New law allows for warrantless spying on Australians – where next?
By Kit Klarenberg | RT | November 30, 2021
The Australian Signals Directorate, Canberra’s equivalent of Britain’s GCHQ or the US National Security Agency, will be granted sweeping new powers to spy on Australians for the first time since its November 1947 founding.
The move allows the agency to collect signals intelligence on individuals within the country without a warrant, although allegedly only in situations where there is an “imminent risk to life.” Domestic terror suspects are cited as a key target in the Directorate’s crosshairs, and it will also collect intelligence in conjunction with the Australian Defence Force for military operations, with ministerial authorization.
Rules governing the reform and protecting citizens’ privacy will be published on the agency’s website, and subject to review and scrutiny by the Australian parliament’s security and intelligence committee. While framed as sincerely concerned with keeping Australians safe, experts have expressed grave reservations about the development. Among them is John Blaxland, Professor of International Security and Intelligence Studies at the Australian National University, himself a military intelligence veteran, who warned the powers were ripe for abuse.
“I’m a former insider… I have a much greater appreciation of the need for checks and balances, because power tends to corrupt,” he cautioned. “My concern is the legislation we put forward is being drafted by insiders, it’s drafted with their own concerns in mind.”
Drafted by insiders, the legislation certainly was – it’s inspired by the findings of an extensive review by Dennis Richardson, former chief of Australian Security Intelligence Organisation, the country’s FBI, conducted in close consultation with Australia’s assorted intelligence services, in a manner akin to foxes being quizzed on how best to guard a henhouse.
Published in December 2020, his appraisal’s discussion of “authorisations” noted that these agencies can already conduct warrantless intelligence-gathering if they believe it to be “necessary, proportionate, reasonable and justified” in certain circumstances, and “would like the ability” to not only use various investigative techniques without official permission, but also with “protection from criminal liability” when doing so.
Leaked documents exposed by journalist Annika Smethurst in April 2018 showed that high-level plans for untrammeled domestic spying by the Australian Signals Directorate date back even further. They revealed how the respective heads of Australia’s Defence and Home Affairs ministries had discussed allowing the agency to access citizens’ emails, bank records and text messages without approval, or trace. A government source told Smethurst they were “horrified” by the proposals, given “there is no actual national security gap this is aiming to fill.”
Australian Federal Police raided both the alleged leaker of the files and Smethurst the next year. In a perverse irony, the charges against her were dropped in May 2020, as Australian High Court judges unanimously ruled that the warrant secured from a magistrate in relation to the raid was invalid, because it not only “misstated the terms of the offence” but was also ambiguous if not outright absurd.
“[The warrant] lacked the clarity required to fulfil its basic purposes of adequately informing Smethurst why the search was being conducted and providing the executing officer and those assisting in the execution of the warrant with reasonable guidance to decide which things came within the scope of the warrant,” the High Court damningly concluded.
In other words, it was impossible to know from the warrant’s wording what the investigation actually concerned, what evidence or information was sought, and what, if any, crime she may or may not have committed. That this baseless and broad investigative authorization was formally granted at all renders the Directorate’s newfound power to conduct warrantless surveillance all the more disquieting. If such procedural perversion can occur even with putative oversight, what abuses will be engaged-in without any meaningful supervision?
Misuse of these capabilities is almost inevitable. In 1973, the US Supreme Court ruled warrants were mandatory for domestic intelligence gathering. Two years later, a Senate investigation found that the NSA and other US intelligence agencies had nonetheless been engaged in unauthorized spying on American citizens, including anti-war protesters, civil rights activists, and political dissidents, monitoring all their private communications from telephone conversations to telegrams. This led to the 1978 Foreign Intelligence Surveillance Act, which made it a dedicated criminal offense to eavesdrop on American citizens without judicial oversight.
Yet,it was revealed in late 2005 that the NSA had all along continued illegally intercepting the phone calls and digital communications of US citizens, with the witting help of major telecoms giants, which passed copies of all emails, web browsing and other internet traffic to and from its customers at home and abroad to the agency, and its British counterpart GCHQ. Files disclosed in 2013 by whistleblower Edward Snowden confirmed this criminal dragnet was truly global in scale, and very much ongoing.
Key components of this international spying network, known as ‘Five Eyes,’ are situated in Australia, at the Pine Gap and Kojarena satellite surveillance bases. According to investigative legend Duncan Campbell, around 80% of the messages intercepted by the latter – which employs US and British staff in key posts – are sent automatically to GCHQ and the NSA. While every Five Eyes member can theoretically veto requests for such material, “when you’re a junior ally” like Canberra, “you never refuse,” Campbell records.
One can’t help but wonder if the Directorate’s new domestic purview is an experiment, gauging levels of backlash and controversy among the Australian public, before similar measures – provably or potentially already in operation – are openly codified across all Five Eyes member states. Ongoing legal battles against mass data collection in various jurisdictions clearly necessitate the practice being legalized and legitimized. If Canberra’s American and/or British friends politely requested they run such a pilot scheme, would or even could they decline?
Reinforcing this interpretation, mere days after the Directorate’s remit was expanded, the Australian government pledged to introduce new laws forcing social media giants to “unmask” anonymous users who post offensive comments, with hefty fines doled out to those companies which are unwilling or unable to do so. The reasons for Canberra’s haste are unclear, although it’s surely no coincidence that London and Washington have battled for many years to end online anonymity for good – it’s only due to intense domestic opposition that these efforts have so far failed.
Kit Klarenberg is an investigative journalist exploring the role of intelligence services in shaping politics and perceptions.
The English data on vaccines and mortality, revisited
By Alex Berenson | November 28, 2021
Last Saturday morning I posted a short post with a very simple chart – two lines in all.
One line tracked the number of weekly deaths per 100,000 vaccinated people aged 10-59 in England. The other tracked the number of deaths per 100,000 unvaccinated people in England. The chart showed that vaccinated people in this age group were dying overall at a higher rate than unvaccinated people.
I’m never exactly sure which posts will “land” – gain traction and go viral. This chart landed. Hard. Someone wrote me that it broke the Internet. It didn’t break the Internet, only Kim Kardashian’s ass can break the Internet, but it has rocketed around ever since. It has been seen over 800,000 times on this page alone and many millions more in screenshots and Twitter posts elsewhere.
Clearly, the reason the chart has gained so much attention is that it quickly and simply provides a way for people who are concerned about the vaccines to provide apparent visual proof that they are increasing all-cause mortality – overall death rates.
The chart has also engendered a fierce backlash from the usual fact-checkers and vaccine fanatics who say it is – wait for it – “misinformation.” (To be clear, I didn’t actually create the chart, but I checked the underlying British government report to make sure it accurately represents the report’s figures. It does, as everyone agrees.)
The “fact-checkers” have two primary complaints about the chart.
The first is that the vaccinated and unvaccinated groups are not exactly the same. A smaller percentage of teenagers than fifty-somethings are vaccinated, so the unvaccinated group overall skews somewhat younger than the older group. Since death rates rise with age, that difference may be enough to explain the gap between the two groups.
The second is that overall death rates in people over 60 (who are not covered in the chart) are much higher than those in the 10-59 range and appear to be lower in the vaccinated over the unvaccinated.
Another way to look at the objections: the first is that the chart doesn’t say what it seems to say, because of a hidden flaw in the data. The second is that it would be basically meaningless even if it did, because other more robust datasets contradict it.
—
Part of being on Team Reality is acknowledging reality, and acknowledging when your critics have a factually correct objection. So I want to acknowledge that, like the chart itself, these objections BOTH are valid and factually accurate, viewed individually.
What the fact-checkers and vaccine fanatics appear incapable of understanding is that the two objections effectively cancel each other out – and do nothing to address concerns over the long-term failure of Covid vaccines or their impact on all-cause mortality.
These folks think they are sophisticated thinkers who have blown up apparent evidence that the vaccines are dangerous. In fact, just as they have for the last several months, they are telling themselves what they want to hear instead of listening to what the data are saying – and, increasingly, shouting.
—
They have identified and latched on to ONE complication of using population-level data to judge vaccine effectiveness – the fact that differing rates of uptake by age may make the Covid vaccines seem less effective than they are.
But they – deliberately or out of ignorance – are ignoring another one, one that makes the vaccines seem MORE effective than they are.
The second problem is not a secret to epidemiologists.
It has been quietly discussed for flu vaccines for more than a decade, and I have written about it repeatedly in the last year. The problem is this: the popular belief that sick people are more likely to be vaccinated than healthy people is entirely wrong.
People who receive vaccines are healthier overall than those who do not. They care more about avoiding sickness, and they have the time and energy and money to find their way to a vaccination site. They are not healthier because they get vaccines; they get vaccines because they are healthier.
Older people who receive flu vaccines die – of both the flu and all causes – at much lower rates than unvaccinated people after they receive flu shots. But they also die at much lower rates BEFORE they receive the vaccines. The seminal study demonstrating this relationship is now more than 15 years old; it was published in the International Journal of Epidemiology in April 2006.
“The reductions in risk before influenza season indicate preferential receipt of vaccine by relatively healthy seniors,” the authors wrote.
This paradox helps explain why a huge study of flu vaccines in the United Kingdom showed that increasing vaccination levels in older people did not reduce the number of hospitalizations or deaths from the flu.
The researchers took advantage of the fact that Britain prioritizes people 65 and older for vaccinations and that people are much more likely to get a shot when they are 65 or 66 than 64 or 63. Vaccination levels rose sharply as people turned 65, but the health of the people who received the shots did not improve.

(SOURCE: https://www.acpjournals.org/doi/10.7326/M19-3075?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed)
The same pattern is visible in the United States, where a massive increase in the number of flu vaccines in the last generation has made no apparent difference in the number of flu deaths. In fact, in 2005, researchers noted that although vaccinations had risen from 20 percent of elderly people in 1980 to 65 percent in 2001, “unexpectedly, estimates of influenza-related mortality in this age group also increased [emphasis added] during this period.”
In other words, influenza vaccines only seem to work. Any observational estimate that compares death rates in people who have gotten shots to those who have not will be inherently untrustworthy, no matter how hard researchers try to correct for the healthy recipient bias.
—
What is true for flu vaccines appears to be even more true for Covid vaccines.
The relentless vaccination push means that in many countries, more than 90 percent of elderly people are vaccinated. The split is even more stark in countries like England, where 2.44 million people 80 and over have been fully vaccinated, compared to 69,000 who are unvaccinated (and 24,000 who have received the first dose but not the second).
Look at those numbers again.
2,440,000 people in England 80 and over vaccinated. Almost 97 percent of the total number of elderly people.
69,000 80 and over unvaccinated. Less than 3 percent.
These two groups cannot remotely be compared.
How do they differ? I can’t find any hard data, but we know that at least a fraction of the elderly unvaccinated are too ill to be vaccinated. Some are in hospice care. Norway recommended against giving people in hospice the Covid vaccine in January following deaths in terminally ill patients.

A paper published online in March in the Journal of Pain and Symptom Management noted that “communication from hospice organizations has primarily emphasized the vaccination of hospice staff without the same priority mention for patients” and called for hospices to do more to offer vaccines to patients.
The paper’s title was even starker:
A Shot at Inclusion: Reconsidering Categorical Exclusion of Hospice Patients from COVID Vaccine Allocation.
How many Covid deaths in unvaccinated elderly people are actually “with Covid” deaths in people dying in hospice? Again, we don’t know. But what we know is that even a small number of those deaths will hopelessly bias the relative risk ratio for unvaccinated to vaccinated Covid deaths, because the overall number of unvaccinated people is so small.
As of September, about 30 to 35 unvaccinated English people 80 and over died of or with Covid each week, compared to about 250 fully vaccinated people a week.
So trying to measure vaccine effectiveness by looking at the relative risks of the vaccinated and unvaccinated elderly is impossible. But that is exactly what the health authorities and their servants in the media do when they put out figures that seem to show the risk of death from Covid is much lower in elderly people who have been vaccinated.
They are lying with truthful data, and they (some of them, anyway, though probably not the reporters who are writing the stories) are smart enough to know exactly what they’re doing.
—
Meanwhile, they are ignoring a much more important indicator – trends in both Covid and all-cause mortality are very much going the wrong way in the vaccinated elderly population.
In the last four weeks for which British data are available, roughly coinciding with September, about 1,000 vaccinated English people 80 and over died from Covid and 16,000 from all causes.
Compare those numbers to four weeks in May, when fewer than 70 vaccinated English people 80 and over died from Covid and 13,000 from all causes.
Put another way, overall deaths rose more than 20 percent in the vaccinated elderly from May to September, and Covid deaths 15-fold. And this was not because many more people were vaccinated. The number of vaccinated elderly people rose only about 4 percent from May to September.
Compare that to the mortality trends in unvaccinated English people 80 and over.
About 800 died of all causes in four weeks in May (at the time, there were about 77,000 unvaccinated elderly people, compared to 69,000 in September). Fewer than 20 of those died of Covid.
In September, about 140 unvaccinated elderly people died of Covid – a eight-fold increase compared to the 15-fold increase in the vaccinated.
(All data from the British government:
See tables 3 and 4 in downloaded file.)
But that difference isn’t the striking part.
The striking part is that only 700 unvaccinated elderly English people died OF ALL CAUSES in those four weeks in September – FEWER than back in May. (The trend roughly tracked the overall drop in the elderly unvaccinated population. It appears that about 1 percent of those folks die a month, at least in warmer months.)
This trend is stunning for two reasons.
First, the fact that 100 more unvaccinated elderly people (supposedly) died of Covid in September yet 100 fewer of them died overall strongly suggests that many of those reported deaths are actually with and not from Covid.
Second, per capita all-cause mortality – not just Covid mortality, all-cause mortality – rose close to 20 percent in the very large group of the vaccinated elderly. Some of those extra deaths came from Covid. But most did not.
And though death rates are still somewhat higher in the unvaccinated – as they should be, given the fact that vaccine recipients are healthier – but that fact is far less relevant than the notable rise in the vaccinated.
What’s behind the rise in those deaths in the vaccinated elderly? We don’t know. But we’d better find out. Especially since we are now stuffing boosters into their arms.
—
All of this is somewhat complicated, I’ll admit. The data has lots of confounders and continues to evolve. And trying to explain relative changes in all-cause mortality in the context of healthy vaccine recipient bias using papers about flu vaccine – well, it’s not a soundbite.
Which comes back to the chart from last week.
The chart IS a soundbite.
It is a simple and factually accurate way to say:
Something is wrong. The promises that the health authorities have made over the last 12 months about the vaccines are not coming true. Despite near-complete levels of adult vaccination in Europe, many countries are seeing skyrocketing Covid cases and deaths. And worst of all, all-cause non-Covid mortality is running well above normal in country after country.
Not everyone is going to wade through this article. But everyone can read that chart from last week. It’s not perfect, but it uses real data to raise a crucial issue.
That’s why it landed. And that’s why the vaccine fanatics hate it so much.
Whatever You Do, Don’t Think of the Children

By Toby Young • The Daily Sceptic • November 29, 2021
Like most parents across the land, I received a letter from the local council’s Director of Public Health this morning (forwarded by the school in an email) explaining that they have “advised [sic] schools that parents/carers/other visitors are not invited” to nativity plays this year. Not the end of the world in the grand scheme of things, of course – just another depressing example in the long litany of examples of children’s priorities being cast under a bus due to adult panic during the course of this pandemic.
Much more concerning, because of what it said about the mindset of the Director of Public Health in question, was this alarmingly blithe justification for continued restrictions in schools, buried in the body of the letter:
Much as we would all like it to be, the pandemic is not over. Whilst it is clear that the vaccination programme is effective in preventing serious disease and deaths, the vaccine is never going to stop all transmission, and resultant harm, on its own. [Emphasis added]
You couldn’t get a starker admission than this that we long ago moved beyond “flattening the curve” or staving off a dire public health emergency in a once-in-a-lifetime, never-to- be-repeated year. No: we are now in a different place altogether – one in which we must stop transmission “and resultant harm” for its own sake, forever. For how else are we supposed to interpret this statement? On what grounds will parents ever be allowed back into schools to watch nativity plays (or even properly meet their children’s teachers), if the requirement is for “all transmission and resultant harm” to end? We will never be in that position. So in what circumstance does the Director of Public Health envisage there ever will be a return to normal schooling? Ought this not to be made clear to local parents?
More broadly, this incident raises the question of how it is that something so fundamental – children’s schooling – has ended up beholden to the whim of unelected, largely unaccountable, public officials such as this. The local Director of Public Health in any given local authority cannot be voted out. They are not challenged by probing interviews in prominent media outlets. The means by which they are appointed is entirely opaque. And their policy positions, political backgrounds, and motivations are subject to essentially no public scrutiny. Yet they possess the power, at the sweep of a pen, to disrupt the lives of literally tens of thousands of people within their bailiwicks, with the only possible avenue of challenge being a prohibitively expensive and time-consuming claim for judicial review. This ought to be intolerable in a free society. Yet it is the position in which we find ourselves.
Once again, the Covid pandemic and its response have shone a harsh light on British democracy, and revealed it to be in a dilapidated state indeed.
Higher Infection Rates in Vaccinated Not an Artefact of Wrong Population Data, New Analysis Shows
By Will Jones • The Daily Sceptic • November 26, 2021
Back in October, when the critics rounded on the UKHSA for publishing vaccine data that didn’t fit the narrative, front and centre of their complaints was the claim that they were using poor estimates of the size of the unvaccinated population, and thus underestimating the infection rate in the unvaccinated. Cambridge’s Professor David Speigelhalter didn’t hold back, writing on Twitter that it was “completely unacceptable” for the agency to “put out absurd statistics showing case-rates higher in vaxxed than non-vaxxed” when it is “just an artefact of using hopelessly biased NIMS population estimates”.
To the UKHSA’s credit, while it conceded other points, it never gave in on this one, sticking to its view that the National Immunisation Management System (NIMS) was the “gold standard” for these estimates. It pointed out that ONS population estimates have problems of their own, not least that for some age groups the ONS supposes there to be fewer people in the population than the Government counts as being vaccinated.
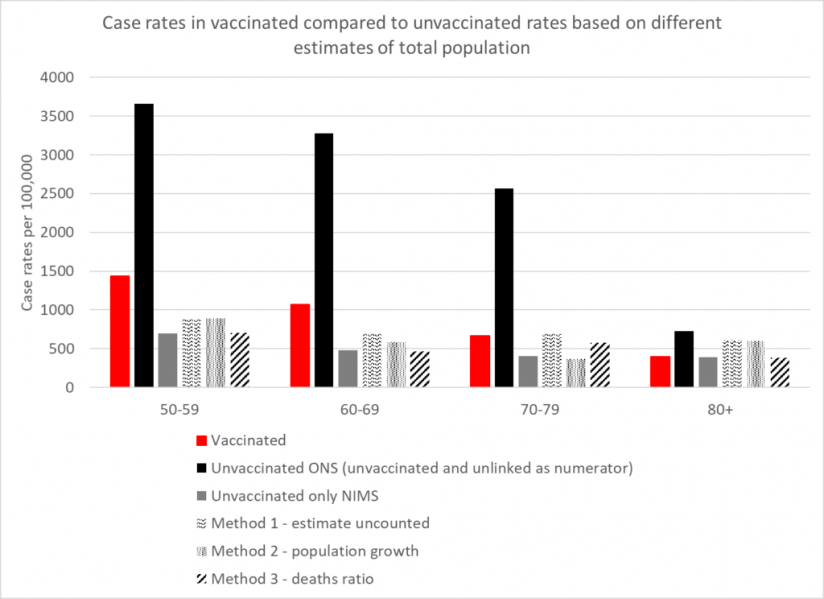
How can we know which estimates are more accurate? A group of experts has applied analytical techniques in order to estimate the size of the unvaccinated population independently of ONS and NIMS figures. Using three different methods, experts from HART found that estimates from all three methods were in broad agreement with the NIMS estimates, whereas the ONS estimate was a much lower outlier.
The first method involves recognising that people not within the NHS database system still catch Covid and still get tested. Assuming these people have the same infection rates per 100,000 people as the unvaccinated, you can calculate how many people there are outside of the database system and add these to the NIMS totals.
The second method involves looking at the rate of growth of people with an NHS number, which has been remarkably steady at around 2.9% per year. If you assume that people who are not yet registered in the NHS will sometimes become sick enough to seek healthcare, and thus a record will be created for them, applying this growth rate to the 2011 ONS population estimates give another figure for the total population.
The third method involves assuming that, in low-Covid weeks, deaths within an age bracket should occur at a similar rate in vaccinated and unvaccinated, allowing the size of the total population to be inferred from the percentage of deaths in the unvaccinated.
The results in terms of reported infection rates according to the five different estimates are depicted in the chart above. They show that the ONS is a clear outlier, its estimates sitting far too low, and NIMS is likely to be much more accurate. The ONS puts the unvaccinated population at around 4.59 million whereas NIMS puts it at 9.92 million, a difference of 5.33 million. That’s a lot of people not to be included in estimates, and suggests, among other things, that the ONS has not adequately estimated the magnitude of illegal immigration into the country.
As well as vindicating the UKHSA in its decision to stick with NIMS over ONS, HART’s analysis also indicates that, contrary to the assertions of Prof Spiegelhalter, the UKHSA data showing infection rates higher in the vaccinated compared to the unvaccinated is not a mere artefact of using the wrong population estimates. There may be other biases in it, but this is not one of them.
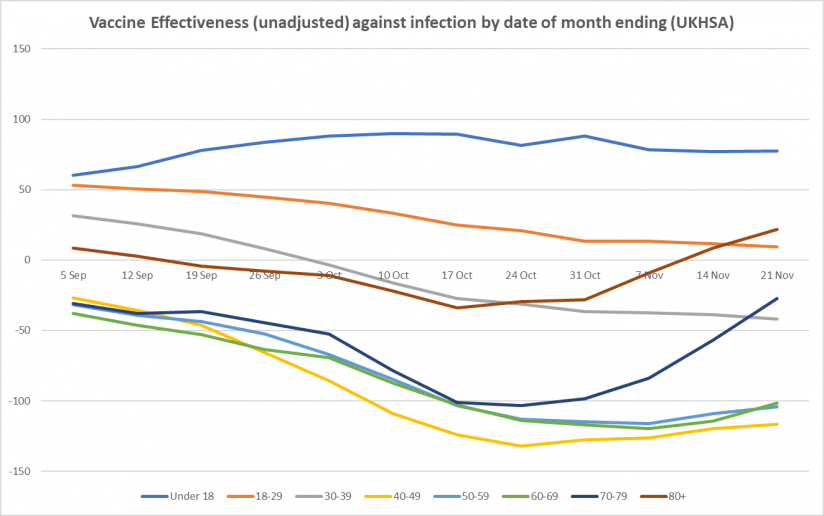
Here is the weekly update on unadjusted vaccine effectiveness based on the raw data in the UKHSA Vaccine Surveillance report. The unadjusted vaccine effectiveness estimates against infection have remained low in all adult age brackets this week, particularly in those aged 40-70, though there is little sign of further decline; in the older age groups (over 40), the recent vaccine effectiveness revival continues, possibly as a result of the third doses. There is also a sign of a rise in vaccine effectiveness against hospitalisation in the over-70s.



Vaccinated “No Less Infectious” Than Unvaccinated, CDC Study Finds
By Will Jones • The Daily Sceptic • November 24, 2021
A pre-print study out this week from the U.S. Government’s Covid Response Team at the Centers for Disease Control and Prevention (CDC) has found vaccinated people to be “no less infectious” than unvaccinated people.
The study tested inmates in a federal prison with high vaccination rates daily during a SARS-CoV-2 Delta variant outbreak.
The study was very thorough. Inmates who tested positive for SARS-CoV-2 were, where willing, PCR-tested for 10 consecutive days and reported symptoms via a questionnaire. The researchers performed whole genome sequencing and viral culture analysis on a high proportion of the 978 specimens collected, allowing them to assess the duration of PCR positivity and viral culture positivity.
There were 95 participants in total, of whom 78 (82%) were double vaccinated and 17 (18%) were not double vaccinated (two having received one dose and 15 having received none). No significant differences were found between double vaccinated and not double vaccinated either in duration of PCR positivity (13 days each) or in duration of culture positivity (five days each).
The authors conclude that “clinicians and public health practitioners should consider vaccinated persons who become infected with SARS-CoV-2 to be no less infectious than unvaccinated persons”.
This is in line with the findings of Public Health England and others.
While this sounds like more good news for countering vaccine passports, vaccine mandates and all other vaccine-based coercion and discrimination, it may be less good news for ending general restrictions and interventions. The authors state: “These findings are critically important, especially in congregate settings where viral transmission can lead to large outbreaks.” Which suggests they think the lack of efficacy against transmission is a reason to intervene more generally to prevent “large outbreaks” in “congregate settings”. It could be a long winter.
Why another lockdown would be met with mass non-compliance
By Andrew Devine | TCW Defending Freedom | November 25, 2021
LIKE many people, I went along with the first lockdown. I wasn’t very keen, and I was somewhat critical of it, but I believed the lie that it would be a temporary one-off measure. From the time of the second lockdown, I have been vehemently opposed to the policy. While I have never denied that Covid can be a nasty life-threatening illness for some people, I am critical of the way that governments have manipulated data to exaggerate the extent of the threat.
When Covid 19 vaccines were first rolled out in the UK and around the world in late 2020, we were promised by Western governments and their teams of scientific ‘experts’ who wield enormous, unaccountable power, the media and Big Pharma that the vaccines were a game-changer and that mass vaccination would lead us back to some kind of normality. I was initially very resistant to take the vaccine because it is a new drug with no long-term data regarding side effects and risks. I also have two autoimmune conditions, and while they are easily treated, I am genetically predisposed to a third one that can be quite serious.
However, in the end, and with much hesitation due to the already known side effects and autoimmune risks, I took the Pfizer vaccine. I did so for several reasons. Firstly, I am around my elderly parents a lot, and I thought I would be protecting them as I believed the ‘experts’ that the vaccines would significantly reduce transmission.
This has turned out to be false.
Secondly, I was convinced by the data that seems to show that getting vaccinated almost entirely eradicates the chances of someone my age ending up in hospital with a severe case of Covid. Due to fitness and age, my risk of serious illness was already low, but as a neurotic who is sometimes prone to viewing the glass half empty, I admit to having moments when I worried that I might be one of those outliers for my age group cut down prematurely by Covid and so this was an added factor, but not the main one, in my capitulation. The final reason was because I currently reside in the Republic of Ireland where the government have been very keen to enforce some of the harshest lockdowns globally with draconian rules on both inward and outward travel as well as compulsory vaccine certificates for access to various sectors. Therefore, one of my main reasons for getting jabbed, while I still defended vehemently the rights of others not to do so, was that I thought I would be doing my bit to put an end to these hideous lockdowns and other excessive restrictions once and for all. Looking at what has happened in Austria and Holland and the refusal of both the UK and Irish governments to rule out more lockdowns, it is now clear how very wrong I was. Another way of putting it is that I’ve realised how easily I have been duped.
In recent weeks, I have become even more sceptical of everything that the UK and Irish governments and their appointed health experts tell me with regard to Covid-19. For a start, if they were wrong about the effectiveness of the vaccines with regards to transmission, why would I trust them with regards to how rarely serious side effects occur? There would be far more political and career capital at stake to motivate suppression of this data. I’m not accusing governments, scientific ‘experts’ or Big Pharma of doing so, merely noting that there is a much bigger price for them to pay if they didn’t.
With regards to coercive measures and the removal of rights from the unvaccinated, governments don’t even have recourse to the dubious argument that it’s for the greater good as we now know that the vaccinated can also transmit the virus. I keep making the argument to vaccine zealots that people can exercise their right to abstain from taking any medications due to the risks of side effects, but that many governments now believe this right should be removed solely with regard to Covid vaccines. There is no compelling moral argument for why Covid vaccines fall into an exceptional category that warrants the state using coercion whether it be direct (vaccine mandates) or indirect (segregation and removal of rights) to force its citizens to reluctantly take a medicine they would otherwise refuse.
The enthusiasm for vaccines and excessive restrictions are now articles of faith for their proponents. It has become an ideological stance that no amount of reasoned scrutiny can alter. Rational analysis of the extent of the threat from Covid and strategies to deal with it have been abandoned for the simplistic dogma of ‘vaccines good’ and ‘lockdowns and restrictions good’. The truth is much more nuanced than the doom-mongering analysis which permeates the mainstream media. Lockdown enthusiasts and vaccine zealots, like all ideologues, have opponents whom they despise and whom they seek to demonise. This is why only ‘far Right conspiracy theorists’ and ‘anti-vaxxers’ would have an issue with mandatory vaccines which can have serious side effects being given to children to protect them from a virus that rarely makes children very ill.
How have we reached a stage in Western liberal democracies when those of us questioning and disagreeing with extreme public health policies that strip individual citizens of their inalienable rights under false pretences are the ones deemed to be the extremists? Asking questions and being critical of government policy is now viewed by the obedient media class and the political elites and partisan scientific ‘experts’ they serve as being synonymous with the far Right. In truth, it is your democratic duty to question all government policies and especially more so those that would remove your fundamental freedoms. For any government to wish to suspend the rights of its citizenry on a temporary basis, it must first seek consent from the people after explaining the exceptional circumstances in which they seek to do so. There has been no public debate and little media scrutiny across the English-speaking world about whether the threat posed by Covid-19 meets the very high threshold that could justify temporary lockdowns and other extreme restrictions imposed on the citizenry.
If the UK or Irish government or any of the devolved administrations try to impose another lockdown, I predict there will be mass non-compliance. It is very likely that much of the population of these islands will conclude that if several lockdowns, mask mandates and ‘game changing’ vaccines have not eradicated transmission, why comply with another lockdown, possible financial ruin and separation from loved ones? What would be the purpose? As someone once said (it wasn’t actually Einstein): ‘Insanity is doing the same thing over and over and expecting different results.’
Guardian Claims Covid in Hospitals Has “Largely Become a Disease of the Unvaccinated” – Data Shows Opposite
By Will Jones • The Daily Sceptic • November 23, 2021
An article appeared in the Guardian this week written by an anonymous NHS respiratory consultant claiming that “in hospital, COVID-19 has largely become a disease of the unvaccinated”.
Of course, there are people who have their vaccinations but still get sick. These people may be elderly or frail, or have underlying health problems. Those with illnesses affecting the immune system, particularly patients who have had chemotherapy for blood cancers, are especially vulnerable. Some unlucky healthy people will also end up on our general wards with Covid after being vaccinated, usually needing a modest amount of oxygen for a few days.
But the story is different on our intensive care unit. Here, the patient population consists of a few vulnerable people with severe underlying health problems and a majority of fit, healthy, younger people unvaccinated by choice. … If everyone got vaccinated, hospitals would be under much less pressure; this is beyond debate. Your wait for your clinic appointment/operation/diagnostic test/A&E department would be shorter. Your ambulance would arrive sooner. Reports of the pressure on the NHS are not exaggerated, I promise you. … Most of the resources that we are devoting to Covid in hospital are now being spent on the unvaccinated.
This reads to me like a blatant attempt to stigmatise the unvaccinated as selfish, a burden on society and a threat to the vaccinated. (The clue is in the headline: “ICU is full of the unvaccinated – my patience with them is wearing thin.”) Given the polling (which may not be very reliable of course) showing that 45% of U.K. adults would support an indefinite lockdown of the unvaccinated, this is all starting to look and sound rather ugly.
The most frustrating thing about this anonymously written article is it doesn’t cite any data even though its arguments are based on claims which only data can validate. It consists instead only of a single medic’s subjective impressions, with no sources provided to see if his claims holds water.
Are the hospitalised mostly unvaccinated? Not according to Government data from the UKHSA. Here is the breakdown of hospitalisations by vaccination status in England for the four weeks up to November 14th from the latest Vaccine Surveillance report.

Adding these figures up we find that 3,200 of 9,831 or 33% of Covid hospitalisations are of unvaccinated people, leaving 67% of Covid hospital patients in the vaccinated category, most of them with two doses. Focusing just on adults, we find 2,692 of 9,278 or 29% of Covid hospitalisations are unvaccinated, leaving 71% vaccinated. Seeing as just 68% of the U.K. population is double vaccinated, 67% of Covid hospital patients having received at least one dose hardly seems like a strong result. Indeed, it suggests the unvaccinated are barely over-represented in hospitals at all.
What about Covid deaths – are the unvaccinated over-represented there? Here’s the table from the same report.

Adding them up we find that 675 of 3,676 or 18% of Covid deaths in the month up to November 14th are in unvaccinated people, leaving 82% in the vaccinated, most with two doses. Only in the under-40s do deaths in the unvaccinated outnumber those in the vaccinated.
It’s hard to square this data with the picture painted by the anonymous medic. Far from COVID-19 having “largely become a disease of the unvaccinated”, with most Covid hospital resources “now being spent on the unvaccinated”, a large majority of hospitalisations and deaths are occurring in the vaccinated, not the unvaccinated.
But what about ICU admissions? And is it true that the vaccinated-sick all have underlying health issues whereas the unvaccinated-sick are all healthy?
The problem with addressing these claims is that we don’t have the data to check them out. The data on ICU admissions by vaccination status has not been updated since July as far as I can see (if you are aware of a more recent update do let me know), and I am not aware of any data on co-morbidities (again, if you are aware of any please drop me a line).
The anonymous writer states: “I can’t think of a single case offhand of a person who was previously fit and healthy who has ended up needing intensive care after being fully vaccinated. It may not stop you from catching Covid. But it can save your life when you do.” But again, this is anecdotal and therefore not terribly helpful.
It’s fair to note that much data does appear to show that the vaccines protect people well against severe disease and death, at least for several months, though some recent analysis has questioned whether such efficacy has been overestimated.
But however well the vaccines protect against severe disease, that is no excuse for turning the unvaccinated into pariahs or scapegoats and blaming them for the strains on the health service. Such moralised blaming of a minority for supposedly disadvantaging the majority (‘Can’t get a doctor’s appointment? Surgery been cancelled again? The unvaccinated are to blame!’) has a very ugly history and rarely ends well. It’s particularly odd to see this scapegoating in a supposedly liberal newspaper. It needs to stop now.
Lethal Injection; Frontline E.R. Doctor Gives Chilling Account of Unusual Vaccine-Induced Illness
BY MIKE WHITNEY • UNZ REVIEW • NOVEMBER 20, 2021
“Americans are scared to death… People are walking off the job, not because they want to lose their jobs, but they don’t want to die from the vaccine! … They say, ‘Listen, I don’t want to die. That’s the reason I’m not taking the vaccine.’ It’s that clear.” Dr. Peter McCullough
A report in the U.K. Telegraph explains how the Covid-19 vaccine has led to a sharp rise in excess deaths. Here’s an excerpt from the article:
“Nearly 10,000 more people than usual have died in the past four months from non-Covid reasons, as experts called for an urgent government inquiry into whether the deaths were preventable…
Latest figures from the Office for National Statistics showed that England and Wales registered 20,823 more deaths than the five-year average in the past 18 weeks. Only 11,531 deaths involved Covid.” (“Alarm grows as mortuaries fill with thousands of extra non-Covid deaths,” UK Telegraph )
Mortality is rising because more people are dying. And more people are dying because more people have been vaccinated. There’s a link between rising mortality and the Covid-19 vaccine. Naturally, the media wants to shift responsibility for the fatalities to “delayed treatments” and “the lack of preventable care”. But this is just a diversion. The primary cause of death is the injection of a toxic pathogen into the bloodstreams of roughly 70% of the population. That’s what’s causing the clotting, the bleeding, the pulmonary embolisms, the heart attacks, the strokes, and the premature deaths. It’s the vaccine. Here’s more
“Weekly figures for the week ending November 5 showed that there were 1,659 more deaths than would normally be expected at this time of year. Of those, 700 were not caused by Covid.
The excess is likely to grow as more deaths are registered in the coming weeks.
Data from the UK Health Security Agency show there have been thousands more deaths than the five-year average in heart failure, heart disease, circulatory conditions and diabetes since the summer.
The number of deaths in private homes is also 40.9 per cent above the five-year average, with 964 excess deaths recorded in the most recent week, which runs up to November 5.” (“Alarm grows as mortuaries fill with thousands of extra non-Covid deaths“, UK Telegraph )
The sudden surge in mortality is not a meaningless blip on the radar. It’s a red flag indicating a significant break in the five-year trend. Something has gone terribly wrong. Mass vaccination was supposed to reduce the number of cases, hospitalizations and deaths. Instead, the fatalities continue to rise.
Why?
The answer to that question can be found in the data itself. As the author admits, there has been a sharp uptick in heart failure, heart disease, circulatory conditions and strokes. (Diabetes is the outlier) These are precisely the ailments one would expect to see if one had just injected millions of people with a clot-generating biologic that triggers a violent immune response that attacks the inner lining of the blood vessels inflicting severe damage to the body’s critical infrastructure. So, yes, all-cause mortality is up, and it is certain to climb even higher as more people are vaccinated and gradually succumb to the (frequently) delayed effects of a hybrid concoction that is the cornerstone of a malign plan to dramatically reduce global population. Check out this chart followed by a brief comment by diagnostic pathologist, Dr Claire Craig:

Dr Clare Craig @ClareCraigPath
“Since summer there have been twice as many covid deaths, but seven times as many excess deaths as last year.” (Twitter)
And here’s another blurb from Craig:
“If you start at week 22 and add up all the deaths since for each year, then something very abnormal is happening this year among 15-19 yr old males.”

So, not only are more people dying, but the demographic has shifted downwards as younger and younger people are drawn into the vaccine vortex. Simply put, the number of young people dying from vaccine-inflicted cardiac arrest and myocarditis continues to increase with no end in sight.
Not surprisingly, all-cause mortality is higher among the vaccinated than the unvaccinated which, again, makes it easier to trace the problem back to its root, a cytotoxic “poison-death shot” that suppresses the innate immune system, damages vital organs and shaves years off the lives of normal, healthy people.
Perhaps, you’ve seen one of the many short videos of fit, young athletes who suddenly have dropped dead on the field of play or been rushed to hospital shortly after getting injected. If not, here’s a link to two of them. (Athletes collapse following vaccination: See here and here)
According to Israeli Real-Time News, there has been a “500% increase in deaths of players in 2021… Since December, 183 professional athletes and coaches have suddenly collapsed! 108 of them died!”
“500% increase in the deaths” of athletes?!? What are we to make of this?
For starters; the Covid-19 vaccine is not a medication. It is the essential component in the elitist plan for industrial-scale extermination. It is designed to inflict severe physical injury on the people who take it. It’s shocking that people are so deep in denial that they can’t see what’s going on right before their eyes. (Please, watch the video clips of the athletes. These are the fittest people on the planet and, yet, they are being struck down by the mystery substance in the vaccine.) Here’s how South African doctor Shankara Chetty summed it up in a recent video posted on Bitchute:
“The pathogen that is causing all the deaths from the illness is the spike protein. And the spike protein is what the vaccine is supposed to make in your body. … Spike protein is one of the most contrived poisons that man has ever made. And, the aim of this toxin, is to kill billions of people without anyone noticing it. So it is a poison with an agenda.” (“South African Physician Dr. Shankara Chetty Talks about “The Bigger Plan”, Bitchute)
There it is in a nutshell. And Chetty is not alone in linking the vaccine to the agenda of the globalist elites who plan to use the cover of a pandemic to implement their “population management” scheme. Former Pfizer vice president, Mike Yeadon, offered a similar view just days ago on his website. He said:
“We are in the midst of the biggest depopulation program the world has ever seen, where most of humanity are acting as useful idiots to it and to their own demise.”
Indeed, and we have tried to provide as much information as possible on the biologic agent that is being used to pursue this malign agenda, the spike protein. In early reports we passed along the research of Dr. Patrick Whelan who grasped the danger of the spike protein before anyone else. Here’s a brief recap of his analysis from a letter he submitted to the FDA on December 8, 2020:
“I am concerned about the possibility that the new vaccines aimed at creating immunity against the SARS-CoV-2 spike protein have the potential to cause microvascular injury to the brain, heart, liver, and kidneys in a way that does not currently appear to be assessed in safety trials of these potential drugs.
… Meinhardt et al…. show that the spike protein in brain endothelial cells is associated with formation of microthrombi (clots)… In other words, viral proteins appear to cause tissue damage without actively replicating virus…. The Pfizer/BioNTech vaccine (BNT162b2) is composed of an mRNA that produces a membrane-anchored full-length spike protein. The mouse studies suggest that an untruncated form of the S1 protein like this may cause a microvasculopathy in tissues that express much ACE2 receptor.
… it appears that the viral spike protein… is also one of the key agents causing the damage to distant organs that may include the brain, heart, lung, and kidney. Before any of these vaccines are approved for widespread use in humans, it is important to assess in vaccinated subjects the effects of vaccination on the heart…. As important as it is to quickly arrest the spread of the virus by immunizing the population, it would be vastly worse if hundreds of millions of people were to suffer long-lasting or even permanent damage to their brain or heart microvasculature as a result of failing to appreciate in the short-term an unintended effect of full-length spike protein-based vaccines on these other organs. (“FDA shrugs off dire warning about lethal spike protein“, Truth in the Age of Covid)
From the very beginning, government regulators and their allies in the public health establishment have ignored (or censored) the warnings of capable physicians and researchers. They also waved-off career immunologist and vaccinologist, Dr Byram Bridle who was the first in his profession to identify the spike protein as “a specific causative agent of disease”; aka–“a pathogen”. Here’s Bridle:
“‘We have known for a long time that the spike protein is pathogenic… It is a toxin. It can cause damage in our body if it’s in circulation. Now, we have clear-cut evidence that . . . the vaccine itself, plus the protein, gets into blood circulation.’”
Once that happens, the spike protein can combine with receptors on blood platelets and with cells that line our blood vessels. This is why, paradoxically, it can cause both blood clotting and bleeding. ‘And of course the heart is involved, as part of the cardiovascular system… That’s why we’re seeing heart problems. The protein can also cross the blood-brain barrier and cause neurological damage…
‘In short,… we made a big mistake. We didn’t realize it until now. We didn’t realize that by vaccinating people we are inadvertently inoculating them with a toxin.”… (“Vaccine scientist: ‘We’ve made a big mistake’“, TCW Defending Freedom )
Here again, we have a highly-regarded immunologist, with more than 3 decades of experience under his belt, who offered his informed and evidence-based research on an issue that should have been of great interest to the regulators that were making decisions about the long-term safety of the experimental drug they were foisting on millions of people across the country. But there was no interest at all. Despite the fact that the science supported his conclusions, Bridle was viciously attacked, censored, dragged through the mud, and forced to leave his place of employment.
Why?
Because he drew the same conclusions as Dr. Patrick Whelan. There’s really no substantive difference between the two except that Bridle’s comments attracted more attention in the media which made him a greater threat to the “universal vaccination” strategy. That was his real crime; he discovered the truth and made his findings available to the public, basically alerting them to the dangers of the “poison-death shot”. For that he was crushed.
Bridle has since made other claims that should concern anyone whose cancer might be in remission. Here’s what he said in a recent interview:
“What I’ve seen way too much of is people who had cancers that were in remission, or that were being well controlled; their cancers have gone completely out of control after getting this vaccine. And we know the vaccine causes a drop in T-cell numbers, and those T-cells are part of our immune system and they are part of the critical weapons our immune system has to fight off cancer cells; so there’s a potential mechanism there. All I can say, is I’ve had way too many people contact me with these reports for me to feel comfortable. I would say that is my newest major safety concern, and it’s also the one that’s going to be the most under-reported in the adverse data base, because if someone has had cancer before the vaccine, there’s no way public health officials will ever link it to the vaccine.” (“Dr Byram Bridle speaks”, Bitchute, :55 second-mark)
So, the vaccine suppresses the immune system?
Yes, it does, and author Alex Berenson provided evidence of this just recently in an article he posted on Substack. Here’s an excerpt:
“… the British government… admitted today, in its newest vaccine surveillance report, that:
“N antibody levels appear to be lower in people who acquire infection following two doses of vaccination.” (Page 23)
What’s this mean?…
What the British are saying is they are now finding the vaccine interferes with your body’s innate ability after infection to produce antibodies against not just the spike protein but other pieces of the virus…
This means vaccinated people will be far more vulnerable to mutations in the spike protein EVEN AFTER THEY HAVE BEEN INFECTED AND RECOVERED ONCE…
… it probably is still more evidence the vaccines may interfere with the development of robust long-term immunity post-infection.” (“URGENT: Covid vaccines will keep you from acquiring full immunity EVEN IF YOU ARE INFECTED AND RECOVER”, Alex Berenson, Substack)
Berenson’s observations square with research that was compiled earlier in the year by scientists in The Netherlands and Germany who:
“… warned that the … (COVID-19) vaccine induces complex reprogramming of innate immune responses that should be considered in the development and use of mRNA-based vaccines… the research team from Radboud University Medical Center and Erasmus MC in the Netherlands… showed that the vaccine altered the production of inflammatory cytokines by innate immune cells following stimulation with both specific (SARS-CoV-2) and non-specific stimuli.
Following vaccination, innate immune cells had a reduced response to toll-like receptor 4 (TLR4), TLR7 and TLR8 – all ligands that play an important role in the immune response to viral infection…. an unexplored area is whether BNT162b2 vaccination has long-term effects on innate immune responses …
This could be very relevant in COVID-19, in which dysregulated inflammation plays an important role in the pathogenesis and severity of the disease,” writes the team. “Multiple studies have shown that long-term innate immune responses can be either increased (trained immunity) or down-regulated (innate immune tolerance) after certain vaccines or infections.” (Research suggests Pfizer-BioNTech COVID-19 vaccine reprograms innate immune responses, new-medical-net)
Berenson’s finding also align with with cutting-edge research showing that the spike protein greatly “impedes adaptive immunity” by preventing DNA from repairing damaged cells. The paper suggests that the spike protein does in fact “impact on the nucleus of the cell, where we store our DNA, our core genetic material.” Here’s more from Berenson’s breakdown of the paper:
“… our cells have mechanisms to repair their own DNA.
But – at least in the experiments these two scientists ran – the spike protein appeared to interfere with our own DNA repair proteins: “Mechanistically, we found that the spike protein localizes in the nucleus and inhibits DNA damage repair by impeding key DNA repair protein BRCA1 and 53BP1 recruitment to the damage site.”
To be clear, the scientists did NOT prove the spike protein was causing these problems in people, or even animals… Nonetheless, at a time when advanced countries that have high mRNA (and DNA/AAV) vaccination rates are seeing unusually full hospitals and higher-than-normal death rates, they are yet more cause for concern. As the authors explained:
“Our findings reveal a potential molecular mechanism by which the spike protein might impede adaptive immunity and underscore the potential side effects of full-length spike-based vaccines.” (“URGENT: Worrisome paper about the spike protein’s impact on DNA and DNA repair”, Alex Berenson, Substack)
Bottom line: If the vaccine does in fact inhibit the body’s innate immune response, then people are going to get alot sicker from seasonal infections that routinely spread through the population. Their path to recovery will also be alot more difficult.
But rather than belabor the immunity angle, let’s move on to the research of Dr Charles Hoffe who was the first physician to provide hard evidence that the vaccines generate blood clots by triggering an immune response in which the body attacks the thin layer of cells lining the walls of the blood vessels. Hoffe found that 62% of his patients that had been vaccinated tested positive for blood clots on a D-dimer test. Naturally, he was alarmed by what he found, particularly since the vaccine “was causing serious neurological events, and even death. When he raised his concerns with the BC College of Physicians, they immediately implemented a gag order, and reprimanded him in an attempt to intimidate, and silence him.”
Hoffe has been interviewed a number of times and always provides a detailed and riveting account of his findings. In a recent interview, he predicted that some vaccinees suffering from clot-related issues would likely die in just three years. Here’s what he said:
“… once you block off a significant number of blood vessels to your lungs, your heart must pump at a much greater resistance to get the blood through your lungs. That causes a condition called pulmonary artery hypertension, which is high blood pressure in your lungs because so many of the blood vessels in your lungs are blocked. And the terrifying thing about this is that people with pulmonary artery hypertension usually die of right-sided heart failure in three years… And not only is the long-term outlook very grim, but with each successive shot, the damage will add and add and add. It’s going to be cumulative because you are getting more and more damaged capillaries.” (“Shock: Doctor Warns That Majority Of Vaccinated Patients Could HavePermanent Heart Damage, Some May Die Within Three Years”Permanent Heart Damage, Some May Die Within Three Years”, Infowars; Minute 6:10)
Once again, there is no discrepancy between the analysis of Whelan, Bridle and Hoffe. And while the focus of their attention might vary slightly, their conclusions are the same. These experimental injections pose serious risks for anyone who allows himself to be inoculated.
Now check out how similar Hoffe’s analysis is to Dr. Rochagne Kilian who was an Emergency Room physician at the GBHS hospital until she resigned in protest. This is a particularly important video as it describes the “oddball” symptoms and exceedingly rare conditions that are now presenting in emergency rooms everywhere following the mass vaccination of millions of people with the “poison-death shot”. (I transcribed the video myself, so there could be errors.)
Dr Rochagné Kilian – Blows the Whistle on Covid-19 Vaccines and D-Dimer Levels
“What I was seeing in my ER department especially in the last 8 to 9 months is related to the D-Dimer levels. We use D-Dimers specifically related to pulmonary embolisms as well as Deep Vein Thrombosis. D-Dimer detects any thrombosis (clots) in the body but it doesn’t give you a diagnosis it gives you a basis for going further and doing an ultrasound and CT scan to either confirm or deny the presence of a pulmonary embolism or Deep Vein Thrombosis.
The first part of 2020 was probably the slowest ever in the emergency department, but when we went into 2021 and the vaccination rollout started, we ended up seeing an increase in stroke, transient ischemic attacks and stroke like presentations. (There were) definitely significant larger numbers of those people coming in. I ended up doing D-dimer tests on these people and never before in my clinical experience had I seen D-dimers and the amount of people with positive D-dimers higher than 2,000, higher than 3,000 and higher than 5,000. My clinical experience told me a needed to go look for a large clot either in their legs or their lungs. And I ended up doing a CT scan on these people. Most of them, and I will say almost all of them, had negative scans which started making me think that if there was not a significant clot in their lungs, but my D-dimer was so much higher than what I was usually seeing, it might not be concentrated in one clot. But that it is multiple micro-thrombi extended throughout the body, and that is so easy to miss because the CT scan is not going to pick it up.
“These people coming into the ER were all people anywhere from about a week to four months after receiving their 2nd injections. There are certain factors that can influence a D-dimer test that can give you a sense of a higher level than would be expected in the body. That said, the patients I was doing D-Dimer tests on did not have a level of maybe a positive 500 or 400 reading. It was more than 3500, more than 5000 ng/ml. So those are significantly positive without any proof of having a pulmonary embolism. If I was seeing high levels of D-dimer without a definite diagnosis, I needed to ask more questions.
One study said, never ignore extremely elevated D-dimer levels. They are specific for serious illness, including venous thrombosis, sepsis, and/or cancer. Even if sharply elevated D-dimer are a seemingly solitary finding, clinical suspicion of severe underlying disease should be maintained.
There were two conditions that stood out and the first one was disseminated intravascular coagulation also known as DIC. The second one is antiphosphlipid syndrome. Both of these conditions are related to an abnormality in either the initiation or the feedback of the coagulation pathway as well as thrombosis or the thrombosis cycle where clots are being broken down. DIC is a serious sometimes life threatening situation in which the proteins in the blood involved in blood clotting become overactive. It’s a cascade that’s difficult to stop once it’s reached a certain level. There are certain conditions that trigger DIC; significant sepsis, underlying viruses, trauma, major surgery, pregnancy and childbirth. And less common causes toxic drug reaction, blood transfusion reaction, and organ transplants. So there was a connection with intravascular products and a possible DIC.
Most cases of DIC are diagnosed rapidly and suddenly which is the acute presentation. But there are cases where it develops gradually, occurring over a longer period of time. This is known as a chronic form of DIC and I would go as far to say a subacute form of DIC that is very easy to miss. Simultaneous clotting and bleeding can occur with chronic DIC. The bleeding part comes in blood in the urine, headaches and other symptoms associated with brain bleeds, bruising, inflammation of red, small dots on the limbs, bleeding at sites of wounds and mucosal bleeding. which means bleeding out of the gums and nose. I definitely saw an increase in nose bleeds and bleeding from previous wound sites. ulcers, as well as rashes that couldn’t be explained. Blood clotting symptoms and signs were symptoms like chest pains, heart attacks, strokes, TIAs, and headaches either related to bleeding or not. As well as symptoms related to kidney failure, because of the clotting of those smaller blood vessels that go to the kidneys. Antiphosphlipid syndrome is a very similar type of condition. But the basis of the antiphosphlipid syndrome is an autoimmune disorder meaning that the body’s immune system makes proteins–known as antibodies–that mistakenly attacks its own body or tissues. That gives the skin the cascading effect of clotting disorder but it is linked to an autoimmune trigger. Basically, it presented in exactly the same way; high blood pressure which I was seeing alot of; first diagnosis of high blood pressure, heart attacks, strokes, TIAs, heart valve problems, repeated headaches or migraines, vision loss, balance and mobility problems, difficulty concentrating or thinking clearly,
The astute listener would start forming a picture of what we’ve been told about Covid-19, and there are research papers connecting Covid 19 with an underlying vascular disease. One of these was a study called “Covid 19; unraveling the clinical progression of Nature’s Virtually perfect Biological weapon.”
“SARS-Cov-2, presenting as Covid-19 syndrome, was not a respiratory basis, but an underlying vascular basis. which had certain phases of incubation, pulmonary phase, pro inflammatory phase, (which once again comes into a cytotoxic inflammation process) then moves into a protothrombic phase . Covid-19 is a thrombotic disease. implications for prevention, antithrombotic therapy and follow up…
This picture shows us certain risk factors, Homeostatic Abnormalities, as well as clinical outcomes. It indicates increased D-dimer levels. It also mentions Venous Thromboembolism, Myocardial Infarction, and Disseminated Intravascular Coagulation that is connected to postulated mechanisms of coagulathopy as well as parthenogenesis of thrombosis in Covid-19…
I started asking the question, if we are able to detect certain connections between vascular abnormalities and Covid-19, and we based our proposed treatment on the spike protein, which includes the Pfizer and Moderna injections, shouldn’t we be looking for similar side effects or complications from that same injection?
If we are mandating certain treatments, we do need to do the due diligence to make sure what the side effects and complications especially in a time where there has not been long term studies.”And that’s what led me to focusing on D-dimers.” (“Dr Rochagné Kilian – Blows the Whistle on Covid-19 Vaccines and D-Dimer Levels“, Bitchute)
Kilian’s statement should be read over and over again. It is the most detailed description we have of the mysterious and deeply sinister machinations of a laboratory-engineered bioweapon that, in effect, turns the vascular and immune systems against the person who was vaccinated. Disseminated intravascular coagulation and antiphosphlipid syndrome are names that are entirely unknown to the American people, and yet, these freakish conditions are now responsible for a growing number of patients that are experiencing bleeding, clotting, headaches, rashes, bruising, high blood pressure, and inflammation . And– in more extreme cases– chest pains, heart attacks, strokes, heart-valve problems, and brain bleeds. One can only guess how the media will try to cover-up these extraordinarily-rare and potentially life-threatening conditions??
When Kilian asks:
“If we are able to detect certain connections between vascular abnormalities and Covid-19… shouldn’t we be looking for similar side effects or complications from that same injection?”
Bingo! If the spike protein produced by the vaccines, inflicts the same internal damage as Covid-19, then shouldn’t doctors expect to see the same symptoms?
Yes, they should. And if the symptoms are the same, then there’s a good chance that vaccine-induced injuries are being misdiagnosed as Covid-19.
Think about that for a minute. That would be the perfect scenario for the pandemic managers and their billionaire backers who’d love to see the impending mountain of carnage blamed on the waning virus instead of on their own poison-death shot.
And that is the evil-genius of the globalist strategy; to remove the fingerprints from the smoking gun before the investigators even arrive at the scene of the crime.
The amount of planning that must have gone into this scam, is simply breathtaking.

Featured Video

Iran Walks Out On Peace Deal Due To Trump’s Threats
or go to
Aletho News Archives – Video-Images
From the Archives
Neocons confess: “We did 9/11-anthrax”
By Kevin Barrett | Press TV | September 6, 2014
As the 13th anniversary of the crimes of September, 2001 approaches, the neoconservatives are shrieking from the rooftops – and effectively confessing that they were the real perpetrators of the 9/11-Anthrax false flag operation. (The neocons, you may recall, openly called for a “new Pearl Harbor” in September, 2000 – and got one exactly one year later.)
Every year at this time, the neocons orchestrate and hype a series of public relations stunts designed to magnify fears of “radical Islam” and reinforce their crumbling 9/11-Anthrax cover story. But this year’s propaganda campaign is so extreme that it represents a tacit confession: The neocons know that the truth about the 9/11-Anthrax operation is slowly closing in on them; so they are over-reacting by desperately trying to stoke the dying embers of the so-called War on Terror, in order to maintain the myth that Muslims (rather than neoconservative Zionists) attacked America in the autumn of 2001.
When a hysterical person exhibits guilty demeanor by trying too hard to blame a crime on someone else, that person is almost certainly the real perpetrator. As the neocons try much too hard to blame Islam for 9/11 and “terrorism” in general, their hysteria inadvertently reveals their own culpability. Like Shakespeare’s Lady MacBeth, the neoconservative movement has blood on its hands and “doth protest too much.” … continue
Blog Roll
 Aletho News
Aletho News- Report highlights US munitions crisis: Missiles cannot be replenished quickly even with al the money in the world
- Iran’s Oil Spigot Could Open Soon But Hurdles Remain
- Trump’s Attempt to End the Iran War Infuriates the Uniparty
- First round of Swiss-hosted Iran-US talks ends with 5 key agreements
- What Is Hay Fever?
- IRAN WALKS OUT ON PEACE DEAL DUE TO TRUMP’S THREATS – w/ Prof. Seyed Mohammad Marandi
- Moderna’s mRNA Flu Vaccine Gets Unanimous Thumbs-Up Despite Risks, Low Efficacy
- UK Speech Regulator’s Telegram Questions Point Toward Private Chats
- Cuban FM blasts Rubio for ‘chronically lying’ about US fuel blockade
- Al-Jazeera demands punishment for Israeli officials following latest assassination of cameraman
- If Americans Knew
- Gaza Soccer Player Who Dreamed of Competing in World Cup Can Now Barely Watch It
- Gaza baby loses mom and a leg; Palestinian prisoner tortured to death – Daily Update
- JNS Policy Summit to kick off in Israel
- Fatalities From Israel’s Vast Gaza Genocide Deliberately Undercounted
- ‘Reproductive genocide’ in Gaza; death toll in Lebanon tops 4,000 (during a ceasefire) – Daily Update
- Israelis Invaded Lebanon And Then Cried Victim When Their Soldiers Got Killed
- FARA Docs: Israel is Spying On Millions Of Christian Americans In Their Churches
- Why US presidents from both parties end up cursing Benjamin Netanyahu
- Israel Asked Facebook to Censor Iran War Content, Internal Documents Show
- Deaths in Gaza undercounted, possibly by 100s of thousands; “Psychopath” Ben-Gvir talks trash – Daily Update
- No Tricks Zone
- THE TRANSCEIVER PARADOX: Why Organoid Intelligence (OI) Could Become Our Ultimate Alien Predator
- German Wind Turbines Face Regulatory Shutdown Due To Excessive Noise
- New Study: Chile’s Relative Sea Level Was 3.2 Meters Higher Than Today During The Mid-Holocene
- Beyond The Pitch: Why FIFA’s World Cup Is One Of Humanity’s Best Investments
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
