Russian drilling rig shelled again
Samizdat | June 26, 2022
A Russian offshore drilling rig in the Black Sea has been shelled, in the second similar attack in less than a week, a spokesperson for Crimea’s emergency services told TASS on Sunday, blaming the strike on the Ukrainian military.
Earlier, the Baza Telegram channel, citing its own sources, reported that a projectile which had hit the Chernomorneftegaz-owned Tavrida floating drilling rig overnight, left a hole in the platform’s helipad.
“This is shelling by the Armed Forces of Ukraine, there are no casualties,” the region’s emergency services spokesman said without providing further details.
On June 20, the head of Crimea, Sergey Aksyonov, revealed that Ukraine had shelled Chernomorneftegaz drilling platforms 71km from Odessa.
Three platforms were damaged, including the Tavrida. One of the platforms (BK-1) was completely destroyed. Seven people are missing, and three sustained injuries. In total, there were 109 people on the platform, with the majority of them subsequently evacuated.
The Russian Investigative Committee opened a criminal case in relation to the June 20 shelling.
Earlier this month, the Ukrainian presidential representative for Crimea, Tamila Tasheva, said Kiev is now relying on military means to ‘return’ Crimea to Ukraine, and that Russia’s military campaign prompted Kiev to largely abandon diplomacy regarding the peninsula’s ‘de-occupation’.
Ukrainian troops have been losing territory to Russia and allied forces in Donbass, even as Western nations supply more sophisticated weapons to Kiev. Several Ukrainian officials have stated that the pledge to not use foreign weapons to attack targets in Russia does not apply to Crimea, which Kiev considers part of its territory.
Russia attacked the neighboring state in late February, following Ukraine’s failure to implement the terms of the Minsk agreements, first signed in 2014, and Moscow’s eventual recognition of the Donbass republics of Donetsk and Lugansk. The German- and French-brokered protocols were designed to give the breakaway regions special status within the Ukrainian state.
The Kremlin has since demanded that Ukraine officially declare itself a neutral country that will never join the US-led NATO military bloc. Kiev insists the Russian offensive was completely unprovoked and has denied claims it was planning to retake the two republics by force.
Israel Murders Iranians While Biden Kills the Iran Deal
By Connor Freeman | The Libertarian Institute | June 23, 2022
In a clear message to Tehran, an American B-52 flew over the Persian Gulf as soon as Joe Biden entered the White House. Biden promised to return the U.S. to the Iran nuclear deal. But indirect talks to revive the Joint Comprehensive Plan of Action (JCPOA), which began last April, have stalled for three months without a resolution in sight. Counting on the reliable support of Biden and bipartisan Iran hawks in Congress, the nuclear-armed Israeli apartheid regime intends to kill the deal entirely.
Tehran, a decades-long signatory of the Non-Proliferation Treaty, is neither seeking nor has ever sought nuclear weapons. But the Islamic Republic, once Tel Aviv’s “best friend,” serves as Israel’s favorite boogeyman, superficially justifying billions of dollars in American military aid each year. The JCPOA threatens the racket.
Formally known for years as “Israel’s man in Washington,” President Biden is essentially pursuing ultra-Zionist Donald Trump’s foreign policy regarding Iran and supporting, tacitly or otherwise, Tel Aviv’s relentless attacks against Iran and its allies. Biden is continuously imposing yet more sanctions, increasing the “Maximum Pressure” on the economically crippled Iranian people.
The rial has hit all-time lows. With a population of 82 million, almost half of all Iranians live below the poverty line, and inflation is somewhere between 40-50%.
America’s self-styled sanctions artists delight in seeing the results of their economic war on Iran: excess deaths, severe medical shortages, prohibitively high prices for staple goods, plummeting incomes, and social unrest over food costs.
This year, Tel Aviv has been bombing Syria, Tehran’s ally, at the usual weekly rate. A recent strike, coming from the illegally occupied Golan Heights, attacked Damascus International Airport. The airstrike targeted the facility’s only working runway Israel had not yet destroyed, rendering the airport temporarily inoperable.
Shortly afterwards, The Wall Street Journal put out a story confirming that Tel Aviv coordinates with the Pentagon on many of its strikes in Syria.
The Israelis just wrapped up month-long war drills, the largest held in decades, aimed squarely at Tehran. Exercises over the Mediterranean Sea, with over 100 aircraft and navy submarines, spanned 10,000 kilometers and were designed to simulate repeated airstrikes on Iran and their civilian nuclear facilities.
Early reports were that the U.S. Air Force would participate, providing refueling planes, but this reportedly did not come to pass. Although General Michael Kurilla, the new head of U.S. Central Command (CENTCOM), observed some of these Chariots of Fire exercises.
On May 22, 2022, the Israelis carried out a high profile assassination of a senior colonel in the Iranian Revolutionary Guard Corps (IRGC), Col. Hassan Sayyad Khodaei. Shortly afterwards, citing an unnamed intelligence official, The New York Times reported Tel Aviv had informed Washington that it was responsible. Israel’s attacks seem to be primarily focused on the Iranians’ drone program, namely killing people who work on drone technology and attacking related sites.
As Dave DeCamp, Antiwar.com news editor, reported,
Israel was immediately suspected of the assassination since it has a history of carrying out targeted killings and other attacks inside Iran. Israel rarely officially acknowledges such operations, and it’s typical that its responsibility is revealed by leaks to the media, often by Israeli officials.
Israeli officials claimed to the Times that Khodaei was in charge of a secret covert IRGC group known as Unit 840, which Iran denies exists. The Israelis claim Khodaei was involved in plots to kill and kidnap Israeli civilians and officials around the world, but there’s no evidence Tehran was planning to target Israelis abroad.
Two people affiliated with the IRGC told the Times that Khodaei was a logistics officer who played a key role in transporting drone and missile technology to Syria and Hezbollah in Lebanon and advised militias in Syria. Iran has said Khodaei was involved in the fight against ISIS in Iraq and Syria.
Israel is suspected to have subsequently poisoned and murdered two Iranian scientists including Ayoub Entezari, an aerospace engineer, who reportedly worked on missile and drone projects, and Kamran Aghamolaei, a geologist.
Last month, a few dozen miles south of Tehran, quadcopter suicide drones attacked the Parchin military complex. The drones hit a building being used for drone development and killed a young engineer. In February, Israel used six quadcopter drones in a strike targeting another Iranian drone facility in Kermanshah which did significant damage. In Tabriz, there were reports of another Israeli attack on a drone factory, as many as three people may have been killed. This month, two additional IRGC members also working in the aerospace industry died during mysterious accidents in Iran. Both deaths were declared “martyrdoms.”
In the midst of these soaring tensions, Robert Malley, Biden’s Iran envoy, is telling Congress “all options are on the table.”
The U.S. Senate overwhelmingly voted to pass a non-binding resolution which insists they would never support a restoration of the JCPOA if the IRGC were removed from the Foreign Terrorist Organization (FTO) blacklist. The FTO designation is ostensibly one of the final sticking points preventing the deal’s straightforward revival. Congress has been sending messages, loud and clear, to Tehran and Biden that the deal has virtually no support.
Meanwhile, Secretary of State Antony Blinken is peddling baseless stories about Tehran attempting to assassinate his predecessor Mike Pompeo. Pompeo enthusiastically supported Trump’s Maximum Pressure campaign as well as the drone strike murder of top Iranian General Qasem Soleimani, leader of the IRGC Quds Force. Though these claims of Pompeo’s life being endangered remain unproven, U.S. taxpayers pay millions per month for a security detail to put his and Blinken’s mind at ease.
Much like Tel Aviv’s unproven accusations that the IRGC is out to kidnap and murder Israelis, especially in Istanbul for some reason, this obviously plays well with the overall anti-JCPOA campaign.
The IRGC is the only state military organization on the terrorism blacklist. Considering the myriad preexisting sanctions on the unit, it is a superfluous insult. In 2019, Trump implemented this policy at the behest of Israeli-partisan hawks like Mark Dubowitz at the Foundation For Defense of Democracies, a notoriously anti-Iran think tank. This is one of the largest bricks in the so called “sanctions wall” precluding any of Trump’s successors from ever returning to the deal for fear of the built-in political toxicity. It is enough to keep Biden and the cowardly Democrats from backing what is ultimately Barack Obama’s deal in favor of a neoconservative-style Iran policy.
As May began, Israel started making these claims about a global Iranian plot to kill Israelis. At that time, the JCPOA negotiations were seemingly stalled irrevocably because of the IRGC-FTO issue. But then the Vienna talks’ broker, European Union nuclear negotiator Enrique Mora, traveled to Tehran. He took meetings with Iran’s lead negotiator Ali Bagheri Kani as a last ditch effort to break the deadlock. Mora was sent by EU foreign policy chief Josep Borrell. As a result of the American led sanctions blitz on Russia, Europeans are in desperate need of another crude supplier as Borrell has noted. The same week, the emir of Qatar, Sheikh Tamim bin Hamad Al Thani, also made a trip to Tehran and pushed for progress during meetings with President Ebrahim Raisi as well as Ayatollah Ali Khamenei. On May 13th, Borrell announced Mora’s mission went “better than expected,” Vienna talks had been unblocked, and a final deal was within reach.
Days later, coinciding with Israeli Defense Minister Benny Gantz’s visit to Washington, and his meetings with National Security Adviser Jake Sullivan and Pentagon chief Lloyd Austin, Khodaei was murdered in the drive-by shooting. Israel’s assassination campaign had commenced.
Two days after the Khodaei killing, Politico reported that the final decision to keep the IRGC on the FTO list was made. On Twitter, Israeli Prime Minister Naftali Bennett thanked Biden for the “principled decision and for being a true friend of the State of Israel.”
Following Trump, Biden’s administration is also continuing to seize tankers, stealing Iranian oil and pirating it for profit. Ironically, after Russian President Vladimir Putin invaded Ukraine, there was some talk from Biden officials about making a deal with the Islamic Republic to put Iran’s abundant oil back on the market to reduce global energy prices. But this was apparently never taken seriously.
Biden instead prefers to kowtow to the genocidal Saudi regime which along with Abu Dhabi and Washington have starved to death and bombed over 400,000 Yemenis, including more than 263,000 children.
Those deaths mean little to the Abraham Accords caucus. This bipartisan coalition in Congress is working to ensure Washington arms these tyrants further while the Pentagon assists them in joining forces, as well as integrating missile defenses with Tel Aviv eyeing Tehran. As Biden heads to the Middle East, there is even talk of the U.S. offering security guarantees to the United Arab Emirates.
For almost a year, the Israelis have been pushing an anti-Iran, NATO-style, U.S. led alliance in the Middle East. In recent weeks, Gantz has openly promoted this strategy which Bennett is said to have suggested to Biden during a White House meeting last year.
As Iran is encircled militarily and strangled economically, the American Empire is refusing to allow them any breathing room. Each day the U.S. forgoes lifting sanctions and restoring the deal the likelihood of a hot war increases.
Given the size of Iran, its population, its geostrategic location, substantial ballistic missile deterrent, its Axis of Resistance partners, and the wide variety of U.S. military targets in the region, a war with Tehran would likely dwarf the catastrophic damage, scope, and deaths of America’s other Middle East wars.
If the JCPOA fails, the hawks armed to the teeth surrounding Iran may try to goad Tehran into leaving the NPT. Whether this happens ultimately or not, Israel may use the coming breakdown in diplomacy to justify instigating its long desired war. Rightfully, the Iranians will see such an Israeli attack as an American declaration of war.
This week, Tehran has formally dropped their demand for removing the IRGC from the FTO list. Washington has not yet responded. Contrary to the corporate press narrative, the ball is now firmly in Washington’s court.
Iran called Biden’s bluff. It is imperative that the American people now assert our support for terminating the unjustified and brutal Maximum Pressure campaign as well as denounce Israel’s murderous aggressions.
The Iranian people deserve to live and trade in peace.
Israeli forces beat up international activists in Masafer Yatta

Israeli soldiers beat up a handcuffed international activist in Masafer Yatta
WAFA – June 22, 2022
HEBRON – Israeli forces today beat up a number of international solidarity activists in Masafer Yatta in the southern Hebron hills, according to local sources.
Coordinator of the Protection and Steadfastness Committee in Masafer Yatta, Fuad al-Amour, said the heavily-armed soldiers brutally assaulted a number of international activists while protesting the military drills close to and in al-Markez, and held two others for a long period.
The Israeli army have been conducting drills in al-Markez, one of 12 hamlets making up the Masafer Yatta, which rely heavily on animal husbandry as the main source of livelihood, for the second day in a row.
Al-Amour added that the army has built mock-ups as targets between the makeshift dwellings of the hamlet residents and has been conducting training with heavy weaponry, spreading panic among the residents.
The army has also deployed military checkpoints in the vicinity of the hamlets in the area, in preparation for military training, and perhaps paving the way for an imminent removal of the Palestinian residents.
Recently, Israel’s top court gave the army the green light to forcibly expel some 1,300 Palestinians living in twelve villages or hamlets making up the Masafer Yatta area marking one of the largest expulsions carried out by the State of Israel in recent decades.
Located in Area C of the West Bank, under full Israeli administrative and military control, the area has been subjected to repeated Israeli violations by settlers and soldiers targeting their main source of living – livestock.
It has been designated as a closed Israeli military zone for training since 1980s and accordingly referred to as Firing Zone 918.
Israeli violations against the area include demolition of animal barns, homes and residential structures. Issuance of construction permits by Israel to local Palestinians in the area is non-existent.
CDC Admits It Never Monitored VAERS for COVID Vaccine Safety Signals
By Josh Guetzkow, Ph.D. | The Defender | June 21, 2022
In a stunning development, the Centers for Disease Control and Prevention (CDC) last week admitted — despite assurances to the contrary — the agency never analyzed the Vaccine Adverse Event Reporting System (VAERS) for safety signals for COVID-19 vaccines.
The admission was revealed in response to a Freedom of Information Act (FOIA) request submitted by Children’s Health Defense (CHD).
In September 2021, I published an article in The Defender in which I used the CDC’s published methodology to analyze VAERS for safety signals from COVID-19 vaccines.
The signals were loud and clear, leading me to wonder “why is nobody listening?”
Instead, I should have asked, “Is anybody even looking for them?”
After that article was published, I urged CHD’s legal team to submit a FOIA request to the CDC about its VAERS monitoring activities.
Since CDC officials stated publicly that “COVID-19 vaccine safety monitoring is the most robust in U.S. history,” I had assumed that at the very least, CDC officials were monitoring VAERS using the methods they described in a briefing document posted on the CDC website in January 2021 (and updated in February 2022, with minor changes).
I was wrong.
The lynchpin of their safety monitoring was to mine VAERS data for safety signals by calculating what are known as proportional reporting ratios (PRR’s).
This is a method of comparing the proportion of different types of adverse events reported for a new vaccine to the proportion of those events reported for an older, established vaccine.
If the new vaccine shows a significantly higher reporting rate of a particular adverse event relative to the old one, it counts as a safety signal that should then trigger a more thorough investigation.
The briefing document states, “CDC will perform PRR data mining on a weekly basis or as needed.”

And yet, in the agency’s response to the FOIA request, it wrote that “no PRRs were conducted by CDC. Furthermore, data mining is outside of the agency’s purview.”
The agency suggested contacting the U.S. Food and Drug Administration (FDA), which was supposed to perform a different type of data mining, according to the briefing document.
![]()
CDC officials repeatedly claimed they have not seen safety signals in VAERS.

For example, on April 27, 2021, CDC Director Dr. Rochelle Walensky stated the CDC did not see any signals related to heart inflammation.
But a PRR calculation I did using the number of myo/pericarditis reports listed in the first table produced by the CDC obtained via the FOIA request reveals clear and unambiguous safety signals relative to the comparator vaccines mentioned in the briefing document (i.e., flu vaccines, FLUAD and Shingrix).
The table is dated April 2, 2021, almost four weeks before she made those remarks.
In fact, among the 15 adverse events for adults included in that week’s tabulations, PRRs I calculated also show loud-and-clear safety signals for acute myocardial infarction, anaphylaxis, appendicitis, Bell’s palsy, coagulopathy, multisystem inflammatory syndrome in adults (MIS-A), stroke and death.
The actual monitoring the CDC did diverges from the one promised in the briefing document in other ways.
For example, the CDC never created tables of the top 25 adverse events reported in the previous week, tables comparing different vaccine manufacturers, or tables of auto-immune diseases.
And it only began monitoring in early April 2021, even though reports from COVID-19 vaccines had been flooding VAERS since mid-December of the previous year.
To be clear, VAERS is not the only database the CDC uses to monitor COVID-19 vaccine safety.
For example, the CDC sponsored several studies of COVID-19 safety using the Vaccine Safety Datalink (VSD), which is comprised of millions of medical records from HMO’s across several states.
Those studies do not raise many safety concerns. However, they make many questionable methodological choices.
To give one example, a major safety study based on VSD data published in September 2021, in “JAMA,” compares adverse event rates that occur within 1-21 days of vaccination to the rate of occurrence from 22 to 42 days after vaccination.
It makes no comparison between vaccinated and unvaccinated individuals, or before vaccination versus after in the same individuals.
Moreover, the VSD is far from infallible, having failed initially to detect the increase in myocarditis rates.
In contrast, although calculating PRR’s is a blunt pharmacovigilance tool and far from perfect, it nevertheless has the advantage of being straightforward and difficult to manipulate with statistical sleight of hand.
PRRs are one of the oldest, most basic and most well-established tools of pharmacovigilance. The calculations are so straightforward that the CDC automated it several years ago, so it could have been done at the press of a button.
It simply beggars belief that the CDC failed to do this simple calculation. Even now, a paper published by CDC staff in March on the safety of the mRNA COVID-19 vaccines remains purely descriptive with no PRR calculation.
Meanwhile, a study published by a researcher not affiliated with the CDC in February in “Frontiers in Public Health” analyzes VAERS and EudraVigilance data using a method similar to PRRs, revealing clear and concerning safety signals.
And while it is true that VAERS is not the only database the CDC can use to monitor COVID-19 vaccine safety, it is of critical importance because it can reveal signals much faster than any other method — if anybody cares to look for them.
It remains to be seen if the FDA was properly monitoring VAERS. That will be the subject of a future FOIA request.
But even if it was, it doesn’t change the fact that the CDC completely failed in its promise to monitor VAERS for safety signals.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Washington supports blockade of Russian exclave by NATO member Lithuania
Samizdat | June 22, 2022
The US says that it “appreciates” anti-Russian sanctions imposed by EU nations and that its military is committed to the defense of Lithuania, after the country banned some Russian goods from passing through its territory to the Russian exclave of Kaliningrad.
Ned Price, the spokesman for the US state department, dismissed Moscow’s displeasure with the Lithuanian blockade of its territory as “saber-rattling” and “bluster.” Speaking at a daily briefing, he said he didn’t want to “give it additional time.”
“We, of course, appreciate the unprecedented economic measures that many countries around the world… including in this case Lithuania, have joined us in taking against Russia for its unprovoked war in Ukraine,” he said.
Price said that the US would protect Lithuania from any military attack, as is due under its NATO obligations.
“Lithuania has been a stalwart partner in this. We stand by NATO. We stand by our NATO Allies, and we stand by Lithuania,” he said.
The row between Russia and its Baltic neighbor erupted last week after Lithuania started blocking the transit of goods between mainland Russia and Kaliningrad region. The partial restrictions came into force last Saturday, with Vilnius claiming it was a natural part of enforcing EU sanctions against Russian trade. Roughly half of the traffic is estimated to be affected. The banned items include coal, metals, and construction materials.
Moscow said the restrictions were crossing every line and warned that there would be serious consequences for what it described as a Lithuanian blockade of its exclave. The decision clearly violated international law, the Russian government noted. Some experts suggested that it could even amount to a casus belli – a cause to start a war over.
Kaliningrad region is sandwiched between Poland and Lithuania and has access to the Baltic Sea, which technically allows Russia to ferry goods to it. The relatively small exclave also hosts a significant number of Russian troops and weapon systems, making it a key component in the country’s national security.
Canada threatens to bring back vaccine passports

By Ken Macon | Reclaim The Net | June 21, 2022
Canada may not have seen the last of the mandatory COVID-19 vaccine passports. Proposed restrictions could even be harsher than before, likely to require three to four inoculations in order to travel.
It’s worth noting that the mandate is not set in stone, but the government is preparing for the possibility of introducing the measures in the Fall. Health Minister Jean-Yves Duclos made the announcement during a press conference. The vaccine passport mandate for federal employees and other travelers might be over for now, but Duclos made it clear that it’s likely to return this fall.
In addition to officially denouncing passport mandates, Duclos took the opportunity to explain some changes in wording regarding vaccine requirements. Canada will no longer refer to people who have had all of their vaccinations as “fully vaccinated.” Instead, the language in any official documents will read “up-to-date.” This is because the government says three doses are no longer enough for many people, with some people being told to get four or even five doses.
These changes came after Dr. Theresa Tam, the chief public health officer, told reporters that several studies had just been completed.
Initially, according to the report, two doses of a vaccine would allegedly give a person 50 to 80 percent protection; however, that number falls to just 20 percent against Omicron and newer variations of the coronavirus.
Canada’s goal is now to convince people to get their third and fourth doses and restricting civil liberties has been a controversial way of forcing that over the last couple of years. Over 90 percent of Canadian adults have two doses, but less than 60% have received their booster.
The Conservative Party of Quebec has already started fighting back against the possibility of a third dose being required for a vaccine passport. For them, it’s a personal choice that shouldn’t be mandated. Many in Canada are ready to put the last few years behind them.
The Covid vaccine paper on declining sperm counts is even worse than it seems at first
By Alex Berenson | Unreported Truths | June 20, 2022
On Friday, the journal Andrology published a peer-reviewed paper showing large decreases in sperm counts among men after the second dose of Pfizer’s mRNA Covid jab.
Based on counts from men who donated sperm to three fertility clinics in Israel, this finding is devastating – medically and politically.
It cuts to the heart of the hottest button question of all about the mRNA shots, whether they have hidden fertility risks. That issue has simmered since early 2021, following my reporting that data showed the shots had caused excess miscarriages in rats – and other reports showing that measurable amounts of vaccine reached the ovaries and testes in tests in rats.
Ever since, media “fact-checkers” and public health authorities have dismissed and mocked the concerns and anyone who raises them:
—
Now – after a half-billion men have received mRNA shots – the skeptics appear to be right. Again. The Israeli paper offers hard evidence that the vaccines may present a systemic risk to men’s sperm counts. What was a conspiracy theory is now just a theory. AGAIN.
The paper raises questions about mechanism of action that must be answered immediately. And on top of the myocarditis risk, the finding is more evidence that encouraging – much less forcing – men under 40 to take the mRNA vaccines was a catastrophic mistake.
—
However, the authors qualified their findings by reporting that after five months, sperm levels recovered. Thus the decreases were only temporary, they wrote.
Put aside the fact that a five-month decrease hardly qualifies as temporary for someone trying to start a family – or compared to a “vaccine” that loses effectiveness against Omicron within weeks or months.
As other writers have pointed out, the actual data in the paper do not really support the argument that sperm levels returned to normal after five months. In fact, by some measures, levels continued to decline.
Rather than acknowledging this fact, the authors offered the best possible spin on their data, while at the same time publishing the figures themselves near the end of the paper so that other researchers could see the reality for themselves.
This tactic is now commonplace among researchers putting out data that might raise concerns about the mRNA shots. It is likely a response to the overwhelming political pressure to hide the deepening crisis around the safety and efficacy of shots that governments have given to over a billion people worldwide.
Below is the crucial chart, which shows that “total motile count” – the number of sperm in the ejaculated semen – plunged 22 percent three to five months after the second shot (T2) and barely recovered during the final count (T3), when it was still 19 percent below the pre-shot level.
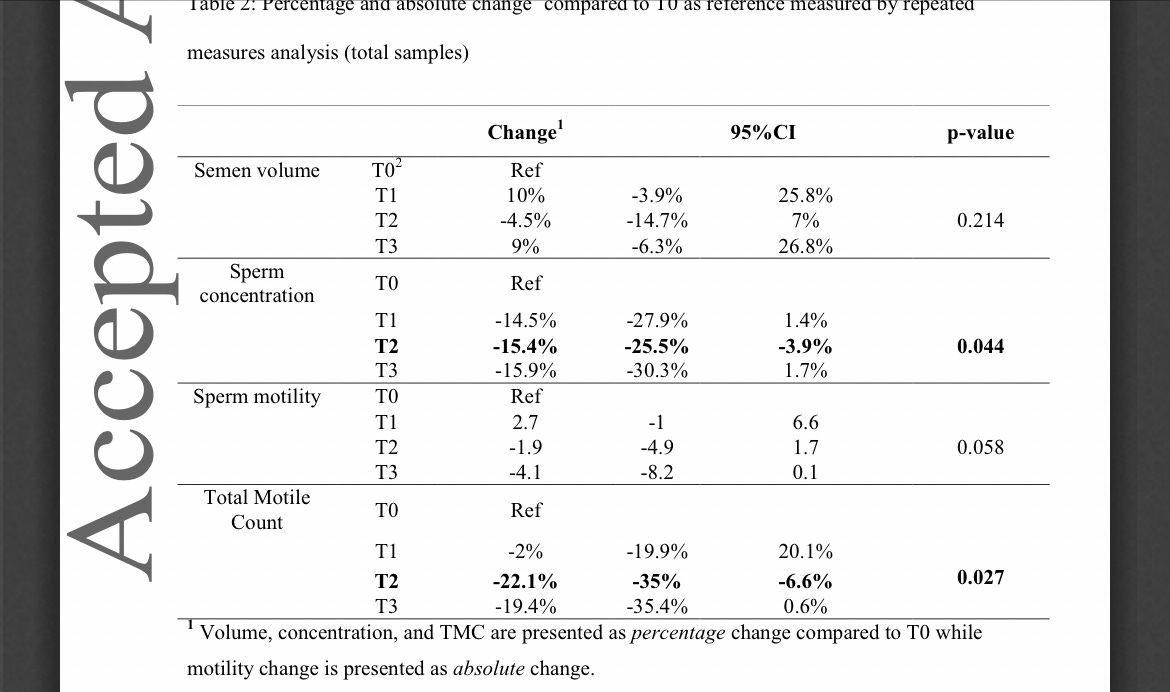
SOURCE
Even more importantly, the fall in sperm counts CANNOT be blamed on short- or even medium-term inflammation as mRNA-generated spike proteins causes our immune cells to ramp up the systemic production of anti-spike antibodies. If that were the case, one would expect to see a short term decrease in sperm count that reverses over time. Instead, total sperm counts are unaffected shortly after the mRNA shots, then decrease months later and hardly recover.
To play down this unpleasant reality, the researchers instead focused on the fact that median rather than average counts did recover after five months. (The median is the numerical midpoint of a series; If a series goes 1, 2, 3, 4, 20, the median will be 3, but the average will be 30 divided by 5, or 6.)
Both the median and the average can be valuable statistics. Using the median rather than the average will hide extreme outliers. In this case, the fact that the average fell much more than the median is a sign that some of the men probably had near-zero sperm counts in both the second and third time periods – and that fact is arguably more important than the median change.
All of which is to say that this data cannot be easily explained away and should not be ignored, as badly as the media would like to do so. The fall in sperm counts is part of an emerging and increasingly dark picture about the long-term health impacts of the mRNA shots – and should all by itself convince parents not to risk exposing their children to these powerful biotechnologies.
Punishing Dissident Physicians
CA Assembly Bill 2098 would muzzle physicians and severely punish those who challenge covid public health measures
By Aaron Kheriaty, MD | Human Flourishing | June 21, 2022
I will be heading to Sacramento next Monday to testify at a Senate committee hearing on California Assembly Bill 2098. The bill, sponsored by Senator Pan—who has been in Pharma’s back pocket for years and the source of much legislative health policy mischief in my home state—would give the medical board the authority to punish any physicians who challenge the safety and efficacy of covid vaccines. This bill is advanced even as evidence continues to emerge of safety problems with the mRNA shots, including a study this week showing the vaccines lower sperm counts in men:

But this proposed measure seeks to enshrine in law “scientific” conclusions which are highly dubious:
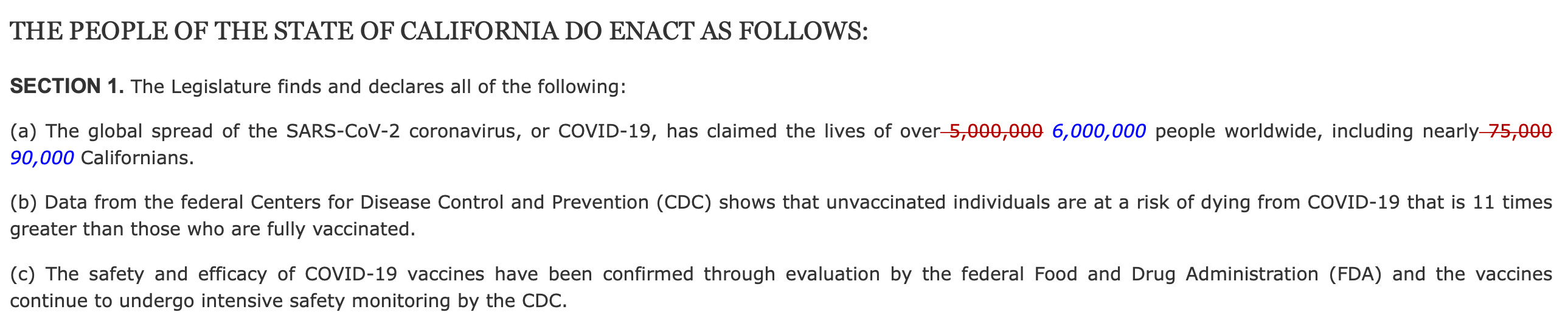
All three of these statements are demonstrably false: (a) The death count figures cited are grossly overestimated by hospitals failing to distinguish dying from covid vs. dying with covid and the financial incentives from the Centers for Medicare and Medicaid Services (CMS) to overestimate covid deaths; (b) the efficacy of vaccines has declined with time and new variants, so the statistic cited here is no longer true of the vaccines against omicron; (c) the CDC has consistently failed to follow-up on serious safety signals, apart from myocarditis, and the post-marketing surveillance data acquired from our FOIA request showed serious safety issues in the first three months of vaccine rollout.
If this bill passes, any physician who raises these or other inconvenient scientific facts or study findings could be disciplined by the medical board, as the text of the bill explains:
It shall constitute unprofessional conduct for a physician and surgeon to disseminate misinformation or disinformation related to COVID-19, including false or misleading information regarding the nature and risks of the virus, its prevention and treatment; and the development, safety, and effectiveness of COVID-19 vaccines.
The supposed scientific “facts” mentioned in the bill make it clear just what information will be considered “misinformation” under this law. This bill will spell the end of scientific integrity and medical freedom in California. I worry that if it passes, other states could follow suit. As I have said before, California is the tip of the spear:
Here is the text of a letter I submitted last week to the committee where the bill is currently being reviewed:
13 June 2022
To: California Legislators and Committee Members
RE: AB 2098: Physicians and Surgeons: Unprofessional Conduct – OPPOSE
As a licensed physician in California I strongly oppose the proposed California bill AB 2098 and urge you to vote no and oppose as well.
Advances in science and medicine typically occur when doctors and scientists challenge conventional thinking or settled opinion. This is the very nature of scientific progress. Fixating any current medical consensus as “unchallengeable” by physicians will stifle medical and scientific advances and give undue authority to a few gatekeepers who act as guardians of the consensus. As I testified in January at a U.S. Senate panel on Covid policy: “The scientific method suffered [during the pandemic] from a repressive academic and social climate of censorship and silencing of competing perspectives. This projected the false appearance of a scientific consensus—a ‘consensus’ often strongly influenced by economic and political interests.”
One need only look at the last two years to see how frequently public health recommendations and consensus thinking about Covid changed from one month to the next with the advent of new information. It was frontline ICU physicians who discovered and spoke out about bad outcomes when patients were prematurely placed on ventilators. This shifted the consensus in the direction of avoiding ventilation as much as possible. Likewise, it was frontline physicians who discovered that placing covid patients face-down in the prone position while they were ventilated could improve outcomes, challenging another consensus. Both of these advances came by way of challenging the way things were currently being done. Other physicians challenged the early consensus, which did not recommend the use of steroids to treat Covid. Eventually, this dissenting opinion gained ground and now represents conventional thinking: corticosteroids for critically ill covid patients are now standard care. Many other examples regarding guidelines on masks, social distancing, and other Covid policies could be cited here.
Allowing the free interchange among competing perspectives is absolutely necessary for scientific and medical progress. Good science is characterized by conjecture and refutation, lively deliberation, often fierce debate, and always openness to new data. The censorship of free speech in AB 2098 spells not only the demise of civil liberties and constitutional rights, but the end of the scientific enterprise when it comes to dealing with Covid in CA.
Patients will not trust physicians if they believe their physician has been muzzled by the law and cannot speak his or her mind honestly. Patients want to know that if they ask their physician a question, including a question about Covid, they will get their doctor’s honest opinion—regardless of whether they follow that opinion, seek a second opinion, or whatever. Patients will not trust physicians if they know their doctor is simply parroting a consensus judgment that he may or may not agree with or endorse.
This bill will not help us to deal with Covid more effectively. Doctors will be punished for practicing medicine according to their best judgment. Informed consent, the foundation of good medical ethics, will be seriously compromised, and the trust necessary for the doctor-patient relationship will be shattered. I strongly urge you and your fellow lawmakers must oppose AB 2098. It will harm not only physicians and medical institutions in California, but even more concerningly, it will harm patients.
Sincerely,
Aaron Kheriaty, MD
Here is a link to information from The Unity Project on what you can do to oppose this bill—especially important if you happen to live in California. Please spread the word.
Lithuania illegally blocking Kaliningrad
By Lucas Leiroz | June 21, 2022
European authorities are stopping the transit of Russian goods in the Kaliningrad region, which is officially a part of the Russian territory. Such a measure tends to significantly increase tensions on the European continent and contribute negatively at a time of major concerns about international peace and security.
On June 18, the governor of Kaliningrad Anton Alikhanov reported to media agencies that the Lithuanian state-owned company “Lithuania Railways” has banned the rail transport in the Russia’s Kaliningrad territory regarding all sanctioned goods, entirely isolating the Russian exclave in Europe. Apparently, the reason for such a radical measure would have been the international pressure exerted by the rest of Europe for Lithuania to comply with the “EU’s restrictions”.
Commenting on the case, Lithuanian Foreign Minister Gabrielius Landsbergis said that “this is not a Lithuanian decision. These are European sanctions that came into force on June 17, and the railways are now applying the sanctions”.
EU foreign policy chief Josep Borrell confirmed the Lithuanian minister’s words and tried to “defuse” the situation, saying that there is no blockade, as only goods that have received sanctions are being barred from transit:
“There is no blockade. The land transit between Kaliningrad and other parts of Russia has not been banned. Second, transit of people and goods that are not sanctioned continues. Third, Lithuania has not taken any unilateral national restrictions. (…) We are in a precautionary mood. We will double-check the legal aspects in order to verify that we are completely aligned with any kind of rule. (…) But Lithuania is not guilty. It is not implementing national sanctions. It is not implementing their will. Whatever they are doing has been the consequence of previous consultation with the commission, which has provided guidelines”.
What seems unacceptable, however, is the fact that such pressure is aimed at blocking the transit of products inside the Russian sovereign space, preventing them from leaving Kaliningrad and reaching the rest of Russian territory. No country has the right to prevent another from transporting its goods to other parts of its own territory. In this case, it is not just about “sanctions against Russia”, but about an illegal attitude that violates all elementary norms and principles of public international law.
Stating that there is simply “no blockade” as the restrictions are only being applied to sanctioned products sounds also totally inappropriate. In addition to obstructing Russian intra-territorial traffic, the products sanctioned by the West are precisely those of greater strategic value, which directly affect Moscow’s national interests. Kaliningrad is undoubtedly isolated at this time and the consequences of this isolation strongly affect both the rest of the Russian territory and the one million Russian citizens who inhabit the exclave.
The Russian government expressed its concern about the case, as can be seen in the words of Kremlin spokesman Dmitry Peskov: “This decision is truly unprecedented. It is a violation of everything. We understand it to be connected to the relevant decision made by the European Union – to extend sanctions to transit. We also consider it illegal (…) We need a serious, in-depth analysis to work out our response decisions”.
In the same vein, Minister of Foreign Affairs Sergey Lavrov made it clear that Moscow reserves the right to respond to illegal attitudes on the part of the Lithuanian State, stating that Russia will defend its interests in the face of the European attempt to prevent the transit of goods between Kaliningrad and the rest of the national territory.
“If the transit of goods between Kaliningrad and the rest of the territory of the Russian Federation through Lithuania is not fully restored soon, then Russia reserves the right to take measures in defense of its national interests”, he said.
It is also necessary to remember that Western think tanks have long suggested that NATO “seize” Kaliningrad. The matter has come to light more recently, after the start of the special military operation in Ukraine, with US and European experts suggesting this type of attitude to be considered as a response to a possible escalation of tensions. Obviously, the current blockade further intensifies Moscow’s concerns about this possible scenario.
There are two possible scenarios for the near future in the face of this new escalation of the European security crisis: either Lithuania immediately breaks the blockade or Russia will respond in some way, probably through the intensification of military naval activities using the Baltic Fleet. Vilnius must act in some way, either sovereignly, refusing to comply with abusive and hostile EU impositions or through diplomatic mediation with the rest of the bloc so that sanctions are eased so that the end of the rail blockade is achieved.
Lucas Leiroz is a researcher in Social Sciences at the Rural Federal University of Rio de Janeiro; geopolitical consultant.
Dr. Clare Craig from the HART group explains the clinical trial used to justify vaccinating kids
Steve Kirsch | June 19, 2022
The HART group is a group of highly respected independent doctors and scientists. My friend, Professor Norman Fenton, is a member of this group.
In this 4 minute video, Dr. Clare Craig, co-chair of the HART group, explains the clinical trial that was used to justify vaccinating our kids. She was appalled.
The only conclusion you can draw after watching this video is that the people running the FDA, CDC and the members of the outside committees approving these vaccines are either completely incompetent or totally bought off.
Everyone should watch this video. It should be required viewing for any parent who is considering vaccinating their child.
Here is the report Pfizer submitted to the FDA referenced in her video. You can see the numbers on page 39 (look in the column headings for the N= numbers).
The CDC says “severe reactions” to the COVID vaccines are rare. That’s not what we found.
Don’t let the title fool you. The survey was created on June 17 and was executed by Pollfish on Jun 18.
By Steve Kirsch | June 20, 2022
A new poll of Americans shows that it’s likely that over 10M Americans were injured by the vaccine. This may explain why there are staffing shortages everywhere, from pilots to pharmacists.
The CDC has always maintained that severe reactions to the COVID vaccines are rare. Since I became a ‘misinformation’ spreader over a year ago, I’ve never believed that.
Yesterday, VSRF engaged the services of a professional polling company (Pollfish) to survey 500 people who were selected entirely at random.
The results were shocking, but they were consistent with the VAERS data which has been “lit up” since January 2021 telling us “the COVID vaccines are the most unsafe vaccines in human history.”
Now we have independent confirmation that the safety signals in VAERS were accurate, just like we’ve always said.
The numbers in this poll are absolutely shocking and there is no way to spin this as a positive.
This article includes the full Pollfish report as well as the individual response data so that anyone can analyze it themselves.
Key results from the poll
The poll was about the COVID vaccine exclusively, not about other vaccines. Stratified responses are age normalized to the US since the respondents who answered didn’t match the overall US demographics.
Doing some rudimentary estimates from the data (rather than stratifying by age which would be more accurate but more time consuming):
- 20% of the respondents reported they were vaccine injured
- The 20% number is remarkable because there was no pre-screening question and only 77.3% of Americans received at least one dose. That means that if you were vaccinated there is a 26% chance that you were injured (computed as 20.46/77.3). Wow.
- 30% of the households have a vaccine injured person
- 45% of the extended families have a vaccine injured person
- In 87% of the cases where there was a vaccine injury, there was either a doctor visit(s) or hospital stay(s) or both.
- 54% of the injured are still impacted today.
- 45% of the vaccine injured said it would shorten their lifespan
- 41% of the injured are unable to hold a job.
- Only 17% said their injury was a minor annoyance.
Putting these results into perspective
If you took the vaccine there is a 26% chance of injury as noted above. We also know that 45% of the injured said it would shorten their lifespan. This means that we are shortening the lifespan of 12% of the people who opt for the jab (since .26*.45=.117).
Shortening the lifespan of 12% of the people who take the vaccine seems like a very high price to pay for a virus that can be easily treated with a near 100% success rate with repurposed drugs.
For example, my friends George Fareed and Brian Tyson now have treated over 12,000 COVID patients using a combination of repurposed drugs and supplements without a single hospitalization or death if they were treated within 5 days of first symptoms. They even have a top-selling book on Amazon with rave reviews. Despite all of that, the FDA, CDC, and NIH continue to ignore them. They can’t get anyone to return their calls. They’ve had their protocol since the very beginning of the pandemic in March 2020 (it’s evolved over time).
It is stunning that the FDA approves the vaccines for our kids under 5 based on the COVID case statistics from just 10 children (7 placebo and 3 in the treatment arm), yet Fareed and Tyson who have treated over 12,000 patients can’t get a return phone call.
We are basically spending billions of dollars to seriously injure over 10 million Americans and kill hundreds of thousands. In the process, we did not reduce COVID, but made the problem worse with nonsensical interventions when all we ever needed was some simple advice:
- If you are sick stay home
- If you test positive, start a proven early treatment protocol ASAP such as the Fareed-Tyson protocol
We never needed the vaccine, masks (which make the problem worse), lockdowns, mandates, social distancing, or new drugs. All we had to do was follow the two simple steps above. It was never more complicated than that.
The data
Here are the full poll results and a spreadsheet with each individual response so you can do you own analysis:
Comparison with the rates of COVID vaccine injury that nurses report among their peers
Does a 12% injury rate seem high to you? That would be 30M people.
You may change your mind when you watch this video where I interview 7 nurses who were willing to speak out publicly and reveal the rate of vaccine injury among their peers.
Note: There are audio and video drop outs on the call. Use the cursor button to skip over this. I’ve reported these issues to Riverside.fm… their product feels like a beta test. Also, the preview has 8 nurses but there were only 7 in the call. Can you spot the duplicate?
Watch the video.
The rates averaged over 10% with some nurses seeing injury rates among their peers exceeding 40%. Sorry this is so hard to watch with the audio drop outs, but this is the best I have for this interview.
Jessica Rose’s take
She just sent me an email:
Steve, this is excellent. And aligns with my perceptions from the data.
Dr. Pierre Kory’s take
I sent him an email with all the data with a Subject line: Re: WHOA!!! this poll will BLOW YOUR MIND
Pierre quickly wrote back:
Wow is right. Those numbers are beyond disturbing, I have been calling this vaccine escapade a humanitarian catastrophe.. and this is what that looks like.
Comparison with VAERS
OpenVAERS shows 831,800 injuries reported domestically. But non-lethal injuries typically are under reported by a factor of 100 or more as we showed in the analysis of the disability data (where the under reporting factor was 128).
100*831K = 80M vaccine injured.
This makes our survey estimate of 30M look quite conservative.
However, if we take the raw, unadjusted numbers of our survey, 30% of all respondents over 18 were vaccine injured. Since there are 258M people over 18 in the US, we get 77M estimated vaccine injured, eerily close to the VAERS estimate.
So maybe VAERS isn’t such a bad estimator after all.
Validation by the government of Israel
Our final validation point is the proactive poll done by the government of Israel to assess vaccine side effects. This article describes that study. Among the highlights:
- About 25% of people with pre-existing auto-immune disorders, depression or anxiety reported a worsening of their symptoms following the booster.
- 4.5% of respondents reported neurological problems
- 17% reported shaking
So our 20% rate of injury isn’t all that far off what the Israeli government found.
What vaccine injury looks like
Many people never recognize vaccine injury because they don’t know what it looks like.
For example, as I am writing this article, I received the following message from one of my subscribers:
So my mom’s very dear friend called me tonight to tell me that her cancer came back. She was diagnosed over 20 years ago and has been cancer-free. I asked her did you get boosted she said yes, I already knew she was vaccinated. She said don’t start asking me these questions. What does that have to do with anything? They now found Cancer all over her uterus and it’s now spreading to her body. You think it’s from the vaccine? She was perfectly fine all these years before getting vaccinated. It makes me so sad she will probably end up dying.
I hear these stories all the time of a new cancer or a cancer that was under control suddenly coming back with a vengeance. These aren’t coincidences. While for any individual case it may be difficult to determine a cause, in aggregate we are seeing rates of cancer post vaccine that are unprecedented.
This is why Dr. Ryan Cole said, “Since January 1, in the laboratory, I’m seeing a 20 times increase of endometrial cancers over what I see on an annual basis.”
It’s amusing to me that when you search for that quote in Google, you only get articles debunking the claim whereas if you search in DuckDuckGo, you get articles with the original quote. This is pretty sad because Dr. Cole is highly respected among his peers for telling the truth. It’s a pity we never get a chance to have a fair debate with people who claim we are spreading misinformation.
And the personal stories
A lot of people tell me they know hundreds of people and none are vaccine injured.
Perhaps.
Or perhaps 95% of the vaccine injured don’t speak out about their vaccine injury.
It feels like for every person who sees nothing, I hear from people with the opposite experience:
I have so many of my relatives, neighbors and acquaintances succumb to this poison. Just yesterday a 30 year old acquaintance died of sudden heart attack. My aunt is suffering from autoimmune mediated arthritis after she got her 2nd Pfizer shot. A neighbor died after receiving the first dose of Sinovac Vaccine. A relative died after receiving 2nd dose of SinoVac… So many to list!!
Replicating the poll
The out-of-pocket cost for the poll is $500. Anyone could replicate it.
I’m sure fact checkers will spend $50,000 to replicate it 100 times until they get the results that match their narrative, and then publish that.
We didn’t do that. We’ve never asked this set of questions ever before. The questions weren’t “gamed” to elicit a specific response. We put together the questions we wanted, we ran the poll, and we published the results.
But the poll is affordable enough that if you don’t believe me, you can replicate it yourself.
Summary
The COVID vaccines are the most dangerous vaccines in human history. There are systemic flaws in the medical system that cause doctors to fail to recognize the evidence in plain sight. But that doesn’t change the reality. The COVID vaccines have killed hundreds of thousands of people and severely injured millions more. Since there is a safe, inexpensive alternative (early treatment protocols) with near 100% efficacy in reducing hospitalization and death, the vaccines should be immediately halted for all age groups. That would be the right thing to do.
But admitting they made a mistake would be an embarrassment to the medical community, government agencies, and Congress. So they will continue to look the other way and find ways to discredit the evidence and the brave people who are speaking out. They will continue to avoid any accountability by agreeing to an open debate. And in the meantime, millions more will be disabled, and hundreds of thousands will die prematurely.
Doctors and nurses know what is going on, but will not speak out as a group because they will lose their jobs and ability to practice medicine. So they keep their heads down.
The other doctors are so blue-pilled, they actually still believe the CDC. When Pfizer presents safety and efficacy data that is appalling to anyone with a working brain, they simply look at the vote count of the outside committees (unanimously approved) and never bother to learn more about what just happened. They won’t even watch this 4 minute video that explains just how bad the trial data was.
When we discovered that there wasn’t a single death from COVID-19 in the entire state of Massachusetts in both 2020 and 2021 in age 5 to 11, did that change anything? Of course not. COVID is an emergency because it might kill kids in the future and you can never be too careful when it comes to saving kids lives. But when large numbers of kids are killed by the vaccine, we simply look the other way. That’s not an emergency; it doesn’t even exist. Their odd causes of death are ignored.
My survey won’t change anything, even if it is replicated over and over. It will just add more evidence to the public record that the medical community is causing great harm and completely incapable of seeing the truth. They will not allow themselves to be held accountable in an open discussion— ever.
The American people won’t change their minds until the doctors change their minds. And the doctors are so well trained to respect the medical authorities like the FDA, CDC, and NIH and/or sufficiently afraid of the repercussions of speaking out, that nothing will change anytime soon.
The truth always comes out sooner or later. The later it comes out, the greater the damage will be to all these institutions that people once trusted.
The other thing I know is that the scale of this deception is unprecedented. When this unravels, which I have no doubt that it will, it will destroy our trust in:
- the medical community
- the HHS government agencies: CDC, FDA, NIH
- the mainstream media
- Congress
- State and local government officials
- CEOs who imposed vaccine mandates
- local health officials
- Mainstream social networks
- Fact checkers
- The Gates Foundation
- Bill Gates
- The Rockefeller Foundation
- the drug companies
- the courts
- clinical trials
- medical journals
- … and more…
This survey is just one more nail in the coffin of the “safe and effective” narrative. Nothing more.
Featured Video

Pediatrician shares 30 yrs of insight on vaccinating vs. not vaccinating children
or go to
Aletho News Archives – Video-Images
Book Excerpt
Biden’s Closed Circle on Russia
An excerpt from ‘The Great Betrayal’
By James W. Carden | The Realist Review | June 14, 2026
Joe Biden’s presidency may ultimately come to be seen as a cautionary tale. Here was a president who showed little interest in entertaining arguments that might have contradicted his most deeply held assumptions.[1] And there were precious few within the upper ranks of the administration who might have attempted to do so, after all, only policy hands and political operatives who had come up through the ranks of the Clinton and Obama administrations or had longstanding ties to the citadels of the foreign policy community were invited into the fold. … continue
Blog Roll
 Aletho News
Aletho News- Terms of Iran-US MoU revealed: Bloomberg
- A California Pediatrician Shares 30 Years of Insight on Vaccinating vs. Not Vaccinating Children
- What Is Defensive Medicine?
- CDC Awards Pfizer $1.24 Billion for COVID Vaccines for Kids and Adults
- Historic blow to South Korea’s military intelligence agency
- Russian frigate fires warning shots in English Channel
- Radio Free Europe, the Cold War ‘Weapon’ Congress Still Funds
- UN: Israel continues to violate Lebanon airspace in defiance of Iran-US MoU
- Araghchi: Israeli occupation of Lebanese land a violation of MoU
- Hezbollah fighters confront intruding Israeli forces in southern Lebanon
- If Americans Knew
- Pro-Israel Donors Power Last-Minute Surge of Espaillat Spending
- “They Stole Our Home and Our Life”: Israel Permanently Displaces Syrians in Quneitra
- Massie Recognizes USS Liberty Attack. Here’s Why That Matters
- The blatant racism and cruelty that define Israel’s settler movement
- Israeli army ‘murdered child’ in Gaza and then dumped body on a roadside
- The Forward’s Hit Piece on Thomas Massie and USS Liberty Veterans
- Israel’s former defense minister compares settler ideology to Nazism
- The Pro-Israel Lobby’s Quiet Cash Shuffle
- Trinity Broadcasting Network (TBN) Propagandizes for Israel’s Wars
- A grim milestone: Gaza’s death toll surpasses 73,000 – Daily Update
- No Tricks Zone
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
