In September 2020 I put together a 500 page book containing the transcripts of the ‘Old Man in a Chair’ videos I had made for YouTube – plus the articles I wrote in that period.
I wanted a paperback version of this book so that those who want to help spread the truth can share copies with those who might be influenced by the facts. It is important to understand – and remember – how this fraud unfolded. Only by remembering and understanding the past can we really understand the extent of the evil that has unfolded.
The book starts with material broadcast on April 28th 2020 (when my earlier book Coming Apocalypse had finished) and continues until September 2020.
The content is as startling and as accurate today as it was when I originally tried to publish it. It provides a blow by blow account and an analysis of how the hoax unfolded.
I tried to publish this book three times and three times it was quickly banned because the information it contained was considered too dangerous.
YouTube removed all the videos and eventually banned me. (I am now banned from accessing YouTube as well as having a YouTube channel.)
For two years, the only place the book was available as a paperback was Japan where the book is available as five volumes. I’m delighted that a publisher has agreed to publish an English language paperback and an eBook. The publisher is not based in the UK or the US.
Throughout the months to which these essays relate, the laws being brought in around the world were changing almost daily. The only consistent factors were the ever-growing power of the World Health Organisation and Bill Gates, and a complete lack of official interest in the science and the truth.
It was in that period that I devised my specially written triptych – designed according to the psy-op principles used on the British people – ‘Distrust the Government: Avoid Mass Media: Fight the Lies.’
I warned about the damage that would be done by the lockdowns (pointing out that they would kill far more people than covid-19, the demonization of cash (and its replacement with digital money) and the explosion in the number of Do Not Resuscitate notices being issued on the elderly and the infirm. I warned about tests being used to collect DNA. I warned about the way that our world was being changed to prepare us for the Great Reset.
Worried by the safety and effectiveness of the promised vaccine, I tried, unsuccessfully, to make a £100,000 bet with Dr Fauci (in the US) and Dr Whitty (in the UK) about the safety and effectiveness of the vaccine.
If you would like a copy please go to: www.korsgaardpublishing.com and press the button marked ‘Our Books’. You’ll then see Covid-19: The Greatest Hoax in History.
Australians can probably still get a Pfizer vaccine in chemists and carparks across Australia, but they still need to fly to Iran to get an Australian-made vaccine. The good news is that at least this week it’s legal for Australians to finally fly to Tehran without taking Pfizer or Moderna shot first — as long as they don’t fly on an Australian airline. (Not mentioning any names, Qantas!)
The people mostly responsible for this situation are the TGA (Therapeutic Goods Association). They’re supposed to be looking after Australians health but somehow all their decisions happen to be exactly what a Pfizer CEO would want. Spooky eh? The TGA rushed the approval for the Pfizer vaccines, but still, millions of doses later, won’t release the procurement contracts, even under FOI. Signed on our behalf, and for our own good, yes? Did they even read the documents that Pfizer AND the FDA tried to hide for 75 years?
Now meet Professor Nikolai Petrovsky from Flinders University, Australia, who had already developed protein based vaccines against the original SARS in 2003 and MERS in 2012, so he was the obvious choice to develop an old fashioned protein based vaccine in Australia. (Hey, but it’s not like we want to develop our own vaccine industry, eh?).
So he went on to make a protein vaccine against SARS-2 and has got approval to use it in Iran. Last I heard (months ago) they had sold 6 million doses to Iran, apparently with great results.
With all the makings of a Great Banana Republic Australia promptly sacked Petrovsky for taking his own vaccine instead of one of the foreign ones approved by The Sacred T.G.A committee. We can’t have vaccine experts at uni picking their own vaccines can we?
Somehow the Australian government spent something like $6 billion on foreign vaccines but asked the small Australian company to pay $300,000 to get approved here. So Petrovsky ran a GoFundMe, and it was so popular it raised a million dollars. Finally he has permission and funding to run Australian trials, but now he doesn’t have permission to talk about it. Who knew he needed that? Apparently the TGA says it will fine him $13,000 or maybe one million (convenient, eh?) if he does. (Updated: I hear it’s an $11m threat now).
If only Australians were smart enough to hear the words of Professors without “protection” by unaccountable committees?
Unfortunately, Australians can’t take the Australian vaccine in Australia, and if they fly to Iran to get it, they still can’t return to their jobs in Victoria or WA. Who voted for the TGA? This committee controls what every doctor and medical professor can say in Australia. But doctors don’t even vote for them.
For those who are interested — Petrovsky’s “Spikogen” vax has no RNA or DNA — just protein, and there’s no Furin cleavage site, or TMP (Trans Membrane Protein) either. Those are two parts of the spike that might make it less likely to get into our cells, or to stick in the cell-membrane of our cells and poke out. (When our cells have those viral spikes displayed they will attract the attention of wayward immune cells and thus increase the risk of myocarditis and other autoimmune reactions). As to how well it works, we hear there are very few side effects. I’ve seen no data yet. If only the Australian Government was trying to help Australian researchers?
The Ministry of Medical-Truth are the same agency that also banned all doctors in Australia from prescribing ivermectin for Covid, because it might reduce the sales of Pfizer, I mean — because “people might not get vaccinated”. They actually said that. They also said they banned doctors from using it because some people who weren’t doctors on social media were getting the doses wrong. Like that makes sense. And apparently we were running out of one of the most common drugs on the planet, and still are, because no one in government thought to order any more from Indiamart?
Just in case you wonder who your rulers are Australians
“The Committee is established under Regulation 39F of the Therapeutic Goods Regulations 1990 and the members are appointed by the Minister for Health.” The ACV was established in January 2017…
But make no mistake, the man responsible for the TGA (at least for a few more weeks) is Greg Hunt, Minister of Health. Once upon a time he was Director of Strategy at the World Economic Forum (2000–2001). Curious.
The TGA is a disgrace. It’s time to shut it down.
If it were completely captured by Big Pharma, which decisions would it have made differently?
Being slow to approve competing drugs might be exactly what it was set up to do?
It has been two weeks since a United States district court struck down President Joe Biden’s mandate, imposed through the Centers for Disease Control and Prevention (CDC), that people wear masks when traveling via public transportation, or by taxi or ride-share service, as well as when at related locations, such as airports. After the court decision, most transportation companies and locations have been quick to make clear that people are free to leave their faces uncovered. Many people have been very happy to do just that.
The CDC, however, has not given up on hectoring people to “wear your mask.” On Tuesday, the CDC released a “media statement” titled “CDC Recommendation for Masks and Travel.” Starting off, the media statement declares that the CDC “recommends that everyone aged 2 and older – including passengers and workers – properly wear a well-fitting mask or respirator over the nose and mouth in indoor areas of public transportation (such as airplanes, trains, etc.) and transportation hubs (such as airports, stations, etc.).” Further, the CDC states that it encourages “operators of public transportation and transportation hubs to support mask wearing by all people, including employees.”
Fortunately, the response of many individuals and businesses to this advice ranges from “whatever” to “leave me alone.” More and more people have gotten over inflated fear of coronavirus that never posed a threat of major sickness or death to most people. People have also progressively become aware of the absurdity and destructiveness of forced business closures, “social distancing,” ubiquitous coronavirus testing, experimental coronavirus “vaccines,” mask mandates, and other pseudoscience actions the CDC has pushed since 2020.
America is largely back to the good old days of most people ignoring for the most part when government “public health officials” and people in the media relate CDC guidance that people do this or that. Plus, given the horrid track record of the CDC through the coronavirus scare, more people are now aware of the charade of CDC guidance than ever before. Instead of just ignoring CDC recommendations, many more people than before will feel the urge to research the recommendations and publicly challenge the recommendations when they are found wanting. There should now hopefully also be much more steadfast resistance from the start to any new effort to morph recommendations from the CDC or other so-called health experts into mandates.
Still, the CDC’s media statement this week and the US government hanging on to other coronavirus crackdown measures, including coronavirus shots and testing mandates, to the extent the measures have not been struck down by courts, show that the threat of grand scale tyranny in the name of countering a new purported health crisis remains. In addition, some state and local governments are both holding on to the remnants of coronavirus tyranny and remaining ready to jump back into much more expansive action suppressing freedom in the name of public health.
People must remain vigilant. People must spread the message that the lesson from the coronavirus crackdown is that government violations of individual rights in the name of advancing public health objectives or countering the new disease of the day must be resisted resolutely and vociferously.
People should also keep in mind that, in a variety of circumstances, doctors and other people working the medical field may provide advice that is grounded in the CDC’s priorities and runs counter to the best medical course.
The lure of evil remains strong. To ensure that respect for freedom regained from the coronavirus crackdown tyrants does not fade away, people must remain on guard against and adamantly refuse to accept new encroachment efforts. To keep what has been regained of the good old days, and even expand upon it, people must take action, starting with saying “no” to the health authoritarians at the CDC and elsewhere.
The question is, do they really tell us anything we don’t already know?
The big revelation doing the rounds at the minute is that the vaccines were never trialled with, and were specifically not recommended for, pregnant women.
But is this new information?
When governments started “recommending” the Covid vaccine to pregnant women in the Summer of 2021, everybody who had been paying attention knew that position was not backed up by any data at all.
In a way, the “not recommended for pregnant women” disclosure is actually good for Pfizer.
Behind a facade of being legally mandated to publish these files, it’s now become public knowledge that Pfizer (allegedly) told people not to give the vaccine to pregnant women, but many countries did it anyway.
This shifts the blame (and potential legal liability) away from Pfizer and onto the governments in question.
A good example of how “forced disclosure” can be used to reinforce and direct a narrative, through a pretence of reluctance.
Going further, shouldn’t we be asking: Can we trust anything in these documents at all?
Just because Pfizer has been (apparently) legally “forced” to release them doesn’t mean they are important, relevant or even real. Who’s verifying the documents? Who’s auditing Pfizer to make sure they release everything? The US government? Some other government or agency?
Do you trust them?
The real damning documents – if such ever existed – have likely been shredded, burned and buried in 20 feet of concrete by now…and that doesn’t matter, because we already know everything we will ever need to know about these Covid “vaccines”:
They were not subject to proper long-term testing.
Professor Harald Matthes of Berlin’s Charite University Hospital said on Tuesday that he has recorded 40 times more“serious side effects” from Covid-19 vaccinations than official German sources have. As Matthes called on doctors to speak up for those allegedly injured, US pharma giant Pfizer released a tranche of data apparently showing its jab was far less effective than claimed.
Matthes has been conducting a study entitled ‘Safety Profile of Covid-19 Vaccines’ for a year, and after surveying 40,000 vaccinated people, he has noticed that one in every 125 have struggled with “serious side effects,” Germany’s MDR television network reported on Tuesday.
“The number is not surprising,” Matthes explained. “It corresponds to what is known from other countries such as Sweden, Israel or Canada. Incidentally, even the manufacturers of the vaccines have already determined similar values in their studies.”
However, Matthes claimed that this risk profile is 40 times higher than that noted by the Paul Ehrlich Institute (PEI), the health ministry agency in charge of the country’s vaccine rollout. The PEI currently states that serious reactions occur in just 0.2 out of every 1,000 vaccine doses administered.
Some of the effects Matthes’ team have recorded include muscle and joint pain, heart inflammation, dysfunction of the immune system and neurological disorders. With 179 million vaccine doses administered in Germany thus far, Matthes claimed that there could be as many as “half a million cases with serious side effects.”
The researcher, whose hospital is regarded as the best in Germany and has treated former Chancellor Angela Merkel, said that doctors need to take action and discuss the prevalence of such side effects “openly at congresses and in public without being considered anti-vaccination.”
In the US on Tuesday, the Food and Drug Administration (FDA) released 90,000 pages of documents from vaccine manufacturer Pfizer relating to the safety and efficacy of its Covid-19 shot. Preliminary analysis of the document dump suggests that during the pharma giant’s own studies, 1,223 people out of 29,914 suffering adverse events died following vaccination, and that the jab reduced the absolute risk of dying from Covid-19 by less than one percent, a point that has already been highlighted by research published in The Lancet medical journal.
Suppose an individual is infected with a novel pathogen, and then sometime later is infected with a related version of the same pathogen. If ‘original antigenic sin’ is present, the individual’s immune system will respond to the antigens carried by the original version of the pathogen, resulting in weaker immunity.
The idea is that, for certain classes of pathogen, the immune system’s response to any particular exposure depends on an individual’s first exposure. If two versions of a pathogen, A and B, are circulating in a population, individuals who were first exposed to A may develop weaker immunity against B, and vice versa.
There is substantial evidence that original antigenic sin applies to influenza: those who gain immunity to one strain of influenza may develop weaker immunity to other strains.
It can also apply to vaccines. As a recent review notes, “if we only immunise to a single strain or epitope, and if that strain/epitope changes over time, then the immune system is unable to mount an accurate secondary response.”
At the end of last year, ‘mainstream’ commentators began discussing the possibility that original antigenic sin applies to the Covid vaccines. If it does, we may have vaccinated millions of young people against a version of Covid that poses little risk to them, at the cost of weakening their immunity to subsequent variants.
Now ‘original antigenic sin’ has been mentioned in the context of Covid vaccines in the pages of the New England Journal of Medicine – the world’s most ‘prestigious’ medical journal.
Noting that boosters are “not risk-free”, the American immunologist Paul Offit writes: “all age groups are at risk for the theoretical problem of an ‘original antigenic sin’ – a decreased ability to respond to a new immunogen because the immune system has locked onto the original immunogen.”
He cites a recent preprint by Matthew Gagne and colleagues, who carried out an experiment on nonhuman primates. They began by giving two groups of primates the Moderna vaccine. After 41 weeks, they gave each group a booster shot. One group received the Moderna vaccine again, while the other group received an Omicron-specific booster.
Finally, both groups were exposed to Covid. The researchers measured memory B cells and found that the Omicron-specific booster “provided no advantage” over the original Moderna vaccine. Indeed, they “did not observe a population of Omicron-only memory B cells before or after the boost that was clearly distinct from background staining”.
This means the Omicron-specific booster did not produce any detectable Omicron-only memory B cells at all, though it did trigger the production of more memory B cells specific to the original SARS-CoV-2 strain. It’s important to note, however, that both boosters did increase memory B cells (and neutralising antibodies) to some extent. (Neither was totally ineffective.)
As Gagne and colleagues note, the fact that memory B cells were no higher in the group that received the Omicron-specific booster “likely stems from the principle of original antigenic sin”. How serious this problem turns out to be will depend on several factors, not least subsequent viral evolution.
Offit writes in the NEJM that it “could limit our ability to respond to a new variant”.
The struggle with weight gain and obesity is a common and costly health issue, leading to an increase in risk for heart disease, Type 2 diabetes and cancer, just to name a few.
According to CDC figures for 2017-18, 19.3% of American children1 and 42.4% of adults2 are now obese, not just overweight. That’s a significant increase over the 1999/2000 rates, when just under 16% of children ages 6 to 193 and 30.5% of adults were obese.
Research has linked growing waistlines to a number of different sources, including processed foods, sodas and high-carbohydrate diets. Risks associated with belly fat in aging adults includes an elevated risk of cardiovascular disease and cancer.4
Researchers have actually predicted obesity will overtake smoking as a leading cause of cancer deaths,5 and recent statistics suggest we’re well on our way to seeing that prediction come true as obesity among our youth is triggering a steep rise in obesity-related cancers at ever-younger ages.
Millennials More Prone to Obesity-Related Cancers
As obesity rates rise, so do related health problems, including cancer. According to a report6 published in 2014 on the global cancer burden, obesity is already responsible for an estimated 500,000 cancer cases worldwide each year, and that number is likely to rise further in coming decades.
As reported in a Lancet study7 by the American Cancer Society, rates of obesity-related cancers are rising at a far steeper rate among millennials than among baby boomers. According to the authors,8 this is the first study to systematically examine obesity-related cancer trends among young Americans.
What’s more, while six of 12 obesity-related cancers (endometrial, gallbladder, kidney, multiple myeloma and pancreatic cancer) are on the rise, only two of 18 cancers unrelated to obesity are increasing. As noted in the press release:9
“The obesity epidemic over the past 40 years has led to younger generations experiencing an earlier and longer lasting exposure to excess adiposity over their lifetime than previous generations.
Excess body weight is a known carcinogen, associated with more than a dozen cancers and suspected in several more … Investigators led by Hyuna Sung, Ph.D., analyzed 20 years of incidence data (1995-2014) for 30 cancers … covering 67 percent of the population of the U.S. …
Incidence increased for 6 of the 12 obesity-related cancers … in young adults and in successively younger birth cohorts in a stepwise manner. For example, the risk of colorectal, uterine corpus [endometrial], pancreas and gallbladder cancers in millennials is about double the rate baby boomers had at the same age …
‘Although the absolute risk of these cancers is small in younger adults, these findings have important public health implications,’ said Ahmedin Jemal, D.V.M., Ph.D., scientific vice president of surveillance [and] health services research and senior/corresponding author of the paper.
‘Given the large increase in the prevalence of overweight and obesity among young people and increasing risks of obesity-related cancers in contemporary birth cohorts, the future burden of these cancers could worsen as younger cohorts age, potentially halting or reversing the progress achieved in reducing cancer mortality over the past several decades.
Cancer trends in young adults often serve as a sentinel for the future disease burden in older adults, among whom most cancer occurs.'”
Changes in Diet Are Driving the Obesity Epidemic
Studies10,11,12 have repeatedly demonstrated that when people switch from a traditional whole food diet to processed foods (which are high in refined flour, processed sugar and harmful vegetable oils), disease inevitably follows.
Below are just a few telling statistics. For more, see nutrition researcher Kris Gunnars’ 11 graphs published in Business Insider showing “what’s wrong with the modern diet.”13
Over the past 200 years, our sugar intake has risen from 2 pounds to 152 pounds per year.14 While Americans are advised to get only 10% of their calories from sugar,15 equating to about 13 teaspoons a day for a 2,000-calorie diet, the average intake is 42.5 teaspoons per day.16 It’s important to realize that it’s nearly impossible to achieve that on a processed food diet.
Not only that, you can’t exercise off the excess calories. For example, to burn off the calories in a single 12-ounce soda, you’d have to walk briskly for 35 minutes. To burn off a piece of apple pie, you’d be looking at a 75-minute walk.17
Soda and fruit juice consumption is particularly harmful, studies18,19 show, raising a child’s risk of obesity by 60% per daily serving.20 Research has also shown refined high-carb diets in general are as risky as smoking, increasing your risk for lung cancer by as much as 49%.21
Between 1970 and 2009, daily calorie intake rose by an average of 425 calories, a 20% increase, according to Stephan Guyenet, Ph.D.,22 who studies the neuroscience of obesity. This rise is largely driven by increased sugar and processed food consumption, and the routine advertising of junk food to children.23
To attract customers and compete with other restaurants, companies often add salt, sugar, fat and flavor chemicals to trigger your appetite. Unfortunately, it turns out additives and chemicals supplemented in processing kill off beneficial gut bacteria, which further exacerbates the problems created by a processed food diet.24
According to epidemiology professor Tim Spector, even eating a relatively small number of highly processed ingredients is toxic to your gut microbiome, which start to die off just days after eating a fast food heavy diet, suggesting excess calories from fast food may not be the only factor to blame for rising weight.
Processed vegetable oils, which are high in damaged omega-6 fats, are another important factor in chronic ill health. Aside from sugar, vegetable oils are a staple in processed foods, which is yet another reason why processed food diets are associated with higher rates of heart disease and other diseases.
Soybean oil, which is the most commonly consumed fat in the U.S.,25 has also been sh
“Ultraprocessed diets cause excess calorie intake and weight gain,” research26 concludes, showing that when people are allowed to eat as much as they want of either ultraprocessed foods or unprocessed food, their energy intake is far greater when eating processed fare.
In just two weeks, participants gained between 0.3 and 0.8 kilos (0.166 and 1.76 pounds) on the ultraprocessed diet, and lost 0.3 to 1.1 kilos (0.66 to 2.42 pounds) when eating unprocessed food.
As These Foods Became the Norm, so Did Chronic Illness
Unfortunately, Americans not only eat a preponderance of processed food, but 60% of it is ultraprocessed27 — products at the far end of the “significantly altered” spectrum, or what you could typically purchase at a gas station.
The developed world in general eats significant amounts of processed food, and disease statistics reveal the inherent folly of this trend. There’s really no doubt that decreasing your sugar consumption is at the top of the list if you’re overweight, insulin resistant, or struggle with any chronic disease.
It’s been estimated that as much as 40% of American health care expenditures are for diseases directly related to the overconsumption of sugar.28 In the U.S., more than $1 trillion is spent on treating sugar and junk food-related diseases each year.29
Any foods that aren’t whole foods directly from the vine, ground, bush or tree are considered processed. Depending on the amount of change the food undergoes, processing may be minimal or significant. For instance, frozen fruit is usually minimally processed, while pizza, soda, chips and microwave meals are ultraprocessed foods.
The difference in the amount of sugar between foods that are ultraprocessed and minimally processed is dramatic. Research30 has demonstrated that over 21% of calories in ultraprocessed foods comes from sugar, while unprocessed foods contain no refined or added sugar.
In a cross-sectional study31 using data from the National Health and Nutrition Examination Survey of over 9,000 participants, researchers concluded that “decreasing the consumption of ultraprocessed foods could be an effective way of reducing the excessive intake of added sugars in the USA.”
Definition of Ultraprocessed Food
As a general rule, ultraprocessed foods can be defined as food products containing one or more of the following:
Ingredients that are not traditionally used in cooking.
Unnaturally high amounts of sugar, salt, processed industrial oils and unhealthy fats.
Artificial flavors, colors, sweeteners and other additives that imitate sensorial qualities of unprocessed or minimally processed foods (examples include additives that create textures and pleasing mouth-feel).
Processing aids such as carbonating, firming, bulking, antibulking, defoaming, anticaking, glazing agents, emulsifiers, sequestrants and humectants.
Preservatives and chemicals that impart an unnaturally long shelf-life.
Genetically engineered ingredients, which in addition to carrying potential health risks also tend to be heavily contaminated with toxic herbicides such as glyphosate, 2,4-D and dicamba.
As described in the NOVA classification of food processing,32 “A multitude of sequences of processes is used to combine the usually many ingredients and to create the final product (hence ‘ultraprocessed’).” Examples include hydrogenation, hydrolysation, extrusion, molding and preprocessing for frying.
Ultraprocessed foods also tend to be far more addictive than other foods, thanks to high amounts of sugar (a substance shown to be more addictive than cocaine33), salt and fat. The processed food industry has also developed “craveabilty” into an art form. Nothing is left to chance, and by making their foods addictive, manufacturers ensure repeat sales.
Processed Food Diet Linked to Early Death
In related news, recent research34 involving more than 44,000 people followed for seven years warns that ultraprocessed foods raise your risk of early death. The French team looked at how much of each person’s diet was made up of ultraprocessed foods, and found that for each 10% increase in the amount of ultraprocessed food consumed, the risk of death rose by 14%.
This link remained even after taking confounding factors such as smoking, obesity and low educational background into account. As you’d expect, the primary factors driving the increased death rate was chronic diseases such as heart disease and cancer.
Nita Forouhi, a professor at the MRC Epidemiology Unit at the University of Cambridge, who was not part of the study, told The Guardian :35
“The case against highly processed foods is mounting up, with this study adding importantly to a growing body of evidence on the health harms of ultraprocessed foods … [W]e would ignore these findings at public health’s peril.
A vital takeaway message is that consumption of highly processed foods reflects social inequalities — they are consumed disproportionately more by individuals with lower incomes or education levels, or those living alone.
Such foods are attractive because they tend to be cheaper, are highly palatable due to high sugar, salt and saturated fat content, are widely available, highly marketed, ready to eat, and their use-by dates are lengthy, so they last longer. More needs to be done to address these inequalities.”
Ultraprocessed Foods Linked to Cancer
Another French study36,37 published last year also found that those who eat more ultraprocessed food have higher rates of obesity, heart problems, diabetes and cancer. Nearly 105,000 study participants, a majority of whom were middle-aged women, were followed for an average of five years.
On average, 18% of their diet was ultraprocessed, and the results showed that each 10% increase in ultraprocessed food raised the cancer rate by 12%, which worked out to nine additional cancer cases per 10,000 people per year.
The risk of breast cancer specifically went up by 11% for every 10% increase in ultraprocessed food. Sugary drinks, fatty foods and sauces were most strongly associated with cancer in general, while sugary foods had the strongest correlation to breast cancer.
According to the authors, “These results suggest that the rapidly increasing consumption of ultraprocessed foods may drive an increasing burden of cancer in the next decades.” Study co-author Mathilde Touvier told CNN:38
“It was quite surprising, the strength of the results. They were really strongly associated, and we did many sensitive analysis and adjusted the findings for many cofactors, and still, the results here were quite concerning.”
Diet Is a Key Factor Determining Your Health and Longevity
Research39 published in 2017 linked poor diet to an increased risk of cardiometabolic mortality (death resulting from Type 2 diabetes, heart disease and stroke).
According to the authors, suboptimal intake of key foods such as fruits, vegetables, nuts and seeds, and animal-based omega-3, along with excessive consumption of processed foods such as meats and sugar-sweetened beverages accounted for more than 45% of all cardiometabolic deaths in 2012. In other words, the more processed foods you eat, and the less whole foods you consume, the greater your risk of chronic disease and death.
Other research published that same year found that eating fried potatoes (such as french fries, hash browns and potato chips) two or more times per week may double your risk of death from all causes.40 Eating potatoes that were not fried was not linked to an increase in mortality risk, suggesting frying — and most likely the choice of oil — is the main problem.
In a 2013 presentation41 at the European Ministerial Conference on Nutrition and Noncommunicable Diseases by Dr. Carlos Monteiro,42 professor of nutrition and public health at the University of Sao Paulo, Brazil, Monteiro stresses the importance of creating “policies aiming the reformulation of processed foods,” and limiting children’s exposure to junk food marketing, in order to tackle the rise in diet-related noncommunicable diseases.
In my view, eating a diet consisting of 90% real food and only 10% or less processed foods is an achievable goal for most that could make a significant difference in your weight and overall health. You simply need to make the commitment and place a high priority on it. To get started, consider the following guidelines:
Focus on raw, fresh foods, and avoid as many processed foods as possible (if it comes in a can, bottle or package, and has a list of ingredients, it’s processed).
Severely restrict carbohydrates from refined sugars, fructose and processed grains.
Increase healthy fat consumption. (Eating dietary fat isn’t what’s making you pack on pounds. It’s the sugar/fructose and grains that add the padding.)
You may eat an unlimited amount of nonstarchy vegetables. Because they are so low in calories, the majority of the food on your plate should be vegetables.
Limit protein to less than 0.5 gram per pound of lean body weight.
Replace sodas and other sweetened beverages with pure, filtered water.
Shop around the perimeter of the grocery store where most of the whole foods reside, such as meat, fruits, vegetables, eggs and cheese. Not everything around the perimeter is healthy, but you’ll avoid many of the ultraprocessed foods this way.
Vary the whole foods you purchase and the way you eat them. For instance, carrots and peppers are tasty dipped in hummus. You get the crunch of the vegetable and smooth texture of the hummus to satisfy your taste, your brain and your physical health.
Stress creates a physical craving for fats and sugar that may drive your addictive, stress-eating behavior. If you can recognize when you’re getting stressed and find another means of relieving the emotion, your eating habits will likely improve.
The Emotional Freedom Techniques (EFT) can help reduce your perceived stress, change your eating habits around stress and help you create new, healthier eating habits that support your long-term health. To discover more about EFT, watch the video at this referenced link on substack.43
*This article has been updated with new information.
One of the more pernicious and morally shocking developments surrounding the covid vaccines is hospitals forcing transplant recipients (and sometimes even their families) to be vaccinated with one of the covid vaccines.
I have heard a number of people defend this vile practice, who were genuinely convinced that there was nothing wrong with it. None of these individuals were “evil”, or anything close. Yet, they genuinely did not see a concern or dilemma that would disqualify the whole policy, or even one that would at least counsel a more thoughtful review before taking such a momentous and consequential step.
It is therefore worthwhile to present a clear explanation why, even assuming that transplant recipient vaccination is objectively beneficial as a purely scientific matter, mandating vaccination as a prerequisite for receiving a transplant is destructive to society and evil.
The following are a few of the more salient reasons why mandating recipient vaccination as a condition to remain eligible to receive a transplant, even assuming that transplant recipient vaccination are objectively beneficial as a purely scientific matter, is unjustifiable, destructive, and evil:
Breaks the Social Compact of Society:
Discriminates on the basis of a controversial political/social issue
Politicizes and undermines the trustworthiness of the medical community
Weaponizes the medical community / medical institutions in the “culture wars”
Drives the Balkanization of society
Is Intrinsically Immoral:
Such a mandate inflicts tremendous psychological torment upon people who are already suffering the stress and physical torment of a life-threatening disease
Erodes the ethics and character of medical professionals, so they regard some people as “inferior” and therefore undeserving of or not worth being treated
This is a policy that cannot be plausibly portrayed as being “in the best interests of patients”
Catch-all: Will cause considerable stress to the entire society
The Broader Context that Informs how People View Such a Mandate – The Medical Community no longer possesses the moral authority or credibility to make this sort of policy decision:
The already heavily damaged reputation and image of the medical community due to covid policies so far
A sizable minority today believes (if not outright majority) that hospitals and doctors are possibly complicit in the deaths of millions around the world and the unimaginable suffering of hundreds of millions more
Breaks the Social Compact of Society:
Discriminates on the basis of a controversial political/social issue
The reality of the current situation is that the covid vaccines are one of the preeminent issues at the forefront of the body politic in the country. This is therefore automatically a consideration when making policies on behalf of society, which any decisions regarding the prioritization scheme of transplant recipients are.
Decisions broadly affecting the whole of society that discriminate or persecute a faction/s of society break the social compact and erode or destroy the moral legitimacy of the major institutions through which political and social power and ideology are disseminated and enforced.
Specifically for this point, discriminating against a political or social minority – and surely where it is literally determining by proxy who lives and who dies – is by definition apartheid in both spirit and practice.
It goes without saying that apartheid policies are both harmful to a healthy and functioning society and evil.
Politicizes and undermines the trustworthiness of the medical community
Enacting a policy that is inextricably intertwined with a highly visible social or political controversy unavoidably conveys – regardless of whether it’s true – that the medical community is:
(A) a political actor that has
(B) vested political interests and objectives – such that it will
(C) pursue using the resources at its disposal
(D) even if/when they are in conflict with the neutral practice of medicine.
The damage from such overt political overtones and imaging (to say the least) to the practice of medicine, and the implications for the physical and mental health of the broader society, is something that does not require elaboration.
Importantly, this is true even for many of the people who agree with vaccination, because they also perceive that the medical community is “allying” with them to promote a political cause. The worse the reputation of the medical community is tarnished with political entanglements, the more difficult it becomes to rehabilitate subsequently.
Weaponizes the medical community & medical institutions in the “culture wars”
The participation of the medical community to coerce political compliance at gunpoint transforms the medical community (more than it is already) from a shared societal institution to a partisan one that one side views as a hostile force or enemy and the other views as a means to achieve political or social objectives.
The obvious (i.e. uncontroversial as factual observations regardless of whether one agrees or disagrees with the underlying position of either side here) societal harms that flow from this are manifold. Transforming the shared social institutions of science/medicine into a partisan weapon will cause the following negative consequences (among others; ‘shared’ is an increasingly tenuous proposition these days):
undermines trust in the practice of science
undermines the integrity of medical scientists by creating and incentivizing political objectives that take precedence over scientific integrity
causes a sizeable portion of society to regard doctors and medical professionals as enemies, which is harmful both to patients who will then not receive the same standards of medical care and to doctors who will suffer constant harassment and demoralizing stresses
encourages the propagation of propaganda as everyone is now incentivized to either deify or demonize medical practitioners and institutions regardless of the factual merits of any specific issue or incident
A society must have shared institutions that are not “playable characters” in the everyday social or political maelstroms that are the domain of politics in order to function and survive as a single political entity.
Drives the Balkanization of society
The most prominent consequence of the politicization and weaponization of the medical community and institutions is that it is a Balkanization of society. Regardless of the factual or scientific merits, even the perception by one faction that another faction is trying (and succeeding) in hijacking and corrupting the medical establishment is the fraying of the society as an organized political and social unit. To actually go ahead and do so is more damaging by orders of magnitude. Medical care is possibly the most foundational institution in a society – consider that the most consequential apartheid policy (besides for outright slavery) is the proscription of medical care by political or social affiliation. Thus proscribing medical care for a highly visible and prominent social faction within society – even if it wouldn’t be an outright death sentence for the patients restricted from medical treatment as is the case here – is tantamount to a declaration of [civil] war against anyone politically affiliated with the group targeted by the mandates.
It should also go without saying that you can’t have a functional society if whether your life and your human rights can be legally and socially vindicated depends upon on your political affiliation or ideological coadunation. There is no rational universe where this is an acceptable tradeoff for the conjectured benefits of restricting transplants to vaccinated patients.
Transplant Vaccine Mandates Are Intrinsically Immoral:
Such a mandate inflicts tremendous psychological torment upon people who are already suffering the stress and physical torment of a life-threatening disease
Any policy decision must consider the entire picture, not just the virtues of the preferred course of action.
Transplant vaccine mandates are dealing with a population that is exclusively comprised of people who are already under extreme suffering that is hard to contemplate or understand for someone bereft of this sort of experience. Adding distress to people already so tormented would therefore be warranted only if there was an exceptionally pressing concern. Even if the covid vaccines are somewhat beneficial as a purely scientific matter to patients awaiting an organ transplant, the marginal benefit of vaccination is hardly something that is so massive that imposing a vaccine mandate – in the context of everything else articulated in this article – can even be plausibly entertained let alone imposed. (The marginal benefit is the absolute risk reduction in all-cause morbidity/mortality gained from vaccination, not the “relative” risk reduction which is not relevant to assessing the real-world value of vaccination.)
Erodes the ethics and character of medical professionals, and influences and/or habituates them to regard some people as “inferior” and therefore undeserving of or not worth being treated
A policy of ‘either you acquiesce to vaccination or you die’ conveys to medical practitioners a clear message that people who reject the covid vaccines are not worthy of medical treatment. This is true regardless of the scientific merits of a (theoretically) objective cost/benefit analysis. Contingency of life-or-death treatment upon a political behavior or choice internalizes to medical practitioners and laypeople alike that it is appropriate to proscribe treatment to people because of political affiliation, so much so that we will even consign them to death. Medical apartheid on the basis of political or social faction characteristics is quite literally in the mold of the ideology and policies implemented in Germany in the 1930’s. Such a comparison is sufficient to retire any further consideration by itself of transplant vaccine mandates.
Such a dynamic is also corrosive to compassion and empathy — two attributes that are already in short supply in healthcare settings these days. The deprivation of treatment, especially in circumstances that are exceptionally heartwrenching, forces practitioners at minimum to suppress their sense of compassion. For many, the internal dissonance between their sense of compassion and the cruelty being inflicted on defenseless patients (& the relegation of a political class to “2nd class citizens”) that some would be complicit in will lead them to zealously embrace rationalizing that the unvaccinated are less than fully human. This is precisely how otherwise civilized people can be indoctrinated into an ideology that if unchecked ultimately enables them to commit or be complicit in the commission of atrocities.
(Requiring adherence to personal behavior standards – such as not consuming alcohol or drugs – whose medical rationale is obvious and apparent to everyone and which have already been standard requirements for decades is an entirely separate matter that has nothing to do with this discussion, and is something that requires its own lengthy dissertation to properly explore and flesh out.)
Like every other enumerated argument here, this point is true regardless of the factual merits of vaccination for transplant patients.
This is a policy that cannot be plausibly portrayed as being “in the best interests of patients”
Medical ethics is organized around the proposition that all decisions or policies must be in the best interests of patients. It is hard to imagine more blatant disregard of patients’ welfare than compromising the integrity and viability of the entire edifice of healthcare provision in the country as millions of people are less able and/or willing to seek and receive medical care as a result of all of the other points articulated above and below (and it is also not in the patients’ best interests for medical treatment to be withheld without which the patient will perish).
Contumeliously discarding the millennia-old foundational ethical principium of medicine ominously portends the possibility of medicine and healthcare unanchored to an ethical North Star.
Catch-all: This will cause considerable stress to the entire society
Polls consistently reveal that people of all social and political affiliations are suffering considerable stress. Policies that antagonize or that are erosive to the body politic spur or inflame the already burdened and fraying psyche of the populace. Even those advantaged by politically prejudicial persecution cannot escape the stresses that beset even those that have the upper hand politically, such as the worry that someday you will become a victim to the same social or political forces, or the stresses of living in a society where the social fabric is frazzled and fragmented. Especially in light of the current mental health apocalypse presently afflicting the country, it surely behooves the medical community to avoid further exacerbating the already overwrought stressors in people’s lives.
The Broader Context that Informs how People View Such a Mandate – The Medical Community no longer possesses the moral authority or credibility to make this sort of policy decision:
The reputation and image of the medical community has already been brutally savaged by the performance of the medical establishment throughout the covid crisis, especially the govt health agencies which are the backbone of the medical community’s authority and credibility. Moreover, at least a sizeable minority of the country believes that hospitals and doctors are complicit in the deaths of millions around the world and the unimaginable suffering of hundreds of millions more through draconian isolation of psychologically/emotionally vulnerable patients, denial of covid treatment, society-wide lockdowns, and vaccine carnage.
As a result, the medical community has lost the moral legitimacy and expert authority that until now was taken for granted. This is a monumental shift that is hard to overstate. The medical community previously was accorded the considerable latitude and deference by society they needed to make life-and-death policy decisions that society wouldn’t reflexively view as illegitimate or political. Without unambiguous and widely conceded moral authority to make controversial life-and-death policy decisions, the medical community ceases to be trusted and neutral stewards whose decisions can determine who lives and dies. Instead, they are no better than any other partisan and unobjective actor with their own biases and agenda. Empowering what is rationally perceived by one half of society as a conflicted and dishonest political actor to determine who lives and dies on the basis of a political characteristic is inherently evil and lacks even a semblance of moral credibility.
This last point is worth restating: This is akin to having a republican decide that democrats are not eligible for transplants unless they switch party affiliation or vice versa. The disfavored group would rightly and accurately perceive that a government that proscribes them from receiving lifesaving treatment lacks legitimacy.
Caveats:
It is important to note that there are many heroic doctors and nurses who do not agree with these policies. In a similar vein, the impact of such a policy (and the other covid policies that are similarly evil or just plainly irrational) is not uniform on all healthcare practitioners – there is a wide range of resiliency and resistance to the mental and psychological influence of this sort of policy.
It is also important to note that there is already considerable damage along the lines of everything stipulated above, so for the most part transplant mandates are aggravating already belabored destructive social pathologies as opposed to initiating or creating new ones.
However, this does not detract from the intensity or imperative of the arguments raised. The fact of the already-widespread devastation underscores how critical it is to reverse these developments – meaning that exacerbating them is that much more unconscionable.
Conclusion
Medical institutions are integral to the translation of medical and scientific knowledge into practice in a manner that will be accepted by the various major factions of society (there are always going to be fringe lunatic groups or cults that repudiate any sort of governing political bodies no matter what). A society without a shared epistemology cannot survive, as there can be no agreement on how to determine factual truth. The medical establishment institutions are fiduciaries to the entire population, granted awesome powers over society, and therefore commensurately responsible for the broader social impact of their actions (something that the medical literature en masse freely embraces, one need only look at the hundreds of papers condemning the medical community for their role in promoting “health inequities” and systemic racism).
It is not just prudent but obligatory to consider the political climate when weighing a policy choice that implicates and will resonate through the exigent political and social realities on the ground such as they are. One would think it would be common sense to go to the farthest practical extreme to avoid even the hint of appearing partisan or political, never mind actually further inflaming the divisive and increasingly weaponized political tensions. This is by no means even remotely controversial. The typical standards that society holds critical non-partisan institutions to is that they must avoid “even the appearance of” conflicts of interest, partisanship, etc. – recusals for these reasons are routine in the legal world for instance.
One would also be forgiven for thinking that the medical community would be embarrassed to be caught openly embracing the same fundamental political philosophy that animated the Nazi’s systematic denudement of the medical community back then of the ethical code synonymous with the practice of medicine.
Enacting a policy that in practice is political discrimination is irreconcilable with both basic medical ethics and the responsibility of the medical community to scrupulously avoid even the appearance of partisanship or other non-medical entanglements. There is no justification or defense for such an egregious lapse of judgement.
The ever-sharp Zacki on Twitter points to this intriguing 2018 study out of New York. The authors administered PCR tests to 2,685 people at a tourist attraction in New York City, between the months of January and July. Over 6% tested positive for one of seven common human respiratory viruses. In the winter, human coronaviruses were the most common; in the summer, rhinoviruses took the lead. By design, the study targeted healthy populations, and so we must imagine that it substantially understates the true rate of virus infection.
The authors don’t find a significant difference in the overall prevalence of positivity between winter and summer. In their small sample, it’s only the mix of viruses that changes. This is another piece of evidence in favour of my crazy theory, that a great part – perhaps a majority – of spring and summer allergies are in fact persistent low-grade rhinovirus infections.
Other studies, particularly on rhinovirus, find even larger incidences of infection. There is this paper, which looks at rhinovirus in infants and finds that 20% of their sample are asymptomatic positives; or this case-control study of all ages, which finds rhinovirus in 17% of their asymptomatic controls.
For perspective: At the height of the alpha wave in the United Kingdom, only about 0.3% of the population was testing positive for SARS-2 every day. School antigen testing in Germany, which is done multiple times a week and finds nearly every detectable infection in school-age children, found Delta 7-day incidences of around 1%, and Omicron 7-day incidences peaking in February at near 4% in specific age cohorts (see the the graph on p. 5). The allegedly hypercontagious SARS-2 looks like it was doing substantially worse, in other words, than garden-variety human coronaviruses in the same month in the New York study.
Respiratory viruses are extremely pervasive; they’re everywhere and this is totally normal. What isn’t pervasive, is virus testing. We’ve only ever tested widely for a single virus. So much of Corona mythology depends upon presenting data in isolation from what we know about the behaviour of all the other pathogens we’ve lived with for centuries. Our governments have spent two years hyperventilating about incidences of infection that turn out to be minuscule, or at worst normal, when compared to the other pathogens that infect us. This should also make you very, very sceptical of uncontrolled studies cataloguing alleged Long-Covid symptoms. If we tested this widely for rhinovirus, imagine all the totally unrelated symptoms we’d find in our vast pool of positive results.
The Pandemic Response and Recovery All-Party Parliamentary Group met this week to hear about visiting restrictions still being imposed by many care homes and NHS Trusts. Co-chaired by Rt Hon Esther McVey MP and Graham Stringer MP, the Group listened to evidence about the devastating effects visiting restrictions in hospitals have on patients and their loved ones. MPs also heard how visiting restrictions in care homes, along with the continued use of rolling lockdowns and over interpretation of testing guidelines, is leading to isolation, neglect and abuse of the residents.
Leandra Ashton, who co-founded The People’s Care Watchdog, Dr. Ammar Waraich, a medical registrar in the West Midlands, Carol Munt, experienced Patient Partner and Advocate and Dr. Ali Haggett, community mental health and wellbeing specialist, told MPs of the obstacles still in place when trying to visit a loved one and the shocking impact on vulnerable hospital patients, care home residents and their families.
All the speakers voiced serious concerns that obstacles are still in place in some healthcare settings. Politicians heard harrowing accounts of the harmful effects of isolation and loss of social contact on physical and mental health, safeguarding problems with medication, dehydration, hygiene and lack of basic care and the failures to uphold existing legislation to protect those who lack capacity.
Leandra Ashton’s mother was arrested in November 2020 for taking her grandmother out of her care home a day before the second lockdown. Two years on, many residents are still being isolated from their loved ones. She told MPs:
When I took the video of my mum being arrested taking my nan out of her care home, I did not think it would go viral. So many families got in touch and it led to us setting up the People’s Care Watchdog. We were struck by how much legislation is in place, such as Article 8 of the Human Rights Act, Deprivation of Liberty and the Mental Capacity Act, to protect those in care homes. These laws are simply not being upheld and instead guidelines are being over-interpreted and the legislation even used to keep people in care homes and hospitals as if they were prisons. The public bodies that are supposed to uphold the protective legislation are not doing so.
There are still obstacles in place when trying to visit a loved one in a care home and the impact has been and continues to be devastating. The safeguarding issues I am seeing and hearing about are atrocious. Residents left for hours in dirty, wet incontinence pads leading to dangerous pressure ulcers. Malnutrition. Dehydration. End of life medication given to patients without their or their family’s consent. Psychological trauma, post-traumatic stress and suicides have resulted because of this. Multiple systems are failing, including Local Authorities and the CQC. It is a complex situation that needs a bold approach by both empowering families and galvanising Government action to hold public bodies to account and stop private equity firms placing profit over people.
Listening to the evidence, Esther McVey said:
I am troubled by the evidence presented by our speakers, particularly the safeguarding issues and neglect that care home residents are suffering as a result. In hospitals, we have heard about patients losing hope and refusing treatment without the encouragement of family. We know patients have much better treatment outcomes when they have support from relatives and friends around them.
Most of the infection control measures that restricted visiting in healthcare settings have been removed, most recently NHS Trusts were told healthcare workers, patients and visitors no longer need to distance in hospitals, so I fail to see why and how these visiting restrictions are still in place in any healthcare setting. I shall be writing to the Secretary of State for Health and Social Care to ask that he makes it absolutely clear that all patients and residents must be able to see visitors.
Highlighting how visitation is an important and necessary part of healthcare, Carol Munt said:
In the same way that we would not stop prescribed medication and treatments, we should not have stopped visits. Why were decisions taken without any consideration for the need of patients and their families to connect? Why do we still have such variation in compassionate care across the country? There is no uniformity among care homes apart from the need to be profitable for their owners. Some care homes made a superhuman effort to arrange visiting, as did the Bristol Nightingale Hospital. There was good practice in some places so there should be good practice everywhere. We should expect more of these endemic situations and we must be prepared for them.
I could not comprehend how any Minister for Health and Social Care could allow this to happen and not make the effort to get his department to look at ways that visiting could be facilitated. I heard and continue to hear the most callous reports of relatives dying alone with no visitors. The same goes for hospital patients. Ultimately, I think we need legislation to ensure that visiting rights are enshrined and protected.
Medical Registrar Dr. Ammar Waraich reported that many hospitals are still preventing visits due to the potential risk of Covid spread:
The policy is cruel, inhumane and unnecessary. Seeing loved ones can be immensely therapeutic and give struggling patients the will to survive. It is deeply traumatic for families to lose loved ones suddenly or see them go through difficult treatment without being there in person. Video calls are not a good enough replacement and we do not have the staff, the time or resources to facilitate calls for all our patients.
Most infection control measures have been lifted as the level of risk is no longer there. Hospitals can no longer function as detention centres and an inpatient stay should not become a sentence. The policy was one of the major mistakes of lockdown. Visiting sick relatives in hospital is, and must remain, a fundamental right, not to be given up.
Co-chair Graham Stringer said:
I find it extraordinary that no visiting is allowed in some healthcare settings, even to this day. It is cruel that family members are being denied access to sick and vulnerable loved ones, often not getting regular updates, living in anxiety about what their relatives may be going through, but knowing they are going through frightening and difficult treatment, often at the end of their lives, without being able to be with them in person.
“At the height of the pandemic it was understandable that there were precautions but there is no longer a basis to that argument. All the restrictions have been lifted and NHS Trusts across England have now been told to ‘return to pre-pandemic physical distancing in all areas’. The government must take action to resolve this situation.
Speaking about her experience working in the community throughout the pandemic, Dr. Ali Haggett said:
I have spent the last eighteen months with the support group Unlock Care Homes, uncovering the plight of many thousands of families who are still denied regular, meaningful contact with care home residents and hospital patients. Even before Covid, we knew that isolating people, particularly older people, has a serious impact on physical and psychological health. We have continued to isolate adults in care and in some hospitals almost continuously for two years. The effects have been felt particularly badly by those with dementia. Many residents no longer recognise their families and have been denied the most basic of human needs.
My concern is that this situation is concealing neglect and abuse on a significant scale. One of my community members sadly died and the hospital has admitted liability partly because he was completely blind and couldn’t reach his food or drink. Had his wife been allowed to visit, this wouldn’t have happened. Families I work with report numerous issues still affecting them, not just visiting restrictions. Rolling lockdowns, over-interpretation of testing, PPE requirements resulting in poor communication and fear, lack of ancillary services such as podiatry or physiotherapy leading to huge health problems, residents asked to isolate when one person tests positive, sometimes for 10 days or more and the one significant visitor recommendation being ignored or rejected. Families must be able to visit openly and check the wellbeing of residents.
Stop Press: MPs and Peers including Esther McVey, Lord Frost, Sir Iain Duncan Smith, Sir Graham Brady, Emma Lewell-Buck, Graham Stringer and Sammy Wilson have written to the Telegraphto say they are “deeply concerned” that visiting is still forbidden in many institutions where “over-interpretation of testing guidelines is leading to isolation, neglect and abuse of vulnerable residents”. They point out that Article 8 of the Human Rights Act and the Mental Capacity Act “could and should have protected against this situation arising” but this legislation is being “wilfully misinterpreted as an excuse” to keep people isolated in care homes and hospitals “as if they were prisons”.
A newly published, peer-reviewed study in Cureus looked to see if there was a correlation between mask compliance and COVID-19 outcomes in Europe. The study was undertaken at the University of Sao Paulo in Brazil.
The authors noted that previous trials about mask effectiveness had produced mixed results and those that concluded that masks were associated with a reduction in transmission and cases were conducted out of season.
“The World Health Organization (WHO) as well as other public institutions…strongly recommend the use of masks as a tool to curb COVID-19 transmission. These mandates and recommendations took place despite the fact that most randomised controlled trials carried out before and during the COVID-19 pandemic concluded that the role of masks in preventing respiratory viral transmission was small, null, or inconclusive. Conversely, ecological studies, performed during the first months of the pandemic, comparing countries, states, and provinces before and after the implementation of mask mandates almost unanimously concluded that masks reduced COVID-19 propagation.
However, mask mandates were normally implemented after the peak of COVID-19 cases in the first wave, which might have given the impression that the drop in the number of cases was caused by the increment in mask usage. For instance, the peak of cases in Germany’s first wave occurred in the first week of April 2020, while masks became mandatory in all of Germany’s federal states between the 20th and 29th of April, at a time when the propagation of COVID-19 was already declining.
Furthermore, the mask mandate was still in place in the subsequent autumn-winter wave of 2020-2021, but it did not help preventing the outburst of cases and deaths in Germany that was several-fold more severe than in the first wave.”
Due to the different levels of masking in Europe (5% – 95% compliance), it gave the authors the opportunity to test masking during a strong COVID-19 wave.
“Data were collected from the following Eastern and Western European countries: Albania, Bosnia and Herzegovina, Bulgaria, Croatia, Czechia, Hungary, North Macedonia, Poland, Romania, Serbia, Slovakia, Slovenia, Belarus, Estonia, Latvia, Lithuania, Republic of Moldova, Ukraine, Austria, Belgium, Denmark, Finland, France, Germany, Greece, Ireland, Italy, Netherlands, Norway, Portugal, Spain, Sweden, Switzerland, United Kingdom, and Northern Ireland. The inclusion criterion was a population size higher than one million people.”
Analysis was undertaken to verify if masking correlated with COVID-19 morbidity and mortality. The data looked at were between October 2020 and March 2021, in the 35 European countries listed above, during which all the countries went through a peak COVID-19 infection wave.
The average proportion of masking was 60.9% with Eastern Europe being slightly higher than Western Europe. However, compliance was much more homogeneous in the East than the West.
Importantly, results showed a weak positive correlation for mask compliance versus morbidity (cases) and mortality (deaths).
Each dot in the diagrams above represent a different country. As you can see, as mask compliance goes up, so do cases/million and deaths/million.
Please note, the positive correlation for mask usage and cases was not statistically significant. However, the correlation for masks and deaths WAS statistically significant.
The correlation was even higher in the West compared to Eastern countries. It is suggested that this could be because larger countries are located in the West. However, even when the largest countries were removed, the correlations hardly changed.
Various other analyses were performed, e.g. using smaller and larger countries but no tests resulted in negative correlations.
The authors conclude by saying that “while no cause-effect conclusions could be inferred from this observational analysis, the lack of negative correlations between mask usage and COVID-19 cases and deaths suggest that the widespread use of masks at a time when an effective intervention was most needed, i.e., during the strong 2020-2021 autumn-winter peak, was not able to reduce COVID-19 transmission. Moreover, the moderate positive correlation between mask usage and deaths in Western Europe also suggests that the universal use of masks may have had harmful unintended consequences.”
Science is finally catching up with the science that disappeared two years ago. Whilst this study is not conclusive, it is quite damning and will be interesting to see what masking mandates or recommendations are brought back, next winter, after this.
THE business magazine Forbes has published a story with the arresting headline: ‘Unvaccinated People Increase Risk Of Covid Infection Among Vaccinated, Study Finds.’
The work to which it refers is not in the normal sense a study but is actually a modelling exercise published by the journal of the Canadian Medical Association. Did the Forbes staff writer read the paper very well? I am quite sure not. At the end of paragraph one of the Method section of the original paper, it describes its model, saying: ‘A vaccine that is 80 per cent efficacious would result in 80 per cent of vaccinated people becoming immune, with the remaining 20 per cent being susceptible to infection. We did not model waning immunity.’
Now I am sure you know that the mRNA vaccines do not stop infection and also wane in effectiveness. In other words mRNA vaccination does not confer immunity and its effectiveness does not remain constant as the paper assumes. So what use is this paper and to what do its conclusions apply? Apparently not to the mRNA Covid vaccines.
Lo and behold, one of the paper’s authors, David Fisman, declares competing interests: ‘He has served on advisory boards related to SARS-CoV-2 vaccines for Seqirus, Pfizer, AstraZeneca and Sanofi-Pasteur Vaccines.’
Another author, Ashleigh Tuite, was ‘employed by the Public Health Agency of Canada when the research was conducted’ (aka the domain of Justin Trudeau).
So why publish this story which on the face of it has little relevance to the real-world data of the current pandemic? Forbes magazine is 51 per cent owned by a Hong Kong-based company, Integrated Whale Investments, about which little is known. The Washington Post has suggested that Forbes’s editorial policy has been influenced as a result, but by whom no one really knows.
At this point in the pandemic, it has become clear that boosted individuals are becoming more vulnerable to Omicron than the unvaccinated. So I can only suggest that it might be advantageous for some scientists and politicians to blame the unvaccinated for everything in order to cover up their own mistaken ideas. Or perhaps there are commercial interests anxious to sell more arguably useless vaccines for billions of dollars. You decide.
If the government and their compliant media friends are our one source of truth, as has happened in New Zealand (by decree), then you have no option except to blame the unvaccinated whatever happens.
The actual situation is that the unvaccinated are currently less likely to be hospitalised than the boosted. Thank you to Grant Dixon for compiling and graphing NZ Ministry of Health data, below.
This morning my mask-exempt friend entered a haberdashery shop, whereupon two other potential customers turned and fled. Yesterday she was turned away from a fabric store. I am sure many of you have had similar experiences. The fact of the matter is that almost the whole of the New Zealand population has become subject to fear-based government-sponsored groupthink.
Are we all being conditioned to vote for Jacinda Ardern in next year’s election based on the carefully constructed myth that she is keeping us all safe? We should be keeping our feet on the ground. We should recognise that public relations experts and propaganda promoters are at work full-time, but they are working out of touch with reality.
Meanwhile our whole economy is becoming ever more dysfunctional. As people are too afraid to associate with one another in public, the whole basis of commercial activity is being undermined.
The two large supermarket chains are laughing all the way to the bank. As small businesses are forced to close and their monopoly grows, supermarket prices and profits are entering the stratosphere. Smart individuals are now ordering their vegetables and groceries direct from Australia (as far away from us as Moscow is from London) because they are so much cheaper.
The government is clueless to control this rampant price inflation, along with most things including the pandemic. The public is hoodwinked, queueing fully masked and fully vaccinated to pay through the nose for everyday items without a squeak of dissent.
The ten-year-old son of a friend asked his mother the other day: ‘Which do you think our society is more like – Brave New World or 1984?’ I doubt if either Aldous Huxley or George Orwell could ever have imagined anything so incomprehensibly doublethinking as 2022 New Zealand.
This is the state we have reached through our government’s careful rationing of information and saturation conditioning.
Time we reopened the floodgates of free speech and social media – hold your horses, we might endanger our one source of truth.
By Kurt Nimmo | Another Day in the Empire | April 20, 2026
In 2025, Alex Karp, the CEO of government and military tech contractor Palantir, published The New York Times best-seller, The Technological Republic: Hard Power, Soft Belief, and the Future of the West. The Wall Street Journalpraised the book as a cri de coeur, a passionate appeal “that takes aim at the tech industry for abandoning its history of helping America and its allies,” while Wired praised the book as a “readable polemic that skewers Silicon Valley for insufficient patriotism.”
On April 18, 2026, Palantir posted twenty-two points to social media summarizing the book. In addition to taking Silicon Valley to task for insufficient patriotism, advocating a role for AI in forever war, and denouncing the “psychologization of modern politics,” the Palantir post on X declares: “National service should be a universal duty. We should, as a society, seriously consider moving away from an all-volunteer force and only fight the next war if everyone shares in the risk and the cost.”
National conscription, a form of involuntary servitude, and the wars it portends, is good for business, especially for corporations within the orbit of the Pentagon, the CIA, and the national security state. Palantir fits comfortably within this amalgamation. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.


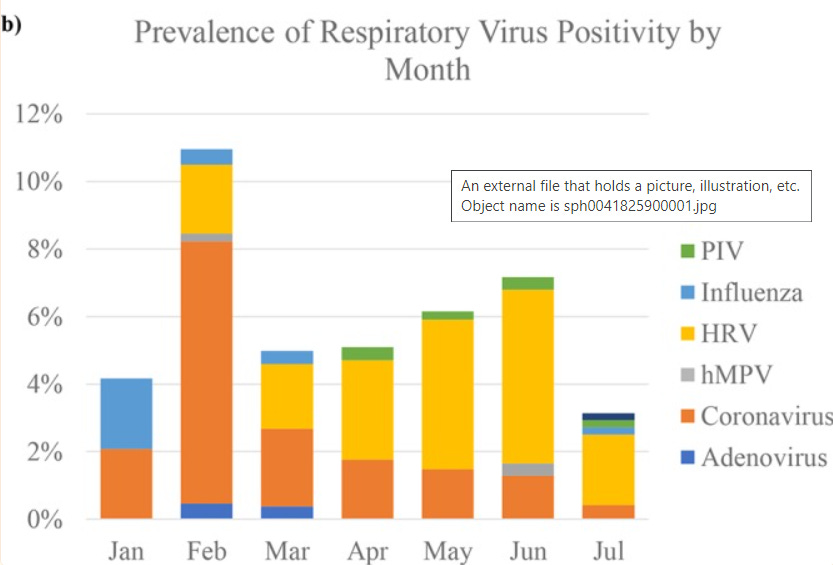
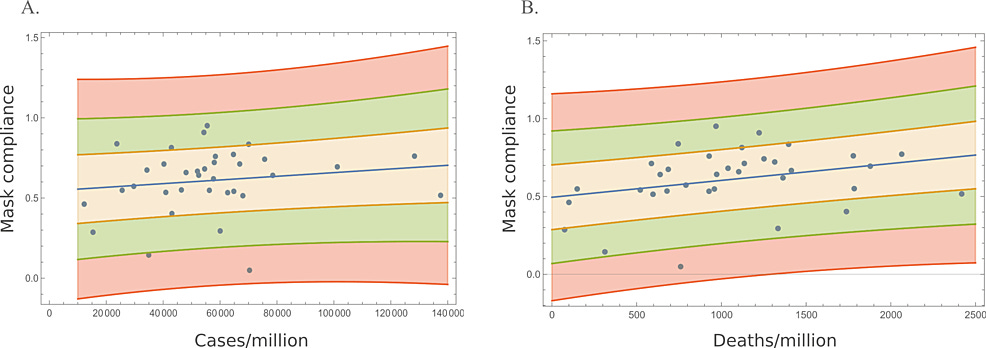


 Aletho News
Aletho News