Doctor and nurse deaths from COVID-19 vaccines were always going to be the focus of cover-ups. The reason is practical: the state needs doctors and nurses to enthusiastically push COVID-19 vaccines on their patients, and it needs these same doctors and nurses to stay silent about COVID-19 vaccine injuries and deaths.
Doctors and nurses mustn’t know that their colleagues are dying suddenly from the same COVID-19 mRNA vaccines that they are pushing daily on their own patients.
31 year old NZ nurse died 4 days after booster shot
Divya Simon, 31, a rest home nurse, had her third COVID-19 booster vaccination four days before suffering a massive heart attack, according to a decision from coroner Luella Dunn released today. (click here)
“She had the booster on January 25 last year, and took the next day off work because she felt unwell. She complained of pain in the left side of her neck and shoulder.
Simon, who had two children aged 4 and 2, worked a night shift on January 28 returning home early the next morning and went to sleep at 10am. After she woke mid-afternoon she went to have a shower and told her husband she felt dizzy and had chest pains. That evening she had a cardiac arrest.
Ambulance arrived and Simon was given adrenalin, shocked and taken to Waikato Hospital. There she was intubated and taken to ICU but was not responsive and continued to deteriorate, dying the next day at 11am.
Dunn said an angiogram was unable to determine the cause of the cardiac arrest and there were no medical records to indicate why Simon would suffer a heart attack.
The pathologist who conducted her autopsy told the coroner Simon’s death was most likely related to an underlying weakness in her coronary arteries.
The pathologist found no evidence to suggest Simon’s vaccination contributed in any way to her death and the Centre for Adverse Reaction Monitoring came to the same conclusion.”
Case Closed!
That’s it. Case closed. A healthy 31 year old nurse had a massive heart attack 4 days after her COVID-19 booster shot and it was definitely not the booster shot, although the pathologist had no idea why she died.
But the pathologist is lying. And I can prove it.
New Zealand does not perform autopsies with immunohistochemical staining of tissue samples for the COVID-19 vaccine spike protein.
So when the pathologist said he “didn’t find evidence” of COVID-19 vaccine damage, that was a lie. He “didn’t find evidence” because he didn’t look for it – he did not conduct the proper staining of the pathology samples, because no one in New Zealand does.
“There is no current test (in New Zealand) that will show the Covid-19 vaccine in the heart tissue” as reported by One News New Zealand (click here)
26 year old NZ man died of myocarditis due to Pfizer COVID-19 Vaccination
Let’s look at a different case where the pathologist linked a sudden death to the Pfizer COVID-19 mRNA vaccine – the case of 26 year old NZ man Rory Nairn (click here)
Rory Nairn died of myocarditis after 1st dose of Pfizer COVID-19 vaccine.
Coroner Sue Johnson opened an inquiry into his death. After hearing evidence from pathologist Dr Noelyn Hung, Johnson said she is satisfied that the COVID-19 vaccine caused the myocarditis from which Nairn died.
Hung carried out an intensive pathological examination of the heart. She stated that the cause of the myocarditis came down to a diagnosis by exclusion.
There is no current test that will show the Covid-19 vaccine in the heart tissue, but Hung was able to exclude other causes of myocarditis. Hung also excluded all other known potential causes including certain medicines.
There was no sign of any infection or any other reason for Nairn’s death except in the myocardium (the middle muscular layer of the heart). Johnson accepted Hung’s medical opinion that the direct cause of Nairn’s death was acute myocarditis – consistent with vaccine-related myocarditis.
What this means
If there is no test available to check for COVID-19 vaccine injury to body tissues, you cannot exclude the vaccine as the cause of death. In the case of the 31 year old nurse Divya Simon, the pathologist cannot conclude “the COVID-19 vaccine didn’t do this” or “there is no evidence the COVID-19 vaccine did this”. It is not possible to come to this conclusion, because the pathologist had no way of proving this.
In the case of 26 year old Rory Nairn, COVID-19 vaccine myocarditis was declared the cause of death because every other possibility was excluded. It was the diagnosis of exclusion.
Notice the difference?
The 31 year old nurse death was a cover-up. The pathologist lied. New Zealand’s Centre for Adverse Reaction Monitoring lied. They covered-up her death. Almost certainly because she was a nurse.
My Take…
It should not surprise anyone by this point, that deaths of doctors and nurses will be treated very differently and will be covered up at all costs.
When 3 Canadian doctors died within days of each other in the same Trillium Health Hospital in Mississauga, Ontario, days after the rollout of the 4th COVID-19 vaccine (2nd booster shot), mainstream media called it a coincidence (click here) (click here)
That’s why my reporting on 132 Canadian doctor sudden deaths since the rollout of the COVID-19 vaccines has been so “controversial”.
The fiercest attacks I have faced from mainstream media so far, were about me exposing the sudden deaths of fully COVID-19 vaccinated Canadian doctors.
So whenever you see a case like this where a coroner or pathologist declares that “COVID-19 vaccine didn’t cause this death”, you will know they are lying, and you will be able to explain exactly why they are lying.
They can allow the occasional citizen’s death to be linked to the COVID-19 vaccine. But they cannot and will not allow a doctor or nurse’s death to be linked to the vaccine.
The Telegraph’s publishing of former UK Health Czar Matt Hancock’s private Whatsapp messages has been dubbed ‘The Lockdown Files.’ The messages detail multiple interactions demonstrating the U.K. Government’s willingness to abandon science and a reasoned approach to Pandemic measures, for coercion and control of the British people.
Former CDC Director, Dr. Robert Redfield, testified before The House Selection Committee on the Coronavirus Pandemic this week, letting loose on Anthony Fauci, Deborah Birx, Francis Collins, gain-of-function research and the lab origin debate detailing what he witnessed in early 2020. His testimonials are nothing short of historical.
By late 2021 it was already clear in the UK that the covid vaccines did not stop infection or transmission. And there were also already plenty of concerning safety signals. So, even though the “vaccine pass” was then required in the UK to participate in daily life, ‘vaccine hesitancy’ was on the increase.
Switching narrative to counter vaccine ‘hesitancy’
Given this increasing resistance against the vaccine programme, the official messaging was changed from “vaccines stop you getting covid” to “vaccines stop you being hospitalised and dying from covid”.
To push this new narrative the Government started pumping out ‘data’ to support the claim that almost all of those ill in hospital with covid were unvaccinated. Here is an NHS text that was sent to everybody registered with a GP in the UK in November 2021:
Vast majority of those vaccinated were not “fully vaccinated”
At the time the text was sent out, “fully vaccinated” in the UK was defined as: “at least 14 days since 3rd jab” or “between at least 14 days and less than 6 months of 2nd jab”. So, the official figure of 8 out of 10 “not fully vaccinated” might have been right but was totally misleading since almost ALL of those who were vaccinated (i.e., had at least one jab) at that time were “not fully vaccinated”.
This creates a false semantic equivalence between ‘unvaccinated’ and ‘not fully vaccinated’.
A particularly serious example was the ludicrous claim made in the BBC documentary “Unvaccinated” by Dr Mehool Patel (Consultant, University Hospital Lewisham). His statement – unchallenged in the programme – was:
“We looked at about 550 patients that were admitted in our trust between the 15th December and 15th January 2022, which in effect would mean that most if not all of them were through due to Omicron variant, and of that there were unfortunately 21 patients who had to be admitted to intensive care who were the most severe patients due to COVID. Of the 21 I’m afraid 20 of them were unvaccinated, that’s 95%.
Just one person was vaccinated. And of the 21 who were on the unit, I’m afraid unfortunately seven of them didn’t make it, all of them were unvaccinated, 100%. So that’s one figure to just illustrate the point.”
“You maintain that this claim was “either false/exaggerated or an unbelievable outlier”.
I have approached the programme makers for information about the data which were quoted by Dr Patel. I have been advised that the figures were compiled by Dr Patel himself for the purposes of research.
“Lewisham and Greenwich Hospital Trust does not record the vaccination status of patients in ICU so Dr Patel’s figures cannot independently be verified.”
Deliberately murky record keeping used to manipulate data
But the scam was based on something even more ludicrous than classifying “not fully vaccinated” as “unvaccinated”.
As a result of Freedom of Information Requests sent to some individual NHS trusts we now know that some hospitals were using the NIMS system to classify vaccine status of patients while others were using their own systems. This meant that, in many cases even if a patient had a vaccination record in NIMS, if the patient was not vaccinated in that particular hospital/Trust they were recorded as unvaccinated. Some hospitals were using a mixture of both systems (NIMS where a death was recorded and an internal system where a covid case was recorded). For those relying on NIMS, since it was not operational until June 2021, all deaths within the hospital would have had an unknown vaccination status between Jan-June 2021. The problem is that some hospitals were classifying “unknown” as “unvaccinated”.
So, deliberately murky record keeping was used to manipulate the data.
To see the implications of this, here are the data on hospital deaths (all deaths, not just covid) from the start of the vaccine programme until the end of 2021 from an undisclosed NHS trust who responded to an FOI request:
Note that every death up until 21 June 2021 was recorded as unvaccinated simply because hospitals in this Trust were using the NIMS system for classifying deaths which was not up and running until then. But, of course, an unknown number (probably most) of these 742 people were vaccinated.
There are plenty of other anomalies in the data. Note the improbable, sudden and dramatic trend changes:
A steady decline in “unvaccinated” deaths from 21 June until 13 Sept. In week ending 13 Sept only 4 out of 46 (less than 9%) were unvaccinated.
The next week (20 Sept) the unvaccinated are suddenly the majority again with 21 out of 31 deaths (68%), and this increases so quickly that just 3 weeks later (11 Oct) all 44 deaths (100%) are ‘unvaccinated’.
But then we get a sudden and rapid decline in the unvaccinated deaths. Just 2 weeks later (25 Oct) the unvaccinated are 13 out of 47 deaths (28%) and by 20 Dec none of 53 deaths (0%) were unvaccinated.
Such changes can only be the result of changes in definition of who should be classified as unvaccinated.
It is easy to see how the Government could cherry pick this kind of data to present the narrative they wanted. When the text messages were being sent out in November 2021 it is reasonable to assume that they were using the cumulative data up to, say, mid-October. Then using the data in the table up to and including 18 Oct 2021 we count:
1051 “unvaccinated” (including 17 with just a single jab)
370 “vaccinated” (with 2 jabs).
That gives 74% of all hospital deaths classified as “unvaccinated”.
But this is all an illusion. In fact, counting just the final three weeks of the data (6-20 Dec), just 18 out of the 144 deaths (12.5%) were unvaccinated.
It is also worth noting that the same NHS Trust provided the following information on “new COVID positives” in its hospitals between 19th Jan 2021 and 19th Jan 2022.
Given what we know about national vaccination take-up rates, and this Trust’s own death data, it is likely that the majority of those classified as ‘unvaccinated’ here would have been vaccinated (with the exception of those in the 0-20 age categories the vast majority of whom would not have been eligible for vaccination).
So, instead of the ‘50% of new covid cases’ being among the unvaccinated – the ‘official’ narrative pushed from this data – the true narrative should have been that the vast majority of new covid cases were vaccinated.
Why does this matter?
It matters a lot because, despite being completely bogus, these kinds of ludicrous figures were so consistently repeated that the message “vaccines stop you being hospitalised and dying from covid (even if they don’t stop infection and transmission)” was almost universally accepted. Even the strongest critics of the Government’s covid response consistently repeated this mantra:
The figures were also used as the basis for the bogus studies claiming millions of lives were saved by the vaccine.
So, yet again, we can see that statistical data was used to create an illusion of vaccine hospitalisation and mortality efficacy by the simplest of means: deliberately murky record keeping ensuring that the vaccinated get recategorized as unvaccinated when they die or are hospitalised.
Update 9 March 2023: Here is a video I made covering this article:
Postscript: A commenter below reports that the USA “was far worse”:
Can you create cutting edge “deep fake” videos, spy on people using household appliances, and make massive data dragnets? If so, the Pentagon wants to hear from you so it can amp up its manipulation efforts.
US Special Operations Command (US SOCOM) has issued proposal requests for a whole host of dodgy services, according to new documents obtained by The Intercept.
Specifically, the Pentagon is looking for “next generation capability to ‘takeover’ Internet of Things (IoT) devices in order to collect data and information from local populaces to enable a breakdown of what messaging might be popular and accepted through sifting of data once received.”
For what purpose? “This would enable MISO [Military Information Support Operations] to craft and promote messages that may be more readily received by the local populace in relevant peer/near peer environments,” according to the document.
Despite publicly obsessing over others’ foreign interference and propaganda, Washington is now openly admitting that it is actively seeking these new technologies for its own “influence operations, digital deception, communication disruption, and disinformation campaigns at the tactical edge and operational levels.” You know, exactly the same kind of thing, over which it drums up fear as a threat to freedom and democracy among the general public.
Earlier this year, a Washington-based advisory firm OODA published a report warning that Chinese-made household items could not only be spying on you, but basically fronting for the Chinese government. The report’s author called for the British government to act on claims that Chinese-made Internet of Things appliances, and even car components, can collect and transmit data through cellular 5G networks to Chinese companies, which could then be ordered to pass it on to the government. The story was hysterically splashed across British media.
OODA describes itself as a “global strategic advisory firm with deep DNA in global security, technology and intelligence issues.” The genetics run deep, indeed: straight to the Pentagon and Western intelligence communities where its executives, experts and advisers have past or current working relationships.
So now it looks like calls to ban Chinese household appliances for their spying potential have turned into Washington wanting to get in on the action by obtaining the best possible front row seat as you stand in front of your refrigerator at midnight, chugging chocolate milk straight from the carton.
The Pentagon also wants to be able to create “deep fake” videos that can realistically portray fake events as real, in an attempt to manipulate the target viewer(s). Or, as the Pentagon puts it, to “generate messages and influence operations via non-traditional channels in relevant peer/near peer environments.” It’s hard to imagine a more glaring example of actual fake news, yet the Pentagon wants to produce it in the way that Netflix makes movies and TV shows.
Finally, the Pentagon says that they want to get their hands on “a next generation capability to collect disparate data through public and open source information streams such as social media, local media, etc. to enable MISO to craft and direct influence operations and messages in relevant peer/near peer environments.”
Some might be tempted to just shrug this off as conventional practice because, when the military is tracking down bad guys, they’re obviously going to want to use every possible tool available at their disposal – and constantly seek to expand that tool box. But recent evidence suggests that military-grade collection and subversion tools targeting online and conventional information platforms have largely been turned on the average citizen for the purpose of protecting the establishment and its various narratives from dissent rather than for reasons of national security.
Last December, for example, Twitter CEO Elon Musk worked with a journalist to reveal the collusion between US government authorities and the social media platform to manipulate and censor public debate over the Covid-19 pandemic. According to internal Twitter documents, one of the first meetings that the Biden Administration requested with Twitter executives was on the topic of Covid vaccines and specific high-profile accounts that deviated from the official narrative. According to the journalist, David Zweig, “Twitter did suppress views – many from doctors and scientific experts – that conflicted with the official positions of the White House. As a result, legitimate findings and questions that would have expanded the public debate went missing.” He added that, “With Covid, this bias bent heavily toward establishment dogmas,” and cited examples of various experts, including prominent epidemiologists, whose views were censored as a result of being qualified by the Twitter staff as Covid “misinformation.”
Earlier this year, a British whistleblower also revealed that critics of Covid-19-related lockdowns and vaccine mandates – including prominent journalists and politicians – were monitored by the UK army’s information warfare brigade. The 77th Brigade, created in 2015 and described by the media at the time as composed of “warriors who don’t just carry weapons, but who are also skilled in using social media such as Twitter and Facebook, and the dark arts of ‘psyops’”.
The Canadian military was also caught using propaganda techniques honed on the battlefield in Afghanistan to shape the Covid debate by boosting the government’s narrative and attempting to head off any civil unrest over the harsh mandates.
The Pentagon’s latest wish list raises concerns that these tools will also be deployed on average Americans or Westerners for purposes of control and manipulation. Last September, the Pentagon vowed to review its secret psyops, but only after public outrage when a group of researchers suggested collusion between US government entities and American online platforms like Twitter and Facebook to control online narratives with fake accounts. Was the lesson learned to stop deploying psyops on average citizens? Or was it just to do a better job of keeping it secret?
Not that there’s any shortage of Western establishment cheerleaders demanding even more psychological manipulation efforts by the US government, if only to counter “disinformation” from foreign adversaries.
It seems that we’ve now come to the point where sticking it to Russia and China means actively cheerleading the increasingly militarized efforts by our self-styled defenders of freedom and democracy to brainwash their own people.
The 1840 Treaty of Waitangi between the British Crown and Maori chiefs was a landmark event in the history of New Zealand. Drafted in English, a Maori translation was prepared, ostensibly to ensure that Maori could have an accurate understanding of the terms. In retrospect, it is less clear that a meeting of the minds was intended:
The English and Māori texts differ.As some words in the English treaty did not translate directly into the written Māori language of the time, the Māori text is not a literal translation of the English text.It has been claimed that Henry Williams, the missionary entrusted with translating the treaty from English, was fluent in Māori and that far from being a poor translator he had in fact carefully crafted both versions to make each palatable to both parties without either noticing inherent contradictions.
“The covid vaccine is 95% effective” is a contemporary Treaty of Waitangi. The original is in the language of clinical trials. It was never translated. The public interpreted this phrase in their native language, normal English. What Pfizer said and what the public heard were quite different. The public would have been far more skeptical of these products had the clinical trial results been translated into normal English.
What we need is a proper translation and an explanation of how miscommunication happened.
The products were never expected to stop infection or transmission.
The clinical trials did not test for their ability to do so.
A clinical trial is designed to test a drug for effectiveness, which is strictly defined by one or more endpoints. An endpoint is a measurable outcome that can be assessed for each participant. With that in mind, prevention of infection was not an endpoint of the BioNTech/Pfizer injection clinical trials. And, this was known in 2020 before the products were approved for emergency use and distributed to the public starting in 2021.
In this New England Journal of Medicine research summary, Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine, under Limitations and Remaining Questions, we find that “whether the vaccine protects against asymptomatic infection and transmission to unvaccinated persons” remains unanswered by the clinical trial.
What did the clinical trial test for, if not the ability of the mRNA vaccine to stop transmission and/or infection? The trial was designed to test the ability of the injections to prevent “symptomatic Covid 19 cases” defined as one or more of a number symptoms and a positive test (see page 7 of the supplementary appendix for details).
@pfizertweeted in Jan 2021 that stopping transmission was their “highest priority”. Their product does not do that, nor did the tweet make a claim that it did so. But it was their highest priority nonetheless. That, and getting as many people injected as possible.
Failure to Prevent Infection Was Known Before the Rollout
In October 2022, a Pfizer executive testified to an EU body that Pfizer had not tested the ability of the vaccine to stop transmission. This story was shocking to some and generated accusations that Pfizer had lied about the capabilities of the shots. But this information had been available since the trial results were released early in 2021. Pfizer had already been criticized for this.
One of the more immediate questions a trial needs to answer is whether a vaccine prevents infection. If someone takes this vaccine, are they far less likely to become infected with the virus? These trials all clearly focus on eliminating symptoms of Covid-19, and not infections themselves. Asymptomatic infection is listed as a secondary objective in these trials when they should be of critical importance.
Will covid-19 vaccines save lives? Current trials aren’t designed to tell us
Peter Hotez, dean of the National School of Tropical Medicine at Baylor College of Medicine in Houston, said, “Ideally, you want an antiviral vaccine to do two things . . . first, reduce the likelihood you will get severely ill and go to the hospital, and two, prevent infection and therefore interrupt disease transmission.”
Yet the current phase III trials are not actually set up to prove either. None of the trials currently underway are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus….
Is It Even a Vaccine?
A vaccine that prevents infection is known as “neutralizing” or “sterilizing”. I am a software engineer with no training in medicine, pharmacology or clinical trials. I consider myself a good barometer of what the average untrained person would think about such things. Prior to 2021 I had thought that immunity was a necessary condition for a drug to earn the title of “vaccine”. If anyone had asked me, I would have told them that the Covid injections were a treatment, not a vaccine.
A vaccine is a biological preparation that provides active acquired immunity to a particular infectious or malignant disease. … A vaccine typically contains an agent that resembles a disease-causing microorganism and is often made from weakened or killed forms of the microbe, its toxins, or one of its surface proteins. The agent stimulates the body’s immune system to recognize the agent as a threat, destroy it, and to further recognize and destroy any of the microorganisms associated with that agent that it may encounter in the future.
Cornell Law provides the following legal definition of vaccine, sourcing 26 USC § 4132(a)(2), which is consistent with the above:
The term “vaccine” means any substance designed to be administered to a human being for the prevention of 1 or more diseases.
The definition published by the CDC prior to 2021 said much the same. But the CDC website changed the definition on or after August 2021. The older version found on the internet archive is here (emphasis added):
Immunity: Protection from an infectious disease. If you are immune to a disease, you can be exposed to it without becoming infected.
Vaccine: A product that stimulates a person’s immune system to produce immunityto a specific disease, protecting the person from that disease.
Vaccine: A preparation that is used to stimulate the body’s immune response against diseases.
The earlier pair of definitions is quite easy to understand. The latter, much more difficult. What exactly is a “preparation”? Does a vaccine stimulate the body or only prepare the body? What is or is not a vaccine according to the new definition?
While the CDC may think that they can change the meanings of words whenever they like, public memory retains the original meaning. The assumption of immunity permeates almost all non-expert level discussion of vaccines. A web search for “why are vaccines good” shows results that assume or imply immunity.
Even the CDC did not finish the job of memory-holing the old language. On the very same CDC website, under 5 Reasons It Is Important for Adults to Get Vaccinated, we read “By getting vaccinated, you can protect yourself and also avoid spreading preventable diseases to other people in your community.” And then, “Vaccines Can Prevent Serious Illness”.
The timing of the CDC’s edit suggests to me that prior to 2021, the CDC had the same understanding of vaccines as I do. I believe that they wanted a new definition because they knew that the products being developed at warp speed were not vaccines in the original sense of the word. And it was important that those products be called “vaccines” for reasons that I will explain later. This incident brings to mind a meme that I no longer have a link to. captioned: “We changed what ‘definition’ means so you can’t say that we redefined anything.”
What Does “95% Effective” Mean?
The “95% effective” message was repeated in nearly all reporting on the clinical trials. But the question, “effective at doing what?” was rarely asked. To answer this requires walking down the links of a chain of terminology from the world of clinical trials.
The first link in the chain is “risk”. Risk is the probability of a bad outcome. These are assumed to happen randomly within a group. A clinical trial must define in advance the bad outcomes that the drug intends to avoid. The next link is “endpoint”. Each distinct bad outcome is an “endpoint”. The trial compares the endpoints between a control group who did not take the drug and a test group, who did.
The purpose of a clinical trial is to determine the ability of a drug to reduce risk. A drug that reduces risk is “effective”. There are two ways of quantifying risk reduction. From the NIH glossary:
the difference in the incidence of poor outcomes between the intervention group of a study and the control group. For example, if 20 per cent of people die in the intervention group and 30 per cent in the control group, the ARR is 10 per cent (30–20 per cent).
the rate (risk) of poor outcomes in the intervention group divided by the rate of poor outcomes in the control group. For example, if the rate of poor outcomes is 20 per cent in the intervention group and 30 per cent in the control group, the relative risk is 0.67 (20 per cent divided by 30 per cent).
The difference between the ARR and RR (also known as “RRR”, to align with ARR) is in the denominator. The ARR divides by the number of participants in one of the groups. The RRR divides by the number of people with bad outcomes in the control group – a necessarily much smaller number.
The ARR is the number most relevant for a drug – such as the Pfizer injections – that was to be given to everyone. But the RRR is the preferred method of presentation for pharma when they want to exaggerate the effectiveness of a drug because it will always be a much larger number. Would you take a drug that could reduce the incidence of a rare disease by 50%? From 10 per 1 million to 5 per 1 million is an 50% RRR and an 0.0005% ARR.
The 95% figure cited for the covid injections is the relative risk. The absolute risk reduction was 0.84%. In a slide deck from the Canadian Covid Care Alliance (CCCA), slide 11 shows how the 91% was achieved (it is 91%, not 95%, because the it refers to an earlier version of the study):
A clinical trial finding of a 1% ARR means that 99% of the people who take the drug either did not experience the condition that the drug treats, or they did experience it, but were not helped by the drug. The 1% both had the condition and were helped by the drug. Another way of saying this is the Number Needed to Treat (NNT). NNT is the reciprocal of the ARR and is the number of people who must take the drug to help one person reach the endpoint. An ARR of 1% corresponds to an NNT of 100 people.
We can now answer the question of the meaning of vaccine effectiveness. The endpoint of the trial was a severe confirmed case of covid at least 7 days after the second dose. This endpoint requires the participant in the trial to have covid symptoms and a positive covid test. “95% effective” means that 95% of the patients who had Covid symptoms and a positive test were in the control group. Five percent were in the test group.
Here’s what “95% effective” did not mean: if you take the shots, then you will have a 95% lower chance of getting covid. But that is how most people understood it because that is what the words mean in normal English.
Then the Lying Started
Once the public had their hopes raised by the false translation of the “95% effective” message, the pandemic-industrial-complex went into high gear to amplify it. They stated the incorrect message loudly, frequently, and as if it were fact. The injections would – with 100% certainty (perhaps 200%) – protect you from infection. Many of the people who said this were doctors or scientific researchers who must have understood how to interpret clinical trials.
Here are some choice quotes that did not age well:
“You’re not going to get Covid if you have these vaccinations.” Joe Biden, CNN Town Hall July 2021
“Now we know that the vaccines work well enough that the virus stops with every vaccinated person. A vaccinated person gets exposed to the virus, the virus does not infect them, the virus cannot then use that person to go anywhere else,” she added with a shrug. “It cannot use a vaccinated person as a host to go get more people. [Vaccines] will get us to the end of this.” – Rachel Maddow, March 2021
“When people are vaccinated they can feel safe that they won’t get infected, whether they’re outdoors or indoors.” – Dr. Anthony Fauci, May 2021 (outdoors: seriously?)
“Vaccination against COVID-19 prevents breakthrough infections, Stanford researchers find.” – Stanford Medicine, July 2021
The public has consistently over-estimated the infection fatality rate of Covid. Some even believed the fatality rate to be above 10%. They believed that we were in great danger. They also believed that the “95% effective” vaccine would bring the pandemic to a quick end, once everyone had taken it. Anyone who refused to do so was therefore risking not only their own life, but everybody else’s as well.
Dr Anthony Fauci estimated herd immunity would emerge when around 60% of the population had taken the vaccine … or perhaps 70, 80, no wait … 85%. Or maybe 100% (which would include large numbers who already had natural immunity). Bill Gates extended that to everyone on earth.
The narrative then turned to demonization of those who refused to submit to vaccine coercion. The selfish anti-social behavior of the anti-vaxxers with their stubborn attachment to “free dumb” that was keeping everyone locked indoors and forcing us all to wear diapers on our faces. Yale University behavioral researchers tested messaging strategies to determine whether shame, embarrassment or fear was most effective.
President Biden said that we the nation was experiencing a “pandemic of the unvaccinated”. Later, Biden ominoulsy warned the unvaccinated that he had been waiting a long time for them to get injected, but “our patience is wearing thin”. In December of 2021 the White House issued a cheery year end greeting to the vaccinated. The unvaccinated, on the other hand, were “looking at a winter of severe illness and death.” Merry Christmas.
Even South Park, which I consider a reliable source of contrarian political opinion, ran a storyline set in the year 2050 in which every single character had to be vaccinated for the 30-year pandemic to end. This episode featured one lone holdout who would not get vaccinated due to a crustacean allergy i.e. for “shellfish reasons”. This gag took aim at people who considered the vaccine to be a violation of body autonomy, and those who objected to components used in its development for religious reasons, thereby scoring a “two for one”.
Volumes can, and will, be written about the intense onslaught of propaganda aimed at getting two needles in every deltoid. I will provide one more example that represents no more than the median level of insanity; plenty of people called for the same or worse. @ClayTravis, in February 2023, tweeted the results of a Rasmussen poll from 2022:
Last January 60% of Democrats wanted to lock everyone who didn’t get the covid shot in their houses. Over 40% of Democrats wanted those who rejected the covid shot sent to quarantine camps. Over 40% also wanted anyone who criticized the covid shot fined & imprisoned. Over a quarter wanted those who didn’t get the covid shot to have their kids seized.
While there were many agendas driving the madness, the Treaty of Waitangi effect was a critical part in carrying it out. If the message had been that “everyone is going to get exposed to covid – injected or not”, then it could not have happened. The misunderstanding convinced the public that mass vaccination would stop the pandemic; and that the holdouts were prolonging it. Without this belief, none of the coercion made any sense: employment mandates, school mandates, quarantine camps, or vaccine passports. As the hysteria fades, the last remaining mandates are being dropped as the reality sinks in that the shots do not stop the spread.
Welcome to Waitangi World. I hope that you have a pleasant stay.
Robert Blumen is a software engineer and podcast host who writes occasionally about political and economic issues.
The mother of two children who were given COVID-19 vaccines without the mother’s consent is suing the doctor who administered the vaccines.
An attorney representing NaTonya McNeil last week filed a lawsuit in Superior Court for the District of Columbia against Janine A. Rethy, M.D., M.P.H.
According to the complaint, on Sept. 2, 2022, McNeil took her two older children, ages 15 and 17, to the KIDS Mobile Medical Clinic/Ronald McDonald Care Mobile clinic, operated by Georgetown Hospital, to complete their required annual physical exam for the 2022-2023 school year.
The lawsuit alleges Rethy, director of the mobile clinic, held the children in the examination room longer than necessary for a regular check-up and vaccinated them against COVID-19 over their objections and without consulting their mother
In order to attempt to obtain the children’s consent — which they are not legally able to provide without a parent or guardian — the doctor falsely informed the children the COVID-19 vaccine was mandatory for school attendance and told them they could not lawfully decline it if they wanted to attend school.
The suit, filed by D.C. Attorney Matthew Hardin, seeks damages for false imprisonment, battery and fraud.
Children’s Health Defense (CHD) is financing the lawsuit because, according to CHD President and General Counsel Mary Holland, “CHD couldn’t just sit still and not allow this wrong to go unpunished and not bring this to the public’s attention.”
In an exclusive conversation with The Defender, McNeil explained why she is suing the the doctor:
“I just feel like people shouldn’t be able to do whatever they want to do to other people and especially not to children. As a mother, I feel like, ‘You all just took all my rights away from me to do what you wanted to do to my kids.’
“I do want justice to be done in this case. I feel like something needs to be done. This can’t just continue to happen.”
‘I feel violated’
According to the complaint, Rethy’s stated goal is to vaccinate all children against COVID-19. The complaint quotes her statement to the press:
“Our goal is to increase vaccination rates in children here in D.C. . . . For more than 30 years our role has been to be in the community to help address the problem of health disparities, bringing families care where they are.
“For this particular effort, we are glad to be partnering with DC Health to provide both regular childhood vaccines and COVID-19 vaccines to all children.”
In addition to her role as director of the mobile clinic, Rethy is chief of MedStar Georgetown University Hospital’s Division of Community Pediatrics and assistant professor of pediatrics at Georgetown University School of Medicine.
McNeil said that when she took her older children to the clinic, she stayed outside the examination room to care for her infant. As soon as the children entered the doctor’s office, she called her daughter’s cellphone to let Rethy know she was just outside the door if the doctor needed to consult her for anything.
According to McNeil, the doctor did not ask or inform her about any vaccinations, and did not ask her to sign anything. At the end of the physical, Rethy came out to talk to her.
McNeil said the doctor explained her son’s asthma treatment plan, but that’s all they discussed.
As they were heading home, McNeil said she was shocked when her daughter complained that her arm hurt “pretty bad.” When McNeil asked her why it hurt, her daughter said she was given the COVID-19 shot, even though she told the doctor she didn’t want it.
When McNeil asked her why she allowed the doctor to administer the shot, her daughter said:
“When she had the needle in her hand and she was coming towards me, I backed up and I asked her what is that needle, and she said it was the COVID shot and I … told her I didn’t want it and she said, ‘Well it is mandatory, you have to get it in order to go to school.’”
Rethy allegedly administered the shot to her daughter, and then to her son. McNeil said:
“He’s 14 and he said they didn’t even ask him if he wanted it or not, but when they gave it to him, he said he thought he had to get it because his sister got it.”
According to the complaint, both children received the Pfizer/BioNTech vaccine, authorized for emergency use, and the meningococcal vaccine. Her son was also injected with TDaP.
Both children were upset and angry they had been coerced into vaccination, the complaint says.
No school mandate, despite what clinic and doctor alleged
When she got home, McNeil said she called the doctor’s office, and asked them why they vaccinated her children without her consent.
“I would have never consented to you all vaccinating my children,” she said. “I’m not vaccinated and I’m not getting vaccinated and my kids were never supposed to be vaccinated for COVID period, under no circumstances.”
She said the person on the phone said they were supposed to get them for school.
After hanging up, McNeil said she was “so irritated I even started crying” because she couldn’t believe “they put this poison” into her children’s bodies.
In July 2022, D.C. public schools imposed a vaccine mandate for schoolchildren ages 12 and up for the 2022-2023 school year. But on Aug. 26, just weeks after imposing the mandate, officials walked it back, postponing it until 2023.
That means when McNeil’s children saw the doctor, there was no school vaccine mandate in place, despite what the Rethy allegedly told the children.
The age of consent
The District of Columbia in March 2021 enacted the D.C. Minor Consent for Vaccination Amendment Act of 2020 (D.C. Minor Consent Act), allowing children 11 and older to consent to the administration of any vaccine — including COVID-19 shots — recommended by the Advisory Committee on Immunization Practices (ACIP) — without parental knowledge or consent if the medical provider believed “the minor is capable of meeting the informed consent standard.”
The law also required healthcare personnel to provide accurate immunization records to the Department of Health and to the student’s school, but not to parents with religious exemptions.
CHD and Parental Rights Foundation filed a lawsuit seeking a court order to declare the D.C. Act unconstitutional.
A judge for the U.S. District Court for the District of Columbia on March 18, 2022, granted a preliminary injunction prohibiting the D.C. mayor, Department of Health and public schools from enforcing the law.
That means at the time McNeil’s children visited the clinic, they could not legally provide consent to be vaccinated without their mother’s consent.
McNeil said:
“To do that to my little children, my innocent children. They took her rights. When she backed away from you [the doctor] and said she didn’t want it, that should have been the end of it.
“Or you [the doctor] should have called me on the phone to find out what I feel about the situation. But you [the doctor] basically told my child a lie so you [she] could do what you [she] wanted to do to my kid.”
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
A week ago I reported the story of Dr. Kirk Moore—a plastic surgeon who was recently indicted by a federal grand jury in Utah for conspiracy to defraud the US; conspiracy to convert, sell, convey, and dispose of government property; and conversion, sale, conveyance, and disposal of government property and aiding and abetting.
I initially assumed the federal investigators and prosecutors involved in the case must have found evidence to support their assertion in the indictment that Dr. Moore had “benefitted” from these transactions—that is, that HE received all or part of the $50 per procedure.
However, shortly after I posted my essay, I was contacted by people familiar with the matter who claimed that the indictment’s assertion is false. To check their assurance, I contacted Dr. Moore and conducted a long interview with him.
Dr. Moore insists that never received a single dollar for administering early treatments to COVID-19 patients or for issuing COVID-19 vaccine cards to patients who feared the mRNA gene transfer injections are not safe. A plastic surgeon by trade, he insists he administered early treatment and issued the cards solely as a charitable endeavor—that is, to help the sick stay out of hospital and to help his fellow citizens who were mandated to receive the injections in order to retain their student and job positions.
In other words, according to Dr. Moore, the federal indictment’s assertion that HE benefitted from the $50 per procedure is FALSE. Because most patients expressed their desire to pay him at least some fee for his invaluable service, he adopted the practice of instructing each to make a $50 donation to a medical freedom charity from which he received no funds. He assumed that keeping this practice strictly charitable would protect him from the charge that he received financial benefits for his actions. He claims the evidence presented in his forthcoming trial will prove that he received no benefit.
An especially intriguing detail he related in my interview is the strange fact that—though he knew he was under investigation because HHS and DHS agents visited him at his office and served him a search warrant to seize his cell phone—he was NOT subsequently served with notice that a federal prosecutor had impanelled a grand jury and secured an indictment.
He only learned about this alarming action in a press report, from which he also learned the date and time of his arraignment.
We encourage our Substack readers to learn more about Dr. Moore’s case by visiting his website: https://www.standformoore.com
After ICAN obtained the v-safe data and published to the world that 7.7% of v-safe users sought medical care (and that the CDC hid this number from the public for two years), Reuters reached out to my firm stating it had received comment from the CDC regarding this figure.
Incredibly, CDC told Reuters that the 7.7% figure was grossly inflated because it claimed there were 10 million records in v-safe, not 10 million users. Here is the exact email I received from Reuters:
“CDC says v-safe has 10 million records, not 10 million users, and that one person could submit multiple records of seeking medical care for the same adverse event. Which makes the 7.7% statistic problematic… Is that something ICAN was aware of or able to adjust for?”
Based on the CDC’s claim, the major news outlet asked if ICAN would be modifying its claim of 7.7%. But it was the CDC’s claim that was categorically false!
ICAN was correct: there were 10 million v-safe users, not 10 million records; and the 7.7% also did not double-count because it was the number of unique v-users who submitted one or more reports of seeking medical care.
The CDC was plainly pushing the major news to declare ICAN’s claim false and, hence, characterize it as misinformation.
Had Reuters just accepted the CDC’s claim, as typically occurs, it likely would have published a story declaring ICAN’s 7.7% figure to be false information.
Luckily, to its credit and because one of its reporters proceeded objectively and with integrity, this news outlet did not just take the CDC’s word for its claim. It actually gave us an opportunity to respond to this claim. (Albeit not by asking if ICAN believed it was wrong but by asking if it would adjust the figure it published.)
CDC Proven Wrong
Showing that the CDC was wrong was simple. All we had to do was use the CDC’s own data it provided to ICAN!
The data the CDC provided to ICAN clearly and without any doubt showed that ICAN was using the precise and correct number of v-safe users and the number of unique v-safe users who reported needing medical care. Meaning, the 7.7% was absolutely accurate – without any doubt.
We sent this proof and asked Reuters to please ask that CDC substantiate with actual proof, not just conclusory assertions, how ICAN was supposedly wrong and spreading misinformation. And again, to Reuter’s credit, because it demanded proof from the CDC, the CDC eventually relented!
The CDC finally conceded that v-safe did in fact have approximately 10 million users and, hence, the 7.7% figure of those who reported seeking medical care was accurate.
With that, I expected that interaction would be one heck of a story in and of itself! I foresaw a Reuters story that disclosed this CDC behavior – here was the CDC trying to get a major news outlet to publish false information! It was trying to get it to write that the 7.7% figure was incorrect.
That should have been its own major story. And although Reuters did publish a story about v-safe, thus far, these behind-the-scenes communications have not been published. I expect they never will, other than in this article.
CDC Asks Reuters to Ask ICAN for a Copy of CDC’s V-Safe Data
It gets even worse. Making plain that the CDC officials communicating with Reuters were not concerned about the facts, and instead were focused solely on pushing their “safe and effective” mantra which is typically not questioned, they further revealed the agency’s disfunction: the CDC officials asked Reuters if it could get a copy of the v-safe data from ICAN and send it back to the CDC representatives Reuters were dealing with so they can review that data. If that sounds nutty, it is because it is.
Just so you don’t think you misread the foregoing, let me repeat: CDC asked Reuters to get the v-safe data that CDC had given to ICAN days before, and then send that data back to the CDC to review.
You can’t make this stuff up. Mind you, the data had already all been made public on ICAN’s website.
What this shows is that these CDC officials were driving forward to push a major news outlet to claim to the world that ICAN’s claim of 7.7% was false without actually looking at the data to assure their claim was accurate. It also shows an incredible level of disfunction at the CDC; instead of getting the data internally, they had to ask a news outlet to get its own data produced to ICAN to then send it back to CDC.
And these are the folk that have effectively dictated what level of civil and individual rights most Americans would have over the last three years!
CDC Seeks to Deceive Again
When the foregoing gambit by the CDC did not work, it had a new gambit. It tried to get Reuters to publish that the 7.7% figure was misleading by claiming to Reuters that “[i]n the first week after vaccination, reports of seeking any medical care … range from 1-3% (depending on vaccine, age group and dose).”
But as we explained to Reuters, even this is not true. For example, 3.36% of those younger than 3 years old reported receiving medical care within one week of receiving the Moderna vaccine.
Even if all combinations of vaccine, age group, and dose resulted in between 1% to 3% of infants, children, or adults seeking medical care within one week, that is not necessarily an insignificant figure! Why is this somehow comforting? Especially in the context of vaccinating the entire country.
And why should the reports of medical care on days 14 or 21 or 28 be ignored? Is it because the CDC thought it was not relevant information? And, if so, why in the world ask v-safe users to submit this information on these days? Or is it because the CDC did not like what the numbers showed? I will let you be the judge.
As noted above, and a sad irony, when medical care is sought during the first seven days, the CDC presumably attributes that to expected reactogenicity and tells the public to not be concerned. And if it occurs beyond seven days, it pretends as if that data does not exist – even though harms from COVID-19 vaccines, as the CDC well knows, can occur well after the first seven days, as discussed in depth in part 7 of this v-safe substack series.
Also, here, we are talking about a novel medical product, hence heightening the need for assessing its long-term safety – certainly beyond 7 days post-vaccination.
This shows how the sausage is made in mainstream media. But for the actual tenacity – I would even say courageous – pushback from a Reuters reporter, the story around ICAN’s v-safe claims could have ended very differently.
The real story I can only imagine this reporter would have liked to publish, the one I told above, however, would no doubt be a step too far for Reuters as an organization – at least for now, until brave journalists become the typical journalist.
This is the fourth part of a series in which Paula Jardine examines how the Covid vaccine programme was conceived by US defence planners nearly 20 years ago as a 21st century ‘Manhattan Project’ for biodefence. You can read Part 1 here, Part 2 here and Part 3 here.
Bill Frist was the 2003-2007 US Senate majority leader who championed the USA’s biodefence projects and promoted the concept of a ‘Manhattan Project’ against a pandemic, described in Parts 1, 2 and 3 of this series. He was also the politician who sponsored the Public Readiness and Emergency Preparedness Act (PREP) Act of December 2005 as soon as the World Health Organisation’s International Health Regulations had been amended to include a provision enabling WHO to declare Public Health Emergencies of International Concern (PHEIC). Critically it was this Act that established indemnity for the manufacturers of therapeutics, vaccines or diagnostics released during the course of a public health emergency against any and all harm caused.
Also working to influence US national biosecurity policy was Dr Robert Kadlec, described in Part 3. Working with him, and principally under the auspices of the Johns Hopkins Centre for Health Security (founded by Dr Tara O’Toole in 1998) were other participants in Operation Dark Winter, the code name for a senior-level situational simulation conducted on June 22-23, 2001, designed to wargame a covert and widespread smallpox bio-terrorist attack on the United States. These biosecurity hawks included O’Toole and Tom Inglesby of the Johns HopkinsCenter for Civilian Biodefense Strategies(CCBS).
‘O’Toole supported every flawed decision and counterproductive policy on biodefense, biosafety, and biosecurity during the Bush Administration. [She] is as out of touch with reality, and as paranoiac, as former Vice President Cheney . . . It would be hard to think of a person less well suited for the position . . . She was the single most extreme person, either in or out of government, advocating for a massive biodefense expansion and relaxation of provisions for safety and security’. Dr Ebright concluded: ‘She makes Dr Strangelove look sane.’
It was Kadlec who formed the Bipartisan Commission on Biodefense in 2014 and began the planning his Manhattan Project in earnest. Those involved with him in this commission included Tom Ridge, the first Homeland Security Secretary, Donna Shalala, a former Health and Human Services (HHS) Secretary, Dr Margaret Hamburg, a former Food and Drug Administration (FDA) commissioner, Scooter Libby, formerly of Project for a New American Century (PNAC), William Karesh, the vice president of EcoHealth Alliance and an adviser to the WHO on reforms to the International Health Regulations (IHR), and Kenneth Wainstein, now the Under Secretary of Homeland Security for Intelligence and Analysis.
The Commission’s National Blueprint for Biodefense published in2015 called for major ‘reform’. Consider it the blueprint for Kadlec’s Manhattan Project, for the CEPI (Coalition for Epidemic Preparedness Innovations) strategy and for the subsequent changes to the WHO IHR required to make the plan work.
The list of the BioDefense Commissions ‘we must’ demands follows:
· revolutionise the development of Medical Countermeasures (MCM, which are vaccines and therapeutics) for emerging infectious diseases;
· fully fund and incentivise the MCM enterprise;
· remove bureaucratic hurdles to MCM innovation;
· develop a system for environmental detection that leverages the ingenuity of industry and meets the growing threat;
· overhaul the Select Agent Program (which oversees the possession, use and transfer of risky biological agents and toxins) to enable a secure system that simultaneously encourages participation by the scientific community;
· help lead the international community toward the establishment of a fully functional and agile global public health response apparatus.
Three years later in May 2018 when Johns Hopkins ran Clade X, a table top simulation around a novel parainfluenza virus, O’Toole was involved once again. Johns Hopkins CHS also co-hosted with the Bill and Melinda Gates Foundation the better-known coronavirus simulation Event 201 in October 2019.
It was during a Clade X discussion on manufacturing capacity sufficient to end the fictitious pandemic through vaccination that O’Toole said: ‘Industry are more than willing to help but vaccines are very specific creatures that are difficult to turn to new purposes. We’re going to have to go to innovative manufacturing methods that will require a lot of leniency from the FDA and the understanding of the American people that we’re doing things on an emergency basis so every box in terms of safety and risk assessment may not be checked. But the vaccine is the only way forward.’ [My emphasis]
This was clear advocacy for vaccines as the exit strategy for the Clade X novel parainfluenza virus pandemic, and later once the Covid pandemic was underway, was to be the only exit offered to lockdown.
Today, O’Toole is an executive vice-president of the CIA spin-off venture capital firm In-Q-Tel in charge of a strategic initiative called BiologyNext. In April 2020 in a presentation to the Centre for Strategic and International Studies (CSIS) she said:
‘The bio-revolution is really founded on several core technologies that I’m going to simplify greatly. But it is all about being able to read, write, and edit the code of life. One of the most important recognitions of the past century in science, at least, is that life is written in code. And as Jason Kelly of Ginkgo Bioworks has put it: Biology is essentially programmable . . .
‘Ron Weiss, who is a synthetic biologist, predicted in 2014 that an RNA-based delivery method that allowed you to use RNA as a kind of platform to deliver new bits and pieces inside the cell would be a game-changing inflection point in synthetic biology. And the Covid-19 pandemic is giving us a chance to test that out. You may know that one of the vaccines that is coming on very quickly is made by Moderna. And it is a messenger RNA-based vaccine. So if that works, Ron Weiss’s prediction may come true.’ [My emphasis]
In August 2019 Kadlec’s department ran yet another table-top simulation, the Crimson Contagion. It simulated the impact of and response to the arrival in the US of an avian flu from China. It was a scoping exercise to identify legal authorities, US federal government funding resources and manufacturing capabilities for vaccines. It concluded that $10billion would be required to respond to a novel pandemic influenza strain.
A month later on September 19, 2019, President Trump signed the Executive Order on Modernizing Influenza Vaccines which launched the Manhattan Project by directing various US government departments and the US Department of Defense to propose a plan and a budget within 120 days – by January 17, 2020, to be precise.
On January 23, 2020, after the Moderna vaccine announcement in Davos, Fauci had a conference call with Dr Richard Hatchett, CEPI’s CEO, and the following day, a Saturday, he had a senior leadership update with Dr Kadlec in advance of a meeting with Stephane Bancel of Moderna on Monday January 27. Perhaps Kadlec, Hatchett and Bancel were amongst the unnamed people on Fauci’s January 15 conference call.
On January 30, 2020, when the WHO declared a SARS CoV2 Public Health Emergency of International Concern, just 7,818 patients were said to be sick with Covid, of whom only 82 were outside China. As far as Kadlec was concerned, this was now a shooting war.
Following CEPI’s announcement in Davos on January 23, US-based manufacturers Innovio Pharmaceuticals were miraculously ready to begin developing a Covid vaccine, and Moderna already had its funding to begin manufacturing the first batch of the vaccine co-owned and co-developed with Anthony Fauci’s National Institute of Allergy and Infectious Diseases (NIAID) for use in a human clinical trial.
The legislation that he and Frist had shepherded through Congress between 2003 and 2005 had concentrated power in the hands of the US Health and Human Services Secretary (and the US Administration for Strategic Preparedness and Response) during public health emergencies.
The basic goals of the architects had been achieved. These, the American investigative paralegal Katherine Watt has argued, were to set up legal conditions in which all governing power in the United States would be automatically transferred from the citizens and the three constitutional branches into the hands of one person, the Health and Human Services Secretary, ‘effective at the moment the HHS Secretary himself declared a public health emergency, legally transforming free citizens into enslaved subjects’.
The HHS Secretary Alex Azar, to whom ASPR’s Kadlec reported, was the senior legal counsel at HHS when the PREP Act was passed in 2005. Azar co-operatively declared a public health emergency on January 30, 2020, backdating it to January 27.
He then made a PREP Act declaration on February 4, enhancing liability protection for any person or firm involved in developing countermeasures, including Innovio and Moderna.
The announcement said: ‘The world is facing an unprecedented pandemic. To effectively respond, there must be a more consistent pathway for Covered Persons to manufacture, distribute, administer or use Covered Countermeasures across the nation and the world.’
Further research by Katherine Watt into another PREP Act declaration for medical countermeasures by Azar in March 2020 shows it effectively sidestepped the Nuremberg Code by stipulating that the ‘use’ of any counter measures ‘shall not be considered to constitute a clinical investigation’ while also removing the right to informed consent. As there is, by decree, no clinical trial, there are no stopping conditions for the use of said countermeasures.
It is startling how Dr Kadlec and his few associates have, over a period of more than 20 years, managed to orchestrate an undemocratic and unethical bio-security coup with global reach.
The Manhattan Project was renamed Operation WarpSpeed when it was launched in May 2020. The involvement of the US Federal Government which through the NIAID owns the patent for the spike protein used in the vaccines, and its Department of Defense that ran and financed Operation WarpSpeed, arguably elevates this War on Microbes Manhattan Project to an unprecedented bioweapon attack on humanity using an under-tested novel injectable pharmaceutical.
Paula Jardine is a writer/researcher who has just completed the graduate diploma in law at ULaw. She has a history degree from the University of Toronto and a journalism degree from the University of King’s College in Halifax, Nova Scotia.
Two publications by the Ministry of Health itself present evidence that within the government there is knowledge that the Pfizer mRNA Covid vaccine cannot be regarded as safe and effective. Therefore, from now on, there is no credible legal defence that the government can advance to cover its failure to openly inform individuals and the public at large of the inherent health risks of Covid vaccines.
Until now the government’s public announcements, including your own under the previous administration, relied on the argument that the government is ‘following the science’ and monitoring international Covid journal publishing. This was never credible, but allowed room for a fanciful defence (certainly a weak argument) of ‘accident, ignorance, misapprehension, or misdirection’ in any possible legal case brought under criminal or civil law. This can no longer be the case.
Firstly, a paper was published on February 3 2023 in the Lancet authored by our own Ministry of Health, Adverse Events Following the BNT162b2 mRNA COVID-19 Vaccine (Pfizer-BioNtech) in Aotearoa New Zealand. The paper reveals there is a statistically significant association between Pfizer mRNA vaccination and both myocarditis and acute kidney injury (AKI). The study examined the comprehensive medical records of four million NZers. There were 1,778 more cases of AKI than predicted from historical pre-pandemic rates, an alarming rate of one case for every 2,200 vaccinations. In addition to AKI and myocarditis, researchers also found elevated rates of blood clots and platelet damage.
Secondly, information concerning mortality in 2021, 2022, and 2023 correlated with vaccination status has been released by Health New Zealand following a Freedom of Information (OIA) request. The figures are signed off by Astrid Koornneef, Interim Director of Prevention, National Public Health Service.
The released figures include all NZ registered deaths by month. The figures show that for the last six months of 2022, 80 per cent of all people dying in New Zealand had received Pfizer mRNA booster shots. Yet, according to official government figures updated 14 February 2023, only 73.2 per cent of those eligible (18+ years) have received a booster. In other words, booster recipients are disproportionately represented among registered all-cause deaths. For more analysis refer here.
These two data sets certainly point towards serious risks associated with Pfizer mRNA Covid vaccination and stand in need of further investigation. The first investigated outcomes only within 21 days of Covid vaccination, the second indicates serious effects persist in the general population past 21 days. Taken together these point to a need for analysis of the causes of the current high rates of hospital admissions and deaths with reference to vaccination status.
There appears to be a misapprehension among NZ health professionals concerning the reliability of biotechnology vaccine manufacturing standards. Data points to huge variability in safety by vaccine batch. The following chart records serious vaccine injury and death by batch number in the USA sourced from publicly available VAERS data sets. You can see that the number of injuries varies hugely by batch. A few injury numbers are similar to those recorded following flu vaccination, but most batches lead to injury volumes considerably higher, up to 14 times higher.
As early as January 18 2021 Orange County California medical authorities flagged an unusually high pattern of injury and death associated with a single batch they had been administering. Pfizer should have immediately alerted New Zealand authorities to such anomalies. They probably had a contractual obligation to do so. Now that it has become a matter of public comment, it should not be possible to continue to assert Covid vaccine safety. NZ has a code of Good Manufacturing Process for pharmaceuticals. This includes a requirement for uniformity of pharmaceutical medicine contents and action. Apparently, Pfizer Covid vaccines do not meet our code.
The scientific evidence concerning the lack of Covid vaccine safety has not reduced the stitched-up action of government intelligence services, the police, and Te Punaha Matatini’s [a research centre] Disinformation Project in coordination with media and social media to monitor and reduce the reach of those raising pertinent questions. As you know, under the Prime Minister’s office there is interagency co-ordination for mis/disinformation monitoring and response. This involves multiple government departments. If these programmes and participants are not fully informed of the legitimacy of concerns about Covid vaccine safety, this amounts to misdirection and possibly harassment on the part of the Prime Minister’s office itself.
I and many others believe New Zealand has struggled to define its relationship with unregulated global influences in the modern era. There is much scope for commercial and geopolitical misdirection even via established channels of medical, military, and political cooperation. We need to be more alert as a nation to our own sovereign and economic interests especially when we consider health and the legal protections that have been afforded to multinational interests like Pfizer and others.
You are newly appointed to a position of power and influence. You have stated that you intend to reconsider the policies followed under your predecessor. It was therefore very surprising to find your Minister of Health doubling down on vaccine requirements against the weight of her own department’s findings. I urge you to look into this very thoroughly. As a lawyer, you must realise that going against the weight of safety evidence is very much a betrayal of the trust the public has placed in the government.
I hope you will announce a revision and retraction of Covid response policies in the light of the new evidence that is being published. Apparently New Zealand has acquired 1.7million doses of Pfizer bi-valent vaccines. Why? Have you considered returning them as not fit for purpose? The weight of evidence points in that direction, evidence that is accumulating by the week in learned journals.
It seems clear that we have passed a point where policy mistakes can be described as accidental. If continued, they will appear to be deliberate. The public stands in need of an honest explanation. It may take courage to speak out, but doing so will be a mark of integrity and genuine concern for health and safety.
One of the most tiresome features of the covid era has been the growth industry of ‘fact-checkers’ generously funded by Government, Pharma companies and the likes of Bill Gates to silence anybody challenging the ‘official narrative’. The Law, Health and Technology Newsletter has covered this extensively.
There have been a few ludicrous attempts to ‘fact-check’ my own work but, as an example of how biased and incompetent these people are, I present a request I received today from an AFP fact-checker asking me to help ‘debunk’ something …. and my self-explanatory response to it (I have spared the ‘fact-checker’ personal embarrassment by removing their name).
From: XXXXXX Sent: Thursday, March 2, 2023 9:17 PM To: Norman Fenton Subject: Media Request (AFP) – Addressing Misinterpretations of ONS Covid-19 Data
For reference, I will archive examples of these articles making the claims here and here.
Based on this ONS insight and a previous bulletin, which says the data is not intended to show vaccine efficacy, it seems like the article is misinterpreting the dataset. Would you be able to offer comment with a brief explanation as to how this sort of data is supposed to be read and used?
Thank you for your consideration,
XXXXXXXX
Agence France-Presse (AFP)
Office #: (202) 414-0527
From: Norman Fenton Sent: Thursday, March 2, 2023 9:44 PM To: XXXXXXX Subject: RE: Media Request (AFP) – Addressing Misinterpretations of ONS Covid-19 Data
Dear XXXXX
Like all mainstream “fact checkers” you clearly have no understanding of what it is you are checking.
The ONS dataset is so flawed and biased that even the Statistics Regulator agreed with us that it could not be used to make any inferences about vaccine efficacy or safety. But you are missing the big problem here.
Instead of focusing on those who are using the data to suggest the vaccine is not as safe and effective as claimed, what you should be focused on are the government and mainstream media who (against the advice of the Statistics Regulator) are using the ONS data to claim the vaccine is safe and effective. Have a look at this article in the Daily Mail – this is one you should be fact checking. Why aren’t you doing that?
Our most recent article covers this whole issue of the ONS data:
In fact, if you make adjustments for the multiple flaws and biases in the ONS data, then it is increasingly clear that the vaccinated have a higher all-cause mortality in many age groups, especially the under 50’s. In other words, the evidence increasingly points to the need for the covid vaccine programme to be shut down completely. But that isn’t the message you want to portray is it, because your funders are the ones pushing the vaccines?
Only one of the links to examples of reports you were seeking to ‘debunk’ seems to be working, namely the article in The Expose. The claim there is that the ONS report reveals that “the Vaccinated account for 9 in every 10 COVID Deaths over the past TWO Years”. Based on the ONS dataset this is correct. Of course, without knowing the true proportion of vaccinated in each age group, we still cannot conclude that the vaccinated are at higher risk of death from covid. But the article is not claiming that, it is simply stating the FACT that a far higher number of vaccinated people have died of covid than unvaccinated since Jan 2022. That the number of vaccinated people who have died of covid is 25,768 is relevant, because we were told by people like you that this could not possibly happen; the vaccines were supposed to have ‘stopped hospitalisation and death from covid’.
This essay got me thinking about all the institutions in the world that now seem to be completely captured; more specifically, all the institutions that are supposed to exist to “search for the truth” and now clearly exists to conceal truths and advance untruths.
At the top of this list are these five institutions:
Journalism organizations
I think tens of millions of Americans would agree with me that mainstream or corporate news organizations should not be trusted to provide fair and balanced coverage of the issues most important to the public.
As I have pointed out in other articles, it’s virtually impossible to find any serious articles that question any of the “authorized” Covid narratives. Not only does the establishment press push and endorse bogus or dubious storylines, they censor and attack people who are skeptical of official pronouncements.
Genuine journalists would be skeptical of the pronouncements of powerful figures and should always “search for the truth.” The fact this objective no longer applies in corporate newsrooms has tremendous and detrimental implications for society … today and in the future.
Scientists, science organizations and public health organizations
Those who practice real science are also supposed to make their living “searching for the truth.” By nature, a “scientist” should question, challenge and test accepted theories to see if they are, in fact, true.
Again, thanks to Covid, tens of millions of Americans are now beginning to question whether the majority of credentialed “scientists” are actually performing this vital task.
Many people now believe that scientists are unwilling to debunk false or dubious scientific theories. Instead, many (government-funded) scientists argue that the “science is settled” when it’s clearly not. Just like the corporate journalists, these scientists inflict further harm on society by attacking, censoring, bullying and cancelling their colleagues who do perform this vital role.
In short, they effectively prevent superior science from informing public policy.
For millions of citizens, the difference between false and correct science can be the difference between life and death. Millions of additional citizens are forced to needlessly endure life-altering pain and suffering as a result of “accepted” science that is wrong.
I would argue that journalism and science are the two most important professions and institutions in the world as the public needs to be able to discern what is true and what is not true if correct or wise policies are to be pursued.
Policies based on incorrect premises have the potential to cause harm to virtually every citizen on the planet. The fact “science” now seems to be corrupted – and is no longer interested in “searching for the truth” – constitutes one of the gravest and most ominous developments of our times.
Academia
As Eugyppius reinforces with his provocative essay, “academia” is another institution that is supposed to exist to “search for the truth.”
Euggypius focuses on the shortcomings of college academics. Again, I think all would agree that college is the place we send our children so they can increase their knowledge of important subjects. As all the great philosophers tell us, the quest for knowledge is found through a search for the truth.
However, what if large expanses of the “knowledge” these professors are imparting to students is dubious or wrong? What if, just like so many scientists and journalists, these academics are concealing real truths and intentionally or unintentionally spreading dangerous non-truths?
If this is the case, our college system is “educating” our future leaders by promulgating bogus or dubious “accepted truths.” Even worse, they are preventing the spread of ideas that could save lives and improve the quality of life of the world’s citizens.
Of course, it should be noted that the majority of “science” performed in today’s world comes from scientists who work for colleges.
Colleges are also supposed to teach and develop critical-thinking skills in students. However, it seems increasingly obvious that the vast majority of academics lack the ability to think critically. This, or many academics seem more interested in promoting their personal agendas instead of questioning what is true and what is false or uncertain.
In the past, colleges did seem to have many professors who valued a search for the truth. Today, the groupthink among college professors and administrators is approaching 100 percent.
All colleges celebrate “diversity,” but they recoil against diversity of thought and scholarship. In reality, they are afraid of genuine debate or, more specifically, any campus voices that push back against their dogma.
As these academics influence tens of millions of students who are supposed to become “future leaders,” the long-term detrimental effects of this “indoctrination” are impossible to calculate (but frightening to ponder).
Agencies or officials of government
Certain employees who work in government are also supposed to seek the truth and expose individuals and organizations that are perpetrating untruths (fraud).
Members of Congress have oversight over every government department or agency that is allocated taxpayer dollars. If government agencies and officials are concealing truths that could harm countless citizens, it’s Congress’s job to expose this.
Yet again, I’m sure tens of millions of Americans would agree with me that senators and representatives have abdicated this responsibility. They effectively allow fraudulent and Unconstitutional edicts and “emergency orders” to control the lives of every citizen in the country.
Prosecutors are also government employees. No one would deny that it is the job of prosecutors to “search for the truth” (find the real facts) and bring criminal charges against individuals who are harming others by promoting untruths and/or violating the law or Constitution.
The third branch of government, the Judiciary, must also be questioned as judges at all levels have the power to control what cases can (and cannot) be tried in a court of law.
Once a criminal or civil case is placed on the docket, the same judges have the power to influence how these cases are tried. By not approving important prosecutions or lawsuits or by hamstringing the efforts of advocates to fully present their arguments, judges can also “conceal the truth.”
Elected representatives and government prosecutors (and too many judges) seem to have increasingly made an intentional decision to not perform their oversight or regulation duties, which effectively conceals the truth from the public.
Trial lawyers and plaintiff law firms
Trial lawyers are another important professional class as attorneys can file lawsuits on behalf of clients who have been injured or harmed by the actions of defendants. Lawsuits are also filed by family members of those who may have died as a results of defendant actions.
Significantly, trial lawyers can demand testimony under oath and compel defendants to turn over important evidence or documents (discovery). They can cross-exam witnesses who may be lying, which allows a jury to determine whose testimony is or isn’t believable.
While this “search for the truth” can and has been abused with lawsuits that lack merit, the ability of any injured or harmed citizen to seek redress for wrongs is a vital component of our system of justice.
In the Covid era, it’s already clear that the plaintiff’s trial bar (with a few exceptions) is not going to represent clients who have suffered deaths, medical harm or financial damages (or citizens whose civil liberties have been violated by ignoring the language include in the first ten amendments to the U.S. Constitution).
If injuries have occurred, the legal proceedings that would document these “truth” are not taking place (again, with a few exceptions). By not filing lawsuits on the behalf of tens of millions of citizens who suffered some form of harm, the trial lawyers are, in effect, concealing the truth.
SUMMARY
Our society includes at least five key institutions or professions whose most important function is to seek the truth. All five of these institutions are supposed to expose untruths, especially those which have the potential to produce great harm among the citizenry.
As I see it, all five institutions are now “captured” and – at least as it involves Covid subjects – are more interested in concealing truths that challenge the authorized narratives.
However, a deeper treatment of the “how” question would highlight the important role played by the above-cited institutions and professions. It took many years for all of these institutions to become largely or completely “captured,” but the fact this happened also explains how so much harm was inflicted on legions of victims who have not received any form of justice.
I’ll conclude this essay with the same sentence I wrote in a July 2020 Covid article published by uncoverDC.com.
When a genuine search for the truth is increasingly viewed as taboo or off-limits, the prognosis for a nation we all want to see survive and prosper is probably bleak.
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.



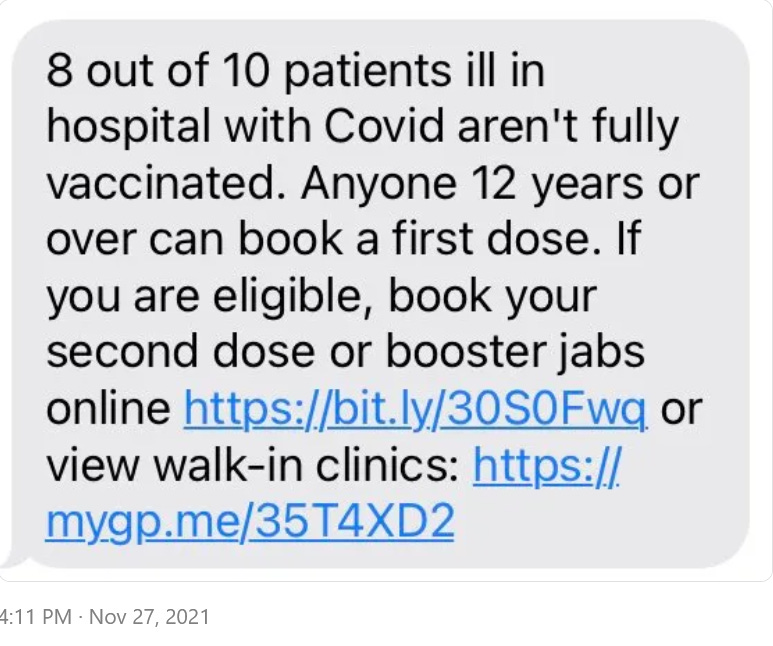




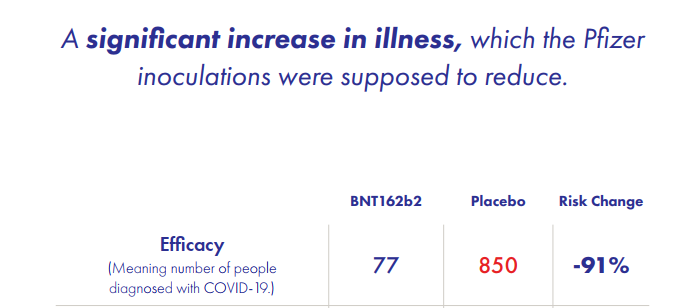




{kind=link}
{kind=link}