On February 14, 2022, Canadian Prime Minister Justin Trudeau invoked a sweeping nationwide measure, the kind of which hadn’t been used since his father, former Prime Minister Pierre Elliott Trudeau, during the October Crisis of 1970, amid a rash of terrorist incidents perpetrated by Francophone separatists in the province of Quebec.
The federal Emergencies Act, which replaced the War Measures Act used in 1970, as well as during both World Wars, is supposed to be used in cases of serious threat to national security or public welfare. So what was the threat that caused Trudeau to pull out the big guns? A convoy of truckers and their supporters — coined the Freedom Convoy — headed to Canada’s capital city of Ottawa to defend the notion of equal rights of all Canadians to work, assemble, enjoy indoor leisure activities, and travel regardless of anti-Covid vaccine status. The fact that these fundamental aspects of everyday life could no longer be taken for granted was a testament to how authoritarian the Canadian government had already become. And when Canadians finally decided to demonstrate that they were fed up, the Trudeau government’s response was an unprecedented crackdown that put Canada on par with countries that it in-turn criticizes.
“We are broadening the scope of Canada’s anti-money laundering and terrorist financing rules so that they cover crowdfunding platforms and the payment service providers they use. These changes cover all forms of transactions, including digital assets such as cryptocurrencies,” deputy prime minister and finance minister, Chrystia Freeland, said during the Emergency Act announcement. She also introduced an order “authorizing Canadian financial institutions to temporarily cease providing financial services where the institution suspects that an account is being used to further the illegal blockades and occupations. This order covers both personal and corporate accounts.”
It’s hard to imagine that the conflation of Freedom Convoy protesters and terrorism was just coincidental. Western governments use the tactic frequently. The European Union, for example, routinely evokes “Russia” and “ISIS” in the same breath when arguing for the need to control “disinformation” or “propaganda”. Putting two very different things in the same rhetorical basket served to associate them in people’s minds. So people end up thinking that these average Canadians are like terrorists, and then end up supporting the blocking of their bank accounts by government order.
During an inquiry into the use of the Emergency Act, whose results are expected to be made public just after the one year anniversary of the events, it emerged that a CEO of one of Canada’s banks encouraged Freeland to make this designation. “Label them as terrorists,” he said. “Seize the assets and impair them.” Apparently the government simply dutifully complied.
Trudeau ended up lifting the order nine days later on February 23, 2022, before it could be defeated in a challenge, but the damage was done. As a Canadian born and raised near Vancouver, my earliest memories of protests and strikes roughly date back to the same time that I learned to walk. The Freedom Convoy protests weren’t any different from others. Many public demonstrations are loud, and block traffic. I can’t even count the number of times that traffic was halted on a particular Vancouver area bridge and into the downtown core, all because of environmental protesters perched in old growth trees. The cops usually just end up charging them with mischief, but no one calls a national emergency over it.
Freeland has argued that the extraordinary measures were needed to protect Canada’s economic interests. “What was happening was profoundly jeopardizing the Canadian economy and putting investment in Canada at risk,” she told the inquiry. Sorry, not buying it. How many protests against Canadian oil and gas pipeline projects, which are clearly critical to Canada’s economic security, have lasted for months on end while the government just sat back and let the police do their jobs as they see fit?
As civil rights groups have pointed out, wielding the Emergencies Act was like using a jackhammer on a thumbtack. It failed to specify who in Canada could be targeted by it, and in theory could have been used against anyone or any cause. “By invoking the Emergencies Act, Cabinet gave itself power to enact wide-reaching orders without going through the ordinary democratic process. Using this Act, the federal government gave police increased authority to shut down peaceful protests, on any issue, right across Canada,” argued the Canadian Civil Liberties Association. And that’s without even getting into the merits of the cause.
At the same time, the Canadian government invested a billion dollars to help Canadian provinces set up an integrated digital passport system that linked health and jab records to a digital QR code, much like the European Union’s digital Covid certificate that determined who had received the number of jabs mandated by the government as a prerequisite for access to all the old basic freedoms of daily life. The more people were coerced into getting jabs so they could travel, keep their job, or work out in a gym, the more digital identities could be tied to digital QR codes.
While the mandates have since largely fallen away, that digital tracking infrastructure hasn’t. It is still firmly in place. As long as it persists, it will serve as a reminder of Canada’s authoritarian turn under a questionable but convenient sanitary pretext — and of the government overreach that the Freedom Convoy fought against.
Pfizer missed a deadline to turn over internal studies on myocarditis, per an FDA order. The deadline came and went. Now, they quietly have a new date in June. Why the delay on such important data? And, why does the FDA set arbitrary deadlines which aren’t enforced?
As Biden announces the coming end of the Covid Public Health Emergency in the US, the new majority in Congress appear to not be letting agencies off the hook. The past three years of remarkably poor public health policy have placed the CDC, WHO, and Social Media companies in the sights of numerous committee investigations, and new legislation seeking answers and medical freedom.
Airline pilot and co-founder of US Freedom Flyers, Josh Yoder, and Clinical Cardiologist, Dr. Thomas Levy, join Del to discuss the recent FAA change to the heart test limits and the coincidental timing of the change coming amid increasing concerns over myocarditis from the COVID-19 vaccine.
As far as I am concerned, here are the Covid numbers that matter most.
N = 40,000 – Estimated number of mainstream “journalists” in America.
N = 0 – Estimated number of these journalists who have published a major story questioning any of the authorized Covid narratives.*
Note: For the purposes of this article, I’m not counting journalists who work for, say, Fox News or The Epoch Times as “mainstream journalists.” If I did, the above number would not be 0 … but it would still be minuscule.
*At the end of this article, I list 29 elements of the “authorized Covid narrative.”
N = 100,000 – Estimated number of credentialed “scientists” in America. (Note: About 2,000 per state).
N = 95,000 – Estimated number of credentialed scientists in America who support all the Covid narratives.
N = 5,000 – Estimated number of contrarian scientists who do not support all the Covid narratives.
N = 0 – Number of scientists who support the Covid narrative who have been banned by social media.
N = 2,500 – Estimated number of contrarian scientists who do not support the narrative who have been banned by different social media platforms (50 percent).
N = 5,000 – Estimated number of active physicians who have publicly disagreed with key parts of the authorized Covid narrative. (About 100 physicians in each state).
N = 99.995 percent – Approximate percentage of active U.S. physicians who have been unwilling to speak out against any of the authorized Covid narratives. (Approximately 0.046 percent have been willing to speak out publicly against the authorized narrative).
N = 600 – Approximate number of U.S. Senators and Congressmen who have served in Congress since the official pandemic began.
N = 5 – Approximate number of members of Congress who have publicly and consistently challenged key aspects of the authorized Covid narrative. (0.083 percent of Congress – less than 1 percent).
N = 0 – Number of Covid tribunals or Commissions authorized by U.S. government to date.
N = 60 percent – Approximate number of federal politicians who would have to support such tribunals to create them.
N = 500 – Approximate number of Substack authors who routinely challenge elements of the authorized Covid narrative.
N = 5 million – Approximate number of regular readers of “Covid contrarian” Substack sites.
N = 300 – Approximate number of “mainstream” press organizations in America (about 250 large newspapers and about 50 national sites).
N = 250 million – Approximate number of Americans who get Covid stories from “mainstream” news sources.
N = 2,040 – Estimated number of coroner or medical examiner officials/offices in the U.S. in 2018.
N = 0 – Number of CEOs of Fortune 500 companies who publicly challenged elements of the authorized Covid narrative.
Expressed differently …
About 0-in-40,000 mainstream journalists and editors (not counting a few at Fox News or The Epoch Times) are willing to speak out against the official Covid narrative.
About 0-in-2,040 medical examiners/coroners are willing to speak out about possible vaccine deaths and injuries.
About 0-in-500 CEOs of Fortune 500 companies criticized elements of the official Covid narratives.
About 1-in-200 physicians have been willing to challenge the authorized Covid narratives.
About 1-in-120 elected members of Congress have been willing to challenge at least some elements of the authorized Covid narrative.
As a percentage …
Zero percent of “mainstream” journalists have challenged parts of the official Covid narrative.
Zero percent of CEOs at Fortune 500 companies challenged parts of the official Covid narrative.
Zero percent of coroners and medical examiners have raised any questions about an increase in all-cause deaths.
Fewer than 1 percent of the members of Congress have spoken out in a conspicuous and consistent manner.
Zero percent of Democratic politicians at the state or national level have spoken out against parts of the Covid narrative.
On the other hand …
Maybe 75 percent of “alternative media” or Substack journalists who write about Covid have challenged aspects of the authorized Covid narrative.
The Question …
Given the above estimates, what’s the probability something substantial or meaningful will be done to expose elements of the Covid narrative as false or even as “crimes against humanity?”
I would say the probability of this happening is very close to zero percent.
I would also argue that maybe 80 percent of Americans don’t care or want any of the possible Covid lies or frauds exposed as such.
However, I would argue that maybe 20 percent of Americans do care passionately about seeing “the truth” exposed, and would like to see the officials who are most guilty/responsible exposed and punished.
What all of the above tells me is …
What this thought exercise (or “by-the-numbers” presentation) shows is that Congress, elected officials, the mainstream press, corporate leaders and almost all physicians and scientists do not care at all about the views of approximately one-fifth of the country.
This also tells me that the only things that really matters are the views of the mainstream press and the politicians. Really, the only organizations that could hold substantive hearings or tribunals that would “have teeth” and make a difference (change narratives) are official elected office holders.
I’ve always assumed politicians DO or will respond to pressure from voters or the public … but the only pressure or media they pay attention to is the “mainstream” media reports … so the mainstream media does matter.
So far at least, the reporting and commentary of “the alternative” media – which is actually sane and still capable of critical thinking and is still willing to be skeptical of pronouncements of officials and experts … and which is growing in size – doesn’t matter.
Basically, a significant population cohort (20 percent, per my estimate) is being ignored by officials and the mainstream press, but is still fighting as hard as they can to bring attention to issues that the people and organizations “that matter” still don’t want to discuss or investigate.
In short, the dichotomy of views on “what’s important” – and what should change or be exposed regarding Covid topics – is nothing short of stunning.
“Our” side is definitely in the minority, but 20 percent of people is still a significant percentage of the population.
In a nutshell, the mainstream press, politicians, bureaucrats, corporate leaders, physicians, scientists, coroners, etc. hold views that are 180-degrees opposite the views of 20 percent of the country.
Re-stated: All the important people and organizations think nothing like myself and probably 99 percent of my readers … or the millions of readers who now visit Substack or “alternative media” sites every day.
All I can say is that all of this is… bizarre.
***
Defining the ‘Authorized Covid Narrative’ …
Above, I make many references to organizations or groups that supported all or most elements of the “authorized Covid narrative.” So what are the parts of the “authorized Covid narratives?”
Here’s a quick effort to define these elements. Most of these statements are still considered to be “settled science.” For what it’s worth, I would argue that every one of these ‘authorized” narratives is/was dead wrong.
N = 29 – Elements of the “authorized Covid narrative” (Partial list).
N = 0 – Groups or individuals cited above who challenged or disputed any of the following statements.
The Covid vaccines are “safe” – i.e. they don’t produce adverse reactions and/or have never led to any deaths. Anyone who died after a vaccine didn’t die from the vaccine.
The Covid vaccines are “effective” – they prevent infection and transmission.
Vaccines are superior to natural immunity at preventing infection and spread.
Alternative treatments like ivermectin or HCQ do not work and should not be allowed or prescribed by doctors. (C19 is not a “treatable” illness via existing medications).
Asymptomatic spread is a major cause of transmission. (People who don’t have symptoms are a major or important avenue of virus spread).
The virus can be spread from physical surfaces.
The virus can be easily spread outdoors.
Masks prevent the spread of the virus and prevent people from getting infected … and should thus be mandated.
C19 poses a serious mortality risk to everyone, including children and healthy people under the age of 60.
Testing of non-symptomatic people is an excellent way to prevent infections and spread and should either be mandatory or strongly encouraged by employers and officials.
Remdesivir saves lives and should be given to many people.
More than one million Americans have died “from” Covid.
There has NOT been an increase in “excess” mortality in America in the last two years. And if there has been, the cause of these deaths must be Covid – even after widespread administration of Covid vaccines, which are 95 percent effective at preventing severe cases and deaths.
There has been no increase in deaths of people 18 to 64.
There has been no increase in deaths from young people playing sports.
Lockdowns prevented cases and thus serious infections and deaths. Absent lockdowns, millions more people in the world would have died from Covid.
Closing schools saved countless lives. Ceasing routine medical procedures and diagnostic surgeries saved many lives. Cancelling church services saved many lives. Not allowing family members to visit their loved ones in the hospital or nursing home saved countless lives.
Closing non-essential businesses saved the economy by preventing countless Covid cases and deaths.
Lockdowns and business closings did not increase suicides, suicide attempts, drug overdoses, depression, alcohol abuse or domestic abuse …. or, if they did, dying from suicide or drug overdose is better than dying from Covid.
Trillions of dollars in Covid expenditures did not accelerate or cause inflation.
Censorship of “disinformation” has saved countless lives.
Cancelling sporting events, concerts, plays, family reunions and keeping people from traveling to see family saved countless lives.
The novel coronavirus did not begin to spread around the world until “latter January” 2020. There were zero cases of Covid in communities in America before January 2020.
Everyone who had Covid symptoms before mid-January 2020 had the flu or some other virus, but not Covid, because Covid was not spreading until February 2020.
Wide-spread use of ventilators were very important to saving lives. Officials saved countless lives by getting more ventilators in hospitals and doctors saved countless lives by making sure they put patients on ventilators.
Boosters save lives.
People who have been vaccinated or boosted get Covid far less often than people who do not.
If you have been vaccinated or boosted, your case of Covid will be less severe than people who have never received a shot.
The New York City Department of Health and Mental Hygiene set up a “Misinformation Response Unit” to monitor what it would determine to be “dangerous misinformation” posted on social media, non-US sites, and non-English media in the US.
This “misinformation” mostly had to do with Covid vaccination – the Department was determined to drive vaccination rates up by spreading its word, and in this gathered over 100 partners whose job was to craft positive messaging around the controversial subject.
Among those the dedicated new unit is working with is Public Good Projects, otherwise known for receiving funding from a lobbying group representing two major Covid vaccine manufacturers, Pfizer and Moderna.
Their “good” work here also included sending Twitter, on a weekly basis, lists of posts slated for censorship.
In an article published by the NEJM Catalystjournal, those behind the effort are now assessing the Unit’s work as successful, what with it being able to “rapidly identify messages” deemed as containing inaccurate information about the virus, vaccines, treatment, etc.
And although admitting that “vaccine hesitancy” remains high around the world even two years after the vaccines were first introduced – and this is something attributed to “disinformation and misinformation” and continues to worry the World Health Organization (WHO) and the US Surgeon General, as well as “medical experts” – the New York City Health Department thinks that it did well in getting its own narrative out, particularly in traditional media.
However, it needed help on the internet and so, in 2021, the NYC Health Commissioner penned a letter to the largest social networks asking them to engage in “broader efforts to curtail deliberate disinformation, particularly from the most notorious spreaders of disinformation and from non-English language sources.”
This is also where the Public Good Projects came in, to enlist social media “microinfluencers” to spread pro-vaccine messages, and train others to come up with campaigns.
The email Dave A. Chokshi, New York City health commissioner, addressed to then Twitter CEO Jack Dorsey and Facebook CEO Mark Zuckerberg, with the subject line reading, “Vaccine Misinformation,” urges the pair to “take immediate action to stop the spread of fraudulent and inaccurate information about COVID-19 vaccines” on their platforms.
Chokshi wanted this action to be “effective and vigorous” and asserted that misinformation on these sites, as understood by the city’s Health Department, was “costing New Yorkers their lives.”
Twitter and Facebook were then urged to do the following: “Consistently and promptly remove all misinformation regarding COVID-19 vaccines from your platforms and ban any user that repeatedly posts misinformation, including the Dirty Dozen; redesign the algorithms used by your platforms to avoid amplifying misinformation, particularly among non-English languages; provide greater transparency to your data to allow health departments to better identify, track and understand the spread of misinformation, and amplify messaging from trusted public health experts and local partners.”
The term ‘moral injury’ is a new one for me, as it probably is for most. It’s more commonly applied in a military context and only recently in health and social care, since 2020 to be precise. Indeed, the literature gently, knowingly or unknowingly, nudges us into believing that moral injury, reframed as occupational moral injury, isn’t a new concept but an inevitable consequence of working in an ethically challenging health and social care system.
Moral injury is understood as the damage done to an individual’s conscience or moral compass when they perpetrate, witness or fail to prevent acts that transgress their own moral beliefs, values or code of ethics. The term is thought to have originated after the Vietnam war when returning veterans and their carers struggled to make sense of high levels of anguish, anger and alienation that couldn’t be explained in terms of a mental health diagnosis such a post-traumatic stress disorder. It doesn’t take much stretch of the imagination to understand why veterans were morally injured but the Moral Injury Project at Syracuse University in New York cites examples such as using deadly force in combat and inadvertently causing harm or death to civilians and colleagues, giving orders which result in the injury or death of colleagues, failing to provide medical aid to civilians or colleagues and failing to report incidents such as sexual assaults.
When lockdowns were implemented in 2020, the health and social care workforce faced insurmountable and intolerable challenges when it was deemed unsafe in many situations to have close contact with fellow human beings who were in need of assistance. In essence, a workforce who function on the need for human contact could endanger life by simply doing their job. Subsequently, care and support was withdrawn or compromised through almost non-existent face-to-face interactions or time limited, with minimal physical contact if they took place at all.
Moral injury therefore makes sense in the context of health and social care. Staff were forced to deny medical and compassionate care to the injured and dying, leave adults and children in risky situations which in some cases led to death and injury, isolate frail older people from the life-giving company of family and friends and ignore or dismiss situations that previously justified urgent attention; all done while hiding smiles and humanity behind useless and potentially dangerous masks.
Moral injury during the pandemic can surely be applied across most professions and indeed the population: the police officer investigating a peaceful family gathering, the funeral director separating distressed relatives, the religious leader closing the door of a place of worship or the teacher who forced children to wear masks for hours on end. There were also the children who isolated their parents and parents who isolated their children, neighbours and community groups who withdrew essential help and support, and friends and family who got angry or fell out with those they disagreed with. Emotions and tensions ran high, leading me to think that many of us are morally injured to some degree or another. Is it any wonder that so many are struggling with poor mental health?
The growing number of articles drawing attention to moral injury, the most significant in the BMJ in July 2020 and a reference point for further articles, all focus on reassuring staff that a conflict of morals and the potential for injury is a normal consequence of doing what was necessary to prevent illness and death from Covid-19. At no point are the logic and morality of the rules called into question, which is surprising because the Moral Injury Project makes reference to two other potential causes of moral injury that are not referred to in recent literature:
‘Following orders that were illegal, immoral, and/or against the Rules of Engagement or Geneva Convention’;
‘A change in belief about the necessity or justification for war, during or after one’s service’.
As the realisation slowly dawns on the world that the inhumane actions which staff were forced to take were in fact unnecessary and based on flawed concepts with no robust evidence base, are we facing a rising tide of the morally injured? All measures were applied in the absence of risk/benefit analysis, despite common knowledge that blanket approaches to managing risk are likely to cause more damage than the presenting problem. Yet the whole population was terrified into believing we were all at equal risk of severe illness or death from a lethal virus, to which we had no natural immunity and was quietly spread from those with no symptoms, especially children. Lockdowns, school closures, testing, mask wearing, social distancing, mass vaccination programmes and subsequent passports were said to be necessary but in reality were unjustified and immoral. Dismissing the question of the necessity and morality of these measures and normalising moral injury as a natural consequence of a warlike situation places accountability solely on those who enforced the polices and vindicates those who created them.
A morally injured workforce is evidence that the response to Covid-19 was morally wrong. None of us know how we would have behaved in the shoes of the workers who enforced immoral policies that contravened their conscience and moral compass. However, we can be sure of one thing: many of the injured will need support to come to terms with the realisation they have inadvertently played a part in injuring some of the very people they intended to protect.
The CDC’s information page on Covid-19 vaccines contains the following bullet points on “How mRNA COVID-19 vaccines work:”
First, mRNA COVID-19 vaccines are given in the upper arm muscle or upper thigh, depending on the age of who is getting vaccinated.
After vaccination, the mRNA will enter the muscle cells. Once inside, they use the cells’ machinery to produce a harmless piece of what is called the spike protein…. After the protein piece is made, our cells break down the mRNA and remove it, leaving the body as waste.
Or, in other words, as we have long been told, “it” – the mRNA – “stays in the arm.” And then, after having instructed the muscle cells to produce the spike, is disposed of.
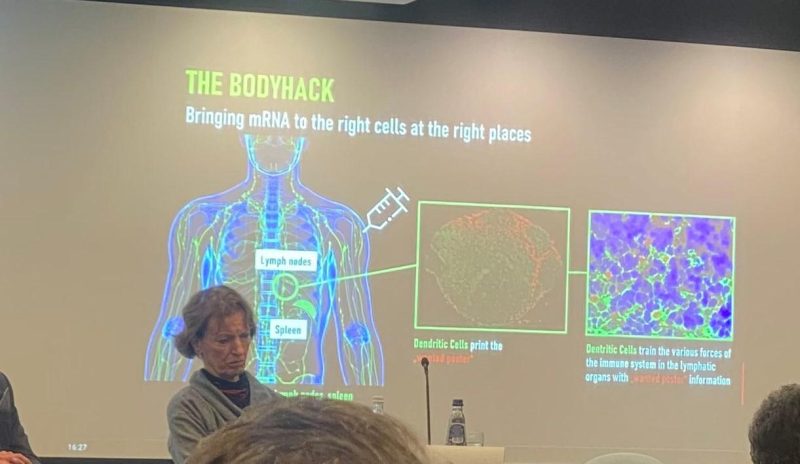
But look at the below picture from a recent presentation on mRNA vaccination at the European Parliament. The picture was posted on Twitter by Virginie Joron, a French member of the parliament. The speaker is no less an authority than Özlem Türeci, the Chief Medical Officer of BioNTech: the German biotech company that developed what has come to be known to most of the world as the “Pfizer” Covid-19 vaccine.
Have a closer look at Türeci’s slide, which tells a very different story than that which the CDC has been telling Americans for the last two years.
Far from “staying in the arm” and entering the muscle cells at the injection site, the injection site is only the point of departure for a journey that is supposed to take the mRNA rather to the lymph nodes. The subtitle of the slide is “Bringing mRNA to the right cells at the right places.” The deltoid is not the right place; the lymph nodes are.
Once in the lymph nodes, a specific sort of cell, the dendritic cells, is supposed to manufacture the spike protein: here colorfully described as the “wanted poster” that will help the immune system to identify the SARS-CoV-2 virus in case of subsequent exposure.
A passage from The Vaccine, the book that Türeci and her husband, BioNTech CEO Ugur Sahin, wrote which journalist Joe Miller, explains why BioNTech’s platform specifically targets the lymph nodes:
What Ugur learnt was that the location to which a vaccine delivers its ‘wanted poster’ really mattered. The reason for this, the couple’s team in Mainz later realised, was that not all dendritic cells … were created equal. The ones that resided in lymph nodes – of which the spleen is the largest – were particularly adept at capturing mRNA and making sure the instructions it carried were acted upon. These kidney-bean shaped organs, found under our armpits, in our groins, and at several other outposts in the body, are the information hubs of the immune system. (p. 98)
Indeed, Sahin and Türeci were so determined to get their mRNA into the lymph nodes that they had an earlier mRNA construct injected directly into the patient’s lymph nodesin the groin (p. 104).
Needless to say, such an approach was not likely to obtain wide acceptance as a vaccine! This is why the couple, as explained in their book, needed to package the mRNA in lipid nanoparticles, in order to ensure that mRNA administered by way of an intramuscular injection would, nonetheless, be widely distributed around the body and thus reach the lymph nodes.
This is to say that the wide biodistribution of the mRNA that came to light after rollout was never a bug. It is a feature of BioNTech’s mRNA technology. Having elicited an immune response by way of injection into the groin, Sahin is even said to have wondered, “How substantial could the immune response be if a vaccine got into all lymphatic tissues around the body, and recruited all the resident DCs [dendritic cells] into action?” (p. 105)
So, why has the CDC been lying about this for the last two years and insisting that the mRNA “stays in the arm?” Well, the obvious answer is that the idea of the mRNA staying at the injection site is reassuring, since otherwise we could fear systemic adverse effects of precisely the sort that have emerged since rollout.
It is worth noting, moreover, that in developing its vaccine, as discussed in my earlier article here, BioNTech simply skipped the so-called safety pharmacology studies whose purpose is precisely to test a candidate vaccine for potential systemic adverse effects – and regulators, including the FDA, let the company do it.
Robert Kogon is a pen name for a widely-published financial journalist, a translator, and researcher working in Europe.Follow him at Twitter here. He writes at edv1694.substack.com.
Austrian physician: vaccine has to be avoided, especially when “a corrupt state and an even more corrupt medical association, made up of puppets of the pharmaceutical industry, coerce people into a potentially lethal vaccination.”
Physician Dr. Andreas Sönnichsen was accused in 2022 of issuing digital exemption certificates for the Covid 19 vaccine for 20 euros to patients who did not want the new controversial medical mRNA technology injected into their bodies.
Despite the privacy rights between patient and doctor, Austrian authorities dragged Sönnichsen to a Salzburg court on charges of fraud and usurpation of authority.
Yesterday, the Salzburg court ruled in favor of Sönnichsen. The acquittal is viewed as a major victory by proponents of patient-physician rights, medical privacy and bodily autonomy.
Compulsory vaccination was introduced in Austria in February, 2022, but was suspended already in March before being dropped altogether in the summer after heated protests.
The courageous Sönnichsen was an outspoken critic of the Austrian government’s harsh COVID measures and used scientific arguments to refute the charges against him.
“Sönnichsen pleaded his innocence in the trial. The judge could not recognize a subjective factual element or an intent to enrich,” Der Standard reports. Prosecutors claimed the doctor’s certificates “were issued via the Internet without the patients having been conscientiously examined”, but the defendant “argued that the certificates very much had a medical value”.
The court agreed and acquitted
“According to the judge, the physician had wanted to issue a medical certificate as a doctor to help people not to have to go vaccinate,” Der Standard reports. “After the acquittal, Sönnichsen strongly criticized the Covid policy in an interview with ORF Salzburg. Those who had not been vaccinated had been severely defamed and discriminated against.”
“Biggest medical scandal” and “a crime”
At the end of 2021 in a press conference, Sönnichsen called COVID 19 the “biggest medical scandal of all time”, and at a press conference in Salzburg in November 2021, he warned that the risk-benefit ratio of vaccination against Corona was “highly likely to be negative for most healthy people and especially for children.”
In an open letter to the Salzburg Medical Association at the end of October 2022, Sönnichsen called the Covid vaccination of healthy people “a crime because the harm is much greater than the benefit”.
“Puppets of the pharmaceutical industry”
And now that the overwhelming evidence for the harmfulness of vaccination has come to light, Sönnichsen says the Hippocratic Oath “obliges” him to issue vaccination exemption certificates, especially “when a corrupt state and an even more corrupt medical association, made up of puppets of the pharmaceutical industry, coerce people into a potentially lethal vaccination.”
The Centers for Disease Control and Prevention (CDC) on Thursday added COVID-19 vaccination to its routine immunization schedule for children and adults.
Although the CDC does not have the authority to set requirements itself, the agency’s immunization schedule provides formal guidance for state and local public health officials who set the rules for which vaccines are required to attend school.
The schedule also is the basis for vaccine recommendations made by most physicians.
“Given all that we have learned about the dangers and ineffectiveness of COVID-19 shots over the last two years, it is horrifying to see the CDC now recommend this as a routine shot to children,” Mary Holland, Children’s Health Defense (CHD) president and general counsel told The Defender.
“Although it is unsurprising given the agency capture, it is nonetheless tragic,” she added.
Under the new guidelines, the CDC recommends healthy children 6 months to 11 years old receive a primary series of two doses of the mRNA Moderna or Pfizer-BioNTech monovalent COVID-19 vaccine, followed by a booster of the bivalent shot.
It recommends that healthy people age 12 and older receive two doses of either the Moderna, Pfizer or Novavax vaccine followed by a bivalent booster.
All COVID-19 vaccines being administered in the U.S. to people under 18 are Emergency Use Authorized (EUA) products. The U.S. Food and Drug Administration (FDA) did grant full approval to Pfizer’s Comirnaty COVID-19 vaccine for ages 12 and older, however, the Comirnaty vaccine is not available in the U.S. — which means all children who get the Pfizer vaccine are getting an EUA product.
In Wednesday’s congressional hearing on the Biden administration’s response to COVID-19, Rep. Dan Crenshaw (R-Texas) asked CDC Director Dr. Rochelle Walensky, why the CDC broke with its own norms and put an EUA vaccine on the childhood immunization schedule for a disease that poses very little risk to children and for which the vaccine poses many potential side effects without preventing transmission.
Walensky responded:
“The reason that the ACIP [Advisory Committee on Immunization Practices] recommended the CDC put the COVID-19 vaccine on the pediatric schedule was only because it was the only way it could be covered in our ‘Vaccines for Children’ program.
“It was the only way that our under-uninsured children would be able to have access to the vaccines … That was the reason to put it there.”
Data collected by the CDC through its Vaccine Adverse Event Reporting System (VAERS) and a growing number of other sources indicate serious health risks associated with COVID-19 vaccination for children.
“The COVID vaccines have not been shown to be either effective or safe for children,” CHD argued in an amicus brief filed in Louisiana last year. “The benefits to children are minuscule, while the risks — including the risk of potentially fatal heart damage — are ‘known’ and ‘serious,’ as the FDA itself has acknowledged.”
Other changes to the childhood schedule include adding the PVC15 shot, a pneumococcal conjugate vaccine used to help protect against pneumococcal bacteria and only recently approved for children; updated guidance for the flu and hepatitis B vaccines; and new recommendations for the measles, mumps and rubella (MMR) and polio vaccines.
The CDC now recommends an additional dose of the MMR vaccine in places where there is a mumps outbreak. It also recommends an additional poliovirus vaccine for children and adults if new polio cases emerge.
This would mean the childhood vaccination schedule would increase the number of recommended injections from 54 to 72 over the course of a person’s childhood, between the ages of 6 months and 18 years, The Defender reported last year.
CDC schedule protects pharmaceutical companies from liability for vaccine injuries
Vaccine makers are not liable for injuries or deaths associated with EUA vaccines but can be held liable for injuries caused by a fully licensed vaccine — unless that vaccine is added to the CDC’s childhood vaccination schedule.
Parents of children injured by vaccines listed on the childhood schedule can seek compensation through the taxpayer-funded National Vaccine Injury Compensation Program (NVICP), a no-fault alternative to the traditional legal system for resolving vaccine injury claims.
However, the revisions voted on by the ACIP committee last year explicitly state (slide 24) that the pneumococcal polysaccharide vaccine (PPSV23) and COVID-19 vaccines are not covered under the NVICP.
Instead, the COVID-19 vaccines added to the childhood schedule will remain covered by the Countermeasures Injury Compensation Program (CICP). To date, only 19 claims related to COVID-19 filed with the CICP have been found eligible for compensation, though no compensation has yet been paid.
Since it was established in 2010, the CICP only compensated 30 of the nearly 12,000 claims filed.
Are we seeing ‘the beginning of the end of Big Pharma’s reign’?
The addition of the COVID-19 vaccine to the immunization schedule “helps ‘normalize’ this vaccine and sends a powerful message to both healthcare providers and the general public that everyone ages 6 months and older should stay up to date with recommended COVID-19 vaccines (including a booster, when eligible), just as they would with any other routinely recommended vaccine,” Dr. Neil Murthy and Dr. A. Patricia Wodi said in a statement reported by CNN.
This “normalization” comes at a time when over 85% of the U.S. population hasn’t been boosted, despite the massive government-sponsored media push.
Nationally, only 12% of children ages 6 months to 4 years have received one dose of the vaccine. Only 58% of children ages 12 to 17 and 32% of children ages 5 to 11 have received two doses of the vaccine. Numbers vary widely across states.
Holland commented on the implications of adding this shot to the schedule:
“The childhood schedule is already unscientific and unjustifiable. Adding this shot may well be the straw that breaks the camel’s back. Parents are likely to resist, finally calling the entire childhood vaccine schedule into question.
“That day has been long in coming, but it is now here. I believe we are now watching the beginning of the end of Big Pharma’s reign over the nation’s children.”
At Wednesday’s congressional hearing, lawmakers repeatedly raised concerns about how regulatory agencies’ flawed recommendations led to a lack of confidence in public institutions.
Rep. Cathy McMorris Rodgers (R-Wash.) said, “There’s serious distrust today with our public health agencies. [Polling indicates] 40% of the public does not trust our public health agencies to handle the next public health emergency.”
Walensky indicated that vaccination rates for all vaccines on the childhood schedule among kindergarten children declined last year, dropping from 95% to 93% over the last two years, amounting to hundreds of thousands of parents opting not to comply with the childhood vaccination schedule.
VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S. While reports submitted to VAERS require further investigation before a causal relationship can be confirmed, VAERS historically has been shown to report only 1% of actual vaccine adverse events.
According to Retsef Levi, Ph.D., with the Massachusetts Institute of Technology, the vaccines “cause unprecedented levels of harm, including the death of young people and children.”
Multiple studies have determined that the vaccines increase the risk of myocarditis and pericarditis, particularly in young men.
An October 2022 study revealed the CDC was aware of the safety signal for these side effects months before it informed the public.
At the recent FDA vaccine advisory committee meeting, several committee members also raised concerns about recommending annual bivalent boosters for children given the lack of data.
Dr. Archana Chatterjee, Ph.D., committee member and dean of the Chicago Medical School and vice president for medical affairs at Rosalind Franklin University said:
“As we look at this question [simplifying the vaccination schedule] for young children, the data is just too few for us to really make scientifically sound decisions regarding this question. The trial data need to be much more robust than we have seen in the past.”
In light of data like this, vaccination for COVID-19 for children and healthy people is losing public and even governmental support in some places.
Under public pressure and facing a series of lawsuits, last week California dropped its plan to mandate COVID-19 vaccination for school children.
As of Feb. 6, 21 states have legislation or executive orders banning student vaccine mandates, according to the National Academy for State Health Policy, a nonpartisan organization of state health policymakers.
Only the District of Columbia currently has a vaccine mandate for school children, although it is not set to go into effect until the 2023-2024 school year.
Denmark ended its universal COVID-19 vaccination campaign for healthy individuals in February 2022.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
The State of Maryland has introduced a bill for consideration (Senate Bill 378) that would allow healthcare workers to vaccinate a child who is deemed “able to understand the benefits and potential consequences of getting vaccinated” without parental consent. The determined age of consent for a child to “choose” to be vaccinated is 14, though, such laws are often a slippery slope as guidelines and goalposts can be adjusted once a bill is passed to include even younger people.
It should be noted that Maryland law prevents children of 14 or older to refuse vaccination ordered by parents. In other words, they are considered competent enough to get vaccinated without parent’s knowledge, but not competent enough to refuse vaccination with parent’s knowledge. The push among some states to provide or legalize medical procedures on minors without advising parents has been growing in multiple sectors of healthcare the past few years, from abortions to gender affirmation surgeries.
It sounds like a remnant from two years ago when Democrat run states like New York were talking seriously about the forced internment of people who were “potential dangers” to public health. The concept of constitutional rights were going out the window and the US barely dodged an Orwellian end. Parental rights are often considered a vital barrier to state interference with vulnerable children who are easily manipulated into accepting procedures that could affect their rest of their lives.
The potential consequences are obvious – Schools and other government institutions could very easily exploit medical personnel to convince children that they MUST submit to vaccination. They could also influence minors to believe it was “all their idea.” The same scenario could involve overzealous doctors or nurses in a hospital setting. With the informed parental shield removed, the sky is the limit in terms of what the state can do to the younger generation.
Though the bill mentions that decisions by minors be made “without coercion”, a child may not be able to identify coercion when it happens. Not all manipulation requires open and obvious threats.
Democratic State Sen. Cheryl Kagan introduced Bill 378 on Wednesday. The bill is set to go before a hearing in the Senate Finance Committee on Feb. 22. The language is broad and seems to include all possible vaccinations rather than a set list.
Even in the case of a child voluntarily asking for medical treatments without deception, it is the job of parents to sometimes protect their kids from themselves. Without developed critical thinking skills minors require guidance to avoid rash decisions. When pressure is coming from officials with perceived authority, children are less likely to say no. The Maryland bill ignores these factors and opens the door to a wide range of abuses.
In his State of the Union address on Tuesday night, President Biden rewrote the history of the pandemic. Biden lamented, “Covid had shut down our businesses. Schools were closed. We were robbed of so much.” But it wasn’t Covid that issued the shutdown edicts.
We were robbed by politicians like Biden who disrupted lives in a futile effort to thwart a virus that infected hundreds of millions of Americans anyhow. There was never solid evidence to justify shutting businesses or schools but that did not deter politicians from promising to save humanity by destroying freedom.
After Pfizer and Moderna, Biden was perhaps the biggest Covid profiteer in America. In 2020, Biden ran one of the most fear-based presidential campaigns in modern history. Biden talked as if every American family had lost a member or two from this pestilence. He routinely exaggerated Covid death tolls by a hundred- or a thousand-fold, publicly asserting that millions of Americans had been killed by Covid-19. Biden was helped mightily by fear-mongering media coverage.
A Brookings Institute analysis noted, “Democrats are much more likely than Republicans to overestimate [Covid] harm. Forty-one percent of Democrats… answered that half or more of those infected by COVID-19 need to be hospitalized.” At that time, the rate of hospitalization was between 1 percent and 5 percent – so those Democratic voters overestimated the risk of hospitalization by up to 20-fold.
In the final debate between the presidential candidates in October 2020, Biden blamed Trump for every Covid fatality: “220,000 Americans dead…. Anyone who’s responsible for that many deaths should not remain as president of the United States.” Biden promised, “I will take care of this. I will end this. I’m going to shut down the virus, not the country.” In a speech on the day before Election Day, he declared, “We’re going to beat this virus. We’re going to get it under control, I promise you.” Biden won the presidency as a result of only 43,000 votes in three swing states. The disruption and damage caused by lockdowns were invoked as proof of Trump’s negligence, rather than seen as evidence of an unprecedented political panic-mongering and repression.
After taking office, Biden issued a flurry of edicts, including mandating masks for anyone on federal property. In September 2021, he mandated that more than 100 million be injected with Covid vaccines, despite proliferating evidence that the vaccines were failing to prevent transmission or infections. In an October 2021 CNN Town Hall, Biden vilified vaccine skeptics as murderers who only wanted “the freedom to kill you” with Covid.
On Tuesday night, Biden announced, “Covid no longer controls our lives.” But Biden extended the official Covid emergency at least until May 11, entitling him to sweeping additional power. Biden still claims that Covid miraculously entitles him to “forgive” half a trillion dollars in federal student debt. And the Biden administration is fighting to perpetuate vaccine mandates on foreign visitors to America and to preserve the president’s prerogative to impose mask mandates.
The carnage from Covid crackdowns is still being tabulated. A 2022 Johns Hopkins University analysis of 24 studies on the impact of lockdowns in the United States and Europe found “no evidence that lockdowns, school closures, border closures, and limiting gatherings have had a noticeable effect on COVID-19 mortality.” The pointless shutdowns did far more damage than Biden will ever admit:
A National Bureau of Economic Research analysis estimated that young Americans suffered “171,000 excess non-Covid deaths during 2020 and 2021… a historic, yet largely unacknowledged, health emergency.” Many of those fatalities were “collateral damage” from shutdowns and other Covid policies.
Millions of jobs were lost thanks to lockdowns, a major reason why life expectancy in the United States had its sharpest plunge since World War Two.
Forced isolation was a Grim Reaper. Deaths from drug overdoses set an all-time record of 108,000 in 2021 and alcohol-related deaths jumped 25% in the first year of the pandemic.
The Biden administration suppressed free speech on Twitter and other social media based on a single theme: “Be very afraid of Covid and do exactly what we say to stay safe,” as journalist David Zweig summarized in the TwitterFiles. Official fear-mongering helped boost the percentage of Americans reporting struggling with depression or anxiety by more than 300 percent.
If Biden can shift blame for disastrous Covid policies, politicians will be more likely to pointlessly lock down the nation in the future. Americans deserve to see all the federal records and all the state government records to expose the recklessness and deceit that permeated Covid policies. America will not recover from the pandemic until all the COVID lies and abuses by officialdom have been exposed.
James Bovard, 2023 Brownstone Fellow, is author and lecturer whose commentary targets examples of waste, failures, corruption, cronyism and abuses of power in government. He is a USA Today columnist and is a frequent contributor to The Hill. He is the author of ten books.
Former Twitter executives looked at times uncomfortable, but betrayed their staunch anti-free speech biases during a House Oversight Committee heading on Wednesday.
The hearing was called to investigate the role government played, specifically the FBI, with regards to censorship of the Hunter Biden laptop report by the New York Post.
Former Twitter Chief Legal Officer Vijaya Gadde, Former Deputy General Counsel James Baker, and Former Global Head of Trust & Safety Yoel Roth were grilled by Representatives, with Congressman Clay Higgins telling them they could be arrested for interfering with the 2020 presidential election.
“The bottom line is that the FBI had the Biden Crime Family laptop for a year. They knew it was leaking. They knew it would hurt the Biden family. So the FBI used its relationship with Twitter to suppress criminal evidence from being revealed about Joe Biden one month before the 2020 election,” Higgins asserted.
“You, ladies and gentlemen interfered with the United States of America 2020 presidential election! Knowingly and willingly!” he continued, adding “That’s the bad news! It’s gonna get worse! Because this is the investigation part! Later comes the arrest part, your attorneys are familiar with that.”
“I’d like to spend five hours with these ladies and gentlemen doing depositions surely yet to come,” the Congressman added.
Elsewhere during the hearing, Rep. Nancy Mace blasted the former executives for also, as highlighted by the Elon Musk’s release of The Twitter Files, working to suppress information regarding COVID.
“I along with many Americans have long term effects from COVID. Not only was I a long-hauler, but I have effects from the vaccine,” Mae declared.
She continued, “It wasn’t the first shot but it was the second shot. I have now developed asthma that has never gone away since I had the second shot. I have tremors in my left hand. And I have the occasional heart pains that no doctor can explain. And I’ve had a battery of tests.”
“I find it extremely alarming Twitter’s suppression spread into medical fields,” Mace told the former execs.
“You’re not a doctor, right?” Mace directly asked Gadde, adding “What makes you think you or anyone else at Twitter have the medical expertise to censor actual, accurate CDC data?”
Gadded pathetically claimed she was not familiar with these particular situations.”
“Yeah, I’m sure you’re not,” Mace shot back.
Republican Ohio Rep. Jim Jordan told them they “got played by the FBI” over the Hunter Biden laptop, forcing Roth to admit that the New York Post report didn’t violate any Twitter policies in his opinion, but was censored anyway.
“This to me is the real takeaway,” Jordan said, going on to state “51 former intelligence officials, five days after you guys take down the Hunter Biden story and block the New York Post’s account, five days later, 51 former intel officials send a letter and they say, ‘the Hunter Biden story has all the classic earmarks of a Russian information operation.’ The information operation was run on you guys, and then by extension then run on the American people. And that’s the concern.”
Republican Rep. Lauren Boebert asked the former Twitter executives “Who the hell do you think you are?” for shadow banning people they disagree with on the platform.
Boebert also asked the execs if they had shadow banned her own account.
“I can reach out to Elon and to his staff, and I can see what’s happened ,and I can sit here today and hold you all in account,” Boebert concluded, adding “I am angry for the millions of Americans who were silenced because of your decisions, because of your actions, because of your collusion with the federal government. They can’t reach out to Elon. They can’t sit here today and hold you in account.”
The chair of the Committee, Rep. James Comer of Kentucky highlighted Tweets made by Roth in the past calling Republicans ‘Nazis’.
Republican Rep. Marjorie Taylor Greene of Georgia told Roth “You permanently banned my Twitter account but you allowed child porn all over Twitter.”
The former execs mostly either claimed ignorance and denied any wrong doing.
James Baker said he can’t recall speaking with the FBI while working at Twitter, and denied that he acted unlawfully.
Meanwhile, Roth attempted to argue that censorship on Twitter under his watch helped to create more freedom of speech.
Roth also admitted that he finds it “regrettable” that the conservative account LibsOfTikTok is still allowed to be active on Twitter… More videos
‘Just an ear infection, here’s some antibiotics,’ was my hospital diagnosis after a five-minute assessment; strange, as I couldn’t understand how an ear infection could make my eye swell and deliver an excruciating head pain akin to being hit with a hammer four days earlier.
I had an Oxford University/AstraZeneca Covid-19 vaccine on March 28, 2021. I was 54. The government said it would enable people to get back to some kind of normality, both family and work (I was in the clothing industry). It was implied that it was our duty to protect those around us by being vaccinated. Thirdly, I was the carer for my frail 87-year-old father, living alone since my mother’s death in 2006.
The ‘ear infection’ pain got worse, the symptoms debilitating, I thought at one point I was going to die. I’m not a moaner but I just wasn’t comfortable with what I was told, and so began my road-blocked journey to VITT (vaccine-induced immune thrombocytopenia and thrombosis) diagnosis.
Once a diagnosis is given, it is nigh on impossible to get it changed, and for three months after I was told I had an ear infection I went back and forth to my GP, writing letters explaining my symptoms, asking for neurological referral, all to no avail.
I was eventually granted eye and blood tests. The eye test result recommended neurological assessment, but the killer was being handed my blood test results without explanation, just some notations stating ‘Abnormal see Doctor’.
Now very worried, I decided to see a private neurologist. I hadn’t even sat down before the neurologist, sizing me up in an instant, said ‘Something’s not right’ and suddenly I was an NHS emergency.
NHS MRI/CT scans and blood tests followed and then silence. All the adrenaline ebbs away and one gets back to life . . . until that moment when the phone rings, you see the word HOSPITAL on the display, and your pulse starts racing. It’s that call, and the calm voice you are hearing is telling you there’s a blood clot in your brain.
I didn’t take it in, I started shaking. I asked the neurologist (who is wonderful) to slow down as I couldn’t understand any of it.
A few days later I’m talking to a haematologist, again a wonderful person, and with pills and blood tests under way I had gathered myself and was able to ask questions.
I later wrote to my hospital and GP telling them of my diagnosis. I’ve got the ‘Sorry about that’ letters, the ‘we learned a lot/the MHRA didn’t tell us’ etc reasons. And I still have the blood clot I first told them I thought I had as a consequence of my vaccine.
Today, I feel if I’d been admitted on first presentation I’d have recovered. Instead, my NHS-diagnosed VITT blood clot and head pain are a constant reminder, my walking stick an embarrassment, and all the rest: my drooping eye, the vision fluctuation, the increased cranium pressure and broken teeth from my falls, the loss of my driving licence, PTSD, the lumbar puncture, blood thinners and the other procedures/appointments I now have after taking a ‘safe and effective’ vaccine – I can’t even work any more.
The impact has been just as bad for my father. I was pretty much his only link with the outside world, but because of my injury and all that goes with it (not being able to drive, for example) I can’t provide care for him. His health and well-being have suffered greatly. Now he has full-time live-in care, which he has to pay for, and has been in and out of hospitals since.
It’s all dreadfully sad. I have apologised to him and my family for my taking the vaccine. I wish I could turn the clock back and be a normal husband, dad and son again, but all that’s been ripped away from me. Everyone in a family suffers when it’s a vaccine injury, not just the vaccinated.
If you are vaccine injured, or know someone who is, you can contact or read about the the Covid-19 vaccine injury support group, UK CV Family, here.
In December 1945 and January 1946, the British Mandate authorities carried out an extensive survey of Palestine, in support of the work of the United Nations Special Committee on Palestine. The results were published in the Survey of Palestine, which has been scanned and made available online by Palestine Remembered; all 1300 pages can be read here.
This site is provided as a research and reference tool. Although we make every reasonable effort to ensure that the information and data provided at this site are useful, accurate, and current, we cannot guarantee that the information and data provided here will be error-free. By using this site, you assume all responsibility for and risk arising from your use of and reliance upon the contents of this site.
This site and the information available through it do not, and are not intended to constitute legal advice. Should you require legal advice, you should consult your own attorney.
Nothing within this site or linked to by this site constitutes investment advice or medical advice.
Materials accessible from or added to this site by third parties, such as comments posted, are strictly the responsibility of the third party who added such materials or made them accessible and we neither endorse nor undertake to control, monitor, edit or assume responsibility for any such third-party material.
The posting of stories, commentaries, reports, documents and links (embedded or otherwise) on this site does not in any way, shape or form, implied or otherwise, necessarily express or suggest endorsement or support of any of such posted material or parts therein.
The word “alleged” is deemed to occur before the word “fraud.” Since the rule of law still applies. To peasants, at least.
Fair Use
This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available in our efforts to advance understanding of environmental, political, human rights, economic, democracy, scientific, and social justice issues, etc. We believe this constitutes a ‘fair use’ of any such copyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17 U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed a prior interest in receiving the included information for research and educational purposes. For more info go to: http://www.law.cornell.edu/uscode/17/107.shtml. If you wish to use copyrighted material from this site for purposes of your own that go beyond ‘fair use’, you must obtain permission from the copyright owner.
DMCA Contact
This is information for anyone that wishes to challenge our “fair use” of copyrighted material.
If you are a legal copyright holder or a designated agent for such and you believe that content residing on or accessible through our website infringes a copyright and falls outside the boundaries of “Fair Use”, please send a notice of infringement by contacting atheonews@gmail.com.
We will respond and take necessary action immediately.
If notice is given of an alleged copyright violation we will act expeditiously to remove or disable access to the material(s) in question.
All 3rd party material posted on this website is copyright the respective owners / authors. Aletho News makes no claim of copyright on such material.





{kind=link}