CHD Funds Lawsuit Against CDC Over Program That Forces Pediatricians to Give COVID Vaccines to Kids on Medicaid
By Michael Nevradakis, Ph.D. | The Defender | April 28, 2025
A California pediatrician is suing the Centers for Disease Control and Prevention (CDC) over a federal program that requires doctors in her state who treat children enrolled in Medicaid to give those children all of the vaccines recommended by the CDC.
Children’s Health Defense (CHD) is supporting the lawsuit, filed April 25 in the U.S. District Court for the Central District of California, Santa Ana Division.
Dr. Samara Cardenas lost her medical practice after the CDC Vaccines for Children Program kicked her out of the program because she wouldn’t give COVID-19 vaccines to healthy kids.
California, like most states, requires pediatricians who treat Medicaid patients to be enrolled in the Vaccines for Children Program. The program, in turn, requires doctors to strictly follow the CDC’s childhood immunization schedule.
In late 2023, the Vaccines for Children Program informed Cardenas that her vaccine orders “were being scrutinized” for not including COVID-19 shots. She was later expelled from the program. As a result, she lost her Medicaid contract, forcing her to close her practice.
The Vaccines for Children Program primarily serves low-income populations by providing free vaccines to uninsured or underinsured children and children who are eligible for or enrolled in Medicaid. Medicaid compensates pediatricians for the costs associated with administering the vaccines.
In her first-of-its-kind lawsuit, Cardenas alleges the CDC’s Vaccines for Children Program violates the Fifth Amendment’s equal protection and due process provisions by subjecting children enrolled in Medicaid to different treatment standards and compelling doctors to act against their professional judgment.
The lawsuit also questions the safety and necessity of administering COVID-19 vaccines to children, the inclusion of COVID-19 shots on the CDC’s childhood immunization schedule and the impartiality of the CDC Advisory Committee on Immunization Practices (ACIP), which makes vaccine-related recommendations.
In California, 3 in 7 — or about 5 million children — are enrolled in Medicaid. Nationally, about 40% of all kids — or about 29.2 million children ages 0-17 — are covered by Medicaid.
The suit names CDC Acting Director Susan P. Monarez, as the defendant. Monarez is also President Donald Trump’s nominee to lead the agency.
Cardenas ‘followed her conscience and the science’
Attorney Rick Jaffe, who represents Cardenas, said this is “the first federal lawsuit challenging the CDC’s coercive use of the VFC [Vaccines for Children] program to enforce experimental, emergency-authorized COVID-19 vaccination as a condition of Medicaid access.”
Cardenas “followed her conscience and the science,” Jaffe said. “The VFC framework gave her no choice: vaccinate all kids or lose access.”
Kim Mack Rosenberg, CHD general counsel, said the lawsuit places policies that disproportionately affect Medicaid recipients under scrutiny, as the Vaccines for Children Program’s policy “essentially mandates these experimental shots for a population historically vulnerable to medical experimentation.”
Cardenas is not seeking compensatory damages. Instead, the lawsuit “seeks to compel the CDC to abandon its misguided and scientifically untethered policy, and stop the unnecessary mass vaccination of the nation’s poorest children.”
“We’re asking the court to say the government can’t make scientific compliance a prerequisite to serving poor patients,” Jaffe said.
Pediatrician Dr. Michelle Perro said that by requiring physicians to administer all vaccines on the childhood vaccination schedule, “medical autonomy is abolished” while “low-income children are left with fewer options and less continuity of care.”
Perro said many doctors are reluctant to oppose these policies. “The threat of speaking out is financial ruin and the potential loss of their ability to practice,” Perro said. “This is coercion and harassment.”
‘The unknowns are enough to never let these products anywhere near children’
In October 2022, ACIP, the CDC’s vaccine advisory panel, unanimously recommended adding COVID-19 vaccines for children as young as 6 months old to the CDC childhood schedule.
The complaint alleges that before making that recommendation, the CDC failed “to compile and analyze vaccine injury data.” It also alleges that ACIP is “compromised by conflicts of interest,” as many of its members “have financial or professional ties to vaccine manufacturers or related interests” — for which the CDC has granted conflict-of-interest waivers.
According to the complaint, by not presenting evidence of the vaccine’s clinical benefit, ACIP violated the Administrative Procedure Act, a federal law banning government agency actions that are “arbitrary, capricious, an abuse of discretion, or otherwise not in accordance with law.”
The lawsuit cites data from the U.S. government-run Vaccine Adverse Event Reporting System (VAERS) showing reports of “hundreds of thousands of adverse events” related to the COVID-19 vaccines, including “serious adverse events and deaths.”
As of March 28, VAERS listed 72,924 reports of adverse events in people 18 and younger, including 6,122 serious adverse events and 201 deaths.
Albert Benavides, a VAERS expert and founder of VAERSAware.com, said the true figures are higher, as many VAERS report summaries indicate the victim’s age even if the report officially lists the age as “unknown.” His analysis of reports shows that “there is more than double the amount of dead children” — 556 in total.
According to the complaint, the CDC failed to “reevaluate or rescind its blanket recommendation for COVID-19 vaccination,” and that ACIP is instead doubling down on its COVID-19 vaccine recommendations.
The complaint cites this month’s ACIP meeting, during which the committee considered revising its blanket COVID-19 vaccine recommendation and switching to risk-based recommendations.
ACIP member Dr. Denise Jamieson opposed the proposal, claiming that the “U.S. has a history of not being able to implement such variable recommendations,” which would confuse the public.
“This is not merely arrogance,” the lawsuit states. “It is government-by-committee at its most dangerous — where unelected public health advisors retain extraordinary power to shape national policy.”
Attorney Ray Flores, senior outside counsel for CHD, questioned why the CDC added COVID-19 vaccines to the childhood vaccination schedule even though they were not licensed, but only issued under emergency use authorization (EUA).
“It shocks the conscience,” Flores said. “Physicians in California must be free to exercise their best judgment, especially when it comes to administering experimental injections.”
Releasing the vaccines under EUA meant they were subject to less testing than a licensed vaccine, said Karl Jablonowski, Ph.D., senior research scientist for CHD. “The unknowns are enough to never let these products anywhere near children. There are heavy compromises made when you skip the already insufficient regulatory steps with an emergency use authorization.”
‘Can the government tell a doctor what she must inject in order to treat the poor?’
In 2022, Sweden and Denmark stopped recommending COVID-19 shots for children. In 2023, the U.K. ended its COVID-19 booster program for healthy people ages 50 and younger. That year, the World Health Organization said healthy children and teens should be considered low priority for COVID-19 vaccines.
Several recent studies have also called the practice of vaccinating healthy children for COVID-19 into question.
A December 2024 study published in the Journal of the Pediatric Infectious Diseases Society found that children under 5 who received the Pfizer COVID-19 vaccines were more likely to become infected with COVID-19 than unvaccinated children with natural immunity.
A May 2024 preprint observational study of 1.7 million U.K. children and teenagers found myopericarditis only in the group that received Pfizer’s COVID-19 vaccine and that the vaccine provided only 14 to 15 weeks of protection against infection.
Pfizer documents publicized last year showed that the company quietly studied myocarditis in children a month before its COVID-19 vaccine received an EUA for children ages 5-11.
A peer-reviewed study published earlier this month in Immunity, Inflammation and Disease, found that young adults who received a Pfizer COVID-19 vaccine exhibited spike protein production a year or more after vaccination — significantly longer than the spike protein was expected to remain in the body.
Jaffe said the lawsuit “isn’t about vaccine skepticism. It’s about professional freedom, patient-level nuance, and constitutional limits on administrative coercion.”
“Can the government tell a doctor what she must inject in order to treat the poor? That’s what this case asks. And the answer should be ‘no.’”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
The False Claims of WHO’s Pandemic Agreement
By David Bell | Brownstone Institute | April 28, 2025
One way to determine whether a suggestion is worth following is to look at the evidence presented to support it. If the evidence makes sense and smells real, then perhaps the program you are asked to sign up for is worthy of consideration.
However, if the whole scheme is sold on fallacies that a child could poke a stick through, and its chief proponents cannot possibly believe their own rhetoric, then only a fool would go much further. This is obvious – you don’t buy a used car on a salesman’s insistence that there is no other way to get from your kitchen to your bathroom.
Delegates at the coming World Health Assembly in Geneva are faced with such a choice. In this case, the car salesman is the World Health Organization (WHO), an organization still commanding considerable global respect based on a legacy of sane and solid work some decades ago.
It also benefits from a persistent misunderstanding that large international organizations would not intentionally lie (they increasingly do, as noted below). The delegates will be voting on the recently completed text of the Pandemic Agreement, part of a broad effort to extract large profits and salaries from an intrinsic human fear of rare causes of death. Fear and confusion distract human minds from rational behavior.
WHO Likes a Good Story?
The Pandemic Agreement, and the international pandemic agenda it is intended to support, are based on a series of demonstrably false claims:
- There is evidence of a rising risk of severe naturally occurring pandemics due to a rapid (exponential) increase in infectious disease outbreaks
- A massive return on financial investment is expected from diverting large resources to prepare for, prevent, or combat these
- The Covid-19 outbreak was probably of natural origin, and serves as an example of unavoidable health and financial costs we will incur again if we don’t act now.
If any of these were false, then the basis on which the WHO and its backers have argued for the Pandemic Agreement is fundamentally flawed. And all of them can be shown to be false. However, influential people and organizations want pandemics to be the main focus of public health. The WHO supports this because it is paid to.
The private sector invested heavily in vaccines, and a few countries with large vaccine and biotech industries now direct most of the WHO’s work through specified funding. The WHO is obligated to deliver what these interests direct it to.
The WHO was once independent and able to concentrate on health priorities – back when they prioritized the main drivers of sickness and premature mortality and gained the reputation they now trade from. In today’s corporatized public health, population-based approaches have lost value, and the aspirations of the World Economic Forum hold more sway than those dying before sixty.
Success in the health commodities business is about enlarging markets, not reducing the need for intervention. The WHO and its reputation are useful tools to sanitize this. Colonialism, as ever, needs to appear altruistic.
Truth Is Less Compelling Than Fiction
So, to address these fallacies. Infectious disease mortality has steadily declined over the past century despite a minor Covid blip that took us back just a decade. This blip includes the virus, but also the avoidable imposition of poverty, unemployment, reduced healthcare access, and other factors that the WHO had previously warned against, but recently actively promoted.
To get around this reality of decreasing mortality, the WHO uses a hypothetical disease (Disease X), a placeholder for something that has not happened since the Spanish flu in the pre-antibiotic era. The huge Medieval pandemics such as the Black Death were mostly bacterial in origin, as were probably most Spanish flu deaths. With antibiotics, sewers, and better food, we now live longer and don’t expect such mortality events, but the WHO uses this threat regardless.
Thus, the WHO has been reduced to misrepresenting fragile evidence (e.g. ignoring technology developments that can explain rising reports of outbreaks) and opinion pieces by sponsored panels in order to support the narrative of rapidly rising pandemic risk. Even Covid-19 is getting harder to use. If, as appears most likely, it was an inevitable result of laboratory manipulation, then it no longer even serves as an outlier. The WHO’s pandemic agenda is squarely targeted at natural outbreaks; hence the need for “Disease X”.
The WHO (and the World Bank) follow a similar approach in inflating financial Return on Investment (ROI). If you received an email promoting over 300 to 700 times return on a proposed investment, some may be impressed but sensible people would suspect something amiss. But this is what the Group of Twenty (G20) secretariat told its members in 2022 for return on investment on the WHO’s pandemic preparedness proposals.
The WHO and the World Bank provided the graphic below to the same G20 meeting to support such astronomical predictions. It is essentially subterfuge; a fantasy to mislead readers such as politicians who are too busy, and trusting, to dig deeper. As these agencies are intended to serve countries rather than fool them, this sort of behavior, which is recurrent, should call into question their very existence.
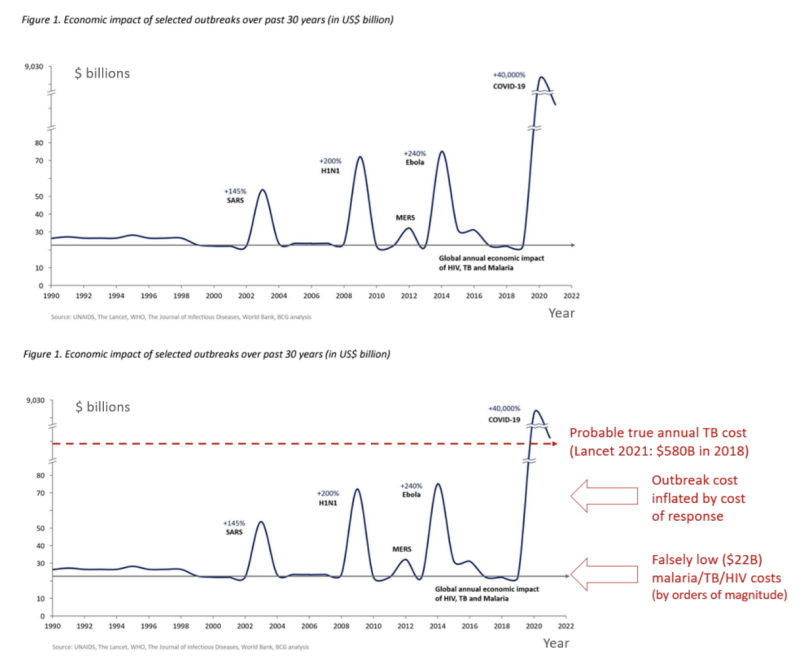
Figure 1 from Analysis of Pandemic Preparedness and Response (PPR) architecture, financing needs, gaps and mechanisms, prepared by WHO and the World Bank for the G20, March 2022. Lower chart modified by REPPARE, University of Leeds.
A virus like SARS-CoV-2 (causing Covid-19) that mostly targets the sick elderly with an overall infectious mortality rate of about 0.15% will not cost $9 trillion unless panicked or greedy people choose to close down the world’s supply lines, implement mass unemployment, and then print money for multi-trillion-dollar stimulus packages. In contrast, diseases that regularly kill more and much younger people, like tuberculosis, malaria, and HIV/AIDS, cost far more than $22 billion a year in contrast.
A 2021 Lancet article put tuberculosis losses alone at $580 billion/year in 2018. Malaria kills over 600,000 children annually, and HIV/AIDS results in similar numbers of deaths. These deaths of current and future productive workers, leaving orphaned children, cost countries. Once, they were the WHO’s main priority.
Trading on a Fading Reputation
In selling the package, the WHO seems to have abandoned any attempt at meaningful dialogue. They still justify the surveillance-lockdown-mass vaccinate model by the logic-free claim that over 14 million lives were saved by Covid vaccines in 2021 (so we all have to do that again). The WHO recorded a little over 3 million Covid-related deaths in the first (vaccine-free) year of the pandemic. For the 14 million ‘saved’ to be correct, another 17 million would somehow have been due to die in year two, despite most people having gained immunity and many of the most susceptible having already succumbed.
Such childish claims are meant to shock and confuse rather than educate. People are paid to model such numbers to create narratives, and others are paid to spin them on the WHO websites and elsewhere. An industry worth hundreds of billions of dollars depends on such messaging. Scientific integrity cannot survive in an organization paid to be a mouthpiece.
As an alternative, the WHO could advocate for investment in areas that promoted longevity in wealthy countries – sanitation, better diet and living conditions, and access to basic, good medical care.
This was once the WHO’s priority because it not only greatly reduces mortality from rare pandemic events (most Covid deaths were in people already very unwell), but it also reduces mortality from the big endemic killers such as malaria, tuberculosis, common childhood infections, and many chronic non-communicable diseases. It is, unequivocally, the main reason why mortality from major childhood infectious diseases like measles and Whooping cough plummeted long before mass vaccinations were introduced.
If we concentrated on strategies that improve general health and resilience, rather than the financial health of the pandemic industrial complex, we could then confidently decide not to wreck the lives of our children and elderly if a pandemic did arise.
Very few people would be at high risk. We could all expect to live longer and healthier lives. The WHO has elected to leave this path, instill mass and unfounded fear, and support a very different paradigm. While the Pandemic Agreement is not essential to it, it is an important part of diverting further funds to this agenda and cementing this corporatist approach into place.
The United States has done well by stepping out of this mess, but continues to push many of the same fallacies and was instrumental in sowing the mess we now reap. While a few other governments are questioning, it is hard for any politicians to stand with truth when a sponsored media stands squarely elsewhere.
Society is once more enslaving itself, at the behest of an entitled few, facilitated by international agencies that were set up specifically to guard against this. At the coming World Health Assembly, the pandemic fairytale will almost certainly prevail.
The hope is that a well-deserved erosion of trust will eventually catch up with the global health industry and too few countries will ratify this treaty for it ever to come into force. To fix the underlying problem though and derail the pandemic industry train, we will need to rethink the whole approach to cooperation in international health.
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. David is a former medical officer and scientist at the World Health Organization (WHO), Programme Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland, and Director of Global Health Technologies at Intellectual Ventures Global Good Fund in Bellevue, WA, USA.
Klaus Schwab, Sophist

By Laurie Calhoun | The Libertarian Institute | May 1, 2025
The existence of Klaus Schwab became known to much of the thinking world during the Coronapocalypse, when so-called conspiracy theories began to flourish about the use of the novel COVID-19 virus as a pretext for reconfiguring the world. The “Great Reset” and the “New Normal” began to be spoken of fondly by bureaucrats back in 2020, shortly after the in some ways incomprehensibly influential Schwab co-authored with Thierry Malleret a short book extolling just those concepts: Covid-19: The Great Reset.
The work, or paraphrased excerpts of it, must have been spam-emailed to every government official and mainstream media journalist on the planet, because in no time pundits and their parrots in the press were gushing about the Great Reset, essentially a Brave New World to come (had none of them read Aldous Huxley’s classic work, or did they simply not understand it?). Nearly every influential person with a microphone was emitting the expression “Everything has changed,” insisting that this was because of the emergence of the novel coronavirus, not the government policies enacted in response to it. Schwab was lurking behind the scenes from the beginning, proffering gaslighting homilies and question-begging arguments camouflaged as benevolent recommendations and facts:
“The worldwide crisis triggered by the coronavirus pandemic has no parallel in modern history.”
In truth, “Everything changed” only because government officials changed everything, by closing national borders, locking down entire populations, preventing groups from assembling, and shutting down schools and all but specially designated “essential” businesses. Human beings were required to wear masks nearly everywhere they went, and those who demurred were treated as miscreants and pursued by the police. The insistence by politicians, bureaucrats and other opinion makers that “Everything has changed” was curiously reminiscent of how officials rationalized a massive and ruthless assault on Afghanistan and Iraq in the aftermath of crimes committed on September 11, 2001, by a small group of persons hailing primarily from Saudi Arabia. (Induction on two cases: when someone starts chiming, “Everything has changed!” in order to persuade you to do something or to support some initiative, you should probably turn around and walk away.)
Klaus Schwab founded and led the World Economic Forum (WEF) for more than fifty years. Many of what were revealed during the pandemic period to be the most brazen authoritarians among ostensibly democratic world leaders have connections to the organization. Canadian Prime Minister Justin Trudeau, New Zealand Prime Minister Jacinda Ardern, and French President Emmanuel Macron are notable examples of leaders who punished and even ostracized citizens for daring to defy their administration’s draconian COVID policies. Schwab recently resigned from his position, but whether that was because of age—he was born in 1938—or scandal matters little at this point, for his legacy has been secured throughout much of the world.
Key features of the Great Reset were to foist ESG (Environmental, Social and Governance investing) on people transnationally or, perhaps more accurately, meta-nationally. We have seen that elements of Schwab’s Weltanschauung have indeed made their way into not only federal government policies, with Green New Deals and carbon-limiting programs imposed in many parts of the planet, but also global corporate initiatives, as many companies now boast about their “environmental and social conscience,” using this as a marketing tool. Under the “Social Governance” guise of the ESG program, enthusiastic efforts to expand DEI (Diversity, Equity, and Inclusion) frameworks throughout the spheres of education and business have led to the appearance of “trans flags” waving alongside national flags at government buildings in what can only be characterized as a bizarre obsession with the subset of human beings, oddly in ascendance, who are said to have been born with the wrong set of genitalia.
One of the more extreme consequences of DEI has indeed been the effusive promotion of a radical trans agenda, which is arguably both homophobic and misogynistic, promoting as it does a grotesque caricature of femininity, exemplified by the skimpily clad and seemingly ditsy Dylan Mulvaney (remember the Budweiser ads?), while essentially denying the possibility of androgyny. In the name of inclusion, biological males (persons in possession of a Y chromosome) have been allowed to compete with females (persons devoid of a Y chromosome) in sports, with female competitors predictably forced to forego awards and scholarships as a result. Female athletes whose sports involve contact with competitors have been physically endangered by the admission of males into their sphere, as is evidenced by the case of volleyball player Payton McNabb and the 2024 Olympic boxing controversy, when two competitors who had previously failed a female gender test (for Y chromosome and testosterone levels) were permitted to compete. On top of all of those clear and present dangers, females in locker rooms have been faced with the prospect of seeing a penis dangling before them as they change their clothes or shower. Rather than attempt to protect females, policymakers were somehow persuaded by radical trans activists that males who decreed themselves to be female needed to be protected instead.
The incomprehensible power of the radical trans facet of the DEI agenda also brought about the enactment of laws which criminalize the “mis-pronouning” of persons who, despite having been born male, self-identify as female, or vice versa. Or neither, which necessitates, by law in some places now, that their interlocutors restrict personal pronoun usage to ‘they/them’. The latter is needless to say a no-win arrangement, for in complying with pronoun laws, one is thus obliged to commit a crime of grammar.
On the New Green Deal front, the European Union is continually devising new policies which attest to its commitments to the New Normal as envisioned by Schwab’s WEF, perhaps the most notorious slogan of which is “You’ll own nothing and be happy.” Countless memes have satirized the WEF leader for exhorting people to eat insects and stay in their “pods,” on the grounds that livestock and travel are allegedly a menace to the future of the planet. (Note: the persons who attend the ever-proliferating conferences on the environment or serve as parliament members of the EU generally fly to their meetings, sometimes in private jets.) Earnest discussion of the possibility of “15-minute cities,” where people do not need to (or are not allowed to) travel farther than fifteen minutes from their domicile has been taken up among local council members in “green-savvy” communities.
The list of rules and regulations already imposed by the European Union is seemingly endless, but to offer only two recent examples: plastic bottles sold in Europe are now required to have their caps affixed to them, and single-serving portion containers (such as are used at bed and breakfast hotels for jam, butter, honey, etc.) are in the process of being outlawed, despite having been devised as a means not only of convenience but also to prevent cross-contamination between unrelated guests. Only time will tell whether bureaucrats eventually side with public health officials or environmentalists in the latter case.
Far more important for the future of free people are the persistent censorship measures in the United Kingdom, Europe, Australia and beyond, modeled after anti-misinformation and surveillance policies aggressively enforced in many countries during the COVID period. To the shock of many thinking people, governments have taken it upon themselves to monitor the social media posts of citizens and to criminalize the expression of what are deemed unacceptable opinions, an obvious legacy of the COVID period, when persons who disagreed with the government were roundly denounced as agents of misinformation who needed to be de-platformed and silenced, lest they kill anyone with their dangerous ideas. Strikingly, reports of vaccine injury were not even false (misinformation), according to the censors themselves, but instead “malinformation,” which officials regarded as having the potential to prevent people who needed the “vaccine” from getting it.
Looking back at the surprising convergence among governments about the necessity of global lockdowns and, later, universal vaccination in the face of a virus which primarily endangered elderly and already infirm persons, it is clear that Schwab’s work served as a sort of template for how to communicate with constituents and conduct public affairs. Paternalism reigned (or, if you prefer, “maternalism” à la Nurse Ratched), as citizens were spoken to by political leaders in condescending tones as though they were toddlers who needed to be protected from themselves. This approach to governance can be summed up in a phrase: Children are to be seen, not heard.
Citizens were told that it was wrong to do their own research because only “the experts,” such as pandemic guru Anthony Fauci knew what they were doing. Despite having repeatedly lied in insisting that the virus had emerged naturally, having somehow leapt from a bat to a human being (when someone in Wuhan ate a bowl of soup?), Fauci himself, we now know, promoted and funded the gain-of-function research which culminated in the very existence—and potency—of the virus. Throughout this period of history, persons who dared to dissent from the dictates and narratives of the government were decried as enemies of humanity who needed to be controlled in order to protect other people from their nefarious tendencies. Notably, Robert F. Kennedy, Jr., author of The Real Anthony Fauci (a true tale of moral horror), who now serves as secretary of Health and Human Services (HHS) in Donald Trump’s second administration, was publicly derided and discredited as an insane conspiracy theorist throughout Joe Biden’s presidency.
The conduct of governments during the period of history from 2020 to 2023 was so confounding and preposterous that a plethora of bona fide conspiracy theories continued to emerge, reaching a peak with the release of the alleged miracle vaccine, which everyone on the planet was first encouraged (through coaxing and bribery) and then, in some cases, required to line up for, on pain of punishment for failure to comply. Some of the theories were quite creative, asserting, for example, that the shots were introducing microchips into the bodies of the recipients, or would turn them into frogs. But the term antivaxxer was affixed to anyone who declined the shot, whatever their reason, with everyone in that group assimilated and depicted as intellectually inept for defying what were claimed by officials at the time to be the dictates of common sense.
Some people, whether with formal training in science or simply endowed with critical thinking skills, understandably expressed skepticism about the new m-RNA therapy shot which they were told would eradicate the virus, while being simultaneously told that natural immunity was inadequate and that persons who already recovered from the virus would still need to undergo vaccination. Because a vaccine, by definition, exploits the subject’s own immune system, anyone with even a modicum of logical acumen must have understood that the new miracle vaccine, which depended on the immune system itself, would only work as advertised if, in fact, natural immunity was possible. This flagrant contradiction was not recognized or acknowledged as such by inept (or, in some cases, mercenarily corrupt) government officials and public health pundits, but it was the most obvious sign to people yet to be indoctrinated into the COVID cult (or not on the Big Pharma dole) that something was seriously awry.
The “Natural immunity is not possible, but this vaccine is necessary and will save you!” contradiction no doubt inspired some of the ever-mutating and proliferating theories about what was really going on. In Covid-19: The Great Reset, Schwab himself refers to antivaxxers as a dangerous impediment to getting through the crisis, and the term came swiftly to be used to denounce anyone who raised even doubts grounded in logic and science about the wisdom of submitting to an experimental treatment in cases where the person’s chances of death from the virus were quite low, as was true for all healthy young persons, and had already been demonstrated in each particular case of anyone who had recovered from previous infection.
The Pentagon required all service persons to take part in the experimental trial of the mRNA therapy, whether or not they had already recovered from infection. The more than 8,000 troops who refused the shot were discharged without pay in 2021, and the military vaccine mandate was not rescinded until 2023. Since assuming office in 2025, Pete Hegseth, Trump’s new defense secretary, has been apologizing to those persons and attempting to make amends, acknowledging that the order to take an experimental vaccine was in fact illegal and that no one was obliged to follow illegal orders. The true motives and sincerity of the new administration on this matter will be seen in how they treat the persons who suffered vaccine injury as a result of having undergone the procedure, under the erroneous belief that Joe Biden’s secretary of defense, Lloyd Austin, knew what he was doing when he ordered the entire military corps to follow his über-masked, serially vaccinated and boosted example. If the government extends its offer of compensation only to healthy troops, in an effort to woo them back into service, and ignores the persons who were disabled by the vaccine, or the individuals and families wrecked by being plunged precipitously into penury, then it will be safe to conclude that Hegseth’s apology tour is no more and no less than a measure intended to mitigate the ongoing recruitment crisis.
There seemed to be grounds for hope that the United States had managed to extricate itself from the totalitarian clutches of meta-bureaucrats such as Klaus Schwab and their “Fifty Year Plans” for humanity when Donald Trump defeated Kamala Harris (who to this day has pronouns in her profile at X) in the November 2024 presidential election. The new president immediately rescinded all DEI initiatives implemented under Biden and enacted numerous executive orders in an effort to protect women, and restore a modicum of sanity to what had become a surreal situation, by boldly asserting the biological fact that no matter how many body parts a male human being chooses to cut off or modify, every remaining cell in his body will still contain a Y chromosome. Trump also acted swiftly to criminalize the scandalous medical practice of mutilating the genitalia of minors. Both Trump and his vice president, J.D. Vance, repeatedly pronounced that free speech would always prevail in the United States as a fundamental pillar of democracy, and they vociferously denounced the censorship going on abroad.
Vestiges of the New World Order, however, can be seen in the United States, for example, the requirement that all citizens who wish to travel or enter a federal building be in possession of a Real ID. This measure, too, which begins in May 2025, having been planned long ago, in the aftermath of September 11, 2001, bears similarities to some of what was going on during the COVID period, when tracking apps and data collection at borders were nearly ubiquitous. More and more data about citizens continues to be collected by governments, and remnants of the health documentation requirements during the COVID period can be seen in the visas now needed to travel to countries where formerly a passport sufficed. Restriction of movement reached a peak during the COVID period, but the apparatus now exists and with a bit of tweaking could be used to stop anyone, anywhere, from relocating at the caprice of government officials, whoever they may be, and whatever their priorities.
The removal of students from campuses in the United States for daring to speak out against the government’s continuing support of the indiscriminate bombing of Gaza suggests that Trump, like Biden and Harris, supports free speech only so long as it does not threaten his own plans for the country or its satellite state, Israel. The libertarians who voted for Trump were needless to say thrilled when he followed through on his promise to pardon Ross Ulbricht, the founder of Silk Road who had received a double life sentence plus forty years with no possibility of parole. In choosing to vote for Trump, however, libertarians had somehow forgotten or chose to ignore the fact that Julian Assange was thrown into Belmarsh prison under Trump’s watch. (I am aware that many persons vote according to a “lesser evil” calculation, but the fact remains: the worst persecution of Assange occurred under Trump.) The fact that U.S. government drones are now acknowledged to be flying above U.S. skies (they were under Biden as well, although this was denied at the time), reveals that surveillance of residents remains a priority of the ostensibly new administration.
Antiwar activists—some of whom voted for Trump—were hopeful that he was sincere when he promised on the campaign trail not to start but to end wars. Even more welcome, albeit frankly astonishing, was Trump’s assertion on February 13, 2025, not long after having re-assumed the presidency, that he would like to cut the $800 billion Pentagon budget in half and work for the abolition of nuclear weapons. Pacific hopes were swiftly dashed less than two months later when, immediately after hosting Israel Prime Minister Benjamin Netanyahu (for the second time in 2025), Trump announced on April 7, 2025, a new, even bigger, $1 trillion defense budget, accompanied by his customary raving about how splendid the U.S. military will be, thanks to his management.
In a welcome change to citizens concerned about government overreach and the massive federal debt, the Department of Government Efficiency (DOGE), under the direction of Elon Musk, has been purging programs and canceling contracts relating to DEI and other parts of the Schwab “New Normal” agenda, including regulations intended to promote the Green New Deal and expand government power over citizens’ lives. The era of big government, however, is obviously not behind us. Along with his sudden imposition of extreme tariffs and announcement of a shocking 25% increase in defense spending, Trump’s strange fascination with the future possible annexation of Greenland, Canada, and Gaza, does not bode well for the future of free people. The idea that the leader of one country may simply “buy” another country or a part of another country (in the case of Gaza) reflects the very megalomania intrinsic to supra-national organizations such as the WEF and characters such as Klaus Schwab who attempt to impose their will on the rest of humanity.
Setting all of those substantial concerns aside, at the very least we can take solace in the fact that Klaus Schwab is no longer calling the WEF shots and penning flagrantly sophistic pamphlets replete with non sequiturs and gaslighting guidance masquerading as benevolence. Goodbye and good riddance, Herr Professor Doktor Schwab, we will not miss you. Alas, the WEF continues on (funded by not only a congeries of self-interested global corporations, but also NGOs and, by transitivity, unwitting taxpayers), and the danger it poses thus remains. Self-deluded officials named as global thought leaders will continue to comply with the WEF, as was exemplified by former New Zealand Prime Minister Jacinda Ardern, who is explicitly singled out for praise in Covid-19: The Great Reset.
Bureaucrats, for their part, will continue to conduct themselves as bureaucrats do, amassing power, devising new rules and regulations, and imposing arbitrary policies by all means necessary, as we witnessed throughout the COVID era. Peter Brabeck-Letmathe, the recently named interim chairman of the WEF, is a former CEO of Nestlé who famously claimed that people have no right to water. Unbeknownst to many of the millions of people who purchase and imbibe bottled water everyday, much of it derives from government-treated municipal water supplies filtered and then poured into plastic bottles to look as though it was sourced from natural spring wells such as Evian, Perrier, Pellegrino, Gerolsteiner, et al. It is unclear how much power Brabeck-Letmathe will exert, or for how long, but he does happen to look empirically indistinguishable from the super villains depicted in movies, so there is some chance that if he begins spouting out gaslighting prescriptions about how all human beings ought to behave, at least some among us will shudder, turn around and walk away.
COVID VACCINE INJURIES CONFIRMED BY NEW DATA
The HighWire with Del Bigtree | April 24, 2025
Del and Jefferey reveal newly uncovered CDC data tying COVID-19 vaccines to neurological, cardiac, and autoimmune injuries, including brain inflammation and heart complications. As evidence mounts, the failure of health officials to warn the public threatens to shatter what little trust remains.
Battle Space Advancing To Decide Fate of America’s Covid-19 Shot
By Jefferey Jaxen | April 24, 2025
Corporate media articles are now buzzing about the possibility of the U.S. Centers for Disease Control and Prevention (CDC) narrowing, and even reversing, some of its previous Covid vaccine recommendations.
CNN’s commentary from health experts give an impression that even a consideration of narrowing the shot recommendations would be a dangerous endeavor. Yet under their article’s opening paragraph, they let slip the obvious:
“The change would more closely align the US with guidance given in other countries. Unlike countries such as the United Kingdom, Canada and Australia, the US alone recommends an annual Covid-19 vaccine for healthy younger adults and children.”
The U.S. appears to be the anti-scientific outlier in pushing these shots on adults and children.
The move would be made by the CDC’s ACIP committee which is scheduled to meet in June.
POLITICO is warning that the Covid shot may be removed from the childhood vaccine schedule… according to “two people familiar with the discussions.”
The Politico-CNN tag team to shape the battle space on this topic ahead of the anticipated June ACIP meeting is weak at best.
In a recent interview with FOX NEWS host Jesse Waters, HHS head RFK Jr responded by stating:
“The recommendation for children was always dubious because kids had almost no risk for Covid-19.”
He continued:
“We need to give people informed consent and we shouldn’t be making recommendations that are not good for the population.”
There is a real, rapidly growing call from the American public to outright ban the mRNA Covid vaccine from use. Much like ending water fluoridation, states have not waited for the federal government to act on this as 11 are now seeking a formal ban.

The removal of recommendations represents a midrange target on the continuum of potential actions concerning this injectable, liability free mRNA product line.
The bottom line effect if CDC makes good on their recommendation removal for health children and/or adults would secure a near guarantee that any form of school or business Covid vaccine mandate would be a nonstarter.
The recommendation removal would not in any way change the broken compensation program surrounding the Covid shot. The mRNA Covid vaccine, along with other ‘countermeasures’ is covered from legal liability by the PREP Act until 2029.
Currently the ‘black hole’ program those harmed or killed by the shot are funneled into is called the Countermeasures Injury Compensation Program (CICP). It has a 1 year statute of limitations, not from the time one recognizes their vaccine injury, but from the day of injection.
Author of Vaccine Court 2.0 The Dark Truth of America’s Vaccine Injury Compensation Program Wayne Rohde writes of the latest CICP injury payouts:
“Of the 4,111 decisions related to COVID-19, nearly all 4,044 have been denied.”
EU state’s PM issues Covid vaccine warning
RT | April 23, 2025
Slovak Prime Minister Robert Fico has called for an immediate halt to government purchases of Covid-19 vaccines, citing a recent report that found mRNA jabs contain extremely high levels of DNA and substances that were not disclosed by the manufacturer.
Bratislava initially considered outright banning the vaccines when a commission led by Peter Kotlar, an orthopedic doctor and member of the ruling Slovak National Party, published a report in October claiming that the mRNA jabs alter human DNA, have been inadequately tested, and therefore should not be administered until they are proven safe.
Kotlar has also described the Covid-19 pandemic as an “act of bioterrorism” and a “fabricated operation,” and has accused vaccine manufacturers Moderna and Pfizer of turning vaccinated people into “genetically modified organisms.”
His report, however, was met with significant pushback from opposition parties, as well as former Slovak Health Minister Zuzana Dolinkova, who cast doubt on Kotlar’s qualifications with regard to the subject. She subsequently resigned from her position that same month, citing government backing for an anti-vaxxer and insufficient prioritization of health care.
In a post on X on Wednesday, Fico published a video in which he stated that ignoring the findings of the Kotlar-led commission on the quality of the Covid-19 vaccines would be “extremely irresponsible.”
Fico noted that in March, he instructed the Health Ministry to establish a working group to address the findings of the expert report submitted by Kotlar, but acknowledged that this may not produce results quickly enough.
The prime minister said he would try to resolve the issue in “a reasonable timeframe” and propose during an upcoming government meeting that apart from the working group, the Slovak Academy of Sciences (SAV) would also be asked to conduct a quantitative analysis of the presence of DNA and other substances in the vaccines.
Fico also suggested that the government should inform the population about the “serious findings” regarding the jabs. “Although Covid-19 vaccination rates are extremely low, people deserve such a warning,” he said.
The prime minister went on to propose that Slovakia suspend the purchase of additional vaccines from the unspecified manufacturer, which it is obligated to do under a contract signed by the former government in 2023.
Bratislava is still expected to procure nearly 300,000 doses of Covid-19 vaccines in 2025 and 2026, which is estimated to cost around $6.6 million, Fico said, stressing that “until the results of the additional quantitative analysis are delivered, the government should not procure further vaccines from this manufacturer or pay for them.”
How Your Family Doc Became a Vaccine & Drug Enforcement Agent
The rise of pharmaceutical compliance officers in primary care
By Dr. Roger McFillin | Radically Genuine | Apr 3, 2025
Remember when your family doctor was actually your doctor? That quaint historical period when physicians made independent medical judgments instead of reading from pharmaceutical scripts? When they looked at you as a unique human being rather than a collection of compliance metrics needing correction?
Those days are fucking gone.
Today’s primary care physician is something entirely different—a pharmaceutical compliance officer with a prescription pad, a corporate protocol to follow, and overlords tracking their every move. They’ve transitioned from healers to hustlers, from medical professionals to medication pushers, from trusted advisors to glorified drug dealers with better parking.
I recently had a conversation with a pediatrician that exposed the naked truth of modern medicine. He confessed to me—with a mixture of resignation and discomfort—that he was “mandated” to administer the PHQ-9A (depression screening) to every adolescent, and if they scored above a certain threshold, he MUST offer an SSRI antidepressant.
“What if the teen is just going through a breakup or having normal adolescent mood swings?” I asked.
He shrugged helplessly. “Doesn’t matter. If they hit the number on the screening, protocol says I have to offer medication.”
“But you know these drugs more than double the risk of suicidal events in teenagers,” I pressed. “The black box warning exists for a reason.”
His response chilled me: “If something happened to the teen and I didn’t follow protocol—if I didn’t offer the medication—I could be held liable. My hands are tied.”
And there it was—the perfect analogy hiding in plain sight. This highly educated physician with years of training wasn’t making independent medical decisions. He was a street-level drug dealer who feared what would happen if he didn’t move enough product for his overlords. The corner pusher fears his supplier’s enforcers; the modern physician fears “liability” and “protocol violations.” Different vocabulary, identical dynamic.
Primary care has been transformed from a healing profession into a pharmaceutical distribution network with doctors serving as glorified vending machines in white coats. They’re the street-level dealers in the medical-industrial complex, pushing products with the ruthless efficiency of a cartel but with better branding and tax benefits.
The parallels between how primary care physicians push psychiatric drugs and vaccines are so perfect they deserve admiration from a purely marketing perspective. It’s the same hustle with different packaging—one comes in pill form, the other in a needle, but the script is identical.
The SSRI Hustle
God forbid you or a family member is unfortunate enough to schedule a routine checkup during a particularly bad week. Walk into that sterile exam room while grieving a loss, stressing about work, or just experiencing one of life’s inevitable rough patches, and you’ll walk out with a ‘mild to moderate depression’ diagnosis faster than you can say ‘pharmaceutical kickback.
Within minutes, you’re handed a questionnaire with loaded questions like: “Feeling bad about yourself or that you have let yourself or your family down or that you are a failure?” (You just watched your ex’s vacation photos on Instagram while eating ice cream for dinner in your unwashed sweatpants, so… is this a trick question?)
Answer honestly, and congratulations! You’ve just self-diagnosed with “mild to moderate depression.”
You mean what we used to call sad?
Your doctor spends approximately 90 seconds validating this with probing questions like “And how long have you felt this way?” before reaching for the prescription pad.
“I think Lexapro would really help take the edge off,” they say with practiced compassion, already halfway through writing the prescription. “It will balance your brain chemicals.”
But it’s when you express hesitation that the real sales pitch begins—fear. This is where doctors transform into pharmaceutical fear merchants:
“You know, untreated depression can be very serious,” they warn ominously. “It can worsen over time. It can affect your relationships, your work, your entire life. Depression is a serious medical condition—in fact, it’s the leading cause of disability worldwide.”
The implication hangs in the air like a guillotine blade: refuse this medication, and you’re gambling with your life. They may even pull out the suicide card: “Depression can lead to suicidal thoughts if left untreated.” The cosmic irony of using suicide as a scare tactic to prescribe drugs with black box warnings about increasing suicidal ideation seems lost on them.
For teenagers, the fear tactics are directed at parents. “You don’t want to take chances with your child’s mental health, do you?” they ask, making parents feel like monsters for questioning whether their teen’s temporary sadness requires a medication that doubles their risk of suicidal events.
This isn’t medical counseling. It’s emotional manipulation through fear—the same tactic used by predatory salespeople in every industry. “Better safe than sorry” becomes the catch-all dismissal of legitimate concerns about medications with profound risks and modest benefits.
What they don’t mention:
The “chemical imbalance” theory of depression was thoroughly debunked years ago, joining phrenology and bloodletting in medicine’s hall of shame. SSRIs have never proven to be clinically meaningful beyond placebo.
Complying with their prescription pad evangelism could result in permanent sexual dysfunction—as in forever, as in the rest of your life.
Withdrawal can be so brutal and protracted that patients often mistake it for “proof they need the medication” rather than recognizing it as drug dependence.
And here’s the cosmic punchline: in the 4-6 weeks it takes for these medications to supposedly “work,” most situational “depression” would have naturally improved anyway.
When that happens?
The doctor smugly nods and thinks, “See, the drugs I prescribed fixed them!” Never mind that time, human resilience, and your own natural healing did all the heavy lifting while the medication was just along for the expensive, side-effect-laden ride.
The Vaccine Hustle
Now let’s watch the vaccine version of the same performance:
You visit for a completely unrelated issue—perhaps a sprained ankle or a skin rash. Before addressing your actual concern, your doctor casually mentions, “I see you haven’t had your COVID or flu shot this year.”
The framing is already perfect—you’re “behind” on something, implying non-compliance with an expected standard. Your medical record has been flagged for a deficiency that needs correcting, like a car overdue for an oil change.
Express hesitation, and witness the same script unfold: “These vaccines are very safe and effective. Side effects are usually just a sore arm or mild fatigue for a day.” (Myocarditis? Menstrual disruptions? Neurological issues, complete hijacking of my immune system? Those are so rare they’re not worth mentioning, apparently.)
Ask about actual risk reduction—like how the flu vaccine isn’t efficacious and doesn’t prevent you from contracting the flu—and watch them shift uncomfortably.
Why would I even risk Guillain–Barré syndrome for this Doc? I am healthy and not that scared of the flu? Regardless of the low risk of complications… why even take that risk?
Dare to question whether a perfectly healthy 17-year-old who already recovered from COVID needs an experimental mRNA intervention that doesn’t prevent transmission—and has now been shown to actually INCREASE susceptibility to infection over time, not to mention the myocarditis risks, menstrual disruptions, and other “rare” side effects conveniently minimized in the sales pitch—and watch their face transform before your eyes.
First comes the reflexive smile-cramp, that frozen rictus of medical authority being questioned. Then the slightly widened eyes as they process your heretical departure from the script. Finally, that subtle hardening around the jaw as they shift from healthcare provider to pharmaceutical enforcement officer.
It’s like watching someone toggle between “friendly neighborhood doctor” and “COVID compliance commissar” in real-time, all because you had the audacity to weigh risks against benefits for your own child.
But regardless of whether they’re pushing pills or jabs, we see the identical sales pitch every time—a masterclass in pharmaceutical propaganda. They dramatically exaggerate even the most microscopic potential benefits while feverishly minimizing, dismissing, or flat-out denying any risks with the practiced ease of a seasoned con artist. Watch them transform a 1% absolute risk reduction into ‘90% effective!’ while simultaneously downgrading ‘known serious adverse events’ to ‘extremely rare side effects that aren’t worth discussing.’ It’s as if they’ve never read a single page of the actual scientific literature on the subject.
Spoiler alert: they haven’t.
Most haven’t ventured beyond industry-funded continuing education modules and pharmaceutical company press releases since medical school. The journal articles gathering dust in their mental libraries are pharmaceutical marketing materials disguised as science, cherry-picked datapoints that support the sales pitch while burying inconvenient truths beneath statistical sleight-of-hand. Their ‘expertise’ is just regurgitated talking points from the last drug rep who bought them lunch.
Your Doctor Now Reports to Corporate Masters
The corporate takeover of medicine didn’t happen overnight—it was systematically engineered, with the Affordable Care Act delivering the knockout blow to independent practice. While marketed as expanding “healthcare access,” Obamacare buried small practices under an avalanche of regulatory requirements, EHR mandates, and compliance costs that made independence financially impossible.
Before the ACA, over half of physicians owned their practices; today, that number has plummeted below 30%. The rest were forced to sell out to corporate healthcare systems where their compensation and job security now depend on following protocols—including pharmaceutical prescribing patterns and vaccination targets—established by administrators who’ve never touched a stethoscope.
Your family doctor didn’t willingly transform into a pharmaceutical enforcement agent; they were legislated into compliance, their medical autonomy sacrificed on the altar of corporatized healthcare while maintaining the illusion of independent judgment.
Primary care healthcare professionals are now following protocol with the unquestioning obedience of a first-grader desperate for a gold star sticker. It makes you wonder how many who flock to primary care medicine were those perfect little rule-followers their entire lives—the ones who color-coded their highlighters in medical school, memorized every algorithm without asking why, and spent their formative years as professional hoop-jumpers. The straight-A students who never risked a teacher’s disapproval, never colored outside the lines, never questioned authority figures even when those figures were demonstrably wrong. The ones whose entire identity became wrapped up in following instructions perfectly to achieve the next credential, the next white coat, the next professional validation.
Is it any surprise that these same personalities now cling to protocols like religious scripture, unable to exercise independent clinical judgment when a human being’s complex situation doesn’t fit neatly into their laminated flowchart? Critical thinking requires the courage to ask uncomfortable questions—a skill that was systematically extinguished in these pristine academic specimens long before they wrote their first prescription
Next time your primary care physician tries to prescribe you an SSRI for being human or jab you with the latest pharmaceutical subscription service, remember: you’re not a patient—you’re a customer they’re trying to upsell.
Their script may be polished, but your bullshit detector doesn’t need a medical degree to function properly. Ask the uncomfortable questions they’re afraid to answer. Demand actual data, not rehearsed talking points. Walk out if necessary.
Find the rare physicians who still practice medicine instead of pharmaceutical compliance. And if your doctor looks horrified when you decline their latest pill or shot, smile sweetly and say, “Don’t worry, I’ll make sure my chart notes that YOU failed to convince ME—not the other way around.”
After all, the most rebellious act in modern healthcare isn’t refusing treatment—it’s insisting on informed consent in a system designed to eliminate it.
Your body, your mind, your choice. No prescription required.
RESIST
Pregnant women deserve better than “trust us” science
A major study has been used to reassure pregnant women that Covid-19 vaccines are safe. But the data behind the claim are fatally flawed.
By Maryanne Demasi, PhD | April 12, 2025
In medicine, few assurances carry more emotional weight—or greater responsibility—than the claim that something is “safe during pregnancy.”
Pregnant women are justifiably cautious about what they expose themselves to during this vulnerable time, and history has given them every reason to be.
The thalidomide disaster, diethylstilboestrol (DES), and other cautionary tales have shown what can happen when scientific rigour is sidelined in favour of commercial interests.
So, when a new study published in Pediatrics – the official journal of the American Academy of Pediatrics – claimed that Covid-19 vaccination in early pregnancy was safe, it came with an air of authority and reassurance.
News headlines followed suit, and public health recommendations continued to promote the vaccine’s safety in pregnancy.

But scratch the surface of this study, and something starts to unravel.
Not only are the data unverifiable and privately sourced, but the study contains a fatal flaw that renders its conclusions virtually meaningless.
The fatal flaw
The study analyzed 78,052 pregnancies that ended in a live birth—but left out 20,341 pregnancies that ended in miscarriage or other non-live outcomes.
That’s not a minor oversight.
The very purpose of studying vaccine safety in pregnancy is to assess whether exposure in utero leads to adverse outcomes—like miscarriage, birth defects, or foetal death. Yet one-fifth of the pregnancies were excluded from the analysis, removing exactly the kind of outcomes the study was supposed to detect.
This introduces what’s known as live-birth bias—a selection bias that arises when research includes only live births, disregarding the possibility that harmful effects may have caused some pregnancies to end prematurely.
Put plainly, if you only study babies who made it to birth, you’re ignoring the ones who didn’t—and any harm that may have played a role.
Even the study’s authors acknowledge this limitation, conceding that the exclusion “could lead to an underestimation of identified outcomes.” Still, they move forward to conclude there’s no association between the vaccine and birth defects.
Omitting over 20,000 pregnancies isn’t just a technicality – it’s a fatal flaw.
If even a small fraction of those pregnancies ended in miscarriage or birth defects linked to vaccination, the entire outcome could tip the other way.
Commercial data with no accountability
Then there’s the source of the data itself—a point entirely overlooked.
Rather than using clinical records from hospitals or national birth registries, the study relied entirely on a commercial database from Merative® MarketScan® Research Databases.
These databases are vast, aggregating de-identified insurance claims, prescriptions, lab results, and hospital records from more than 263 million Americans. But they are also privately owned, and their inner workings are entirely opaque.
Researchers using MarketScan data cannot verify whether the patients are real or theoretical, whether records have been altered, or how the data has been cleaned or processed before delivery.
In essence, they are working with a black box, one that comes with no guarantee of integrity.
Experts have already noted that the data from this unverified source shows signs of being unreliable.
The authors ran 93 separate statistical tests to look for differences in outcomes like birth defects. By chance alone, you’d expect a handful to be statistically significant. But none were.
The probability of that happening randomly is just 0.8%—a sign that the dataset may have been fabricated, or that its integrity is in question.
When two of the study authors – Dr Stacey Rowe and Dr Annette Regan – were asked if they had verified the authenticity of the MarketScan database—that is, if they could confirm these were ‘real’ patient data—they did not respond.

L: Dr Stacey Rowe, R: Dr Annette Regan
This isn’t a hypothetical problem.
The medical literature has already been rocked by the Surgisphere scandal, where fraudulent hospital datasets were used to produce papers in The Lancet and The New England Journal of Medicine.
Those papers were eventually retracted, but only after independent researchers demanded to see the raw data and were denied – the data were likely fabricated.
Reassurance without evidence
Despite these glaring problems, the study’s conclusions are being used to reassure pregnant women.
In Australia, for example, the government’s official guidance recommends Covid-19 vaccination in pregnancy, stating that the “recommendations for pregnant women are the same as the general population.”
This, despite the fact that pregnant women were excluded from the pivotal clinical trials and no randomised studies have ever been completed to assess the vaccine’s safety in early-pregnancy.
The result is a landscape where pregnant women are asked to make a “shared decision” with their doctors—based on scientific literature that’s increasingly built on unverifiable data, flawed assumptions, and little to no independent scrutiny.
We are drifting into a new era where conclusions are based on data that sit behind corporate firewalls. An era where trust is expected, but no longer earned.
The Pediatrics study is a case in point.
It carries the imprimatur of authority, published in the flagship journal of the American Academy of Pediatrics. But, in reality, the analysis was based on commercial datasets that cannot be independently verified, and a methodology that systematically excludes the very outcomes it was supposed to assess.
This isn’t just bad science—it’s misleading by design.
And when it comes to pregnancy, where the stakes are literally life and death, that kind of scientific chicanery is a betrayal.
Pregnant women deserve better than a “trust us” approach to medicine.
They need full access to the data, honest communication about uncertainties, and above all, respect for their right to make informed decisions based on real evidence, not selective reporting.
Until that happens, we should remain sceptical of any study that asks us to believe in the evidence without seeing it.
Did Head of CDC Vaccine Safety Office Delete COVID Vaccine Injury Records?
By Michael Nevradakis, Ph.D. | The Defender | April 11, 2025
A key official at the Centers for Disease Control and Prevention (CDC) responsible for monitoring vaccine safety and reports of vaccine injuries may have mishandled or deleted official records subpoenaed by Congress, Sen. Ron Johnson (R-Wis.) alleged earlier this week. The New York Post first reported the story on Thursday.
Dr. Tom Shimabukuro, director of the CDC Immunization Safety Office, maintained the records in question. Shimabukuro previously authored a key paper and participated in public messaging claiming the COVID-19 vaccines were safe and effective for pregnant women.
Johnson, chairman of the U.S. Senate Permanent Subcommittee on Investigations, requested the records in a subpoena sent in January to the U.S. Department of Health and Human Services (HHS). The subpoena pertained to an investigation into internal COVID-19 vaccine safety communications.
According to the New York Post, the subpoena led HHS to discover “potential discrepancies” in the emails maintained by Shimabukuro.
“HHS officials recently informed me that Dr. Shimabukuro’s records remain lost and, potentially, removed from HHS’s email system altogether,” Johnson wrote in a letter he sent earlier this week to U.S. Attorney General Pam Bondi, FBI Director Kash Patel and HHS Principal Deputy Inspector General Juliet Hodgkins.
Johnson called Shimabukuro’s possible mishandling of his official records “highly concerning.”
Journalist Paul D. Thacker, a former U.S. Senate investigator, said, “Every American should be concerned about government scientists deleting or hiding federal information to shape a political agenda. That information belongs to the taxpayers.”
Nebraska chiropractor Ben Tapper, whose questioning of the COVID-19 vaccines led the Center for Countering Digital Hate to add him in 2021 to its “Disinformation Dozen” list of the “leading online anti-vaxxers,” said he was “not surprised” by Johnson’s allegations.
“For years, I’ve seen patterns like this before regarding vaccine safety data. The public health establishment often prioritizes profits over people and continuously seems to protect the lies over the truth. The idea that critical records might vanish — whether through negligence or intent — fits a familiar playbook,” Tapper said.
California attorney Rick Jaffe said Johnson’s allegations are “troubling, but not surprising, given longstanding concerns about transparency at the CDC.”
In response to a Freedom of Information Act (FOIA) request last year, the CDC told Children’s Health Defense the agency has no records of certain internal email communications relating to the agency’s follow-up investigation of safety signals associated with COVID-19 vaccines.
HHS, CDC and Johnson’s office did not respond to requests for comment.
Missing records ‘could contain unfiltered insights’ into vaccine adverse events
Citing an unnamed aide from Johnson’s office, the New York Post said it is unclear which specific records are missing. But according to Johnson’s letter, Shimabukuro’s role included “monitoring adverse events relating to the COVID-19 vaccines.”
Tapper said Shimabukuro may have been “handling sensitive data on adverse events linked to the COVID-19 vaccines,” including data from the U.S. government-run Vaccine Adverse Event Reporting System (VAERS) and the V-safe database, as well as studies, raw data and internal communications on vaccine-related safety signals.
Tapper said:
“These records could contain unfiltered insights into side effects that were downplayed or unresolved during the pandemic. For example, I’ve seen cases in my practice where patients developed symptoms like persistent fatigue or heart palpitations post-vaccination, yet struggled to get clear answers from authorities.
“Missing records could hide similar signals, undermining efforts to validate patient experiences or refine vaccine protocols.”
Internal medicine physician Dr. Clayton J. Baker said, “Such records would likely be very damning to all CDC officials who perpetuated the false ‘safe and effective’ narrative about the COVID-19 vaccines from 2021 until the present.”
“Given how damning any evidence of ignored or falsified safety signals would be, I think it is highly likely that Biden-era officials might try to destroy such records if they could. Better to be accused of destruction of federal records than to be charged as an accessory to mass negligent homicide,” Baker said.
In an April 2023 presentation to the CDC Advisory Committee on Immunization Practices, Shimabukuro claimed that surveillance conducted by international regulatory and public health partners “has not detected a safety concern for ischemic stroke following bivalent COVID-19 mRNA booster vaccination.”
Yet, a peer-reviewed study published in November 2024 found that mRNA COVID-19 vaccines pose a 112,000% greater risk of brain clots and strokes than flu vaccines, and a 20,700% greater risk of those symptoms than all other vaccines combined. The study called for a global moratorium on mRNA vaccines.
In 2021, Shimabukuro was the lead author of a study in The New England Journal of Medicine (NEJM) on the safety of COVID-19 vaccines for pregnant women. The study concluded that “preliminary findings did not show obvious safety signals among pregnant persons who received mRNA Covid-19 vaccines.”
However, a peer-reviewed study published in 2022 showed that the authors of the NEJM study performed a “statistical sleight-of-hand” that substantially lowered the miscarriage rate in pregnant women, presenting it as 12.6% instead of 82%.
In a Substack post, epidemiologist Nicolas Hulscher said Shimabukuro’s “potential involvement in the deliberate manipulation of critical safety data on COVID-19 mRNA injections during pregnancy carries grave implications — resulting in immeasurable harm to mothers and their unborn children worldwide.”
Shimabukuro ‘may have violated multiple federal laws’
According to a press release from Johnson’s office, Shimabukuro’s actions, if proven to have occurred, “may have violated multiple federal laws.”
Those laws include the Federal Records Act, which requires federal employees to preserve materials “made or received by a Federal agency under Federal law or in connection with the transaction of public business,” the New York Post reported.
Johnson wrote that the destruction of records subpoenaed by Congress may also be “grounds for contempt of Congress,” which, according to the New York Post, is punishable by up to a six-figure fine and 12 months in prison.
Jaffe said Shimabukuro may also face other penalties. He said:
“Under federal law, he could be charged with obstruction of justice or destruction of official records — risking fines, restitution and up to 20 years in prison. His federal pension could also be garnished to satisfy any judgment against him.
“Beyond criminal penalties, he faces permanent disqualification from federal service and career-ending reputational harm.”
In addition, if records relating to vaccine-injured people are missing or destroyed, impairing their legal cases, “courts could impose evidentiary sanctions or presume the destroyed records were unfavorable to the government,” Jaffe said.
Johnson’s letter also referred to Dr. David Morens, an employee of the National Institute of Allergy and Infectious Diseases who was a close aide of the agency’s former director, Dr. Anthony Fauci. Morens allegedly deleted emails and instructed colleagues to contact him at a personal email account to sidestep FOIA rules.
In his letter, Johnson accused HHS of a “lack of transparency” and failure to investigate the allegations against Morens.
“I had always suspected that Dr. Morens was not the sole evader of federal record-keeping requirements at HHS,” Johnson wrote. “The extent to which HHS officials systemically mishandled, deleted, or destroyed their communications, data, and other information relating to the COVID-19 pandemic and the vaccines must be thoroughly investigated.”
Johnson’s letter asks the FBI, the U.S. Department of Justice and the HHS Inspector General’s Office to investigate the matter, including whether records were intentionally destroyed to “avoid or subvert Congressional oversight or the Freedom of Information Act.”
The letter builds on Johnson’s efforts to investigate COVID-19 vaccine safety.
Earlier this week, Johnson sent letters to the heads of four COVID-19 vaccine manufacturers, requesting they turn over records related to the development and safety of the COVID-19 vaccines and their communications with Big Tech platforms about vaccine-related adverse events.
In November 2024, Johnson wrote a letter to HHS, CDC and FDA, asking the agencies to “preserve all records referring or relating to the development, safety, and efficacy of the COVID-19 vaccines.”
In an October 2023 letter to the then-heads of CDC and FDA, Johnson accused the agencies of an “appalling” lack of transparency regarding COVID-19 vaccine safety signals, depriving Americans of “the benefit of informed consent.”
During the Biden administration, Johnson wrote over 70 letters to HHS officials and its health agencies requesting information on COVID-19 vaccine adverse events and related communications, according to a Jan. 29 press release.
Last year, Johnson hosted a congressional roundtable to discuss the risks of COVID-19 vaccines. Medical experts, political figures, journalists and whistleblowers were among the participants.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
HHS Ousts Peter Marks, Sending Vaccine Stocks Tumbling and Biopharma Lamenting Loss of ‘Ally’ at FDA

By Michael Nevradakis, Ph.D. | The Defender | March 31, 2025
Pharma stocks tumbled today after Peter Marks, M.D., Ph.D., director of the agency within the U.S. Food and Drug Administration (FDA) responsible for authorizing vaccines, resigned under pressure from his new boss, Health and Human Services (HHS) Secretary Robert F. Kennedy Jr.
“If Peter Marks does not want to get behind restoring science to its golden standard and promoting radical transparency, then he has no place at FDA under the strong leadership of Secretary Kennedy,” an HHS official said in a statement.
Shares of Moderna, BioNTech, Novavax and Pfizer declined 11%, 7%, 6% and 2%, respectively, on the news, Fast Company reported. STAT News reported that Marks’ departure “is a worst-case scenario realized” for investors and “a biopharma industry that saw him as an ally.”
“Given Dr. Marks’ influence on the development of biologics and uncertainty as to who will replace him and how his legacy might continue, his departure will create a significant near-term overhang,” William Blair analyst Matt Phipps told Reuters.
The Biotechnology Innovation Organization, an industry lobbying group, said it was “deeply concerned” Marks’ resignation would “broadly impact the development of new, transformative therapies to fight diseases for the American people.”
Brian Hooker, Ph.D., chief scientific officer for Children’s Health Defense (CHD), said the reaction to Marks’ departure on the part of the markets and the pharmaceutical industry is indicative of the influence Big Pharma had over the FDA. He said:
“Marks gave an over $100 billion gift to Pfizer and Moderna via the woefully undertested and outright dangerous COVID-19 mRNA vaccine. So, yes, for the short term, I would imagine that some investors would not like his departure from the FDA.
“Marks’ departure also signals a shift from ‘sick care’ and ‘customers for life’ where, unfortunately, Pharma invests now, to ‘Make America Healthy Again’ where everyone benefits from ending chronic disease in the U.S.”
John Gilmore, executive director of the Autism Action Network, welcomed Marks’ departure. “The American people are well-served by Marks’ resignation.” Gilmore cited the “institutional failure” of the Center for Biologics Evaluation and Research (CBER) “to use the highest standards for evaluating the safety and efficacy of products that are injected in almost all American children.”
Marks has led the FDA’s CBER since 2012 and “played a key role,” The Wall Street Journal reported, in Operation Warp Speed in 2020, leading to the development of the COVID-19 vaccines.
In his resignation letter, Marks wrote: “It has become clear that truth and transparency are not desired by the Secretary, but rather he wishes subservient confirmation of his misinformation and lies.”
Marks’ ‘support of immunizations conflicted with Kennedy’s skepticism’
According to the Journal, an HHS official gave Marks a choice between resigning or being fired. His resignation is effective April 5. Marks wanted to remain in his position, but “his support of immunizations conflicted with Kennedy’s skepticism.”
“Undermining confidence in well-established vaccines that have met the high standards for quality, safety, and effectiveness that have been in place for decades at FDA is irresponsible, detrimental to public health, and a clear danger to our nation’s health, safety. and security,” Marks wrote in his resignation letter.
Marks said he was “willing to work to address” Kennedy’s concerns on vaccine safety, including through a series of public meetings, but that these proposals were rejected. He also accused Kennedy of spreading “misinformation and lies” during the “ongoing multistate measles outbreak.”
But in a post on X, Steve Kirsch, founder of the Vaccine Safety Research Foundation, said that while Marks “claimed he wanted to stop misinformation,” he “refused all offers to meet with the ‘misinformation spreaders’ to settle the question on just who is spreading the misinformation.”
While Marks claimed he was willing to address questions on vaccine safety, he also wrote, “Efforts currently being advanced by some on the adverse health effects of vaccination are concerning.”
One day before Marks’ resignation, Kennedy announced the creation of a new sub-agency under the Centers for Disease Control and Prevention (CDC) to focus on vaccine injuries — part of a broader restructuring of public health agencies, including the FDA.
In February, Kennedy promised that under his watch, HHS and CDC would develop a better system for tracking vaccine injuries.
Earlier this month, Reuters reported that unnamed sources within the CDC said the agency was planning to study the possible link between vaccines and autism. The story triggered negative mainstream news reports claiming the study isn’t needed.
Last week, The Washington Post, citing anonymous sources, reported that HHS had tapped researcher David Geier — a researcher and expert on the connections between toxic exposures and autism — to lead a study of possible links between vaccines and autism. The Post and other media outlets used the opportunity to attack Geier and the need for such a study.
Marks’ resignation also came as the FDA is considering a petition a group of scientists submitted earlier this year, calling upon the FDA to suspend or withdraw the mRNA COVID-19 vaccines.
Marks ‘became a cheerleader for the jab’
Writing on Substack, investigative journalist Maryanne Demasi, Ph.D., said it’s “evident there was a significant clash over vaccine safety” that led to Marks’ resignation. She said Marks’ departure “may be an opportunity for the FDA to refocus on its mission of protecting public health rather than rubber-stamping new vaccine approvals.”
Epidemiologist Nicolas Hulscher agreed. “Those who believe vaccine safety must not be questioned do not belong in our regulatory agencies. When it comes to injectable products, safety is more important than blind faith in vaccine ideology.”
According to The New York Times, while Marks “was viewed as a steady hand by many during the Covid pandemic,” he was criticized “for being overly generous to companies that sought approvals for therapies with mixed evidence of a benefit.”
The Times cited Marks’ role in pressuring two FDA scientists to approve full licensure of Pfizer’s mRNA COVID-19 vaccine in 2021, leading to the researchers’ resignation. Pfizer’s vaccine was fully licensed in August 2021 — one day later, the Biden administration mandated COVID-19 vaccination for military service members.
The rushed licensure of the Pfizer vaccine was the topic of a congressional hearing last year in which Marks testified. In a post on X Saturday, Rep. Thomas Massie (R-Ky.) wrote, “Instead of verifying safety and efficacy of the shots, Marks swept things under the rug and became a cheerleader for the jab.”
“In order to get the vaccines to people in need when thousands of people were dying, we actually allowed the safety to be authorized with just two months of median follow-up, rather than the normal six to 12. But we were confident that that would capture adverse events,” Marks testified at last year’s hearing.
‘It was clear that he did not want to know about our injuries’
While Marks was actively engaged in the licensure of the Pfizer COVID-19 vaccine, he “remained steadfast” in dismissing concerns about injuries related to the COVID-19 vaccines as “misinformation,” Demasi wrote.
In 2023, The BMJ wrote that “more than once” during FDA meetings, Marks “expressed confusion about why it would matter to doctors whether or not regulators acknowledged that a condition might be related to the vaccine.”
Documents CHD obtained last year through a Freedom of Information Act request showed that Marks was aware of COVID-19 vaccine injuries in early 2021 when several vaccine injury victims emailed him for help. Marks blew off scheduled meetings with them.
According to TrialSite News, even though Marks was aware of the growing number of COVID-19 vaccine injuries, “vaccine injury became a political hot potato under the Biden administration,” leading Marks to abandon the vaccine-injured.
Brianne Dressen, co-founder of React19, an advocacy group for the vaccine-injured, sustained serious injuries after participating in a clinical trial for the AstraZeneca COVID-19 vaccine in 2020 and later sought meetings with Marks but was rebuffed.
“Constant emails and calls with Marks … sent while I was in constant pain, literally begging for help, begging for them to help others, begging for a lifeline. A lifeline that never ever came,” Dressen said.
Dr. Danice Hertz, a retired gastroenterologist from California injured by the Pfizer COVID-19 vaccine, also communicated with Marks but said he “brushed off anyone who contacted him regarding vaccine side effects.”
“He systematically refused to hear our pleas for acknowledgment and help,” Hertz said. “This is why the medical community is unaware of these injuries and cannot help us. One would think that the FDA would want to know about serious adverse reactions to the novel COVID vaccines. I can say from first-hand experience that they don’t … It was clear that he did not want to know about our injuries.”
Dressen said it “didn’t matter what we said or how we said it, COVID vaccine injuries were not a priority at the FDA. Didn’t matter if it was safety signals for MIS-V, dysautonomia, neuropathy, tinnitus or reports of suicides. It was never enough. We begged, we pleaded, we pushed as hard as we could, and came up with nothing.”
According to Demasi, Marks instead “blurred the line between regulation and promotion” by participating in FDA videos promoting the COVID-19 vaccines and by authorizing COVID-19 mRNA vaccines for children without sufficient testing.
“Without randomized data regarding clinical outcomes, he repeatedly approved COVID boosters for kids as young as 6 months,” Dr. Vinay Prasad, professor of epidemiology and biostatistics at the University of California, San Francisco, wrote on Substack, calling these “some of the biggest regulatory errors in the 21st century.”
Demasi said Marks “repeatedly pointed to the Vaccine Adverse Event Reporting System (VAERS) as proof of rigorous safety monitoring, yet failed to improve its efficiency.”
During last year’s congressional hearing, Marks claimed that numerous false reports of vaccine injuries are submitted to VAERS, a government-run database. However, he acknowledged, “We probably have not done a good enough job of communicating sometimes the actual numbers of deaths versus what’s in VAERS.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Canadian PM Mark Carney Downplays Role in Freedom Convoy Crackdown Despite Backing Emergency Measures
Carney called protest “sedition” and Urged financial chokehold
By Didi Rankovic | Reclaim The Net | April 1, 2025
Canada’s Prime Minister Mark Carney recently gave a masterclass in the art of political evasion and deflection – all the more “masterful” since one of the arguments he went for was that he is not really a politician.
This unfolded before TV cameras in the area of the 2022 Freedom Convoy blockade, which the authorities led by former PM Justin Trudeau and his Liberals clamped down on using unprecedented measures.
They included invoking the Emergencies Act to target the protesters against restrictive Covid-era policies with anything from extreme vilification to freezing their bank accounts.
“Sedition,” is what Carney decided to brand the civil protest in an op-ed published in the Globe and Mail on February 7, 2022, and, true to his previous roles in Big Finance, proposed to put an end to the protest (he called it “this occupation”) by “choking off the money” that funded it.
Now – given his current “affiliation” with the Liberal party, the new prime minister was asked to send a message to those Canadians who lost trust in the previous cabinet because of its handling of the protest.
Instead of doing that, Carney first sought to “distanced himself from himself” – saying that he has only been a politician for two months, and claiming that he took on his new role because he “knew this country needed big change.”
And he then proceeded to list all the allegedly significant changes achieved during his short time in office so far, thus deflecting from the Freedom Convoy question.
Despite his best efforts to paint himself as no more than a conscientious citizen determined to help his country through difficult times – three years ago this former governor of the Bank of Canada and the Bank of England was an informal advisor to Trudeau.
And he not only accused the Freedom of Convoy protestors of committing “sedition” and those donating to the cause of “funding sedition,” but was also mentioned in the Public Order Emergency Commission documents (which investigated the invocation of the Emergencies Act).
Spoiler: Carney supported that decision, along with the freezing of citizens’ bank accounts because they protested against the government.
But Carney’s failed upward now to become prime minister, and “re-earn trust” – not to mention, introduce “big change.”
Featured Video

Trita Parsi: Iran War Ends Today? Threats of Deporting Trita Parsi
or go to
Aletho News Archives – Video-Images
From the Archives
Iran UN ambassador calls for destruction of all nuclear weapons

Iran’s ambassador to the UN Gholamali Khoshroo
Press TV – March 29, 2017
Iran’s ambassador to the UN Gholamali Khoshroo has called for the total eradication of nuclear weapons.
Khoshroo reiterated Iran’s call during a UN conference aimed at creating a nuclear weapons ban treaty in New York on Tuesday.
“Iran, as a victim of chemical weapons, strongly feels the danger posed by the existence of weapons of mass destruction and is determined to engage actively in international diplomatic efforts to save humanity from the menace of nuclear weapons,” he said.
Khoshroo stressed that Iran is committed to its Non-Proliferation Treaty (NPT) obligations, which include negotiations based on effective nuclear disarmament measures.
He added that several countries continue to ignore international calls and treaties for nuclear disarmament and even continue to increase their nuclear stockpiles. “They do not have political determination to abandon doctrines of nuclear deterrence and nuclear terror,” he went on to say.
Iran’s UN ambassador noted that boycotting the talks by many countries, including the US, shows that the world’s nuclear powers are by no means committed to the eradication of nuclear arms. Britain and France were also among the some 40 countries that did not join the talks.
“We note that prohibition of nuclear weapons must be accompanied by the elimination of such weapons. There can be no doubt that without complete abolition of nuclear weapons, there will be no absolute guarantee against the danger of nuclear war and the use of such weapons,” Khoshroo added.
Blog Roll
 Aletho News
Aletho News- The Crusades – colliding narratives
- Trita Parsi: Iran War Ends Today? Threats of Deporting Trita Parsi
- What Is SIDS?
- DHS docs: Govt bracing for nationwide anti-AI riots, preparing to crack down on dissent
- India signals rethink over West Asia
- Israeli Ex-Navy Chief admits massive damage from Iran missiles
- The strategic arsenal US lost in war against Iran – and why replenishment will take years
- Documents Suggest Fauci Knew COVID Was Created in Wuhan Lab, and mRNA Vaccines Wouldn’t Work
- No return to pre-war status for Strait of Hormuz – Iran’s top diplomat
- Ex-South Korean President sentenced for trying to provoke conflict with Pyongyang
- If Americans Knew
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- Oxfam: More Palestinians killed by Israel across West Bank in last 3 years than previous 17 years combined
- US-Iran ceasefire may be imminent, but will Israel blow it up? – Daily Update
- The Issue of Israel Is Ending Democracy In Michigan
- Israel is stealing homes, livelihoods, and lives in West Bank
- Gaza is not an aberration – Israel planned this genocide decades ago
- Israel is changing the face of Lebanon, mainstream media is normalizing it – 3 articles
- Genocide lobby benefits from EU anti-racist fund
- Watching the World Cup from Gaza
- No Tricks Zone
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
