn, the “digital cooperation” promoted by the agreement will purportedly “meet the needs of the Fourth Industrial Revolution while seeking to advance global analysis, dialogue and standards for digital governance and digital inclusiveness.”
However, despite rhetoric preaching “inclusiveness,” individuals and entities that have refused to go along with applications such as vaccine passports have faced repercussions in their personal and professional lives.
Such was the example of a Canadian doctor who was fined $6,255 in June over her refusal to use the country’s ArriveCAN health information app — which is being investigated over privacy concerns — to enter the country.
Dr. Ann Gillies said she was fined when re-entering Canada after attending a conference in the U.S.
Andrew Bud, the CEO of biometric ID company iProove, a U.S. Department of Homeland Security contractor, described vaccine certificates as driving “the whole field of digital ID in the future,” adding they are “not just about COVID [but] about something even bigger” and that “once adopted for COVID [they] will be rapidly used for everything else.”
Michael Nevradakis, Ph.D., is an independent journalist and researcher based in Athens, Greece.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
U.S. Declares Monkeypox Health Emergency, FDA Offers Vaccine to Some Kids Despite No Clinical Trials
By Megan Redshaw | The Defender | August 5, 2022
The U.S. declared monkeypox a public health emergency to raise awareness and allow for additional funding to fight the disease’s spread, U.S. Department of Health and Human Services Secretary Xavier Becerra said on Thursday.
“We’re prepared to take our response to the next level in addressing this virus, and we urge every American to take monkeypox seriously and to take responsibility to help us tackle this virus,” Becerra said.
Becerra said he also is considering a second declaration that would allow federal officials to expedite medical countermeasures — such as potential treatments and vaccines — designed to ensure drugs are safe and effective.
President Biden said in a tweet he remained “committed to our monkeypox response: ramping-up vaccine distribution, expanding testing, and educating at-risk communities.”
“That’s why today’s public health emergency declaration on the virus is critical to confronting this outbreak with the urgency it warrants,” Biden said.
The last time the U.S. declared a public health emergency was in January 2020, for COVID-19.
According to the Centers for Disease Control and Prevention (CDC), more than 7,100 cases of monkeypox have been reported in the U.S., including five cases in children.
Symptoms of monkeypox infection are usually mild and include fever, rash and swollen lymph nodes, and occasionally intense headache, back pain, muscle aches, lack of energy and skin eruptions that can cause painful lesions, scabs or crusts.
The virus is rarely fatal and no deaths have been reported in the U.S.
Monkeypox primarily is spread through skin-to-skin contact during sex and affects mostly gay and bisexual men, public health officials say, although the virus can affect anyone.
According to the CDC, about 98% of monkeypox patients who provided demographic information to clinics identified as men who have sex with men.
Public health emergency paves way for vaccine for kids
Now that the Biden administration has declared the monkeypox outbreak a public health emergency, the U.S. Food and Drug Administration (FDA) can move to issue an Emergency Use Authorization for the JYNNEOS vaccine for children under 18.
There are two vaccines that may be used “for the prevention” of monkeypox virus infection: JYNNEOS — also known as Imvamune or Imvanex — and ACAM2000, which is licensed by the FDA for use against smallpox and “made available for use against monkeypox under an Expanded Access Investigational New Drug application.”
The FDA told ABC News on Thursday that while the current monkeypox vaccine, JYNNEOS, is approved only for adults ages 18 and older, it will be available for kids on a case-by-case basis.
The JYNNEOS vaccine, delivered in a two-dose series, was not tested through clinical trials in children.
However, the FDA confirmed to ABC News that “numerous” children have been granted access to the vaccine through a special permission process, but declined to state exactly how many children have received the vaccine to date through this process.
“If a doctor decides a person under 18 was exposed to monkeypox and the benefit of the vaccine is greater than any potential risk, they can submit a request to the FDA,” ABC News reported.
According to the CDC, the “immune response” takes “14 days after the second dose of JYNNEOS and 4 weeks after the ACAM2000 dose for maximal development.”
The CDC website also states: “No data are available yet on the effectiveness of these vaccines in the current outbreak.”
According to the latest data from the Vaccine Adverse Event Reporting System (VAERS), between June 14 and July 21, 2022, 31 adverse events were reported following vaccination with JYNNEOS — manufactured by Bavarian Nordic.
The World Health Organization (WHO) declared monkeypox a global health emergency after more than 26,000 cases were reported across 87 countries.
A global emergency is the WHO’s highest level of alert, but the designation does not necessarily mean a disease is particularly transmissible or lethal.
The U.S. makes up 25% of confirmed cases globally although the U.K. was the first to alert the world to the outbreak in May after confirming several cases.
A monkeypox fictional simulation was held in March 2021
As The Defender reported in May, the Nuclear Threat Initiative, in conjunction with the Munich Security Conference, in March 2021 held a “tabletop exercise on reducing high-consequence biological threats,” involving an “unusual strain of monkeypox virus that first emerged in the fictional nation of Brinia and spread globally over 18 months.”
This is similar to “Event 201,” a “high-level pandemic exercise” organized by the Johns Hopkins Center for Health Security, along with the World Economic Forum and the Bill & Melinda Gates Foundation — just weeks before the COVID-19 outbreak — that mirrored what later followed with COVID-19 pandemic.
According to the Nuclear Threat Initiative, the monkeypox exercise, which was “developed in consultation with technical and policy experts,” brought together “19 senior leaders and experts from across Africa, the Americas, Asia, and Europe with decades of combined experience in public health, biotechnology industry, international security, and philanthropy.”
The fictional start date of the monkeypox pandemic in this exercise was May 15, 2022. The first European case of monkeypox was identified on May 7, 2022.
Key participants in the simulation included Johnson & Johnson and Janssen, the Bill & Melinda Gates Foundation, the Chinese Centers for Disease Control and Prevention, the Nuclear Threat Initiative, GAVI — the Vaccine Alliance, Merck and the WHO.
Several of the participants listed above also “participated” in Event 201.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
WHO Wants To Run the World?
By Paul Frijters, Gigi Foster, Michael Baker | Brownstone Institute | July 11, 2022
In Geneva in late May at the 75th meeting of the WHO’s decision-making body, the World Health Assembly (WHA), amendments to its International Health Regulations (IHRs) were debated and voted upon. If passed, they would grant the WHO the right to exert unconscionable pressure on countries to accept the WHO’s authority and health policy actions if the WHO decides that there is a public health threat that might spread beyond a country’s borders.
As Ramesh Thakur, the second man at the UN for years, noted, the amendments would mean “the rise of an international bureaucracy whose defining purpose, existence, powers and budgets will depend on outbreaks of pandemics, the more the better.”
This is the first clear instance of a globalist coup attempt. It would subvert national sovereignty worldwide by putting real power into the hands of an international group of bureaucrats. It has long been suspected that the authoritarian elites arisen during covid times would try to strengthen their positions by undermining nation states, and the this 75th jamboree is the first solid evidence of this being true.
What an opportunity then to see who is in the conspiring club. Who drafted the amendments? What was in them? Which individuals supported them or spoke out against them?
WHO were the conspirators?
The amendments on the table at the May WHA meeting had been transmitted to the WHO by the US Department of Health and Human Services on January 18, circulated by WHO to its member states (‘States Parties’) on January 20 and formally introduced to the WHA on April 12.
The proposals, according to an announcement on January 26, were co-sponsored by 19 countries plus the European Union. Even if some co-sponsors had little direct involvement in drafting them, they all would have approved in principle the overarching goal of tightening up the WHO’s authority over member states in the face of a public health event.
Loyce Pace, the HHS’s Assistant Secretary for Global Affairs – the leading US official nominally responsible for the proposed amendments – arrived at the Biden administration fresh from a stint as executive director of an advocacy organization called the Global Health Council.
That council receives funding from the Bill & Melinda Gates Foundation and its members include Eli Lilly, Merck, Pfizer, Abbott Labs, and Johnson & Johnson. You get the idea. Via one of the foxes-turned-chicken-guard, it appears the HHS ‘worked closely’ on these amendments with large pharmaceutical companies, who will be chomping at the bit for a more proactive (read: profitable) response to any public health emergency, real or imagined.
So the conspiring club consists primarily of the US government and its Western allies in lockstep with Big Pharma, and they are looking to undermine both the sovereignty of their own governments and that of other countries, presumably with the idea that the Western elites would do the running.
What was in them? A blizzard of acronyms and euphemisms
To understand what the US proposed at the WHA, we need first to understand how things have worked in the WHO to this point.
The IHRs in their current form have been in force as international law since June 2007. Among other things, they impose requirements on countries to detect, report and respond to ‘public health events of international concern,’ or PHEICs. The WHO Director-General consults with the state where a possible public health event has occurred, and within 48 hours they are meant to come to a mutual agreement on whether or not it actually is a PHEIC, whether or not it needs to be announced to the world as such, and what counter-measures, if any, should be taken. It’s essentially an early-warning system on major health crises. This is a good thing if it’s run by people you can trust and if it has checks and balances to rein in expansionary tendencies.
The proposed amendments would greatly strengthen the power of the WHO relative to this baseline, in a number of ways.
First, they lower the threshold for the WHO to declare a public health emergency by empowering its Regional Directors to declare a ‘public health event of regional concern’ (PHERC, italics ours) and for the WHO to put out a new thing called an ‘intermediate public health alert.’
Second, they permit the WHO to consider allegations about a public health event from non-official sources, meaning sources other than the government of the state concerned, and allow that government only 24 hours to confirm the allegations and a further 24 hours to accept the WHO’s offer of ‘collaboration.’
Collaboration is essentially a euphemism for on-site assessment by teams of WHO investigators, and concomitant pressure at the whim of WHO personnel to enact potentially far-reaching measures such as lockdowns, movement restrictions, school closures, consumption of medicines, administration of vaccines and any or all of the other social, economic, and health paraphernalia that we have come to associate with the covid circus.
Should the state’s government acceptance of the WHO’s ‘offer’ not be forthcoming, the WHO is empowered to disclose the information it has to the other 194 WHO countries, while continuing to pressure the state to yield to the WHO’s invitation to ‘collaborate.’ A non-collaborating country would risk becoming a pariah.
Third, the proposal includes a new Chapter IV, which would establish a ‘Compliance Committee’ consisting of six government-appointed experts from each WHO region tasked with permanently nosing around to ensure the member states are complying with IHR regulations.
There are more crossings-out of the existing IHR language and new language added in, but the flavour of what the US-led alliance is shooting for is a WHO that can unilaterally decide whether there is a problem and what to do about it, and can isolate countries that disagree.
Compliant WHO member states could act as a supporting cast in the isolation effort, through the distribution of their own health budgets and their ‘health-related’ policies, which would include travel and trade restrictions. The WHO would become a kind of command-and-control center for globalist agendas, pushing the produce of (Western) Big Pharma.
Why and how would this work?
We learned during covid times why it would make sense that the US and its allies are insisting on these amendments.
Lowering the bar for declaring a global (or regional) public health threat triggers a huge opportunity for Western pharmaceutical companies. As legal experts have observed: “WHO emergency declarations can trigger the fast-track development and subsequent global distribution and administration of unlicensed investigational diagnostics, therapeutics and vaccines.
This is done via the WHO’s Emergency Use Listing Procedure (EULP). The introduction of an ‘intermediate public health alert’ in particular will also further incentivise the pharmaceutical industry’s move to activate domestic fast-track emergency trial protocols as well as for advance purchase, production and stockpile agreements with governments before the existence of a concrete health threat to the world’s population has been detected, as is already the case under WHO’s EULP via the procedures developed for a ‘pre-public health emergency phase’.”
You can bet that the WHO ‘expert teams’ sent in to make on-the-ground assessments, under the banner of ‘collaboration’ with the host country experiencing the health event, will be chock-a-block with operatives from the CDC and who knows what other Western agencies, all poking around potentially sensitive facilities that a host government might justifiably claim a sovereign right to keep to itself. Likewise with the ‘Compliance Committee’ proposed by the US under the new Chapter IV of the IHRs: its government-appointed members have an open-ended brief, enshrined in international law, to be busybodies.
In layman’s terms, the WHO would be turned into an international thug, with its member states offered the role of backyard gang members.
As a bonus for Western elites, the proposals are a sneaky form of rewriting history. By cementing authority within an international organisation to determine the existence of public health crises and direct potentially draconian emergency responses, Western governments would get to enshrine and legitimise their own extreme responses to the covid outbreak, as we have pointed out previously. Their backsides would thereby be given some protection from legal challenges.
The refusniks: Developing countries
The proposals were pushed primarily by Western countries: the US was joined by Australia, the UK and the EU in arguing for passage. The resistance was led by developing countries who saw it as a colonialist ambush in which their ability to set policy and respond to health threats in a manner commensurate with their domestic situations would be overridden.
Brazil reportedly went so far as to threaten to withdraw from the WHO, and the African group of almost 50 countries, along with India, argued that the amendments were being rushed through without adequate consultation. Russia, China and Iran also objected.
Failure on the first try, but the US and its allies in the West will get more shots to push it through.
How do we expect them to do this? Well, when a proposal gets bogged down inside a giant bureaucratic machine like the WHO, the inevitable response is to set up committees to work in the background and circle back with a new set of proposals to be presented at a future meeting. True to form, a ‘working group’ and ‘expert committee’ are being assembled to accept member state proposals on IHR reform by the end of September this year. These will be ‘sifted through’ and reports will be prepared for review by the WHO’s executive board in January next year. The objective is to have a fresh set of proposals on the table when the WHA convenes for the 77th time in 2024.
Not all was lost
Salvaging something from the fact that the WHA failed to get a consensus around its biggest agenda item, the US and its allies got a small victory on the point of when they can try again – though in their desperation they needed to violate the IHRs’ own rules to accomplish it. Article 55 of the IHRs states unambiguously that a four-month notice period is required for any amendments.
In this instance, revised amendments were presented on May 24, the same day that the first lot were rejected. These were discussed, further amended on May 27 and then adopted on the same day. The approved amendments halve the two-year period for any (further) approved amendments to the IHRs to take effect. (The IHRs that came into force in 2007 were agreed to in 2005 – but under the new resolution, anything agreed to in 2024 would come into effect in 2025 rather than 2026.)
Yet, what was achieved in terms of fast-tracking the force of new amendments was lost in slow-tracking their implementation. Nations would have up to 12 months – double the previous suggestion of six months – to implement any IHR amendments that newly enter into force of law.
State of play
Where is all this going?
If the WHO takes the reins on decisions about what constitutes a health crisis, and can pressure every country into a one-size-fits-all set of responses that it, the WHO, also determines, that’s bad enough. But what about if its invitation to ‘collaborate’ with countries is backed up with teeth, such as sanctions against those who demur? And what about if it then broadens the definition of ‘public health’ by, for example, declaring that climate change falls under that definition? Or racism? Or discrimination against LBTQIA+ people? The possibilities thereby opened up for running the world are endless.
A global ‘health’ empire would bring huge harms to humanity, but a lot of power and money is pushing for it. Don’t think it can’t happen.
Paul Frijters is a Professor of Wellbeing Economics at the London School of Economics: from 2016 through November 2019 at the Center for Economic Performance, thereafter at the Department of Social Policy
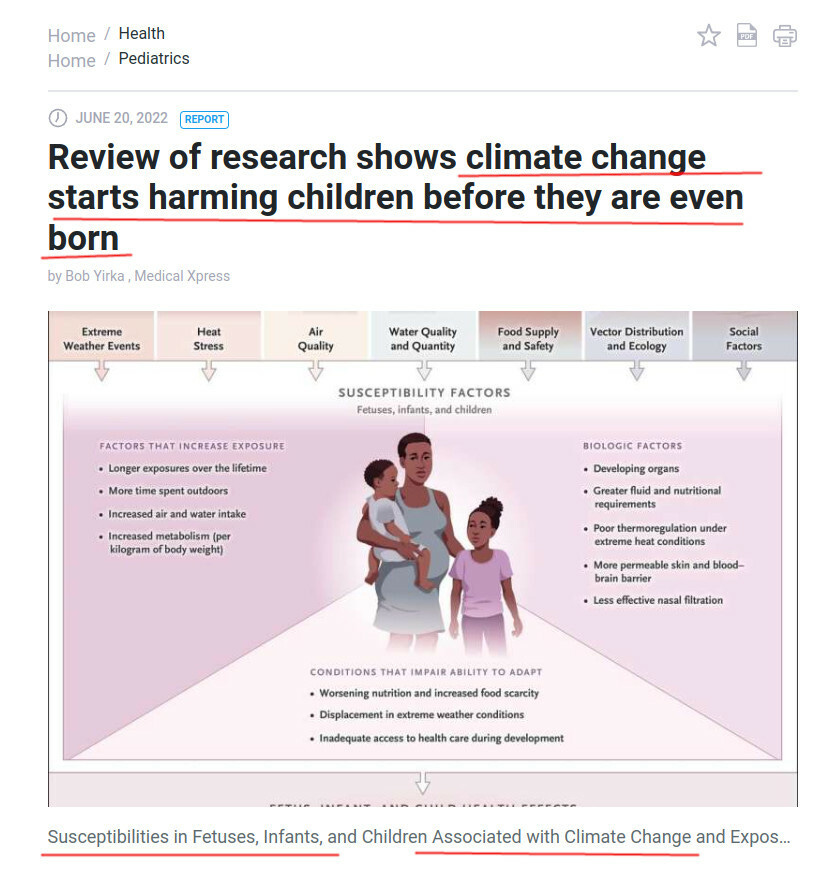
NEJM: Global Warming Causes Stillbirths, Birth Defects, Infant Heart problems
Finally you can laugh a bit
By Igor Chudov | June 28, 2022
Okay, enough birth rate sadness, let’s lighten up a bit. We have a long road ahead of us, we cannot be sad all the time, so it is time to smile.
We have some climate change news.
Remember that a couple of days ago, I asked, why is the birth rate in Germany dropping? What is going on with a 23% drop in live births in Taiwan? Why are births dropping 10% in Switzerland this year? Why is the UKHSA vaccine surveillance report not reporting live births since February, for which it showed a 10% year-to-year drop in live births, and nothing since?
Fortunately, science has an answer for us. These baby problems have a known cause. It is climate change. Here’s an amazing article. It came out just in time for the birth rate scandal, which is obviously just a coincidence.
This article refers to a study, published in New England Journal of Medicine, a prestigious bellwether of medical science and a guide to all doctors worldwide.

The article explains that global warming may cause many problems in developing and unborn children. “All children are at risk”, says the study. Some of these problems are very familiar to us, and I am glad that scientists finally could attribute them to global warming.
Let me list them, coming verbatim from the NEJM article:
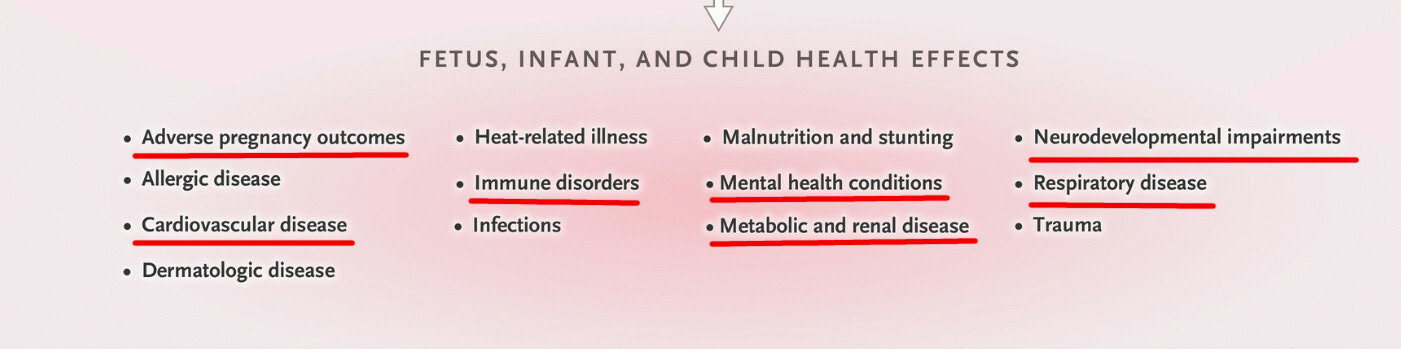
The article, further, admonishes physicians to be aware of the new medical consensus:
Protection of children’s health requires that health professionals understand the multiple harms to children from climate change
So if parents ask a doctor, why are their children having heart problems, neurological issues, etc, the doctor would be able to cite the NEJM article and explain how those problems are caused by climate change.
One of the two coauthors of this global warming article, Kari Nadeau, is a well-published scientist who also published an interesting study explaining why vaccine-induced immunity is better than natural immunity. That study was, purely coincidentally, financed by the Bill and Melinda Gates Foundation. It also contradicts everything that we know from practical experience, of course. What else did you expect?

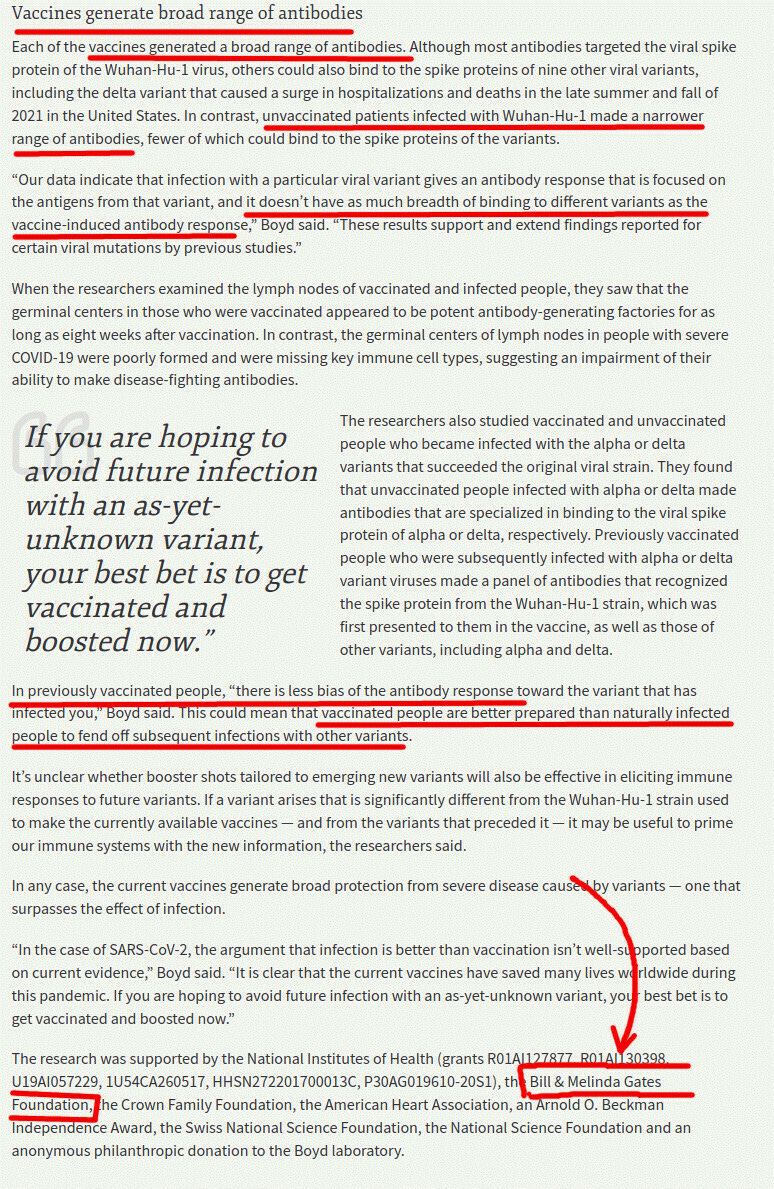
Financing of such authors by the Bill and Melinda Gates Foundation, obviously, is nothing to worry about. I also wonder, how can Kari Nadeau be equally good at writing on matters of immune imprinting and immunology, as well as on totally unrelated matters of climate change? I am not sure.
WHO Recommends New Gates-Funded Polio Vaccine to Address Vaccine-Derived Polio Outbreak in U.K.
By Megan Redshaw | The Defender | June 27, 2022
Health officials in the U.K. this month identified the country’s first polio outbreak in 40 years, and believe the outbreak was caused by a strain of polio found in the oral polio vaccine.
Health officials in Britain warned parents on June 22 to ensure their children have been vaccinated against polio after multiple closely related versions of the virus that cause the disease were found in sewage water at the London Beckton Sewage Treatment Works — the largest water treatment plant in the U.K.
“The Global Polio Laboratory Network has confirmed the isolation of type 2 vaccine-derived poliovirus (VDPV2) from environmental samples in London, United Kingdom, which were detected as part of ongoing disease surveillance,” the World Health Organization (WHO) states on its website.
The U.K. Health Security Agency (UKHSA) said it believes the virus was “vaccine-derived,” meaning it came from someone who received the live polio vaccine. That person then passed the virus to individuals in London, who shed the virus into their feces.
The viruses’ genetic sequences suggest “there has been some spread between closely linked individuals in north and east London,” the UKHSA said.
The virus was isolated from environmental samples collected between February and May, and no related cases of paralysis have been detected, the WHO said. “Additional sewage samples collected upstream from the main waste-water treatment plant’s inlet are being analyzed.”
People vaccinated with the live oral polio vaccine (OPV) shed traces of the virus in their stool — which eventually end up in sewage wastewater, NPR reported. Scientists believe a person brought the virus into London and then spread it to others who were unvaccinated.
“We are urgently investigating to better understand the extent of this transmission,” Vanessa Saliba, an epidemiologist who consults for the UKHSA, said in the statement.
The risk to the general public is thought to be “extremely low” but the agency encourages anyone not fully vaccinated to receive a polio vaccine.
WHO approves Gates’ oral polio vaccine for emergency use
The WHO on Nov. 13, 2020, granted Emergency Use Listing (EUL) to a new novel oral polio vaccine called nOPV2, designed to treat the type of polio outbreak occurring in the U.K.
Based on the WHO’s review of data and research available on nOPV2, the Strategic Advisory Group of Experts on Immunization (SAGE) recommended Gates’ nOPV2 become the “vaccine of choice” for responding to type 2 polio outbreaks caused by OPV.
The Bill & Melinda Gates Foundation provided 100% of the funding for the development and clinical trials of the vaccine.
The Global Polio Eradication Initiative (GPEI) states on its website:
“The Bill & Melinda Gates Foundation has funded all development and clinical trials of nOPV2 to date, working closely with GPEI partners throughout the process to ensure resources are going toward a tool that could prove critical to helping end all forms of polio.
“Based on promising data from clinical trials, and the public health emergency that cVDPV2 [vaccine-derived poliovirus type 2] constitutes, the Foundation is funding at-risk production of 160 million doses of nOPV2 to ensure it can be deployed immediately following the issuance of WHO’s interim Emergency Use Listing (EUL) recommendation for use.”
“The emergency use listing, or EUL, is the first of its kind for a vaccine” designed to “pave the way for potential listing of COVID-19 vaccines,” the WHO said on its website.
On December 31, 2020, the WHO issued its first EUL listing for a COVID-19 vaccine. According to the WHO, the agency granted the listing for the Pfizer Comirnaty vaccine.
The EUL is a regulatory pathway that allows the WHO — whose second-largest financial donor is the Gates Foundation — to distribute an unlicensed product for a “Public Health Emergency of International Concern,” which the organization claims polio has been since 2014.
The EUL allows vaccines and medicines to be made available more quickly to address health emergencies, without long-term phase 3 data, and is the same mechanism used for distribution of Zika, Ebola and COVID-19 vaccines.
According to the WHO, in “very rare cases,” the administration of OPV results in vaccine-associated paralytic polio associated with a “reversion of the vaccine strains to the more neurovirulent profile of wild poliovirus.”
In addition to causing vaccine-associated paralytic polio, vaccine strains have the capacity to cause disease of the nervous system and to transmit from person to person resulting in infectious poliomyelitis.
Based on the WHO’s review of data and research available on nOPV2, the Strategic Advisory Group of Experts on Immunization (SAGE) recommended Gates’ nOPV2 become the “vaccine of choice” for responding to type 2 polio outbreaks caused by OPV.
According to the Global Polio Eradication Initiative (GPEI), the nOPV2 was developed to address vaccine-derived poliovirus type 2 outbreaks, which “can emerge when the weakened strain of the vaccine virus circulates in under-immunized populations and, with time, can genetically revert into a form that causes paralysis.”
In other words, “under-immunized” populations — not the OPV — are to blame for the vaccine-related polio strains.
In an email to The Defender, Dr. Brian Hooker, Ph.D., P.E., Children’s Health Defense chief scientific officer and professor of biology at Simpson University said:
“Once again, Big Pharma, fueled by the Gates Foundation, has created a huge problem that only they can solve. The introduction of the new OPV in the U.K. has predictably led to polio virus in the sewage (i.e., where poliovirus propagates) and now the “only solution” is to inject U.K. citizens with the nPOV2 to prevent the spread of OPV-induced polio. If this isn’t a scam, I don’t know what is!”
The U.K.’s Medicines and Regulatory Health Products Agency (MHRA) on June 17 said in a tweet: “An exciting new global study, co-authored by our lead scientist Javier Martin, shows that new polio vaccine nOPV2 is an effective tool in reducing the risk of Vaccine-Derived Polio Viruses.“
The tweet linked to a study published by the Centers for Disease Control and Prevention (CDC) advocating for the use of Gates’ nOPV2 vaccine.
Between the launch of nOPV2 in March 2021 and late May 2022, more than 350 million doses had been administered across 18 countries.
The GPEI confirmed, as of May 30, 16 other countries are “ready to use nOPV2” and an additional 17 are in the midst of preparations.
WHO, GPEI and other organizations pushing Gates-funded vaccine
According to UNICEF, the GPEI is a public-private partnership led by national governments with six core partners: Rotary International, the WHO, the CDC, UNICEF, the Gates Foundation and Gavi, the Vaccine Alliance.
The Gates Foundation, in addition to funding the nPOV2 vaccine, GPEI and the WHO, also funds Rotary International, UNICEF, Gavi and the CDC Foundation.
The entity in charge of monitoring vaccine adverse events following administraton of nPOV2 is the WHO’s own Global Advisory Committee on Vaccine Safety (GACVS).
“The GACVS Sub-Committee on nOPV2 Safety will advise WHO and its Member States on safety outcomes following the use of initially pre-licensed type 2 novel oral poliovirus vaccine, during the EUL period, prior to the availability of Phase III clinical trial results,” according to GPEI.
In essence, the Gates Foundation funded the creation, development and clinical trials for the new nPOV2 polio vaccine, funds the organizations that administered millions of doses to be given under EUL without any long-term data, funds the organizations implementing its roll-out and surveillance and funds the entity monitoring adverse events associated with nPOV2’s use.
The Gates Foundation is also a funder of NPR and NPR’s blog, which have published numerous articles on VDPV2 and paved the way for Gates’ nPOV2 vaccine as the solution.
Oral polio v. inactivated polio vaccines
According to the WHO, the original OPV uses a mixture of “live attenuated poliovirus strains of each of the three serotypes,” selected for their ability to mimic the immune system’s response following infection with wild polioviruses, but with a reduced chance of spreading to the central nervous system.
To achieve the desired immune response, three or more doses of OPV are required spaced out over a period of time.
The U.S. and some western countries use an inactivated (killed) polio vaccine (IPV) developed by Dr. Jonas Salk and first used in 1955.
Scientists claim the inactivated virus poses no risk of spread, although the Vaccine Adverse Event Reporting system shows two reported cases of poliomyelitis reported following vaccination with IPV.
The U.S. stopped using OPV in 2000 because it caused paralytic polio.
According to NPR, countries in Africa, the Middle East and parts of Asia are experiencing a rise in cases of vaccine-derived polio. These countries mostly use the OPV developed by Albert Sabin and first used in 1961.
Gates’ nOPV2 vaccine is a modified version of Sabin’s existing OPV vaccine.
“The spread of vaccine-derived polio virus from OPV vaccine in multiple countries throughout Africa and Asia resulted in 1,612 cases of paralytic polio from 2017 through 2020,” Dr. Liz Mumper, pediatrician and former medical director of the Autism Research Institute told The Defender.
“Since these polio virus samples are in wastewater in a developed country, those who have access to clean water should not be at risk,” Mumper said. “However, the media is raising alarms. This is a setback for the Global Polio Eradication Initiative.”
According to the CDC, three cases of paralytic polio caused by the OPV vaccine have been reported in the U.S. since the vaccine was discontinued in 2000.
The CDC’s Vaccine Adverse Event Reporting System, or VAERS, shows 66 reports of polio following administration of the OPV.
VAERS also shows 14 reported cases of poliomyelitis following vaccination with IPV. Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
“Polio Outbreak” – The WHO, Bill Gates, emergency vaccines & more of the same
By Kit Knightly | OffGuardian | June 24, 2022
Polio is on the front pages of British newspapers again for the first time in decades. What a time to be alive.
For those who missed it, two days ago the UK government declared a “national incident” after traces of the polio virus were detected in sewage from North London.
Yes, a “national incident”… for traces… found in sewage.
This is a massive escalation, even compared to the pandemic. Covid and Monkeypox at least had the good taste to wait for a single person to actually have the disease (allegedly) before hitting the big red panic button.
In a somewhat startling coincidence, just two days before the “polio in London” news broke, Forbes published an article headlined…
There May Be A New Polio Epidemic On Its Way- If So, What We Can Do
It’s totally unrelated, talking about a “polio-like” enterovirus that hasn’t yet had a vaccine approved in the US, and never mentions London once.
The same (or similar) news hitting headlines around the world for (supposedly) totally different reasons makes my inner-cynic twitch.
So, what’s going on here?
While it may look like polio is suddenly back in the news, it’s actually been there longer than you’d think and has been building to this point.
The truth is it all fits into a very predictable pattern.
In November of 2020, a new “genetically engineered” and “triple-locked” polio vaccine was the first vaccine to be granted “emergency use listing” by the World Health Organization, despite there being only around five thousand cases of polio in the world over the last decade.
In October 2021, the government of Ukraine declared a “biological emergency” due to the “re-emergence” of polio, which was blamed on low vaccine uptake.
This was steadily reported in back pages of the news for months. Culminating in headlines like “Polio Makes a Comeback in Ukraine as War Halts Vaccination Campaign”, following Russia beginning its “special operation”.
Later, in March of this year, Israel reported they too had a “re-emergence” of polio after allegedly detecting “vaccine-derived” polio in the stool of a young girl suffering from paralysis.
At this point, the Global Polio Eradication Initiative (GPEI) started speaking out. GPEI is a project co-funded by the WHO, the US CDC, GAVI the vaccine alliance and the Bill and Melinda Gates Foundation.
… in other words, exactly who you’d expect.
Following the reported case in Israel, GPEI released a statement calling for “enhanced surveillance”…
The GPEI partnership urges all health authorities to enhance surveillance for poliovirus and implement enhanced vaccination response to prevent further transmission, so that no child is at risk of lifelong paralysis from a disease that can so easily be prevented. GPEI is committed to assisting the health authorities in their efforts to stop the cVDPV3 outbreak.
A month later, in April of this year, using alleged “re-emergence” as a springboard, GPEI called for “renewed efforts” to combat polio, launching their new “Strategy” and claiming to need a further 4.8 billion dollars in funding.
Then in late May, at the WHO’s 75th World Health Assembly, “global health leaders” called for “urgent action to end polio once and for all before a unique window of opportunity closes for good.”
The same week, the WHO’s Director-General Tedros Adhanom Ghebreyesus addressed the assembly regarding polio [emphasis added]:
“Worrying developments in recent months highlight how fragile this progress [of eradicating polio] is […] This year, we have the real opportunity to halt wild poliovirus transmission. At the same time, we must respond faster and better to cVDPV outbreaks, to interrupt all transmission by end-2023.”
… which brings us to June, and scare-stories on both sides of the Atlantic warning of “low vaccination rates”
Note that the WHO report claims the virus entered the UK on someone who received a “live vaccination” overseas, and the alleged outbreak in Israel is “vaccine-derived”.
Do you see how this works yet?
- The WHO approves “emergency use vaccine”, bypassing need for trials and safety data
- A handful of cases of polio are reported (as they are every year)
- Gates/WHO funded thinktank calls for “increased surveillance”, meaning more testing (using PCR tests)
- More testing inevitably finds more “cases”
- Cases are blamed on the old vaccines
- New “modern” and “safer” vaccines are rolled out.
- Everyone makes a LOT of money.
In October, at the World Health Summit in Germany, GPEI is launching a “pledging moment” to try and raise around 5 billion dollars to “achieve a polio-free world”.
Given the headlines, they should pass that mark pretty easily, wouldn’t you think?
It’s interesting to note that market researchers found the polio vaccine market had “stagnated” through 2020 and 2021, due to the Covid19 “pandemic”.
No more stagnation now.
Fake Meat, Fake Breastmilk and Food Shortages
By Dr. Joseph Mercola | June 2, 2022
Fake food is being poised as a panacea to end world hunger and food shortages, but there’s nothing miraculous about synthetic, lab-made food. It can’t compare to food that comes from nature in terms of nutrition or environmental protection, and as we’re seeing with the mysterious infant formula shortages, when you’re dependent on fake food, your very survival is also dependent on the handful of companies that manufacture them.
With parents getting desperate in the search for infant formula, it’s eye-opening that campaigns haven’t been started to encourage new mothers to breastfeed — the best food for infants and one that also happens to be free and readily available in most cases. If you haven’t read my article on the best workaround for infant formula for those that are unable to breast feed, it is on Substack.
In the video above, you can watch a concerning timeline about why this may be, as Bill Gates appears to be behind the push to stop breastfeeding and encourage uptake of BIOMILQ, a cell-cultured “human milk” made in a lab,1 along with other varieties of fake food.
Bill Gates’ Formula for Disaster
In June 2020, Bill Gates announced startup company BIOMILQ, which is using biotechnology to create lab-made human milk for babies. Using mammary epithelial cells placed in flasks with cell culture media, the cells grow and are placed in a bioreactor that the company says “recreates conditions similar to in the breast.”2
This synthetic lab-made breast milk replacement raised $3.5 million in funding from Gates’ investment firm Breakthrough Energy Ventures.3 Gates has also contributed at least $319 million to the media,4 including The Guardian, allowing him to control and dictate what they print. The day after the Gates Foundation paid The Guardian its annual funding in May 2022, it released a hit piece on breastfeeding titled, “Turns out breastfeeding really does hurt — why does no one tell you?”5
U.S. Customs and Border Protection (CBP) offers also seized 588 cases of infant formula from Europe in April 2021 because it lacked appropriate nutritional labeling. In February 2021, CBP officers said they inspected 17 separate shipments of infant formula from Germany and The Netherlands, leading to a warning against buying infant formula online from overseas.
At the time, Keith Fleming, CBP’s acting director of field operations in Baltimore, Maryland, said in a news release:6
“Consumers should be very careful when contemplating the purchase of items over the internet from an international source, because they may not get what they expect. People expect that the products they purchase comply with existing U.S. health and safety laws and regulations and they’ll be safe for them or their family. That’s not always the case.”
While warning Americans against purchasing infant formula from overseas, in February 2022 the U.S. Food and Drug Administration announced bacterial contamination at the Abbott Nutrition’s Sturgis, Michigan facility,7 which is behind the current infant formula shortages. While Gates is clearly behind the push to stop breastfeeding and encourage BIOMILQ in lieu of breastmilk or formula, the formula shortages highlight the risks of consolidated food production.
Abbott Enriched Shareholders While Formula Sickened Babies
Corporate consolidation is rampant in the U.S. baby formula market, of which 90% is controlled by four companies. Abbot is among them, responsible for 43% of baby formula production in the U.S.8 Yet, according to a whistleblower filing from October 2021, equipment at the company’s Sturgis facility was “failing and in need of repair.”
Pitting and pinholes reportedly existed in a number of pipes, allowing bacterial contamination. Leadership was aware of the failing equipment for up to seven years before the February 2022 outbreak, according to the whistleblower’s report.9
With equipment in need of repair, and a bacteria outbreak in their formula sickening babies, Abbott used its massive profits from 2019 to 2021 to announce a lucrative stock buyback program.10 According to The Guardian :11
“Abbott detected bacteria eight times as its net profits soared by 94% between 2019 and 2021. And just as its tainted formula allegedly began sickening a number of babies, with two deaths reported, the company increased dividends to shareholders by over 25% while announcing a stock buyback program worth $5bn.”
Speaking with The Guardian, Rakeen Mabud, chief economist for the Groundwork Collaborative, added, “Abbott chose to prioritize shareholders by issuing billions of dollars in stock buybacks instead of making productive investments.”12
Big Meat and Dairy Companies Dominate Fake Meat Industry
The increasing number of plant-based fake foods and lab-grown meat companies give the illusion that consumers are getting more choices and the food industry is becoming less consolidated. However, there are still relatively few firms that are controlling the global grab for “protein” markets.
In a research article published in Frontiers in Sustainable Food Systems, Philip Howard, a faculty member in the department of community sustainability at Michigan State University, and colleagues explain how this “protein” industry convergence is further jeopardizing the resilience of the food system and reducing genetic diversity of livestock and crops:13
“Recent years have seen the convergence of industries that focus on higher protein foods, such as meat processing firms expanding into plant-based substitutes and/or cellular meat production, and fisheries firms expanding into aquaculture. A driving force behind these changes is dominant firms seeking to increase their power relative to close competitors, including by extending beyond boundaries that pose constraints to growth.
The broad banner of “protein” offers a promising space to achieve this goal, despite its nutritionally reductionist focus on a single macronutrient. Protein firm strategies to increase their dominance are likely to further diminish equity in food systems by exacerbating power asymmetries.”
Tyson and Cargill, two of the largest meat processors in the world, for instance, have invested in fake meat company Memphis Meats, which also has backing from Bill Gates and Richard Branson. Other billionaires invested in fake foods include Sergey Brin (Mosa Meat), Peter Thiel (Modern Meadow) and Marc Benioff (Eat Just).
“These companies wouldn’t be making these investments if they didn’t expect that the intellectual properties held by these start-ups will lead to monopoly profits,” Howard notes.14 In “The Politics of Protein,” a report from the International Panel of Experts on Sustainable Food Systems (IPES-Food), Howard explains:15
“Nearly every large meat and dairy processor/manufacturer has also acquired or developed plant-based meat and dairy substitutes, establishing footholds in a market that is growing approximately 20% per year.
More than a dozen of these firms have also invested in start-ups that are attempting to commercialize lab-grown meat and fish. Meanwhile, Vanguard and BlackRock — two of the world’s biggest asset management firms — have investments in almost all the largest meat, dairy, and animal feed companies.”
It is important to understand why all of these fake meat products are an absolute metabolic disaster relates to the fact that they are using vegetable fats to replace animal fats. Not only are they devoid of important vitamins like vitamin A and vitamin K2, but they are loaded with the dangerous omega-6 fat linoleic acid LA.
In some cases they contain up to 10 to 20 times the amount found in meats, which will radically contribute to diseases like diabetes, obesity, cancer and heart disease.
Lab-Grown Food Is an Environmental Catastrophe
The push for fake food is being made on the platform that it will somehow save the environment from the ravages of factory farming, which has devastated the environment with its concentrated animal feeding operations and monocultures. But this, too, is misleading.
In February 2021, the Good Food Institute (GFI), a nonprofit group behind the alternative protein industry, released a techno-economic analysis of cultivated meat, which was prepared by consulting firm CE Delft.16 In it, they developed a model to reduce the current costs of cultured meat production down to a point that would make it economically feasible in full-scale plants by 2030, a model they said is “feasible.”
In attempting to create cultured meat on the scale that would be necessary to feed the world, logistical problems are numerous and, possibly, insurmountable. There are waste products — catabolites — to deal with, as even cultured cells excrete waste that is toxic.
And, the oxygen and nutrients available must be adequately distributed to all the cells — something that’s difficult in a large reactor. Stirring the cells faster or adding more oxygen may help, but this can cause fatal stress to the cells.17
The environmental “benefits” are also on shaky ground when you factor in soy production as well as the use of conventional energy sources. When this is factored in, GFI’s life-cycle analysis found that cultured meat may be worse for the environment than conventionally produced chicken and pork.18,19
Farmer and historian John Lewis-Stempel also points out that the world’s farmers already produce enough food for the global population: “[A]ny discussion of global food policy needs to begin with one plain fact: there is … no actual food shortage. Already, the planet’s farmers produce enough food to cater for the projected 10 billion humans of 2050. The problem is waste and distribution.”20
Yet, the push for the creation of fake protein sources continues. In the foreword to Navdanya International’s report “False Solutions That Endanger Our Health and Damage the Planet,” Vandana Shiva also details how lab-grown foods are catastrophic for human health and the environment, as they are repeating the mistakes already made with industrial agriculture:21
“In response to the crises in our food system, we are witnessing the rise of technological solutions that aim to replace animal products and other food staples with lab-grown alternatives. Artificial food advocates are reiterating the old and failed rhetoric that industrial agriculture is essential to feed the world.
Real, nutrient-rich food is gradually disappearing, while the dominant industrial agricultural model is causing an increase in chronic diseases and exacerbating climate change. The notion that high-tech, “farm free” lab food is a viable solution to the food crisis is simply a continuation of the same mechanistic mindset which has brought us to where we are today — the idea that we are separate from and outside of nature.
Industrial food systems have reduced food to a commodity, to “stuff” that can then be constituted in the lab. In the process, both the planet’s health and our health have been nearly destroyed.”
Signs the Fake Meat Industry Is Stalling
For all of its fanfare, there are signs that the fake meat industry may be failing before it ever gets off the ground. Shares of Beyond Meat, for one example, lost $6 billion since March 2020 due to weak sales growth and has resorted to partnering with PepsiCo to release a plant-based jerky product.
“My analysis is the launch will do very little to increase the company’s fortunes,” writes business development consultant Victor Martino in Just Food.22 He argues that the “plant-based meat revolution” is just a PR stunt, a narrative that’s set to implode:23
“The fact is, despite increased product availability in terms of brand choices and added retail outlets, plant-based meat sales stalled in 2021, recording zero growth, according to recent research from SPINS, data commissioned and released by The Plant-Based Foods Association and The Good Food Institute.
According to the research, the total annual sales of plant-based meat in the US remained stable at $1.4 billion. That’s a continuation of the 1.4% share of total meat category sales.”
Shares of Beyond Meat and Oatly, a plant-based milk substitute, have lost more than half their value in 2022,24 but this isn’t to say that their executives are suffering. Beyond Meat’s former chief growth officer Chuck Muth sold shares valued at more than $62 million from 2019 to 2021, while Biz Stone, a current board member and Twitter co-founder, has made millions on Beyond Meat stock.25
The fact remains that when private companies control the food supply, they will also ultimately control countries and entire populations. Biotech will eventually push farmers and ranchers out of the equation and will threaten food security and human health. In other words, the work being done in the name of sustainability and saving the planet will give greater control to private corporations while weakening the population.
To save the planet and support your health, skip all the fake meat alternatives and opt for real food that’s being raised the right way instead. When you shop for food, know your farmer and look for regenerative, biodynamic and/or grass fed farming methods, which are bringing you truly sustainable food for a healthy population and planet.
Sources and References
- 1, 3 Rumble May 17, 2022
- 2 BIOMILQ, Our Science
- 4 MintPress News November 15, 2021
- 5 The Guardian May 9, 2022
- 6 U.S. Customs and Border Protection April 5, 2021
- 7 U.S. FDA May 17, 2022
- 8, 9, 10 Children’s Health Defense May 23, 2022
- 11, 12 The Guardian May 20, 2022
- 13 Front. Sustain. Food Syst., 16 August 2021
- 14 Civil Eats September 22, 2021
- 15 IPES-Food, The Politics of Protein, Executive Summary, Page 3
- 16 Techno-Economic Analysis for the production of cultivated meat February 2021
- 17, 19 The Counter September 22, 2021
- 18 LCA of cultivated meat – February 2021, Page 3
- 20 Unherd May 17, 2022
- 21 Children’s Health Defense April 5, 2022
- 22, 23 Just Food March 30, 2022
- 24 CNBC May 14, 2022
- 25 Michele Simon March 1, 2022
Bill Gates’ media control dream

By Keean Bexte | The Counter Signal | May 19, 2022
The Bill and Melinda Gates Foundation has doled out over $319 million in grants, awards, and charity to media organizations, including $38 million to so-called “investigative journalism” centres.
According to Mint Press News (MPN), which sorted through over 30,000 documents, Bill Gates has given roughly $38 million to investigate journalism centres aimed at training journalists. Of this sum, over $20 million has gone to the International Center for Journalists, which “builds the expertise and digital skills journalists need to deliver trustworthy news essential for vibrant societies.”
The generous donations given to the ICFJ over several years have been given with the express purpose of producing journalists who focus on “data-driven health and development news reports to help African media to better contribute to setting development agendas and furthering public accountability,” according to the Bill and Melinda Gates Foundation’s website.
Producing health-obsessed investigative journalists is a common trend with Gates.
According to the Foundation’s website, the Premium Times Centre for Investigative Journalism received its grant ($3,800,357) to “support sustained high-quality, evidence-based, and solutions-oriented media coverage of global health and development issues in Primary Health Care systems, Agriculture & Financial Inclusion.”
Other recipients of over $1 million include The Pulitzer Center for Crisis Reporting ($2,432,552) to “support editorial projects focused on global health issues,” Fondation EurActiv Politech ($2,368,300), International Women’s Media Foundation ($1,500,000), Center for Investigative Reporting – $1,446,639, InterMedia Survey institute ($1,297,545), and The Bureau of Investigative Journalism ($1,068,169).
Put simply, it appears Bill Gates wants to install a personal army of professional scrutineers in various media outlets that disseminate his position on healthcare and propaganda about public officials who deviate.
Gates also, of course, funds the journalism programs of several universities, including Johns Hopkins University, Columbia University, the University of California Berkeley, Tsinghua University, Seattle University, Rhodes University, and Montclair State University.
Harvard University (of which Gates is a dropout), the University of Southern California, Boston University, and Ahmadu Bello University have also received money from Gates’ Foundation to take on various media projects.
Producing new journalists isn’t the only area in media that Gates is focusing on, though. He also targets experienced journalists in legacy media organizations. According to MPN’s report, a total of $166.2 million has been given to well-known legacy media organizations.
“The money is generally directed towards issues close to the Gateses hearts. For example, the $3.6 million CNN grant went towards “report[ing] on gender equality with a particular focus on least developed countries, producing journalism on the everyday inequalities endured by women and girls across the world,” while the Texas Tribune received millions “to increase public awareness and engagement of education reform issues in Texas.” Given that Bill is one of the charter schools’ most fervent supporters, a cynic might interpret this as planting pro-corporate charter school propaganda into the media, disguised as objective news reporting,” reports MPN.
Just over one decade ago, Bill Gates was under fire for his attempt to control the media through spread-out donations, but this fire seems to have flickered out until recently.
“Beyond their subject matter, these [health report stories] have something else in common: They were all bankrolled by the Bill & Melinda Gates Foundation,” the Seattle Times wrote in 2011.
“Better-known for its battles against global disease, the giant philanthropy has also become a force in journalism.”
“The foundation’s grants to media organizations such as ABC and The Guardian, one of Britain’s leading newspapers, raise obvious conflict-of-interest questions: How can reporting be unbiased when a major player holds the purse strings?”
Unsurprisingly, the Seattle Times and the Blethen Corporation do not appear to have ever received money from Bill Gates.
Featured Video

US Marines Seized Panama in 1903
or go to
Aletho News Archives – Video-Images
From the Archives
Precedents for Pizzagate
Marc Dutroux, Belgian pedophile, sadist, and serial killer with friends in high places
By Aedon Cassiel | Counter – Currents | December 23, 2016
To reiterate a point that should be clear to the more astute reader, my goal in this series (part 1, part 2) has not been to defend “Pizzagate” as such. My goal has been to defend the people who want to investigate it against specific accusations levied against them by people who think Pizzagate has revealed no intriguing information at all—for a specific reason, which I will be honing in and focusing on much more directly in this closing entry.
Whereas the mainstream critics of Pizzagate would have you believe that the dividing line is between paranoid conspiracy theorist followers of “fake news” and level-headed people who follow trustworthy news sources and rely on cold, hard reason to determine the truth, my goal has been to show that—whatever is or is not happening with Pizzagate itself—this framing of the issue is arrogant, insulting, and the product of extremely narrow tunnel vision. … continue
Blog Roll
 Aletho News
Aletho News- Israeli firms transform cars into intelligence devices: Reports
- Zionist-controlled companies to surveil British citizens
- THE CHILDREN GAMBIT
- A note on comment posting at Alethonews
- Trump stalls over Iran strike plan, Iran holds all the aces
- Zelensky’s Ceasefire for Elections is Strategic Gambit, Not Democratic Move
- US and Dutch pilots flying F-16s for Ukraine – Western media
- West’s Claims of Non-Involvement in Ukraine Conflict ‘Epitome of Hypocrisy’ – Expert
- Putin aide urges retaliation to ‘Western piracy’
- The Depth Charge in the Womb
- If Americans Knew
- Israel’s Favorite American President
- Israel’s “Yellow Line” Is a Death Trap for Palestinians. We Drove Into It.
- Why Israel’s expanding occupation in Syria presents a critical legal test
- Gaza is not a natural disaster. It is the victim of genocide enabled by global inaction
- Netanyahu’s plan to “end” US aid to Israel is to give even more money under a different name
- Israel ceased firing on Gaza for just 15 days of the “ceasefire” – Not a ceasefire Day 130
- In Gaza, “rats run over our faces” – Not a ceasefire Day 129
- Israel-backed border guards, GHF-linked aid – Not a ceasefire Day 128
- Israel battles Palestinian right of return, one Palestinian at a time – Not a ceasefire Day 127
- Noor’s short life of unimaginable suffering
- No Tricks Zone
- New Study: A 4°C Warmer Beaufort Sea Had ‘No Sea Ice’ 11,700 – 8200 Years Ago
- Unfudging The Data: Dutch Meteorological Institute Reinstates Early 20th Centruy Heat Waves It Had Erased Earlier
- German Gas Crisis…Chancellor Merz Allegedly Bans Gas Debate Ahead of Elections!
- Pollen Reconstructions Show The Last Glacial’s Warming Events Were Global, 10x Greater Than Modern
- Germany’s Natural Gas Storage Level Dwindles To Just 28%… Increasingly Critical
- New Study Rebuts The Assumption That Anthropogenic CO2 Molecules Have ‘Special’ Properties
- Climate Scientist Who Predicted End Of “Heavy Frost And Snow” Now Refuses Media Inquiries
- Polar Bear Numbers Rising And Health Improving In Areas With The Most Rapid Sea Ice Decline
- One Reason Only For Germany’s Heating Gas Crisis: Its Hardcore-Dumbass Energy Policy
- 130 Years Later: The CO2 Greenhouse Effect Is Still Only An Imaginary-World Thought Experiment
