Prominent Scientists Go Public: ‘Fauci Fooled America’
By Jeremy Loffredo | The Defender | November 2, 2021
In an op-ed, “Fauci Fooled America,” published Monday in Newsweek, two scientists accused Dr. Anthony Fauci of bungling the government’s response to COVID by getting “major epidemiology and public health questions wrong.”
Martin Kulldorff, Ph.D., an epidemiologist at Harvard Medical School, and Jay Bhattacharya, M.D., Ph.D., professor of Health Policy at Stanford University School of Medicine wrote: “Reality and scientific studies have now caught up with him.”
Kulldorff and Bhattacharya, both senior scholars at the Brownstone Institute and signers of the Great Barrington Declaration, had this message for Newsweek readers:
“The evidence is in. Governors, journalists, scientists, university presidents, hospital administrators and business leaders can continue to follow Dr. Anthony Fauci or open their eyes. After 700,000-plus COVID deaths and the devastating effects of lockdowns, it is time to return to basic principles of public health.”
The authors ticked off a list of “key issues” Fauci got wrong, including failure to recognize natural immunity, protecting the elderly, school closures, masks and contact tracing.
“By pushing vaccine mandates, Dr. Fauci ignores naturally acquired immunity among the COVID-recovered, of which there are more than 45 million in the United States,” the authors wrote. “Mounting evidence indicates that natural immunity is stronger and longer lasting than vaccine-induced immunity.”
Kulldorff and Bhattacharya cited a study from Israel, which concluded the vaccinated were 27 times more likely to get symptomatic COVID than the unvaccinated who had recovered from a prior infection.
They pointed out that the scientific community has known about natural immunity from disease “at least since the Athenian Plague in 430 BC.”
On Fauci’s dictates to mandate the vaccine for healthcare workers, the two argued: “Under Fauci’s mandates, hospitals are firing heroic nurses who recovered from COVID they contracted while caring for patients. With their superior immunity, they can safely care for the oldest and frailest patients with even lower transmission risk than the vaccinated.”
On school closures they wrote: “Considering the devastating effects of school closures on children, Dr. Fauci’s advocacy for school closures may be the single biggest mistake of his career … While children do get infected, their risk for COVID death is minuscule, lower than their already low risk of dying from the flu.”
Kulldorff and Bhattacharya pointed to Sweden, noting that during the 2020 spring wave of COVID, the country kept daycare and schools open for all 1.8 million children ages 1 to 15, with no masks, testing or social distancing.
According to the authors, Sweden’s strategy resulted in “zero COVID deaths among children and a COVID risk to teachers lower than the average of other professions.”
The authors argued contact tracing “was a hopeless waste of valuable public health resources that did not stop the disease,” and that Fauci failed at protecting the vulnerable.
“After more than 700,000 reported COVID deaths in America, we now know that lockdowns failed to protect high-risk older people,” they said.
On collateral public health damage, they argued that a “fundamental public health principle is that health is multidimensional; the control of a single infectious disease is not synonymous with health.”
They wrote that Fauci: “ … failed to properly consider and weigh the disastrous effects lockdowns would have on cancer detection and treatment, cardiovascular disease outcomes, diabetes care, childhood vaccination rates, mental health and opioid overdoses, to name a few. Americans will live with — and die from — this collateral damage for many years to come.”
In private conversations, Kulldorff and Bhattacharya said, most of their scientific colleagues agree with them on these points but few have spoken up out of fear of “financial censorship.”
“Many are afraid of losing positions or research grants, aware that Dr. Fauci sits on top of the largest pile of infectious disease research money in the world,” they wrote.
In his forthcoming book, “The Real Anthony Fauci,” Robert F. Kennedy, Jr. includes a comprehensive discussion of Fauci’s influence and power over the scientific community, revealing how Fauci uses the “financial clout at his disposal to wield extraordinary influence over hospitals, universities, journals and thousands of influential doctors and scientists — whose careers and institutions he has the power to ruin, advance or reward.” Kennedy’s book is due out Nov. 16.
Jeremy Loffredo is a freelance reporter for The Defender. His investigative reporting has been featured in The Grayzone and Unlimited Hangout. Jeremy formerly produced news programs at RT America.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Biden blames Russia & OPEC for high oil and gas prices in US
RT | November 3, 2021
President Joe Biden has called out Russia and OPEC countries for causing US energy prices to rise, even as he implements policies to curtail domestic oil and natural gas production.
“If you take a look at, you know, gas prices and you take a look at oil prices, that is a consequence of, thus far, the refusal of Russia or the OPEC nations to pump more oil,” Biden told reporters on Tuesday at the COP26 climate summit in Scotland. “We’ll see what happens on that score sooner than later,” he added.
Prices for the leading US crude benchmark, West Texas Intermediate (WTI), have surged to around $84 per barrel from $48 per barrel since the beginning of 2021, contributing to the nation’s highest inflation rate in 13 years. Gasoline prices are at a seven-year high. The key natural gas benchmark, Henry Hub, is nearing $6/mmBtu in Nymex futures trading after starting the year below $2.50/mmBtu.
While the president pointed the finger at Russia and OPEC for failing to help bring down oil prices, he said that inflation more broadly is being spurred by the Covid-19 pandemic’s impact on supply chains. US Transportation Secretary Pete Buttigieg said on Sunday that the supply-chain woes will continue until the pandemic ends.
The Biden administration called on OPEC in August to help bring oil prices down, raising the ire of major US producers, who argued that he should be encouraging higher domestic supplies.
The day he took office in January, Biden revoked a federal permit for a new pipeline needed to bring more Canadian oil to US refiners. A week later, he suspended the leasing of new oil and gas properties on federal lands and waters as part of his plan to slash reliance on fossil fuels.
The US surpassed Russia and Saudi Arabia as the world’s largest crude producer in 2018 and became the third-biggest exporter of liquefied natural gas in 2019. That same year, the country achieved net energy independence for the first time since the 1950s – reaching a goal that many observers thought impossible.
But US oil and gas output stumbled last year amid the Covid-19 pandemic, and domestic volumes are projected to decline again in 2021.
CDC Advisors Unanimously Endorse Pfizer’s COVID Vaccine for Kids 5-11 Despite Expert Concerns Over Clinical Data
By Megan Redshaw | The Defender | November 2, 2021
The Centers for Disease Control and Prevention’s (CDC) vaccine advisory panel today unanimously recommended Pfizer’s COVID vaccine for children 5 to 11, despite concerns raised during the meeting about Pfizer’s clinical data, the fact that children who previously acquired natural immunity to COVID were included in clinical trials and evidence showing COVID poses little risk to children.
If Dr. Rochelle Walensky, the CDC’s director signs off on the decision, children ages 5 through 11 could start receiving COVID vaccines as early as tonight.
The younger age group will receive one-third of the dose authorized for those 12 and older in two shots at least three weeks apart. The doses will be delivered by smaller needles and stored in smaller vials to avoid a mix-up with adult doses.
The CDC’s guidelines for the vaccine’s use are not legally binding, but heavily influence the medical community’s practice.
Prior to today’s decision by the CDC’s Advisory Committee on Immunization Practices (ACIP) the Biden administration enlisted more than 20,000 pediatricians, family doctors and pharmacies to administer the vaccines — with 15 million doses already packed with dry ice, loaded into small specialized containers and shipped via airplanes and trucks to vaccination sites across the country, federal officials said on Monday.
Walensky sent a clear signal during the ACIP meeting about where she stands, CNN reported. “We have been asking when we will be able to expand this protection to our younger children,” Walensky said in opening comments to the committee.
“As you review the data today, it will be key to keep in mind the specific risks to children from this virus and the pandemic, and to put that risk into context of other vaccine-preventable diseases,” Walensky said.
Walensky noted that children are routinely vaccinated against diseases like chickenpox — which results in far fewer hospitalizations and deaths in children compared to COVID.
During today’s meeting, ACIP members reviewed and discussed the science behind the U.S. Food and Drug Administration’s (FDA) authorization last week of Pfizer’s COVID vaccine in all children 5-11 years old.
That authorization was based mostly on a Pfizer-BioNTech study of 4,600 children worldwide, of whom approximately 3,100 got the low-dose vaccine and about 1,500 got a placebo.
These studies showed the vaccine is about 91% effective against COVID. The immune system response to the vaccine, as measured by antibodies, was comparable to the response seen in 16- to 25-year-olds, NPR reported.
During the meeting, the CDC said 745 children under 18 have died of COVID since the beginning of the pandemic — although the COVID-19 team admitted 79% were confirmed to be hospitalized for COVID, while the rest were hospital admissions for other causes.
“The chance that a child will have severe COVID, require hospitalization or develop a long-term complication like MIS-C [multisystem inflammatory syndrome] remains low, but still the risk is too high and too devastating to our children, and far higher than for many other diseases for which we vaccinate children,” Walensky said.
Efficacy of Pfizer’s COVID vaccine in children
The CDC said Pfizer’s COVID vaccine was 90.9% effective against symptomatic COVID and none of the adverse events experienced during clinical trials were assessed by “the investigator” as related to the vaccine.
To determine the efficacy of the Pfizer-BioNTech COVID vaccine, Pfizer measured the blood of 264 children for antibodies.
“There were 3,000 vaccinated children in the trial. Why isn’t blood from the other 2,700-plus being measured for antibodies?” asked Dr. Meryl Nass, a member of the Children’s Health Defense Scientific Advisory Panel.
“Pfizer never explains why, when they have an important clinical trial in which over 3,000 children were injected in this age group, only a subset of less than 10% were used to assess efficacy,” Nass said.
Nass explained:
“Pfizer claims three cases of COVID in the vaccinated group versus 16 in the placebo group show efficacy of the vaccine. But the FDA did not accept this claim. Note that all cases were mild, none hospitalized or died. So are they planning to vaccinate 28 million kids to prevent colds?”
Nass noted Pfizer also enrolled kids who had prior evidence of having had COVID in the clinical trial, “which should never have been allowed.”
“Of the kids who were already immune at the start of the trials, none developed COVID,” Nass said. “About 150 kids in the placebo group were recovered and none got COVID.”
Nass said kids with preceding COVID infection did not have their antibody levels checked after the first dose, as Pfizer stated they did not collect the data because they “tried to minimize blood draws in children.”
“The real reason they did not want to collect data is because it might support the fact that kids who already had COVID might only need one vaccine dose, or none at all,” Nass said.
During the brief public comment session, Patricia Neuenschwander, a registered nurse noted there was no prevention of hospitalization, death or multisystem inflammatory syndrome in children — a condition being used to justify vaccinating younger children against COVID, despite numerous cases of MIS-C having been reported after receipt of a COVID vaccine.
Neuenschwander reminded the ACIP that vaccinations do not prevent infection or transmission. It is a mild illness in the vast majority of children, she said, and prior immunity is being ignored — the expansion group was only followed for 17 days.
David Wiseman, a research scientist with a background in pharmacy, pharmacology and experimental pathology, asked the CDC panel why the efficacy study was not validated by the FDA, and why Pfizer changed the buffer [see page 14] in the vaccine but did not test it in animals or kids — planning to use an untested version of the vaccine in 5 to 11-year-olds.
Wiseman said the FDA abandoned its responsibility, and he asked if the ACIP would do the same.
Myocarditis and COVID in 5- to 11-year-olds
One side effect that generated considerable discussion at today’s meeting was myocarditis — a form of heart inflammation.
The CDC said 1,640 cases of myocarditis have been reported to the CDC’s Vaccine Adverse Event Reporting System in people under age 30 after having received a COVID vaccine, but only 877 met the CDC’s case definition.
The CDC said there were nine reported deaths in people with myocarditis, but then the agency reduced the number to three, with two cases pending evaluation and one case without adequate information.
“I have to say that it is beyond belief that CDC could whittle down 877 cases reported in young people to three actual cases. Where did the rest go?” Nass asked.
“According to the CDC’s Vaccine Safety Datalink, 7 of 16 12- to 17-year-olds with myocarditis were still on exercise restriction three months after diagnosis — that is 44% could not exercise three months later,” Nass said. “This is huge.”
Nass further noted 25% of 250 myocarditis cases were still symptomatic at three months, and only 74% of cases were designated by cardiologists as definitely resolved at 3 months.
As it pertains to safety, some who testified during a public comment period, as well as other commentators, questioned whether the study used by the FDA to grant Emergency Use Authorization is large enough to assure parents that the vaccine is safe in young children.
“The bottom line is getting COVID, I think, is much riskier to the heart than getting this vaccine,” said Dr. Matthew Oster, a pediatric cardiologist at Children’s Hospital of Atlanta.
Dr. Tom Shimabukuro covered vaccine safety monitoring from the CDC’s surveillance system in children. Shimabukuro said COVID is getting the “most intensive vaccine monitoring program in history,” yet he did not go into detail on surveillance data.
Acknowledging that some parents are hesitant about vaccinating their children right away, Dr. Matthew Daley, a member of the ACIP said, “we hear you loud and clear and of course you only want what’s best for your child. I encourage you to talk to your family physician or pediatrician, they can walk through this with you.”
Megan Redshaw is a freelance reporter for The Defender. She has a background in political science, a law degree and extensive training in natural health.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
The EU is not revealing the details of its contracts with vaccine makers. Why?
By Robert Bridge | RT | November 3, 2021
As some Europeans continue to resist mandatory vaccine measures, a group of parliamentarians have upbraided the Commission for allowing pharmaceutical companies to ‘run roughshod over democracy.’
One of the most important lessons people learn early in life is to never plunk down hard-earned cash on a product before reading all of the fine print contained in the contract. ‘Caveat emptor,’ as every subject of the Roman Empire instinctively understood.
Yet, it seems that few bureaucrats in Brussels have purchased a new home, used car or some newfangled device lately, because that’s exactly what these bumbling fools have done. In an effort to ‘protect the health of their constituents,’ they bought millions of batches of Covid vaccines from various pharmaceutical companies without letting lawmakers sneak a peek at the contracts.
As it turns out, entire pages of these documents – the few that have been made public, that is – have been heavily redacted. This has raised more than one eyebrow in the European Union, and perhaps none more conspicuously than that of Romanian MEP Cristian Terhes.
At the weekend, Terhes appeared at a press conference in Brussels with several other EU lawmakers at this side, all visibly shaken by the news that they would be required to produce, starting on November 3, a digital ‘green pass’ to gain entry into Parliament. Like many EU citizens, these lawmakers have declined to get the vaccine not because they are ‘anti-vaxxers’ but because they have been denied critical information regarding the product and procedures. Now they will be refused entry into Parliament, the place where the will of their people is (supposedly) represented.
Terhes revealed that, back in January, EU lawmakers were demanding “full access to the contracts signed between these companies that produce the vaccines and the European Union.” To say the parliamentarians were disappointed would be a gross understatement.
The Romanian MEP, who represents the Christian-Democratic National Peasants Party, quoted from a Euractiv article that reported: “The contract, signed between pharmaceutical company CureVac and the European Commission in November, was made available to MEPs [on January 12, 2021] in a redacted format after the company agreed to open the contract up to scrutiny.”
That is really putting the cart before the horse, for how can something that has been so grossly redacted be opened up to scrutiny? Terhes railed that Brussels is “imposing a medical product on European citizens without them knowing what’s in these contracts.” That’s simply inexcusable and should be easily struck down by even a third-rate lawyer.
More astonishing is that not even the EU members of Parliament know the details of the agreements.
To prove his point, the Romanian MEP held up individual pages of the CureVac contract, each one heavily redacted like some kind of imitation of artist Kazimir Malevich’s ‘Black Square.’ It doesn’t get any less concerning when we drill down to which parts of the contract were blacked out. According to an analysis conducted by Euractiv, “4.22% of the liability section and 15.38% of the indemnification section was found to be redacted, while 0% of the section on the processing of personal data was redacted.”
Meanwhile, the contract’s annexes, which delve into the nitty-gritty details of the agreement, were redacted by some 61%. In total, almost 24% of the contract was hidden. Now ask yourself this simple question: Would you sign up for a home mortgage if it was discovered that one-quarter of the agreement was missing? I’ll crawl out on a limb and guess ‘no.’ Nor would anyone think you were ‘anti-mortgage’ or ‘mortgage hesitant’ if you did so.
The truth is that you, and millions of other rational people exactly like you, are simply ‘pro-transparency.’ Yet these medical consumers are being treated like second-class citizens for simply wanting more information before they agree to be injected with something. ‘My body, my choice’ is a battle cry that no longer applies, as millions of people are quickly discovering, in the current authoritarian climate.
Keep in mind that it is on the basis of these contracts that Europeans must come to a decision, based on “informed consent,” that they will ‘voluntarily’ take the jab so as not to be ostracized from polite society. Unless they agree to take one of the available vaccines, citizens of the EU face potentially being denied the right to work, enter a store, buy medicine, take their children to school and freely travel from one country to another.
Naturally, this makes the stakes for not taking the jab incredibly high, but that only makes it worse that details are being deliberately withheld from the public. It is no secret that the pharmaceutical giants enjoy full indemnity in the event that an individual suffers death or injury after receiving a Covid shot. And although such unfortunate occurrences appear to be rare, even Pfizer-BioNTech, which has been granted approval to extend vaccinations to 12 to 15-year-olds in the EU, seems uncertain as to what the long-term effects of the vaccines may be.
“Additional adverse reactions, some of which may be serious, may become apparent with more widespread use of the Pfizer-BioNTech Covid-19 Vaccine,” it clearly states on its website.
In February, the Bureau of Investigative Journalism released a damning report on Pfizer, saying negotiators for the drug company had behaved in a “bullying” manner with several Latin American countries. In Argentina they demanded “additional indemnity” against civilians seeking legal compensation after suffering adverse effects from their vaccines. In the agreements, Pfizer takes great care to ensure that all financial responsibility for compensating citizens injured from the inoculations is that of the respective government.
The company also enjoys the protection of non-disclosure agreements with many of its nation clients, including the European Commission and the US government. With regards to the EU, Brussels is forbidden from disclosing information that would be “material to Pfizer without the consent of Pfizer,” Public Citizen reported.
In fact, CureVac was being quite generous with the EU Commission, considering it was the only pharmaceutical company that agreed to release its contract to the light of day. Of course there wasn’t much to inspect with all of the redactions, but beggars can’t be choosers, right?
In light of the steady pressure bearing down on Brussels, much of it happening behind closed doors, the European Commission has obliquely admitted – almost one year too late, and after the rights and freedoms of European citizens have been crushed underfoot – that they failed to use good judgment when ramming through these emergency vaccines.
Last week, in an overwhelmingly passed resolution (458 in favor, 149 against and 86 abstaining), the EU Parliament demanded legislation that would make “the process of researching, purchasing and distributing Covid-19 vaccines more transparent, stating:
“This would enable MEPs to effectively scrutinize EU vaccine policies. At the same time, the Commission should be discussing these policies more openly with citizens.”
This shocking statement by the EU Parliament shows how little respect Brussels had for democratic principles when it was negotiating with the vaccine makers, who have, incidentally, reaped a windfall from the pandemic. The parliamentarians, who are coming under fire at home, demanded that “the Commission discloses who negotiates vaccine purchases on its behalf. It should publish purchase agreements made with vaccine suppliers, including details of public investments and vaccine costs, and publicise any potential breaches of contract.”
Then, in what comes off as the understatement of the century, the MEPs are of the opinion that “more information could help counter vaccine hesitancy and disinformation, and pharmaceutical companies should also release extensive clinical trial data and reports.”
Oh, you think so?
The following question is not an idle one: Why are MEPs ONLY NOW talking about the total lack of transparency and democracy that occurred between the EU Commission and Big Pharma? A more cynical person would be tempted to say it’s because the draconian vaccine mandates have finally reached the very door of Parliament, where the power brokers find themselves locked out of their offices, much like thousands of people on the street. Welcome to the club.
In any case, the fact that Brussels has withheld the details of its agreements with the vaccine makers for almost a year, while at the same time casually destroying the civil liberties of its citizens, totally disqualifies them from punishing those people who are ‘hesitant’ about receiving the vaccine. ‘Informed consent’ is essential to any functioning democracy, and Europeans were clearly denied that right. Do the right thing, Brussels, and release these heavy chains from your people. The world is watching.
Robert Bridge is an American writer and journalist. He is the author of ‘Midnight in the American Empire,’ How Corporations and Their Political Servants are Destroying the American Dream.
Journalists’ unions seek ICC probe into systematic targeting of Palestinian journalists
![Israeli soldiers shoot tear gas near reporters as they disperse Palestinian protesters on July 31, 2021 [JAAFAR ASHTIYEH/AFP via Getty Images]](https://i1.wp.com/www.middleeastmonitor.com/wp-content/uploads/2021/11/GettyImages-1234355773-scaled-e1635944533233.jpg?resize=1200%2C799&quality=85&strip=all&zoom=1&ssl=1)
Israeli soldiers shoot tear gas near reporters as they disperse Palestinian protesters on July 31, 2021 [JAAFAR ASHTIYEH/AFP via Getty Images]
MEMO | November 3, 2021
There are “strong grounds” to conclude that Israel’s systematic targeting of journalists working in Palestine and its failure to properly investigate killings of media workers amount to war crimes, a complaint being submitted to the International Criminal Court (ICC) will say.
The International Federation of Journalists (IFJ), working with the Palestinian Journalists’ Syndicate (PJS) and the International Centre of Justice for Palestinians (ICJP), has asked Bindmans and Doughty Street Chambers to submit a complaint to the ICC detailing “the systematic targeting of Palestinian journalists on behalf of four named victims – Ahmed Abu Hussein, Yaser Murtaja, Muath Armaneh, and Nedal Eshtayet – who were killed or maimed by Israeli snipers while covering demonstrations in Gaza. All were wearing clearly marked PRESS vests at the time they were shot.”
“At least 46 journalists have been killed since 2000 and no one has been held to account,” the IFJ said in a statement on its website.
The complaint will also include the “bombing of the Al-Shorouk and Al-Jawhara Towers in Gaza City in May 2021″.
IFJ General Secretary Anthony Bellanger said: “The targeting of journalists and media organisations in Palestine violates the right to life and freedom of expression. These crimes must be fully investigated. This systematic targeting must stop. The journalists and their families deserve justice.”
America’s dramatic rise in ‘hate crimes’ has a surprisingly logical explanation
By Frank Furedi | RT | November 3, 2021
The gubernatorial election in Virginia saw another example of a ‘racism hoax’ that caused media outrage before the truth emerged. It’s little wonder these stunts are becoming more common in a country fixated on identity politics.
At a time when the mere hint of a badly worded sentence invites accusations of racism, many race entrepreneurs feel incentivised to fabricate claims of incidents that can provoke howls of outrage.
This week’s election for the post of governor of Virginia saw just how the phenomenon of a race hoax works. Supporters of the Lincoln Project – an anti-Trump advocacy group – dressed up as Neo-Nazi white supremacists and, clutching tiki torches, photographed themselves next to the campaign bus of the Republican candidate, Glenn Youngkin. Chanting “we’re all in for Glenn,” they sought to promote the impression that a vote for Youngkin was a vote for racial hatred.
The hoax provoked the intended reaction of outrage. “To my fellow Virginia residents,” tweeted NBC’s legal analyst, Glenn Kirschner, “please vote against this blatant display of racism, hatred and intolerance. Please vote FOR a kind, welcoming, diverse Virginia. Please vote @TerryMcAuliffe for governor. Because #JusticeMatters.” The tweet was subsequently deleted.
The Lincoln Project’s dirty trick soon got the Jewish Democratic Council of America on board. It published a tweet – also subsequently deleted – demanding that Youngkin condemn the tiki torchbearers or risk being denounced for endorsing anti-Semitism.
More broadly, Democrats were quick to exploit the performance of the Lincoln Project as an illustration that their opponents’ political base was steeped in white supremacy. America’s cultural fixation with race means that they are primed to perceive episodes of racism in the most innocuous of settings. The race hoax perpetrated by the Lincoln Project was designed to feed the American media’s voracious appetite for sensational incidents of hate crimes.
In recent times, the most widely reported alleged race hoax involved the black American actor Jussie Smollett, who claimed he was assaulted in the early hours of the morning in Chicago by two men wearing MAGA hats. He insisted that he was subjected to homophobic and racial slurs and that some unknown chemical substance was poured on him and a noose tied around his neck.
Smollett’s account of this ‘lynching’ provoked anger, and numerous well-known public figures – including the now-Vice President Kamala Harris – lined up to demonstrate their support. Once the police discovered that Smollett apparently made up the attack – he is facing a criminal case – an embarrassed media moved on to find other instances of hate crime.
As it happens, the manufacturing of a race hoax is far from a rare event. Inventing victimhood is not uncommon, particularly within higher education. For example, in September 2017, five black students at the US Air Force Academy Preparatory School discovered racial slurs written on their doors. An investigation later found that one of the students supposedly targeted was responsible for the vandalism.
In his book, ‘Hate Crime Hoax: How the Left is Selling a Fake Race War’, published in 2019, Wilfred Reilly examined over 100 high-profile incidents of so-called hate crimes that never actually occurred. He pointed out that he was “able to rather easily assemble a data set of 409 hate hoax cases,” concentrated heavily in the previous five years. According to Reilly, his data set has since swelled to become a list of 608 unique hate hoax case studies, containing more than 800 individual incidents of hoaxes.
The fake reporting of hate crimes is encouraged by the singular focus of criminal justice agencies on this issue. In effect, hate crime has turned into a political weapon used to promote the dogma of systemic racism. The eagerness with which claims of hate crime are publicised to prove a point has created an incentive to present oneself as its victim. The proliferation of the phenomenon of race hoax is the inexorable consequence of cultural attitudes that perceive the world through the prism of racism.
The constant obsession with white privilege, whiteness, and systemic racism has created a cultural terrain that is hospitable to the flourishing of race hoaxes.
So, next time you hear that racism is on the rise and society is facing an epidemic of hate crime, take a reality check – because it may turn out that what is at issue is an epidemic of fake news.
Frank Furedi is an author and social commentator. He is an emeritus professor of sociology at the University of Kent in Canterbury. Author of How Fear Works: The Culture of Fear in the 21st Century.
The News is being Nudged
A joint report from Sky and the UK government’s Nudge Unit reveals a startling collaboration
By Laura Dodsworth | November 2, 2021
propaganda, n
The systematic dissemination of information, esp. in a biased or misleading way, in order to promote a political cause or point of view.
– Oxford English Dictionary
Is the news still news when it is being nudged by the UK government’s behavioural scientists?
Sky announced this week that behaviour change on climate can be driven by TV. It released a video which opened with the lines, “We cannot understate the urgency. But faced with issues of such enormity, what role can we play?”
It’s not actually a question, they have already decided their role. Sky announced that it was collaborating with the “independent Behavioural Insights Team”. That sounds more palatable than collaborating with the government doesn’t it? But the Behavioural Insights Team (BIT) is one third owned by the Cabinet Office and appears to be on permanent tenure at Downing Street. Can a company which is one third owned by the government be fairly described as “independent”?
BIT’s report The Power of TV: Nudging Viewers to Decarbonise their Lifestyles makes a number of startling admissions.
“Behaviour change via broadcasting and traditional media has historically been aimed at improving public health, boosting gender equality, and reducing violence. Imagine the potential for emissions reductions if the same methods were used to encourage sustainable behaviours!”
The key word is “historical”. If you have ever suspected that social and political issues were being confected somewhat artificially in TV programming, you were right. This is an admission of social engineering.
According to a joint survey by Sky and BIT, 70% of people across Europe are willing to change their behaviour to address the climate crisis and 80% support TV broadcasters ‘nudging’ viewers to think about the environment, whether that’s through documentaries, advertising or increasing the coverage of environmental issues in the news.
Climate policy is a tricky nut to crack – persuading us to have under-performing and expensive boilers, asking us to switch insects for meat, stop taking foreign holidays and drive our cars less is going to be a hard sell. So the nudgers are going to use the telly box to persuade the recalcitrant masses.
The survey itself uses ‘social conformity’. Ah, you are supposed to think, if 80% of people think TV programming should be used to ‘nudge’ us, then that’s what I think too. Notoriously, however, there is a gap between what people say they want in surveys and what they actually want. The ultimate proof will be in behaviour and ratings.
The report states that broadcasters and content creators have a “unique opportunity to make a difference for the planet”. (I wonder what difference it would make if Sky’s CEO stopped commuting transatlantically by private jet?)
According to the report, the British public are unwilling to take supposedly “high impact” actions, such as eating less meat and dairy, switching to electric vehicles, using public transport, and switching to green pensions.
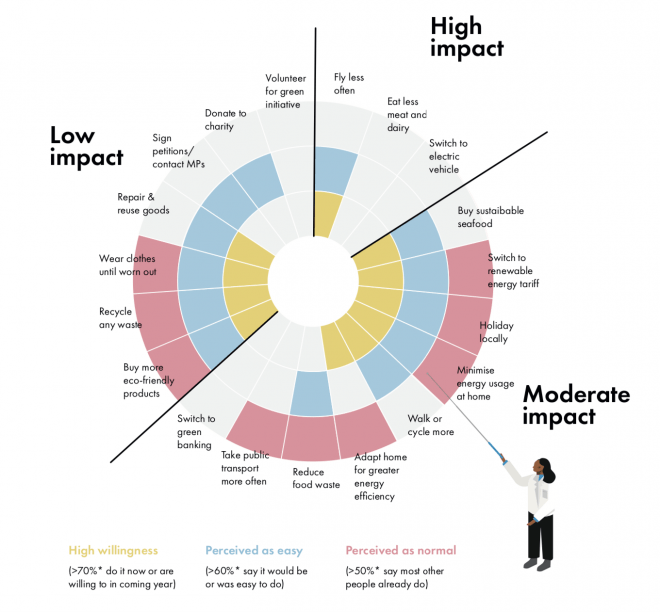
The Power of TV: Nudging Viewers to Decarbonise their Lifestyles
The report is audaciously bossy about how broadcasters and content creators should change the British public’s behaviour.
Advice such as “Frequency of exposure to green themes could be enhanced by building ecological beliefs and traits into core characters within a show so that green issues can fluently be raised time and time again,” sounds potentially tedious.
You will see fewer characters “carelessly drinking from a plastic bottle”. But you will see more kids programming centre on green issues to influence you as well as the kids to promote “intergenerational spillover”.
Suggestions continue with “a family could discuss reducing their waste” in a comedy show. Making that funny is quite the gauntlet throw. News segments could “explore barriers to acting green and share stories for overcoming them,” which doesn’t sound particularly newsworthy. An episode of a drama could include references to buying an electric vehicle and, of course, characters should order vegetarian options in restaurants.
Plump the cushions, grab a cuppa and get ready for the green themes in your favourite psyopera, I mean soap opera. During COP26, storylines are converging on the environment. Soap ratings have diminished over the years and is it any wonder? People don’t want to be preached to. Creativity cannot be programmed and storytelling is an art. It is naïve arrogance to believe this sort of technocratic tinkering will engage viewers. We gravitate to good stories.
Mercifully, BIT suggests that broadcasters “avoid a negative tone” and warns that “fear-mongering, guilt-tripping, blaming, or preaching can be counter-productive.” (I wonder if a certain book had an impact?)
In addition to Sky, another eleven major UK media brands, including the BBC, ITV, Channel 4, RTE, Britbox and Discovery, have pledged to increase the amount and “quality” of their climate coverage. So expect the airwaves to be flooded with the techniques suggested in the BIT report. At the same time, expect very little media scrutiny of this astonishing collaboration between nudgers and newscasters. And in print and online, the BBC, The Guardian, The Times and the Financial Times have added specific climate sections to their news.
A few months after the publication of A State of Fear, a government advisor told me that the behavioural scientists are “very pleased with themselves” and “Britain is seen as leading the way in how to manipulate people. There is skipping in Whitehall corridors. The public have been proved to be incredibly sheepish, so there’s more nudge coming.” And so there is.
My book concluded that the UK government’s use of behavioural science during the Covid epidemic lacked transparency and was anti-democratic. BIT’s report might appear to rebut both accusations. Don’t be fooled. It rests upon a survey which says people want to be nudged through the media. But research conducted by biased and vested parties is not a substitute for a democratic mandate. The British public never voted for or consented to the creation of a Nudge Unit to subliminally influence them and then set the news agenda. Furthermore, when behavioural scientists – and by extension the government – influence the news, it risks the inquiry, debate and balance that the media owes the public.
Whatever you believe about climate, or Covid-19, or any other agenda, can any mental contortions justify the news being nudged? We would criticise such blatant propaganda if it happened in any other country and we should not tolerate here. We should switch it off.
What is the Number Needed to Vaccinate to prevent a single COVID fatality in kids 5 to 11 based on Pfizer’s EUA application?
And what are the risks that go along with injecting that many kids?
By Toby Rogers | October 31, 2021
Number Needed to Vaccinate (NNTV), the standard policy tool that Pharma, the FDA, & CDC no longer want to talk about
A funny thing happened this afternoon. Not funny as in “haha”. More like funny as in, “ohhhhh that’s how the FDA rigs the process.”
I was reading the CDC’s “Guidance for Health Economics Studies Presented to the Advisory Committee on Immunization Practices (ACIP), 2019 Update” and I realized that the FDA’s woeful risk-benefit analysis in connection with Pfizer’s EUA application to jab children ages 5 to 11 violates many of the principles of the CDC’s Guidance document. The CDC “Guidance” document describes 21 things that every health economics study in connection with vaccines must do and the FDA risk-benefit analysis violated at least half of them.
Today I want to focus on a single factor: the Number Needed to Vaccinate (NNTV). In four separate places the CDC Guidance document mentions the importance of coming up with a Number Needed to Vaccinate (NNTV). I did not recall seeing an NNTV in the FDA risk-benefit document. So I checked the FDA’s risk-benefit analysis again and sure enough, there was no mention of an NNTV.
Because the FDA failed to provide an NNTV, I will attempt to provide it here.
First a little background. The Number Needed to Treat (NNT) in order to prevent a single case, hospitalization, ICU admission, or death, is a standard way to measure the effectiveness of any drug. It’s an important tool because it enables policymakers to evaluate tradeoffs between a new drug, a different existing drug, or doing nothing. In vaccine research the equivalent term is Number Needed to Vaccinate (NNTV, sometimes also written as NNV) in order to prevent a single case, hospitalization, ICU admission, or death (those are 4 different NNTVs that one could calculate).
Pharma HATES talking about NNTV and they hate talking about NNTV even more when it comes to COVID-19 vaccines because the NNTV is so ridiculously high that this vaccine could not pass any honest risk-benefit analysis.
Indeed about a year ago I innocently asked on Twitter what the NNTV is for coronavirus vaccines.
Pharma sent a swarm of trolls in to attack me and Pharma goons published hit pieces on me outside of Twitter to punish me for even asking the question. Of course none of the Pharma trolls provided an estimate of the NNTV for COVID-19 shots. That tells us that we are exactly over the target.
Various health economists have calculated a NNTV for COVID-19 vaccines.
- Ronald Brown, a health economist in Canada, estimated that the NNTV to prevent a single case of coronavirus is from 88 to 142.
- Others have calculated the NNTV to prevent a single case at 256.
- German and Dutch researchers, using a large (500k) data set from a field study in Israel calculated an NNTV between 200 and 700 to prevent one case of COVID-19 for the mRNA shot marketed by Pfizer. They went further and figured out that the “NNTV to prevent one death is between 9,000 and 100,000 (95% confidence interval), with 16,000 as a point estimate.”
You can see why Pharma hates this number so much (I can picture Pharma’s various PR firms sending out an “All hands on deck!” message right now to tell their trolls to attack this article). One would have to inject a lot of people to see any benefit and the more people who are injected the more the potential benefits are offset by the considerable side-effects from the shots.
Furthermore, the NNTV to prevent a single case is not a very meaningful measure because most people, particularly children, recover on their own (or even more quickly with ivermectin if treated early). The numbers that health policy makers should really want to know are the NNTV to prevent a single hospitalization, ICU admission, or death. But with the NNTV to prevent a single case already so high, and with significant adverse events from coronavirus vaccines averaging about 15% nationwide, Pharma and the FDA dare not calculate an NNTV for hospitalizations, ICU, and deaths, because then no one would ever take this product (bye bye $93 billion in annual revenue).
Increased all cause mortality in the Pfizer clinical trial of adults
As Bobby Kennedy noted in personal correspondence with me, Pfizer’s clinical trial in adults showed alarming increases in all cause mortality in the vaccinated :
In Pfizer’s 6 month clinical trial in adults — there was 1 covid death our of 22,000 in the vaccine (“treatment”) group and 2 Covid deaths out of 22,000 in the placebo group (see Table s4). So NNTV = 22,000. The catch is there were 5 heart attack deaths in the vaccine group and only 1 in placebo group. So for every 1 life saved from Covid, the Pfizer vaccine kills 4 from heart attacks. All cause mortality in the 6 month study was 20 in vaccine group and 14 in placebo group. So a 42% all cause mortality increase among the vaccinated. The vaccine loses practically all efficacy after 6 months so they had to curtail the study. They unblinded and offered the vaccine to the placebo group. At that point the rising harm line had long ago intersected the sinking efficacy line.
Former NY Times investigative reporter Alex Berenson also wrote about the bad outcomes for the vaccinated in the Pfizer clinical trial in adults (here). Berenson received a lifetime ban from Twitter for posting Pfizer’s own clinical trial data.
Pfizer learned their lesson with the adult trial and so when they conducted a trial of their mRNA vaccine in children ages 5 to 11 they intentionally made it too small (only 2,300 participants) and too short (only followed up for 2 months) in order to hide harms.
Estimating an NNTV in children ages 5 to 11 using Pfizer’s own clinical trial data
All of the NNTV estimates above are based on data from adults. In kids the NNTV will be even higher (the lower the risk, the higher the NNTV to prevent a single bad outcome). Children ages 5 to 11 are at extremely low risk of death from coronavirus. In a meta-analysis combining data from 5 studies, Stanford researchers Cathrine Axfors and John Ioannidis found a median infection fatality rate (IFR) of 0.0027% in children ages 0-19. In children ages 5 to 11 the IFR is even lower. Depending on the study one looks at, COVID-19 is slightly less dangerous or roughly equivalent to the flu in children.
So how many children would need to be injected with Pharma’s mRNA shot in order to prevent a single hospitalization, ICU admission, or death?
Let’s examine Pfizer’s EUA application and the FDA’s risk-benefit analysis. By Pfizer’s own admission, there were zero hospitalization, ICU admissions, or deaths, in the treatment or control group in their study of 2,300 children ages 5 to 11.
So the Number Needed to Vaccinate in order to prevent a single hospitalization, ICU admission, or death, according to Pfizer’s own data, is infinity. ∞. Not the good kind of infinity as in God or love or time or the universe. This is the bad kind of infinity as in you could vaccinate every child age 5 to 11 in the U.S. and not prevent a single hospitalization, ICU admission, or death from coronavirus according to Pfizer’s own clinical trial data as submitted to the FDA. Of course Pfizer likes this kind of infinity because it means infinite profits. [Technically speaking the result is “undefined” because mathematically one cannot divide by zero, but you get my point.]
Estimating an NNTV and risk-benefit model in children ages 5 to 11 using the limited data that are available
Everyone knows that Pfizer was not even trying to conduct a responsible clinical trial of their mRNA shot in kids ages 5 to 11. Pfizer could have submitted to the FDA a paper napkin with the words “Iz Gud!” written in crayon and the VRBPAC would have approved the shot. They are all in the cartel together and they are all looking forward to their massive payoff/payday.
But let’s not be like Pharma. Instead, let’s attempt to come up with a best guess estimate based on real world data. Over time, others will develop a much more sophisticated estimate (for example, Walach, Klement, & Aukema, 2021 estimated an NNTV for 3 different populations based on “days post dose”). But for our purposes here I think there is a much easier way to come up with a ballpark NNTV estimate for children ages 5 to 11.
Here’s the benefits model:
- As of October 30, 2021, the CDC stated that 170 children ages 5 to 11 have died of COVID-19-related illness since the start of the pandemic. (That represents less than 0.1% of all coronavirus-related deaths nationwide even though children that age make up 8.7% of the U.S. population).
- The Pfizer mRNA shot only “works” for about 6 months (it increases risk in the first month, provides moderate protection in months 2 through 4 and then effectiveness begins to wane, which is why all of the FDA modeling only used a 6 month time-frame). So any modeling would have to be based on vaccine effectiveness in connection with the 57 (170/3) children who might otherwise have died of COVID-related illness during a 6-month period.
- At best, the Pfizer mRNA shot might be 80% effective against hospitalizations and death. That number comes directly from the FDA modeling (p. 32). I am bending over backwards to give Pfizer the benefit of considerable doubt because again, the Pfizer clinical trial showed NO reduction in hospitalizations or death in this age group. So injecting all 28,384,878 children ages 5 to 11 with two doses of Pfizer (which is what the Biden administration wants to do) would save, at most, 45 lives (0.8 effectiveness x 57 fatalities that otherwise would have occurred during that time period = 45).
- So then the NNTV to prevent a single fatality in this age group is 630,775 (28,384,878 / 45). But it’s a two dose regimen so if one wants to calculate the NNTV per injection the number doubles to 1,261,550. It’s literally the worst NNTV in the history of vaccination.
If you inject that many children, you certainly will have lots and lots of serious side effects including disability and death. So let’s look at the risk side of the equation.
Here’s the risk model:
- Because the Pfizer clinical trial has no useable data, I have to immuno-bridge from the nearest age group.
- 31,761,099 people (so just about 10% more people than in the 5 to 11 age bracket) ages 12 to 24 have gotten at least one coronavirus shot.
- The COVID-19 vaccine program has only existed for 10 months and younger people have only had access more recently (children 12 to 15 have had access for five months; since May 10) — so we’re looking at roughly the same observational time period as modeled above.
- During that time, there are 128 reports of fatal side effects following coronavirus mRNA injections in people 12 to 24. (That’s through October 22, 2021. There is a reporting lag though so the actual number of reports that have been filed is surely higher).
- Kirsch, Rose, and Crawford (2021) estimate that VAERS undercounts fatal reactions by a factor of 41 which would put the total fatal side effects in this age-range at 5,248. (Kirsch et al. represents a conservative estimate because others have put the underreporting factor at 100.)
- With potentially deadly side effects including myo- and pericarditis disproportionately impacting youth it is reasonable to think that over time the rate of fatal side effects from mRNA shots in children ages 5 to 11 might be similar to those in ages 12 to 24.
So, to put it simply, the Biden administration plan would kill 5,248 children via Pfizer mRNA shots in order to save 45 children from dying of coronavirus.
For every one child saved by the shot, another 117 would be killed by the shot.
The Pfizer mRNA shot fails any honest risk-benefit analysis in children ages 5 to 11.
Even under the best circumstances, estimating NNTV and modeling risk vs. benefits is fraught. In the current situation, with a new and novel bioengineered virus, where Pfizer’s data are intentionally underpowered to hide harms, and the FDA, CDC, & Biden Administration are doing everything in their power to push dangerous drugs on kids, making good policy decisions is even more difficult.
If the FDA or CDC want to calculate a different NNTV (and explain how they arrived at that number) I’m all ears. But we all know that the FDA refused to calculate an NNTV not because they forgot, but because they knew the number was so high that it would destroy the case for mRNA vaccines in children this age. Your move CDC — your own Guidance document states that you must provide this number.
Featured Video

Alexander Mercouris: NATO Will Soon Panic & Risk War with Russia
or go to
Aletho News Archives – Video-Images
From the Archives
Remembering Fallujah: The War Crimes Committed under Command of Jim Molan and Jim Mattis
Defending Australian Values in Iraq
By David Macilwain | American Herald tribune | February 8, 2018
Ross Caputi, a former Marine who was “witness and accomplice to the atrocities” committed in Fallujah in November 2004 during “Operation Phantom Fury”, wrote this about his unit’s entry into the city:
Perhaps it was just too painful of a realization for many of us to make, because we saw ourselves as the liberators, the good guys, and to admit that we were hurting innocent people would have contradicted everything that we claimed to stand for. I can only speculate about what the motives were for the people who dreamed up that mission and decided to make the people of Fallujah flee into the desert. Was it also too painful for the decision makers to admit to themselves that we were hurting innocent people? Or were they so evil that they just did not care who we were hurting? Whatever their reasons for doing it were, the fact of the matter is that our entire command was aware that we had forced the majority of the city’s population, about 200,000 people, into refugee status, but nobody took responsibility for their wellbeing, as international law required of us.
Central to that command was Major General Andrew “Jim” Molan, an Australian who was seconded to the US military in 2004 and took overall command of US coalition forces in Iraq, alongside the current US defence secretary Jim Mattis.
What happened in the so-called “second battle of Falluja” however, went far beyond a failure to attend to the needs of the civilian population who were able to flee the city before the US assault. Those who remained found themselves imprisoned in a “free-fire zone” for 10,500 US troops and 850 UK special forces, along with 2000 Iraqis loyal to the Occupation government in Baghdad.
While the “Battle for Falluja” has been glorified and celebrated as the most destructive and significant US battle since Vietnam, intended to be a final stand against insurgents who had become concentrated there, it has also been recognised as one of the worst war crimes committed by US coalition forces during the whole occupation of Iraq. … continue
Blog Roll
 Aletho News
Aletho News- Doctors Are Dangerous An Essay on the First Leading Cause of Death
- Ukraine attacks Iranian ship, kills sailor – Tehran
- Nablus: When the killer becomes the victim
- Beijing blacklists 14 EU firms after Brussels targets Chinese companies in latest Russia sanctions package
- Bankrupt and fraudulent: EU sanctions Russia while silent on U.S., Israeli genocide
- Iran slams EU ‘Human Rights concerns’ as sheer hypocrisy
- Fars: US evacuates bases in Qatar and UAE, satellite images show
- US CONTRADICTIONS ON IRAN EXPOSED Glenn Diesen & Lt Col Daniel Davis
- British Army faces Kenya setback amid row over troops’ crimes
- Kiev hitting civilian targets in Russia to provoke mirror response – ex-Pentagon analyst
- If Americans Knew
- McCarthyism in Massachusetts
- Israeli settlers, soldiers on a rampage in West Bank – Daily Update
- Rebuilding of Gaza to cost seven times more than all previous wars: Oxfam
- James Woolsey, front man who promoted US wars for Israel, dies at 84
- Despite Israel’s multi-million propaganda project, some anti-genocide candidates are winning
- She Was a Bright Student. An Israeli Strike Ended Her Dreams.
- US House passes $1.15 trillion military bill expanding Israel cooperation
- Gaza teeters on the edge of famine (again) – Daily Update
- ISRAELI MEDIA: ‘An Inferno’: Gazans Face Sweltering Conditions in Tent Camps for Third Summer in a Row
- Israel’s Coordinated Campaign to Propagandize Conservatives in America
- No Tricks Zone
- ECMWF Models Throwing Cold Water On Extreme Germany Heat Wave Forecast Next Week
- Greenland’s Ice Sheet Was Supposed To Be Rapidly Melting Away. It Hasn’t Been.
- Global Temperature Trend Has Cooled Over The Past 6500 Years, Scientists Have Found
- Wind Energy Means Going Back To The Middle Ages, Says German Professor Horst-Joachim Lüdecke
- New Study: A 40-Fold Increase In Earth’s Main Greenhouse Gas Contributes To Cooling The Ocean
- New Study Highlights The ‘Dominant Role’ Of Aerosol/Cloud Interactions In Shaping Climate
- Munich’s First-Ever Green Party Mayor Declares First Ever City Water Use Restrictions… Fines Up to 50,000 €!
- Experimental Lab Research: The Climate Sensitivity To A 400-Fold Increase In CO2 Is 0.1°C
- Fatal Snobbery: In France, It’s Better To Die From A Heatwave Than To Do As Americans
- New Study: NASA’s Models Wildly Underestimate The Capacity Of Clouds To Alter Solar Radiation
