Photoshopping, fraud and circular logic in research

By Mike Hearn | Daily Sceptic | July 22, 2021
It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgement of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine.
Check out this image from a peer reviewed research paper that supposedly shows skin lesions being treated by a laser:

Left: before treatment for keratoses. Right: after they were airbrushed out. (image diff is available here)
On being challenged the authors said:
The photograph was taken in the same room with a similar environment; unfortunately the patient wore the same shirt.
The journal found this explanation acceptable and forwarded the response to the complainants.
It’s becoming clear that science has major difficulties with not only a flood of incorrect and intellectually fraudulent claims, but also literally faked, entirely made up papers with random data, imaginary experiments and photoshopped images in them. Some of these papers are sold by organised gangs to Chinese doctors who need them to get promoted. But others come from really sketchy outfits like (sigh) the National Health Service, to whom we owe the masterpiece seen above.
The British Government hasn’t noticed that its doctors are massaging medical evidence. Instead this example comes from Elizabeth Bik, who runs a blog where she and a few other volunteers try to spot clusters of fraudulent papers. She embarrassed the journal in public here, and the paper was finally retracted. But she’s just a volunteer who raises money on Patreon for her work. Here’s her assessment of what’s going on:
Science has a huge problem: 100s (1000s?) of science papers with obvious photoshops that have been reported, but that are all swept under the proverbial rug, with no action or only an author-friendly correction… There are dozens of examples where journals rather accept a clean (better photoshopped?) figure redo than asking the authors for a thorough explanation.
As the only people trying to spot these fake papers are bloggers, we can safely assume that far larger numbers of papers are fake than the “thousands” they have already found and reported. For example,
0.04% of papers are retracted. At least 1.9% of papers have duplicate images “suggestive of deliberate manipulation”. About 2.5% of scientists admit to fraud, and they estimate that 10% of other scientists have committed fraud.
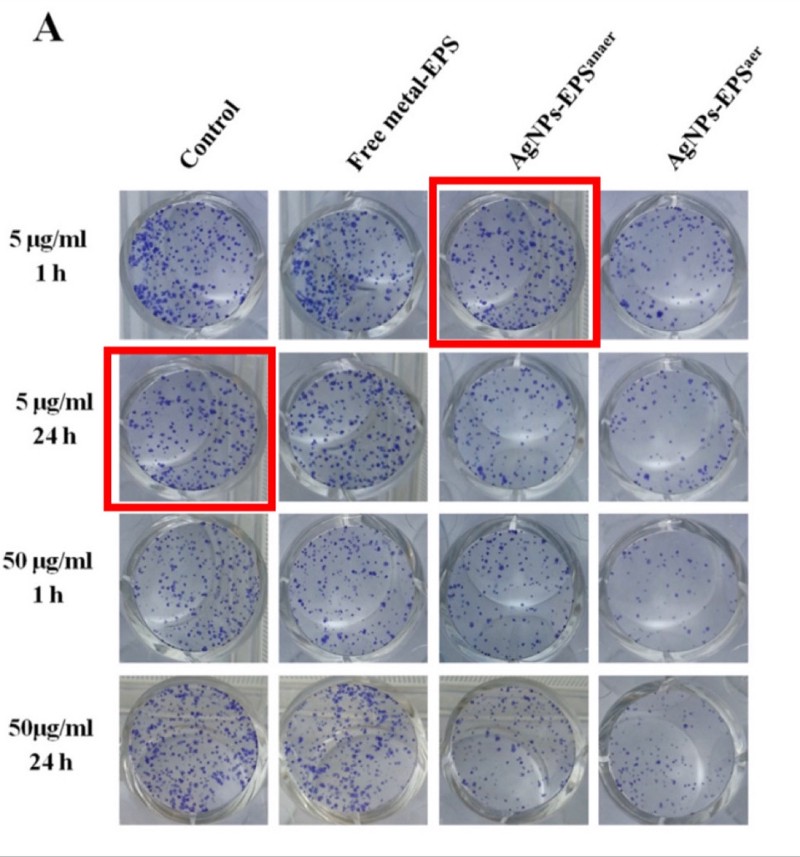
Photos of supposedly different samples in which two images are identical. From “Anticancer activity of biogenerated silver nanoparticles: an integrated proteomic investigation”. The journal investigated and concluded that this is fine.
It’s been known for years that a lot of claims made by scientists can’t be replicated. In some fields, the majority of all claims appear to not replicate due to a large mix of issues like overly lax thresholds for claiming statistical significance, poor study design and other somewhat subtle errors. But how much research is deliberate falsehood?
The sad truth is the size of the fraud problem is entirely unknown because the institutions of science have absolutely no mechanisms to detect bad behaviour whatsoever. Academia is dominated by (and largely originated) the same ideology calling for the total defunding of the police, so no surprise that they just assume everyone has absolute integrity all the time: research claims are constantly accepted at face value even when obviously nonsensical or fake. Deceptive research sails through peer review, gets published, cited and then incorporated into decision making. There are no rules and it’d be pointless to make any because there’s nobody to enforce them: universities are notorious for solidly defending fraudulent professors.
So let’s turn over the rock and see what crawls out. We’ll start with China and then turn our attention back to more western types of deception.
Chinese fraud studios
In 2018, the U.S. National Science Foundation announced that: “For the first time, China has overtaken the United States in terms of the total number of science publications.” Should the USA worry about this? Perhaps not. After some bloggers exposed an industrial research-faking operation that had generated at least 600 papers about experiments that never happened, a Chinese doctor reached out to beg for mercy:
Hello teacher, yesterday you disclosed that there were some doctors having fraudulent pictures in their papers. This has raised attention. As one of these doctors, I kindly ask you to please leave us alone as soon as possible… Without papers, you don’t get promotion; without a promotion, you can hardly feed your family… You expose us but there are thousands of other people doing the same. As long as the system remains the same and the rules of the game remain the same, similar acts of faking data are for sure to go on. This time you exposed us, probably costing us our job. For the sake of Chinese doctors as a whole, especially for us young doctors, please be considerate. We really have no choice, please!
Note the belief that “thousands of other people” are doing the same, and that these doctors need more than one paper to keep being promoted, so the 600 found so far is surely the tip of an iceberg given China’s size. There are about 3.8 million doctors in China implying that there are quite possibly tens of thousands, maybe hundreds of thousands of these things in circulation.
The fake papers are remarkable:
- They are so good they are undetectable in isolation. The NHS photo is an aberration – normally these papers get spotted by noticing re-used technical images across papers that claim to be different experiments by different people. The fake papers are probably produced by real scientists with access to real lab equipment. The use of spammy-looking Gmail accounts is also a signal because Gmail is banned in China (e.g.
BrendaWillingham12192@gmail.com,RosettajKirkland3814@gmail.com,CaseyPeiffer8311@gmail.com). The reliance on bot-generated Gmail accounts implies enormous scale. - They are peer reviewed and published in western journals. For instance, the Journal of Cellular Biochemistry by Wiley or Biomedicine & Pharmacotherapy by Elsevier. They claim to be doing advanced micro-biology on serious diseases: a typical title is something like “MicroRNA-125b promotes neurons cell apoptosis and Tau phosphorylation in Alzheimer’s disease”. Journals have no way to detect these papers and aren’t trying to develop any.
- Some of them present traditional Chinese medicine as scientific. TCM is more or less the Chinese equivalent of homeopathy with lots of herbal remedies, eating body parts of exotic animals to cure erectile dysfunction, and so on. But the Chinese Government is obsessed with it and thinks it’s the same as normal medicine. From the top down, Chinese scientists are expected to produce papers claiming that TCM works, and they do! Mostly this stuff stays in Chinese but the ever increasing reliance of western universities on Chinese funding means it’s now finding its way into the English language literature as well, e.g. “Probing the Qi of traditional Chinese herbal medicines by the biological synthesis of nano-Au” was published by the Royal Society of Chemistry.

Advert by a research faking operation. Credit to “Smut Clyde” and “TigerBB8”.
Most western scientists are too clever to buy a completely fake paper (or so we hope). But their promotion incentives are identical, and there are other techniques that let you publish as many fake papers as you want. Let’s turn our attention to…
Impossible numbers in western science
The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue.
Richard Horton, editor of the Lancet
How many scientists just make up their data? A well known recent case of this was the Surgisphere scandal, in which a paper appeared in The Lancet that claimed to be based on a proprietary dataset of nearly 100,000 COVID-19 patients across over 670 U.S. hospitals. This figure was larger than the official case counts of some entire continents at the time, and there was no reason for hospitals to share tightly controlled medical data with a random company nobody had heard of, so the claim was implausible on its face. Sure enough, when challenged it turned out none of the authors had ever actually seen the data, just summaries of it provided by one guy, who on investigation had a long track record of dishonesty. The Lancet probably accepted this paper because it made Trump look bad and the editor (Horton, quoted above) appears to hate Trump more than he hates bad science.
There are some other cases like this that came to light over the years, like the story of Brian Wansink, or that of Paolo Macchiarini, who left a trail of dead patients in his wake. But while anecdotes about individual cases are interesting, can we be more rigorous?
One clue comes from automated tools that scan research papers looking for mathematically impossible numbers, which can sometimes be detected even in the absence of the raw original data. In recent years a few such tools have been developed and deployed, mostly against psychology and food science.
- The statcheck program showed that “half of all published psychology papers… contained at least one p-value that was inconsistent with its test”.
- The GRIM program showed that of the papers it could verify, around half contained averages that weren’t possible given the sample sizes, and more than 20% contained multiple such inconsistencies.
- The SPRITE program detected various experiments on food that would have required subjects to eat implausible quantities (e.g. a child needing to eat 60 carrots in a single sitting, or 3/4 kilogram of crisps).
Being flagged by a stats checker doesn’t guarantee the data is made up: GRIM can detect simple mistakes like typos and SPRITE requires common sense to detect that something is wrong (i.e., no child will eat a plate of 60 carrots). But when there are multiple such problems in a single paper, things start to look more suspicious. The fact that half of all papers had incorrect data in them is concerning, especially because it seems to match Richard Horton’s intuitive guess at how much science is simply untrue. And the GRIM paper revealed a deeper problem: more than half of the scientists refused to provide the raw data for further checking, even though they had agreed to share it as a condition of being published. This is rather suspicious.
One of the difficulties with detecting scientific fraud is that the line between dishonesty and simple absurdity can get quite blurry. Sometimes scientists “calculate” data that is clearly wrong, but don’t actually try to hide or it may even admit to it in the paper, knowing full well that nobody cares and nonsensical data won’t actually matter. Here’s an example from a COVID modelling paper:
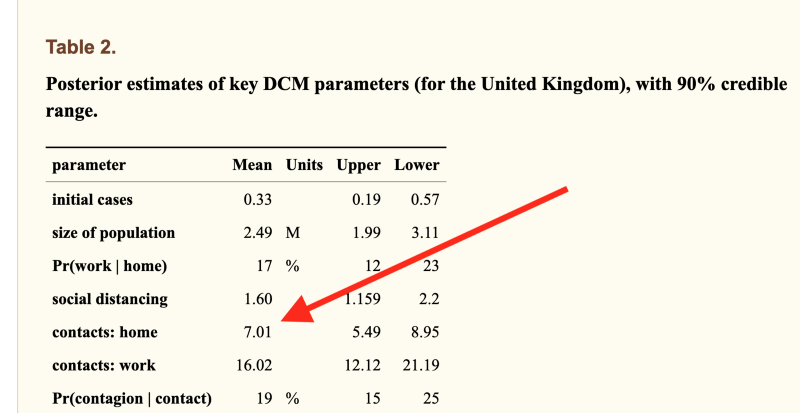
The model was allowed to calculate that the average Brit must live with 7 other people, because it couldn’t obtain data fit otherwise (actual number=2.4). This one comes from University College London, is written by 12 neuroscientists, passed peer review and has 37 citations. The peer reviewer noticed that the incorrect number was in the paper but signed off on it anyway.
For decades psychiatrists published research into the “gene for depression” 5-HTTLPR. They created an entire literature not only linking the gene to depression but explaining how it worked, linking it to parenting styles, developing treatments based up on it. Over 450 papers were published on the topic. Eventually a geneticist discovered what they were doing and used DNA databanks to point out that none of those papers could possibly be true.
Sometimes numbers aren’t “wrong” but are instead logically vacuous. The Flaxman et al paper from Imperial College that tried to prove lockdowns work had the usual problem of statistically implausible numbers, but more importantly was built on circular logic: their model assumed only government interventions could end epidemics. This is obviously nonsense and they breezily admitted it in the paper, where they said their work was “illustrative only” and that “in reality even in the absence of government interventions we would expect Rt to decrease”. No problem: this fictional illustration got published in Nature and the authors presented the model’s outputs as scientific proof of their own assumption to the media. The paper is vacuous mathematical obfuscation, but scientists either can’t tell or don’t care: it has racked up over 1,300 citations and the number is still growing rapidly. To put that number in perspective, in physics the top 1% of all researchers have around 2,000 citations over their entire career.
Time to assume that health research is fraudulent until proven otherwise?
Earlier this month, the BMJ published an astounding blog post with the same title as this section. There’s no need to add anything because simply quoting it is sufficient:
The anaesthetist John Carlisle analysed 526 trials submitted to Anaesthesia and found that… when he was able to examine individual patient data in 153 studies, 67 (44%) had untrustworthy data and 40 (26%) were zombie trials… [Ben] Mol’s best guess is that about 20% of trials are false. Very few of these papers are retracted.
We have now reached a point where those doing systematic reviews must start by assuming that a study is fraudulent until they can have some evidence to the contrary.
Richard Smith
Richard Smith is a former editor of the BMJ, cofounder of the Committee on Medical Ethics (COPE), for many years the chair of the Cochrane Library Oversight Committee, and a member of the board of the U.K. Research Integrity Office.
Or put another way, an overseer of the Research Integrity Office believes research has no integrity.
What can be done?
600 fraudulent papers here, 450 over there, 1300+ citations of just one bad paper… pretty quickly it starts adding up.
We’re often told science is self-correcting. Is that true? Probably not. “The Science Reform Brain Drain” is perhaps the bleakest essay I’ve read this year. Reformers like the men who developed SPRITE and GRIM have been giving up and leaving science entirely. Pointing out in public that your colleagues are dishonest is never a great career move, and the work was often futile. One scientist who quit and went into industry summed up his fraud detection work like this:
The clearest consequence of my actions has been that Zhang has gotten better at publishing. Every time I reported an irregularity with his data, his next article would not feature that irregularity.
Even when a bull enters the China shop and gets a few papers retracted, it doesn’t actually matter because it has little effect: retracted papers keep getting cited for years afterwards and actually may be cited more than non-retracted papers, because one of the effects of retraction is that the article becomes free to download.
In the past year most talk of bad science has been about models with bad assumptions. This is an issue but has been hiding problems that are far worse: scientists are buying fake papers, Photoshopping evidence, refusing to upload their data, knowingly publishing numbers that cannot be correct, citing papers that were retracted for being fraudulent and (of course) presenting mathematical obfuscations of what they want to be true as if it were science. Journals usually ignore fraud reports entirely, or when put under pressure let scientists submit “corrected” versions of their papers. And worst of all, the journal editors that are responsible for scientific gatekeeping know all this is happening, but aren’t doing anything about it.
In fact, very little can be done because above all, universities rely on reputation and don’t want anyone to find out about bad behaviour, so they fight tooth and nail to protect academics no matter how badly they are behaving. There are no rules. Any rules that are alleged to exist turn out when tested to be illusions.
Claims made by scientists are automatically trusted by the majority of people. Maybe they shouldn’t be?
Mike Hearn is a former Google software engineer. You can read his blog at Plan 99.
Why are the Vaccines working so much better in the US than in Israel?
Is it plausible that the vaccinated make up 0.8% of COVID deaths in the US but 75% in Israel?
By Marko Marjanović | Anti-Empire | July 20, 2021
Fauci says that an incredible 99.2% of those who die of COVID in the US are now unvaccinated:
Fauci, the country’s top public health official, has said that in June, 99.2% of Covid deaths in the US could be attributed to those who are unvaccinated.
92% would be a high enough number to raise eyebrows but 99.2% is just incredible. But hey, the better these things work the happier. Who doesn’t love a nice life-saving medical intervention?
The problem is this. In Israel the 60% who are vaccinated instead contributed 75% of the deaths so far in July.

The upper left, the bottom left, and the bottom right are broken down between vaccinated (green) and unvaccinated (red). Orange are vaccinated with one dose.
Vaccinated Israelis are also contributing the clear majority of COVID hospitalizations, and of severe cases.
Some days all new severe hospitalizations are vaccinated Israelis.
Sure enough, the sample size in Israel is small. They’ve had just 12 deaths whole July (of which 9 were vaccinated) so far. Thus one shouldn’t rush to too many conclusions from here.
Also, one always has to keep in mind that the vaccinated are considerably older on average, so it is not surprising that they remain overrepresented among hospitalizations.
Much of the unvaccinated in Israel is made up of children who are not going to end up hospitalized with COVID either way:

Nonetheless, the discrepancy between the vaccine outcome reported by Fauci and reported in Israel is just too big to be accepted without an explanation.
How is it that the 60% vaccinated Israelis contributed 75% of Israeli COVID deaths in July, but the 52% Americans vaccinated by June contributed just 0.8% of deaths that month?
How come the difference in COVID outcomes between the two groups is so much greater in America than in Israel? How come the vaccines work so much better in Americans than in Israelis?
Is the vaccine anti-semitic?

The Great Betrayal

By Will Jones • Daily Sceptic • July 21, 2021
Destroy their education. Destroy their jobs and their job prospects. Destroy their social life, their friendships, their mental health. Force them to work long hours at school or in physically demanding jobs in uncomfortable and breath-inhibiting face masks. This is what our country has done to our young people in the past 16 months.
Why? In an attempt (and not a very successful one) to protect a small minority of mostly elderly folk who are particularly vulnerable to one disease while we wait in limbo to develop a vaccine and roll it out to the vulnerable population.
Then do we give them back their freedom? Not at all. Then we move the goalposts, making freedom conditional on more and more people getting the vaccine. Until we make it to so-called ‘Freedom Day’, a month later than originally planned, and Boris Johnson chooses then to tell young people that their freedom to do the things they enjoy will be dependent on receiving a vaccine.
A vaccine that uses experimental technology and was rushed through trials without waiting for the full safety data (trials which will never now conclude as the control groups have been vaccinated). A vaccine, or rather vaccines, which the authorities now acknowledge increase the risk of dangerous blood clotting and heart conditions, particularly in younger people. Vaccines for which there are now more reports of fatalities in the U.S. than all other vaccines put together for the past 30 years.

OpenVAERS
The E.U.’s own infectious disease journal Eurosurveillance has just published a study concluding that, when it comes to the AstraZeneca vaccine and blood clots, “in young adults, the risks were similar or higher than the benefits”.
Bear in mind this is just considering one side effect based on the reported incidence. It doesn’t take into account other side effects and under-reporting.
That’s the AstraZeneca vaccine, which is now discouraged for under 40s in the U.K. Are Pfizer and Moderna vaccines much better? Warnings have recently been added to them that they cause serious heart conditions in some cases. What else might emerge as the data is properly analysed?
The decision whether to take a particular vaccine, given the risk and potential benefit, is a personal one, and we can hardly blame the minority of young adults who appear to be concluding they’d rather take their chances with the virus, from which they’re also likely to get better immunity.
Any kind of threat of withdrawal of benefits for failure to take a medicine, let alone an experimental medicine, undermines informed consent. For that matter, the paucity of information provided on the real risk of side effects and the real age-specific level of benefit undermines informed consent.
Our young people have been betrayed again and again by this Government, which seems to have reached a place where it regards them primarily as vectors of disease who must be coerced into taking the prescribed medicine to make them clean enough to allow out and about. Yet the evidence that the vaccines are particularly good at preventing the spread of infection is patchy at best.
Our leaders should be ashamed of themselves for how they have abused young people and their trust, jeopardised their health and strangled their aspirations.
Sadly, I don’t think enough of them are sufficiently alive yet to the full horror of what has been pointlessly done to them in the last year and a bit to realise how angry they should be. But if they ever do wake up to it, there will be a terrible political reckoning.
Delete NHS App + Stop Getting Tested = Scamdemic Over
By Richie Allen | July 21, 2021
 Friends, gammons, countrymen, lend me your shell-likes. Take out your phone. Press your thumb or forefinger on the NHS app. Hold it down for a second. It’ll give you options. Choose delete app. Good job. Now, never take a PCR or lateral flow test again.
Friends, gammons, countrymen, lend me your shell-likes. Take out your phone. Press your thumb or forefinger on the NHS app. Hold it down for a second. It’ll give you options. Choose delete app. Good job. Now, never take a PCR or lateral flow test again.
Congratulations. You have ended the scamdemic. Go about your business. By the way, it’s not a bad idea to switch off the 24-hour news channels either.
Listening to BBC radio this morning, I was genuinely surprised to learn that a significant proportion of the population is labouring under the misapprehension that keeping the NHS app on their phones is compulsory. It isn’t. It’s entirely voluntary.
Problems arise when you are pinged and then contacted by a track and trace call-centre to inform you that you were in contact with someone who tested positive. At that point you risk being fined if you don’t isolate for the specified time and answer your phone when they call you to confirm that you are complying.
So delete the feckin app! Do it now and stop being tested. How thick do you need to be to have a test when you are healthy? Use your God given brain. It’s a trap.
How can I put it in a way that it is universally understood? Healthy man take test. Test faulty. Test come back positive. Man must isolate. Government say cases rising. Must impose restrictions. People must have jab.
It’s Kafkaesque, but the people still hold all the aces. It’s very simple. Delete the bastard app and tell them to get stuffed when they ask you to have a test. If you haven’t had a jab yet, don’t. You’ll be amazed at how quickly this will go away.
Why the EU’s Carbon Border Tax will Fail to Stop Carbon Leakage
By Eric Worrall | Watts Up With That? | July 20, 2021
The EU is once again attempting to impose a carbon tax on all imports, to stop “carbon leakage”, the loss of manufacturing or other businesses relocating to lower cost countries. But a few simple economic calculations demonstrate why the EU’s plan will not stop the ongoing haemorrhage of business activity.
Carbon Border Adjustment Mechanism: Questions and Answers
Why is the Commission proposing a Carbon Border Adjustment Mechanism?
The EU is at the forefront of international efforts to fight climate change. The European Green Deal sets out a clear path towards realising the EU’s ambitious target of a 55% reduction in carbon emissions compared to 1990 levels by 2030, and to become a climate-neutral continent by 2050.
The July 2021 package in support of the EU’s climate targets is an integral part of our strategy to achieve this, and will further seal the EU’s reputation as a global climate leader. As part of these efforts, the Carbon Border Adjustment Mechanism (CBAM) is a climate measure that should prevent the risk of carbon leakage and support the EU’s increased ambition on climate mitigation, while ensuring WTO compatibility.
Climate change is a global problem that needs global solutions. As we raise our own climate ambition and less stringent environmental and climate policies prevail in non-EU countries, there is a strong risk of so-called ‘carbon leakage’ – i.e. companies based in the EU could move carbon-intensive production abroad to take advantage of lax standards, or EU products could be replaced by more carbon-intensive imports. Such carbon leakage can shift emissions outside of Europe and therefore seriously undermine EU and global climate efforts. The CBAM will equalise the price of carbon between domestic products and imports and ensure that the EU’s climate objectives are not undermined by production relocating to countries with less ambitious policies.
…
Read more: https://ec.europa.eu/commission/presscorner/detail/en/qanda_21_3661
Why does this tax put an EU producer at a disadvantage?

EU Border Tax – No Sale
Simple – selling to another EU entity is price competitive, so far, but selling outside the EU is impossibly expensive, because you are competing with other sellers who don’t pay EU carbon taxes. An exporter outside the EU has an advantage over a manufacturer inside the EU, even if they have to pay a carbon border adjustment.
What about if the EU tries to level the playing field for EU based exporters, and applies a tax credit to exports? This opens the door to massive global carbon carousel fraud.

EU Carbon Tax Carousel Fraud
Either the EU destroys their own exporters, in an attempt to protect their domestic industry, or they have a big firefight on their hands, trying to contain carbon carousel fraud, which will only get worse any time they try to ratchet up their carbon price.
What about the effect of carbon pricing on businesses inside the EU carbon tax zone?

Classic supply and demand graph, showing the impact on quantity of a tax driven rise in price per unit.
In this case quantity is assumed to be a proxy for economic activity.
Ever visited a shopping centre, and wondered why all the interesting shops are slowly replaced by clothes shops or other high turnover businesses? The reason is all those interesting shops are not profitable enough to pay the rent, and over time they are replaced by simpler, less interesting businesses – safe, boring, profitable, but still a contraction in the diversity of life choices available to consumers.
Pretty much the same thing would happen to domestic high carbon businesses afflicted by EU carbon pricing.
The EU at least in principle likely hopes that revenue from the carbon tax will drop to zero, as people discover low carbon or zero carbon alternatives to the high carbon goods they currently use such as alumina, or simply learn to live without.
But this is a huge gamble. The only reason for carbon leakage in the first place is because the carbon intensive goods targeted by the EU are difficult to replace with low carbon alternatives, and difficult to live without.
If a carbon intensive good is irreplaceable, continued dependency on that high carbon good will be an ongoing anchor dragging on the European economy.
Of course you could make an argument that the benefits the people of the EU receive from reduced CO2 emissions outweigh the costs, that one day our descendants will thank us for giving them the opportunity to experience cold weather. But this does not help consumers and businesses today.
In conclusion, the EU carbon border adjustment will do nothing to prevent carbon leakage. The EU does not control enough of the global economy to make it more than an inconvenience for multinationals. The only people the EU border carbon adjustment will hurt are people living in the EU, who will see their choices and opportunities contract.
Covid vaccines: We’ve been misled from the very start
By Neville Hodgkinson | The Conservative Woman | July 20, 2021
IT IS truly amazing how self-deceiving a profession that sets out to help and heal sick people can be when it comes to acknowledging that the cure is sometimes worse than the illness. Evidence is mounting that just such a state of denial is manifesting in the mass rollout of the Covid vaccine.
Decades ago, I examined evidence for the effectiveness of flu vaccine and found that it rested entirely within studies showing an increase in antibodies to the circulating virus, but that this did not translate into less illness.
A group of GPs who were uneasy about the impact of the vaccine on old and frail people set up a trial of their own in which they found that those who had the jab had no less flu, but more non-specific illness, in the ensuing year compared with a group of similar frailty who were not inoculated.
Similarly, doctors at two boarding schools who conducted trials among their own pupils dropped the vaccine after finding it was of no benefit.
It would be almost impossible to do similar studies today because the NHS mounts such a relentless campaign every winter to have everyone vaccinated. It is in effect the marketing arm for the flu vaccine manufacturers, of which GlaxoSmithKline, Sanofi and AstraZeneca are leading players, making billions from the jabs.
The UK-based Cochrane research network, however, has been constantly evaluating global studies on the effectiveness of flu vaccinations since 1999. Put together, the data from dozens of well-conducted studies covering more than 80,000 participants fails to prove a reduction in deaths from flu or flu-like illnesses, and shows that vaccinations could even increase the number of hospitalisations.
Germany’s renowned Robert Koch Institute has found clear evidence that for the over-60s, in the 2017/18 and 2018/19 flu seasons, vaccination increased the risk of flu instead of protecting against it.
The fact that despite the scientific evidence, illusions still continue about such a commonly used vaccine bodes ill for hopes that governments and their advisers will listen to the evidence with regard to Covid-19.
The mantra that the jab is ‘safe and effective’ is becoming a sick joke. There is now massive evidence of harm and mounting evidence that it does not work anything like as well as hoped.
The harm is there for all to see. As of mid-June, UK regulators received 276,867 adverse events reports, including 1,332 deaths; in the US, there were more than 6,000 deaths, and 400,000 events serious enough to be reported; and in the European Union, some 1,500,000 injuries and 15,000 deaths.
Claims that these reports are unconfirmed as cause-and-effect related are countered by the argument ‘Where is the proof that they are not?’ Under-reporting is known to be common, and many of the injuries occurred within hours or days of the victim receiving the jab. There has never been a vaccine with anything like this measure of recorded harm.
Government agencies assert that thousands of lives have been saved by the vaccination drives. But wherever the claims are examined carefully, as opposed to being passed on by doctors and journalists who accepted them uncritically and are now desperately hoping they are true, the evidence is found to be increasingly thin.
As Dr Will Jones noted in the newly launched Daily Sceptic (formerly Lockdown Sceptics), latest data from the ZOE app, the world’s largest ongoing study of Covid-19, shows that as of July 12, infections in the vaccinated (at least one dose) in the UK now outnumber those in the unvaccinated for the first time, as the former continue to surge while the latter plummet.
What does Germany’s Robert Koch Institute, which seems more independent-minded than leaders of the UK’s state-run NHS, tell us about the Covid vaccine?
It published a 74-page paper last January in which the effectiveness in the age group 75 and over was said to be ‘subject to a high degree of uncertainty’ and no longer statistically significant. What’s more, the quality of the data across all age groups, based on proof of prevention of serious illness, was ‘very low’.
Reporting these findings, the German magazine Multipolar said it was scandalous that they are not mentioned in their government’s information services, and that the big media remain silent on the topic.
In truth, we have been misled about the vaccine from the start. Repeatedly publicised claims of 95 per cent ‘efficacy’ do not mean you are 95 per cent protected against Covid if you have the jab.
They are based on studies such as Pfizer’s in which 40,000 participants in different countries were divided into two groups, one of which received the vaccine and the other a placebo. There were no deaths in either group, so the trial told us nothing about risk of death. But 162 of the placebo group were designated Covid cases, compared with only eight among those vaccinated. The diagnosis was on the basis of the participants having one or more symptoms of the disease, confirmed through a lab test.
Eight compared with 162 gives what is called a relative risk reduction (RRR) of 95 per cent. It is a self-contained figure that has only a marginal bearing on the experience of the trial participants generally.
What we rarely hear about is what is known as the absolute risk, that is, the percentage of cases reported in each group of 20,000. For the vaccinated individuals, their chances of becoming a case were 0.04 per cent, and for the placebo group, 0.75 per cent. That represents an absolute risk reduction (ARR) of 0.71 per cent (0.75 per cent minus 0.04 per cent) which does not sound like much to write home about. Even that was probably an exaggeration, because side-effects in the vaccinated group would have been obvious to observers, making them less likely to report them as cases.
It gets even worse. One of the criteria of a ‘case’ in the trials was that it should be contracted not earlier than seven days after the second jab. That helped keep the number down enormously – to only eight – in the vaccinated group. This is because so many vaccine recipients have Covid-like symptoms in the first few days after the jab.
A subsequent analysis, hidden away in a report by the US Food and Drug Administration, found that when Covid-like symptoms reported in those first few days were included, there were 407 cases among the vaccinated compared with only 287 in the placebo group, an entirely different risk-benefit picture and one consistent with many studies showing an increase in death rates among the elderly immediately after the jab.
All of this means we should not be surprised to find that ‘a disturbing trend’ has appeared among the most vaccinated nations in the world, as TrialSite News reports. In Gibraltar, Malta, Seychelles, UAE and the Isle of Man, Covid cases are considerably up, including deaths in some of these nations, despite ‘overwhelming’ percentages of their populations being vaccinated.
Israel, too, with 81 per cent of its adult population fully vaccinated and cases that went right down to a handful a day, is now seeing a surge in new infections, of which an estimated 40-50 per cent are in vaccinated individuals.
Is this because of a new variant of the virus, against which the existing vaccines don’t work? Will it mean subjecting ourselves to booster shots, with the accompanying risks, every few months? Or is it because there is ultimately going to be no escaping actual infection with the virus?
We just do not know.
There is one light in the darkness. Several studies have shown that once an individual has had the infection, even if only mildly, their immune system develops lasting protection against the toxic spike protein encoded by the genetically engineered virus.
Featured Video
House Resolution Calls for Tech Companies to Censor Speech
or go to
Aletho News Archives – Video-Images
From the Archives
Israel’s recurring use of terror on civilians

By Bob Finch | January 26, 2009
Insanely disproportionate use of violence against unarmed civilians… continue
Blog Roll
 Aletho News
Aletho News- Iran replaces UAE ports with Pakistan corridor to break US blockade
- Iran sets one-month deadline for end to US-Israeli war, blockade: Report
- At the edge of the Strait: A superpower in a narrow sea
- Iran unveils new control measures over Strait of Hormuz transit
- House Resolution Calls for Tech Companies to Censor Speech
- Ceasefire no longer viable after 200 days of Israeli violations: Hamas
- Israeli strikes intensify across southern Lebanon, casualties reported
- Left in Disbelief: Israel in Panic over Hezbollah FPV Drone Nightmare
- Trump Taps Israel Lobbyist From Mossad Cutout FDD To Join Iran Negotiations
- Trump’s Blockade Snatches Defeat from the Jaws of Victory
- If Americans Knew
- As Palestinians die, Ben-Gvir celebrates birthday with golden noose cake – Daily Update
- Israel’s New Ambassador to the ‘Christian World’ Served as Envoy to Azerbaijan During the Ethnic Cleansing of Christians from Nagorno-Karabakh
- US set to sell $1B “Advanced Precision Kill Weapon System” to Israel – Daily Update
- Israeli Strikes Kill at Least 32 Across S Lebanon, Including Children – Amid “Ceasefire”
- Israel to pour $730m into propaganda arm amid reputational crisis
- Real Cost of Iran War Likely Double the $25 Billion Figure the Pentagon Gave to Congress
- Israel conducts farthest-ever strike in long history of attacks on Gaza humanitarian aid flotillas
- In Gaza, Israel commits 10+ ceasefire violations a day – Daily Update
- US ships 6,500 tons of munitions, equipment to Israel in 24 hours
- A New Library in Gaza Rises From the Ashes of Destruction
- No Tricks Zone
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
