CA Bill would punish Doctors over COVID ‘Misinformation,’ as other states move to protect Doctors’ rights
By David Charbonneau, Ph.D. | The Defender | February 23, 2022
Before the U.S. Supreme Court last month blocked the Biden administration’s COVID-19 vaccine mandates for large employers and allowed the mandate for healthcare workers to stand, all eyes were on the feds when it came to COVID-related policies.
But state lawmakers also have been busy drafting bills in an effort to shape COVID policies closer to home.
The California Assembly, for example, introduced over the past six months a flurry of bills designed to strengthen vaccination mandates and regulate treatment options for patients.
For example, Sen. Richard Pan (D-Sacramento) last month introduced legislation proposing COVID vaccine mandates for all K-12 students in California schools.
And this month, Assembly Member Evan Low (D-Campbell) introduced legislation (AB 2098) that, according to the Los Angeles Times, would “make it easier for the Medical Board of California to discipline doctors who promote COVID-19 misinformation by classifying it as unprofessional conduct.”
The bill defines “unprofessional conduct” as any action a physician or surgeon takes “to disseminate or promote misinformation or disinformation related to COVID-19, including false or misleading information regarding the nature and risks of the virus, its prevention and treatment; and the development, safety, and effectiveness of COVID-19 vaccines.”
Under the bill, disciplinary action could be brought against a physician for disseminating information that “resulted in an individual declining opportunities for COVID-19 treatment or prevention that was not justified by the individual’s medical history or condition.”
Additionally, doctors could be disciplined for “misinformation or disinformation” that is contradicted by contemporary scientific consensus to an extent where its dissemination constitutes gross negligence” by the physician.
Commenting on the criteria, Dr. Meryl Nass, an expert in epidemiology and vaccine injury and member of the Children’s Health Defense scientific advisory committee, said:
“I think this is clearly an attempt to legislate that the government of California or the Medical Board of California will define what is truth and what is misinformation, and medical providers will have to follow lockstep with that definition.
“This, of course, is the same thing as the Ministry of Truth in George Orwell’s “1984,” and if the California legislature actually votes for this bill, the intent of the action will be to enforce a one and only truth.
“Nowhere does this legislature define what is misinformation and disinformation. They do talk about contemporary scientific consensus but as we know in the last two years, the so-called scientific consensus — or the public health agency consensus — on masks, on vaccination, on boosters, etc. has flip-flopped all over the place. So we have adequate examples that the concept of “contemporary scientific consensus” is basically meaningless in this context.”
Contrary to typical board practice, under AB 2098, physicians could also be disciplined for public speech, including social media posts, unrelated to the actual treatment of patients.
Supporters of Low’s bill insist the legislation does not impinge on doctors’ freedom of speech.
“This isn’t a call for a policing of free speech,” Nick Sawyer, an emergency room doctor who founded a group called No License for Disinformation, told the LA Times. “This is a call for protecting the public against dangerous misinformation, which patients are parroting back to us in our emergency room departments every day.”
Nass disagreed:
“The result is removing options from doctors and patients. And the longer-term consequence is that doctors will become irrelevant if they are not needed to assess each individual’s personal risks and benefits from each type of medical care.
“The government and its partners in the healthcare industries can simply prescribe one-size-fits-all healthcare for everyone.”
Low’s bill, introduced as part of a larger effort by a group of Democratic state legislators to strengthen vaccination laws, set off a contentious debate over how far the state should go in pursuing COVID mandates.
Other COVID-related bills introduced in California include:
- Assembly Bill 1993, authored by Buffy Wicks (D-Oakland), would require employees and independent contractors to be vaccinated against COVID as a condition of employment unless they have an exemption based on a medical condition, disability or religious beliefs.
- Assembly Bill 1797, introduced by Akilah Weber (D-San Diego), allows California school officials to more easily check student vaccine records by expanding access to a statewide immunization database.
- Senate Bill 866, introduced by Sen. Scott Wiener (D-San Francisco) would let children 12 and older be vaccinated without parental consent.
Other states pursue efforts to support alternative treatments
In contrast to California, several state legislatures are moving to provide legal support for off-label prescriptions and alternative approaches supported by physicians.
In New Hampshire, legislators last month held public hearings on a bill that would allow for over-the-counter dissemination of ivermectin at pharmacies, provided certain treatment plan requirements were met.
New Hampshire HB 1022 would permit pharmacists to dispense the ivermectin by means of a standing order entered into by licensed healthcare professionals.
Sponsors of the bill argued many healthcare workers are unable to prescribe ivermectin, either because of hospital politics or outside professional pressures.
The bill has support from Dr. Paul Marik, who traveled from Virginia to testify at the public hearing.
A former professor of medicine and chief of pulmonary and critical care medicine at Eastern Virginia Medical School, Marik sued the hospital he worked for after it banned physicians from prescribing ivermectin for COVID patients.
Marik resigned late last year in protest of the ban.
During his testimony in New Hampshire, Marik described ivermectin as “cheap, exceedingly safe and exceedingly effective.”
“If ivermectin had been promoted at the beginning of this pandemic, we would not be sitting here today,” Marik said.
Kansas lawmakers last month advanced a bill supporting the prescribing of ivermectin and hydroxychloroquine. The model legislation, also introduced in Tennessee, would require pharmacists to fill prescriptions for the off-label use of ivermectin and hydroxychloroquine.
In direct contrast to the California legislation, the Kansas bill also would mandate that doctors not be subject to disciplinary action for any “recommendation, prescription, use or opinion … related to a treatment for COVID-19, including a treatment that is not recommended or regulated by the licensing board,” Kansas Department of Health and Environment or the U.S. Food and Drug Administration.
“Such actions,” the bill states, “could not be considered unprofessional conduct.”
Kansas lawmaker Sen. Mark Steffen (R-Hutchinson) supports the bill. Steffen, an anesthesiologist, said he’s under investigation by the University of Kansas Health System with which he is affiliated for prescribing ivermectin to COVID patients.
Dr. Festus Krebs III, a physician representing the Catholic Medical Association of Kansas City, also spoke in favor of the bill:
“With ivermectin and hydroxychloroquine, we now have 76 ivermectin COVID-19 controlled studies which show 66 percent overall improvement and 57 percent decreased mortality.”
Meanwhile, in Florida, legislation that would extend protection for hospitals against patient lawsuits over COVID care sits on the desk of Gov. Ron DeSantis, awaiting signature or a veto.
And in New York, the state’s comptroller — citing the investment of the state’s public pension plan in Spotify — sent a letter to the company asking it to increase its screening of “misinformation” on their platform.
© 2022 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Leading law firm issues Facebook letter of complaint over ‘anti-Palestinian bias’
MEMO | February 23, 2022
Leading law firm Bindmans LLP has sent a formal letter of complaint to Facebook over its “anti-Palestinian bias.” Instructed by the International Centre of Justice for Palestinians (ICJP), the London based firm demanded explanation for the “systematic” and “far-reaching” censorship of content and accounts related to Palestine.
The complaint was also sent to the United Nations Special Rapporteur on the promotion and protection of freedom of opinion and expression. It requests an urgent review of, and explanation for, the decisions made by Facebook, which was rebranded last October as Meta Inc, to suspend accounts and posts which are affiliated to Palestinian news agencies, commentators and journalists.
Monday’s letter of complaint to Facebook is the second in nine months sent by Bindmans LLP to the social media giant. A previous communication submitted in May 2021 was made on behalf of five journalists and news agencies in Palestine. Facebook is said to have interfered with their accounts and/or posts and was accused of breaching their fundamental right to freedom of expression as well as its own Corporate Human Rights Policy.
In the May 2021 complaint, the main questions posed by Bindmans LLP included whether the censorship decisions were carried out by an algorithm or by a person exercising their discretion, and details regarding Facebook’s policy in justifying their censorship decisions, in addition to steps taken by the company to resolve unfair censorship.
In its response to the letter, a month later, Facebook said that it had investigated the accounts referenced in the letter and, after further review, has restored content and/or accounts where applicable. Notably, no substantial answers were provided to any of the main questions cited in the original communication.
Despite the commitments made by Facebook in their letter sent in June 2021, the censorship remained, said ICJP in its press release detailing the content of the complaint. The centre is an independent organisation of lawyers, academics and politicians that work to promote and support Palestinian rights.
Monitoring group, Sada Social, which has been documenting the suspension of Palestinian content and accounts on Facebook, recorded in 2021 alone, hundreds of instances of inappropriate censorship of social media content in support of the rights of Palestinians. This censorship was exacerbated significantly during the last Israeli offensive on Gaza in May 2021.
The complaint reinstates the request that Meta/Facebook discloses and reviews its decision-making process, and explains why the accounts were closed, suspended or posts taken down, and whether in doing so an algorithm or human discretion was used.
World Economic Forum pushes digital ID system that will determine access to services
By Tom Parker | Reclaim The Net | February 22, 2022
The World Economic Forum (WEF), an international organization that works to “shape global, regional and industry agendas,” recently published its latest dystopian proposal – a far-reaching digital ID system that will collect as much data as possible on individuals and then use this data to determine their level of access to various services.
This digital ID proposal is outlined in a report titled “Advancing Digital Agency: The Power of Data Intermediaries” and builds upon a digital ID framework that the WEF has published previously.
Under this framework, the WEF proposes collecting data from many aspects of people’s “everyday lives” through their devices, telecommunications networks, and third-party service providers.
The WEF suggests that this data collection dragnet would allow a digital ID to scoop up data on people’s online behavior, purchase history, network usage, credit history, biometrics, names, national identity numbers, medical history, travel history, social accounts, e-government accounts, bank accounts, energy usage, health stats, education, and more.
Once the digital ID has access to this huge, highly personal data set, the WEF proposes using it to decide whether users are allowed to “own and use devices,” “open bank accounts,” “carry out online financial transactions,” “conduct business transactions,” “access insurance, treatment,” “book trips,” “go through border control between countries or regions,” “access third-party services that rely on social media logins,” “file taxes, vote, collect benefits,” and more.

In this Advancing Digital Agency: The Power of Data Intermediaries report, the WEF positions this digital ID framework as the part of the solution to a “trust gap in data sharing” and notes that vaccine passports, which were mandated across the world during the COVID-19 pandemic, do “by nature serve as a form of digital identity.”
The WEF also praises the way vaccine passports have allowed governments to harvest data from their populations without “notice and consent”:
“At a collective level, vaccine data is an incredible public health asset. The United Kingdom Government in particular has acknowledged this and has suggested that anonymization, pseudonymization and data shielding techniques could be harnessed in a controlled environment to allow for the reuse of that highly sensitive data. In such cases, notice and consent is not required per se for the reuse of the data but the intermediary processes the data undergoes must be done in a controlled environment so that the findings of the data set are made available rather than the data itself.”
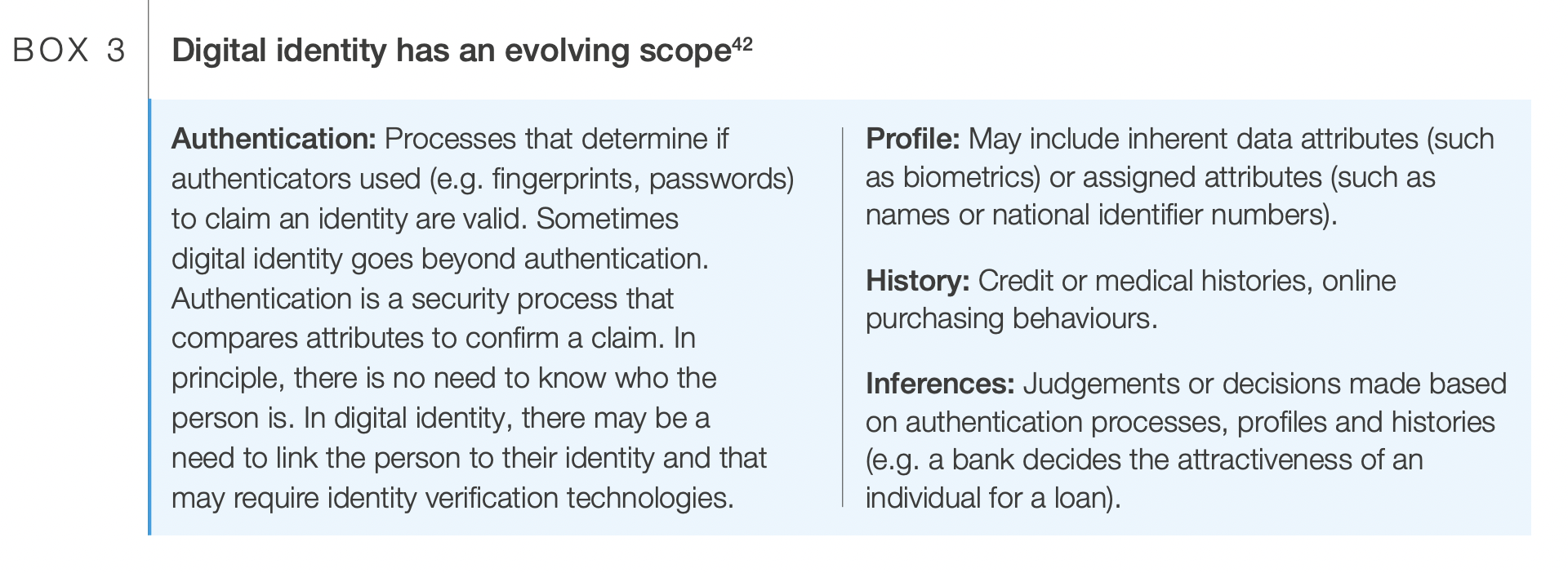
Additionally, the WEF provides a specific example of how digital IDs could be used to authenticate a user (by using fingerprints, a password, or identity verification technology) and decide whether they should be granted access to a bank loan by judging their profile (which may include their biometrics, name, and national identity number) and history (which may include their credit, medical, and online purchasing history).
The WEF goes on to suggest that digital IDs will “allow for the selection of preferences and the making of certain choices in advance” and ultimately pave the way for “automated decision-making” where a “trusted digital assistant” “automates permissions for people and effectively manages their data across different services” to “overcome the limitations of notice and consent.”
This push for an invasive digital ID system from the WEF follows it proposing other similar surveillance systems such as turning your heartbeat into a digital ID. Throughout the pandemic, the WEF has consistently advocated for vaccine passports and digital ID.
Beyond these specific proposals, the WEF is infamous for its globalist and transhumanist agendas such as the “Great Reset” (which proposes that people will “own nothing” and “be happy”) and the “Fourth Industrial Revolution” (which, according to WEF founder and chairman Klaus Schwab, will lead to “a fusion of our physical, our digital, and our biological identities”).
Governments and private corporations are increasingly embracing digital IDs. Some governments are also pushing a similar notion – social credit-style apps that monitor citizens’ behavior and reward them for engaging in state-approved actions.
Details of Russia-Donbass cooperation treaty emerge
RT | February 21, 2022
While the treaties of friendship and cooperation between Russia and the newly recognized republics of Donetsk and Lugansk are still in the draft stage, the Russian State Duma has released the proposed documents on Monday, showing that they will include common defense against external aggression and the right to use each other’s military infrastructure, among other things.
Russian President Vladimir Putin has recognized the people’s republics of Donetsk and Lugansk – two breakaway regions in eastern Ukraine – as independent states on Monday.
The State Duma overwhelmingly voted in favor of recognizing the rebel regions last week. The draft treaties of friendship and mutual assistance with both newly recognized states – due to last at least 10 years – have now been published on the legislature’s website.
Of particular interest is Article 5, which gives both contracting parties the right to “build, use and improve military infrastructure, bases and other objects on their territory.” The Kremlin has already ordered Russian troops to deploy into the two areas as peacekeepers, pending a formal treaty on military cooperation.
Article 6 bars both parties from “entering any blocs or alliances directed against either of them” and will not allow their territory to be used for launching attacks against one another.
Article 11 envisions free movement of citizens between the contracting parties, and obligates both Russia and the republics to “develop and implement an agreed set of measures to regulate the regime of entry into and exit from their territory of citizens of third countries.”
Article 13 also obligates the contracting parties to protect the “ethnic, linguistic, cultural and religious identity of national minorities in their territories and create conditions to preserve and develop” these identities while guaranteeing individual and collective minority rights “without being subjected to any attempts of assimilation against their will.”
Donetsk and Lugansk declared independence from Ukraine in 2014, after US-backed nationalists overthrew the democratically elected government in Kiev. They sought recognition from Russia at the time, but Moscow declined, insisting their conflict was an internal Ukrainian matter.
Russia had joined France and Germany in the so-called Normandy Format to mediate an armistice between Kiev and the rebels in Minsk in 2014-2015. The process envisioned Ukraine giving the two regions broad autonomy, but Kiev repeatedly declined to live up to its obligations – instead changing Ukraine’s constitution to make that impossible.
Putin cited this development and accused Ukraine of wanting to conquer the two regions by force, in his speech on Monday announcing the recognition of the Donbass republics as a move “long overdue.”
The Ugly Face of Trudeau Regime Tyranny in Canada’s Capital
By Stephen Lendman | February 21, 2022
According to local media reports, Trudeau regime storm troopers arrested 191 nonviolent freedom-fighting truckers and supporters through Sunday.
Towing removed 57 vehicles.
The Ottawa police tweeted that operations continue “to remove all vehicles parked” near parliament Hill.
According to interim police chief Steve Bell:
“We will continue to work through the night, through the coming day and/or days until” streets are cleared.
As of Sunday, 103 peaceful protesters, threatening no one, face phony charges, including mischief and obstructing police.
According to Ottawa mayor Jim Watson, (illegally) seized vehicles may be sold instead of returning them to their rightful owners.
Defying the rule of law, Watson falsely claimed the right to “confiscate…vehicles and sell them (sic),” adding:
“I want to see them sold. I don’t want (them) return(ed).”
So-called investigations of police state violence against peaceful protesters assure coverup and denial whitewashing ahead.
Bell signaled what’s coming by claiming that police on horseback didn’t trample anyone.
Two protesters “collided” with horses, he said, falsely blaming the injured for police state violence.
Saying “no one (was) seriously injured (by) police actions. Safety is our priority” ignored trampling, beating, pepper-spraying and other violence against peaceful protesters by Trudeau regime goon squads.
Draconian actions flagrantly breached Canada’s Charter of Rights and Freedom.
Trudeau regime tyranny abolished it.
The Ottawa Police Service (OPS) also tweeted:
“If you are involved in this protest, we will actively look to identify you and follow up with financial sanctions and criminal charges.”
A Freedom Convoy 2022 statement said:
“The use of more force will only be used to punish people, and not preserve or establish order.”
Commenting on Trudeau regime police state tactics, GOP Senator Rand Paul said the following:
“The Emergency edict that Trudeau has done in Canada allows him to do some horrendous things.”
“It allows him to stop travel, allows him to detain people without trial.”
Separately, Paul tweeted:
“Canada became Egypt…ruled by emergency edict that allows prohibition of public assembly, travel, and the commandeering of private companies without your day in court.”
Last week, Canadian Law Professor Ryan Alford condemned Trudeau’s “power grab.”
At a time when no national emergency exists, an invented one alone, Alford stressed that “not a single violent incident” justified Trudeau’s abuse of power.
He “failed to meet the requirements for invoking the Emergencies Act.”
“His doing so is clearly unconstitutional.”
Over the weekend, US Rep. Yvette Herrell said she’ll “introduc(e) legislation (to) temporarily grant asylum to innocent Canadian protesters who are being persecuted by their own government.”
“We cannot be silent as our neighbors to the north are treated so badly.”
At this time, constitutional law in Canada is null and void.
Trudeau regime tyranny replaced it.
A Final Comment
On February 23, US truckers comprising the People’s Convoy will depart from Adelanto Stadium in southern California for Washington, DC.
They’ll be joined by “frontline doctors, lawyers, first-responders, former military servicemen and women, students, retirees, mothers, fathers and children – on this peaceful and law-abiding transcontinental journey toward the east coast.”
Their mission is all about “freedom and unity…restor(ing) accountability…lifting (draconian) mandates and ending a state of emergency when none exists.
Organizations involved in the freedom-fighting mission include:
The Unity Project
The America Project
Advocates for Citizens’ Rights
US Freedom Flyers
The American Foundation for Civil Liberties & Freedom
Faith groups from every spectrum
Independent journalists are accompanying the truckers to report accurately on their peaceful, law-abiding mission.
It’s being assisted by retired military personnel and security experts.
At this time, arrival in Washington is expected on March 5.
ThePeople’sConvoy.org is the official website of the mission for accurate information.
The Truckers’ Declaration states the following:
“We the People of the United States, in Order to restore our once perfect Union, re-establish Justice, insure domestic Tranquility, provide for the common defense of all, promote the general Welfare, and secure the Blessings of Liberty, do ordain and establish the restoration movement of The People’s Convoy for the United States of America.”
“WE DEMAND THE DECLARATION OF NATIONAL EMERGENCY CONCERNING THE COVID-19 PANDEMIC BE LIFTED IMMEDIATELY AND OUR CHERISHED CONSTITUTION REIGN SUPREME.”
“WE ARE THE PEOPLE OF THE UNITED STATES OF AMERICA AND WE STAND TOGETHER UNDER THE BANNER OF FREEDOM – FREEDOM IS THE ONE THING THAT UNITES US ALL.”
“LIBERTY FLOWS THROUGH ALL OF OUR VEINS.”
Trudeau regime tyranny suggests what likely awaits the People’s Convoy in Washington on arrival or in the days that follow.
The choice of freedom-loving people everywhere is unambiguous.
Eliminate draconian health and freedom-destroying mandates or they’ll eliminate us.
American Truckers are launching The People’s Convoy, a peaceful and unified transcontinental movement

FOR IMMEDIATE RELEASE
For media inquiries contact:
Email: thepeoplesconvoy@protonmail.com
American Truckers are launching The People’s Convoy, a peaceful and unified transcontinental movement, on February 23 from Adelanto Stadium in Southern California
ADELANTO, Calif., (Feb. 20, 2022) American truckers are launching The People’s Convoy, a peaceful and unified transcontinental movement, on Wednesday, February 23, 2022, from the Adelanto Stadium in Southern California. Starting at 10:00 a.m., hundreds of truckers will hear words of encouragement and blessings from a group of speakers including FLCCC President Dr. Pierre Kory and Godspeak Church Pastor Rob McCoy. The truckers and blue-collar workers of the United States will be joined by freedom-loving supporters from all walks of life – frontline doctors, lawyers, first- responders, former military servicemen and women, students, retirees, mothers, fathers and children – on this peaceful and law-abiding transcontinental journey toward the east coast. The truckers encourage one and all to come out to the stadium in the heart of Adelanto, California to wish them well, see them off and join in the journey.
This convoy is about freedom and unity: the truckers are riding unified across party and state lines and with people of all colors and creeds – Christians, Muslims, Sikhs, Mormons, Agnostics, Blacks, Hispanics, Asians, Native Americans, Republican, Democrats. All individuals are welcome to participate by either attending the launch gathering – at 10:00 a.m. on Wednesday February 23, at Adelanto Stadium – or by getting in their own vehicles and following the big rigs from Adelanto toward the east coast!
The message of The People’s Convoy is simple. The last 23 months of the COVID-19 pandemic have been a rough road for all Americans to travel: spiritually, emotionally, physically, and – not least – financially. With the advent of the vaccine and workable therapeutic agents, along with the hard work of so many sectors that contributed to declining COVID-19 cases and severity of illness, it is now time to re-open the country. The average American worker needs to be able to end-run the economic hardships of the last two years, and get back to the business of making bread – so they can pay their rents and mortgages and help jumpstart this economy. To that end, it’s time for elected officials to work with the blue collar and white-collar workers of America and restore accountability and liberty – by lifting all mandates and ending the state of emergency – as COVID is well-in-hand now, and Americans need to get back to work in a free and unrestricted manner.
The People’s Convoy is a non-partisan, trucker-led effort supported by a cross-cultural and multi-faith contingent of supporters including
- Dr. Pierre Kory and the doctors of the Frontline Covid-19 Critical Care Alliance (FLCCC)
- Liberty-minded lawyers such as Tom Renz and Joey Gilbert (Gubernatorial candidate – Nevada)
- Pastors like Rob McCoy and Rick Brown of Godspeak Church
- Transportation workers including rail workers and pilotsA broad consortium of organizations including
- The Unity Project
- The America Project
- Advocates for Citizens’ Rights
- U.S. Freedom Flyers
- The American Foundation for Civil Liberties & Freedom
- Faith groups from every spectrum
Newsmax and Eric Bolling have indicated they will do a ride along and live daily updates from the convoy with Maureen Steele. The Epoch Times and a variety of other journalists, media outlets and podcasters will also be embedding. Children’s Health Defense’s CHD.TV will be covering the convoy – and the activists on the ground and across the country – with live updates every day at 10 am EST at https://live.childrenshealthdefense.org/.
The convoy is being assisted by retired military personnel and security experts, who are spearheading logistics in order to ensure a 100% safe, lawful, and peaceful journey.
The People’s Convoy Route*
*Route subject to change
Day 1: Wednesday, February 23
Morning – Depart Adelanto Stadium, CA
Evening – Arrive in Kingman, AZ for overnight stay
Day 2: Thursday, February 24
Morning – Depart Kingman, AZ head east on I-40, toward Lupton, AZ Evening – Arrive in Lupton, AZ for overnight stay
Day 3: Friday, February 25
Morning – Depart Lupton, AZ on I-40 eastbound thru New Mexico Evening – Arrive in Glenrio, TX for overnight stay
Day 4: Saturday, February 26
Morning – Depart Glenrio, TX
Evening – Arrive in Elk City, OK area for overnight stay
Day 5: Sunday, February 27
Morning – Depart Elk City, OK area
Evening – Arrive in Vinita, OK area for overnight stay
Day 6: Monday, February 28
Morning – Depart Vinita, OK area
Evening – Arrive in Sullivan, MO area for overnight stay
Day 7: Tuesday, March 1
Morning – Depart Sullivan, MO area
Evening – Arrive in Indianapolis, IN area for overnight stay
Day 8: Wednesday, March 2
Morning – Depart Indianapolis, IN area
Evening – Pause for rest in Indianapolis, IN area for overnight stay
Day 9: Thursday, March 3
Morning – Depart Indianapolis, IN area
Evening – Arrive in Cambridge, OH area for overnight stay
Day 10: Friday, March 4
Morning – Depart Cambridge, OH area
Evening – Arrive in Hagerstown, MD area for overnight stay
Day 11: Saturday, March 5
Morning – Depart Hagerstown, MD area Evening – Arrive in the DC Beltway area
The People’s Convoy will abide by agreements with local authorities, and terminate in the vicinity of the DC area, but will NOT be going into DC proper.
Stay tuned for opportunities for elected officials and regular folks to go “Ridin’ Shotgun” with an actual trucker for a day – as well as an opportunity to bid on one seat that will be sold on our Operations Vehicle – for a similar ride-along opportunity. Details will be posted to the website soon.
To support the truckers, see the routes, or find out more, please visit: http://www.ThePeoplesConvoy.org This website and the official social media handles are the ONLY source of accurate data about this
peaceful, law-abiding convoy – we hope to see America there!
Instagram: https://www.instagram.com/thepeoplesconvoyusa/ Twitter: https://twitter.com/peoplesconvoyus
An Open Letter to the Professional Bodies of Counsellors and Psychological Therapists in the UK
Therapists for Medical Freedom | February 17, 2022
We write as a group of registered counsellors, psychotherapists and psychologists in clinical practice in the United Kingdom.
We are contacting you to express our grave concerns around Vaccines as a Condition of Deployment (VCOD) mandates for health and social care professionals, and the implications that these could have for our profession.
Whilst we welcome the recent suspension of the NHS vaccine mandate [1] to allow space for further public consultation, we are also aware that Sajid Javid, the Secretary of State for Health and Social Care, has made it clear that the debate on mandatory vaccination is far from over. He was quoted in The Times on 7th February as demanding that medical regulators send the “clear message” that healthcare workers must be vaccinated against coronavirus. [2]
The implication here is that the onus of enforcing and policing the vaccination status of healthcare workers could be shifted from employers to professional/regulatory bodies. We are concerned about the silence of our professional bodies on this matter and now seek urgent clarification on their positions.
We call upon our professional bodies to publicly reject any policy of mandating COVID-19 vaccines as a condition of registration and/or deployment amongst their membership – either now or at a future point. Furthermore, we urge them to commit to protecting the right to informed consent and bodily autonomy, both for their professional membership and the clients we serve.
In particular, we would like the professional bodies to consider and respond to our professional concerns on the following points:
1. Mandatory vaccination policies conflict with our professional ethics as counsellors and psychological therapists.
One of the core principles common to the Ethical Frameworks of all our professional bodies is that of upholding client autonomy and their right to informed consent to treatment.
As health practitioners, we rightly understand that no medical or clinical intervention can be considered universally safe. We know from our own practice that even authorised, regulated and ethically sound medical treatments can still pose significant risks and have the potential to cause harm at an individual level.
As such, suitability for any medical treatment needs to be assessed on a case-by-case basis and can only be authorised with informed consent from the client (so long as they have the capacity to do so), after they have been given full and accurate information around any potential risks.
This principle of informed consent is not only vital to our ethical practice, it is upheld as a central principle within wider medical ethics and international human rights law. For example, in the UK all medical interventions in the NHS must be fully voluntary and in line with this principle of informed consent:
The decision to either consent or not to consent to treatment must be made by the person, and must not be influenced by pressure from medical staff, friends or family… If an adult has the capacity to make a voluntary and informed decision to consent to or refuse a particular treatment, their decision must be respected. [3]
In March 2015, a significant judgement about the nature of informed medical consent was made in the UK Supreme Court. [4] The court clarified that doctors must: “take reasonable care to ensure that the patient is aware of any material risks involved in any treatment,” in which, “a reasonable person in the patient’s position would be likely to attach significance to the risk, or the doctor is aware that the particular patient would be likely to attach significance to it”.
The court ruled that UK doctors can no longer rely on simply sharing the consensus of a body of medical opinion (‘the Bolam test’) as a basis for a patient’s informed consent, but a personalised risk assessment must be given. In the case of COVID-19 mandates, this means that generic claims that ‘the science is settled’ or ‘vaccines are safe and effective’ – cannot be used to justify their safety for an individual. [5]
The public and professional discourse on COVID-19 vaccination mandates are an example of how social pressure can be exerted on individuals to have a particular health intervention, even without a full individual risk assessment or any long-term safety data. As such, mandates can be considered medically coercive and in direct violation of the legal principle of informed consent.
We call on our professional bodies to recognise that coercion does not equal informed consent.
2. COVID-19 vaccines are far from universally ‘safe and effective’.
COVID-19 vaccinations use novel technologies which have been in widespread use for little more than a year, are still in clinical trials and for which by definition no long-term safety data is available.
Since the start of the vaccine rollout, we have already seen a significant shift from the COVID-19 jabs being promoted as being ‘safe and 100% effective’ [6][7][8][9] – to a recognition that there can be serious, even fatal side effects for a small minority of people. Their overall efficacy, especially in reducing transmission and preventing the spread of Coronavirus, is also far from what was originally hoped for.
Furthermore, since their general release, some COVID-19 injections have now been discontinued for use within certain demographics due to safety concerns. For example, the AZ and Moderna vaccines have been discontinued for young people in several countries after safety concerns arose around the risks of blood clots, following several high-profile deaths. In more recent months there have been emerging scientific studies showing the risks, particularly to younger males, of serious side effects such as myocarditis and pericarditis following vaccination, as well as ongoing concerns about the impact of vaccines on the female menstrual cycle. Both concerns have led to the commissioning of major safety investigations through additional clinical trials.
Whatever the outcome of these investigations, the fact remains that our understanding of these novel COVID-19 vaccines and the risks they pose to human health is far from comprehensive or complete.
Whenever there is risk of significant harm from a medical intervention, especially when the treatment is newly developed and those harms could be life-threatening, it is imperative that there is free choice for the individual to refuse that treatment without fear of negative consequences.
For professional bodies to require mandatory vaccination as a condition of professional registration, for acceptance on professional training courses, or as a condition of employment, would amount to unethical coercion of its professional members. To do so would place the professional bodies in direct violation of the principle of informed consent.
We ask that the professional bodies join us in speaking out against the unethical nature of mandatory vaccination policies, and publicly affirm their commitment to the ethical principle of informed medical consent.
3. Informed consent goes beyond issues of safety and risk.
As counsellors and therapists, we recognise that assessing the safety profile of a specific intervention is only one aspect of the complex decision-making process that informs our consent to medical treatment.
An individual’s moral, spiritual and political beliefs, as well as their cultural practices, life experiences and approach to managing their health, will also have an impact on their willingness to give, or withhold, informed medical consent.
Many of us take a holistic, person-centred approach to working with our clients. As such, we believe in the validity, authority and importance of these broader factors that can be drawn upon to inform medical consent. We see these wider factors as valuable, essential and equal; individuals have a right to refuse a medical treatment on wider grounds than its official safety profile or potential side effects. We are particularly concerned about the impact of mandates on those who have complex health conditions, those who have prior experiences of being harmed by medical treatments, those who favour their natural immunity, and those with religious or ethical concerns about the development process of the vaccines.
Current government guidelines for vaccine mandates only grant ‘medical exemption’ to staff with a tiny number of officially permitted medical conditions [10], with no allowance for many broader concerns that could be central to someone deciding not to consent to a COVID-19 injection. We believe that the government has no lawful right or moral authority to draw up a set of very limited medical criteria and then insist that these are the only permitted circumstances in which someone can be officially ‘exempted’ from vaccine mandates without facing redeployment or job loss.
As counsellors and psychological therapists, we uphold the right of every individual to make an informed choice about whether to take a COVID-19 vaccination, or indeed any other medical intervention, based on their own personal circumstances and medical history. We call on our professional bodies to uphold that right for practitioners and the clients we serve.
4. Professional bodies are failing in their duty of care to members who are affected by NHS vaccination mandates.
It would be incongruent for professional bodies to enshrine the principle of informed consent within their ethical codes of conduct for working with clients, whilst their professional members are not permitted to make autonomous decisions about their own medical treatment.
Mandatory vaccination policies, and the loss of the right to informed medical consent, is causing significant psychological distress to many UK counsellors and therapists, especially those working in the NHS. Many of these affected practitioners have been loyal, paying members of their respective professional bodies for decades. The silence and seeming lack of engagement from our professional bodies around this issue is both disturbing and disappointing given how severe the consequences are for members who face job loss.
The exact number of counsellors and psychological therapists who stand to be affected by NHS vaccine mandates is uncertain, as to our knowledge, there has been no formal consultation process around this issue by any of the professional bodies.
However, Therapists for Medical Freedom have now facilitated numerous free, volunteer-run support workshops for affected therapists, which have often been full to capacity. We have also had hundreds of communications from distressed members who are under significant stress from the vaccine mandate process. Many have complained to us about experiencing an utter lack of clarity, guidance or support from their professional body.
Professional bodies have a duty to represent the interests of their paying members, especially at times where their human and employment rights are under threat in a professional context.
Therapists affected by vaccine mandates deserve better treatment and representation than they are currently getting from professional bodies. This situation must change, and we appeal to professional bodies to address this with the utmost urgency.
5. Vaccine mandates will have negative consequences for clients accessing therapeutic services.
NHS England estimated that had the vaccine mandate policy been implemented in April as planned, this would have left the NHS down by at least 80,000 staff, as many planned to leave the profession rather than comply with the policy. [11]. This number would increase exponentially if vaccines were mandated as part of the professional registration process, thereby affecting health professionals working outside of NHS services, which applies to most therapists and counsellors in the UK.
To lose a significant number of counsellors and therapists at a time of national crisis could pose significant harm to clients. COVID-19 and the wide-ranging impact of restrictions on the population has left a legacy of new and worsening existing mental health problems. The Centre for Mental Health estimates that 8 million adults and 1.5 million children will need mental health support in the years following the pandemic. [12]
Those of us who have worked to provide psychological therapies throughout this challenging time are now seeing an unprecedented rise in demand for NHS and voluntary sector counselling and therapy services, to the point where people in need now face dangerously long waiting times. [13] Across the UK, even private therapy services and individual practitioners are in short supply, with many having to make difficult decisions to turn away people in need because they simply do not have the resources to treat them. At a time of increased mental health need, vaccine mandates would therefore be detrimental for current and future clients.
We call upon the professional bodies to provide reassurance that clients’ access to therapeutic support will not be restricted based on vaccination status, either now or in the future. We also call on them to reject policies that will risk the loss of experienced practitioners, put further strain on existing services and staff, and potentially dissuade others from training to enter the field.
6. It is essential to consider the wider context to mandatory vaccination policies and to remember the lessons of history.
As counsellors and psychological therapists, when faced with an ethical dilemma, we are encouraged to look beyond the issue itself and consider the wider field and context – including any relevant historical, sociological and political factors. Therefore, when considering the ethics of vaccine mandates, we must consider more than just the risk posed by COVID-19 vs the benefits and risks of vaccination.
When we step back and consider the wider socio-political context, we can clearly see that:
- Governments do not always act in the best interests of the public they are appointed to serve, whatever their political rhetoric might be. We are seeing numerous examples of this emerging now, for example the conflicts of interests in the awarding of PPE contracts and the flouting of COVID-19 rules by senior government figures. [14]
- There have been numerous instances in human history, especially at times of ‘national emergency’, where government bodies have actively lied to the population, exploited the situation to further their own aims, or have sought to conceal important information, especially when it could harm their wider political agenda. [15][16][17]
- The health care system has a long history of being vulnerable to exploitation by political lobbyists, corporate donors or becoming compromised by internal pressures from within government or from regulatory bodies. Consider examples from our recent history – public health advice given to reassure the public of the safety of tobacco, pesticides, GMOs – which have later been proven to be manifestly unsafe, despite the proclamations of the government-sanctioned public health experts of the time. [18][19][20]
- Many authorised medical treatments have later been discovered to be causing significant harm to human health and have been withdrawn from public use, despite having passed required safety checks and being widely embraced by the medical orthodoxy of the time. [21][22][23]
- We are being exhorted to “trust the science” when there is no such thing as ‘the’ science. Rather, science has always comprised a breadth of opinions, conclusions, methods and ethical standpoints. History has shown us that public trust has not always been as safe as we would hope for in the hands of scientists and medical professionals, especially when there are financial interests at stake. [24][25]
- Politicians, pharmaceutical companies, peer-reviewed medical research, clinical trials, regulatory bodies and individual expert opinion – all of these are vulnerable to human error, corruption and conflicts of interest which are not always declared or formalised. [26][27][28]
In the context of our collective history, as ethical health practitioners, we have a responsibility to ask difficult questions if we see draconian policies such as vaccination mandates being introduced in our society. We must continue to think critically about who would profit and benefit most from such policies. Might there also be vested interests, whether in government, science and medicine or the pharmaceutical industry, that could stand in the way of open and transparent discussion? [29][30]
It is not the terrain of ‘conspiracy theory’ for therapists and other health professionals to demand that government and medical experts are scrutinised and held to account for the policies they impose upon the public. As a profession, we must make room for alternative perspectives and difficult questions without these legitimate concerns being dismissed or slandered as ‘anti vax’, ‘dangerous disinformation’ or even more alarmingly, as ‘far-right extremism’.
It is not acceptable for our Professional Bodies to simply dismiss or silence any dissenting voices within their membership, or to ignore these difficult questions. Nor is it acceptable for heavy-handed policies such as COVID-19 vaccine mandates to be supported and justified by our professional bodies on the sole basis that they are acting in line with ‘official legislation or government guidance’ without any independent analysis of the actual effectiveness, ethics, or impact of the guidelines – or any acknowledgement that governments do not always act solely in the public interest.
Our professional bodies have a duty to carefully scrutinise any mandated public health measures that compromise our medical autonomy. They must not be accepted on face value as being in the public interest simply based on the assurances of government and its approved health advisors, or pharmaceutical companies with vested interests.
Recommended Actions:
It is time for the professional bodies who represent counsellors and psychological therapists in the UK to show courage and break their collective silence on the issue of mandatory vaccination in our profession.
In light of all the above, we call on our professional bodies to:
- Uphold the values that are written and protected within their own ethical codes by publicly affirming their commitment to protecting the right of therapists and clients to freely give or withhold their consent to medical treatment without fear of coercion or punishment.
- Affirm that their commitment to upholding the right to informed consent will stand regardless of the emergence of new future variants, waves of disease or novel medical treatments.
- Engage with Therapists for Medical Freedom and other groups of concerned professionals in a process of dialogue around the ethics and legality of vaccine mandates in our profession.
- Pledge to protect the rights of therapists and clients who have exercised their lawful right to informed consent to refuse COVID-19 vaccinations.
- Use their authority as professional membership bodies to prohibit the implementation of discriminatory policies around COVID-19 vaccinations within their organisational membership and associated training institutes – and to publicly speak out against such discriminatory practices in the wider field.
- Remind their members that we each have an ethical responsibility to think critically for ourselves when assessing any government health advice, especially when it is mandated. Professional bodies should help facilitate this broader risk assessment process within their membership, especially the potentially negative impact that any existing or future public health advice might have on practitioners and clients.
- Take into account the broader historical, social and political context when assessing the ethics of mandatory health interventions. We cannot forget the harm that has been caused to human health and civil liberties when the right to refuse medical treatment has been denied to populations at other times in history.
We await to hear your considered responses on these important matters of professional ethics, legislation and human rights, and look forward to beginning a process of dialogue with you.
Yours sincerely,
Therapists for Medical Freedom
Principal Signatories:
Jennifer Ayling, Psychotherapeutic Counsellor, UKCP
Clare Beatson, Counsellor, BACP
Elizabeth Bentley, Psychotherapist, BACP
Johann Burton, Counsellor, NCS
Paula Charnley, Counsellor, BACP
Ben Harris, Psychotherapist, MBACP
Julie Horsley, Counsellor, NCS
Frances Kandler-Singer, Psychotherapist, BACP
Naintara Land, Psychotherapist, UKCP
Rachel Maisey, Counsellor, BACP
Kate Morrissey, Psychotherapist, BACP
Melanie Pickles, Counsellor, BACP
Dr. Bruce Scott, Psychoanalyst, UKCP & CP-UK
Dr. Gary Sidley, Clinical Psychologist (Retired)
Deborah Short, Psychotherapist, UKCP
Elizabeth Smith, Psychotherapist, Pre-Accred
Leanne Ward, Clinical Psychologist, HCPC
Sarah Waters, Psychotherapist, MBACP
Supporting Signatories:
Marc Allen, Trainee Therapist, Pre-Accred
John Bates, Psychotherapist, UKCP
Antoine Bowes, Counsellor, BACP
Dr. Faye Bellanca, Clinical Psychologist, HCPC
Caroline Brett, Psychotherapist, BACP
Jacqueline O’Brien, Psychotherapist, (retired)
Sheila Burchell, Clinical Psychologist, HCPC
Dr. Erika Filova, Clinical Psychologist, HCPC
Dr. June Golding, Psychotherapist, UKCP
Andrew Harry, Counsellor, UKPTA
Susan Hayes, Psychotherapist
Jessica Horton, Counsellor, BACP & BPS
Isla Hunter, Psychotherapist, BABCP
Gabrielle Lake Mitchell, Trainee Therapist, BACP
Maggie Leathley, Psychotherapist, BACP
Jane Margerison, Psychotherapist, BACP
Jonathan Martin, Psychotherapist, UKCP
Gary McKeever, Counsellor, BACP
Caroline Montanaro, Psychotherapist, UKCP
Dr. Naomi Murphy, Clinical Psychologist, HCPC & A-CP
Dr. Rachel Newton, Clinical Psychologist, HCPC & BPS
Sue Parker Hall, Psychotherapist, UKCP
Kay Parkinson, Psychotherapist, UKCP
Dr. Helen Payne, Psychotherapist, UKCP & ADMP UK
Carolyn Polunin, Psychotherapist, UKCP
Dr. Kate Porter, Clinical Psychologist, HCPC
Tracy Rees, Trainee Therapist, Pre-Accred
Dr. Helen Ross, Clinical Psychologist, HCPC
David Scott, Clinical Psychologist, HCPC
Patricia Taddei, Psychotherapist, UKCP
Dr. Lucie Turner, Clinical Psychologist, HCPC
Dr. Alice Welham, Clinical Psychologist, HCPC
Tracy Williams, Counsellor, BACP
Dominique Wynn, Psychotherapist, (Retired)
Sign the Open Letter
Are you a Counsellor, Psychotherapist or Clinical Psychologist based in the UK who is concerned about the impact of vaccine mandates on the profession? (whether you are personally vaccinated or not).
If so, please sign the letter.
Featured Video

Seyed M. Marandi: Iran Rejects U.S. Deal – War Is Likely Imminent
or go to
Aletho News Archives – Video-Images
From the Archives
World War II Didn’t End The Great Depression
Stark Realities with Brian McGlinchey | April 4, 2024
A principal goal of Stark Realities is to “expose fundamental myths across the political spectrum” — and few myths are as universally embraced as the notion that US participation in World War II (1941-1945) lifted the American economy out of the Great Depression.
This myth is dangerous not only because it leads citizens and politicians to see a bright side of war that doesn’t really exist, but also because it helps foster a belief that government spending is essential to countering economic downturns. That belief, in turn, has helped propel us to a point where the national debt now exceeds $34.6 trillion, with interest payments alone on pace to reach $1 trillion a year in 2026, inviting financial catastrophe. … continue
Blog Roll
 Aletho News
Aletho News- Seyed M. Marandi: Iran Rejects U.S. Deal – War Is Likely Imminent
- 46 IPCC Scientists Break Rank, Publicly Challenge Long-Standing Dogmatic Climate Claims
- Coming Off Seroquel Alone
- Iran’s ‘threat’ to Western hegemony is not nuclear weapons
- Iran warns UAE, Bahrain over alignment with US, Israeli interests
- ‘Little Sparta’: Why The UAE Attacked Iran for Israel’s Sake
- Iran Blames European Tanker for Oil Slick Near Kharg
- Hamas leaders say targeting families will fail to extract concessions
- Harrowing testimonies expose Israeli torture of Gaza hospital director
- UAE provides $100m for US-backed Gaza police force vetted by Shin Bet
- If Americans Knew
- Group indicted for insider trading allegedly used ‘going to Israel’ as code for illegal sales
- Israel is enabling a possible plague in Gaza – Daily Update
- A Conservative’s View: Trump’s War on Iran Is Destroying America
- Israel’s war on the West Bank comes for Palestinian greenhouses
- New $270 million Israeli-only roads project in the West Bank is Netanyahu’s latest bid to impose de facto annexation
- Gaza investigation: A family’s fight to find their missing relatives
- MSF: Israel’s deliberate restriction of food and aid led to alarming malnutrition levels in Gaza
- Israel earmarks $270M for Israeli-only roads (that’s apartheid) – Daily Update
- Two Supreme Court Justices were secret agents who helped Israel cover up its attack on the USS Liberty
- Bari Weiss ‘Meddles’ With ‘CBS Sunday Morning’ Story on Palestine
- No Tricks Zone
- New Study: Declining Trends In 1980-2023 Tropical Cyclone Frequency, Accumulated Energy
- 46 IPCC Scientists Break Rank, Publicly Challenge Long-Standing Dogmatic Climate Claims
- Another Study Links Warming To Cloud Forcing, Shortwave Radiation, Natural Atmospheric Circulation
- Wind Energy Is Toxic, Hazardous To Human Health, Scientific Review Shows
- Oversupply Of Volatile Solar Energy Leads To Record NEGATIVE Prices!
- New Study: Extreme Heat Records, Heatwaves, Extreme Cold Records Declining Across US Since 1899
- It’s The Cold, Stupid! Cold 20 Times More Lethal Than Heat, Multiple Studies Show
- European Institute For Climate And Energy: “Climate Debate is Seldom About Science”
- New Study: The Climate May Be 5 Times More Sensitive To Solar Forcing Than Commonly Assumed
- EV Industry Reached $70 Billion In Losses In 2024 Due To Delusional Green Ideologies
