On August 31, the Nation magazine published an article entitled “Chile: The Secrets the US Government Continues to Hide,” which details the CIA’s continued steadfast insistence on keeping its records secret that relate to the agency’s 1970-1973 efforts to bring regime change to Chile.
The CIA’s continued secrecy, of course, brings to mind the agency’s equally steadfast insistence on keeping its JFK-assassination related records secret into perpetuity.
The CIA, needless to say, cites the two magic words — “national security” — to justify its continued secrecy in both events.
I suggest that two other words are the real reason for the CIA’s continued secrecy in both events: “criminal cover-up.”
After all, the JFK assassination took place 60 years ago and the Chilean coup took place 50 years ago. The notion that the release of CIA assassination-related and coup-related records would threaten “national security,” no matter what definition is used for that ridiculous, meaningless term, is laughable to the extreme.
Actually, the Chilean coup bears a relationship to the JFK assassination. That’s because the national-security establishment’s mindset toward its regime-change operation in Chile reflected its mindset toward its regime-change operation in Dallas. My hunch is that those still-secret records relating to Chile would provide further circumstantial evidence pointing toward the reasons for the operation in Dallas.
In 1970, Chilean voters delivered a plurality of vote to Salvador Allende in the presidential election. Since Allende had not received a majority of votes, the election was thrown into the hands of the Chilean congress.
U.S. officials deemed Allende a grave threat to U.S. national security, on two grounds: that he was a socialist but, more important, that he was befriending the communist world, including Cuba and the Soviet Union, something that Kennedy had done as well in his famous Peace Speech at American University a few months before he was assassinated.
The CIA embarked on a campaign of bribing the members of the Chilean congress to vote against Allende (which, of course, is somewhat ironic given the fierce U.S. reaction to supposed Russian involvement in U.S. elections).
At the same time, the U.S. national-security establishment made plans for a Chilean military takeover. What’s interesting is that the CIA did not assassinate Allende. Instead, it convinced the Chilean national-security establishment that Allende posed a grave threat to Chilean national security and, therefore, that the Chilean national-security establishment had a moral duty to violently prevent Allende from assuming the presidency.
That’s a very important and very revealing point, one that undoubtedly comes across loud and clear in those still-secret CIA records relating to the Chile coup. The point reveals the U.S. national-security establishment’s conviction that it had the moral duty to violently remove JFK from power in order to protect America from a president whose policies, they concluded, posed a grave risk to “national security.” (See FFF’s book JFK’s War with the National Security Establishment: Why Kennedy Was Assassinated by Douglas Horne.)
Much to the chagrin of the U.S. national-security establishment, however, the commanding general of Chile’s armed forces, Gen. Rene Schneider, opposed the idea of a coup. His position was that the Chilean constitution did not permit a coup as a way to remove a democratically elected president from office. He said that Chileans would have to wait until the next election.
Therefore, the CIA simply orchestrated a violent kidnapping of Schneider which left him dead from gunshot wounds on the streets of Santiago. Ironically, the CIA’s kidnapping and assassination of this innocent man boomeranged because the Chilean congress, faced with tremendous anger over Schneider’s murder among the Chilean citizenry, rejected the CIA’s bribes and installed Allende into power.
Three years later, however, the U.S. national-security establishment prevailed in its efforts and helped military strongman Gen. Augusto Pinochet violently take over the reins of power. By the end of the war between the executive and national-security branches of the government, Allende was dead, just as Kennedy was ten years before.
With the full support of the Pentagon and the CIA, Pinochet’s henchmen rounded up some 60,000 innocent people and proceeded to torture and/or rape most of them. They also killed or disappeared around 3,000 of them.
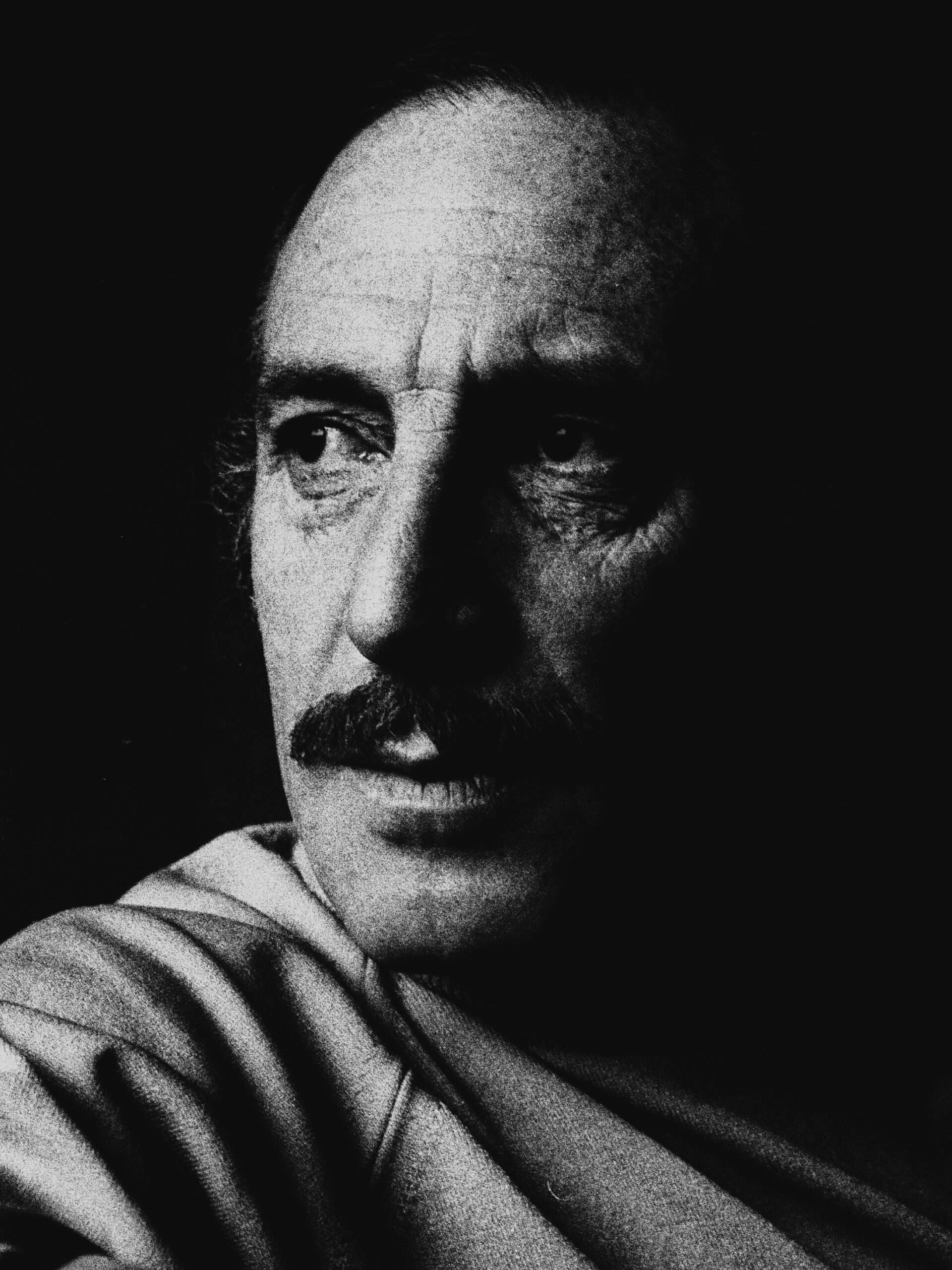
Orlando Letelier
Among those rounded up was Orlando Letelier, a highly respected man who had served in the Allende administration as ambassador to the United States, minister of foreign affairs, minister of the interior, and minister of defense. After being tortured in captivity, world pressure forced Pinochet to release him.
Letelier moved to Washington, D.C., where he joined a leftist think tank and began lobbying against the Pinochet regime. Pinochet and his national-security establishment deemed Letelier to be a grave threat to Chilean “national security.”
On September 21, 1976, Letelier was killed by a car bomb on the streets of Washington, D.C., along with his young assistant Ronni Moffitt.
It was determined that Pinochet’s secret Gestapo-like internal police force, which was called DINA and which worked with the CIA, had orchestrated and carried out the Letelier assassination. Among those convicted of the crime was a DINA agent named Michael Townley, who was a U.S. citizen.
As part of what was clearly a sweetheart deal, Townley pled guilty in U.S. District Court as part of a plea bargain with U.S. officials. Get this: He was sentenced to only ten years in jail for what amounted to the cold-blooded murder of two innocent people. To put that in perspective, compare it to the 22-year jail sentence that a U.S. District Judge recently meted out to a man convicted of simply participating in the January 6 protests. Townley was also given immunity from prosecution in Chile for another national-security assassination in which he had allegedly been involved.
But that’s not all. After serving only 62 months in jail, get this: He was admitted into the federal witness protection program! That meant that the feds gave him a secret identity and let him live a normal life somewhere in the world.
The Letelier assassination has always been blamed on Pinochet. Is it possible that the CIA, working with DINA, was also embroiled in that assassination, on grounds of “national security”? My hunch is that those records relating to Chile that the CIA steadfastly continues to keep secret would help provide an answer to that question, which, needless to say, would be a good reason for wanting them to kept secret.
September 10, 2023
Posted by aletho |
Civil Liberties, Deception, Subjugation - Torture, Timeless or most popular, War Crimes | Chile, CIA, JFK Assassination, United States |
Leave a comment
Far from bringing down the final curtain, it seems that the Covid comedy show is going to run and run.
First up (as they say), there is the seemingly unending stream of Covid variants. It is almost as if someone is making them up. In the middle of August, I wrote in these pages about Eris, but now others have emerged such as BA.2.86 which may evade the Covid vaccines (code for ‘we need more vaccines’) and Pirola. While we are exhorted to ‘be worried’, if you dig deep into the details it transpires that there is little to worry about.
After all, we have been here before. We were warned about BA.4 and BA.5 (‘variants of concern’) late in 2021 but, probably much to the surprise of the doom-mongers, humanity has survived. Who can forget Omicron which even those who discovered it described as nothing to worry about? But we were urged to worry about it nevertheless. Even more baffling is that some people who did not fall for the Covid vaccine propaganda are still with us. Quelle surprise!
Next on the bill is animal-to-human transmission. There has long been speculation that Covid may spread from humans to animals, so they could become a reservoir for the virus which could then spread back to humans. Early in 2020 the British government issued mundane advice (e.g. ‘wash your hands’) for people with animals and provided a list of the creatures to which it was considered Covid-19 may spread. The list was extensive and may as well have proclaimed ‘the animal kingdom’ as a potential reservoir for the virus. Though little advice related to specific animals, the government saw fit to include a specific section: ‘If you own a ferret’. Sadly, it did not contain the advice ‘don’t put it down your trousers’; a comedy opportunity missed, in my view.
There remains concern that humans are spreading Covid to deer. We first read about this early in the pandemic but, unless we are concerned about the welfare of deer, which surely have better things to worry about than Covid, it is unclear why we should be concerned now. It is suspected (not confirmed) that three humans have contracted Covid from deer in the United States from a population of around 334,233,000 where 120 people are killed annually in road accidents involving deer. The animal crackers continue with the risk of zoo employees contracting Covid from lions. It may just be me, but if I was working with lions, catching a dose of Covid would be way down my list of concerns.
Long Covid is an old favourite on the comedy circuit, and by special request, it is here tonight courtesy of our sponsors Medscape. Concern is now turning to long Covid in children, and we are told: ‘Long Covid most often strikes seniors and adults, but children are also affected, even though they get less attention, new research shows.’ It was only a matter of time, and the irony is lost on the authors that children were given undue attention by the vaccine obsessed during the ‘pandemic’ given that they were at such low risk from Covid. Some children are suffering from extreme debilitation but the possibility of this resulting from vaccine injury is not even contemplated.
In another Medscape article the ‘mystery’ of long Covid is explored. A single case is presented of someone disabled with post-viral symptoms. His symptoms are not in doubt, but the cause seems to be unknown, yet Medscape is convinced this is long Covid. After all, it must be as the list of symptoms associated with long Covid, having been whittled down to a mere seven, now seems to have expanded again to 37, which does not exactly narrow down to a precise diagnosis.
In breaking news, again in that redoubtable organ Medscape, ‘some people with long Covid tested negative for Covid-19’. Intellectual gymnastics from various sources are drawn on to explain this phenomenon. Primarily it is attributed to not diagnosing the original Covid infection properly (code for ‘we need more Covid testing’). It never seems to enter the heads of these Covid boffins that long Covid either does not exist or is something else altogether. We already know that half of people reporting long Covid symptoms also reported that they had never had Covid and that some long Covid symptoms in women bear a remarkable resemblance to early onset menopause. Nevertheless, it is clear that someone has an interest, presumably financial, in perpetuating the long Covid narrative which, if they succeed, may well prove to be as lucrative as the HIV/AIDS narrative which is still giving good returns forty years on.
However, the team at TCW are at pains to let you know that there is no cause for alarm, be it scariant variants, transmission from rampaging lions or the dreadful prospect of long Covid (everyone has at least one symptom after all). We are here to spread a message of hope and that comes with the information that our caring and sharing government are going to prepare new vaccines against the new variants and bring forward the autumn vaccine programme. What’s more, some of you lucky people who received the Pfizer or Moderna vaccines will continue to produce harmless spike proteins . . . for ever. So, you see, there is absolutely nothing to worry about.
Truthstream Media | September 4, 2023
September 9, 2023
Posted by aletho |
Timeless or most popular, Video | Covid-19 |
Leave a comment
Here’s what never happened in the hospital during COVID: a doctor sat down next to a patient and said, “You have a choice. We can give you Remdesivir, which killed 53 percent of the patients in an Ebola trial. It was so bad the trial had to be shut down. And you’ll notice here in Remdesivir’s fact sheet, it says, ‘Not a lot of people have used Remdesivir. Serious and unexpected side effects may happen.’ Or we can give you ivermectin, a safe and effective drug that’s been successfully used for decades, and send you home. Which do you prefer?”
The reason that conversation never happened is that it would have cost the hospital too much money. If the hospital gave you ivermectin and sent you home, the federal government paid the hospital $3,200. If the hospital gave you Remdesivir, the federal government paid the entire hospital bill, plus a 20 percent bonus. So the hospital executives’ choice was to receive $3,200 or $500,000, which was the average hospital bill. No contest. Patients were going to get Remdesivir — whether they wanted it or not.
Informed consent died a grotesque death in the hospitals during COVID, and we need an autopsy. There was no information, and there was no consent, and without them, patients are reduced to helpless victims, exploited for corrupt financial gain and immoral experiments.
Informed consent has been enshrined in numerous judicial rulings as the foundation of ethical medical practice and seared into the public’s conscience from the Nuremberg trials. Seven Nazi doctors were hanged in Germany by an American military tribunal for “murders, tortures, and other atrocities committed in the name of medical science.” Yet murders, tortures, and other atrocities are exactly what was committed by medical staff in the hospitals against thousands of Americans during COVID.
Take, for example, Ray Lamar, who arrived in the emergency room with a message written with a black sharpie pen on his arm: “NO VENT NOREMDESIVIR.” On his other arm, he wrote the same message and added his wife’s name and phone number. Yet the doctors gave him Remdesivir anyway, without ever informing him. His widow Patti told me she constantly wonders what she could have done to save him.
Christine Johnson told the doctors that she discussed all her medications with her daughter, who is a nurse, and she concluded that she didn’t want Remdesivir. It didn’t matter. Christine was given Remdesivir while she was sleeping, and now her daughter Michelle doesn’t have her mother.
Rebecca Stevens was an avid reader of Epoch Times, where she learned about Remdesivir’s dangers. She declined Remdesivir on five separate occasions, as her hospital records confirm. But the medical staff didn’t care what Rebecca wanted. She was given Remdesivir without her knowledge, and now Rebecca’s five grandsons are bereft.
I asked Michael Hamilton how it’s possible to give Remdesivir to patients without them knowing. Hamilton is a lawyer for several families who are suing California hospitals for the murder of their loved ones, and he’s heard thousands of victims’ stories. “They would lie right to your face,” he said. “You’d tell the nurse that you didn’t want Remdesivir and she’d say, ‘Fine. But you’re a bit dehydrated, so let’s get some fluids in you.’ And she’d hook up the IV, but it wasn’t fluids. It was Remdesivir.”
Hamilton told me that another favored tactic was to knock out patients with sedatives like morphine and fentanyl. While they lay there in a stupor, they were injected with Remdesivir.
If secret injections of Remdesivir weren’t enough to kill you, the hospitals had more torture lined up. After all, the federal government paid hospitals a big bonus to ventilate patients — so patients were going to get ventilated, whether they wanted to or not. A lot of patients turned down being vented, because the whole process is a nightmare. You’re painfully intubated, rendered unable to talk; your lungs start shredding, and you may acquire bacterial pneumonia, which the hospital will refuse to treat.
But “no” is not an acceptable answer when the hospital has money at stake. The medical staff’s preferred method for gaining “consent” was relentless bullying, screaming, coercion, and threats until the patient finally caved. Patti Lamar, Ray’s widow, told me that when she refused to let them ventilate her husband, the doctors screamed at her over and over, “You’re killing him! You’re killing him! You’re killing him!” When she couldn’t take it anymore, she reluctantly gave in. Ray died shortly thereafter, and Patti lives with the trauma of that moment.
Michael Hamilton told me the fate of his friend who was a nurse, hospitalized in the place where she had worked for 26 years. When she refused ventilation, the doctor shrieked, “You’re refusing medical advice! Now your insurance company won’t pay your hospital bill when you die! Do you want to bankrupt your family? Do you? Do you?” The nurse panicked, and to protect her family, she “consented.” Two days later, she died.
“This was a very common technique,” Hamilton said. “I’ve heard it hundreds of times. You tell the patient that unless they do what the doctor says, they’ll bankrupt their family because insurance won’t pay the hospital bills. Nobody wants to do that to their family.” Does this sound like informed consent to you? It sounds more like medical battery to me.
The entire hospital environment was a hellscape of abuse in which informed consent wasn’t even a distant memory. Hamilton told me that patients were routinely denied all access to food and water, stupefied with 50 medications that included drugs contraindicated for each other, tortured with oxygen machines set at such high levels that they couldn’t breathe, and zip-tied to the bed till their wrists bled and their hands turned black. His stories align with 1,000 collected testimonies of the COVID-19 Human Betrayal Memory Project, which documents the victims’ fates.
The ultimate denial of informed consent was the hospitals’ refusal to allow the patients to leave. “Patients lost all rights when they went in the hospital,” Senator Ron Johnson told Patty Myers in her documentary, Making A Killing. “They became prisoners.” A cottage industry of hospital rescues cropped up, as desperate family members hired lawyers to try to spring their loved ones out of hospital “care.” Ralph Lorigo, a lawyer in Buffalo, told me that in every case when he succeeded in getting a patient’s case before a judge and the judge ruled in the family’s favor, the patient went home and survived. In all cases where the judge refused to hear the case or ruled against the family, the patient died.
Every American is a sovereign individual with inalienable rights to life, liberty, and the pursuit of happiness, not a sack of meat to be treated as a profit opportunity. Informed consent must be revived from the grave if Americans are to have a fighting chance against powerful financial interests allied against them.
Stella Paul is the pen name of a writer in New York who has covered medical issues for over a decade. In 2021, she lost her husband in a locked down nursing home in New York City where he had been brutally isolated for almost a year. He died one week after getting the vaccine. Stella is focused on exposing the Hospital Death Protocol to honor her husband’s memory and to support thousands of bereaved families.
September 9, 2023
Posted by aletho |
Corruption, Timeless or most popular, War Crimes | Covid-19, United States |
Leave a comment
Lancet Paper Inadvertently Discloses Data on Vaccination Worsening Long-COVID Symptomatology
I have seen patients in my practice become progressively more ill with fatigue, weakness, hair loss, headaches, effort intolerance, sleep disturbance and in some cases cardiac and neurological symptoms with progressive mRNA injections every six months. Meanwhile the Biden Administration US HHS National Action Plan on Long COVID-19 has been running a billion dollar research plan with no consideration that the vaccine could be the cause of symptoms. The medical literature is loaded with papers on long-COVID ignoring the fact the same patient groups have all been taking COVID-19 vaccines. In essence, there is a global coverup of vaccine injury syndromes as “long-COVID.”
Mateu et al studied 548 individuals, 341 with long-COVID, followed for a median of 23 months (IQR 16.5–23.5). With continued vaccination, only 26 subjects (7.6%) recovered from long-COVID during follow-up; almost all of them (n = 24) belonged to the less symptomatic cluster and importantly the syndrome finally lessened when they dropped vaccination. The authors fail to include vaccination in their multivariate models, thereby missing this effect in the patient population. However, they inadvertently show the impact of COVID-19 vaccination on persistent long-COVID in a figure shown in the Lancet manuscript.
No wonder people are sick with long-COVID! The vaccines install long-lasting genetic code for the Wuhan SARS-CoV-2 Spike protein which deposits in tissues and organs and directly causes cardiovascular, neurological, thrombotic, and immunologic disease which is being blamed on “long-COVID.” Thus an important part of treatment for long-COVID is to stop ill-advised every six-month mass vaccination.
Peter A. McCullough, MD, MPH
President, McCullough Foundation
www.mcculloughfnd.org
Lourdes Mateu, Cristian Tebe, Cora Loste, José Ramón Santos, Gemma Lladós, Cristina López, Sergio España-Cueto, Ruth Toledo, Marta Font, Anna Chamorro, Francisco Muñoz-López, Maria Nevot, Nuria Vallejo, Albert Teis, Jordi Puig, Carmina R. Fumaz, José A. Muñoz-Moreno, Anna Prats, Carla Estany-Quera, Roser Coll-Fernández, Cristina Herrero, Patricia Casares, Ana Garcia, Bonaventura Clotet, Roger Paredes, Marta Massanella, Determinants of the onset and prognosis of the post-COVID-19 condition: a 2-year prospective observational cohort study, The Lancet Regional Health – Europe, 2023, 100724, ISSN 2666-7762, https://doi.org/10.1016/j.lanepe.2023.100724. (https://www.sciencedirect.com/science/article/pii/S2666776223001436)
September 9, 2023
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
Nearly all of the alleged anthropogenic link to climate change can be removed simply by exchanging and/or replacing biased temperature and solar activity data sets.
A new study authored by 37 scientists in the journal Climate finds using rural-only Northern Hemisphere temperature data (i.e., removing artificial, non-climatic urban heat effects) reduces the post-1850 warming trend from 0.89°C per century to 0.55°C per century.
Further, using a total solar irradiance (TSI) dataset neglected by the IPCC (Hoyt and Schatten, 1993, updated to present) allows TSI to explain up to 87% of modern warming.
Variations in cloud cover, albedo, and natural ocean circulations may also be factors arising from internal climate variability that could explain modern climate changes.
In summary, then, much of modern global warming’s alleged link to human activity may have been formulated by selecting data that align with the hypothesis, and neglecting or dismissing data which do not.
September 9, 2023
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular |
Leave a comment
Dismal UK CFD auction results may be a landmark moment
The Government has today announced the results of the fifth auction of Contracts for Difference subsidies for renewable electricity generation. Its has been a failure, and may represent a landmark moment for renewables policy.
Only 3.7GW of new capacity has bid successfully, mostly through small projects, as compared to nearly 12GW last year. There were no bids for offshore wind, the UK’s flagship renewable generator.
Participants in the auction bid for guaranteed prices, below a cap set by ministers in advance of the auction. The cap for offshore wind was set at £44/MWh (in 2012 prices, equivalent to around £70/MWh today). This is higher than successful bids in the past, yet no wind farm developers felt able to bid at this price. Wind industry claims that this is due to rising prices are implausible – CfD contracts are index-linked.
While offshore wind’s failure to bid may be surprising to some, perhaps even to the Government, it will come as no shock to those familiar with the long-term capital and operating cost trends for wind power, as revealed in audited financial statements. Costs have not been falling dramatically as the industry claimed. All around the world the wind industry is in trouble for the same reasons; costs remain high, and high levels of subsidy are needed to reward investors.
In addition, the latest auction round closes down the loophole that allowed windfarms to reap huge windfall profits by failing to activate their contracts so that they could benefit from higher prices in the open market.
The fact is that wind power, wherever, is an expensive way of generating energy. That isn’t surprising either; wind is a physically low-quality fuel and the cost of turning it into electricity is intrinsically high.
The previously successful low bids for offshore wind were unrealistic, a point we made at the time. Even when built, wind farms delayed taking up their contracts so they could operate on a merchant basis, taking advantage of temporarily high wholesale prices.
Importantly, the cap for onshore wind bids in this round of the CFD auction was higher than that for offshore, at £53/MWh (2012 prices). There were a substantial number of successful bids at this price, though they are all located in Scotland, where land rents are lower and where the developers can expect to make extra income through the infamous “constraint payments”, where a wind farm is paid to reduce output. (Demand in Scotland is low and the grid links to England are congested, limiting exports.) Even so, we doubt that these successful onshore bids are strongly economic.
Andrew Montford, director of Net Zero Watch, said:
Government seems to have believed the spin about falling offshore wind costs, and set a low cap on bids for new contracts, thus calling the wind industry’s bluff by accident. Doubtless, the industry will now beg for new and higher subsidies, blaming inflation and supply chain problems. Government should not believe this spin. As global experience shows, wind power is extremely and intrinsically expensive.”
Dr John Constable, energy editor of Net Zero Watch, said:
The CfD auction results are symptomatic of a wider failure of wind power around the world. The industry is in a crisis from which it is unlikely to recover, because its costs are simply too high to be sustainable. The time has come for Government to admit that renewables have failed, and to start looking at realistic energy policies.
September 9, 2023
Posted by aletho |
Economics, Malthusian Ideology, Phony Scarcity, Timeless or most popular | UK |
Leave a comment
Dr Ros Jones, the founder of CCVAC and long-term critic of the Government’s advisory body on vaccine policy JCVI, has just written to them again to ask why, in defiance of the evidence, are they recommending an autumn booster for healthy 12-64s who live with an immunocompromised household member. Here she explains her concern.
SCARY and ill-informed headlines like ‘New Covid fears as kids return to school and daily rates numbers double in a month’ have given grist to the government’s mill that an increase in Covid cases justifies them in bringing forward the autumn booster programme from October to September 15.
If you think this is irrelevant for most healthy children, it is not. The proposed schedule, though excluding the majority of healthy under-64s, recommends that perfectly healthy 12-64s get a booster if they are a household contact of someone with immunosuppression, for example someone who has been under cancer treatment. Once again guilt is being exploited. Whose needs do parents prioritise, their healthy teenage son or daughter or their elderly immunocompromised mothers and fathers? The simple answer is they have to do neither: their child does not need a booster for his or her own health and it is abundantly clear that the vaccines do not prevent infection or transmission, and may well have the opposite effect. There is good evidence that repeated boosters actually increase the likelihood of infection, particularly in the first week or two after vaccination, quite apart from all the other immediate and long-term potential risks of harm.
This is why I, with more than one hundred health professionals and academics, have once again written to Professor Wei Shen Lim, chairman of the JCVI’s Covid-19 committee, to point out the total lack of logic or indeed ethics in the current guidelines. The letter is published below and can also be found on the Hart group website here: Professor Lim, how can boosters protect others? – HART (hartgroup.org)
***
4th September 2023
Professor Wei Shen Lim and all members, Joint Committee of Vaccination and Immunisation
Rt Hon Stephen Barclay MP, Secretary of State, Department of Health and Social Care
cc Dr Camilla Kingdon, President, Royal College of Paediatrics and Child Health
Dear Professor Lim and Mr Barclay,
re: JCVI advice for Covid-19 vaccination of healthy young adults if living with an immunocompromised household member
I, and many of my co-signatories, have written to you on several occasions since May 2021[i], when you were first deliberating over whether to recommend Covid-19 gene-based vaccines for healthy children, given the lack of any robust safety data on these new mRNA technologies and the acknowledged low impact of SARS-CoV-2 on children.
It is very gratifying to see that this autumn’s booster programme [ii] has now been dropped for almost all healthy under-65s. However, there is one group still being offered a booster that causes us serious concern, namely the offer of a booster to healthy over-12s if they have an immunocompromised household member. We set out our reasons below.
1. It is clear that Covid-19 vaccines are failing to prevent infection by or transmission of SARS-CoV-2.
2. There is now good evidence that multiple boosters actually increase the likelihood of a SARS-CoV-2 infection [iii].
3. There is good evidence of a specific rise in infection risk in the first 7-10 days after vaccination, thus putting family members at increased rather than reduced risk [iv],[v].
4. The more recent omicron variants are poorly covered by the original vaccines, but even the newer bivalent boosters generate a much lower response against the non-Wuhan sequences in the vaccines, indicative of immune imprinting [vi].
5. The potential benefit of vaccination now for healthy young adults is low, and for children is effectively zero, given the poor efficacy of the vaccines and the high prevalence of naturally-acquired immunity [vii].
6. The safety profile of these vaccines is woefully inadequate for use in a healthy low-risk population, especially children, giving a poor risk : benefit balance. The hazard of myocarditis, recognised early on as an increased risk in younger age groups [viii], has still been poorly delineated, but risks as high as 1 in 25 are reported for subclinical myocarditis in a recent study from Switzerland [ix], confirming similar findings from Thailand. Although symptoms usually resolve quickly, scarring has been demonstrated on cardiac MRI scans [x] and has been found to persist at 6-12-month follow-up [xi]. Pfizer’s own 5-year follow-up study is not due to report until 2027; likewise a large FDA-sponsored study in the US [xii].
7. Many other adverse effects have been reported and listed in our previous letters [xiii], [xiv], perhaps the most worrying of which is the deleterious effect on the immune system [xv],[xvi]. Basic pharmacokinetics of these products are only just being reported, with a paper this week, as we write, reporting findings of vaccine-derived spike protein persisting in the circulation for many months (or longer) after vaccination [xvii],[xviii]; with serious implications for prolonged effects of any vaccine injuries.
8. The issue of excess all-cause deaths in younger age groups in 2022 and 2023 has yet to be properly investigated and a link to vaccines cannot be ruled out until this is done[xix].
9. Even if there was good evidence that vaccination could protect vulnerable household contacts, there would be major ethical concerns around asking children to take a vaccine with any potential risks of harm, to protect family members. The Universal Declaration on Bioethics and Human Rights [xx] Article 4 and Article 7 make it clear that all medical interventions must be in the best interest of the individual concerned, particularly in the case of children who are not able to give consent. If a booster was in the best interests of a healthy 12-17-year-old, then surely the JCVI would be recommending it for all, but it is clear that these children are being offered the vaccine merely in a likely unsuccessful attempt to benefit other household members.
10. Whilst it may be argued that technically these products have now been approved and are therefore no longer a research tool, these ethical principles and the precautionary principle must still apply, especially since the approval itself is still based on much less evidence than would be expected for other drugs.
Please could you urgently provide the following, under a FOI request:
- minutes of the meetings at which these decisions were made;
- calculations of numbers of healthy 12-17-year-olds (and of all household members aged 12-64) needed to vaccinate to prevent the hospitalisation of one vulnerable family member;
- any legal advice taken on how these unnecessary booster doses to children comply with UK and international law.
We look forward to hearing from you as a matter of urgency before the commencement of the vaccine booster rollout to healthy 12-17-year-olds .
Yours sincerely
Dr Rosamond Jones, MD, FRCPCH, retired consultant paediatrician, convenor of CCVAC (Children’s Covid Vaccines Advisory Council) and many others….
Professor Anthony J Brookes, Professor of Genomics & Health Data Science, University of Leicester
Professor Angus Dalgleish, MD, FRCP, FRACP, FRCPath, FMedSci, Professor of Oncology, University of London; Principal, Institute for Cancer Vaccines & Immunotherapy
Professor Richard Ennos, MA, PhD. Honorary Professorial Fellow, University of Edinburgh
Professor John A Fairclough, BM BS, BMed Sci, FRCS, FFSEM(UK), Professor Emeritus, Honorary Consultant Orthopaedic Surgeon
Professor David Livermore, BSc, PhD, retired Professor of Medical Microbiology
Professor Karol Sikora, MA, MBBChir, PhD, FRCR, FRCP, FFPM, Honorary Professor of Professional Practice, Buckingham University
Professor Roger Watson, FRCP Edin, FRCN, FAAN, Honorary Professor of Nursing, University of Hull
Professor Keith Willison, PhD, Professor of Chemical Biology, Imperial, London
Lord Moonie, MBChB, MRCPsych, MFCM, MSc, House of Lords, former parliamentary under-secretary of state 2001-2003, former consultant in Public Health Medicine
Dr Roland Salmon, MBBS, MRCGP, FFPH, former Director, Communicable Disease Surveillance Centre (Wales)
Dr Ali Ajaz, Consultant Psychiatrist
Dr Shiraz Akram, BDS, Dental surgeon
Dr Victoria Anderson, MBChB, MRCGP, MRCPCH, DRCOG, General Practitioner
Julie Annakin, RN, Immunisation Specialist Nurse
Wendy Armstrong, Practice Nurse
Helen Auburn, Dip ION, MBANT, NTCC, CNHC, Registered Nutritional Therapist
Dr Ancha Bala-Joof, MBChB, MRCGP, General Practitioner
Dr Michael Bazlinton, MBChB, MRCGP, DCH, General Practitioner
Dr Mark A Bell, MBChB, MRCP(UK), FRCEM, Consultant in Emergency Medicine, UK
Dr Michael D Bell, MBChB, MRCGP, retired General Practitioner
Dr Ashvy Bhardwaj, MBBS, DRCOG, MRCGP (2018)
Dr Alan Black, MBBS, MSc, DipPharmMed, Retired Pharmaceutical Physician
Dr Gillian Breese, BSc, MB ChB, DFFP, DTM&H, General Practitioner
Dr Ian Bridges, MBBS, retired General Practitioner
Dr Emma Brierly, MBBS, MRCGP, General Practitioner
Dr Elizabeth Burton, MB ChB, Retired General Practitioner
Dr David Cartland, MBChB, BMedSci, General practitioner
Dr Peter Chan, BM, MRCS, MRCGP, NLP, General Practitioner, Functional Medicine Practitioner
Dr Bernard Choi, MBBS, MRCGP, DCH, DRCOG, General Practitioner
Michael Cockayne, MSc, PGDip, SCPHNOH, BA, RN, Occupational Health Practitioner
Mr Ian F Comaish, MA, BM BCh, FRCOphth, FRANZCO, Consultant ophthalmologist
James Cook, BN, MPH, NHS Registered Nurse
Dr Clare Craig, BMBCh, FRCPath, Pathologist
Dr David Critchley, BSc, PhD, 32 years in pharmaceutical R&D as a clinical research scientist
Dr Sue de Lacy, MBBS, MRCGP, AFMCP UK, Integrative Medicine Doctor
Dr Christine Dewbury, retired General Practitioner
Mr Keith Dewbury, retired Consultant Radiologist
Dr Jayne Donegan, MBBS, DRCOG, DCH, DFFP, MRCGP, homeopathic practitioner, retired NHS GP
Dr Damien Downing, MBBS, MRSB, private physician
Dr Jonathan Eastwood, BSc, MBChB, MRCGP, General Practitioner
Dr Jonathan Engler, MBChB, LlB (hons), DipPharmMed
Dr Elizabeth Evans, MA(Cantab), MBBS, DRCOG, Director UKMFA
Dr Chris Exley, PhD FRSB, retired professor in Bioinorganic Chemistry
Dr Brian Fitzsimons, MBChB, DipOccMed, FRCGP, General Practitioner, Occupational Health Physician, Pre-Hospital Emergency Care Practitioner
Dr John Flack, BPharm, PhD. Retired Director of Safety Evaluation at Beecham Pharmaceuticals 1980-1989 and Senior Vice-president for Drug Discovery 1990-92 SmithKline Beecham
Dr Charles Forsyth, MBBS, FFHom, Ecological and Homeopathic Physician (Retired)
Dr Sheena Fraser, MBChB, MRCGP (2003), Dip BSLM, General Practitioner
Sophie Gidet, RM, Midwife
Dr Jenny Goodman, MA, MBChB, Ecological Medicine
Dr Ali Haggett, Mental health community work, 3rd sector, former lecturer in the history of medicine
Mr David Halpin, MBBS, FRCS, Orthopaedic and trauma surgeon, retired
Alex Hicks, MEng, MCIPS, Compliance Director (Supply Chain)
Mr Anthony Hinton, MBChB, FRCS, Consultant ENT surgeon, London
Dr Richard House, PhD, CPsychol, AFBPsS, CertCouns, Chartered Psychologist, former senior lecturer in Psychology (Roehampton) and Early Childhood (Winchester), retired psychotherapist
Dr Keith Johnson, DPhil, former patents officer
Dr Timothy Kelly, MB BCh BSc, NHS doctor
Dr Tanya Klymenko, PhD, FHEA, FIBMS, Senior Lecturer in Biomedical Sciences
Dr Caroline Lapworth, MB ChB, General Practitioner
Dr Branko Latinkic, BSc, PhD, Molecular Biologist
Dr Theresa Lawrie, MBBCh, PhD, Director, Evidence-Based Medicine Consultancy Ltd
Dr Jason Lester, MRCP, FRCR, Consultant Clinical Oncologist
Dr Felicity Lillingstone, IMD DHS PhD ANP, Doctor, Urgent Care, Research Fellow
Dr Nichola Ling, MBBS, MRCOG, Consultant obstetrician and digital advisor to NHS England
Katherine MacGilchrist, BSc (Hons) Pharmacology, MSc Epidemiology, CEO, Systematic Review Director, Epidemica Ltd
Dr C Geoffrey Maidment, MD, FRCP, retired consultant physician
Mr Ahmad K Malik, FRCS (Tr & Orth), Dip Med Sport, Consultant Trauma & Orthopaedic Surgeon
Dr Ayiesha Malik, MBChB, General Practitioner
Dr Kulvinder S. Manik MBChB, MRCGP, MA(Cantab), LLM, Gray’s Inn
Dr Fiona Martindale, MBChB, MRCGP, General Practitioner in out-of-hours
Julie Maxwell, MBBCh, MRCPCH, Associate Specialist Community Paediatrician
Dr Fatou Mbow, MD(Italy), MRCGP, DFFP, General Practitioner
Dr Sam McBride, BSc(Hons) Medical Microbiology & Immunobiology, MBBCh BAO, MSc in Clinical Gerontology, MRCP(UK), FRCEM, FRCP(Edinburgh), NHS Emergency Medicine & geriatrics
Kaira McCallum, BSc, retired pharmacist, Director of strategy UKMFA
Mr Ian McDermott, MBBS, MS, FRCS(Tr&Orth), FFSEM(UK), Consultant Orthopaedic Surgeon
Dr Janet Menage, MA, MBChB, retired General Practitioner
Dr Franziska Meuschel, MD, ND, PhD Affiliations, IDF, BSEM, Nutritional, Environmental and Integrated Medicine
Dr Scott Mitchell, MBChB, MRCS, Associate Specialist, Emergency Medicine
Dr Alistair J Montgomery, MBChB, MRCGP, DRCOG, retired General Practitioner
Dr Alan Mordue, MBChB, FFPH, Retired Consultant in Public Health Medicine & Epidemiology
Margaret Moss, MA(Cantab), CBiol, MRSB, Director, The Nutrition and Allergy Clinic, Cheshire
Dr Claire Mottram, BSc Hons, MBChB, Doctor in General Practice
Dr Greta Mushet, MBChB, MRCPsych, retired Consultant Psychiatrist in Psychotherapy
Dr Angela Musso, MD, MRCGP, DRCOG, FRACGP, MFPC, General Practitioner
Dr Sarah Myhill, MBBS, Dip NM, Retired GP, Independent Naturopathic Physician
Dr Chris Newton, PhD, Biochemist
Dr Rachel Nicoll, PhD, Medical researcher
Tim Nike, Specialist Neurological Physiotherapist
Sue Parker Hall, CTA, MSc (Counselling & Supervision), MBACP, EMDR. Psychotherapist
Dr Dean Patterson, MBChB, FRCP. Consultant Cardiologist
Dr Christina Peers, MBBS, DRCOG, DFSRH, FFSRH, Menopause Specialist
Rev Dr William J U Philip MB ChB, MRCP, BD, Senior Minister The Tron Church Glasgow, formerly physician specialising in cardiology
Dr Angharad Powell, MBChB, BSc (hons), DFRSH, DCP (Ireland), DRCOG, DipOccMed, MRCGP, General Practitioner
Dr Gerry Quinn, PhD, Microbiologist
Dr Jessica Robinson, BSc(Hons), MBBS, MRCPsych, MFHom, Psychiatrist and Integrative Medicine Doctor
Dr Jon Rogers, MB ChB (Bristol), retired General Practitioner
Mr James Royle, MBChB, FRCS, MMedEd, Colorectal Surgeon
Dr Charlie Sayer, MBBS, FRCR, Consultant Radiologist
Sorrel Scott, Grad Dip Phys, Specialist Physiotherapist in Neurology, 30 years in NHS
Dr Rohaan Seth, BSc (Hons), MBChB (Hons), MRCGP, Retired General Practitioner
Dr Rajendra Sharma, MBBCh, BAO, LRCP&S(Ire), MFHom, Private Doctor, Medical Director, Dr Sharma Diagnostics
Natalie Stephenson, BSc (Hons) Paediatric Audiologist
Dr Noel Thomas, MA, MBChB, DObsRCOG, DTM&H, MFHom, Retired Doctor
Dr Livia Tossici-Bolt, PhD, NHS Clinical Scientist
Dr Helen Westwood, MBChB (Hons), MRCGP, DCH, DRCOG, General Practitioner
Dr Carmen Wheatley, DPhil, Orthomolecular Oncology
Dr Samuel White, MBChB, MRCGP, Functional Medicine Specialist, former General Practitioner
Dr Ruth Wilde, MBBCh, MRCEM, AFMCP, Integrative & Functional Medicine Doctor
Dr Stephanie Williams, Dermatologist
Dr AZ, MBChB, NHS Specialty doctor
[i] https://www.hartgroup.org/open-letter-to-mhra-17-05-2021/
[ii] https://www.gov.uk/government/publications/covid-19-autumn-2023-vaccination-programme-jcvi-advice-26-may-2023/jcvi-statement-on-the-covid-19-vaccination-programme-for-autumn-2023-26-may-2023
[iii] Shrestha NK, Burke PC, Nowacki AS et al. Effectiveness of the Coronavirus Disease 2019 Bivalent Vaccine, Open Forum Infectious Diseases 2023;10 (6): doi.org/10.1093/ofid/ofad209
[iv] Shrotri M, Krutikov M, Palmer T et al. Vaccine effectiveness of the first dose of ChAdOx1 nCoV-19 and BNT162b2 against SARS-CoV-2 infection in residents of long-term care facilities in England (VIVALDI): a prospective cohort study. Lancet Infect Dis. 2021. doi.org/10.1016/S1473-3099(21)00289-9
[v] Bar-On YM, Goldberg Y, Micha, M et al. Protection by a Fourth Dose of BNT162b2 against Omicron in Israel, N Engl J Med 2022; 386:1712-1720. https://www.nejm.org/doi/full/10.1056/NEJMoa2201570
[vi] Fujita S, Uriu K, Pan L et al. Impact of Imprinted Immunity Induced by mRNA Vaccination in an Experimental Animal Model, The Journal of Infectious Diseases, 2023;, jiad230, https://doi.org/10.1093/infdis/jiad230
[vii]https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1131409/appendix-1-of-jcvi-statement-on-2023-covid-19-vaccination-programme-8-november-2022.pdf
[viii] Oster M, mRNA COVID-19 Vaccine-Associated Myocarditis, 2022, https://www.fda.gov/media/153514/download
[ix] Buergin N, Lopez-Ayala P, Hirsiger JR et al. Sex-specific differences in myocardial injury incidence after COVID-19 mRNA-1273 booster vaccination. European Journal of Heart Failure 2023. https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.2978
[x] Jain SS, Steele JM, Fonseca B et al. COVID-19 Vaccination–Associated Myocarditis in Adolescents. Pediatrics 2021; 148 (5): e2021053427. doi.org/10.1542/peds.2021-053427
[xi] Yu CK, Tsao S, Ng CW et al. Cardiovascular Assessment up to One Year After COVID-19 Vaccine-Associated Myocarditis. Circulation 2023; 148(5): 436–439. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10373639/
[xii] https://www.nymc.edu/news-and-events/news-archives/us-fda-awards-dr-supriya-jain-19-million-to-support-research-on-covid-19-vaccine-associated-myocarditis.php
[xiii] https://www.hartgroup.org/open-letter-to-the-jcvi-pause-vaccines-for-children-pending-urgent-review/
[xiv] https://www.hartgroup.org/open-letter-to-the-jcvi-2/
[xv] Uversky VN, Redwan EM, Makis W, Rubio-Casillas A.IgG4 Antibodies Induced by mRNA Vaccines Generate Immune Tolerance to SARS-CoV-2’spike Protein by Suppressing the Immune System. Vaccines 2023; 11(5): 991. https://doi.org/10.3390/vaccines11050991
[xvi] Noé A, Dang TD, Axelrad C et al. BNT162b2 COVID-19 vaccination in children alters cytokine responses to heterologous pathogens and Toll-like receptor agonists. Front Immunol 2023; 14:1242380. doi.org/10.3389/fimmu.2023.1242380
[xvii] Castruita JAS, Schneider UV, Mollerup S et al. SARS-CoV-2 spike mRNA vaccine sequences circulate in blood up to 28 days after COVID-19 vaccination. APMIS 2023; 131: 128-132. https://doi.org/10.1111/apm.13294
[xviii] Brogna C, Cristoni S, Marino G et al.Detection of recombinant Spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms. Proteomics Clinical Applications 2023; https://doi.org/10.1002/prca.202300048
[xix] https://vigilantnews.com/post/excess-mortality-just-got-even-worse-ed-dowd-drops-alarming-new-data
[xx] https://www.unesco.org/en/legal-affairs/universal-declaration-bioethics-and-human-rights
September 8, 2023
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19, COVID-19 Vaccine, UK |
Leave a comment

The vast majority of the population of Haiti is unvaccinated for COVID-19 but the impoverished Caribbean nation recorded virtually no deaths from the virus.
Haiti remains one of the least vaccinated countries in the world while also showing the lowest Covid death rate.
As of the end of April, just 254 people have died in Haiti from what authorities agree constitutes Covid, according to reports.
However, this figure is likely overblown considering SARS-CoV-2 has never even been isolated and proven to exist.
Compared to the United States, which currently has a COVID-19 death rate of around 1,800 per one million people, Haiti has a Covid death rate of just 22 per one million people, or 0.0022% – basically 0 percent.
NPR admits in a report about Haiti that Covid restrictions were never enforced there.
Nobody there wears a mask, people are mostly unvaccinated, and daily life is normal with busy and crowded buses and markets.
For most Haitians, the pandemic never happened.
“And Haiti hasn’t yet administered a single COVID-19 vaccine,” NPR‘s Jason Beaubien further reveals.
It turns out that Haiti had its own version of Tony Fauci, a man named Dr. Jean “Bill” Pape, who headed up a commission during the “pandemic” to deal with the fallout. In the end, however, the commission was dissolved because Haiti was, and continues to be, COVID-free.
“The reason mainly is because we have very, very few cases of COVID,” Pape said about why the commission was ultimately disbanded.
GHESKIO, the local health agency that Pape heads, also closed its COVID units last fall due to a lack of patients.
While the Western world is stricken with hordes of “fully vaccinated” people who are now sick as dogs, Haiti is back to normal thanks to its rejection of the shots.
“Sometimes it’s two, sometimes zero, sometimes it’s 20 cases,” Pape said.
“But we are not seeing a second wave as we thought would happen.”
Unlike much of the rest of the world, Haiti remained open during the “pandemic.”
Outdoor markets were never closed, and people there continued working because sheltering in place and remote employment are not things that the average Haitian can afford.
“Most people don’t wear a mask,” Pape added, noting that Haitians continued working as normal throughout the pandemic because “if they don’t work, they don’t eat – their family doesn’t eat.”
When AstraZeneca tried to peddle its COVID injection in Haiti, the Haitian government denied a shipment of it.
It turns out that the medical community in Haiti heard about all the “rare” side effects of the jab and thus rejected it.
“COVID did not impact us as badly,” said Dr. Jacqueline Gautier, who serves on the national technical advisory group on COVID vaccination in Haiti.
“People don’t think [the vaccine] is worth it, actually.”
Another factor that makes Haiti an incredible success story compared to other nations is the fact that its population is very young.
The average age in Haiti is around 23, while in the United States, it is closer to 40.
Younger people tend to have stronger immune systems than older people.
And without COVID jabs to destroy them, Haiti’s millions of unvaccinated people fared well compared to the rest of the world.
“Also, there are many other major problems the country is facing,” Gautier added.
“So people don’t see COVID as our major, as a major, problem for us.
“And who can blame them?”
September 8, 2023
Posted by aletho |
Timeless or most popular | Covid-19, COVID-19 Vaccine, Haiti |
Leave a comment

Years before emerging as Kiev’s top private weapons trafficker, ex-legislator Serhiy Pashinsky played a key role in the 2014 US-backed coup which toppled Ukraine’s democratically-elected president and set the stage for a devastating civil war. Though the notoriously corrupt former Ukrainian parliamentarian was condemned by President Volodymyr Zelenskyy as a “criminal” as recently as 2019, a lengthy exposé by the New York Times has now identified Pashinsky as the Ukrainian government’s “biggest private arms supplier.”
Perhaps predictably, the report makes no mention of evidence implicating Pashinsky in the 2014 massacre of 70 anti-government protesters in Kiev’s Maidan Square, an incident which pro-Western forces used to consummate their coup d’etat against then-President Viktor Yanukovych.
In an August 12 report on Ukraine’s new weapons-sourcing strategy, the New York Times alleged that “out of desperation,” Kiev had no option but to adopt increasingly amoral tactics. The shift, they say, has driven up prices of lethal imports at an exponential rate, “and added layer upon layer of profit-making” for the benefit of unscrupulous speculators like Pashinsky.
According to the Times, the strategy is simple: Pashinksy “buys and sells grenades, artillery shells and rockets through a trans-European network of middlemen,” then “sells them, then buys them again and sells them once more”:
“With each transaction, prices rise – as do the profits of Mr. Pashinsky’s associates – until the final buyer, Ukraine’s military, pays the most,” the Times explained, adding that while using multiple brokers may technically be legal, “it is a time-tested way to inflate profits.”
As the seemingly endless supply of cash from Western taxpayers provides a bonanza for arms manufacturers such as Raytheon and Northrop Grumman, it similarly benefits war profiteers like Pashinsky. His company, Ukrainian Armored Technology, “reported its best year ever last year, with sales totaling more than $350 million” — a whopping 12,500% increase from its $2.8 million in sales the year before the war.
Pashinsky is not the only racketeer benefitting from the elimination of anti-corruption measures in wartime Ukraine. Several suppliers previously placed on an official blacklist after they “ripped off the military” are now free to sell again, according to the Times investigation. The outlet downplayed this as an unfortunate, but ultimately necessary measure.
“In the name of rushing weapons to the front line, leaders have resurrected figures from Ukraine’s rough-and-tumble past and undone, at least temporarily, years of anticorruption [sic] policies,” the Times asserted, describing “the re-emergence of figures like Mr. Pashinsky” as “one reason the American and British governments are buying ammunition for Ukraine rather than simply handing over money”:
“European and American officials are loath to discuss Mr. Pashinsky, for fear of playing into Russia’s narrative that Ukraine’s government is hopelessly corrupt and must be replaced.”
However, even the seemingly critical Times report overlooks a key aspect of Pashinsky’s unsavory biography. Conspicuously absent from the coverage was any explanation of his role in carrying out the infamous massacre of anti-government activists and police officers in Kiev’s Maidan Square in late February 2014.
A defining moment in the US-orchestrated overthrow of Ukraine’s elected government, the death of 70 at the hands of mysterious snipers triggered an avalanche of international outrage that led directly to the ouster of President Viktor Yanukovych. Even today, these killings officially remain unsolved.
However, firsthand testimony by individuals who claimed to have helped carry out the false flag attack suggest Kiev’s most prolific gun runner was intimately involved in the grisly affair.
Maidan massacre organizer ‘takes no prisoners’
In November 2017, Italy’s Matrix TV channel published eyewitness accounts by three Georgians who say they were ordered to kill protesters by Mamuka Mamulashvili. Then the top-ranking military aide to Georgian president Mikhael Saakashvili, Mamulashvili later founded the infamous mercenary brigade known as the Georgian Legion, whose fighters were widely condemned after they published a gruesome video of themselves gleefully executing unarmed and bound Russian soldiers in April 2022.
The documentary, “Ukraine: The Hidden Truth,” features an Italian journalist’s interviews with three Georgian fighters allegedly sent to orchestrate the coup. All described Pashinsky as a key organizer and executor of the Maidan massacre, even alleging the corrupt arms dealers provided weapons and selected specific targets. The film also featured footage of him personally evacuating a shooter from the Square, after they had been caught with a rifle and a scope by protesters and surrounded.
One of the Georgian fighters recalled how he and his two associates arrived in Kiev in January, “to arrange provocations to push the police to charge the crowd.” For almost a month, however, “there were not many weapons around,” and “molotov [cocktails], shields and sticks were used to the maximum.”
This changed around mid-February, they said, when Mamualashvili personally visited them alongside a US soldier named Brian Christopher Boyenger, a former officer and sniper in the 101st Airborne Division, who personally gave them orders they “had to follow.”

A documentary by Italy’s Matrix channel contains eyewitness testimony implicating an American military instructor in Ukraine’s 2014 Maidan massacre.
Pashinky then personally moved them along with sniper rifles and ammunition to buildings overlooking Maidan Square, they alleged. At that point, Mamualashvili reportedly insisted that “we have to start shooting, so much, to sow some chaos.”
So it was that the Georgian fighters “started shooting two or three shots at a time” into the crowd below, having been ordered to “shoot the Berkut, the police, and the demonstrators, no matter what.” Once the killing was over, Boyenger moved to the Donbas front to fight in the ranks of the Georgian Legion, which Mamulashvili commands to this day.
In the meantime, Ukrainian journalist Volodymyr Boiko, who headed the civic council of the Prosecutor General Office of Ukraine after Maidan, has alleged that in order to obscure his role, Pashinsky personally hand-picked the figures leading the official investigation into the massacre, and even bribed the prosecutor who headed it.
Despite these shocking claims, Pashinsky’s involvement in the Maidan massacre has never been officially investigated, let alone punished, and his most recent experiences with the Ukrainian judicial system suggest it is unlikely to be heavily scrutinized by officials in Kiev. While a member of Ukraine’s Verkhovna Rada, he was arrested for shooting and wounding a pedestrian in a traffic-related dispute, but was ultimately acquitted in 2021.
When Israeli journalists confronted Pashinsky about his role in the Maidan massacre, the arms dealer warned that they would be tracked down in their home country, where his associates would “tear them apart.” They could be forgiven for believing it was not an idle threat; there is a troubling tendency for Pashinky’s detractors to end up viciously beaten or shot dead in the street.
September 7, 2023
Posted by aletho |
Corruption, False Flag Terrorism, Timeless or most popular, War Crimes | Ukraine |
Leave a comment
By Lucas Leiroz | September 7, 2023
The US appears to be less and less concerned about the risks of escalation in its proxy conflict with Russia. In yet another irresponsible and anti-humanitarian maneuver, the Biden government announced its decision to send depleted uranium (DU) weapons to the Kiev regime. As is well known, these weapons are extremely dangerous for everyone involved in the conflict, including the soldiers who use them. But the western side does not seem to care about these issues, planning only to prolong hostilities as long as possible.
The announcement was made on September 6, with Pentagon’s spokespersons informing the media that DU munitions will be included in a new military aid package valued at 175 million dollars. The munitions are expected to be used on more than thirty M1 Abrams tanks previously shipped to Ukraine. In addition to radioactive weapons, artillery, anti-tank equipment and other types of arms are also included in the package.
Although the US has already taken several escalating measures and violated many Russian red lines, this is the first time that the country has announced its intention to send radioactive shells to Ukraine. So far, only the UK has sent DU weapons to Kiev. With the US assisting in this supply, the situation worsens significantly, removing any hope of easing tensions in the short term.
As well known, the effects of these weapons on human health are disastrous. There are several reports about the negative impact of DU ammunition on the lives of soldiers and civilians in the regions where it was used. Cancer, fetal deformity, deficiency of fertility and several other diseases are linked with the handling of DU ammunition. Commenting on the arrival of these weapons in Ukraine months ago, Doug Weir, an expert linked to the Conflict and Environment Observatory, explained that “[DU munitions] fragment and burn, generating chemically toxic and radioactive DU particulate that poses an inhalational risk to people.”
Despite evidence of health problems caused by DU arms, they are considered “low” risk by the British and Americans. This is why they were used on a large scale in NATO’s invasions against Serbia and Iraq, generating thousands of victims. The excuse for considering them “low risk” is that depleted uranium has a low radiation level, but this does not appear to be a solid argument, as obviously it does not have to be highly radioactive to be toxic and dangerous to human health.
Another important aspect to be discussed is how to classify these weapons according to international law. Since they are radioactive, there are experts who believe it appropriate to classify them in the same way as nuclear weapons. Other experts consider this interpretation exaggerated, since the radiation level of DU ammunition is low, but even so, there seems to be a consensus that the correct thing would be to ban them given their risks and their little strategic relevance.
These ammunitions are generally used to pierce armor vehicles and hit tanks. Despite giving a certain advantage to the side that uses them, their role can normally be performed on the battlefield by other types of weapons, which do not emit substances that are so toxic to human health. Russia, for example, has been efficient in neutralizing enemy tanks using artillery, drones and mines, without any radioactive substance. So, these weapons are obviously replaceable by other less dangerous ones, which is why they should be banned once and for all.
In addition to a lack of concern for human health and the environment, the American attitude also reflects a kind of “despair”. The US is running out of conventional weapons to send to Kiev, which is why it has recently started sending banned weapons, such as cluster munitions, and now even radioactive ones, such as DU. With the massive destruction of NATO equipment on the battlefield, Washington is becoming unable to continue producing conventional weapons for its own forces and for Kiev simultaneously, so it is now turning to controversial and illegal arms in the Ukrainian aid packages.
On Russia’s side, the stance remains one of avoiding escalation and trying to neutralize the radioactive threat with high-precision strikes. Most of the DU ammunition previously supplied by the British was prevented from being used on the battlefield due to the Russian attack on Khmelnitski in May, which destroyed the depot where the weapons were stored. With this kind of high-precision strike, Moscow prevents these ammunitions from being used against innocent civilians, who are the main targets of the Kiev regime.
The Russian response could be much tougher, even nuclear, since DU ammunition can be considered nuclear weapons, as they do not have specific regulation in international law. However, unlike the West, Moscow continues to maintain a posture of avoiding escalation as much as possible.
Lucas Leiroz, journalist, researcher at the Center for Geostrategic Studies, geopolitical consultant.
You can follow Lucas on Twitter and Telegram.
September 7, 2023
Posted by aletho |
Timeless or most popular, War Crimes | Iraq, Serbia, Ukraine, United States |
Leave a comment
The UN condemned the use of depleted uranium ammunition on Wednesday, after the US government said it would send Ukraine a number of such rounds for M1 Abrams tanks as part of a $175-million military aid package.
“We are against the use of depleted uranium ammunition anywhere in the world,” Farhan Haq, the deputy spokesman for UN Secretary-General Antonio Guterres, told TASS.
Haq’s comments came after the Pentagon revealed that an unspecified number of 120mm DU rounds will be sent to Ukraine as part of the newest package of military assistance. The anti-tank rounds are intended for use by the 30-odd M1 Abrams tanks promised to Kiev by the White House in January. The first batch of tanks are supposed to be delivered later this month.
Washington is following in London’s footsteps in providing the controversial munitions to Kiev. The UK sent a number of DU rounds to Ukraine earlier this year, intended for use with its Challenger 2 tanks. The delivery of DU ammunition was teased by the Wall Street Journal in June and leaked to Reuters last week.
The British military dismissed Moscow’s objections to the use of the toxic heavy metal by saying the ammunition had “nothing to do with nuclear weapons or capabilities.” The US has also insisted the munitions are not radioactive, citing studies by the International Atomic Energy Agency (IAEA) that DU residue “does not pose a radiological hazard to the population of the affected regions.”
Critics who seek to ban DU ammunition have pointed to skyrocketing rates of cancer and birth defects in places like Iraq and Serbia, claiming that uranium dust is toxic when handled or inhaled.
Anonymous British and American officials have glibly dismissed Russian concerns about environmental contamination, suggesting instead that Moscow was afraid of the “highly effective” rounds.
The US and its allies have sent over $100 billion worth of weapons, ammunition and military equipment to Ukraine over the past 18 months, while insisting that this does not make them a party to the conflict. These deliveries have included cluster munitions banned by most NATO members. Ukraine reportedly has to account for their use directly to the Pentagon. Russia has documented multiple instances in which such ordnance was used against civilian targets.
September 7, 2023
Posted by aletho |
Environmentalism, Timeless or most popular, War Crimes | DU, Ukraine, United States |
Leave a comment