French researchers identified possible safety signals in babies coinciding with the rollout of Beyfortus, a recently approved monoclonal antibody treatment for respiratory syncytial virus (RSV) in newborns.
The discovery comes as public health authorities ramp up warnings about the spread of respiratory viruses and step up their promotion of the drug.
In interviews with The Defender, the researchers — French independent scientist and author Hélène Banoun, Ph.D., and French statistician Christine Mackoi — explained that data from France’s National Institute of Statistics and Economic Studies (INSEE) indicates an improbably high rate of deaths of babies between 2 and 6 days old in France during September and October 2023.
INSEE is the authority that compiles official birth and death data in France.
This increase, the researchers said, coincides with the introduction of Beyfortus in French hospitals, which began on Sept. 15, 2023. In an interview with cardiologist Peter McCullough, M.D., MPH, Banoun said that over 200,000 newborn babies in France have been injected with Beyfortus since that date.
The Centers for Disease Control and Prevention (CDC) recommended Beyfortus in August 2023, while the European Medicines Agency (EMA) authorized the drug in September 2022.
Beyfortus was developed jointly by AstraZeneca and Sanofi.
The drug is offered as a “one-time shot for infants born just before or during the RSV season and for those less than 8 months old before the season starts,” and for some high-risk 8- to 19-month-old infants.
According to The Associated Press, “In the U.S., about 58,000 children younger than 5 are hospitalized for RSV each year and several hundred die.” CNBC reported that “RSV is the leading cause of hospitalization among infants in the U.S.” According to the CDC, nearly all children are infected with RSV before the age of 2.
But the French researchers and other medical experts who spoke with The Defender warned that no long-term studies have been conducted involving Beyfortus and newborns and that the administration of monoclonal antibodies on this population is unprecedented. They also pointed to data indicating RSV’s low risk to babies.
Dr. Meryl Nass, an internist, biological warfare epidemiologist and member of the Children’s Health Defense (CHD) scientific advisory committee, told The Defender, “Giving newborns any drug or biologic should be done with extreme caution, let alone a novel, injected monoclonal antibody. You cannot tell if the infant is damaged by the shot, when you don’t yet know how healthy the newborn is and how it normally behaves. This should be a huge red flag for manufacturers as well as parents.”
According to Banoun, “The French government is recommending that Beyfortus be injected into newborns before they leave the maternity ward, from Sept. 15, 2023, even though the product has not been tested on this age group,” Banoun said.
Nass pointed out that the CDC published a paper in 2021 on all U.S. RSV deaths over the preceding 12 years. The CDC reviewed death certificates, and found there were only 26 deaths per year with RSV, and only 17 deaths per year in the entire U.S. caused by RSV in babies under one year old.
According to McCullough, “Among the 22.4 million children under age 5 years, the annual risk of RSV hospitalization is well under 1%.”
Excess deaths among newborns ‘alarming,’ ‘disturbing’
Mackoi told The Defender, “There is an excess of deaths for the months of September and October. The excess deaths in October are very alarming. It is very worrisome that this happened in two consecutive months.”
According to Mackoi, the increase in these excess deaths coincides with the introduction of Beyfortus in France.
“There is a strong concomitance with the Beyfortus injection since Sept. 15, 2023,” she said. “In France, babies receive injections of Beyfortus before leaving the maternity hospital. They leave the maternity hospital three or four days after their birth … These excess deaths are abnormal.”
According to Mackoi, the data show “a 50% increase in deaths of babies between 2 and 6 days of life compared with what would be expected,” noting that “the reference is obtained by dividing the number of deaths by the total number of births in 2018 and 2019; the result is 0.69 deaths between 2 and 6 days per 1,000 births.”
In September, the observed mortality rate was 0.97 deaths per 1,000 births, and in October, it was 1.05 deaths per 1,000 births, Mackoi said. “It is anomalous that this very significant increase should be found two months in a row. It may well be due to the injection of Beyfortus since Sept. 15, 2023.”
“Although of no scientific value, I have received testimonials from relatives and via the internet from families of healthy babies who were hospitalized in intensive care with respiratory distress syndrome immediately after the injection,” Banoun added.
Mackoi said that using the official INSEE data, which she described as “reliable [but] underestimated,” she “calculated for each month, the rate of babies born the month in question and died between 2 and 6 days of life,” and used a Poisson distribution to identify abnormal mortality rates, compiling the findings on her website.
According to the INSEE data, 54 deaths were recorded for 55,489 births in France in September 2023, despite the average number of expected deaths being 38, based on historical averages.
For October 2023, the data showed 61 deaths out of 57,940 births, despite the average number of expected deaths being 40.
Mackoi said that the probability of the September 2023 death figure occurring by chance is 0.9%, while the probability of the increased mortality in newborns in October 2023 is even lower, at 0.1%. She also noted that “there are no excess deaths less than 48 hours after birth,” and that this is “one more indication” that Beyfortus is causing the deaths, because they are not receiving the monoclonal for the first 48 hours of life.
“The coincidence of Beyfortus injections with excess infant deaths is disturbing,” Mackoi said.
Monoclonal antibodies may exacerbate symptoms rather than prevent them
These revelations came as the White House announced on Dec. 14, 2023, that it would make 230,000 additional doses of Beyfortus available last month, in addition to 77,000 doses that were released in November 2023.
A study published in the New England Journal of Medicine (NEJM) on Dec. 28 concluded, “Nirsevimab protected infants against hospitalization for RSV-associated lower respiratory tract infection and against very severe RSV-associated lower respiratory tract infection in conditions that approximated real-world settings.”
The study was funded by AstraZeneca and Sanofi.
According to Banoun, official data do not indicate that Beyfortus is effective. The data do, however, indicate a high prevalence of adverse reactions — including bronchiolitis — even though the treatment is supposed to protect recipients from respiratory illness.
“The most frequently reported adverse events are upper respiratory tract infections, including bronchiolitis,” she said.
Banoun added that data from the French National Authority for Health (HAS) do not “support a possible impact of Beyfortus in terms of reduced length of hospital stay, transfer to intensive care units, and mortality.”
“According to HAS, in the trials, the absolute risk of RSV infection was reduced by 3.8% in the five months following injection, and the absolute risk of hospitalization was reduced by 1% to 2% over the same period,” she said.
Banoun said the trials were not conducted on newborns, whereas the French government recommends injection from the first days of life in the maternity ward.
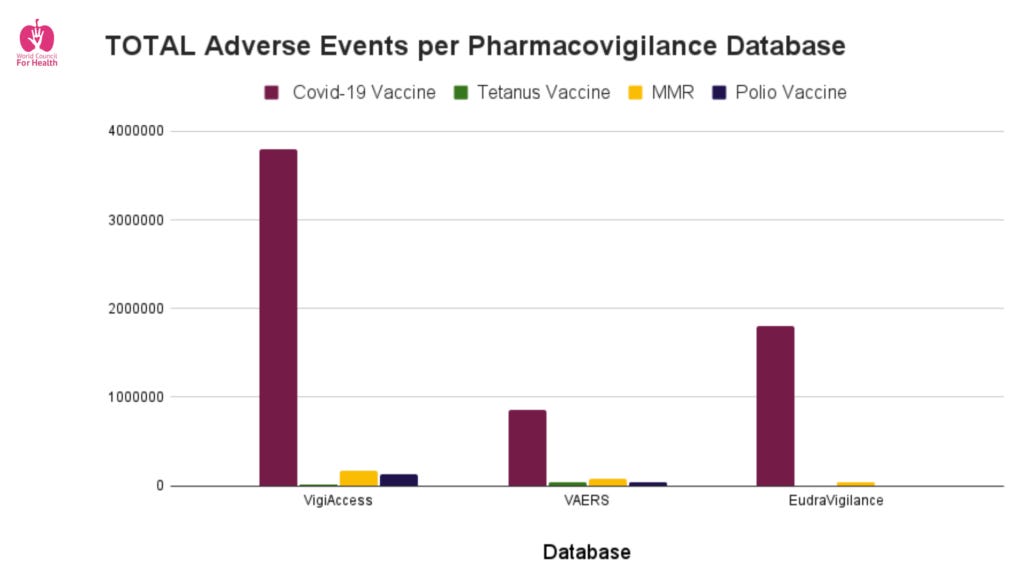
According to EudraVigilance, as of Dec. 24, 2023, there were 64 adverse events related to Beyfortus in those 1 month old or younger, and 68 for those between 2 months and 2 years of age. One death, that of a baby below 1 month old, was recorded, as were 60 records containing the word bronchiolitis. And according to VigiAccess, there were 104 adverse events reported, including 57 infections and respiratory disorders.
Another study, concerning premature babies and newborns suffering from heart or lung disease that compared Beyfortus with monoclonal antibodies previously used on high-risk babies, recorded six deaths — five due to bronchiolitis. Of the six babies that died, five had been treated with Beyfortus.
Yet, “these bronchiolitis cases are not attributed to the treatment by the investigator, who is also the manufacturer of the products,” Banoun said. “All this suggests that nirsevimab [generic name for Beyfortus] could facilitate and aggravate bronchiolitis: these injections take place during periods when the virus is circulating.”
“Let’s not forget that this whole bronchiolitis ‘prevention’ campaign is supposed to avoid overcrowding hospitals with babies suffering from the disease,” Banoun said. “If this product doesn’t significantly reduce hospital admissions, what’s the point?”
According to NTD, “Monoclonal antibodies are copies of an antibody that seek out foreign material to destroy them,” but the treatments come with a “risk that the body might trigger a strong reaction to the antibodies.”
Complications may be serious and can include “acute anaphylaxis or life-threatening massive allergic reactions and cytokine release syndrome that can result in organ damage.” This phenomenon is one of the adverse effects of Beyfortus.
In his interview with Banoun, McCullough said, “Antibody-dependent enhancements [ADE] have always been something we’ve been worried about because if antibodies bind the virus but not very tightly, that means they don’t neutralize the virus. And then, [a] fragment [Fc] of the antibody binds to a cell receptor. In a sense, the antibody can bring the virus into the cell.”
McCullough told The Defender, “The antibodies will invariably affect the development of natural immunity with repeated exposures to RSV during childhood. Beyfortus-resistant strains can be expected with indiscriminate use.”
Banoun cited a study in which “two of the 25 subjects in the nirsevimab group with RSV … had an RSV isolate containing substitutions associated with resistance to nirsevimab,” while “No subject in the placebo group had an RSV isolate containing substitutions associated with resistance to nirsevimab.”
Banoun also referred to a September 2022 EMA report, which found that during failed RSV vaccine trials in the past, children died of severe bronchiolitis in the vaccinated groups, but none from the control groups died.
“This ADE is due to the deleterious effect of antibodies which, instead of neutralizing the virus, facilitate its entry into the cell via the receptor of the Fc fragment of immunoglobulins. And it’s precisely this Fc region of nirsevimab … that industry has seen fit to modify,” Banoun said.
“Manufacturers are looking for the beneficial effects of this phenomenon and are wary of deleterious effects, which is why they have investigated the risk of ADE with Beyfortus in animal models,” Banoun added. “They claim not to have detected it, but the EMA points out, unmoved, that no histopathological evaluation of rats was carried out after treatment and infection with RSV: This is the only recognized marker of ADE.”
On his Substack, McCullough wrote that this effect may be triggered by aerosolized RSV virions present in hospitals.
“This means as ambient aerosolized RSV virions are present in hospitals, clinics, and home, the monoclonal antibody may backfire and enable the inhaled virion to gain access to the bronchial epithelial lining and cause worse bronchiolitis than the baby would have with their own developing natural immunity,” he wrote.
Beyfortus administered on newborns despite being tested on older babies
During the clinical trial leading up to approval of Beyfortus by the CDC and the U.S. Food and Drug Administration (FDA), a total of 12 infant deaths were recorded. However, the FDA claimed the deaths were “unrelated” to the antibody.
CNBC reported in June that of the 12 infants, “Four died from cardiac disease, two died from gastroenteritis, two died from unknown causes but were likely cases [of] sudden infant death syndrome, one died from a tumor, one died from COVID, one died from a skull fracture, and one died of pneumonia.”
“Fact-checkers” were quick to respond to any stories indicating that the infants’ deaths were related to Beyfortus, with factcheck.org writing in August 2023, “There isn’t evidence the [Beyfortus] shots have killed any babies, contrary to social media claims.”
But according to Banoun, “According to the HAS and EMA, 11 deaths were reported in the nirsevimab groups, one death in the pavilizumab (former equivalent drug) group and three deaths in the placebo groups. The FDA counted 12 deaths in all treated groups versus three in the placebo groups, not including the one that occurred after the follow-up period.”
“It should be noted that all deaths in the placebo groups concerned premature babies in the Griffin study,” Banoun said. “In trials involving full-term babies, all deaths involved treated subjects.”
Banoun said:
“The FDA has added one death in the placebo groups which occurred after the end of follow-up, but no mention is made of any deaths in the treated groups which occurred after this same period. Similarly, a significant number of babies are withdrawn from the trials and therefore no longer followed up after their withdrawal. This imbalance is therefore potentially more serious than published.”
Other studies also showed infant deaths connected to Beyfortus. McCullough told The Defender, “I am concerned about 3 versus 0 deaths with Beyfortus and placebo respectively in the MELODY trial published in NEJM, 2022.”
Nass pointed out another such anomaly in clinical trial results where “The deaths were said to be disproportionate between the placebo and nirsevimab groups.”
“I don’t trust the data as being reliable,” Nass said, “For instance, in this NEJM-published trial, 9.5% of babies who did not receive nirsevimab wound up with pneumonia and ‘lower respiratory tract’ RSV infections.”
“This seems awfully high,” Nass continued, “Especially when the CDC’s own study showed only 17 babies per year die from RSV. I find it hard to rely on the NEJM data.”
“The problem is that, with potentially billions of dollars riding on the outcome of a few clinical trials, there may be tremendous pressure to come up with the desired results. And there are many ways in which the desired results can be achieved,” she added.
Banoun also pointed out that while Beyfortus is administered to newborns, clinical studies tested the drug on older babies.
If we refer to the descriptions of the deceased babies, in the Domachowske study, “Only 1 was less than a month old at the time of injection (23 days), while all the others were between 1 and 7.5 months old,” she said. “We find the same panel of babies in all the other studies … in the Griffin study, the babies have a median age of over 6 months, in the Hammitt and Domachowske studies, only half the babies are under 3 months old … in the Hammitt study, the median age is 2.6 months (range 1.05 to 4.5 months).”
According to Banoun, public health authorities are aware of this discrepancy, noting that in the HAS Transparency Commission’s report on Beyfortus, Sylvie Chevret, M.D., Ph.D., professor of public health and biostatistics at France’s Université Paris Cité, said:
“In these trials, they included children who were essentially said to be in good health, so tomorrow, do you intend to give this drug to all newborns, bearing in mind that the studies did not include newborns?
“They included children who were less than three months old, of course, but up to more than 6 months.”
“The FDA and the American Association of Pediatrics jumped the gun in 2023 and were reckless in the approval and recommendation of Beyfortus for mass deployment in babies without carefully considering these issues,” McCullough told The Defender.
‘Expectant mothers should be prepared to resist’ Beyfortus for their babies
Despite these indications and possible safety signals, Banoun said that there has been no reaction so far from public health authorities in France or elsewhere.
“The only reaction to my posts was censorship and a video that was supposed to debunk my claims but actually confirmed them,” she said. “Like all critical scientists, I am censored: strict control over social networks, in particular Twitter, where we have been rendered virtually invisible since December 2023, when the European Digital Commissioner threatened Twitter with heavy fines.”
“When all debate is censored, all criticism discredited, even penalized and ostracized, can we still speak of ‘science’?” Banoun questioned, tying the censorship she’s experienced and the promotion of drugs such as Beyfortus to the concept of biopolitics.
Banoun explained that biopolitics was theorized by French philosopher Michel Foucault “to explain how power is exercised over human populations … on a global level” and “which, in our time, tends to impose health standards on all human populations [and] increasingly relies on vaccination as an alternative to care in infectiology.”
“Biopower today is exercised by an alliance of governments and health agencies with big industry. Biopolitics [also] concerns the control of populations in fields other than health: digital identity and climate,” she added.
For Banoun, financial interests are a key reason for this stance on the part of public health authorities and pharmaceutical companies.
“The market for bronchiolitis prevention will therefore represent several billion dollars for Big Pharma in the years to come. Why such a large market for a disease that is benign in the vast majority of cases? … The giants of the pharmaceutical industry are in permanent financial difficulty because of the fines and compensation they have to pay.”
“To compensate for these fines, manufacturers have to launch ‘blockbusters’ — highly profitable products that sell very well,” Banoun said, adding that the vaccine liability shield afforded to vaccines by laws such as the National Childhood Vaccine Injury Act of 1986 may be extended to treatments and drugs other than vaccines.
“It is feared that this exemption from liability will be extended to preventive therapies such as Beyfortus,” Banoun said, pointing out that U.S. and European authorities have mixed the classification of Beyfortus, considering it a vaccine in some instances and not in others.
In the U.S., the CDC’s Advisory Committee on Immunization Practices recommended adding Beyfortus to the childhood vaccine schedule, providing its manufacturers with a waiver of liability, but also recommended coding it as a drug for insurance purposes and leaving it out of the National Vaccine Injury Compensation Program (NVICP).
In addition to this liability shield, Banoun said that, in France, midwives and nurses reportedly “receive a bonus for each injection — Sanofi pays a sum to each hospital, which is then redistributed to the injectors.”
Experts advised parents and physicians to be wary of Beyfortus.
“Physicians and parents should be conservative in deciding on Beyfortus. I do not recommend it for parents who are expecting healthy newborns or babies without severe pulmonary disease,” McCullough told The Defender.
Banoun said “Expectant mothers should be prepared to resist,” noting the White House’s and CDC’s efforts to promote Beyfortus and pressure placed on new mothers in French hospitals, where “nursing staff insist on giving it to the mother up to four or five times during her stay in the maternity ward.”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
January 3, 2024
Posted by aletho |
Mainstream Media, Warmongering | Beyfortus, France, Nirsevimab, RSV |
Leave a comment
An “elite” and influential group of obesity specialists over the last decade pocketed at least $25.8 million in payments from Novo Nordisk, maker of weight loss drugs Wegovy and Saxenda, in exchange for promoting the drugs in their lectures, treatment guidelines, clinics and medical societies, according to an investigation by Reuters.
“Those payments are part of a campaign to convince U.S. doctors to make Wegovy one of the most widely prescribed drugs in history — and to persuade skeptical insurers to pay for it,” according to the report.
Wegovy and Saxenda have rapidly transformed the treatment of obesity in the U.S., with a boom in prescriptions so big in 2023 that JP Morgan doubled its 10-year sales projection, predicting sales of $71 million for the drugs by 2032.
Despite the drugs’ serious side effects — including major gastrointestinal issues, self-harm behaviors and cancers — the Association of American Pediatrics recommends the drugs in its new clinical guidelines, the American Medical Association urges insurance carriers to cover the drugs, and the mainstream and medical press heavily promote them.
‘They have pushed for urgent prescribing of Wegovy’
Reuters examined data from the federal Open Payments database, which reports payments made by pharmaceutical companies to doctors, other medical professionals and teaching hospitals for consulting, speaking, research, travel or meals. It analyzed payments for speaking, consulting, food and travel for two of Novo’s obesity drugs, Wegovy and Saxenda.
The analysis also excluded payment for research.
Overall, Reuters found at least 57 U.S. physicians each accepted a minimum of $100,000 from Novo in payments related to the two drugs over 10 years. It also found Novo made other large payments to some of those same doctors, but the payments were not classified as related to a particular drug and were not counted in the $25.8 million total.
Of that group, 41 of the physicians run weight-management clinics, work at academic hospitals, write obesity-treatment guidelines or hold top positions at medical societies.
Collectively, the report said:
“[They] have pushed for urgent prescribing of Wegovy and similar medicines to a large proportion of patients with obesity and for comprehensive coverage by government and private insurers. The company and some of its paid experts have called denying coverage tantamount to discrimination against people with obesity, rooted in the faulty notion that they are to blame for their condition.”
Reuters also analyzed Novo’s spending among experts involved in writing five prominent sets of obesity-treatment guidelines for doctors. Among the 109 guideline writers and editors, 53 had accepted payments from companies selling or developing obesity drugs — $8 million of the total $12.4 million of those payments were from Novo.
In a statement provided to Reuters, Novo said, “Responsible engagement between pharmaceutical companies and the medical community is good for patients and advances care and science.”
Since the Affordable Care Act created the Open Payments system over a decade ago, it has been easier to expose the kinds of financial conflicts of interest identified in the report.
However, the increased transparency hasn’t stemmed the flow of industry money, Reuters found. “Companies’ annual payments have surged from $6.5 billion in 2014, the first full year data were collected, to $12.6 billion last year,” the report stated.
Dr. Arthur Kellermann, a health administrator and former dean of the Uniformed Services University of Health Sciences, the U.S. military’s medical school, told Reuters the investigation sheds light on a long-standing problem in the drug industry.
He called the payments “morally and ethically way over the line,” adding:
“The pharmaceutical industry still sees value in paying medical thought leaders to promote their products, and too many of them are happy to sign up for a six- or seven-figure check …
”As sales grow, Medicare and the insurance industry come under intense pressure to pay for these hugely expensive drugs … The end result is that everybody’s healthcare costs go up.”
Another recent report by investigative journalist Lee Fang similarly found a wide network of celebrities, physicians, patient advocacy groups, public health experts, academics, and community leaders have appeared in dozens of media outlets to tout the drugs without disclosing their financial ties to Novo Nordisk.
Which doctors take money from Novo Nordisk?
The report profiled several key physicians taking money from Novo.
For example, Novo paid Lee Kaplan, M.D., Ph.D., chief of obesity medicine at Dartmouth’s medical school, former head of Obesity, Metabolism and Nutrition Institute at Massachusetts General Hospital, and associate professor of medicine at Harvard, $1.4 million for consulting work and travel related to the two drugs between 2013 and 2022.
It also paid him another $976,019 million during that same period for unspecified reasons.
Kaplan, who teaches a popular obesity course taken by physicians seeking certification in obesity medicine or continuing education credits — for which Novo contributed $10,000 this year — dismissed the idea that he is a mouthpiece for the drugmaker. He told Reuters he accepts money from numerous companies and “that he’s not beholden to any one drugmaker.”
Another physician, Dr. Donna Ryan, former president of The Obesity Society and member of The Diplomate at the American Board of Obesity Medicine, has taken more than $1 million from Novo over the last decade, including $600,691 related to Wegovy and Saxenda.
Ryan was instrumental in persuading the U.S. Office of Personnel Management to cover Wegovy and similar drugs for millions of federal workers, an agency official told Reuters.
In the process, she connected government officials with two key groups: the Obesity Action Coalition, a nonprofit advocacy group, and the STOP Obesity Alliance at George Washington University. Both have ties to drugmakers.
Novo is the Obesity Action Coalition’s top corporate donor, paying it more than $500,000 annually.
STOP medical director Dr. Scott Kahan, who will assist in writing The Obesity Society’s new “standards-of-care” guidelines that primary-care doctors commonly use as a quick-reference guide, has accepted more than $300,000 from Novo.
Dr. Jamy Ard, of Wake Forest University, the incoming president of The Obesity Society who will oversee the guideline writing, has taken over $200,000 from Novo.
Ryan told Reuters she had no qualms about taking such payments, “Being a purist isn’t helping anyone,” she told Reuters.
The report also quoted Ryan speaking to a group of doctors at a conference, where she argued that these blockbuster drugs have been positive for both patients and investors. “There is nothing wrong with money,” Ryan said.
She and obesity specialist Dr. Ken Fujioka, director of the Scripps Clinic Nutrition and Metabolic Research Center in San Diego, have taken 130 Novo-paid trips over the past decade, traveling to make speeches and do consulting.
They said the travel allows them to provide medical advice that is valuable to patients, physicians and the manufacturer.
But other doctors disagreed. Dr. Adriane Fugh-Berman, a professor of pharmacology and physiology at Georgetown University Medical Center who studies pharmaceutical marketing practices, told Reuters :
“These highly paid doctors end up drowning out the voices of people who aren’t being flown around to every medical meeting. As a result, there’s not a lot of resistance to the prevailing industry-funded view.”
‘Serious and under-discussed risks for pregnant women’
The 2020 U.S. approval of Novo Nordisk’s Saxenda, a once-daily injection for weight loss, opened a new era of pharmaceutical-based weight management, The Defender reported.
This was followed, in June 2021, by the licensing of Wegovy, and less than a year later of Ozempic, which is indicated for Type 2 diabetes, but contains the same active ingredient, semaglutide, as Wegovy, and is prescribed off-label for weight loss.
Semaglutide drugs are taken as a once-weekly injection, which is considered a benefit compared to a once-daily jab. Liraglutide is a daily shot. Semaglutide is also available as a once-daily pill under the brand name Rybelsus, another Novo drug.
These drugs mimic the GLP-1 hormone, which assists patients in losing weight by regulating their appetite.
In November 2023, the FDA approved Eli Lilly’s Zepbound, another injectable diabetes drug, for weight loss. The active ingredient in Zepbound, tirzepatide, sets this drug apart from Wegovy and Ozempic but it works similarly through a weekly injection.
Tirzepatide is sold by Eli Lilly as a diabetes drug under the trade name Mounjaro.
These approvals were accompanied by what Fang called a Novo Nordisk-driven “aggressive campaign to persuade Americans of the merits of semaglutide.”
According to a KFF Health poll, 45% of adults would take a “safe and effective prescription weight loss drug,” including 59% of those trying to lose weight.
Enthusiasm fell to just 23%, however, when they learned that treatment involved a routine injection, to 16% if either insurance did not cover the high monthly cost or if the drug was not specifically approved for weight loss.
The surging popularity of the medication led to shortages and made Novo Nordisk one of the most valuable global pharmaceutical companies, behind Johnson & Johnson and Eli Lilly.
The shortages raised concerns because the drugs are not made for short-term use. Studies show that when people stop taking them, they regain much of the weight they lost, or potentially gain even more weight. Most people who start taking the drugs and want the effects to last will have to stay on them long-term.
But recent pharmacy claims data shows that most people who start taking Wegovy stop taking it within a year, some because of side effects and some because of the high cost of the drugs.
In addition to suicidal ideation and thoughts of self-harm, pancreatic cancer and gastrointestinal disorders, other adverse effects linked to semaglutide are also becoming apparent. A study using data from EudraVigilance, also found metabolic, nutritional, eye, renal, urinary and cardiac disorders were also reported.
The drugs also carry serious and under-discussed risks for pregnant women.
Despite the high drug cost and the associated risks, there is an ongoing debate about whether insurance companies and Medicare should cover the cost of weight loss drugs, which would increase profits exponentially.
Reuters reported that Wegovy’s U.S. prescribing label recommends the drug for anyone with a body mass index (BMI) of 30 or higher, the threshold for obesity and for people with a 27 BMI who also have a weight-related medical condition.
That would cover about 46% of American adults — about 120 million people, according to the report.
A study published in March in the NEJM estimated that if Medicare were compelled to cover Wegovy, with an estimated 23% discount, it would cost $27 billion to treat just 10% of patients with obesity enrolled in Medicare. That would equal nearly a fifth of the yearly spending for Medicare’s program covering prescription drugs.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
December 10, 2023
Posted by aletho |
Corruption, Science and Pseudo-Science, Timeless or most popular | United States |
Leave a comment
During the UK Parliamentary debate on the WHO Treaty there was a noticeable contrast between those supporting the petition and those opposing it. This article analyses the arguments made by those rejecting the petition, drawing on insights from Behavioural Science.
On 17 April 2023, a petition [1] was debated in the UK Parliament calling for the Government “to commit to not signing any international treaty on pandemic prevention and preparedness established by the WHO, unless this is approved through a public referendum.” The petition had received 156,086 signatures. Of the thirteen Members of Parliament (MPs) who spoke during the debate [2] four strongly supported the motion, three took a more neutral stance, and six strongly opposed the petition or elements of the argument. Examples of arguments in support of the petition can be viewed in a collation of clips taken from the video of the debate [3].
There was a noticeable contrast between the arguments presented by MPs supporting the petition — who exhibited concern for the constituents who had signed the petition and approached them directly — and those opposing it. All those who, like the petitioners, were concerned about the growing power and influence of WHO and threats to national sovereignty were familiar with the contents of the so-called ‘pandemic treaty’ [4], since labelled the WHO CA+, as well as proposed amendments to the International Health Regulations (IHR) [5]. While some opposing the petition were also familiar with the document, others had not even read it, prompting Andrew Bridgen (MP for North West Leicestershire) to plead with members to do so.
Those concerned about these proposals presented well-reasoned arguments reflecting an understanding of the history of WHO [6], its many failures during Covid-19, and its current problematic relationships with non-state funders [7,8]. Those supporting WHO’s proposals uncritically supported WHO, focusing on its public health successes and ignoring obvious concerns. Perturbed by the lack of parliamentary scrutiny of the Covid response measures, some MPs worried that the UK government, having played a leadership role in drafting the treaty, might ratify it without parliamentary debate. This reservation was flatly denied by those opposing the petition, with some denying that WHO would in any way threaten UK sovereignty, that its role would remain advisory in nature, and that those opposing the treaty were in effect opposing international cooperation.
This article analyses the arguments made by those rejecting the petition, drawing on insights from Behavioural Science. During the debate, these MPs tended to rely on the following tactics:
- Using derogatory language or false claims to discredit speakers and their arguments
- Making inaccurate and unsubstantiated statements
- Using globalist slogans
- Patronising the petitioners
- Using the debate as an opportunity for party-political point-scoring
- Downplaying or normalising threats to sovereignty
- Promoting internationalism over sovereignty.
The debate was a sad reminder that it is not necessarily the quality of arguments, or even the sincerity of the individuals making them, that wins the day.
1. Using derogatory language and labels to discredit speakers and their arguments
A tactic used to shut down discussion and debate was to attach derogatory labels to those supporting the petition. In the debate, two such labels used in relation to the Covid event and the pandemic treaty were ‘conspiracy theory/theorist’ (ten references made by four speakers) and ‘anti-vax’ (one speaker). Some opposing the petition used these labels early in their presentations, their comments and tone indicating that these were untenable positions that no sane person could possibly subscribe to.
Using such labels at the beginning of the debate set the scene, immediately employing a behavioural science tactic to prime the participants and the wider audience. Priming is a ‘nudge’ [9] tactic; techniques that are used to modify people’s behaviours or emotions in a way that is unconscious and therefore difficult to identify or counter. Priming [10] occurs when the emotional attachment or views held about one issue are then used to influence the emotional attachment on a separate and unrelated issue; an emotional contagion if you like. This can be utilised to produce a positive or negative relationship. Over the past three years in particular, the phrase ‘conspiracy theorist’ has become strongly and negatively associated with an archetype of someone whose views are not based in fact and who are not community minded, and therefore not socially acceptable. By stating in his introductory comments that “I have no time for conspiracy theories”, leader of the debate Nick Fletcher (MP for Don Valley) activated this already negative mental construct and associated it with the question of the WHO pandemic treaty. Whether this was purposeful or not is debatable but concerns about conspiracies do seem strangely placed in a debate which should be about publicly documented proposals, and UK and international legislation.
Similarly, Sally-Ann Hart (MP for Hastings and Rye), who herself was committed to representing the concerns of constituents who had signed the petition, warned that, “We must be wary of … conspiracy theories distorting the facts and scaring people. Transparency of debate is therefore needed to squash those conspiracy theories.”
Some comments could only be described as invective. Language such as that used by John Spellar (MP for Warley) was entirely inappropriate in the context of a Parliamentary debate:
… the poisonous cesspit of the right-wing conspiracy theorist ecosystem in the United States … an appalling subculture of those who live by conspiracy theories … Unfortunately, we have some people — a very limited number … who wallow in the realm of conspiracy theories.
The ‘conspiracy theorist’ label has become a catch-all term used to discredit numerous perspectives that disagree with the dominant narrative. It has also taken on the power of a curse, which those who hope to remain accepted by their peers must protect themselves from by declaring their immunity.
Another such label is ‘anti-vax’, used by Mr Spellar who interjected early in Mr Fletcher’s introduction:
I thank the hon. Gentleman … for highlighting both smallpox and polio. Is the fact of the matter not that it has been a worldwide vaccination programme that has enabled us to achieve that? Does that not demonstrate the falseness of the anti-vax campaigns?
This is another example of priming, where an exceptionally negative construct (anti-vax), which was set up in mainstream and social media over the past few years, is associated with those who may have genuine concerns about the powers being delegated to a non-elected body. When attached to a person, the related term ‘anti-vaxxer’ is an example of an ad hominem attack [11], which is an example of a false argument. Instead of the argument being discussed on its own merit in terms of data or facts, the audience and other participants are misdirected toward a perceived ‘failing of character’ in those who might have a different view and legitimate questions.
Mr Spellar used this terminology to discredit those wary of vaccinations, in particular the Covid-19 genetic therapy. He continued his interruption of Mr Fletcher’s introductory remarks with the following tirade against academic gastroenterologist Dr Andrew Wakefield who, in 1998, co-authored a research study in The Lancet, linking inflammatory bowel symptoms in 12 autistic children to the Measles-Mumps-Rubella (MMR) vaccine:
Part of this argument has been about vaccination. We go back to Dr Wakefield and that appalling piece of chicanery that was the supposed impact of the measles, mumps and rubella vaccine, which has now been completely exposed and discredited. Indeed Mr Wakefield is now no longer a recognised doctor.
This argument is an example of ‘false equivalence’ [12], another propaganda tool that has the effect of misdirecting the audience away from the key facts of the debate. Those who doubt the safety and efficacy of the novel Covid ‘vaccine’ have not necessarily questioned the safety and efficacy of all other vaccines, and should therefore not be considered ‘anti-vaxxers’. By associating arguments against the Covid shot with the MMR vaccine debacle, the purpose is to tar objections to this entirely novel and inadequately tested therapy with the same brush as arguments levied against an earlier, unrelated, conventional vaccine.
Mr Spellar’s interjection also reflects another tactic of those who wish to quash debate, namely the use of threats to intimidate those who might be inclined to consider alternative narratives. The story of the suppression of harms caused by the MMR vaccine has much in common with the current censorship of reports of serious adverse events and deaths following the Covid injections. Raising the 25-year-old case of Dr Wakefield who is “no longer a recognised doctor” represents a threat, already a reality for many ethical doctors and scientists, that those who speak out against the harms caused by the Covid injections face being dismissed and deregistered.
2. Using inaccurate and unsubstantiated statements
Justin Madders (MP for Ellesmere Port and Neston) also used derogatory language in denying concerns about threats to national sovereignty posed by global organisations such as WHO:
On the absurd side, a narrative has been created that the World Health Organization is a body intent on world domination. Borrowing tropes from conspiracy theories, I found one website referring to the WHO as ‘globalists’ … That sentiment is clearly ludicrous, as is the reference to the WHO being owned by Bill Gates or the Chinese Government.
The treaty has nothing to do with Bill Gates, and it is not the first step in creating a world-dominating authoritarian state.
The first sentence in the quote above is an example of a behavioural science nudge tactic called ‘framing’. In framing, words, metaphors and perspectives are used in a way that makes the message more attractive and activates certain emotional reactions. The image created by the MP’s statements is quick to evoke a mental picture of a film-like villain plotting to take over the world. Being ‘absurd’ (untrue) and a ‘narrative’ (story), this should clearly be discounted.
Beyond the language used, Mr Madders’s claims are not substantiated and as such are simply opinions. Firstly, as the United Nations (UN) agency responsible for global public health, WHO can indeed be considered a ‘globalist’ organisation, along with numerous other international bodies such as other UN agencies, the World Bank and International Monetary Fund, the World Economic Forum (WEF), and international corporations and foundations. But, largely due to the growing influence exerted over national governments by WHO and other unelected supra-national bodies during Covid, the term ‘globalist’ has taken on more sinister connotations. Its use by those critical of the dominant narrative may account for Mr Madders treating the term as a ‘red flag’.
Secondly, Mr Madders may be unaware of the significant changes to WHO’s funding model that have taken place in recent years, with assessed contributions [13] from Member States having declined to less than 20% of WHO’s financing, and Bill Gates now being one of its major funders. WHO’s own website records that, as of Quarter 4 of 2021, the Bill and Melinda Gates Foundation (BMGF) was their second-largest donor (9.49%) after Germany [14]. While on this point, Steve Brine (MP for Winchester) asserted that “the UK is the second-largest contributor to the WHO”, which is incorrect; in fact, the UK is the sixth-largest contributor (5.99%). Gates is also a founding partner and second-largest contributor to Gavi, the Vaccine Alliance, which is the fifth-largest funder of WHO (6.43%). And with 56.14% of BMGF’s funding going to support WHO’s Headquarters [15], it is unlikely that “The treaty has nothing to do with Bill Gates”, as asserted by Mr Madders.
Many unsubstantiated statements regarding Covid ‘vaccine’ safety and effectiveness were also made during the debate. Anne-Marie Trevelyan (Minister of State, Foreign, Commonwealth and Development Office) asserted that “AstraZeneca saved lives worldwide”, despite the use of this adenovirus viral vector vaccine being restricted or suspended in numerous countries due to many reports of recipients suffering blood clots [16].
Similarly, Mr Spellar, referring to the Pfizer mRNA ‘vaccines’, stated that it “certainly was not unproven or unsafe, and it had a huge beneficial impact across the world.” There is, in fact, mounting evidence showing that the Covid injections, released under emergency use authorisation before adequate testing could be undertaken, have been neither safe nor very effective. All vaccine adverse events tracking systems, including the Medicines and Healthcare products Regulatory Agency (MHRA) Yellow Card system in the United Kingdom, the European Medicines Agency’s EudraVigilance system in the European Union, and the Vaccine Adverse Events Reporting System (VAERS) in the United States, have recorded unprecedented numbers of serious adverse reactions, including deaths. Furthermore, an increasing number of studies are reporting evidence of a broad range of serious adverse events [17]. An independent systematic review of serious harms of the Covid-19 vaccines, currently in pre-print, adds significant weight to these findings [18].
Furthermore, after a group of scientists and medical researchers successfully sued the United States Food and Drug Administration (FDA) under the Freedom of Information Act (FOIA) [19] to release many thousands of documents related to licensing of the Pfizer-BioNTech Covid-19 vaccine, it was revealed that early trials had resulted in hundreds of adverse reactions [20 (Appendix 1)]. This information had been withheld from the public by the authorities.
The injections have also been been unable to stop SARS-CoV-2 infection or transmission, with Dr Peter Marks of the FDA admitting in a letter responding to a citizens’ petition that proof of efficacy had not been required for authorisation [21]:
It is important to note that FDA’s authorization and licensure standards for vaccines do not require demonstration of the prevention of infection or transmission. (p.11)
Furthermore, the applicable statutory standards for licensure and authorization of vaccines do not require that the primary objective of efficacy trials be a demonstration of reduction in person-to-person transmission. (p.13)
In addition, there is growing concern that claims that the boosters prevent severe illness and deaths amount to a “wishful myth” [22].
Three years of pro-vaccine propaganda and ongoing efforts to censor reports of vaccine harms have effectively blinded many people to the possibility that the rollout of Covid injections may be related to the sharp rise in excess deaths now being experienced in many countries [23; 24]. This is despite the fact that many vulnerable people, such as the elderly and those with multiple comorbidities, had died previously as a result of Covid-19, lockdown measures and medical interventions.
Despite having had the opportunity to peruse the evidence presented by the petitioners, Mr Spellar was still sure that the vaccination campaign had been a huge success, stating:
… mobilisation of [the] intellectual power and production capacity [of the major pharmaceutical companies] in producing a vaccine in record time to stem the tide of covid was absolutely magnificent.
3. Using globalist slogans
Just as certain terms (conspiracy theorist, anti-vaxxer) have become modern-day curses causing those so labelled to be socially shunned, so have other terms and slogans become the mantras of those wishing to demonstrate their membership of the mainstream. These catchy but often meaningless slogans are building blocks of a collective reality, introduced and normalised through the presentations, publications and public relations communications of powerful individuals, and globalist organisations such as the UN, WHO, WEF and BMGF.
Mr Madders, for example, echoed Bill Gates [25] when he stated: “We need to be better prepared for the next pandemic.” This also represents an unsubstantiated claim, as it ignores the reality that pandemics are actually extremely rare. Since 1900, only five pandemics, each responsible for over one million deaths, have broken out, namely the Spanish flu (1918-1920), the 1957-1958 influenza pandemic, the Hong Kong flu (1968-1969), the AIDS pandemic (ongoing since 1981), and Covid-19 [26]. It also powerfully illustrates the effectiveness of presupposition, where the speaker inserts a statement or assumption as a fact agreed by all and therefore requiring no evidence of its own. The phrase “the next pandemic” provides a nudge by inserting itself unconsciously into the psyche of the listener and readily bypassing the conscious thought process [27].
The Covid event did, however, demonstrate that a pandemic can mean big gains for certain people. It can literally be used to “reset our world” [28], creating unprecedented numbers of billionaires while destroying the lives of billions or others, stripping citizens of their rights and freedoms, unleashing a tyrannical and repressive security apparatus, and creating a ‘polycrisis’ [29], in response to which governments and even citizens will beg for unprecedented levels of global control.
One of the most meaningless slogans, which appears to have been invented by the UN at the beginning of the Covid event, and which has become a mantra reiterated by countless organisations and individuals, is ‘nobody is safe until everyone is safe’. It is not clear what this unsubstantiated statement even means, but what is clear is that it is demonstrably untrue. Nonetheless, this mantra was recited in some form by four speakers, with Anne McLaughlin (MP for Glasgow North East) stating, “It is only when the world is safe from Covid-19 that any of us are truly safe.”
Not only does such an obvious fallacy, a propaganda trope, have no place in a parliamentary debate, its use as some type of rational fact by four MPs across the political spectrum does bring into question the quality and independence of any literature provided to them ahead of this event. It is worth considering this much-used slogan and its ramifications in terms of any safety incident. The ideology underpinning it is one of collectivism, even socialism, in that the individual and their relative safety is merely incidental compared to the safety of all. Some might argue that this contradicts the fundamental principles of the International Declaration of Human Rights, which puts the individual at its core. Certainly, it is not an idle statement and reflects the underlying changes being proposed by WHO, which is seeking under their ‘One Health’ initiative [30] a more far-reaching remit where ‘everyone’ will include not only all sovereign citizens of participating nations, but animals and the environment as well.
Slogans infuse documents produced by UN agencies such as WHO. In referring to the zero-draft of the Pandemic Treaty, Preet Kaur Gill (MP for Birmingham, Edgbaston) used a number of them, including: ‘leave no country behind’, ‘global health is local health’, ‘we are stronger together’, and ‘vaccine equity’. Trotting out vacuous statements like this might be appropriate at a protest rally but should have no place in a parliamentary debate. Slogans are rallying cries. They are right-sounding and apparently well-meaning, even moral, in nature. Their repetition is quite hypnotic and they seem to act as spells, potentially binding those who faithfully recite them to an outcome they may live to regret [31].
The repetitive nature of any phrase or slogan is a tool of both behavioural science and propaganda. Both the repetitive effect and the rhythmic phrasing allow such phrases to easily enter the unconscious. Over time we simply accept the statement as true, as it bypasses our conscious thought processes that might critically assess such a phrase and see it as false or simply nonsensical. The use of such tactics, particularly by people in positions of authority or trust, allow the effect to be amplified. This is known as the ‘messenger effect’. Simply put, we are more likely to trust the message because it was issued by someone representing expertise and trust [32].
One such case relates to the slogan ‘vaccine equity’. Referring to the “terrible divide in coverage between richer countries and the global south,” Ms Gill lamented that “just 27% of people in low-income countries have received a first dose of a Covid vaccine.” What she does not go on to say, disappointingly, is that there was no correlation between high vaccination rates and low death rates from Covid-19. Indeed, some low-income countries (especially in Africa) with young populations and low vaccination rates experienced very low death rates due to Covid-19, while the USA, one of the richest and most highly vaccinated countries in the world, had one of the highest Covid-19 death rates [33].

Figure 1: Comparing Covid-19 deaths in Africa and the USA [33]
4. Patronising the petitioners
Regarding the aim of the petition, which was to request that a referendum be held before the Government could agree to signing the pandemic treaty, Mr Fletcher declared:
Referendums are divisive; they polarise positions and leave a lasting legacy of division. Whether a referendum is appropriate is for the Government to decide, and if they think it is, they must make all the facts known. I suggest that petitioners, while playing their part in the education process, must do so in a sensible manner.
The patronising tone of this comment is ironic. While the referendum on Brexit did indeed sharpen the edge between ‘Leavers’ and ‘Remainers’, the UK Government’s Covid-19 response was possibly even more effective at dividing the populace into camps and pitting one side (those who complied with the mandates) against the other (those who chose not to comply). Furthermore, insisting that citizens should be “sensible” ignores the fact that constituents in favour of a referendum contacted their MPs to raise thoughtful, well-researched concerns, while some MPs arguing against the referendum tended to rely on slogans, unfounded generalities, and invective, rather than “sensible”, factual, reasoned arguments.
Mr Spellar not only used disparaging language to deny the request for a referendum, but also predicted that it would be rejected by the House:
We cannot be arguing to have [a referendum] for every bloomin’ issue, every policy and every treaty. … What we are seeing is overreaction and hysteria, and I would argue that we should give the petition a firm rejection, as I am sure we would do if it ever came to the Floor of the House of Commons.
Inasmuch as MPs in the UK are supposed to represent and take seriously the concerns of their constituencies, it is disturbing that an elected Member should respond with such contempt to a petition signed by more than 150,000 people.
5. Party-political point-scoring
Disappointingly, despite the importance of the debate and the number of citizens who had taken the time to express their concerns about the pandemic treaty, Ms McLaughlin and Ms Gill spent much of their time criticising the Conservative Government’s response to the Covid event. Instead of focusing on the debate, they chose to score party-political points by indicating the readiness of the Scottish National Party and Labour Party to implement WHO’s agenda, including enabling vaccine equity; sharing technology, knowledge, and skills; and strengthening global health systems using, ironically, the failing National Health Service as a model.
6. Downplaying or normalising threats to sovereignty
The Covid-19 event has been a classic case of the popular dialectic of ‘Problem-Reaction-Solution’. The engineered over-reaction to the problem of Covid-19 (whether or not there was an engineered virus), and the subsequent societal fall-out, have left traumatised people and their governments desperate to be better prepared for the much-anticipated ‘next one’, and ready to accept a ‘solution’ that few would have countenanced just four years ago.
In her presentation, Ms Gill expressed the need for an international approach to tackle transnational threats and improve global public health:
Negotiating an effective international treaty on pandemic preparedness is an historic task, but, if we can achieve it, it will save hundreds of thousands of lives.
If we can use the WHO to support basic universal healthcare around the world, infectious diseases are less likely to spread and fuel global pandemics.
It is through multilateral efforts, strengthened through international law, that we can ensure that the response to the next pandemic is faster and more effective, and does not leave other countries behind.
… the Opposition absolutely support the principle of a legally binding WHO treaty that sets the standard for all countries to contribute to global health security.
We need a binding, enforceable investment and trade agreement among all participating countries to govern the coordination of supplies and the financing of production, to prevent hoarding of materials and equipment, and to centrally manage the production and distribution process for maximum efficiency and output in the wake of a pandemic being declared.
The last few comments (underlined above) point to one of the most worrying issues for those concerned about sovereignty: if accepted, the pandemic treaty and amendments to the IHR would no longer be non-binding recommendations subject to government oversight but would become legally binding. WHO would be given legislative powers to mandate medical and non-pharmaceutical interventions; to commandeer intellectual property, production capability and resources; and to sanction those who refused to comply.
Some MPs downplayed concerns about these threats to national sovereignty. Mr Madders stated that “creating a global treaty [was] entirely reasonable and responsible” and that it was possible to “both protect our values of freedom and democracy and work more closely with other countries in the face of a global threat.”
Mr Spellar agreed, noting that they were “signatories to hundreds of treaties around the world” and that signing trade treaties was “part of engaging with the world.” He added that during Covid, “international scientific cooperation” had “enabled us to produce a vaccine within something like twelve months instead of the normal ten years … [thus] stabilising the situation.” What was not mentioned is that it was not primarily international collaboration among scientists that allowed the rapid deployment of these Covid-19 countermeasures, but the institution of emergency use authorisations, which allowed inadequately tested products to be dispensed worldwide. Far from “stabilising the situation”, these injectables continue to cause unprecedented numbers of adverse events and deaths, resulting in ongoing destabilisation of society post-Covid.
Steve Brine (MP for Winchester) observed that, “We cede sovereignty through membership of organisations. We cede the sovereignty to go to war by being a member of NATO.” It is true that all manner of treaties exist between countries and that these are essential for international cooperation; but cooperating as sovereign nations is entirely different to taking instructions from an unelected, supra-national body that is unaccountable to populations. Once in place, WHO’s pandemic treaty and the amendments to the IHR threaten to reduce national sovereignty, giving full power to WHO and its director-general to call pandemics and health emergencies and to regulate the responses of member states.
Those in favour of the pandemic treaty provided no evidence that a one-size-fits-all, legally mandated response to future pandemics would actually prove effective. In fact, Covid-19 was an object lesson in the foolishness of imposing the same public health ‘solutions’ on radically different nations and communities. In reality, mandating centralised protocols disrespects human rights, cultural diversity, national sovereignty, the scientific method, and innovation in healthcare. Instead of trusting human ingenuity to create a multitude of locally appropriate responses, it increases the risk of spectacular failure should the single global solution prove ineffective.
In an attempt to counter fears about a loss of sovereignty, Mr Madders stated that “We live in a liberal democracy and … are determined to keep it that way.” He denied people’s:
fears that the treaty will restrict freedom of speech to the extent that dissenters could be imprisoned, that it will impose instruments that impede on our daily life, and that it will institute widespread global surveillance without warning and without the consent of world leaders … [and that] Under this treaty, those things will apparently be done without our Government having a say.
He did, however, acknowledge that the measures mentioned above were “already in the power of the Government under the Public Health (Control of Disease) Act 1984.” Referring, without giving any details, to “fact checkers” and an unnamed “WHO spokesperson”, he reassured citizens that “WHO would have no capacity to force members to comply with public health measures.” The tyrannical actions during Covid of governments worldwide against their own citizens — many of whom assumed that they did, in fact, live in a “liberal democracy” — makes one wonder why these governments would behave any more independently in future, especially if legally required to follow WHO’s dictates. The repressive regulations and laws passed in various countries since 2020 suggest that this is unlikely, as governments seem to have become addicted to the sweeping emergency powers granted them by this convenient global ‘pandemic’.
Mr Madders and Ms Gill also attempted to allay citizens’ fears by pointing out that there was “over a year of negotiations to go” and that the treaty “would still have to be ratified by the United Kingdom”. Ms Gill also commented that:
The draft treaty is primarily about transparency, fostering international cooperation, and strengthening global health systems … the very first statement in the zero draft text reaffirms “the principle of sovereignty of States Parties” [and that] the implementation of the regulations “shall be with full respect for the dignity, human rights and fundamental freedoms of persons.”
Noting the dismissive attitude of the majority of MPs to the petitioners’ concerns, there is little chance that another year of negotiations will convince the UK Government to reject the treaty.
7. Promoting internationalism over sovereignty
The UK, as an erstwhile imperial and colonial power, continues to play a leadership role internationally. This may be why some MPs, such as Ms McLaughlin, could not believe that WHO might threaten UK’s sovereignty:
The treaty would have absolutely no effect whatsoever on the UK’s constitutional function and sovereignty … [Imagine a] terrible situation whereby the UK might be unable to make its own decisions if it is outvoted by other countries … the UK is a leading member of the WHO and a primary architect of the treaty, so that is not what is happening here.
Anne-Marie Trevelyan (Minister of State, Foreign, Commonwealth and Development Office) also stressed that the UK was:
a sovereign state in control of whether we enter into international agreements … with its voice, expertise and wisdom, and our trusted partner status with so many other member states in the UN family, [it] is respected and listened to.
Ms Trevelyan also referred to the UK’s role as “a global leader, working with CEPI, Gavi and the WHO,” stating that she was “proud to lead the fundraising for Gavi and COVAX.”
A deep chasm appears to have formed between the UK Government and its people. The discussions during this debate suggest that a minority of MPs [3] [link to PANDA video] view themselves as representatives whose duty it is to serve their constituents and respond to their concerns. Most, however, appear to have shifted their focus and allegiance to the international sphere, identifying as members of the “UN family”, playing a leading role in developing WHO’s pandemic instruments, and raising funds, which will ultimately benefit vaccine manufacturers and their investors, impoverishing the majority in the process. Under these circumstances, it is clear why Parliament is unwilling to risk a referendum on WHO’s Pandemic Treaty. There are just too many globalist interests at stake.
At home, increasing numbers of UK citizens are growing weary of a government that speaks glibly of ‘no country left behind’, while leaving its own nation in the dust. Where the people are concerned, trust is gone.
As Danny Kruger (MP for Devizes) warned:
At the moment, we do not have a commitment from the Government that they would bring the proposals to Parliament, which is very concerning. They say that in our interconnected world we need less sovereignty and more co-operation, which means more power for people who sit above the nation states. I say that in the modern world we need nation states more than ever, because only nation states can be accountable to the people, as the WHO is not.
Concluding comments
After two-and-a-quarter hours of deliberation, Mr Fletcher concluded the debate by thanking the Minister for assuring Members that UK sovereignty was not at risk, and then delivering the most inconclusive resolution:
That this House has considered e-petition 614335, relating to an international agreement on pandemic prevention, preparedness and response.
For the 156,086 citizens and their representatives who had made the effort to engage Parliament thoughtfully and actively using the relevant democratic process, this ‘resolution’ resolved nothing at all. The exercise amounted to all form and no substance; not only were requests for a referendum dismissed out of hand without adequate discussion, but there were indications that the matter might not even be discussed in the House of Commons.
Illustrating just how little impact was made by those representing the petitioners despite the strength of their arguments, subsequent to the debate and in response to this petition, the government’s official response published on their website [1] commenced with the words:
To protect lives, the economy and future generations from future pandemics, the UK government supports a new legally-binding instrument to strengthen pandemic prevention, preparedness and response.
This ominous response was followed by the now familiar slogan that would sit comfortably in the pages of Orwell’s 1984 but has no place in an official government statement: “Covid-19 has demonstrated that no-one is safe until we are all safe.” Its use further erodes the expectations that such debates will be carried out without bias, undue influence, or ignorance.
MPs have a duty of care to their constituents to ensure that they are as knowledgeable as possible about the issue being debated, and that they consider the facts rationally and honestly; and citizens deserve to have their concerns taken seriously. Yet two critical questions remain unanswered: firstly, having explicitly stated their support for WHO’s pandemic instruments, will the UK Government bring this matter to Parliament to be debated? And secondly, would agreement with these instruments, ‘in effect’ if not legally, mean the relinquishment of sovereignty? After all, if the only way the UK will be able to make a sovereign decision in future is by removing itself from membership of WHO, then why would the country wish to sign this treaty in the first place?
References
- UK Government and Parliament, Petition: ‘Do Not Sign Any WHO Pandemic Treaty Unless It is Approved Via Public Referendum’, (Debated 17 April 2023) <https://petition.parliament.uk/petitions/614335> [accessed 15 June 2023]
- parliamentlive.tv, ‘Video Recording of Westminster Hall Debate: e-petition 614335, Relating to an International Agreement on Pandemic Prevention, Preparedness and Response’, (17 April 2023) <https://parliamentlive.tv/Event/Index/d667d23f-1bd5-4c71-8237-3dd240de0651> [accessed 25 June 2023]
- PANDA Video
- World Health Organization, ‘Bureau’s text of the WHO convention, agreement or other international instrument on pandemic prevention, preparedness and response (WHO CA+)’, (2 June 2023) <https://apps.who.int/gb/inb/pdf_files/inb5/A_INB5_6-en.pdf> [accessed 25 June 2023]
- World Health Organization, ‘Article-by-Article Compilation of Proposed Amendments to the International Health Regulations (2005) submitted in accordance with decision WHA75(9)’, (2022), <https://apps.who.int/gb/wgihr/index.html> [accessed 25 June 2023]
- David Bell, ‘The World Health Organization and COVID-19: Re-establishing Colonialism in Public Health’ Panda, (5 July 2021) <https://pandata.org/who-and-covid-19-re-establishing-colonialism-in-public-health/> [accessed 29 June 2023]
- David Bell, ‘International Health Regulations and Pandemic Treaties – What is the Deal?’ Panda, (19 May 2022), <https://pandata.org/international-health-regulations-and-pandemic-treaties-what-is-the-deal/> [accessed 28 June 2023]
- David Bell, ‘The Myths of Pandemic Preparedness’, Panda, (29 November 2022), <https://pandata.org/the-myths-of-pandemic-preparedness/> [accessed 28 June 2023]
- Richard Thaler and Cass R. Sunstein, Nudge: Improving Decisions about Health, Wealth and Happiness (New Haven: Yale University Press, 2008)
- Psychology Today, ‘Priming’, <https://www.psychologytoday.com/us/basics/priming> [accessed 29 June 2023]
- Pierpaolo Goffredo, Shohreh Haddadan, Vorakit Vorakitphan, Elena Cabrio and Serena Villata, ‘Fallacious Argument Classification in Political Debates’, Proceedings of the Thirty-First International Joint Conference on Artificial Intelligence (IJCAI-22), (2022) 4143-4149 <https://www.ijcai.org/proceedings/2022/0575.pdf>
- Stephanie Sarkis, ‘This is Not Equal to That: How False Equivalence Clouds our Judgment’, Forbes, (19 May 2019) <https://www.forbes.com/sites/stephaniesarkis/2019/05/19/this-is-not-equal-to-that-how-false-equivalence-clouds-our-judgment/?sh=569a0b335c0f> [accessed 29 June 2023]
- World Health Organization, ‘Assessed Contributions’ <https://www.who.int/about/funding/assessed-contributions> [accessed 15 June 2023]
- World Health Organization, ‘Contributors’ <https://open.who.int/2020-21/contributors/contributor> [accessed 15 June 2023]
- World Health Organization, ‘Contributor: Bill & Melinda Gates Foundation’ <https://open.who.int/2020-21/contributors/contributor?name=Bill%20%26%20Melinda%20Gates%20Foundation> [accessed 15 June 2023]
- Reuters, ‘All the Countries That Restricted or Suspended Use of AstraZeneca and J&J Covid-19 Vaccines’, IOL, (24 April 2021), <https://www.iol.co.za/news/world/all-the-countries-that-restricted-or-suspended-use-of-astrazeneca-and-j-and-j-covid-19-vaccines-15e22cb0-3fef-4dab-9176-ebb7862fa6bb> [accessed 25 June 2023]
- Joseph Fraiman, Juan Erviti, Mark Jones, Sander Greenland, Patrick Whelan, Robert M Kaplan and Peter Doshi, ‘Serious Adverse Events of Special Interest Following mRNA COVID-19 Vaccination in Randomized Trials in Adults’, Vaccine 40 (2022), 5798-5805 <https://doi.org/10.1016/j.vaccine.2022.08.036>
- Peter Gøtzsche and Maryanne Demasi, ‘Serious Harms of the COVID-19 Vaccines: A Systematic Review’, Preprint with medRxiv, (2023) <https://doi.org/10.1101/2022.12.06.22283145>
- United States District Court for the Northern District of Texas Fort Worth Division, ‘Case 4:21-cv-01058-P Document 35’, (Filed 6 January 2022), <https://www.scribd.com/document/551589334/FDA-Foia-Request-010722#> [accessed 26 June 2023]
- Worldwide Safety Pfizer, ‘5.3.6 Cumulative Analysis of Post-Authorization Adverse Event Reports of PF-07302048 (BNT162B2)’, (Received 28 February 2021, Approved 30 April 2021), <https://phmpt.org/wp-content/uploads/2021/11/5.3.6-postmarketing-experience.pdf> (Appendix 1) [accessed 26 June 2023]
- Peter Marks (Director, Center for Biologics Evaluation and Research, FDA), Letter sent to Linda Wastila, Coalition Advocating for Adequately Labeled Medicines (CAALM), Re: Citizen Petition, Docket Number: FDA-2023-P-0360, (18 April 2023), <https://www.documentcloud.org/documents/23786932-fda-letter-on-covid-19-vaccine-labeling> [accessed 18 June 2023]
- Yaakov Ophir, Yaffa Shir-Raz, Shay Zakov and Peter A. McCullough, ‘The Efficacy of COVID-19 Vaccine Boosters against Severe Illness and Deaths: Scientific Fact or Wishful Myth?’ Journal of American Physicians and Surgeons, 28(1) (2023), 20-27 <https://jpands.org/vol28no1/ophir.pdf> [accessed 25 June 2023]
- Thomas Fazi and Toby Green, ‘Why Are Excess Deaths Still So High? We Can’t Just Blame a Failing NHS’, Unherd, (30 January 2023) <https://unherd.com/2023/01/why-are-excess-deaths-still-so-high/> [accessed 25 June 2023]
- Martin Neil and Norman Fenton, ‘The Devil’s Advocate: An Exploratory Analysis of 2022 Excess Mortality’, Where are the Numbers? (14 December 2022), <https://wherearethenumbers.substack.com/p/the-devils-advocate-an-exploratory> [accessed 27 June 2023]
- Bill Gates, Bill and Melinda Gates on Preparing for the Next Pandemic, online video recording, YouTube, 10 January 2013, <https://youtu.be/Wn0xzZH1dJA> [accessed 18 June 2023].
- David Bell, ‘The Myths of Pandemic Preparedness’, Panda, (29 November 2022) <https://pandata.org/the-myths-of-pandemic-preparedness/> [accessed 27 June 2023]
- Andrew Mullen, ‘The Propaganda Model after 20 Years: Interview with Edward S. Herman and Noam Chomsky’, Westminster Papers in Communication and Culture, 6(2) (2017), 12-22 <https://doi.org/10.16997/wpcc.121>
- Klaus Schwab, ‘Now is the Time For a “Great Reset”’, World Economic Forum, (3 June 2022) <https://www.weforum.org/agenda/2020/06/now-is-the-time-for-a-great-reset/> [accessed 26 June 2023]
- Simon Torkington, ‘We’re On the Brink of a “Polycrisis” – How Worried Should We Be?’ World Economic Forum, (23 June 2020) <https://www.weforum.org/agenda/2023/01/polycrisis-global-risks-report-cost-of-living/> [accessed 26 June 2023]
- World Health Organization, ‘One Health’, (21 September 2017) <https://www.who.int/news-room/questions-and-answers/item/one-health> [accessed 15 June 2023]
- John T. Cacioppo and Richard E. Petty, ‘Effects of Message Repetition and Negativity on Credibility Judgments and Political Attitudes’, Basic and Applied Social Psychology, 10(1) (1989), 3-12 <https://richardepetty.com/wp-content/uploads/2019/01/1989-basp-cacioppopetty.pdf>
- Christopher J. Anderson and Sara B. Hobolt, ‘Creating Compliance in Crisis: Messages, Messengers, and Masking up in Britain’, West European Politics, 46(2) (2023) 300-323 <https://doi.org/10.1080/01402382.2022.2091863> [accessed 29 June 2023]
- Edouard Mathieu, Hannah Ritchie, Lucas Rodés-Guirao, Cameron Appel, Charlie Giattino, Joe Hasell, Bobbie Macdonald, Saloni Dattani, Diana Beltekian, Esteban Ortiz-Ospina and Max Roser ‘Coronavirus Pandemic (COVID-19)’. Published online at OurWorldInData.org, (2020) <https://ourworldindata.org/covid-deaths> [accessed 25 June 2023]
September 7, 2023
Posted by aletho |
Deception, Science and Pseudo-Science | Covid-19, UK, WHO |
Leave a comment
Everyone seems to know someone taking Ozempic these days. But, it’s not all roses for the wonder weight loss drug, with serious side effects including suicidal ideations and stomach paralysis. Jefferey Jaxen reports.
A Louisiana woman who sued the manufacturers of popular diabetes and weight loss drugs Ozempic and Mounjaro is alleging the drugmakers failed to warn the public about the risk of severe gastrointestinal problems.
Jaclyn Bjorklund, 44, who on Wednesday filed the 26-page lawsuit in U.S. District Court for the Western District of Louisiana Lake Charles Division, claims she was “severely injured” after taking the two medications.
According to the complaint, Novo Nordisk and Eli Lilly, the manufacturers of Ozempic and Mounjaro, respectively, “downplayed the severity of the gastrointestinal events,” such as gastroparesis and gastroenteritis, caused by the drugs.
Gastroparesis, a disorder that “slows or stops the movement of food from your stomach to your small intestine, even though there is no blockage in the stomach or intestines” is frequently caused by diabetes. Narcotics and antidepressants also are linked to gastroparesis.
Ozempic (semaglutide) and Mounjaro (tirzepatide) are injectable diabetes medications, approved by the U.S. Food and Drug Administration (FDA), CBS News reported. Mounjaro was approved in May 2022. Ozempic was first approved in December 2017, and approved at a higher dose in March 2022.
According to NBC News, Bjorklund is the first person to come forward alleging that the drugs in question cause gastrointestinal injuries.
The two drugs are part of a new category of medicines known as glucagon-like peptide-1, or GLP-1, receptor agonists. They are intended to help people with Type 2 diabetes manage their blood sugar levels. However, the medications are also commonly prescribed off-label for weight loss.
According to CBS News, “These drugs were originally developed to treat patients with Type 2 diabetes as they produce insulin and lower blood sugar. They also release a hormone that slows down digestion and keeps food in a patient’s stomach longer.”
However, their long-term impact is unknown.
According to CNN, “The lawsuit is seeking compensatory and punitive damages for past and future pain and suffering Bjorklund will have including health care costs and medical monitoring as well as her attorney’s fees and court costs.”
Attorneys Paul Pennock and Jonathan Sedgh, of Orlando-based Morgan & Morgan, said during a press conference, that the basis of the lawsuit is “a failure to warn,” CBS News reported. Pennock told the press:
“It is our opinion that these drugs are causing these problems. We think that the evidence is sufficient for us to be able to prove it or we would not have filed the case, and we intend to file many more in the coming days and weeks.
“[Bjorklund’s] problems have been so severe that she’s been to the emergency room multiple times, including last weekend. She’s actually even thrown up so violently that she’s lost teeth.”
This is the first lawsuit alleging the two drugs caused gastrointestinal injuries, however, lawyers representing Bjorklund said hundreds more similar lawsuits are ready to be filed by victims across the U.S.
Ozempic recently was linked to a range of other health issues, including kidney disorders and causing suicidal thoughts.
Plaintiff suffered from ‘severe gastrointestinal events’
The lawsuit states that Bjorklund, who was diagnosed with Type 2 diabetes in 2017, was prescribed Ozempic and took the drug for more than a year before switching to Mounjaro.
During this period, she experienced “severe gastrointestinal events,” including severe vomiting — which also led to the loss of teeth, gastrointestinal burning and stomach pain. As a result, the complaint states, Bjorklund “sustained severe and permanent personal injuries, pain, suffering, and emotional distress, and incurred medical expenses.”
The lawsuit also alleges the two companies “knew of the association between the use of GLP-1 receptor agonists and the risk of developing severe gastrointestinal issues, including gastroparesis and gastroenteritis.”
The companies’ “failure to disclose information that they possessed regarding the association between the use of GLP-1 receptor agonists and the risk of developing severe gastrointestinal issues, including gastroparesis and gastroenteritis, rendered the warnings for this medication inadequate,” the lawsuit adds.
According to The Hill, “While the labels for both medications note that they delay gastric emptying and can cause a variety of stomach problems — including nausea, vomiting, diarrhea, abdominal pain and constipation — they do not explicitly warn of gastroparesis as a risk.”
CNN reported that “Ozempic’s prescribing information says the most common adverse events related to the drug are nausea, vomiting, diarrhea, abdominal pain and constipation. Under a section on drug interactions, it says that Ozempic delays gastric emptying, which may impact absorption of oral medications.”
Similarly, “Mounjaro’s prescribing information also says nausea, diarrhea, decreased appetite, vomiting, constipation, dyspepsia, and abdominal pain are the most common adverse events, and that Mounjaro delays gastric emptying, which may impact medication absorption.”
However, due to the lack of an explicit warning regarding gastroparesis, the lawsuit alleges that Bjorklund “was and still is caused to suffer from severe gastrointestinal issues, as well as other severe and personal injuries which are permanent and lasting in nature, physical pain, and mental anguish.”
In statements, both companies defended their products. Novo Nordisk claimed that gastrointestinal events are “well-known side effects of the GLP-1 class,” according to CBS News. The company added:
“For semaglutide, the majority of GI side effects are mild to moderate in severity and of short duration. GLP-1’s are known to cause a delay in gastric emptying, as noted in the label of each of our GLP-1 RA medications. Symptoms of delayed gastric emptying, nausea and vomiting are listed as side effects.”
And, as reported by The Hill :
“Patient safety is of utmost importance to Novo Nordisk. … We are continuously monitoring the safety profile of our products and collaborate closely with authorities to ensure patient safety, including adequate information on gastrointestinal side effects in the label.”
Eli Lilly said patient safety is its “top priority,” according to CBS News, and the company is “actively engage[d] in monitoring, evaluating and reporting safety information for all our medicines.”
NBC News cited FDA spokesperson Chanapa Tantibanchachai, who said it’s “unclear” whether GLP-1 medications are connected to occurrences of gastroparesis.
A separate FDA statement cited by CNN states the agency has “received reports of gastroparesis with semaglutide and liraglutide, some of which documented the adverse event as not recovered after discontinuation of the respective product at the time of the report.”
‘This medicine made my life hell’
However, lawyers for Bjorklund say that many more patients are ready to come forward with lawsuits of their own.
According to CBS News, Pennock’s firm “is investigating 400 other inquiries from clients across 45 states,” while according to The Hill, Pennock ultimately expects to see “thousands of such cases.”
Several patients also spoke to media outlets regarding their injuries.
Brea Hand told CBS News, “The stomach pain was just unbearable and I couldn’t keep anything down. I would drink something and within minutes, like five, 10 minutes later, I would be throwing up.”
Hand visited the hospital six times while taking Ozempic and was admitted to an intensive care unit. She is not involved in the lawsuit.
A July 25, CNN featured the stories of other patients, including Louisiana resident Joanie Knight, 37, who said “I wish I never touched it. I wish I’d never heard of it in my life,” referring to Ozempic. “This medicine made my life hell. So much hell.”
And Emily Wright, a 38-year-old teacher from Toronto, began taking Ozempic in 2018. Today though, despite not having taken the medication “for a year,” she said, “I’m still not back to my normal.” She told CNN she is now vomiting so frequently that she was obliged to take a leave of absence from her job.
In recent months, several reports have indicated that Ozempic in particular is linked to a range of other health problems.
Last month, health regulators in Iceland, followed by the European Medicines Agency, began investigating reports that Ozempic and other popular weight-loss drugs are linked to the inducement of suicidal thoughts.
In June, a report by Dr. Joseph Mercola referenced studies based on data from Eudravigilance, Europe’s system for analyzing adverse reactions to medications. The data showed a link between Ozempic and a high prevalence of gastrointestinal disorders. This confirmed findings from a separate study conducted in 2018.
Ozempic also was linked to an increased risk of adverse kidney events, diabetic retinopathy, and metabolic, nutritional, eye, retinal, urinary and cardiac disorders.
And in April, the FDA warned that Ozempic should be discontinued at least two months prior to pregnancy because it takes that long for the body to eliminate the drug.
However, those warnings are buried, and long-term testing won’t be completed for years. The drug was not studied in pregnant women during clinical trials.
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
August 4, 2023
Posted by aletho |
Deception | FDA, United States |
Leave a comment
Over 400 doctors, scientists and professionals from more than 34 countries this morning declared an international medical crisis due to “diseases and death associated with the ‘COVID-19 vaccines’”.
Launched at a press conference on Saturday, September 10th, the declaration states: “We are currently witnessing an excess in mortality in those countries where the majority of the population has received the so-called ‘COVID-19 vaccines’. To date, this excess mortality has neither been sufficiently investigated nor studied by national and international health institutions.”
It continues:
The large number of sudden deaths in previously healthy young people who were inoculated with these ‘vaccines’ is particularly worrying, as is the high incidence of miscarriages and perinatal deaths which have not been investigated.
A large number of adverse side effects, including hospitalisations, permanent disabilities and deaths related to the so-called ‘COVID-19 vaccines’, have been reported officially.
The registered number has no precedent in world vaccination history.
The declaration, which originates among concerned medics and professionals in India, makes eight “urgent” demands, including an immediate stop to the vaccinations and investigation of all deaths in previously healthy people.
Read the full text below, and if you are a doctor, scientist or other professional, do consider signing.
DECLARATION OF INTERNATIONAL MEDICAL CRISIS DUE TO THE DISEASES AND DEATHS CO-RELATED TO THE ‘COVID-19 VACCINES’
We, the medical doctors and scientists from all over the world, declare that there is an international medical crisis due to the diseases and deaths co-related to the administration of products known as ‘COVID-19 vaccines’.
We are currently witnessing an excess in mortality in those countries where the majority of the population has received the so-called ‘COVID-19 vaccines’. To date, this excess mortality has neither been sufficiently investigated nor studied by national and international health institutions.
The large number of sudden deaths in previously healthy young people who were inoculated with these ‘vaccines’, is particularly worrying, as is the high incidence of miscarriages and perinatal deaths which have not been investigated.
A large number of adverse side effects, including hospitalisations, permanent disabilities and deaths related to the so-called ‘COVID-19 vaccines’, have been reported officially.
The registered number has no precedent in world vaccination history.
Examining the reports on CDC’s VAERS, the U.K.’s Yellow Card System, the Australian Adverse Event Monitoring System, Europe’s EudraVigilance System and the WHO’s VigiAccess Database, to date there have been more than 11 million reports of adverse effects and more than 70,000 deaths co-related to the inoculation of the products known as ‘Covid vaccines’.
We know that these numbers just about represent between 1% and 10% of all real events.
Therefore, we consider that we are facing a serious international medical crisis, which must be accepted and treated as critical by all states, health institutions and medical personnel worldwide.
Therefore, the following measures must be undertaken on an urgent basis:
- A worldwide ‘stop’ to the national inoculation campaigns with the products known as ‘COVID-19 vaccines’.
- Investigation of all sudden deaths of people who were healthy previous to the inoculation.
- Implementation of early detection programmes of cardiovascular events which could lead to sudden deaths with analysis such as D-dimer and Troponin, in all those that were inoculated with the products known as ‘COVID-19 vaccines’, as well as the early detection of serious tumours.
- Implementation of research and treatment programmes for victims of adverse effects after receiving the so-called ‘COVID-19 vaccine’.
- Undertaking analyses of the composition of vials of Pfizer, Moderna, Astra Zeneca, Janssen, Sinovac, Sputnik V and any other product known as ‘COVID-19 vaccines’,
by independent research groups with no affiliation to pharmaceutical companies, nor any conflict of interest.
- Studies to be conducted on the interactions between the different components of the so-called ‘COVID-19 vaccines’ and their molecular, cellular and biological effects.
- Implementation of psychological help and compensation programmes for any person that has developed a disease or disability as a consequence of the so-called ‘COVID-19 vaccines’.
- Implementation and promotion of psychological help and compensation programmes for the family members of any person who died as a result of having been inoculated with the product known as ‘COVID-19 vaccines’.
Consequently we declare that we find ourselves in an unprecedented international medical crisis in the history of medicine, due to the large number of diseases and deaths associated with the ‘vaccines against COVID-19’. Therefore, we demand that the regulatory agencies that oversee drug safety as well as the health institutions in all countries, together with the international institutions such as the WHO, PHO, EMA, FDA, UK-MHRA and NIH respond to this declaration and act in accordance with the eight measures demanded in this manifesto.
This Declaration is a joint initiative of several professionals who have been fighting for this cause. We call on all doctors, scientists and professionals to endorse this statement in order to put pressure on the entities involved and promote a more transparent health policy.
September 10, 2022
Posted by aletho |
Science and Pseudo-Science, War Crimes | COVID-19 Vaccine |
1 Comment
Medical ethics is about protecting society from medical malfeasance and the self-interest of the humans whom we trust to manage health. It is therefore disturbing when prominent people, in a prominent journal, tear up the concept of medical ethics and human rights norms. It is worse when they ignore broad swathes of evidence, and misrepresent their own sources to do so.
On July 8th 2022, The Lancet published a ‘Viewpoint’ article online: “Effectiveness of vaccination mandates in improving uptake of COVID-19 vaccines in the USA.” The article, which acknowledges the controversial nature of vaccine mandates, primarily concludes that coercing people to take a medical product, and reducing options for refusal, increases product uptake.
It further concludes that the best way to implement such mandates is for employers and educational institutions to threaten job security and the right to education.
The use of coercion goes against the established ethics and morals of Public Health, and could be argued to be anti-health. In this case, the article justifies it by stating that “the current evidence regarding the safety of COVID-19 vaccines in adults is sufficient to support mandates.” However, it offers scant evidence to back this assertion, and ignores all evidence to the contrary. They apparently consider the ability to work and support a family, or gain formal education, as something that is to be granted or taken away, not a human right.
The Lancet was once a credible journal with a rigorous policy of peer review. However, in this article it appears to have dropped its former standards, promoting medical fascism (coercion, threat and division to achieve compliance with authority) without insisting on a rigorous evidence base to justify such an approach. This suggests an attempt to normalize such approaches in mainstream public health.
Past experience has shown us where fascism behind a façade of public health can lead. The sterilization campaigns aimed at coloured and low-income populations of the US Eugenicist era, and the extensions of similar programs under Nazism in 1930s and 1940s Europe, relied heavily on the normalization of such approaches.
Leading public health voices from Johns Hopkins School of Public Health and other institutions championed a public health approach of sanitizing populations rather than environments, encouraging the idea of a tiered society where health ‘experts’ determine the rights and medical management of those deemed less worthy.
Avoiding the discomfort of evidence
The authors of this Lancet paper, ranging from academics and medical consultants to the daughter of a prominent politician, attempt to rewrite human rights in medicine as if precedent never existed. Their argument for coercion in mass vaccination recognizes that ‘vaccine mandates,’ whether issued by governments, employers or schools, all involve a loss of rights. No serious attempt is made to provide a medical justification for mass vaccination with a non-transmission-blocking vaccine.
The paper focuses on the premise that coercion, commonly considered a form of force, makes humans do things they would not otherwise do. Banning fellow humans from making their own health choices on pain of loss of normal participation in society has an impact on increasing vaccine uptake. This is hardly a revelation to any thinking human, but clearly important enough to justify publication in The Lancet.
The article links to evidence of vaccine mandates used for state school entry that show higher compliance when the right of religious and personal belief exemption is removed, or where onerous requirements for exemptions are put in place. Leaving ethical questions aside, the obvious lack of similarity between the authors’ predicate childhood vaccinations that block transmission and COVID-19 vaccines that have minimal impact on transmission, and may even promote it, is ignored. The one mandated adult vaccine predicate referenced in the article, the influenza vaccine, provides only a 2.5% reduction in pneumonia ‘when the (mandated) vaccine was well matched to circulating strains’ in the reference quoted.
When raising the sacking of non-vaccinated workers, the authors seem comfortable with the approach but coy in admitting its consequences. Their admission that “a few large US employers have terminated hundreds of workers for non-compliance references an article in Money magazine which actually paints a bleaker picture, characterizing it as a ‘great resignation.’
The authors will also have been aware of mass layoffs by large employers such as New York City (over 9,000 sacked or placed on leave), the US Department of Defense (DoD, which sacked 3,400), Kaiser Permanente (laid off 2,200), and the tens of thousands of staff lost from the UK care-home sector . Extrapolated across countries and society to actually provide credible data may have been too uncomfortable for the authors and Lancet editors.
High efficacy and safety are an obvious (though on their own, insufficient) prerequisite for any mandated product. This entire area of safety is dealt with by stating; “The current evidence on the safety of COVID-19 vaccines in adults is sufficient to support mandates,” supported by a single study comparing vaccinated individuals 1-3 weeks and 3-6 weeks post-vaccination, revealing low levels of myocardial infarction, appendicitis and stroke.
The claim that “widespread administration in adults has quickly generated a large evidence base supporting the vaccines’ safety, including evidence from active surveillance studies” suggests that both the authors and The Lancet are unaware of the VAERS and Eudravigilance databases set up for exactly this purpose. No mention is made of growing data on myocarditis, menstrual irregularities, or the excess all-cause mortality and severe outcomes in vaccinated groups in the Pfizer randomised control trials on which the FDA emergency registration was based. Were The Lancet’s reviewers unaware of these sources?
The sole reference to vaccine efficacy discusses COVID-19 ventilated patient outcomes, It ignores the period to 14 days post-previous dose that Pfizer acknowledges can be associated with immune suppression. Fenton et al. have noted that classing a vaccinated person as unvaccinated in the first 14 days post-injection has profound impacts on vaccine effectiveness data.
Ignoring the awkwardness of reality
Post-infection immunity in the unvaccinated is a threat to arguments for mandates. The authors disingenuously state that “evidence suggests that the immunity produced by natural infection varies by individual, and that people with previous infection benefit from vaccination. New variants further undercut the case for adequacy of previous infection.
Two references are used here: one from a study in Qatar and the other a study from Kentucky. The Qatar study finds that “the protection of previous infection against hospitalization or death caused by reinfection appeared to be robust, regardless of variant,” whilst the Kentucky study found Covid reinfection was reduced by vaccination over a 2-month period in the months soon after vaccination, prior to the waning and then reversal of this protection as demonstrated in studies of longer duration elsewhere.
The vast breadth of evidence on relative effectiveness of post-infection immunity is ignored. Either the authors failed to read their references and are unaware of waning and of the vast literature on post-infection immunity, or they do not consider demonstration of efficacy important for coerced medical treatments.
In a previous era, or in a previously credible medical journal, an argument for coercion to support a medical procedure would have required very high standards of evidence of efficacy and safety. It is arguing for the abrogation of fundamental principles such as informed consent that are at the core of modern medical ethics. Failure to address well-known contrary data should prevent an article from even reaching the peer-review stage.
Degrading public health degrades society
We are left with a paper stating that coercion is a good path to increase compliance for a product that does not reduce community infection risk, and has potentially serious side effects. Ignoring both of these aspects of COVID-19 vaccines is a poor approach to justifying mass vaccination. The sole nod to any human rights concern – “Some objectors argue mandates represent undue encroachment on individual liberty” – is an interesting way to characterize removal of the right to income, education and the ability to socialize with others.
Although all these rights are recognized under the Universal Declaration for Human Rights, the authors and The Lancet consider them insufficiently serious to dwell upon.
Public health has been down this road before. We have seen the path society takes when basic public health principles are subverted to achieve an aim that some perceive as ‘good.’ We have also seen how most health professionals will comply, however horrific the actions involved. There is no reason to believe that this round of medical fascism will end differently.
We rely on medical journals such as The Lancet to apply at least the same standards to the purveyors of such doctrines as they do to others and demand a rational and honest evidence base. Anything less would raise legitimate questions as to the role the journal is taking in promoting these doctrines, and their place in a free, evidence-based and rights-respecting society.
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. He is the former Program Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland.
Domini Gordon is Open Science and Open Society Coordinator at Panda.
September 10, 2022
Posted by aletho |
Deception, Science and Pseudo-Science | COVID-19 Vaccine, Human rights, The Lancet |
Leave a comment
In a stunning development, the Centers for Disease Control and Prevention (CDC) last week admitted — despite assurances to the contrary — the agency never analyzed the Vaccine Adverse Event Reporting System (VAERS) for safety signals for COVID-19 vaccines.
The admission was revealed in response to a Freedom of Information Act (FOIA) request submitted by Children’s Health Defense (CHD).
In September 2021, I published an article in The Defender in which I used the CDC’s published methodology to analyze VAERS for safety signals from COVID-19 vaccines.
The signals were loud and clear, leading me to wonder “why is nobody listening?”
Instead, I should have asked, “Is anybody even looking for them?”
After that article was published, I urged CHD’s legal team to submit a FOIA request to the CDC about its VAERS monitoring activities.
Since CDC officials stated publicly that “COVID-19 vaccine safety monitoring is the most robust in U.S. history,” I had assumed that at the very least, CDC officials were monitoring VAERS using the methods they described in a briefing document posted on the CDC website in January 2021 (and updated in February 2022, with minor changes).
I was wrong.
The lynchpin of their safety monitoring was to mine VAERS data for safety signals by calculating what are known as proportional reporting ratios (PRR’s).
This is a method of comparing the proportion of different types of adverse events reported for a new vaccine to the proportion of those events reported for an older, established vaccine.
If the new vaccine shows a significantly higher reporting rate of a particular adverse event relative to the old one, it counts as a safety signal that should then trigger a more thorough investigation.
The briefing document states, “CDC will perform PRR data mining on a weekly basis or as needed.”

And yet, in the agency’s response to the FOIA request, it wrote that “no PRRs were conducted by CDC. Furthermore, data mining is outside of the agency’s purview.”
The agency suggested contacting the U.S. Food and Drug Administration (FDA), which was supposed to perform a different type of data mining, according to the briefing document.

CDC officials repeatedly claimed they have not seen safety signals in VAERS.

For example, on April 27, 2021, CDC Director Dr. Rochelle Walensky stated the CDC did not see any signals related to heart inflammation.
But a PRR calculation I did using the number of myo/pericarditis reports listed in the first table produced by the CDC obtained via the FOIA request reveals clear and unambiguous safety signals relative to the comparator vaccines mentioned in the briefing document (i.e., flu vaccines, FLUAD and Shingrix).
The table is dated April 2, 2021, almost four weeks before she made those remarks.
In fact, among the 15 adverse events for adults included in that week’s tabulations, PRRs I calculated also show loud-and-clear safety signals for acute myocardial infarction, anaphylaxis, appendicitis, Bell’s palsy, coagulopathy, multisystem inflammatory syndrome in adults (MIS-A), stroke and death.
The actual monitoring the CDC did diverges from the one promised in the briefing document in other ways.
For example, the CDC never created tables of the top 25 adverse events reported in the previous week, tables comparing different vaccine manufacturers, or tables of auto-immune diseases.
And it only began monitoring in early April 2021, even though reports from COVID-19 vaccines had been flooding VAERS since mid-December of the previous year.
To be clear, VAERS is not the only database the CDC uses to monitor COVID-19 vaccine safety.
For example, the CDC sponsored several studies of COVID-19 safety using the Vaccine Safety Datalink (VSD), which is comprised of millions of medical records from HMO’s across several states.
Those studies do not raise many safety concerns. However, they make many questionable methodological choices.
To give one example, a major safety study based on VSD data published in September 2021, in “JAMA,” compares adverse event rates that occur within 1-21 days of vaccination to the rate of occurrence from 22 to 42 days after vaccination.
It makes no comparison between vaccinated and unvaccinated individuals, or before vaccination versus after in the same individuals.
Moreover, the VSD is far from infallible, having failed initially to detect the increase in myocarditis rates.
In contrast, although calculating PRR’s is a blunt pharmacovigilance tool and far from perfect, it nevertheless has the advantage of being straightforward and difficult to manipulate with statistical sleight of hand.
PRRs are one of the oldest, most basic and most well-established tools of pharmacovigilance. The calculations are so straightforward that the CDC automated it several years ago, so it could have been done at the press of a button.
It simply beggars belief that the CDC failed to do this simple calculation. Even now, a paper published by CDC staff in March on the safety of the mRNA COVID-19 vaccines remains purely descriptive with no PRR calculation.
Meanwhile, a study published by a researcher not affiliated with the CDC in February in “Frontiers in Public Health” analyzes VAERS and EudraVigilance data using a method similar to PRRs, revealing clear and concerning safety signals.
And while it is true that VAERS is not the only database the CDC can use to monitor COVID-19 vaccine safety, it is of critical importance because it can reveal signals much faster than any other method — if anybody cares to look for them.
It remains to be seen if the FDA was properly monitoring VAERS. That will be the subject of a future FOIA request.
But even if it was, it doesn’t change the fact that the CDC completely failed in its promise to monitor VAERS for safety signals.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
June 22, 2022
Posted by aletho |
Deception, Science and Pseudo-Science, War Crimes | CDC, COVID-19 Vaccine, United States |
1 Comment
Adverse Reactions for Novel Covid-19 Vaccines More Numerous Than for Similar Products by Factor of Between 10 and 169
BATH, UK — A new report prepared by the World Council for Health (WCH) has confirmed that data on adverse drug reactions from the experimental Covid-19 vaccines exist in an amount sufficient for the recall of similar products in the past.
The report was prepared to determine whether sufficient pharmacovigilance data exist on official and public databases (WHO VigiAccess, CDC VAERS, EudraVigilance, and UK Yellow Card Scheme) to establish a safety signal on the novel Covid-19 injections.
On all databases, it was found that adverse drug reaction (ADR) reports linked to Covid-19 injections are more numerous than other similar products by a factor of between 10 and 169 (see graph below). Many of the ADR reports are serious in nature and there exists sufficient evidence of associated harm on these databases to indicate a product recall.

Total Adverse Events per Pharamacovigilance Database
In total, more than 40,000 deaths are linked to the novel Covid-19 vaccines in the official databases analysed.
In addition, the WCH pharmacovigilance report found that several thousand adverse drug reactions on official databases are related to the use of the experimental Covid-19 vaccines among young boys and girls for whom the vaccine had not been approved at the time.
The purpose of pharmacovigilance databases is to provide a signal of safety, and not to prove causality. To ensure that harms are detected in time, suspicion that an event is linked to the administration of the medicine is enough to register an event. “There is no need to prove that the medicine caused the adverse reaction, just the suspicion is good enough,” Dr. June Raine, head of the UK’s Medicines and Healthcare products Regulatory Agency, said in 2006. When sufficient pharmacovigilance data show a signal of harm, administration of the product should be ceased, the product recalled, and the safety signal investigated.
It should also be noted that such systems of passive surveillance result in significantly fewer ADR reports than active surveillance reporting. As a result, the actual number of adverse events that occurred in temporal relation to Covid-19 injections is likely to be much higher than revealed by the available official data.
In December 2021, World Council for Health called on regulators and governments around the world to immediately cease use of all experimental Covid-19 injections.
Dr. Tess Lawrie, co-founder of the World Council for Health, calls for people to come together to raise awareness of vaccine injury so that those harmed can get the help they deserve. “It is concerning that a grassroots organisation has had to do this work and point out that none of these experimental vaccines are safe according to publicly available official data. Why have the regulators not done their job and protected us?“
***
World Council for Health Covid-19 Vaccine Pharmacovigilance Report: https://worldcouncilforhealth.org/resources/covid-19-vaccine-pharmacovigilance-report/
World Council for Health Calls for an Immediate Stop to the Covid-19 Experimental “Vaccines”: https://worldcouncilforhealth.org/campaign/covid-19-vaccine-cease-and-desist/
World Council for Health Statement on Covid-19 Vaccines: https://worldcouncilforhealth.org/news/2021/12/covid-19-vaccines/14001/
World Council for Health Statement on Risk of Myocarditis in Children: https://worldcouncilforhealth.org/news/2022/01/risk-of-myocarditis-in-children/18570/
Contact: Dr. Katarina Lindley at katarina@thewc4h.org
June 12, 2022
Posted by aletho |
Science and Pseudo-Science | COVID-19 Vaccine, European Union, UK, United States |
Leave a comment

The European (EEA and non-EEA countries) database of suspected drug reaction reports is EudraVigilance, verified by the European Medicines Agency (EMA), and they are now reporting 39,997 fatalities, and 3,666,011 injuries following injections of four experimental COVID-19 shots:
From the total of injuries recorded, almost half of them (1,727,226) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through February 12, 2022.
Total reactions for the mRNA vaccine Tozinameran (code BNT162b2,Comirnaty) from BioNTech/ Pfizer: 18,185 deaths and 1,791,261 injuries to 12/02/2022
- 50,761 Blood and lymphatic system disorders incl. 254 deaths
- 61,233 Cardiac disorders incl. 2,638 deaths
- 547 Congenital, familial and genetic disorders incl. 55 deaths
- 23,657 Ear and labyrinth disorders incl. 12 deaths
- 2,077 Endocrine disorders incl. 8 deaths
- 27,111 Eye disorders incl. 39 deaths
- 138,253 Gastrointestinal disorders incl. 706 deaths
- 443,764 General disorders and administration site conditions incl. 5,190 deaths
- 2,025 Hepatobiliary disorders incl. 95 deaths
- 19,243 Immune system disorders incl. 99 deaths
- 84,884 Infections and infestations incl. 1,931 deaths
- 35,665 Injury, poisoning and procedural complications incl. 349 deaths
- 44,308 Investigations incl. 520 deaths
- 11,795 Metabolism and nutrition disorders incl. 289 deaths
- 209,669 Musculoskeletal and connective tissue disorders incl. 228 deaths
- 1,744 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 166 deaths
- 290,349 Nervous system disorders incl. 1,926 deaths
- 2,658 Pregnancy, puerperium and perinatal conditions incl. 75 deaths
- 262 Product issues incl. 3 deaths
- 32,195 Psychiatric disorders incl. 216 deaths
- 6,509 Renal and urinary disorders incl. 272 deaths
- 74,588 Reproductive system and breast disorders incl. 6 deaths
- 75,926 Respiratory, thoracic and mediastinal disorders incl. 1,932 deaths
- 81,815 Skin and subcutaneous tissue disorders incl. 146 deaths
- 4,127 Social circumstances incl. 23 deaths
- 21,849 Surgical and medical procedures incl. 208 deaths
- 44,247 Vascular disorders incl. 799 deaths
Total reactions for the mRNA vaccine mRNA-1273 (CX-024414) from Moderna: 11,138 deaths and 573,035 injuries to 12/02/2022
- 13,383 Blood and lymphatic system disorders incl. 120 deaths
- 19,462 Cardiac disorders incl. 1,169 deaths
- 198 Congenital, familial and genetic disorders incl. 12 deaths
- 6,688 Ear and labyrinth disorders incl. 8 deaths
- 533 Endocrine disorders incl. 6 deaths
- 7,856 Eye disorders incl. 35 deaths
- 46,468 Gastrointestinal disorders incl. 416 deaths
- 152,534 General disorders and administration site conditions incl. 3,672 deaths
- 819 Hepatobiliary disorders incl. 55 deaths
- 5,683 Immune system disorders incl. 21 deaths
- 24,462 Infections and infestations incl. 1,051 deaths
- 10,555 Injury, poisoning and procedural complications incl. 211 deaths
- 12,633 Investigations incl. 395 deaths
- 4,996 Metabolism and nutrition disorders incl. 268 deaths
- 70,107 Musculoskeletal and connective tissue disorders incl. 221 deaths
- 700 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 86 deaths
- 95,946 Nervous system disorders incl. 1,040 deaths
- 925 Pregnancy, puerperium and perinatal conditions incl. 10 deaths
- 101 Product issues incl. 4 deaths
- 9,813 Psychiatric disorders incl. 181 deaths
- 3,157 Renal and urinary disorders incl. 218 deaths
- 14,047 Reproductive system and breast disorders incl. 9 deaths
- 24,308 Respiratory, thoracic and mediastinal disorders incl. 1,178 deaths
- 29,172 Skin and subcutaneous tissue disorders incl. 96 deaths
- 2,325 Social circumstances incl. 45 deaths
- 3,585 Surgical and medical procedures incl. 206 deaths
- 12,579 Vascular disorders incl. 405 deaths
Total reactions for the vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/ AstraZeneca: 8,174 deaths and 1,170,321 injuries to 12/02/2022
- 14,038 Blood and lymphatic system disorders incl. 279 deaths
- 21,330 Cardiac disorders incl. 854 deaths
- 241 Congenital familial and genetic disorders incl. 9 deaths
- 13,580 Ear and labyrinth disorders incl. 7 deaths
- 709 Endocrine disorders incl. 6 deaths
- 20,310 Eye disorders incl. 32 deaths
- 108,425 Gastrointestinal disorders incl. 447 deaths
- 309,230 General disorders and administration site conditions incl. 1,893 deaths
- 1,062 Hepatobiliary disorders incl. 70 deaths
- 5,495 Immune system disorders incl. 40 deaths
- 43,810 Infections and infestations incl. 634 deaths
- 13,918 Injury poisoning and procedural complications incl. 201 deaths
- 26,112 Investigations incl. 206 deaths
- 13,147 Metabolism and nutrition disorders incl. 132 deaths
- 170,055 Musculoskeletal and connective tissue disorders incl. 171 deaths
- 769 Neoplasms benign malignant and unspecified (incl cysts and polyps) incl. 42 deaths
- 236,745 Nervous system disorders incl. 1,199 deaths
- 631 Pregnancy puerperium and perinatal conditions incl. 21 deaths
- 199 Product issues incl. 1 death
- 21,273 Psychiatric disorders incl. 73 deaths
- 4,416 Renal and urinary disorders incl. 82 deaths
- 17,181 Reproductive system and breast disorders incl. 3 deaths
- 42,021 Respiratory thoracic and mediastinal disorders incl. 1,119 deaths
- 52,622 Skin and subcutaneous tissue disorders incl. 69 deaths
- 1,657 Social circumstances incl. 9 deaths
- 2,217 Surgical and medical procedures incl. 33 deaths
- 29,128 Vascular disorders incl. 542 deaths
Total reactions for the COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson: 2,500 deaths and 131,394 injuries to 12/02/2022
- 1,272 Blood and lymphatic system disorders incl. 54 deaths
- 2,671 Cardiac disorders incl. 211 deaths
- 44 Congenital, familial and genetic disorders incl. 1 death
- 1,382 Ear and labyrinth disorders incl. 3 deaths
- 109 Endocrine disorders incl. 2 deaths
- 1,710 Eye disorders incl. 10 deaths
- 9,791 Gastrointestinal disorders incl. 94 deaths
- 35,428 General disorders and administration site conditions incl. 708 deaths
- 160 Hepatobiliary disorders incl. 15 deaths
- 572 Immune system disorders incl. 10 deaths
- 8,881 Infections and infestations incl. 211 deaths
- 1,230 Injury, poisoning and procedural complications incl. 26 deaths
- 6,393 Investigations incl. 134 deaths
- 793 Metabolism and nutrition disorders incl. 63 deaths
- 17,493 Musculoskeletal and connective tissue disorders incl. 57 deaths
- 95 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 9 deaths
- 23,989 Nervous system disorders incl. 248 deaths
- 61 Pregnancy, puerperium and perinatal conditions incl. 1 death
- 31 Product issues
- 1,844 Psychiatric disorders incl. 24 deaths
- 560 Renal and urinary disorders incl. 32 deaths
- 3,189 Reproductive system and breast disorders incl. 7 deaths
- 4,649 Respiratory, thoracic and mediastinal disorders incl. 314 deaths
- 3,894 Skin and subcutaneous tissue disorders incl. 12 deaths
- 429 Social circumstances incl. 4 deaths
- 932 Surgical and medical procedures incl. 75 deaths
- 3,792 Vascular disorders incl. 175 deaths

*These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
February 18, 2022
Posted by aletho |
War Crimes | COVID-19 Vaccine, European Union |
Leave a comment

The European (EEA and non-EEA countries) database of suspected drug reaction reports is EudraVigilance, verified by the European Medicines Agency (EMA), and they are now reporting 38,983 fatalities, and 3,530,362 injuries following injections of four experimental COVID-19 shots:
From the total of injuries recorded, almost half of them (1,672,872 ) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through January 29, 2022.
Total reactions for the mRNA vaccine Tozinameran (code BNT162b2,Comirnaty) from BioNTech/ Pfizer: 17,578 deaths and 1,704,757 injuries to 29/01/2022
- 48,240 Blood and lymphatic system disorders incl. 242 deaths
- 57,541 Cardiac disorders incl. 2,554 deaths
- 522 Congenital, familial and genetic disorders incl. 51 deaths
- 22,590 Ear and labyrinth disorders incl. 11 deaths
- 1,911 Endocrine disorders incl. 6 deaths
- 25,814 Eye disorders incl. 38 deaths
- 133,365 Gastrointestinal disorders incl. 681 deaths
- 422,360 General disorders and administration site conditions incl. 5,024 deaths
- 1,931 Hepatobiliary disorders incl. 90 deaths
- 18,455 Immune system disorders incl. 95 deaths
- 76,443 Infections and infestations incl. 1,878 deaths
- 33,972 Injury, poisoning and procedural complications incl. 331 deaths
- 42,585 Investigations incl. 502 deaths
- 11,344 Metabolism and nutrition disorders incl. 273 deaths
- 201,643 Musculoskeletal and connective tissue disorders incl. 212 deaths
- 1,629 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 153 deaths
- 278,744 Nervous system disorders incl. 1,859 deaths
- 2,513 Pregnancy, puerperium and perinatal conditions incl. 74 deaths
- 251 Product issues incl. 3 deaths
- 30,622 Psychiatric disorders incl. 207 deaths
- 6,150 Renal and urinary disorders incl. 266 deaths
- 68,129 Reproductive system and breast disorders incl. 6 deaths
- 72,531 Respiratory, thoracic and mediastinal disorders incl. 1,884 deaths
- 78,059 Skin and subcutaneous tissue disorders incl. 146 deaths
- 3,871 Social circumstances incl. 22 deaths
- 21,010 Surgical and medical procedures incl. 204 deaths
- 42,532 Vascular disorders incl. 766 deaths
Total reactions for the mRNA vaccine mRNA-1273 (CX-024414) from Moderna: 11,008 deaths and 543,543 injuries to 29/01/2022
- 12,365 Blood and lymphatic system disorders incl. 120 deaths
- 18,287 Cardiac disorders incl. 1,142 deaths
- 190 Congenital, familial and genetic disorders incl. 11 deaths
- 6,310 Ear and labyrinth disorders incl. 8 deaths
- 502 Endocrine disorders incl. 6 deaths
- 7,475 Eye disorders incl. 36 deaths
- 44,340 Gastrointestinal disorders incl. 413 deaths
- 145,153 General disorders and administration site conditions incl. 3,630 deaths
- 793 Hepatobiliary disorders incl. 54 deaths
- 5,370 Immune system disorders incl. 22 deaths
- 23,070 Infections and infestations incl. 1042 deaths
- 10,286 Injury, poisoning and procedural complications incl. 208 deaths
- 12,129 Investigations incl. 393 deaths
- 4,847 Metabolism and nutrition disorders incl. 263 deaths
- 66,358 Musculoskeletal and connective tissue disorders incl. 223 deaths
- 682 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 85 deaths
- 91,230 Nervous system disorders incl. 1,029 deaths
- 907 Pregnancy, puerperium and perinatal conditions incl. 10 deaths
- 98 Product issues incl. 4 deaths
- 9,441 Psychiatric disorders incl. 181 deaths
- 3,030 Renal and urinary disorders incl. 214 deaths
- 12,547 Reproductive system and breast disorders incl. 9 deaths
- 23,251 Respiratory, thoracic and mediastinal disorders incl. 1,162 deaths
- 27,540 Skin and subcutaneous tissue disorders incl. 96 deaths
- 2,239 Social circumstances incl. 45 deaths
- 3,028 Surgical and medical procedures incl. 203 deaths
- 12,075 Vascular disorders incl. 399 deaths
Total reactions for the vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/ AstraZeneca: 7,977 deaths and 1,154,757 injuries to 29/01/2022
- 13,912 Blood and lymphatic system disorders incl. 278 deaths
- 20,984 Cardiac disorders incl. 830 deaths
- 235 Congenital familial and genetic disorders incl. 8 deaths
- 13,406 Ear and labyrinth disorders incl. 7 deaths
- 692 Endocrine disorders incl. 6 deaths
- 20,086 Eye disorders incl. 32 deaths
- 107,453 Gastrointestinal disorders incl. 434 deaths
- 304,993 General disorders and administration site conditions incl. 1,855 deaths
- 1,039 Hepatobiliary disorders incl. 69 deaths
- 5,409 Immune system disorders incl. 40 deaths
- 42,266 Infections and infestations incl. 620 deaths
- 13,630 Injury poisoning and procedural complications incl. 198 deaths
- 25,681 Investigations incl. 205 deaths
- 13,023 Metabolism and nutrition disorders incl. 126 deaths
- 168,174 Musculoskeletal and connective tissue disorders incl. 165 deaths
- 743 Neoplasms benign malignant and unspecified (incl cysts and polyps) incl. 40 deaths
- 234,117 Nervous system disorders incl. 1,178 deaths
- 635 Pregnancy puerperium and perinatal conditions incl. 20 deaths
- 199 Product issues incl. 1 death
- 21,051 Psychiatric disorders incl. 69 deaths
- 4,338 Renal and urinary disorders incl. 78 deaths
- 16,849 Reproductive system and breast disorders incl. 3 deaths
- 41,401 Respiratory thoracic and mediastinal disorders incl. 1,082 deaths
- 52,064 Skin and subcutaneous tissue disorders incl. 65 deaths
- 1,617 Social circumstances incl. 9 deaths
- 1,973 Surgical and medical procedures incl. 30 deaths
- 28,787 Vascular disorders incl. 529 deaths
Total reactions for the COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson: 2,420 deaths and 127,305 injuries to 29/01/2022
- 1,229 Blood and lymphatic system disorders incl. 51 deaths
- 2,552 Cardiac disorders incl. 204 deaths
- 40 Congenital, familial and genetic disorders incl. 1 death
- 1,319 Ear and labyrinth disorders incl. 3 deaths
- 105 Endocrine disorders incl. 1 death
- 1,656 Eye disorders incl. 10 deaths
- 9,588 Gastrointestinal disorders incl. 88 deaths
- 34,487 General disorders and administration site conditions incl. 685 deaths
- 153 Hepatobiliary disorders incl. 13 deaths
- 544 Immune system disorders incl. 10 deaths
- 8,521 Infections and infestations incl. 207 deaths
- 1,147 Injury, poisoning and procedural complications incl. 25 deaths
- 6,086 Investigations incl. 131 deaths
- 756 Metabolism and nutrition disorders incl. 60 deaths
- 17,116 Musculoskeletal and connective tissue disorders incl. 55 deaths
- 86 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 8 deaths
- 23,413 Nervous system disorders incl. 245 deaths
- 55 Pregnancy, puerperium and perinatal conditions incl. 1 death
- 30 Product issues
- 1,766 Psychiatric disorders incl. 22 deaths
- 535 Renal and urinary disorders incl. 31 deaths
- 2,941 Reproductive system and breast disorders incl. 6 deaths
- 4,468 Respiratory, thoracic and mediastinal disorders incl. 304 deaths
- 3,760 Skin and subcutaneous tissue disorders incl. 10 deaths
- 409 Social circumstances incl. 4 deaths
- 867 Surgical and medical procedures incl. 74 deaths
- 3,676 Vascular disorders incl. 171 deaths

*These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
On January 29, 2021 a mass funeral protest for children who have died after receiving a Pfizer vaccine was held in Geneva, Switzerland.
Someone recorded the event and made a short video. This is on our Bitchute Channel, and also on our Telegram channel.
February 4, 2022
Posted by aletho |
Civil Liberties, Video, War Crimes | COVID-19 Vaccine, European Union, Human rights |
1 Comment

The European (EEA and non-EEA countries) database of suspected drug reaction reports is EudraVigilance, verified by the European Medicines Agency (EMA), and they are now reporting 37,927 fatalities, and 3,392,632 injuries following injections of four experimental COVID-19 shots:
From the total of injuries recorded, almost half of them (1,611,423) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through January 15, 2022.
Total reactions for the mRNA vaccineTozinameran (code BNT162b2,Comirnaty) from BioNTech/ Pfizer: 17,054 deaths and 1,624,526 injuries to 15/01/2022
- 45,865 Blood and lymphatic system disorders incl. 238 deaths
- 53,606 Cardiac disorders incl. 2,459 deaths
- 500 Congenital, familial and genetic disorders incl. 52 deaths
- 21,641 Ear and labyrinth disorders incl. 11 deaths
- 1,727 Endocrine disorders incl. 5 deaths
- 24,752 Eye disorders incl. 38 deaths
- 128,813 Gastrointestinal disorders incl. 673 deaths
- 403,800 General disorders and administration site conditions incl. 4,871 deaths
- 1,855 Hepatobiliary disorders incl. 85 deaths
- 17,690 Immune system disorders incl. 88 deaths
- 71,334 Infections and infestations incl. 1,829 deaths
- 31,663 Injury, poisoning and procedural complications incl. 321 deaths
- 40,469 Investigations incl. 492 deaths
- 10,933 Metabolism and nutrition disorders incl. 271 deaths
- 193,866 Musculoskeletal and connective tissue disorders incl. 209 deaths
- 1,534 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 144 deaths
- 266,754 Nervous system disorders incl. 1,807 deaths
- 2,384 Pregnancy, puerperium and perinatal conditions incl. 72 deaths
- 241 Product issues incl. 3 deaths
- 29,339 Psychiatric disorders incl. 198 deaths
- 5,857 Renal and urinary disorders incl. 261 deaths
- 63,007 Reproductive system and breast disorders incl. 7 deaths
- 69,276 Respiratory, thoracic and mediastinal disorders incl. 1,833 deaths
- 74,806 Skin and subcutaneous tissue disorders incl. 140 deaths
- 3,643 Social circumstances incl. 22 deaths
- 18,264 Surgical and medical procedures incl. 185 deaths
- 40,907 Vascular disorders incl. 740 deaths
Total reactions for the mRNA vaccine mRNA-1273(CX-024414) from Moderna: 10,782 deaths and 510,009 injuries to 15/01/2022
- 11,363 Blood and lymphatic system disorders incl. 118 deaths
- 16,962 Cardiac disorders incl. 1,110 deaths
- 188 Congenital, familial and genetic disorders incl. 9 deaths
- 5,960 Ear and labyrinth disorders incl. 6 deaths
- 480 Endocrine disorders incl. 6 deaths
- 7,107 Eye disorders incl. 36 deaths
- 41,950 Gastrointestinal disorders incl. 399 deaths
- 135,810 General disorders and administration site conditions incl. 3,551 deaths
- 773 Hepatobiliary disorders incl. 54 deaths
- 5,003 Immune system disorders incl. 20 deaths
- 20,787 Infections and infestations incl. 1,031 deaths
- 9,730 Injury, poisoning and procedural complications incl. 205 deaths
- 11,563 Investigations incl. 390 deaths
- 4,660 Metabolism and nutrition disorders incl. 260 deaths
- 62,441 Musculoskeletal and connective tissue disorders incl. 215 deaths
- 653 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 81 deaths
- 85,799 Nervous system disorders incl. 1,007 deaths
- 862 Pregnancy, puerperium and perinatal conditions incl. 8 deaths
- 96 Product issues incl. 4 deaths
- 8,976 Psychiatric disorders incl. 178 deaths
- 2,899 Renal and urinary disorders incl. 211 deaths
- 11,475 Reproductive system and breast disorders incl. 9 deaths
- 22,050 Respiratory, thoracic and mediastinal disorders incl. 1,142 deaths
- 26,090 Skin and subcutaneous tissue disorders incl. 95 deaths
- 2,158 Social circumstances incl. 45 deaths
- 2,608 Surgical and medical procedures incl. 199 deaths
- 11,566 Vascular disorders incl. 393 deaths
Total reactions for the vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/ AstraZeneca: 7,749 deaths and 1,136,049 injuries to 15/01/2022
- 13,763 Blood and lymphatic system disorders incl. 271 deaths
- 20,678 Cardiac disorders incl. 812 deaths
- 229 Congenital familial and genetic disorders incl. 7 deaths
- 13,283 Ear and labyrinth disorders incl. 8 deaths
- 673 Endocrine disorders incl. 5 deaths
- 19,849 Eye disorders incl. 31 deaths
- 106,411 Gastrointestinal disorders incl. 422 deaths
- 299,266 General disorders and administration site conditions incl. 1,826 deaths
- 1,017 Hepatobiliary disorders incl. 67 deaths
- 5,311 Immune system disorders incl. 37 deaths
- 39,194 Infections and infestations incl. 591 deaths
- 13,232 Injury poisoning and procedural complications incl. 195 deaths
- 25,062 Investigations incl. 200 deaths
- 12,894 Metabolism and nutrition disorders incl. 122 deaths
- 166,466 Musculoskeletal and connective tissue disorders incl. 157 deaths
- 719 Neoplasms benign malignant and unspecified (incl cysts and polyps) incl. 38 deaths
- 231,313 Nervous system disorders incl. 1,142 deaths
- 605 Pregnancy puerperium and perinatal conditions incl. 19 deaths
- 198 Product issues incl. 1 death
- 20,856 Psychiatric disorders incl. 69 deaths
- 4,281 Renal and urinary disorders incl. 72 deaths
- 16,524 Reproductive system and breast disorders incl. 3 deaths
- 40,829 Respiratory thoracic and mediastinal disorders incl. 1,035 deaths
- 51,563 Skin and subcutaneous tissue disorders incl. 61 deaths
- 1,596 Social circumstances incl. 8 deaths
- 1,804 Surgical and medical procedures incl. 29 deaths
- 28,433 Vascular disorders incl. 521 deaths
Total reactions for the COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson: 2,342 deaths and 122,048 injuries to 15/01/2022
- 1,186 Blood and lymphatic system disorders incl. 48 deaths
- 2,420 Cardiac disorders incl. 196 deaths
- 40 Congenital, familial and genetic disorders incl. 1 death
- 1,260 Ear and labyrinth disorders incl. 3 deaths
- 98 Endocrine disorders incl. 1 death
- 1,591 Eye disorders incl. 10 deaths
- 9,402 Gastrointestinal disorders incl. 88 deaths
- 32,903 General disorders and administration site conditions incl. 659 deaths
- 146 Hepatobiliary disorders incl. 13 deaths
- 527 Immune system disorders incl. 10 deaths
- 7,442 Infections and infestations incl. 198 deaths
- 1,092 Injury, poisoning and procedural complications incl. 25 deaths
- 5,756 Investigations incl. 127 deaths
- 725 Metabolism and nutrition disorders incl. 56 deaths
- 16,739 Musculoskeletal and connective tissue disorders incl. 54 deaths
- 82 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 8 deaths
- 22,885 Nervous system disorders incl. 242 deaths
- 54 Pregnancy, puerperium and perinatal conditions incl. 1 death
- 29 Product issues
- 1,677 Psychiatric disorders incl. 21 deaths
- 506 Renal and urinary disorders incl. 29 deaths
- 2,720 Reproductive system and breast disorders incl. 6 deaths
- 4,322 Respiratory, thoracic and mediastinal disorders incl. 293 deaths
- 3,652 Skin and subcutaneous tissue disorders incl. 10 deaths
- 395 Social circumstances incl. 4 deaths
- 822 Surgical and medical procedures incl. 72 deaths
- 3,577 Vascular disorders incl. 167 deaths

*These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
Full article
January 19, 2022
Posted by aletho |
War Crimes | COVID-19 Vaccine |
Leave a comment

The European (EEA and non-EEA countries) database of suspected drug reaction reports is EudraVigilance, verified by the European Medicines Agency (EMA), and they are now reporting 36,257 fatalities, and 3,244,052 injuries following injections of four experimental COVID-19 shots:
From the total of injuries recorded, almost half of them (1,540,852) are serious injuries.
“Seriousness provides information on the suspected undesirable effect; it can be classified as ‘serious’ if it corresponds to a medical occurrence that results in death, is life-threatening, requires inpatient hospitalisation, results in another medically important condition, or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, or is a congenital anomaly/birth defect.”
A Health Impact News subscriber in Europe ran the reports for each of the four COVID-19 shots we are including here. It is a lot of work to tabulate each reaction with injuries and fatalities, since there is no place on the EudraVigilance system we have found that tabulates all the results.
Since we have started publishing this, others from Europe have also calculated the numbers and confirmed the totals.*
Here is the summary data through January 1, 2022.
Total reactions for the mRNA vaccine Tozinameran (code BNT162b2, Comirnaty) from BioNTech/ Pfizer: 16,471 deaths and 1,546,829 injuries to 01/01/2022
- 42,225 Blood and lymphatic system disorders incl. 230 deaths
- 50,455 Cardiac disorders incl. 2,379 deaths
- 467 Congenital, familial and genetic disorders incl. 45 deaths
- 20,812 Ear and labyrinth disorders incl. 11 deaths
- 1,616 Endocrine disorders incl. 5 deaths
- 23,826 Eye disorders incl. 37 deaths
- 124,211 Gastrointestinal disorders incl. 652 deaths
- 386,451 General disorders and administration site conditions incl. 4,668 deaths
- 1,780 Hepatobiliary disorders incl. 83 deaths
- 17,061 Immune system disorders incl. 86 deaths
- 67,000 Infections and infestations incl. 1,769 deaths
- 28,457 Injury, poisoning and procedural complications incl. 302 deaths
- 38,560 Investigations incl. 487 deaths
- 10,496 Metabolism and nutrition disorders incl. 269 deaths
- 185,798 Musculoskeletal and connective tissue disorders incl. 204 deaths
- 1,451 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 136 deaths
- 255,661 Nervous system disorders incl. 1,756 deaths
- 2,254 Pregnancy, puerperium and perinatal conditions incl. 58 deaths
- 232 Product issues incl. 3 deaths
- 28,114 Psychiatric disorders incl. 193 deaths
- 5,594 Renal and urinary disorders incl. 258 deaths
- 59,397 Reproductive system and breast disorders incl. 6 deaths
- 66,518 Respiratory, thoracic and mediastinal disorders incl. 1,801 deaths
- 71,771 Skin and subcutaneous tissue disorders incl. 136 deaths
- 3,457 Social circumstances incl. 22 deaths
- 13,685 Surgical and medical procedures incl. 157 deaths
- 39,480 Vascular disorders incl. 718 deaths
Total reactions for the mRNA vaccine mRNA-1273 (CX-024414) from Moderna: 10,170 deaths and 465,080 injuries to 01/01/2022
- 9,961 Blood and lymphatic system disorders incl. 113 deaths
- 15,564 Cardiac disorders incl. 1,039 deaths
- 179 Congenital, familial and genetic disorders incl. 9 deaths
- 5,591 Ear and labyrinth disorders incl. 6 deaths
- 443 Endocrine disorders incl. 6 deaths
- 6,731 Eye disorders incl. 36 deaths
- 38,098 Gastrointestinal disorders incl. 380 deaths
- 123,337 General disorders and administration site conditions incl. 3,392 deaths
- 731 Hepatobiliary disorders incl. 51 deaths
- 4,671 Immune system disorders incl. 19 deaths
- 18,236 Infections and infestations incl. 965 deaths
- 9,241 Injury, poisoning and procedural complications incl. 191 deaths
- 10,065 Investigations incl. 321 deaths
- 4,394 Metabolism and nutrition disorders incl. 247 deaths
- 56,097 Musculoskeletal and connective tissue disorders incl. 208 deaths
- 628 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 79 deaths
- 78,044 Nervous system disorders incl. 965 deaths
- 815 Pregnancy, puerperium and perinatal conditions incl. 6 deaths
- 92 Product issues incl. 4 deaths
- 8,416 Psychiatric disorders incl. 169 deaths
- 2,725 Renal and urinary disorders incl. 197 deaths
- 10,682 Reproductive system and breast disorders incl. 9 deaths
- 20,529 Respiratory, thoracic and mediastinal disorders incl. 1,077 deaths
- 24,552 Skin and subcutaneous tissue disorders incl. 90 deaths
- 2,029 Social circumstances incl. 41 deaths
- 2,227 Surgical and medical procedures incl. 172 deaths
- 11,002 Vascular disorders incl. 378 deaths
Total reactions for the vaccine AZD1222/VAXZEVRIA (CHADOX1 NCOV-19) from Oxford/AstraZeneca: 7,371 deaths and 1,117,914 injuries to 01/01/2022
- 13,616 Blood and lymphatic system disorders incl. 261 deaths
- 20,296 Cardiac disorders incl. 788 deaths
- 215 Congenital familial and genetic disorders incl. 6 deaths
- 13,157 Ear and labyrinth disorders incl. 6 deaths
- 664 Endocrine disorders incl. 5 deaths
- 19,618 Eye disorders incl. 30 deaths
- 105,367 Gastrointestinal disorders incl. 393 deaths
- 293,748 General disorders and administration site conditions incl. 1,740 deaths
- 1,004 Hepatobiliary disorders incl. 66 deaths
- 5,228 Immune system disorders incl. 35 deaths
- 36,265 Infections and infestations incl. 564 deaths
- 13,023 Injury poisoning and procedural complications incl. 188 deaths
- 24,589 Investigations incl. 191 deaths
- 12,747 Metabolism and nutrition disorders incl. 113 deaths
- 164,732 Musculoskeletal and connective tissue disorders incl. 144 deaths
- 704 Neoplasms benign malignant and unspecified (incl cysts and polyps) incl. 34 deaths
- 228,601 Nervous system disorders incl. 1,095 deaths
- 586 Pregnancy puerperium and perinatal conditions incl. 19 deaths
- 194 Product issues incl. 1 death
- 20,622 Psychiatric disorders incl. 65 deaths
- 4,226 Renal and urinary disorders incl. 71 deaths
- 16,282 Reproductive system and breast disorders incl. 3 deaths
- 40,154 Respiratory thoracic and mediastinal disorders incl. 963 deaths
- 50,986 Skin and subcutaneous tissue disorders incl. 59 deaths
- 1,581 Social circumstances incl. 6 deaths
- 1,686 Surgical and medical procedures incl. 28 deaths
- 28,023 Vascular disorders incl. 497 deaths
Total reactions for the COVID-19 vaccine JANSSEN (AD26.COV2.S) from Johnson & Johnson: 2,245 deaths and 114,229 injuries to 01/01/2022
- 1,113 Blood and lymphatic system disorders incl. 46 deaths
- 2,196 Cardiac disorders incl. 186 deaths
- 40 Congenital, familial and genetic disorders incl. 1 death
- 1,227 Ear and labyrinth disorders incl. 3 deaths
- 93 Endocrine disorders incl. 1 death
- 1,548 Eye disorders incl. 9 deaths
- 9,141 Gastrointestinal disorders incl. 87 deaths
- 30,336 General disorders and administration site conditions incl. 623 deaths
- 143 Hepatobiliary disorders incl. 13 deaths
- 509 Immune system disorders incl. 10 deaths
- 5,832 Infections and infestations incl. 187 deaths
- 1,060 Injury, poisoning and procedural complications incl. 23 deaths
- 5,197 Investigations incl. 126 deaths
- 709 Metabolism and nutrition disorders incl. 55 deaths
- 16,069 Musculoskeletal and connective tissue disorders incl. 50 deaths
- 80 Neoplasms benign, malignant and unspecified (incl cysts and polyps) incl. 8 deaths
- 21,863 Nervous system disorders incl. 234 deaths
- 52 Pregnancy, puerperium and perinatal conditions incl. 1 death
- 29 Product issues
- 1,627 Psychiatric disorders incl. 21 deaths
- 485 Renal and urinary disorders incl. 29 deaths
- 2,625 Reproductive system and breast disorders incl. 6 deaths
- 4,115 Respiratory, thoracic and mediastinal disorders incl. 283 deaths
- 3,506 Skin and subcutaneous tissue disorders incl. 10 deaths
- 372 Social circumstances incl. 4 deaths
- 785 Surgical and medical procedures incl. 69 deaths
- 3,477 Vascular disorders incl. 160 deaths

*These totals are estimates based on reports submitted to EudraVigilance. Totals may be much higher based on percentage of adverse reactions that are reported. Some of these reports may also be reported to the individual country’s adverse reaction databases, such as the U.S. VAERS database and the UK Yellow Card system. The fatalities are grouped by symptoms, and some fatalities may have resulted from multiple symptoms.
January 6, 2022
Posted by aletho |
Science and Pseudo-Science | COVID-19 Vaccine, European Union |
1 Comment