Indisputable – Covid ‘cures’ caused the excess deaths

By Serena Wylde | TCW Defending Freedom | July 21, 2023
‘Virologists have been exploiting us and screaming fire where there was none’: Dr Denis Rancourt giving his testimony to the National Citizens’ Inquiry in Ottawa, Canada.
This citizen-led, citizen-funded inquiry into Canada’s Covid-19 response, by definition cannot be commissioned or conducted impartially by the government whose responses and actions are the subject of the investigation. It has already held hearings in Vancouver, Ottawa and Quebec City at which scientific, medical, and legal experts have testified under oath, along with journalists and Canadian citizens who have pertinent testimony to offer. On May 17 Dr Rancourt, a scientist with a PhD in physics who has held key research positions in France and the Netherlands prior to becoming a physics professor and lead scientist at the University of Ottawa 23 years ago, gave his evidence.
For the last three years, with a team of statisticians and scientific researchers, he has been conducting a vast number of studies on all-cause mortality. These have focused on North America but have included other Western nations, resulting in more than 30 scientific reports. His findings appear conclusive, and establish that there was no particularly virulent pathogen on the planet in 2020; that excess deaths that year were entirely caused by the measures imposed against a fictitious threat, and then from 2021 onwards, by the vaccines.
He further concludes that none of the various ‘pandemics’ announced by the US and Canada since the Second World War was reflected in excess all-cause mortality. In other words, they too were fiction.
Importantly, at the inquiry hearings Dr Rancourt explained his focus on all-cause mortality data. It is because it contains no bias. It is a simple counting of deaths per age group, by sex, state, city and as a function of time. It enables one to spot and correlate events such as heatwaves, earthquakes, wars, economic depressions; anything that perturbs the population sufficiently to cause mortality. Its ‘power’ is that it provides a clear, unmanipulated picture of a given population.
During a 97-minute testimony he provided detailed evidence to show how he arrived at three core conclusions:
1. ‘If governments had done nothing out of the ordinary, if they had not announced a pandemic, not responded to a presumed new pathogen, done nothing more than what is usually done when there is high seasonal mortality in the winter, there would have been no excess mortality. There was the usual ecology of pathogens which we live with and are always present. People get ill, they recover, some die, but there was no pandemic that caused excess mortality beyond the historic trend, and that would have remained the case if we had just left things alone.’
2. The measures that governments applied were many different forms of assault, all of which contributed to excess mortality.
3. The Covid-19 vaccination campaign has caused huge excess mortality in clearly visible peaks which are seen directly associated with the roll-out of various vaccine doses to different age groups and in different jurisdictions, and likewise with the administration of boosters. The excess mortality occurs immediately following vaccination and lasts a few days, then the curve of mortality declines exponentially over a period of about two months. Dr Rancourt emphasises that it is not possible to have such an unusual pattern without it being causally connected to the injections.
Explaining why there was no pandemic of a viral respiratory disease, Rancourt shows that when one integrates the all-cause mortality in the ‘Covid’ period there were huge variations from area to area, which defies the hypothesis of viral spread.
The US excess mortality in this period was five times higher than that of neighbouring Canada proportionately to its population, which is epidemiologically impossible. These differences were also visible between US states, which means one has to look at social factors to explain the phenomenon. The excess deaths occurred mainly in the Southern states, which have a high incidence of seasonal bacterial pneumonia, and these infections went inadequately treated because during the ‘Covid’ period all Western nations cut antibiotic prescriptions by at least 50 per cent. Another strong population correlation factor was the number of people with disabilities. The US has a large number of registered disabled, and people who rely on outside support for everyday needs cannot function in a society in lockdown. It also has high numbers of poor people, and with the closure of churches, schools and community facilities, these populations were utterly stripped of their usual mechanisms of survival.
Excess mortality in 2020 in Europe was equally inconsistent with the notion of viral spread. Immediately after the pandemic was announced Lombardy in Italy became a hotspot, where hospitals put two people at a time on mechanical ventilators. But Italy’s crisis did not flow into Switzerland, nor did Spain’s high death toll cross the border into Portugal, and Alsace’s peak in Eastern France did not affect neighbouring Germany. This constitutes counter-evidence of a viral respiratory disease. Furthermore, although the lethality of ‘Covid’ was said to be exponential with age, mortality data shows no correlation with age.
Dr Mike Yeadon, who understands the biological effects of fear, told James Delingpole in their recent discussion: ‘Two mg of diazepam, a cup of tea and a biscuit, arm around the shoulder and give them an oxygen mask. I think most people would have gone home, but instead they admitted and murdered them.’
As the fraud began with the seeding of an idea of a pandemic, solid, irrefutable data is key in dismantling the illusion. This Dr Rancourt provided.
He completed his testimony with a plea to scientists and physicians to go back and look at the data of who is dying, and where and when, and what it correlates to. He believes there has to be a reset of thinking to recognise that virologists have been exploiting us and shouting fire where there was really nothing present. Clinicians and emergency staff have donned ‘Covid glasses’, he believes, making them see things as dangerous which at any other time would appear perfectly normal.
He postulates that the way to reset thinking is to use hard data that cannot be disputed, and that is all-cause mortality data. Unless this central data issue is addressed, he fears pandemics will be declared without basis, and populations will be assaulted at will.
NATO adopts new anti-Russia defense plan
RT | July 13, 2023
NATO passed a new defense plan at the Vilnius summit on Tuesday. The whopping 4,400-page document details the defense of critical locations in case of “an emergency” and lists a potential attack by Russia as one of the biggest threats, according to German media. The bloc’s secretary general, Jens Stoltenberg has welcomed what he called “the most comprehensive defense plans since the end of the Cold War.”
The document addresses two “main threats – Russia and terrorism,” and accuses the former of being “the greatest and most immediate threat to the security of allies and to peace and stability in the Euro-Atlantic region,” according to Germany’s Bild tabloid.
German Chancellor Olaf Scholz also called on his country and the other NATO members to “arm ourselves against a threat to our territory,” Bild added. The new plan also lists the military capabilities the bloc’s members must demonstrate, including new member Finland and applicant, Sweden.
The document reportedly claims a “violent” and “revisionist” Russia could potentially attack NATO territory. “We recognized that we could indeed be faced with an Article 5 situation again, in which part of NATO territory is under direct attack,” a military bloc official told German news agency, dpa.
To counter the supposed ‘Russian threat,’ the bloc plans to massively increase its Response Force (NRF) from the current 40,000 troops to over 300,000, comprising land, sea and air units, as well as rapidly deployed Special Forces.
The bloc also plans to significantly increase weapons production and stockpiling. The new strategy includes a “new Defense Production Action Plan to accelerate joint procurement, boost production capacity, and enhance Allies’ interoperability,” the NATO statement said.
According to Bild, the bloc would seek to build up armored “heavy forces,” and deploy more long-range artillery systems and missiles, as well as air defense systems.
NATO also plans to enhance what it calls ‘deterrence measures’ by sending additional forces to the Baltics and Eastern Europe. Battlegroups comprising 1,000 soldiers are to support the national armies of the Baltic States and Poland, Bild reported, citing the document.
The UK will be responsible for Estonia, Canada for Latvia, Germany for Lithuania, and the US for Poland, the German media outlet said. Berlin also plans to station a brigade of 4,000 soldiers in Lithuania, according to the German media.
Germany is also reportedly expected to serve as the NATO logistics hub in case of a major conflict. The bloc is also considering establishing a second Land Command, in addition to the existing station in Türkiye’s Izmir. Wiesbaden in Germany is being considered as a potential location since it already hosts a large US base, Bild reported.
Russia repeatedly stated that it considers NATO’s buildup on its borders as well as the bloc’s expansion to the east a threat to its national security. It also named preventing Ukraine from joining the bloc among the main reasons for launching its military operation in the neighboring country in February 2022.
Iran takes Canada to court for violating sovereign immunity
The Cradle | June 29, 2023
Iran has filed a legal case against Canada at the International Court of Justice (ICJ) under the pretext of violating Iran’s sovereign state immunity by designating the country as a “sponsor of terror.”
The Hague-based court confirmed in a statement that Iran launched the case against Canada on 26 June.
A statement on the official website of the Iranian government said that Canada presented these accusations under “false and wrongful” pretenses.
In the press release by the ICJ, Iran contends that “Canada has adopted and implemented a series of legislative, executive, and judicial measures against Iran and its property [since 2012] in breach of its international obligations.”
Iran argues that “as a sovereign state, it is entitled to sovereign immunities from jurisdiction and from enforcement under customary international law” and requests the Court to adjudge and declare that “by failing to respect the immunities of Iran and its property, Canada has violated its international obligations towards Iran.”
In 2021, a Canadian court awarded 107 million Canadian dollars ($84m) to the families of six victims who were killed when Iranian forces shot down a Ukraine International Airlines flight near Tehran in January 2020, which was labeled an “act of terrorism” by Ontario judge Edward Belobaba.
Iranian officials have said the shooting of the plane was an accident caused by “human error” in operating a surface-to-air defense system due to being on “high alert” following retaliatory strikes on US bases for the killing of Top Iranian General Qassem Soleimani.
In May of 2021, the spokesman for the Iranian Foreign Ministry Saeed Khatibzadeh described the application of Canadian judicial procedures as a “quite political approach,” saying: “the Canadian court, following the US courts, first identifies the accused, then resorts to any relevant or irrelevant information in public sources, especially cyberspace, to find a reason for its biased and predetermined mentality.”
Canada listed Iran as a “sponsor of terror” in 2012 and broke diplomatic ties as relations frayed over Tehran’s support for Bashar al-Assad’s regime in Syria, its nuclear program, and its stance on Israel.
On 13 March, 2012, Canada amended section 6 of the State Immunity Act (SIA) to remove the immunity from the jurisdiction of a foreign State listed by Canada as a supporter of terrorism, the application for the legal case states.
Following the amendment, section 6.1 of the SIA provides that “a foreign state that is set out on the list referred to in subsection (2) is not immune from the jurisdiction of a court in proceedings against it for its support of terrorism on or after January 1, 1985.”
The ICJ was set up after World War II to resolve disputes between UN member states. Its judgments are final but can take years.
15 Signs That You Might Be In An Abusive Relationship…
… With Your Government
The Naked Emperor | June 28, 2023
The Workplace Mental Health Institute delivers mental health training and consultancy to medium and large-sized organizations across the world. On their website they have various resources that you can download and put in your office, to help boost productivity, by addressing mental health issues.
One of their infographic downloads provides 15 signs that your might be in an abusive relationship. You may be in an abusive relationship if they [your partner]:
- Stop you seeing friends and family;
- Won’t let you go out without permission;
- Tell you what to wear;
- Monitor your phone or emails;
- Control the finances, or won’t let you work;
- Control what you read, watch and say;
- Monitor everything you do;
- Punish you for breaking the rules, but the rules keep changing!
- Tell you it is for your own good, and that they know better;
- Don’t allow you to question it;
- Tell you you’re crazy and no one agrees with you;
- Call you names or shame you for being stupid or selfish;
- Gaslight you, challenge your memory of events, make you doubt yourself;
- Dismiss your opinions;
- Play the victim. If things go wrong, it’s all your fault.
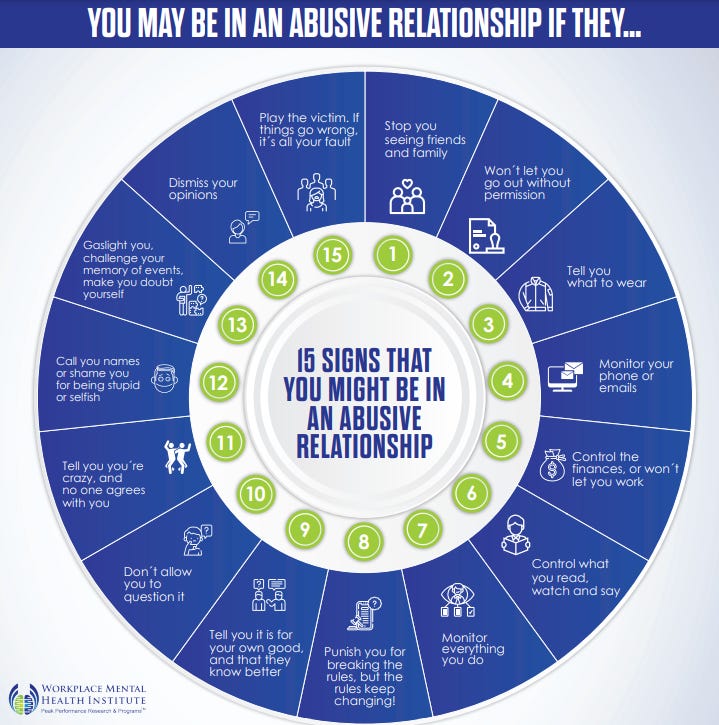
Now go back through that list and see which ones your government has subjected you to over the past three years. For most western countries it is every single one.
Your government has been mentally abusing you for years, in an almost identical fashion as an abusive partner would.
DeSantis Says Would Resume Keystone XL Pipeline if Elected US President in 2024
Sputnik – 26.06.2023
WASHINGTON – Florida Governor and 2024 Republican presidential hopeful Ron DeSantis said on Monday that he would resume work on the Keystone XL oil pipeline between the United States and Canada, in addition to permitting other pipeline projects, if he is elected to be the next US president.
“Hundred percent, yeah. It’s a no-brainer,” DeSantis said during remarks in Texas, when asked whether he plans to restart work on the project.
DeSantis pointed out that pipelines are the safest way to transport energy and pointed to the latest derailment of a train with tanker cars over the weekend in the US state of Montana.
DeSantis also said he plans to permit “a lot of pipelines,” noting that such a move would also be good for national security.
The Keystone pipeline system transports oil from Western Canada to refineries in the United States. The system currently has three phases of the project operational, but with the fourth, Keystone XL, was suspended by the Biden administration.
Keystone XL would run through the state of Montana, where US oil would be added to the system. President Joe Biden rescinded a construction permit for the pipeline granted by former President Donald Trump in 2019.
Last year, the Biden administration said it had no plans to restart the Keystone XL project even amid concerns about rising gas prices and volatility in the energy market.
Was SARS-CoV-2 entirely novel or particularly deadly?
BY THOMAS VERDUYN, DR TODD KENYON, DR JONATHAN ENGLER | PANDA | JUNE 22, 2023
As part of our inquiry into the drivers of excess deaths, we take a step back and address the central theme of the Covid-era narrative: that SARS-CoV-2 is a novel virus that is so deadly that drastic measures were needed to contain it.
In the previous articles of this mini series about excess deaths we looked at how effective the Covid shots were at arresting Covid [1, 2] and also how bad the “first wave” in New York city was.[3] There are good reasons behind why we chose to address these two topics first. One reason is that an honest look at these issues helps establish a balanced understanding of what might be driving excess deaths since 2020. Another reason is that both topics were central to the official narrative emanating from government sources and the mainstream media. We were told that the whole point of the lockdowns was to delay the spread of SARS-CoV-2 until a vaccine could be developed that would spare us from overwhelmed hospitals like what happened in places like New York and Italy.
As has been shown, and to put it mildly, the Covid shots did not perform nearly as well as promised. Sadly, the burden of the adverse events caused by the experimental shots turned out to be worse than the disease.[4] Furthermore, by a close examination of excess deaths in New York city in early 2020, and in particular by a comparison to what happened on the Diamond Princess, it was concluded that the tragedy in New York was not compatible with the spread of a virus such as SARS-CoV-2, let alone any other generally mild respiratory virus.
All of this presses us to take a step back and address the central theme of the Covid-era narrative, namely the idea that SARS-CoV-2 is a novel virus that is particularly deadly; so deadly that drastic measures were needed to contain it. We begin with a look at the idea that the virus is novel.
1. How novel is SARS-CoV-2?
In the field of virology, the term “novel virus” typically means that the virus was recently discovered. This definition, of course, tells us nothing at all about when the virus first existed. Thus, for instance, the first human-coronavirus was found in 1961.[5] It was labeled B814 and identified as a cause of the common cold. This does not mean that this particular cold-causing coronavirus suddenly appeared in that year. No, and much to the rather, it only means someone finally found it. The ability to isolate, identify and sequence RNA viruses is a relatively new science. The patent on the process used in PCR machines was first granted in 1987.[6] It was in 2003, only 20 years ago, that the first human reference genome was sequenced. Despite all the efforts by many scientists, mankind has not yet sequenced every virus on planet earth. It is quite possible we never will. As a result, we are hardly in a position to assert when a particular virus (or strain of a virus) first appeared. Even if sequencing of a virus could prove beyond reasonable doubt that it was made in a laboratory, unless we had lab records to prove when it was made, it would still be nearly impossible to determine when it first infected someone. At best we might be able to estimate a timeframe by using antibody tests applied to stored specimens. The fact that SARS-CoV-2 is a relatively mild virus with symptoms similar to that caused by the flu only compounds the challenge. All we know for certain about this virus is that labs first began testing for it in early 2020.
The real problem with all of this is that during the Covid era the term “novel virus” was used by many outlets (including universities, journals, the media, and government officials) to mean something quite different from “recently discovered.”[7] For example, the GoodRx website has an article in which the authors say that “SARS-CoV-2, the virus that causes COVID-19, is a “novel coronavirus.” This means it’s different from all viruses like it.” They go on to say that “In medicine, novel refers to a virus or bacteria that wasn’t known to affect humans. This means that the bug is either brand new or was only found in animals or other life forms.” [8] Likewise, Dr. Tam, the chief medical officer of Canada, recently wrote, “In March 2020, Canada was faced with a… virulent pathogen… for which there was no natural immunity… and no effective antivirals.” So we see that the official narrative was not only that SARS-CoV-2 was recently discovered, but that it did not exist before late December 2019, was different from other viruses, was newly capable of infecting humans, was entirely new to our immune system, and was outside the scope of what doctors knew how to treat.
Are any of these claims true? Other than the fact that it was recently identified, the other claims are either false or dubious at best. It is useful to examine each claim on its own. We begin with a brief investigation into the possibility that SARS-CoV-2 existed before December 2019. Actually, there is growing evidence that SARS-CoV-2 was around long before it suddenly acquired international attention. For instance, by searching through the public sequencing data archives, a group of researchers found that soil samples collected in Antarctica between Dec 2018 and Jan 2019 contained “sequence fragments matching the SARS-CoV-2 reference genome…” [9] This was so contrary to the official narrative that the authors later suggested that it had to be on account of laboratory contamination issues. But their findings were not unique. For example, by examining human blood samples taken in Italy before the Covid era, researchers found that already by September of 2019 some individuals (none of whom were sick at the time) had SARS-CoV-2 specific antibodies in their blood.[10 11] Other studies have found similarly.[12] Therefore, there is good evidence that the virus existed long before it garnered any attention.
Second, was SARS-CoV-2 that different from other viruses? The very fact that the virus was named “SARS-CoV-2” informs us that virologists think it is similar enough to SARS that it didn’t even warrant an entirely new name. Indeed, the two viruses are said to share “79.5% sequence identity.” [13] Despite the 20.5% difference, and notwithstanding the 17 year time lapse, studies have shown that people that were infected with SARS “possess long-lasting memory T cells… that displayed robust cross-reactivity to the N-protein of SARS-CoV-2.”[14] Therefore, although possessing differences, it cannot be said that this virus is that different from other coronaviruses.
Third, was this virus newly capable of infecting humans? To answer this question, it may help to consider RaTG13, a bat coronavirus that is said to be the closest to our virus. The two viruses are reported to be 96% similar.[15] Although it is commonly assumed that bat coronaviruses cannot infect humans without either a modification to its RNA or via an intermediate host, it is possible that bat coronaviruses jump to humans all the time, only without making us sick. For instance, a study done in 2018 found good evidence to conclude that bat coronaviruses are capable of infecting humans regularly, noting also that the “infections were subclinical or caused only mild symptoms.” [16] Conversely, experiments with blood samples of health care workers known to have had Covid demonstrated efficient neutralization of RaTG13.[15] Of particular significance in this regard is the little known fact that the PCR test for Covid, as designed by Drosten, was initially verified by making sure it detected coronaviruses from “bats in Europe and Asia.”[17] In other words, a positive PCR test may have indicated nothing more or less than the presence of a harmless bat coronavirus already endemic among humans. Although the Drosten test was later superseded by other tests, the official narrative emerged rapidly out of case detection using the Drosten test. Unfortunately, it is not clear to what extent this influenced early test results. In any case, it is certainly not novel that a virus of this sort could infect humans.
Fourth, is this virus entirely new to our immune system? Certainly not, for it was known from early on in the Covid-era that a significant percentage of people were immune to this supposedly novel virus. We previously observed that only 19% (712 of 3711) of the people on board the Diamond Princess cruise ship tested positive for the virus, and of these only a smaller fraction yet actually became ill.[4] Similarly, a group of researchers from Singapore “detected SARS-CoV-2 specific T cells in individuals with no history of SARS [or] Covid-19.” Remarkably, they also detected T cells in people that had no known contact with anyone that had had either SARS or Covid.[14] Likewise, a study in the UK found that many health care workers repeatedly tested negative despite repeated exposure to Covid.[18] The authors of that study concluded that “some individuals may clear subclinical infection before seroconversion.” Why did so many people never get Covid? Multiple researchers have concluded that it was likely a result of memory T-cells from a previous infection with a common cold or flu.[19, 20, 21, 22]
What percentage of people had sufficient prior immunity to prevent illness? Those same researchers found it was about 50%. For instance, a study by Grifoni et al “detected SARS-CoV-2-reactive CD4+ T cells in ~ 40% – 60% of unexposed individuals, suggesting cross-reactive T cell recognition between circulating ‘common cold’ coronaviruses and SARS-CoV-2.” [23] In other words, about half the population was destined to never become noticeably ill from Covid for the simple reason that they recently had a cold. Nor is this particularly surprising since it was known that the original SARS virus had also cross-reacted with other coronaviruses.[24] Thus, the virus was not entirely novel to our immune system.
Fifth, was this virus new to doctors? As may be gathered from the fact that Covid was around long before March 2020, it is almost certain that before doctors were told that they were dealing with a novel virus that they supposedly did not know how to treat, they must have unknowingly treated Covid as if it was any normal respiratory or influenza-like-illness. To the best of our knowledge, there is no record of doctors reporting an unusual increase in untreatable respiratory disease, at least not until the WHO officially declared Covid a pandemic. Even after doctors were advised it was an entirely new disease, treatment protocols were rapidly developed in multiple places.[25, 26, 27]
In summary, SARS-CoV-2 was “novel” only in the sense that it was first discovered in early 2020. It is certain that it existed globally for at least six months before this. Already by January 2020 about half the world’s population was immune to this virus. Nor was Covid outside the parameters of known treatments available for respiratory diseases. These facts should have been front and center in the media, and should have had a strong influence on government policies. Sadly, all this information was buried.
Of course, if Covid was not novel, it is impossible that it should have caused any excess deaths in 2020. It follows from this sobering conclusion that any and all excess deaths had to have been caused by other factors.
2. How deadly was Covid?
As was just pointed out, at least half of the population was essentially immune to Covid. For these people Covid was a non-issue. What about the other half? How lethal was it for them? Central to a proper answer of this question is the fact that our immune system is confronted with novel proteins all the time. Our survival does not depend on us having seen them or anything similar before. Rather, the immune system learns from all foreign material, remembers the experience, and serves to make future encounters less noteworthy. If at some point in the future a virus should arise that was both novel to our immune system and untreatable, even this would not necessarily mean that the virus was something to fear; certainly not to the extent of causing a cataclysm like we have recently witnessed.
In a previous article of this series [1] we made mention of a World Health Organization bulletin that estimated the Infection Fatality Rate (IFR) of Covid to be 0.23%.[28] That same bulletin also advised it might be substantially less than this. As data accumulated, the IFR was indeed found to be lower, eventually converging on a global average of about 0.15%.[29] For people under 70 years old, the average IFR of Covid drops down to 0.07%.[30] Of course these estimates were determined using information from death certificates and PCR test results, which (as shall be explained below) may have introduced significant inflationary errors into the results. The IFR of Covid may therefore be much less than 0.15%.
Moreover, it is well established that severe Covid illness is generally linked to those with underlying medical conditions, meaning it is rare in healthy individuals. For instance, a study looking at more than half a million people hospitalized in the USA with Covid found that 94.9% “had at least 1 underlying medical condition.” [31]
Nevertheless, for the sake of argument let us accept these estimates at face value and proceed to ask how Covid compares with the flu? The IFR of influenza is generally considered to be about 0.1%, and in a typical season about 8% of Americans get sick from the flu.[32] As for Covid, despite the unprecedented numbers of people that were tested for this virus, the total number of Covid cases in the USA during 2020 totaled 19.2 million,[33] or about 5.7% of the population. Thus, by all metrics it would appear that Covid in 2020 was on par with or less than a normal flu season.
The fact that Covid is not a particularly lethal disease was known since early 2020. For instance, the UK government officially declared that “as of 19 March 2020, Covid-19 is no longer considered to be an HCID in the UK.” [34] The acronym HCID stands for “high consequence infectious diseases.” Therefore, for the vast majority of people, the wonderful and immensely complicated human immune system was more than adequate to fight off a Covid infection.
If in fact Covid was only as bad as a normal flu season, why did it garner so much attention? And why have government dashboards suggested that Covid is causing millions of excess deaths in the world? The answer to the first of these two questions will have to be postponed for a future article. As for the second question, it is helpful to look a little closer at excess deaths in 2020. A recent study by Levitt et al analyzed all-cause mortality rates in 33 countries from 2009 to 2021. They found that during this 13 year window, the year 2020 was the worst year with the highest mortality for only four countries: “UK, Italy, Spain and Belgium.” [35] Another 10 countries had “the highest mortality in 2021.” (USA and Poland were the worst). As for the remaining 19 countries, either 2009 or 2010 had the highest mortality.
Was there anything particularly special about 2009 that made it the worst year for more than half these countries? Actually, it was found to be the worst for two simple reasons: mortality rates have in general been decreasing over time, and 2009 is as far back as the study went. Of interest is that in 2009 the WHO declared a pandemic on account of the H1N1 virus. Nothing special came of it, however, for “the total number of influenza-related deaths worldwide… proved similar to the number in a relatively mild year of seasonal influenza.” [36]
The fact that 2020 was the worst year for only 4 of these 33 countries lends support to our conclusion that Covid was about as bad as a normal flu season. The fact that 2021 was the worst year for 10 countries helps reinforce our previous findings that the Covid shots did very little to prevent Covid deaths and instead caused a great deal of deaths from adverse events.
3. Covid Data Issues
How is it possible that a mortality analysis seems to contradict reports about millions of Covid cases and deaths? There are several good reasons for this apparent discrepancy. For starters, and as was mentioned in a previous article,[1] on April 20, 2020 the WHO mandated changes to the way death certificates were to be filled out. The document stated that “a death due to Covid-19 is defined for surveillance purposes as a death resulting from a clinically compatible illness.” [37] In other words, since influenza typically has identical symptoms to Covid, flu deaths were to be labeled as Covid deaths. While this may be useful for “surveillance purposes,” it does not help us determine if Covid caused any excess deaths. Nor is it useful for making accurate comparisons between Covid and the flu. And it most definitely makes it difficult to calculate the IFR of Covid.
The WHO document went on to say: “A death due to Covid-19 may not be attributed to another disease (e.g. cancer)… Always apply these instructions whether they can be considered medically correct or not.” Therefore, even if cancer was the actual cause of death, if the person so much as tested positive for Covid, the death certificate was to say that Covid was the cause of death. The end result of this change in policy is that the number of deaths caused by Covid has been significantly over-counted in most countries.[38, 39, 40, 41] What was not affected by the protocol change was how many people died from all causes. This is why all-cause mortality studies are so relevant during the Covid-era.
Another issue muddying the waters is the PCR test used to identify a Covid case. Despite the fact that the PCR test is based on remarkable technology, it has various shortcomings when used as it was to establish a Covid case. Very briefly, a few such issues are:
- If the cycle threshold is too high, it will return a high number of false positives.[42]
- As disease prevalence decreases, the risk of false positives increases.[43, 44]
- The number and type of primers used for identifying the presence of SARS-CoV-2 has the potential to pick up fragments originating from some other source.[45, 46] (As we saw above, harmless bat coronaviruses may give a false positive.)
- The PCR test is capable of finding virus fragments,or intact virus in the airway, but is not capable of determining if a person is actually infected with Covid. Since clinical symptoms were not required to be present, many uninfected individuals falsely tested positive. [47, 48]
Every issue listed above has the tendency to inflate Covid deaths.
4. Covid in Canada
To put things into perspective, and to tie all these ideas together, it is appropriate to consider one particular country in more detail as an example. Let us consider Canada. Statistics Canada records that 16,151 deaths in 2020 were attributed to Covid.[49] This is slightly more than twice the number of deaths attributed to “Influenza and Pneumonia” in an average year in Canada (7304 deaths/yr). How is it possible that Covid was more than twice as deadly as the flu if the two illnesses are about the same?
The answer is either that the number of Covid deaths was overcounted due to all the issues just mentioned or that influenza deaths were underdiagnosed in the past. Unfortunately, it is now nearly impossible to determine the exact error rate. Nevertheless, by considering only the last of the issues in the above list, it is possible to demonstrate how significant the inflation factor really is.
Dr. Bullard, head of the provincial laboratory in Winnipeg Manitoba, testified that PCR tests do not verify infection and were never intended to be used to diagnose respiratory illness.[50] He went on to say that about 56% of positives in Canada belonged to people that were not infected with Covid. If we accept this percentage, in all likelihood at least 56% of the deaths attributed to Covid in Canada were a result of a false positive. Applying this error rate to Covid deaths in Canada in 2020 brings the number of deaths down to 7,106. It is duly noted that this number is slightly lower than the yearly average for influenza deaths in the preceding four years. If we use this adjusted amount, and plot mortality in Canada in 2020 by the top 15 leading causes of death, we can see the relative significance of Covid in Canada.

Figure 1. Source: Statistics Canada. Table 13-10-0392-01
Covid mortality was adjusted down by 56% to account for false positives.
In Figure 1 above, cancer and heart issues dwarf all other causes of death. The number of deaths attributed to flu and pneumonia is several thousand below average. This resulted from the fact that, according to the WHO mandate, many deaths that would normally have been classified as influenza were labeled as Covid because the two are clinically compatible illnesses. Also, Canadian labs changed the way they tested for the flu: “changes in laboratory testing practices as a result of the public health response to… Covid-19… may affect the comparability of data to previous… seasons.” [51] What is clear from this chart is that Covid was not particularly lethal, was no worse than a normal flu season, and certainly unworthy of the unprecedented attention it received.
Conclusion
In conclusion, it is safe to say that SARS-CoV-2 was “novel” in early 2020 solely because of the simple fact that that is when it was first detected. Not only was Covid treatable, but at least 50% of people had sufficient immunity from a previous common cold to prevent noticeable illness. It can also be said that Covid was not unusually lethal, since the mortality burden was only as bad as a normal flu season. Covid mortality (when adjusted for only one of several factors) ranked ninth among the leading causes of death in Canada, the same rank normally held by influenza and pneumonia.
Of course, it could be argued that the reason Covid deaths were this low is because government mandated lockdowns and other non-pharmaceutical interventions prevented a Covid catastrophe. It is this important topic that we plan to cover in our next article of this series.
References
- Kenyon, Todd et al, “It is impossible that the vaccines saved 14 million lives in 2021,” Panda, 2023, https://pandata.org/drivers-of-excess-deaths-part1/
- Verduyn et al, “How many lives were actually saved by the Covid-19 vaccines?” Panda, 2023, https://pandata.org/how-many-lives-were-actually-saved-by-the-covid-19-vaccines/
- Kenyon, Todd et al, “What the Diamond Princess tells us about NYC in spring 2020,” Panda, 2023, https://pandata.org/what-the-diamond-princess-tells-us-about-nyc-in-spring-2020/
- Verduyn, Thomas et al, “Did side effects from the Covid shots cause an excess mortality?” Panda, 2023, https://pandata.org/did-side-effects-from-the-covid-shots-cause-any-excess-mortality/
- Akronson, Jeffrey, “Covid-19: First coronavirus was described in The BMJ in 1965,” BMJ 2020;369:m1547
- Mulley, Kary, US Patent, 1987, http://patentimages.storage.googleapis.com/cc/f0/3e/dc51b1fb4af2e6/US4683202.pdf
- Morris, Dylan, “Novelty Means Severity: The Key To the Pandemic,” Insight, 2021, https://www.theinsight.org/p/novelty-means-severity-the-key-to
- Billingsley, Alyssa, Pinto-Garcia, Patricia, “The Novel Coronavirus: What Are Novel Viruses, and How Do They Impact Public Health?” GoodRx Health, 2023, https://www.goodrx.com/conditions/covid-19/what-does-novel-coronavirus-mean-science-medical-definition
- István Csabai, Krisztián Papp, Dávid Visontai et al. “Unique SARS-CoV-2 variant found in public sequence data of Antarctic soil samples collected in 2018-2019,” 23 December 2021, PREPRINT (Version 1) available at Research Square https://doi.org/10.21203/rs.3.rs-1177047/v1
- Apolone G, Montomoli E, Manenti A, et al. “Unexpected detection of SARS-CoV-2 antibodies in the prepandemic period in Italy.” Tumori Journal. 2021;107(5):446-451. doi:10.1177/0300891620974755
- Antonella Amendola, et al, “Molecular evidence for SARS-CoV-2 in samples collected from patients with morbilliform eruptions since late 2019 in Lombardy, northern Italy,” Environmental Research, Volume 215, Part 1, 2022, 113979,ISSN 0013-9351, https://www.sciencedirect.com/science/article/pii/S0013935122013068
- Jones, Will, “The Evidence COVID-19 Was Spreading Silently Around the World in Late 2019,” 2022, The Daily Sceptic, The Evidence COVID-19 Was Spreading Silently Around the World in Late 2019 – The Daily Sceptic
- Rossi GA, Sacco O, Mancino E, Cristiani L, Midulla F. “Differences and similarities between SARS-CoV and SARS-CoV-2: spike receptor-binding domain recognition and host cell infection with support of cellular serine proteases.” Infection. 2020 Oct;48(5):665-669. doi: 10.1007/s15010-020-01486-5. Epub 2020 Jul 31. PMID: 32737833; PMCID: PMC7393809
- Le Bert, N., Tan, A.T., Kunasegaran, K. et al. “SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls.” Nature 584, 457–462 (2020). https://doi.org/10.1038/s41586-020-2550-z
- Cantoni, D., Mayora-Neto, M., Thakur, N. et al. “Pseudotyped Bat Coronavirus RaTG13 is efficiently neutralised by convalescent sera from SARS-CoV-2 infected patients.” Commun Biol 5, 409 (2022). https://doi.org/10.1038/s42003-022-03325-9
- Wang, N., Li, SY., Yang, XL. et al. “Serological Evidence of Bat SARS-Related Coronavirus Infection in Humans, China.” Virol. Sin. 33, 104–107 (2018). https://doi.org/10.1007/s12250-018-0012-7
- Corman, Victor M et al, “Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR,” Eurosurveillance, 25, 2000045 (2020), https://doi.org/10.2807/1560-7917.ES.2020.25.3.2000045
- Swadling, L., Diniz, M.O., Schmidt, N.M. et al. “Pre-existing polymerase-specific T cells expand in abortive seronegative SARS-CoV-2.” Nature 601, 110–117 (2022). https://doi.org/10.1038/s41586-021-04186-8
- Jose Mateus et al., “Selective and cross-reactive SARS-CoV-2 T cell epitopes in unexposed humans.” Science, 370,89-94(2020). DOI:10.1126/science.abd3871
- Lipsitch, M., Grad, Y.H., Sette, A. et al. “Cross-reactive memory T cells and herd immunity to SARS-CoV-2.” Nat Rev Immunol 20, 709–713 (2020). https://doi.org/10.1038/s41577-020-00460-4
- Humbert, Marion et al, “Functional SARS-CoV-2 cross-reactive CD4+ T cells established in early childhood decline with age,” PNAS, 2023, https://doi.org/10.1073/pnas.2220320120
- Mahajan, S., Kode, V., Bhojak, K. et al. “Immunodominant T-cell epitopes from the SARS-CoV-2 spike antigen reveal robust pre-existing T-cell immunity in unexposed individuals.” Sci Rep 11, 13164 (2021). https://doi.org/10.1038/s41598-021-92521-4
- Grifoni, Alba et al, “Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals,” Cell, 2020, DOI:https://doi.org/10.1016/j.cell.2020.05.015
- Patrick, David et al, “An Outbreak of Human Coronavirus OC43 Infection and Serological Cross-Reactivity with SARS Coronavirus,” Canadian Journal of Infectious Diseases and Medical Microbiology, 2006, https://doi.org/10.1155/2006/152612
- Front Line Covid Critical Care Alliance, Treatment Protocol, https://covid19criticalcare.com/treatment-protocols/
- Heart Advisory & Recovery Team, Ivermectin, https://www.hartgroup.org/category/ivermectin/
- McCullough PA, et al, “Multifaceted highly targeted sequential multidrug treatment of early ambulatory high-risk SARS-CoV-2 infection (COVID-19).” Rev Cardiovasc Med. 2020 Dec 30;21(4):517-530. doi: 10.31083/j.rcm.2020.04.264. PMID: 33387997.
- Ioannidis, John P A. (2021). “Infection fatality rate of COVID-19 inferred from seroprevalence data.” Bulletin of the World Health Organization, 99 (1), 19 – 33F. World Health Organization. http://dx.doi.org/10.2471/BLT.20.265892
- Ioannidis, John P A. “Reconciling estimates of global spread and infection fatality rates of COVID-19: An overview of systematic evaluations,” European Journal of Clinical Investigation, 2021, https://doi.org/10.1111/eci.13554
- Pezzullo AM, Axfors C, Contopoulos-Ioannidis DG, Apostolatos A, Ioannidis JPA. “Age-stratified infection fatality rate of COVID-19 in the non-elderly population.” Environ Res. 2023 Jan 1;216(Pt 3):114655. doi: 10.1016/j.envres.2022.114655. Epub 2022 Oct 28. PMID: 36341800; PMCID: PMC9613797.
- Kompaniyets, Lyudmyla et al, “Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020–March 2021,” CDC 2021, DOI: http://dx.doi.org/10.5888/pcd18.210123external icon
- Anonymous, “Key Facts About Influenza (Flu),” CDC 2022, https://www.cdc.gov/flu/about/keyfacts.htm
- Anonymous, Our World In Data, Coronavirus (COVID-19) Cases – Our World in Data
- Anonymous, “Guidance High consequence infectious diseases (HCID),” UK government, 2020, https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid
- Levitt, M., Zonta, F. & Ioannidis, J.P.A. “Excess death estimates from multiverse analysis in 2009–2021.” Eur J Epidemiol (2023). https://doi.org/10.1007/s10654-023-00998-2
- Fineberg, Harvey, “Pandemic Preparedness and Response — Lessons from the H1N1 Influenza of 2009,” N Engl J Med 2014; 370:1335-1342 DOI: 10.1056/NEJMra1208802
- Anonymous, “International Guidelines for Certification and Classification (coding) of Covid-19 as Cause of Death,” World Health Organization, 2020, https://cdn.who.int/media/docs/default-source/classification/icd/covid-19/guidelines-cause-of-death-covid-19-20200420-en.pdf (pg 3)
- Audie, Joseph, “Using CDC data and death certificate standards to propose a preliminary estimate for the number of US COVID-19 associated deaths that were caused by or contributed to by SARS-CoV-2 infection,” Research Gate, 2020, https://www.researchgate.net/publication/344228032_Using_CDC_data_and_death_certificate_standards_to_propose_a_preliminary_estimate_for_the_number_of_US_COVID-19_associated_deaths_that_were_caused_by_or_contributed_to_by_SARS-CoV-2_infection
- Fenton, Norman & Neil, Martin & McLachlan, Scott. (2021). What proportion of people with COVID-19 do not get symptoms?. 10.13140/RG.2.2.33939.60968.
- Jensen, Scott, 2023, https://www.youtube.com/watch?app=desktop&v=PHxj_Luclxs&feature=youtu.be
- Beaudoin, John, “500,000 Death Certificates Tell of Signals, Fraud, and Unlawful Deaths,” 2023, https://rumble.com/v2a7wtk-john-beaudoin-500000-death-certificates-tell-of-signals-fraud-and-unlawful-.html
- La Scola B, Le Bideau M, Andreani J, Hoang VT, Grimaldier C, Colson P, Gautret P, Raoult D. “Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards.” Eur J Clin Microbiol Infect Dis. 2020 Jun;39(6):1059-1061. doi: 10.1007/s10096-020-03913-9. Epub 2020 Apr 27. PMID: 32342252; PMCID: PMC7185831.
- Anonymous, “WHO Information Notice for Users 2020/05: Nucleic acid testing (NAT) technologies that use polymerase chain reaction (PCR) for detection of SARS-CoV-2,” World Health Organization, 2021, https://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05
- Deeks, John, “Why the school testing regime needs to change,” The Post, 2021, https://unherd.com/thepost/why-the-school-testing-regime-needs-to-change/
- Neil, Martin, “Put to the test: use of rapid testing technologies for covid-19,” BMJ 2021; 372 doi: https://doi.org/10.1136/bmj.n208
- Neil, Martin, “UK lighthouse laboratories testing for SARS-COV-2 may have breached WHO Emergency Use Assessment and potentially violated Manufacturer Instructions for Use.” Probability and Risk, 2021, https://probabilityandlaw.blogspot.com/2021/02/uk-lighthouse-laboratories-testing-for.html?m=1
- Deeks, Jonathan, “Operation Moonshot proposals are scientifically unsound,” BMJ 2020; 370 doi: https://doi.org/10.1136/bmj.m3699
- Pollock A M, Lancaster J. “Asymptomatic transmission of covid-19” BMJ 2020; 371 :m4851 doi:10.1136/bmj.m4851
- Anonymous, Statistics Canada. Table 13-10-0392-01 “Deaths and age-specific mortality rates, by selected grouped causes” DOI: https://doi.org/10.25318/1310039201-eng
- Anonymous, “Manitoba Chief Microbiologist and Laboratory Specialist: 56% of positive “cases” are not infectious,” JCCF, 2021, https://www.jccf.ca/manitoba-chief-microbiologist-and-laboratory-specialist-56-of-positive-cases-are-not-infectious/
- Government of Canada, “FluWatch annual report: 2019-2020 influenza season,” 2021, https://www.canada.ca/en/public-health/services/publications/diseases-conditions/fluwatch/2019-2020/annual-report.html
James Corbett Testifies at the National Citizens Inquiry
Corbett • 06/12/2023
Podcast: Play in new window | Download | Embed
On May 18, 2023, James Corbett testified to the National Citizens Inquiry in Ottawa on the subject of the WHO’s looming global pandemic treaty, the proposed amendments to the International Health Regulations, and the One Health approach that is being used to justify an even greater centralization of power in the hands of unaccountable institutions in the name of “global health.” The presentation also includes information on the prospect of Canada or other member states withdrawing from the WHO, information on the technocratic roots of the One Health agenda, how states of exception are used to undermine constitutional rights, and much, much more.
For those with limited bandwidth, CLICK HERE to download a smaller, lower file size version of this episode.
Watch on Archive / BitChute / Odysee / Rokfin / Rumble / Substack / Download the mp4
DOCUMENTATION
| National Citizens Inquiry – #SolutionsWatch | |
| Time Reference: | 00:47 |
| National Citizens Inquiry homepage | |
| Time Reference: | 01:17 |
| Quotations from WHO Constitution | |
| Time Reference: | 05:19 |
| Zero draft of the WHO CA+ for the consideration of the Intergovernmental Negotiating Body at its fourth meeting | |
| Time Reference: | 10:12 |
| WHO says COVID emergency is over. So what does that mean? | |
| Time Reference: | 13:20 |
| WHO chief declares monkeypox an international emergency after expert panel fails to reach consensus | |
| Time Reference: | 20:55 |
| Newsweek: PHEIC gives WHO widespread powers, up to and including “mobilizing NATO military assets” | |
| Time Reference: | 21:40 |
| Council of Europe: The handling of the H1N1 pandemic: more transparency needed | |
| Time Reference: | 23:01 |
| BMJ: WHO and the pandemic flu “conspiracies” | |
| Time Reference: | 23:04 |
| Proposed Amendments to the International Health Regulations (2005) submitted in accordance with decision WHA75(9) (2022) | |
| Time Reference: | 23:33 |
| Quote on Global Digital Health Certification Network from Implementation of the International Health Regulations (2005) |
|
| Time Reference: | 25:07 |
| CDC page on One Health | |
| Time Reference: | 33:27 |
| Quadripartite Secretariat for One Health | |
| Time Reference: | 35:24 |
| Sovereignty Coalition Press Conference: Get the US out of the W.H.O. | |
| Time Reference: | 40:12 |
| Biosecurity and Politics (Giorgio Agamben) | |
| Time Reference: | 43:15 |
| State of Exception by Giorgio Agamben | |
| Time Reference: | 51:33 |
| Universal Declaration of Human Rights | |
| Time Reference: | 51:59 |
| Lab-grown meat could be 25 times worse for the climate than beef | |
| Time Reference: | 55:21 |
| Shock: Elon Musk’s Grandfather Was Head Of Canada’s Technocracy Movement | |
| Time Reference: | 57:44 |
| Exploring Biodigital Convergence – Policy Horizons Canada | |
| Time Reference: | 01:01:04 |
| Denis Rancourt on excess mortality during the scamdemic | |
| Time Reference: | 01:15:40 |
| The Independent Panel: “Pandemic Preparedness” scores vs. death rates | |
| Time Reference: | 01:16:31 |
A line in the sand for euthanasia
Health Advisory & Recovery Team | June 6, 2023
It is easy to make an argument for euthanasia. Heart wrenching stories can be told about people who are suffering terribly and genuinely want to see their already imminent death hastened. The argument for not crossing this line is because as soon as it is crossed there is a very slippery slope on the other side. Canada has demonstrated this in a most tragic way.
Canada legalised euthanasia six years ago through the Medical Assistance in Dying bill (MAiD). Since its inception, over thirty thousand Canadians have been euthanized. The number has increased by about a third each year. By 2021 states sponsored homicide accounted for over 3% of all deaths. For comparison diabetes accounts for 2.5% and influenza and pneumonia together accounted for less than 2% in 2020.
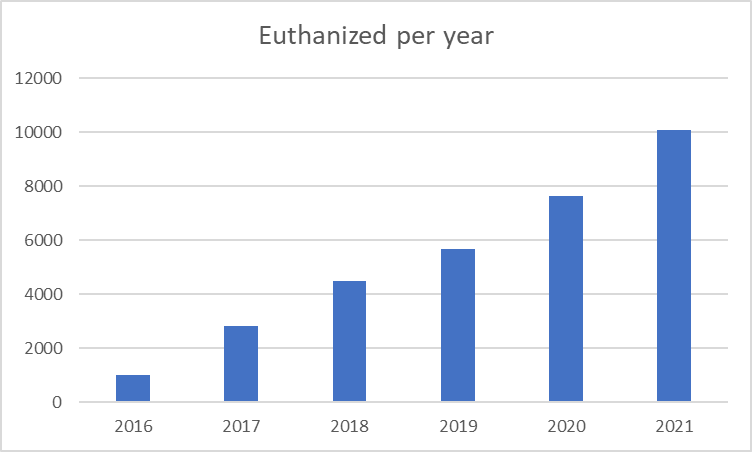
Figure 1: Number of state sponsored deaths per year
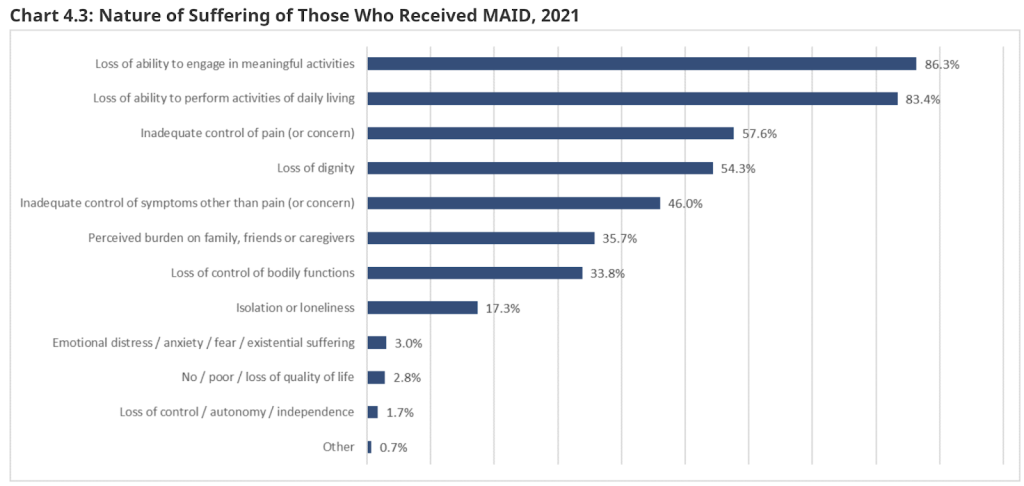
Figure 2: Reasons given for undergoing euthanasia in Canada.
The line in the sand that you do not kill has been utterly trampled over in Canada. Even the religious have lost their moral compass over this. One woman was killed by doctors in her church while religious leaders prayed over her. The church leaders claimed no-one expressed concern about this happening in a church.
Having crossed the line of “do not kill” there seems to have been little thought about drawing a new line in the sand that must not be crossed. There seems to have been little consideration of who and how many should be involved in the decision making. Note that more than a third of those killed felt they were a burden and one in six felt isolated or lonely (figure 2).
One of the most alarming developments from the implementation of MAiD is the case of a Canadian man who was approved for euthanasia due to his dire financial condition. This case underlines a chilling progression from euthanasia as an option for those in unbearable physical pain to a choice for individuals facing socioeconomic challenges. A survey showed that 28% of Canadians support euthanasia for homelessness and 27% for poverty. One family reported to the authorities the death of their depressed loved one in a hospital, where he was killed despite concerns being raised by the family and by nursing staff that he lacked capacity.
The notion of the ‘slippery slope’ is rooted in psychological research, particularly in relation to moral decision-making. An example is an experiment published in the Journal of Applied Psychology. It was found that participants were more likely to cheat when the reward started at a small amount and gradually increased. This gradual acceptance of unethical behaviour over time underscores the crux of the slippery slope effect.
By allowing euthanasia for individuals suffering physical pain, Canada may have unknowingly trampled on the path of ethical ambiguity, leading to euthanasia being used as a solution for conditions like poverty. This parallels the gradual acceptance of laws, cultural trends, and political misconduct that were initially unthinkable.
Drawing parallels with the regulation of public health, a similar ‘slippery slope’ scenario can be observed. While the intention behind banning smoking in public spaces was laudable, this move empowered public health bodies to impose further restrictions, gradually leading to what some critics label a ‘public health totalitarian state.’
To counter the ‘slippery slope’, researchers recommend a ‘prevention focus’, a psychological strategy emphasising vigilance and security. This approach involves considering the potential losses and negative outcomes of decisions before implementing them. Had this approach been more central to the discussion around MAiD, Canada might have avoided some of the ethically contentious situations it now faces.
Euthanasia is now legal in Belgium, Canada, Colombia, Luxembourg, Netherlands, New Zealand and Spain and parts of Australia. It is important that we start a public debate now. It is all the more important given that over the last few years it has become clear that we are living in a society with no respect for bodily autonomy. How long before it is accepted that “being a burden” is a just reason for killing. How much longer before people without capacity are considered to be too much of a burden?
The Canadian example underlines the dangers of the slippery slope in legalising euthanasia. The country’s experience shows that while euthanasia may be intended for individuals in unbearable physical pain, its application can gradually expand to cover other conditions, blurring ethical boundaries. It serves as a cautionary tale for other countries debating euthanasia legislation, urging them to consider potential ‘slippery slope’ implications before taking a decision.
Choked to death by hospital guards, for wearing a Covid mask too low
By Paul Stevens | TCW Defending Freedom | June 6, 2023
May 27, 2023 marked three years since the death of Stephanie Warriner. A coroner’s report records that this was the result of brain injuries consistent with ‘restraint asphyxia following struggle and exertion’, suffered more than two weeks earlier whilst a patient at Toronto General Hospital (TGH), Ontario. Stephanie’s alleged crime was failing to wear a Covid face mask properly. I recommend pausing to take that in.
Stephanie, 43, was a slight figure, 5ft 5in and 120lb. Having experienced long-term mental illness, including bipolar disorder and post-traumatic stress disorder (PTSD), and diagnosed with chronic obstructive pulmonary disease (COPD), the mother of five was admitted to TGH on May 10 with what a civil suit filed by her family describes as a ‘productive cough’. A Covid test had been negative. Having gone in search of a sandwich in the early hours of May 11, she was confronted aggressively by five personnel, four of them security guards, about her improper use of a face mask, which they said was worn too low.
As recorded in the civil suit document, after being ‘berated’ and ‘demeaned’ by guards, Stephanie was forced towards a wall, thrown to the ground and restrained, with weight applied to her back. During this time she was forced into handcuffs. Once the guards removed their weight from her back, she was seen to be ‘limp and lifeless’ but they did not attempt resuscitation or call for help. Instead, they placed her in a wheelchair and removed her from the view of security cameras and witnesses.
About ten minutes later the guards, moving her body into an elevator bay, attempted to resuscitate her but, as the coroner’s report noted, because of the ‘downtime’ between the damage being incurred and measures being taken, she developed a brain injury from which she never recovered.
The majority of the incident was captured on CCTV and may be viewed here. (You will notice that during recording, the CCTV camera appears to be moved. More about this later.) As a result of the restraint, Stephanie went into cardiac arrest, but did not die immediately. In fact, she lived for another 16 days, being first intubated and placed in intensive care and then transferred to Toronto Western Hospital on May 15. No attempt was made to contact her family until May 22, a full 11 days after the incident.
In July, two of the guards were dismissed and two were the subject of unspecified ‘internal disciplinary action’. According to a media report, at this time Toronto police said investigators were ‘awaiting the results of a full autopsy and that the case was in its early stages’. Five months later Stephanie’s sister, Denise, was still awaiting information from the police. Finally, in early December 2020, two guards were each charged with two counts of criminal negligence causing death and one count of manslaughter.
In November, 2022, two and a half years after Stephanie’s death, an Ontario judge quashed the case against the two guards, due to come before a jury last month, saying there was ‘a lack of admissible evidence to support the findings necessary for making a placement order on both counts’. Subsequently, the Federal government declined to pursue further criminal action. This despite the coroner’s report and other evidence, such as the CCTV video and court documents submitted by the Crown for an earlier preliminary hearing which contain evidence that one of the guards lied in his deposition, having initially claimed that Stephanie had ‘delivered several overhand and underhand punches to [Guard A’s] face and was kicking her feet’, but then ‘later on, [Guard B] began sobbing and admitted he had not been truthful in the report, saying: “I’m sorry. I would have never said the things I said in there if I knew there was a video”.’
Speaking of the CCTV footage, over two minutes of it has never been seen – and never will be. During Stephanie’s interrogation and restraint the camera was intentionally moved to point elsewhere. The guard monitoring the CCTV from the security office claimed that he ‘suffers from anxiety’ and moved the camera because he was ‘anxious and concerned about the altercation and use of force between [Guard A] and Stephanie’. In their civil suit, her family make it clear that they believe the camera was moved to ‘shield the other defendant guards from any potential criminal liability’.
This tragedy was the direct result of the febrile atmosphere and enforcement of unevidenced, irrational and petty Covid mask rules. Contrast Stephanie’s case with that of George Floyd, a black man who died in police custody that same month in Minneapolis. Protests were everywhere across the US and the entire world. Movements such as Black Lives Matter (BLM) sprang up. People were ‘taking the knee’ and filling their social media profiles with BLM images. There were calls for police forces to be defunded. Floyd himself achieved something close to beatification, with statues and wall paintings appearing widely. His police attackers received hefty prison sentences.
Stephanie Warriner? Nothing. Not a squeak. Because of a police and judicial embargo, it was barely a month ago that the public could even see the video and read about her death. Those who were implicated have walked free. And the health network which owns Toronto General and Toronto Western hospitals still tells us on its website that ‘in 2019, Toronto General was named among the world’s Top 10 Hospitals by Newsweek magazine’. It insists that its priorities include being ‘compassionate and caring’ with a focus on ‘quality and safety’.
Stephanie Warriner died, at the age of 43, for wearing a Covid face mask improperly. This in the very same city of Toronto where nurses unions’ had twice – in 2015 and 2018 – won cases against hospitals seeking to mask them at work over influenza, with the evidence in favour of masking ruled ‘insufficient, inadequate and completely unpersuasive’. As with so much harm which has been done to so many people in the name of ‘safety’ these past three years, it appears no one in authority questions this, much less cares.
Featured Video
The Iran War has destroyed fertilizer markets and farmers everywhere, almost
or go to
Aletho News Archives – Video-Images
From the Archives
Truth, History and Integrity
By Gilad Atzmon | March 13, 2010
… As devastating as it may be, at a certain moment in time, a horrible chapter was given an exceptionally meta-historical status. Its ‘factuality’ was sealed by draconian laws and its reasoning was secured by social and political settings. The Holocaust became the new Western religion. Unfortunately, it is the most sinister religion known to man. It is a license to kill, to flatten, no nuke, to wipe, to rape, to loot and to ethnically cleanse. … Read full article
Blog Roll
 Aletho News
Aletho News- Iran moved to change the US-Iran equation yesterday
- Former Israeli soldier: I left the Gaza war with shame and regret
- The UK Government Will Persecute Those Vocal about Israel, But Not War Criminals
- Is Hungary about to give Ukraine the EU green light?
- EU pushing Armenia to expel Russian Orthodox Church – intel service
- From Evo Morales to Rodrigo Paz: Bolivia’s Dramatic Shift Toward Israel
- Iran rejects US assassination claim, says Washington trying to whitewash its own crimes against Iranians
- The Iran War has destroyed fertilizer markets and farmers everywhere, almost
- Capitulate or Die: The Gaza ‘peace process’ and Western propaganda
- FSB Blows Lid on Western Plot to Hack Russian Officials’ Phones — But Here’s the Shocker
- If Americans Knew
- The Faustian Bargain of Journalists Embedding with the Israeli Military in Gaza
- AIPAC: Defending the Indefensible
- “You Either Leave Right Now or You Die”—Israel’s Ethnic Cleansing of a Village in Lebanon
- Selling American dead bodies to the US Navy for Israeli military training?
- AIPAC affiliate has funded lavish trips to Israel for dozens of Congress members since 7 October, filings reveal
- Trump called Netanyahu crazy, stopped Israel attack on Beirut: three articles
- ISRAELI MEDIA: Israel’s Education System Isn’t Broken. It’s Doing Exactly What It Was Built to Do
- UN experts alarmed by escalating settler terror and displacement in West Bank
- Israeli soldiers halt Catholic festival preparations in West Bank Christian village
- Congress Is Quietly Making Israel a Permanent Pillar of U.S. Military Modernization
- No Tricks Zone
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
- How Once Hardcore Climate Alarmist Lucy Biggers Realized It Was All A Scam, Brainwashing
