It seems he used to tweet about eugenics. He liked it.
And it seems he remains intrigued with it.
But he was not impressed with the talks by me, Aseem Malhotra, Robert Malone, Sasha Latypova. Guess what? This was not a science conference in Stockholm. It was a conference about what has really been going on these past three years. He likes the straw man argument.
So who is this Kevin Bass, who some commenters to my last post described as a twitter troll regarding nutrition and low carb diets. Why is he apologizing for mistakes that the system made? Like, he admitted to LOTS of mistakes?
He had to explain to his followers that with the Newsweek piece he has reinvented himself. He has decided to stop being an attack dog and instead bring us sweetness and light. Oops. He forgot his new persona, however, when he attacked the Stockholm conference. Who will he be tomorrow?
We could end the debate on COVID vaccine safety instantly. All we need is the death-vax record data. But today, that data is being concealed by the health authorities in every jurisdiction. Here’s why.
Executive summary
A simple database of death-vax records should be made publicly available by the CDC and other health authorities worldwide.
The death-vax records can be analyzed in seconds using a variety of totally objective methods to show whether the COVID vaccines have increased or decreased all-cause mortality in each age range.
No medical records, cause of death, etc. are required or needed. Just the age, date of death, and dates of vaccination are all that is required for each death since the start of the COVID vaccination program.
The death-vax data has been collected, but it has never been made publicly available anywhere in the world. There is no PII or HIPAA violation by disclosing the records.
There is absolutely no excuse for this data not to be made PUBLICLY available now.
Because kids are most at risk, universities in particular should be demanding data transparency of the death-vax records.
It is immoral and unethical for universities to mandate COVID vaccines if the health authorities refuse to show us the death-vax database records that would justify their use.
The death-vax record data
The death-vax data consists of one record for each death since Dec 14, 2020 to the present with these columns:
Age
Date of death
Date of each COVID vaccine administered (blank if unvaccinated)
The CDC could quickly collect this information, do the database join, remove the PII fields, and make this database publicly available.
This would reveal to the entire world whether the vaccines are safe or not. Instantly. No more debates.
No medical records are required. No judgment is required. The analysis is all based on mathematics and the law of large numbers. If the vaccines are saving lives, we’ll know it. If the vaccines are killing people, we’ll know it.
Introduction
EVERYONE should be demanding to see the death-vax record-level data. It can be easily compiled. It is dispositive. We’d know instantly whether the vaccines are safe or not. No more arguments. No more debates. No more censorship. One and done.
Yet, nobody in the mainstream infectious disease or epidemiology community seems to care about seeing this data. Nobody is calling for it. Why is that? Are they afraid of being proven they are wrong?
If the vaccine is so safe, they should be shouting for the release of this data from the rooftops because nearly 80% of the public is no longer drinking the Kool-Aid:
But the authorities are remaining silent and keeping the data under wraps. That can only mean one thing: the data is horrible and they know it. That’s why they are hiding it from public view.
That’s not just a hunch. I did my own data collection and analysis. Even after adjusting for the bias of the reporters (by restricting the analysis to just parents and grandparents of the reporter), the signal of harm was huge.
Science used to be about data. Not anymore.
Science used to be about data and what the data shows. Sadly, today, science is about what the CDC says, even if there is no data in support of the recommendation whatsoever.
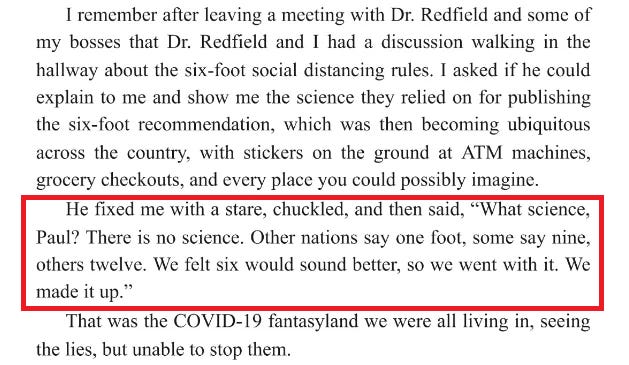
The most stunning example of this is the “six foot rule.” Did you know that it was entirely fabricated out of thin air? From Presidential Takedown page 49:
What is even more stunning is that the CDC has never admitted this publicly. This is evidence that they are a corrupt organization and the corruption goes to the very top of the organization.
We have over two years of data. Why not make it public?
We now have over two years worth of death and vaccination data for people who died after getting a COVID shot, yet nobody wants to see the record level data tied to the vaccination dates?!?!
Let me be perfectly clear:
This is an abject failure of the entire medical community for not demanding to see this data.
People paid for us to see this data with their lives. Why is it being hidden from us?
In the US, hundreds of millions of people participated in a massive clinical trial and have data to share with people. At least 500,000 of the participants paid the ultimate price: they sacrificed their lives to send a message to America about the vaccines. It is extremely disrespectful to these people to ignore their death data and not share it with the public. Why are we not allowing these people to share their data?
Do you think if we could ask those people right before they died, “Do you want to let others know what killed you?” Do you think they would all say, “No! Don’t let anyone know. Please keep it a secret!”?
Every institution in the world that is recommending or requiring COVID vaccination should be DEMANDING to see this data made public
John Beaudoin and I have been calling for the death data to be set free and made public. We have been ignored.
Why aren’t any of these organizations calling for data transparency here so we can learn the truth?
The mainstream medical community
Heads of state throughout the world
The CDC
The FDA
The White House
Congress
The mainstream media
Public health authorities
Any doctor or nurse who recommends the jab to patients
Universities who mandate the vaccines for students, staff, or faculty
Any organization that supports COVID vaccines for their members, employees, or visitors
The data exists in VSD as well. But the CDC won’t allow anyone to see it.
The data exists in every state health department. But you can’t FOIA it because it requires a join to avoid PII problems and FOIA requests are not allowed if they generate effort like that. So FOIA requests won’t work.
It’s time for everyone to demand that our health authorities “Show us the data!”
We should all refuse to comply until they produce it.
In the same way Tom Cruise said passionately “Show me the money,” everyone all over the world should be equally passionate with their doctors and healthcare authorities and demand: “Show me the DATA” before we agree to comply with their requests/demands regarding vaccination.
Civil disobedience in Canada
Check out this video from True North entitled “Show us the data and evidence” that described the civil disobedience in Canada:
Business owners and local politicians are pushing back against the government’s lockdown measures. Their ask of the government is simple – if you’re going to shut us down, show us the data and evidence.
Calling all parents: ask your school why they aren’t calling for the data to be produced
The data that we have shows that the biggest harm is being done to kids.
Therefore, the biggest urgency is to put pressure on any school or university that recommends or requires the COVID vaccines to drop it immediately
Please ask the university president or head of school at any school your child attends to contact the CDC and let them know that if the CDC doesn’t make the death-vax record level data publicly available with the next 30 days, that the school will suspend their COVID vaccination policies until such time as this data is produced and scientists can analyze it. That is the only ethical thing to do.
You can refer to my article in your email.
The public health authorities have been voluntarily keeping the data secret for two years now. That data would end the debate. We should not let them continue to get away with it.
Last Thursday, the FDA convened its Vaccines and Related Biological Products Advisory Committee (VRBPAC) to discuss the future of covid vaccines.
The panel voted 21 to 0 in favour of moving towards a more simplified vaccine schedule – an annual shot which would be updated as new variants emerge – much like the annual flu shot.
Despite the unanimous vote, VRBPAC members did raise concerns about knowledge gaps and questioned the need to boost everyone, as well as the futility of chasing rapidly mutating viruses.
But it all fizzled out quickly, and the FDA promised to reconvene in May or June to discuss the data further.
That said, I had some interesting observations of my own.
Still no correlate of protection
We are three years into the pandemic, and the FDA has still not established a “correlate of protection” for the vaccines.
Eight covid-19 vaccine emergency use authorisations (EUAs)* have been granted, based on their ability to induce “neutralising antibodies,” a surrogate marker of protection.
The idea is, the more antibodies you produce, the better you are protected.
Except, neutralising antibodies do not predict the degree to which someone is protected from infection… and the FDA knows it.
Ofer Levy, VRBPAC member and Professor of Paediatrics at Boston Children’s Hospital first voiced his concern at the April 6, 2022 meeting.
“We’re at risk of doubling down on a failed strategy,” said Levy as the committee discussed a framework for offering annual covid shots for Americans.
“Where is the federal effort to coordinate all of that to develop a public repository around the correlate of protection, and to make sure we have the best available data for the immunogenicity when we make those decisions?”
The FDA’s top vaccine official, Peter Marks, agreed with Levy.
“There is not a clear, perfect, immune correlate of protection” admitted Marks, “We’re using poor man’s immune correlates of protection here — or poor person’s immune correlates of protection with antibody levels.”
In Dec 2022, Peter Marks reiterated these concerns in an article published in JAMA. He and his co-authors wrote:
“Therefore, unless correlates of protection that are strongly associated with duration of protection against COVID-19 can be identified, it is likely that rather than relying on immunobridging to infer vaccine effectiveness, large randomized clinical trials similar to the initial trials of the currently authorized or licensed vaccines for COVID-19 will be required to ascertain the effectiveness of these new vaccines.”
But fast forward to this latest meeting, and it becomes clear that we’re all still in the dark.
We have no correlate of protection, the FDA is relying heavily on real world studies (confounded data) and the agency still has not demanded any randomised controlled trials to show the bivalent booster can reduce severe disease or hospitalisations.
It’s no wonder doctors are coming out in droves, refusing to have any more covid shots until the FDA demands better studies.
“I don’t think we can say with credibility what the objective benefits are for someone like me to take an additional dose, nor what the rate of any rare but important side effects would be,” tweeted Todd Lee, a physician certified in Infectious Diseases and General Internal Medicine in Quebec, Canada.
Similarly, Vinay Prasad, haematologist-oncologist at the University of California San Francisco vowed not to take any more shots until there were data from randomised controlled trials.
“I took at least 1 dose against my will. It was unethical and scientifically bankrupt. I am not done with that error. No more,” he tweeted.
No update on subclinical myocarditis
As part of its post-marketing requirements, Pfizer is legally obligated to conduct a study involving people aged 16 to 30 to look at rates of subclinical myocarditis (i.e. underlying damage to the heart muscle without causing symptoms).
The final report was due 31 Dec 2022, but that deadline lapsed, and the FDA said nothing. There was no mention of the study, neither in the briefing notes ahead of the VRBPAC meeting, or during the meeting.
I asked the FDA directly for access to Pfizer’s study, but the agency said in an email, “You may submit a FOIA request for this information, or if you would like it more quickly, you can reach out to the manufacturer directly.”
Pfizer did not respond to my request, and the FDA refused to confirm whether it had even received Pfizer’s study, before abruptly ending our communication.
Jessica Adams, an expert in drug regulatory affairs pointed out on twitter that the FDA had quietly changed the due date for the study from 31 Dec 2022 to 30 June 2023.
So, now as it stands, millions of young people will receive boosters, mandated or not, without knowing if the vaccine is causing subclinical myocarditis.
FDA still working from home
Finally, the meeting was again held online because the majority of FDA employees are still working from home.
Since all federal employees have been mandated to take the covid-19 vaccine to “protect themselves and those around them,” why aren’t they conducting face-to-face meetings?
“FDA leaders are in a bubble. How much longer will the FDA (18,000-employees) continue to work remotely? It’s mid-day on a weekday and the parking lot is essentially empty” tweeted Marty Makary, surgeon and public policy researcher at Johns Hopkins University.
“The FDA was telling the rest of America to get vaccinated, mask up and go back to work, but the FDA mysteriously did not follow its own advice,” said David Gortler, drug safety expert and former senior advisor to the FDA commissioner.
Well, it’s as though the FDA heard the cries.
Today, the FDA announced that “staff will be transitioning to a hybrid workplace.” This transition will enable face-to-face formal meetings between FDA and industry to resume within weeks.
*FDA issued eight EUAs based on neutralising antibodies (immunobridging studies) – an unproven correlate of protection.
At a time when concerns about serious adverse reactions to the Covid-19 vaccines are escalating, one might reasonably expect the World Health Organisation (WHO) – a specialised agency of the United Nations responsible for international public health – to take immediate and decisive action. Perhaps a recommendation to pause the vaccine rollout would be a reasonable step under the circumstances. Or maybe an urgent request to member states to rapidly undertake thorough investigations of the links between the mRNA vaccines and serious physical harms, such as myocarditis. But no, those responses have not been forthcoming. Instead, the WHO has published communication guidance on how to nullify criticism of the vaccines.
The document, titled Vaccine Crisis Communication Manual – a step-by-step guidance for national immunization programmes, was produced in 2022 by the WHO European office with the stated aim of supporting countries ‘in effectively responding to events which may erode the public’s trust in vaccines and authorities that deliver them’. The manual offers detailed recommendations about how those in authority should respond to a ‘vaccine crisis’ (defined as any occurrence that ‘will most likely or has already eroded public trust in vaccines … and may create uncertainty’). The explicit, overarching goal is to ‘rebuild trust in vaccines’.
The guidance is structured – with military precision – around four sequential phases:
1. Co-ordinate & engage
2. Design communication response
3. Monitor public opinion & the media
4. Inform the public
In keeping with the dominant narrative during the Covid era, the presumption is that vaccinations are always for the greater good. Repeatedly asserted throughout the document is that adverse events may not be causally linked to the jabs. Pre-prepared messages are recommended that ‘emphasize the value of immunization based on a risk-benefit analysis’. Somewhat sinisterly, public health officials are advised to ‘use existing or implement new monitoring tools to monitor public opinion’ and to maintain ‘good relations with key journalists and the media’. And when someone dies in the aftermath of vaccination, communicators are directed to say, ‘We are committing all available resources to the investigation of this unfortunate incident and are doing our utmost to find the cause as soon as possible’; (it is doubtful whether the vaccine-harmed population would concur with this claim). Clearly, the overarching goal of this WHO manuscript is to protect the pro-vaccine narrative under any circumstances.
The tone of this WHO document perpetuates the myth that anyone questioning the net benefits of the jabs is an ‘anti-vaxxer’ who is spreading misinformation. One illustrative example is the reference to an earlier – 2017 – WHO publication, titled ‘How to respond to vocal vaccine deniers in public’. Co-authored by Katrine Habersaat (who is also a co-author of the WHO, 2022, document) the article refers to these ‘vaccine deniers’ as people who have ‘a very negative attitude towards vaccination and are not open to a change of mind no matter the scientific evidence’. According to Habersaat, these agitators ‘censor opposing opinions’ and ‘use personal insults or even legal actions to silence representatives of the scientific consensus’. In light of the widespread vilification and censorship endured by those experts who have, over the last three years, challenged the dominant Covid narrative, the irony of these assertions is off the scale.
There was once a time when the primary aim of the WHO was the provision of accessible and holistic healthcare to all, regardless of socioeconomic status. The content of this Vaccine Crisis Communication Manual provides further evidence that this is no longer the case. The welfare of ordinary people is not the WHO’s priority; the appeasement of their pro-vaccine paymasters now takes precedence.
A preprint paper has just been published in the Lancet authored by the New Zealand Ministry of Health, ‘Adverse Events Following the BNT162b2 mRNA COVID-19 Vaccine (Pfizer-BioNtech) in Aotearoa New Zealand’. The paper reveals that there is a statistically significant association between Pfizer mRNA vaccination and both myocarditis and acute kidney injury (AKI). Here in little New Zealand, you wouldn’t know it though. MSM has not covered it, anywhere.
AKI, also known as acute renal failure (ARF), is an episode of kidney failure or damage which happens within a few hours or days. It causes a build-up of waste products in the blood and makes it hard for the kidneys to keep the right balance of fluid in the body. AKI can affect other organs such as the brain, heart and lungs.
The study examined the comprehensive medical records of 4million people. There were 1,778 more cases of AKI than predicted from historical pre-pandemic rates – an alarming incidence of one case for every 2,200 vaccinations. In addition to AKI and myocarditis, researchers also found elevated rates of blood clots and platelet damage. The finding of AKI is new and concerning, but incredibly the study concludes that its findings provide assurances about the safety of mRNA vaccines. How could they say that? I am not reassured, I am alarmed – and so should you be.
The study compared the background rates of 12 adverse events of special interest (AESI) with their incidence following Covid-19 vaccination. The study included only events that occurred within 21 days after Covid vaccination which resulted in hospitalisation. Therefore the study specifically ruled out effects of Covid vaccination resulting in hospitalisation or death any time after 21 days and also discounted adverse events for which those affected did not immediately seek hospital treatment.
Was this a credible cut-off point? No. Studies have detected markedly elevated levels of full-length spike protein, unbound by antibodies, in the plasma of individuals post-vaccine which can persist well beyond 21 days. For example see here. This indicates that injected mRNA sequences can actively produce spike protein for extended periods. Spike protein is known to be associated with the development of myocarditis for example and is believed to have toxic effects on other organs including the liver.
Was the hospitalisation data a completely reliable measure of the extent of the effects? No, absolutely not. We are a small country and we talk to one another. Multiple people have publicly reported presenting to hospital with concerning symptoms following mRNA vaccination such as tachycardia, chest pains or neurological dysfunction, and being sent home without any investigative tests and a diagnosis of ‘vaccine anxiety’ and an ibuprofen prescription. My daughter-in-law was one of these. My neighbour developed a kidney injury subsequent to vaccination but didn’t report it to a doctor for weeks. She now has difficulty digesting most foods.
GPs and hospital staff have been deliberately manipulated by government propaganda into believing that the mRNA vaccine is safe. GPs who advised their patients that there were risks associated with the jab were told they might be struck off if they persisted – some actually were.
The NZ Ministry of Health did not warn district health boards of the risk of myocarditis until mid-December 2021, near the end of the period covered by the study. This MoH advice described vaccine-induced myocarditis as rare and generally mild. Prior to this there was an obvious incentive to disbelieve and dismiss patients reporting cardiac symptoms. Because GPs were afraid to make any association between the jabs and health conditions, they were also disincentivised to order tests or advise hospitalisation.
There has been no general advice of the risk of renal failure post mRNA vaccination. My local school received a visit from a GP informing staff and students that there were no safety issues with the vaccine and that it had been rigorously tested for over 30 years, a downright lie. As a result, a teacher friend with persistent chest pains had no idea it might be connected with vaccination and did not seek medical help until he unburdened himself to me.
When Jacinda Ardern wrote on her Facebook page that people could comment on adverse effects, expecting a few replies about mild discomfort, 33,000 comments were posted within a matter of hours. Ardern’s staff famously stayed up all night to delete them. As of November 2022, the government has acknowledged only two deaths associated with mRNA vaccination. There are persistent third-party reports circulating that the Ministry of Health made some payments to families whose children died following vaccination on condition that they would not make public comments. As a result, these reports cannot be reliably confirmed or ruled out. If true, possibly these were aimed at reducing vaccine hesitancy among the young.
A concerning issue here is the attitude of the media to reports of vaccine injury. They are ignoring them. Even published studies such as this one are receiving no attention whatsoever. MSM appears to have relinquished its investigative role, leaving the public in the dark.
It is clear that detailed knowledge of adverse effects of mRNA vaccines would enable GPs and hospital staff to deal appropriately and sympathetically with injury. It would also enable doctors and medical staff to relay factual informed consent to patients. This has not happened.
So how far are reporting errors and the 21-day cut-off skewing the authors’ invalid conclusions of vaccine safety? How can we find out? We currently have record rates of excess all-cause mortality, but despite having the data to do so, the MoH has not undertaken any investigation to determine if there is any correlation between all-cause deaths and vaccine status. This simple procedure would settle any controversy, but a mistaken faith in vaccine efficacy has prompted MoH investigators to turn a blind eye to the obvious.
This is exactly the same obfuscation, hiding of data and failure to investigate that governments have promoted around the world. UK Health Minister Maria Caulfield in the House of Commons brushed aside concerns about, and investigation of, excess deaths as if rapidly rising death rates are an entirely ordinary and uninteresting feature of post-pandemic life. Similar requests put to the Minister of Health in New Zealand have been met with silence. Facts don’t count for much when it comes to modern democracy.
With the resignation of Jacinda Ardern, my thoughts were dragged back to Covid once more. Jacinda, as Prime Minster of New Zealand was the ultimate lockdown enforcer. She was feted round the world for her iron will, but I was not a fan, to put it mildly. Whenever I heard her speak, it brought to mind one of my most favourite quotes:
‘Of all tyrannies, a tyranny sincerely exercised for the good of its victims may be the most oppressive. It would be better to live under robber barons than under omnipotent moral busybodies. The robber baron’s cruelty may sometimes sleep, his cupidity may at some point be satiated; but those who torment us for our own good will torment us without end for they do so with the approval of their own conscience.’ C.S. Lewis
At one point she actually said the following:
“We will continue to be your single source of truth” “Unless you hear it from us, it is not the truth.’
If I ruled the world, anyone who said, that, or anything remotely like that, would be taken as far as possible from any position of power, never to be allowed anywhere near it again. Ever.
Yet, there are still many who believe her to have been a great and caring leader. She certainly hugged a lot of people with that well rehearsed pained/caring expression on her face.
Enough of that particular woman. But it got me thinking about lockdowns again and the whole worldwide madness of Covid. This was a time of such blundering idiocy that I find increasingly difficult to believe it ever happened. A bad dream.
‘The sky is falling, the sky is falling…’ Cue, everyone running about in panic. People, allegedly, dropping dead on the streets. Mortuaries, allegedly, overflowing. Freezer lorries, allegedly, stacked with dead bodies. Bring out your dead!
I worked with doctors who strode around the wards in positive pressure protective gear. There were GPs who simply refused to visit elderly residents in nursing homes. On my patch this was all GPs and all nursing homes. Meanwhile I happily visited away with a mask stuck to the top of my head.
During the Covid pandemic I travelled far past angry, to reach a point of utter weariness. Instead of becoming outraged by the latest rubbish that was being pronounced, I very nearly washed my hands of it. However, after learning of Jacinda’s resignation I roused myself to have another look at what actually did happen. Or to be more specific, what was the impact of Covid on overall mortality. The only outcome that really matters.
Rid your mind of the numbers claimed to have died of Covid. The, never to be clarified distinction between those who died ‘of’ or ‘with’ Covid. Or those who read an article on Covid and then, overwhelmed with fear, stepped out in front of a bus. Thus, becoming a Covid related… associated, something, anything to do with Covid, death.
Over time the Covid figures became so ridiculous and unreliable as to become meaningless. I should know, I wrote some of the death certificates myself. Let me think… ‘She died of COVID, she died of COVID not. Eeny, meeny, miney mo…’
I am not saying that Covid did not kill a large number of people. But the fact that deaths from influenza disappeared completely for two years tells me all I need to know. ‘Roll up, roll up, Ladies and Gentlemen, to see the amazing lady influenza disappear before your very eyes.’ An astonishing trick, all the way from La La Land. ‘You expect me to believe that? Ho, ho, ho, very funny…. Oh, sorry, you actually do.’
Anyway, to clear my internal database of horribly unreliable figures, I went back to look at my favourite graphs on EuroMOMO. This website looks at overall mortality, and only overall mortality. Their data comes from countries who do know how to record deaths, honestly. Unlike some others, who shall be nameless … China.
However, the main reason to focus on EuroMOMO is that overall mortality is something you cannot fake. About the only thing you can do to manipulate the figures is hold back data for a month or two – which has been done, but not to any great degree. So, without further ado, let us move onto EuroMOMO. Below is a recent graph. I have deliberately removed most of the information you need to know what it is showing. I wanted people to avoid jumping to conclusions … that they might then find it difficult row back from.
I found myself examining this graph idly and thought. Imagine if you had no idea what you were looking at here. What would you think? It’s a squiggly line, yes. Very good, gold star. What else?
To give you a bit more detail. This is a graph of overall mortality, across a large number of European countries. All of those who provide data to the EuroMOMO database anyway. Norway, the ultimate European lockdown champion, has mysteriously disappeared from the database. Maybe they shall return …. I have begun to see everything as a conspiracy nowadays.
The graph itself begins in January 2017 and finishes in January 2023. As you can see (if not terribly clearly) there are two wavy dotted lines. These lines rise up in the winter, and then fall back down in the summer. Something seen every year. This is because, every year, more people die in the winter than in the summer.
Everyone thinks they know the reason for this winter summer effect, but I am not so sure they do. But that is an enormously complicated topic for another time.
The lower, dotted lines represent the ‘average’ mortality you would expect to see [with upper and lower ‘normal’ limits] year on year. Above those wavy dotted lines sits a solid spikey line. This represents the actual number of deaths that occurred. Not just from Covid, but from everything.
This does raise an immediate question. If we keep seeing more deaths than we would expect in the winter, year on year, then the ‘average’ number of deaths should rise? Thus, the wavy dotted lines ought to be going up and up, in the winter. But they don’t.
I am not entirely sure why this is not the case. But it is a statistical question of such mind-boggling complexity that I am, frankly, unable to answer it. I have looked into it, but I was scared off by the sheer scale and difficulty of the mathematics involved. Too many equations for my poor wee brain.
Anyway, this graph starts in the winter of 2017 and ends about now. The vertical lines are drawn at midnight on Dec 31st each year. Which means that we have almost exactly six years of data. Excellent data, not manipulated in any way. I say this because, whilst the diagnosis of ‘Covid death’ may be disputed, the diagnosis of death cannot.
What stands out? Well, there was a very sharp peak of deaths in early 2020. This, as you have probably worked out, was when Covid first hit. I find it fascinating that it was so transient. It came, it went… gone. For a bit anyway.
Was the precipitous fall due to strict lockdowns? Some will doubtless argue this. However, we all locked down again in autumn 2020 and the death rate went up, and stayed up, for about six months. Until, that is, January came along, and it all settled down again. Which follows pretty much the pattern of 2017, 2108 and 2019. And the pattern of all pandemics. They come, and they go. Some a little earlier, some a little later.
What else do you see – now that we are all pretty much fully vaccinated? I think another thing that stands out is the sudden and sharp rise in mortality in November 2022. Which is virtually identical to the spike in 2020. Strange?
However, to my mind, the thing that shouts most loudly about this graph is that the years of Covid pandemic panic really do not look that much different from the previous three years. Half close your eyes, and there is almost nothing to see. The Covid peaks were a little higher, and a little longer – maybe.
If you knew nothing about the Covid pandemic I don’t think you would exclaim. ‘My God, look at these vast waves of death in 2020, 2021. What amazing, never seen before thing, happened here?’ Yes, first spike of early 2020 was certainly sharp, and unusual, but it was short. And very little different to the spike at the end of 2022. As for the rest?
Now, I would like to turn your attention to Germany. The most populous country in Europe. Here it is even more clear that the years of the Covid pandemic are not remotely unusual. If I had removed the calendar years off this graph, you would be hard pressed to spot the Covid pandemic. In truth, you would be more than hard pressed. You couldn’t.
The 2018 influenza spike was equally dramatic to Covid peak of 2021, if not more so. [You may have noticed that there was no peak in 2020] In addition, at the end of 2022, we have the highest peak of all. Future historians might well look at this graph and ask. ‘Tell me, why did the world go mad in 2020, and remain mad through 2021? Why did everyone lockdown in March 2020, and then do nothing whatsoever in December 2022?’
It almost goes without saying that, had we locked down again in November 2022, it would have been claimed that lockdown saved us all. Look at how quickly it came, then went. Well, they could have claimed it. But we didn’t lock down again, did we? In direct contrast to Germany. What of the people living in Luxembourg?
Luxembourg is surrounded by Belgium France and Germany. People move freely from one to the other, always have done, and still do. The ‘deadly’ Covid pandemic raged all around them. Here, absolutely nothing happened. Mind you, they also seem to have been unaffected by influenza.
Whilst the Germans were dying in large numbers in 2018, the Luxembourgians carried on serenely, not an extra death to be seen. Why? Discuss. [It seems that most/all countries unaffected by Covid, were also unaffected by earlier flu epidemics].
I know some of you may be thinking that Germany is much bigger than Luxembourg so … so what? If you are going to see an effect on mortality, you are more likely to see it happen, more dramatically, and rapidly, in a country with fewer people.
I should explain that the figures on the left axis, on the German and Luxembourg graphs (unlike the first one), do not represent total deaths, they are the ‘Z score’. That is, the deviation from the mean.
The upper dotted line represents a Z score of five. That means, five standard deviations above the mean. It has been decreed that if you hit more than five standard deviations above the mean, for any length of time, this is a signal that ‘something bad’ is happening. The alarm starts goes off, and epidemiologists run around bumping into each other. ‘The sky is falling… etc.’
If you use the Z score it makes no difference how large the population is. It has been specifically designed to make it possible to compare changes in overall mortality, in populations of very different sizes. I feel the need here to make it clear that Luxembourg is not that small. It has more than twice the population of Iceland, for example.
Enough of the maths already.
So, deep breath, and trying to bring all these random thoughts together. What does EuroMOMO tell us? It tells us that Covid was a bit worse than a bad flu season, with 2018 being a good reference point. [There have been far worse flu epidemics than 2018, and I am not talking about 1918/19].
What EuroMOMO makes most clear, at least to me, is that Covid was not, repeat not, a pandemic of unique power, and destructiveness. It could have never remotely justified the drastic actions that were taken to combat it.
Belatedly, this is becoming recognised, as has the damage associated with lockdowns. Here is the abstract of an article from 2022. A bit dry, but worth a read. ‘Are Lockdowns Effective in Managing Pandemics?’
‘The present coronavirus crisis caused a major worldwide disruption which has not been experienced for decades. The lockdown-based crisis management was implemented by nearly all the countries, and studies confirming lockdown effectiveness can be found alongside the studies questioning it.
In this work, we performed a narrative review of the works studying the above effectiveness, as well as the historic experience of previous pandemics and risk-benefit analysis based on the connection of health and wealth. Our aim was to learn lessons and analyze ways to improve the management of similar events in the future.
The comparative analysis of different countries showed that the assumption of lockdowns’ effectiveness cannot be supported by evidence—neither regarding the present COVID-19 pandemic, nor regarding the 1918–1920 Spanish Flu and other less-severe pandemics in the past.
The price tag of lockdowns in terms of public health is high: by using the known connection between health and wealth, we estimate that lockdowns may claim 20 times more life years than they save. It is suggested therefore that a thorough cost-benefit analysis should be performed before imposing any lockdown for either COVID-19 or any future pandemic.’ 1
In the face of such evidence, the argument for lockdown seems to be transforming into a somewhat pathetic whinge. ‘We didn’t know. It’s all very well people saying we shouldn’t have locked down now. We didn’t hear you saying it at the time. We were just following The Science, don’t blame us. Better safe than sorry. Don’t blame us … I think you’re being very nasty to us.’
This, of course, is nonsense. There were plenty of scientists arguing against lockdown at the time. However, they were all ruthlessly censored, attacked, and silenced. Experts such as Prof. John Ioannidis, Prof. Karol Sikora, Prof. Sunetra Gupta, Prof. Carl Heneghan. These last two UK professors argued very strenuously against lockdowns. They were ignored, then vilified. Here from an article written in January 2021:
‘… Sunetra Gupta. She’s been getting flak from the mob for months but it reached a crescendo yesterday when she was on the Today programme. Why is the BBC giving space to a nutter, people asked? She isn’t a nutter, of course. She’s an infectious disease epidemiologist at Oxford University. But she bristles against the COVID consensus and that makes her a bad person, virtually a witch, in the eyes of the zealous protectors of COVID orthodoxy. Professor Gupta has written about the barrage of abuse she receives via email. ‘Evil’, they call her.’
‘… her chief crime, judging from the hysterical commentary about her, is that she is critical of harsh lockdowns. She is a founder of the Great Barrington Declaration, which proposes that instead of locking down the whole of society we should shield the elderly and the vulnerable while allowing other people to carry on pretty much as normal. It is this perfectly legitimate discussion of a social and political question — the question of lockdown — that has earned Gupta the most ire.’ 2
I would like to point out that I was arguing against lockdown, right from the very beginning. Yes, I do enjoy saying, ‘I told you so’ from time to time. It is one of the few satisfactions I get in life nowadays. Here is a section from a blog I wrote in March 2020. Once again, right from the start:
‘… However, there is also a health downside associated with our current approach. Many people are also going to suffer and die, because of the actions we are currently taking. On the BBC, a man with cancer was being interviewed. Due to the shutdown, his operation is being put back by several months – at least. Others with cancer will not be getting treatment. The level of worry and anxiety will be massive.
Hip replacements are also being postponed and other, hugely beneficial interventions are not being done. Those with heart disease and diabetes will not be treated. Elderly people, with no support, may simply die of starvation in their own homes. Jobs will be lost, companies are going bust, suicides will go up. Psychosocial stress will be immense.
In my role, working in Out of Hours, we are being asked to watch out for abuse in the home. Because we know that children will now be more at risk, trapped in their houses. Also, partners will suffer greater physical abuse, stuck in the home, unable to get out. Not much fun.
Which means that we are certainly not looking at a zero-sum game here, where every case of COVID prevented, or treated, is one less death. There is a health cost.
There is also the impact of economic damage, which can be immense. I studied what happened in Russia, following the breakup of the Soviet Union, and the economic and social chaos that ensued. There was a massive spike in premature deaths.
In men, life expectancy fell by almost seven years, over a two to three-year period. A seven-year loss of life expectancy in seventy million men, is forty-nine million QALYs worth. It is certainly a far greater health disaster than COVID can possibly create…’ 3
And lo, the damage is coming to pass. Maybe not so many people dying of starvation as I predicted, at least not in the West. In poorer countries, however …
Another terrible thing that happened during lockdown was the vilification of anyone who dared question the official narrative. Yet almost everything they predicted has come true. Have the likes of Professor Gupta been forgiven and welcomed back into the fold? Have a wild guess on that one.
What of those who deliberately whipped up the panic and led the dreadful behavioural psychology teams. They quite deliberately frothed the population into a state of terror. What of those, whose ridiculous models kicked the whole damned thing off? The Professor Neil Fergusons of this land? Yes, you.
These people are all still comfortably ensconced, advising away. Their positions fully secure. In the UK they were mostly given knighthoods, damehoods, and other shiny gongs to impress their friends with. This, I find hard to swallow.
More worrying is that there will never be an honest review on the pandemic. Why, because so many people in positions of power would be seriously threatened by it. Which means that any such review will end up as a completely bland whitewash. ‘In general the actions taken were reasonable, and in a situation where so much was unknown, it was better to try and protect the public … blah, blah.’ Case closed.
The reality is that these lockdowns were a complete disaster. A complete disaster. The fact that we will never have a proper debate about them, means that we will learn nothing from what happened. This, in turn, means that another disaster is on the way. Those who should be listened to will be attacked, silenced and censored, again.
Those who got it all horribly wrong last time will be handed even greater powers … next time. The reason why lockdowns did not work, they will argue, is because they were not strict enough, or long enough. We need proper lockdowns next time. You have been warned. Cast your eyes over China.
I will leave you with the conclusion of the paper ‘Are lockdowns effective in managing pandemics?’
Neither previous pandemics nor COVID19 provide clear evidence that lockdowns help to prevent death in pandemic
Lockdowns are associated with a considerable human cost. Even if somewhat effective in preventing COVID19 death, they probably cause far more extensive (an order of magnitude or more) loss of life
A thorough risk-benefit analysis must be performed before imposing any lockdown in future.
Which can probably be summed in in the words: Primum non nocere. First, do no harm.
The central guiding principle of medicine that was hurled out of the window in March 2020 by people who seem not to exhibit a scrap of humility, or humanity. Nor apology.
Mark Kerry was a healthy 48 year-old from Worcestershire, a father of three, grandfather of two and a loving husband to his wife Melanie. Together with Melanie, Mark loved life and lived it to the full, they socialised with friends every weekend, loved to travel and loved holidays.
Mark and Melanie run mobile home parks and were heavily impacted in 2020 when the COVID-19 pandemic hit. With the mobile home business being a mixture of residential and holidays, the holiday side was halted when lockdown and heavy restrictions were enforced. As with millions of people worldwide, they found themselves spending most of their time at home.
Like most of us, Mark was eager to get life back to some form of normality and, knowing the business was suffering and being self-employed, the quicker the better.
In late 2020, nine months into the COVID-19 pandemic, it was announced that a Covid vaccine had been approved and was being rolled out to stop the spread of the virus and save lives, ready for use in December 2020.
This was exciting news for Mark and Melanie. Their lives and their business had been placed on hold for far too long and they were ready and eager to resume their lives as they were pre-pandemic; the vaccine was the way out. Mark waited patiently for his turn to have his first jab. While waiting, the media was full of stories of how wonderful these vaccines were and that everyone absolutely must get this vaccine. It was suggested if you don’t get the vaccine you are being selfish. The Prime Minister and Cabinet ministers were telling the public daily on TV that everyone must have it, as well as every news channel and road signs everywhere saying the same. GPs were sending letters, flyers were coming through the door, doctors were all over the TV, with some doctors even suggesting the AstraZeneca vaccine was 100% safe and effective. This of course was what we were all hoping for and most of the population believed.
Finally it was Marks turn to have his vaccine. On March 2nd 2021 Mark had his first dose of the AstraZeneca vaccine. Initially everything was fine and Mark seemed to escape the mild flu-like side-effects and aching arm that people were talking about. That was until the evening of March 15th 2021 when Mark had a headache and noticed blood in his urine. Melanie called 111 and they sent them to Worcester hospital. When the doctor examined Mark he noticed that Mark had a rash on his legs and admitted him straight away. Over the next day Mark’s headache got worse and, following some blood tests, it was revealed that Mark’s platelet count was at a very low rate of 14; normal levels would read between 150 and 450, so this in itself was alarming. On top of that results from a brain scan revealed a blood clot on Marks brain known as Cerebral Venous Sinus Thrombosis (CVST).
CVST is a type of rare blood clot that forms in the venous sinuses in your brain. This is a system of veins found between the layers of the dura mater – the tough outer layer of your brain that lies directly under your skull.
The clot can block the blood in your brain from draining out toward your heart. When this happens, blood cells may break from the pressure, cross the blood-brain barrier and seep into nearby brain tissue. This can cause a haemorrhage, a type of stroke that stems from internal bleeding. CVST can be life-threatening. You need immediate medical attention.
Very quickly the doctors informed Mark and Melanie that they thought it was a reaction to the vaccine. The next day, on March 17th 2021, Mark was getting worse and lost some of the use in his left leg and arm. Another scan was ordered and this revealed the clot was growing. Melanie realised how poorly Mark was. This was extremely distressing as due to the COVID-19 restrictions Melanie was unable to be on the ward with Mark. The nurses brought Mark into the corridor of the hospital in a wheelchair to see her. They told each other how much they loved each other and Mark told Melanie to tell their children how much he loved them. The nurses told Melanie they would get a side room ready for when Melanie came back in the evening so she could stay the night by Mark’s side.
That evening, before Melanie got back to the hospital, the hospital rang to say Mark had deteriorated and was now having seizures. He had also gone into cardiac arrest, and they made the decision to put Mark in an induced coma and on a ventilator. Melanie rushed to the hospital along with family members. They let her and their three children, Mark, Robert and Nicole wait in the corridor to say goodbye to Mark before they moved him to Birmingham Queen Elizabeth hospital. He was in an induced coma and they were told to expect the worst. On March 18th 2021, the hospital told the family that scans were showing Mark had a bleed on the brain and even if he survived there would likely be significant damage and not to expect Mark to walk out of the hospital. Mark’s family couldn’t just leave him and go home so they stayed in their cars outside the hospital all week, but still unable to see Mark due to the COVID-19 restrictions.
The hospital called the family in the afternoon and told them they couldn’t control the seizures and they wouldn’t stop so they needed to perform a thrombectomy to remove the clot. Melanie and the family were devastated and were desperate to see Mark. Melanie was told she could see him before they did the procedure but sadly when she got to the intensive care unit doors, despite Melanie crying and begging, the doctors wouldn’t let her in and she was just told to wait to hear from them.
Fortunately, the thrombectomy went well and Mark survived the procedure. He was then left to rest for a few days. After a few days the medical team couldn’t wake Mark successfully so on March 25th they put in a tracheostomy and on March 26th Mark finally woke. However it wasn’t until April 3rd, when they took the tracheostomy out, that Melanie and the family could finally talk to him on the phone. Mark had lost a lot of use of his left arm and leg, but over the coming days thankfully a lot of this returned. Mark was finally discharged from hospital on April 9th 2021, 26 days after being admitted. Against the odds, Mark proved the doctors wrong and walked out of the hospital, albeit loaded with several medications and a long road ahead.
Once home, Mark had to do a lot of therapy. He has now made a good recovery, considering what was expected. However his three fingers on his left hand are not really working and he still suffers with debilitating side effects. But both Mark and Melanie feel they are very lucky that he survived and thank the doctors and nurses for saving his life.
Even though when in hospital Mark was told that the AstraZeneca vaccine caused the CVST, it wasn’t until sometime after he left the hospital that they fully understood what the cause was. It was explained that Mark was diagnosed with Vaccine induced Thrombotic Thrombocytopenia (VITT).
VITT is diagnosed by having all five of the following:
Onset of symptoms five to 30 days after vaccination against COVID-19.
Presence of thrombosis (blood clots)
Thrombocytopenia (platelet count under 150)
D-Dimer level over 4000
Positive anti-PF4 antibodies on ELISA
Mark had all of these, so his diagnosis was confirmed as VITT induced by the AstraZeneca vaccine. There are approximately 444 confirmed cases of VITT in the U.K. and sadly 81 deaths. However, this number is likely to be much higher as thousands of people who suffered blood clots were not given the relevant tests to detect VITT.
To this day, Mark’s PF4 antibodies are still testing positive, so he is still on the same blood-thinning tablets and blood pressure tablets as he came home from hospital with. He now has blood tests every four weeks. As VITT is a newly identified disease there are uncertainties around the decisions on stopping blood-thinning medications and it is still uncertain what it means when PF4 antibodies are still testing positive. Also, Mark’s latest scan revealed the blood on his brain has not dispersed and he still takes 3000mg of levetiracetam a day to prevent seizures, the same amount he came home from hospital with. The doctor has said with time this will be reduced but he will remain on them for the rest of his life.
Since being discharged from hospital Mark has had to go back in: his platelet levels dropped again and he needed an immunoglobulin infusion (IVIg), which made him feel so poorly he needed to go back yet again. It is now almost two years later but Mark still suffers and his life has been hugely affected. He remains extremely weak and tired; he suffers from debilitating fatigue and has daily headaches. Melanie lovingly explains he really doesn’t complain, saying he is marvellous and they know he is so lucky to be alive.
Following almost two years of living in a nightmare, Mark and Melanie are now trying desperately to return to as much normality as possible. They are self-employed and work together so have been impacted hugely, emotionally and financially. Mark is trying to do as much as he can possibly manage.
They applied to the Vaccine Damage Payment Scheme (VDPS) in April 2021. They really didn’t get much feedback for months. In June 2022, over a year later, they were told that Mark’s claim had been sent to the medical assessors. The medical assessors are the decisionmakers and assessed Mark’s claim solely on his medical notes that were requested early on; no personal assessment would be carried out and no up-to-date medical records would be requested, so the assessment is not based on any ongoing symptoms or any disabilities that have occurred as a result of VITT.
On December 23rd 2022, Melanie and Mark received an email saying a letter had been sent with the medical assessors’ decision. Melanie asked if the decision could be emailed and on December 29th 2022 that email arrived. It said that the medical assessors accepted causation – that the vaccine had caused Mark’s illness – but did not accept that Mark had reached the 60% disablement that is required to be eligible for an award. They only took into consideration Mark’s hand; they didn’t even mention all the medication he needs to prevent seizures, now or in the future, or take into account how Mark’s life has been impacted by fatigue and daily headaches.
So after two years of living in this nightmare, a future that has now been dramatically altered, no help will be offered by our Government – the same Government that spoke on TV daily throughout the COVID-19 pandemic and the months to follow, telling us all that we must have the vaccine to stop the spread and to save lives. The same Government that told us all that the vaccine was safe and effective. The same Government that prevented us from travelling if we weren’t fully vaccinated. And the same Government that told us we were selfish if we didn’t have the vaccine. Mark had done what was asked of him by our Government, and now Mark and Melanie will have to live with that decision and the consequences for the rest of their lives. Any help from our Government has now been rejected.
Mark and Melanie, who are members of VIBUK, will now be asking for a mandatory reconsideration and will be supplying further evidence which was not requested by the VDPS. If this fails then it will go to a tribunal. But one thing is for sure, none of us are giving up and VIBUK will continue to fight and campaign for a reform of the current VDPS which we all agree is unfit for purpose.
The latest VDPS figures show, as of January 10th 2023, there were 491 VDPS claims rejected and only 33 awarded – a success rate of just 6%. Thousands more are still waiting for their decisions, and with the percentage of claims being rejected so high it is expected that there will be many more disappointments in the coming weeks.
This is extremely upsetting for many who are injured, who can no longer live the lives they had pre-vaccine and also for the families of the bereaved. The financial impact is enormous and many claimants and families are desperate for financial help; the VDPS was a lifeline that has now, in more than 90% of cases to date, been taken away.
Many can no longer work due to the injuries caused by the vaccine and many families have been hugely impacted financially and emotionally by the loss of a loved one. Lots of these families have been told they are not eligible for a payment by our Government, some because the medical assessors believed on the balance of probability the vaccine was not the cause of the injuries or death and some because the assessors believed the claimant is not injured enough, that they do not reach the 60% threshold required to be eligible for an award. Some of those rejected on the 60% threshold but accepted on causation, such as Mark, have a range of shocking injuries that vary from brain damage, blindness, permanent seizures, loss of feeling in limbs, loss of mobility, neurological issues, debilitating fatigue and damage to internal organs including serious heart conditions, plus many more. But the medical assessors have based their decisions on their own opinions, ignoring the opinions of the specialist consultants such as neurologists and haematologists. Many of those rejected will now be appealing and asking for a mandatory reconsideration.
Claire Hibbs, who was injured by the AstraZeneca vaccine, is part of Vaccine Injured and Bereaved U.K. (VIBUK), a group of individuals injured or bereaved by the Covid vaccines (with medical or coroners’ reports confirming this) campaigning for a change to the current Government vaccine damage payment scheme (VDPS) to create a bespoke COVID-19 compensation scheme that ensures the adversely affected are appropriately compensated and supported. They also want people similarly affected by the vaccines to know that help is available and for their stories to be heard and not ignored. VIBUK can be found on Twitter and contacted here.
The House of Representatives is very different than it was a year ago. Back then, any notion of ending vaccine mandates was shuffled into a memory hole. Anyone who opposed them was dismissed as an anti-vaxxer. Today, we may be seeing progress. Finally.
On Tuesday, Congressman Thomas Massie gave a speech explaining the reasons the vaccine mandate against healthcare workers must end.
“I rise in support of this resolution because it would facilitate the passage of HR 497, the Freedom for Healthcare Workers Act,” he said. “What does that bill do? It ends the unscientific, illogical, immoral, unconstitutional, unethical vaccine mandate on healthcare workers that is predicated on lies.”
He listed the five predicates for the mandate that turned out to be lies:
The vaccine prevents spread
The vaccines don’t cause any harm
The mandates are scientific
Natural immunity should be ignored
Nobody’s liable for the damage the mandate can cause
As he put it, “We’re living under medical malpractice martial law right now under the PREP Act and the EUAs.”
He concluded by dropping the ultimate truth bomb. “This is the epitome of hypocrisy. Nobody in this room was mandated to take a vaccine, and we’re voting on whether we’re going to force people who want to take care of people whether they have to take the vaccine.”
“We call upon the Charity Commission to conduct an independent and urgent investigation into these very serious allegations relating to the British Heart Foundation.”
Joint Open Letter from Doctors for Patients UK, HART and the UK Medical Freedom Alliance to Helen Stephenson, CEO, Charity Commission
Cc: Dr Charmaine Griffiths, CEO, British Heart Foundation (BHF)
Prof Charalambos Antoniades, BHF Chair of Cardiovascular Medicine
Rt Hon Rishi Sunak, Prime Minister
Rt Hon Steve Barclay, Secretary of State for Health and Social Care
Mr Andrew Bridgen, MP
Re: Allegations that the British Heart Foundation (BHF) is involved in concealing and withholding important information relating to harms to cardiac function caused by the novel mRNA vaccines
31 January 2023
Dear Ms Stephenson
We wish to express our deep concern, regarding allegations that the British Heart Foundation (BHF) is involved in concealing and withholding important information relating to the potential of the novel mRNA vaccines to damage cardiac tissue and function.
It was alleged in the House of Commons that staff working in a cardiology research department at Oxford University withheld information, for fear of losing funding from the pharmaceutical industry, and were therefore prioritising funding over patient safety.
Mr Andrew Bridgen MP stated in Parliament on 13 December 2022:
“It has also been brought to my attention by a whistleblower from a very reliable source that one of these institutions is covering up clear data that reveals that the mRNA vaccine increases inflammation of the heart arteries. It is covering this up for fear that it may lose funding from the pharmaceutical industry. The lead of that cardiology research department has a prominent leadership role with the British Heart Foundation, and I am disappointed to say that he has sent out non-disclosure agreements to his research team to ensure that this important data never sees the light of day. That is an absolute disgrace.”
It was subsequently asserted on GB News that the research department mentioned above was headed by Professor Charalambos Antoniades whose position is funded by the BHF. Despite GB News approaching Professor Antoniades for comment, he has made no public denial that Non-Disclosure Agreements (NDAs) were entered into by members of his department.
Doctors and the public rely on reputable and well-established charities such as the BHF to provide accurate and up-to-date information, as well as to highlight and investigate potential, novel causes of heart damage and heart disease. Concerns should be raised immediately, whenever there are doubts relating to the safety of any pharmaceutical product, so that administration of the product can be halted, protecting the public from unnecessary harm, while an investigation is carried out.
The BHF rapidly dismissed the allegations made by Mr Bridgen and called for those making the allegation to provide specific and credible information in support of it.
Due to the seriousness of the allegations, and given the absence of any public denial or clarification from Professor Antoniades, we are calling for a full and independent investigation into any suppression of data by the British Heart Foundation itself or by senior BHF grant holders.
There are a significant number of signals that COVID-19 vaccines have led to cardiac pathology, which warrants an urgent review of their safety:
The Pfizer trial saw four cardiac arrests in the vaccination group but only one in the placebo group after 6 months (although the numbers are too small to be statistically significant, this was a signal that should have been followed up).
The evidence for vaccine-induced myocarditis is well established and in older patients this may be misdiagnosed as any of the more common forms of heart disease. The rate of myocardial infarction was disproportionately high in the first three days after vaccination.
Studies in Thailand and Switzerland have shown rises in troponin levels consistent with damaged heart muscle in 3% of those vaccinated. Heart cells cannot be replaced and the resulting scarring can lead to electrical conduction issues and sudden death. 30% of the children in the Thailand study had cardiac signs or symptoms.
Vaccine-derived spike protein was detected in the heart biopsies of 9 out of 15 patients with post-vaccination myocarditis.
Vaccinated people had a rise in cardiovascular risk factors that would predict a significantly increased risk of heart disease (from 11% to 25% risk of a heart attack in 5 years). This study has been criticised for not having a control group but is the equivalent of an early phase clinical trial in demonstrating a safety concern.
An Israeli study showed a 25% increase in acute coronary syndrome and cardiac arrest calls in 16-39 year olds associated with the first and second doses of vaccine but not with COVID-19 infection.
There were 14,000 more cardiac arrest calls to ambulances in England in 2021 than 2020.
There has been a rise in cardiac excess deaths and excess deaths have been disproportionately seen in more highly vaccinated groups e.g. less deprived cohorts and people of white ethnicity.
In a report of 35 autopsies in Germany, there were 5 deaths confirmed as caused by a COVID-19 vaccine and a further 20 deaths where a contribution from the vaccination could not be excluded.
Post mortem studies have shown inflammation of the coronary arteries after vaccination, causing death four months later.
A separate post mortem report showed vaccine-derived spike protein in heart muscle, in the absence of COVID-19 infection, in a subject who had myocarditis before he died.
Australian hospitals have experienced intense service pressure since Summer 2021, despite no significant COVID-19 infection rates or reduction in healthcare capacity at that time.
Australians have seen a similarly timed rise in excess non-Covid deaths, with ischaemic heart disease being the biggest contributor. This was despite no significant volume of COVID-19 cases or reduction in healthcare before Omicron as was seen in the UK.
Systematic exploratory analysis of the possible causes in the rise in excess deaths by comparing countries, suggests a link to healthcare quality cannot be excluded but there is no link to COVID-19 or Long Covid. There is a weak link to lockdown severity but a strong correlation with vaccination.
Crucially, data has not been shared to counter the hypothesis that the mRNA vaccinations are linked to recent excess deaths caused primarily by cardiac pathology. The ONS were regularly publishing deaths by vaccination status. The last data was released for May 2022 and showed a higher mortality rate for that month in the vaccinated. No data has been shared since.
As medical professionals, and in the interest of patient safety, we demand that the British Heart Foundation immediately release the following information, in the public interest and in accordance with the requirements of the Freedom of Information Act 2000 (FOIA):
Any and all information and emails regarding potential and actual harms caused by the COVID-19 mRNA vaccines.
A copy of any Non-Disclosure Agreements that have been sent to people working at, or associated with, the British Heart Foundation and Oxford University, relating to COVID-19 vaccine safety and data.
A full list of conflicts of interests that the BHF and Oxford University have relating to the COVID-19 vaccines.
We further call upon the Charity Commission to conduct an independent and urgent investigation into these very serious allegations relating to the British Heart Foundation. Suppression of research findings, conflicts of interest and acting in the interests of commercial entities are in direct conflict with the requirements inherent in holding charitable status.
Thank you for your attention. We look forward to receiving a prompt response.
Professor Richard Ennos, MA, PhD. Honorary Professorial Fellow, University of Edinburgh
Professor John A Fairclough, BM BS, BMed Sci, FRCS, FFSEM(UK), Professor Emeritus, Honorary
Consultant Orthopaedic Surgeon
Professor Dennis McGonagle,PhD, FRCPI, Consultant Rheumatologist, University of Leeds
Professor Anthony Fryer, PhD, FRCPath, Professor of Clinical Biochemistry, Keele University
Professor Karol Sikora, MA, MBBChir, PhD, FRCR, FRCP, FFPM, Honorary Professor of Professional Practice, Buckingham University
Professor Angus Dalgleish, MD, FRCP, FRACP, FRCPath, FMedSci, Professor of Oncology, University of London; Principal, Institute for Cancer Vaccines & Immunotherapy
Professor Roger Watson, FRCP Edin, FRCN, FAAN, Professor of Nursing
Lord Moonie, MBChB, MRCPsych, MFCM, MSc, retired member of House of Lords, former Parliamentary Under-Secretary of State 2001-2003, former Consultant in Public Health Medicine
Dr Najmiah K Ahmad, BM, MRCA, FCARCSI, Consultant Anaesthetist
Dr Ali Ajaz, Consultant Psychiatrist
Dr Shiraz Akram, BDS, Dental Surgeon
Dr Sonia Allam, MBChB, FRCA, Consultant Anaesthetist
Dr Victoria Anderson, MBChB, MRCGP, MRCPCH, DRCOG, General Practitioner
Julie Annakin, RN, Immunisation Specialist Nurse
Wendy Armstrong, RN, BSc, DipHE, Practice Nurse
Dr Abby Astle, MBBChir, BA(Cantab), DCH, DGM, MRCGP, GP Principal, GP Trainer, GP Examiner
Dr Jonathan Eastwood, BSc, MBChB, MRCGP, General Practitioner
Dr Jonathan Engler, MBChB, LlB(Hons), DipPharmMed
Dr Elizabeth Evans, MA(Cantab), MBBS, DRCOG, retired Doctor, Director UKMFA
Dr Chris Exley, PhD, FRSB, retired Professor in Bioinorganic Chemistry
Dr John Flack, BPharm, PhD, retired Director of Safety Evaluation at Beecham Pharmaceuticals 1980-1989 and Senior Vice-president for Drug Discovery 1990-92 SmithKline Beecham
Dr Simon Fox, BSc, BMBCh, FRCP, Consultant in Infectious Diseases and Internal Medicine
Gayle Gerry, BSc(Hons), Registered Nurse
Sophie Gidet, RM, Midwife
Dr Cathy Greig, MBBCh(Hons), General Practitioner
Dr Ali Haggett, Mental Health Community Work, 3rd sector, former Lecturer in the History of Medicine
Mr Anthony Hinton, MBChB, FRCS, Consultant ENT Surgeon, London
Ian Humphreys, UKMFA Programme Director
Dr Keith Johnson, BA, DPhil(Oxon), IP Consultant for Diagnostic Testing
Dr C Geoffrey Maidment, MD, FRCP, retired Consultant Physician
Mr Ahmad K Malik, FRCS(Tr & Orth), Dip Med Sport, Consultant Trauma & Orthopaedic Surgeon
Dr Ayiesha Malik, MBChB, General Practitioner
Dr Imran Malik, MBBS, MRCP, MRCGP, General Practitioner
Dr Kulvinder S Manik. MBChB, MRCGP(2010), MA(Cantab), LlM(Gray’s Inn)
Dr Fiona Martindale, MBChB, MRCGP, General Practitioner
Dr Sam McBride, BSc(Hons) Medical Microbiology & Immunobiology, MBBCh, BAO, MSc in Clinical Gerontology, MRCP(UK), FRCEM, FRCP(Edinburgh), NHS Emergency Medicine & Geriatrics
Kaira McCallum, BSc, retired Pharmacist, Director of Strategy UKMFA
Mr Ian McDermott, MBBS, MS, FRCS(Tr&Orth), FFSEM(UK), Consultant Orthopaedic Surgeon
Dr Scott Mitchell, MBChB, MRCS, Emergency Medicine Physician
Dr Alistair Montgomery, MBChB, MRCGP, DRCOG, retired General Practitioner
Dr Alan Mordue, MBChB, FFPH, retired Consultant in Public Health Medicine & Epidemiology
Dr David Morris, MBChB, MRCP(UK), General Practitioner
Margaret Moss, MA(Cantab), CBiol, MRSB, Director, The Nutrition and Allergy Clinic, Cheshire
Theresa Ann Mounsey, BSc Hons in Midwifery studies.
Dr Alice Murkies, MBBS, MD, FRACGP, General Practitioner and Medical Researcher
Dr Greta Mushet, MBChB, MRCPsych, retired Consultant Psychiatrist in Psychotherapy
Dr Angela Musso, MD, MRCGP, DRCOG, FRACGP, MFPC, General Practitioner
Dr Sarah Myhill, MBBS, Dip NM, Retired GP, Independent Naturopathic Physician
Dr Christopher Newton, PhD, Biochemist, CIMMBER
Dr Rachel Nicoll, PhD, Medical researcher
Tim Nike, BSc(Hons), MCSP, HCPC, Senior Neurological Physiotherapist
Dr Richard O’Shea, MBBCH, BA(Hons) MRCGP, General Practitioner
More good news on vaccine, folks. First, you may be required to take only one Covid-19 shot per year, and if all goes well you will not even have to do that. You will be able to drink or even inhale your vaccine. No more painful injections, just a quick slurp or a snort and the job’s a good ’un. That’s you safe from the deadly virus for another year.
We could even make it fun. Why not hold Covid-19 vaccine parties? A selection of flavours in shot glasses (they don’t call them shot glasses for no reason) or add your vaccine to a vape and puff away until your immune system is primed.
I glean all this garbage from Global Health Now, the daily newsletter from the Johns Hopkins Bloomberg School of Public Health. The first story concerns how the Food and Drug Administration (FDA) in the United States is considering ‘simplifying the Covid vaccination schedule, allowing most people to get the currently available booster, regardless of how many doses they had received before that’. This means that if you are boosted up to the eyeballs or have never had one before and suddenly made the incomprehensible decision to start now, then Bob’s your uncle; roll up your sleeves.
Please note that nothing has changed; there is no new vaccine and no new threat. The FDA is just making an arbitrary decision to change the schedule. Clearly the aim is to get more people to accept the vaccination. But it is also clear that they are making this stuff up as they go along. They have no further evidence that the vaccines will work any better this way.
The information that is available to them is the abundant and accumulating evidence of vaccine harms which, incredibly, the Medicines and Healthcare products Regulatory Agency (MRHA) in the United Kingdom admits can be serious while insisting that the vaccines are safe. If truth is the first casualty of war – it certainly died early in the Covid-19 madness – logic is not far behind it. The MRHA is willing to trade off serious vaccine side effects against minimal protection from a virus which is virtually harmless to the vast majority of people. Perhaps the FDA is trying to reduce the number of boosters it says people will need in the hope that vaccine injuries will go away. Alternatively, it may be keen to accelerate the rollout before the general population wakes up to the fact that they are being conned, if they are lucky, and killed if they are not.
The potential for a drinkable/snortable/inhalable vaccine comes courtesy of US Speciality Formulations, a company which has produced the QYNDR vaccine. If QYNDR is a bit of a consonant-rich mouthful, then be informed that the official pronunciation if ‘KINDER’. And the advent of QYNDR is closer than you think. Phase 1 trials have already been completed in New Zealand (where else?) and all that is required is more funding to proceed with further trials. Apparently, it is very difficult to formulate a vaccine that survives the vicissitudes of the digestive tract.
And why do we need these vaccines? Well, according to US Speciality Formulations: ‘Covid-19 is still here and deadly.’ Also, I imagine that the inventors and investors envisage that this will make them shedloads of money. It clearly pays to perpetuate the Covid-19 narrative and to pepper it with as much panic as possible.
At some point in the panic-demic, the vaccine rollout became a juggernaut. Large and hard to stop. With the widespread and obvious extent to which people are gullible, government and drug manufacturers are willing to lie, health professionals are willing to stay silent and there are bucks to be made, it is unlikely that the juggernaut will be halted any time soon.
Who knows what’s next? Perhaps they will develop a vaccine that one can stick up one’s bottom. Whether or not they do, I strongly advise them that is what they can do with the present products.
Meta’s Instagram and Facebook platforms have removed a video by Project Veritas showing a journalist confronting YouTube’s Vice President of Trust and Safety Matt Halprin about the censorship of a video showing a Pfizer executive talking about mutating viruses.
Both platforms claimed that the video was in violation of Community Standards, specifically the policy prohibiting “content that could lead to identity theft or put someone at risk of physical or financial harm.”
In the video that was removed by both platforms, Project Veritas’ journalist Christian Hartsock asked Halprin why he banned a video showing Pfizer’s Director of Research and Development, Strategic Operations Jordan Trishton Walker talking about mutating viruses.
“How much is Pfizer paying you to run cover for them?” said Hartsock. “Is YouTube brought to us by Pfizer?”
On January 25, Project Veritas posted a video of Walker talking about the company mutating COVID-19 virus. Walker later said he made it up.
“Well, one of the things we’re exploring is, why don’t we just mutate it ourselves so we could preemptively develop new vaccines, right?” said Walker.
“If we’re gonna do that, though, there’s a risk of, as you can imagine, no one wants to be having a pharma company mutating fucking viruses.”
Top Cardiologist and The HighWire Contributor, Dr. Peter McCullough, was sued by health giant Baylor Scott & White, over an alleged violation of his separation agreement. On January 23rd, a Dallas County District Court dismissed the case with prejudice. Del announces the development, and offers his thoughts as well as congratulations to Dr. McCullough over the ‘win for freedom.’
The Covid emergency is over in America… in three more months says the White House. Why now? Is politics at the heart of this decision? And what does it mean for the EUA vaccines and therapies? The HighWire gets to the facts behind the headlines.
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.