When it comes to COVID, public health officials have consistently downplayed and/or ignored natural immunity.
Yet these public health experts and many doctors and scientists know that no vaccine can confer the type of robust, full, sterilizing and life-long immunity to COVID that natural-exposure immunity confers.
Officials at the Centers for Disease Control and Prevention (CDC) and National Institutes of Health (NIH) know anyone exposed, infected and recovered from SARS-CoV-2 has acquired cellular immunity.
They know how natural immunity works, yet they continue to deceive the public on this issue by falsely insisting vaccines are the only answer to “ending the pandemic.”
The authors of a 2008 study on the 1918 pandemic virus showed how potent and long-lived natural immunity is, and how the immune system generates new antibodies if and when needed (re-exposed).
The researchers wrote:
“A study of the blood of older people who survived the 1918 influenza pandemic reveals that antibodies to the strain have lasted a lifetime and can perhaps be engineered to protect future generations against similar strains … the group collected blood samples from 32 pandemic survivors aged 91 to 101 … the people recruited for the study were 2 to 12 years old in 1918 and many recalled sick family members in their households, which suggests they were directly exposed to the virus … The group found that 100% of the subjects had serum-neutralizing activity against the 1918 virus and 94% showed serologic reactivity to the 1918 hemagglutinin.
“The investigators generated B lymphoblastic cell lines from the peripheral blood mononuclear cells of eight subjects. Transformed cells from the blood of 7 of the 8 donors yielded secreting antibodies that bound the 1918 hemagglutinin.
“ … here we show that of the 32 individuals tested that were born in or before 1915, each showed sero-reactivity with the 1918 virus, nearly 90 years after the pandemic. Seven of the eight donor samples tested had circulating B cells that secreted antibodies that bound the 1918 HA. We isolated B cells from subjects and generated five monoclonal antibodies that showed potent neutralizing activity against 1918 virus from three separate donors. These antibodies also cross-reacted with the genetically similar HA of a 1930 swine H1N1 influenza strain.”
The very same CDC that fights against COVID natural immunity, argues just the opposite when it comes to chickenpox.
Guidance on the CDC website, “Chickenpox Vaccination: What Everyone Should Know,” states: “People 13 years of age and older who have never had chickenpox or received chickenpox vaccine should get two doses, at least 28 days apart.”
In this reasonable guidance, the CDC says you need the chickenpox jab if you “have never had chickenpox.” If you have had it, then you do not need the vaccine.
The CDC goes even further, stating: “You do not need to get the chickenpox vaccine if you have evidence of immunity against the disease.” So if someone has had chickenpox and recovered, and can demonstrate that via a laboratory test, they don’t need the vaccine.
Again, this makes sense. All parents know this, and have for generations. You do not need a vaccine for measles, if you already had measles and cleared the rash and recovered. Natural, beautiful robust immunity, typically lasts for the rest of a person’s life.
The same goes for the CDC’s guidance for the measles, mumps, and rubella vaccine (MMR). The CDC clearly states no MMR vaccine is needed if “You have laboratory confirmation of past infection or had blood tests that show you are immune to measles, mumps, and rubella.”
So, what is different for COVID-19? Is something other than science at play here?
We now have a major crisis as the race is on to vaccinate our 5- to 11-year-old children who bring no risk to the table, with a vaccine that has been shown to be sub-optimal and carrying risks.
We even have one of the FDA advisory committee members, Dr. Eric Rubin, who is also lead editor of the New England Journal of Medicine, stating: “We’re never gonna learn about how safe the vaccine is until we start giving it.”
This is a shocking statement by someone who played a role in the decision-making, and should lead us to examine if Rubin and others on that committee were conflicted in terms of relationships to the vaccine developers.
Rubin further stated: “The data show that the vaccine works and it’s pretty safe … we’re worried about a side effect that we can’t measure yet,” he said, referring to a heart condition called myocarditis.
So then why would Rubin and others agree to expose our children to potential harm from a vaccine for an illness that poses little risk to children, if they have serious concerns and admit they have not and cannot yet measure the safety?
This depth of uncertainty should never exist in any drug or vaccine that the FDA regulates, much less a drug officials propose to administer to 28 million children. Something is very wrong here.
An April 2021 study in the Journal of Infection (April 2021) examined household transmission rates in children and adults. The authors reported there was “no transmission from an index-person < 18 years (child) to a household contact < 18 years (child) (0/7), but 26 transmissions from adult index-cases to household contacts < 18 years (child) (26/71, SAR 0=37).”
These findings add to the stable existing evidence that children are not spreading the virus to children but rather that adults are spreading it to children.
Why vaccinate our children for this mild and typically non-consequential virus when they bring protective innate immunity towards this SARS-VoV-2, other coronaviruses and other respiratory viruses?
Why push to vaccinate our children who may well be immune due to prior exposure (asymptomatic or mild illness) and cross-reactivity/cross-protection? Why not consider assessing their immune status?
Dr. Geert Vanden Bossche writes that children’s innate immunity:
“… normally/ naturally largely protects them and provides a kind of herd immunity in that it dilutes infectious CoV pressure at the level of the population, whereas mass vaccination turns them into shedders of more infectious variants. Children/ youngsters who get the disease mostly develop mild to moderate disease and as a result continue to contribute to herd immunity by developing broad and long-lived immunity.”
Here are six studies that make the case for not vaccinating children:
1. A 2020 Yale University report indicates children and adults display very diverse and different immune system responses to SARS-CoV-2 infection which explains why they have far less illness or mortality from COVID.
According to the study:
“Since the earliest days of the COVID-19 outbreak, scientists have observed that children infected with the virus tend to fare much better than adults … researchers reported that levels of two immune system molecules — interleukin 17A (IL-17A), which helps mobilize immune system response during early infection, and interferon gamma (INF-g), which combats viral replication — were strongly linked to the age of the patients. The younger the patient, the higher the levels of IL-17A and INF-g, the analysis showed… these two molecules are part of the innate immune system, a more primitive, non-specific type of response activated early after infection.”
2. Studies by Ankit B. Patel and Dr. Supinda Bunyavanich show the virus uses the ACE 2 receptor to gain entry to the host cell, and the ACE 2 receptor has limited (less) expression and presence in the nasal epithelium in young children (potentially in upper respiratory airways).
This partly explains why children are less likely to be infected in the first place, or spread it to other children or adults, or even get severely ill. The biological molecular apparatus is simply not there in the nasopharynx of children. By bypassing this natural protection (limited nasal ACE 2 receptors in young children) and entering the shoulder deltoid, this could release vaccine, its mRNA and LNP content (e.g. PEG), and generated spike into the circulation that could then damage the endothelial lining of the blood vessels (vasculature) and cause severe allergic reactions (e.g., here, here, here, here, here).
3. William Briggs reported on the n=542 children who died (0-17 years (crude rate of 0.00007 per 100 and under 1 year old n=132, CDC data) since January 2020 with a diagnosis of COVID linked to their death. This does not indicate whether, as Johns Hopkins’ Dr. Marty Makaryhas been clamoring, the death was “causal or incidental.” That said, from January 2020, 1,043 children 0-17 have died of pneumonia.
Briggs reported:
“There is no good vaccine for pneumonia. But it could be avoided by keeping kids socially distanced from each other — permanently. If one death is “too many,” then you must not allow kids to be within contact of any human being who has a disease that may be passed to them, from which they may acquire pneumonia. They must also not be allowed in any car … in one year, just about 3,091 kids 0-17 died in car crashes (435 from 0-4, 847 from 5-14, and 30% of 6,031 from 15-24). Multiply these 3,000 deaths in cars by about 1.75, since the COVID deaths are over a 21-month period. That makes about 5,250 kids dying in car crashes in the same period — 10 times as many as Covid.”
Briggs concluded: “there exists no justification based on any available evidence for mandatory vaccines for kids.”
4. Weisberg and Farber et al. suggest (and building on research work by Kumar and Faber) that the reason children can more easily neutralize the virus is that their T cells are relatively naïve. They argue that since children’s T cells are mostly untrained, they can thus immunologically respond (optimally differentiate) more rapidly and nimbly to novel viruses such as SARS-CoV-2 for an effective robust response.
5. Research published in August 2021 by J. Loske deepens our understanding of this natural type biological/molecular protection even further by showing that “pre-activated (primed) antiviral innate immunity in the upper airways of children work to control early SARS-CoV-2 infection … the airway immune cells in children are primed for virus sensing…resulting in a stronger early innate antiviral response to SARS-CoV-2 infection than in adults.”
6. When one is vaccinated or becomes infected naturally, this drives the formation, tissue distribution and clonal evolution of B cells, which is key to encoding humoral immune memory.
Research published in May 2021 showed that blood examined from children retrieved prior to COVID-19 pandemic have memory B cells that can bind to SARS-CoV-2, suggestive of the potent role of early childhood exposure to common cold coronaviruses (coronaviruses). This is supported by Mateus et al. who reported on T cell memory to prior coronaviruses that cause the common cold (cross-reactivity/cross-protection).
There is no data or evidence or science to justify any of the COVID-19 injections in children. Can the content of these vaccines cross the blood-brain barrier in children? We don’t know because it wasn’t studied.
There is no proper safety data. The focus rather has to be on early treatment and testing (sero antibody or T-cell) to establish who is a credible candidate for these injections, as it is dangerous to layer inoculation on top of existing COVID-recovered, naturally acquired immunity.
There is no benefit and only potential harm/adverse effects (here, here, here).
Dr. Alexander is considered a global expert on COVID-19 generally and in some areas highly expertised. Dr. Alexander holds masters level study at York University Canada, a masters in epidemiology at University of Toronto, a masters in evidence-based medicine at Oxford and a doctorate in evidence-based medicine and research methods from McMaster University in Canada.
It sounds like a script in a science fiction movie, but it’s not: Emails obtained by The Intercept show that the National Institutes of Health worked together with one of its grantees, EcoHealth, to evade gain-of-function (GOF) research restrictions.
While EcoHealth’s plans for the research “triggered concerns at NIH,” staff went ahead and “adopted language that EcoHealth Alliance crafted” so the work could go on. The Intercept added that none of the featured experiments could have triggered the current pandemic, but the idea of the deceptive move shows what persons in a position of authority at the highest levels will do to circumvent safety rules and regulations.
The violations were serious enough to spark concerns from Jesse Bloom, a virologist at the Fred Hutchinson Cancer Research Center. “The discussions reveal that neither party is taking the risks sufficiently seriously,” Bloom told The Intercept.
Simon Wain-Hobson, a virologist at the Pasteur Institute in Paris, minced no words with his opinion on what happened. “It’s absolutely outrageous,” Wain-Hobson said. “The NIH is bending over backward to help people it’s funded. It isn’t clear that the NIH is protecting the U.S. taxpayer.”
Would the doctrine of the “Original Antigenic Sin” (OAS) play a heavy role in the existing COVID vaccine strategy — due to the sub-optimal, non-sterilizing, imperfect COVID-19 vaccine?
Experts agree we should never have tried to vaccinate our way out of a pandemic while in a pandemic.
According to the OAS by Dr. Thomas Francis, the initial priming of the immune system (initial exposure to the virus, either in the wild or via a vaccine) gets ‘fixed’ for life. If the initial priming of the immune system is sub-optimal and biased, then that sub-optimal initial priming can effectively derange and bias the immune response long-term, which would guide all future immunological responses.
We should have known that this initial priming, if deranged and wrong, would severely stagger and hobble our immune response for the rest of our lives.
And so, are we setting up our populations — and dangerously, our children — for disaster? With this imperfect and sub-optimal immune priming using COVID vaccines that do not stop infection or transmission in the first place?
The COVID-19 vaccines being administered in the U.S. only reduce symptoms, thus allowing the host to stay alive (an evolutionary future it did not have) while remaining capable of transmitting.
Evidence shows vaccinated persons are indeed susceptible to infection, and as alarmingly, carry as high a viral load as the unvaccinated.
Are we about to rob our children of their most precious gift — a robust, durable, potent natural innate immunity with these imperfect leaky vaccines — an immunity that has always protected them and helps reduce the infectious pressure and helps contribute to population herd immunity? With vaccines that have been shown to be harmful?
I argue we could potentially kill many children with these vaccines because we simply have not done the proper safety tests and studies for the proper duration of follow-up, so as to “exclude harms.”
If we have not conducted the proper studies, how could we justify the safety of these vaccines for our children? To do so is dangerous and reckless, as it deceives the public and parents. It is illogical and irresponsible, and without any credible basis.
We do not know what will happen to our healthy children long-term. This is potentially catastrophic if COVID mass vaccination is allowed in our children.
These public health officials at the U.S. Food and Drug Administration, Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH), National Institute of Allergy and Infectious Diseases (NIAID) — including Dr. Anthony Fauci and Dr. Rochelle Walensky — have made no valid case as to why our children warrant these vaccines.
Yet they are seeking to vaccinate healthy children with near statistical zero risk — with only the opportunity for harm and no opportunity for benefit.
In addition to the OAS, Read et al also provided us a roadmap to these vaccine and immune system challenges, in their treatise on Marek’s disease in chickens.
In their seminal 2015 PLOS paper, the authors argued some vaccines may boost and enhance the fitness of more virulent strains. They asked a simple question: Could some vaccines drive the evolution of more virulent pathogens?
We say “yes!” This can be explained by natural selection which selects out or culls pathogen strains/variants that are so lethal or “hot” they could kill their hosts if they survive and, thus, inadvertently, kill themselves.
Marek’s disease effect and vaccination may well be at play here with COVID vaccines — moderating symptoms while not stopping infection or transmission, thus posing a danger to the unvaccinated and vaccinated.
We — or at least the virologists and immunologists and vaccine developers — should also have understood the COVID vaccines would drive antibodies against the spike glycoprotein only, while our natural-exposure infection immune response will be broad, robust, durable, long-term — providing immunity against the spike (S) protein, the membrane protein, the nucleocapsid (N) protein, and all the epitopes on the viral ball and all conserved parts of the virus.
No COVID vaccine immunity could be equal to or better than naturally acquired immunity. This should have never even been in question. Assertions otherwise by the CDC, NIH, NIAID or vaccine developers are outright falsehoods and means to deceive the public.
We should have known we could never achieve “zero COVID” as this is a mutable respiratory pathogen. This means, similar to flu and cold viruses, COVID mutates often.
This is what viruses do. They exist to replicate, and the replicating process of their genetic material is unstable and imperfect. Because there are errors in the replication of the genetic material, there will always be mutations.
For example, the original SARS-CoV-2 was the Wuhan strain — now it is the Delta variant. The vaccine for the original strain cannot hit the mutated spike, as the mutations occur on the spike. That’s why we have the immune escape.
So no matter what vaccine you make, you will not be able to vaccinate for the right strain or variant at any time, as the virus would have mutated by the time we vaccinate.
You can never get ahead of a mutating virus with a vaccine.
This is especially true given COVID has an animal reservoir. The virus lives stably in the bat population. Unless we kill off all the bats — and their intermediate hosts, which include civet cats and raccoon dogs and camels — we will always have a “reservoir” for the virus, in animals. Infected animals can in turn infect humans who get close to or interact with them.
This is a very different pathogen and approach than the one taken with smallpox, which did not have an animal reservoir — we only had to remove smallpox from the human population, we didn’t need to worry about it spilling over from other species.
According to Dr. Robert Malone, “The idea that if you have a workplace where everybody’s vaccinated, you’re not going to have virus spread is totally false … a total lie … the vaccinated are actually the “super-spreaders” that everyone was told about in the beginning of the pandemic.”
Malone further states, “if the government isn’t going to disclose what the [vaccine] risks are, and they’re not going to disclose what’s really going on because they think that you can’t handle the news … this is called the noble lie.”
Are we closer to understanding now that vaccinating for COVID under tremendous infectious and vaccine pressure (and ecological pressure) would drive immune escape? That this strategy is indeed a recipe for disaster?
Could COVID-19 vaccines be enhancing the evolution of variants/mutants that are more infectious and capable of spreading much faster and with greater lethality?
Are these COVID-19 vaccines sub-optimally priming the immune system for long-term skewed deranged responding?
Could the use of ‘imperfect’ sub-optimal vaccines enhance the progression of variants that place unvaccinated persons at elevated evolutionary risk of very severe illness, including death? Our children? Is this Marek 2.0?
Where are the safeguards when the proper studies were not done by the vaccine developers, and where is the FDA as the top regulator, in protecting the health and well-being of our children?
Dr. Janet Woodcock, as the head of the FDA, where are you in this? You could not be informed by the science, for there is none to support this grossly reckless and absurd push to vaccinate children.
What is going on here? This certainly is not “about the science.”
I challenge any public health official to sit down with me and my scientific colleagues and explain your science. Debate us. Show us what you are looking at to arrive at these very dangerous statements and decisions.
We may end up killing many children with these vaccines. In fact, not ‘we’, ‘you’ — Fauci and Walensky and Dr. Francis Collins — may end up killing many of our children.
Please stop this insanity, step back and focus on the vulnerable and elderly where there is risk. Leave the children alone!
“If the CDC, NIH, FDA (Walensky, Fauci, Collins, Marks, Woodcock), vaccine developers and all involved in these COVID vaccines, all the television medical experts, all who are absolved thanks to liability protection, if you feel so strongly that these are safe for our children, then do the right thing: Take liability protection off the table. Stand by the vaccine’s safety. Put some skin in the game — for as we speak, only our healthy children are carrying risk and I fear it could be potentially catastrophic for them.
Dr. Alexander is considered a global expert on COVID-19 generally and in some areas highly expertised. Dr. Alexander holds masters level study at York University Canada, a masters in epidemiology at University of Toronto, a masters in evidence-based medicine at Oxford and a doctorate in evidence-based medicine and research methods from McMaster University in Canada.
Sometimes it pays to step back in history to understand exactly how something monumental was created. This is the story of how one Big Lie turned our world upside down and ruined the lives of millions of people.
Hard to believe that one Big Lie could have created all the pandemic controls, especially lockdowns, school closings and quarantines, that devastated our lives, our economy and our society. But it happened.
A very powerful, influential person told the world in early 2020 that the new China virus that leads to COVID-19 infection was especially lethal. It quickly pushed a fast, enormous response to protect public health. Was the truth was being told? It was not. There was an exaggeration of the new virus lethality for the entire population.
In truth, it was only severe for the oldest age category. Helped by corrupt data from CDC, overstatement of COVID lethality continues today to maintain public fear.
But first it is important to discuss the meaning of critically important terms. What the Big Lie was all about had to do with the fatality or death rate of what early in 2020 was seen as an invading new virus coming from China. How should we think about the fatality rate of a virus?
Terminology
One simple and correct way is how many people die from the infection caused by the virus: the Infection Fatality Rate (IFR). But another possible way would be to invoke the Case Fatality Rate (CFR); the fraction of documented cases of people with the virus that resulted in death.
How can you know how many people are infected? A lot of testing would be necessary. For our COVID pandemic there has been, surprisingly, very little wide blood testing across the whole population. Many people with infections have no symptoms or just mild ones and do not seek testing or medical attention. The CDC has done a terrible job of getting good data on infection numbers.
As to cases ascribed to COVID, there are reasons why that number surely underestimates how many people are really infected. Why? Because only some people, usually with symptoms, get tested and if found positive become a case. On the other side, the PCR test method most widely used has often been implemented in a way to get false positive results.
Mainly because the number of cycles the test is run is far too high (above 25) and picks up fragments of the virus (or any coronavirus) that does not document real COVID infection. Thus, the CFR is not a reliable or accurate measure of the real death rate despite widely published case numbers.
Key Moment In History
During a March 11, 2020 hearing of the House Oversight and Reform Committee on coronavirus preparedness, Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Disease, put it plainly: “The seasonal flu that we deal with every year has a mortality of 0.1 percent,” he told the congressional panel, whereas coronavirus is “10 times more lethal than the seasonal flu,” per STAT news. [0.1 percent also expressed as .001]
He also said: “The bottom line: It is going to get worse.” And this: “The stated mortality, overall, of [the coronavirus], when you look at all the data including China, is about 3 percent.”
That figure of 3 percent, far from reliable, is 30 times greater than the figure given for the seasonal flu. Fauci exaggerated to create a crisis. Simply by implying great lethality for everyone infected by the new COVID virus.
And it should be noted that CDC has found the flu IFR ranged from 0.1 percent (the figure cited by Fauci) to 0.17 percent [.0017] from 2014 to 2019, because seasonal deaths vary significantly.
What Fauci said put the country, with the help of big media, into convulsions. It created the foundation for authoritarian contagion controls driving a spike into the lives of Americans. Fauci intentionally created the pandemic by creating fear.
New York City Analysis
An interesting analysis was made for IFR for New York City at the height of the pandemic in May 2020. It illustrates how both death and infection data can be fine-tuned to get an IFR. As to deaths, blood testing found that 19.9 percent of people had antibodies indicating infection, yielding a number of 1,671,351 infected. As to deaths from COVID, there were three components: 13,156 confirmed, 5,126 probable, and 5,148 excess for a total of 23,430, that may have overstated deaths.
Probable meant likely COVID death but not confirmed through testing. Excess meant the number above expected seasonal baseline level. Using the total deaths divided by total infected produces an IFR of .014. Higher than the usual quoted flu value [.001] for the height of the pandemic in high density New York City.
And without consideration of variations among most vulnerable groups. A high rate of fatality for elderly people would cause a deceptive high value for IFR for the entire population.
Deaths certainly have declined significantly in the past year and more (even as high transmissivity delta variant has probably maintained high levels of infections). Why? Because of far better actions in hospitals and because infected people have surely learned a lot about home treatments to catch COVID infection early after initial symptoms and possibly a positive test. Cutting the deaths in half for the same number of infected people results in an IFR of .007, probably a more realistic figure for today.
World Health Organization
At an October 2020 meeting of the World Health organization, Dr Michael Ryan, the Head of Emergencies revealed that they believe roughly 10 percent of the world has been infected with Sars-Cov-2. This is their “best estimate.” This figure was based on the average results of all the broad seroprevalence (blood) studies done around the world. The message was that the virus is nothing as deadly as everyone predicted.
At the time the global population was roughly 7.8 billion people, if 10 percent have been infected that is 780 million infections. The global death toll then attributed to Sars-Cov-2 infections was seen as 1,061,539. That’s an infection fatality rate of roughly or 0.14 percent [.0014]. Consistent with seasonal flu and the predictions of many experts from around the world. And inconsistent with the dire picture given by Fauci.
Great Analysis
Now consider the detailed analysis “Public Health Lessons Learned From Biases in Coronavirus Mortality Overestimation” by Ronold B. Brown published in August 2020. He has doctoral degrees in public health and organizational behavior.
Here are highlights from this article that focused on what Fauci said.
“The validity of this estimation could benefit from vetting for biases and miscalculations. The main objective of this article is to critically appraise the coronavirus mortality estimation presented to Congress.”
[What Fauci said] “helped launch a campaign of social distancing, organizational and business lockdowns, and shelter-in-place orders.”
“Previous to the Congressional hearing, a less severe estimation of coronavirus mortality appeared in a February 28, 2020 editorial released by NIAID [Fauci’s department] and the Centers for Disease Control and Prevention (CDC). Published online in the New England Journal of Medicine (NEJM.org), the editorial stated: ‘…the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1 percent).’
Almost as a parenthetical afterthought, the NEJM editorial inaccurately stated that 0.1 percent is the approximate case fatality rate of seasonal influenza. By contrast, the World Health Organization (WHO) reported that 0.1 percent or lower is the approximate influenza infection fatality rate, not the case fatality rate.“
Brown correctly hit the key semantic issue: CFR versus IFR.
“IFRs are estimated following an outbreak, often based on representative samples of blood tests of the immune system in individuals exposed to a virus. Estimation of the IFR in COVID-19 is urgently needed to assess the scale of the coronavirus pandemic.“ [Now, over a year later this has not happened.]
Brown correctly emphasized “it is imperative to not confuse fatality rates [CFR and IFR] with one another; else misleading calculations with significant consequences could result.” [That is exactly what Fauci engineered.]
Brown said the 1 percent figure in the testimony was consistent with the “coronavirus CFR of 1.8-3.4 percent (median, 2.6 percent) reported by the CDC.” [As I write this data in The Washington Post shows a CFR of 1.6 percent. This substantiates that the health care system has made progress in curbing COVID deaths. But this current CFR is still 16 times higher than the IFR figure for the seasonal flu. IFR remains the issue.]
Now Brown gets to the heart of the problem: “A comparison of coronavirus and seasonal influenza CFRs may have been intended during Congressional testimony, but due to misclassifying an IFR as a CFR, the comparison turned out to be between an adjusted coronavirus CFR of 1 percent and an influenza IFR of 0.1 percent.”
[Did Fauci, the widely lauded expert, not know what he was doing? Hard to believe this. If he knew, then we have the explanation for the Big Lie.]
By May 2020 “it was clear that the coronavirus mortality total for the season would be nowhere near 800,000 deaths inferred from the 10-fold mortality overestimation reported to Congress [emphasis added].
Even after adjusting for the effect of successful mitigation measures that may have slowed down the rate of coronavirus transmission, it seems unlikely that so many deaths were completely eliminated by a nonpharmaceutical intervention such as social distancing, which was only intended to contain infection transmission, not suppress infections and related fatalities.”
As to getting good data to determine IFR, Brown noted: “A revised version of a non–peer-reviewed study on COVID-19 antibody seroprevalence in Santa Clara County, California, found that infections were many times more prevalent than confirmed cases.
As more serosurveys are conducted throughout the country, a nationally coordinated COVID-19 serosurvey of a representative sample of the population is urgently needed, which can determine if the national IFR is low enough to expedite an across-the-board end to restrictive mitigating measures.”
[In other words, with systematic blood testing, if we have an IFR for COVID similar to the IFR for the seasonal flu, then the many disruptive and costly actions by the public health establishment are not justified. And they never were! ]
Another Analysis
The title of this September 2020 article by Len Cabrera is “Mistake or Manipulation.” An initial point made was: “A review of the early events mentioned in Dr. Brown’s paper and the lack of any corrections to the record suggest that the misstatement [by Fauci] before Congress was not a mistake.” If not a mistake, then it was intentional.
This point was dead on: “In his testimony, Dr. Fauci claimed the mortality of flu was 0.1 percent and that the case fatality rate of COVID was 3 percent but could be as low as 1 percent with asymptomatic cases. This is an apples-to-oranges comparison of the flu’s infection fatality rate (IFR) to COVID-19’s case fatality rate (CFR).”
And this critical point was made: “All cases are infections, but not all infections are confirmed cases, so the number of infections always exceeds the number of cases, making IFR less than CFR.” In other words, if the number of deaths is the same, then a lower denominator for calculating CFR compared to that for getting the IFR results in a higher number for CFR.
Are we to believe that the esteemed Fauci did not know this? Or is it reasonable to conclude that Fauci knew exactly what he was doing, namely using some simple data to create a pandemic crisis that required massive authoritarian government actions? Fauci set the stage for his wait-for-the-vaccine pandemic strategy that he sold to President Trump.
This required that the government establish blocks to wide use of the safe, cheap, effective and FDA approved generic medicines already found to cure COVID in early 2020, namely ivermectin and hydroxychloroquine. Details about these early treatment protocols are given in Pandemic Blunder.
Here is another point made: “A careful viewing of the testimony suggests the line [COVID being 10 times worse than flu] was not a mistake.
Dr. Fauci was specifically asked if COVID was less lethal than H1N1 or SARS. Rather than refer to his own NEJM article saying SARS had a case fatality rate of 9-10 percent (3 to 10 times worse than COVID), Dr. Fauci said, “Absolutely not… the 2009 pandemic of H1N1 was even less lethal than regular flu… this is a really serious problem that we have to take seriously.”
He repeated that COVID’s “mortality is 10 times that [of influenza]” and concluded with, “We have to stay ahead of the game in preventing this.”
This also was a prescient view: ”This was a perfect series of switches: IFR to CFR, voluntary isolation for the sick to mandatory isolation for everyone, two weeks to flatten the curve to indefinite lockdown until there’s a vaccine. (If you think it will be voluntary, you’re not paying attention.)”
Add this to the quest for truth: “A study in France looked at all-cause mortality data from 1946 to 2020 and concluded that ‘SARS-CoV-2 is not an unusually virulent viral respiratory disease pathogen” because there is no significant increase in mortality. Of the deaths in 2020, the study said, ‘unprecedented strict mass quarantine and isolation of both sick and healthy elderly people, together and separately, killed many of them.’”
Here is the article’s correct conclusion: “Sadly, many politicians were duped and went along with the recommendations for lockdowns and masks that followed from Dr. Fauci’s 10-times-deadlier testimony. Don’t expect them to admit their mistakes, either. Perhaps the only thing harder for a politician than telling the whole truth is admitting a mistake.”
What Is The Truth?
If you listen to many experts, you hear this truth based on CDC data: 99.8 or 99.9 percent of people across all ages who get infected by COVID do not die. That means that the IFR overall is .001 or .002. In other words, not so terribly worse than the flu IFR, but it does vary with age.
In September 2020 these CDC age related data were reported:
Updated survival rates and IFR by age group:
0-19: 99.997 percent, IFR .003 percent
20-49: 99.98 percent, IFR .02 percent
50-69: 99.5 percent, IFR .5 percent
70+: 94.6 percent, IFR 5.4 percent
Note that through age 49 the IFR is less than the average for flu of 0.1 percent, but higher for older people. And only for the 70+ group is the IFR more than 10 times greater. In other words, only for the oldest group is what Fauci said in his congressional testimony accurate. What if Fauci had said something in tune with that reality? The vaccine program he pushed should have focused on the elderly, not the entire population.
From the important recent report “COVD-19: Restoring Public Trust During A Global Health Crisis” are age data and COVID CFR [through Feb. 16, 2021]. Note these are Case Facility Rate data, meaning that the figures are very exaggerated because the number of infected are very much higher than the number of cases: probably 100 million more infections than cases. Thus, the total across all age groups of 1.701 percent, [.01701] should be corrected to .289 percent [.00289]; this is about three times higher than the cited flu IFR, not the 10 times higher given by Fauci. And it would be much lower for the less than 70 population.
A very recent article said this: “While estimates of COVID-19’s infection fatality rate (IFR) range from study to study, the expert consensus does indeed place the death rate at below 1 percent for most age groups.” Fauci did indeed overhype COVID for all but the very elderly. This supports the view of the eminent Dr. Peter McCollough that a wise COVID vaccine strategy would have been to target the elderly, not the entire population.
The widely acclaimed medical researcher John P. Ioannidis of Stanford University has examined IFR for COVID in considerable detail,
In October 2020 he said this: “The infection fatality rate of COVID-19 can vary substantially across different locations and this may reflect differences in population age structure and case-mix of infected and deceased patients and other factors. The inferred infection fatality rates tended to be much lower than estimates made earlier in the pandemic.”
At that time, he said:” Across 51 locations, the median COVID-19 infection fatality rate was 0.27 percent (corrected 0.23 percent).” Higher than the Fauci quoted value for the flu (0.1 percent), but not 10 times greater.
A new report from the defense department gives data on 5.6 million fully vaccinated Medicare participants age 65 and older. There were 161,000 recent breakthrough COVID infections and the IFR was 0.021. It noted an IFR for this group of0 .12 (about five times greater) during the March to December 2020 period when there was far less effective hospital care and no mass vaccination.
Both IFRs for elderly Americans are greater than the quoted typical flu value, but far from a very lethal viral infection.
Recently, it was reported that according to CDC work “More than 39 million Americans have been diagnosed with coronavirus infection since the pandemic started in 2020.” Using that figure, that may be too low because only 1.4 million blood samples were tested, together with the current CDC value of about 700,000 COVID fatalities results in an average IFR of 0.018.
Why is 39 million infected people low? Because many medical experts have said that there are probably some 100 million Americans with natural immunity resulting from COVID infection.
The key word to question in what CDC did is “diagnosed.” In other words, people who were tested and found positive. But clearly a large fraction of asymptomatic and mildly symptomatic people did not get tested. So, what if you add 100 million to the 39 million figure and then use that as the denominator, with 700,000 deaths in the numerator, and calculate the IFR?
You get an IFR of 0.005. Not ten times higher than the flu value cited by Fauci in his congressional testimony [actually 3 times higher than the high end of flu IFR values].
Podcaster Jack Murphy, who founded Liminal Order, deduced that because the CDC said there were twice as many people who were infected with COVID, then it automatically meant that the lethality rate must be cut in half, commenting that the virus that had killed 646,000 Americans in the last 19 months is “far less lethal than already known.”
Murder Motivation
To accept the entire argument for a Big Lie it is necessary to explain the motivation for Fauci to intentionally tell the public that the new China virus was extremely lethal. So much worse than seasonal flu. So awful that extreme government action was needed.
It is relevant to note that in January 2017 Fauci warned the Trump administration, in a public talk, that no doubt there would be a “surprise outbreak” of a new infectious disease pandemic. “The thing we’re extraordinarily confident about is that we’re going to see this in the next few years,” he said. He got what he wanted.
Maybe all the talk about a “plandemic” was spot on. And maybe Fauci had insights because he was funding the work at the Wuhan Laboratory to develop extremely toxic viruses.
What Fauci said about high lethality set in motion an onerous set of government actions justified on the basis of protecting public health. Why would anyone want to overstate the lethality of the new COVID-19 virus? It was the only way to use onerous pandemic control and management methods that Fauci favored. It was necessary to set in motion a COVID vaccine program. Most of all, his strategy was used to create very high levels of FEAR in the public so that they would accept his favored government actions.
Understand this. Fauci is not a trained public health expert, nor a trained epidemiologist or virologist. He was a plain physician who over many decades as a top NIH bureaucrat accumulated enormous power. He never did what true public health experts have an ethical obligation to do. That is to tell the public both the positives and negatives of public health policies and actions.
The point is this: By pushing the need for pandemic actions to address a very lethal virus a host of government actions produced so much economic, social and personal hardships and dislocations. And many analyses have concluded that more Americans died from the government actions than from the COVID virus.
Perversely, pandemic public health actions actually harmed public health. But with widespread mainstream media support Fauci got away with everything.
Hundreds of thousands of Americans died unnecessarily. Fauci is guilty of criminally negligent homicide stemming from his initial and very public overstatement of the lethality of the COVID virus. Those who have screamed for his prosecution have a valid case.
With his power he created policies that created data to support this lethality claim. One big action was to create a testing protocol using the PCR technology in ways that created very high case levels. The inventor of that technology said it was inappropriate for diagnosing the viral infection. Millions of COVID cases resulted from running PCR equipment at very high cycle rates [high than 25]. Meanwhile the government never did widespread blood testing to get data for knowing the IFR.
The other major way to keep up public support for pandemic controls was to ensure high numbers of COVID deaths. This was done through directives on how death certificates should be filled out and through financial incentives for hospitals to certify deaths as COVID ones.
Recent analysis that in March 2020 CDC changed guidelines on how death certificates were to be filled out. Different than the procedure used for 17 years prior to this change.
This study found a COVID fatality figure of 161,392 with the new reporting versus 9,684 for the older procedure. There is little doubt that COVID death data, even accounting for some overcounting because of people dying not from any COVID influence, have been too high. This means that IFR data have been too high.
The combination of false high levels of cases and deaths helped maintain public fear of a very lethal virus. That is not correct for nearly all people younger than 70 years old.
Conclusions
To sum up: COVID was intentionally over hyped by Fauci as a very deadly disease to justify the most extreme public health actions. This was the Big Lie. Most valid data now show COVID lethality is similar to that for seasonal flu for the vast majority of people. But accepting that truth would not have justified the array of excessive government actions used for the false pandemic.
Yes, many people have died from COVID, but deaths have been overreported and infections underreported. And most deaths – at least 85% – could have been prevented by using generic medicines, such as ivermectin. There is no doubt that a great many people die with COVID but not FROM COVID, also arguing for a low IFR. At one point CDC said that only 6% of deaths resulted only from COVID, making the IFR much lower than the flu IFR.
Finally, recognizing the true lower IFR for COVID the whole rationale for mass vaccination collapses, especially in view of very high levels of adverse effects and deaths from the vaccines themselves.
Which makes perfect sense if you appreciate that the COVID IFR is now similar to the flu IFR for most people. Especially if you recognize that CDC has found the flu IFR ranged from 0.1 percent (the figure cited by Fauci) to 0.17 percent from 2014 to 2019.
Understanding that the lethality of COVID is far from the terrible picture painted by Fauci at the very beginning of the pandemic is key to weighing the risk/benefit ratio when deciding to get vaccinated. For most people the risk from the vaccine is greater than the benefit. Only the elderly have a good reason to get the shot.
Some 81 percent of COVID deaths are for people over 65. As has been pointed out by many people, the average age of most COVID deaths for elderly victims have been consistently higher than average life expectancy ages.
A new article has made important observations. The main one is that countries with low vaccination levels have been doing better than those with mass vaccination programs, like the US. The results are consistent with a widely accepted understanding that the vaccines do not effectively stem virus infection or transmission. More vaccination equated to more viral spreading.
The new study ended with advice to learn “to live with COVID-19 in the same manner we continue to live a 100 years later with various seasonal alterations of the 1918 Influenza virus.”
Dr. Joel S. Hirschhorn is the author of Pandemic Blunder and many articles on the pandemic, worked on health issues for decades. As a full professor at the University of Wisconsin, Madison, he directed a medical research program between the colleges of engineering and medicine. As a senior official at the Congressional Office of Technology Assessment and the National Governors Association, he directed major studies on health-related subjects; he testified at over 50 US Senate and House hearings and authored hundreds of articles and op-ed articles in major newspapers. He has served as an executive volunteer at a major hospital for more than 10 years. He is a member of the Association of American Physicians and Surgeons, and America’s Frontline Doctors.
Did you know that a cancer-causing monkey virus contaminated millions of batches of polio vaccine?
Did you know this virus has now been found inside people and inside their cancers?
The health authorities would like the American public to forget these facts. But it happened, and the repercussions are still with us today.
This known contamination took place at the end of the 1950s and the beginning of the 1960s, but may have continued for the next 40 years. In fact, over the last 60 years, cancer rates for every age group in America have continued to climb.
How did this vaccine contamination happen? And is there a link to the skyrocketing rates of cancer in the United States?
How were polio vaccines contaminated with cancer-causing monkey virus?
Salk’s strains would be inactivated with formaldehyde and injected into children. Sabin’s strains would be attenuated, or weakened, by transferring or passaging the live viruses through different host cells, and then fed to children orally.
Because his goal was to create a live attenuated vaccine, Sabin had to isolate the poliovirus strains and then passage the strains through various host cells in order to attain the right virulence — strong enough to illicit an immune response, but weak enough so as to not cause polio in the recipient.
Sabin’s oral polio vaccine (OPV) is a trivalent vaccine and was, therefore, comprised of three types – Type I, II, and III.
Here’s how Type I was created. In 1941, Drs. Thomas Francis and Thomas Mack isolated the Mahoney poliovirus “from the pooled feces of three healthy children in Cleveland.”
Then, to make his vaccine, Salk subjected the polio virus strain to passages through 14 living monkeys and two cultures of monkey testicular cultures. In 1954, the strain (now called Monk14 T2) was given to Drs. C.P. Li and M. Schaeffer, who subjected the virus to nine more passages through monkey testicular cultures.
Next, the strain (now called Monk14 T11) underwent 15 more passages in monkey testicular cultures, 18 passages in monkey kidney cells, two passages through the skin of living rhesus monkeys, and additional passages through African Green monkey skin and monkey kidney cell cultures.
This strain was now called MS10 T43 or LS-c.
In 1956, Sabin took this polio virus and passaged it through seven cultures of African Green Monkey kidney cells. That same year, the pharmaceutical company, Merck, Sharp & Dohme, passed the strain (now called LS-c, 2ab/KP2) through a rhesus monkey kidney cell culture.
The resulting material, called Sabin Original Merck (SOM), was provided to the pharmaceutical company Lederle in 1960, as the seed material to manufacture its polio vaccine.
Types II and III were created in a similar fashion.
Why was so much ‘passaging’ through animal cells necessary?
The theory of passaging is relatively simple. The idea is that as a virus becomes more adapted to a new animal species, that strain will become less adapted to its original host.
Putting the virus into various monkey tissues or cultures, including monkey kidneys, monkey testicles and monkey skin, was designed to adapt the polio virus to monkeys.
Once it was adapted to monkeys, so the theory goes, the polio virus would be less virulent for humans. While the idea made sense, what did not make sense were the risks of doing this.
Each time the polio virus was harvested from these monkey tissues and cultures, the scientists ran the risk of picking up extraneous monkey viruses mixed in with their polio virus.
This is, of course, what happened. In fact, since kidneys filter the blood and remove toxins, they are uniquely situated to be a potential source of viruses.
But the story gets even worse.
How was polio virus grown for vaccines?
Once their polio seeds were isolated, pharmaceutical companies needed a method to produce the vast quantities needed for nationwide immunization campaigns.
This required a medium or substrate upon which the poliovirus could be efficiently grown and harvested. Kidney cells from rhesus, and later African Green monkeys, were chosen because they were found to be an effective growth medium.
Monkeys were imported in large numbers from various countries. They were killed and their kidneys were removed. A small quantity of poliovirus would then be added to the minced kidneys, and within a few days, large quantities of poliovirus could then be harvested from these pulverized monkey kidneys cells.
There was a problem, however, with using monkey kidney cells to both create the original vaccine strains and grow the vaccine in large quantities: Monkeys are full of monkey viruses.
In fact, there were so many simian viruses identified in the polio vaccines that scientists started numbering them. Simian Virus 1, then 2, etc. Then they started abbreviating them: SV1, SV10, etc.
What is SV40?
SV40 was the 40th virus found in rhesus monkey kidney cells when these cells were used to make the polio vaccine. This particular virus contaminated both the Inactivated Polio Vaccine (IPV) created by Salk, and the oral or “live” Polio Vaccine (OPV) created by Sabin.
As discussed below, SV40 was determined to be oncogenic, or cancer-causing.
The SV40 genome encodes for various proteins, including “Large T-ag.” This protein stimulates host cells to enter the phase where the cell multiplies its genetic content prior to cell division. In addition, T-ag binds to various cellular tumor suppressor proteins.
In other words, SV40 helps stimulate human cells to multiply, and also stops the cellular machinery designed to stop cancer from starting. It’s a deadly “one-two punch.”
How was SV40 discovered in the polio vaccine? Dr. Bernice Eddy of the National Institutes of Health (NIH), Division of Biologics, discovered it when, in 1959, she took the material used to grow polio vaccines and injected it into hamsters.
Tumors grew in the hamsters, so Eddy wanted to isolate the causative agent — and it turned out to be SV40, the 40th simian virus contaminating the polio vaccines.
Her discovery was validated by Drs. Maurice Hilliman and Benjamin Sweet of Merck.
What did the scientists say?
Many scientists knew using monkey kidneys full of simian viruses was a dangerous way to make a vaccine.
As early as 1953, Dr. Herald R. Cox, a scientist working at Lederle Laboratories, one of the polio vaccine manufacturers, published an article in a peer-reviewed scientific journal in which he stated:
“[P]oliomyelitis virus has so far been cultivated only in the tissues of certain susceptible species — namely, monkey or human tissues. Here again we would always be confronted with the potential danger of picking up other contaminating viruses or other microbic agents infectious for man.”
In 1958, a scientific journal reported, “the rate of isolation of new simian viruses (from monkey kidney cells) has continued unabated.”
“Our scientific staff have emphasized to us that there are a number of serious scientific and technical problems that must be solved before we could engage in large-scale production of live poliovirus vaccine. Most important among these is the problem of extraneous contaminating simian viruses that may be extremely difficult to eliminate and which may be difficult if not impossible to detect at the present stage of the technology.”
What did the regulators do?
On March 25, 1961, the federal regulations that controlled the production of oral poliovirus vaccines were amended. These new regulations did not require the vaccine manufacturers throw away their SV40-contaminated poliovirus seeds, which were the source for all subsequent polio vaccines.
Instead, the rules required that “[e]ach seed virus used in manufacture shall be demonstrated to be free of extraneous microbial agents.”
The new regulations also required that each pair of monkey kidneys removed from a monkey for vaccine production “shall be examined microscopically for evidence of cell degeneration.”
Furthermore, fluid from the monkey kidney cells had to be combined with other tissue cultures in order to detect if there was any contaminating virus. The regulations required that “[t]he cultures shall be observed for at least 14 days.”
In essence, these regulations required an SV40 test that was comprised of taking the monkey kidney cells upon which the vaccine would be grown and:
Look at them through a microscope to see if they demonstrated SV40.
Take fluids from them.
Introduce those fluids into other cell cultures.
Wait 14 days.
Determine if the other cell cultures were changed as a result of the presence of SV40.
What were some of the problems with the test?
These tests were not designed to detect the contaminating viruses themselves. One cannot see SV40 or any virus with a standard light microscope or the naked eye.
Instead, the government’s SV40 test relied on the observation of the presumed effect of an SV40 infection on certain tissue cells to demonstrate the presence of the virus.
In fact, the regulations required only a 14-day observation period, even though it was well documented that the effect they were looking for (“vacuolating change”) could take up to six weeks for SV40 to show itself with this method:
“In this laboratory in [Green Monkey Kidney] GMK cultures inoculated with small quantities of virus [(SV40)] (i.e., <100 TCID50), changes were not observed until five or six weeks after inoculation. Therefore to attain maximal accuracy with this method, a long period of observation is required.”
These quality control steps were designed to appease the pharmaceutical companies because they did not require that the companies throw anything away and start over.
The steps also did not protect the public because they did not ensure the removal of SV40 from the vaccines for a number of reasons, including:
The original seed stocks that were known to be contaminated with SV40 were not thrown out, but instead used to make OPV for the next 40 years.
The substrate (monkey kidney cells) used to grow OPV were known to harbor SV40.
The quality control step was completely inadequate. For example, a 14- day observation period would not detect a virus that could take six weeks to grow.
In fact, in the early 1960s there are multiple scientific papers calling attention to this and suggesting better technologies to detect SV40. The government and pharmaceutical industry ignored these concerns and suggestions.
How was the epidemiology flawed?
After SV40 was originally detected in the Salk and Sabin vaccines which had been administered to millions of children around the world, the scientific community held its breath and wondered if these children would be stricken with cancer when they were young, or later as adults.
Indeed, both the pediatric and adult cancer rates have climbed steadily over the last 60 years. But, the few epidemiological studies that looked for a direct link between SV40 and human cancer provided inconsistent conclusions.
Each of these studies suffered from major flaws, including the fact that no one knew who actually received the SV40-contaminated vaccines and who did not — so it was impossible to compare an SV40-exposed group with a non-exposed group.
Most of these were the very same cancers created when SV40 was introduced into animals.
The question left unanswered for decades now faced scientists again — was SV40 responsible for causing or contributing to human cancers?
Over the years, scientists from around the world have made startling and disturbing discoveries. They have found SV40 antibodies in a significant percentage of people, including children who were too young to receive the SV40-contaminated vaccines of the early 1960s.
Scientists also discovered SV40 is actually inside some human cancers. Furthermore, they determined that SV40 interferes with the genes, like p53, which are necessary for making cancer cells die.
In July 2002, the National Academy of Science Institute of Medicine (IOM) Immunization Safety Committee convened a study into SV40 and cancer, which culminated in a report published in October 2002.
“The committee concludes that the biological evidence is strong that SV40 is a transforming [i.e., cancer-causing] virus … that the biological evidence is of moderate strength that SV40 exposure could lead to cancer in humans under natural conditions, [and] that the biological evidence is of moderate strength that SV40 exposure from the polio vaccine is related to SV40 infection in humans.”
In other words, there was scientific evidence that SV40 wasn’t simply a bystander inside human cancer cells — the scientists concluded the monkey virus could be the cause of the cancer in the person.
What was the government’s response?
Nonetheless, the various U.S. government agencies such as the Centers for Disease Control and Prevention (CDC) and National Cancer Institute, disputed these conclusions.
According to the CDC, “SV40 virus has been found in certain types of cancer in humans, but it has not been determined that SV40 causes these cancers.”
According to the NIH, “the NCI is continuing to evaluate the possible link between SV40 infection and human cancers.”
While the government spends decades “evaluating” SV40, this monkey virus:
Has already become prevalent in human populations and inside some human cancers.
Is such a strong carcinogen that a search for scientific articles about “SV40 and cancer” reveals more than 6,100 different scientific articles.
Makes orthodox cancer therapies less likely to be effective so they cannot save the life of the patient.
Conclusion
SV40 is a potentially deadly human carcinogen and it came from FDA approved and mandated vaccines.
To learn more about SV40, vaccines and cancer read “The Virus and the Vaccine: The True Story of a Cancer-Causing Monkey Virus, Contaminated Polio Vaccine, and the Millions of Americans Exposed” and visit SV40 Cancer Foundation and Our Alexander.
Our healthcare system is broken, a fact nobody would have disputed in precovid days. Regulatory capture is a reality, and the pharmaceutical industry is fraught with examples. Yet we trusted private-public partnerships to find an optimal solution to a global pandemic, assuming a crisis would bring out the best in historically corrupt institutions.
Here is a brief list of less-than-savory behavior demonstrated by our titans of healthcare:
Pfizer and Johnson & Johnson plead guilty to “misbranding with the intent to defraud or mislead” and paying “kickbacks to health care providers to induce them to prescribe [their] drugs,” resulting in fines of $2.3 billion in 2009 and $2.2 billion in 2013, respectively.
Pfizer settled another lawsuit for “manipulating studies” and “suppressing negative findings” just a few years later.
Gilead Sciences paid $97 million in fines, because it “illegally used a non-profit foundation as a conduit to pay the Medicare co-pays for its own drug.”
In 2005, AstraZeneca’s drug Crestor was shown to be linked to a life-threatening muscle disease while the company withheld evidence of this and two dozen other effects from the public.
In 2012, GlaxoSmithKline paid $3 billion in fines, as it “failed to include certain safety data” relating to their drug, since labeled as connected to heart failure and attacks.
Thankfully, our public health guardians are in place to protect us from the greed and deceit of the private sector, right? Wrong. Enjoy another brief list:
The Food and Drug Administration (FDA) worked behind the scenes with company Biogen to alter previously conducted trials of their $56,000 per year Alzheimer’s treatment, and “by removing the subset of people for whom the drug didn’t work, they found a slight statistical effect in favor of the drug.” Even after doing this, an advisory committee voted 10–0 against approving the drug. The FDA approved the drug anyway, causing three committee members to resign.
In that case, the third-party advisors did the right thing. This is not always the case: a study by Science Magazine tracking 107 FDA advisors for four years found that 62 percent received money from related drug makers, with 25 percent receiving over $100,000 and 6 percent receiving over $1 million. It only takes a few corrupt advisors to fix a panel and feign medical consensus.
In 2017, it was revealed that the acting Centers for Disease Control and Prevention (CDC) director for heart disease and stroke prevention had been secretly communicating with Coca-Cola, providing guidance on how “to influence world health authorities on sugar and beverage policy matters.”
The American healthcare system remains mired in good old-fashioned crony capitalism, fascism, corporatism, mercantilism, protectionism … fancy words for when private companies work with governments to subvert the forces of competition. The suppression of research into off-patent drugs is a nasty symptom of this problem.
While there are countless drugs to which this applies, we will discuss ivermectin. First, addressing the drug’s dismissal by its own manufacturer, Merck, let it be known that ivermectin is no longer under patent. Merck no longer owns exclusive rights to the drug’s production. The forces of competition have been bestowed upon the drug, thus making it far cheaper. Meanwhile, Merck is also currently rolling out an oral covid treatment, which the US government is providing $1.2 billion in funding to research. This would be under patent and may explain the company’s opposition to using ivermectin.
The usefulness of ivermectin remains debatable. However, it’s important to note that in early April 2020, a study at the University of Monash in Australia suggested it can be effective. Moreover, the drug is FDA approved, has existed for forty years, won a Nobel Prize, and is extremely safe when used at recommended levels. Given the crisis and ivermectin’s safety—safe even if not conferring big benefits for covid sufferers—the rush to condemn use of the drug appears suspect. Indeed, a week after the Australian study was published, the FDA advised against using ivermectin for COVID-19 treatment, forcing desperate people to the black market and to self-prescribe versions of the drug intended for animals.
The FDA noted subsequently that “additional testing is needed.” Yet, to date, there has not been a single completed government-funded study on the effectiveness of ivermectin against covid-19. Meanwhile, they have funneled billions toward research into vaccines and patented treatments. The National Institutes of Health (NIH) funded trials for remdesivir, still under patent with Gilead, despite it being less effective and having more severe side effects than ivermectin. The FDA approved remdesivir under emergency use authorization (EUA) despite published trials, later stating “remdesivir was not associated with statistically significant clinical benefits.”
One would think that if “additional testing” is so important, the US government might be interested in funding research to examine the potential benefits of cheap, safe, and proven drugs that have shown some promise in treating covid. But that’s clearly not what going on. Funding is geared toward helping huge pharmaceutical companies develop new patented drugs. As long Big Pharma wants it, and if there’s a profit to be made, apparently our government will be there to provide funding.
We are not “anti-VAXers.” We were vaccinated because we believed we were being told the truth. Now we know better.
Unfortunately, the current gene-based vaccines (all vaccines on the US market today) were rushed to market without proper testing. They are dangerous and appear to have killed over 30,000 previously healthy Americans so far and disabled an equivalent number.
The Phase 3 trials were structured so that the results looked good because they were allowed to exclude unfavorable data (such as Maddie de Garay, a 12-year old girl who participated in the Pfizer trial and who is now permanently paralyzed due to the vaccine). People with a bad first reaction were allowed to drop out which doesn’t reflect the reality of “full vaccination” requirements of workplaces and schools.
We should stop the current gene-based vaccines ASAP. The risk/benefit justification isn’t there for any age group due to the poor safety profile of these vaccines compared with the alternatives.
Based on analysis of VAERS death data for vaccine deaths and CDC death data for COVID deaths, the younger you are, the less sense vaccination makes. If early treatments didn’t work at all, the toxicity of the current vaccines would only make sense for those over 30 (based data to date). However, the vaccines are too toxic and don’t meet the <50 deaths stopping criteria that we’ve used for the past 30 years, so they should never be used because we have better alternatives available today that can achieve the same goals.
We should never be giving vaccines that disable or kill previously healthy people in huge numbers if safer alternatives are available that can achieve all the same objectives.
Why would anyone in America choose to have lipid nanoparticles which deliver a toxic protein into your brain and where the long term effects are unknown, when safer alternatives are available? What parent would choose to experiment on their kids this way when safer and more effective options are available?
It is tragic that schools are requiring students to be vaccinated in order to attend classes. I’ve asked our top universities for the risk-benefit analysis to justify this action and have received nothing. If the vaccines were perfectly safe, no analysis would be needed. But they aren’t.
The rate of severe life-changing side effects appears to be well in excess of 25,000 people (the number reported disabled is comparable to the number dead). The fact that Facebook groups of vaccine victims had 200,000 users suggests that more than 1 in 1,000 are suffering from significant long-term impacts; people with minor temporary reactions have little incentive to seek out and sign up for a vaccine side-effects group.
People who claim “the clinical trials showed no significant side effects so it must be safe” have a tough time explaining how these facebook groups were so large before they were deleted. If you think the vaccines are so safe, show me the severity analysis of the 200,000 people there. These groups don’t appear with the influenza vaccine. You never see neurological effects like this in such high volume with a safe vaccine.
Some have cited the emergence of the Delta variant as changing the math to favor vaccination even if the vaccine is unsafe. But the case fatality rate (CFR) of the Delta variant is only 0.1 percent compared to the CFR of 1.9 percent for the original virus (alpha) according to UK government data. The argument that the lower CFR of delta is due to the higher number of vaccinated people isn’t very credible since the Eta variant has a 2.7 percent CFR.
Early treatments are a more effective and safer option than the current vaccines. We can achieve all of the objectives of the current vaccination program (herd immunity, eradication of the virus, re-opening our economy, ditching of masks) with fewer deaths and near zero serious side effects. In addition, we would have less problem with variants since variants are less likely to be generated if everyone is naturally immune. So why not promote early treatments? Why not give them a try for a month while we hit the pause button on the vaccines? Would that be so bad?
Allowing natural infection will impart broad natural immunity. We should instruct the population how to treat early with early treatment protocols as soon as they believe they are infected. People should have the drugs on-hand so that treatment can be started without delay after speaking with their doctor. This results in superior risk reduction in terms of fewer fatalities and side effects compared to the current vaccines.
There was never a need for masking or social distancing as COVID is very treatable when treated early. Nobody has to die or be hospitalized. We can get to herd immunity quickly this way. The key is to treat the virus early with a proven early treatment cocktail of repurposed drugs, adding novel antivirals if/when available.
Unfortunately, the NIH has unethically suppressed all early treatments in order to push the vaccine narrative. This is clear with the publication of a systematic review of ivermectin, the highest level of evidence possible. Yet the NIH and WHO pretend that it never happened. It isn’t even acknowledged that the systematic review came out. There has never been a peer-reviewed systematic review that was later overturned. This is why they are the top of the evidence pyramid.
Early treatments were never funded. When evidence came in they worked, the NIH ignored it. The corruption at the NIH and FDA should be corrected by Congress. Now.
If a safe sterilizing vaccine can be developed, we should test it adequately for safety before deploying it. We should not cut corners on safety again; with early treatments, there is no need to rush this.
Major medical journals have lost objectivity in publishing papers that go against the “safe” narrative. For example, the NEJM rejected a Letter to the Editor pointing out a flaw in a paper showing vaccines were safe for pregnant women. The Letter showed an alarming statistic. The NEJM refused to reveal their reasoning for the rejection. Three editors quit a journal after a peer-reviewed paper was published that showed that vaccination may cause more harm than good. Those who quit provided no evidence that the paper was in error.
The censorship of legitimate medical information on social networks must end. These networks are the new “public square” and should be regulated so that people are free to express their opinions to anyone who chooses to listen. There should be heavy monetary penalties for suppressing medical information that has the potential to save lives. Social networks should be required to compensate all those people who have been harmed by their actions.
Never again should we deploy a vaccine on the American public without proper testing and without informed consent. Databases such as V-SAFE that track safety data should be made transparent. Am I the only person who thinks that is a problem?
VAERS reporting should be required and the VAERS system should be modernized so that it is easy to use and results in records with consistent field coding. There should be a smaller lag time to get records into the database, all false reports should be 100% enforced as a criminal act, and the safety signal monitoring should be much stronger.
The cost-benefit analysis of the current gene-based vaccines for anyone of any age is at best a wash according to the scientific literature (new paper published June 24, 2021). This peer-reviewed paper looked at the real cost-benefit analysis and concluded that “This lack of clear benefit should cause governments to rethink their vaccination policy.” As far as I know, this is the most optimistic of all the papers looking at actual death rates of COVID vs. the vaccine. All the other ones are even worse for the vaccine.
Independent analysis by a statistician friend shows a similar effect. Like me, Mathew has no axe to grind here, just trying to get at the truth of the risk/benefit for the current vaccines. His conclusion: “More importantly, I also still disagree with the mass vaccination program. In particular, nearly all lives saved are in the high risk group. While vaccinating those in the low risk group might decrease spread into the high risk group, that’s asking young healthy people to act as human shields.
I also believe that when the vaccine deaths and adverse events are finally tallied and compared to either a ring vaccination strategy or combination ring vaccination and early treatment strategy, the current plan will look quite foolish and possibly even nefarious.”
Since the focus today is on getting kids vaccinated, I ran the numbers in the VAERS database for 20-24 year olds and 25-29 year olds. In both age ranges, the number of deaths caused by the vaccine outnumber the number of deaths saved. The vaccines caused 1.89 deaths per 100,000 (ages 25-29) and 1.74 deaths per 100,000 (ages 20-24).
This means the vaccines are net killing machines since they kill more people than they save (.3 to 1.0 lives per 100K saved according to the most recent CDC presentation). My calculations are in the body of this document and the calculations show no net benefit for any age group based on real-world data from the US and UK.
The comparison is even more extreme if we tell kids to ignore the current CDC advice and use an early treatment program. In that case, we can reduce the death rate by more than two orders of magnitude from COVID, so that the number of lives saved by the vaccine is fewer than 1 in 10M. This means the vaccines need to be less toxic than the influenza vaccine (which has a death rate of 1 in 10M) in order to be considered. They are not even close to that. Not by a country mile.
For older people, the numbers don’t work out either. We looked at the UK data for <50 and >50 and we found that the absolute death rate is very small for <50 group. There was a high relative risk reduction, but the absolute deaths were small. If the vaccine kills more than 1 in 1 million, it’s game over for the vaccine being useful. For age >50, the UK data shows that even if the vaccines killed nobody, it is not beneficial. So when you factor the death rate of the vaccines and early treatment as the other option, the case is extremely lopsided.
In short, because the current vaccines are so dangerous and early treatment is so effective (relative risk reduction of 100 or more with no permanent side effects), there is no reasonable case that can be made for vaccinating any age group.
Although we just looked at deaths in the analysis above, the same can be true for other side effects as well: the range and intensity of side effects from the vaccine dwarf anything seen in natural COVID. It’s even a more stark contrast when early treatment is added to the mix.
Long term, untreated vax patients and untreated COVID patients are virtually identical in terms of symptoms (thanks to Ram Yogendra for that insight). By vaccinating patients, we are essentially giving a portion of those vaccinated long hauler COVID.
The case numbers in the UK (one of the most heavily vaccinated countries) are now climbing. It suggests we should have listened to the arguments of Geert Vanden Bossche, one of the most famous scientists in the vaccine field, which are further clarified in this excellent video by Chris Martenson which points out that there are really only two ways out of the pandemic: a sterilizing vaccine (using the complete virus as the antigen) or allowing infection and treating with early treatment leading to natural immunity.
The Yellow Card system in the UK showed a similar safety signal. Independent analysis of that data by an expert in medical evidence concluded that the vaccines are unsafe for use in humans. It wasn’t a close call. The death rates from the vaccines are far greater than any absolute risk reduction.
This is taken from a very long article. Read the rest here: docs.google.com
The National Institutes for Health (NIH) is exceptionally keen on the study of “Long Covid.” The federal agency recently allocated over $1 billion in funding for this purpose, and NIH Director Francis Collins has made the claimed ailment a recurring subject of his press commentary over the last year. The Department of Health and Human Services similarly signaled that it intends to classify “Long Covid” as a recognized disability for government funding and classification purposes.
So what is Long Covid, and why is it drawing so much attention and funding out of the federal government? As with any respiratory illness, Covid-19 does appear to have long-term sufferers who do not follow the normal recovery pattern and continue to demonstrate symptoms for weeks or months after an infection. At the same time however, the push to make “Long Covid” a distinctive medical classification unto itself appears to be a political phenomenon, wrapped up in clear signs of pseudoscience and linked back to a fringe “alternative wellness” blog that originally coined the term in March 2020.
A recent study published in the Lancet-owned journal EClinicalMedicine purported to document over 200 symptoms of Long Covid, ranging from fairly common Covid-19 ailments such as fatigue, cough, or long-term loss of smell to an eclectic assortment of problems such as hallucination, brain fog, tearfulness, insomnia, and mood anxiety. Media reports breathlessly repeated these findings to press the urgency of funding for Long Covid research, while also hyping the syndrome as a further justification for alarmism in justifying lockdowns and similar measures. After all, if Long Covid afflicts a sizable subset of Covid patients – as some claim – and can strike young people who are at a much lower mortality risk from the virus itself, then perhaps more restrictive measures are warranted on the general population – or so the argument goes.
Many lockdown advocates have seized onto the Long Covid narrative, incorporating it into their defenses of the draconian non-pharmaceutical interventions they have advocated over the last year and a half. The CovidFAQ website – a UK-based project set up by “neoliberal” activist Sam Bowman and British MP Neil O’Brien – invokes the threat of Long Covid in its attacks the Great Barrington Declaration (GBD), arguing that the hypothesized syndrome undermines evidence that the virus is substantially less-severe among younger demographics. Several pro-lockdown scientists and epidemiologists issued coordinated statements attacking the GBD in October 2020 for “ignor[ing] the emerging burdens of long COVID.” These statements are usually offered as declarative assessments, treating Long Covid as an established medical fact.
With billion-dollar budgets and the prospect of additional sweeping policy measures at stake, it only makes sense to ask if the science behind Long Covid is sound. There is no doubt that some Covid-19 victims have symptoms that linger for weeks or months beyond the typical recovery, although that is true of many diseases. Whether it has 200 plus symptoms is another story – and a closer look reveals an alarming amount of outright quackery is currently shaping the scientific and media discourse around Long Covid.
The problem arises from the amorphous definition of the phrase “Long Covid” itself. Far from a careful clinical diagnosis, Long Covid has become a catch-all term for any extended medical ailment, real or imagined, attributed to the effects of the Covid-19 virus. An alarming amount of alleged data about the phenomenon traces back to a single source called the “Body Politic Wellness Collective” – an alternative medicine blog with dubious scientific credentials. To quote one recent study of the term’s origins, “the emergence and recognition of Long COVID as a potentially major public health problem is largely due to advocacy groups such as the Body Politic COVID-19 Support Group, and Patient Led Research For COVID-19” – the latter an affiliated survey administrator that, according to its own website, was “born out of the Body Politic Slack support group.”
The same Body Politic group frequently appears in an already large and growing literature on “Long Covid” in other scientific journals. In September 2020, NIH Director Collins devoted his personal column on the agency’s website to touting the group. He later credited their work when launching the aforementioned $1 billion research initiative. In July 2021, Body Politic reappeared at the center of the aforementionedEClinicalMedicine study along with a spinoff organization called the Patient-Led Research Collaborative. The two groups administered the survey behind the claim that Long Covid carries over 200 symptoms.
Before we get into the survey itself, it’s useful to take a closer look at the Body Politic group. TheWall Street Journal recently ran a lengthy expose of the organization by Jeremy Devine, an Ontario-based psychiatrist. Devine found that the group’s initiatives sprang to life at the outset of the pandemic in March 2020. They first coined the Long Covid moniker around this time, promoting it in a flurry of media appearances. In early April, the New York Times ran an op-Ed by Body Politic’s co-founder calling attention to the syndrome and recounting her own experience as a “long hauler” (which, at the time, consisted of experiencing symptoms for about three weeks after testing positive).
As Devine documented in the WSJ, the Body Politic group’s approach to scientific survey design appeared highly unorthodox. It frequently relied on self-reported descriptions of Long Covid symptoms, instead of independent medical verification. It also had a habit of diagnosing people with Long Covid even after they tested negative for Covid-19 itself. A March 2021 report by Adam Gaffney for StatNews called attention to similar problems with Body Politic’s research design. “[A]t least some people who identify themselves as having long Covid appear never to have been infected with the SARS-CoV-2 virus,” Gaffney noted. They were nonetheless touted by the media as case studies in the alleged syndrome.
A closer look at the Body Politic group itself raises several red flags about their scientific qualifications. The group’s executive board boasts few, if any, actual medical practitioners or scientific experts. Instead we find an eclectic assortment of political activists, musicians, poets, and journalists, many of whom share common interests in “alternative medicine.” Body Politic’s Treasurer and principle support group organizer describes herself as a “practicing Spiritual Medium” who specializes in detecting “invisible illness.” The website’s Vice President is a “social & racial justice activist,” and its Secretary is an “aspiring sex coach.” Other affiliates include a self-described “socialist poet,” multiple “social justice activists,” and people who describe their careers as operating at the intersection between art and natural wellness. The group’s website and social media accounts frequently invoke political terminology from the critical theory literature. They describe themselves as “a queer feminist wellness collective and a space for inclusivity, accessibility, and crucial discussions about the very real connection between wellness, politics, and personal identity.” Their values statement espouses “patient-led” research to “democratize” medicine – descriptions that appear to forgo traditional scientific methods of testing and verification in favor of placing heavier reliance on patient testimonials and personal experience.
While the group’s activism alone does not disqualify their commentary, the unconventional qualifications of its leadership should raise suspicion about their claimed expertise on Long Covid. When NIH Director Collins personally promotes Body Politic’s work, he is creating a false sense of scientific credibility around their work. Few who read Collins’s statements are aware that the group he praises as “citizen scientists” might be better characterized as an odd assortment of psychic healers, magic crystal gurus, and alternative medicine activists. As a leading public health official, Collins’s many endorsements of this quackery border on irresponsible.
Turning to Body Politic’s survey projects, we quickly find that skepticism of their credibility is warranted. The group’s survey design specifically eschews requiring a positive Covid-19 test or antibody test to confirm that their respondents actually had the disease. “[W]e do not believe people’s experiences with COVID-19 symptoms should be discounted because they did not receive a positive test result,” states one justification for this unconventional data collection procedure. To qualify as a sufferer of Long Covid, it seems, a person needs only to claim that he or she suffers from Long Covid. Lived experience of the disease trumps any requirement of scientific verification.
The prevalence of unverified and untested Covid claimants being classified nonetheless as Long Covid sufferers is stunning. In the WSJ, Devine reports the numbers from the group’s first survey, administered through their website in 2020: “Nearly half (47.8%)” of Body Politic’s survey respondents “never had testing and 27.5% tested negative for Covid-19. Body Politic publicized the results of a larger, second survey in December 2020. Of the 3,762 respondents, a mere 600, or 15.9%, had tested positive for the virus at any time.” As Gaffney notes in StatNews, this practice raises the distinct possibility that survey respondents are misattributing other chronic symptoms to the virus.
Their new study in the Lancet’s journal EClinical Medicine does not offer much hope that Body Politic has improved its survey design. Its authors state that “We analyzed responses from 3762 participants with confirmed (diagnostic/antibody positive; 1020) or suspected (diagnostic/antibody negative or untested; 2742) COVID-19, from 56 countries.” Unconfirmed Covid patients with self-reported Long Covid symptoms outnumber confirmed Covid patients by almost 2.7 to 1. To their credit, the group discloses the lack of PCR or antibody testing confirmation among the majority of their respondents. The extremely high rates of unconfirmed cases, however, are more than sufficient to cast doubt upon their claims to have identified over 200 separate Long Covid symptoms.
The survey’s design also appears to self-select for people who are inclined to claim Long Covid symptoms, whether valid or not. According to the paper, the survey consisted of 257 questions, took almost 70 minutes on average to complete, allowed participants to revisit their answers for up to 30 days, and was primarily marketed to readers of the Body Politic group’s various blogs and Slack channels. This design practically ensures that the majority of the people who received and completed the survey were drawn from a readership that already gravitates towards the group’s political messaging and medical eccentricities.
Imagine if a survey on diet products collected its sample entirely from the mailing list of Gwyneth Paltrow’s “Goop” store. And imagine if the CDC decided to use that survey as a basis for a billion dollar program to revise its food nutrition guidelines, claiming that it is a representative study of the average American’s diet. Because that’s essentially what NIH Director Francis Collins has done with Body Politic’s surveys when justifying his current research initiative into Long Covid before the public.
With most Long Covid research at the moment, self-diagnosis by amateur groups appears to have supplanted scientific rigor in driving the NIH’s research priorities. Even minimal scrutiny should cast doubt upon the Body Politic group’s deficit of scientific credentials and surplus of outright “alternative medicine” quackery. Yet in January 2021 the New York Times heavily leaned on testimonials from Body Politic’s resident psychics and alternative wellness healers in a feature story on so-called Long Covid, aiming to demonstrate the scientific validity of the diagnosis.
So did an August 2020 piece in the Atlantic that is widely credited with popularizing the concept. Indeed, the New York Times has turned its opinion page over to Body Politic writers on multiple occasions over the last year, giving them free rein to promote unscientific claims about the concept. Simply scanning over mainstream media coverage of “Long Covid” in the last year reveals that Body Politic-affiliated activists with dubious scientific credentials have become go-to “experts” on the subject. Here they are being interviewed in Vox, in the Guardian, in theWashington Post, on NPR, in Buzzfeed, and on MSNBC.
In calling attention to Body Politic’s influence over shaping the Long Covid narrative, I do not question the possibility that some of the organization’s activists may exhibit genuine long-term Covid-related symptoms, even if they are not a distinct classification unto itself. But scientific assessment of their claims remains woefully inadequate relative to the authority that the media has bestowed upon them. In this sense, much of the Long Covid literature bears striking resemblance to other claimed chronic illnesses that have less-than-robust scientific grounding (for example, consider the difference between Celiac disease – a rare but severe dietary illness involving gluten – and the mid-2010s “gluten sensitivity” craze, which mixed together real and imagined but also self-diagnosed symptoms, fad dietary practices, and dubious scientific attestation)
Despite their scientific shortcomings, Body Politic’s own surveys have found a welcome audience among many academics who should know better. Even leading medical journals now regularly tout Body Politic’s dubious survey results as if they are scientific fact.
Last fall, the BMJ published an article on “Long Covid” from a team of scientists led by Oxford’s Trisha Greenhalgh, an outspoken pro-lockdown regular on the BBC and other UK media circuits. Greenhalgh’s team estimated that perhaps as many as 10% of people infected with Covid develop “Long Covid” symptoms – a number that has since become a standard estimate for Long Covid risks.
Their empirical “evidence” for Greenhalgh’s claim, in turn, derives primarily from Body Politic’s “patient-led survey” of alleged Long Covid sufferers – the same survey where half or more of respondents never even had a confirmed Covid diagnosis. This was no accidental reliance on a substandard source, deriving from insufficient scrutiny of the survey’s methods. Greenhalgh credited the Body Politic group by name on Twitter for inspiring their paper, endorsing the “lived experience” of their “patient-led research.” Echoing the Body Politic survey, Greenhalgh and her co-authors further embrace the proposition “that a positive test for covid-19 is not a prerequisite for diagnosis” for Long Covid. It’s apparently sufficient to simply believe that you had a prior bout with Covid, and attribute your claimed long-term symptoms to the same.
Not surprisingly, Long Covid has become a favored fallback argument among lockdowner epidemiologists to argue for prolonged restrictions. Duke University’s Gavin Yamey has made a name for himself by credulously circulating conspiracy theories about the Great Barrington Declaration by blogger Nafeez Ahmed. Sure enough, he’s also a Long Covid activist, promoting Greenhalgh’s study as well as an assortment of news articles that blur the lines between legitimate reporting of long-term symptoms and quackery.
Although Body Politic is far from the only group advocating for Long Covid research funding, their high-profile promotion by the NIH, by leading news outlets, and by medical journals suggests a similar phenomenon to the pattern seen among other lockdown advocates in allegedly-mainstream epidemiology. We’re witnessing a full-scale breakdown of the screening mechanisms that normally steer scientific discourse away from fringe and conspiracist viewpoints – provided that those viewpoints may be used to advance the alarmist ideologies that have emerged around Covid policy over the last year. The doors have, sadly, been thrown wide open to psychic healing and alternative wellness gibberish. Lockdowner scientists have, in turn, given these suspect claims and defective survey designs a welcome home in the most prestigious institutions of journalism, government, and the ivory tower.
Phillip W. Magness is a Senior Research Fellow at the American Institute for Economic Research. He holds a PhD and MPP from George Mason University’s School of Public Policy, and a BA from the University of St. Thomas (Houston).
Prior to joining AIER, Dr. Magness spent over a decade teaching public policy, economics, and international trade at institutions including American University, George Mason University, and Berry College.
Since COVID-19 hit the scene at the beginning of 2020, one of the key elements driving the fear around this disease is that there appeared to be no cure. And, for people who got infected with COVID-19, the guidance coming from major global institutions such as the NIH (US National Institutes of Health) and the CDC (US Centres for Disease Control) was basically “do nothing, stay home, and when you turn blue go to the hospital.” This public health policy prescription was usually followed by the qualifying caveat, “this is our only approach until a vaccine arrives.”
This, clearly, has terrified people all around the world. For the majority of the world’s population the belief has been that catching COVID-19 is a veritable death sentence. Which leads us to an important question. How would things change if there were, in fact, effective treatments for COVID-19?
I have just come out of a fascinating 90-minute press conference and Zoom call, delivered by the Malaysian Alliance for Effective COVID Control (MAECC). This was very much a “good news” presentation. The main message? There are very effective treatments for COVID-19.
The essence of the discussion in the MAECC session focused on the drug Ivermectin. The Doctors found it necessary to do a press conference and public presentation because the widespread use of Ivermectin in Malaysia is currently illegal. A doctor prescribing Ivermectin for his COVID-19 patients was recently raided by police!
Malaysian doctors are not doing leading edge research here, but simply trying to care for their patients by working to get a proven treatment officially accepted for use in Malaysia. Ivermectin has already been used very successfully in many places around the world where media hysteria did not get it banned from the shelves. Mexico has used it to great effect, as did Peru. Over the last few weeks, reports coming out of India are demonstrating massive benefits from Ivermectin.
There is already a 97% decline in cases in New Delhi, India. Indeed, four other Indian states that are using Ivermectin now report decreases in cases by 60% to 95%. However, other states that have blocked the use of Ivermectin have increases in cases by several hundred percent – the exponential explosion that everyone is terrified of!
As The Desert Review says in their report, “It is a clear refutation of the WHO, FDA, NIH, and CDC’s policies of ‘wait at home until you turn blue’ before you get treatment.”
Before you buy into the criticism that these are only “observational studies” and haven’t been tested by large scale, randomized control trials approved by the WHO, CDC, NIH, FDA etc. it’s important to realize that the only type of studies that are apparently good enough for such institutions these days are those which are so large and complex that only multi-national pharmaceutical companies are able to run and fund them.
That said, you should know that 56 studies on Ivermectin, 17 of them being Randomized Control Trials, have clearly demonstrated very positive effects from Ivermectin. A site doing real-time meta-analysis of all the Ivermectin studies as they get published summarizes the results as follows: “100% of the 17 Randomized Controlled Trials (RCTs) for early treatment and prophylaxis report positive effects, with an estimated improvement of 73% and 83% respectively”.
They also make the point that “The probability that an ineffective treatment generated results as positive as the 56 studies to date is estimated to be 1 in 2 trillion (p = 0.00000000000041).” You can check this information yourself directly on their site (Source: https://ivmmeta.com).
Another effective protocol for prophylaxis and early treatment of COVID-19 is Hydroxychloroquine (HCQ) with Zinc. As of this writing, 248 trials of HCQ used for treating COVID-19 have been completed, by 3,972 scientists, with 378,812 patients. We can see 66% improvement in 26 early treatment trials, 75% improvement in 11 early treatment mortality results, and 24% improvement in 35 randomized controlled trials. These results are publicly available on a database that is tracking all HCQ studies to date. You can see those studies here at https://c19hcq.com.
There are also a number of other effective treatments for COVID-19 that we don’t have space for here.
What’s important to understand is that these effective treatments have been used since mid-2020. Which raises a very important point. If these treatments are so effective, why haven’t we heard about them? Why aren’t they being used everywhere? It appears that, for some reason, information about the effectiveness of these treatments is being suppressed.
For instance, “Fact checkers” will tell you that HCQ or Ivermectin aren’t authorized by major institutions like the FDA, CDC, or WHO (as if such organizations are supposed to set and police policy rather than simply providing guidance). They will also try to discount any positive results using ad hominem attacks and smears, such as pointing out that a person using one of these treatments may have at some time in the past, voiced “anti-vaccine sentiments” (whatever that may be). You can see an example here: https://factcheck.afp.com/ivermectin-and-hydroxychloroquine-are-not-proven-covid-19-treatments
The censorship extends to Social Media. A whole list of front-line doctors who have successfully used some of these treatments have had their accounts removed from Social Media platforms, simply because information they provided about their successes was deemed “contrary to guidelines from the WHO” by the various Big Tech platforms. I have personally witnessed the de-platforming of literally dozens of highly respected, professional, front line doctors and researchers.
De-platforming is not the only concern. It appears that in the attempts to discredit effective treatments for COVID-19, anything goes. A study which came out in The Lancet mid-2020 supposedly showing that HCQ was dangerous was subsequently withdrawn due to the study being fraudulent.
Sadly, this withdrawal happened only after the damage was done, and HCQ had been successfully kicked to the curb in many places around the world – even up to the point that in some jurisdictions doctors could be jailed for prescribing it!
You may ask: “How did these studies that were apparently designed to falsify the effects of a widely used drug, pass peer review in the world’s premier medical science journals – The Lancet as well as The New England Journal of Medicine ?” The details of this sordid tale can be found here: https://ahrp.org/the-lancet-published-a-fraudulent-study-editor-calls-it-department-of-error/
If one digs, it appears that the main reason that we have not heard of these effective treatments is that the WHO and the CDC and other major institutions do not approve of the use of any alternative treatments, unless these are being tested in a clinical trial (which it seems only they can approve of). For instance, the US National Institutes for Health (NIH) guidelines state: “The COVID-19 Treatment Guidelines Panel (the Panel) recommends against the use of any drugs for SARS-CoV-2 pre-exposure prophylaxis (PrEP), except in a clinical trial (AIII).” See the PDF document here: https://files.covid19treatmentguidelines.nih.gov/guidelines/covid19treatmentguidelines.pdf
This is indeed strange, especially in the middle of a pandemic. One would expect that, in order to save patient lives, doctors would look for and try medicines that might possibly work, as long as there were no safety issues. When clearly there is evidence of no-harm, and increasingly powerful evidence that certain treatments can save lives, it would be highly unethical for Doctors NOT to start using such treatments. Doctors use medicines for purposes other than those listed on the label all the time!
Since Ivermectin and HCQ are both on the WHO list of essential medicines and have been so for a long time – decades in the case of HCQ – the world knows about the safety and dosage of these medicines. As an example, since 1992, Ivermectin has only been linked to 16 deaths, whereas deaths linked to the COVID-19 vaccines are now in the thousands (information from the Uppsala Drug Monitoring Centre run by the WHO (https://www.who-umc.org) via Prof Paul Marik, Chief of Critical Care & Pulmonary Medicine, EVM, USA).
Clearly, something appears very much out of balance here. There ARE effective treatments for COVID-19, yet the institutions that we rely on for medical guidance appear to be ignoring, or even suppressing these treatments – even though they are known to be safe after many decades of use. Despite their known safety, neither Ivermectin nor HCQ have been able to obtain even an EAU (Emergency Use Authorization)!
At the same time, new creations that have only had very limited testing, and for which the safety cannot be known in such a short period of time, are approved for emergency use.
The world economy is now in dire straits, with entire populations having been essentially under house arrest for the better part of 18 months. People continue to die from (or with) COVID-19 without treatments being available. And we are now seeing important examples of breakout infections in people who have already been vaccinated against COVID-19. As Reutersreported just a few days ago, “Hundreds of vaccinated Indonesian health workers get COVID-19, dozens in hospital”. This is just one many similar news stories reporting the very same phenomenon.
According to the pharmaceutical manufacturers themselves, the current range of emergency use vaccines do not actually provide immunity and only “reduce severe symptoms” of COVID-19. While this issue has yet to be fully resolved, many in the mainstream are still claiming that these vaccines will “inoculate” the recipient against the novel coronavirus. Therefore, these jabs should rightly be categorised as a type of treatment against the disease of COVID-19, and not a vaccine against the said pathogen, the SARSCoV2 coronavirus.
It goes without saying that the wide availability of cheap and effective drug treatments for COVID would severely undermine the widely touted mainstream claim that mass-vaccinations are the only solution to slowing down or ‘defeating’ a supposed global pandemic.
Clearly, effective treatments are absolutely required at this point. The good news is that there are such treatments available.
With effective treatments in hand, the global COVID-19 situation could end in as little as a few weeks. The world CAN return to normal. Sadly, there seem to be forces at work blocking such an outcome.
We need to ask: why are these effective treatments not being allowed in so many places? Why is information about these treatments being suppressed? Perhaps the fact that treatments like Ivermectin and HCQ are off patent and extremely cheap might give us a clue.
***
Author Chris Lonsdale is a psychologist, linguist, educator, entrepreneur, dialogue facilitator and corporate advisor with over thirty years experience doing business in Asia.
Immediately after Rick Bright was transferred out of his position as head of BARDA and sent to the NIH, he started making a huge fuss. The April 22, 2020 NYT discribed his statements:
“While I am prepared to look at all options and to think ‘outside the box’ for effective treatments, I rightly resisted efforts to provide an unproven drug on demand to the American public,” Dr. Bright said. He went on to describe what he said ultimately happened: “I insisted that these drugs be provided only to hospitalized patients with confirmed Covid-19 while under the supervision of a physician.”
By May 14, 2020 Bright was already before Congress, supposedly as the good guy whistleblower who was trying to get things right for the pandemic against huge odds:
Bright told lawmakers Thursday he and other federal health officials had “worked hard” to resist pressure to allow a significant increase in access to hydroxychloroquine, and instead scaled that back to allowing an emergency use authorization but only “with strict guidelines.”
But he said his “concerns were escalated when I learned that officials were pushing to make that drug available outside that emergency authorization.”
“When I spoke outside of the government and shared my concern with the American public, that I believe was the straw that broke the camels back and escalated my removal,” Bright said.
He later said, “The highest priority we have is safety.”
… Bright’s lawyers said last week that the OSC had told them the investigation already had found evidence that Bright was ousted as head of a health agency for pushing back against increasing use of hydroxychloroquine…
HHS, in an emailed statement, said, “Rick Bright was transferred from his role as BARDA director to lead a bold new $1 billion testing program at NIH, critical to saving lives and reopening America.”
“Mr. Bright has not yet shown up for work, but continues to collect his $285,010 salary, while using his taxpayer-funded medical leave to work with partisan attorneys who are politicizing the response to COVID-19,” the statement said.
“His whistleblower complaint is filled with one-sided arguments and misinformation. HHS is reviewing the complaint and strongly disagrees with the allegations and characterizations made by Rick Bright.”
HHS also said that it was under Bright’s leadership that BARDA identified chloroquine and hydroxychloroquine as potential Covid-19 treatments.
“Rick Bright was the sponsor of getting hydroxychloroquine and praised his team for acquiring the drugs,” HHS said.
Bright’s reward? He was made a senior vice president of the Rockefeller Foundation, after refusing to show up for work at NIH. And who raved about him on the Rockefeller Foundation website? None other than Jeremy Farrar and Michael Ryan. I have not written about Ryan so far, but he is another co-conspirator in the efforts to suppress appropriate treatments, poison patients with excess doses of HCQ and prolong the pandemic, as Executive Director of the World Health Organization’s Health Emergencies Programme.
“If there is something we have learned throughout the COVID-19 pandemic and other high impact epidemics, it is that pandemic preparedness and response cannot be advanced with a siloed approach,” said Dr. Mike Ryan, Executive Director of the WHO’s Health Emergencies Programme. “Few people bring the full package to the table: profound scientific and public health expertise, years of outbreak response experience, a private and public sector background and a collaborative, innovative, and out-of-the-box mindset. Rick Bright combines all these qualities. His leadership will be an enormous asset to The Rockefeller Foundation and to the global health community.”Dr. Bright resigned from government service in protest over the Trump administration’s approach to handling the Covid-19 pandemic, specifically over the level of political interference in science and the spread of inaccurate information that he said was ‘dangerous, reckless and causing lives to be lost.’
“I’m delighted that Dr. Rick Bright has been appointed as Senior Vice President of Pandemic Prevention and Response at The Rockefeller Foundation,” said Dr. Jeremy Farrar, Director of Wellcome. “The Covid-19 pandemic has highlighted the human and economic costs of epidemics and the fact that we need to be better prepared to identify and respond to emerging infections. Dr. Bright is a leading figure in global health with a wealth of experience, and we look forward to working with him over the coming years.”
Bright’s job at Rockefeller is to work on future pandemic planning. Need I say more?
Michael Capuzzo, a New York Times best-selling author, has just published an article titled “The Drug That Cracked Covid”. The 15-page article chronicles the gargantuan struggle being waged by frontline doctors on all continents to get ivermectin approved as a Covid-19 treatment, as well as the tireless efforts by reporters, media outlets and social media companies to thwart them.
Because of ivermectin, Capuzzo says, there are “hundreds of thousands, actually millions, of people around the world, from Uttar Pradesh in India to Peru to Brazil, who are living and not dying.” Yet media outlets have done all they can to “debunk” the notion that ivermectin may serve as an effective, easily accessible and affordable treatment for Covid-19. They have parroted the arguments laid out by health regulators around the world that there just isn’t enough evidence to justify its use.
For his part, Capuzzo, as a reporter, “saw with [his] own eyes the other side [of the story]” that has gone unreported, of the many patients in the US whose lives have been saved by ivermectin and of five of the doctors that have led the battle to save lives around the world, Paul Marik, Umberto Meduri, José Iglesias, Pierre Kory and Joe Varon. These are all highly decorated doctors. Through their leadership of the Front Line COVID-19 Critical Care (FLCCC) Alliance, they have already enhanced our treatment of Covid-19 by discovering and promoting the use of Corticoid steroids against the virus. But their calls for ivermectin to also be used have met with a wall of resistance from healthcare regulators and a wall of silence from media outlets.
“I really wish the world could see both sides,” Capuzzo laments. But unfortunately most reporters are not interested in telling the other side of the story. Even if they were, their publishers would probably refuse to publish it.
That may explain why Capuzzo, a six-time Pulitzer-nominated journalist best known for his New York Times-bestselling nonfiction books Close to Shore and Murder Room, ended up publishing his article on ivermectin in Mountain Home, a monthly local magazine for the of the Pennsylvania mountains and New York Finger Lakes region, of which Capuzzo’s wife is the editor. It’s also the reason why I decided to dedicate today’s post to Capuzzo’s article. Put simply, as many people as possible –particularly journalists — need to read his story.
As Capuzzo himself says, “I don’t know of a bigger story in the world.”
Total News Blackout
On December 8 2020, FLCCC member Dr Pierre Kory gave nine minutes of impassioned testimony to the US Homeland Security Committee Meeting on the potent anti-viral, anti-inflammatory benefits of ivermectin. A total of 9 million people (myself included) saw the video on YouTube before it was taken down by YouTube’s owner, Google. As Capuzzo exhaustively lays out, both traditional and social media have gone to extraordinary lengths to keep people in the dark about ivermectin. So effective has this been that even in some of the countries that have benefited most from its use (such as Mexico and Argentina) many people are completely unaware of its existence. And this is no surprise given how little information is actually seeping out into the public arena.
A news blackout by the world’s leading media came down on Ivermectin like an iron curtain. Reporters who trumpeted the COVID-19 terror in India and Brazil didn’t report that Ivermectin was crushing the P-1 variant in the Brazilian rain forest and killing COVID-19 and all variants in India. That Ivermectin was saving tens of thousands of lives in South America wasn’t news, but mocking the continent’s peasants for taking horse paste was. Journalists denied the world knowledge of the most effective life-saving therapies in the pandemic, Kory said, especially among the elderly, people of color, and the poor, while wringing their hands at the tragedy of their disparate rates of death.
Three days after Kory’s testimony, an Associated Press “fact-check reporter” interviewed Kory “for twenty minutes in which I recounted all of the existing trials evidence (over fifteen randomized and multiple observational trials) all showing dramatic benefits of Ivermectin,” he said. Then she wrote: “AP’S ASSESSMENT: False. There’s no evidence Ivermectin has been proven a safe or effective treatment against COVID-19.” Like many critics, she didn’t explore the Ivermectin data or evidence in any detail, but merely dismissed its “insufficient evidence,” quoting instead the lack of a recommendation by the NIH or WHO. To describe the real evidence in any detail would put the AP and public health agencies in the difficult position of explaining how the lives of thousands of poor people in developing countries don’t count in these matters.
Not just in media but in social media, Ivermectin has inspired a strange new form of Western and pharmaceutical imperialism. On January 12, 2021, the Brazilian Ministry of Health tweeted to its 1.2 million followers not to wait with COVID-19 until it’s too late but “go to a Health Unit and request early treatment,” only to have Twitter take down the official public health pronouncement of the sovereign fifth largest nation in the world for “spreading misleading and potentially harmful information.” (Early treatment is code for Ivermectin.) On January 31, the Slovak Ministry of Health announced its decision on Facebook to allow use of Ivermectin, causing Facebook to take down that post and removed the entire page it was on, the Ivermectin for MDs Team, with 10,200 members from more than 100 countries.
In Argentina, Professor and doctor Hector Carvallo, whose prophylactic studies are renowned by other researchers, says all his scientific documentation for Ivermectin is quickly scrubbed from the Internet. “I am afraid,” he wrote to Marik and his colleagues, “we have affected the most sensitive organ on humans: the wallet…” As Kory’s testimony was climbing toward nine million views, YouTube, owned by Google, erased his official Senate testimony, saying it endangered the community. Kory’s biggest voice was silenced.
“The Most Powerful Entity on Earth”
Malcom X once called the media “the most powerful entity on the earth.” They have, he said, “the power to make the innocent guilty and to make the guilty innocent, and that’s power. Because they control the minds of masses”. Today, that power is now infused with the power of the world’s biggest tech and social media companies. Together social and traditional media have the power to make a medicine that has saved possibly millions of lives during the current pandemic disappear from the conversation. When it is covered, it’s almost always in a negative light. Some media organizations, including the NY Times, have even prefaced mention of the word “ivermectin” — a medicine that has done so much good over its 40-year lifespan that its creators were awarded the Nobel Prize for Medicine in 2015 — with the word “controversial.”
Undeterred, many front-line doctors have tried to persuade their respective health regulators of the unparalleled efficacy and safety of ivermectin as a covid treatment. They include Dr. Tess Lawrie, a prominent independent medical researcher who, as Capuzzo reports, evaluates the safety and efficacy of drugs for the WHO and the National Health Service to set international clinical practice guidelines:
“[She] read all twenty-seven of the Ivermectin studies Kory cited. The resulting evidence is consistent and unequivocal,” she announced, and sent a rapid meta-analysis, an epidemiolocal statistical multi-study review considered the highest form of medical evidence, to the director of the NHS, members of parliament, and a video to Prime Minister Boris Johnson with “the good news… that we now have solid evidence of an effective treatment for COVID-19…” and Ivermectin should immediately “be adopted globally and systematically for the prevention and treatment of COVID-19.”
Ignored by British leaders and media, Lawrie convened the day-long streaming BIRD conference—British Ivermectin Recommendation Development—with more than sixty researchers and doctors from the U.S., Canada, Mexico, England, Ireland, Belgium, Argentina, South Africa, Botswana, Nigeria, Australia, and Japan. They evaluated the drug using the full “evidence-to-decision framework” that is “the gold standard tool for developing clinical practice guidelines” used by the WHO, and reached the conclusion that Ivermectin should blanket the world.
“Most of all you can trust me because I am also a medical doctor, first and foremost,” Lawrie told the prime minster, “with a moral duty to help people, to do no harm, and to save lives. Please may we start saving lives now.” She heard nothing back.
Ivermectin’s benefits were also corroborated by Dr. Andrew Hill, a renowned University of Liverpool pharmacologist and independent medical researcher, and the senior World Health Organization/UNITAID investigator of potential treatments for COVID-19. Hill’s team of twenty-three researchers in twenty-three countries had reported that, after nine months of looking for a COVID-19 treatment and finding nothing but failures like Remdesivir— “we kissed a lot of frogs”— Ivermectin was the only thing that worked against COVID-19, and its safety and efficacy were astonishing—“blindingly positive,” Hill said, and “transformative.” Ivermectin, the WHO researcher concluded, reduced COVID-19 mortality by 81 percent.
Why All the Foot Dragging?
Yet most health regulators and governments continue to drag their feet. More evidence is needed, they say. All the while, doctors in most countries around the world have no early outpatient medicines to draw upon in their struggle against the worst pandemic in century. Drawing on his own experience, Capuzzo describes the absence of treatments for COVID-19 as a global crisis:
When my daughter Grace, a vice president at a New York advertising agency, came
down with COVID-19 recently, she was quarantined in a “COVID hotel” in Times Square with homeless people and quarantining travelers. The locks on her room door were removed. Nurses prowled the halls to keep her in her room and wake her up every night to check her
vitals—not to treat her, because there is no approved treatment for COVID-19; only, if her oxygen plummeted, to move her to the hospital, where there is only a single eective approved treatment for COVID-19, steroids that may keep the lungs from failing.
There are three possible explanations for health regulators’ refusal to allow the use of a highly promising, well-tolerated off-label medicine such as ivermectin:
As a generic, ivermectin is cheap and widely available, which means there would be a lot less money to be made by Big Pharma if it became the go-to early-stage treatment against covid.
Other pharmaceutical companies are developing their own novel treatments for Covid-19 which would have to compete directly with ivermectin. They include ivermectin’s original manufacturer, Merck, which has an antiviral compound, molnupiravir, in Phase 3 clinical trials for COVID-19. That might explain the company’s recent statement claiming that there is “no scientific basis whatsoever for a potential therapeutic effect of ivermectin against COVID-19.
If approved as a covid-19 treatment, ivermectin could even threaten the emergency use authorisation granted to covid-19 vaccines. One of the basic conditions for the emergency use authorisation granted to the vaccines currently being used against covid is that there are no alternative treatments available for the disease. As such, if ivermectin or some other promising medicine such as fluvoxamine were approved as an effective early treatment for Covid-19, the vaccines could be stripped of authorisation.
This may explain why affordable, readily available and minimally toxic drugs are not repurposed for use against Covid despite the growing mountains of evidence supporting their efficacy.
Ivermectin has already been approved as a covid-19 treatment in more than 20 countries. They include Mexico where the mayor of Mexico City, Claudia Scheinbaum, recently said that the medicine had reduced hospitalisations by as much as 76%. As of last week, 135,000 of the city’s residents had been treated with the medicine. The government of India — the world’s second most populous country and one of the world’s biggest manufacturers of medicines — has also recommended the use of ivermectin as an early outpatient treatment against covid-19, in direct contravention of WHO’s own advice.
Dr Vikas P. Sukhatme, the dean of Emory School of Medicine, recently wrote in a column for the Times of India that deploying drugs such as ivermectin and fluvoxamine in India is likely to “rapidly reduce the number of COVID-19 patients, reduce the number requiring hospitalization, supplemental oxygen and intensive care and improve outcomes in hospitalized patients.”
Four weeks after the government included ivermectin and budesonide among its early treatment guidelines, the country has recorded its lowest case count in 40 days.
In many of India’s regions the case numbers are plunging in almost vertical fashion. In the capital Delhi, as in Mexico City, hospitalisations have plummeted. In the space of 10 days ICU occupancy fell from 99% to 70%. Deaths are also falling. The test positivity ratio slumped from 35% to 5% in just one month.
One of the outliers of this trend is the state of Tamil Nadu, where cases are still rising steeply. This may have something to do with the fact that the state’s newly elected governor, MK Stalin, decided to exclude ivermectin from the region’s treatment protocol in favor of Remdesivir. The result? Soaring cases. Late last week, Stalin reversed course once again and readopted ivermectin.
For the moment deaths in India remain extremely high. And there are concerns that the numbers are being under-reported. Yet they may also begin to fall in the coming days. In all of the countries that have used ivermectin widely, fatalities are the last thing to fall, after case numbers and hospitalizations. Of course, there’s no way of definitively proving that these rapid falloffs are due to the use of ivermectin. Correlation, even as consistent as this, is not causation. Other factors such as strict lockdowns and travel restrictions no doubt also play a part.
But a clear pattern across nations and territories has formed that strongly supports ivermectin’s purported efficacy. And that efficacy has been amply demonstrated in three meta-analyses.
India’s decision to adopt ivermectin, including as a prophylaxis in some states, is already a potential game-changer. As I wrote three weeks ago, if case numbers, hospitalizations and fatalities fall in India as precipitously as they have in other countries that have adopted ivermectin, it could even become a watershed moment. But for that to happen, the news must reach enough eyes and ears. And for that to happen, reporters must, as Capuzzo says, begin to do their job and report both sides of this vital story.
BILL Gates’s company Microsoft has changed our lives. It turned him into one of the richest men in the world and allowed him to turn philanthropist. His endeavour began in 1994 when he established the William H. Gates Foundation, soon to be followed by the Gates Learning Foundation in 1997. He merged the organisations in 2000 creating the Bill & Melinda Gates Foundation (GF). After the couple transferred $20billion of their Microsoft stock to the GF it became the largest charitable foundation in the world and over the next twenty years the most powerful charity in the world. Its endowment as of 2019 was $50billion.
The GF made its first donation to the World Health Organisation (WHO) in 1998. Soon after Gates pledged a further $750million to set up the Global Alliance for Vaccines and Immunization (Gavi), the stated aim of which is to increase immunisation rates in low-income countries, with the WHO and the UK amongst its original founders and donors. Last year Boris Johnson pledged Gavi £1.65billion over five years at the June 2020 Global Vaccine Summit replenishment conference, which the UK hosted. Six months later Johnson met Gates and pharmaceutical bosses to discuss Britain’s vaccine rollout and future pandemic plans.
The GF holds a permanent seat on Gavi’s board. Gavi’s core partners today are the GF, the WHO, Unicef and the World Bank, with the GF giving Gavi $4.1billion since its inception. Gavi is also the fifth largest funder of the WHO, giving $355.4million last year. With the WHO, Gavi dominates global vaccination campaigns including the Covid-19 vaccine rollout.
The WHO’s list of top 20 donors for the two-year budget cycle of 2018 and 2019 shows the GF coming second only to the US (their $893million donation accounting for 20 per cent of the WHO’s budget) with a $531 million donation (equal to 12 per cent of WHO’s budget). The GF and Gavi together outstrip all single country donations, except that of the US.
Since its inception the GF has given $54.8billion to a multitude of organisations. It has expanded globally, opening offices in Beijing in 2007 and London in 2010, and funding works in 135 countries. A letter from President Xi Jinping to Bill Gates, which you can read here, suggests Gates’s closeness to the Chinese Communist Party.
Donations from billionaires over the past 25 years have extensively bolstered the GF’s finances. Between 1994 and 2018 Mr and Mrs Gates donated $36billion of their own money, and in 2006 Warren Buffet pledged $30billion.
Eight years after establishing Gavi, Gates stepped down in 2008 as Microsoft CEO to commit more of his time to his foundation. By that time the GF was the largest charitable foundation in the US, and questions were being raised even then about its long reach in shaping US government health policies. After going into financial partnership with the GF, the publicly funded US National Institutes of Health (NIH) shifted their focus from the health and welfare of American citizens to global health. Concerns about the power, complexity and lack of accountability of GF, and Gates’s potential – effectively now realised – to become WHO’s largest donor continue to be articulated.
In 2010, with Warren Buffett, the Gateses launched Giving Pledge, a vehicle through which the very wealthy could donate to charity. To date there are no public details of who donates what through Giving Pledge, though this endeavour has turned into a tax haven for billionaires.
The GF is also a co-founder and funder of CEPI (Coalition for Epidemic Preparedness Innovations), as influential as Gavi but less known. CEPI is a Norwegian venture which invests in vaccines and is also funded by the Indian and Norwegian governments, the British-based Wellcome Trust and the World Economic Forum. Jeremy Farrar, director of the Wellcome Trust and member of Sage, sits on the CEPI board. In 2017 Gates said that the world was unprepared for pandemics and that CEPI’s investments in ‘DNA/RNA vaccines’ would mitigate that. Both the GF and Wellcome Trust have pledged to fund CEPI with $100million annually from 2017 to 2022.
The initial endeavours of the William H. Gates Foundation to support scientific research and local charities have morphed into a global juggernaut with unaccountable power. Vast amounts of money are being channelled according to the thoughts, passions and prejudices of one man with questionable judgment.
In 1998, Gates was hauled before the US Senate to answer questions about Microsoft’s anti-trust practices. His demeanour while giving testimony was dishonest and arrogant. His performance is disturbing to watch, captured in this clip (from 1 minute 29 seconds) where he rocked repeatedly in his chair and insisted he didn’t understand the word ‘concern’.
When the WHO was formed as an intergovernmental organisation, it would have been unimaginable that a private foundation could have such influence or set the global health agenda. Though awareness of the GF’s influence over the WHO and Gavi is growing, what is less well documented is its extensive reach closer to home and its control over British science, medicine and public health. This I will be reporting on in the coming days.
By Jonas E. Alexis | Veterans Today | October 16, 2107
In 1973 Irving Kristol, the godfather of the Neoconservative movement, made a stunning statement which is still relevant to understanding the Israeli influence in US foreign policy. Kristol said:
“Senator McGovern is very sincere when he says that he will try to cut the military budget by 30%. And this is to drive a knife in the heart of Israel… Jews don’t like big military budgets. But it is now an interest of the Jews to have a large and powerful military establishment in the United States…
“American Jews who care about the survival of the state of Israel have to say, no, we don’t want to cut the military budget, it is important to keep that military budget big, so that we can defend Israel.”
Read the statement again very carefully. A big military budget, said Kristol, is only good for Israel, not America or much of the Western World. In other words, precious American soldiers who go to the Middle East to fight so-called terrorism are just working for Israel, not for America.
So, whenever the Neocons use words such as “democracy” or “freedom,” they are essentially conning decent Americans to support Israel’s perpetual wars. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.

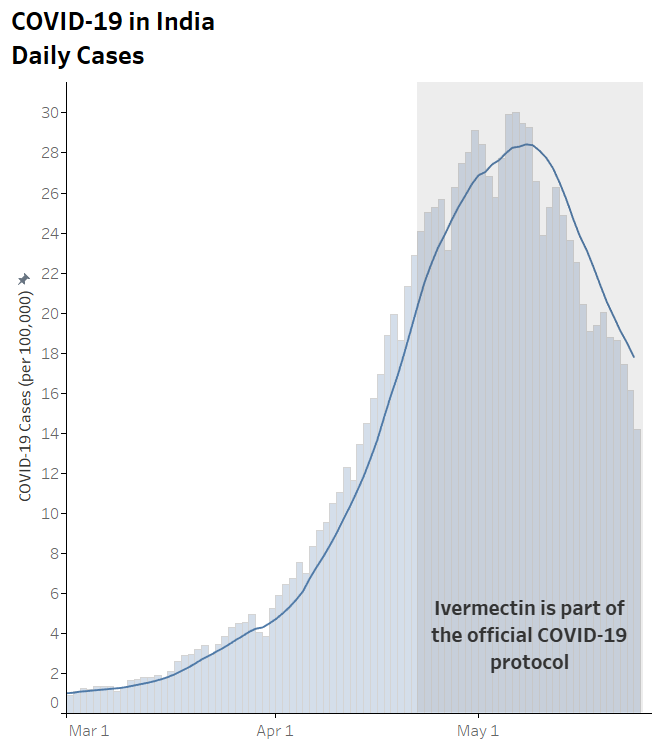

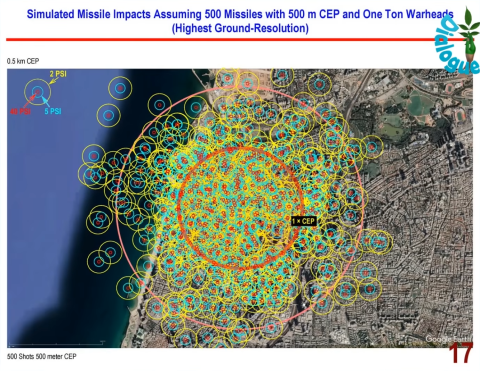

 Aletho News
Aletho News