The term ‘moral injury’ is a new one for me, as it probably is for most. It’s more commonly applied in a military context and only recently in health and social care, since 2020 to be precise. Indeed, the literature gently, knowingly or unknowingly, nudges us into believing that moral injury, reframed as occupational moral injury, isn’t a new concept but an inevitable consequence of working in an ethically challenging health and social care system.
Moral injury is understood as the damage done to an individual’s conscience or moral compass when they perpetrate, witness or fail to prevent acts that transgress their own moral beliefs, values or code of ethics. The term is thought to have originated after the Vietnam war when returning veterans and their carers struggled to make sense of high levels of anguish, anger and alienation that couldn’t be explained in terms of a mental health diagnosis such a post-traumatic stress disorder. It doesn’t take much stretch of the imagination to understand why veterans were morally injured but the Moral Injury Project at Syracuse University in New York cites examples such as using deadly force in combat and inadvertently causing harm or death to civilians and colleagues, giving orders which result in the injury or death of colleagues, failing to provide medical aid to civilians or colleagues and failing to report incidents such as sexual assaults.
When lockdowns were implemented in 2020, the health and social care workforce faced insurmountable and intolerable challenges when it was deemed unsafe in many situations to have close contact with fellow human beings who were in need of assistance. In essence, a workforce who function on the need for human contact could endanger life by simply doing their job. Subsequently, care and support was withdrawn or compromised through almost non-existent face-to-face interactions or time limited, with minimal physical contact if they took place at all.
Moral injury therefore makes sense in the context of health and social care. Staff were forced to deny medical and compassionate care to the injured and dying, leave adults and children in risky situations which in some cases led to death and injury, isolate frail older people from the life-giving company of family and friends and ignore or dismiss situations that previously justified urgent attention; all done while hiding smiles and humanity behind useless and potentially dangerous masks.
Moral injury during the pandemic can surely be applied across most professions and indeed the population: the police officer investigating a peaceful family gathering, the funeral director separating distressed relatives, the religious leader closing the door of a place of worship or the teacher who forced children to wear masks for hours on end. There were also the children who isolated their parents and parents who isolated their children, neighbours and community groups who withdrew essential help and support, and friends and family who got angry or fell out with those they disagreed with. Emotions and tensions ran high, leading me to think that many of us are morally injured to some degree or another. Is it any wonder that so many are struggling with poor mental health?
The growing number of articles drawing attention to moral injury, the most significant in the BMJ in July 2020 and a reference point for further articles, all focus on reassuring staff that a conflict of morals and the potential for injury is a normal consequence of doing what was necessary to prevent illness and death from Covid-19. At no point are the logic and morality of the rules called into question, which is surprising because the Moral Injury Project makes reference to two other potential causes of moral injury that are not referred to in recent literature:
‘Following orders that were illegal, immoral, and/or against the Rules of Engagement or Geneva Convention’;
‘A change in belief about the necessity or justification for war, during or after one’s service’.
As the realisation slowly dawns on the world that the inhumane actions which staff were forced to take were in fact unnecessary and based on flawed concepts with no robust evidence base, are we facing a rising tide of the morally injured? All measures were applied in the absence of risk/benefit analysis, despite common knowledge that blanket approaches to managing risk are likely to cause more damage than the presenting problem. Yet the whole population was terrified into believing we were all at equal risk of severe illness or death from a lethal virus, to which we had no natural immunity and was quietly spread from those with no symptoms, especially children. Lockdowns, school closures, testing, mask wearing, social distancing, mass vaccination programmes and subsequent passports were said to be necessary but in reality were unjustified and immoral. Dismissing the question of the necessity and morality of these measures and normalising moral injury as a natural consequence of a warlike situation places accountability solely on those who enforced the polices and vindicates those who created them.
A morally injured workforce is evidence that the response to Covid-19 was morally wrong. None of us know how we would have behaved in the shoes of the workers who enforced immoral policies that contravened their conscience and moral compass. However, we can be sure of one thing: many of the injured will need support to come to terms with the realisation they have inadvertently played a part in injuring some of the very people they intended to protect.
The CDC’s information page on Covid-19 vaccines contains the following bullet points on “How mRNA COVID-19 vaccines work:”
First, mRNA COVID-19 vaccines are given in the upper arm muscle or upper thigh, depending on the age of who is getting vaccinated.
After vaccination, the mRNA will enter the muscle cells. Once inside, they use the cells’ machinery to produce a harmless piece of what is called the spike protein…. After the protein piece is made, our cells break down the mRNA and remove it, leaving the body as waste.
Or, in other words, as we have long been told, “it” – the mRNA – “stays in the arm.” And then, after having instructed the muscle cells to produce the spike, is disposed of.
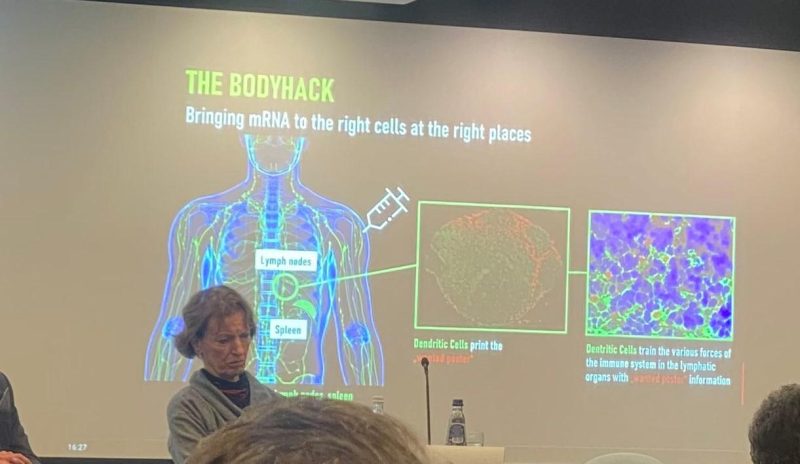
But look at the below picture from a recent presentation on mRNA vaccination at the European Parliament. The picture was posted on Twitter by Virginie Joron, a French member of the parliament. The speaker is no less an authority than Özlem Türeci, the Chief Medical Officer of BioNTech: the German biotech company that developed what has come to be known to most of the world as the “Pfizer” Covid-19 vaccine.
Have a closer look at Türeci’s slide, which tells a very different story than that which the CDC has been telling Americans for the last two years.
Far from “staying in the arm” and entering the muscle cells at the injection site, the injection site is only the point of departure for a journey that is supposed to take the mRNA rather to the lymph nodes. The subtitle of the slide is “Bringing mRNA to the right cells at the right places.” The deltoid is not the right place; the lymph nodes are.
Once in the lymph nodes, a specific sort of cell, the dendritic cells, is supposed to manufacture the spike protein: here colorfully described as the “wanted poster” that will help the immune system to identify the SARS-CoV-2 virus in case of subsequent exposure.
A passage from The Vaccine, the book that Türeci and her husband, BioNTech CEO Ugur Sahin, wrote which journalist Joe Miller, explains why BioNTech’s platform specifically targets the lymph nodes:
What Ugur learnt was that the location to which a vaccine delivers its ‘wanted poster’ really mattered. The reason for this, the couple’s team in Mainz later realised, was that not all dendritic cells … were created equal. The ones that resided in lymph nodes – of which the spleen is the largest – were particularly adept at capturing mRNA and making sure the instructions it carried were acted upon. These kidney-bean shaped organs, found under our armpits, in our groins, and at several other outposts in the body, are the information hubs of the immune system. (p. 98)
Indeed, Sahin and Türeci were so determined to get their mRNA into the lymph nodes that they had an earlier mRNA construct injected directly into the patient’s lymph nodesin the groin (p. 104).
Needless to say, such an approach was not likely to obtain wide acceptance as a vaccine! This is why the couple, as explained in their book, needed to package the mRNA in lipid nanoparticles, in order to ensure that mRNA administered by way of an intramuscular injection would, nonetheless, be widely distributed around the body and thus reach the lymph nodes.
This is to say that the wide biodistribution of the mRNA that came to light after rollout was never a bug. It is a feature of BioNTech’s mRNA technology. Having elicited an immune response by way of injection into the groin, Sahin is even said to have wondered, “How substantial could the immune response be if a vaccine got into all lymphatic tissues around the body, and recruited all the resident DCs [dendritic cells] into action?” (p. 105)
So, why has the CDC been lying about this for the last two years and insisting that the mRNA “stays in the arm?” Well, the obvious answer is that the idea of the mRNA staying at the injection site is reassuring, since otherwise we could fear systemic adverse effects of precisely the sort that have emerged since rollout.
It is worth noting, moreover, that in developing its vaccine, as discussed in my earlier article here, BioNTech simply skipped the so-called safety pharmacology studies whose purpose is precisely to test a candidate vaccine for potential systemic adverse effects – and regulators, including the FDA, let the company do it.
Robert Kogon is a pen name for a widely-published financial journalist, a translator, and researcher working in Europe.Follow him at Twitter here. He writes at edv1694.substack.com.
Austrian physician: vaccine has to be avoided, especially when “a corrupt state and an even more corrupt medical association, made up of puppets of the pharmaceutical industry, coerce people into a potentially lethal vaccination.”
Physician Dr. Andreas Sönnichsen was accused in 2022 of issuing digital exemption certificates for the Covid 19 vaccine for 20 euros to patients who did not want the new controversial medical mRNA technology injected into their bodies.
Despite the privacy rights between patient and doctor, Austrian authorities dragged Sönnichsen to a Salzburg court on charges of fraud and usurpation of authority.
Yesterday, the Salzburg court ruled in favor of Sönnichsen. The acquittal is viewed as a major victory by proponents of patient-physician rights, medical privacy and bodily autonomy.
Compulsory vaccination was introduced in Austria in February, 2022, but was suspended already in March before being dropped altogether in the summer after heated protests.
The courageous Sönnichsen was an outspoken critic of the Austrian government’s harsh COVID measures and used scientific arguments to refute the charges against him.
“Sönnichsen pleaded his innocence in the trial. The judge could not recognize a subjective factual element or an intent to enrich,” Der Standard reports. Prosecutors claimed the doctor’s certificates “were issued via the Internet without the patients having been conscientiously examined”, but the defendant “argued that the certificates very much had a medical value”.
The court agreed and acquitted
“According to the judge, the physician had wanted to issue a medical certificate as a doctor to help people not to have to go vaccinate,” Der Standard reports. “After the acquittal, Sönnichsen strongly criticized the Covid policy in an interview with ORF Salzburg. Those who had not been vaccinated had been severely defamed and discriminated against.”
“Biggest medical scandal” and “a crime”
At the end of 2021 in a press conference, Sönnichsen called COVID 19 the “biggest medical scandal of all time”, and at a press conference in Salzburg in November 2021, he warned that the risk-benefit ratio of vaccination against Corona was “highly likely to be negative for most healthy people and especially for children.”
In an open letter to the Salzburg Medical Association at the end of October 2022, Sönnichsen called the Covid vaccination of healthy people “a crime because the harm is much greater than the benefit”.
“Puppets of the pharmaceutical industry”
And now that the overwhelming evidence for the harmfulness of vaccination has come to light, Sönnichsen says the Hippocratic Oath “obliges” him to issue vaccination exemption certificates, especially “when a corrupt state and an even more corrupt medical association, made up of puppets of the pharmaceutical industry, coerce people into a potentially lethal vaccination.”
The Centers for Disease Control and Prevention (CDC) on Thursday added COVID-19 vaccination to its routine immunization schedule for children and adults.
Although the CDC does not have the authority to set requirements itself, the agency’s immunization schedule provides formal guidance for state and local public health officials who set the rules for which vaccines are required to attend school.
The schedule also is the basis for vaccine recommendations made by most physicians.
“Given all that we have learned about the dangers and ineffectiveness of COVID-19 shots over the last two years, it is horrifying to see the CDC now recommend this as a routine shot to children,” Mary Holland, Children’s Health Defense (CHD) president and general counsel told The Defender.
“Although it is unsurprising given the agency capture, it is nonetheless tragic,” she added.
Under the new guidelines, the CDC recommends healthy children 6 months to 11 years old receive a primary series of two doses of the mRNA Moderna or Pfizer-BioNTech monovalent COVID-19 vaccine, followed by a booster of the bivalent shot.
It recommends that healthy people age 12 and older receive two doses of either the Moderna, Pfizer or Novavax vaccine followed by a bivalent booster.
All COVID-19 vaccines being administered in the U.S. to people under 18 are Emergency Use Authorized (EUA) products. The U.S. Food and Drug Administration (FDA) did grant full approval to Pfizer’s Comirnaty COVID-19 vaccine for ages 12 and older, however, the Comirnaty vaccine is not available in the U.S. — which means all children who get the Pfizer vaccine are getting an EUA product.
In Wednesday’s congressional hearing on the Biden administration’s response to COVID-19, Rep. Dan Crenshaw (R-Texas) asked CDC Director Dr. Rochelle Walensky, why the CDC broke with its own norms and put an EUA vaccine on the childhood immunization schedule for a disease that poses very little risk to children and for which the vaccine poses many potential side effects without preventing transmission.
Walensky responded:
“The reason that the ACIP [Advisory Committee on Immunization Practices] recommended the CDC put the COVID-19 vaccine on the pediatric schedule was only because it was the only way it could be covered in our ‘Vaccines for Children’ program.
“It was the only way that our under-uninsured children would be able to have access to the vaccines … That was the reason to put it there.”
Data collected by the CDC through its Vaccine Adverse Event Reporting System (VAERS) and a growing number of other sources indicate serious health risks associated with COVID-19 vaccination for children.
“The COVID vaccines have not been shown to be either effective or safe for children,” CHD argued in an amicus brief filed in Louisiana last year. “The benefits to children are minuscule, while the risks — including the risk of potentially fatal heart damage — are ‘known’ and ‘serious,’ as the FDA itself has acknowledged.”
Other changes to the childhood schedule include adding the PVC15 shot, a pneumococcal conjugate vaccine used to help protect against pneumococcal bacteria and only recently approved for children; updated guidance for the flu and hepatitis B vaccines; and new recommendations for the measles, mumps and rubella (MMR) and polio vaccines.
The CDC now recommends an additional dose of the MMR vaccine in places where there is a mumps outbreak. It also recommends an additional poliovirus vaccine for children and adults if new polio cases emerge.
This would mean the childhood vaccination schedule would increase the number of recommended injections from 54 to 72 over the course of a person’s childhood, between the ages of 6 months and 18 years, The Defender reported last year.
CDC schedule protects pharmaceutical companies from liability for vaccine injuries
Vaccine makers are not liable for injuries or deaths associated with EUA vaccines but can be held liable for injuries caused by a fully licensed vaccine — unless that vaccine is added to the CDC’s childhood vaccination schedule.
Parents of children injured by vaccines listed on the childhood schedule can seek compensation through the taxpayer-funded National Vaccine Injury Compensation Program (NVICP), a no-fault alternative to the traditional legal system for resolving vaccine injury claims.
However, the revisions voted on by the ACIP committee last year explicitly state (slide 24) that the pneumococcal polysaccharide vaccine (PPSV23) and COVID-19 vaccines are not covered under the NVICP.
Instead, the COVID-19 vaccines added to the childhood schedule will remain covered by the Countermeasures Injury Compensation Program (CICP). To date, only 19 claims related to COVID-19 filed with the CICP have been found eligible for compensation, though no compensation has yet been paid.
Since it was established in 2010, the CICP only compensated 30 of the nearly 12,000 claims filed.
Are we seeing ‘the beginning of the end of Big Pharma’s reign’?
The addition of the COVID-19 vaccine to the immunization schedule “helps ‘normalize’ this vaccine and sends a powerful message to both healthcare providers and the general public that everyone ages 6 months and older should stay up to date with recommended COVID-19 vaccines (including a booster, when eligible), just as they would with any other routinely recommended vaccine,” Dr. Neil Murthy and Dr. A. Patricia Wodi said in a statement reported by CNN.
This “normalization” comes at a time when over 85% of the U.S. population hasn’t been boosted, despite the massive government-sponsored media push.
Nationally, only 12% of children ages 6 months to 4 years have received one dose of the vaccine. Only 58% of children ages 12 to 17 and 32% of children ages 5 to 11 have received two doses of the vaccine. Numbers vary widely across states.
Holland commented on the implications of adding this shot to the schedule:
“The childhood schedule is already unscientific and unjustifiable. Adding this shot may well be the straw that breaks the camel’s back. Parents are likely to resist, finally calling the entire childhood vaccine schedule into question.
“That day has been long in coming, but it is now here. I believe we are now watching the beginning of the end of Big Pharma’s reign over the nation’s children.”
At Wednesday’s congressional hearing, lawmakers repeatedly raised concerns about how regulatory agencies’ flawed recommendations led to a lack of confidence in public institutions.
Rep. Cathy McMorris Rodgers (R-Wash.) said, “There’s serious distrust today with our public health agencies. [Polling indicates] 40% of the public does not trust our public health agencies to handle the next public health emergency.”
Walensky indicated that vaccination rates for all vaccines on the childhood schedule among kindergarten children declined last year, dropping from 95% to 93% over the last two years, amounting to hundreds of thousands of parents opting not to comply with the childhood vaccination schedule.
VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S. While reports submitted to VAERS require further investigation before a causal relationship can be confirmed, VAERS historically has been shown to report only 1% of actual vaccine adverse events.
According to Retsef Levi, Ph.D., with the Massachusetts Institute of Technology, the vaccines “cause unprecedented levels of harm, including the death of young people and children.”
Multiple studies have determined that the vaccines increase the risk of myocarditis and pericarditis, particularly in young men.
An October 2022 study revealed the CDC was aware of the safety signal for these side effects months before it informed the public.
At the recent FDA vaccine advisory committee meeting, several committee members also raised concerns about recommending annual bivalent boosters for children given the lack of data.
Dr. Archana Chatterjee, Ph.D., committee member and dean of the Chicago Medical School and vice president for medical affairs at Rosalind Franklin University said:
“As we look at this question [simplifying the vaccination schedule] for young children, the data is just too few for us to really make scientifically sound decisions regarding this question. The trial data need to be much more robust than we have seen in the past.”
In light of data like this, vaccination for COVID-19 for children and healthy people is losing public and even governmental support in some places.
Under public pressure and facing a series of lawsuits, last week California dropped its plan to mandate COVID-19 vaccination for school children.
As of Feb. 6, 21 states have legislation or executive orders banning student vaccine mandates, according to the National Academy for State Health Policy, a nonpartisan organization of state health policymakers.
Only the District of Columbia currently has a vaccine mandate for school children, although it is not set to go into effect until the 2023-2024 school year.
Denmark ended its universal COVID-19 vaccination campaign for healthy individuals in February 2022.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
The State of Maryland has introduced a bill for consideration (Senate Bill 378) that would allow healthcare workers to vaccinate a child who is deemed “able to understand the benefits and potential consequences of getting vaccinated” without parental consent. The determined age of consent for a child to “choose” to be vaccinated is 14, though, such laws are often a slippery slope as guidelines and goalposts can be adjusted once a bill is passed to include even younger people.
It should be noted that Maryland law prevents children of 14 or older to refuse vaccination ordered by parents. In other words, they are considered competent enough to get vaccinated without parent’s knowledge, but not competent enough to refuse vaccination with parent’s knowledge. The push among some states to provide or legalize medical procedures on minors without advising parents has been growing in multiple sectors of healthcare the past few years, from abortions to gender affirmation surgeries.
It sounds like a remnant from two years ago when Democrat run states like New York were talking seriously about the forced internment of people who were “potential dangers” to public health. The concept of constitutional rights were going out the window and the US barely dodged an Orwellian end. Parental rights are often considered a vital barrier to state interference with vulnerable children who are easily manipulated into accepting procedures that could affect their rest of their lives.
The potential consequences are obvious – Schools and other government institutions could very easily exploit medical personnel to convince children that they MUST submit to vaccination. They could also influence minors to believe it was “all their idea.” The same scenario could involve overzealous doctors or nurses in a hospital setting. With the informed parental shield removed, the sky is the limit in terms of what the state can do to the younger generation.
Though the bill mentions that decisions by minors be made “without coercion”, a child may not be able to identify coercion when it happens. Not all manipulation requires open and obvious threats.
Democratic State Sen. Cheryl Kagan introduced Bill 378 on Wednesday. The bill is set to go before a hearing in the Senate Finance Committee on Feb. 22. The language is broad and seems to include all possible vaccinations rather than a set list.
Even in the case of a child voluntarily asking for medical treatments without deception, it is the job of parents to sometimes protect their kids from themselves. Without developed critical thinking skills minors require guidance to avoid rash decisions. When pressure is coming from officials with perceived authority, children are less likely to say no. The Maryland bill ignores these factors and opens the door to a wide range of abuses.
In his State of the Union address on Tuesday night, President Biden rewrote the history of the pandemic. Biden lamented, “Covid had shut down our businesses. Schools were closed. We were robbed of so much.” But it wasn’t Covid that issued the shutdown edicts.
We were robbed by politicians like Biden who disrupted lives in a futile effort to thwart a virus that infected hundreds of millions of Americans anyhow. There was never solid evidence to justify shutting businesses or schools but that did not deter politicians from promising to save humanity by destroying freedom.
After Pfizer and Moderna, Biden was perhaps the biggest Covid profiteer in America. In 2020, Biden ran one of the most fear-based presidential campaigns in modern history. Biden talked as if every American family had lost a member or two from this pestilence. He routinely exaggerated Covid death tolls by a hundred- or a thousand-fold, publicly asserting that millions of Americans had been killed by Covid-19. Biden was helped mightily by fear-mongering media coverage.
A Brookings Institute analysis noted, “Democrats are much more likely than Republicans to overestimate [Covid] harm. Forty-one percent of Democrats… answered that half or more of those infected by COVID-19 need to be hospitalized.” At that time, the rate of hospitalization was between 1 percent and 5 percent – so those Democratic voters overestimated the risk of hospitalization by up to 20-fold.
In the final debate between the presidential candidates in October 2020, Biden blamed Trump for every Covid fatality: “220,000 Americans dead…. Anyone who’s responsible for that many deaths should not remain as president of the United States.” Biden promised, “I will take care of this. I will end this. I’m going to shut down the virus, not the country.” In a speech on the day before Election Day, he declared, “We’re going to beat this virus. We’re going to get it under control, I promise you.” Biden won the presidency as a result of only 43,000 votes in three swing states. The disruption and damage caused by lockdowns were invoked as proof of Trump’s negligence, rather than seen as evidence of an unprecedented political panic-mongering and repression.
After taking office, Biden issued a flurry of edicts, including mandating masks for anyone on federal property. In September 2021, he mandated that more than 100 million be injected with Covid vaccines, despite proliferating evidence that the vaccines were failing to prevent transmission or infections. In an October 2021 CNN Town Hall, Biden vilified vaccine skeptics as murderers who only wanted “the freedom to kill you” with Covid.
On Tuesday night, Biden announced, “Covid no longer controls our lives.” But Biden extended the official Covid emergency at least until May 11, entitling him to sweeping additional power. Biden still claims that Covid miraculously entitles him to “forgive” half a trillion dollars in federal student debt. And the Biden administration is fighting to perpetuate vaccine mandates on foreign visitors to America and to preserve the president’s prerogative to impose mask mandates.
The carnage from Covid crackdowns is still being tabulated. A 2022 Johns Hopkins University analysis of 24 studies on the impact of lockdowns in the United States and Europe found “no evidence that lockdowns, school closures, border closures, and limiting gatherings have had a noticeable effect on COVID-19 mortality.” The pointless shutdowns did far more damage than Biden will ever admit:
A National Bureau of Economic Research analysis estimated that young Americans suffered “171,000 excess non-Covid deaths during 2020 and 2021… a historic, yet largely unacknowledged, health emergency.” Many of those fatalities were “collateral damage” from shutdowns and other Covid policies.
Millions of jobs were lost thanks to lockdowns, a major reason why life expectancy in the United States had its sharpest plunge since World War Two.
Forced isolation was a Grim Reaper. Deaths from drug overdoses set an all-time record of 108,000 in 2021 and alcohol-related deaths jumped 25% in the first year of the pandemic.
The Biden administration suppressed free speech on Twitter and other social media based on a single theme: “Be very afraid of Covid and do exactly what we say to stay safe,” as journalist David Zweig summarized in the TwitterFiles. Official fear-mongering helped boost the percentage of Americans reporting struggling with depression or anxiety by more than 300 percent.
If Biden can shift blame for disastrous Covid policies, politicians will be more likely to pointlessly lock down the nation in the future. Americans deserve to see all the federal records and all the state government records to expose the recklessness and deceit that permeated Covid policies. America will not recover from the pandemic until all the COVID lies and abuses by officialdom have been exposed.
James Bovard, 2023 Brownstone Fellow, is author and lecturer whose commentary targets examples of waste, failures, corruption, cronyism and abuses of power in government. He is a USA Today columnist and is a frequent contributor to The Hill. He is the author of ten books.
Former Twitter executives looked at times uncomfortable, but betrayed their staunch anti-free speech biases during a House Oversight Committee heading on Wednesday.
The hearing was called to investigate the role government played, specifically the FBI, with regards to censorship of the Hunter Biden laptop report by the New York Post.
Former Twitter Chief Legal Officer Vijaya Gadde, Former Deputy General Counsel James Baker, and Former Global Head of Trust & Safety Yoel Roth were grilled by Representatives, with Congressman Clay Higgins telling them they could be arrested for interfering with the 2020 presidential election.
“The bottom line is that the FBI had the Biden Crime Family laptop for a year. They knew it was leaking. They knew it would hurt the Biden family. So the FBI used its relationship with Twitter to suppress criminal evidence from being revealed about Joe Biden one month before the 2020 election,” Higgins asserted.
“You, ladies and gentlemen interfered with the United States of America 2020 presidential election! Knowingly and willingly!” he continued, adding “That’s the bad news! It’s gonna get worse! Because this is the investigation part! Later comes the arrest part, your attorneys are familiar with that.”
“I’d like to spend five hours with these ladies and gentlemen doing depositions surely yet to come,” the Congressman added.
Elsewhere during the hearing, Rep. Nancy Mace blasted the former executives for also, as highlighted by the Elon Musk’s release of The Twitter Files, working to suppress information regarding COVID.
“I along with many Americans have long term effects from COVID. Not only was I a long-hauler, but I have effects from the vaccine,” Mae declared.
She continued, “It wasn’t the first shot but it was the second shot. I have now developed asthma that has never gone away since I had the second shot. I have tremors in my left hand. And I have the occasional heart pains that no doctor can explain. And I’ve had a battery of tests.”
“I find it extremely alarming Twitter’s suppression spread into medical fields,” Mace told the former execs.
“You’re not a doctor, right?” Mace directly asked Gadde, adding “What makes you think you or anyone else at Twitter have the medical expertise to censor actual, accurate CDC data?”
Gadded pathetically claimed she was not familiar with these particular situations.”
“Yeah, I’m sure you’re not,” Mace shot back.
Republican Ohio Rep. Jim Jordan told them they “got played by the FBI” over the Hunter Biden laptop, forcing Roth to admit that the New York Post report didn’t violate any Twitter policies in his opinion, but was censored anyway.
“This to me is the real takeaway,” Jordan said, going on to state “51 former intelligence officials, five days after you guys take down the Hunter Biden story and block the New York Post’s account, five days later, 51 former intel officials send a letter and they say, ‘the Hunter Biden story has all the classic earmarks of a Russian information operation.’ The information operation was run on you guys, and then by extension then run on the American people. And that’s the concern.”
Republican Rep. Lauren Boebert asked the former Twitter executives “Who the hell do you think you are?” for shadow banning people they disagree with on the platform.
Boebert also asked the execs if they had shadow banned her own account.
“I can reach out to Elon and to his staff, and I can see what’s happened ,and I can sit here today and hold you all in account,” Boebert concluded, adding “I am angry for the millions of Americans who were silenced because of your decisions, because of your actions, because of your collusion with the federal government. They can’t reach out to Elon. They can’t sit here today and hold you in account.”
The chair of the Committee, Rep. James Comer of Kentucky highlighted Tweets made by Roth in the past calling Republicans ‘Nazis’.
Republican Rep. Marjorie Taylor Greene of Georgia told Roth “You permanently banned my Twitter account but you allowed child porn all over Twitter.”
The former execs mostly either claimed ignorance and denied any wrong doing.
James Baker said he can’t recall speaking with the FBI while working at Twitter, and denied that he acted unlawfully.
Meanwhile, Roth attempted to argue that censorship on Twitter under his watch helped to create more freedom of speech.
Roth also admitted that he finds it “regrettable” that the conservative account LibsOfTikTok is still allowed to be active on Twitter… More videos
‘Just an ear infection, here’s some antibiotics,’ was my hospital diagnosis after a five-minute assessment; strange, as I couldn’t understand how an ear infection could make my eye swell and deliver an excruciating head pain akin to being hit with a hammer four days earlier.
I had an Oxford University/AstraZeneca Covid-19 vaccine on March 28, 2021. I was 54. The government said it would enable people to get back to some kind of normality, both family and work (I was in the clothing industry). It was implied that it was our duty to protect those around us by being vaccinated. Thirdly, I was the carer for my frail 87-year-old father, living alone since my mother’s death in 2006.
The ‘ear infection’ pain got worse, the symptoms debilitating, I thought at one point I was going to die. I’m not a moaner but I just wasn’t comfortable with what I was told, and so began my road-blocked journey to VITT (vaccine-induced immune thrombocytopenia and thrombosis) diagnosis.
Once a diagnosis is given, it is nigh on impossible to get it changed, and for three months after I was told I had an ear infection I went back and forth to my GP, writing letters explaining my symptoms, asking for neurological referral, all to no avail.
I was eventually granted eye and blood tests. The eye test result recommended neurological assessment, but the killer was being handed my blood test results without explanation, just some notations stating ‘Abnormal see Doctor’.
Now very worried, I decided to see a private neurologist. I hadn’t even sat down before the neurologist, sizing me up in an instant, said ‘Something’s not right’ and suddenly I was an NHS emergency.
NHS MRI/CT scans and blood tests followed and then silence. All the adrenaline ebbs away and one gets back to life . . . until that moment when the phone rings, you see the word HOSPITAL on the display, and your pulse starts racing. It’s that call, and the calm voice you are hearing is telling you there’s a blood clot in your brain.
I didn’t take it in, I started shaking. I asked the neurologist (who is wonderful) to slow down as I couldn’t understand any of it.
A few days later I’m talking to a haematologist, again a wonderful person, and with pills and blood tests under way I had gathered myself and was able to ask questions.
I later wrote to my hospital and GP telling them of my diagnosis. I’ve got the ‘Sorry about that’ letters, the ‘we learned a lot/the MHRA didn’t tell us’ etc reasons. And I still have the blood clot I first told them I thought I had as a consequence of my vaccine.
Today, I feel if I’d been admitted on first presentation I’d have recovered. Instead, my NHS-diagnosed VITT blood clot and head pain are a constant reminder, my walking stick an embarrassment, and all the rest: my drooping eye, the vision fluctuation, the increased cranium pressure and broken teeth from my falls, the loss of my driving licence, PTSD, the lumbar puncture, blood thinners and the other procedures/appointments I now have after taking a ‘safe and effective’ vaccine – I can’t even work any more.
The impact has been just as bad for my father. I was pretty much his only link with the outside world, but because of my injury and all that goes with it (not being able to drive, for example) I can’t provide care for him. His health and well-being have suffered greatly. Now he has full-time live-in care, which he has to pay for, and has been in and out of hospitals since.
It’s all dreadfully sad. I have apologised to him and my family for my taking the vaccine. I wish I could turn the clock back and be a normal husband, dad and son again, but all that’s been ripped away from me. Everyone in a family suffers when it’s a vaccine injury, not just the vaccinated.
If you are vaccine injured, or know someone who is, you can contact or read about the the Covid-19 vaccine injury support group, UK CV Family, here.
Many papers in the medical literature seem to pit a consequence such as myocarditis or stroke as either occurring as a consequence of COVID-19 illness compared with COVID-19 vaccination. Because the denominator is so large for acutely ill hospitalized patients with COVID-19 especially during the first two years of the pandemic allowing ICD code capture of comorbidities, authors erroneously conclude the illness is “more dangerous” or a “bigger risk factor.” These arguments are daft in my opinion since COVID-19 respiratory illness is treatable and a recent paper from Klaassen et al has estimated 94% are already recovered from COVID-19—so it is water under the bridge. Not true for COVID-19 vaccines which are still mandated by some ill-advised schools, employers, and agencies. One way of looking for what is a more pressing and continued problem is to survey the medical literature.
Martinez-Reviejo et al completed a literature review of varicella-zoster reactivation (shingles) and compared cases arising after vaccination and those with the respiratory infection. There were more manuscripts and cases after vaccination. However, the manifestations of varicella-zoster were more severe in those with acute COVID-19 illness which was also high in disease severity.
Martinez-Reviejo R, Tejada S, Adebanjo GAR, Chello C, Machado MC, Parisella FR, Campins M, Tammaro A, Rello J. Varicella-Zoster virus reactivation following severe acute respiratory syndrome coronavirus 2 vaccination or infection: New insights. Eur J Intern Med. 2022 Oct;104:73-79. doi: 10.1016/j.ejim.2022.07.022. Epub 2022 Aug 1. PMID: 35931613; PMCID: PMC9340059.
I found it curious the authors did not disclose the shingles vaccine status in the tables. The bottom line is that shingles can occur with severe COVID-19 and it is treatable. Acute COVID-19, however is amenable to early therapeutics so severe cases can be avoided and most of us have recovered SARS-CoV-2 infection. COVID-19 vaccination continues to be an ongoing threat for varicella-zoster reactivation syndromes, some of which are very serious including ocular damage and long-lasting painful cutaneous syndromes.
Updated boosters and annual Covid shots mirroring session flu shots are the orders coming out of the recent FDA VRBPAC meeting. What data is supporting these ideas? Was this the plan all along? The HighWire gives their analysis.
One dose of Pfizer, just one! Within 30 minutes, while I was still driving home, I had a sudden feeling of the worst flu. My throat, eyes, lips and neck swelled to double their size and I couldn’t breathe. Within an hour welts appeared on my legs, arms, chest and even in my hair. I was taken by ambulance to A&E and given an epi-pen. Twenty-four months on and I have a formal diagnosis of chronic angioedema and urticaria. I’m no better, every day my lips and face swell. I have drooping eyelids, blurred vision, tremors, uninvestigated and untreated spikes in heart rate for no reason, and protruding veins all over my body. Then there is the horrendous tinnitus and 60 per cent loss in hearing. Sinus problems (lesions in the nasal cavity), pain at the back of the head, stomach pain and an intolerance to more than 200 foods. I can’t go out in sunshine because it literally burns the scalp and skin. This is now my life.
The doctors’ advice is to have the second jab! I don’t think so. It was 18 months and 21 visits to A&E before my GP surgery finally got to see me face to face, and then declared that I was too much of a specialist case for them to treat.
I am no anti-vaxxer. I had the jab in good faith thinking that it would mean life returning to normal, to see my children and grandchildren. The lack of medical care and investigation on any symptoms other than the urticaria and angioedema is both criminal and despicable along with their constant texts and letters telling me to get a second dose.
It’s an emotional journey and a very visual one. I have lost all confidence in socialising; the constant swelling has meant my skin has aged ten years in 24 months. I can no longer see well enough to drive, and that is a loss of independence.
The UK CV Family group https://www.ukcvfamily.org/ is a lifeline for me. I can’t thank the creators of the group enough for giving me the simple realisation I am not alone. Daily we see new members. I welcome them with the same message: welcome and so sorry you have to be here.
Other than a few dead-end doom addicts on social media, most people agree that the COVID-19 pandemic is over. SARS-CoV-2 has entered a stage of endemicity, similar to that of common cold coronaviruses, where there will be sporadic, seasonal outbreaks of cold and flu-like illness as immunity wanes in recovered and vaccinated individuals.
The pandemic was a worldwide disaster, claiming the lives of millions of people. It wasn’t a war against an enemy, as the virus didn’t surrender or sign any peace agreements. SARS-CoV-2 was contained by population immunity, just as similar pandemic viruses have been in the past.
The origin of the virus is still in dispute. Some virologists have tried to shut down any debate while pushing a zoonotic origin as the only possibility. However, a lab leak is no longer a wild theory, it’s a plausible explanation based on evidence from a variety of independentsources.
Yet there was another parallel disaster that was certainly man-made, and that was the US pandemic response. Panicked health officials and politicians failed to implement measures that would protect those most vulnerable to severe COVID-19, including elderly in assisted living facilities, which comprised one-third of all COVID deaths. Instead, leaders insisted on harmful and unfocused measures such as shutdowns, school closures, and universal masking, with little evidence of their benefit.
Attention to other medical issues, such as cancer screenings and diagnosis and treatment of other diseases, as well as childhood vaccinations, all disappeared in a wave of COVID monomania. The consequences of this ill-advised singular focus will be with us for many years. It is of paramount importance that the mistakes that led to this man-made disaster are not repeated.
The governments of European countries have begun to conduct public inquiries into their COVID responses, including Norway, Sweden,The Netherlands, the United Kingdom, and Denmark. It is past time for the United States to join this list, and critical given the worldwide influence of the CDC, FDA, and NIH/NIAID.
Members of the US Congress are conducting such an inquiry, and their efforts require the help of physicians, scientists and public health policy experts to identify key policy decisions and provide a rationale for investigating those policies and the officials and government agencies that devised and implemented them, with the ultimate goal of meaningful reform.
With help from Brownstone Institute, the Norfolk Group was organized in May, 2022, with the goal of providing a blueprint containing key questions for a congressional inquiry into the public health aspects of the US response to the COVID-19 pandemic. The group consists of eight scientists, physicians and policy experts, and seven of us met in person in Norfolk, Connecticut over Memorial Day weekend. All eight members continued to meet virtually over the summer, fall, and winter as the document was written and continuously revised.
Because the group was comprised of individuals from diverse backgrounds, without oversight from any public or private institutions (including Brownstone), we chose to name ourselves The Norfolk Group, and publish our document independently on the website www.NorfolkGroup.org.
The eight members of the Norfolk Group are:
Jay Bhattacharya, MD, PhD; epidemiologist, health economist, and professor at Stanford University School of Medicine; founding fellow of the Academy of Science and Freedom.
Leslie Bienen, MFA, DVM; veterinarian, zoonotic disease researcher, and faculty member at Oregon Health & Science University-Portland State University School of Public Health (through December 31st 2022). She left in January 2023 to work in healthcare policy.
Ram Duriseti, MD, PhD; emergency room physician and computational engineer for medical decision making; associate professor at Stanford School of Medicine.
Tracy Beth Høeg, MD, PhD; physician and PhD epidemiologist in the Department of Epidemiology & Biostatistics, University of California-San Francisco, clinical researcher in healthcare policy and practicing Physical Medicine & Rehabilitation physician.
Martin Kulldorff, PhD, FDhc; epidemiologist and biostatistician; professor of medicine at Harvard University (on leave); founding fellow of the Academy of Science and Freedom.
Marty Makary, MD, MPH; surgeon and healthcare policy scientist; professor at Johns Hopkins University.
Margery Smelkinson, PhD; infectious disease scientist and microscopist whose research predominantly focuses on host/pathogen interactions.
Steven Templeton, PhD; immunologist; associate professor at Indiana University School of Medicine.
The document provides questions and supporting information regarding ten areas of the US pandemic response, including:
Protecting High Risk Americans
Infection Acquired Immunity
School Closures
Collateral Lockdown Harms
Public Health Data and Risk Communication
Epidemiologic Modeling
Therapeutics and Clinical Interventions
Vaccines
Testing and Contact Tracing
Masks
In preparing this document, we did not conduct any interviews or unearth any previously unseen documents. All the information contained in the document was and is publicly available, and we have provided links to each source throughout.
We have detailed evidence that was available at each time point during the pandemic, and have documented instances where the US health agencies, officials, and politicians ignored or suppressed discussion of that evidence. We ask questions that attempt to discover why key individuals failed to consider all aspects of public health instead of engaging in a damaging singular focus on community-wide suppression of an age-stratified and comorbidity-amplified infectious disease. Why was the uncertainty of evidence supporting the effectiveness of mitigation measures not acknowledged? How was pressure from pharmaceutical companies, teachers’ unions, and other special interests related to the abandonment of evidence-based policies? These questions broadly apply to all of the ten areas covered in our document, and together with specific questions and supporting data, resulted in eighty pages. This was no small effort, and I’m proud to have been a part of it.
Our document focuses solely on the public health-related aspects of the US pandemic response. Although the origin of SARS-CoV-2 may be in dispute, our document does not ask questions related to this active area of investigation. Separate committees have been and will be organized to address that issue. We have also avoided the topics of economic mismanagement and the role of media in creating or exacerbating pandemic response crises. A media-focused document was released in July, 2022, and an economics-related document was released in December.
Critics will no doubt reflexively label our document as a partisan effort funded with a secret pile of Koch money. Other than the initial efforts of Brownstone Institute to bring us together, there was no outside influence. Our website is self-funded. Understandably, many of our questions and supporting evidence could and likely will be used for partisan purposes, as one party will lead any COVID-19 response commission while the other may be reluctant to cooperate. It is our hope that despite this messy and partisan process, the truth will emerge, individuals will be held accountable, and an opportunity will emerge for serious reform of dysfunctional government agencies.
An inquiry into the US COVID-19 pandemic response cannot be avoided, and we are trailing other countries in efforts to identify mistakes, demand accountability, and propose solutions. It might be an ugly process, but it is a necessary one. We hope our document will move US leaders and policymakers toward the goal of ensuring that the mistakes of our pandemic response are never repeated.
Steve Templeton is a Senior Scholar at Brownstone Institute, is an Associate Professor of Microbiology and Immunology at Indiana University School of Medicine – Terre Haute. His research focuses on the immune response to the human opportunistic pathogens. He is currently writing a book on infectious diseases and pandemics.
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.





 Aletho News
Aletho News
{kind=link}