Flawed paper behind Covid-19 testing faces being retracted, after scientists expose its ten fatal problems
By Peter Andrews | RT | December 9, 2020
A publisher admitted it is urgently re-investigating research, following revelations that the PCR test it extols is defective, giving too many false-positives. The news comes as a new group plans a legal challenge over the checks.
Last week I reported on an astonishing review conducted by a group of senior scientists on a paper on which most Covid testing is based. It comprehensively debunked the science behind the Corman-Drosten paper, which described a protocol for using the polymerase chain reaction (PCR) technique to detect Covid, finding 10 fatal flaws, including major failings in the operating procedure and potential conflicts of interest among its authors.
The team behind the review demanded that Eurosurveillance, the journal that published the original research, retract it at once, as in their view it clearly failed to meet proper standards. This is of vital importance because the Corman-Drosten paper laid the path for mass PCR testing as the main source of data on the coronavirus. Almost all case numbers, infection rates and even deaths attributed to Covid are based on PCR tests (and all the attendant lockdowns and restrictions on people), and a huge amount of them use the method set out in the Corman-Drosten paper.
But now, the organisation Retraction Watch have reported that Eurosurveillance is considering retracting the paper. In a statement, Eurosurveillance said that they were “seeking further expert advice and discussing the current correspondence in detail. We will, according to our existing procedures, evaluate the claims and make a decision as soon as we have investigated in full.’’ So no retraction yet, but it would not be surprising if one came soon.
Call up Guinness World Records
One of the 10 fatal flaws in the original Corman-Drosten paper was that it was unclear whether it had ever been subjected to proper peer review – before, that is, the panel of experts took it upon themselves to do so. The paper had been submitted on January 22 and published the very next day. Peer review, when it takes place, is normally a long, drawn out process with plenty of back-and-forth, even when it is being rushed as much as possible. That it could be done in a single day beggars belief.
But that is what the authors are asking us to believe, as they are still claiming that their article was “peer-reviewed by two experts on whose recommendation the decision to publish was made.’’ Eurosurveillance may want to consider submitting this feat to Guinness World Records as the fastest peer review of all time – it may not be too late to get into the 2021 edition.
Taking the government to court
It is clear that the wars over PCR tests are hotting up, and the stakes couldn’t be higher. A new organisation in the UK, calling itself PCR Claims, has been set up to challenge in the courts the British government’s handling of PCR testing for Covid-19.
The organisation describes itself as a pro bono network of lawyers, life scientists, and business advisers led by Jo Rogers, a lawyer who runs Navistar Legal.
Rogers told RT.com: “The intention is to expose the controversy of the inappropriate use of PCR in the context of pillar 2 community testing and private sector lighthouse labs.
“PCR was not designed for mass testing because of the sensitivity and risk of contamination. There are serious flaws in many of the protocols employed, which were hurriedly put together, some without peer review. The operational false positive rate is unknown and therefore every positive test could be false, unless accompanied by clinical examination.”
As an example of errors with PCR, the group points to a recent case from Cambridge University. “Our first priority is to gather evidence of the harms from restrictions to life whose policies were driven by PCR test modelling and/or ‘case’ results,” Rogers said. “We believe the cases are a pseudo epidemic, as seen in other places around the world using PCR testing.
“Legal action is progressing and further instances will follow as we receive the evidence of harms. The gathering of that evidence is ongoing nationwide, as well as our raising awareness of errors and negligence.”
As someone who shares their deep concerns over these PCR tests, this is good news. At last, there is somewhere to go for expert legal counsel on the government’s persecution of free-born citizens. And thank heavens also for the stellar work of the entire peer review team for holding this bad science to account. If indeed it is retracted, it will be a major victory for those of us who can see through what Dr Mike Yeadon, one of the paper’s debunkers, rightly calls a “false positive pseudo-epidemic.”
Peter Andrews is an Irish science journalist and writer based in London. He has a background in the life sciences, and graduated from the University of Glasgow with a degree in genetics.
Canadian Health Ministry Exploring “Immunity Passports,” Vaccine “Tracking And Surveillance”

By Steve Watson | Summit News | December 9, 2020
The Health Minister of Ontario in Canada has stoked controversy by suggesting that people who do not take the coronavirus vaccine will face restrictions on where they can travel and spend time.
When asked by reporters about how the government intends to go about convincing people to get the vaccine, Health Minister Christine Elliott warned that those who refuse it will face difficulties reintegrating into society.
“That’s their choice, this is not going to be a mandatory campaign. It will be voluntary,” Elliot said, but adding that “There may be some restrictions that may be placed on people that don’t have vaccines for travel purposes, to be able to go to theatres and other places.”
When another reporter asked if the government would be introducing ‘immunity passports’, or proof of vaccination cards, Elliot said “Yes, because that’s going to be really important for people to have for travel purposes, perhaps for work purposes, for going to theatres or cinemas or any other places where people will be in closer physical contact.”
Following up on Elliot’s comments, The Toronto Sun spoke to her press secretary, who confirmed that the government is exploring several options for vaccine “tracking and surveillance.”
“This includes exploring developing tech-based solutions while also providing for alternative options to ensure equitable access to any potential ‘immunity passport,’” Alexandra Hilkene said.
Sun reporter Brian Lilley notes “That phrase will set off alarm bells and it should, not just for anti-vaxxers, but for anyone who is concerned about Charter rights and governments running roughshod over them.”
Ontario Chief Medical Officer of Health Dr. David Williams has also said that a COVID-19 vaccine may be required for “freedom to move around”.
“What we can do is to say sometimes for access, or ease, in getting into certain settings, if you don’t have vaccination then you’re not allowed into that setting without other protection materials,” Williams said.
The comments of these Canadian officials add to the litany of other government and travel industry figures in both the US, Britain and beyond who have suggested that ‘COVID passports’ are coming, in order for ‘life to get back to normal’
In an essay in The Wall Street Journal on Saturday, former Centers for Disease Control and Prevention director Tom Frieden noted that he expects the so called ‘immunity passports’ will come into widespread use despite any ethical, legal or operational challenges, and despite the fact that it hasn’t at all been determined whether the vaccine equates to immunity.
Everyone is already wearing a mask. They just don’t work.
By Jordan Schachtel | December 7, 2020
One of the most common pro-mask arguments I’ve heard over the course of the past year, both from “public health experts” and your average citizen, sounds similar to the following statement:
“If only everyone would just wear a mask, we would be able to crush the virus and end the pandemic.”
This line of reasoning is frequently espoused by lockdown governors and “public health experts.” You see, the problem isn’t them, it’s you, the citizen, we’re told. Wear a mask, peasant. You’re the problem! You’re the reason why the pandemic is still a problem in this country.
Deaths up? Why aren’t you wearing a mask. Cases up? Wear a mask. Hospitals crowded? The problem is that not enough people are wearing masks, they claim.
The idea that not enough Americans are wearing masks is detached from reality. And we have the data to prove it.
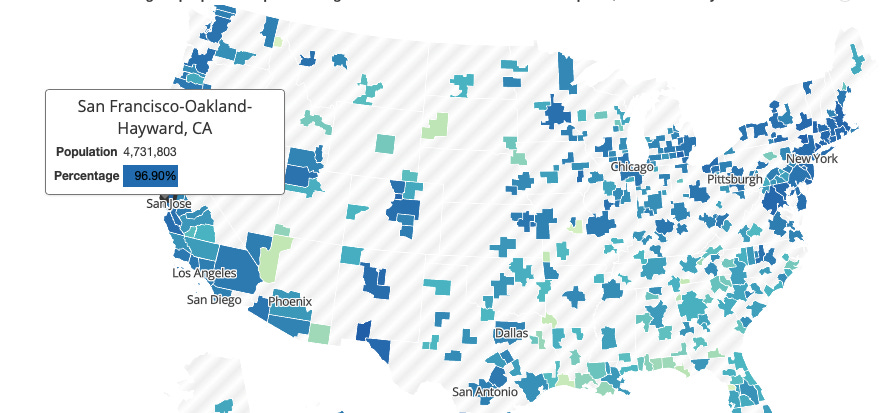
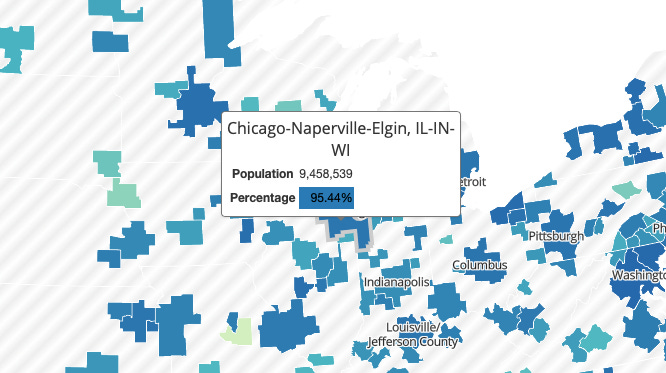
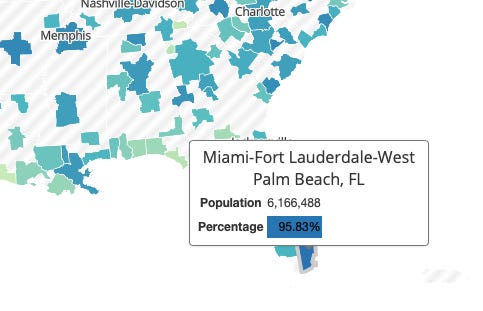
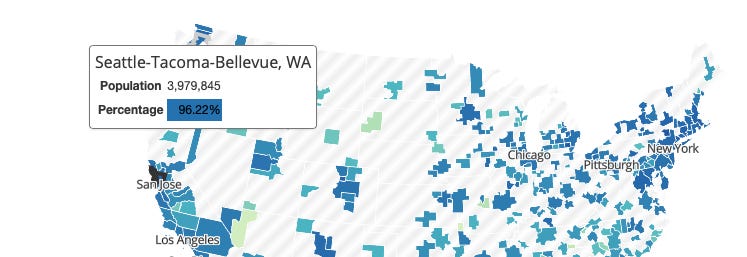
The Delphi group at Carnegie Mellon University has developed a very informative, consistently updated mask compliance tracker. It shows that the overwhelming majority of Americans across the nation are wearing masks. And in virtually every major population center in the United States, especially in areas where COVID-19 cases are rising, mask compliance levels are off the charts high, with most major metro areas registering well over 90 percent compliance.
Early on in the pandemic, when the “new science” told us that masks could stop the virus in its tracks (after the science of early 2020, espoused by the likes of Fauci and many others, rightly pointed to the reality that masks are useless outside of a controlled setting), the CDC and other “public health agencies” claimed that we could essentially eliminate transmission if a large percentage of the population adopted universal masking.
When lockdowns failed to “stop the spread,” masking up at over 80% was hyped as a way to “do more to reduce COVID-19 spread than a strict lockdown.”
“Universal masking at 80 [percent] adoption flattens the curve significantly more than maintaining a strict lockdown,” a much-hyped, highly publicized study, which was treated by many in the scientific community as the gospel, proclaimed.
“We will not only be able to flatten the curve, we will be able to significantly reduce the spread of the virus and return to life as normal sooner rather than later,” De Kai, a research scholar at Berkeley who helped develop the COVID-19 universal masking model, proclaimed.
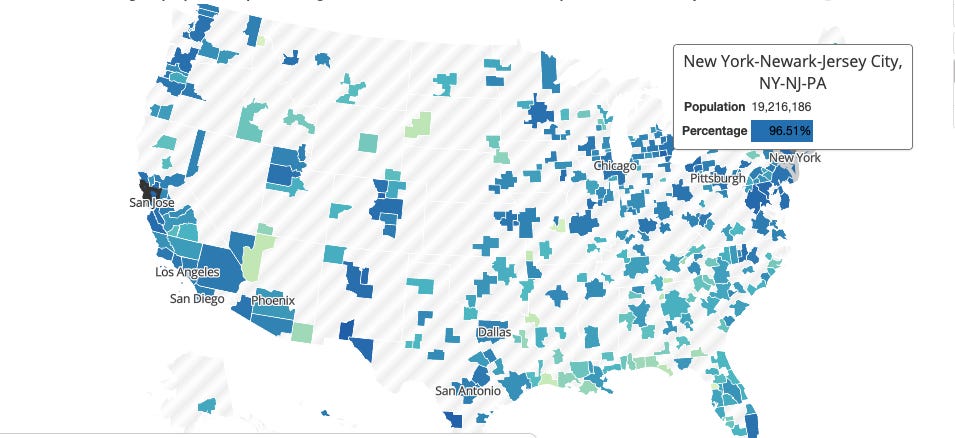
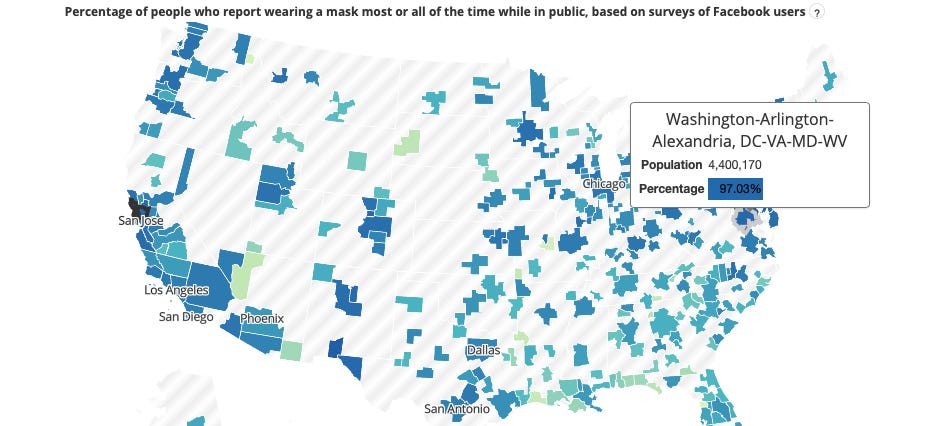
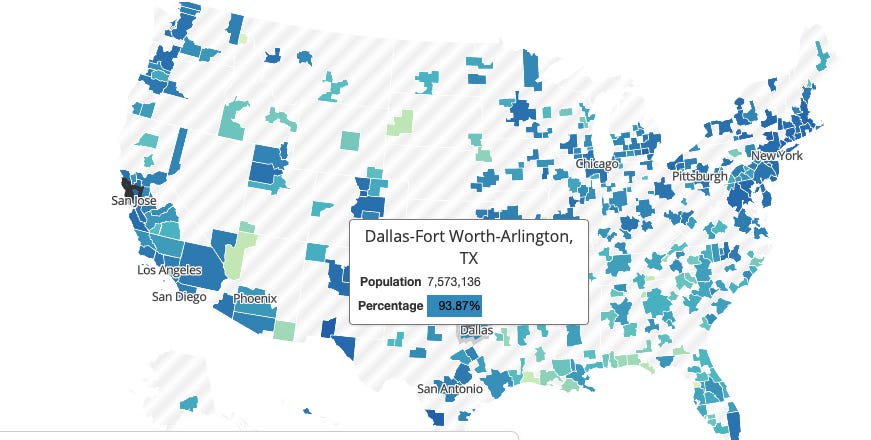
With the help of the CMU mask compliance tracker, let’s take a look at the current COVID-19 hotspots in the United States and the level of mask compliance within these areas.
San Francisco metro area: 97% mask compliance
New York City metro area: 97% mask compliance
DC metro: 97%
Dallas-Fort Worth-Arlington: 94%
Philly area: 96%
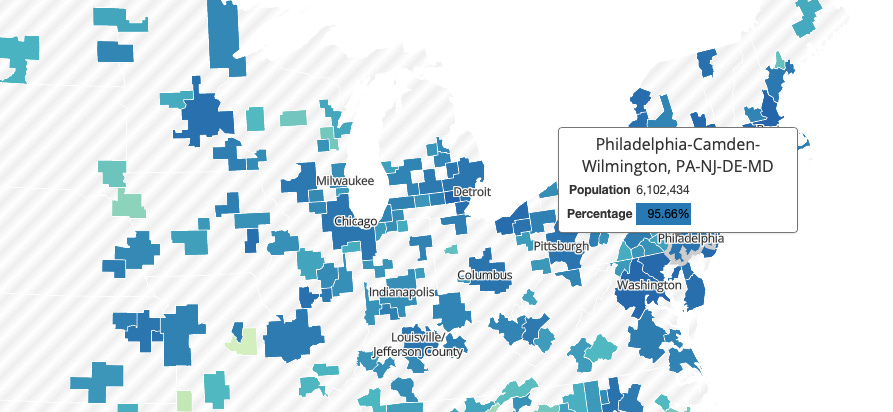
Chicago: 95%
Miami-Ft Lauderdale: 96%
Seattle: 96%
The data demonstrates very clearly that Americans have overwhelmingly exceeded the masking compliance percentages needed to supposedly “flatten the curve” and reduce transmission of the virus. The problem, of course, is that the models have not matched reality. Americans are wearing masks, but the hypothesis behind universal masking has not worked to stop the spread of COVID-19.
Americans have adopted the recommendations of the “public health experts,” but the “public health experts” have failed to follow the science, which now shows that masks are useless when it comes to stopping the spread of COVID-19. Now we’re left with an overwhelming majority of Americans wearing masks for no science-based reason whatsoever.
New Study Claims Vaccinated Children Appear To Be “Significantly Less Healthy” Than Unvaccinated
By Arjun Walia | Collective Evolution | December 4, 2020
A new study published in the International Journal of Environmental Research and Public Health has, according to the authors, discovered that vaccinated children require far more healthcare than unvaccinated children. At least that’s what they found from the group of children used to collect the data.
This type of study is interesting to see given the fact that studies comparing unvaccinated children to vaccinated children are lacking, there aren’t many of them. These studies are, as the authors state, “rarely conducted.”
None of the post licensure-vaccine safety studies have included comparisons to groups completely unexposed to vaccines.
The study concludes that “the unvaccinated children in this practice are not, overall, less healthy than the vaccinated and that indeed the vaccinated children appear to be significantly less healthy than the unvaccinated.
The data source for this study was all billing and medical records of Integrative Pediatrics, a private pediatric practice located in Portland, Oregon.
The study emphasizes the need for more research given the fact that, again, there is hardly any in this area. They concur with Mawson et al., 2017 , who reported: “Further research involving larger, independent samples is needed to verify and understand these unexpected findings in order to optimize the impact of vaccines on children’s health” and with Hooker and Miller 2020, who wrote: “Further study is necessary to understand the full spectrum of health effects associated with childhood vaccination.”
These studies mentioned above also had similar findings.
According to the authors,
Vaccines are widely regarded as safe and effective within the medical community and are an integral part of the current American medical system. While the benefits of vaccination have been estimated in numerous studies, negative and nonspecific impact of vaccines on human health have not been well studied. Most recently, it has been determined that variation exists in individual responses to vaccines, that differences exist in the safety profile of live and inactivated vaccines, and that simultaneous administration of live and inactivated vaccines may be associated with poor outcomes. Studies have not been published that report on the total outcomes from vaccinations, or the increase or decrease in total infections in vaccinated individuals.
This is important because, although vaccinations in some cases may protect against the target disease, what else might they be doing not only on the short term, but in the long term? It’s also important to point out that in other cases, like the HPV vaccine, there is no evidence that they do protect against the target disease.
Another great example comes from a study published in 2017 that examined the introduction of the diphtheria-tetanus-pertussis vaccine (DTP) in an urban community in Guinea-Bissau in the early 1980s. They found that the DTP vaccine was associated with 5-fold higher mortality than being unvaccinated. The authors state the following:
All currently available evidence suggests that DTP vaccine may kill more children from other causes than it saves from diphtheria, tetanus or pertussis. Though (this) vaccine protects children against the target disease it may simultaneously increase susceptibility to unrelated infections.
This new study points out,
Pre-licensure clinical trials for vaccines cannot detect long-term outcomes since safety review periods following administration are typically 42 days or less. Long-term vaccine safety science relies on post-market surveillance studies using databases such as the US Food and Drug Administration (FDA) and Centers for Disease Control and Prevention (CDC’s) Vaccine Adverse Events Reporting System (VAERS) and the Vaccine Safety Datalink. VAERS is a passive reporting system in which, according to Ross 2011, “fewer than 1% of vaccine adverse events are reported.” The Vaccine Safety Datalink (VSD) can, in principle, according to the Institute of Medicine (IOM, 2013), be used to compare outcomes of vaccines and unvaccinated children. Based on the IOM’s recommendation, in 2016, the CDC published a white paper (CDC, 2016; Glanz et al., 2016) on studying the safety of their recommended pediatric vaccine schedule. Unfortunately, to date, no studies have been published comparing a diversity of outcomes of vaccinated and unvaccinated children.
Below is one of many interesting graphs from the study. The orange line represents the vaccinated children, and the blue one represents the unvaccinated.

For methods used, limitations, and more please refer to the study.
The parents that I work with in New York, that I see around the country are very concerned that their rights are being taken away, that their knowledge about the science is being pushed away by an agenda that only says, unvaccinated children are a problem.
No study has every been done in this country, appropriately, to address the health outcomes of children who are vaccinated versus the children who are unvaccinated. I have been seeing families in my practice for over 20 years, that have opted out of vaccination, they are the healthiest children I’ve ever seen. – Dr. Lawrence Palevsky, a NY licensed paediatrician
Why This Is Important: Given the fact that the National Childhood Vaccine Injury Act (NCVIA) has paid out approximately $4 billion dollars to families of vaccine injured children, there are clearly, in my opinion, some valid points here, especially against compulsory vaccinations. Again, as mentioned above, VAERS only accounts for an estimated 1 percent of vaccine injuries, this one percent is what is recorded.
A 2010 HHS pilot study by the Federal Agency for Health Care Research (AHCR) found that 1 in every 39 vaccines causes injury, a shocking comparison to the claims from the CDC of 1 in every million.
Take the MMR vaccine for example, if you search on VAERS, as of 2/5/19, the cumulative raw count of adverse events from measles, mumps, and rubella vaccines alone was: 93,929 adverse events, 1,810 disabilities, 6,902 hospitalizations, and 463 deaths. Again, don’t forget about that 1% figure cited in the study.
There are a number of legitimate concerns about vaccine safety that would require quite a long and very in-depth article, but I just wanted to let the reader know here briefly. Aluminum for example, is another concern I’ve written quite a lot about.
These are a few reasons as to why vaccine hesitancy is at an all time high, even among many physicians and scientists. This has actually been observed for a while. For example, one study published in the journal EbioMedicine in 2013 outlines this point, stating in the introduction:
Over the past two decades several vaccine controversies have emerged in various countries, including France, inducing worries about severe adverse effects and eroding confidence in health authorities, experts and science. These two dimensions are at the core of vaccine hesitancy (VH) observed in the general population. VH is defined as delay in acceptance of vaccination, or refusal, or even acceptance with doubts about its safety and benefits, with all these behaviours and attitudes varying according to context , vaccine and personal profile, despite the availability of vaccine services VH presents a challenge to physicians who must address their patients’ concerns about vaccines and ensure satisfactory vaccination coverage.
At a 2019 conference on vaccines put on by the World Health Organization this fact was emphasized by Professor Heidi Larson, a Professor of Anthropology and the Risk and Decision Scientist Director at the Vaccine Confidence Project. She is referenced, as you can see, by the authors in the study above. At the conference, she emphasized that safety concerns among people and health professionals seem to be the biggest issue regarding vaccine hesitancy.
She also stated,
The other thing that’s a trend, and an issue, is not just confidence in providers but confidence of health care providers, we have a very wobbly health professional frontline that is starting to question vaccines and the safety of vaccines. That’s a huge problem, because to this day any study I’ve seen… still, the most trusted person on any study I’ve seen globally is the health care provider…
Is there not enough information here alone to warrant informed consent? I have a hard time understanding how someone who would take the new COVID-19 vaccine, for example, would be worried about me contracting the virus if they are protected?
Why have we given governments the ability to mandate such actions? Why have we given them so much power to dictate what we do and how we want to live? Is this really how we want to live, is this really the kind of world we want to create?
A Deeper Discussion. What Do We Do About The Increasing Vaccine Pressure?
So many are concerned about mandatory vaccination. Further, many are starting to see that mandated vaccines may not be the future, but that services and options will be denied unless you can prove you have been vaccinated. Is it still the time to point the blame? Or is there a radical new approach we must take? A shift in our worldview, re-examining who we think we are, why we are here and what world we want to create is where we will begin to find the answers we are looking for. Has the dualistic fight the enemy method worked in the past? Are we not still here regardless of having used this method in the past? Maybe it’s time for a new conversation, one that looks at ourselves in a whole new light. This perhaps is how we will solve our ongoing challenges at their core.
Below is a deeper discussion about it from CE Founder Joe Martino. You can follow me, Arjun, here on Instagram.
Featured Video

US Superpower Myth Shattered w/ Trita Parsi
or go to
Aletho News Archives – Video-Images
From the Archives
Israel Is A Genocidal Society
The Israeli Political Spectrum From The “Liberal Left” To The Far Right, Is United In Genocide
The Dissident | May 5, 2026
… The fundamental issue of Israel is not Benjamin Netanyahu, but the fact that Israel is overwhelmingly a bloodthirsty, war-ready, genocidal society.
Historian Zachary Foster has documented that the overwhelming majority of Jewish Israelis have supported every Israeli war since the 2006 invasion of Lebanon, writing:
2006
86% of the Israeli adult population justified “the IDF operation in Lebanon against Hizbollah,” or 2006 Lebanon War, in which Israel killed 1,191 people, the vast majority civilians according to HRW (Note that the % of Jewish Israelis who supported the war was even higher)2008-2009
82% of the Israeli public thought that the 2008-9 war on Gaza was justified (in which Israel killed 1,417 Palestinians, the vast majority civilians.) Note that the % of Jewish Israelis who supported the war was even higher2012
90% of Israeli Jews supported war on Gaza ( in which Israel killed 160 Palestinians, 66% civilians)2014
95% of Jewish Israelis believed the war on Gaza was justified (in which Israel killed 2,310 Palestinians, 70% civilians)2021
72% of Israelis believed the war on Gaza should continue (as of May 21) after Israel had already killed 250 Palestinians in Gaza, vast majority civilians. The % of Jewish Israelis who supported killing more Palestinians was much higher.2024
A January poll found 95% of Jewish Israelis thought the Israeli military was using either the “appropriate” amount of force or “too little” force in Gaza at a time when Israel had already killed >25,700 Palestinians in Gaza.2024
In September, 90% of Jewish Israelis supported the war on Lebanon (in which Israel killed 800+, including hundreds of civilians)2025
In March, 82% of Israeli Jews supported the forced expulsion of residents of Gaza, Israel’s main goal in it’s genocide & war on Gaza.2025
In June, 82% of Jewish Israelis supported the war on Iran known as the “twelve day war”2026
On March 4, 93% of Israeli Jews expressed support for the war on Iran. 97% of “right-wing” Jewish Israelis support it, compared with 93% in the center and 76% on the left.
The overwhelming majority of Jewish Israelis also have openly genocidal views towards Palestinians.
Polls in Israel have shown that:
- 84% of the (Israeli )public gives the IDF an excellent or very good grade regarding the moral conduct of the army
- 75% of Jewish Israelis agree with the idea that ‘there are no innocents in Gaza.’
- A vast majority of Israeli Jews – 79 percent – say they are ‘not so troubled’ or ‘not troubled at all’ by the reports of famine and suffering among the Palestinian population in Gaza.
The fundamental problem in Israel is Zionism, not Benjamin Netanyahu. – Full article
Blog Roll
 Aletho News
Aletho News- Iranian forces strike US vessels in swift retaliation for tanker attack: Top military commander
- Israeli ‘double tap’ strike hits paramedics in south Lebanon hours after renewed bombing of Beirut
- Occupation Bulldozes Farmland, Uproots Vineyards
- ‘Israel’ kills Azzam al-Hayya, son of Hamas chief Khalil al-Hayya
- What has Guterres supported in Gaza?
- UAE received $80m in EU farming subsidies as calls grow for sanctions over Sudan genocide
- Trump gives green light for new arms deliveries to Ukraine
- U.S. Blockade Against Cuba Must End Immediately: China
- US Superpower Myth Shattered w/ Trita Parsi
- Iran War Reality BITES – SPIN HARDER /Lt Col Daniel Davis & Mario Nawfal
- If Americans Knew
- Two Supreme Court Justices were secret agents who helped Israel cover up its attack on the USS Liberty
- Bari Weiss ‘Meddles’ With ‘CBS Sunday Morning’ Story on Palestine
- Zionists Are Gunning for Your Freedom of Speech
- The horrors in Gaza continue: Here are the facts
- Israeli General Is Running a Sophisticated, Sociological Engine of Violence
- Israel has stolen $4.8 billion from Palestinians
- The pro-Israel political consensus is collapsing in both parties
- Prominent Christian Zionist Group Is Lobbying U.S. Lawmakers on Israel—Without Revealing It’s Funded by Israel
- “Most Moral Army” caught desecrating another Christian statue, as famine looms in Gaza – Daily Update
- Israel’s subversion of Foreign Agents Registration Act
- No Tricks Zone
- New Study: Declining Trends In 1980-2023 Tropical Cyclone Frequency, Accumulated Energy
- 46 IPCC Scientists Break Rank, Publicly Challenge Long-Standing Dogmatic Climate Claims
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
