Russia reveals number of victims from drilling rig strikes
Samizdat | June 20, 2022
Three people were injured and seven missing following a suspected Ukrainian attack on drilling rigs off the coast of Crimea, the head of the Russian region, Sergey Aksyonov, revealed on Monday.
Earlier, he said that three missile strikes hit three separate rigs owned by Chernomorneftegaz, a company that develops offshore oil and gas fields.
“So far, 94 people have been evacuated. 15 servicemen remain guarding the operating drilling platforms. Unfortunately, information on 3 wounded and 7 missing has been confirmed,” Aksyonov said in a statement.
He stressed that the search operation will continue and the regional government will contact the families and friends of the missing and injured.
Meanwhile, the Russian Investigative Committee has opened a criminal case in relation to the shelling.
According to the committee’s statement, “the military personnel of the Armed Forces of Ukraine targeted the platform of the gas production tower <…> using weapons with high damaging properties.”
Last Friday, the Ukrainian presidential representative for Crimea, Tamila Tasheva, said that Ukraine is now relying on military means when it comes to what she called “returning” Crimea. She explained that the Russian military offensive had prompted Kiev to largely leave behind its diplomatic strategy for the peninsula’s “deoccupation.”
Tasheva’s remarks came a day after Ukraine’s Defense Minister Alexey Reznikov said that Kiev, using US-supplied weapons, is going to “liberate” all land lost to Russia, including Crimea. Prior to that, Ukrainian President Volodymyr Zelensky vowed to “liberate” Crimea and the Donetsk (DPR) and Lugansk (LPR) People’s Republics, which are recognized by Russia as independent states.
Ukrainian troops have been losing territory to Russia and allied forces in Donbass, even as Western nations supply more sophisticated weapons to Kiev. Several Ukrainian officials have stated that the pledge to not use foreign weapons to attack targets in Russia does not apply to Crimea, which Kiev considers part of its territory. Major General Dmitry Marchenko said last week that the bridge connecting the peninsula with mainland Russia is “absolutely our number one target.”
Russia attacked the neighboring state in late February, following Ukraine’s failure to implement the terms of the Minsk agreements, first signed in 2014, and Moscow’s eventual recognition of the Donbass republics of Donetsk and Lugansk. The German- and French-brokered protocols were designed to give the breakaway regions special status within the Ukrainian state.
The Kremlin has since demanded that Ukraine officially declare itself a neutral country that will never join the US-led NATO military bloc. Kiev insists the Russian offensive was completely unprovoked and has denied claims it was planning to retake the two republics by force.
Casualties reported after strike at Russian drilling platforms in Crimea
Samizdat | June 20, 2022
Suspected Ukrainian attacks targeted drilling rigs off the coast of Crimea in the Black Sea on Monday morning, the head of the Russian region, Sergey Aksyonov, said in a statement. He added that the rigs were manned by 12 workers, five of whom have been rescued so far, including three with injuries.
Aksyonov did not disclose the exact locations of the facilities, but said they were owned by Chernomorneftegaz, a company that develops offshore gas and oil fields. Its ownership has been disputed by Ukrainian energy giant Naftogaz since 2014, when it was nationalized after Crimea voted to re-join Russia.
The head of Crimea later said that three missile strikes hit three separate rigs. Aksyonov said a total of 109 people were in the area at the time of the attacks and that the evacuation of the workers was underway.
The attack targeted offshore rigs located about 71km from the Ukrainian port of Odessa, Olga Kovitidi, who represents Crimea in the upper chamber of the Russian parliament, told RIA Novosti.
Some Ukrainian media reported that earlier in the day, dozens of missiles hit Snake Island, a small islet off the Ukrainian coast, which has been controlled by Russia for months. Ukrainian MP Aleksey Goncharenko claimed that some of the missiles hit the gas rigs instead of the island.
Ukrainian troops have been slowly losing territory to Russia and allied forces in Donbass, even as Western nations supply more sophisticated weapons to Kiev. Several Ukrainian officials have stated that the pledge to not use foreign weapons to attack targets in Russia does not apply to Crimea, which Kiev considers part of its territory. Major General Dmitry Marchenko said last week that the bridge connecting the peninsula with mainland Russia is “absolutely our number one target.”
This month, Kiev reported deploying US-made Harpoon anti-ship missiles as part of its coastal defense systems. Last week, Kiev claimed it had attacked a Russian military tugboat with two of these missiles.
More Vaccine-Injured Pilots Speak Out as Groups Pressure Airlines, Regulators to End Mandates
By Michael Nevradakis, Ph.D. | The Defender | June 17, 2022
Sharp chest pains. Myocarditis and pericarditis. Heart attacks. Strokes and subsequent blindness.
These are just some of the many COVID-19 vaccine-related adverse events reported by commercial airline pilots and by a growing number of advocacy groups representing aviation industry workers.
According to these individuals and groups, the number of pilots speaking out about their vaccine injuries is dwarfed by the number of pilots who are still flying despite experiencing concerning symptoms — but not speaking out because of what they describe as a culture of intimidation within the aviation industry.
These individuals fear they will lose their jobs and livelihoods in retaliation if they reveal their symptoms or go public with their stories, sources told The Defender.
Still, a growing number of pilots are coming forward.
Last month, The Defender published the accounts of several pilots — and of the widow of a pilot who died from a vaccine-related adverse event.
Since then, more pilots have shared their stories, including one who is currently flying for a commercial airline.
A growing number of advocacy organizations, representing workers across the aviation industry and in several countries, are joining these pilots in speaking out.
The Defender previously reported on actions by the U.S. Freedom Flyers (USFF) and other legal advocates in the U.S.
Since then, representatives from the Global Aviation Advocacy Coalition (GAA) and the Canada-based Free To Fly also spoke with The Defender about their initiatives.
Meanwhile, pilots in Canada and the Netherlands recently reported significant legal victories in separate vaccine-related cases.
More pilots come forward, speak to The Defender
Steven Hornsby, a 52-year-old pilot with a legacy passenger airline company, was once an active weightlifter and cyclist, biking 10-26 miles every other day.
He is also a veteran of the U.S. Marine Corps and Operation Enduring Freedom. Per FAA requirements, he passed 24 medical exams in the past 12 years, including 12 electrocardiograms (ECGs).
Hornsby told The Defender, “I’ve never had any cardiovascular issues in my life, nor have I ever had any major health issues … I eat healthy and live what I believe to be a balanced lifestyle.”
Hornsby, however, is not flying today because, he said, he was “coerced … to get the COVID-19 vaccine,” and his employer “made it very clear that all employees would be required to get it and that medical/religious exemptions would be very difficult to get.”
Hornsby’s difficulties began after receiving the second dose of the Pfizer COVID-19 vaccine.
“After my second shot, I initially had zero issues, with little more than light fatigue on day two, Hornsby said. “The 12th day, however, was the culmination of the vaccine and the continuous stress I was adding to my heart from rigorous exercise.”
As he was driving with family, Hornsby said he felt sharp chest pains, “pain radiating through my left arm, and my heart rate spiked as if beating in my neck.”
Hornsby said it took several different diagnoses from doctors and medical practitioners to make a connection between his health issues and the vaccine.
A nurse at an urgent care facility first told him his symptoms did not correlate to a heart attack and were most likely unrelated to the vaccine. Later, at a hospital emergency room, he was again told his symptoms were not likely to be related to the vaccine.
“At that point,” Hornsby said, “I was indignant. Why would a healthcare provider dismiss that perspective? This was my eye-opening reality that a major cover-up was in play.”
Hornsby was ultimately diagnosed with elevated blood pressure but was told he had not suffered a heart attack. Doctors advised him to follow up with a cardiologist, and told him they would not report his case to the Vaccine Adverse Event Reporting System (VAERS).
Hornsby said his cardiologist, after performing blood work, told him his heart was healthy, and though the doctor didn’t dismiss the possibility that his heart issues were connected to the vaccine, he told him the symptoms were “most likely from stress or a musculoskeletal problem.”
“I had to stop trying to force my perceived diagnosis — bias against the vaccine — and listen to the professionals,” Hornsby said, adding “I needed to be patient,” even after a union doctor also dismissed Hornsby’s concerns that his symptoms were related to the vaccine.
Hornsby continued experiencing “intermittent pains,” despite taking home remedies such as tea and supplements to calm his heart rate, which he said were helpful.
It was only in December 2021, when his medical certification was due for renewal, that his aeromedical examiner (AME) advised him to wear a Holter monitor (a type of portable ECG) for one week to monitor his heart.
“That is when I discovered that I had arrhythmia issues, heart palpitations and [an] irregular heart rate, which was occurring almost exclusively at night,” said Hornsby. “I reported back to my AME, who then told me I was grounded and that I should go find a good cardiologist and get healthy.”
The following month, another cardiologist diagnosed Hornsby with vaccine-induced myocarditis.
“My heart was inflamed,” said Hornsby. “After an echocardiogram, it showed my heart mildly dilated with fluid behind my heart.”
Hornsby said he’s “doing much better,” but he’s still not flying. He’s disappointed with the dismissive manner in which several doctors addressed his concerns.
“Had doctors been willing to view my case — and I suspect others — with an open mind, this could have been diagnosed much, much earlier,” he said. “Looking back, had my heart not been healthy, I would have surely died from cardiac arrest like you’re seeing in young athletes.”
Hornsby said he believes other pilots with similar symptoms are still flying.
“I suspect there are many pilots flying around with minor and perhaps major issues,” Hornsby said. “The vaccine is/was experimental and for good cause. No one knows the long-term effects.”
He added:
“How many years have been shaved from my life? Will I develop scar tissue in my heart? Will I get cancer as a result? Has this trash degraded my immune system? Only God knows.”
Pilot injured by Moderna shot: ‘I have a family to feed’
In fact, The Defender interviewed another pilot — currently flying for a commercial airline in the U.S. — who is experiencing such health difficulties.
The pilot, who spoke to The Defender on condition of anonymity, said:
“I was experiencing chest pain, usually at night, almost like somebody had their hand around my heart and was squeezing.
“Generally, [the pain] would subside during the day, but … would appear occasionally out of nowhere and I would need to lie down.
“It would manifest as pain, but also like something was lodged deep in my esophagus, like I had a piece of food or air that was pressing upon my chest area.”
According to the pilot, his symptoms “began about a week after the second Moderna vaccination.”
He said the airline he works for threatened to terminate anyone who didn’t get the vaccine. “I have a family to feed, so I was left with little choice.”
He said he is “on reserve” and not flying often. While his symptoms have recently subsided, he felt that “looking into further treatment would result in an answer that would be unfavorable to my medical [certification].”
He added:
“In the back of my mind though, the thought of what it could mean for my future health is there.
“The current situation I am faced with is that supporting a family is what is most important to me. Fear of loss of my pilot medical [certification] after being mandated to get this vaccine is the path I am currently on.”
Terminated after 19 years for refusing COVID shot, former Australian pilot advocates for others
Australia, like Canada, has a government-level vaccine mandate for airline crew and airport workers. In Australia, this mandate went into effect on Nov. 15, 2021.
Glen Waters is a former captain with Virgin Australia who is now a spokesman for a group of employees from the same airline.
Waters, who had held the rank of captain for 19 years before being terminated by Virgin Australia for refusing the vaccine, spoke to The Defender on behalf of several pilots who are suffering from vaccine injuries.
According to Waters, “none of the pilots suffering from injuries are prepared to talk” because “the company is actively trying to terminate anyone reporting vaccine injury.”
Waters said employees whose health issues are characterized as “unrelated” to the vaccine are being treated by Virgin Australia “as you would expect a company to care for its employees.”
Waters stated “there are several reasons injured pilots will not come forward,” including:
- “There is a stigma attached to anti-vaccine sentiment in any form.
- There is a reluctance on the part of the medical community to get involved with possible vaccine injuries.
- Vaccine makers will actively fight against injury claims.
- Insurance companies have distanced themselves from claims involving the vaccine.
- Pilots don’t want to lose their medical certifications, jobs or careers.
Waters said of approximately 900 pilots flying with Virgin Australia, he is aware of nine who are no longer flying because of medical complications that could be linked to the vaccine.
“No doubt there are many more who are continuing to fly with troubling symptoms,” he said.
These symptoms, according to Waters, most commonly include myocarditis and pericarditis. Some symptoms, however, are even more serious.
Waters told The Defender :
“We have one captain [who had] a stroke and went blind, and another had a heart attack and fell down the boarding stairs after landing.
“There have been complaints of constant headaches and numerous reports of chest pains and shortness of breath.
“A number of cabin crew have reported pins and needles in their limbs, almost like electric shocks that persist for hours at a time.
“I have heard [about cases of] tinnitus, vertigo and brain fog, including temporary blindness, in several crew. Disrupted menstrual cycles are reported frequently, perhaps affecting dozens [of employees].”
However, according to Waters, perhaps due to the work environment, not all pilots are comfortable in stating openly that there may be a connection between their health difficulties and the vaccines.
“I’m only aware of three who say the symptoms started within an hour of the vaccine, one within seven days,” he said.
“The stroke and heart attack victims are not attributing their medical event to the vaccine as far as I am aware. Neither [did] the captain who died of a sudden onset of cancer early this year.”
Some employees may not understand their symptoms might be related to the vaccine, Waters said. “Many of the early warning signs — persistent headaches, chest pains, breathlessness — are not recognized by aircrew as possible adverse reactions,” Waters said.
“The heart attacks and strokes are occurring in otherwise fit and healthy individuals. They are sudden and are a real risk to flight safety.”
Waters explained that Australia’s Civil Aviation Safety Authority, similar to other such bodies globally, has “a 1% rule” for pilots: If they have a medical condition “that presents a greater than 1% chance of resulting in an incapacitation event within the next 12 months, then they are considered medically unfit to fly.”
In light of this, according to Waters, “numerous aviation doctors, including Lt. Col.Theresa Long and Lt. Col. Peter Chambers, have recommended tests that will help determine the real risk to pilots.”
These include the D-dimer test for blood-clotting conditions, a complete blood count, post-vaccination ECG analysis, a cardiac MRI and others.
As pilots speak out, there are some legal victories
Despite what numerous pilots call a hostile environment in the aviation industry toward claims of vaccine injury, a recent series of legal decisions were in pilots’ favor and more legal actions are in progress.
A judge at the Amsterdam Court of Appeals in the Netherlands on June 2 ruled in favor of the Dutch Airline Pilots Association, in a case that challenged vaccine mandates introduced by Dutch airline KLM for new pilots.
According to the ruling:
“It is considered that requesting and demanding a vaccination against corona constitutes an unjustified infringement of the fundamental rights of the candidate pilots.
“In particular, it infringes the privacy (Article 8 ECHR) [the European Convention on Human Rights] of the candidate pilots.
“After all, the decision whether or not to have yourself vaccinated is something that belongs pre-eminently to this private sphere.
“Requiring the candidate pilot to be vaccinated and to give a positive answer to that question about vaccination status, therefore, violates this. KLM thus leaves no choice to candidate pilots who want to join KLM.”
Per the June 2 ruling, KLM is prohibited from requesting or collecting such information from candidate pilots, or rejecting candidates on the basis of their vaccination status, under penalty of €100,000 (approximately $105,000) per violation.
Following the ruling, the Dutch Pilots Association issued a statement, remarking:
“The [association] endorses the government’s position that vaccination is important, but that compulsory vaccination by the employer is not permitted.
“We were of the opinion that KLM did not comply with this and, moreover, violated our agreements about this, without there being any operational necessity.”
In Canada, the federal government on June 14 announced most travel-related vaccine mandates would be lifted as of June 20.
Responding to this announcement, in a statement sent to The Defender, Free to Fly credited those who opposed the mandates, stating:
“This dark season helps reinforce an important maxim; true change only comes about through tenacity, courage, and the relentless pursuit of truth by principled men and women.
“Across our nation, many Canadians refused to give up on freedom and fought for our fragile democracy. We feel no ‘gratitude’ towards an emboldened state for ceasing to violate God-given freedoms.
“We must never forget our recent travails, and cannot be lulled into complacency, certainly with Trudeau’s government openly threatening reinstatement of mandates with any ‘new variant’.
“We will continue to pursue them, insisting on uncompromising standards in our industry and the assurance we never again go down this road of medical segregation.”
In another recent development, Canadian pilot Ross Wightman became just one of a small number of people who have received compensation from Canada’s Vaccine Injury Support Program.
Wightman was diagnosed with Guillain-Barré Syndrome, a rare condition that affects the nervous system and may cause muscle weakness, paralysis or even death.
He developed the condition within days of receiving his first and only dose of the COVID-19 vaccine. For the past year, Wightman has been unable to work, as he has substantially limited mobility in his arms and legs.
Global Aviation Advocacy Coalition pens open letter to aviation industry
In an open letter to the aviation industry, the GAA raised serious allegations regarding industry vaccine mandates, which the GAA said resulted in a growing number of vaccine-injured pilots who are unable to fly and who may never do so again — and an increasing number of pilots who continue to fly while experiencing potentially serious symptoms.
The letter was signed by organizations including the USFF, Free To Fly Canada, the Aussie Freedom Flyers, the UK Freedom Flyers, the International Medical Alliance, the Global Covid Summit, the Canadian Covid Care Alliance, the UK Medical Freedom Alliance, the Association of American Physicians and Surgeons, and several other groups in the U.S., France, the Netherlands, Switzerland and the U.K., as well as more than 17,000 physicians and medical scientists from around the world and “thousands of pilots at over 30 global airlines.
The GAA said it is in communication with pilots at the following U.S.-based airlines: Alaska, American, Delta, Frontier, JetBlue, Southwest, Spirit and United, and 12 major air carriers in Australia, Canada, France, Germany and the Netherlands.
According to the GAA’s open letter, the organization and the scientists and doctors it works with “are hearing daily from vaccine-injured airline pilots” about conditions including “cardiovascular issues, blood clots [and] neurological and auditory issues.”
The injured pilots are experiencing a broad spectrum of symptoms, “ranging up to death,” the GAA wrote, adding the symptoms “at least correlate to receiving COVID-19 vaccinations.”
The GAA wrote that in many instances, these conditions are serious enough that “pilots have lost medical certification and may not recover the same,” while others “are continuing to pilot aircraft while carrying symptoms that should be declared and investigated, creating a human factors hazard of unprecedented breadth,” and “a landscape which should greatly concern airlines and the traveling public.”
Pilots continue to fly despite experiencing such symptoms, said the GAA, because those “who report their injury face possible loss of licensing, income, and career while receiving little to no support from their unions, and a prosecutorial invective from employing airlines.”
The GAA said many pilots were reluctant to receive the COVID-19 vaccine and opposed mandates:
“Pilots are trained to be careful analysts of their environment, recognizing risks and actively mitigating. For many, their training and differential risk analysis led to concerns and negative conclusions regarding the compatibility of COVID-19 vaccination with health and flight safety.
“Not only did many pilots disagree with arbitrary requirements embodied in vaccination mandates, but they also saw risks in the unanswered questions and unjustified speed and pressure behind the vaccine rollouts. They lobbied their airlines and politicians, recommending caution and opposing mandates.”
However, stated the GAA, for many pilots, it was a choice between vaccination and job loss:
“Once airlines mandated vaccination, many pilots steadfastly refused based on risk and were subsequently put on unpaid leave or outright terminated.
“Principled professionals were forced out of aviation and the industry lost hundreds of thousands of hours of experience. Now, the global airline industry is heading into a dire staffing crisis.
“Thousands of other pilots were coerced into vaccination to provide for their families. This has taken a toll on their mental health.”
For the GAA, blame lies with the mandates — and more broadly, with the airlines, regulators and unions:
“ … there appears to be no evidence of aviation regulators, airlines or unions having performed any of their own due diligence into COVID-19 vaccines and the impact on pilot health or performance.
“This is at complete odds with existing aviation medical standards. Questions exist around competence and possible negligence.
“Failure to address this potential medical watershed will make the airlines and unions complicit in a culture shift that has rocked the aviation mantra of ‘safety first, always.’”
The GAA called on civil aviation authorities such as the Federal Aviation Administration, Transport Canada, UK Civil Aviation Authority, the European Union Aviation Safety Agency and Australia’s Civil Aviation Safety Authority to begin fulfilling their regulatory obligations.
“The crisis in pilot health must be publicly addressed by airlines and representing unions to restore flight safety to what we once knew,” their letter stated.
GAA called for:
- “Where it exists, mandated COVID-19 vaccination for aviation workers must be discontinued.
- A permissive environment for self-reporting needs to be reemphasized by regulators and airlines.
- Thorough and objective aviation medical screenings of pilots and cabin crew need to be a high priority. These must be backed by the regulator and should focus on high prevalence harms which are now showing up in the general public and in our flight crews.
- Airlines and regulators hold data about sickness and medical certificate suspension, including symptoms and causal reasons. This data should be analysed by independent third parties to establish or rule out COVID-19 vaccination as a possible cause.”
Free to Fly pursues legal action against Canadian authorities, airline
Canada-based Free to Fly represents close to 3,000 aviation professionals, according to its director, Greg Hill, who spoke to The Defender.
These professionals include pilots, flight attendants, air traffic controllers, maintenance workers and customer service representatives.
According to Hill, industry workers have reported a wide range of health issues, including “generalized chest pains, myocarditis, enlarged heart, blood clots, hearing loss, partial paralysis, lymph issues [and] broad autoimmune dysfunction.”
Some of the injured pilots are “high-end athletes” who experienced a “major decrease in their performance capacity.”
“We’ve had some inexplicable deaths at unreasonably young ages,” Hill said, and “an increase in in-flight diversions with one of our airlines in particular.”
While Hill left open the possibility that at least some of these incidents weren’t vaccine-related, he said that Canadian authorities show “an unwillingness to do a proper investigation.”
“Transport Canada, the airline industry, the airlines and the unions have been uniformly silent on the matter,” Hill said.
Indeed, Hill said the aviation industry, regulators and unions in Canada have not been responsive to outreach from Free to Fly.
Referring to a document, prepared in conjunction with the Canadian COVID Care Alliance, that said flight crew pilots were most at risk of vaccine-related adverse effects due to their work environment, Hill said:
“We gave this to the two largest pilot unions in the country, the Air Canada Pilots Association and ALPA, the Airline Pilots Association … they have refused to respond to it.
“We also sent it to management at two of our largest airlines … they also have refused to even respond to it. And this was raising very explicitly the risks that these medical professionals felt needed, at the very least, to be investigated.
“And as yet, we’ve had nothing but silence formally as far as a response from these groups, as far as adverse events, vaccine injuries.”
The document provides: information on a union’s obligation to its members; a differential risk analysis of COVID-19 versus the vaccines; an analysis of natural versus vaccine-induced immunity; an analysis of adverse reactions to the vaccines and particular risks faced by flight crews; a list of alternate treatment options for COVID-19; and a discussion of informed consent and coercion.
According to Hill, the policy is “no jab, no job” for pilots and aviation professionals in Canada, unless they are granted religious or medical exemptions.
But, said Hill, even in the rare instance when an exemption is granted, those employees nevertheless have found themselves out of work, due to airline practices that Hill described as extortionate.
Hill told The Defender :
“If you’re not willing to take the jab and you can’t be accommodated with a religious or medical exemption, then you are either on unpaid leave or outright terminated. Some of our pilots have already been terminated.
“The vast, vast majority of these accommodations were outright denied … some of the stories of people that were denied medical accommodations are truly shocking, the same on the religious aspect.
“The handful that were approved … are simply another round of extortion. Some of them were denied, then they were approved retroactively … essentially they were approved, but then it didn’t change anything … you continue your unpaid leave, but you’re allowed your benefits.”
Similar to claims made in an open letter hand-delivered to the U.S. Federal Aviation Administration (FAA) and major U.S. air carriers in December 2021, Free to Fly also alleged a violation of existing aviation regulations, this time in Canada.
According to Hill:
“There was, at one point, on the Transport Canada website, this was July 2021, a line that specifically said it remains a general position of Transport Canada … that participation in medical trials is not considered compatible with aviation medical certification.
“A number of us were asking questions … and saying, ‘Well, what’s up with this?’ And the answer was these [vaccines] are approved. And we said, ‘No, they’re not fully approved, they’re approved under interim order.’”
Hill said if you read that interim order, it was quite laughable. It basically said, ‘We’ll roll these vaccines out and we’ll gather data. Right now we feel that they’re okay and we’ll continue to assess as we continue to jab people,’ which just seems insane.
“So we asked these explicit questions, got no suitable answers,” Hill said. “And the week following … they simply memory-holed it, they removed that line and it’s no longer on the website. That was their response.”
Hill also described a culture of intimidation in Canada among pilots and flight crews, resulting in a reluctance to come forward with vaccine injury claims:
“Unless the individuals involved are willing to speak to it, I can’t say … every pilot that’s currently still employed … is living in fear of speaking explicitly, certainly in any public forum … for fear of the retribution that has been rolled out against those of us who no longer have work because we refuse to go down this road and insisted upon medical freedom and in doing a proper analysis of what we’re up against here.”
This has not stopped Free To Fly from pursuing legal action in Canada. According to Hill, in Canada, “… you can’t seek private representation against your company. You have to do it through your union. And when the unions decide to not engage, you’re left between a rock and a hard place.”
Hill added:
“ … if you read through the case law precedent over the past year or two in Canada, the courts have very, very much chosen a side. And the concern is within an English common law system, if we continue to litigate, litigate and lose and lose and lose, you create precedent that makes it harder and harder to dig your way out.
“Unfortunately, in this country, the law is downstream of politics. It’s heavily influenced by it, certainly in my opinion. And politics, of course, is downstream of culture. So unless you impact culture and impact the broader narrative, it’s very difficult to see legal solutions.”
Free to Fly on June 6 sent a letter to Canada’s minister of transport, co-signed by the GAA, containing “important, detailed questions regarding COVID-19 vaccines and flight safety,” according to Hill.
As of this writing, the minister has not responded.
Hill said:
“It’s just mind-boggling … we’ve literally stood the [aviation industry’s] safety culture on its head, and that’s the greatest concern to us.
“It’s not an interest in a desire for conflict. I long for the world before this became an all-consuming role, where we’re pushing to try and get ourselves back to a sense of normalcy and proper risk assessment and risk mitigation, which is what pilots are really dedicated to.
“So that’s all we want: that ability to look at this properly and analyze it properly … aviation medical screenings focusing on some of the high prevalence harms that we’ve seen, that we’re hearing about … these screenings need to be backed by the [Canadian] regulator who, in our opinion, has not done their job properly over the past couple of years.”
As far as suspensions, Hill said, pilots who are off and on have not been able to get their medical [certification] back. And these need to be analyzed by independent third parties.
Some pilots and aviation professionals, in addition to speaking out, are joining advocacy groups.
For instance, Hornsby and the pilot quoted in this story who opted to remain anonymous, have joined USFF, according to its co-founder, Josh Yoder, as are the pilots and air traffic controllers who previously shared their stories with The Defender.
USFF has recently begun filing a series of lawsuits against airlines and federal agencies in response to the vaccine mandates and their aftermath.
Ultimately, though, the public — not just pilots and aviation professionals — must also speak out, according to Hill.
“Whether it’s Canada, the United States, Australia, the United Kingdom, etc., we’d like to see the public as a whole rising up and speaking out publicly about these issues, asking why the regulators haven’t done proper risk assessments in regards to where we’re at with these jabs.”
Michael Nevradakis, Ph.D., is an independent journalist and researcher based in Athens, Greece.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
1.3 million reports of injuries after COVID vaccines, VAERS data show, as CDC rubber-stamps shots for kids under 5
By Megan Redshaw | The Defender | June 17, 2022
The Centers for Disease Control and Prevention (CDC) today released new data showing a total of 1,301,356 reports of adverse events following COVID-19 vaccines were submitted between Dec. 14, 2020, and June 10, 2022, to the Vaccine Adverse Event Reporting System (VAERS). That’s an increase of 6,027 adverse events over the previous week.
VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S.
The data included a total of 28,859 reports of deaths — an increase of 327 over the previous week — and 238,412 serious injuries, including deaths, during the same time period — up 1,645 compared with the previous week.
Of the 28,859 reported deaths, 18,719 cases are attributed to Pfizer’s COVID-19 vaccine, 7,581 cases to Moderna and 2,493 cases to Johnson & Johnson (J&J).
Excluding “foreign reports” to VAERS, 831,801 adverse events, including 13,293 deaths and 84,151 serious injuries, were reported in the U.S. between Dec. 14, 2020, and June 10, 2022.
Foreign reports are reports foreign subsidiaries send to U.S. vaccine manufacturers. Under U.S. Food and Drug Administration (FDA) regulations, if a manufacturer is notified of a foreign case report that describes an event that is both serious and does not appear on the product’s labeling, the manufacturer is required to submit the report to VAERS.
Of the 13,293 U.S. deaths reported as of June 10, 16% occurred within 24 hours of vaccination, 20% occurred within 48 hours of vaccination and 59% occurred in people who experienced an onset of symptoms within 48 hours of being vaccinated.
In the U.S., 590 million COVID-19 vaccine doses had been administered as of June 10, including 349 million doses of Pfizer, 223 million doses of Moderna and 19 million doses of Johnson & Johnson (J&J).

Every Friday, VAERS publishes vaccine injury reports received as of a specified date. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
Historically, VAERS has been shown to report only 1% of actual vaccine adverse events.
U.S. VAERS data from Dec. 14, 2020, to June 10, 2022, for 6-month-olds to 5-year-olds show:
- 1,739 adverse events, including 65 cases rated as serious and 3 reported deaths.
- 4 reports of myocarditis and pericarditis (heart inflammation).
The CDC uses a narrowed case definition of “myocarditis,” which excludes cases of cardiac arrest, ischemic strokes and deaths due to heart problems that occur before one has the chance to go to the emergency department. - 13 reports of blood clotting disorders.
U.S. VAERS data from Dec. 14, 2020, to June 10, 2022, for 5- to 11-year-olds show:
- 11,370 adverse events, including 294 rated as serious and 5 reported deaths.
- 22 reports of myocarditis and pericarditis.
The Defender has noticed over previous weeks that reports of myocarditis and pericarditis have been removed by the CDC from the VAERS system in this age group. No explanation was provided. - 44 reports of blood clotting disorders.
U.S. VAERS data from Dec. 14, 2020, to June 10, 2022, for 12- to 17-year-olds show:
- 32,203 adverse events, including 1,834 rated as serious and 44 reported deaths.
- 62 reports of anaphylaxis among 12- to 17-year-olds where the reaction was life-threatening, required treatment or resulted in death — with 97% of cases attributed to Pfizer’s vaccine.
- 656 reports of myocarditis and pericarditis with 644 cases attributed to Pfizer’s vaccine.
- 166 reports of blood clotting disorders with all cases attributed to Pfizer. VAERS reported 167 cases of blood clotting disorders in the 12- to 17-year-old age group last week.
- 19 cases of postural orthostatic tachycardia syndrome (POTS) with all cases attributed to Pfizer’s vaccine.
U.S. VAERS data from Dec. 14, 2020, to June 10, 2022, for all age groups combined, show:
- 20% of deaths were related to cardiac disorders.
- 53% of those who died were male, 42% were female and the remaining death reports did not include the gender of the deceased.
- The average age of death was 73.
- As of June 10, 5,577 pregnant women reported adverse events related to COVID-19 vaccines, including 1,744 reports of miscarriage or premature birth.
- Of the 3,608 cases of Bell’s Palsy reported, 51% were attributed to Pfizer vaccinations, 40% to Moderna and 8% to J&J.
- 889 reports of Guillain-Barré syndrome, with 42% of cases attributed to Pfizer, 30% to Moderna and 28% to J&J.
- 2,290 reports of anaphylaxis where the reaction was life-threatening, required treatment or resulted in death.
- 1,724 reports of myocardial infarction.
- 14,102 reports of blood-clotting disorders in the U.S. Of those, 6,309 reports were attributed to Pfizer, 5,054 reports to Moderna and 2,701 reports to J&J.
- 4,229 cases of myocarditis and pericarditis with 2,590 cases attributed to Pfizer, 1,438 cases to Moderna and 186 cases to J&J.
- 11 cases of Creutzfeldt-Jakob disease with 5 cases attributed Pfizer, 5 cases to Moderna and 1 case to J&J.
- 264 cases of POTS with 162 cases attributed to Pfizer, 84 cases to Moderna and 17 cases to J&J.
FDA authorizes Pfizer and Moderna COVID vaccines for younger children
Moderna and Pfizer-BioNTech’s COVID-19 vaccines are now authorized for emergency use in infants and young children as young as 6 months, CNN reported.
The FDA on Friday authorized Moderna’s vaccine for use in children 6 months through 17 years and the Pfizer-BioNTech vaccine for children 6 months through 4 years.
The FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) on Wednesday unanimously voted 21-0 to recommend Pfizer and Moderna’s COVID-19 vaccines for infants and young children, stating the totality of the evidence available shows the benefits of the vaccines outweigh the risks of use.
The panel ignored pleas from experts, the vaccine-injured and a congressman representing 17 other lawmakers to halt authorization until questions about the safety and efficacy of COVID-19 vaccines for the nation’s youngest children could be properly addressed.
Pfizer’s three-dose vaccine would cover children 6 months to 5 years old, while Moderna’s two-dose vaccine covers children 6 months to 6 years old.
States have already ordered millions of doses made available prior to FDA authorization by the Biden administration.
White House officials said the administration of vaccines for these age groups could start as early as June 21.
CDC advisors hold impromptu meeting to get vaccines for kids rolled out by White House deadline
During a meeting Thursday, the CDC announced it scheduled a special two-day meeting of the Advisory Committee on Immunization Practices (ACIP) Friday to discuss authorization of Pfizer and Moderna’s COVID-19 vaccines for infants and young children.
The meeting to discuss authorization of Moderna’s COVID-19 vaccine for 6- to 17-year-olds is scheduled for June 22 and 23.
The CDC today discussed the safety, immunogenicity and efficacy of the Moderna shot in kids 6 months through 5 years of age and Pfizer’s vaccine in children 6 months through 4 years of age.
The ACIP is scheduled to vote Saturday.
“The entire process is set up to rubber-stamp the VRBPAC meetings from yesterday,” said Toby Rogers, Ph.D.
In a CHD.TV live blog, Dr. Liz Mumper, a pediatrician and Children’s Health Defense board member, said Pfizer showed an estimate of 80.3% vaccine efficacy but based it on only 7 cases in the placebo group and 3 in the vaccine group.
“These numbers are ridiculously small — the 80% may not stand” if more kids are included in the numbers, Mumper said.
Mumper also pointed out the shots being considered at today’s meeting were based on the original Wuhan strain that is no longer circulating.
“It is not so important how good a vaccine is at generating antibodies to Wuhan strain,” Mumper said. “[We] need long-term data about the impact of the shot on the number of kids who get COVID in [the] community and have severe or mild [cases].
Mumper said:
“U.S. VAERS data from Dec. 14, 2020, to June 3, 2022, for 6-month-olds to 5-year-olds show 1,658 adverse events, including 63 cases rated as serious and 3 reported deaths.
“The risk of a child dying if they have a diagnosis is 1,086/10,700,00 or 1086/10700000 = 0.00010149532. The risk of any child dying of COVID-19 over this time period is 1,086/73000000 = 0.00001487671.”
“Forty-nine states have already bought vaccines for children in the age groups being debated,” she added. “Seems like a done deal.”
FDA’s vaccine advisors endorse Moderna’s COVID vaccine for kids ages 6 to 17
The FDA’s vaccine advisory panel on Tuesday voted unanimously to recommend Moderna’s COVID-19 vaccine for children ages 6 to 17 after determining the benefits of the vaccine outweigh the risks for use.
VRBPAC voted 22 to 0 to recommend Moderna’s two-dose vaccine for 6- to 11-year-olds at half the strength of the adult version, and 22 to 0 in favor of authorizing the shot for 12- to 17-year-olds at the same strength as adults.
During the public comment session, individuals expressed concern over recommending a vaccine for an age group that has an almost zero risk of experiencing severe illness or death from COVID-19 and has already acquired a high level of natural immunity.
Dr. Tom Shimabukuro, a vaccine safety official at the CDC, said some data suggest a higher risk of myocarditis among people 18 to 39 years old after receiving Moderna’s COVID-19 vaccine, but findings were not consistent across various safety databases and were not statistically significant.
The CDC confirmed 635 cases of myocarditis, or heart inflammation, in the 5-to-17 age group out of almost 55 million doses of the Pfizer-BioNTech vaccine administered. The agency said the condition occurred most often in adolescent boys after receiving their second dose.
Florida only state not to preorder vaccines for young children
Florida is the only state in the nation that did not place an order with the federal government for doses of COVID-19 for young children prior to U.S. health agencies authorizing the vaccines, Politico reported.
The deadline for placing a pre-order was Tuesday and 49 other states met the cutoff date.
The Florida Department of Health (DOH), said in a statement to Politico on Wednesday that it did not pre-order vaccines for kids 5 and under because it doesn’t advise all children get vaccinated.
“States do not need to be involved in the convoluted vaccine distribution process, especially when the federal government has a track record of developing inconsistent and unsustainable COVID-19 policies,” the DOH statement said.
Jeremy Redfern, press secretary for Florida’s DOH, confirmed the department “chose not to participate” in the vaccination program.
“It is also no surprise we chose not to participate in distribution of the COVID-19 vaccine when the department does not recommend it for all children,” Redfern said. “Doctors can order vaccines if they are in need, and there are currently no orders in the department’s ordering system for the COVID-19 vaccine for this age group.”
Children’s Health Defense asks anyone who has experienced an adverse reaction, to any vaccine, to file a report following these three steps.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
State Dept. Not Investigating Saudi Use of US Weapons in Alleged War Crimes: GAO

Samizdat | June 16, 2022
The Government Accountability Office (GAO) published a scathing report Monday which found that the Department of Defense and the Department of State “have not fully determined the extent to which U.S. military support has contributed to civilian harm in Yemen.” The news comes on the heels of the announcement that US President Joe Biden will be paying a visit next month to Saudi Arabia, a country which in 2019 he pledged to turn into a “pariah.”
“Despite several reports that airstrikes and other attacks by Saudi Arabia and UAE have caused extensive civilian harm in Yemen, [the Department of Defense] has not reported and [the State Department] could not provide evidence that it investigated any incidents of potential unauthorized use of equipment transferred to Saudi Arabia or UAE,” the GAO report concluded.
In February 2021, US President Joe Biden declared he was ending “all American support for offensive operations” in the Saudi war on Yemen. GAO monitors pointed out that while US Military Training Mission staff claimed that “all of the equipment the US sells… to Saudi Arabia must be for defensive purposes,” the “officials could not provide a definition for equipment that is defensive in nature when asked how they distinguish between equipment used for defensive purposes and equipment used for offensive purposes.”
Instead, the report’s authors noted, State Department officials “told us they have no specific definitions for what constitutes ‘offensive weapons’ and ‘defensive weapons’ to direct the sale of weapons to Saudi Arabia.”
The report also found that from fiscal year 2015 to 2021, the “Department of Defense administered at least $54.6 billion of military support to Saudi Arabia and the United Arab Emirates, of which over a third, or $18.3 billion, came in the form of missiles. The remaining military aid was reportedly spent as follows: $7.6 billion on equipment maintenance, $6.2 billion on aircraft, $4.9 billion on “special activities,” $4.6 billion on communication, detection, and coherent radiation equipment, $3.3 billion on ships, $2.8 billion on training, $1.4 billion on construction, $1.2 billion on ammunition, $1.1 billion on support equipment, $900 million on weapons, and $1.8 billion on other expenditures like combat, tactical, and support vehicles, as well as research and development.
Although “the United Nations has characterized the conflict in Yemen as one of the world’s worst humanitarian crises,” the report’s authors explain that the US has “long-standing security relationships with Saudi Arabia and UAE—two primary actors in the conflict—and has continued to provide them military support, including for operations in Yemen since 2015.”
In April, 32 US Congress members urged Secretary of State Anthony Blinken to commit to a “recalibration of the US-Saudi partnership,” noting that the US’ “continued unqualified support for the Saudi monarchy, which systematically, ruthlessly represses its own citizens, targets critics all over the world, carries out a brutal war in Yemen, and bolsters authoritarian regimes throughout the Middle East and North Africa, runs counter to US national interests and damages the credibility of the United States to uphold our values.”
But with Biden’s announcement that he’ll be flying to Riyadh next month for what the Saudi embassy described as “official talks” between Joe Biden and Prince Mohammed bin Salman, the odds of such an adjustment taking place–and of US agencies taking a more proactive approach towards American involvement in alleged Saudi war crimes–are growing ever-slimmer.
Western media and politicians prefer to ignore the truth about civilians killed in Donetsk shelling

Remnants of the Uragan MLRS rocket which struck the Donetsk maternity hospital June 13. © Eva Bartlett / RT
By Eva Bartlett | Samizdat | June 16, 2022
Following intense Ukrainian shelling of Donetsk on June 13, some Western media sources, in tandem with outlets in Kiev, unsurprisingly claimed that the attack – which killed at least five civilians and struck a busy maternity hospital – was perpetrated by Russian forces.
Why Moscow would launch rockets at its own allies wasn’t explained, nor would it make much sense.
The Donetsk People’s Republic’s foreign ministry reported: “Such an unprecedented. in terms of power, density and duration of fire, raid on the DPR capital was not recorded during the entire period of the armed conflict [since 2014]. In two hours, almost 300 MLRS rockets and artillery shells were fired.”
The Ukrainian shelling began late morning, resumed in the afternoon, and continued for another two hours in the evening, a deafening series of blasts throughout the city, terrorizing residents and targeting apartment buildings, civilian infrastructure, the aforementioned hospital, and industrial buildings.
Locals say this was some of the heaviest bombing of Donetsk since 2014, when the eponymous region declared its independence from post-Maidan Kiev.
In the Budyonnovsky district in the south of the city, Ukrainian shelling of a market killed five civilians including one child. Just two months ago, Kiev’s forces hit another Donetsk market, leaving five civilians dead.
In the hard-hit Kievskiy district, to the north, the shelling caused fires at a water bottling plant and a warehouse for stationery, destroying it. The building was still in flames when journalist Roman Kosarev and I arrived about an hour after the attack. Apartment buildings in the area also came under firer, leaving doors and windows blown out and cars destroyed.
The destroyed gas station was on a street where I stayed in April, which is completely residential.
DPR head Denis Pushilin said, “The enemy literally crossed all the lines. Prohibited methods of warfare are being used, residential and central districts of Donetsk are being shelled, other cities and settlements of the DPR are also under fire now.”
Hypocritical silence after maternity hospital shelling
In a world where media reported honestly instead of manufacturing its own reality, there would be outrage over Ukraine’s attack on the Donetsk maternity hospital. But history shows that is not a world we live in.
As I wrote last year, Western media and talking heads also diligently avoided condemnation when terrorists attacked or destroyed Syrian hospitals, including the shelling of a maternity hospital in Aleppo, which killed three women.
At the damaged Donetsk hospital, I saw the gaping hole in the roof and remnants of the Uragan MLRS rocket which struck it. Most of the windows of both buildings were blown out.
Images shared on Twitter noted, “Both gynecology and intensive care have been bombed.” Other footage, taken by Donetsk war correspondent Dmitri Ashtrakhan, showed dozens of women, some heavily pregnant, taking shelter in the basement of the shelled maternity hospital.
Were these women and this hospital in Kiev, you can bet Western media would be loudly reporting it 24/7 for weeks. Instead, just as the West has steadfastly ignored Ukraine’s eight years of war on Donbass, they also omit reporting on the hospital.
Grotesquely, some Ukrainian and Western media instead disingenuously reported that it was a Russian attack, not Ukrainian, which terrorized, injured and killed civilians on June 13.
Just as Western media’s lack of reporting, or twisting of the narrative, on Ukraine’s shelling was to be expected, so too was the UN’s weak-worded condemnation, with the Spokesman for the Secretary-General, Antonio Guterres, calling it “extremely troubling.” You can bet that were the situation reversed and Russia responsible for bombing a Ukrainian maternity hospital, his words would have been far stronger.
In fact, they already have been: Three months ago, when Kiev accused Russia of an attack on a maternity hospital, in Mariupol.
Back then, the Guterres emphatically tweeted, “Today’s attack on a hospital in Mariupol, Ukraine, where maternity & children’s wards are located, is horrific. Civilians are paying the highest price for a war that has nothing to do with them. This senseless violence must stop. End the bloodshed now.”
A strong reaction to what later emerged to be a hoax claim, when the UN itself even admitted it could not verify the story. But a mild reaction to a documented reality in Donetsk.
The UN did, at least, rightly note the attack on the Donetsk maternity hospital was, “an obvious breach of the international humanitarian law.” So there’s that.
The thing is, Ukraine has violated international law for its eight years of waging war on the Donbass republics, using prohibited heavy weapons and targeting civilians and civilian infrastructure. This is only the latest incident.
Tears flow for hoax hospital bombing
In March, Western corporate-owned media supported Kiev’s claim that Russia had launched air strikes on a Mariupol maternity hospital, claiming three civilians had been killed. At the time, as reported, “The White House condemned the ‘barbaric’ use of force against innocent civilians, and UK Prime Minister Boris Johnson tweeted that ‘there are few things more depraved than targeting the vulnerable and defenceless’.”
As it turned out, witnesses reported there hadn’t been any air strike. There were explosions: just as terrorists bombed an Aleppo home in 2016 and used a mildly injured boy for their propaganda against Syria and Russia, so too did Ukrainian forces in Mariupol, setting the stage to incriminate Moscow.
Russia called the accusations “a completely staged provocation,” analyzing photos from the area and noting “evidence of two separate staged explosions near the hospital: An underground explosion and another of minor power, aimed at the hospital building,” and further noting that a “high-explosive aviation bomb would destroy the outer walls of the building.”
Russia also pointed out that the facility had stopped working when Ukraine’s neo-Nazi Azov Battalion expelled staff in late February and militarized the hospital, as Ukrainian forces did elsewhere in Donbass.
Marianna Vyshemirskaya, one of the women featured in the Western propaganda around the hospital, later spoke out and said there was no air strike, and that prior to the alleged event, Ukrainian soldiers expelled all the doctors and moved pregnant women to another building.
She also maintained that she and other women were filmed without warning by an Associated Press journalist dressed in a military uniform and wearing a helmet.
Even now, two days after Ukraine’s intense bombardment of Donetsk and targeting of the maternity hospital, when still more testimonies have emerged, Western media and politicians remain silent.
The suffering, and deaths, of the people of Donetsk doesn’t fit the Western narrative, so they misreport it or simply just don’t reference it at all, enabling Ukraine to continue to commit war crimes.
Eva Bartlett is a Canadian independent journalist. She has spent years on the ground covering conflict zones in the Middle East, especially in Syria and Palestine (where she lived for nearly four years).
Developmental Disorders in Babies born to Vaccinated Mothers?
Pfizer wants Babies to be Exposed to SIX Vaccine Shots!
By Igor Chudov | June 10, 2022
I will explain that
- Children of Covid vaccinated mothers were never tested for developmental disorders
- CDC recently revised and lowered developmental milestones, and removed some entirely
- Newly born babies will be exposed to SIX doses of mRNA vaccines if the FDA’ approves the Pfizer vaccine.
An interesting article came out:
This article found that at one year of age, babies born to mothers who had COVID (not vaccine), had a roughly twice-higher rate of neurodevelopmental disorders:
those born to the 222 mothers with a positive SARS-CoV-2 polymerase chain reaction test during pregnancy were more likely to receive a neurodevelopmental diagnosis in the first 12 months after delivery, even after accounting for preterm delivery.
Considering that COVID is a bad disease for a sizable minority of people, there is no surprise. Covid is bad and gives people all sorts of problems. Then I started thinking: a lot of adverse effects of Covid vaccines mimic the adverse effects of Covid. The younger is the vaccine recipient, the worse some effects of vaccination (such as myocarditis) are.
A great number of expectant mothers received up to three Covid vaccine shots during pregnancy. Did anyone bother testing one-year-old children of vaccinated and boosted (during pregnancy) women for neurodevelopmental disorders, before approving this vaccine for all pregnant women?
The question is, obviously, rhetorical, since “mRNA Babies” of triple-vaxed-during-pregnancy mothers are only beginning to get born right now and are at most a few months old. Not one such baby reached a year of age. So nobody tested them for developmental disorders at one year of age, before approving the three vaccine shots for expectant mothers.
The usual argument of vaccinators that “since Covid does it too, you should take the vaccine” does not hold water. To a woman who decided to take the vaccine, the probability of getting a vaccine is 100%. The probability of her getting Covid is much less. In the above study, out of 7,772 births, only 222 (2.8%) were exposed to Covid during pregnancy. So while vaccination is 100% guaranteed for those who elect to vaccinate, the chance of Covid is over 30 times less likely. And the “vaccine” does not prevent Covid anyway and does not even reduce the viral load.
There is literally zero data on one-year-old children of triple-vaccinated mothers because the oldest ones are 3-4 months old as of today.
However, there are disturbing developments regarding newborns. Vaccination does seem to have an effect on births and pregnancies.
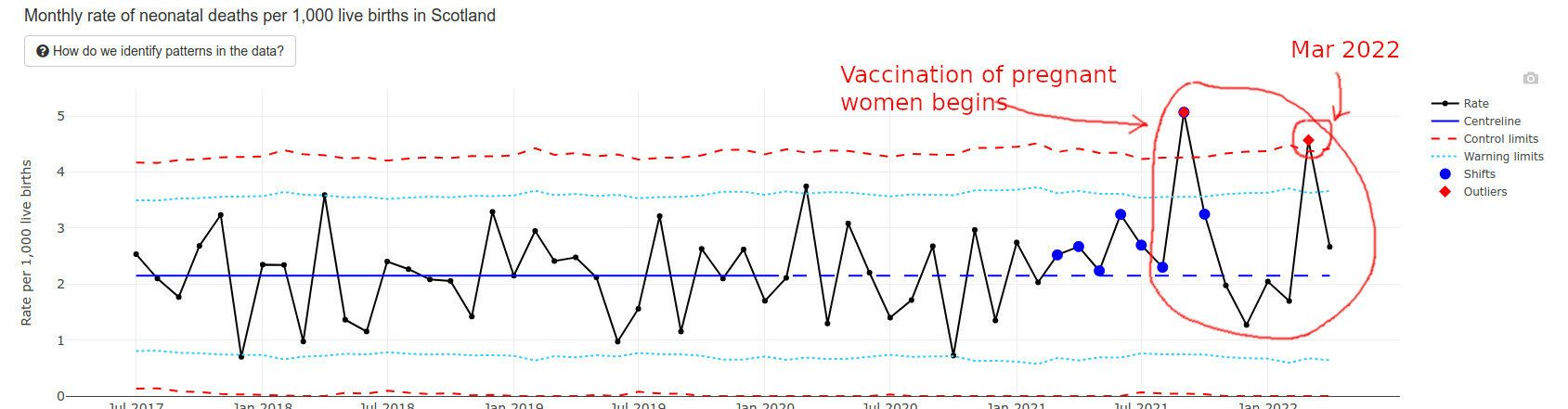
The best data I found regarding recently born newborns happens to come from Scotland. They have an interesting “wider impacts” page that I am quoting below.
Infant deaths are way above average and exceeded “Alert Limits” twice.
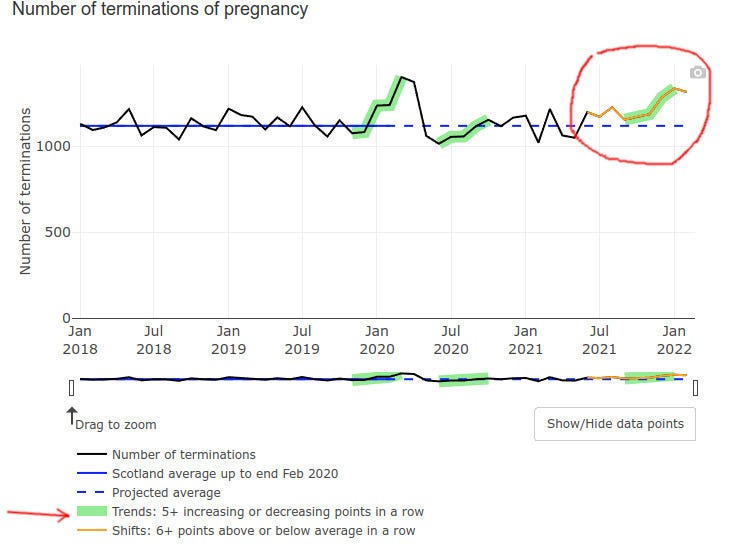
Even pregnancy terminations went up at the end of 2021, possibly but not certainly explained by prenatal vax problems:
Low Apgar score births (for those readers who do not have kids, Apgar score is how healthy is the baby at birth, the best being a score of 10) triggered a green alarm signal:
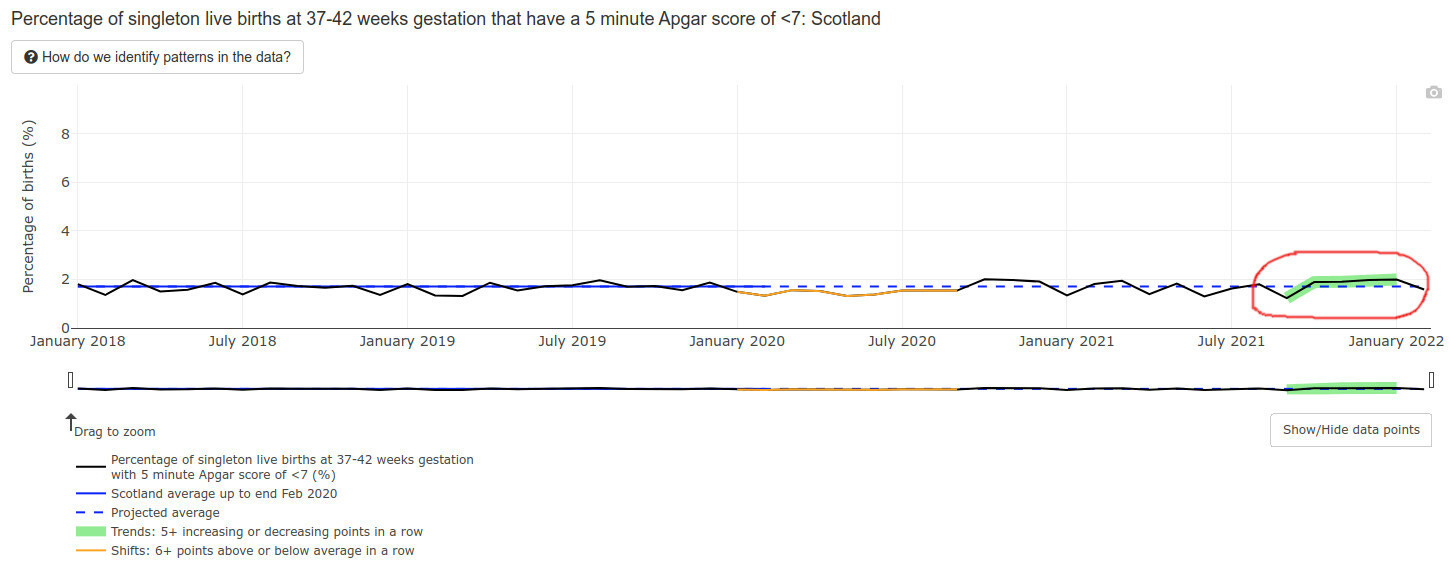
Mind you, an Apgar score is also a developmental evaluation of sorts — at 5 minutes after birth. What will happen to the developmental milestones of those lucky babies of vaccinated mothers, who survived the pregnancies, did not die postnatally, and lived to one year of age? I literally have no idea and nobody else in the world does — the time has not passed yet.
The data we have is NOT encouraging.
CDC Solution: Remove and Lower Milestones
The CDC possibly caught a whiff of this, because in February of 2022 they literally removed half the developmental milestones, bumped some others to higher ages, and lowered standards for yet more of them. (Hat tip @CLesterwood)
About one-third of milestones like fine motor skills have been bumped up to older ages. Because of the setback, children may worsen their developmental delay, making it harder to provide early intervention, explains Jessica Hatfield, MS, OTR/L, a pediatric occupational therapist for TheraTree Pediatric Therapy.
Removing crawling as a milestone??? Are you kidding us? For those of my readers who are parents, do you think that crawling is unimportant as a milestone?
Vaccinated Infants Exposed to SIX Doses of Covid Vaxx in a Year!
Imagine a vaccine enthusiast mother, who gets three doses during her pregnancy. Say, two doses during month 4 and one during the last week of pregnancy. The unborn baby is, obviously, exposed to all that.
Then the baby is born.
If the June 14-15 FDA meeting goes as planned, FDA will approve a three-dose Pfizer vaccine for infants and toddlers. So shortly after being exposed to THREE doses of mRNA vaccines prenatally, the recently born 6 months old baby will get THREE MORE Pfizer mRNA shots.
That’s a total of, drumroll, six spike protein, and nanoparticle exposures. For a tiny newborn, all during one first year of her life.
And what if the mom has several Covids while being pregnant and vaccinated?
They will ask the mom to vaccinate the baby regardless of those covid infections. This literally amounts to six doses within a year or close to, without even counting actual covids that the vaxed moms have. Pfizer will make $132 from these six shots. Not sure if the baby will eventually need much more expensive treatments.
Do you think that it is a little bit too much? Do you think Pfizer or the FDA care?
Injecting 6 mo. olds to 5yo’s? – NO!
Murder has no statute of limitations
By Coquin de Chien | June 13, 2022
The United States Government, at the behest of Pharma oligarchs and government employees who own stock in the Pharma companies, hopes to approve an amendment to the EUA (Emergency Use Authorization) to inject babies 6-months-old to toddlers 4-years-old with the C19 faux-vaccine.
Before the committee meets to recommend the amendment, the FDA allows people to comment on the FDA government web site. One such comment was provided to this author and is offered to you below. The United States of America is indeed facing a government #ClotShot plot.
This comment is NOTICE of possible criminal liability to Lauren K. Roth and members of the Vaccines and Related Biological Products Advisory Committee who owe duties of care, diligence, good faith, and loyalty in recommending “for” or “against” the EUA amendment for COVID-19 mRNA vaccine in children 6 months through 4 years of age.
Only two deaths are listed herein to establish knowledge. If the amendment is approved, it will have been done by committee members “knowing” of felony crimes in context.
Your investigation of these deaths should include death certificates, autopsy records, witness interviews, and immunization records.
Massachusetts Death Certificate 2022 SFN 5980 is a 7yo girl died January 18, 2022 listed as died from U071 “COVID-19”, B49 “unspecified mycosis”, J450 “predominantly allergic asthma”, and R091 “pleurisy”.
VAERS_ID 2038120 is a 7yo girl in Massachusetts, who received her 2nd dose 1/13/2022 and was reported to VAERS 1/15/2022. PRIOR_VAX states, “Severe nausea and vomiting from 5min post vaccination and for the next 8-10 hours.” SYMPTOM_TEXT states, “Spiked a 103 fever, severe stomachache, has not had a bowel movement since the day before vaccination, which makes today 3 days without one. First vaccine caused severe nausea and vomiting from 5minutes post injection and for the next 8-10 hours.”
This little girl suffered immeasurably 4 to 5 days as her intestines shut down due likely to impeded blood vessels servicing intestines.
Massachusetts Death Certificate 2021 SFN 56611 is a 48yo man died 11/16/2021 listed as died from U071 “COVID-19” and E669 “OBESITY”.
SFN 56611 is known to have died less than 24 hours after inoculation.
In both cases, the Medical Examiners listed the cause of death as “COVID-19”, when it was clearly not COVID-19. And in both cases, the Medical Examiners omitted listing causes Y590 “Viral vaccines“ and T881 “Other complications following immunization, not elsewhere classified”, when these clearly were proximate and actual causes.
Death certificates from the state of Massachusetts are sent to the CDC, a federal entity. Thus, fraud on a state death certificate is a federal crime as it affects federal death records. Several federal felony crimes apply in this instance and are listed below.
If you dismiss this NOTICE and recommend the EUA amendment without first investigating these two deaths, you become liable for inchoate crimes and the felony crime of “misprision of felony.” If a single person subsequently dies as a result of the amendment, all the elements will have been satisfied for you to face felony murder charges or involuntary manslaughter. Qualified immunity is not a valid defense.
18 USC § 4 – Misprision of felony
“Whoever, having knowledge of the actual commission of a felony …, conceals and does not as soon as possible make known the same to some … civil or military authority …, shall be fined under this title or imprisoned not more than three years, or both.”
Felony murder is a homicide that occurs during the commission of an inherently dangerous felony, showing a conscious disregard for human life. A jury decides whether recommending an injection, that you “know” caused death, and that you refused to investigate while “knowing” it caused death, is inherently dangerous.
Here are a few federal statutes likely violated by Medical Examiners in Massachusetts. You are duty-bound to call for investigation of:
- 18 USC § 4 Misprision of felony
- 18 USC § 286 Conspiracy to defraud the government with respect to claims
- 18 USC § 287 False fictitious or fraudulent claims
- 18 USC § 371 Conspiracy to commit offense or to defraud United States
- 18 USC § 1035 False statements relating to health care matters
- 18 USC § 1040 Fraud in connection with major disaster or emergency benefits
There were found sixty likely C19 vaccine deaths in a 25-minute perusal of the 2021 and 2022 death certificates, which extrapolates to hundreds, probably thousands of C19 vaccine deaths in Massachusetts.
Refusal to investigate these fraudulent records is a crime that, because of the felony murder aspect, has no statute of limitations. Five, ten, or twenty years from now, if a federal prosecutor were to learn of this NOTICE, he or she would have significant evidence to bring charges for felony murder.
In summary, this NOTICE places you in a position requiring you to investigate these deaths prior to recommending the amendment. If you dismiss this NOTICE, you may be criminally liable for involuntary manslaughter, felony murder, and a list of federal crimes and inchoate crimes.
Please make the appropriate decision for yourselves and for the children of the United States of America.
Comment Tracking Number
l4d-m52d-ge4m
They Attempt to Justify Approval for Use in Infants and Toddlers
They want the COVID-19 vaccine approval for children so bad, Peter Marks himself and his cronies published the very study he has to use to evaluate for approval.
By James Lyons-Weiler | Popular Rationalism | June 11, 2022
As promised, the FDA has ginned up a report that ostensibly will be used to try to justify “approval” (whatever they mean by that now) of COVID-19 vaccines for infants and toddlers (children < 5 years old). Here’s the report for your reference.
This report comes after a torrent of massive reports from Moderna and Pfizer that claim to review studies of the safety and efficacy of COVID-19 vaccines in children. It is not hard to see what shenanigans the FDA has been up to to try to bolster a vaccine that fewer and fewer adults want. It’s more of the same: exaggerate the apparent risk of the virus and minimizing the perception of risk. In other words, lies.
- There is no evidence of clinical urgency. Infants and toddlers (and children in general) do not get COVID-19; they do not (yet) die from COVID-19. All that can change when antibody dependent enhancement kicks in for the vaccinated. FDA’s own reports cites 1,086 deaths “from COVID-19” and 10,700,000 “cases” of COVID-19 in children aged 0-17. There have been 832 days since April 1, 2020 when diagnoses started for COVID-19. For the entire population of children in the US (73,000,000), the risk of COVID-19 infection since the onset of COVID is 10,700,000/73,000,000 = 0.14657. The risk of a child dying if they have a diagnosis is 1,086/10,700,00 or 1086/10700000 = 0.00010149532. The risk of any child dying of COVID-19 over this time period is 1,086/73000000 = 0.00001487671. The per-day risk is on the order of 1.78806611e-8 (0.000000001788). There is no real unmet clinical need and the FDA needs to go back to college to understand how to use RT-PCR correctly. Children do not get COVID-19, and they do not die.
- Inconsistent use of the idea “vaccinated”. This has been the pattern from the very first study. FDA, CDC, Moderna, Pfizer, and others pull out whatever definition of “vaccinated” they want. Examples: “Vaccinated” is defined in the original trials as people who received both doses and who did not develop COVID-19 before two weeks passed after the second exposure to the vaccine. In fact, that means that people who developed COVID-19 due to disease enhancement were dropped from the study calculations. First, this is the first time people were dropped from a vaccine trial for getting infected with the pathogen targeted by the vaccine up to 13 or 14 days after being vaccinated. Second, it’s actually five entire weeks – one month and one week – 44 days – after the first exposure. ALL of the vaccine efficacy being cited by FDA is suspect. Moderna’s and Pfizer’s vaccines never achieved >90% true vaccine efficacy; the best estimate is more like 75%.
- Inconsistent use of the idea “vaccine efficacy”. Over the time period since the first COVID-19 vaccine trials, various definitions of “vaccine efficacy” have been used. Decreased transmission. Reduction in infection rates. Reduced hospitalization. Presence of neutralizing antibodies. Presence of antibodies. All are used and cited in FDA’s report whenever convenient, all in an ad-hoc manner. It’s more than irritating. It’s moving the goal post and represents reckless (and ineffective) attempts to manipulate public perception. This practice continues in the reports and studies that are cited by FDA. I do not trust the efficacy data FDA cites in their report (why would we given Point 1?).Further evidence of the futility of the evidence used to claim efficacy comes from Moderna’s Sponsor Briefing report to the FDA:“3.3 Regulatory Considerations for Clinical Development of COVID-19 Vaccines in Children
Effectiveness
Regulatory precedent with other preventive vaccines provides a basis for inference of vaccine effectiveness in pediatric populations based on immunobridging to a young adult population in which clinical disease endpoint vaccine efficacy has been demonstrated for the same prototype vaccine. The immune marker(s) used for immunobridging do not need to be scientifically established to predict protection but should be clinically relevant to the disease. Based on available data in humans and animal models, FDA considers neutralizing antibody titers (a functional measure of the vaccine immune response against SARS-CoV-2) to be clinically relevant for immunobridging to infer effectiveness of COVID-19 vaccines in pediatric age groups. Because no specific neutralizing antibody titer has been established to predict protection against COVID-19, two immunogenicity endpoints (GMT and SRR) are considered appropriate for comparing the range of neutralizing antibody responses elicited by the vaccine in pediatric versus young adult populations.
Also embedded in this piece of work is the fact that FDA does not need evidence of long-term immunity; they are settling for something called “immunobridging” – guessing at the efficacy of a vaccine in one clinical population from measurements made from other clinical populaton.
They also are making people dependent on vaccines… expecting patients to have antibodies from one vaccine to the next. This makes no sense immunologically. We don’t need continuously high antibody levels against any pathogen. We have memory B-cells and T-cells. In accepting this paradigm, FDA is completely off its rocker and will cause immune exhaustion with constant vaccinations every 3-4 months.
- Incomplete consideration of the scientific data (Barnstable County, Israel, Ontario). We know that months after vaccination, those who are vaccinated are at higher risk of infection and now of hospitalizations. Data actually show negative vaccine efficacy in children (per Jeremy Hammond). See: “Evidence for Negative COVID-19 Vaccine Effectiveness in Children”. From that article:“vaccine effectiveness (VE) in children becomes(sic) negative within several months since receipt of the second dose.Researchers from the New York State Department of Health published a study on the preprint server medRxiv on February 28 noting that the evidence for vaccine effectiveness in children, particularly those aged five to eleven, was “limited”. So, they aimed to provide data to inform policymaking.“During Omicraon variant predominance,” the authors concluded, “VE against infection declined rapidly” for young children in the state of New York, “with low protection by one month following full-vaccination.”Comparing COVID-19 cases during January between unvaccinated and vaccinated children, they estimated initial vaccine effectiveness for children aged twelve to seventeen to be 76 percent, but this dropped to below 50 percent after just five weeks since receipt of the second dose.Moreover, for young children (aged five to eleven), they observed a drop from 65 percent to just 12 percent after only one month.Thereafter, their estimate indicated significantly negative effectiveness for this age group, as shown in Figure 2 of their paper: by 35 to 41 days, VE reached negative 10 percent, and by 42 to 48 days, it reached negative 41 percent.

Jeremy goes on to report (correctly) that the authors of the article misinterpreted their own data. History will remember Jeremy as a reporter with great integrity.
- Moderna and Pfizer reports fail to study long-term risks. Like I said, more of the same shenanigans. In this report, for example, Moderna offers data on myocarditis only up to Day 28 after the vaccine. Why Day 28? Why not “since the vaccine has been administered” to more accurately reflect the real-world clinical situation? They also state that myocarditis in a large concern in people infected with SARS-CoV-2 – but the comparison is to the uninfected, not the vaccinated, and we know that the spike protein is the cause (syncytia among heart muscles caused by the spike protein). The spike protein, of course, is the basis of their mRNA vaccines.
- Incestuous COIs/Unjustified Influence by Regulators. Peter Marks is charged with setting the decisions at FDA whether to consider vaccines for specific populations. Why the hell is he involved in a study conducted to bolster the vaccines he is going to have to decide upon? See “Benefit-risk assessment of COVID-19 vaccine, mRNA (Comirnaty) for age 16–29 years”. That “study” is also guilty of all of the same loose logic as above; it is noteworthy that the study assumes as “worst case scenario” of zero deaths from myocarditis following COVID-19 vaccination (Credit: Toby McDonald, who wrote this to me:“I’m reading the Moderna “Sponsor Briefing Document” and they built their benefit-risk assessment off of Funk et al. (2022). So I looked up Funk and it’s a recent paper by six staffers at the FDA including Peter Marks, Richard Forshee, and Hong Yang (who wrote the dreadful benefit-risk assessment for kids 5 to 11 back in October). Quite literally in their “worst-case scenario” they predict 0 deaths from myocarditis in the vaccine group. It’s a stunning work of fiction.”
- I’m on an email thread with Steve Kirsch (he considers me part of his “debate team”. Last week, Steve challenged Peter Marks to a debate:“Hi Peter,You are right about the vaccine uptake problem. According to independent survey we just commissioned, only 33% of Americans opted to go further than the first 2 doses.You were quoted in that CNN article:“We do have a problem with vaccine uptake that is very serious in the United States and anything we can do to get people more comfortable to be able to accept these potentially life-saving medical products is something that we feel we are compelled to do,” said Dr. Peter Marks, director of the Center for Biologics Evaluation and Research.Isn’t it time for you to end the misinformation problem by debating us in a public forum?My colleagues and I look forward to hearing from you.
The only way to end the misinformation is to debate the top misinformation spreaders. You will never win by trying to censor us.
We would be HAPPY to debate to you to end the misinformation problem. As you can see from this slide deck, all the evidence we’ve been able to find shows there was clinical trial fraud and that the vaccines are very dangerous. We would love to know how we got it wrong
I look forward to hearing from you.
-steve
To my knowledge, Marks has not replied. I replied to Steve and the entire email thread, including Marks, though:
“Steve,
History is going to remember one person on this email thread in a manner in which I would not ever care to be seen associating with.
I would therefore decline to participate in such a debate.
Sincerely,
James Lyons-Weiler, PhD

I could continue and debate dozens more points in the report dump by the FDA. I don’t have to. Marks himself provides evidence of being way off-target immunologically and lying about the “need” for COVID-19 vaccines for children.
Here’s an old video of Prevaricating Peter lying about the need for “high antibody titres” for immunity, and that children’s immune response is “not enough for some of these variants” (no data on that, just words):
The comments in that video have not aged well. Call your Senator and Congressional Reps and demand that Peter Marks resign. Email them this article. Marks and the FDA are NOT basing their considerations on independent fact, science and logic. He and his cronies are either incompetent or working for the industry. Either way, he and his cronies have to go.
Nursing reports from the front lines of the COVID vaccine crisis – A stark reality is finally creeping in
The massive propaganda campaign which led doctors to disassociate from the reality of widespread vaccine injuries is slowly weakening in impact
By Pierre Kory, MD, MPA | Medical Musings | June 13, 2022
I recently posted a deeply referenced compilation of evidence detailing the historic humanitarian catastrophe that has slowly unfolded within most advanced health economies across the world. Caused by a global mass vaccination campaign led by the Pharma masters of BMGF/WHO/CDC that illogically (but profitably) targeted a rapidly mutating coronavirus. They did it with what turned out to be the most toxic protein used therapeutically in the history of medicine. In vials mixed with lipid nano-particles, polyethylene glycol and who knows what else.
I cited studies and reports showing massive increases in cardiovascular deaths and neurologic (and other) disabilities amongst working age adults, beginning in 2021 only. A disturbing signal screaming from the original clinical trials data , VAERS data, life insurance data, disability data, reports of cardiac arrests of professional athletes, rises in ambulance calls for cardiac arrests in pre-heart attack age young people, and the massive increases in illnesses and data manipulations in Department of Defense databases.
As these events become more and more recognized by the average citizen (and occasional journalist), a new pathetic “Disinformation Campaign” was launched in response trying to blame all the young people dying as simply a need for increased awareness of the rare condition called Sudden Adult Death Syndrome (SADS), rather than examples of the legions dying from the vaccines. The fact checkers also came out in support of this narrative, branding anyone who thinks the vaccines are the cause of SADS as a conspiracy theorist. Like this self-appointed social media watchdog. Mentions of SADS are popping up from many countries… all in the last few weeks. Here, here, here, here and.. oh whatever. This article even listed a dozen such publicized deaths in the past few weeks from all over the world… but blamed them all on SADS. You get it. What is nauseating is the tone of purported good intention within these articles, informing folks that if you are related to someone young who died suddenly you should go see a cardiologist to make sure you don’t have an abnormal EKG. After it turns out normal, they will assuredly tell you to get vaccinated, an absurdity atop a mountain of absurdities caused by our bio-medical-media industrial complex over the past 2+ years.
Ugh, lets move on. In this post, I will move away from numbers and data and studies to give a more qualitative view of how the vaccines’ impacts are manifesting in the “belly of the beast,” (i.e. on the inside of a major academic medical center).
I want to first share a comment made in response to another recent post of mine, by my new partner in our COVID/Long Haul/Vax Injury specialty tele-health practice. Scott Marsland is both a COVID-expert and a Nurse Practitioner Extraordinaire (you should see the reviews he gets by his patients – they are over-the-top). Anyway, Scott wrote:
The most profound reflection of this last week came from a patient who is a physician and therapist. She was hospitalized recently for non-COVID reasons and observed: “I think many of the physicians are exhibiting dissociation. It takes an enormous amount of energy to maintain their narrative and hold off the reality hitting them in the face every day.” I thought of this reading the recent piece you referenced from The Annals of Emergency Medicine.
Wikipedia:“The major characteristic of all dissociative phenomena involves a detachment from reality, rather than a loss of reality as in psychosis. Research has suggested that dissociation is inversely related to mindfulness, which is a potential treatment.“
TY PK for this dose of mindfulness.
I thought his comment was the perfect introduction to this post, where I will share disturbing “insider info,” compiled largely from recent correspondences with a senior ICU and ER Nurse, both via email and phone. Although she is not working full-time in ICU’s or ER’s anymore, she still does shifts on occasion, particularly night shifts. Night shifts, although brutal, are WAY more fun and relaxed than day shifts. That is, most of the time, unless you get slammed due to less staff being around. Although the worst shifts of my career were night ones, thankfully they were rare.
What is great about night shifts is the camaraderie and closeness that develops among staff that choose to primarily work nights. The pool of such folks is small, and they choose night shifts for various but often similar reasons (preference, child care responsibilities, other jobs, hatred of day shifts etc). The general atmosphere is more “intimate,” as you end up having conversations, longer and deeper than you would or could in the middle of a hospital day. This is because at night there are no families around, no administrators, most patients are sleeping (sort of), no masses of swirling ancillary specialists like dietitians, physical therapists, occupational therapists, speech therapists, physician sub-specialists, transporters, social workers, food service workers, maintenance folks etc.
Anyway, this was the first email I received from her (editorial note: I wrote out or translated all her abbreviations but made no other edits to substance – I had to do it as her writing style clearly reflected someone who has been writing myriad nursing notes her whole career :).
On May 12, 2022, at 7:47 PM, L. <XXXX> wrote:
I wish I could have you as my doc. Nurse of 20 yrs + ICU – cardiac, neuroICU/ neurosurgical ICU mostly, and ED at Level 1. Vax injured from 2 Pfizer doses mandated by my major University hospital system. Clotting issues, open bleeding, spontaneous with no ability to stop, weeping down arms and legs. Severe leg clot post-surgery in March. Had to get D-Dimer ordered by force at little ED I was in, and use my own portable doppler I brought in from work, b/c they had no Ultrasound techs or equipment access – TPA (clot buster med) finally. Cervical lymph nodes enlarged since vax especially, for over 1.5 yrs. Cannot biopsy at least one as it sits on my Left carotid, now wrapped around it, . Got Covid originally while working ED in March 2020. “N antibody” still high as of Nov 2021. Hit neuro, never respiratory. Had same issues with H1N1 vaccine which was also mandated and then I got Guillain Barre Syndrome and neurological weakness – out of work 5 months. Will not get any boosters or vaccines this year, but have no exemption as all docs took to the “deer in headlight” look and said nothing. I will lose my career this winter if I refuse. Functional med/family practitioner – she has a long wait list and I have no idea how she sits with this data on vaccine injured. My VAERS report – it was deleted. Pharmacist never entered as required so I did. It has vanished. My batch numbers – significant for bad neurologic responses, clotting. I lost my Hematologist-Oncologist doctor to vaccine injury – he is out and never to practice again – in his early 40s. He was a “true believer” and in denial until it was him who was the injured patient. Our cancer hospital – know most of the case managers and many doctors since they were residents. They now have case loads in the 1000s rather than 250-400 over any given quarter. Not enough bed or infusion space for the cancer patients as outpatients. Radiation treatment backlog. All at a huge cancer hospital monstrosity itself. All kinds – brain, lymph, stomach, pancreas, blood, AND EYE CANCERS – orbital especially in younger people recently vaxxed. Microvascular ischemia on rise in vaxxed younger people. Strokes way up in no-risk, no co-morbidities, young to younger-ish. Ask me anything. I’ll tell you inside scoop from the floors and suites. This has to stop. They need to admit the fraud and crime and STOP. The liability must be lifted, mandates ended. They KNOW NOW and many KNEW THEN. Don’t know if you’ll even read this, but I follow all of you on substack and Twitter – those not banned yet! – and read ALL the data. I’ve been a lab rat myself from an issue from a car accident yrs back – I know the process. So much fraud. Keep going. Never give up. Never, never, never give up. Thank you for all you do, hope that you inspire and the confirmation of that little voice in me, that said NO way back, everything was off. I did not have an option or data then. I have data now, and it will keep coming. The option is NO.
Follow up:
Lost 4 practitioners to serious side effects of “strongly encouraged” boosters. 2 hospitalized, one in MICU. The irony is, for most staff, completely lost … All in early 30s to mid 40s. They had no need for boosters while BEING OUTSIDE ALL WEEKEND even if they truly believed in efficacy of them. All had Covid previous, N antibodies fully measurable. One female, one male, both inpatient. Female still nursing newborn.
On Fri, May 13, 2022 at 11:27 AM Pierre Kory <> wrote:
I am stunned by your email. Stunned. We know it’s bad, like real bad but this is the worst inside look I have heard yet. I am on the outside and don’t talk to most former colleagues so don’t have a feel. We should talk. Would you be interviewed on a VSRF (Kirsch’s organization) webinar? I assume not, but who knows, maybe anonymously like with altered voice and blurry screen? This needs to get out. Send me contact… and name? First name is fine… Thanks for this – Pierre
She wrote again before we talked, it was this email below that prompted me to ask her number so we could discuss in more depth:
It’s the inside folks who talk to each other, and you have to speak another language depending on who’s listening. That has been a skill set unto itself. It’s texting, the phone calls from area to area with back stories on patient issues. I was getting texts from my old stat team covering cardiac catheterization lab – the clots. The clots stunned everyone…it continues. My cardiac units – where I spent the bulk of my nursing years – lung and heart transplant included – have so many anomalies presented with patients that never existed before. Re-writing the script for each new problem never encountered. The constant codes (cardiac arrests). Can’t keep up.
Lost quite a few coworkers to either VAX injury itself – took them out of the work force, OR they resigned/accepted firing or retired once mandates were settled. It’s the phone calls I have with my cohorts in the other areas of the system. The real story is in those conversations. The doctors now admitting to injury is growing, but they can’t tell their patients why they are no longer practicing. Losing specialists is big problem not easily solved.
The signaling coming from management MD/PhD administrators has not been towards what winter will bring, but is focused on congratulating everyone on clinical excellence during the last 2 yrs. I think there is great trepidation in their approach because they see the data, they know the inside info on injury, disability/death of faculty and staff not from Covid itself, but the forced vax. We lost only a few to original Covid, with underlying co-morbidities that made outcomes a given in many cases.
I can’t come on a public show, but I can share info. My name is Linda (not her real name). In my current position, I read many charts and see in depth info – so much boosting and reboosting and not following other protocols – it’s a given now that the explosions in diagnosis of the cancers and cardiac issues especially come from these decisions. In some cases, the first thing you see on a chart is huge letters stating VAXXED alongside the pt’s diagnosis, treatments thus far, which is usually at odds with normal disease course, age and projected outcome, etc. They’re pushing the vax status, in bright letters, to the top of the list so it can be considered – not for every patient, but the “challenging cases” … That may be for research purposes.
I will explain the above – what Linda is saying is that practitioners are starting to call out the patient’s vaccination status more clearly on the first screen of the medical record in those cases where they know or suspect the vaccine is related to the patients’s new “mysterious” or “complex” problem. Let’s be clear though, the doctor’s don’t necessarily or explicitly include vaccines as a possible cause in their reasoning/impression/plan section of the patient note. But it seems the nurses and junior docs are now calling it out in some small/large way. Disassociation breaking, ever so slowly?
It makes me just stop, and by end of the week, take into account cases of say, ocular orbital cancer in 20-somethings. Have had 6 in last 2 weeks with no Family History or other indicators. Out of the blue, some with brain mets now. All vaxxed unwillingly, all had Covid and recovered fine prior to employer forced vax. The employers, the areas the patients reside in….nothing in common other than the previous. The actuaries are correct. Excess mortality, let along whatever-life-left disability. Stunning numbers.
I ended up talking to Linda.. about lots of things. She is clearly a fellow spirit, highly experienced in ICU and Emergency medicine, and she told me even more disturbing developments, like the fact that on some night shifts, nurse teams are seeing more cardiac arrests in a single shift than ever before and in unprecedented younger age patients. On some shifts, they have had so many that the “crash carts” are rolled straight from one arrest to another because Pharmacy, especially on night shifts, are not able to re-stock fast enough. This situation has happened maybe once in my whole career… when two arrests happened on the same floor or unit within a short time period.
She also told me that night nurses are more openly discussing the vaccine as the cause of what they are seeing (much more than during day shifts apparently). However, they do this largely in text, and they use “code”. Their code word for a vaccination injury or cause is “that issue,” i.e. in reference to a 22 year old who suddenly arrested on the hospital ward, “he is having that issue.” Note these are nurses.. not the docs.. but some of the docs are talking to her, like the one above who performed 6 enucleations (eyeball removals) this year already in young people (very rare to have to do this, especially in this age group). She also told me about how her interventional cardiologist nurse friends related that some patients are coming in with massive heart attacks, and during the angiogram the interventional cardiologists are seeing such extensive thrombi filling the entire artery (as documented by some embalmers), that they say “I can’t stent or remove this, this guy needs surgery, like now.”
In that conversation with Linda, I was also finally able to confirm a fraud that I had suspected was occurring within U.S hospitals regarding the accuracy (or willful inaccuracy) of the vaccination status listed in the medical record of a patient newly admitted to the hospital. It has long been my strong belief that this fraud drove the U.S data used to support some of the last remaining false narratives (i.e narratives #6 and $7 below) . Note these ever-shifting narratives were all directed at combatting vaccine hesitancy, which as some of you may know, was the primary military objective of the vaccinators.
![]()
BMGF/WHO/NIH et al. had clearly identified vaccine hesitancy as the main enemy in the battle plans they drew up and distributed after their viral pandemic simulation exercises over the past decade. In this prominent medical journal publication on addressing viral pandemics, they state “the World Health Organization has listed vaccine hesitancy among the greatest threats to global health, calling for research to identify the factors associated with this phenomenon.” Vaccine hesitancy is why the HHS gave $1 Billion to U.S media to support a relentlessly positive public relations campaign supporting the uptake of vaccines.
Now let’s get back to this fraud. First, note that during all of 2021, (well, up until late November when I was let go from my last pandemic ICU job on a completely fabricated accusation), I had only taken care of one ICU patient that was officially documented in their medical record as “fully vaccinated.” I knew that it could simply not be true that only one patient that I took care of the entire year was fully vaccinated. I knew this was false based on data from countries that more transparently (mistakenly?) reported vaccination status and hospital outcomes. In multiple reports starting in February 2021, the majority of hospitalizations and deaths (even when adjusted to rates per 100,000) had long been the vaccinated.
One of the more ridiculous attempts to cover this fraud up in the U.S was a media narrative launched in June/July of 2021, created from statements by Fauci and Wollensky, that 99% of patients in hospital and dying were the unvaccinated. They literally did this with a straight face, knowing that they were including in their numerator all the deaths that occurred prior to the start of the vaccination campaign. Yup, if you died in 2020, you were reported as dying in an unvaccinated status. Not subtle. But that was not the only lie. We must never forget the famous slip by the NY times.. when they suddenly and surprisingly called out the CDC for “withholding large amounts of COVID data” throughout the pandemic. Umm.. their actual job is to collect and disseminate data. Not subtle. Even crazier is that at the time of that narrative launch, during a lecture, a CDC slide deck mistakenly showed a slide which revealed that 26% of patients in U.S hospitals were vaccinated. But this number was falsely and fraudulently lower than the actual number. By a long shot.
Here is how I think they falsely suppressed the real rate of vaccinated patients entering U.S hospitals and dying:
In the most popular electronic medical record system in the U.S (EPIC), on the sidebar of every page in the chart are the name, demographics, room number, provider team, and COVID vaccination status of the patient. What I found weird from the outset was that, in EPIC, there were only two categories under the COVID-19 vaccine status section, “Vaccinated” or “Unknown.” There was no “Unvaccinated” status. Also realize that “Unknown” was interpreted by all providers and official data as akin to being “Unvaccinated”. Everyone I took care of in the ICU in 2021, except one, had an “Unknown” vaccination status. How could that be? How come only one ICU patient of mine in the entire year was reported as being “fully vaccinated?” Even if the vaccines worked really well (which I knew they didn’t), something was off, like really off.
There was only one hypothesis I could come up with to reconcile these observations. I suspected that during the admission process to the hospital, there must have been some sort of barrier to deeming someone “vaccinated.” I hypothesized that in order to be documented as vaccinated on admission, you had to have received the vaccine from a primary care physician’s clinic who worked for that same hospital system in a system office, and that they had already documented in the electronic medical record. If you got a vaccine from anywhere else outside that hospital system’s clinic, you were assigned an “Unknown”, i.e. “Unvaccinated” status in the electronic medical record.
And lo and behold, Linda confirmed this was the case in one major health system she worked at. What I found most striking is that she worked in two different hospital systems, in one (the smaller one) it was very easy to document a patient in the record as vaccinated. The admitting nurse could accept any documentation, from a Walgreen’s card to even a verbal report from the patient or family and they could put it in the record on admission and the patient would show up as “vaccinated” on the main screen sidebar.
In the other, larger, major (and I mean major) health system she worked in, if the patient received the vaccine from anywhere but an employed provider’s clinic within the health system (even if the patient had a vaccine card on them), she was forced to put it in an “open field” buried on page 2 of the initial nursing assessment not where nobody, and certainly no physician looked for it. All these patients were automatically documented on the main screen as “Unknown”, i.e “Unvaccinated”, even if the dates of each shot were entered into that nursing note field.
This process is what led the vast majority of U.S doctors to become convinced that the only people dying in hospitals were the unvaccinated. Which made perfect sense, I mean, the vaccinators did not want anyone to know the vaccines were not preventing hospital or death, so it would be helpful to their mission if they could make everyone think that all hospital patients were unvaccinated. This way, all the health care workers would get vaccinated out of fear of dying and would also aggressively insist that all their patients and family members get vaccinated. Which is what happened. It is also why a large percentage of the population (at least the ones I meet at lectures, conferences, and symposia) no longer want to see a “system doctor” or go to a “system hospital,” no matter how grand their brand/reputation once was. Fun fact: a long-time donor of large annual gifts to the Mayo clinic.. decided to direct their donation to the FLCCC this year because they felt the Mayo Clinic had departed from their founding principles and mission. Go FLCCC.
The system docs behaved this way because they saw with their own eyes, “the (false) reality” of what would happen if you were unvaccinated. This, combined with the medical journal propaganda publishing only favorable and selective analyses of vaccine efficacy and safety drove nearly all the nation’s doctors to go completely mad.
Their fervor to vaccinate everyone and everything, even in patients who just recovered from COVID, was something to behold. I saw overt hectoring, harassment and even rage. Twitter was one of the most terrifying places to watch doctors arrogantly propagate the need to be vaccinated.. even for folks who had (often hard-earned) natural immunity. I almost feel bad for some of those docs as history will not judge them kindly. Forgive them for they know not what they do. They were literally screaming across Social Media, Media, and Medical Journal editorials, that you will be OK if you just get vaccinated. The high profile docs were the worst, except I have little sympathy for them as some/many/most were likely complicit in the deception rather than just fooled like the rest. Folks like Eric Topol, Peter Hotez, Alastair McAlpine, Tom Friedan (who I used to deeply admire as NYC Health Department Commissioner), Eric Feigl-Ding-(bat), Jeremy Faust (probably the biggest ignoramus on Twitter, having taken an early lead in that competition since the pandemic broke in 2020), and Monica Gandhi. Leana Wen deserves particular ire as she is the most active prostitute for the Pharma-captured federal health agencies on mass media. A media darling as it were.
Then you started to see doctor walk-outs protesting the unvaccinated, increasing numbers of doctors publicly stating they would start refusing to see unvaccinated patients, heck, the Pharma controlled outlet called Medscape even got an ethicist to argue that it was OK to refuse to treat the unvaccinated. Yup. Crazy town. Clown World. One of my patients who is a hospital pharmacist even told me that at her hospital, the hospitalists were vaccinating patients admitted for COVID..as they were being discharged from the hospital. That’s right, as the patients were being discharged after having recovered from COVID, they were recommending and administering vaccines for the same illness. I even heard of one case where a team of clinicians decided to vaccinate a severely ill COVID patient in the ICU.
I also witnessed aggressive attacks in one of the nation’s largest medical-centers staff physician email forum. Doctors “screaming” that everything would be fine if everyone just got the damn vaccine. Deriding anyone bringing forth arguments about untested safety, suspicious efficacy data, and concerns about mandates violating patient autonomy and medical ethics. Anyone who brought forth “adverse data” towards the vaccines were treated with dismissal and a retaliatory posting of selectively favorable data with the imprimatur of the Pharma captured agencies and Pharma captured journals. I will never forget this time in the history of medicine. Ever.
Some other “insights” into the medical system I haver come across, from another ER nurse:
I have no research to offer but first hand experience from working as an RN
in an ER.Ringing in ears and hallucinations have followed vaccinations in 3 of my
patients. Family members at a loss. I mention the vaccine but most don’t
even hear it…The gentleman with the ringing in the ears (just had his 4th booster the day
before) I suggested he didn’t get any more boosters as ringing in the ears
is an adverse reaction to the vaccine. His wife looked at me and yelled
“his doctor told him he won’t survive the anti-virals for COViD” I was
speechless. The patient continued on and told me about his experience with
the vaccines 1st shot-he had a seizure, doctor recommended 2nd shot. After
2nd shot he was very sick, doctor recommended 3rd shot and he was
hospitalized 4th shot ringing in ears, abdominal bloating and months away
from dialysis. Wife added that she also had seizure after first vaccine and
she had that attitude that it was no big deal.I have said this before, it’s criminal what is happening. I have cried on
my way home from shifts, I tell whoever will listen. The information I have
collected over the last 7 months (time of vaccine/booster in relation to
chief complaint) is jaw dropping.I took a break from working for the summer but continue to keep in touch
with the nurses…My friend told me about an 80yr old man, 4 strokes in the last year and
they all line up with his 4 shots but the doctors response is “he’s 80,
he’s going to have strokes”Has anyone come across research in regards to GI bleeds and low hgb? I have
a lot of this patients, GI bleeds out of the blue… and they are young!I had 28yr old black obese young woman… new diagnosis of enlarged heart
and CHF. Vaccine was roughly 1 month prior to ER admit and I suggested no
more vaccines for COViD and her response was “my doctor told me this
happened because I got the vaccine and a tattoo on the same day”60ish lady…….just got over COViD (after have 3 COViD vaccines) and she told
me she was going in for second booster next week!!!!!!Kids are having random seizures and are put on anti-seizure medication for
2 years…when I ask parents what caused the seizure, the neurologist has no
idea. All these children vaccinated for COViD-100%. NO ONE CONNECTS THE
DOTS.The screenshot below is of 3 days I worked and I’m in the ER for 12 hours
and don’t see all admits. I’m also super busy so it’s hard to check status
of all admit patients… of course this is very limited information but a lot
of the patients have some issue 2-3 months post vaccine/booster.
I’m still shocked we don’t have a “vaccine team” monitoring all the
patients as they come into the ER but no one cares. Not the ER medical
director, not the doctors, not the COViD response team…..no one. Nurses see
it and they are talking but many are fearful of getting fired.Thank you for all that you are doing! Although I can’t read all the emails,
I am just happy to know that there are others out there that are in the
same boat as I am.I’m disgusted with the AMA and AAP. I don’t trust a thing they say. I don’t
trust them with my four children as they have not protected our children
over the past 2 years.Thank you!
And another:
May 26 05:28PM -0400
Katie (not her real name),
Thank you for sharing your story! This is what I live every day and I tell my husband how hard it is to see so much damage. I have had more patients diagnosed with aggressive cancers than I have seen in the last two decades.
… I’ve been so especially concerned about the clotting effects with Total joints treated with Tranexamic Acid. I’ve been keeping track of my patients (that I would consider) have had mild/moderate vax injury. i.e. – reactivation of latent viruses, (oral herpes (not just one or two lesions, but their whole mouth broke out – something that had never happened before) shingles – affecting their eyes, that took more treatment than normal) – Histoplasmosis; *blood clots/Cardiac problems – Stroke from new onset Atrial fib in a patient on blood thinners within 12 hr post injection, Atrial fibrillation in a healthy, athletic 34 yr old male, new onset hypertension without prior history; * Persistent cough, months of diarrhea, migraine, neuropathy of upper extremity to the extent she could not write/type – all extensively checked out without cause. But, all within a few days/weeks/couple months of injection. All my practitioners are still advocating the Vax!!! What do you think we should do??? I’ve got to get the guts to gently visit with our Chief of Staff. CRNA, Colorado
Last one, from a colleague:
Just had dinner with my friend, a colleague friend of his here, Dr XXX renowned YY Physician . PRO Vaccine. Was adamant all physicians should get the vaccine and should not be able to practice without it. Was a trailblazer for the vaccine here. He got boosted around Christmas time, had a stroke less than a week after, lost his eyesight in one eye, lost his practice, cannot be a doctor any longer, and said undoubtedly it was from the Pfizer vaccine and encouraged all of his doctor friends to max out their disability insurance to protect themselves. I know not surprising to you, but this guy was so pro vaccine and clearly admits his stroke and his loss of eyesight from the vaccine!!
And then there is this doozy – another nurse sent me a case history below of an elderly woman whose blood thinner was highly “supra-therapeutic” (i.e. very thin blood at risk of major bleeding), yet she had a massive stroke caused by a blood clot. This simply does not happen.
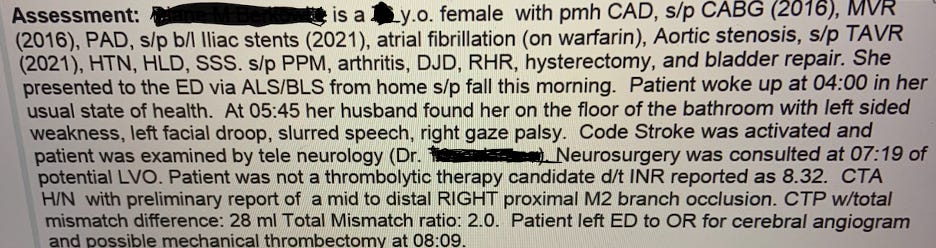
El Fin.
Featured Video

Pediatrician shares 30 yrs of insight on vaccinating vs. not vaccinating children
or go to
Aletho News Archives – Video-Images
Book Excerpt
Biden’s Closed Circle on Russia
An excerpt from ‘The Great Betrayal’
By James W. Carden | The Realist Review | June 14, 2026
Joe Biden’s presidency may ultimately come to be seen as a cautionary tale. Here was a president who showed little interest in entertaining arguments that might have contradicted his most deeply held assumptions.[1] And there were precious few within the upper ranks of the administration who might have attempted to do so, after all, only policy hands and political operatives who had come up through the ranks of the Clinton and Obama administrations or had longstanding ties to the citadels of the foreign policy community were invited into the fold. … continue
Blog Roll
 Aletho News
Aletho News- Terms of Iran-US MoU revealed: Bloomberg
- A California Pediatrician Shares 30 Years of Insight on Vaccinating vs. Not Vaccinating Children
- What Is Defensive Medicine?
- CDC Awards Pfizer $1.24 Billion for COVID Vaccines for Kids and Adults
- Historic blow to South Korea’s military intelligence agency
- Russian frigate fires warning shots in English Channel
- Radio Free Europe, the Cold War ‘Weapon’ Congress Still Funds
- UN: Israel continues to violate Lebanon airspace in defiance of Iran-US MoU
- Araghchi: Israeli occupation of Lebanese land a violation of MoU
- Hezbollah fighters confront intruding Israeli forces in southern Lebanon
- If Americans Knew
- Pro-Israel Donors Power Last-Minute Surge of Espaillat Spending
- “They Stole Our Home and Our Life”: Israel Permanently Displaces Syrians in Quneitra
- Massie Recognizes USS Liberty Attack. Here’s Why That Matters
- The blatant racism and cruelty that define Israel’s settler movement
- Israeli army ‘murdered child’ in Gaza and then dumped body on a roadside
- The Forward’s Hit Piece on Thomas Massie and USS Liberty Veterans
- Israel’s former defense minister compares settler ideology to Nazism
- The Pro-Israel Lobby’s Quiet Cash Shuffle
- Trinity Broadcasting Network (TBN) Propagandizes for Israel’s Wars
- A grim milestone: Gaza’s death toll surpasses 73,000 – Daily Update
- No Tricks Zone
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
