I find it extremely unbelievable that nobody will investigate this entire scam for what it is. The people behind the vaccines should be dragged in to testify what is going on. Moderna has admitted it took them only 2 days to create the vaccine. In Texas, they are trying to launch a criminal investigation. The FDA is no longer trustworthy, for the normal time to get anything approved is 12 years. What has been released in less than one year with no animal studies? There has been NO TESTING to determine side effects on pregnancy, fertility, or lactation.
It is just stunning that we have politicians REFUSING to look at anything, probably because they are too busy counting their bribes. The White House said under NO condition would they ever fire Fauci, meaning under NO condition will they investigate anyone.
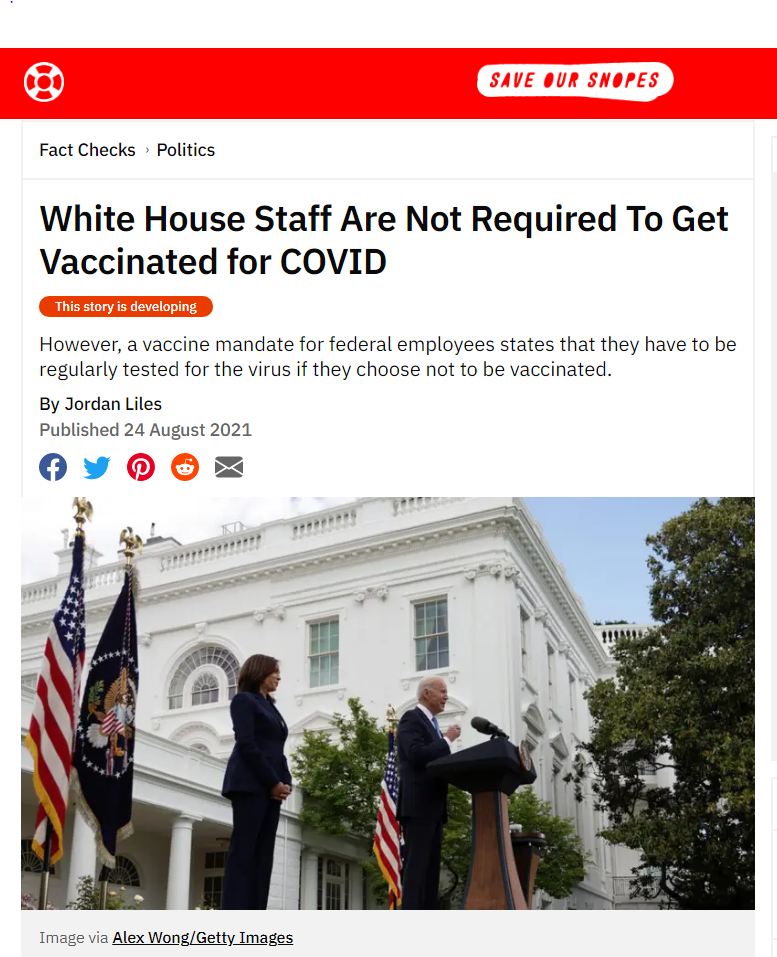
Meanwhile, even the notorious corrupt Snopes had to admit this is TRUE. Despite demanding everyone gets vaccinated, the White House said its own staff DOES NOT need to be vaccinated provided they are routinely checked. So why is the White House the entire exception? Even the military is demanding 100% compliance. Meanwhile, the White House has demanded everyone else receive vaccinations or lose their job.
The fact that they have skipped animal trials is very disturbing. When the government is part of the conspiracy against the public, we will NEVER know the truth about anything. Jack Dorsey has been especially protective of the narrative. Nobody is allowed to question the government no matter what.
Then there are studies revealing that natural immunity to COVID is 13 times better than the vaccines. They try to bury such studies, and they also try to ensure that they are not peer-reviewed in order to discredit them. The Science journalist Alex Berenson was permanently suspended from Twitter one day after his tweets that reported an Israeli study that making this finding that natural immunity from a prior Covid-19 infection is 13 times more effective than vaccines against the delta variant. Twitter is now acting against the very basis of free speech, which is threatening people’s lives. I would love to see Twitter taken down, for they are clearly now responsible for the deaths of many people from vaccine injuries.
To show that this is one giant cover-up, OSHA has instructed employers NOT TO REPORT vaccine injuries suffered by employees if they only “recommend” the shots. Many employers with more than 10 employees are required to keep a record of serious work-related injuries and illnesses. Nobody should volunteer to be vaccinated to satisfy an employer, for you will not be covered for any injury or loss of pay, and you could be fired for not showing up to work for a period of time. However, if employers mandate vaccines to work, then the vaccine injuries should become subject to reporting, lawsuits, and workman’s comp claims.
Antibody testing is the gold standard for determining immunity, says immunologist and physician Dr. Hooman Noorchashm. Yet, the CDC and FDA are actively deterring people from testing their immunity. Why?
In May 2021 the FDA issued an advisory discouraging Americans from testing the status of their antibody immunity to COVID-19, Noorchashm wrote in an editorial on his blog. “Those who are adequately immune to COVID-19 are rarely, if ever, getting reinfected — regardless of whether this immunity comes from vaccination or from a natural infection,” Noorchashm said.
Meanwhile, “those who are NOT immune to SARS-CoV-2 are susceptible to being infected,” he said. He surmises that to end the pandemic upward of 90% of the population need to become immune.
As far as testing for immunity, according to Noorchashm, the FDA advisory prevents people from obtaining critical information necessary to protect themselves during the pandemic. “ … by not encouraging liberal COVID-19 antibody testing, especially in fully vaccinated Americans, the FDA and CDC are preventing vaccinated, but inadequately immune, persons from finding out that they remain susceptible to infection,” he wrote.
Citing his own experience as a physician, he said “patients who hesitate to undergo vaccination are far more likely to do so when they are confronted with a negative antibody test demonstrating they are susceptible.”
Tess Lawrie’s group’s metaanalysis of ivermectin research papers, published in June, has received a great deal of positive attention. It was, as expected, carefully done. The authors graded the quality of the papers they reviewed.
The abstract noted:
“Therapeutic Advances: Meta-analysis of 15 trials found that ivermectin reduced risk of death compared with no ivermectin (average risk ratio 0.38, 95% confidence interval 0.19–0.73; n 5 2438; I2 5 49%; moderate-certainty evidence)…” This means that using only evidence of moderately good quality (high quality is often hard to come by, especially using observational data), if 100 people sick enough with Covid to die are given ivermectin, only 38 will die, and 62% will be saved.
“Low-certainty evidence found that ivermectin prophylaxis reduced COVID-19 infection by an average 86% (95% confidence interval 79%–91%).”
More doctors are using the drug. More patients are hearing about it. I have been getting more calls from patients who want to know about it. The NY Timessaid pharmacists are filling 88,000 scripts a week now.
Covid death rates, compared to the number of cases diagnosed, are way down compared to 2020 and last winter. While the NYT says there are 100,000 Covid patients in hospital now, only 1,500 are dying daily, or 1.5%, a much lower percentage than previous waves.
This is probably due to lower virulence of current variants, some benefit from vaccination, less use of ventilators and more use fo effective therapeutics.
And so now the CDC is coming down hard and many pharmacist have decided to stop filling the scripts in the past week. More on this in my next post.
Respiratory syncytial virus (RSV) — a respiratory virus that causes typically mild cold-like symptoms — has apparently been selected as the next invisible boogey man. Most children have been exposed to RSV by their second birthday.
The fact that most children survive past the age of 2 tells you something about the risks involved. That said, in very rare cases, RSV can progress to pneumonia or bronchiolitis (inflammation of the small airways of the lungs).
RSV Emerges Out of Season Around the World
According to reports, RSV is now raging around the world, from New Zealand1 to Japan2 and the U.S.,3 where it hit so hard in June 2021 that the Centers for Disease Control and Prevention issued an emergency alert4 for parts of the southern United States.
The CDC encouraged testing for RSV among patients who tested negative for COVID-19 but had “acute respiratory illness” symptoms. They also advised health care personnel, child care providers and staff of long-term care facilities to stay home from work if they had respiratory symptoms, even if they test negative for COVID, as they might have RSV.
In New Zealand, health officials said there were few cases of RSV in 2020 during the pandemic and, while it’s normally a winter disease, it’s now making a comeback off-season in 2021. According to Stuff.co.nz,5 the outbreak “was more than twofold greater than the historical average from 2014 to 2019 for this time of year.”
Similar reports have been published in Japan where, in early July 2021, the National Institute of Infectious Diseases warned of RSV infections outside the normal peak period. According to the Japan Times :6
“… the number of RSV patients per medical institution was 3.87 in the week ending June 27 — the highest number of cases since 2019. In 2018, the year the counting system was changed, the infection count peaked in September at 2.46, and it reached 3.45 patients per medical institution a year later.”
August 3, 2021, U.S. health officials reported that RSV had started to taper off by midsummer, but a resurgence is now seen, with a “record-breaking 563 new RSV cases” reported in the week before August 3.7
FDA Fast-Tracks mRNA Shot Against RSV
That same day, August 3, 2021, the Food and Drug Administration granted fast-track designation to Moderna for an mRNA-based injection against this common cold virus. As reported in a Moderna press release:8
“… the U.S. Food and Drug Administration (FDA) has granted Fast Track designation for mRNA-1345, its investigational single-dose mRNA vaccine against respiratory syncytial virus (RSV) in adults older than 60 years of age.
‘We are pursuing an mRNA RSV vaccine to protect the most vulnerable populations — young children and older adults,’ said Stéphane Bancel, Chief Executive Officer of Moderna.
‘We are studying mRNA-1345 in these populations in an ongoing clinical trial and we look forward to sharing data when available … We have accelerated research and development of our infectious disease therapeutic area and we will continue to advance our mRNA vaccines into new areas of high unmet need.'”
Moderna’s press release correctly points out that there’s no approved vaccine available for RSV. What they don’t mention is why. The reason there’s no RSV vaccine on the market is the same reason why there has never been a coronavirus vaccine, and that is because none of them were able to pass trials.
As with coronavirus, previous efforts to develop an RSV vaccine have met with failure as test subjects have a pesky tendency to die or become seriously ill when exposed to the wild virus, thanks to paradoxical immune enhancement (PIE), also known as antibody dependent enhancement (ADE).9
RSV Shot Builds on COVID Jab
Moderna’s RSV shot uses the same lipid nanoparticle as its COVID-19 injection. The primary difference between the two shots is the coding of the mRNA. In the RSV shot, the mRNA encodes for a prefusion F glycoprotein.
Prefusion F protein is a protein that mediates the RSV virus’ entry into your cells and is known to elicit a neutralizing antibody response.10 Under normal circumstances, it’s hard to imagine an RSV vaccine built on a novel mRNA platform getting fast-tracked, but we’re no longer in normal times.
The rollout of mRNA COVID shots have, as predicted, paved the way for any number of new mRNA-based injections going straight to human trials. So, should you ever feel like your body lacks in synthetic mRNA, fear not. This is just the beginning. Those who embrace vaccine passports will surely find themselves called to the nearest vaccine center several times a year for mandatory refills.
Are We Creating a Public Health Disaster?
The decision to fast-track yet another mRNA injection fails to take into consideration the possibility that we might already be creating an avalanche of ADE-related illness from the COVID shot. Adding another injection for a respiratory virus that has historically been associated with ADE could be extremely risky.
As noted in a September 9, 2020, Nature Microbiology paper titled “Antibody-Dependent Enhancement and SARS-CoV-2 Vaccines and Therapies”:11
“Data from the study of SARS-CoV and other respiratory viruses suggest that anti-SARS-CoV-2 antibodies could exacerbate COVID-19 through antibody-dependent enhancement (ADE). Previous respiratory syncytial virus and dengue virus vaccine studies revealed human clinical safety risks related to ADE, resulting in failed vaccine trials …
ADE can increase the severity of multiple viral infections, including other respiratory viruses such as respiratory syncytial virus (RSV) and measles.
ADE in respiratory infections is included in a broader category named enhanced respiratory disease (ERD), which also includes non-antibody-based mechanisms such as cytokine cascades and cell-mediated immunopathology …
Furthermore, ADE and ERD has been reported for SARS-CoV and MERS-CoV both in vitro and in vivo … ADE pathways can occur when non-neutralizing antibodies or antibodies at sub-neutralizing levels bind to viral antigens without blocking or clearing infection …
ADE has been observed in SARS, MERS and other human respiratory virus infections including RSV and measles, which suggests a real risk of ADE for SARS-CoV-2 vaccines and antibody-based interventions …
Going forwards, it will be crucial to evaluate animal and clinical datasets for signs of ADE, and to balance ADE-related safety risks against intervention efficacy if clinical ADE is observed.”
In case you missed it, the authors specifically point out that ADE can worsen the severity of RSV. Theoretically then, if you get the COVID shot and end up with ADE, then contracting RSV could turn into a far more serious problem than it would otherwise.
Have COVID Policies Weakened Immune Systems?
While the COVID shot could play a role if we start seeing severe RSV in adults, it’s unlikely to be part of the equation when it comes to children, as the shot is still not authorized for children under the age of 12. More than likely, the out-of-season rise in RSV among children is related to the easing of restrictions after not being exposed to normal pathogens for extended periods of time.
During the past 18 months, as most of the world has been masked up, locked down and otherwise distanced from one another, children and adults have not been exposed to viruses and bacteria as they normally would.
On the one hand, there has been a significant reduction in the number of people reporting colds, flu and other infectious diseases. On the other hand, some health experts are questioning if this lack of exposure may have increased the risk for some to experience more illnesses as children reenter school and adults reenter the workforce.12
The two main parts of your immune system are your innate immune system, which you were born with, and your adaptive immune system, which is developed as you’re exposed to pathogens.13 A healthy immune system keeps a record of every pathogen to which it has been exposed so that it can quickly recognize it if exposed again. Your immune system is activated when you’re exposed to a protein it doesn’t recognize, called an antigen.
Since the system is so complex, there are several potential ways in which things can go wrong. If your immune system doesn’t work correctly it can result in immunodeficiency diseases, resulting in more and longer-lasting sickness.
Some health experts are concerned that children may have experienced greater harm to their immune system than adults since they have spent the better part of the last 18 months isolated from nearly every exposure.14
From what researchers are now finding, it is infants and children who may have the most detrimental response to social distancing.15 Since the beginning of 2020, doctors and hospitals have noticed a significant reduction in the number of bacterial and viral infections children have been contracting. This includes bronchiolitis, measles, varicella, RSV and pertussis.
A paper16 published in August 2021, from the Pediatric Infectious Disease Group postulated nonpharmaceutical interventions imposed during 2020 could result in larger epidemics of infectious diseases once these interventions are lifted.
Rising Number of Infants With RSV Related to Immunity Debt
Some experts are calling a rising number of RSV infections in babies a “debt of immunity” created because infants born during 2020 had a lack of exposure to normal pathogens.17 Once infants and children are introduced to these environmental pathogens en masse, it can instigate a precipitous rise in cases.
According to The Guardian,18 New Zealand reported a 99.9% reduction in flu and 98% reduction in RSV during 2020. This nearly eliminated the spike of deaths that happens during the winter months from flu and RSV. In the short-term, it may have prevented an overload of the health care system while others were being treated for COVID-19.
However, in the long run, it may have created an additional problem in infants and children. When the immune system is not challenged at an early age, it can lead to larger outbreaks, which again taxes the health care system. As of early July 2021, New Zealand had reported nearly 1,000 cases of RSV over five weeks. The usual number reported is 1,743 over 29 weeks.
Doctors are hoping this doesn’t necessarily mean there will be more RSV cases, only that they are occurring in more rapid succession early in the season. The current outbreak has stretched the resources in New Zealand and Australia, which is also experiencing a surge in cases. New Zealand’s director general of health Dr. Ashley Bloomfield commented to a reporter from The Guardian saying he was:19
“… certainly concerned about the sharp surge in RSV cases … There’s some speculation that [the current outbreak] may be partly exacerbated by the fact we didn’t have any last year and so there is a bigger pool of children who are susceptible to it.”
In Canada, Wellington-based epidemiologist Michael Baker warns that his country may also see a similar trend in cases of RSV in the next year, warning that babies who were born prematurely are most at risk.20
That said, while Canada may see a rebound in RSV infections, Baker does not think that a lack of exposure to pathogens at an early age will have “in any way impeded the development of a healthy immune system.”
Is a Fast-Tracked RSV Shot the Answer?
Considering the multitude of problems associated with the gene-based COVID shots, I’m not optimistic about the development of a fast-tracked mRNA “vaccine” against RSV. The risks are numerous. Already, we’re seeing trends that could signal that ADE is at play in older people who got the jab (but not younger people).
In the U.K., as of August 15, 2021, 68% of COVID patients admitted to hospital who were over the age of 50 had received one or two COVID injections. Mortality statistics reveal the exact same trend. In the over-50 group, 70% of COVID deaths were either partially or fully “vaccinated.”21
Could this be because older people are developing ADE and therefore suffer more serious infection when exposed to the SARS-CoV-2 virus? In the under-50 category, the unvaccinated make up a majority of hospitalizations and deaths in the U.K., so perhaps the shot affects different age groups differently.
Older people are also the target group of the RSV shot, and infants and young children are a target for both COVID shots and RSV shots. Time will tell what the ramifications of programming the bodies of the very young and the very old to produce more than one antigen might be. But my guess is it won’t be good.
According to Facebook’s content transparency report for the first quarter of 2021, released in mid-August 2021, the most popular article shared on the platform between January 2021 and March 2021 was about a 56-year-old Miami, Florida, obstetrician who died two weeks after his first Pfizer injection.1
The story initially ran in the South Florida Sun Sentinel 2 April 8, 2021, and was republished by the Chicago Tribune that same day.3 The doctor, Dr. Gregory Michael, received his first dose December 18, 2020.
Three days later, he developed small spots on his hands and feet, which prompted him to go to the emergency room, where they found he had an abnormally low blood count. Platelets stop bleeding by clotting, and when platelets drop too low, internal bleeding can occur, resulting in what looks like blood blisters on the skin.
Michael remained in intensive care for two weeks, but no matter what they did, his platelet count refused to budge. During the night of January 3, 2021, he died of a massive stroke. According to the coroner, the COVID injection could not be ruled out as a contributing or causative factor.
In a Facebook post, Michael’s widow stated he’d been “very healthy” and that he’d been a COVID-19 vaccine advocate. His death caused her to question the safety of the shot, however.
“I believe that people should be aware that side effects can happen, that the vaccine is not good for everyone and in this case destroyed a beautiful life, a perfect family and has affected so many people in this community.” she wrote. “Please do not let his death be in vain please save more lives my making this information news.”4
Even Viral Content Has Minor Reach
According to The New York Times,5 Facebook held off on publishing the first-quarter report for fear the findings might “look bad for the company.” Executives decided they wanted to make some “key fixes to the system” before releasing it. That’s why it wasn’t published until August.
Interestingly, the report reveals that even when something goes viral, the total number of views is still a tiny fraction of the overall content. Even the biggest accounts make up but a small portion of overall content views. Combined, the top 20 accounts with the most views during the first quarter — which included UNICEF, The Dodo and LADbible — accounted for only 1.18% of all U.S. content views.
As noted in the report, this “shows that, even though it may seem like a page or post has extensive reach on the platform, that isn’t the case when measured against the total amount of content available on the platform.”
Facebook Calls Out CCDH for Manufacturing ‘Faulty Narrative’
As you may know, an obscure one-man organization funded by dark money called the Center for Countering Digital Hate (CCDH) has published several reports, including “The Anti-Vaxx Playbook,”6 “The Disinformation Dozen”7 and “Disinformation Dozen: The Sequel,”8 in which the founder, Imran Ahmed — an unregistered foreign agent — claims to have identified the top most influential “anti-vaxxers” in the U.S.
In a completely unexpected turn of events, Facebook is now calling out the CCDH for having manufactured a faulty narrative without evidence against the 12 individuals targeted in its reports (myself included).9
This is important, seeing how the CCDH reports have been the primary “reference” source of authority used by media and government officials to smear, threaten and infringe on American citizens’ right to free speech.
The U.S. Department of Homeland Security even lists promulgating “false narratives” around COVID-19 as a top national security threat, which basically puts a “domestic terrorist” target on the backs of those of us who have been identified by the CCDH as the most prolific “superspreaders” of COVID misinformation.
As reported by GreenMed Info :10
“Google now shows an astounding 84,700 search results for CCDH’s defamatory phrase ‘disinformation dozen. ’Amazingly, this includes 16,000 news stories within the international press, approximately 100% of which are word-for-word amplifications of CCDH’s claims/defamatory statements and reported uncritically as fact.
In addition, the Surgeon General Vivek Murthy, the White House Press Secretary Jen Psaki, and president Biden all used CCDH’s report as the sole source for their own defamatory accusations, reaching a dangerous rhetorical climax on July 20th when Biden stated that these 12 individuals are literally “killing people” [by spreading misinformation].”
No Evidence to Support ‘Misinfo Superspreader’ Claim
In an August 18, 2021, Facebook report, Monika Bickert, vice president of Facebook content policy, sets the record straight, and in the process, demolishes the CCDH’s claims:11
“In recent weeks, there has been a debate about whether the global problem of COVID-19 vaccine misinformation can be solved simply by removing 12 people from social media platforms. People who have advanced this narrative contend that these 12 people are responsible for 73% of online vaccine misinformation on Facebook. There isn’t any evidence to support this claim …
That said, any amount of COVID-19 vaccine misinformation that violates our policies is too much by our standards — and we have removed over three dozen Pages, groups and Facebook or Instagram accounts linked to these 12 people, including at least one linked to each of the 12 people, for violating our policies.
We have also imposed penalties on nearly two dozen additional Pages, groups or accounts linked to these 12 people, like moving their posts lower in News Feed so fewer people see them or not recommending them to others. We’ve applied penalties to some of their website domains as well so any posts including their website content are moved lower in News Feed.
The remaining accounts associated with these individuals are not posting content that breaks our rules, have only posted a small amount of violating content, which we’ve removed, or are simply inactive.
In fact, these 12 people are responsible for about just 0.05% of all views of vaccine-related content on Facebook. This includes all vaccine-related posts they’ve shared, whether true or false, as well as URLs associated with these people.”
It’s worth restating the key point in this quote: Combined, the top 12 individuals and organizations identified by the CCDH as being responsible for a whopping 73% of vaccine misinformation on Facebook, are in fact only responsible for 0.05% of vaccine-related content — 1,460 times lower than the CCDH’s outrageous claim. That’s no small discrepancy.
CCDH Claims Blasted as Unjustified and Biased
Bickert goes on to refer directly to the CCDH report “The Disinformation Dozen,”12 stating:
“The report13 upon which the faulty narrative is based analyzed only a narrow set of 483 pieces of content over six weeks from only 30 groups, some of which are as small as 2,500 users.
They are in no way representative of the hundreds of millions of posts that people have shared about COVID-19 vaccines in the past months on Facebook.
Further, there is no explanation for how the organization behind the report identified the content they describe as ‘anti-vax’ or how they chose the 30 groups they included in their analysis. There is no justification for their claim that their data constitute a ‘representative sample’ of the content shared across our apps.”
CCDH Meets Definition of ‘Hateful Extremists’
Ironically, while the CCDH claims to “counter hate” online, and Ahmed sits on the Steering Committee of the U.K. Commission on Countering Extremism, CCDH itself actually meets the Commission’s definition of hateful extremists.14 In the 2019 Commission document, “Challenging Hateful Extremism,” the term is defined as:15
“Behaviours that can incite and amplify hate, or engage in persistent hatred, or equivocate about and make the moral case for violence; And that draw on hateful, hostile or supremacist beliefs directed at an out-group who are perceived as a threat to the wellbeing, survival or success of an in-group; And that cause, or are likely to cause, harm to individuals, communities or wider society.”
In addition, in the forward of the report, lead commissioner Sara Khan notes that “Hateful extremists seek to restrict individual liberties and curtail the fundamental freedoms that define our country.”
All of these definitions and clarifications of what hateful extremism is fit the CCDH to a T. Ahmed manufactured data to create a false narrative that 12 individuals pose a threat to the well-being and survival of the whole world, and then used that narrative to incite hate against us and curtail our freedom of speech.
Who Fact Checks the Fact Checkers?
In related news, the self-appointed arbiter of factual truths, NewsGuard, has had to backpedal in recent months and issue dozens of corrections to “fact checks” in which they’ve labeled the Wuhan lab leak theory as a debunked conspiracy theory with no basis in fact.
Since the beginning of the COVID pandemic, NewsGuard has wrongly down-rated 225 websites for articles mentioning the lab leak theory.16 In reality, there’s far more evidence to support the lab leak theory than any other theory, but it took over a year before the weight of this evidence became too obvious for the media to ignore.
NewsGuard’s erroneous fact checks were recently highlighted in an August 11, 2021, report by the American Institute for Economic Research (AIER).17
AIER decided to take a closer look at NewsGuard after receiving a request for comments on a NewsGuard fact check article regarding AIER and the Great Barrington Declaration — a statement written by public health experts from Harvard, Stanford and Oxford that calls on government to implement focused protection rather than lockdowns and self-isolation. AIERS investigation found that:18
“… NewsGuard falls far short of the very same criteria for accuracy and transparency that it claims to apply to other websites. Most of the company’s fact checkers lack basic qualifications in the scientific and social-scientific fields that they purport to arbitrate.
NewsGuard’s own track record of commentary — particularly on the Covid-19 pandemic — reveals a pattern of unreliable and misleading claims that required subsequent corrections, and analysis that regularly conflates fact with opinion journalism in rendering a judgement on a website’s content.
Furthermore, the company’s own practices fall far short of the transparency and disclosure standards it regularly applies to other websites … NewsGuard’s staff primarily evaluates scientific claims by appealing to the authority of public figures who they designate as ‘experts’ on the subject in question.
Their approach generally avoids direct examination of the evidence surrounding contested claims, and instead cherry-picks a figure to treat as an authoritative final word … many of their preferred authorities are political officeholders rather than persons trained in scientific or social-scientific methods.
By selectively curating cherry-picked political authorities rather than evaluating evidence directly, NewsGuard’s approach to fact-checking effectively sidesteps the scientific method. This strategy is rendered even more problematic by the general lack of scientific expertise within NewsGuard’s team of writers.
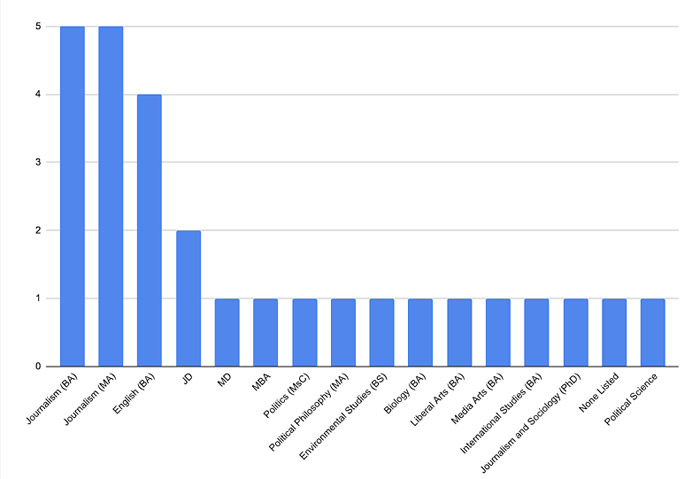
We examined the educational credentials, including the highest degree listed, for 28 publicly identified staff members on NewsGuard’s website. The company’s staff page reveals shockingly little expertise in either the hard sciences such as medicine or social sciences such as public policy, economics, and related fields …
Most NewsGuard articles on Covid-19 topics and policies are written by [NewsGuard Deputy Editor for Health, John] Gregory, whose only identified qualification is a bachelor’s degree in Media Arts … Gregory would not qualify as an expert in most of the fields he is responsible for fact-checking …
Of course, non-experts have every right to offer opinions on scientific and social-scientific matters. Whether or not they should be taken seriously as fact checkers or act as arbiters of scientific disputes is another question entirely.”
NewsGuard Staff by Field and Highest Degree Attained
NewsGuard Apologizes for Erroneous Fact Checks
After being confronted about its erroneous fact checks on the lab leak theory, NewsGuard offered the following apology in a statement sent to AIER:19
“NewsGuard either mischaracterized the sites’ claims about the lab leak theory, referred to the lab leak as a ‘conspiracy theory,’ or wrongly grouped together unproven claims about the lab leak with the separate, false claim that the COVID-19 virus was man-made without explaining that one claim was unsubstantiated, and the other was false.
NewsGuard apologizes for these errors. We have made the appropriate correction on each of the 21 labels.”
AIER commented on the apology:20
“Gregory and his colleagues appear to have simply decided that their own premature dismissal of the lab leak hypothesis equated to ‘fact’ and proceeded to penalize other sites not for factual errors, but rather for diverging from NewsGuard’s own editorial position on the same subject.
When this position turned out to be mistaken, NewsGuard pivoted to remove the errors — albeit in non-transparent ways that downplay the significance or pervasiveness of their mistake.”
NewsGuard Fails to Fulfill Its Own Credibility Criteria
In their report, AIER goes on to apply the criteria NewsGuard uses to evaluate a website’s credibility to NewsGuard itself. It’s ranking? A paltry 36.25 out of 100. According to AIER:21
“This website fails to adhere to several basic journalistic standards, and should be used with extreme caution as a source for verifying the reliability of the websites it purports to rate …
When we see fact checkers like NewsGuard, who not only fail to uphold their high-sounding principles but even publicly encourage working with the government to suppress speech, we should raise red flags.”
The NewsGuard ratings are meant to influence the reader, instructing them to disregard content with cautionary colors and cautions. That it would serve as the thought police of the technocratic establishment that seeks to silence dissent and bury information that doesn’t help move the Great Reset agenda forward is no surprise.
Especially considering its primary startup capital came from Publicis Groupe,22 a PR group that represents most of Big Pharma, including vaccine makers, and Big Tech. NewsGuard is also backed by Microsoft23 and Google.
The Publicis Groupe has been manipulating what people think about commercial products for nearly a century. Over that century, this advertising and communications firm bought or partnered with targeted advertising avenues, beginning with newspapers, followed by radio, TV, cinema and the internet.
With revenue avenues secured, Publicis’ clients and partners built a global presence that dominated the advertising world. Be it tobacco or sugar, Publicis Groupe found a way to promote and strengthen big industries. Publicis was recently sued24 for its deadly and illegal marketing of Purdue Pharma’s opioid products.
When you consider that Publicis describes its business model approach as putting clients and their needs and objectives at the center of all they do so their clients can “win and grow,” it’s easy to see what’s driving NewsGuard.
Overall, NewsGuard is just another big business aimed at keeping the chemical, drug and food industries, as well as mainstream media, intact by discrediting and eliminating unwanted competitors and analysts who empower you with information that runs counter to any given industry’s agenda.
If you’re as disturbed by censorship as I am, be sure to contact your local library today to find out if they’re one of the more than 700 libraries using NewsGuard. If they are, then ask them if they’re aware of NewsGuard’s censorship of truthful news that is now encroaching on scientific freedom and threatening the very roots of our democracy.
If your local library is using NewsGuard, it would be helpful to start a campaign to get it removed. Contact your neighbors and let them know what is happening so they can kick out this public health threat. Likewise, whenever you see someone referencing reports by the CCDH, call them out on it.
I’ve just been informed via someone senior in the vaccination authorities that they will begin VACCINATING ALL SCHOOL CHILDREN AGED 12 – 15 years old STARTING SEPTEMBER 6th 2021.
WITH OR WITHOUT YOUR CONSENT.
Children are at no measurable risk from SARS-CoV-2 & no previously healthy child has died in U.K. after infection. Not one.
The vaccines are NOT SAFE. The USA reporting system VAERS is showing around 13,000 deaths in days to a few weeks after administration. A high % occur in the first 3 days. Around 70% of serious adverse events are thromboembolic in nature (blood clotting- or bleeding-related).
We know why this is: all of the gene-based vaccines cause our bodies to manufacture the virus spike protein & that spike protein triggers blood coagulation.
The next most common type of adverse events are neurological.
Death rates per million vaccinations are running everywhere at around 60X more than any previous vaccine.
Worse, thromboembolic events such as pulmonary embolisms, appear at over 400X the typical low rate after vaccination.
These events are serious, occur at a hideously elevated level & are at least as common in young people as in elderly people. The tendency is that younger people are having MORE SEVERE adverse events than older people.
There is literally no benefit whatsoever from this intervention. As stated, the children are unquestionably NOT AT RISK & vaccinating them WILL ONLY RESULT IN PAIN, SUFFERING, LASTING INJURIES AND DEATH.
Children rarely even become symptomatic & are very poor transmitters of the virus. This isn’t theory. It’s been studied & it pretty much doesn’t happen that children bring the virus into the home. In a large study, on not one occasion was a child the ‘index case’ – the first infected person in a household.
So if you’re told “it’s to protect vulnerable family members”, THAT IS A LIE.
The information emerging over time from U.K. & Israel is now showing clearly that the vaccines DO NOT EVEN WORK WELL. If there’s any benefit, it wanes.
Finally, the vaccines ARE NOT EVEN NECESSARY. There are good, safe & effective treatments.
IF YOU PERMIT THIS TO GO AHEAD I GUARANTEE THIS: THERE WILL BE AVOIDABLE DEATHS OF PERFECTLY HEALTHY CHILDREN, and severe illnesses in ten times as many.
And for no possible benefit.
KNOWING WHAT I KNOW FROM 40 years TRAINING & PRACTISE IN TOXICOLOGY, BIOCHEMISTRY & PHARMACOLOGY, to participate in this extraordinary abuse of innocent children in our care can be classified in no other way than MURDER.
It’s up to you. If I had a secondary school age child in U.K., I would not be returning them to school next month, no matter what.
The state is going to vaccinate everyone. The gloves are off. This has never been about a virus or public health. It’s wholly about control, totalitarian & irreversible control at that, and they’re nearly there.
In a nutshell: Yesterday CDC asked its advisory committee to “recommend” the Comirnaty vaccine for 16 and 17 year olds. And it agreed, unanimously. Or pusillanimously.
The vote may seem silly or superfluous, because it had already been recommended for this age group as an EUA.
But this vote was anything but superfluous. This seemingly minor recommendation, which did not get headlines, moves the licensed Comirnaty vaccine from a place where the manufacturer is legally liable for injuries, to a berth within the Childhood Vaccine Injury Compensation Program, for which there is no manufacturer liability. Instead a $0.75 excise tax is charged per dose, which goes into a fund administered by DHHS to pay for injuries, if one is lucky enough to convince the special masters (judges) in the program that a vaccine caused your injury. Once a vaccine is recommended for children, its liability is waived no matter who receives it.
But the important part is that once this process is complete (which I expect to be only a very few weeks), Pfizer can roll out stocks of the licensed vaccine while still having its liability waived. That means that the loophole I told you about last week is being backfilled by the USG, with the help of the supine and spineless ACIP committee members, and will soon disappear.
I say spineless with true conviction, because the briefings they received yesterday were a load of fraud and hogwash. Yet no one challenged the data nor the conclusions. It is hard to believe that the lot of them are really that stupid that they believed what they heard. It is also hard to believe that none of them had a conflict of interest, which they all asserted along with their vote.
Furthermore, no one ever actually said why the vote was held: which was for liability purposes, nor that the vote would lead to mandates, which could not be implemented under the EUA.
So, it is disappointing.
Children’s Health Defense went to court today in Tennessee to challenge the FDA on issuing both a license and EUA for the same product. AFLDS also went to court today in Colorado challenging the mandate. More on these cases later.
SOTT Editors: We are publishing below, with permission, an email from a top executive at an American company whose clients include 100 of the Fortune 500 companies. The email was sent in reply to another executive asking for the writer’s thoughts on whether he plans to be vaccinated himself or mandate it for his employees as a requirement for returning to the office. All names and company references have been redacted for privacy reasons.
Unlike most of us who are worried about being on the receiving end of vaccine mandates by employers, this executive also has to worry about pressure from other executives and investors to mandate it on others. Few such business leaders are actively fighting for the rights, dignity, peace, and financial security of their employees. This exec is currently the only voice in his company opposing the madness.
Email to the executive:
Hey [REDACTED] – are you giving any thoughts to getting vaccinated with all this Delta variant stuff going on? We’ve been having management committee discussions here about mandatory vaccinations to be able to come in to the office. We have office support people coming in most days that are not vaccinated and some of those with kids don’t want to come in when they are in the office or invite clients into the office for meetings. Just curious as to how you are approaching it. Thx, [REDACTED]
The executive’s reply:
From: [REDACTED]
Date: Fri, Aug 27, 2021 at 9:56 PM
Subject: MY POV on Mandating Employee Vaccinations
To: [REDACTED]
I appreciate you reaching out. What follows is admittedly lengthy (though I do provide my “summary POV” a couple paragraphs down before I dive into supporting detail). I tried to be succinct, but practically speaking your question for me was akin to “hey, so what’s your take on management?” The analogy here being I’m passionate about both subjects so it was hard to choose between sending back a brief 2-minute POV, or filling this email with enough content fit for a university level course. I didn’t know what you had an appetite for, so I just simply did my best to try and be helpful (and heck, even had some fun while I was at it…).
My framework for this entire POV: in the famous words of W. Edwards Deming, “In God we trust. All others must bring data.” As I hope you’ve come to know me by now, I care more deeply about facts & morals than I do ideology or identity politics (for the latter I just don’t give a shit). If you give me a good reason to do something, I am 100% all over it. But if you give me either faulty reasoning or an unethical ultimatum, I simply cannot get on board out of a moral obligation to do what’s right.
So to answer your questions with that sole framework in mind, here’s my summary POV:
(#1) I still have no plans to get vaccinated anytime in the foreseeable future (unless something radically changes the risk equation), given:
(a) The virus at present poses de minimis risk for me personally (and virtually zero risk to any healthy child (a reference to your initial inquiry)); and
(b) Because these vaccines carry –> confirmed low/moderate short term — inferred moderate medium term — and expected high long-term health risk for what could be [though yet unknown] a majority of individuals who get the jab
(#2) I remain vehemently opposed to vaccine mandates for this specific virus (primarily on the basis of (i) 1b above, (ii) the medical literature, which strongly suggests that these vaccines will prolong this pandemic indefinitely through never-ending variants, and thus/therefore (iii) on moral grounds, as, if (i) and (ii) are true, then any decision to proceed with mandates would be nothing short of a descent by the West towards fascism**, the likes of which hasn’t reared its ugly head since the early 20th century. Finally, at a distant, distant second, I am against these mandates from a logistical perspective*.
*E.g., how will you account for boosters (i.e., will those who were vaccinated too far in the past e.g., January and thus have substantially waning transmission protection also be excluded from the office)? What about those who got a different jab (e.g., AstraZeneca, Sputnik, CoronaVac, etc.), each of which has varying levels of effectiveness (and varying levels of effectiveness reduction over time) against different variants? How will you handle those that already had COVID-19 (and therefore (a) have even higher immunity than the vaccinated, and (b) who face higher health risks if they get vaccinated post- natural infection)? What will you do with the immunocompromised (folks with organ transplants, lung problems or cancer patients) who got the vaccine but have low viable antibodies because they require evermore booster shots? What will you do when future variants require different jabs? I could go on, but I trust you get the point. My real question for you is, will you be responsible for coordinating monthly/quarterly management meetings to update & maintain these ever-changing mandate policies covering ever-growing future use cases?
**And if you think I’m exaggerating, look no further thanNY State Assembly Bill A416, which proposes forcibly putting carriers of COVID-19 who do not conform to the state’s medical guidelines into something akin to internment camps, where they will be forced into a treatment deemed appropriate by the state and detained indefinitely until they comply. Imagine a U.S. legislative policy so bad, thateven Russia Today was able to shit all over itas being far too draconian.And it’s not just the state of NY, but the CDC as well.
===================
Last comments before I dive into supporting details
To not lose sight of being pragmatic as it pertains to your inquiry, I want to point out that at this juncture even a discussion about vaccine mandates is mostly moot.
We already know (confirmed) that those who are vaccinated/infected carry as much viral load as the unvaccinated. Which, coupled with waning transmission prevention efficacy means for all practical intents & purposes those vaccinated and those unvaccinated pose similar risks to one another.
And this is notwithstanding even more cutting edge research (not even yet published i.e. currently pre-print in The Lancet), which suggests those vaccinated carry significantly(upwards of 200x) moreviral load than the unvaccinated (which would, if peer-reviewed, flip the risk equation on its head even further in that those vaccinated would pose far greater risk to one another than those unvaccinated). (And it is worth noting that this development would be consistent with what has been found with other vaccines — in this 2017 study, for example, it was assessed that those who were vaccinated for influenza shed 6.3x as much virus as those who are unvaccinated. Crazy stuff.)
All of this is to say, despite the nationwide pushes you’re seeing for private & federal workplace vaccination mandates (which may have made at least some sense much earlier on), such mandates are unfortunately no longer effective models at this stage, unsupported by what we now understand via the latest science. Instead, if you really want to make a difference in improving workplace safety at this juncture, I would suggest implementing either the 1st, or both, of the following policies:
(1) Everyone at the company must perform a daily (pre-commute) self-assessment health survey, whereby all individuals must confirm they are not exhibiting any of the known symptoms of COVID-19 (i.e., if you can’t smell, have fever/chills, shortness of breath, etc., you can’t come in to the office, period), without any pressure from management to respond they are symptom-free.
(2) (Optional) everyone, irrespective of vaccination status, must get tested weekly for COVID-19, such testing to be reimbursed by the company. If you test positive, you aren’t allowed to come in until you test negative.
You asked how we’re handling it, and I can tell you that we’re doing the first one at [my company], and I would recommend utilizing the second one for any in-person company events. That’s it. No mandates. Anything beyond that will lead you into a logistical nightmare (at best), foster a false sense of security as it isn’t effective (worse), and in my humble opinion, is purely unethical (worst of all, which I’d like to think is a decent enough reason not to do something) at this stage.
So anyways, all of the above is the summary of my current POV. What follows below is/are the supporting details for the conclusions I reached in my summary POV 1(a), 1(b), and 2(i) above, if you’re interested in the data.
Always happy to chat/update further as the saga continues ✌
best, [REDACTED]
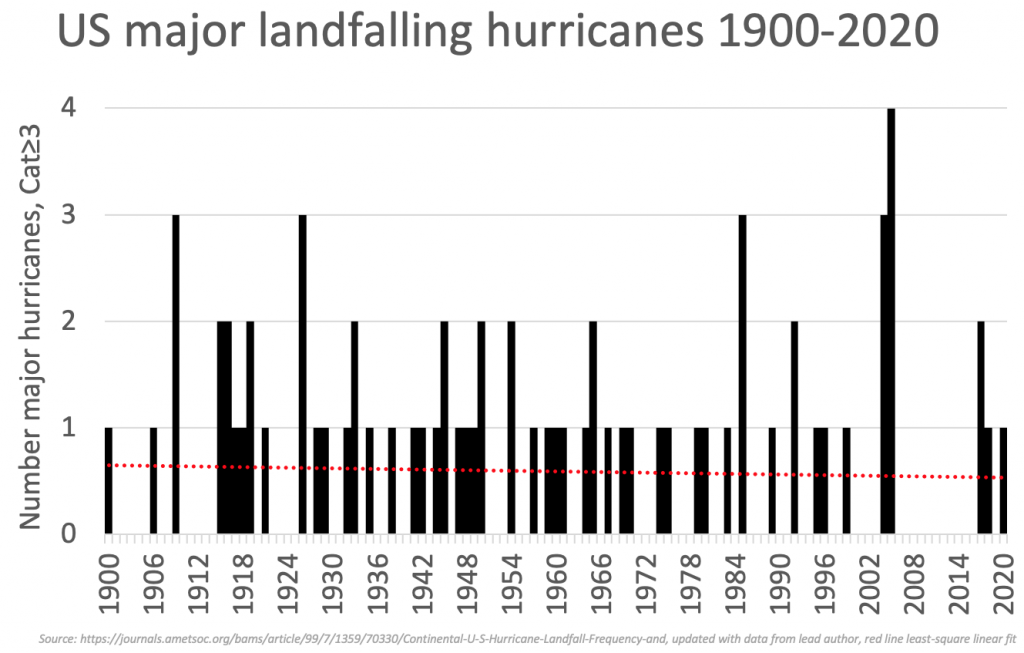
P.S. if you’re going to skip Parts 1 & 2 below*, then no worries… I get it, I probably wrote far more than you were looking for. But if indeed you do skip them, try to make it to the ‘Closing Thoughts’ section way down below — I’ve sourced a nifty chart down there that might give your colleagues pause in their ongoing discussions about mandates before they consider the unvaccinated to be idiots for whom behavioral mandates are the only appropriate solution.
*Though I highly recommend Part 1 (where it says “TWO OTHER THINGS TO CONSIDER” (then scroll to find #2)) as this contains a suggestion for how to naturally protect yourself from COVID-19.
===================
PART 1: RISK OF COVID-19 DEATH —> DE MINIMIS FOR ME
First I’ll address why I do not view COVID-19 as dangerous for me personally: from the CDC’s own data, available here, you can see current the Count of Cases and Count of Deaths by age ->
(Though before I go further, pardon me for abstaining from a lengthy discussion on the reliability of data from an organization that even Dr. Deborah Birx herself — (an individual who received a Meritorious Service Medal from the U.S. Department of Defense in 1991 and a Medal of Excellence from the CDC in 1994) — was quoted as sayingshe didn’t trust a single word from. Hmm, I wonder why she didn’t “trust” the data, could it be because they were —>overinflating “COVID-19 deaths”? <—… I digress.)
Anyways, according to the CDC, being 32, my “risk” stands at 0.14% (purely averages speaking, irrespective of the analysis below); a “starting statistic” you could call it.
The immediate issue with this data, unfortunately, is we’re only able to count cases with confirmed COVID-19 PCR (or other) test results, undercounting materially true case counts to date. As you might imagine, those asymptomatic do not test themselves regularly or out of nowhere. I mean, personally speaking, I am obviously not testing myself on any basis on any cadence — I’d only get tested if I had reason to. Thus is the reason, that the CDC already stated well early on in this pandemic that true case counts were “likely” to be upwards of 10x higher than we have documented (which they concluded based on widespread antibody testing).
Deaths in the U.S., on the other hand, are religiously tested for COVID-19, capturing the vast majority (if not nearly all) deaths, where a COVID-19 infection was present.
Using these two bits of information from the CDC, we can adjust for a “truer” baseline risk. Now, while I could exercise the luxury of taking on more than a 10x spread (because those younger tend to be more asymptomatic), I’ll be conservative just for the sake of it and just use the “10x average” figure. And so, a true starting statistic for me isn’t 0.14%, but a markedly lower 0.014%.
Next, we can use Exhibit B, taken right from the CDC website:
For… 5% of… [COVID-19] deaths, COVID-19 was the only cause mentioned on the death certificate. For deaths with conditions or causes in addition to COVID-19, on average, there were 4.0 additional conditions or causes per death.
Again, this is nothing new and has been known since very early in the pandemic, as you can see from this study for example listing the leading comorbidities as measured in NY as early as April 2020:
And herein lies my second issue with folks who preach to me that vaccines are necessary for my survival (the first being my initial lowly baseline risk).
Knock on wood, but I have no non- COVID-19 induced comorbidities — zero. My takeaway is just that: for someone like me, COVID-19 is mostly a virus known to exacerbate serious pre-existing conditions to the point of overwhelming the system definitively.
Put another way, imagine a motorcycle rider trying to assess their risk of death from riding (i.e., catching COVID-19). They see a study which puts the risk of death for those motorcycle riders who were (1) drunk (2) doing a wheelie on the highway (3) during a rainstorm, and (4) while texting with a friend (i.e., analogous to four comorbidities). It would be flawed reasoning for a rider who doesn’t do any of those things to put themselves in the same risk category as those who do. So while no one is saying motorcycles aren’t dangerous — they certainly are — they’re nowhere even in the vicinity as dangerous as riding while doing all the other things. Likewise, neither should a healthy teenager dwell on their COVID-19 risk with the same fervor as a 100 year-old morbidly obese individual with terminal cancer.
Okay, let’s revisit my personal risk again. First, I will ignore the 5% “no comorbidities” statistic above, because out of fairness I want to account for likely COVID-19 induced comorbidities like Respiratory Failure, Sepsis, etc. as well as possible ones like Renal Failure, Cardiac Arrest, and the like. So, let me simply reduce my risk not by 95%, but 57% (conservatively even rounded down further to a clean 50%), which removes just 1 non- COVID-19 induced comorbidity for my age group.
And just like that, my adjusted risk is downgraded to 0.0069% annually (annually, because it’s only once a year — after which time abetter-than-vaccinationnatural immunitykicks in for that season).
So what really is 0.0069%, you might ask? After all, we humans aren’t terribly good with numbers like that. To help you put it in perspective, consider that according to the National Highway Traffic Safety Administration, your (or my) risk of dying from a freak car accident in any given year, is 1 in 5,407 or 0.018%.
Let that sink in: based on what we know today, I personally am 268% more likely to die in a car accident tomorrow (or any day this year) than COVID-19. But do you really think that in pre-pandemic times, the “1 in 5,407” statistic kept me locked up inside my house? You think even today (in the middle of a pandemic) that figure stops me from taking a leisurely drive to grab ice cream with my nephews? or catching a movie with my brother? or — God forbid!! — hanging out with and actually talking with my friends? No!, and it never could. Because life, my friend, is about dancing in the summer rain, not cowering in fear of getting struck by lightning. But hey, maybe that’s just me…
In any case, I want to come back to your comment about concerns your colleagues have regarding young children. When we look at the statistics available (table above), the results are even more stark: for kids aged 5-11, their odds of a fatal COVID-19 infection are 1 in 137,000 when you factor in asymptomatic cases. And again, we’re talking about a risk inclusive of those with comorbidities. For kids 5-11 who are perfectly healthy, you can consider their risk nil. Okay, well obviously it could never be actually zero, because we both know sometimes kids also fall off a bike and kill themselves — that’s life. But you don’t exactly see people running around freaking out over bicycles all day long, do you? Which is ironic as hell now that we’re on the subject, consideringalmost exactly the number of kids have died from bicyclesas from COVID-19 in the same time frame.
So when I hear about folks taking their kids for a bike ride on the weekend (how awful), or worse!, maniacally driving their kids for ice cream (putting those precious kids at 5,091% (51x) the risk of death as COVID-19), but then trembling at the thought of walking into an office the following Monday because there’s an unvaccinated person there, so they feel the need to demand forcing medical decisions on those people (like getting jabs with vaccines made by companies whose rap sheets (Pfizer, J&J) would satisfy essay requirements at most colleges, approved by an organization that finds safety issues in 1/3 of its drugs post-approval), I come to the simple conclusion that common sense has left the building — it’s mass hysteria.
Alright, enough beating the completely de minimis personal risk dead horse because the point is clear. But let me add two more small things before getting to the dangers of the vaccine:
TWO OTHER THINGS TO CONSIDER
The section above looked at the whole thing purely from a mathematical risk perspective with neither proactive measures in mind, nor accounting for simple and effective (though IMO criminally suppressed) treatment options available to thwart COVID-19 risk even further.
(1) First, on the treatment side. Look, I know there was the whole “orange man (Trump) bad, the FDA disagrees” political BULLSHIT thing going on. Like I said above, I do not give a shit about the political angle of any of this. I require data, and the data could not be more ironclad on the subject matter. I will simply leave these two links here, and avoid another 5 pages in this POV on why IMO this is being criminally suppressed by federal agencies:
First, Ivermectin (links to the studies: (Link A & Link B)). Summary table as follows:
Second, Hydroxychloroquine (link to the studies). Summary table as follows:
By the way, it is worth noting I have a friend right now who has COVID-19. He has felt like shit for the past week. I sent him the studies, and he bought Ivermectin 3 days ago without a prescription from a local store I pointed him to. After a week of feeling like shit, it took him less than a day to get close to symptom free. But hey, I am not a doctor, and “your mileage may vary.” There are a dozen other treatments in addition to the ones above that aren’t getting approved for mass application, either. Go figure.. I could send you the studies if you want, but anyways let’s move on.
(2) As it pertains to the proactive side — okay, sit tight because I’m going to perform a holy miracle here and give you one of several simple things you can do to essentially ensure never needing to worry about COVID-19 again. Not for you, not for the kids, and not even for the neighbor’s dog. Ready? Okay drumroll please… . Did you catch that? If you didn’t, I’ll decipher it for you. It’s your new friend Vitamin D.
The first study is striking all on its own and worth internalizing, but unfortunately it did group an entire category called “normal” into a single bucket. FYI “normal” is what the medical world considers to be ~20ng/mL. But that’s all it is as a level: normal… but far from what we want, which is excellent.
That’s where the second study becomes helpful. It puts the explosive nature of the findings into real perspective: at levels of 25ng/mL in the study, no severe or critical hospitalized outcomes were observed.While at levels of 40ng/mL or greater, there were not even hospitalizations.
Now personally, I regard it as nothing less than a crime against humanity that neither the WHO nor CDC are PUSHING these (and dozens other peer-reviewed studies on the subject) onto the forefront of our collective media screens. But as for the reason, I must digress, because again I could go down a long and nasty rabbit hole about perverted incentives in the system in terms of why you likely haven’t seen them.
In any case, here’s what is just so awesome for me… remember when we concluded I had a higher risk of crashing & dying from my trip to the local ice cream shop than from COVID-19? Well, it just got a WHOLE lot better, because my Vitamin D levels happen to be considerably well above 40ng/mL. Which means we need to be honest with ourselves and admit that I effectively have a ZERO clinically observed risk of death from COVID-19. I mean shit…. at this point really the only way I can die of COVID-19 is by having it and then getting into a car accident. Then sure, I will die “with COVID-19” (and, as you’ll recall from the link above, they would count it!).
So my advice is as follows: get your dang sunshine first thing in the morning. Do not lockdown. In fact, I’d argue it’s what caused so many deaths. People were heavily Vitamin D deficient from sitting at home all day, and it literally increased their risk of death instead of reducing it. And what the CDC did in this regard was at best negligently or at worst intentionally, criminal, and I have nothing but disdain for the way they went about that. Don’t even get me started on the youth suicides it led to, the increases in domestic violence, increases in drug overdoses, infanticide, denial of healthcare, and let’s not dismiss the whammy of the sheer economic devastation to jobs and small businesses the world over, the bleak economic prognosis for the poorest (how convenient), and the future impact of staggering U.S. debt right here at home. All caused by the incompetence or criminality of the CDC and WHO.
Honestly — my personal advice if you want to stop worrying about COVID-19 for the rest of your life (if you still even are), would be to follow the Dan Miller protocol. Each of his bits of advice is like an extra layer of bulletproof glass on top of Kevlar against COVID-19. And remind your colleagues, too, to stop relying on the “American way” of taking a pill to solve all their problems and blaming the unvaccinated. That is not only completely debunked now as I’ve demonstrated throughout, but it is weak morally. It’s high time we all do the hard self-work of making ourselves physically resilient, and stop feebly making outward demands of others to inject into their bodies vaccines that are only now being tested, in vivo, on large numbers of human beings.
Speaking of which… perfect segway.
===================
(VERY BRIEFLY) PART 2: LONG-TERM RISKS OF [SPECIFICALLY] THE COVID-19 VACCINE –> HIGH
As I’m sure you’ll remember, a while back I mentioned I would send you a thorough, synthesized summary outlining the dangers of the COVID-19 vaccines and how the risks they carry far outweigh the risks of the virus itself. Unfortunately, I am not even a fraction of the way through the hundred plus pages of medical literature showing that conclusion — I’m still working through it. I absolutely feel terrible for not having lived up to my promise, though I’m sure you can appreciate the sheer herculean nature of synthesizing 7 months’ of research involving almost a thousand individual pieces of data, and weeks’ worth of video testimonials by researchers, all into something “succinct and digestible”, all the while working on [my company] in the middle of it all.
In any case, it would be disingenuous of me if I didn’t at least provide a sneak peak of a random assortment of links I had handy for why I will not get the vaccine (aside from the fact that COVID-19 poses no risk to me, per the first section):
Podcast: The High Wire — A Sea of Lies (in depth discussion about perverse incentives driving bad decisions by the CDC (particularly the second half of the video))
Short & Sweet: Why non-lethal pressure on the virus is bad (versus natural immunity) -> Part 1 | Part 2
+100 more videos and podcasts on the subject to anyone who asks (unsynthesized, of course)
===================
CLOSING THOUGHTS
If you made it this far and checked out even any of the content, kudos. Most folks here in the Northeast stop listening to me once I say “hey, there’s something not right here in this data” or “I’m not too worried about COVID-19 personally”. They think I’m a nut. Now, if you’ve made it this far and checked out most of the content, then I already know you’re starting to wonder if you’re losing your mind, because boy do I have a club pass with your name on it, if you’d like one.
Alas, contrary to popular belief it’s far from a nut club, despite how strong the external pressure is these days to try to make it out to be the case. Rather, It’s a club filled with precisely the very people who we’re supposed to be listening to as a society:
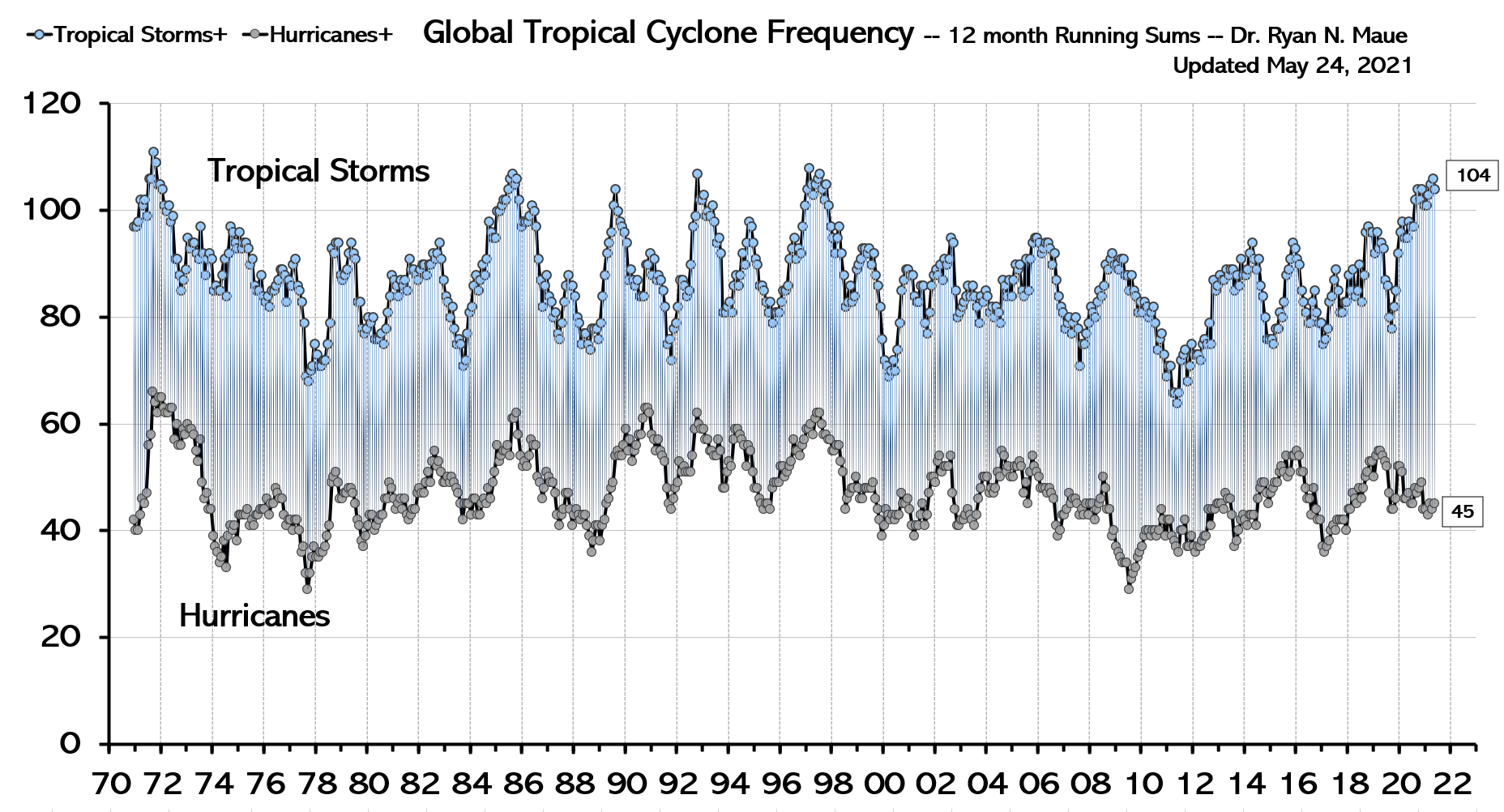
The CDC would have you believing it is just the crazy and uneducated who are most wary of their (and the FDA/WHO’s) conclusions — you know, it’s all the rednecks down south! And they’re right, it is the uneducated (left of the chart). But it is disingenuous for them to try and ignore on the nightly news research like this out of Carnegie Mellon suggesting the biggest group of those most vaccine-hesitant happen to be the smartest folks in the world — the ones I’ve certainly not been ignoring, despite their being shamed, cancelled off of social media, and publicly silenced.
Put another way, I would only posit the simple question of when in the history of the world have you ever had thousands of scientists, doctors, and researchers, some of the brightest minds* in their fields around the world sounding an alarm, and the official response be to label them all as batshit crazy and prevent them from speaking?Hint. Personally, I can’t support it. A free society must allow all open discussion without ridicule well before we dare discuss collectively forcing medical decisions on people using actual threats against their autonomy. We’re too far past that Vietnam-level of government lying bullshit that results in unholy suffering for society for this barbaric nonsense to continue, and it’s time for this country to start acting like we learned something about the importance of asking questions. I simply cannot place any trust in the idea I’m not being lied to until every scientist worth their salt has had an opportunity to speak up freely, and the nature of their concerns investigated transparently. And neither should anyone else.
*Such a fun fact it is that among this ocean of scientist voices being smeared & erased from history are (1) the guy who helped invent mRNA vaccine technology, and (2) the former Chief Scientific Officer (CSO) of Pfizer (who held that role for 16 years and focused on respiratory illnesses), both of whom are saying we have to stop vaccinations at once for those who aren’t at actual high-risk with COVID, because for everyone else they’re not only toxic & dangerous but will be the very cause of this never ending pandemic. Now I don’t know about you, but I neither invented mRNA technology nor worked at Pfizer for 16 years as CSO, but if I did, I’d sure prefer the American people heard my concerns, you know, sans the childish smear tactics part. Until then, I will not — cannot — accept any mandates on moral grounds.
And so there you have it. My opinion on mandatory vaccinations at this stage: if this were the Bubonic Plague, I’d be the first in line to get the shot. Same for Polio, Tetanus, and a whole lotta other great vaccines. But for COVID-19? Let’s just say I wouldn’t even know what to tell Saint Peter at the Pearly Gates to apologize sufficiently if I — knowing what I know now — supported a mandate. Come to think of it, there’s a quote that comes to mind here that I think is a nice way to wrap up this write-up, and commemorate those who continue to protect the rights of society:
‘The hottest places in Hell are reserved for those, who in time of moral crisis, preserve their neutrality.’ ~ unknown
========
DISCLAIMER –> OBLIGATORY
I obviously have to say this before I sign off.
At the end of the day, I’m not a doctor, I do not have an MD, a Ph.D., or any other useful acronym. All I am is an individual who values truth above hysteria & ideology. I will go wherever the truth points me to without regard for what “side” that puts me on. If it’s a contrarian side, then shit I guess I’m going to have to get in some fights. If I’m on the side of the majority, I guess I’ll rest easy. But wherever it is, I’m willing to go there, and as I said in my opening statement and reiterated to the group — I will always remain open to thoughtful and productive dialogue and my POV on every topic is subject to change through lifelong reflection. All I ask for these days is for those who disagree with me to either have the sincerity to work with me using the scientific method to get the facts on this subject, or if they have no interest in that, to let me do it alone without the constant coercion, which is how I’m sure the folks in your office who are unvaccinated, feel.
Anyways, for the actual disclaimer part: we all have to make our own decisions, do our own research (though I’m always happy to keep sending stuff I come across), and take our own risks. Freak accidents can happen, and just like I wouldn’t want to be responsible for a car accident that happens if you decide to go to a particular ice cream shop I recommend, it is the same for anything I’ve sent above and anything you or anyone you may share any of the information with do as a result of it. Always seek and follow professional, accredited advice! <– the disclaimer part.
Anyone who sees the vaccine as having more benefit than risk, should absolutely take it. I agree 100% with an 85 year-old with five comorbidities getting the jab — shit if that was me, I’d be getting quadruple jabbed walking around with a gas mask. No really, I would. Because for them the virus is actually very dangerous. And I’ve recommended it for some that I know personally would benefit from the vaccine because they are at high risk. But that’s where it ends. And not a single, inch, further.
It started with an experiment on locusts in 1991. David Raubenheimer and Stephen Simpson, two zoologists who were at the time doing research at Oxford University, wanted to know what would happen to locusts if they varied the relative proportions of protein and carbohydrate in their diets. They therefore conducted an experiment in which they fed locusts pellets containing varying proportions of protein and carbohydrate, and the results astounded them so much that they ended up determining the course of their research over the next thirty years, which they’ve chronicled in their book, Eat like the animals.
What Raubenheimer and Simpson found was that the locusts were not eating until they’d satisfied their overall need for calories. Rather they ate until they’d satisfied their need for protein, so that overall, all the locusts were consuming the same total amount of protein. This meant that the locusts on the high protein diet were consuming much less food overall than the locusts on the low protein diet. Consequently, the locusts on the high protein diet became extremely lean, while the locusts on the low protein diet became fat (which they describe in their book as equivalent to an overweight knight squeezing in to a suit of armour that is a few sizes too small).
This led Raubenheimer and Simpson to conclude that protein is the dominant macronutrient in terms of determining how much we eat – At least if we’re locusts. They wanted to see if the same pattern would be seen in other species. They started off with flies, and the results were similar, which was encouraging. But flies and locusts are relatively closely related, at least in the sense that they’re both insects. What Raubenheimer and Simpson really wanted to know was whether they’d stumbled on a general dietary principle, that could be applied to all animals.
For reasons of practicality, they next chose mice. Unlike locusts and flies, which subsist pretty much entirely on protein and carbs, mice also eat fat, so in order to get a full understanding of how macronutrients impact body composition, this variable also needed to be part of the experiment. Additionally, Raubenheimer and Simpson wanted to increase the scope of their research, to look not just at the effect of various macronutrient combinations on body composition, but also on longevity. They were also curious to see what effect differing levels of dietary fibre would have on the mice.
The experiment took five years to carry out. 856 mice were sorted in to 25 different groups, that were fed identical pellets but with varying compositions of protein, fat, carbs, and fibre. They were followed from birth to death. In terms of body composition, the results were largely as expected. The mice fed a high protein diet all became lean and muscular. When it came to the mice fed a high carb diet, however, there was more variation. Those on a high carb diet that was low in fibre grew fat, while those on a high carb diet that was high in fibre remained slim.
The fact that fibre mattered so much to the body composition of the mice on a high carb diet is interesting. It provides a reasonable explanation for why people in traditional agrarian societies usually aren’t fat, even though their diets are very high in carbohydrates, and for why the current obesity epidemic coincided with a massive increase in intake of processed foods that were rich in carbs but lacking in fibre. It also provides an explanation for why people are able to lose weight both on a paleo/carnivore/keto diet that is low in carbs, and on a vegan diet that is high in carbs but also high in fibre. Fibre appears to provide a kind of “get out of jail free” card that lets you consume lots of carbs without becoming fat.
What about fat? Fat was found to be neutral in terms of it’s effect on how much the mice ate. In other words, fat intake didn’t have any limiting effect on appetite, so the mice on a high fat low protein diet grew fat, just like the mice on a high carb low protein diet that was low in fibre. If this result were to apply also to humans (which is, of course, not necessarily the case), it would suggest that LCHF/keto diets don’t work because people are replacing carbs with fat, but rather because they’re replacing carbs with protein.
Ok, so we know how the various macronutrient combinations affected body composition. What about the effect on life span? Here, the results as presented in Eat like the animals surprised me. Alot. The longest lived mice, according to Raubenheimer and Simpson, were the ones following a high carb low protein diet. Whether they ate a high or low fibre diet didn’t seem to matter. So the fat high carb mice were actually living longer than the lean, muscular high protein mice!
Baffled by these results, I decided to go and take a look at the data, to confirm that they weren’t just trying to pull a fast one, as nutrition researchers so often do when presenting their research. Hidden away in the supplement to the published study, is this table:
Two things immediately jump out at me. The first is that the group with the longest median lifespan was on a 42% protein diet. Hardly low protein!
If instead of looking at the median lifespan, we look at the maximum, we get a different picture. We see that the extremely low protein mice did best. But their median lifespans were far more average. The authors have obviously based the claims in their book, and in their published research article, on the maximum lifespan, rather than the median. That is something I find very odd.
Personally, I assume I’m going to live an average amount of time for people like me, following my type of lifestyle. I don’t assume I’m going to be the outlier who lives to 120! The median provides a much better picture of the effect of a diet on a group than the maximum lifespan seen in a few individuals.
Apart from that, they’ve chosen an odd definition of maximum life span. They’ve defined it as the top 10% with the longest life span in each group. Which is suspicious. Why the top 10% rather than just the top individual, which would be the more common way to define “maximum”? And why not the top 20%? Or top 30%? The definition really seems to have been chosen specifically because it gave the desired result, which is what is usually referred to as “torturing the data”.
I can only imagine that they chose to base their claims on their odd definition of the maximum rather than on the more appropriate median because the maximum showed a picture more in line with their own biases, possibly shaped by an environmental or animal rights agenda, or by the fact that it’s easier to get research published if it feeds in to the dominant dogmas.
The second thing that jumps out from the table is that the mice eating a high fibre diet (i.e. with a low energy density) lived much shorter lives than the other mice. That is by far the biggest difference, much bigger than any difference induced by varying protein or carb concentrations. Does this mean fibre is deadly and should be avoided it like the plague?
Well, no. The pellets that the mice were fed only contained one fibre, cellulose, which is hardly representative of the full spectrum of fibres that exist in real food. So it’s impossible to draw any conclusions from this about the effects of fibre on longevity. What we can say is that cellulose appears to be toxic to mice.
Next, I took the data from the table and re-tabulated it in a form that would allow for easier analysis of the data, which you can see here:
So what we see is that the low protein mice do appear to live the longest, but the differences between the groups are small and hardly linear. The difference between the 5% protein mice and the 42% protein mice is only 2 weeks, equivalent to about a year and a half if translated to a human lifetime. Since there’s no evidence of a linear relationship between protein intake and life expectancy, it’s hard to say that that result isn’t just caused by chance.
If we move on to carbs, then it again isn’t clear that the high carb diet leads to a longer life. The longest lived group is actually the one consuming a moderate 29% carbs, and again, there is no evidence of a linear relationship. The same is also true for fats.
So overall, the claims the authors make about a high carb low protein diet resulting in the longest life expectancy don’t hold up to close inspection. They’ve tortured the data until they’ve gotten the result they want.
What can we conclude?
If you want to be lean, muscular, and beautiful, then you should eat a high protein diet. If you just want to lose weight and be slim, then you can either go high protein or high fiber, or do a combination of both.
Well, as long as you’re a lab mouse, that is. Whether all of this also applies to humans is harder to say for certain. The results from the experiments mentioned here and others have led Raubenheimer and Simpson to develop the “protein leverage hypothesis” of obesity, which basically states that the modern obesity epidemic is due to the fact that modern diets are lacking in protein and fibre. This has come to be one of three main hypotheses that try to explain the rise in obesity. The other two are the “carbohydrate-insulin model”, which argues that the rise in obesity is due to the high consumption of carbohydrates and their downstream effects on insulin levels and thus body fat storage, and the traditional “calories in vs calories out model”, which argues that the rise of obesity is due to the fact that modern foods taste too good and are too readily available while our lifestyles have become too sedentary. From my perspective, Raubenheimers and Simpson’s hypothesis is the one of the three that fits the known facts the best. Their book, Eat like the animals, is therefore well worth a read, even though the claims they make about diet and longevity are unsupported by the evidence they present.
A story in the Washington Post, titled “How climate change helped make Hurricane Ida one of Louisiana’s worst,” with Hurricane Ida as its news hook, asserts human caused climate change is driving more intense hurricanes. This is false. Data show tropical storms and hurricanes are neither more numerous nor more powerful than they have been historically. Not in Louisiana and not anywhere else.
By the time Hurricane Ida made landfall in Port Fourchon, La., on Sunday, it was the poster child for a climate change-driven disaster. The fast-growing, ferocious storm brought 150-mile-per-hour wind, torrential rain and several feet of storm surge to the most vulnerable part of the U.S. coast. It rivals the most powerful storm ever to strike the state.
“People there are going to get blasted,” said Kerry Emanuel, an atmospheric scientist at the Massachusetts Institute of Technology who studies the physics of hurricanes and their connection to theclimate. “This is exactly the kind of thing we’re going to have to get used to as the planet warms.”
As powerful as Ida was when made landfall, the Post and Emanuel are wrong to link Ida or any particular hurricane to climate change.
Ida may rival the most powerful hurricanes ever to strike Louisiana, but that does not make it unique. Research shows since 1957 alone five hurricanes have made landfall in Louisiana with wind speeds exceeding 150 mph. The most powerful of those five hurricanes, 1969’s Category 5 Camille, had wind speeds exceeding 190 mph. Three of the five Category 4 or higher hurricanes Louisiana has experience in the past 70 years occurred during late 1950s and 1960s during a period when the earth was undergoing a period of modest cooling, and many scientists were warning of a coming ice age.
Data from the U.S. Environmental Protection Agency and the National Oceanic and Atmospheric Administration’s National Hurricane Center (NHC) show hurricanes have neither become more numerous or more powerful during the past half-century of modest warming.
Since 1878, about six to seven hurricanes have formed in the North Atlantic every year. Roughly two per year make landfall in the United States. The total number of hurricanes (particularly after being adjusted for improvements in observation methods) and the number reaching the United States do not indicate a clear overall trend since 1878.
EPA’s conclusion that hurricanes have not become more numerous in recent years is unsurprising, because, U.N. Intergovernmental Panel on Climate Change (IPCC) 2018 interim report came to essentially the same conclusion. As illustrated in figure 1 below, IPCC data demonstrates no increasing trend in tropical cyclone or hurricane numbers.
Figure 1. Tropical cyclone frequency through August 2021. Dr. Ryan Maue
NHC data indicate hurricane impacts on the United States are at an all-time low. The United States recently went more than a decade, 2005 through 2017, without experiencing a major hurricane measuring Category 3 or higher, making landfall—the longest such period in recorded history.
This can be seen in Figure 2 below showing the large gap with no major landfalling hurricanes (Category3 or greater) in the U.S. on the right-hand side.
Figure 2. Landfalling hurricanes category 3 or greater through 2020. Dr. Roger Pielke Jr.
Also from 2009 through 2017, the United States experienced the fewest number of hurricane strikes over any eight-year period, since records have been kept.
The U.N. Intergovernmental Panel on Climate Change’s 6th Assessment Report, released in early August, also finds limited evidence human caused climate change is causing more frequent or stronger hurricanes.
“There is low confidence in most reported long-term (multidecadal to centennial) trends in TC frequency- or intensity-based metrics,” writes the IPCC.
This is not surprising. As explained in Climate at a Glance: Hurricanes, warm ocean water is just one factor driving the formation and intensification of hurricanes. Wind shear inhibits strong storms from forming and rips apart storms that have already formed. Science indicates global warming is likely to cause more wind shear in places where hurricanes form and intensify. This is precisely what happened to Henri, in mid-August, with wind shear shredding its top reducing it from a minor hurricane to a tropical depression in a relatively short period of time.
While the human toll and economic costs of Hurricane Ida have yet to be totaled up, they are likely to be great. However, contrary to the Washington Post’s article, there is no evidence the recent modest warming of the earth contributed to Ida or any other recent hurricane’s formation or intensity. The facts show, recent hurricane numbers and wind speeds are well within historical norms. The Post should stop selling unwarranted climate alarmism on the back of real human misery.
H. Sterling Burnett, Ph.D. is managing editor of Environment & Climate News and a research fellow for environment and energy policy at The Heartland Institute.
… Groupthink was extensively studied by Yale psychologist Irving L. Janis and described in his 1982 book Groupthink: Psychological Studies of Policy Decisions and Fiascoes.
Janis was curious about how teams of highly intelligent and motivated people—the “best and the brightest” as David Halberstam called them in his 1972 book of the same name—could have come up with political policy disasters like the Vietnam War, Watergate, Pearl Harbor and the Bay of Pigs. Similarly, in 2008 and 2009, we saw the best and brightest in the world’s financial sphere crash thanks to some incredibly stupid decisions, such as allowing sub-prime mortgages to people on the verge of bankruptcy.
In other words, Janis studied why and how groups of highly intelligent professional bureaucrats and, yes, even scientists, screw up, sometimes disastrously and almost always unnecessarily. The reason, Janis believed, was “groupthink.” He quotes Nietzsche’s observation that “madness is the exception in individuals but the rule in groups,” and notes that groupthink occurs when “subtle constraints … prevent a [group] member from fully exercising his critical powers and from openly expressing doubts when most others in the group appear to have reached a consensus.”[2]
Janis found that even if the group leader expresses an openness to new ideas, group members value consensus more than critical thinking; groups are thus led astray by excessive “concurrence-seeking behavior.”[3] Therefore, Janis wrote, groupthink is “a model of thinking that people engage in when they are deeply involved in a cohesive in-group, when the members’ strivings for unanimity override their motivation to realistically appraise alternative courses of action.”[4]
The groupthink syndrome
The result is what Janis calls “the groupthink syndrome.” This consists of three main categories of symptoms:
1. Overestimate of the group’s power and morality, including “an unquestioned belief in the group’s inherent morality, inclining the members to ignore the ethical or moral consequences of their actions.” [emphasis added]
2. Closed-mindedness, including a refusal to consider alternative explanations and stereotyped negative views of those who aren’t part of the group’s consensus. The group takes on a “win-lose fighting stance” toward alternative views.[5]
3. Pressure toward uniformity, including “a shared illusion of unanimity concerning judgments conforming to the majority view”; “direct pressure on any member who expresses strong arguments against any of the group’s stereotypes”; and “the emergence of self-appointed mind-guards … who protect the group from adverse information that might shatter their shared complacency about the effectiveness and morality of their decisions.”[6]
It’s obvious that alarmist climate science—as explicitly and extensively revealed in the Climatic Research Unit’s “Climategate” emails—shares all of these defects of groupthink, including a huge emphasis on maintaining consensus, a sense that because they are saving the world, alarmist climate scientists are beyond the normal moral constraints of scientific honesty (“overestimation of the group’s power and morality”), and vilification of those (“deniers”) who don’t share the consensus. … Read full article
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.