Yesterday, I was listening to a classical-music station when NPR came on with the news. Addressing the controversy surrounding former President Trump’s efforts to keep secret his records relating to the January 6 protests at the Capitol, the NPR reporter referred to the “deadly attack” on the Capitol.
I immediately thought to myself, “Well, that’s certainly an interesting use of language.”
When I hear the word “attack,” I think of weapons, specifically guns, grenades, or missiles that are intended to kill people. For example, when the Pentagon fired a missile at that family in Afghanistan shortly before exiting its 20-year war in that country, I would term that an “attack” — and a “deadly attack” at that, especially given that many innocent people, including children, were killed by that missile.
One of the fascinating aspects of the “attack” on the Capitol is that the “attackers” didn’t have guns. In fact, as far as I know, they didn’t even have any swords. To me, that’s one unusual “attack.” In fact, I’ll bet that there haven’t been many other “attacks” in history in which the “attackers” failed to use weapons to commit their “attack.”
What about words? Yeah, the Capitol “attackers” certainly employed a lot of words during the course of their “attack.” Maybe that is what NPR means when it describes what happened as an “attack” — that the “attackers” were engaged in a “word attack” on the Capitol. Imagine how frightening that “attack” must have been — with “attackers” hitting one victim with some particular word — maybe “Tyrant!” — followed by some other word, perhaps “Thief!”
Now, I think you would agree with me that that would be one scary “attack”!
In fact, it was so scary that one Capitol police officer shot and killed one of the “attackers” because he was so afraid that the “attackers” were coming to get him. He wasn’t the only one who was afraid. Many members of Congress were equally terrified of the Word-Attackers.
Hey, don’t judge these people too harshly. You don’t know how you would react if a bunch of Word-Attackers were coming after you and flinging and hurling nasty words at you.
Another interesting aspect of the NPR news broadcast was the reporter’s reference to the “deadly” attack on the Capitol. Now, when I hear that someone has engaged in a “deadly” attack, I immediately think that the attackers have killed people in the course of their attack.
Yet, here, the “attackers” didn’t kill anyone. Instead, the only person killed was one of the “attackers.” Her name was Ashli Babbitt. She was shot dead by that Capitol policeman who was terrified that Babbitt and the “attackers” were coming to get him and members of Congress. It’s still not clear why he didn’t fire a warning shot over her head. If he had done that, she undoubtedly would have backed off, especially since she was unarmed, well, except for words in her vocabulary.
For a while, the news media was reporting that Capitol police officer Brian Sicknick was beaten to death by the “attackers.” For example, the New York Times reported that he “was overpowered and beaten by rioters from the mob at the Capitol.”
Could that be what NPR is referring to when it cites the “deadly” attack on the Capitol?
I don’t think so because as things turned out, what the Times reported about Sicknick turned out to be incorrect. An autopsy revealed that Sicknick died of natural causes, to wit: strokes.
The New York Times also reported that a woman named Rosanne Boyland, who was one of the “attackers,” “appears to have been killed in a crush of fellow rioters during their attempt to fight through a police line.”
Alas, what appeared to be true wasn’t. An autopsy revealed that she died of a drug overdose, not trampling.
Two other “attackers” — Kevin Greeson and Benjamin Phillips — died of a heart attack and a stroke.
Thus, five people died during the “deadly attack.” One “attacker “was killed by a terrified Capitol police officer. One Capitol police officer and two of the “attackers” died of natural causes. Another “attacker” died of a drug overdose.
Given the nature of those deaths, is it really proper to refer to the “deadly” attack on the Capitol? Doesn’t the use of the term “deadly” imply that the attackers deliberately shot or killed people as part of their “attack”?
Maybe NPR is saying that the words that the “attackers” were employing as weapons caused those people to have heart attacks, strokes, and drug overdoses. Maybe their words are what caused that police officer who killed Ashli Babbitt to become terrified.
Ironically, as far as I know, the Justice Department hasn’t charged any of the January 6 protestors with murder or even a massive conspiracy to initiate a “deadly attack” on the Capitol.What’s up with that? Those federal prosecutors need to start listening to NPR.
November 11, 2021
Posted by aletho |
Fake News, Mainstream Media, Warmongering | NPR, United States |
Leave a comment
The New York Times has obtained ‘privileged communications’ of Project Veritas founder James O’Keefe, raising suspicions that an FBI source might have leaked the newspaper confidential data obtained during recent raids.
FBI agents raided the home of Project Veritas founder James O’Keefe last Saturday as part of an investigation into the acquisition of a diary purportedly written by President Joe Biden’s daughter Ashley. On Thursday, less than a week after the raid, the New York Times published an article claiming to have obtained “internal documents” from Project Veritas’ attorney.
The article sparked outrage among conservatives, who accused the FBI of leaking private communications from the organization to the newspaper.
“The FBI raided Project Veritas on a pretext and is now leaking their privileged communications to the New York Times. This is a scandal,” tweeted lawyer and Human Events co-publisher Will Chamberlain, who called for the article’s co-author, Adam Goldman, to be “subpoenaed tomorrow and forced to reveal his criminal source.”
Chamberlain also raised further legal concerns, noting that Project Veritas “is currently in litigation with the New York Times” over a separate issue, which would make any leaks to the newspaper an even bigger scandal.
“This isn’t journalism, this is straight up theft,” he concluded.
Attorney Harmeet Dhillon – who is currently representing Project Veritas and O’Keefe – also accused the New York Times of publishing a “private, privileged correspondence” which “they have no legal right to possess,” while political commentator and lawyer Mike Cernovich wrote, “This is not a grey area. It’s black letter criminal felonies committed by the FBI and the New York Times.”
A federal court ordered the US Justice Department to stop extracting information from O’Keefe’s devices on Thursday.
The FBI took two of O’Keefe’s phones during its raid on his home and the Project Veritas founder said his devices contained confidential material, including information relating to his journalistic sources.
“This is an attack on the First Amendment by the Department of Justice,” said O’Keefe this week, adding, “I’ve heard ‘the process is the punishment.’ I didn’t really understand what that meant until this weekend.”
O’Keefe said he “wouldn’t wish” the situation “on any journalist.”
November 11, 2021
Posted by aletho |
Civil Liberties | FBI, New York Times, United States |
Leave a comment
You would assume that if the CDC was going to crush the civil and individual rights of those with natural immunity by having them expelled from school, fired from their jobs, separated from the military, and worse, the CDC would have proof of at least one instance of an unvaccinated, naturally immune individual transmitting the COVID-19 virus to another individual. If you thought this, you would be wrong.
My firm, on behalf of ICAN, asked the CDC for precisely this proof (see below). ICAN wanted to see proof of any instance in which someone who previously had COVID-19 became reinfected with and transmitted the virus to someone else. The CDC’s incredible response is that it does not have a single document reflecting that this has ever occurred. Not one. (See below.)
In contrast, there are endless documents reflecting cases of vaccinated individuals becoming infected with and transmitting the virus to others. Such as this study. And this study. And this study. And this study. It goes on and on…
But it gets worse. The CDC’s excuse for not having a shred of evidence of the naturally immune transmitting the virus is that “this information is not collected.” What?! No proof! But yet the CDC is actively crushing the rights of millions of naturally immune individuals in this country if they do not get the vaccine on the assumption they can transmit the virus. But despite clear proof the vaccinated spread the virus, the CDC lifts restrictions on the vaccinated?! That is dystopian.
The facts about natural immunity are simple. Every single peer reviewed study has found that the naturally immune have far greater than 99% protection from having COVID-19, and this immunity does not wane. In contrast, the COVID-19 vaccine provides, at best, 95% protection and this immunity wanes rapidly. I am no mathematician, but a constant 99% seems preferable to a 95% that quickly drops. And, while the vaccinated readily transmit the virus, not so for the naturally immune.
The lesson yet again is not that health authorities should never make mistakes. They will. It happens. The lesson is that civil and individual rights should never be contingent upon a medical procedure. Everyone, the naturally immune or otherwise, who wants to get vaccinated and boosted should be free to do so. But nobody should be coerced by the government to partake in any medical procedure.
FOIA Request
FOIA Response
November 11, 2021
Posted by aletho |
Aletho News | CDC, United States |
Leave a comment
In a week when the UK has seen a prominent academic forced from her post by an activist mob, the Global Warming Policy Foundation has published a new paper that describes the 15-year hounding of environmental studies professor, Roger Pielke Jr.
Professor Pielke, one of the world’s leading environmental scientists, has been a vocal supporter of decarbonisation efforts, but this has not prevented green activists from engaging in an extraordinary campaign to silence him because he refuses to support claims that extreme weather is worsening.
And he is still being hounded today, with the University of Colorado Boulder launching and then dropping an investigation of his conduct, and forcing Pielke – their most senior environmental studies professor – to move to a tiny windowless office.
The paper’s author, civil liberties journalist Donna Laframboise said:
“The hounding of Roger Pielke has been abhorrent. It is time that university administrations stood up to cancel culture and the outrage mobs.”
And Laframboise points to this week’s announcement of a new university in Austin Texas, dedicated to the cause of academic freedom:
“Universities that behave this way will lose their best people to new and independent institutions that protect free thinking.”
GWPF Director Dr Benny Peiser said:
“The witch-hunt against Roger Pielke Jr. is symptomatic of a problem that we are seeing in universities across the developed world, with activists trying to silence dissenting opinions, and with the tacit, and in many case the active, support of administrators.
“Universities need to take great care – if the public lose faith in the system, public funding and generous donations from alumni can dry up very quickly.”
Donna Laframboise: The Hounding of Roger Pielke Jr. (pdf)
November 11, 2021
Posted by aletho |
Full Spectrum Dominance, Science and Pseudo-Science, Timeless or most popular | United States |
Leave a comment
Libya’s much-hailed first female Foreign Minister, Najla Mangoush, has been suspended by the country’s Presidential Council. The decision on 6 November concluded that the minister had been “acting unilaterally and without consultation” with the council as required by the political agreement of 9 November 2020 that divided authority between the Council of Ministers and the Presidential Council. The suspension decree also said that Mangoush is to be investigated by two experts who will submit their findings to the council within the next two weeks.
However, the real reason for the suspension and investigation is a comment in her interview with the BBC. The minister said that her government is “open” to the possibility of extraditing a Libyan citizen wanted by the United States in connection with the Lockerbie bombing in 1988. On the 32nd anniversary of the bombing on 21 December last year, the then US Attorney General William Barr accused a former Libyan intelligence officer, Abu Agila Mohammed Masud, of involvement in the atrocity. Despite what Mangoush told the BBC, though, it is unlikely that Masud will be extradited.
Two hundred and seventy people, mostly US citizens, were killed on that fateful night, including 11 people on the ground, when Pan Am Flight 103 blew up over the Scottish town of Lockerbie. A Libyan intelligence officer, Abdel Baset Ali Al-Megrahi, was convicted of the atrocity and sentenced to life imprisonment in a 2001 trial. He was released in 2009 for health reasons — he was suffering from prostate cancer — and died in his Tripoli home in 2012.
Al-Megrahi protested his innocence to the end and his family launched a posthumous appeal to clear his name. The third appeal is now being considered by the UK Supreme Court in London after it was rejected by Scotland’s Court of Appeal in January.
His Glasgow-based lawyer, Aamer Anwar, was outraged by Mangoush’s comments. In a statement shared with MEMO he wrote, “Shame on you [Najla Mangoush] for broadcasting to the world, the words ‘positive outcomes’ are coming.” When asked about the possibility of extraditing Masud to the US the minster had used that phrase, implying that the issue is being discussed among ministers and a decision to collaborate with the US has already been made.
Anwar went on to question her motives by asking, “What reward are you expecting from the United States, a country that has bombed, humiliated and sanctioned your people?” He accused the minister of breaking Libyan law, which bans the extradition of Libyan citizens to be tried abroad.
Faced with a wave of public outrage, the Ministry of Foreign Affairs and International Cooperation denied on 7 November what was attributed to the minister in the BBC interview. It insisted that Mangoush “never mentioned” Masud. It’s true that she did not refer to him by name, but the context of the interview clearly refers to him. The BBC released a clip of the interview in which Mangoush answered a question about extraditing Masud to the US and she said: “I don’t know but I think we, as a government, are very open in terms of collaboration in this matter.”
Prime Minister Abdul Hamid Dbeibeh came out quickly in her support, and said that the Presidential Council does not have the authority to suspend the foreign minister. Citing the political agreement that paved the way for the current government and council to share power, Dbeibeh said that the latter “has limited power” which does not include appointing or suspending ministers.
A top Libyan Supreme Court judge, Ali Al-Zuraiqi, confirmed in a televised interview said it is “illegal to extradite a Libyan citizen” to be tried in another country. He added that such a matter is in any case “for the judiciary in Libya to decide.”
Libyan commentators overwhelmingly rejected Mangoush’s statement, accusing her of reopening the Lockerbie case which, many say, has long since been closed. Indeed, in 2008 the US and Libya signed what is known as a Claims Settlement Agreement that ended all claims in connection, not only with the Lockerbie bombing, but also many others that involve violence and acts of terror committed before 2006.
Former Foreign Minister Mohamed Sayala was asked about his successor’s comments. “The Lockerbie case was completely closed,” he pointed out, “[and] its revival opens hell’s door” to Libya, particularly, in terms of financial compensation for the victims’ families. In the 2008 agreement with the US, Libya agreed to pay a total of $2.7 billion to victims’ family in order to “buy the peace”, as its then Prime Minister, Shukri Ghanem, described it.
Libya has never accepted responsibility for the Lockerbie tragedy and “mounting evidence” since the 2001 trial has pointed to Al-Megrahi’s innocence. Dr Jim Swire, whose daughter was killed on board the doomed flight, is certain that Al-Megrahi is a “victim of a miscarriage of justice.” Swire is one of the campaigners pushing for his conviction to be overturned.
Ferial El-Ayeb, a consultant to Al-Megrahi’s defence team in Scotland, told MEMO that such comments by Foreign Minister Mangoush are “outrageous and insulting to us in the defence team.” She added that Libya is in “a weak situation now” and the kind of comments heard from the minister “will increase US pressure on the country to hand over Masud.”
A source in the foreign ministry, speaking anonymously, told MEMO yesterday that Mangoush was in her office despite the Presidential Council’s decision. The source added that she is expected to take part in tomorrow’s conference on Libya hosted by the French in Paris.
The only certainty, the source concluded, is that the “negative public backlash against [Mangoush] will act as a ‘deterrent’ to her and other officials to be careful when discussing sensitive issues.”
November 11, 2021
Posted by aletho |
Timeless or most popular | Libya, United States |
Leave a comment
When we last looked at Indonesia their massive wave in Covid cases had just peaked after ivermectin was approved again on July 15th. Since then the cases have dropped from 50,000 a day to about 900. On a per capita basis today Indonesia is managing Covid about ten times better than Australia. Think about that.
Remember the reason for the Indonesian surge. In June, they had a controlled rolling caseload of 5,000 a day. It was not rising thanks to a philanthropist called Haryoseno who had been arranging for ivermectin supplies at low cost to help people. But in a fit of modern-medicine, in line with the deadly WHO recommendations, the Indonesian government banned ivermectin on June 12th. Cases took off. Mayhem ensued. And about 90,000 people died in the following surge.
By early July the anti-parasitic drug ivermectin was hot property in Indonesia, even if it was banned. A number of high-ranking politicians championed it, and people were flocking to buy it.
“Indonesians have ignored health warnings to stock up on a “miracle cure” for COVID-19 backed by leading politicians and social media influencers, as an out-of-control virus surge sweeps the country.”
— July 8th, NDTV
By July 15th the Indonesian government relented, and BPOM approved Ivermectin as Covid-19 Therapeutic Drug. By July 18th new daily cases peaked across Indonesia and now they are lower than they were before. During the surge, at least two million Indonesians were infected.
Perhaps Governments shouldn’t run around banning a wonder drug so safe that researchers in Australia feed it to small children to kill head lice.

All bell curves look the same, but some are bigger than others. Timing is everything. OWID
Google Trends show Indonesians were searching for ivermectin in early July. The average Indonesian apparently knows more about treating Covid than our Minister of Health. More even than our Chief Medical Officer.

There was one popular search in Indonesia as cases rocketed.
Greg Hunt could have managed the Covid debacle so much better if he’d just phoned up a pharmacist in Bali.
Compare the Rich-mans Vax plan
Australia, on the other hand, decided to vaccinate 15 million people or 70% of the entire population and still has twice as many cases as Indonesia does — even though Indonesia has ten times as many people and only on third of the government revenue.
The Australian TGA committee banned ivermectin on Sept 11th, by the way, possibly to make sure we didn’t accidentally eliminate Covid, or Pfizer’s third quarter profits. Who can tell?
That lockdown-and-vax plan and the roadmap to freedom doesn’t seem to be working too well. In Australia billions of dollars were burnt at the stake, not to mention the health risks of using experimental prophylactics, while Indonesia reduced Covid cases by 98% for about point-one percent of the cost and the main side effects were the deaths of worms, lice and bed bugs.
If Gladys had just dished out the Ivermectin — Uttar Pradesh style — on July 5th, the outbreak would have been over in a few weeks.

Australia vaccinated 70% of the population and locked down its two largest states to control Covid and still hasn’t succeeded. Source: OWID
Since July 18th when Indonesia cases peaked, Australian cases have grown from 31,000 to 150,000.
The only thing more scary than the Ministry of Health’s incompetence is that politicians and philanthropists in the third world have more freedom than Australian ones do. The Indonesian media is more worth watching than the Australian ABC.
At this point people are still dying who could be saved.
As David Archibald says “It means that Australia could end its covid problem anytime it wanted to at hardly any expense at all. Our government would be aware of what the Indonesians have achieved. It also means that any covid deaths from here on are state-sanctioned murder. “
___________________________________________________________
The wonder drug that disappeared
My summary of Ivermectin
If you only email friends one link — make it this story. It’s the biggest medical scandal since 1850— Why is a cheap safe drug being ignored? Could it be that there would be no medical emergency and no need to rush out other riskier new treatments which are still classed as “experimental” if there was a safe alternative? There are billions of reasons to ask this question but newspapers wouldn’t publish the story. In desperation, some Americans are going to court to get rulings to order doctors to use Ivermectin on their loved ones. Even if they win, sometimes hospitals still refuse to use it on patients with few options left. One family hired a helicopter to take their mother away from intensive care in a hospital that refused to give Ivermectin (and had a happy ending). The debate is so suppressed, there are rumours the US President was treated with it in secret last year.
For peer reviewed studies read: The BIG Ivermectin Review: It may prevent 86% of Covid cases.
Ivermectin has also been used, with apparent success in India, Peru and Mexico (and so many other places). Covid cases fell in the states of India that approved Ivermectin use but rose in Tamil Nadu where it wasn’t permitted. Despite the success, India’s Health dept suddenly stopped Ivermectin use again and people in India are suing the WHO in disgust. In Peru, Ivermectin cut covid deaths by 75% in 6 weeks.
The FDA and others will say there is little evidence of success so far, but that’s a scandal in itself. Why are there no large trials? And why are other drugs like Remdesivir approved with only one trial? Ivermectin is so safe some 3.7 billion doses have already been used around the world. The inventors won a Nobel Prize for its discovery in 2015. We’ve known it might be useful since April last year, when an Australian group searched through many cheap safe drugs looking for any that might help against Covid. The news then was “Another possible cure for coronavirus, found in sheep dip: Ivermectin”. This was just a lab study, and it suggested doses would need to be too high. Even so, successes keep turning up in the real world? By July last year there were already signs Ivermectin could save as many as 50%. Why were large trials not started then? The UK trial is hobbled from the start.
November 11, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, War Crimes | Australia, Human rights, Indonesia, WHO |
Leave a comment
LinkedIn has decided that a video about the efficacy of Covid vaccines, originally posted on YouTube and featuring Dr. Aseem Malhotra was violating its “professional community policies.”
Interviewer Maajid Nawaz posted a screenshot of the message he received from LinkedIn on Facebook, informing him of the removal and that only he can now see the post.
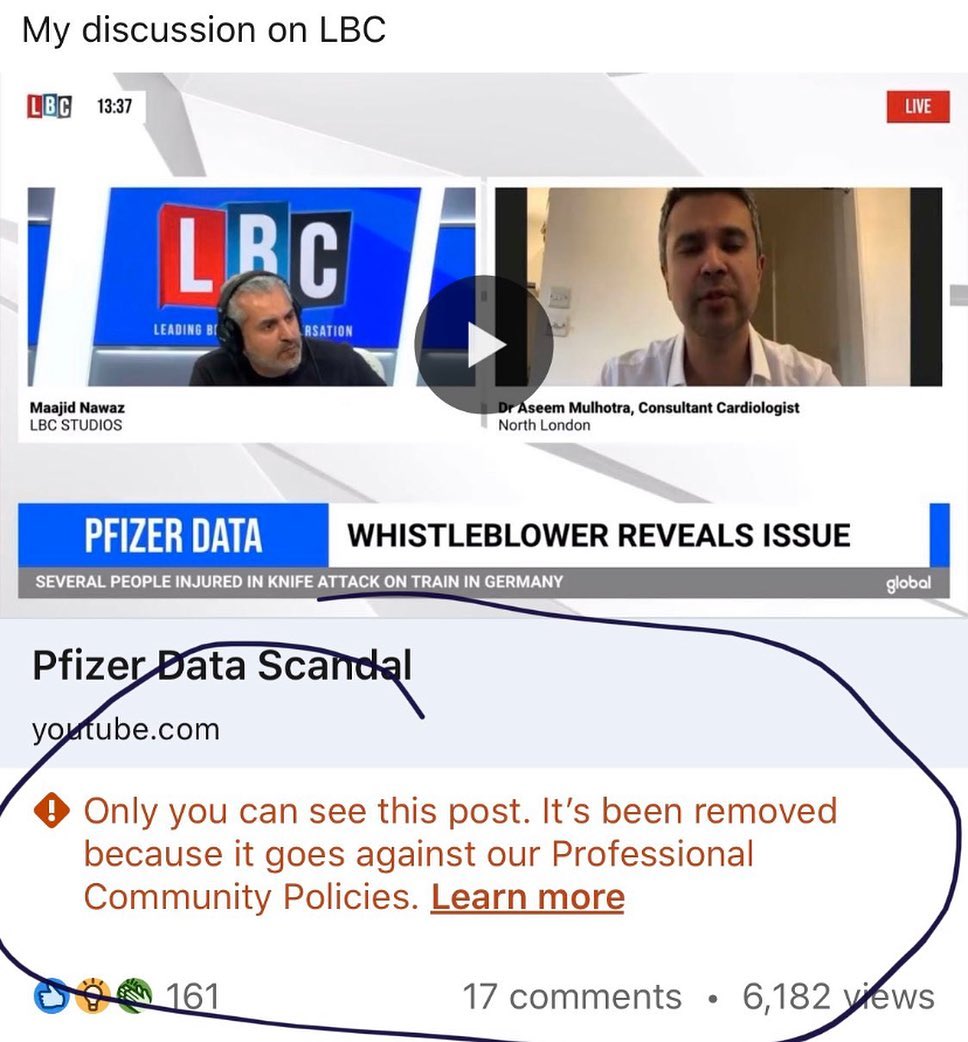
No other details for the censorship were given, other than a link presumably leading to LinkedIn’s policy page which requires users to be “safe, civil and respectful,” trustworthy by using their real identity and sharing “real and authentic” information, as well as make sure the content users posts is professionally relevant.
The video, which is still available on YouTube as of this writing, features Dr. Malhotra interviewed on the LBC talk radio station, posted under the headline, “Pfizer data scandal.”
Dr. Malhotra’s conversation with LBC’s Maajid Nawaz shown in the video focused on vaccine mandates, which he believes to be unethical, and the cardiologist’s belief that the healthcare crisis is the result of what he called “the corporate capture of public health.”
Dr. Malhotra also does not think that getting the jab has proved to significantly reduce transmission of the virus, he revealed during the interview, accusing Big Food and Big Pharma industries of chasing profits rather than looking for ways to improve health, and as more willing to pay billions in fines over the years, than changing their way of doing business.
He also commented on a whistleblower revealing that a Pfizer contractor was falsifying Covid vaccine trials data, which would mean that the effectiveness of the vaccine might have been overstated.
Speaking more broadly about the problem in the pharmaceutical industry and in the healthcare system, Malhotra said that clinical decisions are made on what he said were incomplete, biased, “and in many cases potentially corrupted data.”
The doctor also revealed that he was vaccinated with both doses earlier in the year believing he was protecting his patients from getting infected by him – but that he now thinks this belief was false.
“What’s now very very clear, as this data’s evolving,” Malhotra said, “is that there’s no significant reduction in transmission from taking the vaccine.”
However, he also noted that he thinks there is valid data showing the vaccine does prevent serious illness and death – but that healthy and young individuals likely don’t benefit from it.
November 11, 2021
Posted by aletho |
Full Spectrum Dominance, Science and Pseudo-Science |
Leave a comment
 Two Lowell Graded School parents demanding their second-grade daughter be taught in the classroom without a mask were warned by a state trooper Thursday, Nov. 4 to take her home or risk arrest for trespass or loss of custody of their child.
Two Lowell Graded School parents demanding their second-grade daughter be taught in the classroom without a mask were warned by a state trooper Thursday, Nov. 4 to take her home or risk arrest for trespass or loss of custody of their child.
The live Facebook video was recorded by the girl’s father, Andre “Mike” Desautels. In March, a Vermont judge sided with Vermont Attorney General TJ Donovan and ordered Desautels to require his employees to wear masks.
As the video opens, Desautels explains he and wife Amy have a note from a doctor exempting his daughter from wearing a mask. However, the parents have been told that a doctor’s note isn’t enough and that the school needs to see a formal medical diagnosis in order to develop a 504 plan. Such plans are intended to ensure that a child who has a disability identified under the law and is attending an elementary or secondary educational institution receives the necessary accommodations.
“We did not agree to this as she did not need any special accommodations from anyone,” Amy Desautels explained via social media. “We had provided the doctor’s note which is what was stated on the NCSU guidelines for what they required and it did not specify what needed to be on the note.”
As seen on the video, Vermont State Trooper Andrew Jensen talked briefly with the couple, took a phone call, and then returned and then politely but firmly gave them three options.
“Your options are: Take your child, go home, fight this through the courts, through your lawyer, whatever,” Jensen said. “Option B: We escort your child out here, you refuse to take her home, and you refuse to leave. Therefore we place both of you under arrest for trespassing. Option C: you leave, but leave your child here, we contact DCF, possibly placing her in state custody for abandonment.”
“I cannot believe that you guys would get involved, especially because we have done everything required with our paperwork. And you’re going by what he (Castle) is telling you,” Desautels responded. He also said a child in Walden – another Northeast Kingdom town – is attending mask-free.
The school has the right to make the rules,” Jensen said.
“But we’re following the rules,” Desautels said.
“But not exactly,” Jensen said.
Given those options, the couple elected to take their child home that day.
* * * * * *
Earlier in the day, Castle answered Vermont Daily Chronicle questions about school policies on masking.
Chronicle: What are the options for parents who do not want their children to wear masks in school?
Castle: “A parent may obtain an exemption to having their child wear a mask if they have a certified diagnosis from a physician of a medical reason for not wearing a mask or from a physician or mental health provider for a psychological reason. The school would need to review the medical information within a formal IEP or 504 process to determine if the accommodation is necessary to ensure the child is able to access their education.”
Chronicle: Please describe the reasoning behind removing a child from school for not wearing a mask.
Castle: “Schools that have established a mask requirement are doing so to mitigate the transmission of COVID-19 in the interest of public health for students and staff. Allowing staff or students without a legitimate exemption to not wear a mask would result in many individuals opting out and thus increasing the risk of transmission. A student’s non-compliance with a mask requirement is considered unsafe and in violation of school procedures.”
November 11, 2021
Posted by aletho |
Civil Liberties | Human rights, United States, Vermont |
Leave a comment
you can check in any time you like, but there might not be any doctors…
president brandon and his merry band of miscreants have been busy mandating covid vaccines for health care workers. many states have done so as well.
this is going to create severe staffing crunches.
18% of front line HCW’s are not planning to vaccinate.
this rises to 24% in nursing homes.
this winter when hospitals are having “weather disruptions” like american and southwest airlines because the winds of “i do not wish to be vaccinated against my will” among health workers are reaching gale force, just remember:
this is not covid.
this is bad policy.
this is literally an attempt by health officials to:
“make hospitals and assisted living facilities safe by preventing doctors and nurses from making healthcare choices.”
no sane public health official would do this.

this has NOTHING to do with a virus. if it did, you’d trust acquired immunity and the medical judgement of doctors.
these people are wreckers.
they WANT these systems to break. they want a hospital crisis because that will create “an emergency” that allows them to step in and regulate or grab control or nationalize.
do NOT fall for this. this is a game of chicken and the doctors who want to have their own bodies be their own choice are in the right.
support health workers as they strike and stand up for themselves.
they were there for us. be there for them.
not only is this the morally correct thing to do, but it’s also in your own self-interest if you ever again want to be able to have your own medical choices be between you and your chosen physician.
can you seriously believe that a system that will not allow doctors to make THEIR OWN healthcare choices can be trusted to let them help you make YOURS?
this is not about your health, it’s about their power. their regulatory edifice seeks to subsume all of healthcare and to do it, they’re seeking to BREAK all healthcare.
this will not be market failure.
this will be market sabotage.
be sure you blame the right people.
and be sure you repay wreckers with being wrecked in return.
November 11, 2021
Posted by aletho |
Deception, Science and Pseudo-Science, Solidarity and Activism | COVID-19 Vaccine, United States |
Leave a comment
This article defines a more effective public health strategy for the current COVID pandemic.
The core issue is that there is a huge array of reactions to both COVID infections and vaccines based on diverse biology, genetics and medical conditions of individuals. Missing from current policy is recognition and support of personalized medical methods.
First, medical history tells us the wisdom of making the medicine fit the person. This is the cornerstone of what is called personalized or individualized medicine. Good physicians also find the combination of drugs to best address an illness or disease. This contrasts with mass use of off-the-shelf, one-size-fits all drugs. Proposed here is an approach to tailor or fine tune medical solutions to individual biologic and genetic characteristics, and personal medical needs and circumstances.
As an example of how trying to get the public to accept a mass medicine is the case of seasonal flu vaccines. A large fraction of the public does not take them. During the 2019-2020 season, 63.8 percent of children between six months and 17 years got a flu shot. Among adults, just 48.4 percent of people got flu shots.
Why is this? Because it is common knowledge that their efficacy rate is relatively low. On average, people who get the flu shot are between 40 and 60 percent less likely to catch the virus than unvaccinated individuals. The truth is that the annual flu vaccine does not fit every individual. Even though there is little medical evidence that taking a flu vaccine poses significant health risks. But people know that the flu infection fatality rate is relatively low.
Many individuals make a sensible risk/benefit analysis, concluding that there are insufficient benefits. Others, especially older people with serious medical conditions and possibly weak immune systems get annual flu shots. The public health system has allowed a personalized approach to seasonal flu vaccines.
And it turns out, based on government data, that low risk is also the case for the current COVID pandemic. For the vast majority of people getting coronavirus infection either means no symptoms or only mild ones not much different than the flu or a very bad cold, and which pass in relatively few days. Here is the reported truth about low coronavirus death risks for healthy people:
“CDC showed that 94 percent of the reported deaths had multiple comorbidities, thereby reducing the CDC’s numbers attributed strictly to COVID-19 to about 35,000 for all age groups.”
This stands in contrast to the widely reported total of over 730,000 COVID related deaths. What this shows is the huge variations in how people respond to COVID infections because of their innate differences.
What COVID infected people do get is natural immunity to this virus that abundant medical research and clinical studies have shown is better than vaccine immunity. The latter declines in about six months, whereas natural immunity lasts longer and better defends against new variants.
Combination Of Medicines
Besides making the medicine fit the patient is established clinical wisdom for using a combination of drugs. And often, in this pandemic, some doctors use a combination that includes more than several generic medicines and, especially in hospitals, government approved drugs. Also widely used are vitamins and supplements. The eminent Dr. Peter McCollough has been the leading proponent of using individualized combinations to treat and prevent COVID infection disease. All this is an alternative to the strategy of mass vaccination for everyone.
Today, anyone without too much effort can find a host of combination protocols to treat and prevent COVID.
The Missed Opportunity Discussed Early In The Pandemic
Between the early 2020 months of the pandemic and the roll out of mass vaccination in late 2020 there was interest in applying the personalized medicine approach to managing the pandemic.
Consider what the Mayo Center for Individualized Medicine said for the COVID-19 response. The document detailed a number of initiatives Mayo was pursuing to address the pandemic by obtaining medical data that could lead to personalized pandemic solutions. This is what Mayo wanted to do:
“When COVID-19 spread across the U.S. in March 2020, the Mayo Clinic Center for Individualized Medicine urgently responded to accelerate research, development, translation and implementation of novel tests, lifesaving treatments and diagnostics. Now, collaborative teams of scientists are continuing to unravel the mysteries of the novel virus, including using advanced genetic sequencing technologies to investigate how the virus can infiltrate a person’s immune system and wreak havoc on organs, tissue and blood vessels, leaving some patients with long-term effects.”
A September 2020 article had the intriguing title “How to use precision medicine to personalize COVID-19 treatment according to the patient’s genes.” Here are excerpts:
“In recent years, a gene-centric approach to precision medicine has been promoted as the future of medicine. It underlies the massive effort funded by the U.S. National Institutes of Health to collect over a million DNA samples under the “All of Us” initiative that began in 2015.
But the imagined future did not include COVID-19. In the rush to find a COVID-19 vaccine and effective therapies, precision medicine has been insignificant. Why is this? And what are its potential contributions?
If precision medicine is the future of medicine, then its application to pandemics generally, and COVID-19 in particular, may yet prove to be highly significant. But its role so far has been limited. Precision medicine must consider more than just genetics. It requires an integrative “omic” approach that must collect information from multiple sources – beyond just genes – and at scales ranging from molecules to society.
The situation becomes yet more complicated for infectious diseases. Viruses and bacteria have their own genomes that interact in complex ways with the cells in the people they infect. The genome of SARS-CoV-2 underlying COVID-19 has been extensively sequenced. Its mutations are identified and traced worldwide, helping epidemiologists understand the spread of the virus. However, the interactions between SARS-CoV-2 RNA and human DNA, and the effect on people of the virus’s mutations, remain unknown.”
… there is an opportunity to begin gathering the kinds of data that would allow for a more comprehensive precision medicine approach – one that is fully aware of the complex interactions between genomes and social behavior.
The NIH has said: “The National Institutes of Health’s All of Us Research Program has announced a significant increase in the COVID-19 data available in its precision medicine database, adding survey responses from more than 37,000 additional participants, and virus-related diagnosis and treatment data from the nearly 215,000 participant electronic health records (EHRs) that are currently available.”
The specialty germane to a personalized pandemic strategy is called pharmacogenomics. It is the study of the role of the genome in drug response. It combines pharmacology and genomics to discover how the genetic makeup of an individual affects their response to drugs, including vaccines.
It deals with the influence of acquired and inherited genetic variation on drug response in patients by correlating genetic factors of an individual with drug or vaccine absorption, distribution, metabolism and elimination. It deals with the effects of multiple genes on drug and vaccine response.
The central goal of pharmacogenomics is to develop rational means to optimize drug therapy, including vaccination, with respect to the patients’ genotype, to ensure maximum efficiency with minimal adverse effects.
By using pharmacogenomics, the goal is that pharmaceutical drug treatments, including vaccination, can replace or at least complement what is dubbed as the “one-drug-fits-all” approach. Pharmacogenomics also attempts to eliminate the trial-and-error method of prescribing, allowing physicians to take into consideration their patient’s genes, the functionality of these genes, and how this may affect the efficacy of the patient’s current or future treatments (and where applicable, provide an explanation for the failure of past treatments).
An August 2020 journal article was titled “Pharmacogenomics of COVID-19 therapies.” Here are its optimistic views and findings:
“Pharmacogenomics may allow individualization of these drugs thereby improving efficacy and safety. … Pharmacogenomics may help clinicians to choose proper first-line agents and initial dosing that would be most likely achieve adequate drug exposure among critically ill patients; those who cannot afford a failure of ineffective therapy. It is also important to minimize the risks of toxicity because COVID-19 particularly affects those with comorbidities on other drug therapies.
We found evidence that several genetic variants may alter the pharmacokinetics of hydroxychloroquine, azithromycin, ribavirin, lopinavir/ritonavir and possibly tocilizumab, which hypothetically may affect clinical response and toxicity in the treatment of COVID-19. … These data support the collection of DNA samples for pharmacogenomic studies of the hundreds of currently ongoing clinical trials of COVID-19 therapies.
One of the biggest success stories in the field of pharmacogenomics was for a drug used to treat another, highly lethal, infectious disease: abacavir for HIV. … In an acute illness such as COVID-19, pharmacogenetics would only be useful if the genetic test results were already available (i.e., pre-emptive pharmacogenetic testing) or rapidly available (i.e., point-of-care genetic testing). …
In the face of unprecedented challenges posed by the COVID-19 pandemic, collaborative efforts among the medical communities are more important than ever to improve the efficacy of these treatments and ensure safety. Some large national COVID-19 trials are evaluating pharmacogenomics, which will inform the role of pharmacogenomics markers for future clinical use.”
A July 2020 NPR show was titled “Research On Personalized Medicine May Help COVID-19 Treatments.” This was deemed newsworthy:
The nationwide All of Us Research Program aims to tailor medical treatments of all kinds, including treatments that may be developed for the new coronavirus. So far more than 271,000 people nationwide have signed up to share data with the initiative. All of Us started under President Barack Obama in 2018 [sic] and involves institutions across the country.
“This is an exciting opportunity for our participants to have a direct impact on COVID-19 research, watching how their participation in this historic effort is truly making a difference,” said Dr. Elizabeth Burnside. “This focused initiative could be especially important for members of communities that are often underrepresented in health research and who may question the overall and personal benefit of research participation.”
In sum, there was legitimate medical interest early in the pandemic to use personalized medicine, in which drugs and drug combinations are optimized for individuals or certain population demographics. The central goal is minimization of drug and vaccine toxicities and adverse reactions and deaths.
But one thing is now clear. The personalized approach to managing the COVID pandemic has not been aggressively pursued by public health agencies. They have placed their resources and hopes with mass vaccination, both encouraged, coerced and increasingly mandated. The hope that we can vaccinate ourselves out of this pandemic has lost credibility.
In contrast, an alternative personalized approach, used by hundreds of physicians, based on generic medicines, vitamins and supplements have been more blocked than supported by the public health establishment as detailed in Pandemic Blunder.
Proposed New Public Health Strategy
Part One: Individuals decide either on their own or with the advice of their personal physician to be vaccinated for COVID. And to accept what government officials have decided are the best COVID medical solutions for outpatients and inpatients.
Part Two: Individuals choose a preferred medical professional who, on the basis of their education, training, experience and successful clinical results, offers alternatives to vaccination and government promoted medical solutions for outpatients and inpatients. The medical professional uses the patient’s medical history, conditions, needs and unique personal biologic and genetic circumstances to reach the best personalized medical solution.
The new public health strategy is, therefore, twofold. Widely available vaccination becomes focused or finely tuned to meet the desires and needs of part of the population. Along with use of the second part there is no sacrifice of true public health protection in the pandemic.
Part Two of the strategy directly addresses the widespread resistance to COVID vaccination by some Americans.
This is a rational perspective consistent with the belief in medical freedom. If one believes that there are some certain medical benefits of COVID vaccines, then traditional medical practice supports use of them on an individual therapeutic basis. This is a free personal decision, perhaps in consultation with their physician to accept that COVID vaccine risks are outweighed by its benefits.
Risks and benefits may be based on personal research of available medical information on vaccines. Or on information from government agencies, often without advice from their doctor.
Not to be ignored is increasing negative information on COVID vaccines reaching the public. One recent example from a published medical research article is that “cost-benefit analysis showed very conservatively that there are five times the number of deaths attributable to each inoculation vs those attributable to COVID-19 in the most vulnerable 65+ demographic.”
From this same study: within “eight days post-inoculation (where day zero is the day of inoculation), sixty percent of all post-inoculation deaths are reported in VAERS.” This study concluded: “It is unclear why this mass inoculation for all groups is being done, being allowed, and being promoted.”
In seeking to implement the wisdom of fit the medicine to the person, requires accepting the science that no two people, medically, genetically and biologically speaking, are exactly the same; this cannot be disputed. This is why using pharmacogenomics has a role to play. Looking at average statistical vaccine outcomes ignores and disrespects individual biologics, medical conditions, concerns and needs. This is an overselling of vaccines.
Americans have always wanted to see themselves as unique individuals. This translates to medical actions. Mass vaccination for everyone ignores and devalues this traditional belief by Americans.
There are also legitimate concerns that giving informed consent to a shot has not been based on a full, easily understood presentation of data on risks for different kinds of people with various medical histories.
Those who are resisting vaccination have a right to question that government agencies have not strictly followed medical science, data and experience. For example, a vast literature concludes that stay-at-home mandates, lockdowns and masking have not been effective in controlling pandemic impacts.
And there is now considerable evidence that those who are vaccinated can get breakthrough infections and spread the virus. “We have data now through the first week of August from the Center for Medicaid and Medicare Services, showing that… over 60 percent of seniors over the age of 65 in the hospital with Covid have been vaccinated,” noted the esteemed Dr. Peter McCullough recently.
This erodes the credibility of public health agencies and their medical authority and destroys public trust in federal agencies implementing pandemic policies.
The Fallacy Of Only One Medical Solution
If the government would let some part of the public choose personalized treatment to deal with COVID infection and another part to choose vaccination (and other government actions) why is that not an acceptable public health policy? The two-part strategy will become increasingly important as the government promotes or mandates regular booster shots over months or years.
Choice is rational if, indeed, there are personalized treatment options other than vaccination that can be obtained from some medical professionals. Indeed, there is now a vast medical literature on treatment protocols not only to cure but also to prevent COVID infection. They are being used very successfully by hundreds of American physicians.
And some information reaching the public like the very successful use of the generic ivermectin in India and Indonesia reinforces the inclination of some people to seek alternative medical solutions. Also, that 100 to 200 members of Congress have used this generic.
Moreover, now there is also a vast medical literature, increasingly known to the public, supporting the strong effectiveness of natural immunity obtained through previous COVID infection. It is a rational personal decision to conclude that one’s natural immunity is sufficient medical protection without taking on any vaccine risks. They have the right to seek a medical professional that agrees with that medical reality.
The only conceivable “loser” for this approach would be vaccine makers having a smaller market.
Physicians should have the freedom to advise their patients to either use a generic medicine treatment protocol or help document their natural immunity (with valid testing) to allow patients to embrace personalized medical action rather than be vaccinated.
In this two-part policy approach, of promoting a choice between personalized medical protection versus mass vaccination, the entire population could be fully protected without sacrificing medical freedom and without various forms of vaccine mandates. Public health does not require total public acceptance of one medical solution.
This strategy is consistent with what many physicians said early in the pandemic. Namely that vaccination should be targeted on those with the highest risks of serious COVID impacts, not the entire population. It is widely known by the public and accepted by the medical establishment that this pandemic does not pose a serious threat of either illness or death for people below the age of about 70, unless they have serious comorbidities or serious illnesses. Infection fatality rates for most of the public do not argue for vaccination.
Much of the public wants and deserves the choice to use something other than a vaccine shot to protect themselves. That choice becomes operational only if the government allows and supports medical professionals to offer their patients alternatives to vaccines.
Here is the ethical and medical truth: Protecting individual health trumps protecting public health but is not antithetical to protecting public health. Overly coercive public health actions, such as vaccine mandates, are antithetical to protecting individual health for many people who fear even low probability negative reactions to vaccines.
Here is the ultimate medical truth: When all available medical science and means are fully used then the result is safely protecting public health without sacrificing medical freedom of both physicians and individuals.
The Current Strategy Has Failed
As we approach two years of dealing with this pandemic there is abundant evidence that the emphasis on mass vaccination has largely failed. The US has the highest number of COVID deaths on the planet. Even now, after wide use of the mass vaccination approach, recent 2,000 daily deaths are related to COVID infection. Every week more people are counted as COVID deaths than the 3,000 people who died in the 9/11 disaster.
Not to be ignored is the widely cited journal study titled “Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States.”
Breakthrough infections among the fully vaccinated are mounting. Because after about six months vaccines lose much of their effectiveness, especially against variants. And fully vaccinated people can and do carry and transmit the coronavirus.
If one wants first-hand accounts of how US physicians have documented their own negative impacts of COVID vaccines as well as those of their patients, then read a number of their affidavits.
Conclusions
A new public health strategy that no longer adheres to single-minded mass vaccination can obtain broad public support. Now is the time to endorse and support personalized medicine applied to the pandemic.
Much of the public may not yet know this. But missing from the new CDC definition of vaccine as of September 1, 2021 are these key phrases: “protecting the person from that disease” and “to produce immunity.” The new vaccine definition should reduce public confidence in current COVID vaccines. In fact, these changes reflect what is now known about the limitations of these vaccines. Fully vaccinated people can still get COVID disease and really do not have long lasting effective immunity to it.
Promoting choice is a far better public health approach than wide use of authoritarian pandemic controls that have devastated lives and produced mental stress and many collateral deaths.
On that last point, CDC has now recognized mood disorders put people at high risk for severe COVID cases. Compare pre-pandemic 2019 to 2020 when there were 53 million new cases of depression globally, a 28 percent increase, as reported in The Lancet. Surely, promoting more medical choice for addressing COVID would help people stay both mentally and physically healthy.
Resistance to vaccine mandates should not be seen as unpatriotic or as creating harm for others. Supporting personalized medicine is a way to avoid negative impacts on the American economy because of rigid, inflexible vaccine mandates that compel many Americans to accept job loss that in many ways imperil public safety.
Lastly, staying alive and safe surely is the presumed goal of all people. We have more tools than vaccines to help people meet their goal. Now we need the public health establishment to let all the tools be freely chosen.
Joel S. Hirschhorn’s new book Pandemic Blunder here: amazon.com
November 11, 2021
Posted by aletho |
Civil Liberties, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, Human rights, United States |
Leave a comment
View this video on Bitchute or Rumble.
By P Gosselin – No Tricks Zone – 10. November 2021
Over 95% effective and safe, so insisted vaccine manufacturers, government agencies and mainstream media. Everyone should get out and take the jabs so life could get back to normal. Those who expressed doubts and warnings were immediately branded crackpots and banned by social media.
Pfizer CEO Albert Bourla even said that people who spread disinformation about (against) coronavirus vaccines were “criminals.”
But while the US and much of the media continue to pretend that the vaccines are safe, more and more countries across Europe are advising or even banning the use of certain types for certain age groups due to “cardiovascular side effects”, which have been occurring at an unusual frequency. … continue
November 11, 2021
Posted by aletho |
Timeless or most popular, Video | COVID-19 Vaccine |
Leave a comment