Always Follow the … ‘Incentives.’

Dr. Karen Landers is widely admired in my state and is a hero to journalists and editors at our state’s largest news organization … But I’m not a big fan.
BY BILL RICE, JR. | AUGUST 8, 2023
As my readers know, I write articles and make posts anywhere I can which try to advance my hypothesis that the novel coronavirus was spreading widely in late 2019.
After I made yet another “early spread” post, a colleague made a reply that sums up everything far better than I’ve done to date. Here’s his astute post:
“There is absolutely no incentive for about 99%+ of the scientists in the world (administrative state, academic, private, corporate) to ever want to truly trace down the origin timing (and a case zero may be an impossibility). They would all look like quack minions if they discovered something other than the narrative. Too many threw all of their chips into the narrative ship and should that ship sink…”
All this fellow skeptic did with this post was frame the debate using incentives as the psychological motivating factor that explains everything that happens. In doing this, he reminded me to always examine every topic from a “risk-reward” perspective.
The incentives – positive or negative – are all that really matter.
Why do many people, especially those in leadership positions, act in nefarious, disingenuous ways? Why are they not interested in exposing untruths?
To answer this question, one has to imagine the repercussions or harm such people would suffer if the truth was exposed. (These would be professional “risks”) […]
… and then compare these negative outcomes (disincentives) to the rewards or benefits that would (and did) accrue to these same individuals if they simply went along with authorized narratives many of these people must have known were either lies or, at least, very possibly, falsehoods.
Two case studies from my own state …
To illustrate my point, I can reference two “public health leaders” in my own state as case studies.

Dr. Fauci’s successor … that’s ‘high cotton’ as we say in Alabama.
The first example is Dr. Jeanne Marrazzo, who previously served as director of UAB’s Division of Infectious Diseases, and was recently named as Dr. Anthony Fauci’s successor at the NIAD.
The second example is Dr. Karen Landers, one of the top officials at the Alabama Department of Public Health and the primary media spokesperson for this high-profile public health agency.
In my strong opinion, both public health leaders enthusiastically and daily promoted myriad Covid falsehoods.
I also do not think either person could have risen to these high-ranking positions without having some intelligence. At some point, it must have occurred to both individuals that the positions they were championing weren’t necessarily supported by certain statistics, data or scientific studies.
Still, they supported all of these false or dubious positions.
Also, significantly, they took absolutely no steps to debunk any of these false or dubious narratives.
I’m confident in writing that both Dr. Marrazzo and Dr. Landers …
Supported draconian and civil-liberty-eviscerating lockdowns as a non-pharmaceutical “mitigation” measure, unprecedented measures they assured the public would slow or stop the spread of the coronavirus.
They both supported mask mandates that did nothing to slow virus spread and probably caused harm to the people forced to wear masks 8 to 12 hours a day for months or years.
They supported school closings and, once schools re-opened, student masking and social distancing.
They pushed the bogus narrative that Covid was a serious health risk to every citizen, including children who faced virtually zero mortality risk.
They endorsed the proposition that proven drugs like ivermectin and HCQ should not be used to treat Covid patients.
They either endorsed or didn’t criticize the myriad new “Covid protocols” used in hospitals even though these treatment protocols probably caused numerous unnecessary deaths.
They supported endless testing of asymptomatic citizens with PCR tests, testing which accomplished little if nothing to slow or stop spread or future cases.
They also never mentioned or questioned the fact the 40 to 45-cycle PCR tests were producing millions of bogus or dubious “cases.”
As far as I’m aware, neither Dr. Marrazzo nor Dr. Landers ever questioned the safety of Remdesivir, which many (ignored) scientists and doctors say killed many patients. (Update. Read this. Yes, Dr. Marrazzo “supported” Remdesivir. Big-time).
They never took any interest in investigating the possibility the coronavirus was spreading widely in America by late 2019 (although I myself presented both of them compelling evidence this was almost-certainly a fact).
And, of course, they strongly supported everyone over the age of 6 months getting a “vaccine.”
They both enthusiastically participated in the campaign to vilify the unvaccinated and spread the false narrative this was a “pandemic of the unvaccinated.”
Today, they both still say the vaccine is incredibly safe and poses no real risks for anyone who got the original series of shots or now the extra “boosters,” which they still encourage everyone to get, including pregnant women and children.
Of course, these examples are my opinion, but these are opinions backed up by millions of skeptics, including countless intelligent scientists, doctors and writers/thinkers.
If our opinions are wrong, neither of these two alleged experts and public health authorities have ever agreed to a public debate to engage with these skeptics. This factual observation tells us these are not real scientists, who are happy to engage in scientific debates.
So what consequences have these alleged experts suffered from being spectacularly and stunningly wrong about so many important public health subjects?
Answer: There were no negative consequences. In fact, the careers of both ladies flourished.
As noted, Dr. Marrazzo just got the biggest promotion in the world of science, replacing “Science Himself” Dr. Fauci as the head of the agency that basically controls scientific research in America.
As far as I know, Dr. Landers didn’t get a promotion, but she’s still one of the public faces of the Alabama Department of Public Health, an agency which has never had more power or influence.
She certainly never had to worry about losing her cushy and prestigious job.
And both are literally celebrated as heroes of public health in my state.
In a recent article about Dr. Marrazzo’s big promotion, I pointed out that al.com (the largest “news organization” in Alabama) wrote a glowing piece on Dr. Marrazzo as a leader who “made a difference” in Alabama. In fact, the headline said Dr. Marrazzo actually made the citizens of our state “smarter.”
The same news organization also celebrated the contributions of Dr. Landers in a series of articles that told readers who Alabamians should exalt as brave and all-knowing public health heroes.
This series – “21 Alabamians who made a difference in 2021 – ” (highlighted) people who … made our state a better place to live this year.”
Excerpt: “Landers … has become a key public figure as the state battles COVID-19. Her calm demeanor and straight-forward answers have been a reassuring voice amid the changing health landscape …”
Regarding those alleged “straight-forward answers,” I’ve interviewed Dr. Landers and sent her office many emails trying to find out why the ADPH didn’t investigate two people who almost certainly had Covid in late 2019; trying to find out how many Alabama children really died “from” Covid and what the cycle threshold was on the PCR tests the agency used to determine Covid “cases.”
I can report I’ve never gotten one “straight forward answer” from this lady and/or this public health agency.
I also speculate I’m probably the only journalist in my state who doesn’t consider the information disseminated by this agency as infallible.
But my main point is the point my colleague made at the beginning of this article. That is, these two people clearly personally benefitted from spreading false or dubious Covid (dis)information.
Today’s thought exercise considers what would have happened to their careers if they’d acted like me and actually questioned a few of the authorized Covid narratives.
I can make these predictions with high levels of confidence: Dr. Jeanne Marrazzo wouldn’t be getting ready to replace Dr. Fauci … and Dr. Karen Landers would now be retired from the ADPH.
Nor would either person have been the subject of the fawning feature stories al.com published.
Above, I write neither of these ladies is stupid. That is, they figured out all of the above on their own:
“Go along with the authorized narrative” = “Fantastic career accolades and unlimited prospects.”
“Challenge the authorized narrative” = “That’s it for my public health career.”
And one can multiply these two “cost-benefit” case studies by every public health official in the world and by just about every political leader or every person who leads any important organization.
All the operative incentives point to … one authorized narrative being protected and pushed … forever and ever, I guess.
While I would argue the actions and statements of these public health officials contributed to many unnecessary deaths and immeasurable harm to countless Alabamians and made residents of our state dumber not “smarter,” from their perspective or from their (selfish) mental calculations … they definitely “chose wisely.”
I’ll end with a “case study” of someone who did challenge the authorized narratives – me.
Did I suffer any professional or personal “harm” by opposing the authorized narrative?
Well, I lost friends. Some family members are embarrassed by my efforts and rarely talk to me anymore.
My Facebook account was suspended and de-boosted repeatedly, which meant a professional writer couldn’t do any writing that would reach a large audience using that speech platform.
I could find only one news organization (uncoverDC.com) that would pay me to write contrarian Covid articles.
My main job or skill set is as a “journalist,” but I’m now-un-hirable at 100-percent of corporate news organizations.
However, if I wrote the type articles al.com journalists write, I’d probably have no problem landing a real (paying) job in journalism. If I’d kept my real views private, all my former friends would still think it was okay to interact with me. Family members wouldn’t be nervous about engaging with me.
My professional and financial prospects would probably be much better than they are today.
So about that “road less travelled” … before you take it, you better think long and hard about where it might lead.
Actually, though, the world and all its roads can lead us to interesting places. God might have a larger plan for all of us, even the contrarians.
As it turns out, I’m as poor as I’ve ever been, but my writing (thanks to starting a Substack newsletter) has reached more people than ever and my words might be influencing more “debates” than ever.
I certainly don’t want this article to come across as whining because I wouldn’t change anything I’ve done.
If a few people like me didn’t criticize people like Dr. Marrazzo and Dr. Landers, who would?
The world does need at least a few contrarians … and I guess this is my lot/purpose in life.
When you write as much as I do, you have to do a little thinking about the topics you’re writing about.
At least I now understand why the world is full of “leaders” like Dr. Marrazzo and Dr. Landers.
In investigative journalism, “follow the money” is supposed to guide our thinking. But I might adjust that maxim to say … follow the incentives. They’re all backwards, but at least this tells us why the world’s like it is.
CDC, Pharma Giants Angle for Annual COVID Shots Despite ‘Unclear’ Science
By Monica Dutcher | The Defender | August 7, 2023
The U.S. House of Representatives Select Subcommittee on the Coronavirus Pandemic wants to know more about plans by the Centers for Disease Control and Prevention (CDC) to recommend annual COVID-19 vaccines.
During a July interview with Spectrum News, CDC Director Mandy Cohen said she “anticipate[s] that COVID will become similar to flu shots, where … you get your annual flu shot and you get your annual COVID shot.”
As part of the House investigation into federal COVID-19 vaccination mandates and policies, Rep. Brad Wenstrup (R-Ohio) last week sent a letter to Cohen, stating:
“It is unclear if the science supports such a recommendation. If this anticipated CDC recommendation occurs, it will mark a significant change in federal policy and guidance regarding COVID-19 vaccines and the way in which they are utilized.”
Wenstrup requested all documents and communications about any annual — “or any other time-based iteration” — recommendation for COVID-19 booster shots, including correspondence between or among the CDC, U.S. Department of Health and Human Services (also under the subcommittee’s investigation), the White House, the CDC Foundation, CDC contractors and any other CDC stakeholders.
Pfizer, Moderna and Novavax are slated in September to release new single-strain COVID-19 shots targeting the Omicron subvariant XBB.1.5. These vaccines are not yet approved by the U.S. Food and Drug Administration (FDA), but manufacturers are following the June 15 recommendations of the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC).
The committee of 21 independent advisers in June voted unanimously that any new vaccine should protect against just one strain of the virus — a departure from the available bivalent vaccines — and should target one of the three Omicron subvariants currently circulating, including XBB.1.5.
The XBB.1.5 variant spread globally in the first quarter of 2023, reaching dominance in North America, and other parts of the world by April, according to the FDA’s briefing document for the June meeting.
‘We really don’t know what the COVID season is’
FDA advisers in January raised concerns about shifting to a yearly schedule for COVID-19 vaccines. Unlike the flu, which thrives in the winter months, COVID-19’s spread has proved erratic, consistently mutating into new variants.
Dr. Mark Sawyer, professor of clinical pediatrics at the University of California, San Diego, told CNBC that describing COVID-19 as seasonal “could be problematic” because “we really don’t know what the COVID season is.”
Dr. Peter McCullough, author of “The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex,” told The Defender :
“COVID-19 respiratory illness is now like a mild head cold. There is no seasonal pattern. The COVID-19 vaccines have failed to stop transmission or protect against hospitalization and death.
“The products on the market have theoretical efficacy of less than six months. Annual COVID-19 shots have no clinical indication, medical necessity, are not durable for 12 months and have never been tested for use on a yearly schedule.
“On Dec. 7, 2022 in a U.S. Senate panel on vaccines, I called for all COVID-19 vaccines to be removed from the market because they are not safe for human use. There has been no objection to that testimony from public health officials.”
NBC News reported that Dr. Peter Marks, the FDA’s top vaccine regulator, acknowledged during an FDA advisory committee meeting in January that “simplifying the COVID-19 vaccine schedule to be exactly like the flu may not be possible.”
Pfizer hopes otherwise. The drug company’s chief scientific officer, Dr. Mikael Dolsten, thinks an annual COVID-19 vaccine would improve vaccine sentiment, telling CNBC the public grew dissatisfied with mandates during the earlier stages of the pandemic.
He said:
“Unfortunately some people see vaccines as part of that [the mandates].
“I think of it like the introduction of seat belts for cars. People didn’t want to wear them at first, but over time they realized how much seat belts protect them. Now everyone uses them today. That’s kind of how the vaccine story needs to be reimagined.”
An annual schedule, Dolsten added, may help people view COVID-19 shots as another “very natural part” of protecting their health.
CDC director ‘very worried about parents not vaccinating kids’
In addition to the ambiguity surrounding COVID-19 vaccine scheduling, there is no consensus among medical experts on which patients would be recommended for an annual jab.
Dr. Paul Offit, a vaccine scientist, professor of pediatrics in the Division of Infectious Diseases at the Children’s Hospital of Philadelphia and a member of VRBPAC, took issue with not only the annual model but also with administering COVID-19 vaccines to low-risk groups.
Offit told CNN:
“If the goal of the vaccine is the stated goal, which is protection against severe disease, do you really need a yearly vaccine for otherwise healthy people less than 75? I mean, is this the flu model? Because I would argue it shouldn’t be.”
Health advocacy groups and doctors argue against authorizing mRNA shots in young children and babies. As of July 28 — when data were last updated in the Vaccine Adverse Event Reporting System (VAERS) — there were 6,591 reports of adverse events following COVID-19 vaccination in children under age 6.
Cohen said she is “very worried about parents not vaccinating kids,” telling Spectrum News, “There’s plenty of other things that are hard as parents that we can’t do. This is one we can do to protect our kids.”
McCullough described Cohen as “fully entrenched in the bio-pharmaceutical complex” and “on the wrong side of every pandemic public health intervention.”
Jeffrey A. Tucker, founder and president of the Brownstone Institute, said Cohen’s career has been punctuated by “heartbreaking fear-mongering, pseudo-science, and propaganda,” adding that “she passed with flying colors all three tests of compliance: closures, masking, and vaccine mandates.”
Reduced trust in vaccines and the CDC concerns Cohen, who plans to rehabilitate that trust by focusing on “transparency, execution and building relationships with the public, health leaders and politicians.”
A survey by the Harvard T.H. Chan School of Public Health published in the journal Health Affairs found that roughly a quarter of Americans have little to no trust in the CDC for health information, including 10% who do not trust the agency at all.
The CDC currently recommends the primary series of mRNA shots, or the first two doses of the updated vaccine be given weeks apart, followed months later by a booster shot. The FDA updated its guidance for these shots in August 2022 to contain a bivalent formulation targeting the original viral strain plus the BA.4 and BA.5 Omicron subvariants.
Pfizer is working on a combined flu/COVID-19 vaccine, expected to be available after 2024. Moderna is also working on a “next-gen flu-COVID combo” vaccine. Other vaccine makers are following suit.
Monica Dutcher is a Maryland-based senior reporter for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Everything you need to know about Covid’s “Eris” Variant
By Kit Knightly | OffGuardian | August 7, 2023
The big news the last couple of days is that “Covid” is back… again. This time it’s the “Eris” variant, named after the Greek goddess of strife and discord, it supposedly is causing a spike in cases for the first time in… who cares how long.
The bulk of reporting on it is detailing how it’s supposedly related to Omicron or Arcturus or all the other names they flash in the headlines.
That, or the symptoms.
They are a runny nose and a sore throat and…well, you know. The only noteworthy thing to mention here is that the “loss of taste of smell” – so long sold as Covid’s calling card – is no longer considered a common symptom.
Yahoo even reported – without a shred of irony – that the alleged up-tick in “cases” was due to people spending more time indoors:
Bad weather encouraging people to spend more time indoors and waning immunity have been blamed for the rise
… a peculiar position to take, considering lockdown is meant to have helped, last time.
Anyway, without further ado, here is everything you really need to know about the Eris variant:
It’s bullshit.
Just like all the others.
Nothing else really needs to be said, does it?
Sure the media are setting up softballs for us to hammer over the fence, talking about the “symptoms” and “infection” rate again as if the past three years haven’t rendered all those words meaningless. But we are – or should be – well past that point of arguing against the mainstream.
We know everything we need to know about the symptoms – they are “generally mild” and “flu-like”, because Covid is nothing but re-branded endemic respiratory diseases. We know the death statistics are made up and the tests don’t work except to manufacture cases.
We know all this, even this repeating of it is unnecessary, to be honest.
The only aspect of Eris worth discussing is why it’s in the papers, and even that answer is briefer than usual.
Eris exists because the “Cerberus” heatwave is over, and July was unseasonably cold and damp in the UK. Because Autumn will be setting in soon enough and there are no more major sporting events for Just Stop Oil to disrupt for a while.
In short, Eris is what happens when people refuse to panic about climate change.
In fact, we can probably expect headlines linking Eris to the climate in the next few days.
The trouble with that is, just like climate change, people can only be scared by words for so long. The media repeated “global warming” so much the words lost their meaning, and filled the papers with so many apocalyptic predictions that never came to pass that people got numbed to it, they filter it out now even if they don’t realise they do.
The same will happen with covid; the more they bring it back for a jump scare, the less people will jump.
That’s probably why they’re laying the groundwork “the next pandemic” of “disease X”.
COVID QUESTIONERS DEEMED ‘DOMESTIC TERRORISTS’
The Highwire with Del Bigtree | August 3, 2023
A trip down memory lane chronicling how Homeland Security labeled us all ‘domestic terrorists’ for trying to warn people about the harms of the COVID shots, masking kids, warnings and attacks meant to achieve COVID compliance. Will the same op be run during a climate emergency?
How the current version of the WHO’s Pandemic Treaty (aka Bureau Text) encourages rather than prevents pandemics
BY MERYL NASS | AUGUST 5, 2023
Weapons of Mass Destruction: Chem Bio
Traditionally, Weapons of Mass Destruction (WMD) were Chemical, Biological, Radiologic and Nuclear (CBRN).
The people of the world don’t want them used on us—they are cheap ways to kill and maim lots of people at once. And so international treaties were created to try to prevent their development (sometimes) and use. First was the Geneva Protocol of 1925, banning the use of biological and chemical weapons in war. The US and many nations signed it, but it took 50 years for the US to ratify it, so we believed we were not bound by it.
The US used chemical weapons subsequently. The US probably used biological weapons in the Korean War, and perhaps in Vietnam, which experienced an odd outbreak of plague during the war. The use of napalm, white phosphorus, agent orange (with its dioxin excipient causing massive numbers of birth defects and other tragedies) and possibly other chemical weapons led to much pushback, especially since we had signed the Geneva Protocol and we were supposed to be a civilized nation.
In 1968, a young Seymour Hersh wrote a book about the US chemical and biological warfare program. In 1969 Congressman Richard D. McCarthy wrote the book “Ultimate Folly” about the US production and use of chemical and biological weapons. Prof. Matthew Meselson’s review of the book noted,
Our operation, “Flying Ranch Hand, ” has sprayed anti-plant chemi-
cals over an area almost the size of the state of Massachusetts, over
10 per cent of it cropland. “Ranch Hand” no longer has much to do with
the official justification of preventing ambush. Rather, it has become
a kind of environmental warfare, devastating vast tracts of forest in
order to facilitate our aerial reconnaisance. Our use of “super tear
gas” (it is also a powerful lung irritant) has escalated from the originally
announced purpose of saving lives in “riot control-like situations” to the
full-scale combat use of gas artillery shells, gas rockets and gas bombs
to enhance the killing power of conventional high explosive and flame
weapons. Fourteen million pounds have been used thus far, enough
to cover all of Vietnam with a field effective concentration. Many
nations, including some of our own allies have expressed the opinion
that this kind of gas warfare violates the Geneva Protocol, a view
shared by M cCarthy.
A Biological Weapons Convention
Amid great pushback over US conduct in Vietnam, in November 1969 President Nixon announced to the world we were going to end the US biowarfare program (but not the chemical program). In February 1970 Nixon announced we would also get rid of our toxin weapons (snake, snail, frog, fish, bacterial and fungal toxins that could be used for assassinations, etc.). Furthermore, Nixon said the US would initiate an international treaty to prevent the use of these weapons ever again. And we did: the 1972 Convention on the prohibition of the development, production and stockpiling of bacteriological (biological) and toxin weapons and on their destruction, or Biological Weapons Convention (BWC) for short, which entered into force in 1975.
The BWC established conferences to be held every 5 years to strengthen the Convention. The expectation was that these would add a method to call for ‘challenge inspections’ to prevent cheating and would add sanctions (punishments) if nations did not comply with the treaty. However, the US has consistently blocked the addition of protocols that would have an impact on cheating. By now, everyone knows that cheating occurs and is likely widespread.
A leak in an anthrax production facility in Sverdlovsk, USSR in 1979 caused the deaths of about 60 people. A clear BWC violation. US experiments with anthrax production during the Clinton administration, detailed by Judith Miller et al. in the 2001 book Germs were also thought by experts to have transgressed the BWC.
In 1997 a Chemical Weapons Convention came into force. It took over 20 years, but all official stocks of chemical weapons have been destroyed by the USA and by Russia and the other 193 member nation signatories.
Pandemics or Biological Warfare?
So here we are. It is 2023 and the WHO Director General has declared 2 pandemics (the current terminology is ‘Public Health Emergency of International Concern’) over the past 3 and a half years: COVID-19 and monkeypox, which was renamed MPOX to “avoid stigma.” I am sure the monkeys were relieved by the name change.
I have previously (in my substack) described why I believe both SARS-CoV-2 and MPOX were bioengineered pathogens that came from labs. I do not know if they leaked or were deliberately released, but I am leaning toward deliberately released for both of them, based on where they appeared, how they spread, and in particular the official responses to each—neither of which was explained accurately to the public, and yet we never changed course, even when the lack of efficacy with masks, social distancing, EUA drugs and vaccines had become clear.
Vaccines: the Chicken or the Egg?
Both the monkeypox vaccines (there are two, Jynneos and ACAM2000) are known to cause myocarditis, as do the two COVID-19 mRNA vaccines and the Novavax vaccine. The Novavax vaccine was first associated with myocarditis during its clinical trial in Australia. I have written about all this previously on substack.
How frequently does myocarditis occur after these vaccines? If you use elevated cardiac enzymes as your marker, ACAM2000 caused this in one in thirty people receiving it for the first time. If you use other measures like abnormal cardiac MRI or echo, according to the CDC it occurs in one in 175 vaccinees. We do not know the number for Jynneos, but there was some degree of elevation of cardiac enzymes in 10% and 18% of recipients in two small prelicensure studies. My guess for the mRNA vaccines is that they are somewhere in this range. I don’t know about Novavax’ vaccine.
Why would our governments push 5 separate vaccines all known to cause myocarditis on young males who have been at extremely low risk from COVID, and who simply get a few pimples for 1-4 weeks from monkeypox unless they are immunocompromised? It’s an important question. It does not make medical sense. Especially when the vaccine probably does not work — Jynneos didn’t on the monkeys in whom it was tested. And CDC has clammed up about the 2,000 Congolese healthcare workers on whom CDC tested it for efficacy and safety in 2017. (I have detailed this too in earlier substacks.)
The health authorities could have just been ignorant—that could explain the first 8 months of the COVID vaccines’ rollout. But once they figured out, and even announced in August 2021 that the vaccines did not prevent catching COVID or transmitting it, why did they still push it on low risk populations who were clearly at greater risk from a vaccine side effect?
Once this is acknowledged, you realize that maybe the vaccines were not made for the pandemic, and instead the pandemic was made to roll out the vaccines. I’m not sure. But I’m suspicious. And the fact that multiple countries contracted for 10 doses per person makes me even more suspicious—for vaccines whose safety and efficacy had not been established. WHY would you want ten doses apiece? Three maybe. But ten?
Furthermore, you don’t need a vaccine passport aka digital ID aka justification to convert to all-electronic money unless you are giving out regular boosters. Were the vaccines conceived of as the pathway to getting our vaccinations, health records, official documents and financial transactions all online—as Ukraine has already done?
A Pandemic Treaty and Amendments: Brought to you by the same people who mismanaged the past 3 years, to save us from themselves?
The same US government and western governments that imposed draconian measures on their citizens to force us to be vaccinated and take dangerous, expensive, experimental drugs and withheld the good drugs, decided in 2021 we needed a pandemic treaty to prevent and ameliorate future pandemics or biological warfare events… so we would not suffer as we did with the COVID pandemic.
Except COVID was a disaster due to its mismanagement (or should I say dismanagement or malmanagement?) by our nations’ rulers, their bosses and the WHO. Hundreds of millions of our fellow human being were slammed into extreme poverty—by nations following guidelines issued by the WHO, whose main job it was to protect exactly those people. Tens of millions died from starvation as a result. Yet the WHO blathers on about equity, diversity and solidarity—having itself caused the worst (manmade) food crisis in our lifetimes. Have you heard any apology or explanation?
How can anyone with a brain believe the public health officials who messed up COVID so badly want to spare us from another medical and economic disaster, after they imposed the last one on us? And the fact that no governments or health officials will admit their mistakes — especially how they made it nearly impossible to obtain the cheap and safe drugs that effectively treat COVID — why would we let them plan anything, let alone an international treaty that will bind our governments to obey the WHO’s dictates? How thoughtful of these officials to want to spend a king’s ransom of our money to prevent the next government-caused disaster.
We are fed up with secret vaccine contracts, waivers of liability for junk medical products, and spikes in sudden deaths and chronic disabilities. No more secret negotiations. Please shove your pandemic planning where the sun…
The Gain of Function farce
Obviously, the best way to spare us from another pandemic is to immediately stop funding “Gain of Function”* research, and get rid of what has already been funded and created. Let all the nations make big bonfires and burn up their evil creations at the same time, while allowing other nations to inspect their biological facilities and records.
But the WHO in its Bureau Text of the draft Pandemic Treaty has a plan that is the exact opposite of this. In the WHO’s world, which almost all nations’ rulers have bought into, all the governments will share any and all viruses and bacteria they come up with that have “pandemic potential” — share them with all the other governments. They are supposed to sequence them and then put the sequence online. No kidding. Then the WHO and all the Faucis of the world would gain access to every Frankenstein virus, at once. Presumably a bunch of hackers would also gain access to the sequences. Does this make you feel more secure?
The WHO Treaty draft incentivizes Gain Of Function research
At least this plan makes clear whose side everyone is on. Fauci, Tedros and their ilk at the WHO, and those managing biodefense and biomedical research for nation states are on one side, the side that gains access to even more biological weapons, and the rest of us are on the other, at their mercy.
This crazy plan used to be called proliferation of weapons of mass destruction—and it is almost certainly illegal. But it is their plan. Governments will all share the weapons. And they are to put a lot more money into biolabs, and especially into genomic sequencing. Presumably so they can make even better weapons, and maybe they will even get around to cures or antidotes. But who will get the cures? It wasn’t us during the COVID-19 pandemic. Here is where you can read the current Treaty draft:
https://apps.who.int/gb/inb/pdf_files/inb5/A_INB5_6-en.pdf
Pages 10 and 11:




What else is in the Treaty? Gain of Function research (designed to make pathogens more transmissible or more virulent) is explicitly incentivized. Administrative hurdles to it must be minimized, while unintended consequences (pandemics) should be prevented: (page 14)

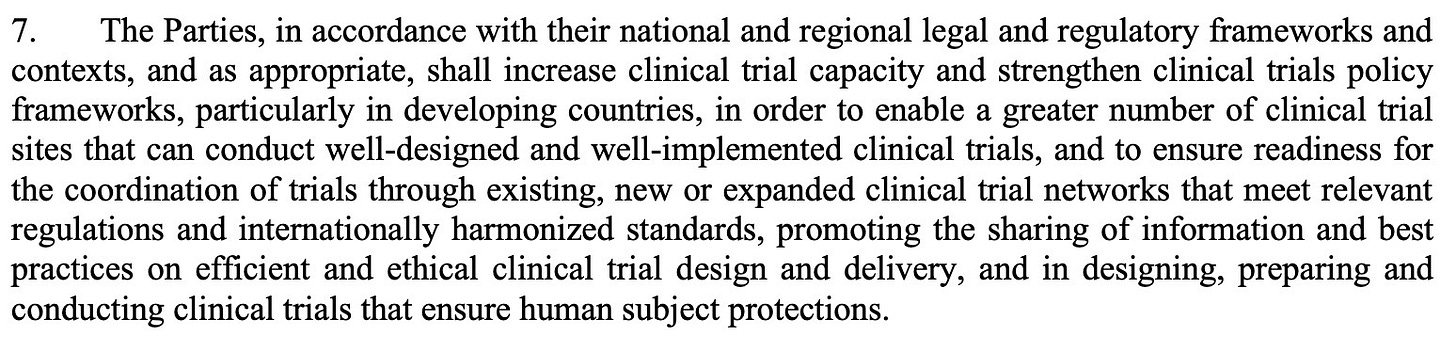
Vaccines will be rolled out speedily under future testing protocols
Just in case you thought the COVID vaccines took too long to be rolled out, the WHO has plans to shorten testing. There will be new clinical trial platforms. Nations must increase clinical trial capacity. (Might that mean mandating people to be human subjects in out-of-the-way Africa, for example?). And there will be new “mechanisms to facilitate the rapid interpretation of data from clinical trials” as well as “strategies for managing liability risks.” (page 14)
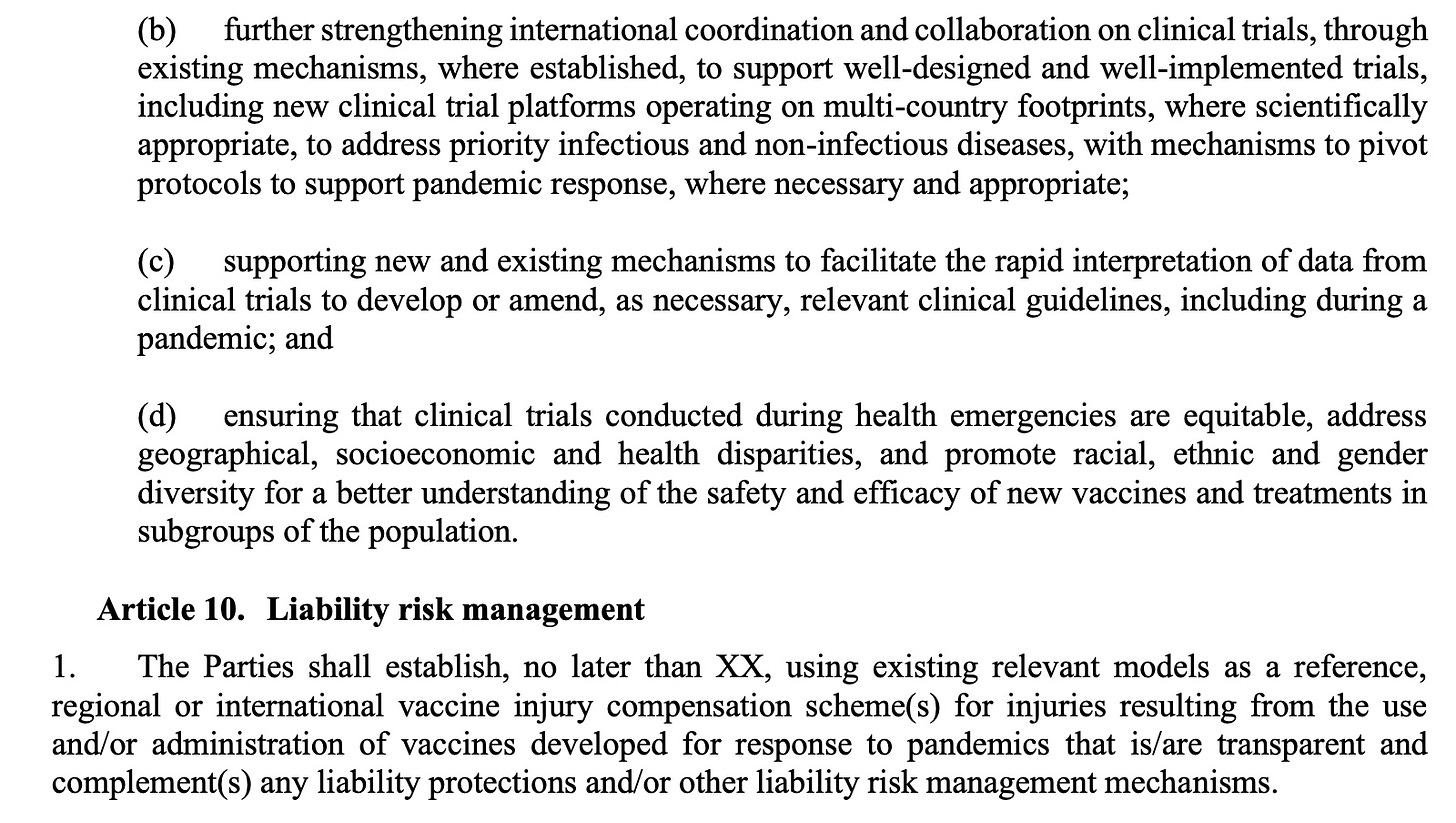
Manufacturer and government liability will be “managed”
Nations are supposed to use existing models as a reference for compensation of injuries due to pandemic vaccines. Of course, most countries do not have vaccine injury compensation schemes, and when they do the benefits are usually minimal. The US government scheme for injuries due to COVID pandemic products (the Countermeasures Injury Compensation Program or CICP) has compensated 4 (yes, FOUR) people as of July 1, 2023. All pandemic EUA drugs and vaccines fall into this program (monoclonal antibodies, early remdesivir, paxlovid, molnupiravir, some ventilators and all COVID vaccines). There have been nearly 12,000 claims made to the CICP related to a COVID product. Slightly over 1,000 have been adjudicated while 10,886 are pending review. Twenty claims were deemed eligible and are waiting to see whether they can collect. A total of 983 people, or 98% had their claims denied. About 90% of all claimants filed for a vaccine injury.

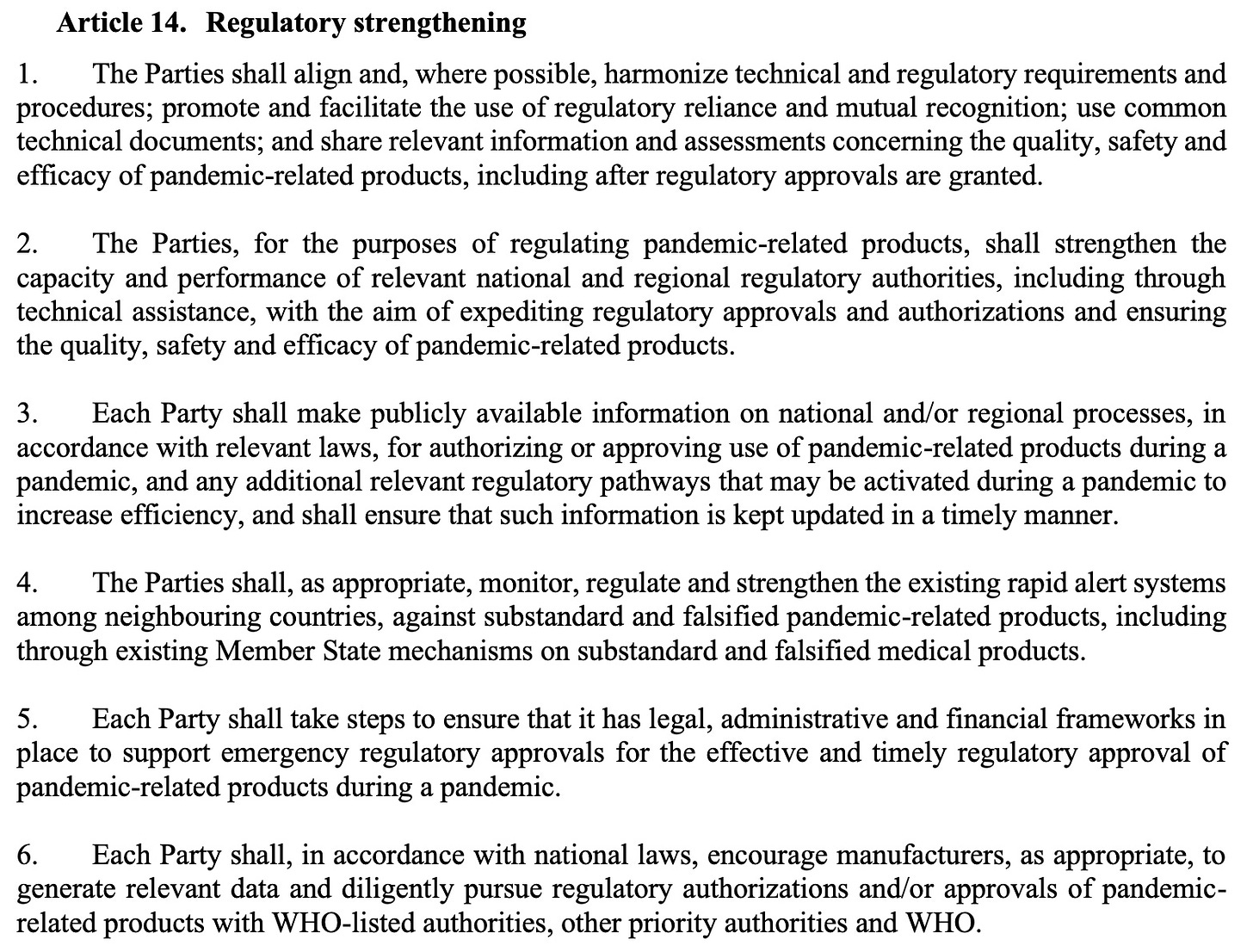
The treaty draft also demands weakening the regulation of medical drugs and vaccines during emergencies under the rubric of Regulatory Strengthening. As announced in the UK last week, where ‘trusted partner’ approvals will be used to speed licensure, this is moving toward a single regulatory agency approval or authorization, to be immediately adopted by other nations (p 25)
Why would any developed country sign up for this? Is this what we the people want?
The WHO did sweeten the pot, however. Remember how the need to respect “human rights, dignity, and freedom of persons” was removed in the WHO’s draft IHR Amendments that are being negotiated? Well, WHO apparently did not like us pointing that out—so the old human rights language that was removed from the International Health Regulations draft has been added to this newest version of the Treaty.
There is much more I could say about problems with this draft of the Treaty, but I will save them for another time.
Please share this brief analysis of the WHO’s Pandemic Treaty. We must EXIT the WHO.
*Gain of Function is a euphemism for biological warfare reserch or germ warfare research. It is so foolhardy that it was banned in the US for SARS coronaviruses and avian flu viruses from 2014-2017 due to public outcry by scientists. Then in 2017 Fauci and Collins lifted the moratorium, claimed they were putting safeguards in place, which were just a handwaving exercise, and off we were to the races: creating new bioweapons. Fauci and Collins had the nerve to publish their opinion that the risk was ‘worth it.’
PSYOP-19 UPDATE: New Variant Spreading Across UK – As Overall Cases Continue to Rise
2nd Smartest Guy in the World | August 5, 2023
The followup “pandemic” trial balloon intended to gauge the level of future societal “mandate” compliance has now been officially deployed.
According to the latest Mockingbird article by SKY NEWS entitled, COVID-19: New variant spreading across UK – as overall cases continue to rise:
A new COVID variant is spreading across the UK, according to the UK Health Security Agency (UKHSA) – and already makes up one in seven new cases.
Scientifically known as EG.5.1, it is descended from the Omicron variant of COVID.
The UKHSA has been monitoring its prevalence in the country due to increasing cases internationally, particularly in Asia, and it was classified as a variant here on 31 July.
Since viruses never mutate into more virulent strains, we must ask: is this another gain of function (GoF) release by the usual Intelligence Industrial Complex criminals, and their useful idiot “expert” apparatchiks ahead of the fall and winter flu season, or is this a consequence of the “vaccinated” genetically modified humans incubating and transmitting new viral mutations as a function of the Modified mRNA slow kill bioweapon injections?
In the week beginning 10 July, one in nine cases were down to the variant.
The latest data suggests it now accounts for 14.6% of cases – the second most prevalent in the UK.
It appears to be spreading quickly and could be one reason why there has been a recent rise in cases and hospitalisations.
COVID-19 rates have continued to increase – up from 3.7% of 4,403 respiratory cases last week to 5.4% of 4,396 this week.
The latest data also shows the COVID-19 hospital admission rate was 1.97 per 100,000 population, an increase from 1.17 per 100,000 in the previous UKHSA report.
Officials say they are “closely” monitoring the situation as COVID case rates continue to rise.
It is no surprise that the wholly fraudulent PCR tests are what these “officials” are yet again referencing; in other words, they are up to their same old junk science tricks.
“We have also seen a small rise in hospital admission rates in most age groups, particularly among the elderly,” said Dr Mary Ramsay, head of immunisation at the UKHSA.
“Overall levels of admission still remain extremely low and we are not currently seeing a similar increase in ICU admissions.
“We will continue to monitor these rates closely.”
Senicide is the gift that keeps on giving, as said “officials” happily discharge liabilities and assets of the elderly useless eaters. Any eugenics program worth it’s salt always commences with the oldsters, and then works it way across ever larger swaths of society.
The Arcturus XBB.1.16 variant – another descendant of Omicron – is the most dominant, UKHSA figures show. It makes up 39.4% of all cases.
Another variant with a menacing name and lots of decimals, another opportunity for the One World Government’s main eugenics node in the WHO to fear-monger:
The World Health Organisation (WHO) started tracking the EG.5.1 variant just over two weeks ago.
As this Substack has exposed on several occasions now, the WHO’s director-general is a Marxist war criminal deliberately selected for his extreme sociopathy by the Rockefeller Crime Syndicate’s most prominent puppet and genocidal frankenmosquito advocate Billy Boy Gates:
WHO director-general Tedros Adhanom Ghebreyesus said though people are better protected by vaccines and prior infection, countries should not let down their guard.
“WHO continues to advise people at high risk to wear a mask in crowded places, to get boosters when recommended, and to ensure adequate ventilation indoors,” he said.
They also just can’t let up on the absurdly useless MK Ultra masks, because ensuring that the genetically ruined slaves reinforce their mass induced fear slavery is an effective means of self-policing into ever more mindless compliance.
“And we urge governments to maintain and not dismantle the systems they built for COVID-19.”
Of course, the WHO urges that their unconstitutional and anti-human systems for PSYOP-19 not to be dismantled because they need their said systems for their followup PSYOP-23 “pandemic” this fall.
What the WHO certainly does not want you to know is that inexpensive repurposed drugs will act as prophylaxis against all of their “pandemics,” along with the associated plethora of their “vaccine” induced adverse events like turbo cancers, and prion-based diseases, all while also protecting the genetically unmodified refuseniks from “vaccine” shedding, and environmental damage.
Do NOT comply.
Pfizer Ad Spreads Misinformation
BY DAVID ZWEIG | SILENT LUNCH | AUGUST 1, 2023
A Pfizer ad on Twitter claims that 3 out of 4 US adults are at “high risk” for severe Covid-19.
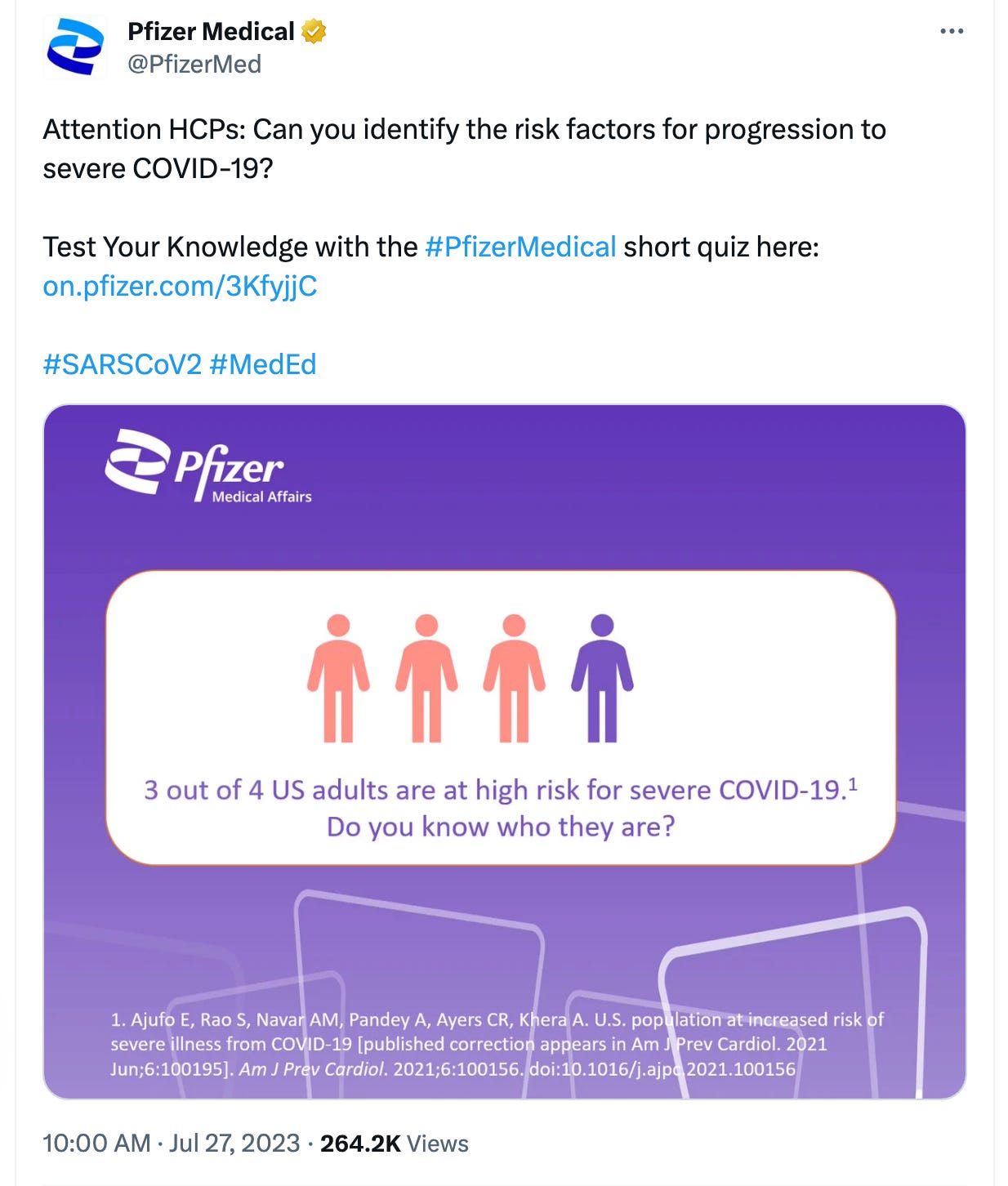
This ad is highly misleading or, arguably, outright false.
Problem 1: What is “high” risk?
We don’t know because Pfizer doesn’t define it.
The graphic in the ad cites a study as the source of its claim “3 out of 4 US adults are at high risk for severe Covid-19.” Except the study never uses the term “high risk.” Rather, the study is on people at “increased risk.”
“Increased risk,” of course is quite different from “high risk.” Obviously, high risk is worse than merely increased risk. I need not explain why Pfizer would choose language in its ad that exaggerates the risk of Covid.
Problem 2: The cited study itself doesn’t even define “increased risk.” Does that mean a 0.1% increase, a 1% increase, 20% increase, 1000% increase? On this point, the study includes the following caveat: “the effect size of each risk factor was not taken into account in our analysis, so this report does not address degree of risk. Effect estimates of severe COVID-19 risk factors are widely variable and ultimately unreliable.”
Digging a little deeper, the study links to a CDC webpage that gives a list of conditions for people who are “more likely to get very sick with COVID-19” and uses “higher risk,” “increased risk,” “greater risk” and “high risk” in its text, seemingly interchangeably. The page gives a long list of medical conditions—from cancer to diabetes to depression. Still, we don’t know what “more likely” or “increased risk” actually means. This webpage, in turn, links to another CDC webpage that describes “Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19.”
We’ve gone from the scary “high” risk (not defined), to “increased” risk (also not defined), to “higher risk.” How is “higher risk” defined? Here is what the page says:
Higher risk is defined as an underlying medical condition or risk factor that has a published meta-analysis or systematic review or underwent the CDC systematic review process. The meta-analysis or systematic review demonstrates a conclusive increase in risk for at least one severe COVID-19 outcome.
So we are now three layers deep and we still don’t have a quantifiable definition for what, exactly, “high,” “increased,” or “higher” even means, nor a clear differentiation of what the first study acknowledges is a wide variability in estimates of risk factors. I’m sure there is a quantifiable threshold defined somewhere, but I stopped digging because this isn’t even the main problem.
Problem 3 (the main problem): The data from the cited study in the Pfizer ad saying 3 out of 4 US adults are at high (aka increased) risk of severe Covid are from 2015-2018. But this ad is being run in July 2023—after nearly the entire population has either already been infected, vaccinated, or both, each circumstance, we have been told, decreases one’s risk of severe Covid. In other words, Pfizer’s own ad suggests that prior infection and vaccination have not reduced the number of people at high risk of severe Covid. Does Pfizer want us to believe that its product—the vaccine—did not lower the rate of people at high risk of severe Covid?
The fact is, 3 out of 4 US adults are not at “high” risk of severe Covid. This statement is based on data from before accounting for the protective effect of infection and vaccination. Moreover, “high risk” is not defined and appears to simply be a made up description.
We’ve heard a lot about “misinformation” in the past few years. Generally, the government and media have pointed the finger at so-called “anti-vaxxers” and “conspiracy theorists.” A critical spotlight from the government has rarely seemed to shine on claims made by Pfizer. Advertisements like this misinform and unnecessarily scare people, perhaps pushing some of them into taking additional doses of the vaccine, or therapeutics like Paxlovid (also made by Pfizer), that have potential harms, and for many people, especially now, without clear benefit.
Document Specials: Dr. Peter McCullough about mRNA-vaccine death
Dr. Peter McCullough | July 27, 2023
Death counts were very important for government and public institutions during the Covid-19 pandemic and yet again death is being used as fearporn to scare people into accepting climate change, whilst sudden death, an increase in hospitalizations and an increase in diseases somehow never seemed to interest governments nor the public institutions. Why? Because it’s all connected to the “safe and effective” mRNA-products.
Dr. Peter McCullough, cardiologist and president of the McCullough Foundation, has yet again experienced censorship as the medical journal The Lancet removed a study written by Dr. McCullough and his colleague, within the first 24 hours of it being published. Dr. McCullough and his colleagues found that 74 percent of 325 autopsies of people who died after covid vaccination, were caused by the vaccine.
In this interview Dr. McCullough fills us in on the study, why it was removed and also what was found in the Danish study, which shows that the Pfizer vaccine was an experiment with peoples lives.
Welcome to Document Specials.
Follow Dr. Peter McCullough:
Website, www.petermcculloughmd.com
President, McCullough Foundation, www.mcculloughfnd.org
Author, Courage to Face COVID-19, www.couragetofacecovid.com
Radio Show, www.americaoutloud.com/author/dr-peter-mccullough/
Substack, petermcculloughmd.substack.com/
Follow our Document News Rumble channel where all our international broadcasts are streamed and uploaded.
Mask Indoctrination is Strong in Boston
The Naked Emperor’s Newsletter | July 28, 2023
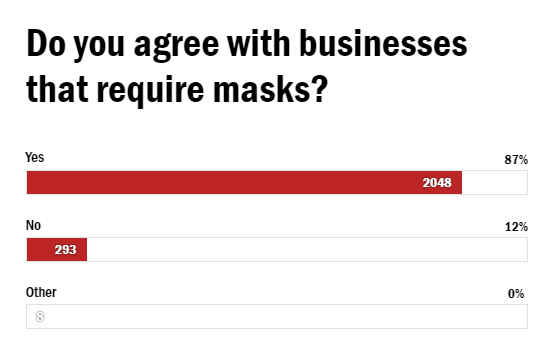
Boston.com, a regional website providing news and information about the Boston, Massachusetts region, posted an article a few days ago that reads as if it was from 2021.
Many businesses in the Greater Boston area have decided to continue requiring masks in stores because they are concerned about the 745 confirmed Covid cases! With that in mind, Boston.com asked their readers whether they agree with the businesses who still require masks. 87% of 2,300 readers who responded agreed that wearing masks is the right thing to do.
One of the main reasons given for masking was to protect the immunocompromised and vulnerable. Great if that worked or made a difference, but it doesn’t.
Sammie H. from Boston says that wearing masks to stop the spread can show that one cares about others.
“Preventing spread of illness shows that you care about others around you,” she said. “Masking is one small way to do just that. You might even save some lives, like the lives of those who are immunocompromised.”
Readers also decided masking was the correct course of action to prevent Long Covid.
“[Long COVID] took out myself, my partner, and many people I know with fatigue, lung issues, cold like symptoms and weird stuff like stomach issues. Masks help limit the spread and save people years of pain for a few minutes of minor discomfort, like a seatbelt,” said reader Berinthia from Somerville.
Many readers still think that preventative measures are needed for good now that Covid is endemic and will always be around.
“Nothing has changed, there is still a virus circulating that has killed millions and is continuing to do so, as well as disabling countless more,” she said. “When we all wear masks, we are all protected. It’s good for business and it’s good for people’s health.”
Other reasons given included:
- “I think essential services, especially medical settings, and transportation should still require masks so they are safe for people who can’t avoid them, and I applaud any businesses that choose to require masks — it reduces community spread and helps everybody.”
- “It would be much more physically safe for me, both as a retail employee and as a customer, if masks were still required in businesses around town.”
- “I want to stay alive and want others to be alive too.”
- “Because I care about keeping others safe(r) from COVID and other airborne disease. And because ‘high risk’ people (which include people who’ve been infected with COVID once or more) deserve to have access to spaces that are too high risk if everyone is unmasked. “
- “We should follow the science, not the latest fashions of political fanaticism. Wearing a mask is a minor inconvenience; long COVID or death is not.”
- “COVID-19 is still very much with us — killing and disabling a mass amount of people every day. Masks are an effective way to protect yourself and others, especially the most vulnerable. I want those that I know and love, and even those that I don’t, to live a long, long time.”
- “Business owners who require masks are doing community service by keeping themselves safe (thus able to stay healthy enough to continue operations) and our communities safer by reducing viral spread.”
The brainwashing is strong in Boston.
How Real-World Evidence Contradicts ‘The Science’
BY DR CLARE CRAIG | THE DAILY SCEPTIC | JULY 29, 2023
In September 2020, I became one of the first U.K. doctors to speak out about damaging Covid policy. Since January 2021, I have co-chaired the multidisciplinary HART group, publishing evidence-based analysis on Covid issues in an attempt to educate the public.
In 2021 it became clear that it was very challenging to persuade people face-to-face that the Government had chosen a dangerous path with its Covid policies. If someone listened long enough to understand one crucial point, the conversation would end with them in cognitive dissonance, unable to reconcile their other beliefs with what they had just learned.
The obvious answer to requiring someone’s attention for a little longer was to write a book. The challenge was to write in a way that ensured no reader would feel angry or foolish. The result was, Expired – Covid the untold story, a book that tackles 12 key Covid myths related to virus spread, lockdowns, asymptomatic infections and the efficacy of masks. Each one is addressed from the starting point of what was the dominant belief system before showing where the arguments did not fit. Each of these beliefs is interspersed with chapters which investigate the psychology of our beliefs, why we believe what we believe, the impact of fear and what it takes to change our minds.
It is a readable book for a layperson and consequently it is not the maths book that many people expected me to write. Instead, it is a summary of what the evidence shows and leaves the details to be referenced elsewhere. It is rich with metaphors and analogies to ensure that even complex concepts are digestible. It also covers far more than just science and psychology. To fully understand the issues requires a history lesson, a bit of religion and plenty of understanding of human failing!
A central theme is the significantly overlooked role of aerosols in exhaled breath – a crucial factor in virus transmission. A comprehensive understanding of this sheds light on why lockdowns and other restrictions failed to yield expected results. However, the physicists specialising in aerosols, despite their expertise, were disregarded and silenced by the medical community, which was tenaciously holding on to a misinformed belief about aerosols that almost unbelievably centred on the wrong number being used in a textbook.
Complicating the matter, the medical community still held onto echoes of a 150 year-old debate between germ theory and miasma theory, causing physicians to dismiss the possibility that microorganisms could be airborne via aerosols, despite a substantial body of evidence supporting this.
The irony is that the proponents of germ theory, who had to fight fiercely for their views to be accepted, adopted some beliefs, specifically about close-contact transmission and asymptomatic transmission, which were not supported by empirical evidence. Because these ideas had been entrenched in medical education and textbooks, they were perceived as fact and seldom challenged.
I have always enjoyed reading non-fiction but was always in awe of how much work the authors must have put into their books. It turns out I was right about just how much work such a book takes! The meticulous research meant that I learnt a lot on the way too so I hope that even if some of the story is familiar to you, there will be plenty for you to learn too.
More than any of the above, Expired is a call to action to reinforce the ethical principles that have guided Western societies for centuries, highlighting the damage done by overriding them during the pandemic and the urgent need to restore them.
Now that the fear and panic era of Covid is finally dissipating it is time for a rational and calm reanalysis of events. The Covid Inquiry is years away from reporting on political decision-making and so far there is marked evidence of bias in the approach being taken. Expired makes sense of the real-world evidence and exposes how ‘The Science’ was based on flawed assumptions that led to devastating policy.
I thoroughly explored avoiding Amazon altogether and using independent publishers, warehousing and shipping but it was simply not economically viable. It is therefore available exclusively on Amazon. It is available as a paperback, on Kindle or as an audiobook (read by me). The reviews so far have been overwhelmingly positive and I would really appreciate your feedback too.

Dr. Clare Craig is a diagnostic pathologist and co-Chair of the HART group. She is the author of Expired – Covid the untold story.
Featured Video
US Military: Who’s Pulling the Strings? /Lt Col Daniel Davis
or go to
Aletho News Archives – Video-Images
From the Archives
From glorious millennia to death and destruction: Zionists rewrite Palestine’s story

By Miko Peled | MintPress News | September 20, 2021
One of the great tragedies of Palestine is that almost every day there is a commemoration of one massacre or another, the death of a child or destruction of a home or village, leading one to think that the Palestinian narrative is one of death and destruction, which is what Israel wants people to think. But the truth is that this is not the case. The Palestinian narrative is one of a glorious history with periods of great sadness and tragedy. It is the Zionist story that is full of killing, stealing and destruction and not, as they try to sell it, one of creation and growth.
September 16, 2021, marked 39 years since the massacres at Sabra and Shatila refugee camps in Lebanon. As people remember and mourn the thousands of unarmed civilians who were butchered and the countless who survived suffering terrible injuries and emotional scars, we must also remember the man that stood behind this bloodbath.
This was a man whose complicity even the Israeli authorities could not ignore, the former general and renowned war criminal Ariel Sharon. And although he was momentarily penalized and banished from politics, he very quickly returned, and for a quarter of a century, he was the most powerful and influential man in Israeli politics. … continue
Blog Roll
 Aletho News
Aletho News- US Military: Who’s Pulling the Strings? /Lt Col Daniel Davis
- University of Vienna Student Assembly votes for academic boycott of Israeli universities
- Pro-Israel voices win out, kill bill to stop US-Israel military integration
- Khamenei: US-Israeli System of Domination Has Been Defeated
- Iran to deepen ties with ‘principal strategic partner’ China: Ghalibaf
- House Votes to Terminate Iran War, While Preparing to Vote to Ramp Up the Ukraine War
- IRGC: No peace without Israel’s withdrawal from occupied Lebanese territories
- Israeli war chief vows continued strikes on Lebanon as part of ‘conditional’ truce
- UNIFIL peacekeeper killed after shells strike position near Marjayoun
- Hours after reiterating ‘ceasefire’, ‘Israel’ targets car in S.Lebanon
- If Americans Knew
- The battle for Al-Aqsa: How Israel is reshaping the status quo
- Israeli study finds starvation in Gaza was result of deliberate policy
- US-Israel integration in NDAA is far from ‘America First’ – Joe Kent
- Now will the world believe? Israeli study finds starvation in Gaza was deliberate policy – Daily Update
- The Faustian Bargain of Journalists Embedding with the Israeli Military in Gaza
- AIPAC: Defending the Indefensible
- “You Either Leave Right Now or You Die”—Israel’s Ethnic Cleansing of a Village in Lebanon
- Selling American dead bodies to the US Navy for Israeli military training?
- AIPAC affiliate has funded lavish trips to Israel for dozens of Congress members since 7 October, filings reveal
- Trump called Netanyahu crazy, stopped Israel attack on Beirut: three articles
- No Tricks Zone
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
- Germany’s AfD Party Calls Debunked Climate Scenarios “Greatest Fraud In Human History”
- Researchers Find Rapid Global Warming Phase At End Of Last Ice Age (Ca.18,000 Years Ago)
- Even The DNA Of Single-Celled Plankton Can Upend Alarmist Arctic Sea Ice Melt Claims
- Scandal: Although Climate Panic Is Canceled By IPCC, Europe’s Policymakers Continue With Their Crushing Policies
