Counting Covid’s Deceptive Deaths
A look at the unorthodox way in which Covid-19 deaths are registered shows the numbers don’t add up
By Bernard Marx | OffGuardian | June 2, 2021
Four-thousand, nine-hundred and forty one. And rising. This number can only increase or, at best, stay the same. It can never go down.
Of all the innovations that governments and media around the world have come up with, seemingly independently of each other, during the ongoing Covid period, perhaps the most insidious is the daily running total of deaths.
As I write, the number given for Ireland stands at 4,941. And rising.
I have often wondered what the purpose of this number is. At a time when we are frequently told by our betters in the media and in the halls of government to ‘follow the science’, what could be more unscientific than a figure which, even when nobody is dying, looms above us as a warning that danger is ever present and nothing has improved. Bow down before its power, there’s nothing else to be done.
Take the number of people who are unemployed. Here’s a figure that has reached terrifying proportions without any sophistry or assistance from the behavioural science people. In fact, a lot of effort is expended on massaging this number down from the actual amount to levels which are considered more palatable for public consumption.
But imagine that we calculated the number of people who are unemployed by concocting a total of all the people who have been unemployed, at any time and for any duration, during the past 14 months? Or since unemployment began, a running total of all the people who have been unemployed ever?
What function would that number serve? Might it help prevent future unemployment? Might it better inform us of the skills and training required for our workforce? Might it be useful for analysis and reporting? As Frankie Howerd used to say, “Nay, nay, and thrice nay.” I wager any civil servant who proposed such an idea would soon be on their way to early retirement, as popular with politicians as those Gardai who do breathalyzer duty outside Leinster House.
Yet that’s exactly what we do with the running death total (and its near-twin the running case total). If the purpose of this number was to show us where we currently stand amidst the ebbs and flows of the pandemic, then surely a monthly or a weekly total would do the job better. We could then, as we do with the unemployment figure, compare this month to last (or this week to last) and judge which way we’re going. Are we moving steadily forwards? Are we tumbling hopelessly backwards? You get the idea.

Why haven’t we ever had a running total of deaths from cancer, heart attacks or diabetes? If we’d started even a year ago, these numbers would be at impressive levels now. They’d give the Covid tally a run for its money. There’d be opportunities for new betting markets based around causes of mortality, although spread bets might be distasteful for the contagious diseases.
I’m surprised Worldometer hasn’t tried to do something like this. To many of us, Worldometer is the central hub of running Covid death totals. At this very moment, it trumpets a formidable 609,767, deaths for the United States, a daunting 127,782 for the United Kingdom and, as mentioned at the start, a not inconsiderable 4,941 for Ireland.
But what do these frightening numbers refer to? Well, they refer to the number of Covid-19 deaths. So what’s all the fuss about? The fuss is about what constitutes a Covid-19 death. And what is meant, exactly, by a Covid-19 death? Ah, now that’s where it starts to get a bit complicated.
On 16th April 2020, the World Health Organisation (WHO) issued a document entitled “International Guidelines for Certification and Classification (Coding) of Covid-19 as Cause of Death”. This document provided strict rules for the registration of Covid-19 deaths, rules which were fundamentally different to those which were in place for the registration of deaths from other causes.
Some doctors expressed concern about what they felt would give a misleading picture of causes of mortality. These rules, they said, were unprecedented: they would lead to the overreporting of deaths from Covid-19 and the underreporting of deaths from other causes. Their warnings went unheeded and, for the most part, unreported. There was no place for prudence and common sense amid the frenzy and hysteria of the early days of the pandemic.
Since then, however, more and more medical professionals have added their voices to this dissenting chorus. The latest is Patrick O’ Connor, coroner for Mayo and public information officer of the Coroners Society of Ireland.
O’Connor has expressed his discomfort at official reporting of Covid-19 deaths in this country: “I think numbers that are recorded as Covid deaths may be inaccurate and do not have a scientific basis”, he said earlier this month.
Let’s take a look at the International Medical Certificate of Cause of Death (MCCD). For this section I am indebted to Dr. No, the author of the ‘Bad Medicine’ blog, for his succinct explanation of how the MCCD works and how, in practice, the WHO guidelines affect this process. I recommend you read his article about this if you would like a more detailed understanding of the topic.
The MCCD was introduced by the WHO in 1948. Its purpose was to create an international standard for the recording of deaths and to describe the sequence of events which led to a death, rather than just the immediate cause (as was common in many countries at that time).

Frame A (above) is the most important part of the MCCD. It is here that all significant information about a death is recorded. As you can see, Frame A has 2 boxes. Box 1 is for recording the cause of death, Box 2 is for recording contributing conditions. Box 1, the cause of death box, has four lines: the first line records the immediate cause of death, the remaining lines record any conditions which led to the immediate cause of death, with the last line containing the underlying cause of death. The idea is to record the sequence of events which led to the death.
To give an example. A person with diabetes dies from a heart attack, which was caused by heart disease.

So the first line in Box 1 contains ‘Myocardial Infarction’ (the clinical name for a heart attack) because a heart attack was the immediate cause of death. The second line contains ‘Ischaemic Heart Disease’ (the clinical name for heart disease) because this is the underlying cause of death. This is the condition which initiated the sequence of events which culminated in the person’s death: the heart disease led to a heart attack.
The remaining lines in Box 1 are left blank because this person had no other conditions which contributed to the sequence of events leading to their death. Diabetes is recorded in Box 2 because this is a contributing condition, rather than being a part of the sequence of events which led to death. This death will be registered as ischaemic heart disease (or simply heart disease) because this is the underlying cause of death.
Another example. A person dies from internal bleeding due to a ruptured artery as the result of a road traffic accident.

The first line in Box 1 contains ‘Internal Bleeding’ because this is the immediate cause of death. The second line contains ‘Ruptured Artery’ because this is what led to the internal bleeding. The third line contains ‘Road Traffic Accident’, as this was the underlying cause of death: it was a road traffic accident which initiated the sequence of events that led to the death.
In this instance, Box 2 is left blank as there were no contributing conditions. So, the road traffic accident led to the ruptured artery which led to the internal bleeding. This death will be registered as a road traffic accident.
The WHO’s guidelines define a Covid-19 death as “a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID disease (e.g. trauma).” This is an extremely vague definition and one which allows for a rather broad interpretation of what can be considered a Covid-19 death.
As can be seen from the HSE’s website or that of the UK’s NHS, there is a large overlap between the symptoms of Covid-19 and those of any number of other respiratory conditions or Influenza Like Illnesses (ILIs). Any of these other conditions can be considered a “clinically compatible illness”.
You will note that Covid does not have to be confirmed: a “probable” case is sufficient for inclusion as a death. As Dr. No puts it, “If it looks like Covid-19, it is Covid-19.”
The guidance goes on:
A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of preexisting conditions that are suspected of triggering a severe course of COVID-19.”
This is very important. What physicians are being told here is that, when they have identified a Covid-19 death (using the loose “if it looks like Covid” definition), then regardless of any pre-existing conditions which may have triggered severe Covid-19, the death must be registered and counted as a Covid-19 death. This goes against all conventions for identifying the cause of death.
So how does this relate to our MCCD form? Well, in our earlier examples of somebody dying from a heart attack and somebody dying in a road traffic accident, there should be no difference in the way the deaths are recorded. In fairness to the WHO, they are quite clear in their guidance that these two types of death should not be recorded as Covid-19.
(Unfortunately, this has not stopped overzealous authorities around the world from registering heart failure, motor accidents, suicides and murders as Covid deaths).
However, when it comes to most other types of death, we start getting into murky waters.Take the example of a person who dies from pneumonia, caused by immobilisation, which itself was caused by multiple sclerosis.

In this case, the underlying cause of death is multiple sclerosis. Why? Because multiple sclerosis led to immobilisation which led to pneumonia. So this death will be registered as multiple sclerosis.
Now, let’s imagine this person had tested positive for Covid-19.

Notice anything strange? Because of the WHO guidelines, the underlying cause of death is no longer multiple sclerosis, but is instead Covid-19. Multiple sclerosis (and immobilisation) gets moved to Box 2, it’s now been relegated to a contributing condition. This death will be registered as Covid-19. Remember the WHO said in their guidelines:
A death due to Covid-19 may not be attributed to another disease and should be counted independently of pre-existing conditions.”
A further issue with the above example is that the presence of Covid-19 is determined solely on the basis of a positive PCR test result.
According to the WHO’s clinical coding instructions, a death must be registered as Covid-19 if the patient received a positive test result, even if they never displayed any symptoms.
I’ll be looking at the problems with PCR testing in a future article, but it’s sufficient to say here that they are notoriously unreliable, with even the WHO themselves warning of their tendency to produce false-positive results.
So here we have the case of an unfortunate individual whose multiple sclerosis, over many years, caused them to become immobile. Immobility, sadly, can lead to pneumonia which, especially for the aged and/or immunocompromised, often results in death. However, because of the WHO guidance, the presence of a positive PCR result alone means that all of their medical history, the entire chain of events which led up to the person’s death, is cast aside and replaced by the misleading explanation of Covid-19.
But the issue goes even deeper. You’ll recall that the WHO’s definition of a Covid-19 death includes “probable” cases as well as “confirmed” ones. Our final example describes an individual who dies from acute respiratory distress syndrome (ARDS), caused by pneumonia, which itself was caused by chronic obstructive pulmonary disorder (COPD).

As you can see, the underlying cause of death is COPD, which led to pneumonia, which led to ARDS. This death will, of course, be registered as COPD.
But what if this person had had contact with someone known to have Covid-19 or even with a person suspected of having it? Here’s what would happen to the MCCD:

The underlying cause of death is now ‘suspected Covid-19’, which, in the figures we see on the nightly news and in the vast majority of statistics made available by governments, is treated in exactly the same way as a confirmed Covid-19 death. The WHO’s clinical coding instructions insist that it is, so long as the deceased had “contact with (a) confirmed or probable case.” The COPD which caused this person’s pneumonia is cast aside, no longer considered to have played a part in the sequence of events that led to their death.
This is absurd. Yet this is how deaths around the world are now being recorded and registered.
If somebody is dying of heart disease, liver disease, respiratory disease, cancer, dementia or any other terminal illness, and they have a positive PCR test or have simply been in contact with somebody suspected of having Covid, their death is now registered and counted as a Covid-19 death.
Any pre-existing condition, no matter how serious and no matter what part it played in their ultimate demise, is moved to Box 2 of the MCCD and not recorded as the underlying cause of death. The WHO guidelines state, in the section entitled “Comorbidities”, that “if the decedent had existing chronic conditions…they should be reported in Part 2 of the medical certificate of cause of death.”
Conditions which for more than seventy years, since the introduction of the MCCD form, have been understood as underlying causes of death, are now rebranded as contributing factors. All to make way for the mighty Covid.
The result is a massive inflation of the numbers of Covid-19 deaths. As Patrick O’Connor, the Mayo coroner, says, when speaking about terminally ill patients,
If they prove to be Covid positive in a test, it is that (Covid) which is recorded as the principal cause of death — even though that person may have been terminally ill with a short life-expectancy prior to such testing.”
And, as we have seen, a test is not even necessary, as the WHO’s guidelines instruct physicians to include “probable” with “clinically compatible” illnesses in the tallies.

Patrick O’Connor
Even before the WHO issued their guidelines on 16th April last year, Italian authorities had been using a similar method to register Covid deaths, with 88% of patients there (up to 20th March 2020) having at least one comorbidity and many having two or three.
In addition to hugely inflating the number of deaths from Covid-19, this bizarre way of counting also distorts the mortality rate of the disease, making it seem far more deadly than it actually is.
In 2020, a total of 73,444 people died in England and Wales with Covid-19 recorded as their underlying cause of death. In response to a freedom of information request, on 29th March 2021, the UK’s Office for National Statistics revealed that only 9,400 (12.8%) of that number were recorded without pre-existing conditions.
On July 3rd last, Ireland’s then acting Taoiseach, Leo Varadkar, tweeted,
In Ireland we counted all deaths in all settings, suspected cases even when no lab test was done, and included people with underlying terminal illnesses who died with Covid but not of it”
… revealing that the numbers of Covid-19 deaths in Ireland were vastly exaggerated and in no way reflected the lethality of the disease in this country.
Although the complete death statistics for 2020 have not yet been made available for Ireland, two weeks ago Kildare coroner Professor Denis Cusack published a report analysing deaths in that county during the pandemic. Of 230 deaths recorded with Covid-19 as the underlying cause, 228 (99.13%) had pre-existing conditions.
I would have thought that this was a significant finding, that fewer than 1% of the people who died from Covid-19 in County Kildare did not have comorbidities. But, like anything else that doesn’t fit in with their campaign of terror against the Irish people, the Irish media was having none of it.
While both RTE and The Irish Times gave coverage to Professor Cusack’s report, neither had anything to say about the 99.13% of Kildare’s Covid dead who had pre-existing medical conditions. Nor was there a mention of the average age of death in this cohort being 82.2 years of age.
Both news services instead chose to focus on selected aspects of the report which they used to support the ‘lethal virus’ narrative they have long favoured. Is this censorship? Maybe it’s just extremely poor journalism.
The running total of deaths is one of the pillars that supports this whole charade. The narrative of a deadly pandemic would never have worked without the impression of huge numbers of fatalities, countless lives ‘lost to Covid’. The unprecedented changes in the way deaths are counted allowed this to happen.
You would imagine such a fundamental change, one which has had such a colossal impact on every man, woman and child on the planet, would be widely reported and discussed. Yet it is almost impossible to find a mention of it anywhere in the mainstream media.
Although most of us have suffered under the heel of draconian Covid regulations, and will continue to suffer, some have profited greatly from this fiasco. We have seen how health scares have been manipulated for gain in the past, none more so than the Swine Flu pandemic that never was, in 2009, when governments, the WHO and pharmaceutical corporations colluded to profit at our expense.
There needs to be an urgent investigation, on a global scale, to find out how the Covid pantomime was allowed to happen. And we need one in Ireland, to determine who knew what and when, and exactly who has benefitted.

The current narrative being spun in Ireland is that we are close to ‘finding a way out’ of lockdown and that, if we behave ourselves, we might be permitted some limited freedoms during the summer. This is hardly surprising. We’re coming to the end of coronavirus season, which means it’s so much harder to inflate ‘cases’. And because mortality rates in the northern hemisphere are typically at their lowest during the summer months, it’s not as easy to attribute huge numbers of deaths to Covid-19. It was the same last summer.
But the government has been preparing for this. Already, there are 5 walk-in testing centres in operation in Ireland, with many more planned – a perfect way to boost the numbers up and keep us on our toes for the summer months. And, of course, the government reserves the right, at any moment, to slap us all back into lockdown.
At the same time, it has been made abundantly clear that whatever limited freedoms we might be permitted will be contingent on mass vaccination and, before long, vaccine passports and digital identity.
And don’t forget, coronavirus season comes around again in September. But, as we have seen, the lethality of this disease, for which we’ve radically changed the way we live and have forsworn so much of our freedom, has been blown out of all proportion by the fraudulent way in which deaths are registered.
We suffered under austerity for a decade. It’s hard to believe that the same politicians who decimated our health service, causing untold hardship and death, now want to protect us.
Do we trust they are spending our money honestly and wisely? How much is being spent on mass vaccination, testing, tracing, the vaccine passport infrastructure? And what is the cost of the Covid period to our economy? The whole circus makes a mockery of the years of austerity and of every person who suffered because of them.
Then there is the cost to our health.
Many have lost their lives because of this deception, but you don’t see a running total of their deaths on the news every night. How many have died due to a lack of primary health care, which has been sidelined and neglected, sacrificed at the altar of Covid? How many cancelled surgeries and missed screenings? What about those in urgent need of treatment who were too frightened to attend a hospital? And those who were turned away before they even reached a hospital, because Gardai at a checkpoint deemed their need not sufficiently urgent?
The mental health of our nation has taken a nosedive, not due to Covid but because of lockdowns and other unwarranted sanctions against our people. Loneliness, depression and despair have all taken their toll. The US Centres for Disease Control and Prevention (CDC), hardly a radical anti-lockdown stronghold, has estimated that one third of all excess mortality in the United States during 2020 was due to reasons other than Covid-19.
We’ve been deceived. When important facts are left out of a narrative in order to foster a misconception, we call it lying by omission. We have been lied to by politicians, public health officials, wealthy media barons and the stooges who write for them. And we have paid a terrible price. In the twilight of our freedom, it’s time for us to stand up for the truth.
Bernard Marx is the pseudonym used by a writer and teacher based in Ireland. Bernard’s areas of interest include history, politics and popular music. You can read more his work are Notes from the New Normal
TRANSHUMANISM: THE WAR ON HUMAN NATURE
By Dave Cullen | June 1, 2021

Dave Cullen’s latest video throws further light on concerns about the Fourth Industrial Revolution – transhumanism. Smart cities and VR matrix style existence is likely not the plan set out for us by the globalist elite.
The vast majority of humanity is being rendered obsolete. The fourth industrial revolution is a further indicator of this. Humans are assets only as long as their labour has production value. As the fourth industrial revolution takes hold, the production value of humanity will reduce to zero, and therefore humanity will become a liability.
Cullen indicates that the globalist billionaire class are not going to build smart cities for us “liabilities”. They will not plug us into a wonderful new matrix. The media and government are engaged in mass deception of this agenda – it is all smoke and mirrors covering the most probable outcome, which is the mass culling of liabilities.
More at www.bitchute.com
Israel, Don’t Raise the Roof Beams High As You “Resettle” Lifta; Its Owners Will Return

By Rima Najjar | Global Research | June 1, 2021
The latest crisis in Palestine cannot be set aside as another passing episode in Israel’s forever war against the Palestinian people.
We are now witnessing shocks within Israel behind the Green Line, something that Israel had hitherto been able to contain. In the process, it pretended, along with much of the western world, that it is the “longest-lived democracy in the Middle East” and that only its continued occupation of the West Bank and its harsh blockade of Gaza undermine its “constitutional ideals”- ideals now exposed for what they’ve always been: Jewish supremacist in nature.
We know, as CJ Werleman wrote in Inside Arabia on May 14, 2021,
“Israel is a country built on racism, dispossession, and genocide. The recent rise in attacks by Israeli settlers, vigilante groups, and lynch mobs targeting Palestinians are a continuation of that history and must be addressed.”
There is an unbreakable thread between the Palestinian man lynched by Israeli Jews on the pavement after being pulled from his car in Jaffa and then beaten unconscious recently and the killings and massacres at the hands of Zionist militia in Jaffa and elsewhere in 1948 that resulted in the deaths of hundreds of Palestinian civilians, as recounted by Israeli historian Benny Morris.
The myth, amplified by Wikipedia, is that historians [presumably Israeli] disagree “concerning the effect these killings and massacres had on the Palestinian refugee flight and whether or not these killings and massacres were carried out with the intent of hastening it.”
Palestinian historians have absolutely no doubt about what happened then and why, just as we Palestinians have no doubt about what is happening now in occupied Jerusalem and the rest of the West Bank, in Gaza and in several towns and cities behind the Green Line where Israel has imposed states of emergency — and why.
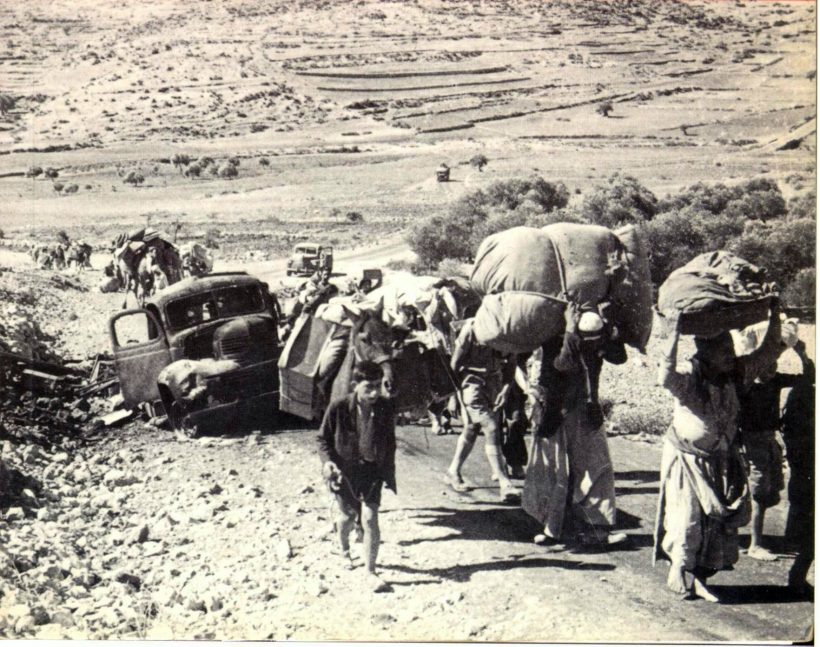
Take, for example, my own father’s village of Lifta on the northwestern edge of Jerusalem. It is the last remaining Palestinian village that was ethnically cleansed of its population in the 1948 Nakba. Now, Israel is set to destroy what remains of it.
The Jerusalem Post (JP), an Israeli English newspaper where facts are shaped by a narrative driven by Zionist values instead of knowledge, reported on this deeply disturbing piece of news this month by denying, like those Israeli historians who are still disputing historical facts, that any ethnic cleansing took place in Lifta — apparently, my grandfather just up and put his eight children and wife in a truck and abandoned his home so that, 73 years later, his village would be “resettled” by Israeli Jews and a luxury hotel built there.
The Israeli newspaper published the following shameful headline:
“Arab village of Lifta, abandoned in ’48, to house new Israeli neighborhood: The western neighborhood in Jerusalem which was abandoned in ’48 will be resettled with 259 housing units, including a luxury hotel.”
A report by Hidden Palestine: a News & Media Website, which, unlike JP, is a site driven by a narrative that values freedom from oppression, provides us with the following facts:
The Israeli land authority announced this month that it is taking bids from construction companies to take charge of the real estate development of Lifta, with the contract set to last 98 years.
The agreement includes the construction of 259 buildings, as well as commercial and business units, in addition to a hotel. If it moves forward, the deal would also see the majority of the Palestinian village’s remaining buildings razed to the ground.
Thanks to petitions by its past Palestinian residents, Lifta was declared as one of 25 endangered sites on the 2018 World Monuments Watch list. It also appears on UNESCO’s tentative list of World Heritage Sites, which has led to threats from Netanyahu that Israel would withdraw from UNESCO.
Lifta has few parallels anywhere in the world. The Palestinian village, lying on a slope at the entrance to Jerusalem, is the last ethnically cleansed Palestinian village to be frozen in time. Here, hundreds of beautiful Palestinian stone houses have continued to stand the test of time, empty and neglected for the past 73 years.
With a history dating back at least 700 years as a Palestinian Arab village, Lifta was among the wealthiest communities in the Jerusalem area, and the women were known for their fine embroiders. Thob Ghabani bridal dresses were sewn in Lifta, which were made of ghabani, a natural cotton covered with gold color silk floral embroidery produced in Aleppo. The village’s clothing stores attracted Palestinians and Arabs from across the Levant.
The entire population was forced out following brutal attacks by the invading Hagannah militias in early 1948. It is an incredible but depressing place to visit, and its destruction would contribute to the continued erasure of Palestinian culture and heritage.
The Jerusalem Post’s story made it sound as though the “resettling” of Lifta was a preservation and development project. What it is, in fact, is a rewriting of history.
Destroying Lifta destroys opportunities for Palestinians to uncover the past of both Palestinians and Israelis: “Lifta has a lasting value in its own right, as it can link restitution to the right of return. Moreover, its preservation will be an opportunity to assert the restoration of dignity in the Palestinian as well as the Jewish community. Finally, by halting the new development in Lifta, UNESCO will affirm its global credibility in response to cultural cleansing.” [See LIFTA AFTER ZIONIST PLANNING and PLANNING AS A CRIMINAL ACT]
Israel’s expulsions of Palestinian families from their homes in Sheikh Jarrah and Silwan, Jerusalem neighborhoods just outside the Green Line, are motivated by the same Zionist objective that resulted in the expulsion, also known as ethnic cleansing, of Palestinians like my family from Lifta, which is just inside the Green line. (See Israeli 2019 map of so-called “Greater Israel” below with Lifta, Sheikh Jarrah and Silwan circled). That objective is Israel’s desire to Zionize/Judaize all of Jerusalem and all of Palestine.
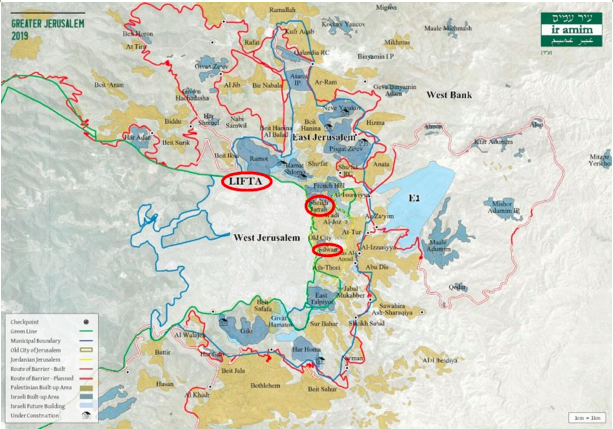
Israeli 2019 map of so-called “Greater Israel” below with (left to right) Lifta, Sheikh Jarrah and Silwan circled
I hope the ongoing worldwide protests on social media against Israel’s crimes will now add the rallying cry of #SaveLifta, in addition to #SaveSheikhJarrah and #SaveSilwan.
If you are still in doubt about Israel’s intention, listen to two Palestinian citizens of Israel reacting to the message they have heard loud and clear all their lives from successive Israeli governments:
Eva Najjar, Haifa-based lead designer and developer at Just Vision, writes:
“I knew I was bringing my children into an ethnic-supremacist state when they were born. But after these past weeks, I don’t know how I can continue to raise them here.” (In The Washington Post : Palestinian citizens of Israel like me are facing terrifying new attacks)
Diana Buttu wonders:
“How do I explain to my 7-year-old son what being a Palestinian citizen of Israel means? What future can he look toward, when the leaders of the government incite hatred against him? What audacious hope can he have when he is bound to face racism and discrimination in education, employment and housing? For now, I try to shield him from the images on television and on our phones, but there will soon come a time when I cannot shield him from the reality that he is surrounded by people who consider him a second-class citizen.” (In The New York Times : The Myth of Coexistence in Israel)
I am heartened by the United Nations Human Rights Council (HRC) Special Session held on May 27, which for the first time has included a geographic scope encompassing Israeli violations targeting the Palestinian people on both sides of the Green Line.
Israel’s institutionalized regime of racial domination and oppression targets the Palestinian people as a whole, including those no longer in Lifta through no fault of their own, who have more right by far to reconstruct their homes in Lifta than Israeli Jews have in constructing housing and luxury hotels to “resettle” the village. We will return, so don’t raise the roof beams high, Israel.
*
Rima Najjar is a Palestinian whose father’s side of the family comes from the forcibly depopulated village of Lifta on the western outskirts of Jerusalem and whose mother’s side of the family is from Ijzim, south of Haifa. She is an activist, researcher and retired professor of English literature, Al-Quds University, occupied West Bank.
Revealed: The American Money Entwined with Israel’s Jewish Terrorist Groups
By Jessica Buxbaum | MintPress News | May 28, 2021
JERUSALEM — As Israel rained rockets down on Gaza in mid-May, inside 1948-occupied Palestine (Historic Palestine and modern-day Israel), another kind of Israeli terror emerged. Jewish supremacists stormed cities with high Palestinian populations chanting “Death to Arabs!,” attacking scores of Palestinians and vandalizing their properties.
The mob violence killed two Palestinian citizens of Israel, according to the Mossawa Center: the Advocacy Center for Arab Citizens of Israel. And despite calls for calm, the attacks are ongoing. On Thursday, a Jewish mob dragged a Bedouin driver out of his car and beat him with glass bottles in northern Historic Palestine. Earlier, footage posted on social media showed Arab gas station workers lying on the ground after being surrounded and beaten by a Jewish mob in the town of Binyamina:
The American Jewish community condemned the wave of anti-Palestinian violence, under the assumption these attacks stem from the fringes of Jewish society. In reality, however, these Jewish supremacists receive financial support from a network of charities in the United States.
Jewish extremists organizing online
As the Israeli government orchestrated a bombing campaign on Gaza, right-wing Israeli activists were coordinating their own war-like operations online.
According to HaBloc, an Israeli nonprofit organization monitoring anti-democratic activity, tens of new groups have been created in the last two weeks on WhatsApp and Telegram. The number of participants in each group ranged from the tens, hundreds, and even thousands. About 2,200 people in total were active in these groups.
HaBloc’s observation of these ultra-right-wing groups reveals how they used social media to organize attacks in advance offline. The groups exchanged information, sold weapons like knives, bats, and pepper spray, used inflammatory rhetoric such as calling for revenge against Palestinian citizens of Israel and documented themselves rioting in the streets.
“This is far more than what’s happening on a daily basis within the far right in Israel,” Ran Cohen, co-founder of HaBloc, said of the extremist activity.
News media reported that the main groups behind the recent rampage were Lehava, a Jewish supremacist organization opposing assimilation and coexistence, and La Familia, a far-right group supporting the Israeli Premier League football club Beitar Jerusalem.
The Israel Religious Action Center (IRAC), the public and legal advocacy arm of the Reform Movement in Israel, has been monitoring Lehava’s activity for more than a decade.
“Lehava is an organization that claims to work against assimilation, but basically wants to create a Jewish-only space in Jerusalem and in Israel in general,” Rabbi Noa Sattath, IRAC’s director, told MintPress News. “In this last wave of violence, they were certainly instigators in several of the cases.”
IRAC demanded Lehava be labeled a terrorist organization in a letter sent this week to Israeli Minister of Defense Benny Gantz, Attorney General Avichai Mandelblit, and Head of the Shabak (General Security Service) Nadav Argaman.
Researchers within HaBloc, cautioned, though, attaching the violence to specific organizations.
“The role of Lehava in what happened is not direct,” HaBloc said. “It’s not like there was a central command and they’re sending people into the streets. It was really something that sort of spread out in a more organic way.”
“But the infrastructure and the ideology of Lehava is present and it contributes to what happened in the past few weeks,” HaBloc added.
The American charities bankrolling Lehava
Ben-Zion Gopstein is the leader of Lehava (or “flame” in Hebrew) and founded the organization in 2005. He is a notorious right-wing activist and disciple of Rabbi Meir Kahane, an American-Israeli extremist who founded the Kach Party, a political movement espousing racist beliefs.
After a brief stint in the Knesset (Israeli parliament) in the 1980s, the Kach Party was banned from Israeli politics and deemed a terrorist organization by both Israel and the U.S.
Kahane called for the expulsion of Palestinians and Arabs from the Holy Land and advocated for the outlawing of marriage between Jews and non-Jews.
Four years after Kahane’s assassination in 1990, Baruch Goldstein, an ardent Kahane follower, opened fired at the Ibrahimi Mosque in Hebron—killing 29 worshippers.
Kahane and Goldstein have become revered within the Israeli settler movement. Settlers have shared Kahane’s teachings on social media and have prayed at his grave.
Lehava is considered the successor to Kach, and Kahane’s racist ideology, Kahanism, runs deep within Lehava circles.
In addition to following right-wing interactions online, HaBloc’s research has also found a complex web of nonprofits in Israel and the U.S. connected to Lehava.
Lehava is not a registered charity in Israel so it can’t accept donations. Instead, money is funneled to Lehava through the Israeli nonprofit, the Foundation for the Salvation of the People of Israel, or Hakeren Lehazalat Am Israel in Hebrew. Israeli fund, Chemla or “mercy” in Hebrew has also been linked to Lehava until about 2014, according to HaBloc.
The Foundation for the Salvation of the People of Israel did not respond to requests for comment via email. The email address may be Gopstein’s as “benzion” is part of it. When contacted at the telephone number associated with the organization’s GuideStar (a nonprofit database) profile, the person said this was not the foundation and hung up. Contact information for Chemla is not publically available.
Two tax-exempt charities in the U.S. fund Kahanist activity in Israel: Charity of Light and the American Friends of Yeshivat HaRa’ayon HaYehudi.
Charity of Light funnels money to Chasdei Meir (which translates roughly into “charity which shines” in Hebrew). Chasdei Meir was named after Kahane, according to the fund’s website. As evidenced on Charity of Light’s tax returns, Chasdei Meir is related to the Chemla Fund. Charity of Light donated $72,000 to Chasdei Meir/Chemla Fund in 2018, according to its most recent tax filing.

Armed members of Chasdei Meir are shown wearing jumpsuits emblazoned with portarts of Meir Kahane
The American Friends of Yeshivat HaRa’ayon HaYehudi directly supports Yeshivat HaRa’ayon HaYehudi or the Jewish Idea Yeshiva, a Jewish education institution founded by Kahane.
“This is sort of the place for indoctrination of Kahanist ideology,” HaBloc said. “It’s where Benzi Gopstein studied and other prominent Kahanist figures.”
The charity gave $154,000 to Yeshivat HaRa’ayon HaYehudi in 2018, according to the most recent tax report. The yeshiva is even classified as a terrorist organization by the United States. The yeshiva’s dean, Rabbi Yehuda Kroizer, is also part of Chasdei Meir. The yeshiva did not return a request for comment.
The nonprofits’ tax filings list Levi Chazan as the director of Charity of Light and American Friends of Yeshivat HaRa’ayon HaYehudi, and Steven Goldrich is listed as a director of Charity of Light and treasurer of American Friends of Yeshivat HaRa’ayon HaYehudi. Chazan was convicted in a 1984 bus shooting in the Occupied West Bank, which wounded seven Palestinians. Both did not respond to requests for comment.
HaBloc explained this entanglement of Israeli and American organizations is not directly supporting Lehava with monetary contributions, but rather aiding the network around it.
“The relationship between [Lehava] and groups that are funded with American money are two separate issues,” HaBloc’s Cohen said. “There are connections, of course, but we cannot say that these groups that were active in the last two weeks were funded with American dollars.”
Other financial players
The aforementioned charities are largely linked to Kahanism and Lehava, but other American foundations have also been tied to Israeli extremism.
The Traditional Fund gave $51,000 to American Friends of Yeshivat HaRa’ayon and $11,500 to American Friends of Chasdei Meir in 2018. The American Friends of Chasdei Meir is not listed in any available nonprofit database, however, Chasdei Meir’s website does name the American Friends of Chasdei Meir as its contact. The Traditional Fund did not respond to press inquiries.
According to T’ruah: The Rabbinic Call for Human Rights, the Central Fund of Israel (CFI) funds Chemla and Yeshivat HaRa’ayon HaYehudi. The organization filed a complaint with the Internal Revenue Service (IRS) in 2018 to revoke CFI and the American Friends of Yeshivat HaRa’ayon’s charitable status on the grounds these groups are funding terrorism.
IRS charity law states that terrorist activities are considered substantial means for disqualifying an organization’s tax-exempt status. This is in accordance with engaging in illegal acts contrary to standard U.S. policy.
A litany of private foundations supports the CFI. Most notably, the foundations belonging to the late American billionaires Sheldon Adelson and Irving Moskowitz. The Moskowitz family foundations have contributed more than $8 million to CFI since 2018 and Adelson’s foundation gave $50,000 to CFI in 2018.

Israeli soldiers and settlers attack Palestinian protesters in the Occupied West Bank town of Salfit, Nov. 30, 2020. Majdi Mohammed | AP
Jay Marcus of CFl said in a statement to MintPress News that, “The Central Fund of Israel absolutely rejects violence and does not support any organizations that promote violence. Furthermore, if an organization that we once supported ever started promoting violence, CFI would not support them in the future.”
Marcus claims that he hasn’t heard of Lehava, adding, “having had rockets indiscriminately showered down on my head, I would certainly disagree with your myth about which ‘groups start violence.’”
The Falic family, owners of the major retail chain Duty Free Americas, has supported The Fund for Saving the People of Israel in the past, providing a total of $60,000 to the association from 2007-2017. The money is wired through the Falic’s Israel-based foundation, the Segal Fund. The Falics could not be reached for comment.
Kahanism’s surge in Israel
Kahane’s Kach Party was banned from entering Israeli politics in 1988. But thanks to Israeli Prime Minister Benjamin Netanyahu, Kahanists are now infiltrating the halls of the Knesset (Israeli parliament).
In the lead-up to Israel’s March election, Netanyahu pushed for a right-wing alliance with Itamar Ben-Gvir, a Kahanist, a defense lawyer for price tag campaigners, and leader of the far-right Otzma Yehudit (Jewish Power) party. Otzma Yehudit partnered with the anti-LGBTQ Noam Party and the National Union-Tkuma faction to form the Religious Zionism bloc in the last election. The coalition allowed the electoral list to secure six seats in the Knesset and for a Kahanist to gain political power. Rabbi Sattath pins the blame squarely on Netanyahu for Jewish supremacists’ rise in government.

A Jewish settler wears a T-shirt with the image of Meir Kahane near the city of Ramallah. Bernat Armangue | AP
“Because the prime minister was in such a dire situation and was desperate for every vote, he gave [Otzma Yehudit] the legitimacy,” Rabbi Sattath said. “What we’re seeing here in Israel and around the world is that one of the symptoms of democracies in decline is when the extreme right takes over the center right. The fact that the prime minister and some of the right-wing parties gave the Jewish Power Party legitimacy has then increased their power. And that’s what enabled them to use these methods they’ve used for over a decade on a large scale in the last wave of violence.”
Upon reflecting back to Kahane’s short time in the Knesset, Rabbi Sattath said he faced opposition from every politician and was immediately ostracized.
“When he got into the Knesset, he got the bare minimum [of votes] to get one seat. But what happened in the eighties was he was boycotted by every other Knesset member. Nobody would sit in the plenum when he was speaking,” Rabbi Sattath said. “Everybody from the left and the right understood that these ideas were dangerous and extreme and had to be restrained.”
Today, the political climate in Israeli politics is different.
“What we’re seeing now is that the restraint is completely over,” Rabbi Sattath continued. “And we’re hoping that by shedding light on the past weeks’ violence, we can return to the understanding that there needs to be a red line, that these violent militias and racist, Jewish supremacists have to be stopped.”
Jessica Buxbaum is a Jerusalem-based journalist for MintPress News covering Palestine, Israel, and Syria. Her work has been featured in Middle East Eye, The New Arab and Gulf News.
COVID Corruption: Assaulting Human Norms

By Omar Khan | Uncommon Wisdom | May 31, 2021
Well, the seminal errors of the Covidian narrative stockpile so fetidly, you keep thinking one day, the stench will be so overpowering, that even those who have essentially put their critical faculties into suspended animation, will rally, finding that this reeks to high Heaven. Some restoratives surely, we think, will thaw their frozen wits.
I keep meandering back through the history of this ill begotten assault on life and liberty.
Imagine this being designated a “novel” Coronavirus. Well, if it was “massaged” in a Wuhan lab as it now seems all the craze to assert, perhaps there was some novelty to it. Otherwise, as we are advised, there are numerous coronaviruses parading around. Even C-19 is now relegated to only being the fourth most widespread in the US.
And now we find, from antibody tests and more, that some varietal was already doing the circuit in 2019. At any rate, some prior immunity exists. And if this is truly the descendant or even Frankensteinian stepchild of SARS, then as former Chief Medical Officer of Pfizer, Michael Yeadon has reminded us, though it is 80% identical, the immune systems of those exposed to SARS seem to “recognize” SARS-CoV-2, even these 17 years hence. Novelty therefore takes another nosedive.
So, this first assertion, right out of the gate, meant to terrorize us by suggesting an unknown pathogen without parallel, that could hoodwink our immune system completely, was poppycock. And we knew soon enough, it was far more infectious than SARS, but far less lethal. And mortality is where we should have kept our eyes fixed, not the delusions of asserted “cases” from unreliable tests. So, no, not so “novel” at least in impact.
Then, you have to wonder, if even mistaken as “novel,” surely there would be extraordinary curiosity, not fixated dogmatism, about this pathogen. However, it took only a few months, before torrential disdain was showered on any who raised questions as to whether we were over-reacting.
There was censorious outrage lavished on some of the world’s most eminent research experts in meta-analysis like John Ioannidis of Stanford, when he pointed out the lethality seemed less than was being forecasted for example, or when the Diamond Princess Cruise Ship kindly offered itself up as a floating case study, or when Knut Wittowski “sacrilegiously” suggested sunshine and fresh air are lethal to viruses with seasonality as a fairly evident way to corroborate that, and so many others. They were literally chased from the public sphere.
They have been only vindicated since, and why rationally, anyone actually interested in public health as a leader, wouldn’t have wanted a big tent of diverse views, a kind of Manhattan Project to tackle this virus and grapple with providing care, cannot be logically answered, except by accepting they were engaged in a charade of public health only, and other agendas were afoot that could brook no dissent.
In fact, if you consider it, how could they know who to censor? In other words, how with a “novel” coronavirus, could you have so readily stress tested alternatives to arrive at any credible consensus by then? Surely if genuinely interested in leadership and health, immensely experienced and credible experts indicating we may be overzealous, that this may be less deadly, more treatable and more manageable, would be manna from heaven. Such views would surely be welcomed, and would be carefully assessed, with trials done before the world was blown up, and irrevocable harm done to urban centers, small businesses, people needing desperate attention for other health issues, and before children’s lives and educations were turned topsy turvy. Yes, “if.”
By the way, it wasn’t even just Ioannidis and Wittowski. Similar alarms were raised and alternatives suggested by luminaries as diverse as Dr. Sucharit Bhakdi, specialist in microbiology and one of the most cited research scientists in Germany; Dr. Pietro Vernazza, Swiss specialist on Infectious Diseases at the Cantonal Hospital St. Gallen; Professor Hendrik Streek, Professor of virology and director of the Institute of Virology and HIV Research at Bonn University; Dr. David Katz founding director of the Yale University Prevention Research Center; Dr. Peter Goetzsche, Professor of Clinical Research Design and Analysis at the University of Copenhagen; Dr. Sunetra Gupta, Professor of Theoretical Epidemiology at the University of Oxford and later co-author of The Great Barrington Declaration; Dr. Anders Tegnell, that sainted man, Swedish State Epidemiologist who showed the world all of these contrary views were essentially right; Dr. Pablo Goldschmidt, Argentine-French virologist, Professor of Molecular Pharmacology at Universite Pierre et Marie Curie Paris; Dr. Jay Bhattacharya, Professor of Medicine and Public Health at Stanford and later co-author of The Great Barrington Declaration; Dr. Tom Jefferson, British epidemiologist based in Rome; Dr. Michael Levitt, Professor of Biochemistry at Stanford; German Network of Evidence Based Medicine… and so many more (distillations of their points can be found archived on Off-Guardian who collated these remarkable instances of “informed lack of consent.”)
When such a phalanx of experience, talent and credibility speaks at a seemingly desperate time, how could jurisdiction after jurisdiction, pillory them, ostracize them, mischaracterize what they had to say? Why that, rather than be desperately curious, and gratefully keen to explore their insights?
This is particularly so as you cannot possibly imagine that this constellation of talent had any motivation other than wishing to save and serve our global and local cultures, lives and livelihoods. And that they have continued to do so, despite media attacks, smears, economic disincentives, renders every word more plausible. After all, we know there are evident incentives of being proponents of the prevailing mythos. We cannot assert any incentive other than integrity and genuine conviction for refusing to acquiesce to the pervasive gaslighting and whitewashing.
Mass Manipulation
While stifling what should have been real life-lines, and once more we are seeing virtually all of their assessments vindicated today, we were run over by a freak-show of blatant stupidities.
With constant panic porn flashing incessantly, a multi-billion dollar industry of fraudulent tests is pushed through a 2-day peer review, by Dr. Doom (Drosten, who helped create the application of the test, sat on the review board of the publication “validating it” and profits from the tests that were mysteriously ready for production and shipping almost ahead of need). We were to ignore demonstrations of false positives, the need for amplification settings to be below 30 (WHO and others initially set them between 35 and 45, at the latter, a papaya fruit tested positive), as well as clarifications the test is not meant to be diagnostic (as per its inventor and as per the literature found in each test and finally “confessed” to post Trump by WHO as well).
And in one of the greatest bits of medical fraud, in plain sight, known by all, but still glossed over, a “case” was converted from someone who had symptoms to “someone who tested positive.”
The latter could be manipulated by the above settings, further counted on to be magnified via false positives, which ironically get worse in percentage terms as incidence goes down. The whole world held hostage to the vagaries of a non-diagnostic test, whereas had we focused on the symptomatic, no one would even have known we were in more than a really ugly influenza season.
Next, we were invited to ignore the age stratification, as the median age of death was over 80. So, lest people be cut down in the bloom of their 70’s and 80’s (and even there we can improve their odds with early treatment, which has been scrupulously avoided, or again smeared, or else “slow walked” almost catatonically en route to being reviewed), we were ready, for the first time in history, to quarantine the healthy!
We asserted “asymptomatic transmission” of which no credible instance has been found in over 14 months, being confirmed again and again even with the recent UK trials done with 9 large, teeming events that barely scraped together 16 “cases” from 60,000 people applying no COVID protocols, including a football FA Club Final and Brit Awards. You will have noticed, a very appreciable lack of media coverage of this “welcome” news. And the US CDC, now in the “vaccine selling” business has instructed clinics to only count as an instance of post-vaccination reinfection, those who, wait for it, have “symptoms.” The blood curdles at these fork tongued guideposts.
So, when the authors of The Great Barrington Declaration pointed out that when risk profiles are so vastly different, we should address and target care accordingly, there was howling and venting and the attacks were unleashed far and wide. They had pointed out this particular pathogen seems to focus on the elderly and so this pandemic tracks normal mortality and therefore in terms of both population size and adjusting for age, is considerably less lethal than the Hong Kong Flu of 1968 and the Asian Flu of the late 50’s, saying nothing of the epochal Spanish Flu in 1918 which infected one third of the global population of that time of which 10% perished!
By comparison, the current Indian death tally after all the shamefully imbalanced reporting is about 325,000 (despite the most egregious liberties with death certificates there, reported on by 161 doctors from N.I.C.E, National Influenza Care Experts, on May 24th in a letter to Prime Minister Modhi claiming guidelines given to them indicate that if PCR test is positive, even if someone died of accidents or clearly of other causes, the cause of death is to be recorded as C-19). Yet applying conventional death certificates, where only direct causation led to an entry, India lost 20 million in the Spanish Flu.
Painfully but necessarily, life went on. High time to adjust our hackles… and self-imposed shackles.
The Indian instance cited above is simply symptomatic of another fraud we embarked upon early on, taking liberties with how death certificates were filled out. Riddle me this, if truly so lethal, why was this necessary suddenly, after norms of indicating primary cause of death were the mainstay of medical practice for decades?
Why did we have to, in the US, incentivize via insurance, labeling COVID deaths? Why in the UK did we originally say anyone tested positively in the last 6 months, irrespective of comorbidities was a COVID death? This shrieks of outright dark comedy or at least ludicrous parody. But that was “fixed” to only doing that for those who tested positive in the last 28 days! So no one knows. Families have howled outrage, reported of course in secondary media, about their loved one being mis-tagged in this way, when they clearly passed from other causes. Who cares? Can’t interfere with the noxious narrative. In parts of South Asia, with cancer and blood poisoning along with a positive test on the death certificate, you guessed it, COVID wins the prize!
And the booby traps for sanity abounded. And the question to be asked is, why? For example,
why do we “lock down”?
This is a penal remedy, never applied before, disdained in public health literature until 2020, indicated in a 2019 report by WHO to
“not be done in any circumstances.”
One month in Wuhan blows up centuries of experience? Really? Are we welding doors shut next? Or staging collapsed bodies on streets with people in alien suits standing over them (you wondered about all those UFO sightings… voila!)?
As Dr. Risch of Yale has pointed out, with such tonic simplicity, “locking down” is not even coherent once the pathogen has spread! It’s fairly obvious once that’s pointed out. And it’s airborne, and almost all infections are in tight indoor spaces. Anyone not pledging fealty to a cult religion, can work this out. And in the face of non locked down jurisdictions with open societies and economies (US States, Sweden, Bulgaria) flourishing, and 30+ studies confirming no benefit from this illogical imposition, and the Oxford Stringency Index showing an inverse relationship between degree of shutdown and health outcomes, we are truly “stoned” on some narcotic to keep invoking this. Oh, and the belligerence if you question it, as if some canonical certainty was being desecrated.
Masking was not recommended by Fauci or WHO, and suddenly realizing that it could be a signature of totemic compliance, it was asserted, though study after study and simply common sense indicates it is a life leeching absurdity, to have you inhale your own waste, while choking off your oxygen supply. As one eminent, also censored, once tenured professor of Physics, Denis Rancourt says,
“The magical ‘one way mask’, which does not protect the wearer but acts as ‘source control’, is an invention of propaganda. It is contrary to the physics of breathing aerosol particles suspended in the fluid air. It is ridiculous fantasy.”
Frankly, the size of the particles are so small as to make this beyond fantasy. And if we truly believed they captured viral particles, would we blithely be leaving these masks lying around, or even throwing them in the open trash, so their harvest can waft at will? The boxes the cloth masks come in, have disclaimers to confess they don’t protect you against C-19. After all, they have openings so you can breathe and see. And there is no correlation between masking or its absence and COVID results. Again, the open US States have put that to rest. But thou must not question! “They say,” is the holy homily, and it must prevail.
So the round-up is: stifle dissent (which admits we have an agenda), create a “test” that doesn’t test and which can be manipulated, change all the guidance based on one month in Wuhan and Italian nursing home deaths (of which later authorities said 12% only could be directly ascribed to C-19), “order” indefinite mass incarceration, and decide without debate that this one source of harm, this one consideration, trumps everything else in the world: health, wealth, family, work, education, poverty, everything.
Why? Who says? A few models. Hmm. Sounds pretty sane. I’m ready to jettison everything I worked for, lived for, my city, culture, neighborhood, travel, way of life, on “asserted apocalypse” without discussing less destructive mitigation with a slew of the world’s most eminent doctors and scientists who say, based on data, we can do better. No agenda there. And if you don’t want the above poison pill, you’re out to kill everyone!
You’re out to kill me, the holy, carcass preserving, center of all global paranoia, me!
Vaccinating Sense
I don’t want to go over past ground to make the necessary point here. As medical luminaries like Dr. Peter McCullough and Dr. Pierre Kory and many others have pointed out, we know there are clearly effective, preventive treatments, and even some real treatments post hospitalization far more effective than the ‘wait and see’ nihilism that so many of these doctors at the forefront of treatment consider “medical malpractice.”
Of course, these treatments were slandered, fraudulently attacked, even though these are widely in use, no side effects, with multiple studies and numerous countries where they’ve been shown to work magnificently (Mexico, India, Zimbabwe, South Africa, parts of the US and more). But since our so called “vaccines”, perhaps the real “point” of this whole inhuman grotesquerie, are only approved tentatively for “emergency use” (safety trials won’t be complete until 2023), then other treatments if established, would remove “the emergency necessity” and that would jeopardize the whole scabrous scam.
Serial entrepreneur Steve Kirsch has even offered $2 million to anyone who can demonstrate that all the randomized trials and global as well as research evidence is wrong, and that the NIH and WHO concern about Fluvoxamine and Ivermectin is justified. A straight $2 million windfall or grant. No one has taken him up on it. His credibility as a medical entrepreneur and philanthropist is unimpeachable.
A few points. You don’t have to remotely be an “anti-vaxxer” (those who oppose them on principle) to be concerned by any or all of the following:
Safety protocols are incomplete
The mRNA treatments are not “vaccines” they are symptom suppressors. Since the vulnerable were not part of the clinical trials, and those trials had such a small subset of the population anyway (‘nominal’ is a generous term), we really don’t know how well they do for the elderly, the vulnerable, etc. And how in that period could we know anything about “safety” and “efficacy?” Booster shots are already being discussed.
All of them have blood clotting issues, 4,000 deaths plus in the US, 10,000 in Europe, both very likely an undercount, as only a small percentage make it into the adverse effects database, and we have swelling evidence, of doctors extremely reluctant to link “anything” to a vaccine, even if a healthy person, within days, dies. Of course you can say, “healthy people also die.” But since in tabulating COVID lethality the norms were at the other extremity, where a “whiff” of COVID put it on the death certificate, we can clearly see again, wanton inconsistency, and again narrative protection at all costs. These deaths are more than the cumulative recorded death from all other vaccines combined, for an illness you have to be tested for to even know you have!
Re-infection has been rife, and mass surges in cases and deaths after mass vaccination in populations (Israel, UK, Gibraltar, Seychelles, Maldives), and now with the Chinese vaccines, Bahrain, Chile and UAE, either no improvement or serious spikes in cases and deaths.
How can anyone call this normal? And so people are opting out, and mania has set in. To induce you to get vaccinated, free ice cream, drinks, the NYC Mayor offering free burgers, lotteries linked to vaccination, dating apps linked to incentivize sexual license.
Yet, as noted, we hear people are getting re-infected? Doesn’t matter, speed past that, just get a jab in every arm. And children? They have no risk, they don’t transmit the disease, shown over and over, Sweden had no deaths in schools with schools open throughout. But suddenly, a 12-year-old can consent in North Carolina to being “jabbed”? Can they also vote, drive, have sex, smoke and drink while they’re at it?
Can anyone call this remotely normal? Experimental gene therapy asserting “safety” you cannot possibly even know (Salk Institute Study indicates that the spike proteins being injected themselves, without even a virus involved, can cause the virus). Future impact is unknown, people are understandably spooked. How is this anywhere close to “informed consent” by the Nuremberg standards?
And what has happened to the EU? But for a few standouts like Denmark and Sweden, they are ready to require “vaccine passports” thereby ignoring those who have recovered and don’t need experimental substances in their body, or those below 60 and healthy with no statistical risk, or children with a truly non-existent risk profile (symptoms easily treatable for them), and with abundant, far safer, preventive treatments? With plummeting numbers, no “pandemic” in Europe, no excess mortality for 2020, what in God’s name is the panic to just jab everything and everyone in sight, including innocent children we are conducting “human trials” on?
This is horror movie material, but chillingly real.
By the way, despite a nominal surge (large in a relative sense as their numbers are so tame), Japan still has among the lowest numbers of deaths per million in the world. 1% of the population is vaccinated.
None of it makes sense, none of it is plausible, any more than the face diapers, penal lock ups, fake non-diagnostic tests, death certificate manipulation, avoiding treatment that reduces hospitalization risk by over 85%, censoring new insights from the most credible experts. All this while blowing up the economy, magnifying poverty, killing children through hunger and awaiting the reckoning when all the currency printing eventually comes home to roost.
So, we have to stop “asking” for relief and move to “demanding” it. And we have to stop acquiescing and trying to “persuade.” No one is this villainously stupid. Villainous maybe. So you can’t “persuade” someone out of a pathology or a psychosis. We can be respectfully, lawfully, civilly disobedient, and make our voices heard, in concert, and purposefully.
This isn’t Life
C.J. Hopkins, writing from “New Normal” Germany describes this version of “living”:
“Perfectly healthy, medical-masked people are lining up in the streets to be experimentally ‘vaccinated’.”
Lockdown-bankrupted shops and restaurants have been converted into walk-in “PCR test stations.” The government is debating mandatory “vaccination” of children in kindergarten. Goon squads are arresting octogenarians for picnicking on the sidewalk without permission.” Sound appealing?
Should I await docilely to be told when to go out, where to go out, what experimental substance to have shot into my body and that of my family? Should I welcome no stimulus, no abandon, no real laughter or mirth, no experiencing of human aptitudes, or going freely to other lands and immersing in other cultures or relishing the world as a part of my birthright? Is it really all right for us to have these political scavengers pick on the remains of our autonomy?
Poet laureate Seamus Heaney writes so unforgettably:
“History says, don’t hope
On this side of the grave.
But then, once in a lifetime
The longed-for tidal wave
Of justice can rise up,
And hope and history rhyme.”
Time to see if we can’t catch one of those waves.
The prose, the poetry, the rhymes, the chimes, of our lives are at stake. And there we must all decide to take a stand, however, whenever and wherever we can, for the future we seek.
“I Don’t Know of a Bigger Story in the World” Right Now Than Ivermectin: NY Times Best-Selling Author
So why are journalists not covering it?
By Nick Corbishley | Naked Capitalism | May 25, 2021
Michael Capuzzo, a New York Times best-selling author, has just published an article titled “The Drug That Cracked Covid”. The 15-page article chronicles the gargantuan struggle being waged by frontline doctors on all continents to get ivermectin approved as a Covid-19 treatment, as well as the tireless efforts by reporters, media outlets and social media companies to thwart them.
Because of ivermectin, Capuzzo says, there are “hundreds of thousands, actually millions, of people around the world, from Uttar Pradesh in India to Peru to Brazil, who are living and not dying.” Yet media outlets have done all they can to “debunk” the notion that ivermectin may serve as an effective, easily accessible and affordable treatment for Covid-19. They have parroted the arguments laid out by health regulators around the world that there just isn’t enough evidence to justify its use.
For his part, Capuzzo, as a reporter, “saw with [his] own eyes the other side [of the story]” that has gone unreported, of the many patients in the US whose lives have been saved by ivermectin and of five of the doctors that have led the battle to save lives around the world, Paul Marik, Umberto Meduri, José Iglesias, Pierre Kory and Joe Varon. These are all highly decorated doctors. Through their leadership of the Front Line COVID-19 Critical Care (FLCCC) Alliance, they have already enhanced our treatment of Covid-19 by discovering and promoting the use of Corticoid steroids against the virus. But their calls for ivermectin to also be used have met with a wall of resistance from healthcare regulators and a wall of silence from media outlets.
“I really wish the world could see both sides,” Capuzzo laments. But unfortunately most reporters are not interested in telling the other side of the story. Even if they were, their publishers would probably refuse to publish it.
That may explain why Capuzzo, a six-time Pulitzer-nominated journalist best known for his New York Times-bestselling nonfiction books Close to Shore and Murder Room, ended up publishing his article on ivermectin in Mountain Home, a monthly local magazine for the of the Pennsylvania mountains and New York Finger Lakes region, of which Capuzzo’s wife is the editor. It’s also the reason why I decided to dedicate today’s post to Capuzzo’s article. Put simply, as many people as possible –particularly journalists — need to read his story.
As Capuzzo himself says, “I don’t know of a bigger story in the world.”
Total News Blackout
On December 8 2020, FLCCC member Dr Pierre Kory gave nine minutes of impassioned testimony to the US Homeland Security Committee Meeting on the potent anti-viral, anti-inflammatory benefits of ivermectin. A total of 9 million people (myself included) saw the video on YouTube before it was taken down by YouTube’s owner, Google. As Capuzzo exhaustively lays out, both traditional and social media have gone to extraordinary lengths to keep people in the dark about ivermectin. So effective has this been that even in some of the countries that have benefited most from its use (such as Mexico and Argentina) many people are completely unaware of its existence. And this is no surprise given how little information is actually seeping out into the public arena.
A news blackout by the world’s leading media came down on Ivermectin like an iron curtain. Reporters who trumpeted the COVID-19 terror in India and Brazil didn’t report that Ivermectin was crushing the P-1 variant in the Brazilian rain forest and killing COVID-19 and all variants in India. That Ivermectin was saving tens of thousands of lives in South America wasn’t news, but mocking the continent’s peasants for taking horse paste was. Journalists denied the world knowledge of the most effective life-saving therapies in the pandemic, Kory said, especially among the elderly, people of color, and the poor, while wringing their hands at the tragedy of their disparate rates of death.
Three days after Kory’s testimony, an Associated Press “fact-check reporter” interviewed Kory “for twenty minutes in which I recounted all of the existing trials evidence (over fifteen randomized and multiple observational trials) all showing dramatic benefits of Ivermectin,” he said. Then she wrote: “AP’S ASSESSMENT: False. There’s no evidence Ivermectin has been proven a safe or effective treatment against COVID-19.” Like many critics, she didn’t explore the Ivermectin data or evidence in any detail, but merely dismissed its “insufficient evidence,” quoting instead the lack of a recommendation by the NIH or WHO. To describe the real evidence in any detail would put the AP and public health agencies in the difficult position of explaining how the lives of thousands of poor people in developing countries don’t count in these matters.
Not just in media but in social media, Ivermectin has inspired a strange new form of Western and pharmaceutical imperialism. On January 12, 2021, the Brazilian Ministry of Health tweeted to its 1.2 million followers not to wait with COVID-19 until it’s too late but “go to a Health Unit and request early treatment,” only to have Twitter take down the official public health pronouncement of the sovereign fifth largest nation in the world for “spreading misleading and potentially harmful information.” (Early treatment is code for Ivermectin.) On January 31, the Slovak Ministry of Health announced its decision on Facebook to allow use of Ivermectin, causing Facebook to take down that post and removed the entire page it was on, the Ivermectin for MDs Team, with 10,200 members from more than 100 countries.
In Argentina, Professor and doctor Hector Carvallo, whose prophylactic studies are renowned by other researchers, says all his scientific documentation for Ivermectin is quickly scrubbed from the Internet. “I am afraid,” he wrote to Marik and his colleagues, “we have affected the most sensitive organ on humans: the wallet…” As Kory’s testimony was climbing toward nine million views, YouTube, owned by Google, erased his official Senate testimony, saying it endangered the community. Kory’s biggest voice was silenced.
“The Most Powerful Entity on Earth”
Malcom X once called the media “the most powerful entity on the earth.” They have, he said, “the power to make the innocent guilty and to make the guilty innocent, and that’s power. Because they control the minds of masses”. Today, that power is now infused with the power of the world’s biggest tech and social media companies. Together social and traditional media have the power to make a medicine that has saved possibly millions of lives during the current pandemic disappear from the conversation. When it is covered, it’s almost always in a negative light. Some media organizations, including the NY Times, have even prefaced mention of the word “ivermectin” — a medicine that has done so much good over its 40-year lifespan that its creators were awarded the Nobel Prize for Medicine in 2015 — with the word “controversial.”
Undeterred, many front-line doctors have tried to persuade their respective health regulators of the unparalleled efficacy and safety of ivermectin as a covid treatment. They include Dr. Tess Lawrie, a prominent independent medical researcher who, as Capuzzo reports, evaluates the safety and efficacy of drugs for the WHO and the National Health Service to set international clinical practice guidelines:
“[She] read all twenty-seven of the Ivermectin studies Kory cited. The resulting evidence is consistent and unequivocal,” she announced, and sent a rapid meta-analysis, an epidemiolocal statistical multi-study review considered the highest form of medical evidence, to the director of the NHS, members of parliament, and a video to Prime Minister Boris Johnson with “the good news… that we now have solid evidence of an effective treatment for COVID-19…” and Ivermectin should immediately “be adopted globally and systematically for the prevention and treatment of COVID-19.”
Ignored by British leaders and media, Lawrie convened the day-long streaming BIRD conference—British Ivermectin Recommendation Development—with more than sixty researchers and doctors from the U.S., Canada, Mexico, England, Ireland, Belgium, Argentina, South Africa, Botswana, Nigeria, Australia, and Japan. They evaluated the drug using the full “evidence-to-decision framework” that is “the gold standard tool for developing clinical practice guidelines” used by the WHO, and reached the conclusion that Ivermectin should blanket the world.
“Most of all you can trust me because I am also a medical doctor, first and foremost,” Lawrie told the prime minster, “with a moral duty to help people, to do no harm, and to save lives. Please may we start saving lives now.” She heard nothing back.
Ivermectin’s benefits were also corroborated by Dr. Andrew Hill, a renowned University of Liverpool pharmacologist and independent medical researcher, and the senior World Health Organization/UNITAID investigator of potential treatments for COVID-19. Hill’s team of twenty-three researchers in twenty-three countries had reported that, after nine months of looking for a COVID-19 treatment and finding nothing but failures like Remdesivir— “we kissed a lot of frogs”— Ivermectin was the only thing that worked against COVID-19, and its safety and efficacy were astonishing—“blindingly positive,” Hill said, and “transformative.” Ivermectin, the WHO researcher concluded, reduced COVID-19 mortality by 81 percent.
Why All the Foot Dragging?
Yet most health regulators and governments continue to drag their feet. More evidence is needed, they say. All the while, doctors in most countries around the world have no early outpatient medicines to draw upon in their struggle against the worst pandemic in century. Drawing on his own experience, Capuzzo describes the absence of treatments for COVID-19 as a global crisis:
When my daughter Grace, a vice president at a New York advertising agency, came
down with COVID-19 recently, she was quarantined in a “COVID hotel” in Times Square with homeless people and quarantining travelers. The locks on her room door were removed. Nurses prowled the halls to keep her in her room and wake her up every night to check her
vitals—not to treat her, because there is no approved treatment for COVID-19; only, if her oxygen plummeted, to move her to the hospital, where there is only a single eective approved treatment for COVID-19, steroids that may keep the lungs from failing.
There are three possible explanations for health regulators’ refusal to allow the use of a highly promising, well-tolerated off-label medicine such as ivermectin:
- As a generic, ivermectin is cheap and widely available, which means there would be a lot less money to be made by Big Pharma if it became the go-to early-stage treatment against covid.
- Other pharmaceutical companies are developing their own novel treatments for Covid-19 which would have to compete directly with ivermectin. They include ivermectin’s original manufacturer, Merck, which has an antiviral compound, molnupiravir, in Phase 3 clinical trials for COVID-19. That might explain the company’s recent statement claiming that there is “no scientific basis whatsoever for a potential therapeutic effect of ivermectin against COVID-19.
- If approved as a covid-19 treatment, ivermectin could even threaten the emergency use authorisation granted to covid-19 vaccines. One of the basic conditions for the emergency use authorisation granted to the vaccines currently being used against covid is that there are no alternative treatments available for the disease. As such, if ivermectin or some other promising medicine such as fluvoxamine were approved as an effective early treatment for Covid-19, the vaccines could be stripped of authorisation.
This may explain why affordable, readily available and minimally toxic drugs are not repurposed for use against Covid despite the growing mountains of evidence supporting their efficacy.
Ivermectin has already been approved as a covid-19 treatment in more than 20 countries. They include Mexico where the mayor of Mexico City, Claudia Scheinbaum, recently said that the medicine had reduced hospitalisations by as much as 76%. As of last week, 135,000 of the city’s residents had been treated with the medicine. The government of India — the world’s second most populous country and one of the world’s biggest manufacturers of medicines — has also recommended the use of ivermectin as an early outpatient treatment against covid-19, in direct contravention of WHO’s own advice.
Dr Vikas P. Sukhatme, the dean of Emory School of Medicine, recently wrote in a column for the Times of India that deploying drugs such as ivermectin and fluvoxamine in India is likely to “rapidly reduce the number of COVID-19 patients, reduce the number requiring hospitalization, supplemental oxygen and intensive care and improve outcomes in hospitalized patients.”
Four weeks after the government included ivermectin and budesonide among its early treatment guidelines, the country has recorded its lowest case count in 40 days.
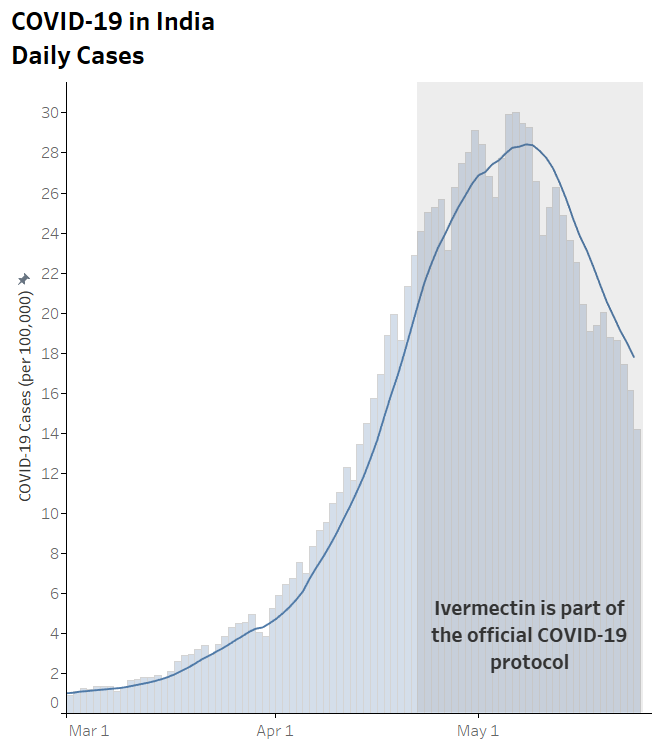
In many of India’s regions the case numbers are plunging in almost vertical fashion. In the capital Delhi, as in Mexico City, hospitalisations have plummeted. In the space of 10 days ICU occupancy fell from 99% to 70%. Deaths are also falling. The test positivity ratio slumped from 35% to 5% in just one month.
One of the outliers of this trend is the state of Tamil Nadu, where cases are still rising steeply. This may have something to do with the fact that the state’s newly elected governor, MK Stalin, decided to exclude ivermectin from the region’s treatment protocol in favor of Remdesivir. The result? Soaring cases. Late last week, Stalin reversed course once again and readopted ivermectin.
For the moment deaths in India remain extremely high. And there are concerns that the numbers are being under-reported. Yet they may also begin to fall in the coming days. In all of the countries that have used ivermectin widely, fatalities are the last thing to fall, after case numbers and hospitalizations. Of course, there’s no way of definitively proving that these rapid falloffs are due to the use of ivermectin. Correlation, even as consistent as this, is not causation. Other factors such as strict lockdowns and travel restrictions no doubt also play a part.
But a clear pattern across nations and territories has formed that strongly supports ivermectin’s purported efficacy. And that efficacy has been amply demonstrated in three meta-analyses.
India’s decision to adopt ivermectin, including as a prophylaxis in some states, is already a potential game-changer. As I wrote three weeks ago, if case numbers, hospitalizations and fatalities fall in India as precipitously as they have in other countries that have adopted ivermectin, it could even become a watershed moment. But for that to happen, the news must reach enough eyes and ears. And for that to happen, reporters must, as Capuzzo says, begin to do their job and report both sides of this vital story.
Featured Video

Trita Parsi: Iran War Ends Today? Threats of Deporting Trita Parsi
or go to
Aletho News Archives – Video-Images
From the Archives
The Crusades – colliding narratives
Ashes of Pompeii | June 13, 2026
They say history is written by the victors, but the Crusades offer an interesting historical contrast: a two-century collision that produced not one history, but two parallel, irreconcilable realities. The dates and the battles are identical in both accounts, but the moral axis is entirely flipped.
In the traditional Western narrative, the Crusades are framed as a heroic, if tragic, epic. The First Crusade is a pious pilgrimage; the knights are romanticized figures of chivalry in shining armor, bravely holding the line in a hostile, exotic land. The eventual loss of the Holy Land is mourned as the “fall of Outremer,” a tragic retreat of European civilization. In this telling, the East is often reduced to a passive backdrop, its inhabitants viewed through a lens of mystique or backwardness, mere obstacles to a divine mandate.

But cross the Mediterranean, and the exact same timeline reads like a chronicle of foreign invasion and eventual, hard-won restoration against the barbarous northerners. The dates do not change, but the adjectives do. Here is the history as it is remembered in the Levant… continue
Blog Roll
 Aletho News
Aletho News- The 12 Screenings That Manufacture the Patients They Claim to Find
- Iran deputy FM says MoU with US finalized, to be signed in Geneva on Friday
- With one strike, Netanyahu tries to kill two peace deals
- Iran warns ‘no point’ in deal with US if Israel remains unrestrained
- Ukraine as a laboratory of ‘techno-fascism’
- Desperate Starmer choosing piracy as distraction over UK crime crisis – Putin envoy
- The Crusades – colliding narratives
- Trita Parsi: Iran War Ends Today? Threats of Deporting Trita Parsi
- What Is SIDS?
- DHS docs: Govt bracing for nationwide anti-AI riots, preparing to crack down on dissent
- If Americans Knew
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- Oxfam: More Palestinians killed by Israel across West Bank in last 3 years than previous 17 years combined
- US-Iran ceasefire may be imminent, but will Israel blow it up? – Daily Update
- The Issue of Israel Is Ending Democracy In Michigan
- Israel is stealing homes, livelihoods, and lives in West Bank
- Gaza is not an aberration – Israel planned this genocide decades ago
- Israel is changing the face of Lebanon, mainstream media is normalizing it – 3 articles
- Genocide lobby benefits from EU anti-racist fund
- No Tricks Zone
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
