I just sent the email below to nearly 300 people at the CDC who are known to be involved in the COVID vaccine program.
I pointed out that existing autopsy protocols cannot find vaccine deaths and asked why isn’t the CDC notifying medical examiner and pathologists how to find COVID vaccine-related deaths?
Do you think I’ll hear back? Do you think they will do anything differently?
Here is the full text of the email:
I wanted to make sure everyone who is involved in the COVID vaccination program understands exactly why the CDC isn’t finding any vaccine associated deaths.
The short answer is because they aren’t looking for them properly even though the methodology to do so is in plain sight. That methodology is ignored. This is why the pathologists find nothing.
A simple analogy: if the PCR test were run with just 5 cycles, we’d never find any COVID virus. We’re basically doing the same thing with the tests we do post-vaccine: we didn’t change the tests to FIND the vaccine.
This is unethical.
I wanted to make sure everyone who works at the CDC is aware of this.
At the very least, the CDC needs to publicly acknowledge this clear failing.
As I said recently on Fox News, hundreds of thousands of Americans have been killed by the COVID vaccines.
People who were skeptical of my numbers found that document very convincing.
Fox News REFUSED to look at my data or discuss it. Why not? Because they are paid not to challenge the narrative. Over $1B is being paid out to promote the vaccines and ignore anything that goes against the narrative.
Even worse, nobody will go on camera to try to refute any of this. Why not?
The reason the CDC finds no deaths is because they aren’t looking for them with tools that will find the deaths.
You need to run specialized tests to determine an association with the vaccine. The standard tests run by medical examiners are NEVER going to find an association. That was clear in their paper and it was independently validated by Dr. Ryan Cole who is a very experienced board certified pathologist.
The question you all should be asking is:
Why isn’t the CDC requiring that for anyone who dies 30 days after getting a vaccine an autopsy protocol that can find an association with the vaccine using the necessary specialized tests?
Such a protocol already exists and it is proven it works. See this article.
Dr. Cole points out that YOU NEED SPECIALIZED TESTS to find the association.
How many pathologists are doing these tests in America? Just one as far as he knows.
I am absolutely baffled as to why the CDC has never done any of these tests and why nobody has talked to Dr. Cole.
Do you know why? Can you tell me?
While there may be a better protocol, this protocol is proven to detect vaccine involvement in 93% of the cases studied. These are all tissue samples from people dying shortly after vaccination where the medical examiners were unable to find any association.
If this protocol is insufficient, where is the CDC document explaining why and proposing a better one that finds more association?
If the CDC has been doing adequate tests, where is the documentation of that?
It seems pretty clear to me that the CDC isn’t finding vaccine-caused deaths because they refuse to look.
They can even go back to the autopsy tissue samples they already have and re-stain them to see how many were missed in the initial analysis as documented in the Rosenblum paper in Lancet.
The Rosenblum paper should have reported that none of the autopsies used stains that were necessary to show an association. But this was never mentioned. Shouldn’t that paper be corrected?
I tried to talk to the authors, but Martha Sharan at the CDC ignored every email and phone call I left for her.
Is this how science is done? By not allowing anyone to challenge your work?
My article also explains very clearly why doctors are not finding vaccine-related deaths. The interview with Gina Doane makes it clear her dad died from the vaccine yet the doctor in charge refused to even consider this as a possibility even though NONE of his other explanations fit, and the vaccine hypothesis fit perfectly. That’s not how science works. This is corruption. You don’t need a medical degree to figure it out. It’s all in the video.
But that second video shows you first hand how doctors are looking the other way.
I hope you will find the two videos and the content of the post eye opening. One commenter wrote: ” One of the best and most revealing pieces of research on the net….very telling. Thank you.”
It’s well worth your time. I’ve written over 700 articles on the COVID vaccines and the content presented in these two interviews are the most important interviews for everyone at the CDC to watch because it shows you how 1) the tests are inadequate and 2) even with overwhelming evidence, the doctors are deliberately NOT acknowledging vaccine death.
If you want to chat, I can be reached at <redacted>.
-steve
Am I flogging a dead horse?
No. I’m just putting hundreds of people at the CDC on the record as having been notified of what is going on.
And who knows. Maybe ONE person is honest.
The CDC has backed off their earlier “guidance” and have removed things from their website that were untrue.
But for the programme itself the BBC commissoned a large survey which, we show, revealed that 26% were unvacinated.
To understand why it is so critical to get an accurate estimate of the proportion of unvaccinated see this 2 minute accompanying video: https://youtu.be/8It4qI9yhzQ
In 2015 a team of researchers employed by the medical services of the US military published a peer-reviewed paper on the incidence of myocarditis and pericarditis after smallpox vaccination (SPX) and vaccination with an inactivated trivalent influenza vaccine (TIV).
Despite being published 7 years ago before anyone had heard of “covid”, the findings in this study could have very significant implications for the Covid-19 mRNA injections.
In this study, the researchers found that:
When active surveillance systems are used, significantly more myocarditis cases were identified than in earlier studies which had relied on more passive reporting.
The incidence of cases of possible myocarditis without symptoms – detected by testing all subjects vaccinated regardless of symptoms – was far higher than the cases in which subjects developed symptoms such that they would seek medical help.
Given these observations, it seems highly likely that the incidence rates of myocarditis following Covid vaccination have to date been severely underestimated.
The background to the study was that the US military rolled out a limited program of SPX following a perceived threat that smallpox might be used as a weapon in a bioterrorism incident. By the time of the paper’s publication, >2m doses had been administered, but the US had 290m doses in reserve to use for the general population if required. Concerns had been raised about a possible risk of myocarditis after this vaccination. This study sought to quantify these risks.
Key aspects of the study design:
Subjects were selected from previously healthy military personnel presenting for either SPX (1081 subjects) or TIV (189 subjects). A battery of baseline tests were performed and these were repeated either once or twice 5-8 days after vaccination and / or 9-28 after vaccination.
The notable difference between this and other studies assessing myocarditis and pericarditis rates was that the assessments were performed on all subjects and they included measurements of cardiac troponin levels (a protein which is released by damaged heart muscle cells) and ECG, in an attempt to detect possible “subclinical” cases of myocarditis – ie those which did not result in symptoms and so ordinarily would not gain the attention of healthcare systems.
Clinical myocarditis and pericarditis were determined according to published epidemiological case definitions that require the development of new onset cardiac symptoms soon after vaccine exposure, and each case was confirmed by an independent adjudicator.
Possible subclinical myocarditis and pericarditis were diagnosed whenever troponin levels rose by or to a certain level[1], or by ECG changes respectively, in the absence of symptoms.
Incidence rates were compared to background incidence rates calculated from a 2002 study among 1,390,352 service members (no exposure to any vaccines).
Key results:
Subjects receiving SPX were predominantly young (mean 23 years) and male (88%), those in the TIV cohort were more evenly balanced (54% male) and older (mean 36 years)
8.8% of the SPX recipients reported severe cardiac symptoms (defined as >3 out of 10 on a visual scale for at least 2 days).The most frequently reported cardiac symptoms were chest pain and dyspnea on exertion.
Despite no significant differences in pre-vaccine health self-assessment between the cohorts and fewer reported physical limitations in the SPX cohort, there was a significantly higher incidence of new onset cardiac symptom(s) post-SPX (10.6%) compared to the older post-TIV cohort (2.6%), p<0.001. These differences remained 4-5 fold higher in the SPX cohort after adjusting for group differences in age, sex, weight, race, smoking, and physical limitations, and also when symptoms were limited to consideration of those above 3 out of 10 on the visual scale.
The incidence rate of clinical myocarditis / pericarditis after SPX was 5 cases out of 1081 (4 were myocarditis and one pericarditis), equating to 463 per 100,000, which was >200 x background expected rates.
The incidence of possible subclinical myocarditis / pericarditis after SPX was 2868 per 100,000, or nearly 3%, which was 6 x the rate of clinical myocarditis.[2] This could not be compared to an expected background rate as this had never been measured before in this way.
No cases of either clinical or subclinical myocarditis were detected after TIV.
Implications.
Before going on to discuss the implications of this study for the Covid-era, it must be emphasised that “full recovery” from myocarditis is a misleading term: whilst the patients may initially become symptom-free, all should ideally receive regular cardiological follow-up to detect cardiomyopathy and / or arrhythmias later in life, and there is a significantly raised risk of cardiac morbidity and mortality.
Moreover, in several case series, for example this one published in JAMA, “Late Gadolinium Enhancement” on cardiac MRI[3] indicative of long term heart damage was found in the majority of clinical myocarditis cases which underwent detailed investigation. This finding is not consistent with mRNA-induced myocarditis having a more benign course than other forms, as was originally hoped.
For the above reasons, it is important to try to accurately capture all possible cases of myocarditis, both for the individuals concerned (so they can receive proper follow-up) and for calculating the extent of any added risks from vaccination.
In respect of the accurate detection of myocarditis cases, this study raises several important concerns relevant to the Covid injections:
Passive surveillance misses many cases.
Before this study, the rate of clinically diagnosed myocarditis / pericarditis had been previously estimated to be 16.1 cases per 100,000 in a cohort of US service members receiving smallpox vaccination, nearly 7.5-fold higher than the expected background rate of 2.16 per 100,000 observed among comparable unvaccinated service members.
The rate of clinical myocarditis observed in this SPX study was approximately 28 times higher than the previous estimate, at 463 per 100,000 – several hundred times the expected background rate. The higher incidence rate detected is almost certainly due to the active surveillance systems in place, where cases were pro-actively sought out and participants and their physicians made aware of their possibility.
As the authors state:
Prior to the present study, the incidence of myocarditis / pericarditis following smallpox vaccination was estimated from passive surveillance registries and population databases, with an inherent bias towards underestimation of disease incidence.
Myocarditis cases may be easily dismissed as musculoskeletal in origin.
Myocarditis is usually self-limiting in its acute phase, improving with self-treatment by a non-steroidal anti-inflammatory drug such as ibuprofen. It could quite easily be confused with “expected” aches and pains following injection, or with musculoskeletal injury, and this would be more frequent in the young, especially if active in sport.
The authors make the point that:
“3 of the 5 clinical cases would not have sought medical care without study interventions including enhanced education and surveillance.”
With the Covid mRNA injections, not only have we experienced a lack of active surveillance and a reliance on passive adverse event reporting, but there has been an atmosphere of discouragement of reporting. Many physicians have reported censure by hospitals or other health authorities for even discussing a possible vaccine origin for adverse events, and even subjects themselves have received opprobrium online after questioning the origin of their symptoms.
Hence, whatever factors the authors noted in 2015 in relation to underreporting of myocarditis following SPX are likely to be even more in evidence now for the Covid vaccines.
Because of this, there must be a very significant possibility that the actual numbers of clinical myocarditis cases caused by the mRNA injections have to date been very significantly underestimated.
The frequency of subclinical cases may dwarf the clinical cases.
This was actually the first study to attempt to detect possible subclinical cases of myocarditis (ie those without discernible symptoms) following vaccination. It is highly likely that, just as there is a spectrum of outcomes with symptomatic cases, such that a proportion have zero long-term problems, so with the subclinical cases an unknown proportion may well go on to have cardiac problems. Given that heart cells are irreplaceable and that scar tissue in the heart can disrupt electrical conduction the degree of concern about heart damage must be much more than with, say, damage to the skin, which can self-repair and still perform its primary function.
The actual proportion of subclinical cases which go on to manifest in cardiac disease later in life is unknown, however the authors selected a threshold for the measured troponin levels by which to define a subclinical case which is known to be associated with an increased risk of adverse outcomes. In the paper cited by the authors in support of their chosen troponin criterion it had been concluded that:
“In the general population, cTnT [troponin – protein released from heart damage] elevation is rare in subjects without CHF, LVH, CKD, or DM, [Congestive Heart Failure, Left Ventricular Hypertrophy, Chronic Kidney Disease or Diabetes Mellitus] suggesting that the upper limit of normal for the immunoassay should be <0.01 μg/L. Even minimally increased cTnT may represent subclinical cardiac injury and have important clinical implications, a hypothesis that should be tested in longitudinal outcome studies.”
*Definitions in [ ] with bold added by this author
The rate of possible subclinical myocarditis detected after SPX (3% of subjects) was 6 x the rate of symptomatic myocarditis. That these findings are or might be significant rather than chance fluctuations is supported by the fact that zero such cases were detected in the TIV cohort.
Moreover, the authors point out that even this may be an underestimate (bold added):
“While assumptions about benign troponin release from the myocardium have been made, there is a growing body of literature suggesting that even in generally healthy populations with no known cardiac disease risk, small elevations in troponin (stratified below the levels measured by the assay in this study) are associated with increased risk of all cause and cardiovascular mortality. Therefore, the rate of reported elevations in this study may actually be an underestimate of the true incidence of vaccine related subclinical myocarditis.“
There seem no reasons to suggest that possible subclinical myocarditis might not also be occurring after Covid injections, and also at higher rates than clinical cases. In fact, given the use of active surveillance for clinical cases employed in the SPX study, it is likely that the ratio between possible subclinical and reported clinical myocarditis cases for the Covid vaccines may in fact be higher than the 6-fold seen after SPX, because of the significant underreporting of clinical cases after Covid vaccines for the reasons mentioned above.
It should be stressed that little is known about the long-term prognosis of myocarditis / pericarditis, whether infective in origin or otherwise. No follow-up to the Engler et al paper (now 7 years old) measuring cardiac status in either the clinical or possible subclinical cases has been published to date.
A 2005 paper reported a well-conducted follow-up study of 67 cases detected following smallpox vaccination of 540k military personnel and found normalisation of echocardiography, ECG, and functional status (measured by ECG exercise-testing) in all subjects including those who initially had depressed cardiac function. This is encouraging, although the median follow-up period was just a few months and none were followed for more than one year after the myocarditis; hence concerns must remain regarding cardiac function in later life, especially in those in whom cardiac reserve falls secondary to other cardiac pathology such as coronary artery disease.
Concluding remarks
The authors conclude their paper with this warning:
Our study identified a rate of myocarditis/pericarditis following SPX immunization that is significantly higher than previously described, and highlights the challenges of post-licensure vaccine safety surveillance to identify adverse events that are not well understood or previously unrecognized.
Applying the incidence described in this study to a SPX immunization program that has delivered over 2 million doses, largely to young, healthy primary vaccinees, there are potentially thousands of vaccine associated cases, many undiagnosed because of self-medication or lack of provider awareness].
In our study, 3 of the 5 clinical cases would not have sought medical care without study interventions including enhanced education and surveillance. The recognition of potential adverse events following immunization requires accurate diagnosis of new onset clinical symptoms.
Our study reinforces the need, as part of all post-vaccine (and potentially new drug related) adverse events surveillance, to include specific standardized inquiry about new onset cardiac symptoms and to highlight the value of dynamic pre to post immunization cardiac troponin increases as a potential biomarker of risk in future safety surveillance studies.
Two million doses of SPX sounds a large number, but it is sobering to consider where we are today in respect of our understanding of the association of the Covid vaccines to myocarditis, having rolled out several billion doses, a program which is now continuing with 3rd or even 4th doses (whereas the incidence studies published to date have been based on 2 doses only).
It is accepted now that there is a definite association between mRNA vaccination and myocarditis, yet the precise rates of increased risks reported vary hugely between different studies, which probably reflect vastly different methodologies between investigators and countries according to prevailing local reporting standards and customs.
Moreover, initial claims that myocarditis risk might be higher after Covid infection compared to vaccination have not held up to scrutiny. The latest study – based on a large (~200k) cohort of adults in Israel – found no increase in the incidence of pericarditis or myocarditis in adult patients recovering from COVID-19.
In addition to the high, yet underreported, rates of clinical myocarditis, there remains a distinct possibility that there may have been very large numbers of subclinical myocarditis cases caused by Covid vaccines, the long-term outcomes for which are uncertain.
Approximately 3% of those receiving a single SPX vaccination met the criteria for having developed possible subclinical myocarditis, and given that billions have now received Covid mRNA products (many multiple times), if the frequency is similar to SPX the number of such cases following mRNA injections could well be in the millions.
Despite these worrying data, we have inexplicably witnessed the rollout of multiple booster doses, including in many countries to young adults and even children, despite there having been:
No active surveillance for myocarditis, only passive reporting
No prospective studies of troponin levels (which would be relatively simple to perform).
No standardised inquiries about new onset cardiac symptoms
One could be forgiven for thinking that the reason for this is that those who have relentlessly pushed this program into younger and younger people at little to no risk from Covid, simply do not want to know, and prefer to maintain a degree of “plausible deniability”.
Footnotes:
For subclinical myocarditis, the criteria for diagnosis were: the development of any one of the following: a) elevated post-vaccine levels of cTnT ≥ 0.02 ng/ml with pre-vaccine cTnT levels <0.01 ng/ml; or b) a post-vaccine cTnT level of 0.02 ng/ml greater than the pre-vaccine level based on the imprecision profiles of the assay.
The absolute subclinical cTnT elevations post SPX vaccine ranged from 0.02 to 0.24 ng/ml with the majority (n = 28, 90.3%) ranging from 0.02 to 0.07 ng/ml
This is a radiological feature seen on cardiac imaging which is indicative of myocardial damage consistent with a high risk of poor long-term prognosis.
Great news! New York City is closing “Infant COVID Vaccination Sites”, citing lack of demand, next week!
In effect, New York is really forced to do the same thing as DeSantis did in Florida — it is closing vaccination clinics for infants, which DeSantis never even opened. While in Florida it was done thanks to the Governor, in New York it happened because parents refused to give their children the Covid vaccine.
The ridiculous explanation NYC gave, is that they are “pivoting to monkeypox”.
This is a huge win for New Yorkers and for people everywhere.
This also means that our anti-Covid-vax activity, broadly speaking, is NOT a waste of time. Mind you, the media keeps lying, as usual. The New York Times, the most important newspaper in New York, is mum about this closure. Google does not show any articles about it except the one I quoted, either.
But people noticed and the public opinion has turned from most people wanting COVID vaccines a year ago to 90% not wanting any extra doses. It did not just happen by itself. We made it happen.
I want to thank my readers who shared my anti-Covid-vaccine-for-babies articles like crazy. That helped, perhaps to a very tiny extent, to warn parents of the danger of giving their kids Covid vaccines.
If people like us did not spread it, nobody would know the truth!
In 2020, government orders to stay home — along with lockdown-produced job losses, public fear of COVID-19 and other factors — led to dramatic declines in in-person utilization of healthcare services among adults and children, both in the United States and globally.
“Well-baby” and “well-child” visits were some of the noteworthy casualties.
In the U.S., children’s and teen’s vaccination rates plummeted dramatically, falling that year by as much as 91% depending on the age group, including a noticeably lower uptake of diphtheria, tetanus and pertussis vaccines (DTaP or DTP), meningitis shots and human papillomavirus (HPV) vaccines.
Public health officials expected this “pandemic hangover” to dissipate by 2021, but instead, the change in parents’ vaccine-seeking behavior for their kids persisted.
Internationally, 6 million fewer children worldwide got at least one dose of DTP vaccine in 2021 versus 2019, causing the head of UNICEF to lament “the largest sustained drop in childhood immunization in a generation.”
And in the Philippines — where the president threatened to jail COVID-19 vaccine refusers — 2021’s percentage of children receiving a first DTP dose was just 57% versus 92% a decade previously.
Stateside, Washington State reported flu shot uptake in children under age 5 was down by around 25% in November 2021, compared to the two previous flu seasons. And Michigan’s state registry for March 2022 showed that 24% fewer toddlers “were considered vaccinated” compared to March 2020.
When Michigan compared its 2020 vaccination data against the 2016-2019 period, it found vaccination coverage had declined in “all milestone age cohorts, except for birth-dose hepatitis B coverage.”
At this juncture, state officials are openly speculating that COVID-19 shots — thus far rejected by the parents of 97% of under-5-year-olds — are the reason parents are increasingly ambivalent about childhood vaccination more generally.
Referring to this “spillover doubt,” a Michigander public health spokesperson said parents who once accepted childhood vaccination without question are now saying, “Wait a minute. Do I really need these vaccines?” and asking, “How are these vaccines made?”
According to another Michigan official, “vaccination” — the “V-word” — has become a “trigger word” for irate parents who believe government not only overstepped its authority during COVID-19 but is fraudulently pushing unsafe vaccines on their little ones.
Fewer babies dying is no ‘disaster’
In October 2020, three scientists from the U.S. and U.K. authored the Great Barrington Declaration and condemned — quite gloomily — the steep decline in childhood vaccination resulting from COVID-19 lockdowns.
As long-time proponents of vaccination — professionally involved in vaccine development, promotion of the dangerous HPV vaccine and accepting of COVID-19 vaccines as a solution to lockdowns — the three declaration authors positioned the decline in childhood vaccination rates at the head of their list of “disastrous” lockdown consequences.
Far from witnessing a disaster, however, observers by June 2020 had begun noticing a wonderful silver lining — a “surprising” pandemic effect on the death rate among infants, in particular, with 200-plus fewer infants dying per week, amounting to a 30% reduction in expected child deaths within a few months.
To explain the “something mysterious” saving the lives of infants, these analysts, along with Children’s Health Defense (CHD) Chief Scientific Officer Brian Hooker, pointed out how the missed infant vaccines coincided with a “precipitous drop” in reports of sudden infant death syndrome (SIDS) to the Vaccine Adverse Event Reporting System (VAERS).
SIDS deaths — which by definition affect children who are normal and healthy — and sudden unexplained deaths in children over age 1 typically occur in close temporal proximity to vaccination, with nine out of 10 SIDS deaths following two- and four-month “well-baby” visits.
An analysis of three decades of VAERS data found 75% of reported post-vaccination SIDS cases occurred within seven days of childhood shots.
Japanese pathologists who identified SIDS cases taking place within a week of vaccination agree that “suspicious cases do exist,” leading them to encourage forensic pathologists to “devote more attention to vaccination” in SIDS events.
Naturally, “fact-checkers” dispute the hypothesized association between 2020’s lower vaccination rates and the decreased deaths in young children.
Additional clues
CHD has reviewed dozens of studies showing dramatically better health in unvaccinated children while finding “no studies that show superior health outcomes in vaccinated children.”
However, because the effects of vaccination are complex, cumulative and synergistic with other toxic exposures — and because most chronic disease data sets have not yet caught up to the pandemic — it is not so easy to tease out other upsides resulting from 2020’s lower childhood vaccination rates.
There are a few clues, however.
Consider the decline in emergency department (ED) visits and the fact that the largest declines were in persons under age 15.
Ordinarily, an estimated one in seven children experiences an ED visit every year.
An analysis comparing 2020’s pediatric ED visits to ED encounters over the previous decade found “substantial” decreases for certain diagnoses — notably abdominal pain, ear infections, asthma, pneumonia, upper respiratory and urinary tract infections and trauma — while visits for diagnoses such as seizures and complications of diabetes held steadier.
Although there is no surefire way to know why ED visits declined for those specific conditions, all of the diagnoses in question show up in vaccine package inserts as post-vaccination occurrences — along with nearly 400 other acute and chronic symptoms and conditions.
Abdominal pain may not sound serious, but it can be a sign of acute pancreatitis (sudden-onset inflammation of the pancreas), so much so that clinicians advise “always” considering acute pancreatitis “in the differential diagnosis of abdominal pain in children.
And case reports are now flooding in (for example, from the U.S., Japan, Poland and New Zealand) describing severe pancreatitis in the aftermath of COVID-19 vaccination.
Moreover, acute and chronic pancreatitis began mysteriously surging in children following the childhood vaccine schedule’s expansion in the 1990s and 2000s, and juvenile diabetes and pancreatic cancers in young adults — two conditions associated with pancreatitis — began escalating soon thereafter.
COVID vaccines — a line in the sand?
Most observers attributed the sudden drop-off in routine childhood vaccination in 2020 purely to circumstance-imposed foregone care (“the gap between perceived need and actual utilization of healthcare services”).
Now, however, it is COVID-19 vaccines — and particularly the unscientific authorization of the jabs for teens and young children — that appear to be the principal reason many parents no longer “perceive a need” to rush back into the vaccine fold.
Even the propagandistic New York Timesadmitted to a hardy new contingent of vaccine “skeptics” whose questioning was forged in the crucible of COVID-19 restrictions, COVID-19 vaccine mandates and, tragically for some, a child’s adverse reaction to the COVID-19 shots.
As a physician tweeted from the “frontlines of medicine” in early August, “Parents are DONE with giving their kids any and all [syringe emoji]. Not only that but they’re disgusted with what they had already allowed to be injected into their kids. They wish they could turn back.”
Public health’s tired old strategy for recapturing these wayward parents appears to be (surprise, surprise) badgering parents to “catch up as many vaccines as possible in a single visit” — bolstered by the false claim that it is to a child’s advantage to get a bunch of shots at once — while also stoking worries about a resurgence of so-called “vaccine-preventable” illnesses.
Thus, following a single case of paralysis ascribed to “polio,” New York State is busily trying to conjure up a polio outbreak, never mentioning the decades of manipulation of the “polio” diagnosis intended to mask nonviral causes of paralysis that include vaccination and poisoning.
Florida, meanwhile, is urging college students and other groups to get meningococcal vaccines following the deaths of seven gay and bisexual men, allegedly from meningococcal disease.
Why did the deceased men develop meningitis to begin with? No one has shared information about their COVID-19 vaccination status, but researchers around the world are reporting meningitis as a post-COVID-vaccination adverse event in adolescents and adults — for example, in Japan, Singapore, Korea, Iraq, Belgium and Germany.
Meningitis also is a listed adverse event for DTaP, hepatitis A and B, influenza and MMR vaccines, and vaccines containing Haemophilus influenzae type b (Hib) and polio components.
And a 28-year-old physician who volunteered in Brazil’s clinical trials for AstraZeneca’s COVID-19 vaccine died after receiving the meningitis vaccine given to the “control group.”
What kids really need
Sadly, whatever temporary or longer-lasting silver lining may have emerged from the COVID-19-induced lull in childhood vaccination, children and their parents still face many challenges.
According to a Centers for Disease Control and Prevention study, the weight status of children and adolescents who were already overweight or obese worsened significantly during 2020, and children’s food insecurity is rising both domestically and internationally.
In addition, the massive social and behavioral changes commanded through government restrictions have prompted dire headlines about young people’s mental health — although experts caution these could counterproductively lead to overdiagnosis and overmedication with black-box-warning drugs known to cause violence and suicide.
Rather than more vaccines or drugs that have never delivered on their hype or promises, what children and youth need to thrive are the slower-but-surer public health fundamentals — such as solid nutrition, safe housing and economic security — and the loving attention of their parents.
EXCESS all-cause mortality in New Zealand is running at record levels. About 100 people are dying each day in a country with a population of five million. A few times during the last couple of months, we have asked a key question: What are people dying of?
Ministry of Health data records that about seven people are dying each day with Covid, but only about a maximum of three of these because of Covid. That is just three per cent of deaths. Occupancy of intensive care beds with Covid hovers around three to five per cent Therefore it is not Covid that is overwhelming our hospitals, so what is?
The Ministry of Health and mainstream media have been talking vaguely about a bad flu season, but a quick check of the FluTracking website reveals that the 2022 flu season is not even as bad as 2019.
My plumber was doing a job for me last week and complained about staff falling ill continuously. Sick leave among teachers in New Zealand is up by 80 per cent. The newspapers are reporting businesses are closing because of staff shortages exacerbated by ‘winter illness’, but as the incidence of flu is not that high, what could be going on?
An article on the Stuff news website contains an important hint: Te Whatu Ora Taranaki hospital emergency department clinical nurse manager Therese Manning said while there had not been much change in the number of presentations to department in the last five years, the patients tend to be more unwell and therefore likely to stay in hospital longer.’
Acute presentations at emergency departments are increasing, but what are the patients ill with? We aren’t being told and may never be, if our health czars are allowed to continue to deny access to information.
This week it has been reported (correctly) that six Canadian doctors died suddenly (at least three of them immediately after receiving their mandatory fourth Covid shot), but hospitals refused to release the cause of death or vaccination status, citing privacy concerns. The authorities have vehemently denied that the deaths could be related to mRNA vaccination. See this article for a summary.
I don’t know if you have noticed, but stories about sudden death incidents seem to have dropped off the mainstream media radar. Three years ago a sudden unexplained death might have made the headlines, but today if they are reported at all, they only remain on the visible online page for a very short time. You might have missed this one.
Yet, as the Taranaki Hospital emergency department data and the all-cause mortality data reveal, acute illness and sudden death are at an all-time high. Life insurance data from the US paints a similar picture.
So have our newspapers ceased to care, or are they, like the hospitals and emergency services, too inundated to cope? Having heavily promoted mRNA vaccination for 18 months, are they too embarrassed to ask questions?
Not everyone is keeping silent. Professor Shmuel C Shapira, longtime head of the Israeli Institute of Biological Research, has been speaking out about the failure of the Israeli mRNA Pfizer vaccination programme, describing it as a house of cards about to come tumbling down.
He tweeted: ‘I am not against vaccines, I am against stupidity, false science and management that is not professional and ignores matters of fact.’
Dr Clare Craig, a former NHS diagnostic pathologist, is also raising her voice. On GB News, she analysed official German government data. This shows that one in every 5,000 doses causes a serious reaction to Covid vaccines. But it doesn’t stop there. The German government conducted a survey of more than half a million vaccine recipients. It found that one in 500 reported a serious adverse reaction after an mRNA dose (more than ten times the underreported official count).
If you are worried that lightly-affected Germans are inflating the figures, don’t be. The definition of a serious adverse reaction requires that a person be hospitalised or suffer a permanently life-changing event.
Dr Craig invited us to step back from the modelling and government guidance about efficacy and safety, and consider that Covid data from around the world does not show that mRNA vaccination leads to any reduction in deaths. Most illustrative are comparisons between comparable countries with high and low vaccination rates.
For example, compare Israel, with close to 100 per cent vaccinated (and most boosted with four doses), with Palestine, with just 40 per cent double-vaccinated.
Israel has 1,204 Covid-related deaths per million population and Palestine 1,182 deaths per million – roughly the same. It thus becomes apparent that mRNA vaccination does not reduce the Covid death rate.
Look at the Covid data from Africa and the picture becomes more concerning. Africa has a vaccination rate of 15 per cent, a population three times larger than Europe, and nine million confirmed Covid cases. Whereas Europe has 240million cases, and a Covid vaccination rate around 90 per cent.
Just remember that analysis of Covid death data does not include rising all-cause deaths unrelated to Covid infection. The evidence points to reduced immunity as a result of mRNA vaccination.
Dr Craig reported that the UK public are voting with their feet and failing to come in for boosters (and they are stopping bringing in their children for this dangerous jab). Aren’t we all in sympathy? We are waiting for our doctors to speak up and our courts to do the math.
The CDC has dropped special quarantine recommendations for unvaccinated persons, finally admitting that natural immunity should be considered and that vaccines don’t stop infection.
“CDC’s COVID-19 prevention recommendations no longer differentiate based on a person’s vaccination status because breakthrough infections occur, though they are generally mild, and persons who have had COVID-19 but are not vaccinated have some degree of protection against severe illness from their previous infection,” their update reads.
The CDC removed the recommendation that unvaccinated persons quarantine after they’re exposed to the virus. They now recommend that individuals wear a mask for ten days post-exposure and get tested after five days.
The CDC further acknowledged that the Omicron variant of COVID poses a smaller risk of hospitalization and death than previous variants.
This announcement will likely pressure Canada’s health authorities (and Trudeau) to follow suit. Although numerous countries dropped their medical segregation policies long ago, Canada remains one of the last to do so.
Moreover, each consecutive variant appears to be weakening, with immunity (including natural immunity) being widespread. Although Canada has an abnormally high amount of mask and vaccine fanatics, the remaining medical segregation could soon be a thing of the past.
With that said, Canada’s health authorities have done nothing but warn of a return to restrictions and upcoming waves of COVID, telling Canadians that the pandemic is not over.
Additionally, the University of Toronto recently mandated that young health students living on residence get a 3rd vaccine.
Facebook has hidden posts with the “#diedsuddenly” hashtag because it claims that some of these posts violate its far-reaching community standards. When users search for this hashtag, no results are displayed and Facebook shows a message stating that the results are hidden.
While Facebook doesn’t specify which rules these posts allegedly violated, Twitter users have been using the hashtag to share news stories about people who died suddenly. Most of these Twitter posts note that those who died were fully vaccinated for COVID-19 and allude to there being a connection between the vaccines and their deaths.
If Facebook users are posting similar content under this hashtag, the posts are likely to violate the tech giant’s ban on a wide range of COVID-19 vaccine claims. Facebook prohibits claims that “vaccines are toxic, dangerous, or cause autism” and reduces the distribution of “shocking stories” about the vaccines. One of Facebook’s examples of a shocking story is “Uncovered: See the 632 reports made of people who died within a week of having the new COVID-19 vaccine.”
The tech giant has previously used hashtag blocking to censor many other topics including “#buchamassacre” (a block that it later said was a mistake), “#Revolution” (which was blocked on a July 4th weekend), and “#SaveTheChildren.”
A new study published in the New England Journal of Medicine has demonstrated that people who are triple-vaccinated (boosted) against COVID recover significantly more slowly from COVID infection and remain contagious for longer than people who are not vaccinated at all.
The study did not deal with the severity of illness with or without a vaccine.
Researchers swabbed infected people and cultured the swabs, repeating the process for over two weeks until viral replication was not observed.
At five days post-infection, less than 25 percent of unvaccinated people were still contagious, whereas around 70 percent of boosted people were still carrying viable virus particles. For those partially vaccinated, around 50 percent were still contagious at this point.
Even more strikingly, at ten days post-infection, one-third of boosted people (31 percent) were found to still be carrying live, culturable virus. By contrast, just six percent of unvaccinated people were still contagious at day 10.
In other words, people who have received a booster shot are five times more likely still to be contagious at ten days post-infection than are unvaccinated people.
The findings go a long way to explaining why Paxlovid, Pfizer’s anti-viral medication, is often not effective for people who have been vaccinated against COVID, with many experiencing a recurrence of symptoms along with a positive COVID test after completing the five-day regimen (as recently occurred with quadruple-vaccinated Dr. Anthony Fauci). This phenomenon is known as COVID rebound.
Meanwhile, Israeli Health Ministry data shows that in the older population (those over the age of 60), having submitted to more COVID shots often correlates to a greater likelihood of becoming infected with COVID.
Israel Ministry of Health
The blue line represents the unvaccinated; light-green is the partially-vaccinated; dark-green is those who have received a booster shot within the past six months.
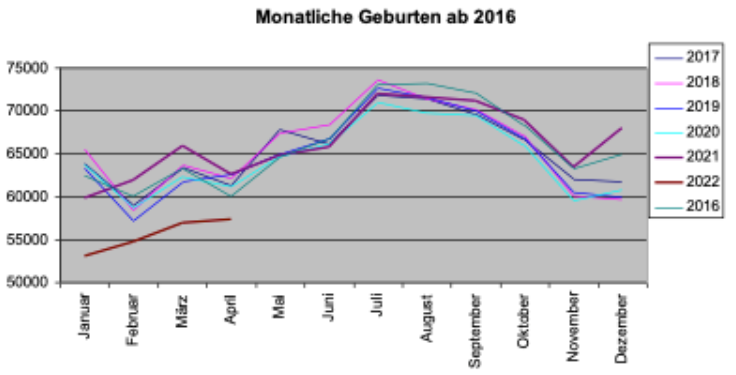
Germany has seen a “dramatic drop” in birthrate during the first 4 months of 2022, according to transitionnews.de, leading to rising suspicions over COVID vaccine safety.
“Compared to the previous year, the number of births has fallen by 12 percent – that’s about 25,000 fewer births in the first four months of 2022,” reports Sternfried Müller of transitionnews.de.
The above chart shows the number of births for the January-April period each year since 2018. During the Corona years of 2020 and 2021, Germany saw a rise in the number of births, climbing to 250,000 births. But in 2022, the number of births mysteriously plummeted a whopping 12%!
Something unusual must have triggered the phenomenon. Going back 9 months prior to the January-April 2022 period takes us to the April to July 2021 period, which coincides to COVID vaccination of younger adults in earnest. Remarkably, Germany’s media have been silent on the latest published statistics, issued by the German Federal Statistical Office (Destatis).
The next transitionnews.de chart shows the monthly number of births and just how dismally 2022 lags so far compared to the previous years:
A number of reasons have been proposed to explain the dramatic decline, among them fewer marriages. But that remains highly doubtful.
There are increasing suspicions that it is vaccine linked, as some studies already suggest: see here and here.
For the time being German authorities obstinately continue to remain in denial mode when it comes the the adverse effects of the COVID vaccines. Currently the Ministry of Health is gearing up to roll out another mass wave of vaccinations and restrictions in the run-up to the fall flu season.
A former Washington State University football coach is seeking $25 million from the university for wrongful termination after he was fired last year for refusing to get vaccinated against COVID-19, The Seattle Times reported Tuesday.
A tort claim was filed April 27 on behalf of Nick Rolovich with the state’s risk management office. Filing a claim is a prerequisite to filing a lawsuit against a state agency.
There’s a 60-day waiting period between when a claim is filed and when the claimant can file a lawsuit. As of Wednesday, a spokesperson for Attorney General Bob Ferguson said no suit had been filed, according to The Washington Post.
After denying Rolovich’s request for a religious exemption from Gov. Jay Inslee’s COVID-19 vaccine mandate for state employees, the university in October 2021 fired Rolovich.
At the time of his firing, Rolovich was subject to a five-year contract with three seasons remaining and was paid $3.2 million per year — the highest public salary in the state. He had coached 11 games with the Cougars over two seasons.
Rolovich’s attorney, Brian Fahling, said at the time his client would take legal action for religious discrimination. He filed a 34-page letter with the university appealing the university’s decision to fire Rolovich, but the appeal was denied.
Rolovich, a Catholic, is not the first person to file a claim for wrongful termination or religious discrimination over an employer’s failure to grant a religious exemption to a COVID-19 vaccine mandate.
Liberty Counsel on July 29 settled the nation’s first class action lawsuit on behalf of healthcare workers who were unlawfully discriminated against and denied religious exemptions to the COVID-19 vaccine mandate by their employer, Chicago-based NorthShore University HealthSystem.
The $10,337,500 settlement, filed in the federal Northern District Court of Illinois, compensates NorthShore employees who were “punished for their religious beliefs against taking an injection associated with aborted fetal cells.”
As part of the settlement agreement, NorthShore also will change its unlawful “no religious accommodations” policy to make it consistent with the law and must provide religious accommodations in every position across its numerous facilities.
In addition, employees who were terminated because they refused to receive a COVID-19 vaccine on religious grounds will be eligible for rehire if they apply within 90 days of the final settlement approved by the court, and they will retain their previous seniority level.
The amount of individual payments from the settlement fund will depend on how many valid and timely claim forms are submitted during the claims process.
If the settlement is approved by the court and nearly all of the affected employees file valid and timely claims, it is estimated employees who were terminated or resigned because of their religious refusal of a COVID-19 vaccine will receive approximately $25,000 each.
Also under the settlement, employees who were forced to get the shot against their religious beliefs to keep their jobs will receive approximately $3,000 each.
The 13 healthcare workers who are lead plaintiffs in the lawsuit will receive an additional approximate payment of $20,000 each for their role in bringing this lawsuit and representing the class of NorthShore healthcare workers.
Lawsuits over denied exemptions or insufficient accommodations to COVID-19 vaccine requirements began last September after the U.S. Food and Drug Administration granted full approval to the Pfizer-BioNTech Comirnaty vaccine, allowing more employers to enact vaccine mandates.
Workers as of May 19, 2022, had filed at least 66 lawsuits since September 2021 against private employers for refusing to grant exemptions to COVID-19 vaccine requirements, according to Bloomberg Law.
Judges rejected workers’ requests for immediate court orders blocking enforcement of mandates in 22 cases.
In one case involving United Airlines Inc., the airline changed its policy allowing accommodations rather than contest the lawsuit.
According to Bloomberg Law, 59% of lawsuits filed over COVID-19 vaccine mandates are related to an employer’s response to faith-based requests for accommodation.
About 22% of lawsuits involve contesting a company’s handling of both religious and disability requests and 5% involve health-related accommodations.
Megan Redshaw is a staff attorney for Children’s Health Defense and a reporter for The Defender.
In this in-depth interview series with Kirsten Murfitt of NZLSOS, we highlight the key points and outline the crucial yet-to-be-answered questions from Kirsten’s excellent Open Letter to Parliament, which she penned on 22 July 2022. This is Part 1.
Please share this interview. Please also utilise the steps involved at the end of the interview in order to put pressure on the government to answer our important questions:
The 3 main questions are:
1.) Why doesn’t the Government require mandatory reporting of deaths and serious adverse reactions, following the administration of a vaccine which has only provisional approval?
2.) Why does the Government refuse to investigate the safety and contents of the vaccine, given both the emerging overseas data and the court-ordered release of Pfizer’s documents?
3.) Why did the Government market the vaccine as “Safe and Effective”, when it knew that neither of those statements was true?
By Daniel Ken | TCW Defending Freedom | May 20, 2023
Over more than two decades in the classroom I’ve taught thousands of children and teenagers: some were lovely and lots were hard-working. On the other hand, quite a number were disruptive and argumentative, and a number were violently opposed to learning. But I don’t think I’ve taught more than a handful of kids who could be properly described as having the symptoms of ADHD. And that handful could just as easily have had something else wrong with them. Because here’s the thing: despite the fact that the best part of a million children are medicated for the condition, ADHD doesn’t exist.
There’s no definitive medical test for it, experts can’t agree on what it actually means, and most of the symptoms disappear if the child in question has lots of exercise, good diet and, crucially, a set of clear behavioural boundaries, preferably set early in childhood and, for the boys at least, enforced by a stable adult male living at home. … continue
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.