A warning is appropriate. Reading this article with a large amount of medical science information will likely increase your anxiety and fear. The views of many distinguished medical experts paint a bleak view of COVID vaccines.
The likely reaction to the science is very different than the fear constantly propagated by the evil Dr. Fauci and his supporters. Here is the difference: They want you to fear the COVID virus and to accept vaccination, masking, lockdowns, school closings, and other forms of medical tyranny. With extensive data and expert assessments, this manifesto defines a vaccine dystopia.
It is a terrible condition where fear of the virus is replaced by fear of the vaccines – supposedly the remedy for the virus. This manifesto supports a different solution to the virus: Give greater attention and importance to a host of treatment protocols that can and should replace unsafe vaccines.
Another dimension to revolting against the vaccine dystopia is the need to reclaim personal medical freedom – your right to determine what medicine and vaccine to put into your body, not the government, especially when the government has a biased, one-sided view of vaccine safety.
Introduction
We are at the edge of history, in a global society where there is great suffering and injustice because of the widespread commitment to getting the entire population jabbed with COVID vaccines that the government claims are safe.
As shown below, in truth there are ever-increasing deaths and harmful health impacts from all the COVID vaccines. But governments do not give credence to the many awful health impacts of the vaccines, no matter how many esteemed physicians and medical researchers present evidence for stopping vaccination efforts.
The political and medical establishments keep using the same insensitive argument. No matter how many people die from the vaccines – often within days of getting jabbed – those in power proclaim that more lives are saved from using the vaccines against COVID than are lost due to them.
So many thousands of people worldwide have died from the jabs, probably 100,000 or more based on data from CDC, the European Union, and other nations. But negative vaccine impacts are largely ignored by big media, the public health system, and authoritarian politicians.
Sneaking into the public limelight are some famous people dying from the shots from the realms of sports, entertainment, and politics. But these are easily forgotten or ignored. Or seen as exceptions, statistically speaking.
In our quickly evolving vaccine dystopia, the vaccinated are granted many rewards and the unvaccinated are shamed, castigated, and bullied.
We have not yet reached the critical inflection point where the many medical voices against vaccines (given below) prevail. Their voices are suppressed by big media; their medical science arguments and data are ignored. The result is that most of the population remain victims and slaves to massive propaganda about the benefits of vaccines.
Ignored are not only the ill vaccine effects but also the enormous financial benefits obtained by makers of vaccines. Medical experts are unable to win the battle despite their science-based critiques of the vaccines. Yet what else can they do than to keep offering their expert medical advice?
Insanity is often defined as maintaining behavior that is proven wrong, destructive, and unhealthy. In our nascent vaccine dystopia, those with power keep pushing more vaccinations even as the death toll and harmful health impacts keep mounting, and vaccine effectiveness shrinks.
Keep pushing more shots as if a magical solution to COVID will emerge. Medical experts say it will not. COVID will never be completely eradicated. Proven cheap, safe and effective treatments using generic medicines like ivermectin must be seen as safe and effective alternatives to vaccines.
Perhaps over time vaccine-induced deaths and serious adverse health impacts will become so visible that the powerful vaccine machine will grind to a halt. Why? Because authoritarian and dystopian societies eventually collapse. However, only after incredible numbers of people have died and suffered.
The many anti-vaccine medical experts cited below will have little pleasure from being ignored and criticized for so long only, eventually, to be seen as correct. Some kind of revolution is needed to overturn the multi-pronged vaccine empire.
Below are data, scientific judgments, and new studies and analyses that present compelling evidence against mass COVID vaccination. This is all we can do right now to fight vaccine dystopia and nourish the needed revolution.
New analysis of all major vaccines
Physician J. Bart Classen published an extremely valuable analysis. He examined clinical trial data from all three of the major vaccine makers and found their vaccines cause more harm than good. Here are highlights from his article.
Data were “reanalyzed using ‘all-cause severe morbidity,’ a scientific measure of health, as the primary endpoint. ‘All-cause severe morbidity in the treatment group and control group was calculated by adding all severe events reported in the clinical trials.
Severe events included both severe infections with COVID-19 and all other severe adverse events in the treatment arm and control arm respectively. This analysis gives a reduction in severe COVID-19 infections the same weight as adverse events of equivalent severity. Results prove that none of the vaccines provide a health benefit and all pivotal trials show a statically significant increase in ‘all-cause severe morbidity’ in the vaccinated group compared to the placebo group.”
In other words, he found that each of the vaccines caused more severe events in the immunized group than in the control group. No safety.
This was his main conclusion:
“Based on this data it is all but a certainty that mass COVID-19 immunization is hurting the health of the population in general. Scientific principles dictate that the mass immunization with COVID-19 vaccines must be halted immediately because we face a looming vaccine induced public health catastrophe.”
Manipulation of data
So many actions are pure fraud, designed to deceive the public and push a media story that makes unvaccinated people look bad.
The trick used by CDC that was revealed in some publications, but not big media, is to count the deaths of fully vaccinated people as unvaccinated if the deaths occurred within 14 days of their final vaccination.
Their goal was to make unvaccinated people look like pandemic culprits causing the continued spread of COVID. Indeed, what big media did produce to influence public opinion was that unvaccinated people were the problem.
All this to convince more people to get vaccinated.
In truth, the medical reality is that vaccinated people are dying for two reasons. Some are inflicted with serious health impacts from the vaccines themselves, such as blood clots that kill people from strokes and other maladies. Second, many are victims of breakthrough COVID infections that can cause death because vaccines over time become increasingly ineffective in protecting against COVID.
One astute critic said this: “This means if someone was hospitalized, admitted to ICU, required mechanical ventilation, or died within two weeks of getting the jab they are being counted as ‘unvaccinated,’” said Kelen McBreen. “The entire [CDC] report can basically be tossed into the trash thanks to the inclusion of the recently vaccinated in the unvaccinated category,” wrote McBreen.
“This intentionally misleading data is now being used to infringe on the rights of the people of California and across the entire United States as vaccine mandates and passports are being rolled out nationwide.”
To add more context to what CDC has done, consider the following report of a revelation by a whistleblower.
In sworn testimony, she claimed to have proof that 45,000 Americans have died within three days of receiving their COVID-19 shot.
The declaration is part of a lawsuit America’s Frontline Doctors (AFD) against U.S. Department of Health and Human Services Secretary Xavier Becerra. That is a remarkably higher number than CDC has reported.
According to the whistleblower’s sworn document, she is “a computer programmer with subject matter expertise in the healthcare data analytics field, an honor that allows me access to Medicare and Medicaid data maintained by the Centers for Medicare and Medicaid Services (CMS).”
After verifying data from the CDC’s adverse reaction tracking system VAERS, the whistleblower focused only on individuals who died within three days of receiving their shot.
“It is my professional estimate that VAERS (the Vaccine Adverse Event Reporting System) database, while extremely useful, is under-reported by a conservative factor of at least 5,” she added. She came to that conclusion by examining the Medicare and Medicaid data in respect to those who died within three days of vaccination.
It should be noted that some years ago a Harvard study found that the system could be undercounting by a factor of 10 to 100.
Her statement also made an important point regarding how the COVID pandemic is not being managed the way previous vaccines have been treated. “Put in perspective, the swine flu vaccine was taken off the market which only resulted in 53 deaths,” said the statement.
EXAMPLE OF WHY 12 -DAY CDC PRACTICE IS FRAUDULENT
Back in January, there was a news story about the death of 56-year old Florida doctor Gregory Michael who died from a rare autoimmune disorder he developed on December 21 three days after receiving the Pfizer vaccine. His wife said that in her mind his death was 100% linked to the vaccine.
One doctor came forward publicly to say he also believed the vaccine caused the victim to develop acute idiopathic-thrombocytopenic-purpura (ITP), the blood disorder, and brain hemorrhage that killed him.
Dr. Jerry L. Spivak, an expert on blood disorders at Johns Hopkins University, who was not involved in Dr. Michael’s care, said “I think it is a medical certainty that the vaccine was related. It happened and it could happen again.”
His medical reasons were that the disorder came on quickly after the shot, and “was so severe that it made his platelet count ‘rocket’ down.” Over the following months, huge amounts of medical research documented vaccine-induced blood problems, including the one that hit the Florida physician.
There is still more to the data corruption designed to send a deceitful message to the public. A July story noted: “a physician contacted the Globe and said testing protocol from Scripts [health care system] is indicating that they aren’t testing the vaccinated in the hospitals – they are only testing the unvaccinated for COVID despite the many COVID breakthrough cases reported.
The physician contacted another hospital and reported to the Globe : ‘They HAVE NOT been testing the vaccinated for COVID routinely like they have the unvaccinated, but they JUST changed their policy to begin doing this.’ Unbelievable! So all this BS in the newspapers has been spewing about the vaccinated NOT having COVID BECAUSE THEY DON’T TEST FOR IT!”
All this was done very likely in hospitals all over the nation so that big media could push the story that there was a “pandemic of the unvaccinated.”
There is still more corruption to acknowledge.
In 2020 CDC issued new instructions for medical examiners, coroners, and physicians to give more credit for COVID as the cause of death. Pre-existing conditions or comorbidities were to be recorded in Part II rather than Part I of death certificates.
This was a major rule change from the 2003 handbooks to be used for reporting deaths. This single change resulted in significant inflation of COVID-19 fatalities by instructing that COVID-19 be listed in Part I of death certificates as a definitive cause of death regardless of confirmatory evidence, rather than listed in Part II as a contributor to death in the presence of pre-existing conditions, as would have been done using the 2003 guidelines.
The result was significant inflation in COVID fatality totals by as much as 1600% above what they would be had the CDC used the 2003 handbooks. It comes down to what many people now understand, namely so many people die with COVID but not FROM COVID.
As a final example of data corruption and shortcomings, consider what was revealed at a recent meeting of nurses. They explained what they are facing in their hospital work, which also helps explain why so many nurses and physicians have refused vaccination.
One nurse said she ran an ER department, and that it was tragic that they were seeing so many heart attacks and strokes, and that it is obvious that they are related to the COVID-19 shots. Another nurse stated that she was never trained about how to submit a report to VAERS about vaccine adverse events, and did not even know it existed until she did some research on her own.
She said there is pressure to NOT report vaccine injuries and deaths, and it takes about 30 minutes to fill out the report, which few will do.
In our blossoming vaccine dystopia, you cannot trust information coming from big media, the government, and the medical establishment.
British and other International data show vaccine truths
A new report with detailed data from Public Health England provides some startling numbers. For the period of February 1 through August 2, there were COVID Delta variant cases for 47,000 people who had received 2 vaccine doses, and for 151,054 people who were unvaccinated.
In the first group of vaccinated people, there were a total of 402 deaths. In the second much larger group with more than three times unvaccinated people, there were just 253 deaths. In other words, of the total COVID deaths 61 percent were in fully vaccinated people.
To get the death rate you divide the number of deaths by the total number of infection cases. That gives a death rate of .86 percent among the vaccinated and .17 percent among the unvaccinated.
That is an amazing difference. The death rate among vaccinated was just over five times greater than that for the unvaccinated.
Five times greater! In other words, unvaccinated people who got infected were enormously safer from death. Proving that COVID vaccines are not safe.
How can we explain this huge difference in terms of medical science?
It should also be noted that it was determined that the measured viral load in both groups was the same. So, why are vaccinated people dying more frequently than the unvaccinated? Here are some plausible explanations.
First, there is something very dangerous and unsafe in the COVID vaccines associated with spike proteins that are causing people to die at a higher rate.
For example, as discussed elsewhere, all current vaccines have been associated with serious blood problems, notably both large and microscopic blood clots. Many people have died from brain bleeds and strokes, for example.
There are also many, many other types of adverse side effects causing a host of medical problems.
Two famous virologists warned against using the current vaccines because they are fundamentally unsafe and could be killing people. They envisioned a vaccine dystopia and loudly proclaimed that the mass vaccination program should be halted.
Instead, they advocated the use of treatments using generic medicines like ivermectin, as detailed in Pandemic Blunder. As well as strengthening natural immunity.
Second, it is reasonable to believe that most unvaccinated people have acquired natural immunity from some prior COVID infection. And that natural immunity is far more protective than the artificial or vaccine immunity obtained from jabs. Their natural immunity translates to fewer deaths.
Yet the US like many other countries does not give credit for natural immunity on a par with vaccine immunity when it comes to COVID passports and mandates. Though a few nations do the right thing by honestly following the science.
Third, vaccinated people are susceptible to breakthrough infections, which means that they are not protected against infection after they have been originally infected. Phony and dangerous COVID vaccines do not destroy the virus, nor prevent transmitting it to others. Some breakthrough infections are lethal.
Putting aside problems with CDC data, the death rate found in the UK for vaccinated people translates to about 1,300 deaths for vaccinated Americans. Indeed, an August report revealed that new CDC data indicated 1,507 people of those fully vaccinated died.
It seems like these figures are only for breakthrough infection deaths because the CDC VAERS database indicates more than 6,000 vaccine deaths (through August 27) that are reported as vaccine adverse effects. [But nearly 14,000 deaths apparently when non-US data are included.]
A higher death rate from COVID for vaccinated people in the US compared to other countries might be related to a generally unhealthier population with more serious health conditions, notably high levels of obesity.
Just days ago, it was reported that West Virginia saw a 25 percent increase in deaths of people that are fully vaccinated over the last eight weeks. At the same time, it was reported that in Massachusetts 144 people fully vaccinated also died from COVID, an 80 percent increase from several weeks earlier, and that new total translates to about 4,800 for the whole nation.
In New Jersey, there was a 16 percent increase in breakthrough deaths recently.
The new data from England involving very large numbers of people should be headline news. But the biased and dishonest big media suppress this kind of critical data. Why?
Clearly, if vaccinated people die at a much higher rate than unvaccinated people, then why should people be enthusiastic about being vaccinated for initial shots or later booster ones? They should not. This is especially true for the millions of people who have natural immunity.
Data from other countries merits attention because of still more proof of the deficiencies of the COVID vaccines.
In August director of Israel’s Public Health Services, Dr. Sharon Alroy-Preis announced half of all COVID-19 infections were among the fully vaccinated.
Signs of more serious disease among fully vaccinated are also emerging, she said, particularly in those over the age of 60.
A few days later, Dr. Kobi Haviv, director of the Herzog Hospital in Jerusalem, reported that 95 percent of severely ill COVID-19 patients are fully vaccinated and that they make up 85% to 90% of COVID-related hospitalizations overall.
In Scotland, official data on hospitalizations and deaths show 87% of those who have died from COVID-19 in the third wave that began in early July were vaccinated.
In Ireland, 18 percent of COVID deaths were in fully vaccinated people.
There is only one rational conclusion from examining all the foreign data: COVID vaccines are both unsafe and ineffective.
Great article on vaccine failure
This recent article displays a lot of wisdom about COVID vaccines; here are some excerpts.
“The Corona vaccines don’t work very well. Ubiquitous statistics showing that the vaccinated enjoy substantial protection against serious illness and death seem wrong. In some cases, they are probably manipulated. They are certainly confounded by the different testing regimes to which the vaccinated and the unvaccinated are subjected. Once you forget the specifics of efficacy and look at the broader picture, it is easy to see where we are. The vaccines have not reduced Corona mortality compared to the same time last year in any jurisdiction that I know of. Countries with high vaccination rates are now seeing the same number of deaths, or more, as they had at the beginning of September 2020.
“The vaccinated remain substantially protected against serious illness or death, but the unvaccinated are entering the hospital and dying at very high rates indeed as if to compensate. Thus Israel has maintained the same case fatality rate of around 0.7%, before and after mass vaccination.
“Vaccines against coronaviruses have been used in animals for decades, and none of them work very well. Generally, they begin to fail after a few months. Despite their technical sophistication, our mRNA and vector vaccines against SARS-2 are no different. They had some success when they were first rolled out, but if anything that probably made things worse.
“Our universal vaccination campaigns worked just well enough to speed up the evolutionary processes that are always and everywhere optimizing Corona.” That means the virus keeps outwitting us.
“It is impossible to believe that this failure was not foreseen. The scientists who developed the vaccines knew for sure how things would play out. That’s why they concluded the trials after three or four months and vaccinated their controls. It’s why they have been talking about boosters from the very beginning. It’s why, if you listened carefully, you never heard Zero Covid sloganeering coming from Team Vaccine. Only the comparative morons on Team Lockdown ever talked like that.
“Our politicians and our new public health dictators, on the other hand, remained oblivious to the limited potential of the vaccines. They continue to insist on universal vaccination and green passes, while it is obvious that these will do nothing to influence the course of the pandemic.
“Corona policy in every western country has unfolded more or less according to the same script, devised by the World Health Organisation at the end of February 2020. The final act was supposed to be the wide-scale eradication of Corona after mass vaccination. It is now clear that this will never happen. For the first time since March 2020, there is no obvious international consensus on the way forward.
“A few countries, or perhaps even a few prominent politicians or public health pundits who do not have their heads up their asses, could change everything. Everyone who is not crazy needs to start insisting on the same simple message:
“We have to live with Corona, it will always be with us. Biannual boosters for the entire population will not solve anything. They will only reduce the effectiveness of vaccines by encouraging antigenic drift. The vaccines are, at best, a solution for the elderly and the vulnerable only. Everyone will get Corona, even the vaccinated, and children need to get it while they are still young and while it poses no risk to them. In this way, SARS-2 will become an unimportant virus in the coming years.”
But will that happen before we suffer through a vaccine dystopia?
This article gave no attention to treatments, but here is one of the many comments that addressed this issue well:
“When do the powers that start focusing on TREATMENTS for those who contract covid, regardless of vaccination status?? No other infection, condition, disease, etc… don’t have treatment options, except for covid… they, the powers that be, go so far as to block treatment options or make them incredibly hard to get.
“It’s past time to make the various treatments readily available… they don’t have to be 100% successful, but we should be given the choice to try them!!”
Vaccine dystopia seen by some esteemed scientists
If the material above has made you depressed, you may not want to keep reading. Some great medical scientists have gone public with very negative views of the future because of mass COVID vaccine use.
Chief among these forecasters of vaccine doom is Dr. Judy Mikovits. She became widely seen as a conscientious whistleblower when she talked about “mass murder” and said that 50 million Americans will die because of the vaccines.
Her medical science credentials are impeccable, including a long stint at the National Cancer Institute. Her views may seem extreme to some people, but they are based on a deep scientific understanding and are consistent with the highly frightening forecasts of other scientists and physicians.
Here are some of her views:
“Most people don’t realize the [COVID] vaccines do not prevent infection. You’re injecting the blueprint of the virus and letting a compromised system try to deal with it. And worse, it doesn’t go in the cells that a natural infection would, that have lock and key receptors, gatekeepers, so that only certain cells can be infected, like the upper respiratory tract for a coronavirus. Now you’re making it in a nanoparticle which means it can go in every cell without that receptor. So, can you imagine the damage of bypassing God’s natural immunity and allowing the blueprint for coronavirus that also has components of HIV in some strains, meaning you can infect your white blood cells. So now you’re going to inject an agent into every cell of the body. I just can’t even imagine a recipe for anything other than what I would consider mass murder on a scale where 50 million people will die in America from the vaccine. The numbers from the XMRV’s (xenotropic murine leukemia virus-related virus) and the vaccine injuries for the (past) 40 years support that.”
Her warning that these injections can cause death is confirmed by Dr. Sucharit Bhakdi, an award-winning researcher and former head of the Institute of Medical Microbiology and Hygiene in Germany; he was a professor of virology and microbiology for 30 years in Germany.
In the statement shown below, he warns that by taking these injections, killer lymphocytes already present in our body will cause an auto-immune attack with terrible consequences for our health and even death. He made this statement:
“The big, big danger about this vaccine is you are shooting the gene of the virus into your body. It is going to go through the body and go to entering cells that you don’t know. These cells are going to start making, not the whole virus, but virus protein, and these cells are going to put the waste of that spike protein in front of their cells. And the killer lymphocytes will see the waste, and, you know, anyone who does not understand there is going to be an autoimmune attack because the killer lymphocytes are already there. It is with this that I will say, “Bye bye,” (death) because you don’t realize what you are going to do. You are going to plant the seed of autoimmune reactions.”
Dr. Sherri Tenpenny is board certified in emergency medicine and osteopathic manipulative medicine and author of several books on the impact of vaccines. When she was specifically asked about the forecast from Dr. Mikovits, she said:
“If they don’t die, they’re going to be seriously injured. There are some things in life that are worse than death, you know, having to live with chronic inflammatory drug induced hepatitis, you know, having chronic seizure disorders, having debilitating autoimmune diseases. Some people are so sick it would be merciful if they died.”
Add to these views the warnings from Dr. Michael Yeadon, former Vice President of Pfizer with a Ph.D. in respiratory pharmacology, and Dr. Wolfgang Wodarg, former head of the Public Health Department in Germany and a doctor of pneumology. They sent an urgent petition to the European Union demanding a halt to COVID-19 vaccine studies due to safety concerns.
They specifically identified the following serious side effects:
Infertility
Allergic, potentially fatal reactions due to polyethylene glycol (PEG) which is contained in the vaccine.
Exaggerated immune reactions, especially when the vaccine recipient is confronted (later in life) with the real “wild” virus. They report that these exaggerated immune reactions to corona vaccines have long been known from experiments with cats. 100% of the vaccinated cats died after catching the wild virus.
Here are a few more examples of dire predictions about the COVID vaccines:
Dr. Luc Montagnier, a French virologist and recipient of the 2008 Nobel Prize in Medicine for his discovery of the human immunodeficiency virus (HIV) is worth listening to. He has a doctorate in medicine and has received more than 20 major awards. Montagnier refers to the mass vaccine program as an “unacceptable mistake” and is a “scientific error as well as a medical error.” His assertion is that “The history books will show that… it is the vaccination that is creating the variants.”
In other words: “There are antibodies, created by the vaccine,” forcing the virus to “find another solution” or die. This is where the variants are created. It is the variants that “are a production and result from the vaccination.” He is talking about the mutation and strengthening of the virus from a phenomenon known as Antibody-Dependent Enhancement (ADE).
ADE is a mechanism that increases the ability of a virus to enter cells and cause a worsening of the disease. His bottom line: “Faced with an unpredictable future, it is better to abstain.” But most people will find it extremely difficult to resist all the coercion and vaccine mandates.
As to the much talked about and hope for herd immunity, he has said: “the vaccines Pfizer, Moderna, Astra Zeneca do not prevent the transmission of the virus person-to-person and the vaccinated are just as transmissive as the unvaccinated. Therefore, the hope of a ‘collective immunity’ by an increase in the number of vaccinated is totally futile.”
Dr. Vanden Bossche has considerable credentials that make his views worth consideration. He has a Ph.D. in Virology from the University of Hohenheim, Germany, and has held faculty appointments at universities in Belgium and Germany. He was at the German Center for Infection Research in Cologne as Head of the Vaccine Development Office.
He has said: “Given the huge amount of immune escape that will be provoked by mass vaccination campaigns and flanking containment measures, it is difficult to imagine how human interventions would not cause the COVID-19 pandemic to turn into an incredible disaster for global and individual health.”
He talks about selective viral ‘immune escape’ where viruses continue to be shed from those who are infected [both vaccinated and nonvaccinated] because neutralizing antibodies fail to prevent replication and elimination of the virus.
A frightening forecast by Bossche is that the worst of the pandemic is still to come. Hard to believe considering all the bad news propaganda about cases, hospitalizations, and deaths. But he thinks we are now experiencing the calm before the ultimate storm. Imagine a new wave of infection far worse than anything we’ve seen so far is how Bossche thinks. How does this happen?
There will be more mutants or variants to which the adaptive immune system from vaccine shots provides little resistance. At the same time, there will be decreased innate or natural immune effectiveness. Unless people take a number of steps to boost their natural immunity.
Here is his big picture view: “There is only one single thing at stake right now and that is the survival of our human race, frankly speaking.” This too is a very strong view. The “mass vaccination program is… unable to generate herd immunity.” If true, there is little hope of seeing the COVID pandemic ending.
In a public comment to the CDC on April 23, 2021, molecular biologist and toxicologist Dr. Janci Chunn Lindsay, Ph.D., called on CDC to immediately halt Covid vaccine production and distribution. Citing fertility, blood-clotting concerns (coagulopathy), and immune escape, Dr. Lindsay explained to the committee the scientific evidence showing that the coronavirus vaccines are not safe.
She holds a doctorate in biochemistry and molecular biology from the University of Texas, and has over 30 years of scientific experience, primarily in toxicology and mechanistic biology. “I strongly feel that all the gene therapy vaccines must be halted immediately due to safety concerns on several fronts,” she said.
Also noted was that “Covid vaccines could induce cross-reactive antibodies to syncytin [a protein], and impair fertility as well as pregnancy outcomes.” Yet another issue was this: “there is strong evidence for immune escape, and that inoculation under pandemic pressure with these leaky vaccines is driving the creation of more lethal mutants that are both newly infecting a younger age demographic, and causing more Covid-related deaths across the population than would have occurred without intervention.
That is, there is evidence that the vaccines are making the pandemic worse.”
Dr. Theresa Deisher warned about the dangers of mRNA permanently re-writing our genetic code by making changes to our DNA. She graduated with honors and distinction from Stanford University and obtained her Ph.D. in Molecular and Cellular Physiology from the Department of Molecular and Cellular Physiology, Stanford University. “The vaccines that are messenger RNA (mRNA), what they do is they act like a virus and they hijack the cell’s machinery to turn that mRNA into the protein. Now, messenger RNA can also be what’s called reverse transcribed into DNA. Okay, an RNA virus uses a reverse transcriptase in our cells to make itself into DNA and permanently insert into the genome. Viruses can do that. There is a possibility that the messenger RNA could be made into DNA and be permanently inserted. It doesn’t have all of the efficient components of a virus but the spontaneous possibility is there. In a gene therapy trial, the experts said the danger is 10 to the minus 13 (which is one in a trillion). Four of nine boys (participating in the trial) had DNA insertions and developed leukemia. Four of nine is a lot different from one in a trillion.”
Dr. Johan Denis, a medical doctor and homeopath from Belgium, warns, “This vaccine is just not proven safe. It has been developed too quickly. We have no idea what the long-term effects will be. It needs much more investigation. There is no hurry or emergency. It might possibly change your DNA. This is irreversible and irreparable for all future generations.”
A report in May by 57 top scientists and physicians sent a clear message about COVID vaccines. “The recently identified role of SARS-CoV-2 glycoprotein Spike for inducing endothelial damage characteristic of COVID-19, even in absence of infection, is extremely relevant given that most of the authorized vaccines induce the production of Spike glycoprotein in the recipients.
Given the high rate of occurrence of adverse effects, and the wide range of types of adverse effects that have been reported to date, as well as the potential for vaccine-driven disease enhancement, Th2-immunopathology, autoimmunity, and immune evasion, there is a need for a better understanding of the benefits and risks of mass vaccination, particularly in the groups that were excluded in the clinical trials.”
“Despite calls for caution, the risks of SARS-CoV-2 vaccination have been minimized or ignored by health organizations and government authorities.”
“In the context of these concerns, we propose halting mass-vaccination and opening an urgent pluralistic, critical, and scientifically-based dialogue on SARS-CoV-2 vaccination among scientists, medical doctors, international health agencies, regulatory authorities, governments, and vaccine developers.”
Conclusions
Ponder this for a while: Even though we probably have entered vaccine dystopia can we still save humanity and our society?
So many people have already been jabbed and for those who have died and been stricken with various health problems, it is too late. But many millions have not yet been jabbed. And now many millions must accept or reject booster shots.
Many have strong natural immunity from prior COVID infection that the weight of scientific evidence says is better than vaccine immunity. For them, vaccine shots are unnecessary and potentially dangerous.
All COVID vaccine decisions are difficult. How informed are people really? Is consent just a mindless formality? Sign and get jabbed. Then what?
But the more you know about vaccine data and science, the more likely you will be motivated to seek alternatives to the vaccines. It will be hard work to regain medical freedom. The pro-vaccine army that permeates all big media will keep saying that vaccines are needed to save lives.
They conveniently ignore all the deaths and adverse health impacts. The unknown is whether these will increase enough to show the folly of their argument. Will the vaccine doomsayers be proven correct?
If the forces of evil pushing medical tyranny prevail, then a very dark vaccine dystopia probably awaits us.
About the author: Dr. Joel S. Hirschhorn, author of Pandemic Blunder and many articles on the pandemic, worked on health issues for decades. As a full professor at the University of Wisconsin, Madison, he directed a medical research program between the colleges of engineering and medicine. As a senior official at the Congressional Office of Technology Assessment and the National Governors Association, he directed major studies on health-related subjects; he testified at over 50 U.S. Senate and House hearings and authored hundreds of articles and op-ed articles in major newspapers. He has served as an executive volunteer at a major hospital for more than 10 years. He is a member of the Association of American Physicians and Surgeons and America’s Frontline Doctors.
Chile’s September 11, in 1973, brought a brutal end to Salvador Allende’s socialist rule. In its wake, violence permeated Chilean society, through the U.S.-backed military coup which was to provide gruesome inspiration for the later regional systematic surveillance and elimination of socialists and communists known as Operation Condor, in which several Latin American countries were involved.
The mass arrests of Chileans loyal to Allende and socialist politics became a long purge in the country. The Caravan of Death – one of the earlier dictatorship operations aimed at instilling terror within the country – was carried out in the coup’s aftermath, between September 30 and October 22, 1973, after securing Santiago by means of brutal suppression, torture and killings. Dictator Augusto Pinochet’s purge was aimed at silencing dissent throughout the country, and also to ensure the military’s loyalty towards the dictatorship – any negligence or lenience exhibited by any individual would be punished by methods used against dissenting Chileans. The ultimate aim, according to retired Lieutenant Colonel Marcos Herrera Aracena, was “to bring an end to the remaining legal processes… In other words, finish with them once and for all.”
The Caravan of Death massacres are considered to be among the most brutal not only due to the extermination methods involved – at times the corpses were unrecognizable due to bludgeoning – but also because many Chileans willingly turned themselves in for interrogation.
Army officers travelled in Puma helicopters throughout Chile, inspecting detention centres and giving orders for execution, or carrying out the executions themselves. Testimony from La Serena indicates that 15 prisoners were executed by firing squad and their bodies buried in a mass grave. To prevent any possible dissemination of knowledge, at least in the immediate aftermath, the official version publicized by the dictatorship was that the prisoners had attempted an escape.
While at first the dictatorship seemed adamant on making its brutality known to quash any resistance, the more refined methods of disappearance and secret extermination sites hastened a culture of impunity and oblivion. The Calama massacres – the last stop in the Caravan of Death – was such an example. Relatives of the disappeared sought information about the whereabouts of their loved ones to no avail. It was the female relatives of the disappeared in Calama who took matters into their own hands and started physically searching for the bodies of their loved ones in the Atacama Desert. The dictatorship had forbidden any leaking of information due to the extent of mutilations the victims had been subjected to by the execution squads. As the women’s resilience increased, so did the dictatorship’s efforts to prevent any discovery of the bodies through exhumation and reburial of remains.
The Rettig Commission established that 75 Chileans were killed and their bodies disappeared throughout the operation, headed by Brigadier General Sergio Arellano Stark, and with the participation of agents Manuel Contreras, Marcelo Moren Brito, Sergio Arredondo Gonzalez, Armando Fernandez Larios and Pedro Espinoza Bravo – all of who played prominent roles in the torture and disappearances of dictatorship opponents throughout Pinochet’s rule. Contreras headed the National Intelligence Directorate (DINA), Brito oversaw torture at Villa Grimaldi, while Fernandez Larios was involved in the assassination of Chilean economist and diplomat Orlando Letelier in Washington, carried out by double agent for DINA and the CIA, Michael Townley.
Although indicted by Judge Juan Guzman Tapia on December 1, 2000 for ordering the Caravan of Death killings, dictator Pinochet escaped justice on account of purported health reasons. In relation to dictatorship memory and rupture, the Caravan of Death stands as a forewarning of what was to be unleashed in Chile throughout Pinochet’s rule and its aftermath. Particularly in Calama, the women’s resilience against the dictatorship can be seen as one of the earliest expressions against the nationwide oblivion through which Pinochet attempted to crush any questioning, let alone investigations, into dictatorship-era crimes.
Here is how I know the forced vaccination program is not intended to protect me and others from Covid but has some other, unspoken purpose(s):
1. People with pre-existing immunity are being required to get the vaccine, though it provides no additional benefit and only confers the risk of side effects. This is based on the totality of the evidence, not a few cherrypicked studies. Recovered people have stronger and longer-lasting immunity, which acts against many more epitopes than just spike protein.
2. People with pre-existing immunity are not being allowed to get an antibody test to use to show they are already immune, although such tests were approved by FDA for use by vaccine manufacturers to screen subjects in all their Covid vaccine clinical trials for immunity.
3. People with PCR evidence of prior infection cannot use this to avoid vaccination, even though CDC counts each one as a case. T cell tests cannot be used to demonstrate existing immunity and avoid a shot either.
4. The US government, the EU and some other countries have signed contracts for several doses per person plus the option to purchase 8 or 9 doses PER PERSON. How did they know, last winter-spring, they would need them? They didn’t. They don’t need them, because they barely work against current variants.
5. They must have contracted for them because they planned to use this many doses before they had any idea of the duration of effectiveness of current vaccines.
6. Antibody tests done in the UK suggested that over 90% of the population was already immune. Most likely we too have surprisingly high rates of immunity in the population.
7. Israel, with the highest population rate of vaccination and even highest rate of people who have received 3d doses, currently has the highest rate of active Covid cases in the world.
I hope this is crystal clear: you are not being vaccinated to give you immunity, but for one or more other purposes. The current plan is to revaccinate you every 5-8 months, either with the same or perhaps tweaked vaccines. In Israel, the vaccine passport now expires without the third dose.
Imagine implementing passports here, and in a few years your passport will expire without the 8th or 15th dose… and your ‘privileges’ like shopping or jogging disappear…
It is currently not possible to know exactly what is in the vial you receive. Different types of complex and expensive tests need to be done, but it is very difficult to get a vial and prove a chain of custody. Not all vials may be identical.
We do have laws on the books guaranteeing bodily autonomy, informed consent, the right to privacy, the right to practice your religion, and no forced treatment with experimental products.
Yes, these laws are being ignored. It is our job to make them known, to insist they are followed, and to resist illegal edicts.
During the last 18 months, social media platforms have often used the recommendations of the CDC as a basis of censorship online. The CDC’s own “Myths and Facts” section explained clearly, and still does at the time of publication, that the federal government does not mandate vaccines and that it’s a matter for states and local governments.
Social media users who suggested that Biden was going to introduce a federal mandate were censored online and told they were providing misinformation, likely falling back on the fact that the CDC’s own statement on the issue (a go-to source for mainstream social media platforms) said it was false and Speaker of the House Nancy Pelosi had also made it clear that the federal government doesn’t have the power to exert such authority.
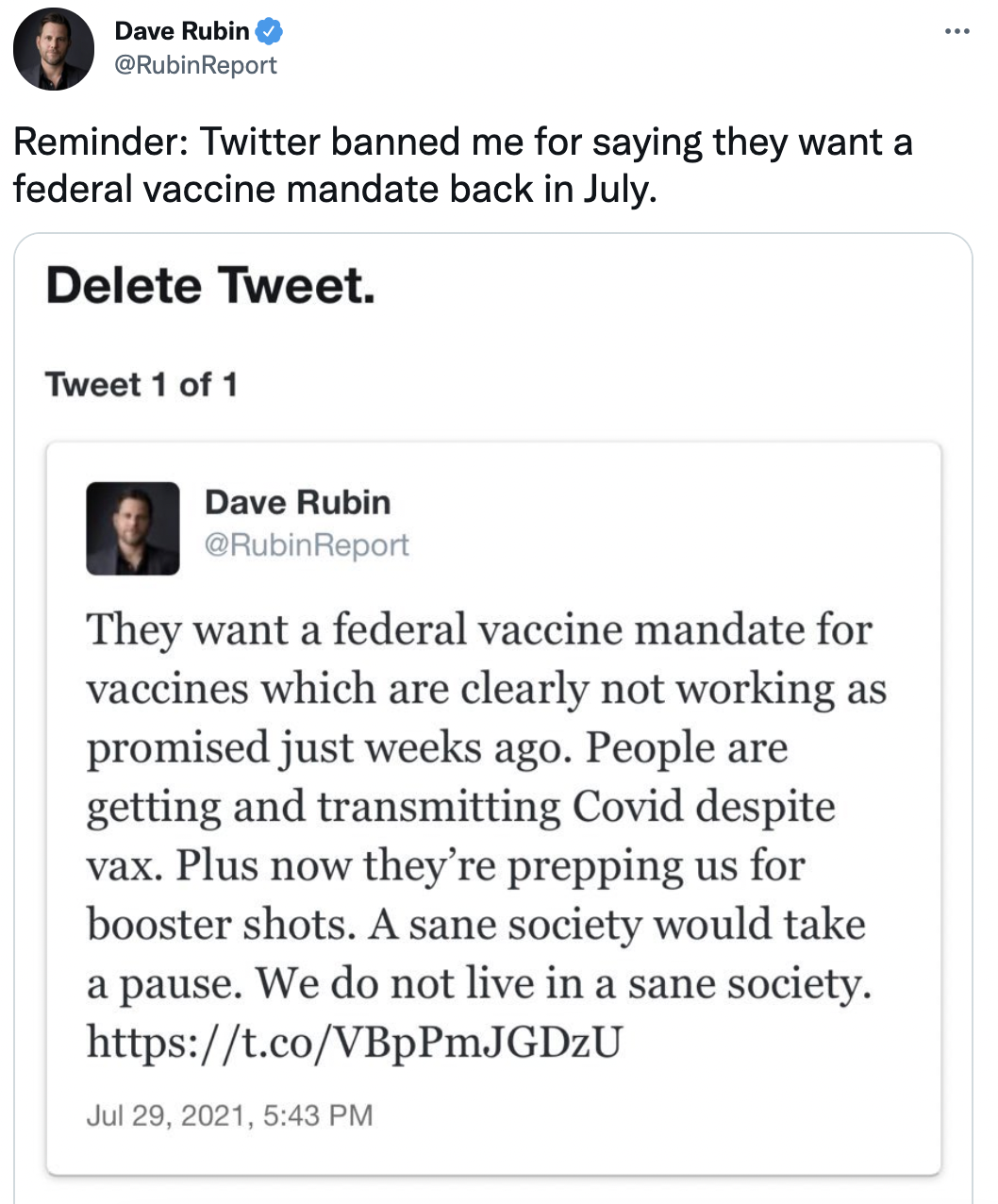
Back in July, Dave Rubin, an author and political commentator, was locked out of Twitter for saying the Biden administration wanted a federal vaccine mandate.
“They want a federal vaccine mandate for vaccines which are clearly not working as promised just weeks ago. People are getting and transmitting Covid despite vax. Plus now they’re prepping us for booster shots. A sane society would take a pause. We do not live in a sane society,” read his original tweet.
On Friday, he took to Twitter to remind people of his suspension for predicting something that was going to happen.
Alongside a screenshot of the original tweet, he wrote: “Reminder: Twitter banned me for saying they want a federal vaccine mandate back in July.”
He had to remove the tweet for his account to be restored.
Similarly, the popular YouTube commentary channel MrObvious, had a video removed by YouTube for making a similar statement; that Biden would federally mandate vaccines.
“About a week ago I made a video on YouTube about vaccine federal mandates and YouTube took down that video. I don’t know why – maybe they thought that I was simply – I don’t know – jumping the gun saying that Biden was going to do these federal mandates,” Mr Obvious said in a recent video. “Well guess what? Mr Obvious was in fact right.”
THE British historian Guy de la Bédoyère claims that ‘Australia is falling apart’. Off Guardian suggests that we are ‘going full fascist’. Daily reports in France, Russia and everywhere in between and beyond, hover between pity, amusement and disbelief. How did this happen – in Australia? The overseas storytelling can barely keep up with the never-ending stream of new announcements designed to grind us into the ground. But on and on it goes.
There is, at last, a book-length account of Australia’s eighteen months of madness that will either warm the hearts of Covid realists, remind us of all the Covid policy absurdities or perhaps simply provide yet more chilling evidence of the sinister forces at work that are changing us irrevocably.
Unfolding Catastrophe: Australia (Sense of Place Publishing, 2021), by John Stapleton, restores – though perhaps only a little – the faith we ought to have in the journalist class, so utterly diminished by their sitting out the crushing of our lives (at best) and their active collaborating in the spread of Covid propaganda (at worst).
Recognising early on the biggest story of all of our lives, Stapleton set out to record in graphic detail and with authenticity the developing catastrophe, from the toilet paper crisis at the start to the emerging apartheid regime for those who refuse the State Injectible.
Stapleton records with palpable astonishment the now familiar litany of harms that have been done, not only to the body politic, but to our core values, indeed, to our very sense of our country. Our place. They include the impositions of lockdowns that do not work but cause harm beyond telling; the ‘wildly inaccurate’ modelling that predicted catastrophe and instead merely delivered fame and riches for those involved; the succession of non-medical interventions with no basis in science and without popular understanding that this is the case; the low information voter; the punitive policing; the absence of real leadership in the crisis; the incoherent messaging from the top; the disaster that is ‘National Cabinet’; magic money tree economics; the relentless announcables; the Covid cronyism; the entrenching of power by the political class.
This all amounts to ‘a radical social experiment going against decades of epidemiological wisdom’. It has been, Stapleton suggests, ‘demonic’. Not just stupid and deranged, but evil. It has caused, as we now see in all our empty churches, ‘spiritual damage’. Earthly lives gone, and souls lost. A sad tale of deceit and compliance, of induced fear, isolation, economic deprivation, destroyed friendships and civil fracture. A creepy but unmistakable feel of the Biblical End Times, the streets empty. Astonishing submissiveness. A story of manufactured narratives, of a ‘disinformation feedback loop’ as Stapleton reports, his previous faith in the scepticism of his countrymen utterly destroyed. Societal dysfunction. Many ‘conspiracy theories’ across the internet have proved to be spot on.
The book draws upon a broad range of expert observers, who include journalists of every colour and distinguished academics such as the Spectator’s Ramesh Thakur, a breath of fresh air amid the fetid atmosphere of secular decline. Ramesh’s call on the Covid response, as reported by Stapleton: ‘The greatest mistake in history’. World War One is right up there, but this call is no exaggeration.
Rational argument simply does not work with our rulers. Copious evidence relating to the policy disasters of the pandemic never breaches the walls of the bubble. As Stapleton said in an interview with Sydney Criminal Lawyers, ‘it all fell on deaf ears’.
Is the tide of opinion turning against the ever-increasing crush of medical technocracy? Stapleton has cautious optimism. Speaking up for those of us who, mercifully, live outside the cities, he says: ‘But there are no cases or virtually no cases in this area. Nobody knows anybody who has died.’ Pennies may, at last, be dropping. Crisis? What crisis? It is a case-demic of a very mild strain of the initial virus, without the remotest hospitalisation crisis
Chillingly, as Stapleton says, ‘All of this has been done in secret, and in our name.’ The parliaments rarely sit. Public Health Orders trump democratic processes. Reasons are never given for policy actions beyond formulaic tosh. We never signed up for this.
Steve Waterson, one of the few consistently sane voices in the corporate media, describes the book as a ‘devastating indictment of Australia’s response to the Covid pandemic’. I am glad Waterson didn’t confine himself to ‘Australian governments’, for we are, all of us, complicit in this truly diabolical attack on everything we have all lived for. Stapleton uses the term ‘manipulated’ and ‘held hostage’ to describe our corporate media’s role in the fiasco.
Stapleton, alone, it seems, among our publishers and authors, has taken a stand – for freedom, common sense, perspective and Aussie values. His is a stand for life itself. His work shames his colleagues who have chosen to sit quietly in the corner these past eighteen months, or worse, to join in the chanting for the Covid Fascist State. This book is the methodical work of a brave truth-teller who is willing to call a spade a bloody shovel, in the best tradition of fair-dinkum journalism.
As the first draft of history, this magnificent book should be marked ‘essential reading’. Normally one might add here: ‘Send a copy to your member of parliament’. Alas, I fear, in this case, such a course of action would be pointless. Our rulers are in and settled, on a good wicket, and they intend to bat on.
A ‘signal collapse and rearrangement of society’? Who on earth could disagree?
Dr Julie Ponesse, a professor of ethics at the University of Western Ontario and a member of the Canadian Covid Care Alliance on the current vaccine mandates and passports in the context of our existing informed consent laws and commitments to privacy and bioethics.
Covid-19 Vaccine Mandates Are Now Pointless: Covid-19 vaccines do not keep people from catching the prevailing Delta variant and passing it to others
1) Excellent scientific research papers published or posted in August 2021 clearly demonstrate that current vaccines do not prevent transmission of SARS-CoV-2.
2) Vaccines aim to achieve two ends:
To protect the vaccinated person against the illness.
To keep people from carrying the infection and transmitting it to others.
If enough people are vaccinated or otherwise become immune, it is hoped that the disease will stop circulating. We call this herd immunity.
On the way to herd immunity, there is an assumption that people who are immunized can form safe clusters or groups within which no one is carrying or transmitting the virus.
3) Unfortunately, this last assumption (2.b.ii) is no longer true under the new variant of SARS-CoV- 2, Delta (B.1.617.2), which now accounts for essentially all cases worldwide.
4) Delta is more infectious than the Alpha strain (B.1.1.7) that prevailed in the UK from January to May 2021 (and in the US from March to June 2021), meaning that Delta is passed more readily person-to-person than the previous dominant strain. (see section 5, below).
b. From its origin in India, Delta has soared to nearly complete domination of COVID-19 viral strains everywhere in a matter of months, because it spreads so easily and infects both vaccinated and unvaccinated people.
5) New research in multiple settings shows that Delta produces very high viral loads (meaning, the density of virus on a nasopharyngeal swab as interpreted from PCR cycle threshold numbers).
Viral loads are much higher in people infected with Delta than they were in people infected with Alpha.
Viral loads with Delta are equally high whether the person has been vaccinated or not.
Viral load is an indicator of infectiousness. [13,14] The more virus one has in the noseand mouth, the more likely it is to be in this individual’s respiratory droplets and secretions, and to spread to others.
6) Due to evolution of the virus itself, all the currently licensed vaccines (all based on the originalWuhan strain spike protein sequence) have lost their ability to accomplish vaccine purpose 2(b), above, “To keep people from carrying the infection and transmitting it to others.”
7) Vaccine mandates are thus stripped of their justification, since to vaccinate an individual nolonger stops or even slows his ability to acquire and transmit the virus to others.
8) Under Delta, natural immunity is much more protective than vaccination. All severities ofCOVID-19 illness produce healthy levels of natural immunity.
The Documentary Evidence:
Here are three studies whose findings and data support the above statements:
(A) The first is by the Massachusetts Department of Health and the CDC, published August 6, 2021 in the CDC’s Morbidity and Mortality Weekly Report. An outbreak of COVID-19 occurred in Provincetown, Massachusetts in July 2021 during two weeks of heavily attended indoor and outdoor public gatherings. The study focuses on the 469 cases among Massachusetts residents who were in attendance. [1] All successfully gene-sequenced isolates (120) were the Delta variant.
346 of the cases in Massachusetts residents (74%) occurred in fully vaccinated people who had received a 2-dose course of the BioNTech/Pfizer or Moderna vaccine, or a single dose of the Johnson & Johnson. Vaccine coverage at this time among all Massachusetts residents was 69%. This suggests that vaccinated people became infected just as frequently as unvaccinated people in this outbreak.
We do not know the vaccination percentage among actual festival attendees who were Massachusetts residents, but we can assume given the demographics of the festival that it was the state average (69%) or higher. We also do not know the total number of Massachusetts residents who attended. Both of these numbers would be needed to determine actual values for vaccine efficacy in this outbreak.
However, we cannot brush the high percentage of vaccinated people in the infected sample under the carpet quite as easily as the authors do, when they say, “As population-level vaccination coverage increases, vaccinated persons are likely to represent a larger proportion of COVID-19 cases” (p. 1061). This is true, but we would still, if vaccine is protective, find vaccinated cases to be underrepresented in an illness sample compared to the number vaccinated in the whole population of attendees. As best we can tell at this festival, vaccination was not protective against infection, because the proportion of vaccinated in the sample (74%) is in the same numeric range as the proportion vaccinated, 69% or above.
Among the 346 cases who were already vaccinated, 79% were symptomatic, reporting cough, headache, sore throat, muscle aches, and fever. Four of these vaccinated, infected individuals (1.2%) were hospitalized. No one died. The remainder of the vaccinated cases did not report symptoms.
Among the 123 cases who were unvaccinated or partially vaccinated, one was hospitalized (0.8%) and no one died. Percentage with symptoms was not reported.
Vaccinated and unvaccinated cases were found to have very similar viral loads (in a sample of 127 and 84 cases, respectively). This means the PCR tests showed that vaccinated and unvaccinated infected people were carrying similar amounts of virus in their upper respiratory tracts at diagnosis and were thus equally infectious.
(B) The next study, released August 10, 2021, examines the Delta viral load phenomenon in far more detail, and shows clearly that vaccinated people can become infected and pass the infection to other vaccinated people. The Hospital for Tropical Diseases in Ho Chi Minh City in southern Vietnam has about 900 staff members, including an Oxford University Clinical Research Unit. The entire hospital staff was vaccinated with the Oxford-AstraZeneca vaccine two-dose series in March and April 2021, and then enrolled in a post-vaccination study. Thus, a great deal of detailed information was available when the outbreak struck. [2]
The entire hospital staff was PCR negative for SARS-CoV-2 in mid-May 2021. The index case (first known case in a cluster) became mildly ill on June 11 and had a positive PCR with a high viral load. The whole staff was then re-tested. 52 additional cases were identified immediately. Ten more had high viral loads, a number being staff who shared an office with the index case. All the additional cases at first had no symptoms.
The hospital was then locked down. Over the next two weeks, 16 additional cases were identified in subsequent PCR surveys. 62 of the 69 PCR-positive cases participated in this study of the outbreak.
Forty-seven (76% of the 62 subjects) developed respiratory symptoms, three with pneumonia on chest x-ray and one requiring three days of nasal cannula oxygen (this is the least intensive form of oxygen therapy). Everyone recovered fully.
Peak viral loads in this fully vaccinated, infected group were, on average, 250 times higher than peak viral loads with older variants early in the pandemic (March-April 2020), when no one was vaccinated. This is a means of comparing the biology of the variants themselves: the Delta virus has gained the ability to replicate itself enormously in the upper respiratory tract, regardless of vaccination, thereby making itself more infectious.
In the current outbreak, viral loads (and thus infectiousness) peaked in the 2-3 days both before and after symptoms began.
All sequenced isolates were the Delta variant. The genetic sequences from hospital staff were more similar to each other than they were to contemporaneous isolates from the city at large or from more distant parts of the country. This means it is likely that the virus spread among the (fully vaccinated) hospital staff from a single infected (and vaccinated) staff member who brought it from the outside. Given the dynamics of symptoms and positivity among the staff, it is clear that asymptomatic or pre-symptomatic staff members, as well as symptomatic, were infecting others.
PCR tests continued to be positive up to 33 days after diagnosis (averaging 21 days). Case- control comparisons showed that staff members with lower titers of neutralizing antibodies after vaccination and at diagnosis were more likely to become infected. However, there was no correlation between vaccine-induced antibody levels at diagnosis and viral loads or the development of respiratory symptoms.
(C) The third study is an analysis of ongoing population-wide SARS-CoV-2 monitoring in the UK, whose primary purpose is following changes in vaccine efficacy. In the UK study, the PCR tests are done on members of randomly selected households across the UK, following a predetermined schedule that ignores symptoms, vaccination, and prior infection. The current analysis was released on August 24, 2021 and summarized in commentary in the British Medical Journal on August 19, 2021. [3, 4]
The study includes measures of viral load or “burden” under Alpha and Delta predominance. While Alpha was the dominant UK strain (January to mid-May 2021), vaccination or prior COVID- 19 disease strongly reduced viral load compared to unvaccinated people who had never had COVID-19.
The sample size was large and random, obtained as described above. 12,287 new PCR-positives were found in the Alpha-dominant period, of which 88% were unvaccinated and had no evidence of prior infection. Only 0.5% of new positive tests were from fully vaccinated people and 0.6% from people with prior COVID-19 infection. Since it was a large, random sample and vaccination percentages increased dramatically in the UK across this time period, we can safely say that vaccination and prior infection were very protective against becoming infected with the Alpha variant. Virtually all the new infections occurred in unvaccinated people.
After mid-June 2021, when greater than 92% of PCR positives in the UK were Delta, the differences in viral load between vaccinated, unvaccinated, and people with past COVID-19 disease nearly vanished. Viral loads in all three groups were much higher than with Alpha, indicating increased infectiousness. More vaccinated people were now showing symptoms when they became positive, also correlated with viral load.
During the Delta-dominant period, the sample was 1939 new positive PCR tests. Of these, 17% (326) were from unvaccinated people without prior COVID-19 disease, 1% (20) were unvaccinated with evidence of prior disease, and 82% (1593) were fully vaccinated. This is approximately the percentage of the UK population who were vaccinated by August 18, 2021— when 75-83% of UK residents were fully vaccinated and 84-89% had received at least one dose. [5]
Like the Massachusetts study reviewed above, this suggests that the new Delta variant infects vaccinated and unvaccinated people with equal probability. To go from 0.5% of randomly sampled new infections in vaccinated people (under Alpha) to 82% (under Delta) in several months, as the population is becoming more and more vaccinated—these are extraordinary numbers.
If vaccination is still effective in preventing infection, we would expect the proportion of infections in a random population sample to be less than the proportion of the population vaccinated. If 82% of randomly obtained positive tests occur in vaccinated people, and about 82% of people are vaccinated, then vaccination is not reducing the likelihood of infection at all. Efficacy at preventing infection has become zero.
The UK study addresses vaccine efficacy in much more complex ways than the straightforward numbers I present here. The authors conclude that both of the earlier UK-approved vaccines (BioNTech/Pfizer and Oxford-AstraZeneca) have lost some efficacy against Delta compared to Alpha. But both vaccines, they maintain, remain substantially effective at keeping people from becoming infected with the Delta strain, in the range of 67 to 80%. If this is the case, why was 82% of their random sample of new positive PCR tests from vaccinated people?
If a vaccine reduces the risk of becoming infected by two-thirds (67%), we would expect the proportion of vaccinated in the positive sample to be less than the proportion of vaccinated in the population. Say we start with 1000 people in the country, of whom we will randomly sample 100. The country is 80% vaccinated. This means that in our sample of 100 we have 80 vaccinated and 20 unvaccinated people. Let’s say that the virus has infected 10% of the people across the sampling period, or 10 total cases. If 8 of the infected are among the vaccinated, and 2 in the unvaccinated (80% and 20% of the positives, matching the ratio of vaccinated and unvaccinated in the population), the vaccine has made no difference in whether one can get infected (0% efficacy). If the vaccine is 67% effective, the cases in the vaccinated group would be reduced by 2/3 to 2.67 cases, and the total cases would be only 4.67 cases (2.67 vaccinated and 2 unvaccinated). This means that only 2.67/4.67 or 57% of the cases would be in the vaccinated group, and 43% in the unvaccinated. (We can go back to 10% overall being positive just using ratios, yielding 5.7 cases among the vaccinated and 4.3 among the unvaccinated.)
This is why the proportion vaccinated in the infected sample, very close to the proportions vaccinated in the total population, are incompatible with the efficacy numbers generated by the authors. It appears to me—as in the Massachusetts study—that the vaccine is not decreasing susceptibility to infection at all, and is in reality somewhere between slightly (insignificantly) decreasing susceptibility and slightly increasing susceptibility to the Delta variant.
The UK study is clear that viral load (and thus infectiousness to others) is much greater with Delta than with Alpha, and that, with Delta, viral load and infectiousness are equal in vaccinated and unvaccinated infected people.
Discussion #1:
These three different studies in three countries with three different population sampling methods produced the same result: with the current, dominant Delta strain, vaccinated people become infected and carry just as much infectious virus in their upper respiratory tracts when infected as unvaccinated people. The reproducibility of this finding makes it a very strong finding.
The study in Vietnam shows clearly that infected, vaccinated people transmit the infection to others.
Under the current dominance of the Delta variant, being vaccinated or not has no influence on a chief determinant of infectiousness: the size of the viral load carried in the nose and mouth of an infected person. In addition, both vaccinated and unvaccinated become infected in significant numbers, approximating the ratios of vaccinated and unvaccinated in the population.
The rationale for mandates—that each individual has a responsibility to be vaccinated to limit spread of the virus to others—is hereby seriously or even fatally undermined. The decision to be vaccinated, under Delta predominance, has become entirely personal, affecting only the future health and well-being of the individual receiving the vaccine.
Blaming the unvaccinated for the rapid spread of the Delta variant has no merit whatsoever, since both vaccinated and unvaccinated infected people are equally infectious to others, and vaccinated and unvaccinated people are represented in illness samples in proportion to their representation in the general population, showing they are equally likely to become infected.
These findings also equalize vaccinated and unvaccinated in terms of quarantine, vaccine- based exclusion, or the wearing of masks.
The Delta variant has entirely changed our expectations of the effects of vaccination on containing the SARS-CoV-2 virus.
What about natural immunity from previous COVID-19 infection?
What about natural immunity from previous COVID-19 infection, with regard to the change in virus strain? An Israeli study posted on August 25, 2021 powerfully shows that “natural immunity [from previous COVID-19 infection] confers longer-lasting and stronger protection against infection, symptomatic disease and hospitalization caused by the Delta variant of SARS- CoV-2 compared to the BNT162b2 [BioNTech/Pfizer] two-dose vaccine-induced immunity.” If a person is both naturally immune and received one vaccine dose, immunity to Delta infection is even stronger. [6]
To demonstrate this, the authors studied the records of a large Israeli Health Maintenance Organization covering 2.5 million people (26% of the population). They compared the numbers of positive PCR tests from June 1 to August 14, 2021, when the Delta variant was dominant, in people who were either immunized in January-February 2021 or had COVID-19 infection in January-February 2021.
Those who were vaccinated but never had COVID-19 disease were 13 times more likely to develop a new SARS-CoV-2 infection than those made naturally immune by COVID-19 disease. The increased risk was also significant for having symptoms or not.
When the prior COVID-19 disease was allowed to happen earlier in the course of the pandemic, from March 2020 through February 2021, vaccinees who had never had COVID-19 disease were still (a) 6 times more likely to have a positive PCR in June-August 2021 than a naturally immune person, (b) 7 times more likely to have symptomatic disease, and (c) at greater risk for COVID- 19-related hospitalization.
By comparison, under Alpha strain dominance during the first half of 2021, over 50,000 staff members of the Cleveland Clinic in Ohio demonstrated that vaccine-induced immunity (from any of the three US-authorized vaccines) and natural immunity were equally protective against COVID-19 disease. [7]
The Israeli study shows at a later time period how the Delta variant has escaped the control of at least one of these vaccines, while natural immunity to earlier forms of SARS-CoV-2 still confers protection.
A Danish study of 203 recovered COVID patients shows that COVID-19 infection/disease provokes robust immune responses in the vast majority of people regardless of disease severity, including mild cases and even true asymptomatic cases (excluding those with false positive tests). [8]
Discussion #2:
It is difficult to tell anything about the virulence or pathogenicity of the Delta variant itself—how sick it makes people—since the available studies are all done in highly vaccinated populations. Vaccination has protected against severe disease and death with all the other variants, and may well do the same with the Delta variant. This remains the most compelling reason individuals may decide to be vaccinated.
What drives people—especially PhD’s, together with certain minorities [9]—to choose not to be vaccinated? There is substantial recorded and written evidence from first-hand observers and vaccine recipients themselves, and in the immunization “adverse effects” registries of both the US and Europe, that we are tolerating with COVID-19 vaccines a level of severe adverse effects, including death, that would have been unthinkable for any earlier vaccine.
So far, convincing evidence that these effects are “not related to vaccine” has not emerged. Convincing evidence would be research-lab-level autopsy studies of people deceased soon after vaccination (or ill soon after vaccination and eventually deceased), including immunofluorescence or other specific staining for the unique proteins, nucleic acids, and lipids of vaccine or SARS-CoV-2 itself in different tissues. (Some excellent examples of this approach are autopsy studies illuminating the pathophysiology of COVID-19 disease by C Magro and others at Weill Cornell Medical Center [e.g. 10].) Biopsy studies of key tissues in living affected people, such as those with persistent neurologic deficits after vaccination for COVID-19, would also provide powerful evidence. It is highly irregular and indeed unacceptable that such autopsy and biopsy studies have not been done.
Some prominent scientists and a significant number of physicians take these allegations of vaccine-caused injury very seriously. Doctors for Covid Ethics, a British/European/worldwide group of physicians, link the known pathophysiology of clots in COVID-19 disease [10] with a possible pathophysiologic mechanism explaining the numerous cases of thrombosis after vaccination, such as those in published literature due to the Oxford-AstraZeneca vaccine. [11,12] This mechanism would not be unique to one vaccine type or brand, nor are the reports of postvaccination thrombosis unique to one type or brand of vaccine.
In the four major papers reviewed above (Massachusetts, Vietnam, UK, and Israel), the biologic facts of the new Delta variant and its relationship to vaccination are clearly and reproducibly established. This is the value of good science.
Conclusion:
Given all the above evidence, mandating others to take a vaccine is a potentially harmful, damaging act.
Since the principal reason for COVID-19 vaccine mandates—protecting others from infection—has evaporated with the ascendance of the Delta variant, those who mandate COVID-19 vaccines may wish to seek legal counsel regarding their culpability and liability (including personal) for potential long-lasting harm to those whom they pressure into vaccination with threat of exclusion from employment or education or other public activity. Remind your attorney that if an unborn or nursing baby is damaged, liability persists until the child is age 23—plenty of time for discovery of the ways whereby vaccine producers and government regulators may have suppressed important information about harmful effects.
References:
Brown CM, Vostok J, Johnson H, Burns M, Gharpure R, Sami S, Sabo RT, Hall N, Foreman A, Schubert PL, Gallagher GR, Fink T, Madoff LC, MD, Gabriel SB, MacInnis B, Park DJ, Siddle KJ, Harik V, Arvidson, D, Brock-Fisher T, Dunn M, Kearns, Laney AS. 2021. Outbreak of SARS- CoV-2 infections, including COVID-19 vaccine breakthrough infections, associated with large public gatherings –– Barnstable County, Massachusetts, July 2021. MMWR Morb Mortal Wkly Rep 70:1059-1062: https://www.cdc.gov/mmwr/volumes/70/wr/pdfs/mm7031e2-H.pdf; published August 6, 2021.
Chau NVV, Ngoc NM, Nguyet LA, Quang VM, Ny NTH, Khoa DB, Phong NT, Toan LM, Hong NTT, Tuyen NTK, Phat VV, Nhu LNT, Truc NHT, That BTT, Thao HP, Thao TNP, Vuong VT, Tam TTT, Tai NT, Bao HT, Nhung HTK, Minh NTN, Tien NTM, Huy NC, Choisy M, Man DNH, Ty DTB, Anh NT, Uyen LTT, Tu TNH, Yen LM, Dung NT, Hung LM, Truong NT, Thanh TT, Thwaites G, Tan LV, OUCRU COVID-19 Research Group. 2021. Transmission of SARS-CoV-2 Delta variant among vaccinated healthcare workers, Vietnam. Preprints with The Lancet, available at http://dx.doi.org/10.2139/ssrn.3897733; posted August 10, 2021.
Pouwels KB, Pritchard E, Matthews PC, Stoesser N, Eyre DW, Vihta KD, House T, Hay J, Bell JI, Newton JN, Farrar J, Crook D, Cook D, Rourke E, Studley R, Peto T, Diamond I, Walker AS, and the COVID-19 Infection Survey Team. 2021. Impact of Delta on viral burden and vaccine effectiveness against new SARS-CoV-2 infections in the UK. medRxiv preprint: https://doi.org/10.1101/2021.08.18.21262237; posted August 24, 2021.
Griffin S. 2021. Covid-19: Fully vaccinated people can carry as much delta virus as unvaccinated people, data indicate. BMJ 374:2074: http://dx.doi.org/10.1136/bmj.n2074; published 19 August 2021.
6. Gazit S, Shlezinger R, Perez G, Roni Lotan R, Peretz A, Ben-Tov A, Cohen D, Muhsen K, Chodick G, Patalon T. 2021. Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections. medRxiv preprint: https://doi.org/10.1101/2021.08.24.21262415; posted August 25, 2021.
5. BBC News: “Covid vaccine: How many people in the UK have been vaccinated so far?” Downloaded on August 23, 2021. Updated article and graph available at https://www.bbc.com/news/health-55274833
Shrestha NK, Burke PC, Nowacki AS, Terpeluk P, Gordon SM. 2021. Necessity of COVID-19 vaccination in previously infected individuals. 2021. medRxiv preprint: https://doi.org/10.1101/2021.06.01.21258176; posted June 5, 2021.
Nielsen SSF, Vibholm LK, Monrad I, Olesen R, Frattari GS, Pahus MH, Højen JF, Gunst JD, Erikstrup C, Holleufer A, Hartmann R, Østergaard L, Søgaard OS, Schleimann MH, Tolstrup M. 2021. SARS-CoV-2 elicits robust adaptive immune responses regardless of disease severity. EBioMedicine 68:103410, https://doi.org/10.1016/j.ebiom.2021.103410; published June 4, 2021.
King WC, Rubinstein M, Reinhart A, Mejia RJ. 2021. Time trends and factors related to COVID-19 vaccine hesitancy from January-May 2021 among US adults: Findings from a large- scale national survey. medRxiv preprint: https://doi.org/10.1101/2021.07.20.21260795; posted July 23, 2021.
Magro C, Mulvey JJ, Berlin D, Nuovo G, Salvatore S, Harp J, Baxter-Stoltzfus A, Laurence J. 2020. Complement-associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: A report of five cases. Translational Research 220:1–13: https://doi.org/10.1016/j.trsl.2020.04.007; published online April 15, 2020.
Bhakdi, S. et al. 2021. Letter to Physicians: Four new scientific discoveries regarding COVID- 19 immunity and vaccines—implications for safety and efficacy.. Doctors for Covid Ethics website, https://doctors4covidethics.org/letter-to-physicians-four-new-scientific- discoveries-crucial-to-the-safety-and-efficacy-of-covid-19-vaccines/; posted July 9, 2021.
Kantarcioglu B, Iqbal O, Walenga JM, Lewis B, Lewis J, Carter CA, Singh M, Lievano F, Tafur A, Ramacciotti E, Gerotziafas GT, Jeske W, Fareed J. 2021. An update on the pathogenesis of COVID-19 and the reportedly rare thrombotic events following vaccination. Clin Appl Thrombosis/Hemostasis 27:1-14. https://journals.sagepub.com/doi/10.1177/10760296211021498; published June 1, 2021.
Jones TC, Biele G, Mühlemann B, Veith T, Schneider J, Beheim-Schwarzbach J, Bleicker T, Tesch J, Schmidt ML, Sander LE, Kurth F, Menzel P, Schwarzer R, Zuchowski M, Hofmann J, Krumbholz A, Stein A, Edelmann A, Corman VM, Drosten C. 2021. Estimating infectiousness throughout SARS-CoV-2 infection course. Science 373, 180. https://doi.org/10.1126/science.abi5273; published July 9, 2021.
van Kampen JJA, van de Vijver DAMC, Fraaij PLA, Haagmans BL, Lamers MM, Okba N, van den Akker JPC, Endeman H, Gommers DAMPJ, Cornelissen JJ, Hoek RAS, van der Eerden MM, Hesselink DA, Metselaar HJ, Verbon A, de Steenwinkel JEM, Aron GI, van Gorp ECM, van Boheemen S, Voermans JC, Boucher CAB, Molenkamp R, Koopmans MPG, Geurtsvankessel C, van der Eijk AA. 2021. Duration and key determinants of infectious virus shedding in hospitalized patients with coronavirus disease-2019 (COVID-19). Nature Communications 12, 267. https://doi.org/10.1038/s41467-020-20568-4; published January 11, 2021.
* Nina Pierpont is a graduate of Yale University (BA in biology), with a MA and PhD from Princeton University in population biology/evolutionary biology/ecology, and the MD degree from the Johns Hopkins University School of Medicine. She has been a Clinical Assistant Professor of Pediatrics at Columbia University’s College of Physicians & Surgeons. She is currently in private practice in upstate New York, specializing in behavioral medicine.
The 20th anniversary of September 11, 2001 is a particularly somber one, not just because of the horrific nature of events of that day reaching its second-decade milestone, but because of how little we seem to have learned in that amount of time.
The fear and trauma generated by the events of 9/11 were used by the U.S. national security state and its civilian allies to great effect to divide the American population, to attack independent reporting as well as independent thought, to gut the anti-war movement, and to normalize the U.S. government’s overt and persistent degradation of the country’s Constitution. This, of course, is in addition to the illegal U.S. occupations and drone wars in the Middle East and elsewhere that were also born out of this event.
The true beneficiaries of 9/11
As a nation, the U.S. populace has failed to grapple with these realities, and many others, in the two decades since the Twin Towers and WTC Building 7 fell. Far from bringing any benefit to the alleged masterminds of the event, the results of 9/11 instead overwhelmingly favored the ambitions of a powerful faction within the U.S. national security state that had long sought to bring the dissident-elimination efforts it spent decades implementing abroad – from the Phoenix Program in Vietnam to Operation Condor in South America – home to roost.
As a result, the response of the U.S. government to the attack supposedly launched by those “who hate us for our freedom” was to work to reduce our freedoms and civil liberties. Now, 20 years on, the sophisticated “War on Terror” apparatus has been fully turned into a “War on Domestic Terror,” with many of those who once opposed the war on terrorism abroad now cheering on the ratcheting up of its domestic equivalent.
Yet, the domestic terror apparatus being swiftly created and implemented very clearly targets individuals and ideologies on both sides of the political divide. It is also extremely vague, essentially leaving it up to those holding the reins of political power – whether Democrat, Republican or something else – to decide who is “terrorist” and who is not. Perhaps unsurprisingly, it was Joe Biden back in the mid-1990s who introduced legislation that would have given the president sole and unappealable authority to define what constitutes “terrorism,” a fact that was omitted from media coverage of last year’s presidential campaign and the past several months of his presidency.
A crisis of courage
It seems clear at this point that one of the key reasons the U.S. continues to hemorrhage its remaining civil liberties, either as a result of the new “War on Domestic Terrorism” or as a response to COVID-19, is that it is undergoing a crisis of conscience and courage in grappling with not just the true nature of the events of 9/11 itself, but with the orthodoxy over the “official story” of those events.
Even two decades after the fact, it is still deemed too controversial or unthinkable to question whether the official story is an accurate portrayal of the events that transpired on and led to that day. This is despite the fact that the official story itself, presumably the same story told by the 9/11 Commission report, has been labeled incomplete, and unable to answer major questions about that day, by its very authors. In addition, the official story relies heavily on testimony obtained through extreme torture, meaning it is of questionable accuracy.
Many of those who have been quick and vocal to point out the lies of the U.S. government when it comes to the invasions of Afghanistan and Iraq and other consequences of the War on Terror have been unable to even consider that the official story of 9/11 may not be legitimate and may indeed have been dealt from the same pack. This may be for a variety of reasons, including a strong desire to not be de-legitimized by their peers as bearers of the “conspiracy theorist” smear and an unwillingness to face a political reality where U.S. government officials may have been complicit in a deadly attack on American soil. In those two examples, however, the failure of such individuals, particularly in media, to even consider that there may be more to the story boils down to a desire for self-preservation in the case of the former and preservation of a particular worldview in the case of the latter. Yet, in both cases, the casualty is the truth and the cause is cowardice.
By failing as a society to thoroughly examine the events of 9/11 and why those events occurred, the American public has shown the powers that be that their desire to preserve a “safe” worldview — and to preserve their own careers, in the case of certain professional classes — is enough to keep people from questioning world-altering events when they emerge. Those powers are well aware of this refusal and have been using it to their advantage ever since.
The poison remains in our system
Today, with the COVID-19 crisis still dragging on, we are similarly immersed in a situation where nuance and facts are being cast aside, militantly in some cases, in favor of the establishment narrative. Is everyone who chooses not to take this particular vaccine a “conspiracy theorist” and “anti-vaxxer”? Does it really make sense to so dramatically divide the public into groups of vaccinated and unvaccinated through a new ID system when the vaccine claims to reduce the severity of illness but not to stop disease transmission? Should those that question the motivation of politicians, powerful pharmaceutical corporations and mainstream media “experts” be censored from expressing those views online?
You do not need to agree with those who hold such views, but what is wrong with hearing what they have to say and debating their evidence with your own? We are losing the ability to have rational public discourse about these issues — and losing it swiftly, at a speed comparable to what took place in the aftermath of 9/11, when questioning the motives of the Bush administration, U.S. intelligence agencies and other groups, as well as their proposed responses and “solutions,” was deemed “unpatriotic” and even “treasonous” by some. Calls were made to strip an entire class of Americans of their freedom for merely sharing the same ethno-religious identities as those we were told attacked us, and many went along with it. Freedom became treated as a privilege only for certain groups, not as a right, and this insidious fallacy has reared its head yet again in recent months in relation to the COVID-19 vaccine debate and also the war on domestic terror.
Our pandemic of fear
Though the failure to consider explanations for 9/11 that deviate from the official story can be called cowardice, the most enduring lesson 20 years on from 9/11 is perhaps that fear was and remains the most powerful tool that has been consistently used to whittle down our freedom and civil liberties. While the divide-and-conquer strategies have raged on from 9/11 to the present, the largest wealth transfers in history have occurred, creating an unaccountable and ultra-wealthy super-elite that dominates an ever-growing underclass.
The march towards this de facto neo-feudalism certainly didn’t begin on or after 9/11, but our collective failure to grapple with the narrative orthodoxies of that day have prevented us from fully understanding the big picture of that event as well as many subsequent and similarly consequential events. For too long, the desire to preserve our self-image, our reputation, and the worldview we are taught in school has all too often made hard, difficult truths a casualty.
In order to truly understand the War on Terror, the domestic surveillance state and our current reality, we must accept that we were lied to about 9/11. We must ask the hard questions and accept hard truths. We must put an end to the 20-plus-year-long pandemic of fear over “invisible enemies,” fear that has pushed us to surrender the very freedoms that we are told we are protecting.
The United States, and much of the world, is quickly becoming an unrecognizable and authoritarian dystopia. We cannot wait another two decades to grapple with the difficult questions and realities that arose after 9/11 and persist into the present. We will either be remembered as a country that took freedom and liberty for all seriously or we will be remembered as a nation of cowards who, driven by fear, were willing to deprive this group, then that group, of their freedom — before losing that freedom entirely.
Whitney Webb has been a professional writer, researcher and journalist since 2016. She has written for several websites and, from 2017 to 2020, was a staff writer and senior investigative reporter for MintPress News. She currently writes for her own outlet Unlimited Hangout and contributes to The Last American Vagabond and MintPress News
TWO decades after 9/11, which was eleven years to the day after President George H W Bush delivered his famous ‘new world order’ speech, the historical significance of both events is now much clearer.
Two decades of permanent ‘most favoured nation’ trading status for China has produced the largest transfer of wealth, technology, manufacturing capacity and markets in human history, and destroyed the American industrial economy.
Two decades of the ‘War on Terror’ and the cancerous growth of a global surveillance state has destroyed Western liberty and obliterated civil rights.
Two decades of the corporate internet, social media and smartphones has lobotomised Western culture, destroyed key Western institutions, engineered a rolling mass psychosis and transferred regional political and economic power to Silicon Valley and Wall Street.
Two decades of the occupation of Afghanistan, then Iraq, drone war and collateral murder in Pakistan, attacks on Libya, Syria and Yemen has destroyed the authority of the United States and its allies to the point where the senile winner of a crooked election mumbling prepared talking points inside a fortified Capitol is the nominal leader of what was once called the free world.
Before 9/11 it was still almost possible to believe America’s idealised story of itself. Today the USA can be compared to the most corrupt regimes in history, and may even be the most corrupt, given the scale of corruption now possible.
Gangster states, which are merely criminal rather than sadistic and depraved, now look at the United States with justified disgust.
But America is also no longer really America, just as Britain is no longer really Britain. Both are no more than holding companies of a global commercial conglomerate hostile to national power as a barrier to global domination, just as developing national power in an earlier era was determined to weaken regional power.
All this was accelerated after 9/11 through the imposition of a war whose structural outcome, if not objective, was the demolition of the democratic West, and it is now being accelerated yet further via the pandemic.
Once again shock propaganda has been used to declare a state of emergency and enable the seizure of power from the people to State and transnational organs. Here, too, a highly profitable permanent war has been declared against an invisible enemy with no definable conditions of victory, or even coherently stated aims.
Again, the winners are the same global political, economic and security elites who consolidated after 9/11 by destroying the independence and competence of the institutions over which they had acquired control in the process of converting them into instruments of domination.
Here too, beyond a lingering and misplaced respect for institutional authority, the plausibility-effect produced by endless, mantra-like repetition, and the production of irrelevant distractions, the official story remains unpersuasive.
In the days which followed 9/11 questions were already being asked about the relationship between the official story, the actual pattern of the evidence and a series of imponderables, and they have continued to be asked.
What is without question is that one hour after the attack in New York, former Israeli Prime Minister Ehud Barak had identified the likely perpetrator as Osama Bin Laden (Bin Laden would later deny any involvement) and called for the declaration of a global ‘war against terror’ extending beyond the perpetrators of 9/11 itself to confront terror generally.
The paradigm was adopted wholesale by George Bush in a speech to Congress nine days later. ’Our war on terror begins with Al Qaeda,’ Bush said, ‘but it does not end there. It will not end until every terrorist group of global reach has been found, stopped and defeated.’
Islam itself was not the enemy, we were told. Al Qaeda had only ‘hijacked’ Islam for the purpose of ‘remaking the world and imposing its radical beliefs on people everywhere’.
In subsequent years this vague and ambiguous distinction would be used to support the extension of police state surveillance not just of rapidly growing Muslim populations across the West (to monitor evidence of dangerous radicalization) but also anyone articulating suspicion towards Muslims. By 2019 more ‘Right-wingers’ than Islamic activists were being referred to the Prevent programme. Last month the Department of Homeland Security issued a bulletin implying that if Americans question and challenge the COVID shot mandates, they are now considered potential ‘Domestic Violent Extremists’.
In truth, Bush and his associates and masters had hijacked Al-Qaeda and Islam for the purpose of imposing their own radical agenda. Spun between a belligerent discourse of Islamofascism and a police discourse of Islamophobia, a schizoid and insulting fantasy of a liberal Islam became the object of a new imperialism in the stated cause of Western values, and in reality enacting their destruction.
Just as recent calls to ‘Save the NHS’ have served to camouflage the liquidation of the NHS, the rhetoric of ‘nation-building’ efforts to extend Western democracy across the world have, in reality, destroyed democracy everywhere.
Even as mass Muslim immigration into the West accelerated following their destruction of their countries, a steady drumbeat of slaughter and atrocity in London, Madrid, Paris and elsewhere, staged by actors invariably known to intelligence agencies, maintained a climate of hostility and madness to the benefit of the occupational elites. The language of permanent terror bled into a culture (what is a safe space but a refuge from a world of terror?) as a psychologically brutalized population regressed into a cloying “thoughts and prayers” martyrology, in fact promoted or exploded into murderous psychosis, combining in cases like Usman Khan, who shortly before his London Bridge rampage attended a conference on criminal rehabilitation as a rehabilitated criminal. https://www.conservativewoman.co.uk/the-indoctrination-of-the-justice-system/ (The Millwall supporter who helped to disarm him, Roy Larner, was later added to terror watchlist.)
In February 2007, when former US national security adviser Zbigniew Brzezinski denounced before the Senate ‘a historical, strategic and moral calamity . . . driven by Manichaean impulses and imperial hubris’, the full extent of the damage was not yet clear. What now is clear is that the War on Terror was a weapon directed against the West itself which has succeeded beyond all expectations.
Whether through a conscious plan or what Hegel called the cunning of reason, the West has been destroyed. What now exists is a shadow West, which still speaks as if it was the West for camouflage, but in the service of completely different goals. It is not a coincidence that the characters promoted and rewarded for their participation in the War on Terror have either remained in place or returned to play a role in the pandemic: from their perspective there has been no error. What has materialised over the last thirty years, and especially the last eighteen months, is a new system of power, which although still defined within the context of the history of the nation-state, represents its ultimate destruction.
On social media, a Sydney doctor questioned whether vaccines and lockdowns would be effective in ending the pandemic while also scrutinizing how medical authorities were handling treatment. As a result of his postings, New South Wales medical authorities have taken action against Dr. Paul Oosterhuis by suspending him.
Oosterhuis’ social media activities have garnered at least two anonymous complaints to the medical council, the group confirmed on September 2nd.
“Over the last 18 months, I have been increasingly concerned about the misinformation and censorship creeping into science and medicine,” the doctor had stated.
Oosterhuis recommended that medical authorities advise COVID-19 patients to take vitamin D and zinc and to treat them with ivermectin and hydroxychloroquine.
He called the lockdowns “totalitarian” and causing “massive damage to society-wide.”
In a post, he wrote. “The risk of antibody-dependent enhancement of disease… driven by immune escape from the selective evolutionary pressure of vaccinating with a non-sterilizing agent is a real and present danger and needs to be discussed. The danger to millions is distressing me, and discussing that danger is, I believe, unarguably in the public interest.”
According to the Medical Council of New South Wales, Oosterhuis’s social media activity was flagged. He was asked to attend an “immediate action panel” on September 3rd and the anesthetist was questioned by the MCNSW.
“The Council deals with individual doctors whose conduct, performance or health may represent a risk to the public and works with them, where possible, to reduce that risk by for example, placing conditions on their medical registration. Section 150 or immediate action panels are held by the Council when a complaint or notification prompts serious concerns about risk to public safety or the need to otherwise act in the public interest. Panel members include community representatives as well as medical practitioners,” the MCNSW statement read.
The MCNSW provided Reclaim The Net with this full statement here
Ultimately, the MCNSW chose to suspend Dr Oosterhuis’ later that day.
Medical practitioners can be suspended by the medical council under New South Wales’ Health Practitioner Regulation National Law (NSW). The New South Wales Medical Council collaborates with the state Ministry of Health to investigate and resolve complaints about specific doctors and other medical specialists.
According to the council, this law does not give it the power to de-register Oosterhuis or revoke his license and they have no authority to punish him. However, despite his almost 30 years of experience in medicine, his suspension has already barred him from practicing in the medical profession.
Oosterhuis has responded by stating that he will not adjust his behavior to be more compliant. He stated that he intends to challenge the suspension, saying:
“I am very disappointed by the Medical Council’s decision to suspend my registration.
“The material I submitted in support of my evidence-based concerns was not considered. I intend to appeal the decision.
“The council drew upon s150 powers to demand an urgent hearing into some posts I have shared on Facebook on the importance of early treatment, particularly the low hanging fruit of vit D, Zinc, Quercetin, vit C and the repurposed drugs Ivermectin.
“I’m pro choice, pro informed consent… it’s always been a key ethical principle… you need to be able to discuss all the risks, benefits, and alternatives of any medical intervention.”
He later added, “Censorship kills. My responsibility to the Hippocratic oath, and basic ethics compels me to share data that I believe is definitely in the public interest.”
Despite an initial public statement, the MCNSW failed to make any further statements on this issue.
Much attention is focused on President Joe Biden in a Thursday speech announcing that the coronavirus testing alternative United States government employees had been able to use to avoid the mandate to take experimental coronavirus vaccines is being eliminated and that regulations are in the works to require all employees at companies with 100 or more employees to take the “vaccines” or be tested weekly. Less noticed is news that experimental coronavirus vaccines may soon be rolled out for young children. Pfizer-BioNTech is seeking in the next few weeks approval for giving its experimental coronavirus vaccine shots to children ages five through 11, while Moderna is close behind, proceeding with testing of its shots on children 11 and younger. Then come shots for toddlers and babies.
Shots mandates for workers first, shots mandates for children next: That seems to be the situation in America, though it should be noted that some children —especially older children — are workers too.
Of course, as happened Thursday with the testing alternative to shots disappearing for government workers, expect that alternative to go away for people working at private businesses as well. By the time a shots mandate for children comes along, a testing alternative might not be available from the start.
Biden provided in his speech a preview of an argument in favor of mandatory shots for children. First, he asserted that the August 23 expedited Food and Drug Administration (FDA) approval of a Pfizer-BioNTech experimental coronavirus vaccine for people 16 and over means “the time for waiting is over” for people 16 and older who have not taken the shots. Second, Biden suggested that as soon as vaccines are approved for use in an age group of children his conclusion is that the children in that age group should then be given shots:
It comes down to two separate categories: children ages 12 and older who are eligible for a vaccine now, and children ages 11 and under who are not are yet eligible.
The safest thing for your child 12 and older is to get them vaccinated. They get vaccinated for a lot of things. That’s it. Get them vaccinated.
A move to require children to be given the experimental coronavirus vaccine shots should come as no surprise. Children across America have long been mandated to receive many vaccines on a prescribed timeline in accord with the Centers for Disease Control and Prevention (CDC) vaccine schedule or similar state vaccine schedules in order to attend school. And many of the mandates are difficult to avoid. In California, for example, the vaccine mandate applies even to children in private schools and only has a very limited exemption.
The obvious way to introduce the requirement that young children take the experimental coronavirus vaccine shots is to make the shots a prerequisite for attending school. There is plenty of precedent for that from all the other vaccine shots required in the CDC and state vaccine schedules.
Next up, the shots can be required for even homeschooled children, just like the shots requirement for people employed in businesses with a 100 or more employees can be extended to people employed in businesses with under 100 employees, the self-employed, the retired, and the unemployed. Indeed, on Thursday Biden announced he will mandate US government contractors and 17 million healthcare workers take the shots, no matter how many employees their employers have.
There is no constitutional basis for the experimental coronavirus vaccine mandates Biden announced on Thursday. If he can get away with those mandates, what’s to stop him from expanding on those mandates so he can eliminate all the “loopholes,” including the one protecting children from forced shots.
A Florida appeals court has overruled a district judge who sought to block Governor Ron DeSantis from banning mask mandates in public schools, even as President Joe Biden vowed federal support for administrators who do so.
On Friday, the First District Court of Appeals in Tallahassee overruled Leon County Judge John Cooper’s decision to block the enforcement of the mandate ban, meaning schools that try to force children to wear masks can be punished by the governor.
“Upon our review of the trial’s court’s final judgment and the operative pleadings, we have serious doubts about standing, jurisdiction, and other threshold matters,” said the appeals court order, casting doubt on the case the mandate advocates made through a group of parents.
DeSantis is a Republican governor opposed to lockdowns and mask mandates, who has opted for encouraging vaccinations and antibody treatments for Covid-19 instead. He has argued that masking up ought to be voluntary, and that school mask mandates violate the rights of parents and children. Under the rules enacted by DeSantis last month, school administrators who impose mask mandates can be docked pay. Judge Cooper tried to block their enforcement.
Of the 67 school districts in Florida, 13 have adopted strict mask mandates in violation of the state order. So far, DeSantis has withheld the monthly salary of school board members in two counties, Broward and Alachua, while investigating others for non-compliance.
On Thursday, Biden said the federal government would reimburse anyone who defies the mask mandate ban, as part of his push to force some 80 million Americans to get vaccinated or submit to weekly tests under the threat of losing their jobs or paying massive fines. Biden blamed the “unvaccinated” for the surge in Covid-19 cases and said the vaccinated must be protected from them.
“This is not about freedom, or personal choice,” Biden said in a televised speech, later adding, “We’ve been patient, but our patience is wearing thin, and your refusal has cost all of us.”
Biden also said state governors should require vaccinations of all school teachers and staff, imposed a vaccination requirement on 300,000 teachers in the federal Head Start program, and vowed to go after any governors “undermining” his measures.
“If these governors won’t help, I will use my powers as president and get them out of the way,” he said.
Last month, DeSantis vowed to “stand in the way” of Covid-19 mandates, lockdowns, and other restrictions, saying the US can “either have a free society or we can have a biomedical security state.”
… Groupthink was extensively studied by Yale psychologist Irving L. Janis and described in his 1982 book Groupthink: Psychological Studies of Policy Decisions and Fiascoes.
Janis was curious about how teams of highly intelligent and motivated people—the “best and the brightest” as David Halberstam called them in his 1972 book of the same name—could have come up with political policy disasters like the Vietnam War, Watergate, Pearl Harbor and the Bay of Pigs. Similarly, in 2008 and 2009, we saw the best and brightest in the world’s financial sphere crash thanks to some incredibly stupid decisions, such as allowing sub-prime mortgages to people on the verge of bankruptcy.
In other words, Janis studied why and how groups of highly intelligent professional bureaucrats and, yes, even scientists, screw up, sometimes disastrously and almost always unnecessarily. The reason, Janis believed, was “groupthink.” He quotes Nietzsche’s observation that “madness is the exception in individuals but the rule in groups,” and notes that groupthink occurs when “subtle constraints … prevent a [group] member from fully exercising his critical powers and from openly expressing doubts when most others in the group appear to have reached a consensus.”[2]
Janis found that even if the group leader expresses an openness to new ideas, group members value consensus more than critical thinking; groups are thus led astray by excessive “concurrence-seeking behavior.”[3] Therefore, Janis wrote, groupthink is “a model of thinking that people engage in when they are deeply involved in a cohesive in-group, when the members’ strivings for unanimity override their motivation to realistically appraise alternative courses of action.”[4]
The groupthink syndrome
The result is what Janis calls “the groupthink syndrome.” This consists of three main categories of symptoms:
1. Overestimate of the group’s power and morality, including “an unquestioned belief in the group’s inherent morality, inclining the members to ignore the ethical or moral consequences of their actions.” [emphasis added]
2. Closed-mindedness, including a refusal to consider alternative explanations and stereotyped negative views of those who aren’t part of the group’s consensus. The group takes on a “win-lose fighting stance” toward alternative views.[5]
3. Pressure toward uniformity, including “a shared illusion of unanimity concerning judgments conforming to the majority view”; “direct pressure on any member who expresses strong arguments against any of the group’s stereotypes”; and “the emergence of self-appointed mind-guards … who protect the group from adverse information that might shatter their shared complacency about the effectiveness and morality of their decisions.”[6]
It’s obvious that alarmist climate science—as explicitly and extensively revealed in the Climatic Research Unit’s “Climategate” emails—shares all of these defects of groupthink, including a huge emphasis on maintaining consensus, a sense that because they are saving the world, alarmist climate scientists are beyond the normal moral constraints of scientific honesty (“overestimation of the group’s power and morality”), and vilification of those (“deniers”) who don’t share the consensus. … Read full article
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.