We have written about this topic of no COVID-19 vaccination for children several times, raising our strong objections against vaccinating America’s children with the current COVID-19 vaccines, and our work was previously published in the American Institute of Economic Research (references 1, 2). Our core thesis for this op-ed offering encompasses a resounding “NO” against vaccination of children for COVID-19. There is zero science to support this, and there is potential serious harm. It is as simple as that. The benefits do not outweigh the harms, and the CDC and Dr. Fauci, and all who are pushing vaccinating our children with this set of COVID-19 vaccines are being very reckless, unscientific, specious, and dangerous with regard to our children. We call on them to reverse course. We argue that it is very dangerous and reckless to push to vaccinate low-risk children with untested vaccines for safety that could leave children with decades of severe disability if something goes wrong.
We make our argument now and we make it based on ‘No liability incurred by the CDC, NIH, FDA, and vaccine developers translates into no trust by parents’. Parents want to trust what is being done in this regard but how could they at this time when there is no basis for the vaccine? We ask the CDC in general, NIH, FDA, Dr. Fauci, the CDC’s new Director Walensky, and vaccine developers, to show us the evidence, show us and the public the data they are looking at, the science they are looking at, to warrant vaccinating our children. We can see none, we found none. If such exists, we certainly want to see it, if they would like to share it. These so-called ‘medical experts’ make statements and take positions often with no evidence or science to support what they are saying. In this case, we say no more. We want to see the evidence before we vaccinate our children.
Mask Mandate for Children
Firstly, let me/us be as clear as we can. All face masks must be removed from all children immediately unless you are a high-risk child and this is needed. Other than that, all other children, in the US, in Canada, Britain, France etc., all, must immediately rip up the masks and go on with life freely. Throw them away, they are not needed for our children. Nor is social distancing and definitely not in school. It is ridiculous. The CDC and the television medical experts, these talking head senseless and highly illogical people in these Task Forces like Fauci and Birx, have become (and became) contemptible with the drivel they spewed at the public 24/7 about these masks that are ineffective (they do not work and never worked, they just cannot as used) and very harmful. These experts in the CDC, NIH, FDA etc. costed jobs, businesses, and even lives with their corrupted pandemic response—denying early treatment when it existed. Especially the lives of our African-American and minority young people and children who could have least afforded the specious, unscientific, and unsound lockdown edicts.
Many good people and children lost their lives in desperation due to the crushing harms and devastation from the lockdowns and school closures that continue even today due to the CDC and the AFT teachers’ union collusion. Our statements on masks pertain to adults too but our focus here is on our children today, and urgently. These CDC, NIH, and similar agency and medical experts and advisors are all clueless, disgraceful, hysterical, illogical, irrational, specious, and patently absurd. Pure nonsense has been showcased with these masks mandates that they know do not work. After 20 minutes, they are garbage with the moisture they accrue. These CDC and NIH etc. experts reveal a depth of academic sloppiness and cognitive dissonance to any real science or anything that does not line up with their twisted unsound politicized narratives.
We always knew this. They the CDC, have never followed the science on masks as the science says it is junk and useless but do not tell “CDC 365” this (as described below). The surgical and cloth masks are and were all junk. We knew the science, reported it repeatedly, and spoke to it. How insane are these CDC experts? How embarrassing that they are the marque agency, and I am hoping the CDC can return to its former days of glory for at present, it is a non-scientific, pseudoscientific clubhouse for inept political representatives. The CDC does not do science, it does politics. The CDC is like the furniture store where with payment options, you do not pay for one year; you may think you are buying furniture, but they are really selling you ‘money’. You may think you are reading a scientific report from CDC when in fact, it is a political report.
Questions for Our Leaders
We open this op-ed with seven urgent questions for Dr. Fauci, Dr. Walensky (CDC’s Director), the NIH’s Dr. Collins, and the FDA, as well as the vaccine developers:
1) Would Dr. Fauci and Dr. Walensky as well as Dr. Collins of the NIH sign paperwork placing liability on themselves (their agencies) should any child be harmed or die from these vaccines?
2) Since the risk of Covid-19 infection is less than 1% and the Pfizer vaccine reduces the risk of infection by only 0.7% (absolute risk reduction), why are we vaccinating children with a non-FDA approved vaccine that is currently on EUA when their survival rate from Covid-19 is 99.997% according to the CDC? Near zero risk of severe illness or death. So, what is the benefit?
3) We have not seen any clinical trial data for children 12-15? Can we see it, can the public see it? What is the Absolute Risk Reduction measure, NOT the relative risk reduction?
4). How can the vaccine recipients (children) legally provide Informed Consent? Informed consent is not just ‘hey you, roll up your sleeves’…
5.) How do you plan to inform vaccine recipients about the Antibody-Dependent Enhancement risk (ADE) and similar risks, for if not properly informed of these “non-theoretical and ‘real’ compelling” risks, it violates medical ethics standards?
6.) Since studies show that those who have recovered from Covid-19 are at a greater risk of a severe vaccine reaction if they took the vaccine, do you plan to conduct antibody testing first of our children, to see if they have already been infected with Covid-19?
7). Are you aware that the vaccines cannot prevent infection or stop the spread according to Pfizer’s clinical trial data, and Topol/Doshi (New York Times )… it is and was only set up for mild COVID… nothing else… no transmission, no infection, no severe illness, no hospitalization, no death… so if children can get immunity harmlessly and naturally, and are at such low risk of spreading it or getting ill or dying, what is the benefit? It cannot be to drive herd immunity numbers for if you consider cross protection from common cold coronavirus and immunity from prior COVID infection that is cleared, then you do not need children for this… so why place our children at such unnecessary risk?
If our children are to take a vaccine that is not needed based on their risk (a child’s) of becoming infected and spreading the infection or becoming severely ill (and this is clear, stable global science), and a vaccine with questionable efficacy and very real potential harms based on emerging CDC VAERS adverse reporting database reports and anecdotal reports, then the CDC, NIH, FDA, and vaccine developers must take on the risk and consequent liability if our children are harmed.
Must be Held Accountable
We are vehement, that if any child dies or is harmed by these vaccines, then the CDC, NIH, FDA, Dr. Fauci, etc. must be held accountable. The CDC, NIH, FDA, and vaccine developers must be willing to immediately take on the risk if they stand by these vaccines for this is the safety of our children we are talking about. They must be willing to be accountable and put skin in the game. This is a very different situation than that for adults. No liability by the CDC, NIH, FDA, and vaccine developers equals no trust from parents and the public when it comes to our children. As a risk management question, we see no benefit from this vaccine and only potential downsides.
We consider vaccinating children for COVID-19 as dangerous and reckless, as reckless as the recent administering of this set of vaccines that lacks proper safety data, in pregnant women as per CDC’s guidance. We have read the enabling study and it raises many questions particularly the key one being the optimal time duration of study conduct was not done. How do you assess harms for a drug or medical device or vaccine when you are running studies for roughly 4 months? How? It is not possible. Safety signals (especially rare) cannot emerge during this time nor the optimal sample size for study (or event numbers). Where is the correct comparative group to assess the impact of vaccination on pregnant, vaccinated, positive women? Moreover, the initial decision for EUA for the vaccines was based on very small event numbers e.g. one key study had 170 events (162 placeboes and 8 in the intervention arm). This is incredible that such small event numbers enabled EUA for vaccinating hundreds of millions/billions of persons.
Many Questions Raised, With Little Answers
The vaccine trials have raised many methodological questions and we are concerned given the reports of over 3,000 participants’ data being omitted in one study as they were ‘suspected’ but not ‘confirmed’ positive. We find this incredible especially how there is no full accounting by the vaccine developers of why this was done, and when we back calculate and do our own crude modeling, we find the efficacy declines from the reported 95% to 19-20%.
But here is the core issue as we look at the risk for children and this obsession by Fauci and Walensky to vaccinate our children:
i) children do not acquire it readily e.g. studies show less ACE 2 receptors in nasal epithelia
ii) children do not readily spread infection to other children
iii) children do not spread it readily to adults, it is the other way around
iv) children do not readily take it home; arises mainly from home clusters and the adults there
v) children do not become severely ill
vi) children do not die from it
vii) MISC is very rare, very treatable, and almost all leave the hospital… could it be that masking and locking kids down have driven MISC? how come nations with no lockdowns do not report MISC? or strong children masking?
So, given all of this, what is the benefit of vaccinating kids? It cannot be that kids are needed to drive herd immunity threshold for it can only be that, if you disregard cross protection that exists from prior common cold coronavirus, and also that there is existing immunity from persons who had COVID infection and cleared it. So, once you include those portions in the math, there is no need for children to achieve herd immunity, that’s a bogus reason, Dr. Fauci.
Children & the Risk of Spreading Infection
Let us for a moment, look at the issue of masking of our children and when outdoors. This will help demonstrate the ludicrousness and harmfulness of the CDC and what it is advocating for in vaccinating our children. The CDC’s guidance raises serious questions if harms emerge and comports itself to ridicule as much as wearing mask outdoors if vaccinated. As we view the CDC guidance from an eagle-eye perspective, we come to a conclusion that the CDC is not talking science anymore. It is purely nonsensical and confusing. For example, regarding the risk of outdoor transmission, the CDC knows of the Chinese study that showed only one of 7,324 infection events following careful contact tracing was linked to outdoor transmission. They, the CDC, know that the Irish analysis showed that only one in 1,000 infections out of 232,000 infections were linked to outdoor transmission. They know that outdoors has ample ventilation and thus spread is virtually non-existent (CDC originally reported that less than 10% of infection occurs outdoors and one is near 20 times more likely to be infected indoors than outdoors; however CDC’s 10% figure was inaccurate and proper research shows this to be 0.1% and CDC has now backtracked due to their startling error on outdoor transmission).
There remains an absence of evidence supporting the notion that children even spread the COVID-19 virus in any meaningful way, but there is direct evidence showing that they simply do not spread this infection and disease! This has been shown in school settings and as published in other papers. Children typically, if infected, have asymptomatic illnesses. It is well-noted that asymptomatic cases are not the drivers of the pandemic; something particularly important in relation to children as they are generally asymptomatic. A study published in the journal Nature found no instances of asymptomatic spread from positive asymptomatic cases among all 1,174 close contacts of the cases, based on a base sample of 10 million persons. The World Health Organization (WHO) also made this claim that asymptomatic spread/transmission is rare. This issue of asymptomatic spread is the key issue being used to force vaccination in children. The science, however, remains contrary to this proposed policy mandate.
Supporting Evidence
In terms of masking children, which we are vehemently against (in school or out of school), Ludvigsson evidenced the low risk in children by publishing this seminal paper in the New England Journal of Medicine out of Sweden on COVID-19 among children one to 16 years of age and their teachers in Sweden. From the nearly 2 million children that were followed in school in Sweden, it was reported that with no mask mandates, there were zero deaths from COVID and a few instances of transmission and minimal hospitalization.
Similarly, a high-quality robust study in the French Alps examined the spread of the COVID-19 virus via a cluster of COVID-19. They followed one infected child who visited three different schools and interacted with other children, teachers, and various adults. They reported no instance of secondary transmission despite close interactions (to any child or teacher). These data have been available to the CDC and other health experts for over a year. It is not ‘new’ evidence as the CDC seems to allude to. We have science on deck for near 14 months now and the CDC is clearly out of step with the science. Each turn we make. Why?
They, the CDC, also know of a high-quality review study by Madewell published in JAMA that sought to estimate the secondary attack rate of SARS-CoV-2 in households and determine factors that modify this parameter. The study was a meta-analysis of 54 studies with 77 758 participants. Secondary attack rates represented the spread to additional persons and researchers found a 25-fold increased risk within households between symptomatic positive infected index persons versus asymptomatic infected index persons. “Household secondary attack rates were increased from symptomatic index cases (18.0%; 95% CI, 14.2%-22.1%) than from asymptomatic index cases (0.7%; 95% CI, 0%-4.9%)”. This study showed just how rare asymptomatic spread was within a confined household environment.
The CDC also knows of a high-quality randomized controlled trial Danish Study published in the Annals of Internal Medicine sought to assess whether recommending surgical mask utilization outside of the home would help reduce the wearer’s risks of acquiring SARS-CoV-2 infection in a setting where masks were uncommon and not among recommended public health measures. The sample included a total of 3,030 participants who were assigned randomly to wear masks, and 2,994 who were told to not wear masks (i.e. the control arm). The authors concluded that there was no statistically or clinically significant impact of mask-use in regard to the rate of infection with SARS CoV-2.
As a result of the nonsense guidance by the CDC, Dr. Leana Wen (emergency physician and public health professor at George Washington University; former Baltimore City Health Commissioner) has just about had it with the nonsensical capricious CDC guidelines and is reportedly shocked’ by new CDC Mask Guidance and rightly so. “They went from this overly cautious, nonsensical approach to another nonsensical approach — but one that is dangerous, one that throws caution out the window”. We agree, what the CDC is putting out is utter nonsense and actually dangerous. Dr. Marty Makary (Johns Hopkins) has also weighed in stating that this is the “most political CDC in history”, where guidance is “based on discretion not science”. We argue, CDC guidance is based on whimsy and is as far removed from science as possible.
Even the Wall Street Journal (WSJ) is now saying to take off the mask when outside. The WSJ knows that the gig is up with the ineffective masks but also that it is insane to consider masking outdoors when it is properly ventilated and the risk of spread is near zero, if at all. It is insane, illogical, irrational, and pure nonsense that the CDC and Dr. Fauci are advising children and teenagers to wear masks at summer camp, but not if they are vaccinated. It defies logic what is coming out of the CDC at present as to scientific guidance.
Disastrous Public Policy
It is incredible that a marque public health agency like the CDC could be making such disastrous public policy statements and guidance when they are constantly flat wrong and constantly having to reverse them or adjust them. What is going on at the CDC? We want the CDC to succeed and shine and be the ‘go to’ public health agency. But how could they, the CDC, provide guidance that masks are needed outdoors even ‘if vaccinated’. The totality of their argument remains meritless and absurd to date. It is nonsensical. We have argued that masks as currently used, the blue surgical and white cloth masks (or any cloth masks) are ineffective and essentially worthless. It is actually harmful and particularly for our children. We have raised this issue many times as to no benefit and possible harms of masking and it is catastrophic to our children, emotionally, socially, and health-wise. These masks do nothing and it is beyond being ‘neutral’, they are ineffective. It did nothing. Mask mandates have all failed. And now we refocus on the issue of vaccinating our children for COVID.
In this regard, the CDC knows (at least we would hope they do) that if fully vaccinated, if these vaccines do what they were purported to do by conferring sterilizing immunity (which we argue the vaccines fail to do), with the high titers of neutralizing antibodies, then you are effectively immune. You can toss your masks and you are liberated after your second shot. But do these vaccines really work as effectively as reported? Does the CDC know something that the public does not know, and hence the insistence on mask-wearing and distancing away from others, even if vaccinated? Ours is not merely a curiosity, but a legitimate question that remains without a scientific answer from the CDC. We are in full support of vaccines once developed properly with the proper safety testing.
We also find the current mechanisms being employed by the media and some people in shaming others for not being vaccinated is deplorable, while they take selfies and parade on the internet social media and denounce others. Why would you shame someone who is not vaccinated when you are fully vaccinated, if you are immune? If you are immune and, again, if you think you are, then why does it matter if someone else has not taken the vaccine, for they could be COVID recovered and have decided that they do not need the vaccine as they have robust and durable natural exposure immunity? They have this right to make a personal ‘informed’ decision. You are immune, so why be concerned with someone else’s vaccine status? Why infringe on others’ rights and freedoms and use public shaming as a venue to exploit your compliance.
Risk of Death?
But, what does the epidemiological data show as to the risk of death for children? Are children at such elevated risk to warrant vaccinating? Well, the most updated data by the American Academy of Pediatrics showed that “Children were 0.00%-0.19% of all COVID-19 deaths, and 10 [US] states reported zero child deaths. In states reporting, 0.00%-0.03% of all child COVID-19 cases resulted in death.” This is the data.
Based on reporting of CDC data, 266 children aged 0 to 17 years in the US have died of COVID-19 and we mourn each death and we cannot understand the pain for the grieving parents and family. But let us put this in perspective to yearly seasonal influenza. During the 2018-2019 influenza season, 477 children 0 to 17 died of the regular flu, and we did not mask the nation, did not close schools, and did not seek to mass vaccinate children, and did not push them to cower under their beds in fright. This is all so illogical and insane what they have done in terms of COVID-19! In 2019, 2,545 children died in traffic accidents, 776 died due to drowning often in their backyard pools by accident, and 2,156 died due to homicide. As a result, did we stop sending them to school? Did we pave over our swimming pools or ban the driving of cars? No, we have as a society accepted this level of risk and we have learned to live with it. Life goes on. We get up, dress, go to work or school, and we pray for each other daily that we get through the day and live to see another day and we make it home.
Esteemed Dr. Marty Makary out of Johns Hopkins weighed in with his expertise and appeared to suggest that children 12 to 15 years old should be vaccinated. We were surprised and disagree fully with Makary as the risk to these children which he also admitted, was essentially zero. Exceedingly rare. Then why would he advocate for vaccinations? This is confusing as we find no clear evidence, in fact none, that children are at any appreciable risk. He even stated that the ‘rare’ MISC inflammatory condition that is reported, typically ends with the children fully recovering. This is completely treatable also. Again, why would he recommend the vaccine when the risk is so low for severe outcomes and the children can develop natural robust immunity? The immunity conferred by this narrow ‘spike-specific’ immunity cannot provide the broad-based, robust, durable, comprehensive immunity that natural exposure immunity can.
This is basic immunology and the risk-management decisions for parents in our view suggests ‘no’ vaccines when there is no benefit and no potential for tremendous harms. There are adverse events and deaths being reported in the CDC’s own VAERS database due to the COVID-19 vaccines that the media medical cartel is not reporting. We find it is reckless and dangerous for CDC and Fauci and NIH to be advocating for these vaccines in children when they know there are no safety studies to rule out harms and what is planned cannot rule out harms.
At the same time, and we do applaud his bravery, Makary re-iterated that CDC has been ‘consistently late or wrong’ since the pandemic began and on most everything, and the latest CDC guidance on masks in summer camps and school reveals just how out of touch the CDC is with the science. We agree fully with Makary on this and advocate for a renaming of the CDC to ‘CDC 365’ given they are routinely at least nine months to one year behind the science! He claimed that we needed the updated guidance by Fauci 14 months ago. Overall, Makary says para CDC school guidelines are scientifically flawed and being used by Biden to stall reopening and appease teacher’s unions. We agree fully with this too! There is no sound, scientific, no good reason to keep schools closed, no sound reason to mask children in schools, and no sound scientific reason, none, no justification for children to wear masks indoors in school or in summer camps. It is illogical, irrational, hysterical, unscientific and actually absurd guidance by the CDC 365. As usual! What CDC and Dr. Fauci are advocating for in terms of children being vaccinated is dangerous and reckless in our opinion and has no basis, none!
Benefits Do Not Outweight Risks
We again argue that it is very dangerous and reckless to push to vaccinate low-risk children with untested vaccines for safety that could leave children with decades of severe disability if something goes wrong. We are for vaccines but they must be properly developed, and the emerging adverse effects and the lack of safety data raises serious concerns for these vaccines in children. The benefit just does not outweigh the risks and to claim that we need kids taking the jab to get to population-level herd immunity is absurd because you are not, Dr. Fauci and CDC and NIH, factoring in the natural immunity that already exists in the population, and you are not factoring in cross-protection from prior common cold coronaviruses etc. It is also very dangerous to mask our children. There is no basis for this, none! It defies basic common sense.
Thus, we cannot understand, once again, why public health agencies such as the CDC and Dr. Fauci, along with the nonsensical bureaucrats and technocrats would make such senseless statements and provide no basis for them, in that children require vaccination for prevention of COVID-19 when he and they know they are at little, vanishingly small risk! We have serious concerns about the safety of these vaccines for all persons (including questionable efficacy as it has been reported). Let us not pretend. Why? We applaud the tremendous feat under the Trump administration of seeking to bring vaccines in such a short period by cutting the regulatory red tape and circumventing and squeezing out the ‘dead’ time across the different phases of vaccine development. However, this does not obviate us from raising questions when there are troubling signs as to safety signals (rare or otherwise).
We are now seeing reports of the mRNA and adenovirus vector vaccines promoting blood clotting, blood disorders, various bleeding disorders, and that the spike protein on its own is potentially pathogenic. Besides the real documented adverse effects, there are also theoretical risks such as to the brain from lipid nanoparticles (LNPs) that will not manifest for years. Such that we may be mistakenly injecting people with a pathogenic protein. The AAPS has also stated that “blood Clotting Needs to Be Watched with All COVID Vaccines”.
No Liability Means No Trust
With this, the phrase we want the public to adopt is ‘no liability means no trust’ and by this, we mean that we want the FDA and Dr. Fauci, and the vaccine developers to remove the liability waiver from the vaccines for children. We waiver is one thing for adults but not for children given the low risk for infection and spread. The benefit does not outweigh the risk and if our children are being asked to take this untested vaccine, then the vaccine developers must have risk in the game. They must be willing to stand up for the vaccine and as such, be willing to attest to its safety by removing the liability waiver. This will give parents the confidence they need for as it stands, they have none. No liability means no trust in the vaccine. It is that simple. If the vaccine developers and all linked to the vaccine have no liability, then we can have no trust in it. Furthermore, the criteria for emergency use authorization (EUA) in children is not met and thus no EUA is warranted for children.
Building on this, Dr. Patrick Whelan (UCLA pediatrician) (Regulations.gov) shares our grave concerns especially regarding the nascent evidence about the pathogenicity of the spike protein the vaccine is injecting. In December 2020, Whelan warned the FDA that mRNA vaccines could cause microvascular injury to the brain, heart, liver, and kidneys in ways NOT assessed in safety trials. He stated, “I am concerned about the possibility that the new vaccines aimed at creating immunity against the SARS-CoV-2 spike protein (including the mRNA vaccines of Moderna and Pfizer–BioNTech) have the potential to cause microvascular injury to the brain, heart, liver, and kidneys in a way that is not currently being assessed in safety trials of these drugs”. Yes, we are concerned the vaccine developers have been less than forthcoming, and the government and their medical experts are being evasive with their statements. And we are now going to play with the safety and lives of our children? We say NO. No liability equals no trust.
An Uninformed Public
The public is not properly informed about the risks and the safety data is not there. It is just not there and we are being asked to trust? Trust who, the CDC? When on one day the CDC says you do not carry COVID virus if vaccinated then the next day having to retract it? When on one day they advise all pregnant women to get the COVID vaccine and then the next day say only if they are eligible to get it? The CDC has lost its credibility. No liability equals no trust. And what about ‘informed consent’? It is not simply “hey you, roll up your sleeve’.
Alarmingly, additional evidence is emerging that COVID-19 is less of a respiratory disease and more of a vascular disease with the ensuing ill effects all generally having vascular underpinnings. But we are arguing that the spike itself may be ‘potentially’ pathogenic and if it has a role in the damaging of vascular cells (damaging/impairing vascular endothelial cells via downregulating the ACE 2 receptor), then by injecting mRNA code to build the spike protein to derive an immune response, or injecting the complete spike itself, then we may be naively or unwittingly injecting the very deleterious spike protein that will wreak havoc on vaccinated persons. Potentially, but there is a real theoretical risk and some may argue, it is already unfolding based on the nascent reports of blood clots and bleeding disorders. The spike protein may emerge as one of the more damaging ingredients in COVID disease and we are giving it to people deliberately, unknowingly.
Whelan further reports “that ACE-2 receptor expression is highest in the microvasculature of the brain and subcutaneous fat, and to a lesser degree in the liver, kidney, and heart. They have further demonstrated that the coronavirus replicates almost exclusively in the septal capillary endothelial cells of the lungs and the nasopharynx, and that viral lysis and immune destruction of those cells releases viral capsid proteins (or pseudovirions) that travel through the circulation and bind to ACE 2 receptors in these other parts of the body leading to mannan-binding lectin complement pathway activation that not only damages the microvascular endothelium but also induces the production of many pro-inflammatory cytokines. Meinhardt et al. (Nature Neuroscience 2020, in press) show that the spike protein in brain endothelial cells is associated with the formation of microthrombi (clots), and like Magro et al. do not find viral RNA in brain endothelium. In other words, viral proteins appear to cause tissue damage without actively replicating virus”.
Whelan as a pediatrician, has gone even further and must be applauded for his bravery by stating openly that “before any of these vaccines are approved for widespread use in children, it is important to assess in vaccinated subjects the effects of vaccination on the heart… vaccinated patients could also be tested for distant tissue damage in deltoid area skin biopsies… important as it is to quickly arrest the spread of the virus by immunizing the population, it would be worse if hundreds of millions of children were to suffer long-lasting damage to their brain or heart microvasculature as a result of failing to appreciate in the short term an unintended effect of full-length spike protein-based vaccines on these other organs”.
As we consider the implications of the spike itself being potentially pathogenic (and this has to be further validated), we have argued prior against children vaccination for COVID and that the science is clear and settled that children do not transmit COVID-19 virus and that the concept of asymptomatic spread has been questioned severely, particularly for children. Children rarely get infected and biologically, it seems, based on nascent findings, they may be unable to due to less expression of the Angiotensin-Converting Enzyme 2 receptor (ACE 2) in their nasal epithelium (references 1, 2).
The accumulated evidence suggests that children have been less impacted than adults in terms of severity and frequency, accounting for <2% of the cases. Children (as opposed to other respiratory illnesses) do not appear to be a major vector of viral transmission, with most pediatric cases described inside familial clusters. There has been no documentation of child-to-child or child-to-adult transmission and this has remained the trend across the last 15 months of the pandemic and reported pediatric data. This was demonstrated elegantly in a study performed in the French Alps. The pediatric literature is settled science on this.
NO Vaccination of Children for COVID-19
This brings us to our core thesis, this being NO vaccination of children for COVID-19. The reality is that our stance on children getting COVID vaccines is similar to our stance on why children must not be forced to wear masks, and especially children as young as two years old. There is no science or data to support this, vaccine or masks. Whatsoever. Israel has now released data showing that all age group infections have declined substantially, while not vaccinating children under 16. Why? Could it be a clear example that children are not the drivers but rather adults are and that by protecting adults using vaccines, children are automatically protected? The Israeli data seem to provide clear evidence why vaccines are not needed in US children.
We have been arguing this and we ask, why would we do this to children then? Why would CDC and Dr. Fauci take such steps when they know that the safety testing will not be suitable and that our children will be at risk to these vaccines if they are not tested properly? We may be setting vaccinated persons up for a disaster, naïvely, and as such, could we be doing the same to our children? We call for an immediate stop! We must not expose our children to ‘unnecessary’ harm. We must not expose them to a substance that has not been tested on children (or plan to be adequately) in the way it should be and for as long as necessary. We cannot circumvent ‘time’ with elevated sample size or any other tactic. This is a nonsensical methodology. These vaccines must be studied for the appropriate length of time. We must not expose children to a vaccine that based on their risk is absolutely not needed. Moreover, they can become infected naturally, if their immunity is needed.
As such, we are asking for a pause on vaccinating all persons with these vaccines until we understand what is emerging and safety is fully declared. Yet beyond that, we find it so very repugnant and dangerous an idea to submit children to these untested vaccine platforms, that once again we realized that we had to take a stand against testing and/or provision of any of the current vaccines for SARS-CoV-2 in children. Moreover, our view is that the risks of the vaccine far outweigh the benefits of persons under the age of 50, and we even argue up to 70 years of age. There should be no coercion or threat of reprisal if one does not want to be vaccinated and we call for a mass suspension of the vaccination in the US and maybe worldwide to assess the serious safety concerns we have. We are calling for proper ‘informed consent’ for all who decide to take the vaccine. We are being threatened when we raise this issue of safety and we are trying to inform the public.
We find it disturbing that the media has never pressed Dr. Fauci on overtly erroneous assertions and other major self-contradictory statements and continues to let him express an opinion without a deeper probing. We have great respect for his career and his bench work, but he is highly inaccurate and out of step with the science on most things COVID-19, the immunology, and the vaccinology, and I/we do not pretend to be any level of expert. Given what is at stake here now, this being the safety of our children, we felt we should take a stand and demand more. If this goes wrong as we think the potential is certainly there and based on what we are seeing with the adult administration of the vaccine, then our children may be left with a lifetime of morbidity, disability, and far worse, death. We demand that Dr. Fauci layout the childhood vaccination evidence for the scientific community (and the public, the parents) to evaluate.
Runinng Behind, and in the Wrong Direction
That said, we are being declarative in our position that our public health agencies like CDC, NIH, and FDA are running 9 to 12 months behind contemporary data and science and are routinely wrong. Dr. Fauci and CDC are wrong on the vaccination of children science as they were on all of the catastrophically destructive societal lockdown, school closure, and mask/mask mandate policies they advocated and implemented. We believe that the currently promulgated policies by the CDC and Dr. Fauci concerned with vaccinating pregnant women is both reckless and perhaps dangerous, since no long-term data exist on the mother or the fetus and the potential ill effects from mRNA and adenovirus vector vaccines. We believe they are wrong as it relates to our children as well, with these sub-optimally developed vaccines that are largely long-term safety untested and being administered as ‘investigational’ under the Emergency Use Authorization (EUA) without the time-tested and honored Biological License Application.
For example, in the Daily Herald article, whereby Dr. Fauci advocates for kids as young as first-grade to be vaccinated by September 2021, he was quoted stating when asked about vaccinating by September 2021, “I would think by the time we get to school opening, we likely will be able to get people who come into the first grade.” We find this by Fauci to be incredibly dangerous and without any merit. Is Dr. Fauci thinking clearly? We believe that the very low circulating virus especially among children prevents a proper study from being undertaken conclusively and would require a large “n” to get meaningful results. The study will also not be conducted for the proper duration to collect the safety data.
The article expressly admitted it will not be possible to do this by stating, “Since children rarely are hospitalized due to COVID-19, the vaccine’s ability to reduce severe cases would be hard to measure unless the trials enrolled an enormous number of children”. The potential harms to the children must always be considered for any intervention in children. This must not be construed as an anti-vaxxer stand, but a sane and logical argument that must be meted out with the requisite intellectual curiosity and scientifically proven evidence. We, therefore, call for no vaccine for our children in this illness and we only discuss this option after we have properly collected long-term safety data collected from children and including safety data from adults.
Current Vaccination Indications & Supporting Evidence
Currently, in the U.S., the vaccine is indicated only for those ages 16 and up. The article referred to several pediatricians and infectious disease experts opining that “vaccinating children is essential to helping the country, as a whole, reach herd immunity and decrease the threat of new variants”. This is a dangerous and inept statement. The global evidence is quite settled that children do not spread the infection or get severely ill if infected, and that they can become immune naturally with regular exposure that is natural and harmless. If children ‘numerically’ are needed to achieve population-level immunity, then why would they not be allowed to achieve immunity naturally, that confers robust protection e.g. T-cell immunity, for many years? Why expose them to an untested and potentially unsafe vaccine that could damage them lifelong? Moreover, we argue that their math is clearly wrong for they routinely discount the contribution made by prior exposure to coronaviruses (common cold) and thus the cross-protection they already have (T-cell immunity). They also discount in their math the vast amount of immunity that prior exposure and recovery from COVID-19 confers. Thus, the nation and states are potentially near or at herd immunity already.
Currently, we have no evidence that any variants are more lethal and the real issue with the variants is the mistake in making vaccines with a very narrow ‘spike-specific’ immunity. Selection pressures from the vaccine as well as from the natural immunity will cause mutations to continue to happen at a pace commensurate with the replicative ability of the virus. A broad natural immunity is more desirable as protection so long as there is minimal risk involved, as we believe is the case with children.
We are very concerned that the American Academy of Pediatrics has been pushing this childhood vaccination and “really advocating to try and make these trials happen with the same urgency that they happen for adults”. This is very troubling and we ask, do they read the science that is available and that has accumulated on the risk to children? Is the Academy of Pediatrics willing to take this safety risk with our children?
The article states that we are mistaken in thinking that children were immune from SARS-CoV-2. We never said this and we do not think anyone has meant this, for what we did state and still strongly believe is that the risk for children is very small, exceedingly rare in all aspects of this virus and illness (acquiring the infection, spreading it to other kids and to adults, and becoming seriously ill). “Children experience lower infection rates, accounting for less than 10 percent of cases in the United States”. If Dr. Fauci and the CDC think otherwise, again, we request such information to be made public. Stating that children spread the virus “to some extent” is grossly misleading. The CDC, Dr. Fauci, and the writer of this slanted inaccurate piece know that this should have been stated as ‘vanishingly small or exceedingly rare, if at all.’ These people know that evidence from Sweden with fully opened schools showed no significant evidence of spread and no deaths.
Key Drivers of SARS-CoV-2
In this regard, it is evident that neither children (nor asymptomatic adults) are the key drivers of SARS-CoV-2. In the rare cases where a child is infected with SARS-CoV-2, it is exceptionally rare for the child to get severely ill or die. And to reiterate, teachers are not at risk of transmission from children and schools are to be reopened immediately with no restrictions. Schools remain the safest place for children and teachers. They should have never remained closed and we knew this for 15 months now, and our children are being harmed by the unholy alliance between unions and government leaders in certain states. The New York Post recently reported of this relationship whereby the Teacher unions have a hand in the devising of CDC school re-open policy. “Emails show a call between Walensky and Weingarten — the former boss of New York City’s United Federation of Teachers — was arranged for Feb 7. The lobbying paid off. In at least two instances, language “suggestions” offered by the union were adopted nearly verbatim into the final text of the CDC document”. However, despite what the media and the CDC and unions are trying to tell the public, the pediatric literature suggests that this is now settled science as to low risk in children. This is not ‘new’ evidence, this has been settled for over one year now, and certainly since last fall 2020.
Dr. Sarah Lang stated para that the issue of children not being in school will be solved if they got immunized. We find this to be reprehensible for this is a blackmail of parents when the children are being denied schooling with no basis due to risk, but by both the Teacher’s unions and the respective state governments and the federal government. Exact words were “Our current chaos about children not being in schools is just terrible for children, and I think a lot of the concern would be assuaged if children were immunized”. We would ask Dr. Lang if she will like to state conclusively that the vaccines as currently devised are ‘safe’ and what is planned will be safe, knowing what is currently occurring in terms of the emerging adverse events and deaths due to the vaccine. Is she prepared to place our children at this unnecessary risk?
O’Leary also stated para that as young as 6-month-old infants can get vaccinated. He knows that the trials will not be powered to detect meaningful differences (a sample size of 3,000 will not allow for the statistical power) and that the duration will not allow for assessment of safety. What this expert has stated is very dangerous. “That’s enough to prove safety and benefit, experts said, in part, because the adult trials have already paved the way”. We find this statement to be incredibly flawed science and dangerous given there are now emerging adverse effects of the vaccines and also, Pfizer as an example, failed to include over 3,000 suspected but unconfirmed infections (with no explanation) and our own calculations showed that the efficacy for mild COVID would have dropped from 95% to 19% if this omitted data was included.
The article reported, “In the absence of a definitive immune correlate of protection, the trials would compare antibody levels in children with those found in adults and extrapolate that the efficacy should then be similar”. We argue that children are not adults and their biological response will differ and we must not extrapolate especially given the harms we see accumulating with these vaccines. Children are still in a growing phase when their brain, neural, vascular and other systems are developing and thus may be subject to developmental anomalies from these untested vaccines.
The article reported that “Pfizer’s and Moderna’s adolescent trials will focus on evaluating participants’ immune response by measuring antibodies”, and it is likely the trials with younger children will do the same. We ask the vaccine developers and Dr. Fauci, do they think this is an appropriate end-point? We do not, and feel that this does not tell us if the recipient will be protected from infection or from acquiring infection, or from getting seriously ill or dying from it. This in no way tells us if the recipient will be immune once vaccinated. This is what parents will want to know if they are going to make a risk management decision to give their child this vaccine. This again raises many questions as to how these trials will be run, what the end goal is, and why the vaccine is needed in our children in the first place.
The article reported, “In the absence of a definitive immune correlate of protection, the trials would compare antibody levels in children with those found in adults and extrapolate that the efficacy should then be similar”. We argue that children are not adults and their biological response will differ and we must not extrapolate especially given the harms we see accumulating with these vaccines.
It is unfortunate that we have arrived at this stage where untruths are elevated to a daily briefing.
And these daily briefings cause irrational fear, panic, and hysteria among the public. These briefings driven by the media cause unnecessary fear despite “a thousandfold difference in risk between old and young.” Such conflation of the risks between the young and the elderly population with comorbidities and at risk is wrong-headed and creates unnecessary fear for all. It is well known that there is a distinct stratified risk (strongly associated with increasing age and comorbidities).
Ending Statements
We end by again stating that the recent push by the CDC, Dr. Anthony Fauci, and other television medical experts who suggest that we can only get to herd immunity by vaccinating our children is absurd and patently false. They continue to inaccurately discount cross protection immunity from prior coronaviruses and common colds. They are pushing a vaccine that is potentially unsafe to our children especially since we have no data on their safety.
Furthermore, data thus far suggest that the COVID ‘variants’ do not drive infection in children and harm them any more than the original strain. There is no basis for such a statement. For those who are trying to frighten parents by the illogical and absurd statements that a lethal strain may emerge among the variants, then we argue that you are using terms like ‘may’ and ‘could’ and ‘might.’ We can find no evidence to support such claims. It is simply rampant supposition and speculation and fear-mongering! Making such claims is not science, and decisions based on such claims are not evidence-based. We need to see the actual science and not just rampant speculation and supposition by often nonsensical media medical experts. We regard the retraction of the double-mask needs as a rampant abuse of the term “science-based.” Because it wasn’t as was the statement that Covid-19 is 10 times more lethal than the seasonal flu? A very prominent Professor out of Johns Hopkins, Dr. Marty Makary, gets it right now when he calls out these experts and agencies for their foolishness and fear mongering that is often inaccurate. He recently eviscerated CDC’s guidelines and called out Dr. Fauci for his inaccurate claims on herd immunity.
We advocate for the safety of all our children. Parents have a responsibility to ask for and get accurate information from the public sector that governs policy decisions. Parents, so armed, can make appropriate decisions for their children. It is better science to use a more ‘focused‘ protection and targeting that is based on age and known risk factors especially, regarding the children. We abide by the Hippocratic principle of “Primum Non Nocere.”
We conclude that our children must be exempt fully from any of the existing COVID-19 vaccines, and until proper studies are conducted with the proper safety data, and until it can be shown that the benefits far outweigh the risks in the need for the vaccine. There must be no vaccination of our children with these potentially unsafe, untested for safety vaccines. Period! No liability equals no trust and we close by again calling on the CDC, the NIH, the FDA, Dr. Fauci, and vaccine developers to remove the liability waiver. There is no benefit. None. In fact, we call on the CDC, the NIH, the FDA, Dr. Fauci, and vaccine developers to meet with us at any time, to their convenience, collectively or however, to discuss with us, debate with us, why our children should be vaccinated with these vaccines given their risk. We wish this open public discussion to your convenience.
Contact
Paul E. Alexander, PhD … email: elias98_99@yahoo.com
Howard Tenenbaum, DDS, PhD … email: hctkbt822@gmail.com
Parvez Dara, MBA, MD … email: daraparvez@gmail.com
i) Paul E Alexander MSc PhD, McMaster University Canada, University of Oxford, and University of Toronto
ii) Howard Tenenbaum DDS, Dip. Perio., PhD, FRCD(C) Centre for Advanced Dental Research and Care, Mount Sinai Hospital, and Faculties of Medicine and Dentistry, University of Toronto, Toronto, ON, Canada
iii) Parvez Dara MD, FACP, MBA, Consultant, Medical Hematologist and Oncologist
May 20, 2021
Posted by aletho |
Corruption, Science and Pseudo-Science, Timeless or most popular | CDC, COVID-19 Vaccine |
Leave a comment
THERE was a time in the not-too-distant past when our freedoms were predicated on the vulnerable being vaccinated. This was the limiter which justified the continuation of draconian measures into winter after Christmas was stolen. Christmas was stolen to save January. November was stolen to save Christmas. They told us in October that if we didn’t lock down then we would face 4,000 deaths a day. A number they knew at the time to be a gross overestimate. They used it anyway.
We now know unequivocally that we are victims of this government’s unethical psychological campaign of coercion. We know many loved ones believe their relatives’ deaths were falsely certified as Covid deaths on presumption and not evidence. And that a quarter of recently attributed deaths were not caused by the virus. I am still incredulous at the statement ‘deaths of any cause within 28 days of a positive Covid test’ as the caveat to daily reported figures.
We have simply lost our minds.
Of course no one wants to get Covid. Like any seasonal flu it has the potential to be nasty. But it remains a relatively insignificant virus for the vast majority of the population. Despite an average death age for the disease (82) higher than population life expectancy (81), we have been forced to endure an endless campaign of mendacious claims and impositions justified with empty promises.
Now the end of the long and ‘irreversible’ roadmap (which has for several months been at odds with the once solid claim of ‘data not dates’) is being re-framed before our eyes with Sage claiming the possibility of 10,000 hospital admissions per day in July and restrictions continuing beyond June 21.
The justification for this new round of official caution, the ‘Indian variant’, has been promulgated with several weeks of distressing media imagery. Just a few weeks before a similar stream of distress was being transmitted from Brazil.
For those who want to balance the BBC’s scenes of mass graves in Brazil and funeral pyres across India, it may be worth researching these countries’ Covid deaths per million to gain some proportion.
For many of us the past six months has been psychological torture. Endless days of winter isolation leading to a half-life in spring. A persistent sense of atrophy has remained with the dull ache of forced containment. Small businesses placed into induced comas. The nation’s cultural treasures kept under lock and key. Human connection severed. Life’s potential suppressed.
If you are buying into the official narrative you are rewarded with a sense of moral vindication. Your sacrifice is for a greater national good. It’s bad manners to question the motives and morality of what has taken place. Or to entertain the idea that taking an unlicensed medical treatment may not be okay.
If, like me, you are uncertain about the jab for perfectly sensible and personal reasons, you may be preparing for the extraordinary reality that access to your ‘normal’ life, including the things you love, be it cultural, social or leisure, may soon be off limits. You may be wondering if your job is going to be at risk. And whether you will again be allowed to travel abroad.
The Covzealots are now rounding on those of us they label with ‘vaccine hesitancy’. We are determined to be a risk, so it seems fair game to consider people like me to be selfish, idiotic, anti-vaxxer-conspiracy-nuts. The ramping up against us has the signs of becoming a persecutory campaign.
For what it’s worth, I’ve spent eight years of my life in various volunteering roles. Supporting the elderly, the mentally ill and young people. I’m as fallible as the next man. But I’m not going to take lectures on morality because I won’t be bullied or coerced into compliance by the state.
If you are observing the official narrative, you have seen the pattern. You were well prepared for the approaching about-turn on restriction easing. You were prepared for the forthcoming drive to vaccinate children (I was shocked when they announced the recommendation for pregnant women) with a medical device which remains in its trial phase.
The propaganda bomb, created with sophisticated psychological techniques, deployed throughout the media and driven forwards by state activists in the press, has been designed to rattle even the hardiest among us. For many, the commonplace week or two of coughs, aches and sneezes has become the existential terror of ‘is this really it?’
Whilst I understand the power of fear, I cannot grasp how so many fellow citizens have become so blinded. There seem to be two branches of the same pro-Covid narrative playing out within the mainstream: willingness to excuse ‘Boris’ and therefore lend sympathy for his government’s vaccine nationalism, or anger at his incompetence, that enough wasn’t done at the outset, so the endless spiral of restrictions is necessary (according to the ‘experts’). Either way they work together to support compliance.
Before the Iraq war, I was shouted down for questioning an agenda where so many things did not add up. The dodgy dossier latterly proved doubters like me to be correct. The same people are shouting at me again. Many supposedly astute individuals seem to want to lend good faith to another state operation being supported by Tony Blair.
I wonder if those amongst us going along with a monumental attack on truth, freedom and individual liberty would see through the shoddy claims of the government Covid salesmen were they lent the autonomy to be the ‘rational actors’ Sage planners had originally determined the population should be treated as? We will never know.
May 19, 2021
Posted by aletho |
Mainstream Media, Warmongering | Covid-19, COVID-19 Vaccine |
Leave a comment
After rollout under emergency authorisation, manufacturers of covid-19 vaccines now have their sights on regulatory approval. But what’s the rush, asks Peter Doshi, and is just six months of data from now unblinded trials acceptable?
In April 2021, Pfizer and Moderna announced efficacy results at the six month mark from the phase III trials of their respective covid-19 vaccines.1 2
Pfizer CEO Albert Bourla said the company’s data “confirm the favourable efficacy and safety profile of our vaccine and position us to submit a Biologics License Application to the US FDA [Food and Drug Administration].”1 And on 7 May it formally initiated that application which, if successful, will earn the Pfizer-BioNTech product, BNT162b2, the distinction of becoming the first covid-19 vaccine approved by the FDA.
Because lest we forget, all covid-19 vaccines currently in use in the US are available under emergency access only.
(The situation is similar in Europe, where four covid-19 vaccines have been granted “conditional marketing authorisations,” a fast track mechanism that can be used in emergencies. These can be converted into standard “marketing authorisations” pending positive data after authorisation, but this has not yet happened for any covid-19 vaccine being administered.)
As hundreds of millions of people around the world get vaccinated, it may seem like wordsmithing to highlight the fact that none of the covid-19 vaccines in use are actually “approved.” Through an emergency access mechanism known as Emergency Use Authorisation (EUA), the products being rolled out still technically remain “investigational.”3 Factsheets distributed to vaccinees are clear: “There is no FDA approved vaccine to prevent covid-19.”4
The approval-authorisation distinction is often misunderstood by the media,5 even in the scientific press. But it was the focus of much discussion back in September 2020. With large phase III trials by Pfizer and Moderna well under way, and the November US presidential election looming, many worried about political pressure resulting in the rollout of an unsafe or ineffective vaccine.6
The FDA had already come under fire, accused of bending to the White House in granting EUAs for two covid-19 treatments, hydroxychloroquine and convalescent plasma. But those fears largely dissipated when the FDA published a guidance document in early October outlining its expectations for the EUA. According to the document, at least half of a trial’s participants would need to be followed for at least two months.7 This alone made it all but certain no vaccine could cross the line before the election.
The FDA also said it would want a vaccine at least 50% effective (with a confidence interval reaching no lower than 30%) against a primary endpoint of preventing SARS-CoV-2 infection or covid-19 disease of any severity8—parameters it had previously defined as necessary for approval. Even for non-clinical parameters, like manufacturing quality, the FDA characterised its expectations for the EUA as “very similar” to those for approval.3
Six months: enough?
One key difference between EUA and approval (also called “licensure,” and which for vaccines is known as a BLA (Biologics License Application)) was the expected length of follow-up of trial participants. Unlike its clear articulation of two months for an EUA, the FDA has not committed to a clear minimum for approval.
Cody Meissner, a professor of paediatrics at Tufts University and member of the FDA’s advisory committee, was curious. “Is it possible to predict or estimate when conditions of safety and efficacy might be satisfied for BLA?” Meissner asked at the agency’s 10 December meeting which had been convened to consider the FDA’s first emergency authorisation for the Pfizer vaccine.
The FDA’s Doran Fink responded: “I couldn’t predict, but I will say that we typically ask for at least six months of follow-up in a substantial number of clinical trial participants to constitute a safety database that would support licensure.”
An approval based on six months of data would represent one of the fastest for a novel vaccine in FDA history. Among the six “first in disease” vaccines approved by the FDA since 2006, pre-licensure pivotal trials were a median of 23 months in duration, according to a recent analysis.9
Six months also seems substantially shorter than previously conceptualised expectations. A World Health Organization expert group on covid-19 vaccines (which included FDA regulators) in August 2020 called for follow-up “until at least month 12, or until an effective vaccine is deployed locally.”10 Another group, composed of industry and academic authors, similarly wrote in October 2020: “we recommend longer term follow-up of all participants … for at least a year after randomisation.”11
On paper, the phase III studies by Pfizer, Moderna, and Janssen are all of two years’ duration. But the FDA’s official position on minimum follow-up before licensure is unclear at best.
In its formal guidance last June, the agency said that for licensure applications, it wanted participants followed for covid-19 outcomes for “as long as feasible, ideally at least one to two years”12 after the first injection. But the same document states that safety assessments for “serious and other medically attended adverse events” should be studied “for at least six months after completion of all study vaccinations. Longer safety monitoring may be warranted for certain vaccine platforms.”
Asked to clarify whether its guidance is asking for follow-up of at least six months or one year, a spokesperson told The BMJ: “We do not have any further information beyond what is in the guidance document.”
Unblinded and without a control group—what about safety?
Duration of protection is not the only question that longer, placebo controlled trials can address. They also address vaccine safety.
“Very often, it’s the fact that we have that placebo controlled follow-up over time, that gives us the ability to say that the vaccine didn’t cause something at a longer period of time after vaccination,” the FDA’s Philip Krause explained last December.13
Yet there is a gap—currently of unknown size but growing—between any expectation of blinded placebo controlled data, and the reality that within weeks of the vaccines receiving an EUA the unblinding of trials commenced as placebo recipients were offered the chance to get vaccinated.
Steven Goodman, associate dean of clinical and translational research at Stanford University, told the FDA in an invited presentation last December, “Once a vaccine is made widely available and encouraged, maintaining a double blinded control group for more than a nominal period is no longer in the investigator’s (or regulator’s) control and undue pressure to do so may undermine the entire vaccine testing enterprise.”14
Goodman’s recommendation was to rapidly convert the trials into crossover studies, enabling those on placebo to get vaccinated (and vice versa), while maintaining the blind. The companies challenged the feasibility, calling it “onerous,” and a crossover never occurred.15
The BMJ asked Moderna, Pfizer, and Janssen (Johnson and Johnson) what proportion of trial participants were now formally unblinded, and how many originally allocated to placebo have now received a vaccine. Pfizer declined to say, but Moderna announced that “as of April 13, all placebo participants have been offered the Moderna covid-19 vaccine and 98% of those have received the vaccine.”2 In other words, the trial is unblinded, and the placebo group no longer exists.
Janssen told The BMJ: “We do not have specific figures on how many of our study participants have received a vaccine at this time.” But the company confirmed it was implementing an amended protocol across all countries to unblind all participants in its two phase III trials, the earlier of which passed the median of two month follow-up mark in January.
How the FDA will weigh the loss of blinding and placebo controlled follow-up is unclear, but just months ago the agency said these trial properties were vital.
“Continuation of placebo controlled follow-up after EUA will be important and may actually be critical to ensure that additional safety and effectiveness data are accrued to support submission of a licensure application as soon as possible following an EUA. … Once a decision is made to unblind an ongoing placebo controlled trial, that decision cannot be walked back. And that controlled follow-up is lost forever,” the FDA said last October.3
At its next advisory committee in December 2020, the FDA reiterated the importance of the placebo group: “Placebo controlled follow-up can be very important in showing that whatever happened in the vaccine group also happened in the placebo group. Because that’s our best way of knowing.”13
What’s the rush?
The US’s “Operation Warp Speed” delivered on its promise to get a novel vaccine into arms in record time (box). Millions of doses of vaccines are being administered daily across the US, making clear that lack of FDA approval is no barrier to access. So just what benefit is there in seeking, and granting, a BLA?
The BMJ asked the manufacturers why they were seeking a BLA. Moderna did not respond and Janssen only confirmed it intended to apply for a BLA “later in 2021.” Pfizer likewise did not answer but instead quoted an FDA webpage on medical devices, which stated: “Sponsors of EUA products are encouraged to follow up the EUA with a pre-market submission so that it can remain on the market once the EUA is no longer in effect.”16 But EUAs have no built-in expiry date—in fact, 14 EUAs for Zika diagnostic tests remain active despite the public health emergency expiring in 2017.17
Cody Meissner told The BMJ he saw some distinct advantages of a BLA over EUA. An approved vaccine, for one, would provide “an element of assurance,” increasing public trust in the vaccines, particularly for those currently sitting on the fence. It would also pave the way for claims of vaccine injury to be routed through a more established compensation programme, and for adding the vaccine to government funded schemes to reach children in financial need.18 Finally, it may affect the potential for vaccine mandates: “It is unlikely these vaccines will be mandated while an EUA is in place. Remember that currently these vaccines are still considered experimental.”
While still under EUA, an increasing number of educational and other institutions have already mandated vaccines, but debates over the legality of these actions has hinged on the distinction between authorisation and approval.19
But approving a vaccine in order to legally support mandates or convince people of its safety arguably puts the cart before the horse. Meissner responded that a BLA would not be issued until the FDA is convinced of the short and long term safety of these vaccines.
No new biodistribution studies for covid-19 vaccines
Officials have consistently emphasised that despite shaving years off traditional timelines for producing vaccines, no compromises in the process were taken.20 However one type of study, tracking the distribution of a vaccine once injected in the body, was not conducted using any of the three vaccines currently authorised in the US.
Such biodistribution studies are a standard element of drug safety testing but “are usually not required for vaccines,” according to European Medicines Agency policy,21 which adds, “However, such studies might be applicable when new delivery systems are employed or when the vaccine contains novel adjuvants or excipients.”
In the case of covid-19 vaccines, regulators accepted biodistribution data from past studies performed with related, mostly unapproved compounds that use the same platform technology.22232425
Janssen told The BMJ its covid-19 vaccine leverages the same technology as its Ebola vaccine, which received licensure last June. “Our confidence in our adenovirus vector Ad26 is based on our experience with this vector.”
Pfizer and Moderna did not respond to The BMJ’s questions regarding why no biodistribution studies were conducted on their novel mRNA products, and none of the companies, nor the FDA, would say whether new biodistribution studies will be required prior to licensure.
Footnotes
-
Competing interests PD gave a public statement at the October and December FDA advisory committee meetings mentioned in this article (transcripts here: https://faculty.rx.umaryland.edu/pdoshi/#publications), and may continue to engage in public input towards regulatory decision making around covid-19 vaccines. PD is also employed by a university that has mandated covid-19 vaccines for all faculty, staff, and students. The views and opinions expressed here are those of the author and do not necessarily reflect official policy or position of the University of Maryland.
Peter Doshi, senior editor – pdoshi@bmj.com
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
May 19, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine, FDA |
Leave a comment
It’s called SM-102.
Verifying that it is in the Moderna COVID vaccine, I find a 12/30/20 CDC document titled: “COVID-19 Vaccines: Update on Allergic Reactions, Contraindications, and Precautions.” [1]
If you scroll down halfway through the document, you’ll see a chart titled, “Ingredients Included in mRNA COVID vaccines.” (pg 20)
The right-hand side of the chart shows ingredients in the Moderna vaccine. The fifth ingredient down is “SM-102: heptadecan-9-yl 8-((2-hydroxyethyl) (6-oxo-6-(undecyloxy) hexyl) amino) octanoate.”
Now we go to a document published by the Cayman Chemical Company of Ann Arbor, Michigan: “Safety Data Sheet acc. to OSHA HCS.” (04/11/2021) [2]
This data sheet lists the effects of SM-102. Here is the opening note: “For research use only, not for human or veterinary use.”
Far from comforting.
Then the safety data sheet lights up with adverse effects/warnings re SM-102. For example: “Suspected of causing cancer. Suspected of damaging fertility or the unborn child. Causes damage to the central nervous system, the kidneys, the liver and the respiratory system through prolonged or repeated exposure. Very toxic to aquatic life with long lasting effects.”
Several things to point out here. First, what dosage level of, and what duration of exposure to, SM-102 are we talking about? Details on these toxicity factors need to be known. HOWEVER, all that is overridden by the fact that SM-102 is being INJECTED into the body via the Moderna shot. We’re not just talking about inhalation or skin contact.
Obviously, the human body has layers of defense against attack. With injection, a number of those layers are bypassed.
And once deep within the body, where does SM-102 travel as it causes damage along the way?
I doubt that the Cayman safety data sheet even considered the possibility that SM-102 would be injected.
The experts and authorities will assure us SM-102 is safe. They’ll say only miniscule amounts are being injected. They’ll say the clinical trials of the vaccine revealed no problems. They’ll parrot, over and over again, as they always do: “safe and effective.”
You’re walking along a country path. You see a snake lying just ahead of you. He slowly raises his head and looks at you. On his hood, you read the words: “emergency use authorization granted.”
SOURCES:
[1] https://emergency.cdc.gov/coca/ppt/2020/dec-30-coca-call.pdf
[1b] https://www.youtube.com/watch?v=9RcgAXSKQyw
[1b1] https://youtu.be/9RcgAXSKQyw?t=638
[1b2] https://youtu.be/9RcgAXSKQyw?t=840
[2] https://www.caymanchem.com/msdss/33474m.pdf
May 19, 2021
Posted by aletho |
Timeless or most popular | COVID-19 Vaccine |
Leave a comment
THE problem with the Covid-19 vaccines is that we simply do not have enough information about their side-effects, and no one should be shamed (especially not by the President of the United States) or have their lives restricted for having this reasonable, wholly unselfish concern.
Such information does not exist at all for under-18s. The small-scale trials were designed only to test the vaccine on adults. Yet, largely because of media hysteria which has been recently accompanied by outright incitement, local officials have taken it upon themselves to start vaccinating 17-year-olds, citing the bogeyman ‘Indian variant’ in our midst.
The vaccine nudgers in government and the media, aided this week by a multi-million-pound YouTube ad campaign to persuade young people to get vaccinated, deliberately miss the point about the supposedly ‘extremely rare’ side-effects of these experimental vaccines, which include fatal blood clots in some cases.
The trouble is that if our ‘brilliant’ scientists knew nothing about the blood clots when the vaccine was first administered to citizens in December, what else don’t they know about?
Last week, the British regulator MHRA reported 41 new cases and nine more deaths as a result of one of these side-effects, a particular kind of clot known as cerebral venous sinus thrombosis alongside low platelets or thrombocytopenia. To date, there have been 209 cases and 41 deaths reported in the UK for the AstraZeneca vaccine alone. The first were reported in January.
According to an analysis of published MHRA data by Dr Hamid Merchant, a total of 532 ‘blood system events’, including 20 deaths, came through the UK’s Yellow Card system relating to the AstraZeneca jab between January 4 and March 14. There were thousands of non-blood-related reports besides.
Let’s recap on the public guidance regarding the AstraZeneca vaccine. First we were told ‘this vaccine is safe, get vaccinated.’ Then they said, ‘the benefits of this vaccine outweigh the risks, get vaccinated.’ Then the goalposts were moved further: ‘The benefits of that vaccine outweigh the risks if you are over the age of 30, but get vaccinated.’ And now, ‘the benefits of this vaccine outweigh the risks if you are over 40, but get vaccinated, or else!’
If this is how much ‘the science’ has changed in a few months, what will ‘the science’ be a year or two from now? What will we know in the future that cannot be established now? Scientists have not begun to discuss other fatal adverse reactions to have emerged, most significantly the neurological ones for which the AstraZeneca trials were paused.
If countries such as Denmark and Slovakia can suspend the rollout of a vaccine as a precaution, why are individual citizens stupid or callous if they decline the vaccine as a precaution?
In the United States, the government has recorded more deaths after Covid vaccinations than from all other vaccines administered in the country between mid-1997 and the end of 2013, as was reported by Tucker Carlson on Fox News earlier this month. Nothing to see here, of course.
Any reasonable government would have at the very least stopped blackmailing people into getting vaccinated by now. Instead, they have the brass neck to demand that we put our lives in their hands as if we owe it to them. Coerced vaccination is not merely mandatory vaccination, it is mandatory trust, both in government and in ‘the science’, whatever that is.
It is worth reminding those with short memories that tobacco was ‘safe’ for decades. The scientific community promoted smoking not only as safe, but healthy. They were, of course, assisted by celebrities, some of whom would later become senior politicians. And for some 50 years, the overwhelming majority of people were dumb enough to believe it. Who could have guessed that inhaling tar into your lungs twenty times a day, every day, for years, might be bad for your health? We see grim warnings about heart disease, lung cancer and infertility on cigarette packaging today only because scientific outliers of yesterday eventually overwhelmed the consensus with evidence.
More recently and more relevant to the present fiasco, the swine flu vaccine, Pandemrix, was declared safe by regulators in 2009. It was safe, for most. But for some 1,000 people, most of whom were not at any significant risk from swine flu, the vaccine triggered narcolepsy, a crippling chronic sleep disorder that leaves sufferers unable to stay awake. It was only after it was too late for them that the authorities conceded there was a link between Pandemrix and narcolepsy.
One of the victims of Pandemrix, 23-year-old Katie Clack from Peterborough, committed suicide in 2014 because her narcolepsy left her with ‘no quality of life’.
In 2018, the progressive news website Buzzfeed published a powerful feature about NHS workers who had their lives and careers ruined by the side-effects of the swine flu vaccine. Nurse Meleney Gallagher, who now has narcolepsy, told Buzzfeed: ‘I was pressured into it.’
That was in a different era. Earlier this month the same website published a slavish article with the headline: ‘15 anti Vaxxers who were roasted on the internet.’
If history is anything to go by, the idiots out there who think it’s acceptable to bully their vaccine-hesitant friends, colleagues, strangers and even close family are going to look very silly ten years from now.
May 19, 2021
Posted by aletho |
Science and Pseudo-Science | COVID-19 Vaccine, UK |
Leave a comment
New policies artificially deflate “breakthrough infections” in the vaccinated, while old rules continue inflating case numbers in the unvaccinated.
The US Center for Disease Control (CDC) is altering its practices of data logging and testing for “Covid19” in order to make it seem the experimental gene-therapy “vaccines” are effective at preventing the alleged disease.
They made no secret of this, announcing the policy changes on their website in late April/early May, (though naturally without admitting the fairly obvious motivation behind the change).
The trick is in their reporting of what they call “breakthrough infections” – that is people who are fully “vaccinated” against Sars-Cov-2 infection, but get infected anyway.
Essentially, Covid19 has long been shown – to those willing to pay attention – to be an entirely created pandemic narrative built on two key factors:
- False-postive tests. The unreliable PCR test can be manipulated into reporting a high number of false-positives by altering the cycle threshold (CT value)
- Inflated Case-count. The incredibly broad definition of “Covid case”, used all over the world, lists anyone who receives a positive test as a “Covid19 case”, even if they never experienced any symptoms.
Without these two policies, there would never have been an appreciable pandemic at all, and now the CDC has enacted two policy changes which means they no longer apply to vaccinated people.
Firstly, they are lowering their CT value when testing samples from suspected “breakthrough infections”.
From the CDC’s instructions for state health authorities on handling “possible breakthrough infections” (uploaded to their website in late April):
For cases with a known RT-PCR cycle threshold (Ct) value, submit only specimens with Ct value ≤28 to CDC for sequencing. (Sequencing is not feasible with higher Ct values.)
Throughout the pandemic, CT values in excess of 35 have been the norm, with labs around the world going into the 40s.
Essentially labs were running as many cycles as necessary to achieve a positive result, despite experts warning that this was pointless (even Fauci himself said anything over 35 cycles is meaningless).
But NOW, and only for fully vaccinated people, the CDC will only accept samples achieved from 28 cycles or fewer. That can only be a deliberate decision in order to decrease the number of “breakthrough infections” being officially recorded.
Secondly, asymptomatic or mild infections will no longer be recorded as “covid cases”.
That’s right. Even if a sample collected at the low CT value of 28 can be sequenced into the virus alleged to cause Covid19, the CDC will no longer be keeping records of breakthrough infections that don’t result in hospitalisation or death.
From their website:
As of May 1, 2021, CDC transitioned from monitoring all reported vaccine breakthrough cases to focus on identifying and investigating only hospitalized or fatal cases due to any cause. This shift will help maximize the quality of the data collected on cases of greatest clinical and public health importance. Previous case counts, which were last updated on April 26, 2021, are available for reference only and will not be updated moving forward.
Just like that, being asymptomatic – or having only minor symptoms – will no longer count as a “Covid case” but only if you’ve been vaccinated.
The CDC has put new policies in place which effectively created a tiered system of diagnosis. Meaning, from now on, unvaccinated people will find it much easier to be diagnosed with Covid19 than vaccinated people.
Consider…
Person A has not been vaccinated. They test positive for Covid using a PCR test at 40 cycles and, despite having no symptoms, they are officially a “covid case”.
Person B has been vaccinated. They test positive at 28 cycles, and spend six weeks bedridden with a high fever. Because they never went into a hospital and didn’t die they are NOT a Covid case.
Person C, who was also vaccinated, did die. After weeks in hospital with a high fever and respiratory problems. Only their positive PCR test was 29 cycles, so they’re not officially a Covid case either.
The CDC is demonstrating the beauty of having a “disease” that can appear or disappear depending on how you measure it.
To be clear: If these new policies had been the global approach to “Covid” since December 2019, there would never have been a pandemic at all.
If you apply them only to the vaccinated, but keep the old rules for the unvaccinated, the only possible result can be that the official records show “Covid” is much more prevalent among the latter than the former.
This is a policy designed to continuously inflate one number, and systematically minimise the other.
What is that if not an obvious and deliberate act of deception?
May 18, 2021
Posted by aletho |
Deception | CDC, Covid-19, COVID-19 Vaccine, United States |
Leave a comment
I’ve written about this before, and I’m sure I’ll write about it again.
We’re told that the RNA COVID vaccines force the cells of the body to produce a foreign “spike” protein.
There is a little thing you may have heard of called EVIDENCE.
In other words, show me a well-done study, using a few thousand people who have been vaccinated, which proves that all these people’s cells ARE producing that foreign protein and ONLY that foreign protein.
There isn’t such a study.
But if there were—
“Look, a few hundred people didn’t produce the spike protein at all. Wonder what they DID produce.”
“I see a hundred people out of two thousand who produced a huge excess of the spike protein. Wonder what effect THAT is having.”
“I see two hundred people who produced the spike protein plus a bunch of other foreign proteins. A few of those foreign compounds I’ve never seen before. That’s not good at all.”
In fact, show me a large-scale study in which an injection is designed to force the human body to produce ANY specific protein. Let’s see the results.
Can’t find that study, either?
Believing what genetic researchers tell you is like believing what a grifter tells you about how to win at roulette.
For example, are you aware that, after decades of genetic research and tens of thousands of studies linking genes to diseases, there isn’t a single gene-treatment that can cure a disease across the board?
What there is, is a great deal of money that hustlers have raised for bio-tech firms. And there are many sky-blue promises.
And oh yes, there are many examples of errors, in which experimental gene insertions yield unexpected results. Unintended and dangerous results. Unpredicted alterations in genomes.
So the huge numbers of reported injuries and deaths from the COVID RNA vaccines are surely the result of more than just the production of the spike protein.
Why is nobody talking about this?
Because people assume the problem must be the spike protein and only that protein.
The people of planet Earth are part of a guinea-pig vaccine experiment that is much wider than that. We are being subjected to an open-ended genetic spin of the roulette wheel.
And there are no safeguards and no comprehensive follow-ups.
For this reason alone, the entire effort to develop the RNA injections should have been banned from the beginning—until researchers demonstrated convincingly that the risks would be minimal. Of course, they couldn’t make that guarantee.
But the fatuously named Warp Speed program rocketed ahead. Based on pretentious and speculative “science.”
People tend to think—because they watch sci-fi movies—that scientific evil doers are firing a perfectly destructive single arrow at the heart of humanity. But evil-doers are quite capable of launching a thunderstorm of multiple pyrotechnics beyond their control.
As I pointed out in prior articles on this subject, the analogous area of GMO plant genetics is replete with uncontrolled effects—including gene drift, in which injected Monsanto genes move from plants into soil bacteria and human gut bacteria.
Genetic ripple-effects throughout an organism can force the unnatural production of a number of different proteins while modifying others.
This is NOT good; and some of the ways in which it is not good are unknown.
Based on the current level of knowledge in the field of gene-research, the entire program of manufacturing and injecting RNA into the body is an insane criminal enterprise.
As time passes, I expect investigators to discover new ways in which these RNA shots are harming people. And some of those investigators will say, “THIS turns out to be what the vaccine is doing. THIS one thing.” And they’ll be wrong.
It’s five, ten, 20 different things. Caused by ripple effects throughout the genome.
May 18, 2021
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine |
Leave a comment
A long-standing private organization, the National Vaccine Information Center, has analyzed the US government’s database, the Vaccine Adverse Event Reporting System (VAERS).
As of May 7, 2021, VAERS lists 192,954 adverse-event reports associated with COVID vaccines. [1]
These events cover the spectrum from mild transient effects to death.
VAERS has always has multiple problems.
One: Doctors aren’t required by law to report adverse effects. Many of them wouldn’t risk blowback by doing so.
Two: There is no comprehensive effort to determine whether an adverse effect is actually caused by a vaccine.
Three: Patients can make adverse-effect reports—but are often hesitant to do so.
Four: By far the biggest problem is: most Americans aren’t even aware that VAERS exists.
Therefore, on balance, UNDER-REPORTING adverse effects is the primary defect of VAERS.
Many efforts have been made to estimate the degree of under-reporting. These estimates state the VAERS numbers should be multiplied by 10, all the way to 100, to obtain an accurate picture of adverse effects.
Ten times the current number of COVID vaccine adverse effects would equal 1,929,540. A hundred times the current number=19,295,400. Either way, the number is staggering.
The death reports are escalating by the day. As of May 7—4,057.
Here are other very troubling categories of VAERS adverse effects, as of May 7. Permanent Disability=2,475. Doctor’s Office Visit=32,801. Emergency Doctor/Room=25,566. Hospitalized=11,538. Birth Defect=112. Life-Threatening=3,548.
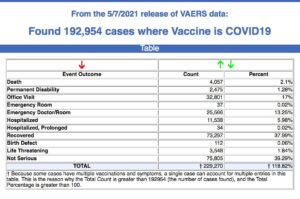
Yet, public officials and news outlets continue to repeat the mantra, “safe and effective,” and urge everyone to take the shot.
Every person who receives the vaccine is supposed to be informed of the risks beforehand. I assure you NO ONE is being given these adverse effect numbers, plus the advice to multiply the numbers by 10 or 100.
Lack of informed consent runs contrary to every medical code.
I can also assure you the FDA, which is considering whether to give full approval to the current COVID vaccines, isn’t multiplying the adverse-effect numbers by 10 or 100.
Here is something else to consider. Even multiplying the VAERS numbers by 100 may not be sufficient, because the RNA COVID shots are employing a new technology which a) has never been used on the public before and b) isn’t a vaccine at all; it’s a genetic treatment.
As I’ve shown in recent articles, the entire field of genetic research is riddled with lies, pretense, and unpredictable ripple-effect consequences. The notion of inserting a single genetic change into a person and limiting its effects to an announced goal is a fiction. Unexpected changes occur. And their negative disruptive effects, long-term, are unknown.
Those effects will never be listed in any database.
SOURCE:
[1] https://www.medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUP1=CAT&EVENTS=ON&VAX=COVID19
May 17, 2021
Posted by aletho |
Deception | COVID-19 Vaccine, Human rights, United States |
Leave a comment
Introduction
Awareness of ivermectin’s efficacy and its adoption by physicians worldwide to successfully treat COVID-19 have grown exponentially over the past several months. Oddly, however, even as the clinical trials data and successful ivermectin treatment experiences continue to mount, so too have the criticisms and outright recommendations against the use of ivermectin by the vast majority, though not all, of public health agencies (PHA), concentrated largely in North America and Europe.
The Front Line COVID-19 Critical Care Alliance (FLCCC) and other ivermectin researchers have repeatedly offered expert analyses to respectfully correct and rebut the PHA recommendations, based on our deep study and rapidly accumulated expertise “in the field” on the use of ivermectin to treat COVID-19. These rebuttals were publicized and provided to international media for the education of providers and patients across the world. Our most recent response to the European Medicines Agency (EMA) and others recommendation against use can be found on the FLCCC website here.
In February 2021, the British Ivermectin Recommendation Development (BIRD), an international meeting of physicians, researchers, specialists, and patients, followed a guideline development process consistent with the WHO standard. It reached a consensus recommendation that ivermectin, a verifiably safe and widely available oral medicine, be immediately deployed early and globally. The BIRD group’s recommendation rested in part on numerous, well-documented studies reporting that ivermectin use reduces the risk of contracting COVID-19 by over 90% and mortality by 68% to 91%.
A similar conclusion has also been reached by an increasing number of expert groups from the United Kingdom (UK), Italy, Spain, United States (US), and a group from Japan headed by the Nobel Prize-winning discoverer of Ivermectin, Professor Satoshi Omura. Focused rebuttals that are backed by voluminous research and data have been shared with PHAs over the past months. These include the WHO and many individual members of its guideline development group (GDG), the FDA, and the NIH. However, these PHAs continue to ignore or disingenuously manipulate the data to reach unsupportable recommendations against ivermectin treatment. We are forced to publicly expose what we believe can only be described as a “disinformation” campaign astonishingly waged with full cooperation of those authorities whose mission is to maintain the integrity of scientific research and protect public health.
The following accounting and analysis of the WHO ivermectin panel’s highly irregular and inexplicable analysis of the ivermectin evidence supports but one rational explanation: the GDG Panel had a predetermined, nonscientific objective, which is to recommend against ivermectin. This is despite the overwhelming evidence by respected experts calling for its immediate use to stem the pandemic. Additionally, there appears to be a wider effort to employ what are commonly described as “disinformation tactics” in an attempt to counter or suppress any criticism of the irregular activity of the WHO panel.
The WHO Ivermectin Guideline Conflicts with the NIH Recommendation
The FLCCC Alliance is a nonprofit, humanitarian organization made up of renowned, highly published, world-expert clinician-researchers whose sole mission over the past year has been to develop and disseminate the most effective treatment protocols for COVID-19. In the past six months, much of this effort has been centered on disseminating knowledge of our identification of significant randomized, observational, and epidemiologic studies consistently demonstrating the powerful efficacy of ivermectin in the prevention and treatment of COVID-19. Our manuscript detailing the depth and breadth of this evidence passed a rigorous peer review by senior scientists at the U.S Food and Drug Administration and Defense Threat Reduction Agency. Recently published, our study concludes that, based on the totality of the evidence of efficacy and safety, ivermectin should be immediately deployed to prevent and treat COVID-19 worldwide.
The first “red flag” is the conflict between the March 31, 2021, WHO Ivermectin Panel’s “against” recommendation and the NIH’s earlier recommendation from February 12th of a more supportive neutral recommendation based on a lower amount of supportive evidence of ivermectin’s efficacy at that time.
Two flawed lines of analysis by the WHO appear to account for this inconsistent result:
- The WHO arbitrarily and severely limited the extent and diversity of study designs considered (e.g., retrospective observational controlled trials (OCT), prospective OCTs, epidemiological, quasi-randomized, randomized, placebo-controlled, etc.).
- The WHO mischaracterized the overall quality of the trial data to undermine the included studies.
The Severely Limited Extent and Diversity of Ivermectin Data Considered by the WHO’s Ivermectin Panel
The WHO Ivermectin Panel arbitrarily included only a narrow selection of the available medical studies that their research team had been instructed to collect when formulating their recommendation, with virtually no explanation why they excluded such a voluminous amount of supportive medical evidence. This was made obvious at the outset due to the following:
- No pre-established protocol for data exclusion was published, which is a clear departure from standard practice in guideline development.
- The exclusions departed from the WHO’s own original search protocol it required of Unitaid’s ivermectin research, which collected a much wider array of randomized controlled trials (RCT).
Key Ivermectin Trial Data Excluded from Analysis
- The WHO excluded all “quasi-randomized” RCTs from consideration (two excluded trials with over 200 patients that reported reductions in mortality).
- The WHO excluded all RCTs where ivermectin was compared to or given with other medications. Two such trials with over 750 patients reported reductions in mortality.
- The WHO excluded from consideration 7 of the 23 available ivermectin RCT results. Such irregularities skewed the proper assessment of important outcomes in at least the following ways:
- Mortality Assessment
- WHO Review: Excluded multiple RCTs such that only 31 total trials deaths occurred; despite this artificially meager sample, an estimate of up to a 91% reduction in the risk of death was found.[1]
- Compared to the BIRD Review: Included 13 RCTs with 107 deaths observed and found a 2.5% mortality with ivermectin vs. 8.9% in controls; estimated reduction in risk of death=68%; highly statistically significant, (p=.007).
- Assessment of Impacts on Viral Clearance
- WHO Review: 6 RCTs, 625 patients. The Panel avoided mention of the important finding of a strong dose-response in regard to this outcome.
- This action in (i) is indefensible given that their Unitaid research team found that among 13 RCTs, 10 of the 13 reported statistically significant reductions in time to viral clearance, with larger reductions with multiday dosing than single-day, consistent with a profound dose-response relationship.[2]
- Adverse Effects
- WHO: Only included 3 RCTs studying this outcome. Although no statistical significance was found, the slight imbalance in this limited sample allowed the panel to repeatedly document concerns for “harm” with ivermectin treatment.
- Compare (a) to the WHO’s prior safety analysis in their 2018 Application for Inclusion of Ivermectin onto Essential Medicines List for Indication of Scabies:
- “Over one billion doses have been given in large-scale prevention programs.”
- “Adverse events associated with ivermectin treatment. are primarily minor and transient.”[3]
- The WHO excluded all RCTs studying the prevention of COVID-19 with ivermectin, without supporting rationale. Three RCTs including almost 800 patients found an over 90% reduction in the risk of infection when ivermectin is taken preventively.[4]
- The WHO excluded observational controlled trials (OCT), with 14 studies of ivermectin. These included thousands of patients, including those employing propensity matching, a technique shown to lead to similar accuracy as RCTs.
- One large, propensity-matched OCT from the US found that ivermectin treatment was associated with a large decrease in mortality.
- A summary analysis of the combined data from the 14 available ivermectin OCTs found a large and statistically significant decrease in mortality.
- The WHO excluded numerous published and posted epidemiologic studies, despite requesting and receiving a presentation of the results from one leading epidemiologic research team. These studies found:
- In numerous cities and regions with population-wide ivermectin distribution campaigns, large decreases in both excess deaths and COVID-19 case fatality rates were measured immediately following the campaigns.
- Countries with pre-existing ivermectin prophylaxis campaigns against parasites demonstrate significantly lower COVID-19 case counts and deaths compared to neighboring countries without such campaigns.
Assessment of the Quality of the Evidence Base by WHO Guideline Group
The numerous above actions minimizing the extent of the evidence base were then compounded by the below efforts to minimize the quality of the evidence base:
The WHO mischaracterized the overall quality of the included trials as “low” to “very low,” conflicting with numerous independent expert research group findings:
- An international expert guideline group independently reviewed the BIRD proceeding and instead found the overall quality of trials to be “moderate.”
- The WHO’s own Unitaid systematic review team currently grade the overall quality as “moderate.”
- The WHO graded the largest trial it included to support a negative assessment of ivermectin’s mortality impacts as “low risk of bias.” A large number of expert reviewers have graded that same trial as “high risk of bias,” detailed in an open letter signed by over 100 independent physicians.
We must emphasize this critical fact: If the WHO had more accurately assessed the quality of evidence as “moderate certainty,” consistent with the multiple independent research teams above, ivermectin would instead become the standard of care worldwide, similar to what occurred after the dexamethasone evidence finding decreased mortality was graded as moderate quality, which then led to its immediate global adoption in the treatment of moderate to severe COVID-19 in July of 2020.[5]
Further, The WHO’s own guideline protocol stipulates that quality assessments should be upgraded when there is the following:
- a large magnitude of effect (despite their data estimating a survival benefit of 81%, the low number of studies and events included allowed them to dismiss this finding as “very low certainty”) or;
- evidence of a dose-response relationship. The WHO shockingly omits the well-publicized reports by their Unitaid research team of a powerful dose-response relationship with viral clearance.
In sum, the WHO’s recommendation that “ivermectin not be used outside clinical trials” is based entirely upon:
- the dismissal of large amounts of trial data;
- the inaccurate downgrading of evidence quality; and
- the deliberate omission of a dose-response relationship with viral clearance.
Consequently, these actions formed the basis of their ability to avoid a recommendation for immediate global use.
Even more surprising is that based on their “very low certainty” finding, the panel goes on to “infer” that “most patients would be reluctant to use a medication for which the evidence left high uncertainty regarding effects on outcomes they consider important.”
This statement is insupportable in light of the above actions. No patient could ever rationally consent to a trial in which they were acutely ill and would be subject to the possibility of receiving a placebo, once informed of: the large amount of relevant and positive trials that the WHO removed from consideration, their avoidance of reporting a large dose-response relationship, and their widely contradicted “very low certainty” grading of large mortality benefits. Such a trial would result in a historic ethical research violation, causing both a widespread loss of life and a resultant loss of trust in PHAs and research institutions for decades to come.
The many methods employed by the WHO to distort the evidence base and arrive at a non-recommendation are made even more suspicious and questionable by the following:
- The WHO GDG did not hold a vote on the use of ivermectin. This highly irregular decision was purportedly based on the Ivermectin Panel’s “consensus on evidence certainty.”
- Unitaid Sponsors allegedly inserted multiple limitations and weakened the conclusions in the preprint, systematic review manuscript by the Unitaid research team, which has recently led to formal charges of scientific misconduct.
- Recent WHO whistleblower complaints of external influences in other WHO Covid reports, as well as attempts by massive external funding organizations to increase their influence in formulating WHO policies.
- The finding of marked differences in the evidence bases used to support prior WHO/BIRD guideline recommendations for ivermectin in other diseases:
-
- WHO: Approved ivermectin in the treatment of scabies based on 10 RCTs that included only 852 patients, despite it being inferior to the standard of care.
- FDA: Approved ivermectin in the treatment of strongyloidiasis based on 5 RCTs that included only 591 patients.
- BIRD: Approved ivermectin in March, 2021, for the prevention and treatment of COVID-19 based on 21 RCTs and 2,741 patients.
Conclusion
As expert clinician-researchers in society, we are firmly committed to ensuring that public health policy decisions derive from scientific data. Disturbingly, after extensive analysis of the recent WHO ivermectin guideline recommendation, we could not arrive at a credible scientific rationale to explain the numerous irregular, arbitrary, and inconsistent behaviors documented above. Further, after consultation with numerous physicians, guideline reviewers, legal experts, and veteran PHA scientists, we identified two major socio-political-economic forces that serve as the main barrier influences preventing ivermectin’s incorporation into public health policy in major parts of the world. They are:
1) the modern structure and function of what we will describe as “Big Science” and;
2) the presence of an active “Political-Economic Disinformation Campaign.”
“Big Science”
Also known as “Big RCT Fundamentalism,” Big Science reflects a dramatic shift in the practice of modern evidence-based medicine (EBM). Beginning before COVID, it has since rapidly evolved into the current system that more tightly meshes the entities of “Big Pharma,” “Big PHA’s/Academic Health Centers” (AMC), “Big Journals,” “Big Media,” and “Big Social Media” into the public health system’s efforts at guiding patient care, research and policy.
The structure and function of “Big Science” in COVID-19 is most simply represented as follows:
- Only arbitrarily defined, “large, well-designed” RCTs (Big RCT), generally conducted on North American or European shores, can “prove” the efficacy of a medicine.
- Only Big Pharma/Big PHA/AMCs have the resources/infrastructure to conduct Big-RCTs. (Many equate Big PHA/AMC with Big Pharma, given the funding source of the former.)
- Only Big RCTs by Big Pharma or Big PHA/AMC can publish study findings in high-impact, high-income country medical journals (Big Journals).
- Only medicines supported by Big Journal publications are deemed to have “sufficient evidence” and “proven efficacy” to then be recommended by Big PHAs.
- Only medicines recommended by Big PHAs are covered by “Big Media” or escape censorship on “Big Social Media.”
Conversely, repurposed, off-patient medications such as ivermectin do not attract Big PHA or Big Pharma sponsors to conduct the mandatory Big RCT. Given this structural handicap, many effective medicines including ivermectin are consequently incapable of ever meeting Big PHA standards for approval in such a system. In the case of ivermectin, it is then considered, first by Big PHAs, then throughout Big Media and Big Social media, to be “unproven” given it lacks “sufficient evidence” and is thus heavily censored from public discussion and awareness. Mentions of ivermectin on Big Social Media led to the removal of a popular Facebook group (“Ivermectin MD Team” with over 10,000 followers). Additionally, all YouTube videos mentioning ivermectin in treatment of Covid-19 were removed or demonetized, as well as Twitter pages locked. Further, in Big Media, even the most credentialed independent and expert groups who recommend ivermectin based on a large body of irrefutable evidence are labeled as “controversial” and purveyors of “medical misinformation.”
A health system structured to function in this manner is clearly vulnerable to and overly influenced by entities with financial interests. Further, in Covid, such systems have evolved into rigidly operating via top-down edicts and widespread censoring. This allows little ability for emerging scientific developments not funded by Big Pharma to be disseminated from within the system or through media or social media until years later when, and if, a Big RCT is completed. This barrier has presented as an enduring horror throughout the pandemic given the widespread loss of life caused by the systematic withholding of numerous rapidly identified, safe and effective, repurposed medicines for fear of using “unproven therapies” without “sufficient evidence” for use. Alternatively, and for the first time in many physicians’ careers, those who seek to treat their patients with such therapies, based on their professional interpretation of the existing evidence are restricted by their employers issuing edicts “from above.” They are then forced to follow protocols that rely predominantly on pharmaceutically engineered therapeutics.
It must be recognized that distinct from “regulatory” agencies such as the FDA, whose system often relies upon the primary importance of a “Big RCT,” stronger foundations used by PHAs are available. One of the long-standing tenets of modern evidence-based medicine is that the highest form of medical evidence is a “systematic review and meta-analysis” of RCTs and not a sole Big RCT. Disturbingly, not one of the Big PHAs mention this established principle or their long-standing reliance on such evidence-based practices for issuing recommendations. In the case of ivermectin, they willfully ignore the multiple published expert meta-analyses of ivermectin RCTs, including almost two dozen trials and thousands of patients, reporting consistent reductions in mortality, time to clinical recovery, and time to viral clearance.
These improvements are found consistently and repeatedly, no matter the RCT design, size, or quality, and from varied centers and countries throughout the world. All studies were done without any identified conflict of interest with the vast majority of double-blind, single-blind, quasi-randomized, open-label, standard of care comparison, combination therapy comparisons, etc., reporting benefits. Satoshi Omura, Nobel Prize-winning discoverer of ivermectin, wrote in his team’s recent review paper that “the probability of this judgement on ivermectin’s superior clinical performance being false is estimated to be 1 in 4 trillion.” This supports our public warnings against further “placebo-controlled trials” given the near absolute certainty of harm to research subjects included in a placebo Big RCT.
Conversely, despite sitting atop the highest form of medical evidence, many non-regulatory Big PHAs around the world cry out for a Big RCT. This is while avoiding the issuance of even one of the several “weaker” recommendation options available to them in the setting of a low-cost, widely available medicine with an unparalleled safety profile and a constantly surging humanitarian crisis, even in the interim. Insufficient evidence, unproven — these are comments from WHO, NIH, Europe’s EMA, South Africa’s SAPHRA, France’s ANSM, United Kingdom’s MHRA, and Australia’s TGA.
Most disturbing to contemplate is our estimation that if the use of penicillin in bacterial infection were to have been tested in these same numbers and types of trials in the 1940s, the graphical display of benefits would look nearly identical to those found with ivermectin. Further, the U.S Cures Act of 2016, “specifically designed to accelerate and bring new innovations and advances faster and more efficiently to the patients who need them” emphasized the importance of using various forms of “real-world evidence” data to aid in regulatory decision-making. We can find no evidence of an organized effort to examine the more than 14, often large OCTs that show evidence of the substantial beneficial use of ivermectin. Further, no PHA has cited the numerous convincing epidemiological analyses that find rapidly falling case fatality rates following ivermectin distribution campaigns.
With the lack of a credible explanation for the absence of even a weak recommendation for ivermectin in the setting of widespread increased death rates from COVID-19, numerous citizens have speculated that this can only be explained by the presence of an active disinformation campaign by entities with nonscientific and largely financial objectives dependant on the non-recognition of ivermectin’s efficacy. We explore the near certainty of this occurring below.
Active Political-Economic “Disinformation” Campaign
“Disinformation” campaigns, best described in the article, “The Disinformation Playbook,” are initiated when independent science interferes with or opposes the interests of corporations or policymakers. Although thankfully rare, in certain cases these entities will actively seek to manipulate science and distort the truth about scientific findings that imperil their profit or policy objectives. First developed by the tobacco industry decades ago, these deceptive tactics include the following;
- The Fake: Conduct counterfeit science and try to pass it off as legitimate research.
- The Blitz: Harass scientists speaking out with results inconvenient for industry.
- The Diversion: Manufacture uncertainty about science where little or none exists.
- The Screen: Buy credibility through alliances with academia/professional societies.
- The Fix: Manipulate government processes to influence policy inappropriately.
Numerous examples of the above disinformation tactics by corporations and policymakers, particularly within the pharmaceutical industry, have been documented:
Most worrisome is that ivermectin appears to be up against one of the largest financial and global policy oppositions in modern history, including but not limited to:
- Numerous Big Pharma companies and sovereign nations selling billions of vaccine doses.
- Concerns of numerous Big Pharma and Big PHA’s that if ivermectin is approved as effective treatment for COVID-19, EUAs for all vaccines would be revoked.
- Numerous Big Pharma/Big PHA concerns that ivermectin’s potential as an alternative to vaccines may increase vaccine hesitancy and disrupt mass vaccination rollouts.
- Opponents include large philanthropic sponsors with global vaccination goals.
- Disinformation: WHO Panel does not review ivermectin prevention trials.
- Numerous Big Pharma company investments in novel, engineered therapies (i.e., oral antivirals by Merck and Pfizer and Gilead) directly compete with ivermectin.
- Disinformation: Merck places a post on their website, without scientific supporting evidence or named scientist authors that: “No evidence of either a mechanism of action, clinical efficacy or safety in COVID-19 exists.”
- Disinformation: A Merck managing director argues against use in the Philippines by stating: “The levels of evidence do not come up to standards.”
- Big Pharma company’s (Astra-Zeneca) investment into a long-acting antibody product for prevention and treatment of COVID-19, which competes with ivermectin.
- Numerous Big Pharma’s monoclonal antibody products that compete with ivermectin.
- Big Pharma’s Remdesivir demand would rapidly decline once hospitalizations were to decrease after ivermectin approval.
Based on the lack of a rational explanation for the above actions by WHO, Merck, FDA, and Unitaid, we conclude that they result from an active disinformation campaign, executed both through the PHA’s, media and the WHO Guideline group recommendations. As highly published researchers, we find the allegations of scientific misconduct in the writing of the WHO/United research team’s meta-analysis manuscript to be deeply disturbing. It clearly represents a disinformation tactic with an intent to distort and diminish the reporting of a large magnitude benefit on mortality among many hundreds of patients. Further, Merck’s demonstrably and blatantly false statements against ivermectin deserve no further discussion. It is yet another entry into the disturbing historical record of actions committed by a Big Pharma entity with the primary intent of protecting profit at the expense of the welfare of global citizens.
For These Compelling and Irrefutable Reasons, The FLCCC Makes a Call to Action
This call to action is no longer just to health authorities, but to citizens everywhere to fight back against these disinformation tactics. We find the advice of the Union of Concerned Scientists (UCS) to be an excellent guide to action in this regard:
Global Citizens
- Share the playbook with your social media networks when you see new examples like those outlined above.
- Set the record straight. When you see someone spreading disinformation on a topic, counter it. There are millions around the world who either have studied the data or have experience with the potent efficacy of ivermectin in COVID-19. It is important to correct false assertions.
- Consider divesting your retirement funds and other investments from companies engaging in disinformation.
Fellow Scientists
- Become a UCS Network Watchdog to help track and resist attacks on science.
- If a governmental or NGO scientist, report actions that diminish their role in policymaking.
Media
- Avoid false equivalencies that distort scientific consensus.
- Correct the record when scientific information is misrepresented, particularly by Big PHA/Big Pharma.
- Report abuses of science in government.
As an expert group of ivermectin researchers, we are unsure of what else to offer in order to correct or counteract this misrepresentation of an important drug. Our belief is that, of the above actions, the most effective counter to the disinformation campaign would be that a whistleblower become active from within WHO, the FDA, the NIH, Merck, or Unitaid. This moment in history demands a man or woman with the courage and conviction to step forward. Urgently.
In both the interests of humanity and to motivate and inspire such a citizen of the world, we leave you with the words of Albert Einstein: “The world will not be destroyed by those who do evil, but by those who watch them and do nothing.”
[1]Special emphasis must be placed on this decision; selecting only trials where very few deaths occurred.
(n.b., the number of events observed within trials is a primary criterion for judging the “certainty of evidence”). This action provides almost the entire basis for the panel’s assessment of a “very low certainty of evidence.” It is in effect, a “smoking gun,” one of the many actions above demonstrating that the primary objective of the Panel was to recommend against use of ivermectin.
[2]This omission is the second most important action allowing the panel to find a “very low certainty of evidence,” given that, per WHO protocol, if a dose-response relationship is found, the certainty of evidence must be upgraded.
[3]Special emphasis must be placed on the harm of excluding trials data supporting ivermectin in the prevention of COVID-19. If the preventive efficacy of ivermectin were to be known or accepted, this would allow deployment in regions without vaccines.
[4]British Ivermectin Recommendation Development (BIRD) panel (2021). The BIRD Recommendation on the Use of Ivermectin for COVID-19. Full report. https://tinyurl.com/u27ea3y
[5]The FLCCC Alliance recommended, as well as gave U.S. Senate testimony in support of, the use of corticosteroids in COVID-19 months before this announcement, during the prolonged period when all PHAs recommended against its use
Sincerely,
The Front Line COVID-19 Critical Care Alliance
Pierre Kory, MD
Keith Berkowitz, MD
Paul E. Marik, MD
Fred Wagshul, MD
Umberto Meduri, MD
Scott Mitchell, MBChB
Joseph Varon, MD
Eivind Vinjevoll, MD
Jose Iglesias, DO
###
May 16, 2021
Posted by aletho |
Corruption, Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine |
Leave a comment
A Whitehall source directly linked to the Covid Response has said that the UK Government have already structured a detailed plan designed to neutralise each stage of lockdown easing, including the compliance of media outlets to help spread fear.
The Whitehall source has said that he has been “increasingly concerned” with how the Government are behaving, and that their “relationship with the truth” is now not even on nodding terms. The latest plan will involve a series of ‘crisis’ around drug supply; mutant strains; and third waves, specifically choreographed to condition the public for further lockdowns and vaccine passports.
The plan, that according to the source is designed to take us to September 27th 2021 is to be released in stages over the summer months and, according to the Whitehall source, is already ‘well underway’.
On March the 8th, the first milestone of the roadmap was implemented, with school children finally returning to class. The following day Chris Whitty gave a pre-written speech to the Commons that said schools reopening would cause another surge in the virus and ended it with “Let me be clear, many, many more people will die before this is over” the soundbite obligingly repeated on every news outlet, with BBC news having it on-loop all day.
On March the 29th, the second milestone of the roadmap was implemented. The Government said – “The evidence shows that it is safer for people to meet outdoors rather than indoors,”. This is why from the 29th March, when most schools start to break up for the Easter holidays, outdoor gatherings (including in private gardens) of either 6 people (the Rule of 6) or 2 households will also be allowed, making it easier for friends and families to meet outside.
The next day (March 30th) the AstraZeneca Vaccine was again stopped due to blood clots fears, despite the medicine’s regulator clearing it only the previous week. Whilst Boris Johnson repeated what he’d said the previous week that the mutated virus on the continent would inevitably “wash up on our shores”.
On April 19th, the third milestone saw pub gardens, and non-essential shops reopen. Followed immediately by news of a second vaccine being halted for fear it was causing blood clots and the discovery of the South African mutation said to be able to avoid them anyway.
The next milestone is due on May 17th with the Government relaxing social contact rules further and the opening of indoor venues. This will be followed by a story that the mutation is ‘more deadly than first thought’ and that young people are now also vulnerable to it, accompanied by the result of the vaccine passport trials have shown that they have a ‘positive effect on virus reduction’.
The final milestone is due on June 21st where ALL restrictions were promised to be lifted. This will not be allowed to happen. Vaccine passports / Track and Trace will be mandatory, as will masks and social distancing. The entire week of the 21st will be taken up by a third wave, which will suddenly be ‘rampant’, and this will be attributed to a new variant which they will declare is more deadly than the previous strains of Covid allegedly doing the rounds. This will be accompanied with yet more issues with vaccine supplies. Authorities will declare that one of the vaccines is effective against the deadlier strain, but a ‘problem’ with its manufacture will emerge.
The Whitehall source went on to say –
“All the measures are aimed at two things, vaccine passports and lockdowns starting next winter,
“The ultimate goal is to have the public, back in their box.
“Note that Boris is now talking down vaccine’s and bigging-up lockdowns, that wasn’t a mistake, that was all part of the plan”.
The plan also includes an ad campaign like the one seen at Christmas, the message this time will be that the pandemic isn’t over and vaccine passports are the ‘solution’.
May 16, 2021
Posted by aletho |
Civil Liberties, Deception, Fake News, Mainstream Media, Warmongering, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine, Human rights, UK |
Leave a comment

Seeing through the COVID-19 spin is a challenge even for those who have been writing and talking for years about the need to limit Big Pharma’s influence on health policy and law. Perhaps the greatest change I have seen in vaccine regulation, policymaking and law over the past four decades has been the development of public-private business partnerships between Big Pharma and the government.1 2 3 4 5 That seismic change has affected how new vaccines are developed, licensed and regulated and is influencing what we see happening today.6 7
Since the coronavirus pandemic was declared by government officials in early 2020, lawmakers have been persuaded to build the entire global pandemic response around a single experimental biological product.8 9 10 That single product is generating billions of dollars in profits for liability free drug companies and their partners.11 12 The COVID-19 spin is reaching dizzying new heights every day,13 14 with fundamental facts about the experimental product’s risks and failures getting lost in the hard sell.
At dinner time, if you turn on any major television network in the U.S., you will see that the evening news has turned into one long COVID vaccine commercial infused with a heavy dose of fear mongering. Before the pandemic declaration, we had learned to ignore prescription drug advertising in-between getting news of the day. Now newscasters and TV docs are Pharma’s new COVID “vaccine” sales reps and the only way to get away from the 24/7 sales pitch is to turn off the TV.
Billions of Dollars Paid to TV Networks for DTC Pharma Ads
We should not be surprised. The U.S. and New Zealand are the only two countries in the world that allow direct to consumer pharmaceutical product advertising.15 16 17 In this country. Big Pharma pays US television networks five billion dollars per year to push use of drugs and vaccines.18
Taking a page out of Big Tobacco’s old book and upping the ante, Big Pharma has become a business partner of government.19 The COVID business deal is perhaps the single biggest one in the history of public health programs.20 21 22
Already wealthy drug companies were given at least nine billion dollars from the. government to develop experimental COVID vaccines in record breaking time,23 shaving five to 10 years off the normal vaccine development, testing and licensing process.24 25 But that wasn’t enough. Congress also handed companies a liability shield from lawsuits whenever the product government paid them to produce fails to work as advertised or a person is hurt by using it.26
If you or a loved one dies or is permanently injured by an experimental or soon-to-be FDA licensed COVID vaccine, you cannot sue the drug company who made it, even if there is evidence the company could have made it less reactive or more effective.
Big Pharma Pays Big Tech Billions of Dollars for Ads, Censorship Campaigns
If you are searching for relief from the hype by turning off the TV and turning on your computer, you will be disappointed. The COVID vaccine ad campaign is in high gear online, especially on social media platforms. The Thought Police hired by Big Tech to censor information that does not conform with pre-approved pandemic narratives are making sure you do not have an opportunity to carefully weigh the vaccine’s benefits and risks.27 28 29
Rational thinking on the World Wide Web is no longer tolerated and neither is freedom of speech. The Internet has become a drug company stockholder’s dream and a consumer’s worst nightmare.
Big Pharma and its business partners have paid a lot of money to Big Tech to eliminate freedom of thought and speech online. Right now the weapon of choice is a social media censorship campaign to de-platform dissenters, including reputable charitable organizations like the National Vaccine Information Center publishing well referenced information.30 31 32 The Internet Thought Police are especially upset when anyone talks about reports of serious vaccine complications and deaths, but reports about COVID-19 disease complications and deaths are allowed without restrictions.33
As COVID social distancing regulations have kept more people at home and on their electronic devices, the healthcare and pharma industry has poured more money into direct to consumer digital ads.34 In 2020, drug and vaccine manufacturers funneled about 10 billion dollars into digital advertising that we view on our computers, tablets and cell phones.35 36
How much of Big Tech’s decision to ghost dissenters from search engine results and de-platform social media accounts is influenced by an infusion of direct to consumer advertising dollars from Big Pharma?37
American Taxpayer Pays for COVID-19 Vaccine Ads
This year, the American taxpayer is also paying for TV and digital advertising to promote the use of the COVID-19 vaccine.38 On April 1, 2021, the government announced a three billion dollar COVID vaccine ad campaign39 to get make sure that every American gets vaccinated, a national ad campaign that is using community and religious leaders, as well as celebrities,40 41 to reach into every community to boost vaccine uptake in stores,42 sports arenas,43 schools44 and churches.45
Right now, Pfizer and Moderna, the two U.S. corporations manufacturing experimental messenger RNA (mRNA) COVID-19 vaccines are leading beneficiaries of the free advertising paid for by tax dollars. The first to secure an Emergency Use Authorization (EUA) from the FDA, Moderna counts the federal National Institutes for Health as a business partner,46 while Pfizer partnered with the German company BioNTech.47 Together, Moderna and Pfizer have captured market share and, by the end of 2020, Pfizer had achieved a 180 percent increase in revenue48 49 and Moderna had scored an eye watering 3,900 percent increase. 50 51
So what has the COVID vaccine advertising blitz done so far, other than convincing half of all adults to get at least one dose of the vaccine by mid-April 2021?52
The most notable achievement of the COVID vaccine campaign has been to keep everyone in a constant state of fear and confusion about what is true and what is false.53 There are so many misunderstandings and false impressions out there about the biological product manufactured by Moderna and Pfizer, a product that most people call a vaccine and other call a therapeutic drug but I call a cell disrupter biological.
No Long Term Safety Studies of Experimental mRNA Vaccines
Whatever you want to call it, the experimental mRNA technology that Moderna and Pfizer employed to create the product has not yet been licensed by the FDA to prevent infections in humans. 54 It is a genetic engineering technology that radically departs from the production methods used for two centuries to make live attenuated and inactivated viral and bacterial vaccines.55 It is an experimental technology that injects synthetic RNA directly into cells and, in effect, attempts to turn the human body into a vaccine manufacturing machine.56 57
There are no long-term studies58 evaluating the range of effects at the cellular and molecular level on the biological and genetic integrity of humans who receive the product. Nobody knows if it will, over time, negatively affect normal immune function and cause autoimmune and other chronic inflammatory conditions in the body,59 60 61 or provoke enhanced disease in vaccinated persons encountering mutated versions of the coronavirus in the future.62
Myth: Pfizer and Moderna mRNA Vaccines Have Been Proven to Prevent Infection and Transmission of SARS-CoV-2
What are the two biggest myths that have been generated by the advertising campaign being conducted with Pharma and taxpayer dollars?
The first big myth is that if you get two doses of the mRNA COVID vaccine, you will get artificial immunity and cannot be asymptomatically or symptomatically infected with the SARS-CoV-2 virus and you will not be able to infect others who come in physical contact with you: you dutifully got vaccinated and now you are immune.63 That is a normal assumption because that is what vaccines are supposed to do, but it is a false assumption.
The Emergency Use Authorization the FDA gave to Pfizer and Moderna was not granted based on scientific evidence that the product prevented infection and transmission of SARS-Cov-2.64 65 In fact, the FDA directed manufacturers in the summer of 2020 to make a product that had at least a 50 percent efficacy rate in either preventing or reducing severity of COVID-19 disease.66
The companies chose to apply for an EUA based on nine months of clinical trial data that the product prevents people from developing severe symptoms of COVID-19 disease 67 and reduces the likelihood they will have serious complications leading to hospitalization and death – not that it prevents infection and transmission. There is a difference.
TAKE HOME FACT: COVID-19 vaccines were not designed and have not yet been proven to prevent infection and transmission of the new coronavirus in the majority of recipients. Apparently, that is why public health officials are telling vaccinated people they have to continue wearing masks and social distancing just like unvaccinated people.68 69
Myth: It is “Good” to Feel Bad After mRNA Covid-19 Shots Because It Means the Vaccine is “Working”
The second big myth being perpetuated by COVID spin is that when you have strong reactions to a COVID-19 shot, it is “good” because it means the vaccine is “working.”70 71
The companies and public health officials admit that the mRNA vaccines are reactive and that the majority of people, especially younger people, who get vaccinated will experience reactions strong enough to require a day or two of recovery and even time off work.72 73 But there is not one credible scientific study published in the medical literature demonstrating that high fevers, chills, headache, joint and muscle aching, disabling fatigue and other symptoms are “good” for the body and indicate the body is successfully producing artificial immunity.
In fact, strong reactions to pharmaceutical products like drugs and vaccines are usually something to be concerned about and a reason to exercise caution, especially with repeat doses. 74 75 76
More concerning are the 68,000 adverse event reports following COVID-19 vaccinations, including over 2600 deaths, 77 that have been reported as of April 8, 2021 to the federal Vaccine Adverse Event Reporting System (VAERS) created under the 1986 National Childhood Vaccine Injury Act.78 79 80 81 More than 70 percent of the reaction reports occurred in people between 17 and 65 years old. And that may be just the tip of the iceberg because one government funded study found that less than one percent of vaccine reactions are ever reported to the vaccine reaction reporting system82 created under the 1986 National Childhood Vaccine Injury Act.
Although Pfizer, Moderna and the government admit that messenger RNA COVID vaccines can cause a lot of reaction symptoms like fever, body pain and disabling fatigue,83 84 85 they adamantly deny that the shots cause sudden death86 87 88 or blood clots89 90 91 92 and bleeding disorders like immune thrombocytopenic purpura,93 cardiac and respiratory arrest,94 95 and other very serious health problems.96
Where is the biological mechanism science that proves it is only a coincidence when people suddenly die within minutes, 97 days or weeks of being given a COVID shot98 and that none of the tens of thousands of bad health outcomes being reported to the Vaccine Adverse Event Reporting System are causally related?99
Where is science backing up the claim that feeling so bad you can’t get out of bed or go to work after getting vaccinated is “good” because being in pain is evidence that the product is effective?
TAKE HOME FACT: COVID-19 shots cause reactions in the majority of people.100 101 There is no scientific evidence that having strong reactions to a drug or biological means that the product is effective.102
Government health officials have said that COVID-19 vaccines will be approved for use in children of any age by early 2022.103 With the majority of adults suffering very strong COVID vaccine reactions, especially younger adults,104 105 why are there plans to give the messenger RNA cell disrupter biological to infants and young children when the CDC says the majority of chilren with COVID-19 disease either have mild symptoms or no symptoms at all? 106
The enormous sums of money that Big Pharma and government is spending on television and digital ad campaigns to make sure that every child and adult in America gets a COVID-19 vaccine is creating false impressions and assumptions. When public policy precedes the science and aggressive advertising campaign blur the lines between facts and myths, truth gets lost in the spin and nobody is safe.
Go to NVIC.org and learn more about SARS-Cov-2 and the biological product being referred to as the COVID-19 vaccine on our new coronavirus information pages.
Go to NVICAdvocacy.org, where you can learn how to help defend informed consent rights in your state so you can make voluntary decisions about vaccination for yourself and your minor children.
References
1 Fisher BL. Here Comes the 21st Century Cures Act: Say Goodbye to Vaccine Safety Science. NVIC Newsletter July 21, 2015.
2 Ramsey L, Friedman LF. The government agency in charge of approving drugs gets a surprising amount of money from the companies that make them. Business Insider Aug. 17, 2016.
3 Fisher BL. End Pharma Liability Shield Endangering Public Health and Human Rights. NVIC Newsletter Nov. 8, 2016.
4 The Vaccine Reaction. Drug Companies Pay FDA and NIH to Fast Track and Market Vaccines. Sept 28, 2018.
5 Fisher BL. WHO, Government, Gates & Government: Who’s Calling the Shots? NVIC Newsletter Jan. 27, 2019.
6 National Academies of Sciences, Engineering, and Medicine. Public–private partnership responses to COVID-19 and future pandemics: Proceedings of a workshop—in brief. Washington, DC: The National Academies Press 2020.
7 U.S. Government Accountability Office (GAO). COVID-19: Federal Efforts to Accelerate Vaccine and Therapeutic Development But More Transparency Needed on Emergency Use Authorization. Nov. 17, 2020.
8 National Institutes of Health. NIH clinical trial of investigational vaccine for COVID-19 begins. NIH Press Release Mar. 16, 2020.
9 Lurie N, Saville M et al. Developing Covid-19 Vaccines at Pandemic Speed. NEJM Mar. 31, 2020
10 Fisher BL. COVID-19 Meltdown and Pharma’s Big Money Win. NVIC Newsletter Apr. 1, 2020.
11 Kollewe J. From Pfizer to Moderna: Who’s making billions from Covid-19 vaccines? The Guardian Mar. 6, 2021.
12 Egan M. Pfizer and Moderna could score $32 billion in Covid-19 vaccine sales – in 2021 alone. CNN Dec. 11, 2020.
13 Megan Garnett Coyle. Ad Tech Leaders Unite to Measure the Ad Council & COVID Collaborative’s COVID-19 Vaccine Education Initiative – the Largest PSA Campaign in US History. Businesswire Mar. 30. 2021.
History
14 Medical Xpress. US launches major COVI vaccination ad campaign. Apr. 1, 2021.
15 Lee B. How is Consumer Drug Advertising Regulated in the United States? June 17, 2019.
16 Harvard Health Publishing. Do not get sold on drug advertising. February 2017.
17 Rapaport L. U.S. health care industry spends $30 billion a year on marketing. Reuters Jan. 8, 2019.
18 Kanski A. Nielsen: Pfizer tops list of biggest pharma advertisers in 2018. Medical Marketing & Media Apr. 2, 2019.
19 Johnson B. Up in Smoke: Documents from the Annals of Tobacco Marketing. Ad Age Mar. 29, 2010.
20 Meyer R. Profiteering off a Covid vaccine. World of DTC Marketing Mar. 25, 2021.
21 Kollewe J. From Pfizer to Moderna: Who’s making billions from Covid-19 vaccines? The Guardian Mar. 6, 2021.
22 Dunleavy BP. Pfizer CEO says need for third dose of COVID-19 vaccine ‘likely.’ UPI Apr. 16, 2021.
23 Weintraub EW. Federal spending on COVID-19 vaccine candidates tops $9 billion, spread among 7 companies. USA Today Aug. 10, 2020.
24 The College of Physicians of Philadelphia. Vaccine Development, Testing and Regulation. The History of Vaccines Jan. 17, 2018.
25 Broom D. 5 charts that tell the story of vaccines today. World Economic Forum June 2, 2020.
26 Fisher BL, Parpia R. 2005 PREP Act and 1986 Act Shield Vaccine Manufacturer’s from Liability. The Vaccine Reaction Aug. 10, 2020.
27 Fisher BL. The New Internet Police Protecting You from Freedom of Thought and Speech. NVIC Newsletter Dec. 3, 2018.
28 Caceres M. When Even the New York Times Doesn’t Pass Facebook Muster. The Vaccine Reaction Dec. 28, 2020.
29 Mercola J. New Thought Police NewsGuard Is Owned by Big Pharma. Jan. 24, 2020.
30 Fisher BL. Vaccination and Censorship: The Truth Will Set Us Free. NVIC Newsletter Jan. 26, 2021.
31 O’Neill J. White House working with social media giants to silence anti-vaxxers. New York Post Feb. 19, 2021.
32 Attkisson S. CENSORED: The National Vaccine Information Center. Mar. 8, 2021.
33 Presson J. Questions linger about COVID-19 vaccine. The Mountaineer Feb. 12, 2021.
34 Droesch B. US Healthcare and Pharma Is Among the Fastest-Growing Digital Ad Spenders. EMarketer Oct. 9, 2020.
35 Droesch B. US Healthcare and Pharma Is Among the Fastest-Growing Digital Ad Spenders. EMarketer Oct. 9, 2020.
36 Silk B. Why Digital Is the Future for Pharma Advertising. Ethoseo Oct. 15, 2019.
37 Robbins R. Get ready for more drug ads: Facebook is making a bid for pharma dollars. STAT News Nov. 1, 2016.
38 Holmes K, Kaufman E. HHS begins national vaccine ad campaign with You Tube ads. CNN Dec. 4, 2020.
39 DHHS. U.S. Department of Health and Human Services Launches Nationwide Network of Trusted Voices to Encourage Vaccination in Next Phase of Public Education Campaign. HHS Press Office Apr. 1, 2021.
40 Facher L. The White House is set to unveil a wide-reaching billion-dollar campaign aimed at convincing every American to get vaccinated. STAT News Mar. 15, 2021.
41 Associated Press. Celebrities Make a Stand for COVID-19 Vaccines on TV Special. Voice of America Apr. 16, 2021.
42 Walmart. Administering COVID-19 Vaccines. Apr. 21, 2021.
43 Hoffman DC. Mass COVID-19 Vaccination Site Set to Open at PPG Paints Arena. KDKA2 Mar. 15, 2021.
44 Archie A. This Indiana school district is helping high schoolers get a COBID-19 vaccine before prom. Louisville Courier Journal Apr. 13, 2021.
45 AdventHealth News. AdventHealth Partners with Churches to Provide COVID-19 Vaccines. Apr. 20, 2021.
46 Collins FS. Statement from NIH and BARDA on the FDA Emergency Use Authorization of the Moderna COVID-19 Vaccine. NIAID Dec. 18, 2020.
47 Pfizer Inc. Pfizer and BioNTech Announce Further Details on Collaboration to Accelerate Global GOVIC-19 Vaccine Development. Businesswire Apr. 9, 2020.
48 Macrotrends. Pfizer Revenue 2006-2020. January 2021.
49 NASDAQ. Pfizer sees about $15 billion in 2021 sales from COVID-19 vaccine. Feb. 2, 2021.
50 NASDAQ. Moderna Earnings Date, Estimates & History. MarketBeat Apr. 16, 2021.
51 CBS News. Moderna forecasts $18.4 billion in COVID-19 vaccine sales. Feb. 28, 2021.
52 Yen H, Mattise J. Half of US adults have received at least one COVID-19 shot. Associated Press Apr. 18, 2021.
53 Syal A. Is It Safe to Visit Grandparents After Getting COVID Vaccine? NBC Feb. 14, 2021.
54 Pfizer Inc. The Facts About Pfizer and BioNTech’s COVID-19 Vaccine. Jan 6, 2021.
55 Banks MA. What Are mRNA Vaccines, and Could They Work Against COVID-19? Smithsonian Magazine Nov. 16, 2020.
56 Trafton A. Explained: Why RNA vaccines for Covid-19 raced to the front of the pack. MIT News Office Dec. 11, 2020.
57 Langreth R, Krege N. Moderna Wants to Transform the Body Into a Vaccine-Making Machine. Bloomberg News Aug. 11, 2020.
58 Harris R. Long-Term Studies of COVID-19 Vaccines Hurt by Placebo Recipients Getting Immunized. NPR Feb. 19, 2021.
59 Pardi N, Hogan MJ et al. mRNA vaccines – a new era in vaccinology. Nature Reviews Drug Discovery 2018; 17: 261-279.
60 Jaffe-Hoffman M. Could mRNA COVID-19 vaccines be dangerous in the long- term? Jerusalem Post Nov. 17, 2020.
61 Odell J. Messenger RNA (nRNA) SARS Coronavirus ‘Vaccines’ and their Potential Autoimmunity Part 2. Bioregulatory Medicine Institute Feb. 24, 2021.
62 Arvin AM, Fink K et al. A perspective on potent antibody-dependent enhancement of SARA-Cov-2. Nature 2020; 584: 352-363.
63 Healthline. How Long Does Immunity Last After COVID-19?: How vaccine-induced immunity after receiving immunization works. Feb. 24, 2021.
64 FDA. Pfizer-BioNTech COVID-19 Vaccine. Dec. 11, 2020.
65 FDA. Moderna COVID-19 Vaccine. Dec. 18, 2020.
66 Heidt A. FDA to Require 50 Percent Efficacy for COVID-19 Vaccines. The Scientist July 1, 2020.
67 Crist C. Early Vaccines Will Prevent Symptoms, Not Virus. WebMD Oct. 28, 2020.
68 Syal A. Is It Safe to Visit Grandparents After Getting COVID Vaccine? NBC Feb. 14, 2021.
69 Rouan R. Fact Check: CDC recommends masks in most cases even after COVID-19 vaccines. USA Today Apr. 22, 2021.
70 Crow S. The CDC Says These 3 Side Effects Mean Your Vaccine Is Working. Yahoo Feb. 15, 2021.
71 Finberg R. No, vaccine side effects don’t tell you how well your immune system will protect you from COVID-19. Yahoo News Apr. 19, 2021.
72 Hendler C. Severe Reactions to COVID-19 Vaccine Close Schools in Michigan, Ohio and New York. The Vaccine Reaction Mar. 8, 2021.
73 Farber M. Is the COVID-19 vaccine effective if you don’t have a reaction to it? Fox News Feb. 9, 2021.
74 Bircher AJ. Symptoms and danger signs in acute drug hypersensitivity. Toxicology 2005; 209(2): 201-207.
75 Davidovici BB, Wolf R. The challenge of drug-rechallenge: Facts and controversies. Clin Dermatol 2010; 281(3): 249-253.
76 GlaxoSmithKline Biologicals. Highlights of Prescribing Information for INFANRIX – diphtheria and tetanus toxoids and acellular pertussis vaccine adsorbed suspension: Contraindications, Warnings and Precautions. Nov. 20, 2019.
77 MedAlerts. Search the VAERS Database.
78 FDA. VAERS Overview. Mar. 29, 2019.
79 CDC. Vaccine Safety: Vaccine Adverse Event Reporting System (VAERS).
80 LaVigne P. The Story Behind MedAlerts. NVIC Newsletter Aug. 20, 2013.
81 The College of Physicians of Philadelphia. Vaccine Injury Compensation Programs: National Childhood Vaccine Injury Act (NCVIA)/National Childhood Vaccine Injury Program (NCVIP). The History of Vaccines Jan. 17, 2018.
82 Harvard Pilgrim Health Care, Inc. Electronic System for Public Health Vaccine Adverse Event Reporting System. AHRQ 2011.
83 The Vaccine Reaction. Moderna’s COVID-19 Vaccine Provokes COVID-Like Symptoms in Phase 3 Trial. Oct. 19, 2020.
84 Fisher BL. Over 3,000 “Health Impact Events” After COVID-19 mRNA Vaccinations. The Vaccine Reaction Dec. 22, 2020.
85 Gale J. COVID-19 vaccine side effects hit some recipients hard; that’s not all bad. Here’s what to do about them. Seattle Times Mar. 11, 2021.
86 Sforza T. Health care worker dies after second dose of COVID vaccine, investigation underway. Orange County Register Feb. 4, 2021.
87 Percy N. Kaiser says Pfizer vaccine likely not cause of Calfornia woman’s death. Mercury News Feb. 15, 2021
88 Brown E. Fact Check: Have 966 People Died After Receiving the COVID vaccine? Newsweek Mar. 8, 2021.
89 Goldstein S. Blood clots prevalent with Pfizer and Moderna Vaccine as with Astra Zeneca’s study. Dow Jones/Market Watch Apr. 16, 2021.
90 Ma A. Schuster-Bruce C. Johnson & Johnson asked other drugmakers to help it study blood-clot risks, and Moderna and Pfizer decline, report says. Business Insider Apr. 16, 2021.
91 Scribner H. Recent vaccine news should improve further confidence, doctor says. Deseret News Apr. 15, 2021.
92 Beusekom MV. Study: COVID much more likely than vaccines to cause blood clot. CIDRAP Apr. 15, 2021.
93 Fisher BL. Miami Obstetrician Develops Bleeding Disorder, Dies After Getting COVID-19 Vaccine. The Vaccine Reaction Jan. 11, 2021.
94 Israel National News. Mexican doctor hospitalized after receiving COVID-19 vaccine. Jan. 2, 2021.
95 Microsoft News. 72-year old man sent to ICU following COVID-19 vaccination; MOH confirms cardiac arrest wasn’t caused by vaccine. Feb. 19, 2021.
96 Fisher BL. Healthy Mom, 39, in Utah Dies of Organ Failure Days After Moderna COVID Vaccination. The Vaccine Reaction Mar. 15. 2021.
97 The Vaccine Reaction. Woman Dies Immediately After Getting COVID-9 Vaccine in Virginia. Feb. 21, 2021.
98 Haglage A. No evidence COVID-19 vaccines cause death epidemiologists say: ‘Coincidences are going to happen.’ Yahoo Feb. 4, 2021.
99 Rouan R. Fact check: CDC data on adverse effects of vaccine cannot determine cause. USA Today Apr. 8, 2021.
100 CDC. Local Reactions, Systemic Reactions, Adverse Events and Serious Adverse Events: Pfizer COVID-19 Vaccine. Dec. 13, 2020.
101 FDA. Moderna COVID-19 Vaccine. Dec. 18, 2020.
102 Finberg R. No, vaccine side effects don’t tell you how well your immune system will protect you from COVID-19. Yahoo News Apr. 19, 2021.
103 Thomas N. Fauci expects almost all children to be eligible for Covid-19 vaccines by first quarter 2022 at the latest. CNN Apr 18, 2021.
104 Koweek M. Younger adults are having harsher Covid vaccine side effects. WHIO TV Mar. 5, 2021.
105 Bendix A. Why you can expect more severe vaccine side effects if you’re younger or a woman. Business Insider Apr. 6, 2021.
106 CDC. COVID-19 in Children and Teens: What You Need to Know. Mar. 17, 2021.
May 16, 2021
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine, United States |
Leave a comment

 Aletho News
Aletho News