Why is Nature Praising the Use of Propaganda During the Pandemic and Calling for More?
BY DR GARY SIDLEY | THE DAILY SCEPTIC | NOVEMBER 15, 2022
Throughout the Covid era, those expressing views at odds with the dominant narrative were often subjected to unprecedented levels of censorship and psychological manipulation. Academic journals played a significant role in this silencing of alternative voices by, for example, ignoring the work of established scholars, perpetuating bias, rejecting research papers that reached conclusions inconsistent with mainstream views, and demonstrating a financial motivation to only publish studies favourable to the pharmaceutical industry. As a consequence of this partiality, the perceived scientific integrity of academic periodicals has suffered considerable damage. Alas, a recent article in the once highly respected Nature journal will have done nothing to improve the credibility of the academic press.
The article, titled “Mastering the art of persuasion during a pandemic“, is a supplementary ‘outlook’ piece written by Elizabeth Svoboda, a Californian science journalist. Drawing on the perspectives of a cluster of social science experts, Svoboda lauds the importance of health policymakers deploying “effective communication strategies” so as to ensure that the populace do the right things when faced with the next global pandemic. She asserts that a range of behavioural science strategies, or “nudges”, will be of central importance in enhancing compliance with public health restrictions when the next novel respiratory virus emerges over the horizon. The article, however, is riddled with highly questionable assumptions and ideological biases.
The Covid science is not settled
Arguably the most blatant distortion, illustrated many times by both the author and the experts cited, is that the Covid science is settled and their version is the definitive truth. The article opens with the ludicrous suggestion that the official advice in early 2020 – that masking healthy people would achieve no benefit – was a “fateful moment”, a missed opportunity “to stop the virus bringing the world to a halt”. In support of this assertion, Rob Willer, a sociologist at Stanford University, describes this initial guidance as “a big credibility mistake”, and goes on to suggest that it was an example of public health experts trying to protect the supply of masks to healthcare. According to Willer, this noble white lie led to many people feeling “resentful” at having been misinformed and it fuelled their reluctance to adhere to subsequent mask requirements. Totally ignored is that most of the more robust, real-world evidence concludes that masking healthy people achieves no meaningful reduction in viral transmission, and the U-turn in mid-2020 towards mask mandates was not the result of new research findings but was – more likely – politically motivated.
Similarly, the raft of unprecedented Covid restrictions (lockdowns, shutting businesses, school closures) inflicted on Western citizens by the public health establishment are all assumed to achieve important benefits so that the only challenge for the pandemic experts is how to persuade the pesky people to comply with them. Consequently, the article cites the ideas of a number of social scientists regarding how to effectively lever compliance with future public health diktats. Varun Gauri, a senior economist, highlights the importance of making it easier for people to ‘do the right things’. Matthew Goldberg, a research psychiatrist, wants the psychological persuasion techniques of behavioural science to be used pre-emptively “so that when the time arises, people can act quickly”, a view echoed by infection-control researcher Armand Balboni. Katy Milkman, a behavioural scientist, promotes her strategies to enhance the take-up of Covid vaccines, including a “regret lottery” where people are informed that their names have been entered into a draw to win a lot of money, but that the “winner” will lose the prize if not vaccinated.
Despite the wealth of accumulated evidence that lockdowns are ineffectual in reducing Covid-related hospitalisations and cause huge collateral damage, alongside the emerging realisation that Covid vaccines may achieve no overall net benefits and can do considerable harm, nowhere in the article is there even a hint of recognition that the restrict-and-jab doctrine of mainstream public health failed to achieve many of its stated aims.
One important negative consequence of the flawed ‘science is settled’ assumption, as displayed by the author and her expert contributors, is that it justifies the censoring and vilification of anyone challenging the dominant narrative. For example, Varun Gauri says, “During the COVID-19 pandemic, disinformation played a major part in sowing division and undermining the authority of health officials” and that this “paved the way for fast viral spread and low vaccination rates”. His solution is for authorities to “take a bigger, legislative approach to the problem” – a euphemism for censorship. Similarly, Katy Milkman warns against allowing “conspiracy theories to slither in”.
The controversy surrounding the acceptability of state-imposed ‘nudging’
It seems that all those involved in the Nature article are blissfully unaware of the controversy surrounding the state’s use of covert psychological strategies (or ‘nudges’) to promote compliance with Government restrictions. Blinded by their fixed belief that the Covid science is settled, and focused only on the goal of persuading the populace to ‘do the right things’, the social scientists cited in the commentary blithely propose a range of behavioural science interventions without any questioning around the appropriateness and ethical acceptability of these clandestine methods.
Nudges are psychological strategies of persuasion that largely impact upon their targets below the level of conscious awareness – that is, people do not know they are being influenced. Such techniques have been heavily deployed throughout the Covid era, and have evoked a range of ethical concerns relating to the acceptability of the state strategically (and non-consensually) increasing the emotional discomfort of its citizens as a means of promoting compliance with unprecedented and largely non-evidenced public health restrictions. Also, as the strategies operate subconsciously, they could often be categorised as manipulative.
The expert contributors referenced in the Nature article repeatedly commend greater deployment of these ethically dubious techniques in future pandemics. For instance, Balboni urges political leaders to ensure human behaviour specialists play a much bigger part in health policy, bemoaning that, during the Covid era, “social scientists, anthropologists and psychologists were not used nearly enough”. Later in the article, the purported benefits of the “pre-emptive deployment of behavioural science” is highlighted.
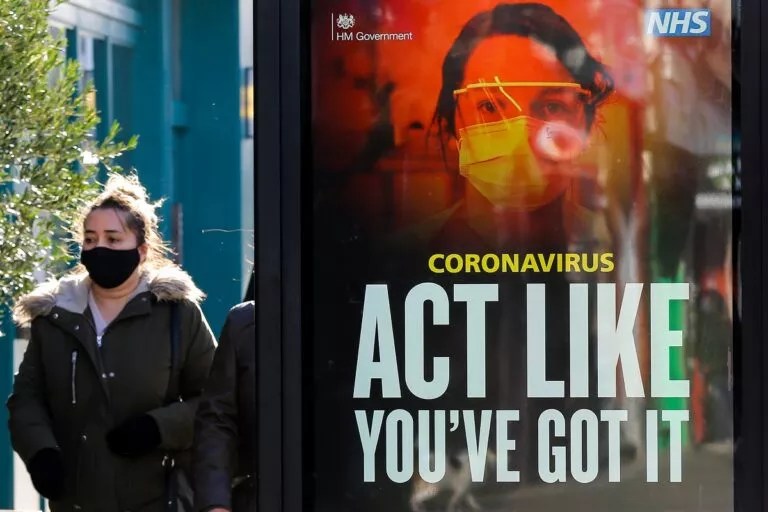
More specifically, the value of equating virtue with compliance with the restrictions is lauded. This particular strategy – an ‘ego’ nudge in behavioural science parlance – was used repeatedly throughout the Covid event, effectively evoking shame in anyone who deviated from the demands of public health diktats and the vaccination doctrine. Many will recall the repeated ‘I wear a face covering to protect my mates’ adverts, the ‘don’t kill your gran’ quips by ministers, and the close-up images of acutely unwell hospital patients with the voiceover, “Can you look them in the eyes and tell them you’re doing all you can to stop the spread of coronavirus?” Of the same ilk was the NHS document (later redacted) advising front-line staff to tell young people that, “Normality can only return, for you and others, with your vaccination” (my emphasis).
The Nature article endorses the same tactic of differentiating the goodies from the baddies. It is stated that, “Encouraging feelings of empathy in people could make them more likely to choose to protect others during a pandemic”. There are also references to the desirability of “invoking of empathy” and emphasising “the vaccines’ collective benefits, such as protecting others”. In the words of Balboni, it is really important to get people to recognise that “through their behaviour, they can actually protect other people”. Clearly, the considerable evidence demonstrating that Covid vaccinations do not prevent viral transmission has yet to reach these nudge enthusiasts.
In a Western supposedly liberal democracy, is it ethical for the state to strategically inflict shame on its citizens? Does the informed consent of the people, as to whether to accept a medical or psychological intervention, no longer matter? Is it acceptable to covertly influence the general population to follow contentious and largely non-evidenced Covid restrictions? Shamefully – pun intended – these key ethical considerations are totally disregarded in this Nature journal commentary.
The role of political ideology and conflict of interests
What might account for the publication of such a partisan article in an academic journal?
Many critics of Covid orthodoxy have raised the spectre of an underlying globalist agenda, removed from any democratic process, shaping Western responses to pandemic management. With the central involvement of the World Economic Forum (WEF), it has been argued that the crisis following the emergence of a novel respiratory virus has been opportunistically exploited in pursuit of wider, pre-existing goals pertaining to tackling climate change and the imposition of Covid Passes and Digital ID, Social Credit Systems, Central Bank Digital Currency and Universal Basic Income (as detailed in Agenda 2030). The authoritarian control over the world’s population (essential to realise such an agenda) is typically legitimised under the banners of ‘the greater good’ and ‘social responsibility’, two themes that run through the Nature article. Is it possible that the author and contributors adhere to this globalist ideology?
Exploration of the ongoing interests of those involved in the compilation of the article is revealing:
- Elizabeth Svoboda is a regular contributor to Greater Good online magazine.
- Varun Gauri is a member of the WEF and an economist at the Development Research Group of the World Bank.
- Rob Fuller is “Director of Polarisation and Social Change Lab” at Stanford University; he recently co-wrote an article in the Los Angeles Times titled, “How to convince Republicans to get vaccinated”.
- Matthew Goldberg is a research scientist at the Yale Program on Climate Change Communication.
- Katherine Milkman is Deputy Director at the “Behaviour Change for Good Initiative“, an enterprise that claims it uses behavioural science to “transform people’s lives for the better”.
Would it be too speculative to suggest that those involved in the Nature article harbour a penchant for a new world order, and that these globalist proclivities may have compromised their objectivity?
Finally, my eye was drawn to a footnote to the article that read: “This article is part of Nature Outlook: Pandemic preparedness, an editorially independent supplement produced with the financial support of third parties.” And who funds this supplement? Astra Zeneca and Moderna.
I rest my case.
Dr. Gary Sidley is a retired NHS Consultant Clinical Psychologist and co-founder of the Smile Free campaign. He blogs at Coronababble.
“I had to stand by idly, watching these people die.”
The crime committed against Dr. Paul Marik and his patients
By John Leake | Courageous Discourse | November 14, 2022
The following post is from The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex, by John Leake and Peter A. McCullough. MD, MPH.

Dr. Paul Marik testifying at the US Senate on January 24, 2022
At the same time that Dr. McCullough was stripped of his job and professorships, his colleague and kindred spirit, Dr. Paul Marik, experienced a similar fate. On October 15, 2021, his hospital’s administration circulated a memo to the entire healthcare system stating that its doctors were authorized to administer remdesivir to COVID-19 patients, but not ivermectin or a host of other repurposed drugs. As Dr. Marik read the memo, he marveled at the sheer perfidy of it. Especially grotesque was the inclusion of “Ascorbic acid” (vitamin C) on the list of banned substances.
The administration issued this directive at a time when seven COVID-19 patients were in the ICU, desperately in need of Dr. Marik’s care. He, in turn, desperately wanted to treat them with the drug regimen that he knew would give them a good chance of recovery. Three months later, at the January 24, 2022 panel discussion (COVID-19: A Second Opinion),hosted by Senator Ron Johnson, Dr. Marik recounted his helplessness. His heart-wrenching testimony (starting at 4:19:30) was probably the most dramatic moment in the extraordinary conference.
This system was effectively preventing me from treating my patients according to my best clinical judgement. … As a clinician for the first time in my entire career, I could not be a doctor. I could not treat patients. I had seven Covid patients [he holds up his hands showing seven digits] including a 31-year-old woman. I was not allowed to treat these people. I had to stand by idly [he clenches and raises his fists with anguish and begins to weep]. I had to stand by idly, watching these people die.
I then tried to sue the system, so then they did something called peer sham review. It is a disgusting and evil concept. They then accused me of seven most outrageous crimes … and [claimed] that I was such a severe threat to the safety of patients, they immediately suspended my hospital privileges because I posed such a threat to these patients—ignoring the fact that under my care, mortality was 50% less than it was under my colleagues. I then went on to this sham peer review. I went to a Kangaroo Court, where they continued this, and the end result was that I lost my hospital privilege and was reported to the National Practitioner Databank. So here I was standing up for my patients’ rights, and this hospital, this evil hospital, ended my medical career.
DR MIKE YEADON COVID DEATH SHOTS IS MEDICAL MURDER
Dr Mike Yeadon – Let’s not put a Gloss on It. The COVID death shots Is Medical Murder
First RSV Emergency Declared as Pfizer and GSK Race to Get Vaccines Approved

By Michael Nevradakis, Ph.D. | The Defender | November 8, 2022
Southern California’s Orange County Health Department this month declared a local health emergency over concerns around the rising number of pediatric cases of Respiratory Syncytial Virus (RSV).
County officials also declared a Proclamation of Local Emergency, allowing them to access state and federal resources in response to the spread of RSV.
The news came amid media warnings of a looming “tripledemic” of RSV, influenza and COVID-19 and news that Pfizer and GlaxoSmithKline (GSK) are close to securing regulatory approval for their RSV vaccine candidates — including Pfizer’s RSV vaccine for pregnant women.
RSV was first identified in 1956, and frequently affects children, with a majority of childhood cases occurring before age 2. For most children, symptoms are similar to those of the common cold, according to the Centers for Disease Control and Prevention (CDC).
It can, however, cause serious symptoms in the very young and the elderly, although childhood deaths are infrequent, according to CDC data.
According to California attorney Rita Barnett-Rose, there’s no evidence to support claims that Orange County hospitals are overextended, or to justify a state of emergency.
In an interview with The Defender, Barnett-Rose drew parallels between Orange County’s emergency declaration for RSV and other state, local and federal emergency declarations for COVID-19:
“One of the other alarming things that happened with COVID is when [Gov. Gavin] Newsom declared the state of emergency in COVID. He also waived the 30 and 60-day review periods for all local governing boards.
“So, yeah, so that’s what everyone is concerned about, this perpetual state of emergency.
“And the other thing that it triggers is it asks, once they declare a state of emergency, aside from getting the funding, it also triggers a request to Governor Newsom to declare a statewide state of emergency and then also to have Newsom ask President Biden to declare a national state of emergency.”
That could lead to Emergency Use Authorization (EUA) of RSV vaccines, according to Barnett-Rose, who told The Defender there may be an avenue to challenge the legality of the latest Orange County emergency declaration.
Is pharma using the COVID playbook to push RSV vaccines?
Dr. Regina Chinsio-Kwong, Orange County’s health officer, said in a press release county officials issued the declaration due to “rapidly spreading virus infections causing record numbers of pediatric hospitalizations and daily emergency room visits.”
The declaration will allow the county to access state and federal resources and to allow non-pediatric hospitals to offer beds to sick children, Chinsio-Kwong said.
Children’s Health Defense (CHD) California Chapter notes that this declaration was unanimously ratified “over the objections by members of the public who showed up to speak against the declarations.”
Dr. Melaine Patterson, chief nursing officer for Children’s Health Orange County, said area hospitals are seeing an “unprecedented” volume of children visiting their emergency rooms — approximately 400 per day, with wait times of “four to 12 hours.”
She also said that, as of Nov. 1, there were 285 patients in her hospital, compared to 188 on that date last year, adding that 11 of those current patients were placed in ICU as a result of RSV infections. RSV cases also are on the rise nationally.
Chinsio-Kwong advised the public to remain “up to date with other vaccinations such as flu and COVID-19” to “reduce the burden on hospitals this fall and winter.”
“Our best shot at protecting ourselves and our children from respiratory illnesses continues to be the same things we practiced throughout the pandemic including the use of masks when indoors around others and staying home when you are sick,” Chinsio-Kwong said.
However, Barnett-Rose said hospitals in Orange County may be overextended not due to an unusually high number of admissions, but due to unvaccinated staff having been let go.
She told The Defender :
“I do think that has a big role in it, and a lot of people pointed that out during the hearings and public comments were made about that.
“They were trying to claim … there were not enough pediatric experts or pediatric-trained doctors and medical professionals, so they needed to go outside of the county. And I do think a big part of that is that they did let go of many pediatric nurses and pediatric physicians that refused to take the vaccines. So I do think that this is a crisis of their own making … if there is even a crisis.”
San Diego County also issued a warning to its residents Nov. 4 over rising RSV cases but stopped short of declaring an emergency.
CHD California questioned why Orange County would declare a “Local Health Emergency” now — even though local COVID-19 states of emergency haven’t been lifted.
Despite claims that the purpose of these new declarations is exclusively meant to help county hospitals, CHD California said, “the language of the emergency Resolutions says something else entirely”:
“Both the Resolution to ratify the Local Health Emergency under Health & Safety Code section 101080 and the Proclamation of a Local Emergency under Government Code section 8630 declare the need for these local emergencies not only based on the asserted need to handle allegedly rising cases of RSV — but also because of other unnamed ‘other respiratory illnesses’ that were not discussed during the special meeting or otherwise disclosed to the public.”
Barnett-Rose provided insights into the legal meaning underlying these declarations. She told The Defender :
“There’s a local health emergency, which is declared by the public health officer as opposed to the [county] board … and that is when the health officer says … ‘I’ve been talking to the hospitals and we’ve done some assessments and there’s an increasing rate of respiratory illnesses and the children’s hospitals, and so, because of this, I am asking to declare a local health emergency.’ …
“But her authority to declare a local health emergency only lasts for seven days unless it’s ratified by our board of supervisors. And so, on Nov. 2, our board ratified that, which means now it’s in place and it needs to be renewed or looked at every 30 days, unless Governor Newsom waives that condition.”
CHD California argued that the “overly broad language used in these emergency declarations should be deeply concerning to anyone wary of a repeat of the “public health” measures ordered under COVID-19,” noting that adding the vague statement referring to “other respiratory viruses” creates “plenty of room for further abuse.”
Barnett-Rose told The Defender that, during the Nov. 2 meeting, Chinsio-Kwong said, “No restrictions are currently [emphasis added] in place,” a statement that “caused … a little bit of an uproar during the hearing because of her wording, which suggests that indeed they may end up rolling out mask mandates or some other mandates.”
Under this type of “slippery language,” argued CHD California, even the common cold could be used to issue an emergency declaration.
Barnett-Rose agreed:
“How do you measure that? How do you dispute it? How do you examine it? How do you end it?
“If you’re going by one infectious disease, at least you can try to find some data on hospitalizations or cases or deaths or ICU beds. But when it’s everything, it can still include COVID, flu, cold, COPD, a whole bunch of things that would qualify as respiratory illnesses.”
Barnett-Rose said that attempts will be made to legally challenge these declarations as “overbroad,” noting, however, that while case law precedent exists to challenge overbroad legislation, there is no such precedent in place for states of emergency.
Barnett-Rose she’s looking into whether there’s some way to litigate against these broad states of emergency.
When statutes are overbroad, she said, sometimes you can challenge them for being overley broad or too vague, but she’s not sure if there’s a similar precedent for challenging an overly broad state of emergency.
Declaring a local state of emergency at the county level could trigger a chain of events leading all the way to a national declaration of emergency, according to CHD California:
“By ratifying and/or declaring these local emergencies, the Board has now triggered an official request to Governor Newsom that he also declare a state-wide state of emergency on the same overly broad basis — and to ask the President of the United States to declare a national state of emergency.”
“A nationally declared state of emergency may trigger all of the same measures that have already deeply divided our country: masks on airplanes, business and school closures, and coercive school and employee mandates for experimental ‘vaccines’ offered as the ‘only solution’ back to Freedom,” CHD California argued.
Barnett-Rose said the emergency declaration in Orange County may be tied to the fact that there are multiple RSV vaccines already in the pipeline:
“The reason this is becoming really huge news is because this is what happened with the COVID state of emergency, too, it kind of went like that in dominoes.
“Once Biden declares a national state of emergency, then that triggers all of the emergency use authorizations that allowed the so-called vaccines for COVID. And I’m sure you already know that there’s vaccines in the works now for RSV that they’re floating out there in the news as well.”
Recounting events that occurred in relation to COVID-19, Barnett-Rose told The Defender that Orange County and some other counties in California declared a state of emergency, “then it went to the state, then it went national, and then, of course, once there’s a national emergency, you can go into Iowa.”
“So I do think that this is very suspicious timing, the articles that we are seeing in the news about being close to this RSV vaccine,” Barnett-Rose said. “And so, I do think that they’re trying to repeat the same playbook.”
Up to 30 RSV vaccine candidates already in pipeline
Pharmaceutical industry publication FiercePharma reported that Pfizer and GSK “moved closer to regulatory approvals” in the past week, and “could each see the first-ever approvals for an RSV vaccine in 2023.”
GSK’s candidate will be reviewed May 3, 2023, while Pfizer is “eyeing an approval filing by year-end.”
In all, up to 30 RSV candidate vaccines have been identified by the National Institutes of Health (NIH).
GSK has secured priority review status for its RSV vaccine following the submission of data from its AReSVi-006 phase 3 trial. The candidate vaccine exclusively targets adults 60 and older, and the data reportedly “showed high overall vaccine efficacy against RSV lower respiratory disease” at a rate of 82.6%, Fierce Biotech reported.
GSK initially intended to develop an RSV vaccine for older adults and for infants, but plans for the latter were shelved due to a “safety concern.” Nevertheless, GSK CEO Emma Walmsley in a call last week with investors described GSK’s new vaccine as “a very significant scientific achievement.”
Previous efforts to develop an RSV vaccine have failed because they “had a persistent tendency to cause worse disease,” due to “a phenomenon known as antibody-dependent enhancement (ADE).”
Dr. Ruth Karron, a pediatrician and professor of international health at the Johns Hopkins Bloomberg School of Public Health, said, “The difference this year is the general public for the first time is probably eagerly awaiting an RSV vaccine, because they’re seeing firsthand just how much of a problem RSV can be,” in a statement drawing a clear connection with the reported increase in RSV cases this year.
Pfizer announced Nov. 1 that its own candidate RSV vaccine wrapped up its phase 3 trial for efficacy early. Unlike GSK’s candidate vaccine, Pfizer’s vaccine targets pregnant women. The vaccine is designed to be administered early in the third trimester with the intent that the vaccine-induced antibodies be passed from the mother to her newborn.
Pfizer, in its Nov. 1 announcement, claimed that its bivalent RSV prefusion vaccine candidate RSVpreF, also known as PF-06928316, delivered “broadly positive” results — namely, a significant reduction in the rate of respiratory illness in newborns and their mothers.
Pfizer claimed 81.8% efficacy against severe cases of RSV for babies up to three months, and 69.4% efficacy after six months.
Pfizer’s MATISSE (MATernal Immunization Study for Safety and Efficacy) trial involved 7,400 pregnant women and their newborns, tracking the infants for one year following birth, and some for two years. It was conducted in 18 countries beginning in June 2020.
Pfizer’s vaccine trial did not deliver statistically significant results regarding the prevention of infant medical visits caused by RSV, including for non-severe cases.
Nevertheless, Pfizer said there are “no major safety concerns” with its product, adding:
“At the recommendation of the DMC [Data Monitoring Committee], and in consultation with the U.S. Food and Drug Administration (FDA), Pfizer has stopped enrollment in the study.
“Based on these positive results Pfizer plans to submit a Biologics License Application (BLA) to the FDA by the end of 2022 for the vaccine candidate followed by other regulatory authorities in the coming months.”
Pfizer’s phase 3 trial data has not yet been vetted by independent experts, and has not been peer-reviewed or published.
On March 2, 2022, Pfizer’s candidate vaccine received a Breakthrough Therapy Designation from the FDA, while previously, in November 2018, the FDA granted it Fast-Track status, according to the Pfizer release.
“Pfizer’s investigational RSV vaccine candidate builds on foundational basic science discoveries including those made at the National Institutes of Health (NIH),” the vaccine maker said in its press release.
The NIH research in question also was “key to the hugely successful COVID-19 vaccines,” according to ABC 7 Los Angeles.
Others looking to develop an RSV vaccine include Moderna and AstraZeneca and Sanofi, in a joint initiative. Moderna received fast-track designation from the FDA on Aug. 3, 2021, for its mRNA-1345 RSV vaccine for older adults, while AstraZeneca and Sanofi are developing a viral vector RSV vaccine by the name of “nirsevimab.”
An August 2021 article in The Defender predicted that RSV would represent the “new frontier for vaccine development,” as pharmaceutical companies would be “lured by the prospect of a large untapped global RSV vaccine market,” leading to a vaccine development “gold rush.”
Media tout benefits, ignore safety concerns
Online news portal Vox described the development of new RSV vaccines as “very, very good news” in a recent article.
Coupled with media coverage about “rising” RSV cases nationwide, it appears the stage is being set to create an emergency in the public consciousness, which could lead to EUAs being granted to the new vaccines and a rush to get the public vaccinated.
Blogger James Roguski, however, called into question the results of the Pfizer phase 3 trial, raising many safety concerns that are indicated in the company’s own data but were downplayed by Pfizer in its public proclamations. In a recent post, he wrote:
“In the Phase II study, researchers found that women who received RSVpreF vaccine containing aluminum hydroxide had a higher incidence of local reactions than those who received RSVpreF vaccine without aluminum hydroxide.
“It seems like 1 of the 117 infants in the placebo group suffered fetal death and 6 infants in the ‘vaccinated’ group are unaccounted for.”
Roguski also highlighted the many adverse events that were recorded for both infants and pregnant mothers who participated in the study, none of which were recorded for the placebo group.
For infants, some of these adverse events included acute respiratory failure, bronchiolitis, cardiac murmur, chordee (bent penis), conjunctival hemorrhage, hypoglycemia, jaundice, low birth weight, neonatal hypoxia, neonatal respiratory failure, seizure, sepsis, upper respiratory tract infection and vascular malformation.
Pregnant women, in turn, experienced adverse events including fetal growth restriction, fetal tachycardia, gestational diabetes, nonreassuring fetal heart rate pattern, premature labor, premature separation of placenta, vaginal hemorrhage and thrombocytopenia.
For some, these safety concerns are conjuring up memories of previously failed attempts to develop an RSV vaccine.
A vaccine tested in 1966 led to the deaths of two toddlers as a result of “enhanced disease symptoms,” while many infants “suffered worse symptoms than usual, and needed to be hospitalized.”
As previously reported by The Defender, RSV itself originated in monkeys housed in a Maryland facility where they were used to conduct polio vaccine research. Remarking on this and the connection to RSV vaccine development today, Brian Hooker, CHD’s chief scientific officer, told The Defender, “It is incredible that the vaccine industry can create a disease — RSV from the polio vaccine — and then create another vaccine to ‘prevent’ that disease. Talk about a business proposition!”
Michael Nevradakis, Ph.D., based in Athens, Greece, is a senior reporter for The Defender and part of the rotation of hosts for CHD.TV’s “Good Morning CHD.”
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Band of Brothers
Dr. Paul Marik and his fellows in the FLCCC fight for patients’ rights. All have paid a heavy price for taking care of patients and telling the truth.
By John Leake | Courageous Discourse | November 12, 2022
Part I in a series on Dr. Paul Marik—a magnificent doctor who was fired from his job and professorship because he successfully treated his COVID-19 patients with FDA-approved drugs and high-dose Vitamin C.
The following post is from The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex, by John Leake and Peter A. McCullough. MD, MPH.
Dr. Paul Marik is to critical care medicine what Dr. McCullough is to cardio-renal medicine. The 65-year-old native of South Africa has published over 500 peer-reviewed papers and books, which made him the second most published critical care doctor in the history of medicine.
Dr. Paul Marik with Dr. Peter McCullough and John Leake at the Nurses Freedom Network Conference in Franklin, TN, June 12, 2022
Upon meeting Dr. Marik, one is overwhelmed by the impression of his vast physical stature. His gentle manners and elegant South African accent conjure accounts of 19th century British gentleman explorers. Since the early days of his career, he’d been keenly interested in discovering how to treat sepsis—the body’s extreme, life-threatening response to an infection. Well into the 21st century, sepsis continued to be a major cause of death. According to the CDC, approximately 1.7 million American adults fall ill with sepsis every year, of which approximately 270,000 die in hospital. Globally, the sepsis burden is estimated at 15 to 19 million cases annually, with a mortality rate approaching 60% in low-income countries.
Dr. Marik knew the literature on sepsis treatment. Several studies had indicated that large doses of IV-administered Vitamin C and Vitamin B1 (thiamine) showed some benefit. Other studies indicated that hydrocortisone showed promise. Dr. Marik reasoned that combining the three into a cocktail could amplify their benefit. As had often been observed in medicine, combining agents seems to affect multiple pathways, causing an overlapping and synergistic effect.
In 2016, he and his colleagues conducted a study in which they compared 47 sepsis patients who received the cocktail to a control group of 47 patients who received sepsis standard of care at the time. The mortality rate of the treatment group was 8.5% compared to 40.4% of the control group—a stunning difference. Skeptics claimed the study was too small and nonrandomized. Nevertheless, what became known as the “Marik Cocktail” was adopted by critical care units all over the world, which reported excellent results with the therapy.
When COVID-19 struck and Dr. Marik’s critical care unit at the Sentara Norfolk General Hospital received its first patients, he observed they were suffering from an inflammatory lung reaction, and he suspected this could be treated with a corticosteroid. He contacted four other critical care specialists—Professor Joseph Varon at United Memorial Medical Center in Houston (who, in the year 2020, would work 268 days straight treating COVID-19 patients in his ICU) Professor Gianfranco Umberto Meduri at the University of Tennessee Health Science Center in Memphis, Professor Jose Iglesias at the Hackensack Meridian School of Medicine in Seton Hall, New Jersey, and Professor Pierre Kory at the University of Wisconsin-Madison. As author Michael Capuzzo pointed out in his marvelous story about these doctors, it would be hard to imagine a more experienced and scholarly team of pulmonary critical care doctors.
Together they formed the Frontline COVID-19 Critical Care Consortium (FLCCC) and got to work on a protocol for saving hospitalized patients. They started their work by focusing on the extreme inflammation they were observing. Often called “cytokine storm” after the proteins produced by the immune system, this was an extreme and maladaptive immune response that had often been observed in other viral illnesses, including virulent influenza. It was this inflammation of the lungs, kidneys, and other organs that killed the patient, and not the virus itself. Thus, the key to treating the syndrome was reducing this inflammation.
Professor Meduri was a leading expert on corticosteroid therapy in critical illness. He conducted an exhaustive review of corticosteroid use against SARS-CoV-1, MERS, and H1N1 and found significant evidence that these agents had been lifesaving in their reduction of extreme inflammation. For decades the corticosteroid methylprednisolone had been the standard medication for suppressing cytokine storm. And yet, despite this glaring fact, every US federal health agency recommended against using corticosteroids against COVID-19 from the outset of the pandemic.
Unlike these agencies, the FLCCC concluded that their best bet for tackling the disease in hospitalized patients was a combination of Methylprednisolone and the antioxidant Ascorbic acid (Vitamin C). To these they added Thiamine (Vitamin B1) to optimize cellular oxygen utilization and energy consumption, and the anticoagulant Heparin to prevent and help in dissolving blood clots that appear with high frequency.
There is nothing experimental about these drugs. Methylprednisolone and heparin had long been FDA-approved for treating inflammation and blood clotting. Vitamin C and B1 were available over the counter, though in the hospital setting they were IV-administered in high doses. The FLCCC doctors began giving this “MATH Protocol” to ICU patients and tracked their progress for a case study. By the end of April, they had treated 100. Of these, 98 survived. The two who died were in their eighties and had other advanced chronic illnesses. None of the patients had long durations on ventilators, were ventilator dependent, and or had long hospital stays.
During this period, Dr. Pierre Kory was in daily communication with ICU doctors in his native New York City, where he’d worked in multiple hospitals. His colleagues reported that they turned the tide in the ICUs as soon as they started using methylprednisolone. Other ICU doctors in hard hit New Orleans reported the same. Kory and colleagues therefore sent letters to the White House, the CDC, and the NIH, presenting their real-world evidence of the corticosteroid’s efficacy—all to no avail.
Dr. Kory’s efforts were drawn to the attention of Wisconsin Senator Ron Johnson, who was chairman of the Senate Homeland Security Committee. Since his daughter had been born with a congenital heart defect—successfully corrected by an innovative operation—Senator Johnson had believed that if citizens were faced with a life-threatening condition for which there was no proven treatment, they should have the right to try drugs or operations that seem to offer some benefit, even if these had not yet passed the conventional FDA-approval process. The alternative was to do nothing and accept the high probability of death.
Critics of the right to try claim that unless procedures and medications are carefully regulated by the FDA, unscrupulous doctors will create false hope by offering them to desperate patients, even if there is little trial data to prove their efficacy. Senator Johnson did not find this argument persuasive and he introduced his federal right to try bill in 2017. A companion bill was introduced in the House, ultimately passed in both houses, and was signed into law by President Trump in 2018.
Upon Senator Johnson’s invitation, Professor Kory addressed the Senate Homeland Security Committee on May 6, 2020. Speaking via WebEx, Kory stated the credentials of the FLCCC doctors, and then explained the rationale for using their protocol. He then reported the success they and other doctors were having with it. This was excellent news, and a naive viewer would likely assume that it would be welcomed by the entire medical profession.
And yet, despite the FLCCC’s well-founded rationale for their therapy, broad consensus for the efficacy of its components in related conditions, and their success with it, they continued to get pushback from the CDC and NIH, which refused to change their advisory against using corticosteroids to treat COVID-19. On four occasions, the FLCCC tried to notify the White House of their favorable results, but they received no reply.
Much Ado About Nothing
By Todd Hayen | OffGuardian | November 12, 2022
Do any of you think we are over-reacting? I don’t think so, but the sheep-folk certainly do. They claim they are willing to let bygones be bygones and just put it all in the past and get on with life.
I am sure everyone reading this is aware of the bombshell editorial The Atlantic dropped recently with their amnesty nonsense. I don’t think I have been more livid reading an article since the days of seeing piece after piece about how effective masks are against viral transmission.
I won’t comment on The Atlantic blather directly here, as there have been many fine responses to it, but wow, what a piece. So typical of a bully trying to pretend he loved his victims all along when he knows he is cornered and about to be punished. One last punch disguised as a kiss.
I just got back from a little cruise. Major ports were Barcelona, Rome, Florence, Monaco, and a smattering of little French and Italian hideaways. I had mixed feelings about going, but realized that if this tsunami we all see coming a few miles off the shore has the potential of wiping out most travel in the foreseeable future, I figured I might as well get something in before the onslaught.
It was nice in a lot of ways, as would be expected, but in other ways unusually disconcerting. For one thing, very, very few people had masks, and thus there was a palatable scent in the air of “Covid is a thing of the past.”
One would think this was a good thing, but instead it exuded a very clear vibe of denial.
Oddly enough, not wearing masks, and believing Covid to be over, to me is just another example of compliance to authority.
I know that seems a stretch, but if Covid were real, coupled with the truth that the vaccines do not work, and we were told again and again that there would be no natural herd immunity without a working vaccine, and we still hear of infections rising, variants being created, and hospitals becoming over crowded, why would people think the disease just died and disappeared? The reason is because we were told it was over.
We were told we suddenly didn’t need masks, that we could party with friends, vaxxed or unvaxxed, that we could gather in huge crowds, get on cruise ships (no one even cared that I was unvaccinated.) We were told what was true, what was real and what to worry or not worry about. And like sheep, most people blindly followed.
So shouldn’t I be happy? If I were, it would be for all of the wrong reasons. It is true we are all happy when the slave owner puts down the whip. Whip or not, however, we are still slaves.
I, too, bask in the sun of my controlled freedom—I went on a cruise didn’t I? After two years of not being “allowed to” — so I am just as guilty of this sort of compliance. I am one step closer to truth though; I know this offer of freedom is a tactic, a ploy, and a ruse.
I’ll take a scrap of bread when it is offered, but I will not succumb to complacency and forgive my master for his cruelty when he behaves, albeit for just a moment, as my friend. Most everyone else seems fine to let bygones be bygones.
I am not, and I suspect most of you reading this are not as well.
The great danger I see here in the masses just carrying on in complacent forgiveness is that they are encouraged to stay blind. Surely if they speak out against the atrocities that the world has experienced over the past three years they would quickly be categorized as a trouble maker, a pariah, and a misfit.
“Just get over it, man, it’s all over.”
Is it? No, of course not, you and I know that, and it is all still going on in various ways under the covers now, in the dark recesses of the culture: persecutions, continued efforts to vaccinate, and particularly vaccinate children, warnings of an “upcoming dark winter” where restrictions will come back into the mainstream. On and on, you know what I am speaking of.
However, the mass attitude now, as per The Atlantic piece, is “nothing all that much really happened.”
No one died unnecessarily due to the Covid response, no one got sick, no one lost their job or their livelihood, no one suffered socially (particularly children wearing masks in school), no one suffered educationally, nothing bad really happened.
If you are still pissed about all that DID happen, then you are overreacting… much ado about nothing.
So get over it, forget and forgive.
Not everyone in the world has read that article, but what I saw in Europe, it seems that most people, at least on physical observation, are basically taking on that attitude.
It breaks my heart.
I think about the countless mothers sitting by their children in countless hospitals nurturing them through a totally unprecedented heart incident.
I think of the countless families standing together at the funeral of a loved one, dead prematurely from a heart attack, blood clotting, or cancer—cause unknown, unless you want to apply the newly created diagnoses, “Sudden Adult Death Syndrome.” What the hell is that?
A novel disease and now a common cause of death? Easy peasy explanation, eh? I think of the countless numbers of people suffering from a myriad of strange afflictions, which suddenly appeared out of nowhere.
I think again of countless people having suffered unconscionably, and pointlessly, after losing their jobs, their businesses, their life savings, and their livelihood—the countless children with lower IQs, and those who have suffered social retardation due to the mask mandates, social distancing, and mandatory online teaching at home with no socialization at all.
I could write 100 pages describing all of this—but most people don’t know, and if they do, don’t care, or just attribute all of this horror to the “cost of living—some are lucky in life, some are not.”
During my recent cruise not a word was uttered about any of this, thousands of people were encountered walking the streets of Rome, Florence, Barcelona, all laughing, eating, drinking, playing. While just beneath their feet, hidden a foot underground, there are skulls and bones of the fallen—all forgotten, and the perpetrators all forgiven.
When I was occasionally shaken from my self-induced and compliant vacation reverie, my heart ached talking to all of the young vibrant crewmembers on our ship.
I would hear of their plans to be married, create families, further their careers and live fully their vibrant lives—followed with the admission that they all had to be vaccinated to get their current jobs on the ship.
What really lies ahead for these beautiful children of God so innocent and full of life? I would shake my head, “maybe none of this is true, and maybe I am making more of it than it really is. Maybe they are right, and it really wasn’t that bad, just a mistake made here and there that we really could get over. It is all fine… let’s move on.”
Then a bone cracks under my foot—just a few inches from the surface of awareness—the truth. And I slip back into reality.
Dr. Clare Craig On The Three Key Factors Of The Pandemic
The Fat Emperor – Ivor Cummins | November 9, 2022
Dr. Clare Craig is one of the best pathologists out there, and deeply understands the scientific details of the pandemic – and I caught her in person at the International health congress in Portugal – all scientific talks are here or will be uploaded shortly https://odysee.com/@MartaGB:2
Featured Video

Did the 9/11 Hijackers Really Fly the Planes?
or go to
Aletho News Archives – Video-Images
From the Archives
Aaron Siri’s Book: Vaccines, Amen
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
Aaron Siri makes it clear in Vaccines, Amen: The Religion of Vaccines that the story we’ve been told about vaccine science rests far more on belief than proof.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
And he does. … continue
Blog Roll
 Aletho News
Aletho News- Did the 9/11 Hijackers Really Fly the Planes?
- ‘Jewish lobby’ deceived Putin – Lukashenko
- The UK Joins the Pirates
- Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report
- Press TV reporter wounded in Israeli drone strike on southern Lebanon
- Time for Trump to Tell Benjamin Netanyahu to Go Away!
- Israeli officials: ‘Security zones’ to remain in Lebanon, Syria, Gaza
- Israel Fails to Sabotage Islamabad Accord… At Least for Now
- Araghchi: US Responsible for Implementing MoU with Iran
- US must cut military, intelligence assistance to Israel to protect Iran deal: Ex-Trump official
- If Americans Knew
- Jared Kushner’s Israel-linked island, and other dubious projects
- Why Are Crypto Billionaires and AIPAC Spending $8+ Million to Elect Adrian Boafo?
- Why the Mainstream Media Should Stop Using the ADL as Their Go-To Antisemitism Source
- Censorship and Thuggery Won’t Save Israel’s Reputation
- Israel Searches for a Red Sea Foothold in Somaliland
- They Weren’t Convicted of Terrorism, But These Palestine Activists Got Sentenced as Terrorists Anyway
- “Ceasefire” is not in Israel’s vocabulary – Daily Update
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- No Tricks Zone
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
