Pfizer: sales before child safety
The inside story of how we held Pfizer to account for misleading parents about Covid vaccine safety

UsForThem · Broken Custodians · February 2, 2023
Free pass promotional opportunity given by BBC to Pfizer
On 2 December 2021, the BBC published on its website, its popular news app and in the BBC News at One programme, a video interview and an accompanying article under the headline ‘Pfizer boss: Annual Covid jabs for years to come’.
The interview by the BBC’s medical editor, Fergus Walsh, conducted as a friendly fireside chat, gave Dr Albert Bourla, the Chairman and CEO of Pfizer, a free pass promotional opportunity that money cannot buy — as the UK’s national public service broadcaster, the BBC is usually prohibited from carrying commercial advertising or product placement.
Perhaps unsurprisingly, Pfizer made the most of that astonishing opportunity to promote the uptake of its vaccine product. As the BBC’s strapline suggests, the key message relayed by Dr Bourla, responding to an obediently leading question from Mr Walsh, was that many more vaccine shots would need to be bought and jabbed to maintain high levels of protection in the UK. He was speaking shortly before the UK Government bought another 54 million doses of Pfizer vaccines.
Misleading statements about safety
Among his explicit and implicit encouragements for the UK to order more of his company’s shots, Dr Bourla commented emphatically about the merits of vaccinating children under 12 years of age, saying “[So] there is no doubt in my mind that the benefits, completely are in favour of doing it [vaccinating 5 to 11 year olds in the UK and Europe]”. No mention of risks or potential adverse events, nor indeed the weighing of any factors other than apparent benefits: Dr Bourla was straightforwardly convinced that we should immunise millions more children in the UK. In fact, it later emerged that the BBC’s article had misquoted Dr Bourla who in the full video interview recording had ventured the benefits to be “completely completely” in favour of vaccinating young children.
Despite the strength of Dr Bourla’s unconditional and superlative pitch for vaccinating under-12s, the UK regulatory authorities would not authorise the vaccine for use with those children until the very end of 2021; and indeed this came just a few months after the JCVI — the body which advises the Government on whether and when to deploy vaccines in the UK — had already declined to advise the Government to roll out a mass vaccination programme for healthy 12 to 15-year-olds on the basis that “the margin of benefit, based primarily on a health perspective, is considered too small to support advice on a universal programme of vaccination of otherwise healthy 12 to 15-year old children…”.
In response, soon after the interview aired, UsForThem submitted a complaint to the UK’s Prescription Medicines Code of Practice Authority (PMCPA) — the regulator responsible for policing promotions of prescription medicines in the UK. The complaint cited the overtly promotional nature of the BBC’s reports and challenged the compliance of Dr Bourla’s comments about children with the apparently strict rules governing the promotion of medicines in the UK.
A year-long, painful process
More than a year later, following a lengthy assessment process and an equally lengthy appeal by Pfizer of the PMCPA’s initial damning findings, the complaint and all of the PMCPA’s findings have been made public in a case report published on the regulator’s website.** Though some aspects of that complaint ultimately were not upheld on appeal, importantly an industry-appointed appeal board affirmed the PMCPA’s original findings that Dr Bourla’s comments on vaccinating 5 to 11-year-olds were promotional, and were both misleading and incapable of substantiation in relation to the safety of vaccinating that age group.
Even after UsForThem involved a number of prominent Parliamentarians, including Sir Graham Brady MP, to help accelerate the complaint, the process was dragged on — or perhaps ‘out’ — while the roll-out of Pfizer’s vaccine to UK under-12s proceeded, and the BBC’s interview and article stayed online. Even now the interview remains available on the BBC’s website, despite the PMCPA in effect having characterised it as ‘misinformation’ as far as vaccinating children is concerned.
When news of the appeal outcome was first revealed in November 2022 by a reporter at The Daily Telegraph newspaper, Pfizer issued a comment to the effect that it takes compliance seriously and was pleased that the “most serious” of the PMCPA’s initial findings — that Pfizer had failed to maintain high standards and had brought discredit upon and lowered confidence in the pharmaceutical industry — had been overturned on appeal.
It must be an insular and self-regarding world that Pfizer inhabits, that discrediting the pharmaceutical industry is considered a more serious matter than making misleading and unsubstantiated statements about the safety of their products for use with children. This surely speaks volumes about the mindset and priorities of the senior executives at companies such as Pfizer.
And if misleading parents about the safety of a vaccine product for use with children does not discredit or reduce confidence in the pharmaceutical industry, it is hard to imagine what standard can have been applied by the appeal board which overturned that initial finding. Perhaps this reflects the industry’s assessment of its own current reputation: that misinformation promulgated by one of its most senior executives is not discrediting. According to the case report, the appeal board had regard to the “unique circumstances” of the pandemic: so perhaps the view was that Pfizer can’t always be expected to observe the rules when it gets busy.
Multiple breaches. No meaningful penalty
Indeed, a brief look at the PMCPA’s complaints log confirms that Pfizer has been found to have broken the UK medicines advertising rules in relation to its Covid vaccine a further four times since 2020. Astonishingly, though, for their breaches in this most recent case, and in each of the other cases decided against it, neither Pfizer nor Dr Bourla will suffer any meaningful penalty (the PMCPA will have levied a small administrative charge to cover the cost of administering each complaint). So in practice, neither has any incentive to regret the breach, or to avoid repeating it if it remains commercially expedient to do so.
And this is perhaps the crux of the issue: the PMCPA, the key UK regulator in this area, operates as a division of the Association of the British Pharmaceutical Industry, the UK industry’s trade body. It is therefore a regulator funded by, and which exists only by the will of, the companies whose behaviour it is charged with overseeing. Despite Pharma being one of the most lucrative and well-funded sectors of the business world, the largely self-regulatory system on which the industry has now for decades had the privilege to rely has been under-resourced and has become slow, meek and powerless.
The UK Medicines and Healthcare Products Regulatory Agency (MHRA) in principle has jurisdiction to hold the BBC accountable for what seems likely to have been mirroring breaches of the medicines advertising rules when it broadcast and promoted Dr Bourla’s comments, but no action has yet been taken.
This case, and the apparent impunity that companies such as Pfizer appear to enjoy, evidence that the system of oversight for UK Pharma is hopelessly outdated and that the regulatory authorities are risibly ill-equipped to keep powerful, hugely well-resourced corporate groups in check. The UK regulatory system for Big Pharma is not fit for purpose, so it is time for a rethink. Children deserve better, and we should all demand it.
** Endnote: an undisclosed briefing document
As part of its defence of UsForThem’s complaint, Pfizer relied on the content of an internal briefing document that had been prepared for the CEO by Pfizer’s UK compliance team before the BBC interview took place. Pfizer initially asked for that document to be withheld from UsForThem on the grounds that it was confidential. When UsForThem later demanded sight of the document (on the basis that it was not possible to respond fully to Pfizer’s appeal without it), UsForThem was offered a partially redacted version, and only then under terms of a perpetual and blanket confidentiality undertaking.
Without knowing the content of that document, or the scope of the redactions, UsForThem was unwilling to give an unconditional perpetual blanket confidentiality undertaking, but reluctantly agreed that it would accept the redacted document and keep it confidential subject to one limited exception: if UsForThem reasonably believed the redacted document revealed evidence of serious negligence or wrongdoing by Pfizer or any other person, including evidence of reckless or wilful damage to the public health of children, UsForThem would be permitted to share the document, on a confidential basis, with members of the UK Parliament.
This limited exception to confidentiality was not accepted. Consequently, UsForThem never saw the briefing document and instead drew the inference that it contained content that Pfizer regarded as compromising and which it therefore did not wish to risk ever becoming public.
The Alarming Trend in Core Mortality Since the Vaccine Rollout
BY NICK BOWLER | THE DAILY SCEPTIC | FEBRUARY 3, 2023
In a previous article I introduced the concept of looking at mortality from non-respiratory causes (i.e., not deaths from flu, Covid or other similar pathogens) as a better indicator of core mortality changes in the U.K. population than either excess deaths alone (or even excess non-Covid deaths). This is because most of the variation in the number of deaths between winter and summer and from year to year are due to respiratory causes; thus, take those out and you get a clearer picture of the underlying health of the population and whether people are generally getting sick and dying more or less than in recent years from causes such as cardiovascular problems, cancer, Alzheimer’s and so on.
I decided to go back and re-analyse the data in order to see how excess non-respiratory mortality has accumulated over the last few years. I discovered that this showed a total for 2021, 2022 and 2023 (thus far) of 49,696 deaths. When one takes into account the mortality displacement for this time period (owing to the pandemic bringing expected deaths forward; explained here), which I estimate as 23,650 deaths, the non-respiratory excess mortality reaches 73,346 deaths.
Comparing this to the number of deaths due to Covid (as underlying cause) over the same time period, which total 89,629 deaths, we see that the Covid figure is just 16,283 or 22% higher. Bearing in mind that it is widely acknowledged that there has been overcounting of Covid deaths (and thus conversely undercounting of non-respiratory deaths), the two tallies are now broadly similar, and thus an emergency situation at least as dangerous as the pandemic itself has arisen, which must surely now be addressed by the authorities.
To highlight the overcounting of Covid deaths, one only need compare the data for ‘deaths due to’ against ‘deaths with’ for COVID-19, and contrast it with the figures for other respiratory diseases. For Covid around 82% of deaths ‘with Covid’ are claimed to be ‘due to’ Covid over the course of the pandemic, yet with all other respiratory diseases only 34% of deaths ‘with’ the disease are claimed to be ‘due to’ it. The reason for the considerable discrepancy is unclear and suggests Covid is being significantly over-attributed as underlying cause.
For this article I calculated the number of excess non-respiratory deaths (relative to 2015-2019 pre-Covid averages) for each week of the year, and then calculated the cumulative values over the course of a full year. These charts confirm the suitability of the concept of non-respiratory mortality to serve as a stable core mortality rate that does not normally vary significantly from year to year. This is because there is a clear tendency (pre-Covid) for the cumulative non-respiratory mortality values to tend back to zero (i.e., the x-axis) if there has been a period of abnormal positive or negative values for an extended time. This indicates the role of mortality displacement in causing overall deaths to even out over time.

In fact, even in 2020 the shape of the curve (orange) looks very similar to the pre-Covid curves, excepting for the sudden spike at the beginning of the first wave of the pandemic when chaotic counting was arguably occurring. Without this the curve would hug the x-axis pretty much all through the year.
When we look at the curves for 2021, 2022 and 2023, however, the pattern changes radically. From week 18 in the spring of 2021 onwards the curve begins to point only upwards, and it further accelerates from the spring of 2022 and once again in the early part of 2023.

Please note all these curves are generated from the raw data from the ONS weekly reports for England and Wales. They are not adjusted for mortality displacement or anything else.
Putting all these curves together on one chart illustrates the changing pattern over the course of the pandemic, and in particular the striking upward turn in the spring of 2021.

Note that there appears to be little evidence of any need for an age-standardised adjustment to prevent an upward drift in death rates owing to an ageing population. Even after six years from the beginning of 2015 through to the end of 2020, the cumulative non-respiratory mortality is still around the zero mark, and even dips a little below in the first three months of 2021 (remember this is mortality with the respiratory deaths including Covid taken out).
Recent articles from Dr. Noah Carl have questioned whether mortality was unusually high in 2022 because, when the figures are adjusted for an ageing population using the age-standardised mortality rate (ASMR), excess deaths come out low. The ASMR is a hypothetical construct that is used to adjust crude mortality data for changes in the age structure of a population. It relies on a standardised population model that provides the weightings in the population of different age groups. This is a very useful model that can make sense of changing mortality rates over time when studying the demography of a population.
However, I would argue that it is not a useful model during times of exceptional change, as it relies on assumptions of weightings that change only incrementally over time and doesn’t take into account when a large number of deaths occur unexpectedly in older age groups. During the Covid pandemic there have been nearly 200,000 excess deaths (relative to the 2015-2019 average), and these are largely concentrated in the oldest age groups, i.e., the groups that provide the bulk of ‘normal’ mortality.
In particular, the over-80 age group comprises just 4.6% of the U.K. population yet delivers almost 60% of deaths in a normal year. As the U.K. population is roughly 67 million people, this puts the over-80s at about three million persons. The occurrence of 200,000 excess deaths in this age group implies a drop in the ‘weighting’ of this age group in the age make-up of the population of some 6.5%.
As the mortality in the U.K. in recent times has averaged about 600,000 deaths per year, a 6.5% adjustment in 60% of them would represent about 24,000 fewer deaths to be expected in 2022 than standardised models would predict, counteracting the ASMR expectation that the number of deaths should rise owing to an ageing population. 2022 has, however, seen something of a record year in overall mortality figures.
This is why, instead of looking at a misleading age-standardised mortality rate, we get a much better picture of what’s going on if we look at non-respiratory mortality as a measure of ‘core’ mortality, taking out the highly variable respiratory deaths. It’s worth noting here that it’s possible that the reason ‘core’ non-respiratory mortality has remained stable over recent years rather than rising as the age-standardised model would predict is because stronger winter flu seasons such as 2017-18 have naturally counteracted the effect of ageing on ‘core’ mortality.
The actuarial profession certainly seems to agree that there is a negative trend in underlying life expectancy based on what has been happening in 2022.
The upshot of this analysis of non-respiratory mortality is that something extraordinary has been occurring in the trends in core mortality since spring 2021, notably around the time of the Covid vaccination rollout. This worrying trend is currently accelerating and requires an urgent inquiry into whether the vaccinations themselves are playing a part or, if not, what is going on.
California to Ditch Plans to Mandate COVID Vaccines for Schoolchildren
By Brenda Baletti, Ph.D. | The Defender | February 2, 2023
California will end plans to mandate COVID-19 vaccines for schoolchildren when the state ends its COVID-19 state of emergency on Feb. 28, California Department of Public Health officials told EdSource, which reported the news on Wednesday.
Commenting on the news, Michael Kane, national grassroots organizer for Children’s Health Defense (CHD) and founder of NY Teachers For Choice, told The Defender :
“We [in the movement] have some really good momentum right now, and what just happened in California is indicative of that.
“People are done with this. They’re done with the most extreme portions of this COVID agenda, the idea of this shot in kids is a no-starter for anybody.”
Gov. Gavin Newsom announced in October 2021, that California would be the first state to require COVID-19 vaccinations for children to attend school. It was also the first to mandate masking and staff vaccination measures.
At the time, state Sen. Richard Pan proposed legislation to strengthen the vaccine requirement even further by eliminating personal and religious exemptions. The legislation didn’t pass.
The vaccine requirement for children was originally set to kick in on July 1, 2022, when it was expected the vaccines, still under Emergency Use Authorization at the time, would be fully approved by the U.S. Food and Drug Administration (FDA).
But in April 2022, California announced it would delay the mandate to July 1, 2023.
The FDA still has not fully approved the COVID-19 vaccines for anyone under age 12. The CDC recommends the vaccines and the bivalent boosters for children ages 6 months and older.
The bivalent boosters were authorized for emergency use without any human clinical trials.
In California, 67% of 12- to 17-year-olds and 38% of children ages 5 to 11 have received two doses of the COVID-19 vaccine primary series. Less than 42% of 12- to 17-year-olds and less than 30% of 5- to 11-year-olds have been boosted.
Those numbers are higher than national averages. Only 58% of children ages 12 to 17 and 32% of children ages 5 to 11 have received two doses of the vaccine.
“The booster uptake is a complete failure, so this idea of routinizing a COVID shot for school every year, which is what they wanted, is failing in all the states they thought it was a guarantee in,” Kane said.
California ended the school mask mandate in March 2022, and ended the vaccine mandate for teachers and school staff in October 2022.
‘This kind of coercion never should have been normalized’
In the last two years, while state lawmakers debated California’s school vaccine mandate, school districts across the state proposed and passed their own COVID-19 vaccine mandates.
Alex Gutentag, former Oakland public school teacher and political analyst, told The Defender :
“Newsom has referred to California as ‘the true freedom state,’ but he more than any other U.S. governor has tried to undermine the medical freedom of kids and their families when it comes to COVID-19.
“It is definitely a positive development that California is ending its plan for a school mandate, but it’s important to remember that many kids have already been coerced into vaccination through the threat of both statewide and local mandates.
“Several California cities, including Los Angeles, told families that COVID vaccines would be required to attend school in person, but eventually had to scrap and delay these plans. It was a clear effort to increase vaccine uptake, and was a major abuse of power. This kind of coercion never should have been normalized.”
The pressure to scrap mandate plans came in part from attorneys and citizen advocacy groups who brought three major lawsuits against the Los Angeles Unified School District (LAUSD), the Piedmont Unified School District and the San Diego Unified School District (SDUSD).
Children’s Health Defense-California Chapter (CHD-CA) and Protection of the Educational Rights of Kids (PERK), a California-based child advocacy group, used state laws to rule out local policies and pause vaccine mandates in the LAUSD and the Piedmont school district.
They sued the LAUSD, the second-largest school district in the U.S., alleging the district lacked the legal authority to impose a COVID-19 vaccine requirement for students ages 12 and older.
The mandate would have excluded 32,000 students from in-person classes.
After Judge Mitchell L. Beckloff ruled the case could go forward in April 2022, the LAUSD announced it would delay the COVID-19 vaccine requirement until July 1, when the state mandate kicked in.
Piedmont also voted to repeal its mandate after a judge granted CHD-CA and PERK’s Application for an Alternative Writ of Mandate and ordered the district to show why its policy could not be struck down.
In San Diego, a group called Let Them Choose filed a lawsuit contesting the SDUSD’s vaccine mandate for school children ages 16 and up. The court ruled, and in December 2022, an appellate court affirmed, that the district’s mandate violated state guidelines.
According to Rita Barnett-Rose, legal director of CHD-CA, the San Diego ruling established that individual school districts cannot institute COVID-19 vaccine mandates at the district level, because there is a statewide statutory scheme in place to set mandates.
That means the end of the California COVID-19 vaccine mandate for children at the state level will effectively end all school mandates in California.
Political will for mandates faltering across the country
Rita Barnett-Rose underscored that California health officials have not yet made the news about ending the mandate for the state’s schools official. However, she said, “Right now it looks like positive news.”
However, Barnett-Rose said, “The question still remains, are they [state legislature] going to try to put something on the legislative agenda this year?”
Gutentag also noted the lack of an official announcement:
“I also think it’s notable that officials only said they were not going to implement the mandate after EdSource pressed them for answers. State leaders probably knew that there were too many legal and logistical challenges, but did not want to admit this in order to save face.
“All Californians should be concerned that our state government is not honest and direct with us about major policy decisions.”
This shift in California’s school mandate decision is the latest in a string of developments calling into question the COVID-19 vaccines and marking a shift in public consensus on vaccines.
“I’m not surprised at all that California is admitting that it’s not politically possible to force a shot that’s unnecessary and dangerous on children to attend school,” Kane said, adding:
“It makes perfect sense to me, given what I am seeing in New York that this same type of pressure is in California.
“The entire thing is political. The whole thing is what can we politically do? They can’t politically force the shot on kids. The fallout is too much. They just can’t risk it, you know.”
Barnett-Rose told The Defender she thinks that when Newsom announced the mandate he thought a lot of other states would follow suit.
“I’m hoping this signifies that the political will to force these mandates on kids is really declining significantly.”
CDC adds COVID shots to child immunization schedule
California reversed its vaccine mandate decision despite the fact that in October 2022, the Centers for Disease Control and Prevention recommended adding COVID-19 vaccines for children as young as 6 months old to the new Child and Adolescent Immunization Schedule, which will be rolled out this month.
The revised recommendations include the Moderna or Pfizer-BioNTech COVID-19 vaccine for children as young as 6 months and the Novavax COVID-19 vaccine for children as young as 12 years.
All COVID-19 vaccines being administered in the U.S. to people under 18 are still Emergency Use Authorized (EUA) products.
The FDA did grant full approval to Pfizer’s Comirnaty COVID-19 vaccine for ages 12 and older. However, the Comirnaty vaccine is not available in the U.S. — which means all children who get the Pfizer vaccine are getting an EUA product.
The FDA also informed a congressional committee in May 2022 that the COVID-19 vaccines for children under 6 would not have to meet the agency’s 50% efficacy threshold required to obtain EUA.
COVID-19 vaccines for adolescents, teens and adults had to meet the requirement.
“If these vaccines seem to be mirroring efficacy in adults and just seem to be less effective against Omicron like they are for adults, we will probably still authorize,” Peter Marks, M.D., Ph.D., director of the Center for Biologics Evaluation and Research at the FDA, told the House Select Subcommittee on the Coronavirus Crisis.
Last week, The Epoch Times reported that recently released emails revealed top officials, including Marks, rushed approval of Pfizer’s COVID-19 vaccine to enable vaccine mandates, despite concern by others in the agency that the rush compromised the integrity of the approval process.
On Dec. 9, 2022, the CDC expanded the use of updated (bivalent) COVID-19 vaccines for children ages 6 months through 5 years. They made that decision despite the fact that the bivalent shots were approved for adults without any clinical data and have yet to show efficacy.
In an amicus brief for a lawsuit challenging the vaccine mandate for school children in the state of Louisiana, CHD wrote:
“Simply put, the COVID vaccines have not been shown to be either effective or safe for children. The benefits to children are minuscule, while the risks — including the risk of potentially fatal heart damage — are ‘known’ and ‘serious,’ as the [FDA] itself has acknowledged.”
The Louisiana Department of Health rescinded the mandate.
Legal struggles continue over age of consent for vaccines
Legal battles over vaccines for children in California and elsewhere are ongoing.
In California, Maribel Duarte is suing the LAUSD and Barack Obama Global Preparation Academy alleging they vaccinated her 13-year-old son without her consent.
A vaccine clinic was set up in his school — Barack Obama Global Prep Academy — and he was allegedly bribed with a pizza to get vaccinated without parental consent.
One of the adults at the clinic requested the teen provide a parent-signed consent form, which he did not have. The child was then told to sign his mother’s name and not tell anyone.
Currently, Sen. Cheryl Kagen of Maryland is proposing Senate Bill 378, which would allow children 14 and up to consent to vaccination themselves and prevent parents from accessing medical records.
California attempted to pass a similar bill, SB 866, for children ages 12 and up.
The District of Columbia also attempted to pass a similar law, for children 11 and older, but a preliminary injunction issued in March 2022 temporarily blocked the district from implementing the law.
CHD and the Parental Rights Foundation sued the district and are seeking to declare the D.C. act unconstitutional.
The D.C. school district still plans to mandate children be vaccinated against COVID-19 to attend school starting in the 2023-2024 school year, just not without their parents’ consent.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
NYT: Covid Vaccine Makers and Bill Gates’ GAVI Screwed Everyone
US Government and Other Governments are Holding The Bag
By Igor Chudov | February 1, 2023
This New York Times story from today is very illustrative of the current times.
Vaccine Makers Kept $1.4 Billion in Prepayments for Canceled Covid Shots for the World’s Poor
Separately, Johnson & Johnson is demanding additional payment for unwanted shots, confidential documents show.
It turns out that makers of Covid vaccines expertly screwed their customers, keeping a large part of the prepayment money advanced to them without shipping vaccine doses that no longer find any demand.
As global demand for Covid-19 vaccines dries up, the program responsible for vaccinating the world’s poor has been urgently negotiating to try to get out of its deals with pharmaceutical companies for shots it no longer needs.
Drug companies have so far declined to refund $1.4 billion in advance payments for now-canceled doses, according to confidential documents obtained by The New York Times.
The worst example is J&J, manufacturer of the Janssen vaccine, which was pulled from use worldwide due to blood clots. Despite that, J&J demands that more money be given to it “because of existing contracts.”
If it cannot strike a more favorable agreement with another company, Johnson & Johnson, it could have to pay still more.
Gavi and Johnson & Johnson are locked in a bitter dispute over payment for shots that Gavi told the company months ago it would not need, but which the company produced anyway. Johnson & Johnson is now demanding that Gavi pay an additional, undisclosed amount for them.
New York Times is lamenting this situation and highlights appeals to the conscience of vaccine makers:
Covid vaccine manufacturers “have a special responsibility” because their products are a societal good and most were developed with public funding, said Thomas Frieden, the chief executive of the global health nonprofit Resolve to Save Lives and a former director of the United States Centers for Disease Control and Prevention.
Who is Thomas Frieden? He is a former director of the CDC and also a convicted sex offender, in my opinion.
Vaccine makers resist Frieden’s appeals to their conscience because they do not have any.
Bill Gates’ GAVI is not asking Pfizer for refunds: Pfizer was paid directly by the US government. Did Bill Gates pull strings to have the US government hold the financial bag in the case of Pfizer?
If so, Bill certainly had personal financial reasons for this!
Bill and Melinda Gates Foundation invested 55 million into Pfizer’s vaccine maker BioNTech in Sep 2019.
This investment was made when BioNTech was an obscure company with no vaccines in the pipeline. That “unexpectedly” changed mere months later when BioNTech was selected to become the largest producer of Covid vaccines. Such lucky timing for Bill!
So, Bill Gates, having a financial interest in BioNTech, did not want his own GAVI to pay for BioNTech vaccines that eventually found no buyer; instead, the US government paid Pfizer directly. Pfizer will keep the funds, giving the US government an “option” to buy vaccines that nobody wants anymore.
Under the revised deal, a total of 600 million Pfizer doses will be made available to the US by the end of the year, giving the administration more time to find countries who want them. Pfizer had originally agreed to sell a billion shots at cost by this month.
Bill Gates-funded GAVI seems to have screwed its donors innovatively: the donors gave money towards Covid vaccinations, which fizzled. Hence, GAVI received back 1.6 billion out of 2.3 donated billions it gave Covid vaccine makers. Gavi, however, will not refund 1.6 billion to the donors and will use the money it recovered for other purposes, inflating its budget:
Had some vaccine manufacturers not been willing to renegotiate their contracts with Gavi, the costs to the organization could have been much higher. Gavi would have been on the hook for $2.3 billion for the doses it wanted to cancel, the documents show, but it saved $1.6 billion by exiting those contracts.
…
Donations for Covid shots substantially inflated Gavi’s budget, and the lost prepayments for canceled Covid vaccines do not threaten its regular childhood-vaccination work.
Such is the current state of the pandemic. The money is gone; vaccines do not work; people are dying suddenly; the government and Big Pharma do not want the public to pay attention.
If you, my reader, are in the United States, remember that the US government’s money is your money. Say bye-bye to it.
Will there be any real investigations?
MHRA Caught Not Doing Its Promised Vaccine Safety Monitoring (Again)
BY NICK DENIM | THE DAILY SCEPTIC | JANUARY 28, 2023
We all know, I hope, about the significant and sustained number of excess deaths since May 2022. Most recently, you probably saw Esther McVey MP asking if the Department of Health would commit to an urgent and thorough investigation.
Maria Caulfield MP, one of the health ministers, replied saying that it’s also happening elsewhere and there is a range of factors. Implicitly, she was refusing to investigate. Outrageous.
However, it actually reminded me that way back in February 2021, MHRA promised to do a whole range of routine population-level data analysis “to quickly detect a potential safety signal” for the Covid vaccines. It announced it here under the section “Rapid Cycle Analysis and Ecological Analysis“. It explains what it involves as follows:
[A]s COVID-19 vaccination records (i.e., those given outside of GP surgeries) begin to get updated within GP systems, the MHRA will implement a form of active surveillance known as ‘Rapid Cycle Analysis’. This method involves proactive, weekly analysis of a range of pre-defined events (theoretical side effects) to quickly identify safety signals – it again involves ‘observed vs expected’ analyses (i.e. comparing rates after vaccination to rates in unvaccinated comparator groups) but doesn’t rely on people directly reporting any concerns through the Yellow Card scheme. It is also a more robust way to quickly determine if rates are likely to be consistent with a coincidental association. It also uses the MaxSPRT approach with adjustments made for the expected delays in the recording of events presenting to and diagnosed in secondary care settings. The list of pre-defined events of special interest is not fixed and can be expanded at any time.The MHRA will also use the CPRD data to conduct ‘ecological analyses’. This involves monitoring trends in the rates of pre-defined events within given population cohorts, based on prioritisation groups for vaccine roll out, to see if they are occurring to a greater extent amongst those targeted for vaccination after it is deployed compared to historical rates from the pre-deployment period. Comparisons can also be made to trends seen in groups not targeted for vaccination at the same time. This approach is most useful when we see high vaccine uptake and is another way to quickly detect a potential safety signal.
So I had a poke around MHRA’s website to see how it is getting on with this. Not very well, it turns out.
One of MHRA’s five divisions is called Clinical Practice and Research Datalink (CPRD) and it maintains a bibliography of peer-reviewed research and reports which have used data provided by MHRA from NHS datasets for things like ICU, A&E, inpatients, outpatients, cancer registration and pregnancy. When I looked, the bibliography had been updated as recently as January 9th 2023. So well and truly up-to-date. So far, so good.
Imagine my surprise when I could only find two population-level studies relating to the Covid vaccines, both relating to thrombocytopenia (low blood platelet count), one from February 2022 and one from October. So just one type of adverse event has been put through MHRA’s promised ecological analysis in the last two years. It doesn’t say much for MHRA’s commitment to use population-level data “to quickly detect a potential safety signal”.
Imagine my further surprise that none of the datasets which MHRA’s CPRD Division provides for research contains data after June 2021.
So in conclusion, all about as useless as the other strand of Covid vaccine surveillance it promised, Targeted Active Monitoring, which I noted in a recent article it quietly dropped 15 months ago.
For me, there are only two possible conclusions: either the MHRA is not doing the Covid vaccine surveillance it promised, or it is doing it and not making the results publicly available. Either way, it’s high time that MPs, the Covid Inquiry and the media started asking MHRA some searching questions.
Until Nick retired a few years ago, he was a Senior Civil Servant in a Government Department.
Researchers bamboozling journalists with mythical comparison of vaccinated and unvaccinated
Where are the numbers? by Norman Fenton and Martin Neil | January 31, 2023
From: XXXXXX
Sent: 30 January 2023 12:33
To: Norman Fenton
Subject: Hart GroupDear Professor Fenton,
Apologies for any intrusion, but I’m contacting you directly since the Hart Group (which I understand you to be a member of), have not replied to my earlier emails – all very busy people, I do understand.
As a small group of individuals who between us have some journalistic and medical-science history, we are working on a presentation (with a further view to establishing a website), which aims to offer a wider range of information concerning Covid policies and treatment than, it appears, is usually available through current mainstream and social media.
Given that our aim is a balanced juxtaposition and presentation of arguments, hopefully allowing better-informed opinions to be arrived at, we do have a range of “issues” we’d love to understand better in order to present them fairly.
You are (I imagine) well-placed to comment on one specific matter, and I would be enormously grateful if you would spare a minute to advise, assuming this enquiry doesn’t create any conflict of interest or other problems for you:
The Times and other media recently reported on a QMUL study* which indicates that unvaccinated individuals with certain medical conditions are more likely to suffer “serious outcomes” than vaccinated individuals. I believe presenting this this demands careful attention to context and contrasting with other possible perspectives.
Dr Aseem Malhotra in a Twitter-hosted video makes reference to de-bunking claims about how this story has been reported, but makes no reference I can find to where such a de-bunking can be found; and sadly, he too seems unavailable to comment!
Probably, Dr Malhotra’s position is not an issue you are required in any way to comment on. However, in general, I do think that those who would like to see “better”, more balanced reporting on Covid should find time to speak to others, like us, who are trying to support exactly that cause – presumably it’s in everyone’s interest. But that’s just a peripheral observation on my part!
It would be truly helpful if you can find a moment to provide some pointers to help us present a balanced picture of the study referred to above.
Many thanks, and best wishes.
Your’s faithfully,
XXXXX
* Also reported on the QMUL website: https://www.qmul.ac.uk/media/news/2022/smd/unvaccinated-individuals-with-heart-problems-up-to-9-times-more-likely-to-die-or-suffer-serious-complications-from-covid-19.html
The study referred to is this one.
Here is my self-explanatory response:
Dear XXXXX
I should make it clear that, although I just briefly discussed this with one or two members of HART, my response below should certainty not be construed as ‘the HART response’.
The most important point to note about the QMUL study is that it certainly does not claim anything like what either you or The Times seem to think it claims, i.e it certainly does not show that “unvaccinated individuals with certain medical conditions are more likely to suffer serious outcomes than vaccinated individuals.” In fact, no comparison with a vaccinated cohort was undertaken.
All the study actually did was look at the outcomes for covid patients with pre-existing conditions like myocarditis. This is something very different to the later studies (such as those Aseem Malhotra referred to) which compared incidence of myocarditis occurring post-vaccination with the base rates for unvaccinated. So, all the study actually shows is that “that individuals with certain pre-existing medical conditions who get covid are more likely to suffer serious outcomes than those without such medical conditions who get covid.” That is hardly novel, since this has been widely known since March 2020.
In fact, the authors of the study are demonstrating a very clear bias by referring to the people in the study as ‘unvaccinated’. Of course, they were unvaccinated – it was a meta-analysis of 110 published studies between 1st Dec 2019 and 16th July 2020. There was, of course, no vaccinations anywhere during that period so referring to these people as ‘unvaccinated’ must have been done to fit a particular mischievous agenda. I am actually pleased you brought this study to my attention since it needs to be exposed for leading people like the Times and yourself to believe it was showing something that it wasn’t.
One major conclusion in the paper seems sensible – that having diabetes or hypertension or ischaemic heart disease predicts for poorer outcomes (although the same could be said for many other conditions so there is hardly anything novel in this). But the first part of the conclusion seems entirely wrong. Just because you see covid hospitalising a lot of people who had pre-existing cardiac comorbidity certainly does not mean that covid caused their comorbidity. It seems that this part of the conclusion may have been influenced by possible conflicts of interests (see below).
There are a number of other specific concerns about the study:
- They included studies published from 1st Dec 2019 – but that was before covid was formally accepted to exist, so how could any study published in Dec2019/Jan2020 have patients with suspected covid? Any study published pre-mid Jan 2020 should be excluded by default, since even the flawed confirmatory PCR test was not available until then. There would be no way of knowing if ‘is covid’ results was a mix of ‘not covid’, ‘possibly covid’ and ‘probably covid’.
- How is ‘suspected’ the same as ‘confirmed’? When the symptoms used for Covid marry to any number of other conditions that are common (and even endemic) then how can you say that suspected covid is even ‘a thing’?
- Someone hospitalised with exacerbation of an existing condition is NOT the same thing as someone who gets a new diagnosis OF that condition after vaccination.
- Including so many Chinese studies clearly biases the work – and using China and USA to predict for LMIC (in the Introduction) is strange to say the least.
A colleague also noted the link between Prof Gupta (the senior author) and the Bill and Melinda Gates Foundation and other potential conflicts of interest:
- In this report Gupta is acknowledged as having provided the statistical support for a report that seeks to help the Bill and Melinda Gates Foundation and the Clinton Foundation find new ways to support medical/health research in the UK. There are also a number of links between Gupta before he came to QMUL and functions (like some project called D3140 for the Rotary Club funded by BMGF in Mumbai, and research out of Imperial College) supported by the Gates Foundation. He is also heavily involved in Wellcome Trust AND the WHO – and is listed on the minutes of meetings between the two.
- Gupta and the lead author (Sher May Ng) are both on this study that was in part funded by the NIH (Grumbach acknowledges an NIH grant while at the UCal Nursing School. My colleague managed to find that she also has an NIH.GOV email address).
- Co-Author Kenneth Rice has worked on studies like this with staff from BMGF.
- Kenneth Rice and Gupta are two of the over 200 doctors who are part of a research collaborative called TOPMed – funded by the NIH with a combination of US Gov and BMGF money.
I hope this helps you.
Yours
Norman Fenton
For clarification of the potential conflict of interest with BMGF, Scott McLachlan has provided the following information:
Bill Gates is the world’s largest single shareholder of Covid-19 vaccine manufacturer stocks and therefore every time Pfizer, Moderna, Lilly (Eli), GSK, CureVac or even AstraZeneca (he had something like 8% in AstraZeneca shares at one point) sell a vaccine, that’s money back in his pocket. (see here)
And while fact checkers claimed Gates would not profit from Gilead (Remdesivir), he actually purchased a significant chunk of Gilead and 27,000 shares in Merck in 2018 in preparation. (Merck are one of the manufacturers who licensed to manufacture Remdesivir in their plants)
The thing that journalists get confused on is the idea that he, through his foundations, made ‘grants’ to Moderna et al. These were not ‘grants’ in the way we get grants from EPSRC or UKRI – they are grant investments. Various companies in control of the BMGF are shareholders in Pfizer and Moderna. In return for sinking $50mil+ into Moderna, Gates’s foundation took a large slice of Moderna’s shares.
Further, Gates sells access to “investment opportunities” through GAVI COVAX and AMC. The ‘investor’ (usually a rich western govt or pharma/healthcare company) gives money to GAVI in their rich country where they make profits and need a tax write-off… then, they get included in the contract with some LMIC govt to sell them vaccines. The whole model works by shifting where the pharma/healthcare company make their profits. Pharma companies ‘invest’ by subsidising vax initially and then, over time the contract shifts to the country’s govt paying extortionate rates for future vax.
As one of the links above says – as the world keeps getting sicker Gates keeps getting richer. He invested $555mil into COVID vax companies during 2019/20 and has made an estimated $4bil return. Nice work if you can get it.
We rightly mourn the dead, but mustn’t forget the disabled
Worrying data from the USA and UK
Health Advisory & Recovery Group | February 1, 2023
Much of the analysis around Covid 19 vaccine harms revolves around counts of deaths, and excess mortality. This is perfectly understandable since “excess deaths” is a “hard” measure in that most countries are able to count the number of their citizens who have died quite accurately so this does allow for some reasonably informative inferences and international comparisons.
The same is of course not the case for “covid deaths” which even the strongest proponents of the establishment covid narrative have had to admit are affected by differences between countries in classification, testing rates, and policies.
However, as well as many countries experiencing excess deaths, there is currently a second huge problem: marked increases in the numbers registering as long-term disabled.
Because registering as disabled is usually done for the purposes of receiving financial assistance or other support from the state, there is a built-in gatekeeping function which limits spurious claims, so we can be reasonably confident that any significant increases represent genuine medical issues.
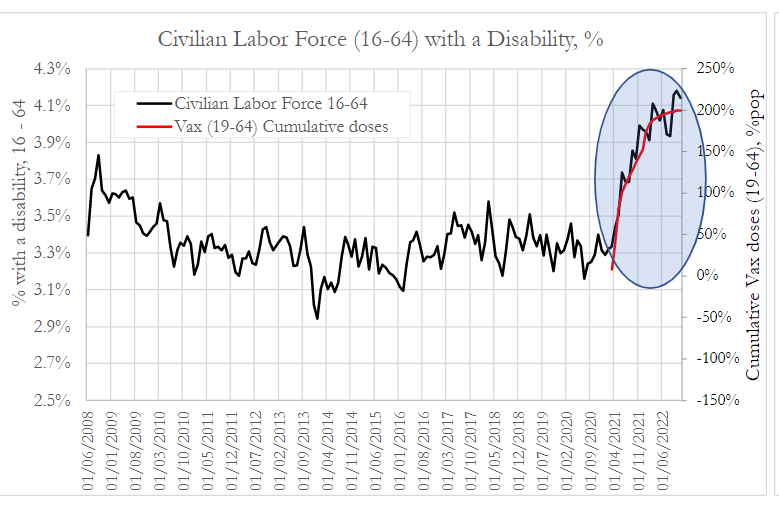
Looking at the USA first, a group called Phinance recently published an analysis of the proportion of the US civilian labor force who are registered as disabled.
This graph shows the % of workers aged 16 to 64 with a disability against the total number of Covid vaccinations administered in the same age group.
Phinance also published this graph which is a regression analysis showing a very strong correlation between the increase in the number disabled and the total number of doses given – something which actually is rather obvious from the above.
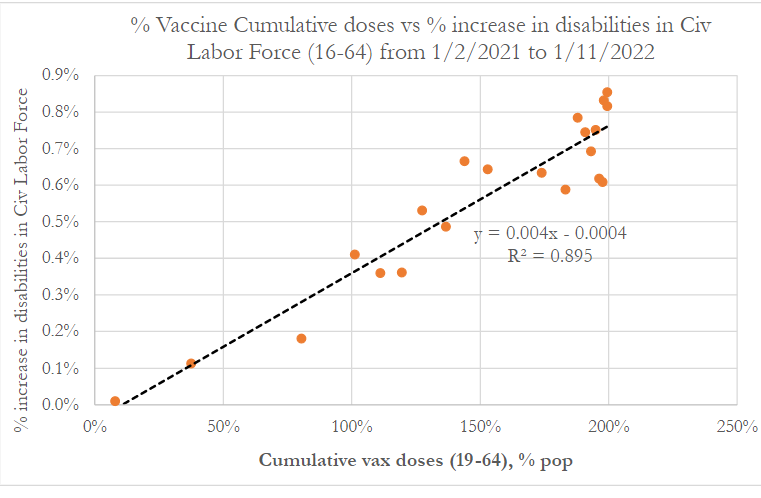
It is fair to point out that such a regression analysis should not in general be performed on cumulative series of data (ie total doses administered), but rather on discrete data (which in this case would be daily or weekly doses). If the measurements can only increase and not fall (as with cumulative data), this limits the significance of any correlation observed, as by default they will rise together.
This is less of a problem here in that only one of the 2 data points (vaccines) is cumulative (for the other axis they have used the increase in the number disabled). However, we wrote to the authors to ask why they didn’t use daily or weekly doses administered.
They responded with the not unreasonable point that because the adverse effects occur over a wide and variable period after dosing, a cumulative series is probably more informative. We agree. Just because fewer doses were given one week does not mean there were fewer people at risk of developing a post vaccination disability in that week.
The extremely experienced medical statistician who blogs as “John Dee” has performed further analysis on the US data above. The article is rather technical but in essence by applying a number of sophisticated statistical tools he concludes that using cumulative data may exaggerate but has not invalidated the findings, which should therefore be regarded as highly suggestive (though not in themselves proof of) a causal relationship.
However, the criticism of the statistical methodology was never really “on point” anyway. Science advances through testing hypotheses by questioning the available data.
The point of the analysis of the disability data was not to conclusively “prove” that the vaccines cause harm, but rather to answer the question: Is there a signal of potential concern which warrants further study? The answer to this appears to be “yes” and anyone finding excuses to not even look further should be regarded as willfully blind.
Of course, the link to vaccination could quite easily be further tested by ascertainment of the vaccination status of a representative sample of the disabled, with comparisons to disability rates in the unvaccinated. That this is not even being discussed must surely be regarded as a red flag.
When a potential signal of concern is replicated internationally, it increases the likelihood that we are dealing with a causal relationship. Not much quality data on disability rates is available from other countries, but one country which does publish some comparable data is the UK.
In the UK, if disabled, a state payment called a personal independence payment (PIP) can be claimed. An official UK government report states that there have been “unprecedented levels of new claims in recent quarters” (in England and Wales).
This has been reported by various news websites, including Yahoo’s article titled “The ‘astonishing’ rise in people claiming one key benefit”.
PIP data is actually downloadable from an official UK government website, and “John Dee” has performed some analysis on it which can be read here and here.
The new claims data plotted against cumulative doses administered looks like this (with thanks to John Dee for the graphs):
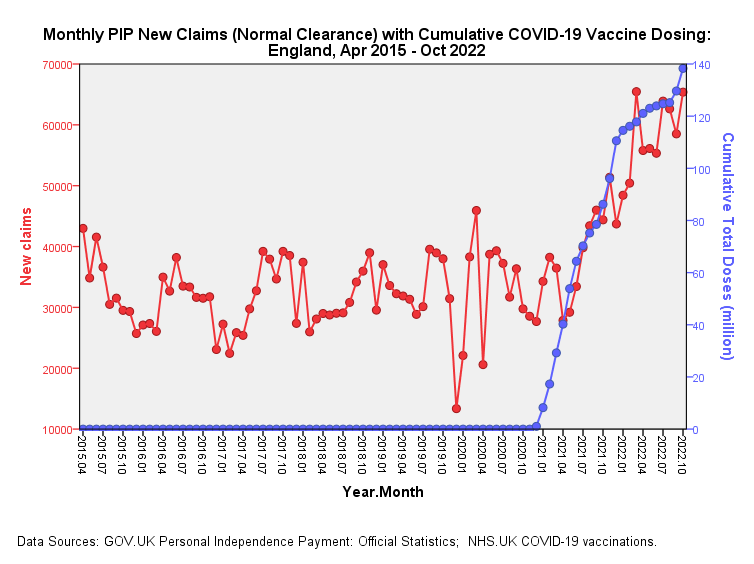
Clearly, this bears an uncanny resemblance to the US data above.
As he did with the US data, John has drilled deeper into the data, showing, for example that whilst claim rates in the pandemic period were similar to those in the pre-pandemic period, there is a huge uptick in the post-vaccine period, with the error bars (and statistical tests of significance) indicating that this is not just random variation.
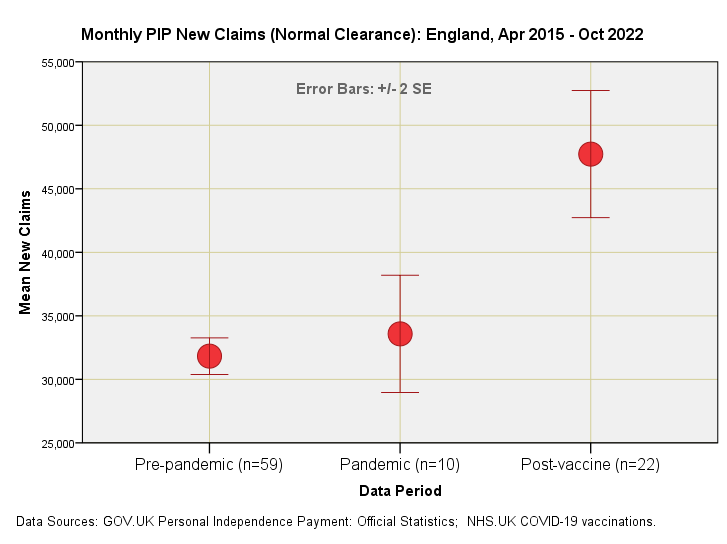
Moreover, he has used a technique called “cross-correlation” which strongly suggests that “the increase in the month-on-month changes in total administered doses is followed three months later by a rise in month-on-month changes in new cleared claims.”
This would appear to add plausibility to the causation argument, in that three months is the period required by the government as a minimum qualifying period before an application for PIP can be filed.
Overall, these datasets surely raise huge concerns, which could be assuaged by further more detailed examination of the data, especially including vaccination status. We urge governments to carry out such an analysis, which need only be performed on a representative sample in order to generate reliable conclusions.
FDA Adviser Inadvertently Confirms Pfizer is Doing Gain-of-Function Research
BY WILL JONES | THE DAILY SCEPTIC | FEBRUARY 1, 2023
They’re starting to come now – the ‘debunkings’ of the Pfizer undercover video sting, in which executive Jordon Trishton Walker, “Director of Research and Development – Strategic Operations and mRNA Scientific Planning”, tells his ‘date’ that Pfizer is looking to mutate the virus “so we could create preemptively developed new vaccines, right”.
Pfizer released a statement on Friday, which notably did not deny that Dr. Walker works for the company (a fact which has anyway been confirmed via internet searches). Now the latest ‘debunking’ effort comes from Medpage Today.
After making the odd claim that “it is currently unclear if the man in the video is actually an employee of Pfizer, and if that is his real name” (journalism isn’t what it used to be), writer Michael DePeau-Wilson notes that Pfizer’s statement “summarily debunk[ed] the claims made in the video”, as the company stated that it “has not conducted gain of function or directed evolution research” related to its “ongoing development of the Pfizer-BioNTech COVID-19 vaccine”.
While it is true that the statement does say this, it also says that “we have conducted research where the original SARS-CoV-2 virus has been used to express the spike protein from new variants of concern”. Furthermore, it admits that:
When a full virus does not contain any known gain of function mutations, such virus may be engineered to enable the assessment of antiviral activity in cells. In addition, in vitro resistance selection experiments are undertaken in cells incubated with SARS-CoV-2 and nirmatrelvir in our secure Biosafety level 3 (BSL3) laboratory to assess whether the main protease can mutate to yield resistant strains of the virus.
Despite the initial denial, then, what is being described here plainly is gain-of-function research – after all, the company is engineering the original virus to express the spike protein from new variants of concern, variants which are ‘of concern’ precisely because their spike protein has immune-evasive properties.
In case there is any doubt about this, FDA vaccine adviser Dr. Paul Offit inadvertently confirms it in the Medpage piece.
“Usually, when people talk about gaining function, they’re talking about making it so that the virus is either more deadly or more easily transmitted or that it now can jump species,” Dr. Offit says.
“[T]rying to make the virus more immune-evasive or more contagious… would be considered gain-of-function research,” he adds.
Right, so exactly what Pfizer has said it is doing – engineering “the original SARS-CoV-2 virus… to express the spike protein from new variants of concern”.
Offit tries to obfuscate, stressing that “Pfizer has been working with an mRNA platform that is coded for coronavirus spike proteins, not a whole virus”.
Yes, the vaccine does not use whole virus. But no one said it does. The matter at hand is what Pfizer is doing to the virus as part of its vaccine development research. And Pfizer is clear that it is engineering “the original SARS-CoV-2 virus… to express the spike protein from new variants of concern”. The whole virus, note.
Offit then implies that it isn’t gain-of-function research because the variant has already been created by “mother nature” and Pfizer is just reproducing what nature has already done.
If there was some evil hand back there that was trying to make the virus more immune-evasive or more contagious, that would be considered gain-of-function research, but it’s not happening. The evil hand is mother nature.
But even if the variant already exists in nature, that doesn’t mean it’s not gain-of-function research to engineer a virus to gain the immune-evasive mutation in the lab. Besides, how can you be sure you’re producing the exact same variant and not some subtly (or not-so-subtly) new and more immune-evasive variant?
Offit then appears to betray an ignorance of the process of making the vaccine, as he says the “remarkably effective” development involved sequencing SARS-CoV-2 in “a matter of months”. In fact, the virus was sequenced several times even in the last week of December 2019, and took a couple of days each time, not months.
Perhaps needing to restore his reputation with the politico-medical establishment after his criticism of the boosters last month (is this why he was given the job of defending Pfizer?), he is now effusive with praise for the mRNA vaccines. “This is the best medical achievement in my lifetime,” he says. “And my lifetime includes the development of the polio vaccine.”
Thus, despite the denials that what Pfizer is doing is gain-of-function research – denials which presumably take advantage of the fact that ‘gain-of-function’ is not rigorously defined – it’s clear that what Pfizer admits to doing falls squarely within the definition cited by Dr. Offit, namely the commonly accepted one, which includes making the virus more “immune-evasive”.
And they appear to tacitly acknowledge that, which is why they make their excuses. In Pfizer’s case, that it is “required by U.S. and global regulators for all antiviral products” and “carried out by many companies and academic institutions in the U.S. and around the world”. In Offit’s case that Pfizer was just copying “mother nature”.
In fact, though, as Dr. Robert Malone has pointed out, Pfizer has previously been upfront that it is doing this research, including in an August 2021 article in STAT News, and almost nothing in the undercover video is new. Why such a fuss was made about scrubbing it from the internet is therefore an interesting question – though this may be more linked to the sensation around it than the facts, which Pfizer’s response anyway did not deny. How could it, when those facts were already on public record?
Perhaps the main lesson, then, is that we all need to be paying more attention.
We also need to think hard about what kind of research should be allowed and what should be banned. The reaction to the Project Veritas video suggests a strong feeling that this kind of work should not be done – including when it is (supposedly) imitating what nature has already created. The fear in the public is real and justified, and relates to the folly of engineering viruses to make them worse. Can this ever be a good idea? My feeling is there’s no need to go beyond the viruses and variants nature already provides us with, and to stick to using real specimens, not engineered ones. But the current regulatory regime and scientific establishment clearly disagrees.
Whatever the right answer, we need to be able to talk about this properly. Not be subject to global, military grade censorship when someone tries to raise the topic as a matter of public concern, albeit in a sensational (and entertaining) way.
Australian Health Authorities Call For More COVID Boosters… But The Public Says No

By Tyler Durden | Zero Hedge | January 30, 2023
Australia and New Zealand suffered some of the worst pandemic mandate conditions of any country in the western world, crossing the line into totalitarianism on a number of occasions. Australian authorities restricted residents of larger cities to near house arrest, with people not being allowed to go more than 3 miles from their homes. Citizens were given curfew hours between 9pm and 5am. They were banned from public parks and beaches without a mask, even though it is nearly impossible to transmit a virus outdoors and UV light from the sun acts as a natural disinfectant.
In the worst examples, Australian citizens received visits from police and government officials for posting critical opinions about the mandates on social media. Some were even arrested for calling for protests against the lockdowns. In Australia and New Zealand, covid camps were built to detain people infected with covid. Some facilities were meant for those who had recently traveled, others were meant for anyone who stepped out of line.
As the fears over covid wane and the populace realizes that the true Infection Fatality Rate of the virus is incredibly small, restrictions are being abandoned and things seems to be going back to normal. It’s important, however, to never forget what happened and how many countries faced potentially permanent authoritarianism under the shadow of vaccine passports. If the passports rules had been successfully enforced, we would be living in a very different world today in the west.
Luckily, the passports were never implemented widely. Australian health authorities are once again calling for the public to take a fourth covid booster shot, but with very little response. Only 40% of citizens took the third booster, and new polling data shows that 30% are taking the fourth booster.
With an astonishing rise in excess deaths by heart failure in Australia coinciding exactly with the introduction of the covid mRNA vaccines, perhaps people are deciding to finally err on the side of caution. Why take the risk of an experimental vaccine over a virus that 99.8% of the population will easily survive?
Let the Crow Eating Begin
Newsweek : “It’s Time for the Scientific Community to Admit We Were Wrong About COVID and It Cost Lives | Opinion”
By John Leake | Courageous Discourse | January 31, 2023
Newsweek just published an editorial by Kevin Bass, a medical school student in Texas, about how the official scientific establishment in the United States got it wrong about COVID-19. At the risk of sounding immodest, all of the realizations that he catalogues in his essay were apparent to me by May of 2020, almost three years go.
People often ask me why I perceived at the beginning of this mess that our public health officials were lying to us. The answer is simple: I am a longstanding student of history (including medical history) and of human nature. It is precisely a lack of education in history that made so many people susceptible to being manipulated and defrauded by the Bio-Pharmaceutical Complex.
Students of political history have often marveled that the Anglo-Irish statesman, Edmund Burke, made all of his accurate predictions about the French Revolution in 1790. Burke foresaw that the Jacobins would grossly mismanage everything and then resort to terror when none of their harebrained schemes worked. He predicted the bloody fiasco would end with the accession to power of a military commander.
Three years after Burke’s Reflections on the Revolution in France was published, the Reign of Terror began. Nine years later, Napoleon Bonaparte came to power through a combination of subterfuge and soldiers with fixed bayonets.
How did Burke make these predictions? He knew history and he understood human nature. He therefore saw that the Jacobins had no idea what they were doing. None of their abstract schemes acknowledged the complex reality of human affairs. Their entire conception of reality was ideological, not practical, and they insisted on imposing it with fanatical zeal.
Precisely the same is true of the Vaccine Syndicate that ran the official Pandemic Response. Its leaders are votaries of the COVID-19 Vaccine Cult, and all of their policies were in the service of getting a needle in every arm. Their monolithic policy totally ignored the complex reality of the problem.
Those familiar with history (and medical history) could see by April of 2020 that “The Science” constantly invoked by our government health agencies was an ideological construct—an Orthodoxy—and not true science. True scientific inquiry was conducted by doctors in the field who had the courage to treat the illness instead of waiting for the heralded “vaccine.”
Kevin Bass’s Newsweek is a good start. May the rest of the Official “Follow the Science” Establishment get out their forks and knives and start eating crow.
Acute Psychosis after COVID-19 Vaccination
Alarming Manuscripts Report Acute Neuropsychiatric Symptoms
By Peter A. McCullough, MD, MPH | Courageous Discourse | January 30, 2023
Unvaccinated patients have mentioned half-jokingly that COVID-19 vaccination in friends and family makes some of them “crazy.” While I have always brushed this off as fear driven vaccine ideology taking over common sense in some zealots, the building literature on neuropsychiatric symptoms is alarming. There are now ~10 papers describing headache, fever, and a range of acute neuropsychiatric symptoms after both mRNA and adenoviral COVID-19 vaccination. The strong bias among editors and publishers has kept countless papers out of the mainstream medical media, hence one has to look far and wide to find information on the topic of vaccine safety. Borovina et al, from Croatia described three cases of acute headache followed by psychosis.
Borovina T, Popović J, Mastelić T, Sučević Ercegovac M, Kustura L, Uglešić B, Glavina T. First Episode of Psychosis Following the COVID-19 Vaccination – A Case Series. Psychiatr Danub. 2022 Summer;34(2):377-380. doi: 10.24869/psyd.2022.377. PMID: 35772162.
All three patients required hospitalization with exhaustive diagnostic testing and medical treatment. One of the cases progressed to attempted suicide with a knife stabbing to the abdomen requiring emergency abdominal surgery. As a doctor I am disturbed by medical evidence demonstrating gene coded SARS-CoV-2 Wuhan Institute of Virology Spike protein in the human brain after vaccination. I wonder how many subtle changes go clinically unrecognized. Even if a small number are affect, the massive numbers who came forward make any “rare” complication a common issue to face in clinical practice.
In conclusion, we should not downplay or attempt to normalize neuropsychiatric symptoms after COVID-19 shots. Every case should be taken seriously. Suicides after December 10, 2020 should be investigated and the brand, doses, and dates of vaccination should be recorded by healthcare personnel and noted by family members.
Featured Video

Did the 9/11 Hijackers Really Fly the Planes?
or go to
Aletho News Archives – Video-Images
From the Archives
Aaron Siri’s Book: Vaccines, Amen
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
Aaron Siri makes it clear in Vaccines, Amen: The Religion of Vaccines that the story we’ve been told about vaccine science rests far more on belief than proof.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
And he does. … continue
Blog Roll
 Aletho News
Aletho News- Did the 9/11 Hijackers Really Fly the Planes?
- ‘Jewish lobby’ deceived Putin – Lukashenko
- The UK Joins the Pirates
- Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report
- Press TV reporter wounded in Israeli drone strike on southern Lebanon
- Time for Trump to Tell Benjamin Netanyahu to Go Away!
- Israeli officials: ‘Security zones’ to remain in Lebanon, Syria, Gaza
- Israel Fails to Sabotage Islamabad Accord… At Least for Now
- Araghchi: US Responsible for Implementing MoU with Iran
- US must cut military, intelligence assistance to Israel to protect Iran deal: Ex-Trump official
- If Americans Knew
- Jared Kushner’s Israel-linked island, and other dubious projects
- Why Are Crypto Billionaires and AIPAC Spending $8+ Million to Elect Adrian Boafo?
- Why the Mainstream Media Should Stop Using the ADL as Their Go-To Antisemitism Source
- Censorship and Thuggery Won’t Save Israel’s Reputation
- Israel Searches for a Red Sea Foothold in Somaliland
- They Weren’t Convicted of Terrorism, But These Palestine Activists Got Sentenced as Terrorists Anyway
- “Ceasefire” is not in Israel’s vocabulary – Daily Update
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- No Tricks Zone
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
