Much Ado About Nothing
By Todd Hayen | OffGuardian | November 12, 2022
Do any of you think we are over-reacting? I don’t think so, but the sheep-folk certainly do. They claim they are willing to let bygones be bygones and just put it all in the past and get on with life.
I am sure everyone reading this is aware of the bombshell editorial The Atlantic dropped recently with their amnesty nonsense. I don’t think I have been more livid reading an article since the days of seeing piece after piece about how effective masks are against viral transmission.
I won’t comment on The Atlantic blather directly here, as there have been many fine responses to it, but wow, what a piece. So typical of a bully trying to pretend he loved his victims all along when he knows he is cornered and about to be punished. One last punch disguised as a kiss.
I just got back from a little cruise. Major ports were Barcelona, Rome, Florence, Monaco, and a smattering of little French and Italian hideaways. I had mixed feelings about going, but realized that if this tsunami we all see coming a few miles off the shore has the potential of wiping out most travel in the foreseeable future, I figured I might as well get something in before the onslaught.
It was nice in a lot of ways, as would be expected, but in other ways unusually disconcerting. For one thing, very, very few people had masks, and thus there was a palatable scent in the air of “Covid is a thing of the past.”
One would think this was a good thing, but instead it exuded a very clear vibe of denial.
Oddly enough, not wearing masks, and believing Covid to be over, to me is just another example of compliance to authority.
I know that seems a stretch, but if Covid were real, coupled with the truth that the vaccines do not work, and we were told again and again that there would be no natural herd immunity without a working vaccine, and we still hear of infections rising, variants being created, and hospitals becoming over crowded, why would people think the disease just died and disappeared? The reason is because we were told it was over.
We were told we suddenly didn’t need masks, that we could party with friends, vaxxed or unvaxxed, that we could gather in huge crowds, get on cruise ships (no one even cared that I was unvaccinated.) We were told what was true, what was real and what to worry or not worry about. And like sheep, most people blindly followed.
So shouldn’t I be happy? If I were, it would be for all of the wrong reasons. It is true we are all happy when the slave owner puts down the whip. Whip or not, however, we are still slaves.
I, too, bask in the sun of my controlled freedom—I went on a cruise didn’t I? After two years of not being “allowed to” — so I am just as guilty of this sort of compliance. I am one step closer to truth though; I know this offer of freedom is a tactic, a ploy, and a ruse.
I’ll take a scrap of bread when it is offered, but I will not succumb to complacency and forgive my master for his cruelty when he behaves, albeit for just a moment, as my friend. Most everyone else seems fine to let bygones be bygones.
I am not, and I suspect most of you reading this are not as well.
The great danger I see here in the masses just carrying on in complacent forgiveness is that they are encouraged to stay blind. Surely if they speak out against the atrocities that the world has experienced over the past three years they would quickly be categorized as a trouble maker, a pariah, and a misfit.
“Just get over it, man, it’s all over.”
Is it? No, of course not, you and I know that, and it is all still going on in various ways under the covers now, in the dark recesses of the culture: persecutions, continued efforts to vaccinate, and particularly vaccinate children, warnings of an “upcoming dark winter” where restrictions will come back into the mainstream. On and on, you know what I am speaking of.
However, the mass attitude now, as per The Atlantic piece, is “nothing all that much really happened.”
No one died unnecessarily due to the Covid response, no one got sick, no one lost their job or their livelihood, no one suffered socially (particularly children wearing masks in school), no one suffered educationally, nothing bad really happened.
If you are still pissed about all that DID happen, then you are overreacting… much ado about nothing.
So get over it, forget and forgive.
Not everyone in the world has read that article, but what I saw in Europe, it seems that most people, at least on physical observation, are basically taking on that attitude.
It breaks my heart.
I think about the countless mothers sitting by their children in countless hospitals nurturing them through a totally unprecedented heart incident.
I think of the countless families standing together at the funeral of a loved one, dead prematurely from a heart attack, blood clotting, or cancer—cause unknown, unless you want to apply the newly created diagnoses, “Sudden Adult Death Syndrome.” What the hell is that?
A novel disease and now a common cause of death? Easy peasy explanation, eh? I think of the countless numbers of people suffering from a myriad of strange afflictions, which suddenly appeared out of nowhere.
I think again of countless people having suffered unconscionably, and pointlessly, after losing their jobs, their businesses, their life savings, and their livelihood—the countless children with lower IQs, and those who have suffered social retardation due to the mask mandates, social distancing, and mandatory online teaching at home with no socialization at all.
I could write 100 pages describing all of this—but most people don’t know, and if they do, don’t care, or just attribute all of this horror to the “cost of living—some are lucky in life, some are not.”
During my recent cruise not a word was uttered about any of this, thousands of people were encountered walking the streets of Rome, Florence, Barcelona, all laughing, eating, drinking, playing. While just beneath their feet, hidden a foot underground, there are skulls and bones of the fallen—all forgotten, and the perpetrators all forgiven.
When I was occasionally shaken from my self-induced and compliant vacation reverie, my heart ached talking to all of the young vibrant crewmembers on our ship.
I would hear of their plans to be married, create families, further their careers and live fully their vibrant lives—followed with the admission that they all had to be vaccinated to get their current jobs on the ship.
What really lies ahead for these beautiful children of God so innocent and full of life? I would shake my head, “maybe none of this is true, and maybe I am making more of it than it really is. Maybe they are right, and it really wasn’t that bad, just a mistake made here and there that we really could get over. It is all fine… let’s move on.”
Then a bone cracks under my foot—just a few inches from the surface of awareness—the truth. And I slip back into reality.
Dr. Clare Craig On The Three Key Factors Of The Pandemic
The Fat Emperor – Ivor Cummins | November 9, 2022
Dr. Clare Craig is one of the best pathologists out there, and deeply understands the scientific details of the pandemic – and I caught her in person at the International health congress in Portugal – all scientific talks are here or will be uploaded shortly https://odysee.com/@MartaGB:2
Good News on Omicron Outcomes from Prison
Captive Environment Allows Real Look at Risk for Hospitalization and Death
By Peter A. McCullough, MD, MPH | Courageous Discourse | November 8, 2022
Prisoners and staff are a prototypical congregate group amenable to epidemiologic study and in the setting of the SARS-CoV-2 outbreak, ideal for study of the patterns of spread and risk for serious outcomes.
Throughout the pandemic, review and interpretation of peer-reviewed manuscripts in widely read journals has required careful review of data in supplementary tables. The conclusions by the authors in many papers must be ignored given the heavy bias for all journals to “promote” mass vaccination. For example, thus far, there has not been a single paper in the New England Journal of Medicine that has concluded COVID-19 vaccines are unsafe, or not indicated, or do not have a favorable risk to benefit ratio.
Prior to COVID-19 for any new therapy or surgery, there are always divergent views where some papers conclude an intervention is beneficial and others do not. Disagreement is normal in medicine. The pervasive heavy-handed government intelligence community and public health agency operations have biased the medical journals to publish a one-sided story on COVID-19 vaccination. The paper by Chin et al, in the New England Journal of Medicine is a perfect example.[i] They studied 59,794 residents and 16,572 staff, using data collected from December 24, 2021, through April 14, 2022. Buried in the supplemental tables are important data on the real risk of hospitalization and death with the Omicron variant in prisoners characterized by whether they had prior COVID-19 and how many doses of a vaccine they had received.
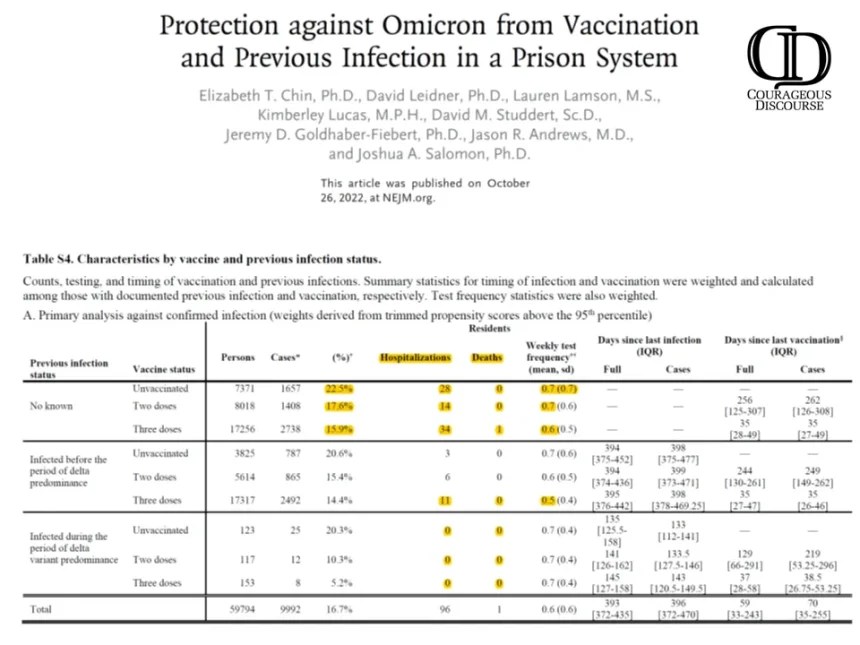
Chin ET, Leidner D, Lamson L, Lucas K, Studdert DM, Goldhaber-Fiebert JD, Andrews JR, Salomon JA. Protection against Omicron from Vaccination and Previous Infection in a Prison System. N Engl J Med. 2022 Oct 26. doi: 10.1056/NEJMoa2207082. Epub ahead of print. PMID: 36286260. Supplemental Tables.
As shown, there is a negligible risk of hospitalization and death with Omicron infection. Specifically, there were zero deaths in the unvaccinated. To demonstrate how far off-base authors and editors are on interpretation, take a look at the paper’s conclusions:
“Our findings in two high-risk populations suggest that mRNA vaccination and previous infection were effective against omicron infection, with lower estimates among those infected before the period of delta predominance. Three vaccine doses offered significantly more protection than two doses, including among previously infected persons.”
My conclusions are considering natural immunity status, COVID-19 vaccination provided no meaningful protection against hospitalization and death with Omicron. Based on these data, a rational prison physician or health administrator would conclude that bivalent boosters for Omicron are not clinically indicated nor medically necessary. So next time you see headlines regarding a journal article, look for a second opinion from “Courageous Discourse” or other reliable stacks and sources of analysis.
[i] Chin ET, Leidner D, Lamson L, Lucas K, Studdert DM, Goldhaber-Fiebert JD, Andrews JR, Salomon JA. Protection against Omicron from Vaccination and Previous Infection in a Prison System. N Engl J Med. 2022 Oct 26. doi: 10.1056/NEJMoa2207082. Epub ahead of print. PMID: 36286260.
Why Are People Losing Confidence in Vaccines?
BY DR DAVID PATON | THE DAILY SCEPTIC | NOVEMBER 8, 2022
A new peer reviewed article in the journal Vaccine has been published comparing surveys data on attitudes to vaccination from before the pandemic with attitudes now.
The authors report that “paradoxically, despite the success of COVID-19 vaccination campaigns, vaccine confidence has significantly declined since the onset of the pandemic”.
I am not quite sure why the authors appear so surprised at their result but a clue can be found in their use of the word “despite”. In many countries the “success” of the COVID-19 vaccination campaign relied in large part in pressuring, bullying and sometimes coercing people to get vaccinated.
Now if governments tell you that getting vaccinated is in your best interests, but that nonetheless those who choose not to get vaccinated will be pilloried in the press and on social media, barred from participating in normal everyday activities and, in some cases, sacked from their employment, perhaps we should not be surprised that people start to doubt whether those governments really do have their best interests at heart.
And those doubts have substance behind them. From a very early stage, it was clear that for many people, the known risks from vaccination probably outweighed any likely benefit. This was most obvious for those who had already had Covid (and for whom the marginal impact of vaccination in preventing a further infection was small), for groups who faced very low risks of serious illness if they contracted Covid and especially for young males for whom vaccination seems to be bring additional risks of heart problems.
But instead of acknowledging that Covid-19 vaccines may make sense for some people and not everyone, too many public health officials, scientists and politicians have systematically downplayed immunity from previous infection, brushed aside concerns over side effects and dismissed concerns that the roll out to the whole population was rushed given uncertainty over long term effects.
The latter was a particularly serious error. Right from the start of the roll out the public was assured that the vaccines had been thoroughly tested. Yet in May 2021, the Government decided to stop providing the AstraZeneca vaccine to under 40s due to the relatively high rate of blood clots. That decision would have been little consolation to the families of the 73 people whose deaths the MHRA report as being linked to that vaccine.
Rather than taking that as a lesson, authorities around the world doubled down and rolled out vaccine mandates, passports and travel restrictions as a way of twisting more arms into receiving the jab. Ironically, these measures were aimed primarily at young people for whom the benefits of vaccination were lowest and (particularly for males) the risks seem highest.
The official rationale for these policies was that vaccination would help protect others from being infected. We now know that there was never any evidence to back this up. And when official data started to suggest that the vaccinated may be getting infected at similar if not greater rates than the unvaccinated, the response of some journalists was not to probe further and investigate but to encourage the authorities to suppress the data. Truly, you could not make it up.
Researchers such as Alex de Figueiredo from the London School of Hygiene and Tropical Medicine warned at the time that coercion was likely to lead to a loss of trust in vaccination more generally. With the latest research paper, we have firm evidence that this is indeed the case.
It is not unreasonable to conclude that the most dangerous ‘anti-vaxxers’ over the past two years have not been fringe conspiracy theorists but governments and the public health establishment itself.
It’s a sorry state of affairs, but where do we go from here? Well public health leaders could start by switching tack. Rather than setting out to persuade everyone to get vaccinated, they could concentrate on providing good information about benefits and risks to help people decide whether vaccination is right for them. If, at the same time, they start to engage honestly with those who have suffered side effects and acknowledge the high level of uncertainty that still exists in the evidence, perhaps they can begin to regain some of the trust they have so negligently lost.
David Paton is Professor of Industrial Economics at Nottingham University Business School.
Pfizer Press Release on New Bivalent Booster Raises More Questions Than It Answers
By Madhava Setty, M.D. | The Defender | November 9, 2022
Pfizer last week announced what some media outlets called “good news” about its COVID-19 bivalent booster, for which the U.S. Food and Drug Administration (FDA) in August granted Emergency Use Authorization on the basis of testing conducted on eight mice.
In a press release, Pfizer summarized the updated data from its phase 2/3 clinical trial on the Pfizer-BioNTech Omicron BA.4/BA.5-adapted bivalent COVID-19 vaccine:
- Bivalent booster elicited approximately 4-fold higher neutralizing antibody titers against Omicron BA.4/BA.5 sublineages compared to the original COVID-19 vaccine in individuals older than 55 years of age.
- One month after a 30-µg booster dose of the bivalent vaccine, Omicron BA.4/BA.5-neutralizing antibody titers increased 13.2-fold from pre-booster levels in adults older than 55 years of age and 9.5-fold in adults 18 to 55 years of age, compared to a 2.9-fold increase in adults older than 55 years of age who received the original booster vaccine.
- Safety and tolerability profile of bivalent booster remains favorable and similar to the original COVID-19 vaccine.
In simplest terms, the bivalent booster increased antibodies to the Omicron sublineages by a factor of 13.2, whereas the original booster increased them by a factor of only 2.9.
This increase was seen only in people over age 55.
Although the new booster produced a more modest increase (9.5 fold) in antibodies in the younger age group (18-55), Pfizer chose not to report what the response was in the age-matched group who received the original booster.
Did the bivalent booster offer any advantage in people younger than 55? Pfizer’s press release sidesteps this important question by focusing only on the results in the 55 or older cohort.
Dr. Ugur Sahin, CEO and co-founder of BioNTech, stated:
“These data demonstrate that our BA.4/BA.5-adapted bivalent vaccine works as conceptually planned in providing stronger protection against the Omicron BA.4 and BA.5 sublineages.”
By “these data” Sahin is referring only to those 55 or older as no comparative results were given in the 18-55 group. But how does he know that this rise in antibody levels will provide “stronger protection against the Omicron BA.4 and BA.5 sublineages?”
Were there any clinical outcome differences in terms of COVID-19 infections? None were recorded. Neither were any recorded in the preliminary data from the same study reported in a previous Pfizer press release.
This was likely why Sahin cautiously stated at that time:
“These preliminary findings are consistent with our preclinical data showing a substantial increase in the neutralizing antibody response against the Omicron sublineages BA.4 and BA.5.”
At what point does an “increase in the neutralizing antibody response” confer “stronger protection?”
Sahin doesn’t know — and neither does the FDA, which insisted that despite this uncertainty, the agency had enough grounds to cajole/compel/coerce those who acquired SARS-CoV-2 antibodies from a previous bout with COVID-19 to get jabbed anyway.
Questions about the two groups
The 36 people over age 55 who received the new bivalent formulation used in this comparison were taken from a larger pool of participants. They were “evenly stratified between those who had evidence of prior SARS-CoV-2 infection and those who did not.”
Furthermore, Pfizer informed us that the “control” group — those people who received the original booster formulation — were also a subgroup of participants but were taken from a different study “while ensuring the same equal stratification.” This group is thus called a “comparator group” and is not a true control group.
How did Pfizer decide which participants to use from the two separate studies?
Pfizer assured us the trial participants they used in the comparative group were “randomly selected.” However, we are not told how Pfizer selected those in the bivalent booster cohort.
Did they choose participants who had particularly high antibody responses? Were those in the comparative group actually chosen randomly — or were they chosen because of their particularly low responses?
In fairness, we are dissecting a press release and not any published research. However, given the company’s poor track record on transparency and integrity, these questions are not entirely unfounded.
In any case, there would be little incentive for Pfizer to cherry-pick participant data to showcase the benefit of its new bivalent booster. The Centers for Disease Control and Prevention (CDC) has already granted Pfizer Emergency Use Authorization for the bivalent booster.
However, Pfizer admitted that there was a difference between the two groups. The interval between the booster and the trial participant’s last exposure to a vaccine was significantly longer in those who received the bivalent booster (10-11 vs. 7 months). Could this difference affect the antibody responses in the two groups?
Pfizer shrugs this off, explaining that “Despite this difference, pre-booster antibody titers were similar for both.”
But pre-booster antibody titers were not the metric of interest — it was the difference in antibody titers before and after that Pfizer was seeking to compare. At least one study indicates that a longer interval between vaccine exposure results in a greater antibody response.
Furthermore, Pfizer’s results indicate that the antibody response was lower in those who had a previous bout of COVID-19, or as they put it, “greater in those without prior infection.”
As early as February 2022, the CDC reported that 57.7% of the U.S. population had been exposed to SARS-CoV-2 through seroprevalence studies. Not only is this most recently available data nine months old, but the CDC also admitted that this was an underestimate because breakthrough infections result in lower anti-N titers (vaccinated people who succumb to COVID-19 generate lower levels of anti-nucleocapsid antibodies than those who are unvaccinated).
In other words, unless you are in the minority and have not had COVID-19, you can look forward to a lower antibody response from the bivalent booster.
What about safety?
“The safety profile remains favorable for the bivalent vaccine and consistent with the original vaccine,” according to Pfizer.
And Pfizer knows this because three dozen bivalent booster recipients didn’t suffer any serious adverse events after one month of observation.
Apparently, Pfizer continues to believe that its original COVID-19 vaccine has a favorable safety profile — despite the more than 31,000 reports of deaths submitted to the Vaccine Adverse Event Reporting System, or VAERS (most occurring in the first seven days after inoculation), the 7.8% of vaccinated people who reported to V-safe that they sought medical attention after a COVID-19 vaccine and the nearly 80,000 serious adverse events and 1,223 deaths reported within three months of the vaccine’s roll-out, according to Pfizer’s own post-marketing analysis.
Ongoing studies will not determine any benefit
Despite reporting only inconsequential data in three dozen people over the age of 55, Pfizer announced in the same press release:
“A booster dose of the BA.4/BA.5-adapted bivalent vaccine has been authorized for emergency use by the FDA for ages 5 years and older and has also been granted marketing authorization in the EU by the European Commission following a positive opinion from the EMA for ages 12 years and older. An application for marketing authorization of the BA.4/BA.5 booster has been submitted to the EMA for children ages 5 through 11.”
And more good news:
“[Pfizer and BioNTech] also initiated a Phase 1/2/3 trial in September 2022, to evaluate the safety, tolerability and immunogenicity of different doses and dosing regimens of the companies’ Omicron BA.4/BA.5-adapted bivalent vaccine among children 6 months through 11 years of age.”
Yes. It is important for parents to know what dose their child can tolerate.
However, conspicuously missing in the design of this ongoing pediatric trial is the determination of efficacy — how good the product is in protecting children from contracting COVID-19 or from negative COVID-19 outcomes (death, hospitalization, ER visits, etc.). Isn’t that the point of a “vaccine” trial?
Apparently not — at least not according to the study description:
“The purpose of this clinical trial is to learn about the safety, extent of the side effects, and immune responses of the study vaccine (called bivalent BNT162b2 Omicron containing vaccine) in healthy children.”
Although having an estimated enrollment of 2,270 children, this ongoing trial will not answer the primary question parents will ask: Will this therapy benefit my kid?
Rather it will only allow Pfizer and BioNTech to determine how powerful their experimental mRNA product is in provoking infants and children to generate Omicron-specific antibodies.
Why are Pfizer and BioNTech not interested in proving their product does anything meaningful? Could it be because they realize this would be an impossible task?
Using data from nine months ago, the CDC reported that at least 75% of children in this age group had already acquired natural immunity to this disease. It is highly improbable that this study could demonstrate any differences in COVID-19 infection rates or outcomes, even with more than 2,000 children enrolled.
Madhava Setty, M.D. is senior science editor for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
British Economy May Be Left Paralyzed Due to Soaring Mental Disorders

Samizdat – 10.11.2022
The number of British citizens neither working nor looking for a job has grown dramatically since the beginning of the pandemic. Much of this can be attributed to mental health issues, which could impede the UK’s economic growth, economists warn.
According to research carried out by a UK media outlet, the number of economically inactive people in Britain rose by 537,500 between June 2019 and June 2022. About 450,000 of these cases were connected to mental health issues. The number of economically inactive people in the UK has skyrocketed to almost nine million. Britons are plagued by depression and anxiety disorders, the research shows.
This trend will have a negative impact on the British economy, the analysts warn. For instance, Deloitte’s research unit states that mental disorders of employees affect the productivity and turnover of companies. According to their report, annual costs associated with poor mental health have increased by 25% since the outbreak of COVID-19.
The epidemic of mental disorders will affect the British economy globally, economists claim.
Many experts claim the “rise in economic inactivity will hold UK growth back.” Economically inactive people do not contribute to public finances. Furthermore, the disability benefits bill in the UK has already reached £14.7 billion.
Mental disorders are among a number of conditions that may qualify for disability benefits. Depression and anxiety disorders are on the list, but in general any mental condition qualifies if it prevents a person from gaining or maintaining employment.
STOP the Infanticide! 5,000% Increase in Fetal Deaths Following COVID-19 Vaccines!

The U.S. Government’s Vaccine Adverse Events Reporting System (VAERS) was updated today, and there are now 4,534 fetal deaths recorded in VAERS following COVID-19 vaccines given to pregnant and child-bearing women. (Source.)
And these recorded fetal deaths are but a fraction of the real number of unborn children who have died since the COVID-19 experimental vaccines were given emergency use authorization, as a previous report published for Department of Health and Human Services stated that fewer than 1% of all vaccine adverse events are actually reported to VAERS. (Source.)
Three of these fetal deaths have followed the new Bivalent COVID-19 booster shots from Pfizer and Moderna, including a 26-year-old woman from Arizona who developed breast cancer following the vaccine, and chose to have chemotherapy and terminate the life of her unborn child.
VAERS ID: 2447825: Began noting a breast lump 9/2021 Biopsied ER/PR + HER 2- breast cancer MRI 3/17/2022 with hepatic mets multiple small pulmonary mets also noted. Liver biopsy 4/1/22 consistent with metastatic breast cancer. Noted to be pregnant when she went for port-a-cath.
Choose to terminate pregnancy 3/31/22 to allow for complete chemo. ACT 4/5/22-7/23/22 . PET noted resolved axillary nodules and pulmonary nodules, Liver mets responding but still with activity. Sarted Lupron and anastrozole 8/10/22, Kisqoli addes 8/23/22.
I am not saying MRNA vaccines caused this but I have seen way more and way younger breast cancer in this remote population in than in a very long career.
We have had 18 new cancers since the vaccines only 1 was unvaccinated. This is the youngest ever. (Source.)
By way of contrast, for the 30 years prior to the emergency use authorization of the COVID-19 vaccines, there were 2,245 reported cases of fetal deaths following all FDA-approved vaccines, or about 75 fetal deaths per year. (Source.)
Taking the total fetal deaths following COVID-19 vaccines for the year 2021, 3,774 fetal deaths (source), that is an increase of 4,943% over the yearly average of fetal deaths following all FDA-approved vaccines for the previous 30 years.
Besides these government statistics from VAERS, medical professionals are corroborating this evidence of infanticide by COVID-19 vaccines based on the increase they are seeing in fetal deaths and stillborn babies following the roll outs of the COVID-19 vaccines.
An alleged leaked email from a “managing nurse” from a hospital in Fresno, California, states that there has been an increase in stillbirths following the COVID-19 vaccines, and that this trend is expected to continue according to Epoch Times.
This follows a report we recently published by Dr. John Campbell regarding the increase in neonatal deaths in Scotland.
And that follows another report we published last month (October, 2022) from Dr. James Thorp, a board certified OBGYN and Maternal Fetal Medicine Physician with over 43 years of obstetrical experience, who was interviewed by Dr. Drew Pensky and stated that in the past two years since the mRNA COVID vaccines were introduced, he has seen an “off-the-charts” rise in sudden fetal death and adverse pregnancy outcomes, such as fetal malformation and even fetal cardiac arrest, among his patients.
Who watches the watchmen?
Health Advisory & Recovery Team | November 8, 2022
Early this month, HART outlined the detailed mechanisms that have been deployed to crush constructive dissent in the Covid era. The assault on the rational mind has been one of shock & awe — a concerted effort to ridicule, gaslight and coerce those considering the ultimate heresy of questioning what they have been told to believe. “Moving at the speed of science” (big pharma terms and conditions apply) seems to imply the opposite of what normal human beings would describe as the scientific method.
Bloated and corrupt monopolies tend, over time, to buckle and collapse under the weight of their own inconsistencies. Discrepancies become harder to paper over; the truth will out. ‘Fact’-checkers — so often funded by those their ‘fact’-checks protect — are increasingly having to back-pedal and deal with periodic humiliation as they post-rationalise their obviously fallible discernment.
Despite all these bloopers, ‘fact’-checkers are still hawking their wares: much like flares and chaff on the battlefield, they distract, distort and deflect efforts to engage in substantive debate. It is usually best to ignore their antics — engaging in serious dissection of straw men erected by po-faced (yet well-funded) narrative ninnies just stymies effort that could otherwise be expending on sorting wheat from chaff. After all — cui bono? If one has spotted a genuine warning signal that might undermine a profitable grift, is it not likely that the peddler of that grift will wish to muddy the waters so as to protect their racket? The more the fact-checkers squirm as they face up to a litany of their own contradictory assertions, the more it highlights the work of those that are scientifically critiquing the pronouncements emanating from big pharma’s marketing mouthpieces.
It is no secret that members of HART devoted some of their spare time in support of Dr Aseem Malhotra whose two peer-reviewed journal papers were recently published in the Journal of Insulin Resistance (the JIR Papers ). Up popped the usual suspects with a cacophony of denigrating ad hominem and otherwise spurious attacks. To be quite honest, the more abusive and baseless these are, the more likely it is that they do not have anything material to contribute, and the noise just brings the papers to the attention of a wider audience.
On a more positive note, some of the ‘fact’-checkers at least sugar-coat their ‘findings’ in polite language. This is to be encouraged — after all, the thrust & parry of scientific discourse requires hypotheses to be challenged. Science Feedback, via their subsidiary Health Feedback, wrote a long article in response to Dr Malhotra’s JIR Papers. It seems they did not really have much of a legitimate complaint, because the first 350-odd words are devoted to ‘criticism by association’. One might paraphrase: “Dr Malhotra has links to HART, who have said things that big pharma do not like!”.
Moving on, Health Feedback attempts to undermine the evidence presented in the JIR Papers that the mRNA injections “might do more harm than good”, which they claim is unsupported, citing a supposed p-hacking issue in the conclusions of one (a pre-print) of the 48 references in the Part I of Dr Malhotra’s papers. It is bold of Health Feedback to attempt to rubbish this claim given the conclusions of a 23 million-strong cohort study published in JAMA Cardiology in April 2022 that supported this statement. Subsequently, a pre-print has also demonstrated that mRNA boosters resulted in 18 severe adverse events for every Covid hospitalisation prevented for 18-29 year-olds, and another new publication from Japanese researchers finds that: “SARS-CoV-2 vaccination was associated with higher risk of myocarditis death, not only in young adults but also in all age groups including the elderly. Considering [the] healthy vaccinee effect, the risk may be 4 times or higher than the apparent risk of myocarditis death. Underreporting should also be considered. Based on this study, risk of myocarditis following SARS-CoV-2 vaccination may be more serious than that reported previously”.
While of course the last two of these papers only became available after their ‘fact’-check, Health Feedback still doubles down on its claims by arguing in a subsequent section that there is little evidence that post-vaccine myocarditis has long-term health implications. This is a classic ‘hostage to fortune’ statement which, over time, will answer itself — in the meantime, why should unsuspecting vaccinees be unwitting guinea pigs in a real-world experiment to find this out? It is somewhat pertinent that this question is being asked in a week that Moderna admitted — deep in the supplementary data from a clinical trial of its mRNA injections — that there had been a “new-onset Type 1 diabetes mellitus and diabetic ketoacidosis” in a one-year-old infant which was considered related by the trial assessors. No need for a ‘fact’-check on this one: this tragedy is both a travesty and the truth.
Health Feedback takes the above criticisms as supporting evidence for the claim that Dr Malhotra has deployed a ‘cherry picking’ strategy to ignore evidence that does not support his conclusions. This is a touch rich. Dr Malhotra covered a lot of ground in the JIR Papers, citing almost 110 references, a large proportion of which are published journal papers. A legitimate response to the JIR Papers is to challenge the specific claims made and to seek to challenge the logic that underpins the conclusions. The p-hacking point (which was invalid as explained by HART member Prof Fenton here) that they bring to bear is a useful challenge that contributed to the debate — it just so happens that Health Feedback’s response strengthens Dr Malhotra’s argument by allowing these other references to be brought to the attention of the reader.
As for the various (slightly pathetic, it has to be said) attempts to ridicule and “play the man, not the ball” with respect to organisations like HART, characterising us as misinformation spreaders: these are particularly noteworthy for their lack of supporting evidence. We would encourage Health Feedback to interrogate our output and come up with specific evidence of their claim. While they are at it, they might like to comment on this somewhat unfortunate statement from one of Health Feedback’s front of house members:
“The experts are saying that the vaccines do not reduce transmission, but that is an inaccurate statement,” [Dr Monica] Gandhi says. “Vaccines have always decreased transmission. What they should be saying is that the clinical trials were not designed to test for asymptomatic infection, but there is every biological reason in the world to believe that they will reduce asymptomatic transmission”.
The highlighted text above is incorrect: it is well known that so-called ‘leaky vaccines’ do “not prevent infection, viral replication or transmission”. Call the ‘fact’-checkers. Oh.
And as for ‘every biological reason’ to ‘believe’… are ‘fact’-checkers in the business of proving things scientifically or amplifying beliefs? Real-world evidence seems to indicate that transmission seems to be somewhat unaffected — or possibly worsened — by the injections.
Given that this statement was published in a March 2021 Association of American Medical Colleges article that was claiming to address vaccine hesitancy (read: coerce people to participate in the mRNA injection scheme), perhaps Health Feedback might wish to look at the plank in its own eye while addressing any motes in Dr Malhotra’s?
HART applauds Dr Malhotra’s attempts to sound the alarm that the precautionary principle is not being adhered to. The Nelsonian ignorance of various ‘public health’ bodies — who keep declaring that they “really do not see the signal” — is the real villain of the piece.
All in all, HART welcomes the publicity that outfits like Health Feedback provide, despite the disappointing ‘fact’-checking moniker. They are, in a somewhat peculiar way, furthering scientific discourse by advertising Dr Malhotra’s work to the wider public. We are honoured to be associated with brave and principled people such as him.
The REAL story behind RSV & the so-called “tripledemic”
MSM sources are now warning of a co-pandemics of flu, RSV and Covid…but is there any reason to be afraid?
By Kit Knightly | OffGuardian | November 9, 2022
The “tripledemic” is upon us, according to the mainstream media. What is a “tripledemic”, you ask?
Apparently, it’s when we have simultaneous pandemics of influenza, Covid and RSV at the same time. At least, according to the LA Times :
A ‘tripledemic’ of flu, RSV and COVID is feared in California
And the Atlantic :
What a ‘Tripledemic’ Means for Your Body
And CBS:
“Tripledemic” in U.S. could bring deluge of patients to hospitals
All three stories – and there are many others out there too – hit the same handful of talking points.
They report that the flu is back after its “mysterious” disappearance during the Covid “pandemic” (the Alantic notes US flu cases reduced by well over 90% and calls it “getting lucky”, the doublethink is unbelievable).
They also warn that Covid is “still around” or “not over”, or some variation on that.
However, the main thrust of the fear is reserved for RSV. Now, you’re all probably more than familiar with “flu”. And you’re definitely tired of hearing about Covid. But RSV could be a new one for you… so let me explain.
THE VIRUS
Respiratory syncytial virus (RSV) is – according to virus theory – one of the many viruses circulating in the general population at all times. To quote the Mayo Clinic’s website [emphasis added]:
Respiratory syncytial virus (RSV) causes infections of the lungs and respiratory tract. It’s so common that most children have been infected with the virus by age 2. Respiratory syncytial (sin-SISH-ul) virus can also infect adults. In adults and older, healthy children, RSV symptoms are mild and typically mimic the common cold.
And according to the CDC:
Almost all children will have had an RSV infection by their second birthday […] Most RSV infections go away on their own in a week or two.
So, according to official sources, RSV is not serious in the vast majority of cases, and almost all of us have already had it.
In fact, seeing as the symptoms are both generic and mild, the odds are you have had it multiple times throughout your life and never really known. It’s simply one of the many viruses known to cause what we refer to as “the common cold”.
THE DECEPTION
There’s a trick being played here, and as usual in the age of the “pandemic”, it’s a trick of language. The powers that be are exploiting linguistic ambiguity in order to generate fear.
Across most of the world, we simply refer to “a cold” or “the flu” almost interchangeably to describe the dozen or so respiratory infections we all get throughout our lifetime.
Most of the time we don’t know what specific virus or bacteria is supposedly the cause, we have no way of finding out and it doesn’t make any difference because the symptoms and treatments are all the same: Cough, fever, headache – bedrest, orange juice and painkillers.
Now, essentially, the media are taking advantage of that ubiquitous ambiguity by naming something that has always been there but pretending it is something new.
Here’s a case in point, the Scientific American published this article on November 4th, which headlines:
RSV Is Surging: What We Know about This Common and Surprisingly Dangerous Virus
Now, although the headline claims RSV is “surprisingly dangerous”, the article seems to go out of its way to prove the opposite.
- “the virus is so common that nearly all children have encountered it by their second birthday.”
- “It’s that ubiquitous,” Flores says. “Even adults are exposed to it repeatedly over time, so we develop some immunity to it.”
- “In healthy adults and children, though, RSV typically presents as a common cold, with symptoms similar to those caused by other “common cold” viruses, such as rhinovirus, adenovirus and a couple of common coronaviruses.”
- “For the average person, RSV is little more than a nuisance”
The article does warn that RSV can be “particularly dangerous for newborn babies and adults older than age 65” and the immunocompromised, but this is true of literally every pathogen. And even then, they go on to add:
only about 1 to 2 percent of children under six months with RSV need hospitalization (usually for a couple of days), and death is rare.
This is a tactic we’re all familiar with – it was routine, throughout the Covid narrative, for official voices to tell us to be afraid, whilst simultaneously explaining there was nothing to be afraid of.
This approach clearly serves some purpose, although I could not say for certain what that may be.
Regardless, the deception is obvious and clearly deliberate.
The question is, why?
THE MOTIVE
To sum up – there is no reason to fear RSV infection. The media are clear about that themselves, even if they bury it under layers of hysterical headlines.
It is just one of the many viruses which cause – or are said to cause – cold or flu symptoms, all of which circulate the whole world constantly, especially at this time of year.
There’s ALWAYS a “tripledemic”, or a quademic or a septemic. The only difference is now they are naming it.
They are taking the routine and pretending it’s exceptional simply to try and frighten you.
Why?
Well, rather predictably, to sell vaccines.
Yes, you’ll be relieved to know that just as RSV is hitting the headlines for the first time EVER, they’ve also just produced the first ever vaccines against it.
On November 1st, Vox reported:
New RSV vaccines are coming. This is very, very good news.
Which claims:
After decades of failed efforts to produce an RSV vaccine, several highly effective ones are finally on the verge of approval.
On the same day, Pfizer announced “positive top-line data” for their new RSV vaccine, with CNN reporting:
After promising trial results for maternal RSV vaccine, Pfizer says it will seek FDA approval this year
That’s right, after decades of trying and dozens of failed attempts, the pharmaceutical companies have finally managed to create not just one but multiple effective vaccines against an endemic virus… just as the virus has hit the headlines.
Now, this all sounds rather familiar, doesn’t it?
If you didn’t fall for this last time you don’t need me to warn you.
If you DID fall for this last time?
Well, fool you once shame on them, fool you twice…
Effects on mother and child that bear out Mike Yeadon’s warnings
By Neville Hodgkinson | TCW Defending Freedom | November 7, 2022
A British scientist with 32 years of experience in the pharmaceutical industry warned right at the start of the Covid vaccine rollout that under no circumstances should the gene-based, mRNA jab be given to women of child-bearing age without studies to confirm it was safe.
Dr Mike Yeadon, former vice president for research at Pfizer, one of the manufacturers of the experimental mRNA products, filed a petition with the European Medicines Agency on December, 1, 2020, urging that even testing the jab on human volunteers was unethical without significant safety concerns being taken into account.
One of these was a similarity between virus proteins targeted by the proposed vaccinations and a protein (syncitin) essential for forming the placenta in pregnancy. If antibodies produced by the jab also acted against those proteins, the petition said, ‘it would result in vaccinated women essentially becoming infertile’.
Co-signed by Dr Wolfgang Wodarg, a leading German physician, the document also warned that the vaccine trials were much too short to flag up late adverse effects. It added that the design was such that the trials could not show whether the product worked either in stopping a person from becoming infected, or from infecting others.
Subsequently, Yeadon became one of the first scientists to highlight evidence from a previously confidential Pfizer study showing that the vaccine products do not stay at the injection site but become widely distributed throughout the body, including the ovaries.
In view of the toxic nature of the ‘spike’ protein that the jab manufactures (summarised here), Yeadon warned in August, 2021: ‘My assumption at the moment is that these vaccines are concentrating in the ovaries of every female who has been given them. We don’t know what that will do, but it cannot be benign and it could be seriously harmful.’
It is now widely acknowledged that the jab neither protects against infection nor transmission, as Yeadon and Wodarg spelled out in their petition. If their knowledge had been sought at the outset of the Covid crisis the UK alone could have been spared the £500billion lockdown bill, with enormous associated social damage.
But what about the fertility warnings? Despite his years of experience at the top of his field, Yeadon has been vilified for speaking out. Is he really no more than ‘a hero of Covid conspiracy theorists’, as the Times described him?
Birth rates have fallen significantly in many countries, including the UK, in the wake of the vaccine rollouts. Various reasons for the fall have been suggested – usually excluding the jab.
Yet Dr James Thorp, a 68-year-old American physician who has practised obstetrics for more than 42 years and sees thousands of high-risk pregnant patients each year, has observed many complications attributable to the jabs, including foetal death and miscarriage. ‘What I’ve seen in the last two years is unprecedented,’ he says.
With help from several colleagues, he compared rates of adverse events following the Covid jabs with those reported post-flu vaccination in women of reproductive age. The focus was on events related to pregnancy and menstruation, using data from the US Vaccine Adverse Event Reporting System (VAERS).
A preprint of their findings published on September 28 shows a thousand-fold increase in menstrual abnormalities after the Covid jab, and significant increases in miscarriage, foetal malformation, growth abnormalities, cardiac disorders, foetal death and stillbirth.
Thorp has also highlighted risks to newborn babies taking milk from their vaccinated mothers. One study found mRNA from the jab in five out of 11 lactating women who had received the vaccination within six months of their delivery.
Last month, in a wide-ranging review in the US-based Epoch Times of these and other findings, US microbiologist and biomedical scientist Dr Sean Lin revealed that Thorp ‘has seen at least three newborns, completely healthy at the time of their birth, who passed away after being breastfed by their recently vaccinated mothers’. This suggested the vaccine components can not only accumulate in the ovaries but can also be passed on to infants via breastfeeding, he wrote.
He added that details of animal experiments performed before the jabs were authorised, recently obtained under freedom of information legislation, showed that mRNA and spike protein can travel through all barriers in a mother rat to enter its foetus. The rats themselves experienced toxicity during gestation, with some becoming infertile and losing the use of their hind legs.
Calling for an end to all Covid shots for pregnant women until long-term safety data become available, Lin writes: ‘The medical field and health agencies should still adhere to the fundamental ethical principle of ‘Do No Harms’.’
A hospital memo leaked to the Epoch Times by a nurse in Fresno, California, revealed how the hospital is experiencing a dramatic rise in the number of stillbirth cases, now upwards of 22 a month compared with an average of one to two every three months previously. This massive increase seems to align with similar evidence from across the country showing a potential rise in problems with fertility, miscarriages and foetal development, the newspaper reported.
Could the vaccine have contributed to a ‘very unusual’ spike in deaths among newborn babies now being investigated in Scotland?
In the UK, one and a half million Yellow Card reports of suspected adverse reactions to the vaccines include 821 miscarriages and 58,171 reproductive/breast disorders.
With tens of millions of doses administered, those numbers have still not persuaded regulators that there is a problem, although real-world adverse effects can be at least ten times higher than those reported. ‘Our advice remains that the Covid-19 vaccines are safe and effective during pregnancy and breastfeeding,’ the Medicines and Health products Regulatory Agency (MHRA) reaffirmed in September.
A review last month in the journal Vaccine declared that based on studies published so far ‘there is no scientific proof’ of any association between the jabs and impaired fertility in either men or women.
It depends on what is meant by ‘scientific proof’. If scientists do not ask the right questions, they can avoid receiving unwelcome answers. Those who drove the vaccine rollout are choosing not to see the thousands of reported disorders as related to the jabs, despite the record numbers, and clearly demonstrated mechanisms of harm.
It took a mathematician/businessman, for example, to point out evidence of a dose-response relationship between the jabs and infant deaths, with significantly more deaths reported when the higher-dose Moderna jab is used during pregnancy than with the Pfizer product.
Igor Chudov, who highlighted this phenomenon using US Centers for Disease Control (CDC) figures, says the Moderna product is associated with nearly twice as many neonatal deaths as the Pfizer vaccine, and 42 per cent more miscarriages.
In the light of these data, he asks: ‘How can Covid vaccine given during pregnancy be safe, and NOT affect infant deaths? How come nobody at the CDC asked this question? How come our media is silent on this?’
It is as though there are parallel universes: one occupied by those who can see no harm, and the other by doctors and scientists who insist a grave situation is staring us in the face.
The latter include three American medical whistle-blowers who found a 2021 rise of nearly 300 per cent in miscarriages among women serving in the US Army compared with the previous five years. There was no increase in 2020, when Covid arrived.
Doctors calling for a halt to Covid vaccination for pregnant women often meet abuse and censorship.
In October 2021, obstetrician and gynaecologist Dr Christiane Northrup told the Epoch Times: ‘Women are having bleedings. The doctors in our area are doing hysterectomies in young women, like 30-somethings. They said “Oh, it’s not unusual”. Let me tell you, as a board-certified gynaecologist, that’s very unusual. Women’s periods are messed up all over the place . . . I’ve had a huge Facebook group of thousands of women talking about this situation that was removed.’
What of Yeadon’s worry that an immune reaction to the spike protein might block pregnancy?
A small study from Singapore, in 15 women, reported that none had developed anti-syncitin antibodies after the jab, but Yeadon says the actual data showed a clear increase, arbitrarily ruled as insignificant by the researchers.
‘It looked like someone had tried to dismiss our concerns by testing for evidence of the particular problem we’d warned about. Unfortunately, all they did is to reinforce our concerns.
‘We’d envisioned the risk that, in responding to the synthetic piece of virus spike protein, women’s immune systems would also make an immune response to their own placental protein. That’s exactly what was reported in the pre-print paper.
‘Based on this concern alone, all these experimental products as a class should have been completely contraindicated in women younger than menopause.’
He insists that a series of toxicology issues meant ‘adverse impacts on conception and ability to sustain a pregnancy were foreseeable from the start . . . There was and still is no data package supporting safety in pregnancy, or prior to conception.’
Featured Video

Russia and China quietly take over natural gas markets in Asia, with Qatar gone
or go to
Aletho News Archives – Video-Images
Book Review
Palantir CEO Calls for Draft to Fight the Empire’s Wars
Involuntary servitude is good for business
By Kurt Nimmo | Another Day in the Empire | April 20, 2026
In 2025, Alex Karp, the CEO of government and military tech contractor Palantir, published The New York Times best-seller, The Technological Republic: Hard Power, Soft Belief, and the Future of the West. The Wall Street Journal praised the book as a cri de coeur, a passionate appeal “that takes aim at the tech industry for abandoning its history of helping America and its allies,” while Wired praised the book as a “readable polemic that skewers Silicon Valley for insufficient patriotism.”
On April 18, 2026, Palantir posted twenty-two points to social media summarizing the book. In addition to taking Silicon Valley to task for insufficient patriotism, advocating a role for AI in forever war, and denouncing the “psychologization of modern politics,” the Palantir post on X declares: “National service should be a universal duty. We should, as a society, seriously consider moving away from an all-volunteer force and only fight the next war if everyone shares in the risk and the cost.”
National conscription, a form of involuntary servitude, and the wars it portends, is good for business, especially for corporations within the orbit of the Pentagon, the CIA, and the national security state. Palantir fits comfortably within this amalgamation. … continue
Blog Roll
 Aletho News
Aletho News- Palantir CEO Calls for Draft to Fight the Empire’s Wars
- Iran War fallout: Russia and China quietly take over natural gas markets in Asia, with Qatar gone
- Hamas dismisses US-backed disarmament plan as ‘collective suicide’
- Israel’s war obsession and the urgency of Palestinian leverage
- Supply chains breaking: The hidden bottlenecks threatening to bring the global economy to a standstill
- Israel’s Expansion Means An Unraveling of Middle East Stability
- Why has Israel’s Security Doctrine begun targeting Turkey?
- US strikes vessel in Caribbean killing three, death toll reaches 180
- NATO’s Baltic Operation Aims to Curb Russian Cargo Traffic
- France’s New Nuclear Strategy to Weaken Security in Europe – Russian Foreign Ministry
- If Americans Knew
- Israel is (still) killing aid workers in Gaza
- Catholics finally splitting with Trump over Iran war and Israel
- Israel’s “Black Wednesday” Massacre Leaves Lebanese Families Giving DNA To ID Loved One’s Remains
- ‘I Felt I Was a Monster’: IDF Soldiers Talk About the ‘Moral Injury’ – and the Silence
- ‘I thought I might die’: A Palestinian mother’s account of Israeli detention
- Mom whose daughter was killed by Israeli bulldozer 23 years ago pleaded with Congress to finally stop funding
- Israeli soldier takes sledgehammer to Jesus statue in Lebanon – Daily Update
- Israel employs ‘Gaza tactics’ in Lebanon, destroying 1,000 homes per day – Daily Update
- Israel relegates another population to life in tents – Daily Update
- Senate again fails to block weapons to Israel
- No Tricks Zone
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
