The BBC vs Donald Trump
By Freddie Attenborough | The Daily Sceptic | July 19, 2021
In March 2021, the BBC reported that one of their investigative teams had, “Been tracking the human toll of coronavirus misinformation”. During this investigation they claimed to have found links to “assaults, arsons and deaths”. Worryingly, experts also told them that, “The potential for indirect harm caused by rumours, conspiracy theories and bad health information could be much worse”. Sounds like an interesting investigation, doesn’t it? Public service output at its finest, you might think. Just the kind of article we’d all like to read.
Alas. Not quite.
The problem with the BBC is that it simply can’t help itself. Having teed an ostensibly interesting story up in this open, investigatory journalistic type of way, its authors then proceed to devote a good-ish chunk of what follows to that most favourite of all BBC pastimes, namely, implicating Donald Trump in the act of mass murder. As with the butterfly so beloved of chaos theory (you know the one: that little blighter who’s always flapping his wings and causing tsunamis to crash into the coast of Bangladesh) no sooner have the BBC shown us Trump tweeting about the FDA’s preliminary research into hydroxychloroquine as a prophylactic against Covid than the magic of non-deterministic linear physics kicks in and people all over Nigeria and Vietnam suddenly start mopping up the old bleach-based products like vacuum cleaners.
In the end, then, the only interesting thing about this article is the way it reminds us just how little time and attention the BBC have paid to exploring the link that surely must exist between Covid ‘misinformation’ (as they themselves insist on calling it) and the huge rise in cases of psychosomatic disorder – health anxiety in particular – that we’ve witnessed in the UK since the dawn of the Age of Lockdown (2020-present). Let me explain what I mean.
And to do so, let me start by asking a question: what might disinformation likely to precipitate new, or to heighten existing, levels of anxiety amongst those suffering from psychosomatic disorders look like? How, in other words, might we define such a thing? Well, perhaps we might say that it would be information that unduly exaggerated the risks associated with Covid. Perhaps we might go further and say that it would represent the risks associated with Covid in a highly misleading and/or a sensationalist way. Come to think of it, perhaps we might end up concluding that it would look rather like the BBC’s recent article, ‘Long COVID funding to unearth new treatments.’ Below is the thumbnail picture accompanying the piece.

As you can see, it depicts two masked patients, chaperoned by two masked nurses, who look unmistakably like they’re having to learn how to walk again. (And by the way, anyone who’s going to counter that it could just as plausibly be a depiction of two patients being tested for, say, oxygen carrying capacity or pulse rate during recovery from a respiratory illness like Covid would need to explain to me why it is that neither patient is shown to be wearing any tracking/monitoring equipment, and, in addition, why neither nurse is shown to be holding/studying any data monitors). The male patient in the foreground of the image looks particularly unsteady on his feet, relying heavily on the metal frame surrounding him for bodily support. One of the masked nurses stands next to him, watching his legs and feet intently, presumably scanning for any warning signs of imminent collapse or a stumble. Her right arm is stretching out towards him, and no doubt a guiding/supportive hand is resting on the patient’s shoulder. Just behind the male patient, you can also see the lower half of the wheelchair in which he will have been brought from his hospital ward and into this rehabilitation class.
But if that’s what it shows, then what kind of patient might actually need rehabilitation of this kind; rehabilitation, that is, in which patients are having to learn how to walk again? It’s the type of thing that you’d imagine is normally reserved for patients needing post-surgery rehabilitation; patients who’ve suffered spinal cord injuries, neurological disorders, car-crashes, amputations and the like. That’s big league, serious stuff. We’re essentially talking about a type of rehabilitative treatment for people who’re on the cusp of, or who’re already suffering from, life-changing injuries/illnesses.
So is this the type of treatment that people suffering from Long Covid are likely to need? I ask because as we’ve already established, it’s the type of treatment that’s depicted in the image the BBC have attached to an article entitled, “Long Covid funding to unearth new treatments” the first paragraph of which reads: “Thousands of people with ‘long Covid’ could benefit from the funding of 15 new studies of the condition, its causes and potential treatments”. To help us on the way towards answering this question, here’s what the NHS guide to the symptoms currently associated with ‘Long Covid’ has to say for itself:
Common Long Covid symptoms include:
- extreme tiredness (fatigue)
- shortness of breath
- chest pain or tightness
- problems with memory and concentration (‘brain fog’)
- difficulty sleeping (insomnia)
- heart palpitations
- dizziness
- pins and needles
- joint pain
- depression and anxiety
- tinnitus, earaches
- feeling sick, diarrhoea, stomach aches, loss of appetite
- a high temperature, cough, headaches, sore throat, changes to sense of smell or taste
- rashes
Now I’m no doctor, admittedly, but I’m not entirely satisfied that a programme of rehabilitative walking usually reserved for wheelchair bound patients in post-surgery recovery is going to prove particularly efficacious when it comes to the treatment of long Covid patients with earache, diarrhoea and changes of smell or taste. In fact, I’m not satisfied at all.
Indeed it rather seems to me that the BBC’s choice of image, when considered as an accompaniment to this particular article, might justifiably be described as misinformation; that is, as information that unduly exaggerates the risks associated with long Covid in a highly misleading or a sensationalist way.
By the way, do you like my definition of misinformation? Thanks. Perhaps it might interest you, then, to know it’s culled from the BBC’s own editorial guidelines. Specifically, therein we find “Section 3, Accuracy”, and, more particularly, “Sub-section 3.3.24”, which states that, “Reconstructions [which this image undeniably is] are when events are quite explicitly re-staged”, and that in order to abide by the BBC’s editorial guidelines, “They should normally be based on a substantial and verifiable body of evidence… [and they] should not overdramatise in a misleading or sensationalist way”.
On this basis, then, is it not the case that the BBC’s own reality-check team, that bastion of fairness and impartiality in a world gone wrong, should hold the organisation to account for spreading long Covid misinformation? Is it not an article that exaggerates and sensationalises the effects of long Covid? Further, is it not likely to generate additional, or indeed to heighten existing cases of, psychosomatic health disorders in the U.K.?
I guess if you’re the type of person who’s already suffering from heightened worry about your health, about lockdown, about physical contact with others, about viruses, about disease; I guess if you surf the web but never really read anything carefully; if you scan the thumbnails on the BBC’s news homepage but never click through to the articles; if you look at an article’s opening image and then only scan the first two or three paragraphs of text thereafter… then I guess, absolutely, it might indeed be considered ‘misinformation.’
“But isn’t this all just a little pedantic?” I hear you ask. “A bit nit-picky?” Oh, absolutely. And doesn’t it feel good to be playing the BBC at their own game for a change. So good, in fact, that you really must forgive me. I’m enjoying myself so much that I’m going to continue to be pedantic for a little while yet.
Because you see I guess, too, that if you’re prone to experiencing psychosomatic disorders of one kind of another, if you’re already well-known to your local GP surgery and A&E, then it might panic you quite a bit to think that the image the BBC have chosen to use here depicts a fate that might lie in store for you too if you ever contracted Covid and then experienced Long Covid. I guess too that if you’re that way inclined, then you might even feel you needed to take the vaccine, any vaccine, right this minute, no questions asked, jab jab jab, please, put it in me doctor, oh God, put it in me… and to hell with any kind of informed consent.
Jabbed or not, if you’re that way inclined then I guess you might nevertheless see that picture, that image of the Long Covid patient struggling to walk in the BBC’s article, and then, at some point later, get around to thinking that you’re experiencing the symptoms of Long Covid, that you’re really ill, that you’re dying, that you’re in need of immediate and very urgent medical attention, that you’ve got to go to A&E immediately because you might end up in a wheelchair unable to walk; I guess, too, that you might see that picture and then end up yo-yo-ing in and out of the healthcare system for the rest of your life, costing the taxpayer money, wasting valuable medical time, worrying that there’s a direct line of causality that “the science” has established between you coughing, you sneezing and you ending up in hospital needing a wheelchair to get you to your rehabilitative walking therapy sessions.
It’s strange, isn’t it? I mean, the BBC is normally so keen, so eager, to castigate others for disseminating what they’ve decreed to be Covid misinformation capable of causing or exacerbating existing physical disorders. Yet in the case of psychosomatic disorders – i.e. panic, hyperventilating, health anxiety, generalised anxiety, hypertension, depression, chills, gastrointestinal disturbances – they’re curiously reluctant to take up those same sanctimonious ‘fact-checking’ cudgels.
It’s a reluctance that matters, though, isn’t it? The sad and unfortunate thing about psychosomatic disorders is that those suffering from them are more likely than almost any other group in society to place unnecessary pressure on the NHS. After all, if you’re worried that you’re seriously unwell and/or in imminent danger of dying, where’s the first place you’re going to go? That’s right: a primary or secondary healthcare provider. The problem, of course, is that people who suffer from those types of disorders are neither seriously ill nor in imminent danger of dying. What they ‘are’ is suffering from severe anxiety. That’s not nothing, of course; but it’s hardly first responder or A&E type stuff, is it?
That this might constitute a problem during a global pandemic of a mild respiratory illness in which we’ve all been told to put our lives, businesses, careers on hold because the NHS is under massive existential pressure, seems obvious. If the NHS is already clogged up with respiratory tract illness and you then go and add a whole bunch of psychosomatic patients to the mix… well, you’ve got a problem, haven’t you? You’d think the BBC would care about that sort of thing, particularly given the pious, reverent tone it normally adopts when it’s representing the NHS. You’d think they’d want to provide balanced, calm, rational reportage of what was going on; reportage that was clear about the extremely low risk Covid poses to the vast majority of people in this country.
I wonder. Could it be that if we were to widen the scope of the concept of ‘misinformation’ to include not only information capable of causing physical harm, but also that likely to cause psychosomatic harm, we’d be forced to conclude that the BBC, with all its Covid exaggerations, its hyperbole, its uncritical, unreflexive treatment of “the science” handed down to it by SAGE, its failure to hold the Government to account, to approach statistics sceptically, to put case numbers into perspective, its obsession with filming death porn reports from inside hospitals (etc etc)… if we were to consider all of that as misinformation too, might we not end up concluding that the BBC has done as much damage to the psychological health and wellbeing of the nation it purports to inform, educate and entertain as Donald Trump ever did with his tweety-tweety chit-chat about preliminary research into hydroxychloroquine as a prophylactic against Covid? I wonder indeed.
Dr Freddie Attenborough is a former academic. You can see his substack account here.
Britain has a choice on Freedom Day: Embrace liberty or slide into total biosecurity tyranny
By Neil Clark | RT | July 19, 2021
Domestic Covid restrictions have ended in England, but the threat to our freedoms remains, with the government urging businesses to adopt vaccine passports. The nightclub industry’s opposition to the scheme shows the way forward.
Freedom has been restored in Merrie England after 16 months of unremitting grimness the likes of which we’ve not seen since the days of Oliver Cromwell’s Commonwealth and Matthew Hopkins’ witch-hunting. Well, sort of. No more state-mandated face masks. No more state-mandated restrictions on crowd sizes at sports venues. No more ‘social distancing’. All good things in themselves – except the message from the government has been massively confused, given that it has spent the past seven days encouraging businesses to maintain restrictions. And, having ruled out vaccine passports not so long ago, the government is now very keen on them again.
Not just for the autumn and winter, but now. Check out the new Step 4 policy document released last week. It states, “The government will work with organisations that operate large, crowded settings, where people are likely to be in close proximity to others outside their household to encourage the use of the NHS COVID Pass. If sufficient measures are not taken to limit infection, the Government may consider mandating the NHS COVID Pass in certain venues at a later date.”
That’s quite a threat, isn’t it? Basically, the government is saying, “If you don’t introduce Covid certification now, we’ll do it for you.” We’ve already had a ‘Whitehall source’ informing the Daily Mail that the scheme could be used to “keep open a much wider range of venues” over the winter, when we always get an increase of people coming down ill with flu and flu-like symptoms.
The source said, “The reason we are trialling Covid certification this summer is partly to get mass events open more safely with bigger crowds, but also partly to get people used to the idea.” Nudge nudge, wink, wink, as Monty Python might have said.
Of course, another lockdown would be ruinous for the hospitality and events sector. But business now needs to call the government’s bluff. The paradox is that rejecting Covid certification won’t make another lockdown more likely, but much less so. Because at the end of the day, this is a ‘compliance test’ and has been for the past 16 months. You defeat people who threaten to close you down, not by doing what they want but by defying them – and making them back down. Otherwise you’ll only face fresh demands.
The nightclub industry shows us the way to go. Full marks to Peter Marks, the CEO of REKOM UK, which owns 42 nightclubs and who said his venues would be operating at full capacity without the need to show a negative Covid test. Marks said that would provide a ‘barrier’ to customer enjoyment. Another big player, Tokyo Industries, has also stated it won’t be going down the Covid certification route. And there’s been rejection from the pub and hospitality industry too.
Just about the only body that seems to be enthusiastically embracing the prospect of Covid passes is football’s Premier League.
It was revealed last week that the EPL was ‘working closely’ with the government and drawing up its own plans for Covid certification. What a terrible own goal that would be. A reminder: the Public Administration and Constitutional Affairs Committee report on Covid passports was absolutely damning. The cross-party group of MPs held there was “no justification” for Covid passports and that the government had failed to make the scientific case for them.
The case for Covid passports was weak enough in June, when the report came out, but is even weaker now, as almost daily we are reading of people who have had both jabs becoming ill, or even hospitalised with Covid. If the vaccine doesn’t stop transmission – which the government admits – why are vaccine passports being promoted? Answer: there is obviously another agenda. The passports are a gateway. To something very sinister indeed.
It should set everyone’s alarm bells ringing very loudly that the most prominent public promoter of the Covid certification scheme is one Anthony Linton Blair. Last September, the man who assured us Iraq had weapons of mass destruction which could be assembled and launched within 45 minutes, said it was “common sense” to move in the direction of digitalised IDs to fight coronavirus.
In June, ‘The Blair Creature’ – to use Peter Hitchens’ memorable description – declared, “The world will move to biometric ID and they will do it because in the end, it is better for people.” But which people? The vast majority of humanity, or those who meet at Davos each year and wish to control us? A ‘temporary’ Covid pass could quite easily morph into a permanent biometric ID system – which is clearly what Blair wants. And we know what that could morph into. A ‘restricted access’ social credit system, in which behaviour which is regarded as ‘good’ by the state authorities is rewarded and that which is ‘bad’ is penalised. Imagine being denied entry to a football ground or railway station, not just because you don’t have the latest Covid booster jab, but also because your ‘social credit’ score is too low after you refused to attend a ‘training course’ on ‘Good Citizenship’?
New technology means that governments have the means to control us in a way that the worst dictators in history could only dream of. It might sound a cliché, but today, on July 19, in England we really are at a crossroads. One path is marked ‘freedom’; the other takes us to a new digital servitude from which it will be very hard, if not impossible, to escape.
Neil Clark is a journalist, writer, broadcaster and blogger. His award winning blog can be found at http://www.neilclark66.blogspot.com.
Do drug trials underestimate side effects?

By Dr Sebastian Rushworth | July 19, 2021
One commonly used trick in drug trials is to exclude any group that might make the drug look worse, such as those that are more likely to experience side effects. A good recent example of this is the covid vaccine trials, which largely excluded people with auto-immune diseases (more likely to develop an auto-immune disease after vaccination), people with allergies (more likely to have an allergic reaction to the vaccine), and, of course, the elderly (less likely to develop immunity after getting the vaccine, and more likely to become seriously sick from it).
These three groups are all frequently excluded from trials, and the exclusion is particularly galling when it comes to the elderly, because they are a big segment of the population, and they are also usually the most likely to end up actually using the drugs being tested.
When drug companies have gotten a drug approved, and move on to market the drug, they will studiously avoid mentioning the fact that large segments of the population were excluded from the trials. When drug reps show their flashy powerpoints to gatherings of doctors, say for a new drug to lower blood pressure, they will always present impressive looking graphs of benefit, and they will of course point out how safe their drug was shown to be in the trials. Not once will they mention that the groups of patients the doctors will primarily be prescribing the drug to weren’t even included in the trials.
The doctors will then happily go off and prescribe the drug to multi-morbid 90 year olds, which might explain why prescription drugs are now the third leading cause of death in the western world.
The manipulation of who is included in trials is probably one of the main reasons why findings of side effects always end up being much higher in reality than in clinical trials. It might explain, for example, why muscle pain is a massively common side effect of statins in the real world, while being vanishingly rare in the statin trials (as Dr. Malcolm Kendrick has written about in detail).
A study recently published in the Lancet Healthy Longevity sought to estimate the extent to which drug trials underestimate side effects. It was funded by the UK Medical Research Council and the Wellcome Trust. The study chose as its particular focus people being treated for high blood pressure with a certain class of blood pressure lowering drugs known as RAAS blockers (which includes all drugs with names ending in -pril and all drugs with names ending in -sartan). The advantage with looking at this particular class of drugs is that there are a ton of trials. Every major pharmaceutical company has its own RAAS-blocker. It should therefore be possible to draw relatively broad conclusions about the results – whatever they show, they apply to the entire pharmaceutical industry, not just to a few specific companies. It’s also reasonable to think that the results apply to other classes of drugs too – there’s no reason to think trials of RAAS-blockers have been done differently than trials of other drug classes.
What the study sought to do more specifically was compare the rate of serious adverse events in clinical trials of RAAS-blockers with the rate observed in the real world. A serious adverse event is any event that is potentially life threatening or that results in death, hospitalization or lasting disability. If a trial has been designed in such a way that it is representative of reality, then the rate of serious adverse events in the trial should largely mirror that seen in the real world.
110 trials of RAAS-blockers were identified by the researchers. Of these, 11 were specifically designed to look at older people (i.e. didn’t recruit anyone under the age of 60). The data on serious adverse events from these 110 trials was extracted and compared to real world data on deaths and hospitalizations taken from a UK government funded database of 55,000 people living in Wales, who were being treated with RAAS-blockers. Deaths and hospitalizations are not exactly the same thing as serious adverse events (which as mentioned above also include “life threatening events”, and could for example include someone who is treated in an emergency department after a fall but not admitted to the hospital), but they’re close enough to allow a reasonable comparison.
So, what were the results?
Let’s begin with comparing the trials of older people with the “standard” trials. The relative rate of serious adverse events in the trials of older people was 76% higher than the rate in the standard trials. This shows the importance of including elderly people in drug trials – they are much more likely to experience adverse events of all kinds (including those actually caused by the drug being tested), and excluding them will therefore likely underestimate side effects.
Considering that many of the drugs in common use show marginal benefits at best (statins have, for example, only been shown to prolong life by a few days on average), this is important information. Why? Because a drug that is beneficial, on balance, to a fifty year old, who has a fully functioning kidney and liver, and is therefore unlikely to suffer side effects, could easily be harmful, on balance, to an 80 year old.
That’s why drug studies done on younger people should not be used to guide treatment of older people. No shock there. Everyone already knows that we shouldn’t be extrapolating results from one group to another (even though it happens all the time, as we’ve seen most recently with the covid vaccine trials).
Next we come to the more important, and perhaps more shocking finding.
The real world patients were between 300% and 400% more likely to experience a serious event than the participants in the trials! That is in spite of the fact that the trials, as mentioned above, were using a broader definition of what constituted a serious event. If the trials were representative of reality, then they should have a higher rate of events than is seen in the real world data. Instead they have a rate that is several times lower!
Interestingly, the trials of older people were just as far from the real world results as the trials of younger people. Clearly, doing trials on the elderly is not enough on its own to produce trials that are representative of reality. What’s happening here exactly?
There are three possible explanations, as far as I can see. The first explanation is that the trials are representative of reality, but that the Welsh die and are hospitalized at a rate that is several times higher than people in the countries where the studies were conducted. Many of the trials were conducted in the US, not in Wales. But Wales has a higher life expectancy than the United States, so that seems unlikely. I think we can discount that explanation.
The second explanation is that the trials are unrepresentative in so many different ways that just correcting the age issue doesn’t make a noticeable difference. That’s probably part of the explanation. The average age even in the trials of “older people” was 73, which isn’t very old from my perspective. And those 73 year olds included in the trials were probably at the healthier end of the spectrum.
The third, more sinister explanation, is that the pharmaceutical companies are hiding serious adverse events… But wait a minute, the trials are randomized and blinded, so the people running the drug trials have no way of knowing if someone experiencing a possible side effect is in the treatment group or the placebo group, right?
Yes, that’s right, so the easiest solution, if you want to avoid finding nasty side effects, is to not report them, regardless of which treatment group the participant is in. That will cut down on total adverse events in both groups, which will make any difference between the groups that does exist smaller in absolute terms, and also less likely to reach the level of statistical significance. Voila – the treatment group and the placebo group end up having similar rates of side effects, and the drug company can conclude that the drug is completely safe.
Is that what’s happened here? Are the pharmaceutical companies hiding adverse events? Well, it’s very strange that the real world data shows a rate of serious adverse events that is several times higher than is found in the trials. It’s hard to see how that massive difference could be explained in any other way.
So, how big a problem is this?
Big. Very big. It should shake the very foundations of evidence based medicine. If the drug trials and the real world data show such wildly different rates of adverse events, then it really begs the question how much we can trust the trials at all. It would be perfectly reasonable in this situation to say that all “evidence” produced by pharmaceutical companies is so suspect that it should be dismissed out of hand, and that only independently funded trials should be used as a basis for medical treatment decisions.
The problem with that is that it would mean saying goodbye to most of the trials that form the basis of modern medical treatment, and there is not much to replace them with. This issue could be solved over the longer term through large tax payer funded investments in new independent trials. But there’s no quick fix.
The problem is most acute when it comes to the many drugs in common use that only show marginal benefits, such as statins. If the rate of side effects is actually 300% to 400% higher than seen in the trials, then the harms of these drugs could easily outweigh the benefits. In other words, the cost-benefit calculation could shift entirely for many of the most commonly used drugs.
Ok, let’s wrap this up. What can we conclude?
Drug trials do no accurately represent rates of adverse events. It is likely that the true rate of side effects is often many times higher than that seen in drug trials.
The WHO Declares all PCR Tests at High CT to be Potentially 100% False Positives
By Judy Wilyman PhD | Vaccine Decisions | July 13, 2021
In December 2020 the WHO declared that any result from a RT-PCR test that was amplified at a high cycle threshold (CT) e.g. above 35 CT is potentially 100% false positive. This leads us to question all the reported ‘cases’ of COVID19 disease in Australia in 2020. This is because Australia has reported that it uses this PCR test at a CT of 40-45 and most of the reported ‘cases’ were people without symptoms.
The question now is ‘What cycle threshold is the Australian government using in 2021?’ Has it been reduced at the same time as the vaccine was introduced to give the appearance that the vaccine has caused a decline in the cases of this disease?
The WHO says that in 2021 a manual readjustment of the PCR positivity threshold must be done to account for background noise in specimens with high cycle thresholds.
There is no transparency in the use of this test that is now allowing government’s globally to claim that healthy people, without disease symptoms, are an asymptomatic case of disease. This also enables the government to claim that healthy people are a risk to society. This is criminal and this PCR test is not a diagnostic tool for any disease.
Many doctors and scientists are stating this and they are being ignored and censored. Here is the inventor of the test, Kary Mullis, also stating ‘it is not a diagnostic test‘. It should never be used when symptoms are not also present.
Traditionally doctors were taught to diagnose disease on a collection of symptoms and the PCR test was sometimes a supportive, but not a diagnostic, tool. This has all changed in 2020 to be able to claim that healthy people are now the cause of these diseases and this has been achieved without having to provide any supportive evidence for this claim.
In addition, it is these ‘cases’ that have been used by the government to enact the emergency powers. Yet the definition of a pandemic that is based on an increase in ‘cases’ of a disease has not been validated by the scientific community. It is not a scientific definition if it has not been validated by the community of scientists – not just elite individuals.
The case-tracing of healthy people with QR codes is fraudulent and it is enabling more ‘cases’ of disease to be obtained and more people to be locked up and falsely declared a ‘case’ of disease. This is industry-pseudoscience and it has all come about because the WHO allowed a small group of individuals, with financial conflicts of interest with industry, to adopt an unscientific definition of a ‘global pandemic’.
This makes the use of the emergency powers invalid and all the directives that have been enacted to control this non-pandemic of a flu-like illness. Please read the full article describing the unscientific definition of a pandemic that has been used by governments and also watch the interview with Elizabeth Hart on Asia Pacific Today. This interview describes the full extent of the Australian government’s conflicts of interest in promoting an untested drug in the population. She also describes the complicity of the mainstream media and research institutions in this fabricated and well planned ‘pandemic’ event.
This crime against the population has also been perpetuated by governments deliberately suppressing the treatments for respiratory viruses that are known to be beneficial. Here is Craig Kelly presenting his evidence of this suppression in an empty Australian parliament. This picture illustrates the type of ‘democracy’ that we have in Australia today. The people’s voice is not being heard by our government.
In this video, Dr. David Martin explains to the International Criminal Court that there was nothing novel about the 2019 coronavirus. This is because it had been patented between 2008 – 2017 under gain of function research carried out in the US and in Wuhan, China. In addition, the fact that it was a mutated coronavirus means that humans would be expected to have some previous immunity to this virus because these are a family of common respiratory viruses that cause the common cold.
It is now clear that this is a ‘pandemic’ in name only. This is why there is no evidence of enormous numbers of deaths and illness in the community. The WHO could not have declared this to be a ‘global pandemic’ in 2020, if the definition of a pandemic had not been changed in 2009.
The ‘cases’ of disease that the media is presenting are healthy people who have had a PCR test but have no symptoms. It is these cases in healthy people that are being used to close borders and quarantine healthy people. This is a media campaign using statistics out of context to encourage the community to accept the governments new regulations that restrict our fundamental rights and freedoms, ultimately harming our health and wellbeing.
Is the Delta variant spreading only in highly vaccinated countries? No.

Does Delta spread only in vaccinated countries? No. (Corona Realism)
Swiss Policy Research | July 18, 2021
A highly viral tweet by “Corona Realism” is making the following claim: “Something really odd is going on: In Europe we are seeing surges at many places where most of the population has already been vaccinated. At the same time, the 15 least vaccinated countries don‘t seem to face any problem. At some point, denying this problem will get painful.”
In reality, the “least vaccinated countries” shown above are simply the Eastern European countries, whose infection cycle has always been delayed compared to Western Europe. They already missed the first spring wave in 2020, which led to the notorious misinterpretation that they were protected by (useless) face masks. Back then, the chief pathologist of Bulgaria famously claimed that covid was a hoax; today, Bulgaria has one of the highest covid death rates in Europe. Vaccination rates in Eastern Europe are lower than in Western Europe primarily for economic reasons.
To make the deception work, “Corona Realism” had to leave out some highly vaccinated countries in Eastern Europe (notably Hungary, Poland and Czechia), whose infection rates are as low as in the rest of Eastern Europe; and he had to leave out the many countries with a low vaccination rate severely affected by Delta, notably Russia as well as many Asian and even African countries. In fact, in many countries with a low vaccination rate, Delta covid deaths have reached an all-time record level.
In conclusion, while many “public health experts” got almost everything wrong during the covid pandemic, skeptics should remain careful not to fall for some of the same fallacies.
See also: “Vaccine failure”? Not really. (updated section on several false claims)
Figure: Delta deaths in some Southeast Asian countries
Delta deaths in some Southeast Asian countries with a low vaccination rate.

Delta deaths in some Southeast Asian countries (OWD)
See also:
Rotten To The Core
NOT A LOT OF PEOPLE KNOW THAT | JULY 18, 2021
There has been a longstanding concern about blatant bias at the BBC, not least in matters of climate change. This certainly dates back at least to January 2006, when they held a seminar of “top scientific experts” to advise them on climate change. The BBC fought tooth and nail to conceal the identity of these experts, but it was subsequently discovered that they were not experts at all, but the usual collection of green lobbyists.
Ever since, the BBC’s coverage of global warming has been woefully one sided and at times inaccurate,
This year they have been publishing a monthly feature, Then and Now, purportedly showing how climate has been changing in a warming world.
One article looked at the recent drought in California, while another claimed that the Victoria Falls had dried up. Both implied that climate change was to blame, with the usual weasel words that while one weather event cannot be linked to climate change, “scientists” say that such events are likely to get worse with global warming.
However both stories omitted crucial information, which would have shown such claims to be nonsensical and untruthful.

https://www.bbc.co.uk/news/science-environment-56902340
California, for instance, has had droughts in the 20thC every bit as bad as the current one. Moreover the official data clearly shows megadroughts there were much worse for much of the last thousand years or so. In short, California is a land of drought. The modest amount of warming there since the Little Ice Age has altered nothing.

The BBC claims about the Victoria Falls were even more absurd. For a start, the Falls did not run dry; every dry season lake levels drop. As the Zambian side is at a higher elevation, the Falls there dry up, while continuing at the other end. This happens every year, but the BBC deceitfully misled readers by showing a split image comparing Jan 2019 with Dec 2019. In January every year water levels rise sharply, and Jan 2020 was no exception.
It is certainly true that there was a drought in the region in 2019, and water levels were lower than average. But the Zambesi River Authority say that there have been six occasions since 1914 when water levels were lower, the worst being in 1995.
Just as with California, the BBC have picked on a drought, but ignored all of the data showing that they are both natural events, with no evidence that droughts are getting more severe or common.
This sort of misreporting of the Victoria Falls is of extreme concern to Zambia’s tourist industry and local businesses, who are naturally worried that tourists may stop visiting if they think the Falls are no longer there.
Which brings us to the point of the story. I complained to the BBC that both stories were grossly misleading and omitted crucial information.
Complaints to the BBC go through three stages. The first response appears to be written by the office junior, who tries to fob you off with a few bland statements.
If you are unhappy, you can resubmit the complaint, which usually gets the same response, though dressed up in sciency sounding language.
Finally you can appeal to the Executive Complaints Unit.
As is usually the case, I effectively received the same reply at all three stages, viz:
- There was a drought
- “Scientists say” climate change is making droughts worse
None of the replies actually addressed my complaint, that the actual data shows droughts are not unusual or getting worse at either location.
The real issue here of course is that the BBC Complaints Dept is all in house, even the ECU. In effect the BBC is marking its own homework.
In theory it is possible to appeal to OFCOM. In practice however they have no obligation to investigate, and would only consider doing so for substantive cases.
Clearly BBC bias will never be addressed until they are subject to a fully independent process, just as the press is.
In the meantime, if Tim Davie is serious about cleaning the stables, he should start by taking his axe to the bloated, fourteen strong Environmental Dept, which is now clearly out of control.
Instances of bias and misinformation, such as these two, are now commonplace in their output, and they seem to believe that they don’t even have to pay lip service to editorial guidelines anymore.
Infections in the Vaccinated Overtake Those in the Unvaccinated For the First Time – But the Graph is Removed From the ZOE App Report
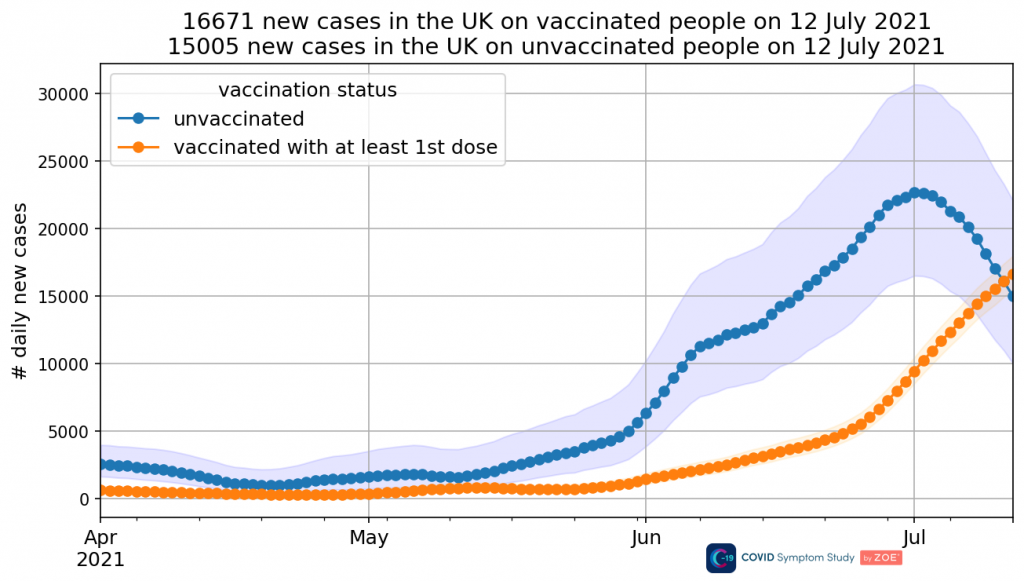
By Will Jones • Lockdown Sceptics • July 17, 2021
Health Secretary Sajid Javid has tested positive for SARS-CoV-2, despite being vaccinated – and he is far from alone. The latest ZOE data shows that, as of July 12th, infections in the vaccinated (with at least one dose) in the U.K. now outnumber those in the unvaccinated for the first time, as the former continue to surge while the latter plummet (see above). (Note that 68% of the population has had at least one vaccine dose, so there are still at this stage disproportionately more new infections in the unvaccinated, though on current trends that may soon change.)
At what point will the Government accept that these vaccines have limited efficacy in preventing infection and transmission, and thus the whole rationale of being vaccinated to protect others – vaccine passports, compulsory vaccination, and so on – is suspect?
The above graph was in yesterday’s report, so I downloaded today’s report (you can get it by signing up to the app and reporting your symptoms) to get the new update. I was dismayed to find the graph was gone. At the bottom, a note explains:
Removed incidence graph by vaccination status from the report as there are very few unvaccinated users in the infection survey, the Confidence Intervals are very wide and the trend for unvaccinated people is no longer representative.
Which I would say is very convenient, just as infections in the vaccinated became the majority. Perhaps ZOE should try to recruit some more unvaccinated people for its survey, so it can continue to report on this as well as have a control group for its vaccine data? That would seem the scientific thing to do, rather than just stop reporting it because it is suddenly “no longer representative”.
It’s doubly odd because Tim Spector, lead scientist on the ZOE app, made the decline among the unvaccinated a feature of his video this week. So the realisation that the trend is “no longer representative” appears to have been rather sudden, even invalidating the contents of a ZOE ‘data release‘ two days earlier.
It seems we will never know how the story ends, which is a shame and a missed opportunity for ZOE.

ZOE data continues to suggest the current Covid surge is peaking and possibly even beginning to decline in the U.K., at least outside England (see above). Yet this is at odds with the daily Covid reports from the Government, which show continued growth.

UK positive tests by date reported (HMG)
Why the discrepancy? Is it because the Government figures include all the lateral flow tests that schoolchildren are taking as they isolate? 839,100 children – 11.2% of the total pupil population, more than one in 10 – were absent from state schools for Covid-related reasons on July 8th. All of them will have been tested and this will be picking up asymptomatic or mild infections that would usually not be noticed. ZOE data is symptom based, with a confirmatory PCR test, so would not be affected by surges in lateral flow testing among schoolchildren picking up asymptomatic infections.
Whatever the explanation, one to watch.
Featured Video
House Resolution Calls for Tech Companies to Censor Speech
or go to
Aletho News Archives – Video-Images
From the Archives
Israel’s recurring use of terror on civilians

By Bob Finch | January 26, 2009
Insanely disproportionate use of violence against unarmed civilians… continue
Blog Roll
 Aletho News
Aletho News- NATO courts screenwriters to embed alliance messaging in film, TV
- Iran replaces UAE ports with Pakistan corridor to break US blockade
- Iran sets one-month deadline for end to US-Israeli war, blockade: Report
- At the edge of the Strait: A superpower in a narrow sea
- Iran unveils new control measures over Strait of Hormuz transit
- House Resolution Calls for Tech Companies to Censor Speech
- Ceasefire no longer viable after 200 days of Israeli violations: Hamas
- Israeli strikes intensify across southern Lebanon, casualties reported
- Left in Disbelief: Israel in Panic over Hezbollah FPV Drone Nightmare
- Trump Taps Israel Lobbyist From Mossad Cutout FDD To Join Iran Negotiations
- If Americans Knew
- As Palestinians die, Ben-Gvir celebrates birthday with golden noose cake – Daily Update
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- No Tricks Zone
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
