What Really Happened in the Pandemic
By Justin Hart | Rational Ground | May 26, 2022
Every year humans endures a “flu season” – a period denoting the high-water mark of that year’s wave of respiratory viral pathogens. Believe it or not we still have strains of the 1889 Russian flu, the 1918 Spanish flu, the 1957 Asian flu, the 1968 Hong Kong Flu, the 2009 H1N1 virus – all these various strains of nasty bugs rear their head every single year.
In late 2019, a new “novel” pathogen appeared on the scene – a bug from the “Coronavirus” family (“corona” describing the spike-like structure of the particles.) The official title was SARS-CoV-2. SARS = “severe acute respiratory syndrome”; CoV-2 = “Coronavirus 2.” This particular virus can cause a disease called COVID-19 (“Coronavirus Disease 2019”). The disease is thought to have originated in China and found significant human-to-human transmission. It is thought to be “novel” because prior infections of other pathogens do not seem to create anti-bodies to tackle this newfound disease within the human body.
Officials raised alarms about the potential mortality witnessed from COVID-19. Governments across the world scrambled to address and protect their populations from what quickly became a pandemic. Efforts ranged from stringent to downright authoritarian. Results were mixed to say the least. In early 2022, it was thought that SARS-Cov-2 and COVID-19 would join the panoply of viruses and diseases we experience during the annual ebb and flow of life.
That’s the short sterile version of what transpired.
Here’s what actually happened:
- Global elites had ramped up significant efforts to reshape the world to address a host of inequalities and imagined boogeymen like climate change.
- These global elites were bolstered by a host of corrupt institutions which included the WHO (“World Health Organization”), big pharmaceutical companies, and world wealth and health players like Bill Gates.
- With the emergence of a new virus these groups pounced at the vulnerable moment to put their plans into action and retool the world with a host of proposals – this was known as The Great Reset. The Coronavirus response was just the first sortie in this plan.
- Governments across the world, under the threat of serious mortality (real or imagined), caved to the plan of action which utilized never-before imagined cram downs on individual rights, massive financial expenses, and enhanced authority overhauls to set the stage for a shift of power.
- Free speech, right to assembly, right to bodily autonomy, representative government all fell within months of the first COVID-19 cases announced in almost every country.
- This newfound power and framework allowed this movement to latch on the decaying carcass of fragile democracies, societal empathies, and eggshell-walking politicos anxious about upcoming elections.
- Unprecedented global lockdowns of populations disrupted the entire flow of commerce and relationships.
- Trillions of tax dollars flowed into the coffers of every connected and corrupt institution under the guise of “protecting” the global populace from this apocalyptic pathogen.
- Disrupted businesses were “bought” off with zero-cost loans and grants to keep employees onboard and keep the money flowing so as not to destroy the economies all at once.
- A massive global testing regime was set up to catch the widest number of COVID-19 infections possible. The chosen test array (the PCR test) could pick up remnants of a virus at 5 days after infection or even 75 days.
- Hospitals were designated as the first point of care ensuring a massive wave of anxiety and alarming centralization of power still felt today.
- Deaths were counted with the widest-possible latitude ensuring a prominent psychological impact at every turn prompting policies mirroring population concerns.
- Governments bought and paid off new entities to ensure compliance. Threats of fines and operational shutdowns were made if new agencies failed to meet expectations.
- A global deterrence was crafted to ward off any pre-hospitalization treatments. The endgame was focused on the ultimate prize: a “revolutionary” vaccination framework thought to be the next generation in global medicine and health.
- An unprecedented wave of funding and government collusion was established to roll out a vaccine across the world.
- Government mandates ranged from coercive inconvenience to full-on house arrest. You could lose your job, your bank account, and your freedom in one fell swoop.
- Simplistic mechanisms of mask wearing were instituted as an outward sign of faith in the “new normal.” Politicians could then wipe their hands of outcomes by pointing to lack-of-use of such procedures.
- Children were targeted for ripe propagandist approaches ensuring that most vulnerable parts of our society were utilized as a bludgeon against anyone going against the grain.
- Wave after wave of virus variants proved a great excuse when vaccines didn’t perform as expected.
- Strategic gaslighting was employed by health officials to distract from their massive failures.
- War followed to cover up the disaster.
All of this was designed to latch onto a virus that many assert has unnatural origins. The ramifications of a man-made virus set loose upon the world by accident or on purpose should frighten us more than the virus itself. Someone was playing god and it appears they are just getting started.
My book, Gone Viral: How Covid Drove the World Insane comes out in September.
DR. MCCULLOUGH ON MONKEYPOX
The Highwire with Del Bigtree | May 26, 2022
As the monkeypox outbreak saturates the news cycle, we check in with Epidemiologist and Cardiologist Dr. Peter McCullough to look into the danger the virus poses to the public.
Is This the Worst Excuse for Vaccine Failure Yet?
By Dr. Joseph Mercola | May 26, 2022
Well, the COVID jab pushers have had to resort to all sorts of obfuscation to hide the fact that the injections don’t work, and now they’re really scraping the bottom of the barrel of excuses. According to a recent Reuters report,1 “Increased contact among vaccinated people can give the false impression that COVID-19 vaccines are not working.”
This irrational explanation has been levied in response to studies showing COVID-jabbed individuals are getting infected at higher rates than the unjabbed, and there are many such studies.
“These studies are likely to involve statistical errors, particularly if they did not account for different contact patterns among vaccinated versus unvaccinated people,” Korryn Bodner, a research associate in infectious disease modeling in Toronto, told Reuters. Bodner is the first author of a preprint study2 posted on medRxiv at the end of April 2022.
Are the Jabbed More Carefree Than the Unvaxxed?
Bodner’s claim is that those who got the jab may be more likely to throw caution to the wind and mingle with others, hence getting infected more frequently, while the unjabbed may be more cautious because they know they’re vulnerable. This rationale is dubious at best, considering:
a)The unvaccinated have continuously been accused of not taking COVID seriously and going about their lives as normal
b)Those who have taken the jab are, by and large, a far more fearful lot; they tend to listen to the “authorities” and take all of their advice to heart, which would include avoiding large gatherings and close one-on-one interactions without wearing a face mask
Check out the following story, reported by Anchorage Daily News :3
“Arianne Bennett recalled her husband, Scott Bennett, saying, ‘But I’m vaxxed. But I’m vaxxed,’ from the Washington hospital bed where he struggled to fight off COVID-19 this winter … Bennett went to get his booster in early December after returning to Washington from a lodge he owned in the Poconos, where he and his wife hunkered down for fall.
Just a few days after his shot, Bennett began experiencing COVID-19 symptoms, meaning he was probably exposed before the extra dose of immunity could kick in. His wife suspects he was infected at a dinner where he and his server were unmasked at times …
‘He was absolutely shocked. He did not expect to be sick. He really thought he was safe,’ Arianne Bennett recalled. ‘And I’m like, ‘But baby, you’ve got to wear the mask all the time. All the time. Up over your nose.'”
Within days of his third dose, he got a serious case of COVID. Yet they blame it on hypothetical exposure to an apparently healthy food server. This kind of irrational reasoning is prevalent among those who got the jabs and who keep going back for more as they are part of the 30% of the population that have been completely brainwashed.
To reiterate what I’ve explained since 2020, asymptomatic spread is likely to be so rare as to be nonexistent.4 It was a lie perpetuated to drive up fear and prop up rising “case” rates that didn’t really exist. It’s basic virology that you cannot transmit a virus unless you have a “hot” infection, and if you have an active, transmissible infection, you have symptoms. The symptoms are a sign that your body’s defenses are kicking in to rid itself of the live virus.
No symptoms, no transmission. So, unless the server was feeling sick and went to work anyway, the simplest explanation for Bennett’s demise was the shot itself. And if the server was sick, the fact that Bennett got so ill suggests the shot is ineffective, even at two doses.
The pro-pharma shills want you to believe there are so many confounding variables, we can’t possibly draw any conclusions from data showing the shots don’t work. Yet looking at data from a wide spectrum of sources, all show the same alarming trends. What “confounding factor” could possibly account for ALL of them being misinterpreted?
An Unproven Hypothesis
Reuters 5 does note that Bodner’s simulations “do not prove that this type of bias affected studies of vaccine effectiveness versus the Omicron variant.” What it does show, according to Bodner, is that “even if vaccines work, increased contact among vaccinated persons can lead to the appearance of the vaccine not working.”
In other words, this is a hypothesis that has yet to be proven. Her modeling suggests it COULD make the jabs appear ineffective IF those who got the jab actually behave very differently from the unjabbed.
But again, it’s highly unlikely that the unvaccinated are avoiding exposure by steering clear of close contacts and crowds to a greater degree than those who got the jab. It’s far more reasonable to suspect that the shots don’t work.
On a side note, Bodner’s study was funded by the Canada COVID-19 Immunity Task Force.6 This task force is housed at McGill University in Montreal, Canada, and McGill University is a long-term recipient of grants from the Bill & Melinda Gates Foundation.7,8,9,10
What Do the Data Say About COVID Jab Effectiveness?
Based on data from around the world, it seems clear that the COVID gene transfer injections are not working. In fact, they’re having the opposite effect of what you’d expect from a real vaccine. According to a Washington Post analysis of state and federal data,11 in September 2021, when Delta was most prominent, 23% of those who died from COVID in the U.S. had received the jab.
In January and February 2022, when Omicron started dominating, that percentage jumped to 42%. In December 2021 and January 2022, just under half of all the COVID patients in intensive care at Kaiser Permanente’s hospital system in Northern California had also received one or more shots.12
Many argue that Omicron was more contagious than Delta, hence the higher death toll. But Omicron was also far milder than Delta, so why would the jabbed die at a higher rate from a less lethal variant than a more lethal one?
One attempt at an explanation is that the fatalities are now occurring primarily among the elderly. Nearly two-thirds of those who died from COVID during the Omicron wave were 75 and older. During the Delta wave, 75-year-olds and older accounted for just one-third of the deaths.13
But that was the case from the beginning, and it still doesn’t answer the question: Why would old people be more likely to die from a milder virus than a more serious one? To answer that question, the injection pushers revert back to the argument of waning potency. Two-thirds of those who died in January and February 2022 did not have a booster shot. According to Anchorage Daily News :14
“Experts say the rising number of vaccinated people dying should not cause panic in those who got shots, the vast majority of whom will survive infections. Instead, they say, these deaths serve as a reminder that vaccines are not foolproof and that those in high-risk groups should consider getting boosted and taking extra precautions during surges.”
So, in other words, the jab only works for a handful of months, and then you have to take another. And another. And another. According to the U.S. Centers for Disease Control and Prevention,15 the first two doses wear off after five months, necessitating a third dose, and the third dose wears off in just four months, at which time you’re supposed to get dose No. 4.
Israeli data16 show the effectiveness of shot No. 4 in preventing severe disease declines by 56% in just seven weeks. So, it appears the protection you get from the shots keeps getting shorter with each dose. Meanwhile, data show the shots can render you increasingly susceptible to all manner of infection and disease, through a wide variety of mechanisms.
Moderna Trial Data Reveal Repeated Infections Are Likely
Among such data is a preprint study17 posted on medRxiv April 19, 2022, which found adult participants in Moderna’s COVID jab trial who got the real injection, and later got a breakthrough infection, did not generate antibodies against the nucleocapsid — a key component of the virus — as frequently as did those in the placebo arm.
Curiously, placebo recipients produced anti-nucleocapsid antibodies twice as often as those who got the Moderna shot, and their anti-nucleocapsid response was larger regardless of the viral load. As a result of this reduced antibody response, those who got the jab may be more prone to repeated COVID infections. As reported by The Defender :18
“[T]he authors found that using the presence of anti-nucleocapsid (anti-N) antibodies to determine whether a person was exposed to SARS-CoV-2 will miss some infections. Thus, the sensitivity of this kind of test, when applied to vaccinated individuals, is not ideal.
However, there are more important implications19,20 of these findings … Specifically, the study implies that the reduced ability of a vaccinated individual to produce antibodies to other portions of the virus may lead to a greater risk of future infections in the vaccinated compared to the unvaccinated.
It is important to note that this is not just another argument for the superiority of natural immunity. Rather, this is evidence suggesting that even after a vaccinated person has a breakthrough infection, that individual still does not acquire the same level of protection against subsequent exposures that an unvaccinated person acquires.
This is a troubling finding, and something investigators conducting the Moderna vaccine trial likely knew in 2020.”
UK Data Confirm Results
These findings are corroborated by data from the U.K. Health Security Agency. It publishes weekly COVID-19 vaccine surveillance data, including anti-nucleocapsid antibody levels. The report21 for Week 13, issued March 31, 2022, shows that COVID-jabbed individuals with breakthrough infections have lower levels of these antibodies — a finding they attributed to the protective benefit of the shot:
“These lower anti N responses in individuals with breakthrough infections (post-vaccination) compared to primary infections likely reflect the shorter and milder infections in these patients.”
However, this interpretation is likely flawed, because less severe infection is associated with lower viral load, and as the study above demonstrated, the “vaccinated” have lower anti-nucleocapsid antibody levels than the unvaccinated at all viral load levels, but especially so at the lowest viral loads. As noted by The Defender :22
“This is one of the most significant findings of the study because it overturns the heretofore unchallenged idea that decreased seroconversion in the vaccinated is due to less severe infection in this population — which is a benefit provided by the vaccine.
However, this new study shows that even at low viral loads, the unvaccinated are more likely to seroconvert than those who are vaccinated. In fact, the difference in seroconversion rates is the greatest at lowest viral loads. The decrease in conversion rates is not a result of a benefit from the vaccine. It is a consequence of it.”
Boosted Now Have Three to Four Times Higher Case Rates
The Defender also reviews other U.K. data showing the COVID case rate is three to four times higher among those who have received a booster shot, compared to the unvaccinated. This is true for all age groups with the exception of children under 18:23
“What could explain such a large increase in infection rates among the boosted? Interestingly, the authors … warn that the unvaccinated may have contracted COVID-19 prior to the observation period — in other words, they may have acquired natural immunity previously, giving them added protection …
But their own data tells the opposite story. The boosted are more likely to contract the disease — by a factor of 3 to 4. How do we know whether the larger infection rates in the boosted are due to more robust immunity in the unvaccinated because of prior infection or due to an immune deficiency in the boosted?
The question can be definitively answered by examining the trend of infection rates [using] … the equivalent table from two months earlier. There is still a greater infection rate among the boosted, but it is only two to three times higher. If the authors’ hypothesis was correct, the more recent data should have shown less of a difference, not more.
If anything, their data support the finding that the decreased seroconversion rates in the vaccinated may be causing a greater risk of repeated infections.”
Walgreens’ Data
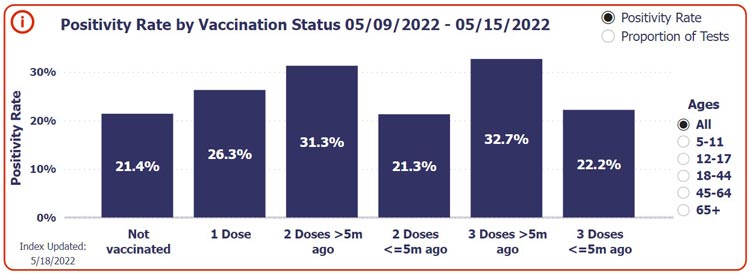
Data from the pharmacy chain Walgreens in the U.S. also reveal the same trend — COVID-jabbed individuals are testing positive for COVID at higher rates than the unjabbed, and those who got their last shot five months or more ago have the highest risk.
As you can see in the screenshot from Walgreens’ COVID-19 tracker24 below, during the week of May 9 through 15, 2022, 21.4% of unvaccinated individuals who got tested for COVID got a positive result. Of those who had gotten just one COVID shot, the positivity rate was 26.3%.
Of those who received two doses five months or more ago, 31.3% tested positive, and of those who received a third dose five months or more ago, the positive rate was 32.7%. So, after the first booster shot (the third dose), people are at greatest risk of testing positive for COVID.
Risk-Benefit Analyses
We also have the benefit of more than one risk-benefit analysis, and all show that, with very few exceptions, the COVID jabs do more harm than good. A risk-benefit analysis27 by Stephanie Seneff, Ph.D., and independent researcher Kathy Dopp, published in mid-February 2022, concluded that the COVID jab is deadlier than COVID-19 itself for anyone under the age of 80.
Another analysis,28 which relied on data in the U.S. Vaccine Adverse Events Reporting System (VAERS), concluded that in those under age 18, the shots only increase the risk of death from COVID, and there’s no point at which the shot can prevent a single COVID death, no matter how many are vaccinated.
If you’re under 18, you’re a shocking 51 times more likely to die from the jab than you are to die from COVID if not vaccinated. In the 18 to 29 age range, the shot will kill 16 for every person it saves from dying from COVID, and in the 30 to 39 age range, the expected number of vaccine fatalities to prevent a single COVID death is 15. Only when you get into the 60 and older categories do the risks between the jab and COVID infection even out.
A third risk-benefit analysis by researchers in Germany and The Netherlands was published in June 2021, in the journal Vaccines.29 The paper caused such an uproar, part of the editorial board resigned in protest.30 The journal retracted the paper, but after a thorough re-review, it was republished in the August 2021 issue of Science, Public Health Policy and the Law.31
These researchers concluded that, “as we vaccinate 100 000 persons, we might save five lives but risk two to four deaths.”32 A fourth, still preliminary, analysis — based on more than 1,700 death reports collected by Steve Kirsch — shows the shots do more harm than good in anyone under age 60. Kirsch writes:33
“Figure 1 below is an analysis of survey data I collected. The analysis shows that the vaccines are harmful to those under 60. The red dots higher than the error bar means more vaccinated people observed dead than expected based on the population of vaccinated to all people.
In other words, if we vaccinated 60% of people (middle of the grey bar) and 70% (red dot) of the deaths are vaccinated, we have a serious problem. The precautionary principle of medicine suggests if you are under 60 and thinking of taking a vaccine, you shouldn’t. These preliminary results are both statistically significant …
The conclusion is very clear: nobody under 60 years old should get the vaccine because there is no evidence of a benefit. In fact, if you are between 40-60, it’s clear that vaccination makes it more likely you’ll die, not less likely.”
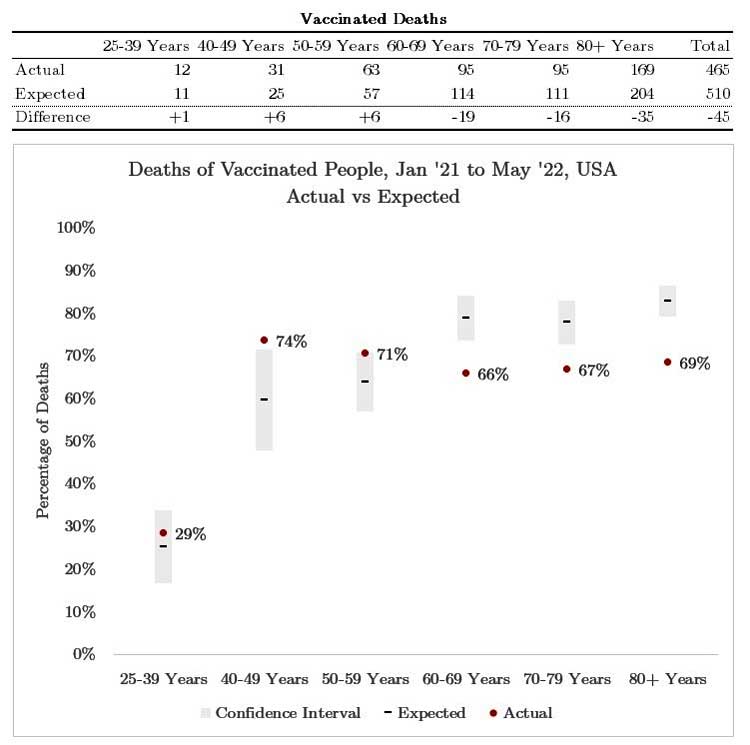
Figure 1. Red dot below error bar = vax works. Red dot above error bar = vax likely causes harm. Red dot inside the error bar = Insufficient evidence to justify taking a new, unproven vaccine. Conclusion: Vaccine shouldn’t be considered unless there is a clear benefit. 60 and older seems to justify use based on the data we have so far. Limitations: we are waiting for others to confirm / challenge the analysis. See text34 for more info. Joel Smalley did the analysis.
While some analyses present a direr picture than others, taken together, it’s clear that there appears to be no long term benefits to the COVID jabs. We’re consistently ending up with a higher cost than can conceivably be considered reasonable. The pro-pharma side will likely continue to lob flimsy excuses at the data, but at some point, the truth will be so clear that even the blind will see it. Until that day, continue to inform yourself and share what you find.
Sources and References
- 1, 5 Medscape May 13, 2022
- 2 medRxiv April 29, 2022 DOI: 10.1101/2022.04.25.22274266
- 3, 11, 12, 13, 14 Anchorage Daily News April 29, 2022
- 4 Nature Communications November 20, 2020; 11 Article number 5917
- 6 medRxiv April 29, 2022 DOI: 10.1101/2022.04.25.22274266, See funding statement
- 7 Gates Foundation Grant to McGill University September 2020
- 8 Gates Foundation Grant to McGill University April 2020
- 9 McGill International Funding Sources
- 10 McGill newsroom December 17, 2015
- 15 CDC COVID-19 Vaccine Booster Shots
- 16 The Defender April 7, 2022
- 17 medRxiv April 19, 2022 DOI: 10.1101/2022.04.18.22271936
- 18, 22, 23 The Defender May 4, 2022
- 19 Igor’s Newsletter April 26, 2022
- 20 Bad Cattitude Substack April 27, 2022
- 21 UK Health Security Agency COVID-19 Vaccine Surveillance Report Week 13
- 24 Walgreens COVID-19 Index
- 25 Twitter TexasLindsay April 23, 2022
- 26 Twitter TexasLindsay April 25, 2022
- 27 COVID-19 and All-Cause Mortality Data Analysis by Kathy Dopp and Stephanie Seneff (PDF)
- 28 COVID Vaccination and Age-Stratified All-Cause Mortality Risk (PDF)
- 29 Vaccines 2021; 9(7): 693
- 30 Science, Public Health Policy and the Law August 2021; 3: 81-86, page 82
- 31 Science, Public Health Policy and the Law August 2021; 3: 87-89
- 32 Clinical and Translational Discovery February 25, 2022; 2(1): e35
- 33, 34 Steve Kirsch Substack May 17, 2022
Even if the Government Can ‘Move On’ From Partygate, the Public are Stuck With the Consequences of Lockdown

By Mark Shaw | The Daily Sceptic | May 25, 2022
“Let’s move on please, there are more important things to deal with.” This is what we often hear in relation to ‘partygate’. I don’t think sceptics are in such a hurry. We all want to move on in life but that is not easily achieved when we have been misinformed, taken for a ride and then taken to the cleaners.
The sceptics aren’t just Daily Sceptic readers but a growing number of the public who are seeing that much of the media have not delivered a full, honest account in reporting the last two years of pandemic restrictions and enforced medical interventions. What I find interesting is that, in much of the media’s eagerness to see the downfall of Boris Johnson, everyone is getting to see a little more of the ‘bigger picture’ the media have, up until now, been trying to hide. How could those enforcing all those ridiculous mandates be indulging in so many parties and social mixing if Covid was such a deadly disease? Why were so many coerced into a trial vaccination programme for a disease that evidently poses so little threat to them?
How we have been deceived! Yet much of the media focus on the minor detail of whether a particular event was a party, what certain photos show, whether Boris Johnson actually knew he was attending a party, whether he should have received more fines etc. They want to know if there is enough evidence to show that the PM misled Parliament because convention dictates that, if that were the case, he should resign – the big news story. The news story for me is whether the Government misled the public, not Parliament.
The scandal that lies before us is one demonstrating how those in power, who determined the rules and directed the hardships of the last two years, are more concerned about themselves and whether they have misled their colleagues than us plebs. The deception has severely affected many of us, the younger generation in particular. There are now increased hospital waiting lists, deaths from delayed cancer diagnosis and treatment and rampant economic inflation – true wrongs that deserve more than a token fine. It is this mendacity and betrayal that have consequences and will continue, possibly for decades, to have grave ramifications from which some may never be able to ‘move on’.
Dr. Mark Shaw is a retired dentist.
The Rise of Hepatitis
By Carla Peeters | Brownstone Institute | May 23, 2022
The number of previously healthy children younger than 16 years of age with mysterious hepatitis cases have doubled in two weeks to 450 cases worldwide, including 11 deaths. Most cases have been reported in the UK (160) and the US (currently, 180). In Europe most cases are found in Italy (35) and Spain (22). Over 8-14% of the patients needed liver transplantation. These children will be on lifelong medication. Until now the real cause of a sudden spark in hepatitis is not clear.
Although 50-72% of the cases tested positive with a PCR test for Adenovirus, tissue and liver samples taken in the UK do not show any typical features that might be expected with a liver inflammation due to this virus.
In the UK, 18% of the reported cases tested positive for SARS-CoV-2 virus and three cases had tested positive 8 weeks prior to admission. The most plausible cause of hepatitis traces to a viral origin. Brodin and Aditi hypothesize a SARS-CoV-2 superantigen mediated immune activation in an Adenovirus-sensitized host.
At this point many of the children with hepatitis are too young to be eligible for COVID-19 vaccination. So far, no common environmental exposure has been found.
Jaundice is characteristic for all children with hepatitis, which could have many reasons including toxins and malnutrition. A search into the peer-reviewed scientific literature on the toxicology of nanoparticles, microplastics, disinfectants and hypercapnia/hypoxia, children have been extensively exposed to during the pandemic makes bio corona formation and accumulation of toxic substances a reasonable explanation for disruption of the liver homeostasis.
The capacity for excessive activation of liver inflammatory pathways has been described for these materials prior to the pandemic. Effects of the complex mixture of these materials and associated chemical pollutants presented have not yet been assessed. Understanding how these materials interact with its biological surroundings during long-term and frequent exposure is of utmost importance.
Pandemic Measures and Liver Toxicity
Early in the pandemic several researchers warned of the unsafe use of facemasks, tests, and disinfectants and their weakening effect on the immune system. Many institutions are starting research on harmful chemicals due to air pollution as they pose a known threat to public health and the economy, representing 10% of global GDP in health costs and 3.75 billion lost working days at the global level in 2060.
Unfortunately, almost no funded research has been started in the area of the safe, cost/benefit use of the mandates. Instead, during the pandemic large amounts of money were spent on less urgent research on non-pandemic related issues.
While Covid-19 was originally thought to be a respiratory infection, various research papers have indicated myocardial inflammation, hepatitis, or neurological experiences independent of severity of Covid-19 and sometimes without evidence of a viral infection. Other researchers found that cardiac damage was more related to clotting and microthrombi were frequent. Almost 25% of people hospitalized develop myocardial injury and many develop arrhythmias or thromboembolic disease.
Lockdowns, with many people experiencing an ongoing state of fear and anxiety and frequent exposure to nanoparticles, microplastics, high CO2 exposure and toxic substances impaired the innate immune system even more.
Furthermore, several studies have indicated a remarkable suppression of the innate immune system after injections with PEGylated lipid nanoparticle (LNP) modified mRNA vaccines. In vivo studies for cytotoxicity and genotoxicity of these vaccines, prior to their release under EUA and being mandated for many people and children, have been neglected.
Unfortunately, more than two years into the pandemic an alarming stage of mysterious rises in infectious and noncommunicable diseases and sudden non-Covid deaths have been reported, even neonatal deaths. The Observer reported one in three people in the UK are experiencing long-term illness.
The Liver Is an Immune Surveillance System
The liver is an important organ responsible for the storage, synthesis, metabolism and redistribution of carbohydrates, fats and vitamins and numerous essential proteins. It is the main detoxification center of the body. A most important organ for generating an effective innate immune response and covering a robust and long-lasting immunity, it works to keep virus, bacteria and excessive inflammations in check.
About 30% of the total blood passes through the liver every minute and is scanned by the mononuclear phagocytic system (MPS) in the liver. The microenvironment in the liver shapes and functions the antigen specific CD4+ T cell population with the capacity for longevity/self-renewal for more than a decade.
High amounts of CD8, Natural Killer T cells, dendritic cells and macrophages (Kupfer cells) in the liver play an important role in the protective innate immune system during injury and infection deciding for tolerance or excessive inflammation. Specific liver cells, hepatocytes, produce 80-90% of the circulating innate immunity proteins in the body including acute phase proteins, complement, bactericidal proteins and more.
Neutrophils, the most abundant leukocytes in the blood, present in the liver perform important functions in inflammation and act as a functional bridge between the innate and adaptive immunity (B cells and T cells) activating antigen specific immune responses.
Homeostatic inflammation is a normal part of a healthy liver. In the complex microenvironment of the liver, the hepatic immune system tolerates harmless molecules while at the same time remaining alert to possible infectious agents, malignant cells or tissue damage. Inflammatory processes are required to rid itself of pathogens, cancer cells or toxic products of metabolic activity. The inflammatory processes are intimately linked to mechanisms that resolve inflammation and promote tissue regeneration.
Excessive and dysregulated inflammatory activity are key drivers of liver pathology, associated with systemic inflammation: chronic infection, autoimmunity and cancer. Mechanisms to resolve liver inflammation are essential to maintain local organ and systemic homeostasis. It is the balance between activation and tolerance that characterizes the liver as a frontline immunological organ. Disrupting this precious surveillance system increases the risk for severe disease and death.
Immune-Liver Disruptors
A possible role of the pandemic measures in excessive inflammation in the human body by immune-liver disruptors is realistic. Independently they may each cause problems of the liver. Serious drawbacks of the measures have become most visible in children, the obese and immunocompromised and the poor.
Nanoparticles (i.e. inhaled graphene oxide, titanium dioxide, Ag from facemasks or swabs) present in the body are cleared from the blood and will preferentially accumulate and sequester in the liver, up to 30-99% from those present in the blood and at much higher quantities as compared to other organs.
Studies in recent years have shown that nanomaterials can modulate and activate neutrophils and other immune cells. Nanomaterials may be considered as a particular case of danger signals that are able to trigger sterile inflammatory responses. Rapid accumulation of nanoparticles in the resident liver macrophages can change the expression of anti-inflammatory genes. Changes of genes related to detoxification and cell cycle have been observed.
Systematically administered nanoparticles may directly interact with circulating erythrocytes leading to erythrocyte aggregation and or hemolysis that is accompanied by hemoglobin release. Surface properties of the nanoparticles are known to play a critical role in nanoparticle-erythrocyte interaction. Most nanoparticles have been known to activate complements by either themselves or through serum proteins. Activation of complements and complement activation pathways could further promote tumor growth.
Nanoparticles develop a specific bio-corona comprising complex and dynamic layers of biomolecules that endow nanoparticles with a new immunological identity.
Studies on polystyrene microplastics (which can be present in facemasks and swabs) showed hepatotoxicity and dysregulation of the lipid metabolism, causing oxidative stress and inflammatory responses. This implicated a potential risk for liver steatosis, fibrosis and cancer and macrophage foam cell formation, a characteristic feature observed during atherosclerosis posing a serious threat to human health.
Another study demonstrated that fish exposed to a mixture of polyethylene with chemical pollutants bioaccumulate the chemical pollutants and suffer liver toxicity and pathology. Moreover 0.1 um microplastics could enter hepatocytes from circulation and result in liver damage even at a low concentration.
Microplastic exposure could induce DNA damage in both nucleus and mitochondria indicating a potential risk of hepatotoxicity and fibrosis. Microplastics are found in the human blood of 80 % of the people tested, in deep lung tissues and human feces.
Covid-19 mRNA vaccines use Acuitas’ PEG (Poly Ethylene Glycol) ylated lipid nanoparticles (LNP). The PEGylated lipids support prolonged circulation and shield the highly inflammatory and cytotoxic effects of the cationic lipids used. If insufficiently shielded by PEG they have been shown to mediate aggregation and interact with and damage the membranes of erythrocytes resulting in hemolysis. PEG content, surface density and conformation of the nanoparticle influence the binding of proteins to a bio corona and the uptake by immune cells.
Despite achieving high dense surface coatings of PEG, no NP formulation has been developed that can completely resist interaction with blood components. Of concern is that 22-25% of individuals who were never exposed to PEGylated therapeutics were found to have PEG antibodies, which is more than two decades ago. PEG coating can improve the penetration of biological barriers including reducing interactions with tissue extracellular matrix cellular barriers and biological fluids such as mucus leading to improved delivery.
After injection of Moderna LNP very low levels could be detected in the brain, potentially indicating that the mRNA LNP could cross the blood brain barrier and reach the Central Nervous System (CNS). Unfortunately, the potential inflammatory nature of these LNPs was not assessed.
In preclinical studies a strong induction of adaptive immune responses by CD4+ T-cell activation and protective humoral immune responses was found. The synthetic ionizable lipid is speculated to have approximately 20-30 days of half-life in humans. It has been shown that plasma protein absorption occurs very rapidly and that it affects hemolysis, thrombocyte activation, cellular uptake and endothelial cell death. The bio corona formation of the PEGylated nanoparticle may change over time.
The increasing number of side effects and reported high potency for eliciting antibody response may partially stem from the LNP’s highly inflammatory nature characterized by leukocyte infiltration and activation of different inflammatory cytokines and chemokines. Antigen-presenting cells presenting vaccine derived peptides/protein might cause tissue damage and exacerbate side effects, which have been linked to autoimmune diseases.
More severe and systemic side effects after the booster shot might be related to an amplification effect of the adaptive immune response induced by the vaccine resulting in high antibody responses. Neutrophils were found to preferentially internalize PEGylated particles in the presence of human plasma. Also, further studies of complement activation in relation to PEG nanoparticles merit rigorous evaluation for immune safe materials. Observational studies found a greater risk for complications following a positive SARS-CoV-2 test. A study of the University of Lund has indicated by in vitro studies that the BNT162b2mRNA vaccine has a fast take-up into human liver cells. In 6 hours of exposure the RNA was reverse transcribed into DNA.
Sennef et al. describes the disruption of the innate immune system by the Covid-19 mRNA vaccines caused by an impaired interferon signaling, release of large amounts of exosomes containing Spike protein, potential disturbances in regulatory control of protein synthesis and cancer surveillance of and their potential direct link to liver disease (with over 2,000 reports in VAERS December 2021) and other inflammatory diseases. The presence of Spike protein has been detected in the blood and 60 days after mRNA vaccine injection in the lymph nodes.
A functional reprogramming of the innate immune responses after BNT 162b2 injection was also observed by Fohse et al. with a lower response of innate immune cells, while the fungi-induced cytokine responses were stronger. A study on Biovrix by Nguyen et al. demonstrated an impaired lipid metabolism and increased lipotoxicity by the Spike protein. Jiang et al observed that the Spike protein localizes in the nucleus and inhibits DNA damage repair by impeding key DNA repair protein recruitment to a damaged site. A mechanism by which the spike protein might impede the adaptive immunity explaining the potential side effects. Suraswaki et al. stated that the virus itself may dysregulate the innate cellular defenses using various structural and nonstructural proteins.
Taking Back Control of Our Bodies
The European Commission Statement from May 12, 2022, announces to shorten (from 300 to 100 days) the product to market cycle to develop safe and effective vaccines, therapeutics, and diagnostics following the identification of new threats and work to make them widely available.
As discussed, the Covid-19 pandemic measures have shown to be far from safe. All materials are known to interact and bind proteins forming bio corona’s depleting the body of essentials for processes to function properly.
Subtle changes in materials and biological fluids of persons can significantly change the protein composition of the bio corona and can either lead to an excessive inflammation or resilient homeostasis. Especially in children who need more proteins, vitamins and minerals for mental, physical, and immune system development, the accumulation of toxic substances in the liver and formation of bio corona can be a serious threat to health.
At this stage, it is not known whether the mysterious rises in diseases are caused by a virus or an intoxication and/or depletion of essentials that result in impaired signaling routes. The Covid-19 routine diagnostic tests used for mass testing have major flaws which make it impossible to ensure the presence of an infectious virus as a single cause of symptoms.
An increasing number of doctors and researchers agree: the pandemic is over. All pandemic measures need to be halted immediately. The highest priority is lifting the mandates for children. Healthy children always had a very low risk for severe Covid-19 and are protected by a strong robust and long-lasting natural immunity. There is no added value to vaccinate any person with natural immunity. Moreover, the risk for side effects of the mRNA vaccine for children is high. mRNA Covid vaccine accumulates in the liver 30 minutes after it is injected.
Deep investigations on quality, reproducibility and contaminations of the materials of personal protective equipment, facemasks, tests, disinfectants and vaccines, being used with their effects on the human body and the environmental ecosystem need to be prioritized and funded.
During the past two years, the immune system of many people has been harmed and even broken. We need programs to regenerate the liver and immune system so people can face with trust and confidence any possible wave of virus attacks.
Carla Peeters is founder and managing director of COBALA Good Care Feels Better. She obtained a PhD in Immunology from the Medical Faculty of Utrecht, studied Molecular Sciences at Wageningen University and Research, and followed a four-year course in Higher Nature Scientific Education with a specialization in medical laboratory diagnostics and research. She studied at various business schools including London Business School, INSEAD and Nyenrode Business School.
COVID-19 Pandemic Could Have Emerged Due to US Experiments on Viruses, Prof Says
Samizdat | May 21, 2022
Scientists have not been able to reach an agreement on the origin of the coronavirus pandemic. While it is widely believed that the deadly virus originated from a wet market in Wuhan, others insist that COVID-19 was man-made, and the pandemic was the result of a laboratory leak.
US experiments on viruses that could jump from animals to people might have contributed to the emergence of coronavirus, Professor Jeffrey Sachs wrote in his article for PNAS journal.
He also called for an independent and transparent investigation into the origin of the coronavirus pandemic. According to Sachs, more transparency from the Chinese authorities could have helped a lot during the early stages of the pandemic, but some US research also raises concerns.
“We argue here that there is much important information that can be gleaned from US-based research institutions, information not yet made available for independent, transparent, and scientific scrutiny,” he wrote in a joint statement with Professor Neil Harrison of Columbia University.
Among the US institutes that could use more transparency Sachs lists the EHA, the University of North Carolina (UNC), the University of California at Davis (UCD), the NIH, and USAID.
“A broad spectrum of coronavirus research work was done not only in Wuhan […] but also in the United States. The exact details of the fieldwork and laboratory work of the EHA-WIV-UNC partnership, and the engagement of other institutions in the United States and China, has not been disclosed for independent analysis,” the professors wrote, adding that “the precise nature of the experiments that were conducted, including the full array of viruses collected from the field and the subsequent sequencing and manipulation of those viruses, remains unknown.”
Sachs pointed out that the denials of being involved in COVID-related research alongside US institutions are “only as good as the limited data on which it is based”. According to the article, the US-Chinese collaborative research was connected to “the collection of a large number of so-far undocumented SARS-like viruses and was engaged in their manipulation within biological safety level (BSL)-2 and BSL-3 laboratory facilities.”
Such experiments raise concerns that an airborne virus might have infected a laboratory worker, along with other possible scenarios suggesting that COVID-19 was man-made.
Sachs emphasised the importance of further independent and transparent investigations into the origin of the pandemic, suggesting that one of the ways to investigate could be “a tightly focused science-based bipartisan Congressional inquiry.”
While the scientific opinions on the origins of COVID remain divided, Beijing suggested that the deadly virus could have also emerged from Fort Detrick, a clandestine bioresearch facility based in Maryland. Washington, in turn, accused China of fuelling the pandemic and concealing the data about the virus, with the allegations being particularly vocal during the presidential tenure of Donald Trump.
Why the World should be very concerned about New Zealand under the Jacinda government
By Guy Hatchard | Waikanae Watch | May 19, 2022
The New Zealand government relies upon a science body known as Te Punaha Matatini (Centre for Science in Society) whose work is funded directly by the office of the Prime Minister and cabinet.
Yesterday, Te Punaha Matatini published a 21-page document entitled “The Murmuration of Information Disorders” (see attached release from the Science Media Centre) designating those opposed to the government’s pandemic policies as violent right wing insurrectionists planning the weaponised storming of parliament and the execution of public servants, academics, journalists, politicians, and healthcare workers.
This is an utterly false characterisation worthy of the worst excesses of historical propaganda.
This 21-page document, represented to the public as a scientific paper, contains not a single discussion of the scientific concerns being raised in opposition to government pandemic policy.
It omits for example analyses of the government’s own official figures which show that the vaccinated are more vulnerable to infection, hospitalisation, and death than the unvaccinated, a fact that has been deliberately hidden from the public.
Prime Minister Jacinda Ardern introduced yesterday’s Te Punaha Matatini report with the words:
“One day it will be our job to try and understand how a group of people could succumb to such wild and dangerous mis- and disinformation. And while many of us have seen that disinformation and dismissed it as conspiracy theory, a small portion of our society have not only believed it, they have acted upon it in an extreme and violent way that cannot stand. We have a difficult journey in front of us to address the underlying cause.”
Since when do reasonable scientifically-based questions asked of the government in good faith constitute violent insurrection?
I am tempted to think that Ardern could just as well be talking about her own government. The Prime Minister and the social scientists(?) working at Te Punaha Matatini might do well to read the New York Times, (although they probably don’t do so because the official policy of the New Zealand government is to discourage any information that is not sanctioned and edited by themselves).
A NYT article on 10 May 2022 entitled “Emergent Hid Evidence of Covid Vaccine Problems at Plant” reports that
“Emergent BioSolutions, a longtime government contractor hired to produce hundreds of millions of coronavirus vaccine doses, hid evidence of quality control problems from Food and Drug Administration inspectors in February 2021 — six weeks before it alerted federal officials that 15 million doses had been contaminated.”
A reasonable observer might conclude that early (and later) concerns being voiced about vaccine safety were justified, but the New Zealand government is far from reasonable.
A succession of scientific papers published in reputable journals during recent weeks (which we and many others have reported extensively and communicated directly to the government) have in fact fully justified concerns about safety and efficacy, but unbelievably our government is in denial and still moving ahead with propaganda advertising of their mRNA vaccination agenda for all ages and, as today’s Te Punaha Matatini report shows, labelling any opposition as a conspiracy with violent aims.
How Did the Transformation of the NZ Government Come About?
New Zealand has a small population of 5 million, but it has been used to trial new products in order to gauge what the public reaction and acceptance might be in bigger markets overseas. Never more so than during the pandemic. Take up of the Pfizer mRNA Covid vaccination has reached up to 95% of the eligible population.
This has been achieved through a transformation in the style of government, media control, science funding, intellectual standards, and international relations unprecedented in the western world, along with the coercion of draconian employment mandates and the pursuit of dissenters through compliant courts.
This has been engineered under the leadership of a person with a bachelor’s degree in communication who grew up in a strict rural Mormon household and cut her political teeth under the Blair administration in London. In keeping with her upbringing and education, Ardern is a leader who is sure she is right and is prepared to enforce her orthodoxy against all opposition and reason.
Her international perspective is one of unquestioning acceptance of the authority and right to rule of global institutions. Her top confidant and mentor Helen Clark, former NZ Labour Prime Minister, is closely associated with this outlook. Ardern recounts that she begins her day with a discussion with Clark over breakfast.
Like Ardern, Clark is renowned for her iron fist management style. She ruffled feathers at the United Nations Development Programme, which she led from 2009 to 2017, reportedly undermining human rights and supporting China’s Belt and Road initiative.
On 9 July 2020 the World Health Organization (WHO) appointed Clark as co-chair of a panel reviewing the WHO’s handling of the COVID-19 pandemic and the response of governments to the outbreak. The Independent Panel for Pandemic Preparedness and Response (IPPR) examined how the outbreak occurred and how future pandemics can be prevented.
Nothing says more about the overt global agenda of Ardern and Clark than this 11 May 2022 statement of the New Zealand government:
“The establishment of a pandemic treaty/instrument was a key recommendation of the Independent Panel for Pandemic Preparedness and Response and is one of New Zealand’s foremost global health priorities”
Like China, New Zealand’s fading international reputation for successful management of the pandemic was actually built on a single policy—control the borders, restrict entry, and impose lengthy quarantine.
The Current Situation in New Zealand is Deeply Concerning
Ardern controls the media and the science dialogue through a mixture of government funding and exclusion of dissent. The government has spent big on saturation advertising advising complete safety and efficacy of the Pfizer vaccine, and continues to do so.
It has instituted funding of cultural groups, GPs, and commercial organisations who promote vaccination. The level of funding is so generous that it has distorted prior long standing economic and political relationships.
So far the government has spent on the order of $100 billion on the pandemic in addition to normal expenditure. To put this in stark perspective, that is equal to the total annual government budget prior to the pandemic—more than $20,000 for every man, woman, and child. This is borrowed money which will have to be repaid through increased taxation of an already struggling population.
We Have No Constitution in New Zealand, the Power of the Government Is Absolute.
The control that Ardern’s government exercises over the courts, government agencies, parliament, media, independent regulators, and over the vast majority of the population is staggering and rigidly enforced. Dissenting medical professionals are excluded from practicing and in some cases prosecuted also. They are also mercilessly hounded and vilified by bought mainstream media.
In an atmosphere of strict government control, more worrying aspects of information control have emerged. In some cases noted by my scientific colleagues, policy and pronouncements that they have demonstrated are in conflict with published research have disappeared from the public record.
Even rare court rulings in favour of caution have been rapidly bypassed by simply passing new laws without debate. Court rulings about mandates have also been openly flouted, as happened when the military vaccine mandate was ruled illegal. With the support of the government, the military said the courts had no jurisdiction over its operation and went ahead anyway.
Ardern has introduced her policies in such a dedicated, persuasive, secretive, and complete way that almost the whole population of New Zealand has complied. They have accepted limitations on medical choice, judicial protections, human rights, press freedom, freedom of information, privacy, employment conditions and opportunities, standard of living, and social interaction.
Ardern’s successful efforts to persuade the population that government should be your only source of truth, have all but negated any of the longstanding mechanisms of government accountability. A majority of the population have all but concurred with Ardern that the unvaccinated may be safely blamed for every government failing and omission; and for all Covid case loads, hospitalisations, and deaths contrary to all evidence.
The opposition parties have apparently accepted that they will in future go about their business using the same Ardern doctrines and techniques. Accordingly they have failed to sound the alarm, investigate Covid science publishing deeply, or oppose draconian legislation. They have joined Ardern in labelling peaceful protest as unacceptable and illegal.
Ardern on the Global Stage
Ardern is about to deploy her international political capital to promote the globalisation of her policies and outlook. Her public persona can be deceptively mesmerising. You should be worried.
The world’s economy also has no constitution. So far Ardern appears to be happy to allow it to be controlled by global economic predators. Pfizer has been uncritically promoted by her, and the notion of WHO control over New Zealand’s sovereign rights is being welcomed with open arms. It fits with her strict hierarchical perspective.
Ardern may be viewed by naive foreign governments as a pandemic success story unfairly criticised in her own country. Stop for a moment and consider that she is about to lend her support to the promotion of a new world order on the global stage using her trademark persuasive techniques of propaganda, coercion, and control of information.
Featured Video

Pediatrician shares 30 yrs of insight on vaccinating vs. not vaccinating children
or go to
Aletho News Archives – Video-Images
Book Excerpt
Biden’s Closed Circle on Russia
An excerpt from ‘The Great Betrayal’
By James W. Carden | The Realist Review | June 14, 2026
Joe Biden’s presidency may ultimately come to be seen as a cautionary tale. Here was a president who showed little interest in entertaining arguments that might have contradicted his most deeply held assumptions.[1] And there were precious few within the upper ranks of the administration who might have attempted to do so, after all, only policy hands and political operatives who had come up through the ranks of the Clinton and Obama administrations or had longstanding ties to the citadels of the foreign policy community were invited into the fold. … continue
Blog Roll
 Aletho News
Aletho News- Terms of Iran-US MoU revealed: Bloomberg
- A California Pediatrician Shares 30 Years of Insight on Vaccinating vs. Not Vaccinating Children
- What Is Defensive Medicine?
- CDC Awards Pfizer $1.24 Billion for COVID Vaccines for Kids and Adults
- Historic blow to South Korea’s military intelligence agency
- Russian frigate fires warning shots in English Channel
- Radio Free Europe, the Cold War ‘Weapon’ Congress Still Funds
- UN: Israel continues to violate Lebanon airspace in defiance of Iran-US MoU
- Araghchi: Israeli occupation of Lebanese land a violation of MoU
- Hezbollah fighters confront intruding Israeli forces in southern Lebanon
- If Americans Knew
- Pro-Israel Donors Power Last-Minute Surge of Espaillat Spending
- “They Stole Our Home and Our Life”: Israel Permanently Displaces Syrians in Quneitra
- Massie Recognizes USS Liberty Attack. Here’s Why That Matters
- The blatant racism and cruelty that define Israel’s settler movement
- Israeli army ‘murdered child’ in Gaza and then dumped body on a roadside
- The Forward’s Hit Piece on Thomas Massie and USS Liberty Veterans
- Israel’s former defense minister compares settler ideology to Nazism
- The Pro-Israel Lobby’s Quiet Cash Shuffle
- Trinity Broadcasting Network (TBN) Propagandizes for Israel’s Wars
- A grim milestone: Gaza’s death toll surpasses 73,000 – Daily Update
- No Tricks Zone
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
