Before the coronavirus pandemic, ivermectin was described as a “wonder” drug by the medical community. And in 2015, Dr. Satoshi Ōmura and Dr. William C. Campbell were awarded half the Nobel prize in Physiology or Medicine for their work that led to the development of ivermectin.
“The importance of Ivermectin for improving the health and wellbeing of millions of individuals with River Blindness and Lymphatic Filariasis, primarily in the poorest regions of the world, is immeasurable,” the Nobel Assembly stated in its press release for the 2015 Nobel Prize in Physiology or Medicine.
But after the pandemic began, the tech giants have gone all out to purge content that recommends ivermectin as a treatment for COVID-19.
And today, these Big Tech policies against ivermectin resulted in one of Ōmura’s speeches where he discussed ivermectin being struck down for “violating YouTube’s community guidelines.”
“When the fascists at YouTube censor the Noble Prize winner Dr. Satoshi Omura, a man whose discoveries have saved a hundred million + from blindness, the world has entered a very, very dark place,” Australian Member of Parliament Craig Kelly tweeted. “I cannot express in words how angry & sad this makes me & fearful for the future.”
Frontline Covid-19 Critical Care, an alliance of physicians and scholars that has committed to “research and develop lifesaving protocols for the prevention and treatment of COVID-19 in all stages of illness,” also spoke out against the censorship and warned that “brilliant scientists and lifesaving science are systematically being gagged.”
Four expert reviewers were satisfied by revisions already made. ‘The effort of the authors is praiseworthy in this pandemic situation,’ one said. Their critiques had been technical: some of the statistical methods break down when there are no ‘events’ (in this case, deaths) in both ‘arms’ of a clinical trial. Our lead statistician ran more checks; we fixed the criticisms. This is what ‘peer review’ is supposed to do. It’s normal.
One might take such a comment from the senior editor as the preamble to acceptance for publication. But no, this was the editors’ reason for not publishing the paper. This isn’t normal. What was the problem?
‘We don’t doubt this is an important paper, and would likely be widely taken up.’ Hang on, Lancet Respiratory Medicine wants to avoid printing something it recognises as an important paper, that four of their own experts have passed, because it might be ‘widely taken up’? This is what they usually want.
Of course, the Lancet has a lot to live down, having moved into the business of publishing fake news, as with the notorious hydroxychloroquine fraud which I reported on for TCW last year. Not only did the Lancet publish an obvious fake, it did so with hostile editorial commentary and briefing to BBC Radio 4 Today for maximum impact. So media briefing for planted fake news, but a Lancet specialist title won’t touch an ‘important paper’.
I was told in January, by a senior clinical researcher who knows him personally, that Richard Horton, editor in chief of the Lancet, was ‘very ashamed’ at having let through the fake news. Horton, whose Twitter bio reads ‘welcome to a permanent attack on the present’, wrote in 2015:
‘Much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness . . . Journal editors deserve their fair share of criticism too. We aid and abet the worst behaviours . . . Our love of “significance” pollutes the literature with many a statistical fairy-tale. We reject important confirmations . . . And individual scientists, including their most senior leaders, do little to alter a research culture that occasionally veers close to misconduct.’
Horton was right. The only aspect that the fake news had going for it was the huge sample size: 96,000 patients. Except that the true number was actually zero, since the paper was fake. The Lancet was certainly seduced by a ‘fashionable trend of dubious importance’, namely ‘Big Data’, a flavour-of-the-month set fair to corrupt many other sciences as well as medicine. The Lancet ‘aided and abetted the worst behaviours’, not just those ‘veering close to misconduct’, but those clearly crossing the line.
Has anything changed? In 2015 Horton bemoaned journals that ‘reject important confirmations’, but in March 2021, ‘after lengthy discussions with the editorial team’, Lancet Respiratory Medicine did it again, rejecting our ‘important confirmation’ (passed by four of their own experts, remember) that yes, ivermectin works for Covid-19.
So there we have it. Horton’s 2015 editorial remains true, but he doesn’t seem to have done anything about it. He’s only the man in charge, after all.
I had feared as much, but we were all keen to give our findings maximum visibility. But Lancet Respiratory Medicine did what its friends wanted, which was ‘kill the story’ for as long as possible, which in the event has been over three months, whilst we searched for a journal with enough integrity to publish an article which had already passed four-fold peer-review at the Lancet, and would get yet further examination elsewhere. As of last Friday the paper is now published in the American Journal of Therapeutics, and you can read it here. More importantly your doctor, or your family’s doctors, can read it too. Take it to them, as many as possible.
So what does this dry-as-dust research paper actually show?
The starting point was another review article on ivermectin for Covid-19, also in the American Journal of Therapeutics, published on May 1. Take that paper to your doctor too. Dr Pierre Kory and his Front-Line Covid Critical Care alliance (FLCCC) of US-based intensive care doctors had their four-times peer-reviewed paper accepted for a special issue on repurposed drugs for Covid-19, but then revoked, by the journal Frontiers in Pharmacology. This unprecedented volte face was charted recently in TCWby Dr Michael Yeadon. The same ‘kill the story’ orders delayed publication by over five months.
The FLCCC know what they are doing with Covid-19. Their ‘MATH+’ treatment delivers the world’s best survivals from serious, late-stage, hospitalised Covid-19. It remains almost unknown in the UK and unused in the NHS. (All Brits should be very angry about this). FLCCC luminary Dr Joseph Varon, mentioned en passant in my coverage of the Oxford RECOVERY trial, has the best track record of them all. The FLCCC have used several anti-virals in their continuing evolution of the best treatments, but by late autumn realised that one drug, ivermectin, stood out because it worked at all stages of the Covid-19 disease, from prophylaxis through to the intensive care that the FLCCC specialise in. They wrote up the evidence, posting a preprint in mid-November.
They explain the back-story to ivermectin, little-known in Western countries but worldwide one of the most widely-used drugs at 3.8 billion doses and counting. Earning the 2015 Nobel Prize in Physiology or Medicine for its discoverers, it has crushed the hideously disabling infestation of onchocerciasis or ‘river-blindness’ across the tropics. A potent anti-parasitic, it is used for threadworms, scabies and head-lice. It costs pence per pill. It is a known anti-viral, working across a range of RNA viruses, (and some DNA ones). It may even be an anti-cancer drug, and has prolonged lives in leukaemia. Specifically against the SARS-CoV-2 virus, a team at Monash University in Australia showed that ivermectin killed off the virus in vitro in April 2020. The usual suspects declared that this meant nothing (which on its own is true), that that you couldn’t get it strong enough in vivo; nevertheless the Monash paper set off a series of clinical trials of ivermectin for Covid-19, usually in Low and Middle Income Countries (LMICs), or in plain English poor countries. There is a good reason for this: if you are dirt poor, you need your medicines to be dirt cheap. Nothing else will be any use. What did they find? Ivermectin works for Covid-19, at entirely tolerable doses.
Kory’s paper showed how cases and deaths in Peru came crashing down where ivermectin was freely distributed, and not where it wasn’t. The same phenomenon has been repeated in India more recently; states such as Goa that adopt mass distribution of ivermectin crush their cases; those that refuse it such as Tamil Nadu (Chief Minister M K Stalin) don’t.
Dr Kory’s paper identifies and charts the evidence, but doesn’t do a formal meta-analysis, which is where Dr Tess Lawrie came in. Her Evidence-Based Medicine Consultancy does nothing but rigorous systematic reviews, and only for public clients such as the NHS and the WHO. Their objectives are clinical practice guidelines, providing the evidence for decisions on licensing and implementation.
A ‘meta-analysis’ is a synthesis of data from multiple sources – typically clinical trials of a new drug – using recognised statistical methods. A meta-analysis of clinical trials that are themselves ‘randomised’ clinical trials (where patients are allocated at random to receive, or not, the treatment) lies at the summit of the ‘evidence quality’ pyramid, in the doctrines of Evidence-Based Medicine, ruthlessly insisted upon by regulatory authorities. To rehearse a cliché, the Randomised Controlled Trial or RCT is the ‘gold standard’ of medical evidence. If so, a meta-analysis of RCTs is platinum.
What makes the paper a first is being carried out according to the standards of the Cochrane organisation, requiring a protocol to be observed (i.e. no favouritism), data extraction from primary sources by two researchers independently, and the ‘grading’ of those sources for the quality of the evidence. Indeed the paper began life as a Cochrane Review, and was finished by the end of January. But to cut short a long story (parts of which are covered elsewhere by the ever-vigilantFrance Soir ) the Cochrane organisation did not want a systematic review on a topic already approved by a specialised researcher and colleagues whose consultancy does nothing else, and who have contributed nearly 80 such reviews between them. Sounds familiar? It should do by now: the ‘capture’ of learned journals by powerful interests who will suppress, by fair means or increasingly by foul ones, any knowledge that threatens those interests.
The reason for doing a systematic review is that that is what is required by regulatory authorities such as the FDA (in the US) the European Medicines Agency (for the EU), our own Medical and Healthcare products Regulatory Agency (MHRA) and the World Health Organisation (WHO). It’s what they require to decide on licensing new drugs (though ivermectin isn’t new at all).
Dr Lawrie didn’t stop at the meta-analysis, but pressed on to a ‘Evidence to Decision’ process, the formal procedure which those regulators are supposed to use in coming to decisions. On February 20, the British Ivermectin Recommendation Development (BIRD) panel voted that ‘ivermectin should be adopted to reduce morbidity and mortality associated with Covid-19 infection and to prevent Covid-19 infection among those at higher risk.’
That was February. The essentials were already clear from Dr Kory’s paper in preprint in November, his testimony to the US Senate in December, Dr Lawrie’s first meta-analysis issued on January 3, and our submission to the Lancet on 5 February (preprint posted March 11). BMC Systematic Reviews were kind enough to post a preprint on March 18 but though they still say it’s ‘under review’ we haven’t heard from them in three months, so it looks like ‘kill the story’ orders apply there too. Our published paper has since been revised and updated.
The paper makes clear that there’s no real doubt that ivermectin is an effective medicine for Covid-19. Multiple clinical trials show it. The Randomised Controlled Trials that our paper analyses are just the tip of the iceberg. Plenty of other trials show it too, but if they were not randomised, according to regulators they don’t count, so our meta-analysis did not include them. Although Risks of Bias are carefully evaluated, disregarding the mountain of evidence from elsewhere, not least the experience and testimony of doctors actually using it, is itself a potent source of bias. You are throwing away all the data that might force you to think. A critic of our paper wrote: ‘a technical tour-de-force based on ritualised ideas’. He’s right, but let’s not argue: our meta-analysis was upon the Regulators’ terms. We played by their rules. That was the point. You want a strict meta-analysis of RCTs only? Take two dozen.
How many do they need? When governments, or regulatory agencies, want to approve medicines, one will do. Dexamethasone, to huge fanfare, was approved last summer on the evidence of just one RCT, though it helps only ventilated patients in the inflammatory stages of the illness, and on its own, by not very much. The FLCCC doctors had been using a different corticosteroid, methylprednisolone, and at higher equivalent doses, long before. In our analysis, ivermectin reduces deaths overall by around 62 per cent, and works at all disease stages. As a prophylactic, it prevents 6 out of every 7 infections that would otherwise occur, and stops household transmission in its tracks. Corticosteroids are vital in the inflammatory phase of the illness, but are useless in the purely viral stage or for prophylaxis.
So where does all this leave ivermectin, for those affected by Covid-19, those worried about it, and vulnerable people at risk?
Ivermectin isn’t new. Its safety record, from those billions of doses, is second to none. Its cost is negligible. The WHO, in its BC (Before Covid) era, listed it as an ‘Essential Medicine’ in their catalogue of the ‘minimum medicine needs for a basic health-care system’ (though our ‘envy of the world’ NHS doesn’t have it).
In the USA, ivermectin is licensed by the FDA, albeit not for Covid, so is available to any American doctor to prescribe ‘off-label’ (i.e. not according to the originally licensed ‘advertising label’). However the fact that it isn’t ‘labelled’ for Covid makes it easy to refuse. Patients’ families have had to go to court for injunctions ordering hospitals to give ivermectin. The FLCCC still swims against the tide, though legal barriers are lower than elsewhere, for open-minded doctors.
In the UK, ivermectin has never been licensed by the MHRA. This makes it easy for doctors to refuse, and for those who want to help to be obstructed. My GP refused me ivermectin for prophylaxis, even after I showed him the evidence. Hospital doctors can’t get it except to special order at pharmacies. The bureaucracy won’t allow them to prescribe it. Listen to Dr Nyjon Eccles having to bring his own ivermectin for his 84-year-old mother in hospital with Covid-19, dependent on oxygen, and failing every time she came off. She was discharged five days after her first dose.
As for the WHO itself, on March 31, 2021, its ‘Living Guideline’ for Covid treatments was updated, declaring: ‘We recommend not to use ivermectin in patients with Covid-19 except in the context of a clinical trial.’ The cherry-picking of studies that helped give the Right Answer, and rejection of those that didn’t, the cavalier appraisal of risks of bias and evidence certainty, make their analysis a complete travesty, but nevertheless potently influential.
In India, seeing the damage that the WHO had done to their Covid-19 policy, and finding the pile of evidence compiled by the FLCCC and BIRD, the Indian Bar Association served two legal notices upon the chief scientist of the WHO, Dr Soumya Swaminathan (an Indian national). The first (May 25) accuses her of a ‘disinformation campaign against ivermectin’ and the second June 13) ups the ante by joining Dr Tedros (director general of the WHO), and accusing them of ‘contempt of court and aggravated offences against humanity by spreading disinformation’. If these move to actual litigation, watch this space.
Meanwhile, patients and their families, and even Bar Associations, should not have to go through the courts or to smuggle medicines into hospital to get treatment for sick patients. At some point, officials who obstruct access to safe medicines are going to have to explain the moral difference between their actions and corporate manslaughter.
This article has been about an anti-viral treatment that is already known, already exists, with an unparalleled safety record, is on the Essential Medicines list of the WHO, costs virtually nothing, and has anti-inflammatory properties to boot. It requires only formal endorsement. Johnson’s Task Force is redundant.
Preparing a formal application to the MHRA, we take comfort from the editors of Lancet Respiratory Medicine: ‘We don’t doubt this is an important paper’.
All dangerous diseases are best treated early. A major failure of the global COVID-19 strategy has been to wait a week for the disease to become dangerous, when breathing becomes a problem. Early treatment of COVID, even for those with mild symptoms, prevents later hospitalization. There are several early treatment drugs showing promise but ivermectin leads the pack regarding safety, effectiveness and price. Unfortunately, the biggest players in Western mainstream media are members of the Trusted News Initiative (TNI). The TNI is a story for another day but it’s remarkable that big media companies barely report that they have agreed to promote global vaccination and to make sure any “disinformation myths are stopped in their tracks”[i]. Unfortunately, as a result early treatment seems to be seen as a disinformation myth and is not mentioned. Early treatment is vital in treating serious diseases and COVID-19 is no exception.
Considering the human and economic cost, the avoidance of early treatment with a very safe, effective and off-patent drug is a criminal tragedy of immense proportions and a winning lottery ticket for some pharmaceutical companies that are designing and selling novel patented drugs that could not compete with ivermectin in a free market. Mercks’ molnupiravir, for instance, is seeking an Emergency Use Authorization (EUA) from the FDA and “Merck will receive approximately $1.2 billion to supply approximately 1.7 million courses of molnupiravir to the United States government.”[ii]
Ivermectin doesn’t need an EUA because it passed trials in 1986. It just needs to be recommended to treat COVID-19. However, if ivermectin was officially recognized as an effective treatment, it would legally prevent molnupiravir’s EUA until it passes trials and thus delay or endanger the $1.2 billion deal. An aggravating factor is the fact that molnupiravir (EIDD-2801) could cause harmful genetic mutations. [iii]
In the face of a public health crisis such as the COVID-19 pandemic, government authorities and international organizations have traditionally looked to the World Health Organization (WHO) for guidance – trusting that the WHO is free of commercial interests. Originally funded entirely by member states, the organization now receives less than 20% of its budget from these states and the rest from donors[iv] with their own financial and strategic agendas. Margret Chan, the previous Director General of the WHO, said in 2015: “I have to take my hat and go around the world to beg for money and when they give us the money [it is] highly linked to their preferences, what they like. It may not be the priority of the WHO, so if we do not solve this, we are not going to be as great as we were”. [v]
Veteran journalist Robert Parsons explains that “the Smallpox eradication program was funded entirely by donors. That may have led to the problem that for special projects it [the WHO] has to raise the funding. But the private sector is unlikely to get involved unless it shows profit … Consequently, there is little independent public health research”.[vi] Since then, the undue financial influence of private stakeholders has further grown at the WHO. Donations come with caveats so that the organization is compromised on a number of issues that involve the interests of its donors.
In 2010, for instance, after the H1N1 flu pandemic, an investigative inquiry by the British Medical Journal (BMJ) and the Bureau of Investigative Journalism found that “key scientists advising the World Health Organization on planning for an influenza pandemic had done paid work for pharmaceutical firms that stood to gain from the guidance they were preparing. These conflicts of interest have never been publicly disclosed by WHO, and WHO has dismissed inquiries into its handling of the A/H1N1 pandemic as ‘conspiracy theories’.” [vii] These advisors managed to convince the UK government to spend more than $7 billion on a vaccine that was never needed.[viii]
As of 2021, conflicts of interest such as these continue to be a problem – the undue influence of private stakeholders being a prime example. The Bill and Melinda Gates Foundation (BMGF) is the second largest funder of the WHO after the USA. Gates, however, also founded and funds The Vaccine Alliance (GAVI). In the period 2018–19, their combined voluntary contribution to the WHO was 27%[ix] greater than the US voluntary contribution, making Gates’ influence pervasive. As funds by the Gates conglomerate are earmarked for specific projects, the WHO doesn’t decide how the respective money is spent, Gates does.
In addition to the undue financial influence exerted by the BMGF, there is also an overlap of personnel between the WHO and Gates’ endeavors. Tedros Adhanom, the current WHO Director General, has previously served on the board of GAVI and as the chair of the Gates funded Global Fund.[x] Arguably, he is still influenced by his previous employer’s ideology and financial power.
Gates’ priorities have become the WHO’s. The main priority of Gates is global COVID-19 vaccination, not public health systems providing early treatment. He has been pushing vaccination onto the global agenda since 2012. The power of Gates Foundation funding has dictated a drive towards vaccinations and away from other essential public health measures, a move which has been criticized for years by international NGOs involved in the health and development field.
Generally, Gates also believes that capitalism is more efficient than public health agencies when it comes to reaching his goals in the area of global health.[xi] Capitalism is usually more efficient than government but it values profits above people. Accordingly, Gates as well as the pharmaceutical companies his foundation is invested in and whose products he is pushing globally are making billions from their endeavors. Morgan Stanley believes that Pfizer, for example, could earn $100 billion from vaccines developed with public tax money from the US, Germany and other places in the next five years.[xii] Pfizer is partnered with BioNTech. The Gates Foundation has investments in both companies, putting $55 million into BioNTech alone in September 2019. The Gates Foundation also owns shares in Merck which is positioning the drug molnupiravir on the market hoping to make billions from it.
When it comes to ivermectin – in its off-patent form, Gates is funding work on a patentable, injectable form.[xiii] Organizations tied to Gates have taken an antagonistic stance thus far. Notably, GAVI has been going all out by running paid google ads against the use of ivermectin in COVID-19.[xiv]
Given the significant financial and ideological conflict of interest of its main donor, the WHO recommendation on early treatment with an off-patent, highly efficient, safe and cheap drug such as ivermectin needs to be critically examined. In the WHO ivermectin guideline, despite showing a reduction of deaths by 80%,[xv] the organization puzzlingly recommends against ivermectin’s use.
The WHO’s guideline document is “based on a living systematic review and network meta-analysis from investigators at McMaster University”.[xvi] McMaster University (including any of its direct affiliates) should have excused itself from conducting the guideline, given it has several objective conflicts of interest when it comes to ivermectin. For one, McMaster itself is designing and producing second generation COVID-19 vaccines.[xvii] It intends to produce hundreds of thousands of doses. It is likely that these experimental products would receive greater scrutiny if there is a viable safe prophylactic and treatment option for COVID-19. Secondly, McMaster University, like the WHO itself, receives millions in funding from the Gates Foundation. Additionally, McMaster, again like the WHO, shares personnel with the Gates Foundation.
Edward Mills, for example, is both a McMaster associate professor and the clinical trial advisor for the Gates Foundation. In addition he has recently been appointed as the principal investigator of the Gates-funded Together Trial that is currently evaluating repurposed drugs such as ivermectin for their use in COVID-19[xviii]. Asked for comment, Mills denied that the Gates Foundation was having any “say on the conduct of the trial” even though he himself is it’s principal investigator and employed by the Gates Foundation. As past experiences show, no product should ever be tested in a trial funded by those gaining or losing financially or ideologically from it. Thus, ivermectin trials are best not done by anyone with a financial and ideological investment in competing drugs and vaccines. No reputable organization or government agency should be basing their opinion of ivermectin on trials conducted by the Gates Foundation or any other party with a conflict of interest.
The recently announced Oxford University trial of Ivermectin shares a similar conflict as Oxford is profiting from the sales of the AstraZeneca vaccine and questions have been raised about the proposed trial possibly sabotaging the result by admitting elderly people already sick for 14 days but limiting the Ivermectin dose to three treatments.
Unsurprisingly, in a recent interview, Edward Mills seemed to be downplaying the effect of ivermectin. “The evidence on prophylaxis use of ivermectin is not very convincing”, Mills doubts, even though ivermectin is not being evaluated as a prophylactic in his own trial. Data from different clinical trials clearly shows that ivermectin is exceptionally effective, specifically as a prophylactic. Bryant et al. (2021) who analyzed the existing data from clinical trials according to conservative Cochrane meta-analysis standards – a gold-standard in science – found that “ivermectin prophylaxis reduced covid-19 infection by an average 86%” with the best-dosed study reaching an effectiveness of 91%.[xviv] There have been several studies that show that the regularity of the prophylactic dose is important with a weekly dose being more effective than bimonthly. Edward Mills curiously doesn’t find the prophylactic data interesting. The big money is not in running generic repurposed drug trials but in pharmaceutical company trials fighting for market share.
Mills also suggests ivermectin might be efficient as a treatment but emphasizes the need for other drug interventions. “I am very optimistic that it will – it will just be one component of the interventions that we need.“[xix] While other components can be useful additions, downplaying the effect of ivermectin is not warranted. An expert meta-analysis by Karale et al. (2021) including researchers from the renowned Mayo Clinic comes to the conclusion that when given early in mild or moderate COVID-19, ivermectin reduces mortality by 90%.[xx] The findings further corroborate the results of the scientific review conducted by Kory et al. (2021) that has been published in the American Journal of Therapeutics and shows ivermectin to be significantly effective in the treatment of COVID-19.[xxi]
Given the conflicts of interest of McMaster University as well as the dubious interrelations between McMaster personnel and private stakeholders such as the Gates Foundation and other industry-related companies, the WHO should not have accepted McMaster’s involvement in the guidelines on ivermectin. Further, the WHO should ensure that no undue influence is exerted by its own donors – a task it has not yet been able to achieve.
Questions sent to the WHO Ethics Office, asking for clarity about its recommendation against the use of ivermectin, were answered. However the organization refused to supply minutes of the meeting on ivermectin. It further declares that no interview will be granted. It does “not consider an assessment of ivermectin for prophylactic use in COVID-19 to be warranted”. It also does not consider trials by drug companies to be “biased per se” even though major pharmaceutical corporations have been repeatedly convicted of substantial fraud, manipulation and concealment of evidence and paying billions of dollars in fines. There was also an intimidatory confidentially clause in the WHO correspondence despite the author stating that they are writing about ivermectin.
The WHO needs to prove that it followed a scientific and ethical process in its recommendation against the use of ivermectin. Public trust is crucial to beat the pandemic. We cannot continue to have the Gates foundation determining the WHO decisions on Ivermectin given the large conflict of interest. The minutes of the meeting in which the recommendation against ivermectin was taken need to be made public. The public needs to be told and shown invoices with regards to who paid for the steps that informed the WHO ivermectin guideline. The conflicts of interest of major WHO donors and the employer (McMaster University) of the scientists that are responsible for the guideline need to be made transparent. Without this, the recommendation against the use of ivermectin, remains mired in suspicion of corporate overreach.
Few incidences make the general problem more apparent than the following: The WHO’s Chief Scientist, Soumya Swaminathan, was on Twitter recently warning Indian nationals in the midst of a deadly COVID-19 wave not to take ivermectin citing Merck marketing material.[xxii] As a reminder, the pharmaceutical giant Merck is hoping to make billions with its potentially mutagenic molnupiravir which won’t happen if off-patent ivermectin is a standard of care. Swaminathan’s statement went against the official Indian recommendation in favor of ivermectin issued by the most highly regarded health association in India after the country had been confronted with a new COVID-19 variant and regions were seeing improvement with early Ivermectin treatment. In the aftermath, the Indian Bar Association served Swaminathan a legal notice for spreading dangerous disinformation and causing a significant number of deaths by discouraging the use of a life-saving drug.[xxiii] Swaminathan’s tweet has since been deleted. The legal notice for aggravated offences against humanity concerning ivermectin has by now been extended to the WHO Director General Tedros Adhanom.[xxiv]
The once noble idea of a global public health system working for mankind’s best interests has been replaced by an organization largely driven by the financial and ideological interests of private stakeholders. This is not a new phenomenon. International groups have long called for a reform of the WHO. In a global pandemic, the disastrous consequences of these pervasive organizational issues become even more apparent.
Distinguished scientists and frontline physicians from all over the world without conflicts of interest have called for the immediate use of ivermectin against COVID-19. Numerous randomized controlled trials (RCTs) and expert meta-analyses performed according to the highest standards of science have proven ivermectin’s effectiveness and reaffirmed its safety. Yet, a front of organizations including a significantly compromised WHO as well as wealthy private stakeholders with financial and ideological conflicts of interest have blocked the usage of this life-saving medication. Some observers have called this a crime against humanity which should be subjected to public scrutiny and an official criminal investigation. Ivermectin, meanwhile, should be used immediately to save lives as it has already been done successfully in a number of places worldwide.
From Wikipedia: ‘During the 2020 COVID-19 pandemic, misinformation was widely spread claiming that ivermectin was beneficial for treating and preventing COVID-19. Such claims are not backed by good evidence.’
WHEN encountering an inexplicable anomaly in human behaviour, common rules of thumb can often give an insight. Oddly, though, these differ from country to country. For Americans it is ‘follow the money’. For Italians it is ‘cui bono?’ – who benefits? The nearest French rule is perhaps ‘cherchez la femme’.
Sometimes none of these help. Sometimes a perverse piece of human nature cannot be explained in terms of money, perquisites or feminine influence. The ivermectin mystery is one such.
Ivermectin is a generic prescription drug, discovered in 1975, developed by Merck and released in 1981. It is used to treat many types of parasite infestations in humans and animals. The researchers who created it were awarded the Nobel Prize for medicine in 2015. It is on the World Health Organisation’s List of Essential Medicines and is approved by the Federal Drug Administration (FDA) as an antiparasitic agent.
It can have very rare serious side effects. By 2020 four billion doses had been administered and 16 deaths are believed to have occurred as a consequence, or one in 250million doses. Although the figures are not directly comparable, the annual increased risk of death for a middle-aged man taking a standard (325 mg) aspirin every day to prevent heart disease and stroke is about one in ten thousand. This is about as risky as driving a car.
Ivermectin is therefore a very safe drug. However, the drug oversight establishment does not think so.
‘EMA has reviewed the latest evidence on the use of ivermectin for the prevention and treatment of COVID-19 and concluded that the available data do not support its use for COVID-19 outside well-designed clinical trials.
‘In the EU, ivermectin tablets are approved for treating some parasitic worm infestations while ivermectin skin preparations are approved for treating skin conditions such as rosacea. Ivermectin is also authorised for veterinary use for a wide range of animal species for internal and external parasites.
‘Ivermectin medicines are not authorised for use in COVID-19 in the EU, and EMA has not received any application for such use.’
‘There seems to be a growing interest in a drug called ivermectin to treat humans with COVID-19. Ivermectin is often used in the U.S. to treat or prevent parasites in animals. The FDA has received multiple reports of patients who have required medical support and beenhospitalized after self-medicating with ivermectin intended for horses.
‘FDA has not approved ivermectin for use in treating or preventing COVID-19 in humans. Ivermectin tablets are approved at very specific doses for some parasitic worms, and there are topical (on the skin) formulations for head lice and skin conditions like rosacea. Ivermectin is not an anti-viral (a drug for treating viruses).
‘The FDA has not reviewed data to support use of ivermectin in COVID-19 patients to treat or to prevent COVID-19; however, some initial research is underway. Taking a drug for an unapproved use can be very dangerous. This is true of ivermectin, too.’
The lack of official support for trials of the efficacy of ivermectin has meant that the typical number of subjects being tested (the ‘cohort’) is fairly small, usually about a hundred. To overcome this a meta-analysis can be undertaken, when the results of many trials are combined and assessed to determine if a trend can be seen. This has been done, most notably by @CovidAnalysis. A paper most recently updated yesterday surveyed 60 properly conducted studies, most with double-blind testing against placebos, with neither the participants nor the researcher knowing who had been given the drug until the trial was over. This report is a preprint, so it has not been peer-reviewed, but the results are conclusive: 93 per cent of the studies show a positive outcome from the administration of ivermectin, with deaths reduced by over 80 per cent.
So why have what might be called ‘Drug Central’ refused to acknowledge this mammoth body of evidence arising from without their bailiwicks? Perhaps because of human nature again. Here they are obeying another rule of thumb commonly seen when institutions encounter new external factors – ‘not invented here’. Perhaps this business school aphorism is also appropriate: ‘Hell hath no fury like a head-office scorned’.
In any event the virucidal properties of ivermectin and its safety have now been established beyond doubt, and we can expect it to be valuable in this role from henceforth. But unfortunately not, perhaps, against Covid-19.
After months of denial, the U.S. government has acknowledged that the COVID-19 catastrophe may indeed have originated in a leak from a laboratory in Wuhan, China.
We are now allowed to talk about what until May 13 was a debunked conspiracy theory. Like many facets of the pandemic of our age, Wuhan was censored with the dreaded “disinformation” label, on Facebook and just about everywhere else. Not anymore.
The Wuhan debacle shows what happens when public health institutions have too much power, and the media plays mouthpiece rather than watchdog. Truth suffers. So does trust.
This commentary isn’t about the media’s wholesale buy-in of a possibly mythical pangolin that caused a pandemic.
This is about other potential Wuhans — issues that social and mainstream media have put to rest and closed to honest examination. We are told: Vaccines are safe. Lockdowns are just. We must protect, and be protected from, children. All those statements should be open to debate — and dispute.
I have spent the last eight months attacking another insidious COVID myth. It holds that there is no early treatment.
This actual disinformation has led to deaths and debility. In reporting it, the guardians of media have endowed public figures and institutions with wisdom they surely did not and do not have. Once definitive, Dr. Anthony Fauci of the National Institutes of Health and Dr. Tedros Ghebreyesus of the World Health Organization have reversed themselves on a potential Wuhan lab leak.
Then: “Extremely unlikely,” WHO said after a cursory probe.
Now: “Not convinced” the virus came from nature, said Fauci.
What else might they have gotten wrong?
‘Trusted’ News
Just months into the pandemic, research suggested that a handful of approved generic drugs could potentially quell COVID and save lives. By late last year, a safe drug that won its developers the Nobel Prize in Medicine in 2015 had risen to the top: ivermectin.
That few Americans know this is a direct result of two things: First is an unreasonably high, and shifting, bar set by the NIH, FDA and WHO, which collectively reject, cherry-pick or ignore what is now a trove of studies. Second is a media campaign that upholds the anti-IVM dictum, using charged language – from “controversial” to “snake oil” — that makes doctors, medical journals and other media fearful of backlash.
In a case of government propaganda, the Food and Drug Administration actually warned against ivermectin last spring, based, it said, on “multiple” people sickened by an animal formulation, which turned out to be four. Moreover, FDA admitted it “hadn’t studied” the considerable data then available on treatment with the human form.
As government failed us, mainstream and social media did something unique in modern history. Google, YouTube, Facebook, BBC, Washington Post, Associated Press, Reuters and others conspired to shape content and coverage in the government’s image.
They called it, ironically, the Trusted News Initiative. It existed to ferret out falsehoods and declare certainty in a rapidly changing information landscape. The media became a COVID fact-checking apparatus, devoid of nuance or meaningful investigation.
From the start, there was no room for both vaccines and treatments under the statute that has allowed millions of Americans to be vaccinated with an unlicensed, largely unstudied substance. The key mechanism on which this turned was the vaccine’s “Emergency Use Authorization,” which can be granted by the FDA only if there is “no adequate, approved, and available alternative to the product for diagnosing, preventing or treating” a disease.
But even as the vaccine was minimally tested and maximally hyped, there was an alternative. Ivermectin.
“It’s the most effective antiviral agent we have,” Dr. Paul E. Marik, co-founder of Front Line COVID-19 Critical Care Alliance, said in a conversation for this article. “If the WHO was to say that or the NIH — were they to approve ivermectin — the EUA for all the vaccines would become invalid.”
Ivermectin, said FLCCC president Dr. Pierre Kory, “would kneecap the entire global vaccine policy around the world.”
The choice was always vaccines OR treatment. Not both. Operation Warp Speed spent three times as much — $18 billion — to develop a vaccine as it did to develop a treatment. Moreover, money for therapeutics went largely toward costly new drugs, some of which failed and others still in development.
The media did not question the oversight of existing drugs and emerging research. Instead, it became an arm of government in a shared single fixed goal: Vaccinate quickly and at any expense.
A Year Lost
America’s COVID Czar Anthony Fauci predicted in July of 2020 that an antiviral would be available by that fall. Then, last December he said his “highest priority” was a quick-acting COVID drug. In reality, NIH waited until April 29, 2021 to announce a large study of safety-tested, FDA-approved drugs. That was roughly 400 days – and nearly 600,000 U.S. deaths — into the pandemic.
Forget a few dozen studies – most from other countries — that universally agreed on ivermectin’s efficacy. Forget a peer-reviewed meta-analysis that showed 83 percent fewer deaths. Forget the experiences of hundreds of real treating doctors in the U.S. and around the world.
Viewed in the kindest possible way, that delay, that lost year, wasn’t so much intentional as institutionalized. U.S. treatments are driven by the integral and outsized influence of pharmaceutical money on the regulatory process, and no one was putting up $20 million for what are considered, questionably, the “gold-standard” of evidence-based medicine: randomized control trials.
Dr. Robert Malone, a vaccine researcher and inventor of mRNA technology, went bankrupt trying to repurpose old antiviral drugs to treat the Zika virus in the 2010s. “The investment community had zero interest because there’s no way to make a buck,” he said in a must-see podcast on pandemic missteps. “The financial incentives around drug repurposing are such that it doesn’t get done.”
Ivermectin is the penicillin of COVID, particularly when combined with other generics like fluvoxamine and the vilified but effective hydroxychloroquine. Now, however, as at the start of COVID, newly infected patients are still denied treatment and turned back into the community, often to infect others.
As Malone put it, “We’re sending people home and telling them not to come back until your lips are blue.”
“Were this a hundred years ago,” a Pennsylvania opthamologist named Neil Chasin told me months ago, “and Ivermectin was available, it would be used everywhere.”
Media Sees No Evil
The dereliction of duty, by the New York Times, Washington Post, Wall Street Journal (with the Wuhan exception), Associated Press, USA Today and other media giants, likely cost many thousands of lives. The questions that were never asked, the issues never investigated, include:
–In April 2020, Fauci endorsed the high-priced anti-viral remdesivir, calling it the “standard of care” before the first study was published. Did anyone in those investigative powerhouses question the financial ties between the NIH and the drug’s maker, Gilead? Did they care that the study showed no mortality improvement, and the trial’s endpoint was changed to improve benefits so marginal that the WHO advises against the drug?
–Hospitals vehemently oppose ivermectin, forcing some patients’ families to obtain court orders to get it. Does this comport with their liberal use of treatments like monoclonal antibodies and convalescent plasma that are still considered experimental? Just 19 deaths were associated with ivermectin in 20 years; 503 were linked to remdesivir in its first year. Annualized, that’s roughly a 500-fold higher toll for remdesivir. Why is ivermectin — safe, FDA-approved — not used off-label, especially in dying ICU patients, when the potential harm is miniscule?
–The COVID pandemic has led to the most widespread, government-sanctioned wave of censorship and authoritarian message control in American history. Rather than fighting this, the media carries the water. When Merck disingenuously disavowed ivermectin’s safety — a drug it gave away by the billion in a life-saving campaign against parasites — widespread media reports failed to note the company’s potential to make big money on patented new drugs on which it was already working.
–More importantly, the evidence in favor of ivermectin aligns so uniformly that the odds of it being wrong are infinitesimal. Why not read the studies? Why not talk to doctors who have used the drug and patients who have taken it?
The unholy alliance of media and money was foreshadowed at a 2016 conference on preparation for the next SARS epidemic. There, Peter Daszak, whose NIH funding for virus research in China is under scrutiny, emphasized the need to use the press. He is quoted in the proceedings:
“A key driver is the media, and the economics follow the hype. We need to use that hype to our advantage … Investors will respond if they see profit at the end of process, Daszak stated.”
So far, the hype has prevailed. But it can be wrong. Can we now talk about ivermectin?
***
Mary Beth Pfeiffer is an investigative journalist and author of twobooks. A list of her article links can be found here.
One should believe the science, and the scientific evidence is overwhelming that ivermectin (IVM) and hydroxychloroquine (HCQ) are effective for preventing and treating COVID, especially when combined with other drugs.
The information has been available since the start of the pandemic. As early as April of 2020, some clinicians were saving their patients and pleading, in vain, with the health authorities to investigate the value of these drugs.
Throughout this time, the major social media companies have suppressed this vital information. Facebook seems to be the most ruthless. YouTube and Twitter are close behind, though some information escapes the eagle eye of the censors.
COVID-19 Response. In response to the COVID-19 pandemic, we launched multiple initiatives to support the global public health community’s work to keep people safe and informed. We took steps to provide our community with access to accurate information, stop misinformation and harmful content, and support global health experts, local governments, businesses, and communities. . . We also launched an information center on Facebook and Instagram to provide our community with real-time updates, information, and the ability to offer and ask for help. We have already connected over two billion people to authoritative COVID-19 information[.]
In its zeal to “keep people safe and informed,” Facebook also deplatforms groups that question the safety of the vaccines.
The wages of this sin of official mendacity and private enforcement of The Official Narrative is death. Of the 600,000 Americans who died of COVID (at least according to official numbers), a defensible estimate is that 500,000 could have been saved. And it continues, even as the evidence in favor of these treatments continues to confirm their value.
These facts raise a puzzling issue of corporate governance. All of these companies are controlled by boards of directors composed of the crème de la crème of the American elite. See the members of the Board of Facebook, Twitter, and Alphabet (which owns YouTube). They are well compensated. For example, Alphabet directors get $75,000 to $100,000 in fees, plus bonuses such as stock options that can boost total annual compensation to almost half a million.
Board members are mostly from the corporate and financial worlds, but not entirely. A Twitter director is Fei-Fei Liu, a Canadian cancer researcher, whose personal opinion would be worth knowing. Facebook’s board includes Peter Thiel, one of the most brilliant entrepreneurs of our time, and chair of the company’s Compensation, Nominating, and Governance Committee. Until 2018, the Alphabet Board included Shirley Tilghman, a distinguished molecular biologist. Her opinion on the censorship would also be interesting.
So what is going on here? These people are far too sophisticated to take at face value all the statements of Anthony Fauci or the World Health Organization. They did not get rich and powerful by being so credulous, and their refusal to look behind the Wizard’s curtain demands explanation.
Because stupidity won’t serve, the most logical explanation is strategic cowardice. As long as the companies can pretend to believe Fauci and WHO, they will not bear legal responsibility for any consequences. Were they to provide alternative information, they have reason to fear a weaponized Deep State, which could make a company’s life hell. All the quasi-monopoly social media outlets need continuing government forbearance.
But neither should one neglect sloth and greed. For an individual director to raise the alarm would require work to review the literature and would risk the loss of a lucrative board seat. It is easier to pretend to believe the staff’s assurances.
As to the moral responsibility for the unnecessary fatalities, remember the old Tom Lehrer song: “Once the rockets are up, who cares where they come down? That’s not my department!” In the end, if cornered, the directors can claim that they were just following orders and blame Fauci.
But one would like to see the news media start asking them for an explanation.
Ivermectin, a common anti-parasite drug, has shown great efficacy in the fight against covid-19. For the first time, medical researchers have documented how ivermectin docks to the SARS-CoV-2 spike receptor-binding domain that is attached to the ACE2 receptor. In this way, ivermectin effectively inhibits viral attachment and replication, assisting a precise antiviral response that can target the SARS-CoV-2 spike protein at its most advantageous cleavage site. The researchers showed how ivermectin interferes with the attachment of the spike protein to the human cell membrane. Ivermectin is a simple medicine derived from the bacterium Streptomyces avermitilis. It weakens and kills parasites by interfering with their nervous system and muscle function. Ivermectin targets the glutamate-gated chloride channels in the parasite’s nerve and muscle cells, bolstering inhibitory effects in the parasite’s own neurotransmission. As the chloride ions permeate, the parasite’s cells are hyper-polarized and then paralyzed, resulting in their demise. In this study, ivermectin docked in region of leucine 91 of the spike protein and at the histidine 378 of the ACE2 receptor. The binding energy and constancy of ivermectin was also measured and found to be sufficient at the ACE2 receptor, proving the anti-parasitic molecule a powerful force for blocking viral attachment of SARS-CoV-2.
Ivermectin blocks SARS CoV-2 at the ACE2 receptor in humans
The 17 randomized controlled trials that use ivermectin for early treatment and prophylaxis report positive effects, with an estimated improvement of 73 percent and 83 percent, respectively. Out of 37 early treatment and prophylaxis studies for ivermectin, 97 percent report positive effects. One of the studies documents how ivermectin inhibits the replication of SARS-CoV-2 in vitro and displays broad-spectrum anti-viral activity against the causative virus (SARS-CoV-2). This study showed a 5,000-fold reduction in viral RNA after just 48 hours. The study also proves that effective treatments and prophylactics can mitigate the replication and spread of a virus thousands of times faster than the paranoid, isolationist approach of social distancing and lockdowns. If antivirals were encouraged early and often, then the spread of actual infectious virus would have been mitigated at rates thousands of times faster than the insane method of treating everyone as if they are infectious. By treating actual infections where symptoms are present, the spread is reduced at magnitudes thousands of times greater, while conveying immunity instead of terror. The SARS-CoV-2 spike protein is designed to attach to angiotensin-converting enzyme 2 (ACE2) in humans. To see whether ivermectin could dock at this receptor site and block viral attachment, the researchers used a program called AutoDock Vina Extended. This docking study showed the crystal structure of the SARS-CoV-2 spike receptor binding domain. The researchers looked specifically at the human ACE2 receptor and calculated the root-mean-square deviation (RMSD) of its atomic positions. A lower RMSD value indicates a more accurate docking capacity. When the RMSD value is three or greater, no docking has occurred at the receptor site. Ivermectin did not dock at nine of the locations; however, it did dock at the leucine 91 region of the spike and histidine 378 at the intersection of proteins between SARS CoV-2 and the ACE2 receptor complex. Previous studies proved ivermectin’s efficacy, but had to use high concentrations of the drug because the study relied on African green monkey kidney epithelial cells, which do not express the human ACE2 receptor. SARS-CoV-2 is specifically equipped to infect human ACE2 receptors, so this study could prove ivermectin to be effective in much smaller dosages. Clinical trials are now underway to determine if ivermectin is an effective treatment for covid-19.
The global conspiracy to suppress effective anti-viral medicines
The World Health Organization, the FDA, and the NIH have repeatedly suggested that no antiviral treatments exist for covid-19, even though multiple antiviral herbs and drugs have been studied during previous SARS and MERS epidemics and found to be effective. This time around, many of these antivirals were used with great effectiveness by doctors who were willing to go out on a limb and save lives. Chinese hospitals used various antiviral herbs to treat covid-19 patients. These hospitals studied the effects of the herbs for impeding virus-cell receptor binding, for stimulation of the host’s immunity, for blocking virus entry into host cells through action on the host’s enzymes, and for prevention of SARS-CoV-2 RNA synthesis and replication. The research found numerous phytochemicals to be effective, including: quercetin, ursolic acid, kaempferol, isorhamnetin, luteolin, glycerrhizin, and apigenin. The top three most effective plants for treating covid-19 included licorice root, (Glycyrrhiza glabra) chicory root, (Cichorium intybus) and hibiscus flowers (Hibiscus sabdariffa). A number of antiviral plants contain compounds that target all three antiviral targets, including olive leaf (Olea europaea), white horehound (Marrubium vulgare), black cumin seed (Nigella sativa), garden cress (Lepidium sativum), Judean wormwood (Artemisia Judaica), guava (Psidium guajava), chrysanthemum (Glebionis coronaria), and Maryam’s flower (Anastatica). Medical systems around the world are not properly equipped to strengthen the human immune response or understand what individuals need to overcome an infection. When it comes to fighting infections, the US FDA and European drug regulators parrot the same narrative of ignorance and apathy, withholding viable antivirals from the public. By the way, this is the only legal way to bring experimental vaccines to the global marketplace, by proving that no effective treatments exist. This suppression of science on antiviral treatments has paved the way for emergency use authorization of experimental vaccines and forced countless patients to suffer (and die) on ventilators, without treatment.
On 25 May 2021, the Indian Bar Association (IBA) served a 51-page legal notice on Dr Soumya Swaminathan, the Chief Scientist at the World Health Organisation (WHO), for:
[H]er act of spreading disinformation and misguiding the people of India, in order to fulfil her agenda.”
The Mumbai-based IBA is an association of lawyers who strive to bring transparency and accountability to the Indian justice system. It is actively involved in the dissemination of legal knowledge and provides guidance and support to advocates and ordinary people in their fight for justice.
The legal notice says Dr Swaminathan has been:
Running a disinformation campaign against Ivermectin by deliberate suppression of effectiveness of drug Ivermectin as prophylaxis and for treatment of COVID-19, despite the existence of large amounts of clinical data compiled and presented by esteemed, highly qualified, experienced medical doctors and scientists,”
And:
Issuing statements in social media and mainstream media, thereby influencing the public against the use of Ivermectin and attacking the credibility of acclaimed bodies/institutes like ICMR and AIIMS, Delhi, which have included ‘Ivermectin’ in the ‘National Guidelines for COVID-19 management’.”
The IBA states that legal action is being taken against Dr Swaminathan in order to stop her from causing further damage to the lives of citizens of India.
The IBA says that Dr Swaminathan has ignored these studies and reports and has deliberately suppressed the data regarding the effectiveness of Ivermectin, with an intent to dissuade the people of India from using it.
However, two key medical bodies, the Indian Council for Medical Research (ICMR) and the All India Institute of Medical Sciences (AIIMS) Delhi, have refused to accept her stand and have retained the recommendation for Ivermectin, under a ‘May Do’ category, for patients with mild symptoms and those in home isolation, as stated in ‘The National Guidelines for COVID-19 management’.
It is interesting to note that the content of several web links to news articles and reports included in the notice served upon Dr Swaminathan, which was visible before issuing the notice, has either been removed or deleted.
It seems that the vaccine manufacturers and many governments are desperate to protect their pro-vaccine agenda and will attempt to censor information and news regarding the efficacy of Ivermectin.
Although a great majority of ivermectin-based studies have indicated real promise, one particular study conducted by a small trial site in Colombia received unprecedented media attention when the study results indicated negligible impact. What hasn’t been disclosed by media is the seriously questionable pharmaceutical industry support of this one trial site. During the study, a handful of some of the largest drug companies in the world gave this site money. What’s not clear is why this occurred and whether the funds are correlated to some nefarious agenda. This author suggests that the publisher should have scrutinized this industry funding perhaps more carefully.
On March 4th, 2021, an article appeared in JAMA titled, “Effect of Ivermectin On Time To Resolution of Symptoms Among Adults With Mild COVID.” It concluded, “The findings do not support the use of ivermectin for treatment of mild COVID-19, although larger trials may be needed to understand the effects of ivermectin on other clinically relevant outcomes.”
Dr. Eduardo Lopez-Medina et al. from Cali, Colombia, randomized 400 mildly ill patients, averaging 37 years old, to ivermectin 0.3 mg/kg or placebo. The time to resolution for ivermectin-treated patients was 10 days and placebo patients 12 days, which was not statistically significant.
Much has been written about the methodologic problems of the study but few read to the bottom of the article to see this:
Conflict of Interest Disclosures: Dr. López-Medina reported receiving grants from Sanofi Pasteur, GlaxoSmithKline, and Janssen as well as personal fees from Sanofi Pasteur during the conduct of the study. Dr. Oñate reported receiving grants from Janssen and personal fees from Merck Sharp & Dohme and Gilead outside the submitted work. Dr. Torres reported receiving nonfinancial support from Tecnoquímicas unrelated to this project during the conduct of the study. No other disclosures were reported.
Considerable press outlets noted this study, we suspect due to the fact that the ivermectin results were negligible, but none of the media addressed the possibility of conflict with industry.
Absolutely nothing has been written about the fact that the study was sponsored by Centro de Estudios en Infectogía Pediatrica and the authors were paid by 3 drug companies making COVID vaccines–Sanofi Pasteur, GlaxoSmithKline, and Janssen– and two making COVID therapeutics–Gilead and Merck.
We have some questions about this. Why did the authors disclose that they were receiving industry sponsor funds during the conduct of the study? Were these funds to actually direct the ivermectin study? That would most certainly be a conflict of interest material.
Merck’s expressed their intent on competing against the ivermectin generic approach. Why would this company be funding this small trial site operation in Colombia?
How could JAMA even think about publishing an article sponsored by 5 drug companies centering on a study targeting a generic competitor? Any layperson seeing this could think that this was highly suspect.
The potential conflict of interest was so severe that no journal should have published it.
Why would anyone do this study?
Was there a pressing need to know if 37-year-old patients got better sooner with ivermectin than placebo? There were a lot of resources put into this study. The only possible reason to do the study was for drug companies to have a vehicle to publish negative data about ivermectin. Is there anyone who believes the study was sponsored to add to the scientific knowledge about ivermectin for the treatment of COVID?
On February 4th, 2021, Merck, who had the original patent on ivermectin, put out a statement regarding ivermectin for COVID:
• No scientific basis for a potential therapeutic effect against COVID-19 from pre-clinical studies;
• No meaningful evidence for clinical activity or clinical efficacy in patients with COVID-19 disease; and
• A concerning lack of safety data in the majority of studies.
If Merck believed these statements to be true, why would they feel the need to go public with them?
Merck’s vaccine had failed. Merck had bought a company, Oncoimmune, for $425 million and gotten $356 million from HHS in taxpayer money to develop a therapeutic agent, CD24c. They had a material conflict of interest. Later, the European Medicines Agency and World Health Organization both quoted Merck’s statement while ignoring the conflict of interest and science in recommending against the use of ivermectin for COVID, other than for research. Were they influenced by Merck? CD24c was dropped, and Merck has oral antiviral molnupiravir in a phase II-III trial. Why would Merck sponsor a trial of ivermectin?
Why would JAMA publish an article showing that young patients who are expected to recover quickly don’t get better much more quickly with ivermectin?
This article did not warrant publication in JAMA. The only possible reason to publish it was to present false, negative information about ivermectin to readers.
Why was the age of the patients not mentioned in the key findings or conclusions?
The age of the patients made the article irrelevant. It could not have been an accident that the age was not mentioned in the key findings and conclusions. That would never happen at JAMA. The authors anticipated that many readers would miss the age of the patients and conclude that ivermectin is ineffective in early COVID. Dr. Adfarsh Bhimraj at Cleveland Clinic who heads the committee writing COVID recommendations for the Infectious Disease Association of America spoke with Helio Medical News on ivermectin. He had a similar observation in the Washington Post.
“This was a well-done, but small trial in patients with mild or moderate disease,” Bhimraj said. He suggested that this is a negative study for a non-mortality outcome, but because the numbers were small, it might not have produced a statistically significant difference in effect size. The evidence is not enough to warrant a recommendation for the use of ivermectin. Other US experts who commented on the article have failed to notice the age of the patients and drug company sponsorship. It has crossed few American physicians’ minds that JAMA could be corrupted and knowingly publish a study with deceptive results in order to help drug companies.
Was the data fraudulent?
If the purpose of the article was to make it appear that ivermectin was ineffective in mild COVID, there is no reason to believe the data was real. There is no published randomized data for comparison. In the Dominican Republic, Dr. Jose Natalio Redondo reported that in 1300 patients with all degrees of illness, the length of illness went from 21 days to 10 days with ivermectin treatment.
Was JAMA aware that there was concern they had been corrupted and the article unreliable?
Sixteen members of the AMA Board of Directors were emailed that it appeared that JAMA had been infiltrated and the article fraudulent on March 10th, 2021. Eleven JAMA editorial board members were emailed about it April 12th. And one was spoken to. The same email was sent to executive editor Dr. Phil Fontanarosa April 13th. This reply was sent:
“Your message was brought to my attention.
I will look into these issues as outlined in your letter.
Please bear with me, as this will take some time, given the number of issues and the complexity of the concerns you raise, as well as other urgent issues and priorities we are addressing right now.”
As of 6/8/21, the article has been read online 759,000 times. How many of those readers concluded that ivermectin is ineffective for mild COVID and, as a result, did not prescribe it for their patients? To put things in perspective, Uttar Pradesh, India, with 210 million people, started ivermectin in August. By December, their mortality rate was 0.26 per 100,000. In the US, in December, it was 11 times higher at 2.8 per 100,000. Admissions in Mexico are down 75% due to ivermectin.
The JAMA article of 3/4/21 was a cleverly devised drug company creation designed to create the false impression that ivermectin was ineffective in mild COVID by claiming it didn’t shorten the duration of illness significantly. They knew people would miss the age of the patients and not read to the bottom of the article to see that it was sponsored by 5 drug company competitors. They knew people would leap to the conclusion that ivermectin was completely ineffective for COVID, not realizing that the article could not address its effects on hospitalization and death. An infectious disease doctor friend sent it to me as proof that ivermectin does not work. Drug companies would not have gone to these lengths if they did not fear ivermectin as a competitor.
JAMA reviewers could not possibly have missed the obvious conflict of interest. It was obviously their intention to spread misinformation. Leaving out the age of the patients was intentional to make readers think it was ineffective in everyone. The article has not only led to patient care being adversely affected but the article has been widely quoted as evidence against the use of ivermectin. WHO says it is the number one article in support of its position.
Doctors should contact JAMA to understand what is going on with the investigation. JAMA should report on their findings as they committed to this author to undertake an investigation.
Michael Capuzzo, a New York Times best-selling author, has just published an article titled “The Drug That Cracked Covid”. The 15-page article chronicles the gargantuan struggle being waged by frontline doctors on all continents to get ivermectin approved as a Covid-19 treatment, as well as the tireless efforts by reporters, media outlets and social media companies to thwart them.
Because of ivermectin, Capuzzo says, there are “hundreds of thousands, actually millions, of people around the world, from Uttar Pradesh in India to Peru to Brazil, who are living and not dying.” Yet media outlets have done all they can to “debunk” the notion that ivermectin may serve as an effective, easily accessible and affordable treatment for Covid-19. They have parroted the arguments laid out by health regulators around the world that there just isn’t enough evidence to justify its use.
For his part, Capuzzo, as a reporter, “saw with [his] own eyes the other side [of the story]” that has gone unreported, of the many patients in the US whose lives have been saved by ivermectin and of five of the doctors that have led the battle to save lives around the world, Paul Marik, Umberto Meduri, José Iglesias, Pierre Kory and Joe Varon. These are all highly decorated doctors. Through their leadership of the Front Line COVID-19 Critical Care (FLCCC) Alliance, they have already enhanced our treatment of Covid-19 by discovering and promoting the use of Corticoid steroids against the virus. But their calls for ivermectin to also be used have met with a wall of resistance from healthcare regulators and a wall of silence from media outlets.
“I really wish the world could see both sides,” Capuzzo laments. But unfortunately most reporters are not interested in telling the other side of the story. Even if they were, their publishers would probably refuse to publish it.
That may explain why Capuzzo, a six-time Pulitzer-nominated journalist best known for his New York Times-bestselling nonfiction books Close to Shore and Murder Room, ended up publishing his article on ivermectin in Mountain Home, a monthly local magazine for the of the Pennsylvania mountains and New York Finger Lakes region, of which Capuzzo’s wife is the editor. It’s also the reason why I decided to dedicate today’s post to Capuzzo’s article. Put simply, as many people as possible –particularly journalists — need to read his story.
As Capuzzo himself says, “I don’t know of a bigger story in the world.”
Total News Blackout
On December 8 2020, FLCCC member Dr Pierre Kory gave nine minutes of impassioned testimony to the US Homeland Security Committee Meeting on the potent anti-viral, anti-inflammatory benefits of ivermectin. A total of 9 million people (myself included) saw the video on YouTube before it was taken down by YouTube’s owner, Google. As Capuzzo exhaustively lays out, both traditional and social media have gone to extraordinary lengths to keep people in the dark about ivermectin. So effective has this been that even in some of the countries that have benefited most from its use (such as Mexico and Argentina) many people are completely unaware of its existence. And this is no surprise given how little information is actually seeping out into the public arena.
A news blackout by the world’s leading media came down on Ivermectin like an iron curtain. Reporters who trumpeted the COVID-19 terror in India and Brazil didn’t report that Ivermectin was crushing the P-1 variant in the Brazilian rain forest and killing COVID-19 and all variants in India. That Ivermectin was saving tens of thousands of lives in South America wasn’t news, but mocking the continent’s peasants for taking horse paste was. Journalists denied the world knowledge of the most effective life-saving therapies in the pandemic, Kory said, especially among the elderly, people of color, and the poor, while wringing their hands at the tragedy of their disparate rates of death.
Three days after Kory’s testimony, an Associated Press “fact-check reporter” interviewed Kory “for twenty minutes in which I recounted all of the existing trials evidence (over fifteen randomized and multiple observational trials) all showing dramatic benefits of Ivermectin,” he said. Then she wrote: “AP’S ASSESSMENT: False. There’s no evidence Ivermectin has been proven a safe or effective treatment against COVID-19.” Like many critics, she didn’t explore the Ivermectin data or evidence in any detail, but merely dismissed its “insufficient evidence,” quoting instead the lack of a recommendation by the NIH or WHO. To describe the real evidence in any detail would put the AP and public health agencies in the difficult position of explaining how the lives of thousands of poor people in developing countries don’t count in these matters.
Not just in media but in social media, Ivermectin has inspired a strange new form of Western and pharmaceutical imperialism. On January 12, 2021, the Brazilian Ministry of Health tweeted to its 1.2 million followers not to wait with COVID-19 until it’s too late but “go to a Health Unit and request early treatment,” only to have Twitter take down the official public health pronouncement of the sovereign fifth largest nation in the world for “spreading misleading and potentially harmful information.” (Early treatment is code for Ivermectin.) On January 31, the Slovak Ministry of Health announced its decision on Facebook to allow use of Ivermectin, causing Facebook to take down that post and removed the entire page it was on, the Ivermectin for MDs Team, with 10,200 members from more than 100 countries.
In Argentina, Professor and doctor Hector Carvallo, whose prophylactic studies are renowned by other researchers, says all his scientific documentation for Ivermectin is quickly scrubbed from the Internet. “I am afraid,” he wrote to Marik and his colleagues, “we have affected the most sensitive organ on humans: the wallet…” As Kory’s testimony was climbing toward nine million views, YouTube, owned by Google, erased his official Senate testimony, saying it endangered the community. Kory’s biggest voice was silenced.
“The Most Powerful Entity on Earth”
Malcom X once called the media “the most powerful entity on the earth.” They have, he said, “the power to make the innocent guilty and to make the guilty innocent, and that’s power. Because they control the minds of masses”. Today, that power is now infused with the power of the world’s biggest tech and social media companies. Together social and traditional media have the power to make a medicine that has saved possibly millions of lives during the current pandemic disappear from the conversation. When it is covered, it’s almost always in a negative light. Some media organizations, including the NY Times, have even prefaced mention of the word “ivermectin” — a medicine that has done so much good over its 40-year lifespan that its creators were awarded the Nobel Prize for Medicine in 2015 — with the word “controversial.”
Undeterred, many front-line doctors have tried to persuade their respective health regulators of the unparalleled efficacy and safety of ivermectin as a covid treatment. They include Dr. Tess Lawrie, a prominent independent medical researcher who, as Capuzzo reports, evaluates the safety and efficacy of drugs for the WHO and the National Health Service to set international clinical practice guidelines:
“[She] read all twenty-seven of the Ivermectin studies Kory cited. The resulting evidence is consistent and unequivocal,” she announced, and sent a rapid meta-analysis, an epidemiolocal statistical multi-study review considered the highest form of medical evidence, to the director of the NHS, members of parliament, and a video to Prime Minister Boris Johnson with “the good news… that we now have solid evidence of an effective treatment for COVID-19…” and Ivermectin should immediately “be adopted globally and systematically for the prevention and treatment of COVID-19.”
Ignored by British leaders and media, Lawrie convened the day-long streaming BIRD conference—British Ivermectin Recommendation Development—with more than sixty researchers and doctors from the U.S., Canada, Mexico, England, Ireland, Belgium, Argentina, South Africa, Botswana, Nigeria, Australia, and Japan. They evaluated the drug using the full “evidence-to-decision framework” that is “the gold standard tool for developing clinical practice guidelines” used by the WHO, and reached the conclusion that Ivermectin should blanket the world.
“Most of all you can trust me because I am also a medical doctor, first and foremost,” Lawrie told the prime minster, “with a moral duty to help people, to do no harm, and to save lives. Please may we start saving lives now.” She heard nothing back.
Ivermectin’s benefits were also corroborated by Dr. Andrew Hill, a renowned University of Liverpool pharmacologist and independent medical researcher, and the senior World Health Organization/UNITAID investigator of potential treatments for COVID-19. Hill’s team of twenty-three researchers in twenty-three countries had reported that, after nine months of looking for a COVID-19 treatment and finding nothing but failures like Remdesivir— “we kissed a lot of frogs”— Ivermectin was the only thing that worked against COVID-19, and its safety and efficacy were astonishing—“blindingly positive,” Hill said, and “transformative.” Ivermectin, the WHO researcher concluded, reduced COVID-19 mortality by 81 percent.
Why All the Foot Dragging?
Yet most health regulators and governments continue to drag their feet. More evidence is needed, they say. All the while, doctors in most countries around the world have no early outpatient medicines to draw upon in their struggle against the worst pandemic in century. Drawing on his own experience, Capuzzo describes the absence of treatments for COVID-19 as a global crisis:
When my daughter Grace, a vice president at a New York advertising agency, came
down with COVID-19 recently, she was quarantined in a “COVID hotel” in Times Square with homeless people and quarantining travelers. The locks on her room door were removed. Nurses prowled the halls to keep her in her room and wake her up every night to check her
vitals—not to treat her, because there is no approved treatment for COVID-19; only, if her oxygen plummeted, to move her to the hospital, where there is only a single eective approved treatment for COVID-19, steroids that may keep the lungs from failing.
There are three possible explanations for health regulators’ refusal to allow the use of a highly promising, well-tolerated off-label medicine such as ivermectin:
As a generic, ivermectin is cheap and widely available, which means there would be a lot less money to be made by Big Pharma if it became the go-to early-stage treatment against covid.
Other pharmaceutical companies are developing their own novel treatments for Covid-19 which would have to compete directly with ivermectin. They include ivermectin’s original manufacturer, Merck, which has an antiviral compound, molnupiravir, in Phase 3 clinical trials for COVID-19. That might explain the company’s recent statement claiming that there is “no scientific basis whatsoever for a potential therapeutic effect of ivermectin against COVID-19.
If approved as a covid-19 treatment, ivermectin could even threaten the emergency use authorisation granted to covid-19 vaccines. One of the basic conditions for the emergency use authorisation granted to the vaccines currently being used against covid is that there are no alternative treatments available for the disease. As such, if ivermectin or some other promising medicine such as fluvoxamine were approved as an effective early treatment for Covid-19, the vaccines could be stripped of authorisation.
This may explain why affordable, readily available and minimally toxic drugs are not repurposed for use against Covid despite the growing mountains of evidence supporting their efficacy.
Ivermectin has already been approved as a covid-19 treatment in more than 20 countries. They include Mexico where the mayor of Mexico City, Claudia Scheinbaum, recently said that the medicine had reduced hospitalisations by as much as 76%. As of last week, 135,000 of the city’s residents had been treated with the medicine. The government of India — the world’s second most populous country and one of the world’s biggest manufacturers of medicines — has also recommended the use of ivermectin as an early outpatient treatment against covid-19, in direct contravention of WHO’s own advice.
Dr Vikas P. Sukhatme, the dean of Emory School of Medicine, recently wrote in a column for the Times of India that deploying drugs such as ivermectin and fluvoxamine in India is likely to “rapidly reduce the number of COVID-19 patients, reduce the number requiring hospitalization, supplemental oxygen and intensive care and improve outcomes in hospitalized patients.”
Four weeks after the government included ivermectin and budesonide among its early treatment guidelines, the country has recorded its lowest case count in 40 days.
In many of India’s regions the case numbers are plunging in almost vertical fashion. In the capital Delhi, as in Mexico City, hospitalisations have plummeted. In the space of 10 days ICU occupancy fell from 99% to 70%. Deaths are also falling. The test positivity ratio slumped from 35% to 5% in just one month.
One of the outliers of this trend is the state of Tamil Nadu, where cases are still rising steeply. This may have something to do with the fact that the state’s newly elected governor, MK Stalin, decided to exclude ivermectin from the region’s treatment protocol in favor of Remdesivir. The result? Soaring cases. Late last week, Stalin reversed course once again and readopted ivermectin.
For the moment deaths in India remain extremely high. And there are concerns that the numbers are being under-reported. Yet they may also begin to fall in the coming days. In all of the countries that have used ivermectin widely, fatalities are the last thing to fall, after case numbers and hospitalizations. Of course, there’s no way of definitively proving that these rapid falloffs are due to the use of ivermectin. Correlation, even as consistent as this, is not causation. Other factors such as strict lockdowns and travel restrictions no doubt also play a part.
But a clear pattern across nations and territories has formed that strongly supports ivermectin’s purported efficacy. And that efficacy has been amply demonstrated in three meta-analyses.
India’s decision to adopt ivermectin, including as a prophylaxis in some states, is already a potential game-changer. As I wrote three weeks ago, if case numbers, hospitalizations and fatalities fall in India as precipitously as they have in other countries that have adopted ivermectin, it could even become a watershed moment. But for that to happen, the news must reach enough eyes and ears. And for that to happen, reporters must, as Capuzzo says, begin to do their job and report both sides of this vital story.
One country that has had remarkable success in the war against the COVID pandemic, but has received little to no global media coverage, is Mexico. Like the rest of the world, COVID cases in Mexico exploded in April 2020, the first hot spots flaring up along the northern border with the United States, in Mexico City and Quintana Roo, a popular tourist destination in the Caribbean. At the beginning of the pandemic, Mexico took recommendations and followed protocol set forth by the World Health Organization (WHO) and watched the virus spread from state to state, engulfing the entire country.
First COVID Outbreak in Mexico
On June 10, the Spanish-speaking media began reporting on the success that Peru was having in controlling the virus using ivermectin as a treatment. Mexico was in the middle of its worst peak of cases and deaths with records breaking daily, and interest in the drug – as well as sales – rose dramatically.
On June 20, the pan-American WHO (OPS/OMS) issued a statement strongly opposing the use of ivermectin. Additionally, other media sources started publishing anti-ivermectin articles all over Mexico. And as the number of deaths slowly decreased, interest in ivermectin subsequently died down.
Google trends. Google seaches in Mexico about iveremctin
In October 2020, cases in Mexico began spiking again; the outbreak this time started in Chihuahua, the state on the border of Texas. Texas was also experiencing an outbreak at this time, so it’s likely that the cases in Mexico were sparked in the US. From Chihuahua, cases spread south and into Mexico City igniting the worst outbreak yet. Mexico City was an inferno of COVID cases and death, and health workers rushed to the capital city from all over the country to help.
Determined to stop the spread at any cost, Mexico City officials held a meeting at the end of December, 2020, and invited the Instituto Mexicano del Seguro Social (IMSS) among other groups of doctors. Together, they decided to begin distribution of ivermectin kits in Mexico City and Mexico State to anyone who tested positive for COVID and wanted to take the drug, and to closely monitor hospitalizations to keep tabs on ivermectin’s efficacy. The kits distributed included ivermectin, aspirin and paracetamol. Between the end of November 2020 and the end of January 2021, more than 200,000 people tested positive for COVID, and of these, nearly 80,000 used the ivermectin kits. Results showed up to 76% reduction in hospitalization in the group that was taking ivermectin.
On January 22, 2021, the mayor of Mexico City, Claudia Scheinbaum, held a live televised press conference where she talked about the positive results from the ivermectin distribution from December. Following the press release, the kits were made available for everyone in the whole of Mexico, and nation-wide results of ivermectin use were monitored. Amazingly, after mass distribution of ivermectin, every single COVID indicator in Mexico improved. Over the course of 18 weeks, COVID cases, hospitalizations, and deaths continuously dropped, and on May 14, the mayor held another televised press conference sharing the positive results of the months’-long campaign.
What is astonishing, however, is that the media outlets in Mexico have not reported on this astounding result. They continued to report on the number of excess deaths from before the ivermectin intervention – and not one has covered the current situation of declining cases and deaths due to wide-spread ivermectin intervention.
Major benefits of ivermectin (IVM) treatment for COVID-19 have been known since the results of 20 such randomized controlled trials (RCTs) were reported, as compiled in January 2021. Of the eight of these RCTs that tracked mortality or morbidity in patients with serious cases, seven showed statistically significant clinical improvements. The pooled mortality reduction in these eight RCTs was 78% in the treatment vs. controls groups, and the RCT that used the highest dose of IVM reported a 92% reduction in mortality (p < 0.001). Three RCTs for IVM prevention of COVID-19 and two animal studies of IVM at low human-equivalent doses likewise reported pronounced efficacy. Here we note the recent publication of RCTs for IVM treatment or prevention of COVID-19 in mainstream scientific journals that confirm these previously reported findings.
Background
The consistently observed, major benefits of ivermectin (IVM) for COVID-19 treatment have been known since a January 2021 meta-study compiled results of 20 such randomized clinical trials (RCTs).1 Of the eight of these RCTs that tracked mortality or morbidity in patients with moderate or severe symptoms (4 double-blind,2-5 1 single-blind,6 and 3 non-blinded7-9), seven showed statistically significant clinical improvements (all but Podder et al.8). The pooled mortality reduction in these eight RCTs for the IVM treatment group vs. controls was 78% (mortality of 2.1% for IVM, 9.5% for controls). The RCT that used the highest dose of IVM, 1,600 μg/kg total, had 2 vs. 24 deaths in the treatment vs. control group (n=200 each),7 a 92% reduction in mortality (p < 0.001).
Complementing these IVM treatment studies, three RCTs evaluated IVM for prevention in subjects exposed to COVID-19 patients. These studies reported relative COVID-19 incidences of 20%, 16% and 13% compared with incidences in controls, with even lower relative incidences for serious such cases. In addition, two animal studies of IVM treatment at low human-equivalent doses for SARS-CoV-2 in hamsters10 and for a closely related betacoronavirus in mice11 likewise found major, highly statistically significant treatment benefits.
Yet some skeptical reviewers had dismissed this overwhelming RCT evidence for clinical efficacy of IVM against COVID-19, claiming insufficient quality of the studies,12,13 as had been indicated by the lack of publication of any in mainstream scientific journals. The recent publication of five such RCTs for IVM in top-tier journals, including Lancet eClinicalMedicine14 and BMC infectious diseases,15 all reporting major, statistically significant clinical benefits against COVID-19, dismantles these skeptical critiques.
Five recently published studies in mainstream scientific journals
Among these five recently published RCTs was a prevention study of April 2021 by Seet et al.16 IVM was administered to 617 subjects, with 2,420 other subjects assigned to either a control group or to one of three other preventative regimens. The subjects were then tracked for onset of COVID-19 symptoms and positive nasopharyngeal PCR tests over a 42-day period. IVM at a dose of 12 mg was given just once on day one, while the three other preventative regimens were each administered daily during this 42-day period. Yet IVM at this single low dose yielded the best clinical results, reducing incidence of symptomatic COVID-19 by 50% (p=0.003) and of ARDS symptoms by 49% (p=0.012) with respect to controls. IVM at that single low dose, however, yielded only a non-significant 8% reduction in relative incidence of positive PCR tests.
Of the four recently published RCTs that studied IVM treatment of COVID-19, Chaccour et al., as previously released in preprint, monitored outcomes for 40 generally young patients with mild COVID-19 symptoms.14 A single dose of IVM at 400 μg/kg significantly reduced the duration of hyposmia/anosmia (p<0.001), but gave only a modest reduction in viral load. Shahbaznejad et al. reported that IVM in a single dose of 200 μg/kg reduced duration of COVID-19 symptoms and hospitalization (p=0.02 for each).17 IVM also reduced duration of coughing (p=0.02) and of shortness of breath (p<0.05). No conclusions could be drawn regarding mortality, since only one patient died, within 24 hours of hospitalization in critical condition, a 78-year old woman in the treatment group with a history of diabetes and heart failure.
Mahmud et al. administered a single dose of IVM at 12 mg plus doxycycline at 100 mg twice daily for five days.18 The IVM treatment group had statistically significant clinical benefits v. controls by four different measures, p=0.001 to 0.003, and had a reduced percentage of positive PCR tests at 14 days with p=0.002. Okumus et al. administered IVM at 200 μg/kg for five consecutive days, in addition to the standard of care used for both the treatment and control groups, which included azithromycin.15 At the end of the five-day study follow-up period, spO2 was increased; CRP, ferritin and D-dimer blood levels were reduced; and percentage of PCR-negative tests were increased vs. controls, all to statistical significance (p=0.032, 0.02, 0.005, 0.03, and 0.01, respectively).
More pronounced reduction by single-agent IVM of COVID-19 morbidity v. infectivity
The findings of two of these five recently published RCTs, Chaccour et al.14 and Seet et al.,16 both fit a pattern established in a prior RCT3 and two animal studies10,11 of more pronounced alleviation by IVM as a single agent of COVID-19-related symptoms and morbidities than reductions in viral load. Indeed, one RCT of IVM at an unusually high dose, 3,000 μg/kg total over 5 consecutive days, yielded a statistically significant reduction in viral load in COVID-19 patients vs. controls only for the subgroup of treated patients (45%) in which the highest levels of plasma IVM levels were obtained.19
This disparity between reduction in morbidity vs. infectivity by IVM for COVID-19 may be explainable by the indicated clinically operative biological mechanism of IVM as reported in seven molecular modeling studies.20-26 Those studies found that IVM bound strongly to regions of SARS-CoV-2 viral spike protein, one subdomain of which (RBD) controls viral binding and replication via host cell ACE2 receptors, with another subdomain (NTD) governing viral attachments to sialic acid (SA) binding sites on blood, endothelial and other host cells.27 The latter such attachments of SARS-CoV-2 to SA binding sites on red blood cells (RBCs) are responsible for the clumping that is observed in vitro when virus is mixed with RBCs in this hemagglutinating virus. Whereas the common cold human betacoronavirus strains contain an enzyme, hemagglutinin esterase (HE), that releases viral-RBC clumps, the three virulent betacoronavirus strains—SARS-CoV-2, SARS-CoV, and MERS—lack HE.27 IVM, if it is found to bind to NTD sites on SARS-CoV-2 spike protein, might thus limit viral virulence by blocking such hemagglutinating bindings.
The biological mechanism of IVM that is operative clinically against COVID-19 remains to be confirmed, as do indications of its greater reduction of morbidity than of infectivity per the studies noted. The recent publication of the five RCTs noted in top tier scientific journals, however, positively confirms the major, statistically significant clinical benefits of IVM, as previously reported in several prior such RCTs, for COVID-19 treatment and prevention.
References
1. Hill A, Abdulamir A, Ahmed S, et al. Meta-analysis of randomized trials of ivermectin to treat SARS-CoV-2 infection. Research Square. 2021;doi:10.21203/rs.3.rs-148845/v1.
2. Babalola O, Bode C, Ajayi A, et al. Ivermectin shows clinical benefits in mild to moderate COVID19: A randomised controlled double blind dose response study in Lagos. medRxiv. 2021;doi:10.1101/2021.01.05.21249131.
3. Kirti R, Roy R, Pattadar C, et al. Ivermectin as a potential treatment for mild to moderate COVID-19 – A double blind randomized placebo-controlled trial. medRxiv. 2021;doi: 10.1101/2021.01.05.21249310.
5. Niaee MS, Gheibi H, Namdar P, et al. Ivermectin as an adjunct treatment for hospitalized adult COVID-19 patients; A randomized multi-center clinical trial. Research Square. 2020;doi:10.21203/rs.3.rs-109670/v1.
6. Hashim HA, Maulood MF, Rasheed AM, et al. Controlled randomized clinical trial on using Ivermectin with Doxycycline for treating COVID-19 patients in Baghdad, Iraq. medRxiv. 2020;doi:10.1101/2020.10.26.20219345.
7. Elgazzar A, Hany B, Abo Youssef S, et al. Efficacy and Safety of Ivermectin for Treatment and prophylaxis of COVID-19 Pandemic. Research Square. 2020;doi:10.21203/rs.3.rs-100956/v1.
8. Podder CS, Chowdhury N, Sina MI, et al. Outcome of ivermectin treated mild to moderate COVID-19 cases; a single-centre, open-label, randomised controlled study. IMC J Med Sci. 2020;14(2):002.
10. Melo GD, Lazarini F, Larrous F, et al. Anti-COVID-19 efficacy of ivermectin in the golden hamster. bioRxiv. 2020;doi:10.1101/2020.11.21.392639.
11. Arévalo AP, Pagotto R, Pórfido JL, et al. Ivermectin reduces in vivo coronavirus infection in a mouse experimental model. Scientific Reports. 2021;11(1):7132.
14. Chaccour C, Casellas A, Blanco-Di Matteo A, et al. The effect of early treatment with ivermectin on viral load, symptoms and humoral response in patients with non-severe COVID-19: A pilot, double-blind, placebo-controlled, randomized clinical trial. EClinicalMedicine. 2021;10.1016/j.eclinm.2020.100720.
15. Okumuş N, Demirtürk N, Çetinkaya RA, et al. Evaluation of the effectiveness and safety of adding ivermectin to treatment in severe COVID-19 patients. BMC Infectious Diseases. 2021;21(1):411.
16. Seet RCS, Quek AML, Ooi DSQ, et al. Positive impact of oral hydroxychloroquine and povidone-iodine throat spray for COVID-19 prophylaxis: An open-label randomized trial. International Journal of Infectious Diseases. 2021;106:314-322.
17. Shahbaznejad L, Davoudi A, Eslami G, et al. Effect of ivermectin on COVID-19: A multicenter double-blind randomized controlled clinical trial. Clinical Therapeutics. 2021;https://doi.org/10.1016/j.clinthera.2021.04.007.
18. Mahmud R, Rahman MM, Alam I, et al. Ivermectin in combination with doxycycline for treating COVID-19 symptoms: a randomized trial. Journal of International Medical Research. 2021;49(5):03000605211013550.
19. Krolewiecki A, Lifschitz A, Moragas M, et al. Antiviral effect of high-dose ivermectin in adults with COVID-19: a pilot randomised, controlled, open label, multicentre trial. SSRN. http://ssrn.com/abstract=3714649. Published 2020. Accessed November 23, 2020.
20. Dayer M. Coronavirus (2019-nCoV) Deactivation via Spike Glycoprotein Shielding by Old Drugs, Bioinformatic Study. Preprints.org. 2020;doi:10.20944/preprints202005.0020.v1.
21. Hussien MA, Abdelaziz AEM. Molecular docking suggests repurposing of brincidofovir as a potential drug targeting SARS-CoV-2 ACE2 receptor and main protease. Network Modeling Analysis in Health Informatics and Bioinformatics. 2020;9(1):56.
22. Suravajhala R, Parashar A, Malik B, et al. Comparative Docking Studies on Curcumin with COVID-19 Proteins. Preprints.org. 2020;doi:10.20944/preprints202005.0439.v2.
23. Nallusamy S, Mannu J, Ravikumar C, et al. Shortlisting Phytochemicals Exhibiting Inhibitory Activity against Major Proteins of SARS-CoV-2 through Virtual Screening. Research Square. 2020;doi:10.21203/rs.3.rs-31834/v1.
24. Kalhor H, Sadeghi S, Abolhasani H, et al. Repurposing of the approved small molecule drugs in order to inhibit SARS-CoV-2 S protein and human ACE2 interaction through virtual screening approaches. Journal of Biomolecular Structure and Dynamics. 2020;10.1080/07391102.2020.1824816:1-16.
25. Agrawal L, Poullikkas T, Eisenhower S, et al. Viroinformatics-Based Analysis of SARS-CoV-2 Core Proteins for Potential Therapeutic Targets. Antibodies (Basel). 2021;10(1).
26. Toor HG, Banerjee DI, Lipsa Rath S, et al. Computational drug re-purposing targeting the spike glycoprotein of SARS-CoV-2 as an effective strategy to neutralize COVID-19. Eur J Pharmacol. 2021;890:173720.
27. Scheim DE. From cold to killer: How SARS-CoV-2 evolved without hemagglutinin esterase to agglutinate, then clot blood cells in pulmonary and systemic microvasculature. http://ssrn.com/abstract=3706347. Published 2020. Accessed March 30, 2021.
By B. J. Sabri | American Herald Tribune | April 19, 2016
Since the Korean War, but particularly since the Iranian Revolution of 1979 until today, the United States has been steadily escalating its military presence in the Persian Gulf. Taking advantage of many colossal events of the past 36 years, [1] the hyper-empire has institutionalized its massive presence on land and sea, and expanded its objectives to include the unambiguous physical control of the area, as well as the clear understanding that local Arab governments should abide by them. The pretext is always the same: in “defense” of the national interests and security of the United States. From observing how the United States has been interacting with the governments of the region, and by judging from the size of its expeditionary force, we could reach a basic conclusion. The United States is occupying, de facto, the entire Arabian Peninsula. (Yemen, devastated by Saudi and American jets is yet to be conquered. Oman? Britain returned not as colonial ruler but as a soft occupying power.)
Under this articulation, Saudi Arabia, Qatar, Kuwait, and the United Arab Emirates are virtually occupied countries. If we compare this type of occupation to the mandate and protectorate regimes of the past, the results might be identical—the nations affected by it lose sovereignty. When Arab governments comply with the objectives of a foreign power that station military forces on their national milieu, then that power controls them in multiple ways including how they react to policy deliberations and what decisions they intend to take on specific issues. A good method to verify the concept of effective occupation is this: take notice of what the United States says and wants, and then compare it to what the gulf rulers do in response. (I shall discuss this detail at some point in the upcoming parts.)
If the presence of US forces or other means of political pressure are a factor in Saudi Arabia’s interventionist Arab wars, then we need to debate this issue. However, from the history of resistance to colonialism, we learnt: if a powerful state imposes its order on a nation by military means or other forms of coercion, and if this nation does not resist that imposition, then a mental subordination to the powerful state will ensue. This is especially true in the case of Saudi Arabia. One single event, 9/11, has transformed it from a US “ally” into an instant political hostage of the American Empire. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.


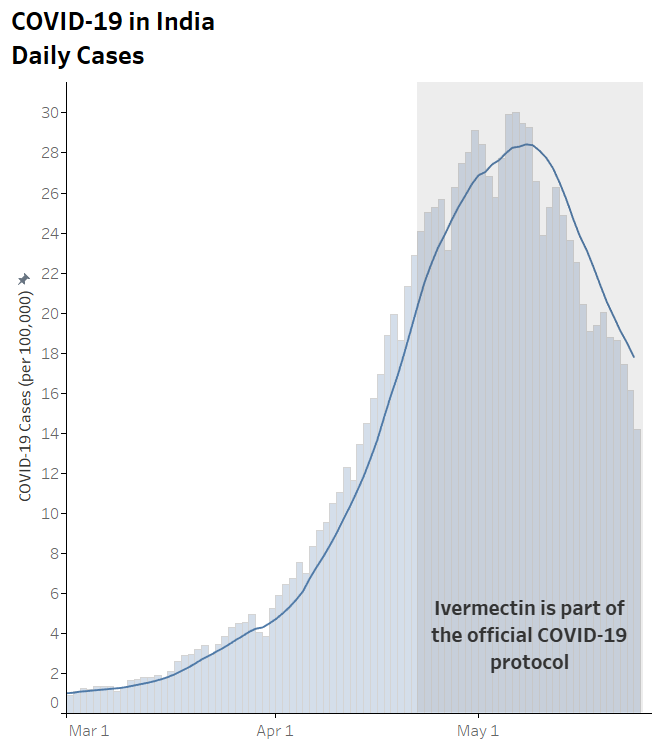








 Aletho News
Aletho News