Taxpayer-Funded Initiative Urges Dentists to Push HPV Vaccines
By Brenda Baletti, Ph.D. | The Defender | November 2, 2023
The National Institute of Dental and Craniofacial Research (NIDCR) awarded over $685,000 to HealthPartners Institute to test strategies for getting dentists to recommend the human papillomavirus (HPV) vaccine to children and young adults ages 11-26, documents obtained by Children’s Health Defense (CHD) via a Freedom of Information Act (FOIA) request revealed.
The NIDCR operates under the government’s taxpayer-funded National Institutes of Health (NIH).
The HealthPartners study is being conducted three years after the U.S. Food and Drug Administration (FDA) added prevention of oropharyngeal cancer, a form of head and neck cancer, to a growing list of indications for the HPV vaccine — despite a lack of clinical evidence to support the claim.
Dentists remain generally reluctant to recommend or administer the vaccine to their patients, studies show.
The NIDCR funding covers the first two years of a six-year, $3.5 million proposal for the healthcare nonprofit to experiment with training dental providers to deliver scripted messages to their patients about why they should get the HPV vaccine.
HealthPartners will then run a clinical trial in 21 dental clinics to determine whether the training and messages lead more dental providers to recommend the vaccine, and more patients to take it.
The grant is one of nearly 50 identified by CHD in June — totaling more than $40 million — awarded by the U.S. Department of Health and Human Services (HHS) to universities, healthcare systems and public health departments to increase HPV vaccine uptake among adolescents.
The NIDCR is the latest of several HHS sub-agencies to fund behavior modification research aimed at providers and patients in order to increase vaccine uptake.
Why would dentists be charged with recommending the HPV vaccine?
Dentists are uniquely positioned to promote the HPV vaccine because they tend to have more regular contact with young patients than other healthcare providers, the HealthPartners proposal states.
The Centers for Disease Control and Prevention (CDC), the American Dental Association and the American Academy of Pediatric Dentistry all recommend that dental providers promote HPV vaccination — but most dental providers don’t see vaccine promotion as part of dentistry.
HPV is the most common sexually transmitted infection in the U.S. Most people will get the infection at some point in their lives, but more than 90% of infections clear on their own with no residual health consequences on clinical follow-up.
High-risk HPV types can cause cervical cell abnormalities that are precursors to cancer, however, HPV infection is not the sole risk factor for cervical cancer.
Regular pap screening has been found to reduce the incidence of and mortality from cervical cancer among women by at least 80%.
Merck’s Gardasil 9 — the only HPV vaccine marketed in the U.S. — is a widely used vaccine commonly administered to teens and young adults before they are sexually active to protect against nine of more than 200 strands of HPV that can be sexually transmitted later in life.
Despite Merck marketing Gardasil as a vaccine that protects against some forms of cancer, clinical trials for Gardasil did not test whether the vaccine protected against any cancer — only whether it had efficacy against the indicated strains of HPV.
Gardasil has been associated with a number of serious adverse events.
Some of the signature impacts observed following HPV vaccination include permanently disabling autoimmune and neurological conditions such as postural orthostatic tachycardia syndrome (POTS), fibromyalgia and myalgic encephalomyelitis/chronic fatigue syndrome.
More than 80 lawsuits against Merck now pending in federal courts allege the drugmaker fast-tracked Gardasil through the FDA’s approval process and deceptively conducted clinical trials to mask serious side effects and exaggerate the vaccine’s effectiveness.
In June 2020, the FDA added the prevention of oropharyngeal and other head and neck cancers to the list of indications for the HPV vaccine under the “accelerated approval licensure pathway.”
That pathway allows treatments to be approved before clinical data demonstrating benefit exists, based on early clinical predictions that the treatment will likely produce a benefit.
Later, if a clinical benefit is never found, the FDA “can seek withdrawal” of the drug from the market.
According to the HealthPartners grant proposal, HPV is the leading cause of oropharyngeal cancers in the U.S., However, the references cited to support that claim are from 2014 — and they don’t appear to support the claim.
The CDC estimates 70% of oropharyngeal cancers in the U.S. are “thought to be” caused by HPV, and qualifies even that claim by adding, “It is unclear if having HPV alone is enough to cause oropharyngeal cancers.”
There is no evidence that the HPV vaccine prevents oropharyngeal cancers, but some trials have found that it does have efficacy against vaccine-type oral strains of HPV.
Top NIH-funded Merck consultants in the field, like Noel Brewer, Ph.D. — who developed and promotes the “announcement approach” to increasing vaccine uptake — have long looked to expand HPV vaccination into settings outside of primary care.
On that basis, the HealthPartners study aims to change dental providers’ behavior so they consistently recommend the HPV vaccine to their patients. Dr. Brad Rindal, a dentist, and Patricia Mabry, Ph.D., a clinical psychologist, are co-leading the study.
The proposal falls within HHS’ mission to understand the mechanisms of behavior change in order to develop methods of “experimental manipulation or intervention” with providers and patients that can help it meet its targets in various aspects of public health.
HHS, through the NIH, has been funding behavioral studies to assess and influence providers’ willingness to recommend and administer the HPV vaccine in order to increase rates of vaccine uptake since shortly after the vaccine was first licensed in 2006.
Study design explicitly waives informed consent for patients
In the study, a team of researchers from HealthPartners — which provides healthcare, coverage, research and education to 1.8 million plan members — will train providers, teaching them about the relationship between the HPV vaccine and the risk of oropharyngeal cancer.
Trained providers also will receive scripts for use in patient conversations tailored to “reduce fear” that such conversations will negatively impact provider-patient relationships. They also will learn how to refer their patients to a vaccine scheduler.
Researchers will then measure changes in provider behavior through direct provider reporting — they press a button in their office when they make a recommendation — and follow-up surveys.
Patients or patient parents or guardians will receive follow-up survey calls after the office visits to assess how effective the provider communication was.
Researchers will measure changes in patient behavior by assessing how many patients receive initial and follow-up doses of the HPV vaccine within 30 days of their office visit.
In the first two years of the study — funded by the initial grant — the team will develop and pilot test their training and scripts. Their control group will receive patient education brochures and untailored scripts and their intervention group will receive the training and the tailored scripts.
In the next phase, they will test the efficacy of these interventions in clinic-randomized trials, comparing the control and intervention groups. Twenty-one HealthPartners Dental Group clinics and their providers will participate.
Patients 11-26 years old who go to HealthPartners dental clinics and whose electronic health records indicate they have not initiated or completed the HPV vaccine series will be automatically enrolled in the study without their knowledge. HealthPartners estimates there will be approximately 8,000 qualifying visits with HPV unvaccinated patients.
Verbal informed consent will be obtained for participation in the post-intervention patient/parent phone survey.
The patients will not otherwise be informed of the study.
The study requests a waiver of informed consent for patients by arguing that the dental providers will only be making recommendations already endorsed by the CDC, the American Cancer Society and the National HPV Roundtable, which is a joint venture of the CDC and the American Cancer Society.
“Therefore,” they state, “the recommendations conform to current standards of care and don’t present a risk to patients that exceed the risks that patients assume when they seek care within any healthcare system focused on disease prevention through vaccination promotion.”
They also argue that the research “would not be feasible without such a waiver” because it would bias the provider involvement and patient response.
They add that patients sign a HIPAA authorization form that allows them to opt out of using health data for research purposes and that they will be certain to check that list.
Finally, they note that “patients can elect not to pursue vaccination despite the recommendation of the dental care provider” — even though the intervention is designed to change their behavior so they don’t make such an election.
Merck, federal public health agencies, and WHO looking to grow market for HPV shots
Merck’s Gardasil was first licensed in 2006 for use in girls and women ages 9-26 to prevent four high-risk strains of HPV.
The FDA in 2009 expanded the license for use in males ages 9-26 for the prevention of genital warts and in 2011, the CDC’s Advisory Committee on Immunization Practices recommended it for routine use in boys.
In 2014, the FDA approved Gardasil 9, designed to protect against 9 HPV strains, for use in the prevention of HPV-related cervical, vaginal and vulvar cancers in females and HPV-related anogenital lesions and anal cancers in males and females.
The FDA also expanded the age range of potential HPV vaccines to males and females between the ages of 9 and 45.
Early marketing strategies focused on promoting the drug as guarding against HPV, a sexually transmitted disease. But in 2016, as vaccination rates lagged, the CDC recommended that doctors stress the HPV vaccine’s cancer-prevention benefits, rather than talking about STDs as a way to get more parents to vaccinate younger kids.
And in 2020, it added oropharyngeal and other head and neck cancers to the list.
Over the last several years, HHS has invested tens of millions of dollars in research to get U.S. HPV vaccine uptake numbers to HHS’ “healthy people” target rates of 80% of children and teens vaccinated by 2030.
Meanwhile, Merck has expanded its ad campaigns beyond teenagers to target parents of young children and adults.
In 2020, the WHO set a goal of vaccinating 90% of teenage girls by 2030. Gavi, the Vaccine Alliance, is currently launching a series of campaigns to vaccinate tens of millions of girls in Africa, following similar campaigns in India and Indonesia.
Last week Merck announced its third-quarter earnings from Gardasil were up 13% to $2.9 billion. Allied Market Research predicts the global HPV vaccine market — in which Merck is the primary player, although GSK also markets its Cervarix outside of the U.S. — will grow to $10.8 billion.
Brenda Baletti Ph.D. is a reporter for The Defender. She wrote and taught about capitalism and politics for 10 years in the writing program at Duke University. She holds a Ph.D. in human geography from the University of North Carolina at Chapel Hill and a master’s from the University of Texas at Austin.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Grooming our children, Part 1: Getting parents out of the picture
By Belinda Brown | TCW Defending Freedom | November 2, 2023
Are parents aware of what children from four years old are being taught about sex in our schools? Belinda Brown thinks not. In a series of articles she makes the case that, with the agreement of the Department for Education, our children are being exposed to what is tantamount to a national grooming programme. The first step of this successful sex educators’ coup, she explains today, was to get parents out of the picture, to take over their role, and then deny them any access to lessons. Miriam Cates is one MP who is fighting back.
IN JUNE Conservative MP Miriam Cates introduced the ‘sex education transparency’ Private Members’ Bill, putting Rishi Sunak under pressure to give schools a legal duty to publish materials used in sex education lessons. Backed by 70 Conservative MPs, the aim of the Bill is to secure parents’ rights to see their children’s Relationships and Sex Education (RSE) lesson plans: rights which parents thought they had, only to find them being denied.
Cates had already called for an urgent Government review into what was being taught in RSE since this programme was rolled out in September 2020, of such concern were the materials and lessons parents gleaned from their children. RSE, it emerged, was the brainchild of the ‘progressive’ independent Sex Education Forum, a busy organisation with a stipend of £200,000 a year and a clear ‘beyond biology’ agenda. The Prime Minister responded to Cates’s call and ordered the review last March. Unaccountably, his Secretary of State for Education, Gillian Keegan, refused to publish the findings and has no plans to do so. Why, we do not know. MPs had claimed the Department for Education’s (DfE) most recent relationships and sex education guidance, produced in 2019 in consultation with the LGBT+ charity Stonewall, had allowed ‘activist groups’ to overly influence teaching materials. The guidance does not set age limits on what can be taught.
In the meanwhile, the position of parents has not changed. One story catalysed Cates’s most recent initiative. Two years ago, Clare Page found out that her daughter had been taught at school that ‘heteronormativity’ (preferring the opposite sex) was a bad thing and had been told that she should be ‘sex positive’. Like any decent mother, she wanted to know more. Her request to see the material used in her daughter’s classroom was turned down, first by the Information Commissioner’s Office and then by a first-tier tribunal. She was not even allowed to find out whether her daughter had been taught by the ‘master fetish trainer’ who worked for the School of Sexuality Education (SSE) employed by her daughter’s school.
Page’s case marks another step in the long march through the institutions whereby parents are being excluded from once personal and family-based aspects of their children’s upbringing, now inappropriately and dangerously taken over by schools.
Her experience is far from exceptional. In Wales, where children are being exposed to a mandatory diet of explicit and highly ideological sex education, parents are not allowed to remove their children from these classes. Attempts to do so are repeatedly turned down.
Likewise, parents such as those trying to protect their children from sexual extremism in the London Borough of Redbridge are portrayed as religious fundamentalists and radical homophobic Islamists.
Some schools and local authorities even have a policy of not informing parents when a child expresses what the school categorises as ‘feelings of gender distress,’ a study found, though this flies in the face of safeguarding rules. More recent research indicates that it could be that the school’s teaching that is the source of distress.
In theory, parents do have rights in law. Under the European Convention of Human Rights, ‘the State shall respect the right of parents to ensure such education and teaching is in conformity with their own religious and philosophical convictions’. The 2002 Education Act Guidance repeatedly emphasises the role of parents. ‘Teaching must be done with respect to the backgrounds and beliefs of pupils and parents . . . All schools should work closely with parents when planning and delivering these subjects. Schools should ensure that parents know what will be taught and when, and clearly communicate the fact.’
Yet this is not happening. Any criticism that teaching places insufficient emphasis on the value of traditional marriage between a man and a woman, for example, is ignored.
When the School of Sexuality Education complained that the Department of Education’s guidance gave ‘problematic credence’ to long-term relationships and marriage, they had the government’s ear (p10). These sex education activists ‘provide in-school workshops on consent, sexual health, porn and positive relationships’. Their approach, they say, is rights-based – whose rights they do not say. They proclaim themselves as ‘sex-positive, non-binary and trauma informed’.
When they criticised the guidance section that suggested that primary schools should only teach pupils about LGBT when it was ‘age appropriate’ rather than from reception, these phrases were obligingly removed by the DfE.
Gillian Keegan should ask herself who these sex education providers are and why they want the material they are pushing at our children to be unrestricted by age.
This contempt for parents was expressed early on in an ‘Educate and Celebrate’ guidebook foisted on schools. Their proposal was that rather than get parents’ permission for children to attend LGBT events, they would organise LGBT events in the school (p24). When parents tried to protect their children from all this, they were told they were breaking the law.
The result of the government’s inadequate guidance, Cates says, is ‘a permission slip for teaching almost anything that is loosely associated with gender, sexuality or sexual practice – often with an assumption of the earlier, the better’ (p71).
Without providing any apparent curriculum, and without parents able to monitor what was being taught, these so-called specialist sex ‘educators’, heavily funded by the government, with clearly articulated curricula and political agendas, have zealously filled the gap.
Foremost of these is the ideology of queer theory that asserts that ‘heteronormativity’ – the natural biological sex preference for the opposite sex, should be ‘smashed’. It rejects all ‘binaries’ including distinctions between homosexuality and heterosexuality, male and female, and even more disturbingly, between adult and child.
This is the ideology that’s the foundation of the RSE curriculum that a Conservative government has sanctioned. It will be explored in greater depth in the rest of the series. Parents have a right to know, reject it and protest.
To be continued.
How Long Has Netanyahu Got Left?
By Martin Jay | Strategic Culture Foundation | November 2, 2023
Is Israel really losing the media war? In a conflict where the truth seems to be the first and most predominant casualty, this might be the only truth, certainly when we look at recent events. The war in Gaza is not an irony-free zone though. Recently, Israel stormed social media with claims that the Palestinians were faking videos and they took one of a medic giving resuscitation to a victim, claiming that the technique was erroneous, and so, therefore, the video must have been faked. How are we to take this? Given that Israel is the expert on faking videos to support its heinous war crimes, was the logic behind the claims “trust us, we know what we’re talking about when we talk about faked videos”? In either case it failed. The mob justice of social media didn’t give any gravitas to the claims and soon enough the Red Cross said that the health worker was using the right technique.
But how interesting that Israel is now resorting to this level, to stoop so low makes many wonder if they are even close to winning the war. It doesn’t smack of a victorious side to do this and there are other examples, even, previously. When the Baptist hospital was bombed, the IDF didn’t seem bothered that there was documented evidence to prove that it had actually warned the bosses of it, that they, the IDF, were about to bomb it. Almost as soon as it was bombed and Israel fed the revolting swine of western journalists feeding from the teat of mother Israel for all of their information with the assertion that the Palestinians actually blew it up themselves by a faulty rocket which Hamas had just recently fired close to the hospital. The IDF even produced audio of a conversation which apparently confirmed this. The problem with this though was that the audio was faked. There is actually a history of the IDF faking audio conversations. Some will remember the 2010 storming of the Turkish aid boat where the IDF murdered in cold blood ten activists at point blank range. Audio tape of the activists insulting Israel’s special forces soldiers turned out to be fake.
Western media are playing a role in helping Israel though simply by accepting the carefully arranged circus that they have been invited into. No western journalists that I can see are working within Gaza as it’s simply too dangerous so they are forced to lap up the information which is handed to them on a plate standing on the touchlines and being really nothing more than a spectator to a secret war which they can’t and won’t understand. The holocaust which is taking place is about the annihilation of the Palestinians in Gaza. We can’t really call it a war as this would suggest that both sides have a fair chance to compete on a level playing field. In Gaza, the Israelis are starving the Palestinians so that even if they survive, they will be too weak to fight when, or if, the IDF finally go in with their tank divisions.
The story which isn’t being reported by western journalists is how Hamas is already having some victories in hitting tanks with RPGs and how phosphorous is being dropped on civilians. Of course Netanyahu has been promised by the Biden administration that he can break every war crime ever recorded with the knowledge that he and his people will never face any legal action. And this is really a big part of America’s support to Netanyahu as what we are witnessing – but are unable to film due to Israel cutting off electricity and internet – are war crimes which we have never really seen before in the last 100 years except with the holocaust itself during WWII.
The total ethnic cleansing of the Palestinians which will never be reported as such by British journalists, which citizens of the free world cannot actually see, so it will continue until only a few hundred thousand Palestinians remain, who then will be convinced by Israel and the West to move onto another location. In fact, there is documentation to prove that the Israelis were planning all along to move out Palestinian citizens out of Gaza all together with the assistance of Egypt.
The big question is time. Time is really an important component in this war. It is only a matter of time before Biden messes up and is drawn into a war with Israel against Iran. Biden doesn’t want this but he is unfortunately stupid and weak and Netanyahu likes American presidents this way. A looming speech from Hezbollah’s secretary general Hassan Nasrallah is expected to give an ultimatum to Israel to stop the mass murder of Palestinians, we will soon be reminded who are the most important players: Iran and Turkey.
Both these countries, although from different Muslim faiths who, in other parts of the Middle East are killing each other, seem to be united in their defiance of Israel. It is no longer a question of if they will react to the Gaza holocaust but when. Biden is out of his depth and the Iranians know this. He has only one real ace to play, which is to get rid of Netanyahu which if he was any other U.S. president, he could probably pull this off. But this is Biden we’re talking about whose foreign policy sheet includes the hugely embarrassing exit from Afghanistan and the 130 billion dollar colossal waste of sending cash to Ukraine, the most corrupt country in the world, which most Americans can’t even find on a map of Europe.
The rumours are that Biden is thinking in the longer term than Israel and that he believes that Netanyahu doesn’t have long in office as many Israelis don’t support his war crimes strategy, a point made by Haaretz recently which pointed out his demise was not long off. Something’s got to give. The servile, revolting, passive international press pack might be all that Netanyahu has left.
“Shedding” of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated – Part 1
It’s happening. The manufacturers and regulators knew it was a risk, yet, like numerous aspects of the Covid vaccine mRNA technology, did not test for excretion potential of spike proteins or LNP’s.
Pierre Kory’s Medical Musings | November 1, 2023
Awareness of the Federal Regulators and Vaccine Manufacturers
The data showing the toxicity and lethality of the vaccines started within weeks of the roll-out with hundreds of thousands of adverse events and hundreds of deaths reported to VAERS in January of 2021, far exceeding previous stopping points of any new medical product or vaccine.
Although ignored (to this day), anyone paying unbiased attention could see a further mountain of evidence develop, including a skyrocketing number of newspaper and television reports of healthy athletes and young people arresting and dying while doing normal everyday activities or sports (countered by corporate/government controlled media with a plethora of fact checking articles using cherry picked data to inform the world that what they are seeing is not factually true).
Then life insurance industry data emerged showing historically unprecedented rises in death claims being paid out amongst the healthiest sectors of society temporally associated with the proliferation of Covid mRNA vaccine mandates within schools, corporations, universities, health care institutions, federal contractors etc. Most telling of the deathly impact of mandates was the fact that the largest increases among the sudden, rapid rises in excess deaths occurred among employed white collar workers.
The reality is that these data are still ignored by media and public health agencies across the world. Even more worrying are the more recent reports finding universal contamination of every studied vaccine vial with large magnitude, excess levels of DNA fragments and DNA plasmids. Then the discovery that the DNA plasmids used in the manufacturing process contained genetic sequences that both promote DNA integration into the human genome as well as promote the development of cancer.
It truly is unimaginable that we now must consider the risks (and reality) of “shedding” of the vaccine products from the vaccinated to the unvaccinated. This now has implications for nearly every human being walking the earth, vaccinated or unvaccinated (including me).
This series will explore the regulatory, scientific, epidemiological, and clinical data indicating that shedding is occurring. The health of who knows how many is now being threatened, with the extent of the risks likely both highly variable and difficult to predict, both in the short term and long term. That is unless we start to seriously study the phenomenon further. So, let’s review what is known.
Within 3 months of the rollout of the global Covid mRNA vaccination campaign, I was consulted by two different unvaccinated women in their late 30’s and early 40’s respectively, who reported that they were suffering acute menstrual abnormalities in the days following close exposure to a recently vaccinated practitioner (one visited a massage therapist and another an acupuncturist). Both had a history of highly regular, uncomplicated menstrual cycles over decades.
Since that time, at least twenty other unvaccinated and vaccinated people, both men and women, have reported to me compelling histories of typical post-mRNA vaccine adverse effects subsequent to close exposure to vaccinated family members, contacts, or friends.
Further, my partner Scott Marsland at our Leading Edge Clinic, who also specializes in treating Long Covid/Long Vax syndromes, has a growing series of detailed case histories of similar “shedding” events occurring. I will revisit this in a later post in this series, but I will briefly say here that our clinical observations conclude that symptomatic shedding events do occur. However, we have little idea of exactly how common it is occurring among the general population.
This is further complicated by the fact that even if it were occurring frequently, the vast majority of people suddenly developing typical vaccine side effects symptoms after exposure to a vaccinated person would never think to relate it to exposure to shed vaccine products. It is my belief that very few people in the general public are aware of the possibility it could occur. You know, because the regulators have assured the country that mRNA technology is “safe and effective.”
However, my general sense is that it occurs largely in people who have increased physiologic sensitivity to environmental exposures, toxins, or pharmaceuticals and that it is generally transmitted by someone recently vaccinated or someone who is producing a lot of spike protein. Note that is my “general sense.” More studies are required to fully understand both the frequency of and physiologic impacts from such events.
My ignorance as to the frequency of symptomatic shedding events is due to the fact that the concept of transmitting spike proteins (or lipid nanoparticles) from a Covid mRNA vaccinated person to another is one of the least studied and published-on aspect of the mRNA vaccine technology.
What is so shocking about that lack of research (actually nothing is shocking anymore) is that shedding has major global implications. Apparently it is not just me who thinks this because, as an expert on several aspects of Covid, I have been lecturing across the U.S, Europe, and South America in conferences, Parliamentary hearings, or invited lectures. Questions about shedding appear everywhere (in the dozens of Q & A’s that I have participated in, it is nearly always the first question. It is also a very common topic in the chat of our FLCCC weekly webinar.
Know that in this tonight’s FLCCC webinar, I will present a 15-20 minute overview of this series along with my private practice partner Scott Marsland. We expect to be deluged with questions after.
Anyway, I believe that by the end of this series on the science, epidemiology, and clinical observations of shedding, you will be convinced that it can and does occur.
From our Federal government, in this FDA document, the term “shedding” is defined as:
“The release of viral or bacterial gene therapy products from the patient by any or all of the following routes: feces (feces); secretions (urine, saliva, nasopharyngeal fluids, etc.); or through the skin (pustules, lesions, sores).”
They forgot to mention “exhaled breath.” More on that later. The “products” they refer to that can be transmitted from a Covid vaccinated person to another include not only the genetically programmed spike protein product, but also the lipid nanoparticle (LNP) containing the mRNA that is in the injections as well as naked mRNA that can be released from the LNP. Even more worrying is the recent shocking discovery that every single Moderna and Pfizer vaccine vial is contaminated with high levels of DNA plasmids potentially capable of integrating into the human genome. Contemplating that last one is disturbing, the implications of which we will not know for some time.
First off, let’s be clear that the Covid mRNA and DNA vaccines are gene therapy medicinal products (GMTPs or GTP’s) as stated in the FDA’s 2015 document on Gene Product Shedding Studies.
“Gene therapy products are all products that mediate their effects by transcription and/or translation of transferred genetic material and/or by integrating into the host genome and that are administered as nucleic acids, viruses, or genetically engineered microorganisms.
Also note that in this European Medicines Agency (EMA) document, the mRNA vaccines also meet their definition of gene therapy medicinal products (GMTP’s).
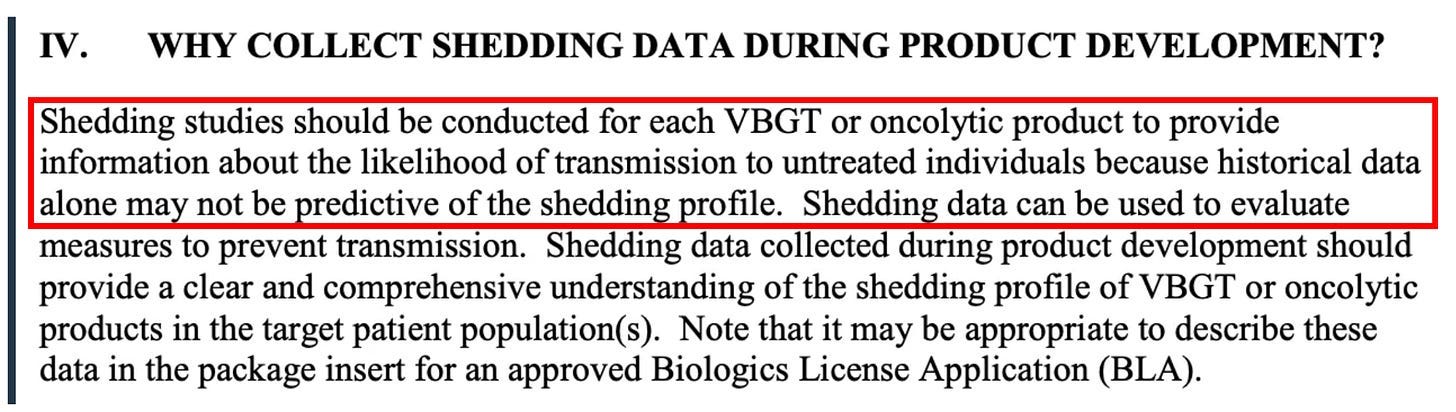
Ok, now that we know what a gene therapy product is and that the Covid mRNA injection is actually a form of gene therapy (marketed to the public as a “vaccine”), what does that have to do with “shedding?” Again from the FDA document regarding the evaluation of the safety of gene therapy products, they emphasize the importance of studying shedding:
Shedding is distinct from biodistribution because the latter describes how a product is spread within the patient’s body from the site of administration while the former describes how it is excreted or released from the patient’s body. Shedding raises the possibility of transmission of virus or bacteria based gene therapy products (VBGT) from treated to untreated individuals (e.g., close contacts and health care professionals).
This guidance represents FDA’s current thinking on how and when shedding data should be collected for VBGT and oncolytic products during preclinical and clinical development and how shedding data can be used to assess the potential for transmission to untreated individuals.
So, with these findings in mind, it may be no wonder why the FDA insists on shedding studies:
Further on in the document, the FDA again emphasizes the importance of shedding studies:
Note that the FDA emphasizes the importance of doing human shedding studies and not just relying on animal studies:
To inform the design of human shedding studies, shedding data may be collected in animals following administration of the VBGT or oncolytic product. These data can help estimate the likelihood and potential shedding profile in humans, particularly when there is concern about transmission to untreated individuals. However, such data cannot substitute for human shedding studies for several reasons.
But again, no studies testing whether excretion of mRNA-containing LNPs, modified spike-encoding mRNA, or spike produced by vaccinated people have been done. Well, I shouldn’t say none, because in this paper the author cites a Pfizer document obtained by FOIA which apparently revealed that shedding was studied in the urine and feces of intra-muscular injected rats. Unfortunately, that document is no longer at the website referenced.
To summarize from the above, the FDA’s position is that:
- the mRNA vaccines are gene therapy products
- Gene therapy products require shedding studies in both animals and humans
- Gene therapy product shedding raises the possibility of transmission from treated to untreated individuals
Note that much of the rest of this series of posts on shedding is guided by a masterful comprehensive review of the topic of gene therapy product shedding by independent researcher (by definition) Helene Banoun in Infectious Diseases Research. Hers is one of the only papers I could find that attempted to meticulously explore what is known about shedding of the mRNA gene therapy vaccines.
As already stated, an important point Banoun makes is:
There was no regulation of mRNA clinical trials prior to RNA vaccines, yet there is strict regulation of gene therapy products. It is difficult to justify that mRNA vaccines are not considered in the same way as gene therapies regarding this regulation; indeed the only difference is that they are (historically) supposed to protect against a disease and not cure it. Gene therapies are intended for a small number of people in poor health, whereas vaccines are used on a large scale on healthy people: it would therefore be wise to apply stricter rules to them.
She further points out another omission of the regulatory process:
Any experiment involving the deliberate transfer of a nucleic acid to a human must be preceded by Institutional Biosafety Committee approval (document on the regulatory standards is here), but approval was not given because of the emergency clearance given to mRNA vaccines.
Therefore, according to both the American and European agencies, mRNA vaccines are gene therapy products and should have been subjected to excretion studies of all secreted fluids (urine, exhaled droplets, saliva, sputum, nasopharyngeal fluids, semen, breast milk, feces, and sweat). Again, these studies were not done for mRNA vaccines nor for the DNA adenovirus vaccine (J&J).
So, where are the clinical human shedding studies? Well, I just learned of one that is about to be published (next ten days?) where the research team exposed a population of unvaccinated women to vaccinated individuals and their assessment outcome was the development of menstrual abnormalities. I know the results but want to respect the research teams right to present their original work. They have promised to share their manuscript with me and Paul Marik as soon as the peer-review and acceptance process is complete. I have no idea what journal they submitted to but I can be highly confident it is not the New England Journal of Medicine.
The entire reason why I did a “deep dive” into shedding science is because shedding was not studied when it absolutely should have been and I believe with near certainty that it occurs. Note my use of “near certain” is only to seem objective but it really is too late for that – both my partner Scott and I have diagnosed and successfully treated a number of shedding “victims.”
The lack of shedding studies prior to the mRNA rollout was, in my opinion, an insanely reckless and irresponsible omission (or willfully criminal, take your pick). As an evolving expert in the evaluation and treatment of Covid mRNA vaccine injury syndromes, I and others have identified the spike protein as the main component responsible for not only the pathogenicity of Covid but also of the vaccines, with this review paper proposing a new field named “spikeopathy” (study of the disease processes triggered by the spike protein).
If vaccine transcribed spike protein can be transmitted in sufficient quantity from vaccinated folks to unvaccinated ones, it stands to reason that adverse effects of the vaccine can develop in some unvaccinated people who came into contact (or close proximity) with vaccinated people. How did they get away with not studying this possibility?
An easy answer is they were doing science at “warp speed.” The more uncomfortable answer is that the “vaccines”, although meeting the definition of a gene therapy product, were actually not even legally considered a medical product at all and thus did not require a diverse range of safety studies (like on genotoxicity, reproductive risks, excretion potential etc). What? Why? How?
The reality is that the Covid vaccines, as a result of successive federal legislative actions which evolved over decades, was legally categorized as a “countermeasure” under a “public health emergency.” Such “countermeasures” require no specific regulatory approval process prior to dissemination. All a countermeasure needs is the recommendation of the Secretary of Health and Human Services that “it may be effective.”
This is the conclusion derived from the legal investigatory work of various independent and legal experts and researchers like Catherine Watts, Todd Callender, and Sasha Latypova. If interested in learning more, I would watch this lecture by Sasha Latypova (scroll down the page to find her lecture). As they have uncovered, “countermeasures” (even gene therapy ones) do not legally require studies of excretion potential, bio-distribution, pharmacokinetics, genotoxicity, insertional mutagenesis etc.
They don’t even require FDA regulated clinical trials of efficacy or safety.
So why did Pfizer and Moderna even do the efficacy trials? Latypova maintains that they did this not only to satisfy the public’s confidence to increase vaccine uptake, but also to “fool” the public into thinking these vaccines were medical products subject to standard (albeit accelerated) pharmaceutical product regulatory processes.
This obscured the reality that they were instead classified as military “countermeasures” against a perceived (if not actual) bioweapon. To wit, the COO of Operation Warp Speed was a General from the Department of Defense (DOD) and the vaccine manufacturers were under contract with the DOD to produce the countermeasure, sometimes referred to as a “demonstration (demo)” and/or a “prototype” in numerous legal documents they uncovered.
Anyway, as a result of this lack of a legal requirement to fully study these products in a public health emergency, the list and types of studies that should have been conducted (but were not) is long. Researchers and clinicians have been screaming about this since they were rolled out. These cries were met with a deafening silence by governmental health agencies across the world.
I know, it is a lot to take in.
But the latest “word on the street” is that the finance and insurance industries may finally be waking up to this fraud and its devastating impacts on U.S disability and death rates. Knowledge of these society-wide impacts largely results from the work of two different research teams led by former Blackrock portfolio manager Ed Dowd and insurance industry consultant Josh Stirling).
This article describes the reasons why Pfizer and Moderna stock are crashing of late. Put more succinctly, from what I hear it is due to the hedge fund guys shorting their stock. I believe Pfizer is in even deeper trouble now that this “forensic” paper just got published finding that they hid vaccine trial deaths which obscured a 3.7 fold increased risk of cardiac death in the vaccinated arm of their trial.
“Shedding” Part 1– Shedding of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated – Part 1
“Shedding” Part 2 – The Bio-Distribution and Excretion Potential of Covid mRNA Vaccine Products
“Shedding” Part 3 – Can You Absorb Lipid Nanoparticles From Being Exposed To a Vaccinated Person?
“Shedding” Part 4 – Evidence of Placental and Breast Milk Transmission of Covid mRNA Vaccine Components
“Shedding” Part 5 – Evidence of Shedding Causing Illness In Others
“Shedding Part 6– Clinical Case Notes Describing Shedding Phenomena Among Leading Edge Clinic Patients
“Shedding” Part 7 – Shedding Via Sexual Intercourse – Clinical Reports
Why a global anti-Hamas coalition pushed by Macron is a bad idea
By Rachel Marsden | RT | November 2, 2023
Last week, standing beside Israeli Prime Minister Benjamin Netanyahu during a visit to Jerusalem, French President Emmanuel Macron suggested recycling the global coalition of 86 nations against Islamic State (IS, formerly ISIS) to focus on Hamas.
“Hamas is a terrorist group, whose objective is the destruction of the state of Israel. This is also the case of ISIS, of Al-Qaeda, of all those associated with them, either by actions or by intentions,” Macron said, betraying a short and selective memory. The stated goal of IS wasn’t to eradicate Israel – it was to establish a caliphate in Syria and Iraq, then broaden it into Arab countries. IS was first and foremost a threat to the stability of Syria – the same country whose government the US and its Western allies actively hindered in its fight against terrorism by making a failed attempt at overthrowing President Bashar Assad through Pentagon and CIA-backed training and equipping of “Syrian rebel” jihadists. As for Al-Qaeda, Israel was even reportedly at one point helping treat wounded militants from the group who were fighting their common enemy, the Iranian-backed Hezbollah, in Syria – in turn effectively hindering the fight against IS, as Syria and Hezbollah worked to destroy it.
The Global Coalition against Daesh (another name for IS), founded in 2014, explicitly excluded Russia, whose invitation by Damascus to help it eradicate the terrorist threat can be largely credited for Syria’s stabilization, and the fact that it’s rare to even hear any talk of IS anymore. Russia’s involvement in neutralizing the terrorist group, coupled with former US President Donald Trump’s refusal to continue funding Washington’s incursion into Syria, beyond hunkering down in the oil-rich Kurdish part, was the ultimate key to IS’ defeat. So with apparently little left for it to do now, Macron recommends that the coalition that mostly sat and watched – while Russia, Iran, and Syria did the heavy lifting – take on Hamas. Who does he think is going to do the work this time? Russia, which is still excluded from the coalition? Syria, which has recently taken incoming missile fire from Israel? Iran’s Hezbollah allies, who lost 1,000 men fighting IS in Syria – and whom Netanyahu has placed in the same basket as Hamas as an enemy of Israel? Good luck with that.
So with the most effective anti-IS fighters excluded from fighting Hamas, who’s left in Macron’s proposed coalition? There’s the Global South, including some African countries that just kicked out French troops for their own failed counterterrorism missions which had led to multiple coups and the flourishing of jihadism. It’s doubtful these nations will now be keen to embark on yet another counterterrorism mission alongside the same forces that they just expelled.
Then there are all those members of the international community who are quietly thinking what United Nations Secretary General Antonio Guterres dared to say aloud last week – that Hamas’ brutal attack on October 7, which left close to a thousand civilians and hundreds of military and security personnel dead, “did not happen in a vacuum.” He was, of course, hinting at Israel’s longstanding, UN-recognized oppression of civilians in Gaza. His statement begs yet another question: Is Hamas really a global threat? Or is it just Israel’s problem?
Anti-Israel unrest has reverberated outside of the immediate conflict zone, including in Western Europe and the US, but these protests have nothing to do with Hamas. Instead, citizens elsewhere in the world are merely reacting to perceived injustices, particularly in light of what they consider to be an overwhelmingly pro-Israel bias on the part of the Western establishment, which initially and drastically minimized concerns over the protection of Palestinian civilians. So any global action against Hamas seems futile.
The anti-IS coalition targeted the terror group’s propaganda, with its website stating that IS’ “use of social media tied to acts of terrorism is well-documented. In response, Coalition partners are working together to expose the falsehoods that lie at the heart” of its ideology. They’re free to do that, but why bother when there’s already open debate among those who have the opportunity to see reports from the ground and assess the situation for themselves? Governments can’t be trusted not to promote their own propaganda under the guise of combating it – all to secure an advantage for their preferred narrative.
Just consider the recent example of propaganda emitted by one of the self-styled gatekeepers of truth: European Commission President Ursula von der Leyen. “Russia and Hamas are alike… their essence is the same,” she said. Nah, actually they aren’t the same at all. And not even Israel has been saying that, but still, “Vladimir Putin wants to wipe Ukraine from the map. Hamas, supported by Iran, wants to wipe Israel from the map,” von der Leyen explained. Besides the hot take on Putin’s intentions regarding Ukraine, that’s like saying that since Warren Buffet has a bank account, and I have a bank account, then I’m also a billionaire. This is exactly the kind of nonsense that Western anti-propaganda campaigns end up spewing.
The anti-IS coalition was made to tackle IS. If that’s no longer an issue, then just toss it in the trash. How many interventionist entities does the West need to spearhead, anyway? There are already more than enough vehicles and coordination mechanisms for intelligence sharing, propagandizing, and security operations. Besides, there’s no proof that better intelligence could have helped Israel when Egyptian and American officials have claimed that Netanyahu had warning of the impending Hamas attack. About the only thing that more useless Western-led bureaucracy would help is the West’s own hunger for more of it.
Rachel Marsden is a columnist, political strategist, and host of independently produced talk-shows in French and English.
As the German Health Ministry drowns in millions of unwanted vaccine doses, Karl Lauterbach begs Germans to please, please line up for their fifth jab

eugyppius: a plague chronicle | November 1, 2023
From the erstwhile vaccine propagandists at Der Spiegel, who I think are also tiring of the insipid autumnal vaccination liturgy and its noxious political enablers:
Federal Health Minister Karl Lauterbach has again called on people to get a booster vaccination. “Despite the pandemic and awareness campaigns, the importance of the Covid booster is apparently greatly underestimated,” he tells Spiegel. “So far, unfortunately, only a fraction of those for whom it is recommended have had a booster vaccination.” He calls on all at-risk groups and older people to catch up and ideally combine it with a flu vaccination.
According to the vaccine uptake statistics of the Robert Koch Institute, only about 2.5 million people have received three or more boosters. This means that only a fraction of those over 60 are likely to have sufficient protection against Covid …
They let Lauterbach flap his gums a little more about population immunity, Long Covid, secondary infections and how the vaccines can make all this better because reasons, before sticking the knife in him:
Lauterbach urgently needs to boost vaccine uptake. The pharmaceutical contracts concluded under his predecessor Jens Spahn have secured much larger quantities of vaccine than are currently being used. Between September and November, about 14.1 million vaccine doses of monovalent vaccine targeted at XBB 1.5. will be delivered. An additional 10.6 million vaccine doses of Novavax XBB 1.5. vaccines will also become available, as soon as they are approved by the European Commission.
Our dissolute snake oil salesmen – who is either so stupid or so desperate that he actually tweeted a link to this not-so-subtle takedown – is currently sitting on 11.5 million Pfizer/BioNTech doses, trembling at the prospect of Novavax dropping another 10 million on his head, with no hope at all that more than 5 million Germans will ever line up for these worthless products. This is despite the best efforts of the regional press, who have been trying to gaslight their elderly readers into getting yet another jab since September. Today the Main Post published a typical piece, claiming that vaccine demand is starting to creep up now, really it is; while yesterday it was the turn of Münchner Merkur to claim that everyone is talking about the shiny new vaccines and to drag in some pulmonologist to talk about the “predominantly positive reception” they’ve enjoyed.
Dear idiot reporters: The official vaccine dashboards may be down, but the RKI still publish day-by-day uptake statistics. Stop lying.
Who keeps spreading the real disinformation?
ANSWER: The government (and its many cronies)

BY BILL RICE, JR. | OCTOBER 31, 2023
Independent journalists Glenn Greenwald and Matt Taibbi recently had a conversation where they highlight a key point of our New Normal times – namely, that all real disinformation comes from government or mainstream media sources.
It occurs to me that our side needs to keep pounding home this point, which might resonate with enough citizens to make the proverbial difference.
What leaders on our side need to do is repeatedly point out that the real disinformation is coming from authorities and “experts.” If enough people accept this truism, the disinformation spreaders might encounter formidable obstacles as they attempt to enforce the rest of their freedom-eradicating agendas.
I’d start by simply pointing out all the allegedly true information promulgated by officials that was really false information.
Just with the categories of “settled Covid science,” most citizens in the world would probably acknowledge they’ve been sold a fraudulent bill of goods.
For example, how many adults really think the Covid “vaccines” and “boosters” prevent infections or stop or slow virus spread?
My guess: There might be 125 (?) people in world who still believe this official disinformation.
Also, if everyone was given a powerful dose of truth serum, I think everyone would admit that they know at least a few people who might have been harmed (or even died) because they received a Covid shot. So the narrative that the “vaccines” are safe or prevent “severe cases” is not really accepted by most people.
Quick thought exercise: If every person did believe the “vaccines” are safe and effective and this virus was a real threat to their health, every person would be getting the latest round of new boosters … instead of maybe five percent of the population. This means 95 percent of citizens are showing their true beliefs by what they are not doing.
This is what one might call a truth “tell.”
It would be interesting if some well-known polling organization surveyed people and simply asked a large sample of citizens two questions:
Question 1: Do you think the Covid vaccines are “effective” at preventing new cases?
Question 2: Have you heard or read about any person who might have suffered a vaccine injury?
I just proposed two common-sense poll questions I know will never be asked by important polling organizations – because I know that every important organization is now captured. (“Every important organization” would include the important public opinion polling organizations.)
This example illustrates how it’s almost impossible to prove that the government and its many cronies are trading in disinformation – because all the exercises that might prove this won’t occur.
I’ve written a thousand times that officials won’t investigate that which they don’t want to confirm. Simple opinion polls would be one example of a truth-seeking tool that can never be employed in our New Normal.
Funding and authorizing a large number of autopsies of all the people who “died suddenly” is another example of taboo investigations.
Yet another example would be all the people who have contacted mainstream media news organizations and told editors or journalists that a loved one died or was severely injured by a vaccine.
Question: How many mainstream journalists followed up on these news tips?
I’m pretty sure the answer is zero. I would also be willing to bet that every news organization in the word has received numerous news tips like this … so this is not some random, outlier anecdote.
Not only have no real investigations of vaccine injuries been performed by the so-called “watchdog” press, the public doesn’t even know how many times these requests have been ignored and dismissed.
The reason I think the public might belatedly accept the truism that it’s officials who spread disinformation is that, by now, many members of the public understand that official narratives of the past have been debunked.
Matt and Glenn discussed one the best-known examples of bogus government-spread disinformation when they discussed the justification for America’s invasion of Iraq. The main justification was, of course, that Saddam Hussein possessed “weapons of mass destruction.”
I’m sure some people still believe this, but I would guess at least 75 percent of thinking citizens now realize this was a lie.
The good news is that many people who supported the invasion of Iraq later came to believe that Iraq didn’t have such weapons and came to believe that American citizens shouldn’t have been stressed out over an impending attack from Iraq.
My take-away, which is very germane to discussions of our Covid times, is that some lies do later get exposed as lies. People are willing to admit they no longer believe the official narrative.
Whether they know it or not, these people are admitting that they were duped by sophisticated disinformation campaigns … and the disinformation didn’t come from kooks on the Internet – it came from the “leaders” of the important organizations in the country.
The “War on Terror” had several components, including several accepted storylines which should now be viewed as dubious disinformation.
One of these storylines is that terrorists were going to attack America with “bio-weapons,” which meant the government needed to spend billions of dollars investigating possible viruses and, most importantly, begin working preemptively on “vaccines” that would protect American citizens if and when such an attack occurred.
The terrorist attacks of 9-11 changed the world, but it might have been the anthrax letters which were mailed shortly after these attacks that changed the world even more.
The (almost-certain) disinformation at the time was that terrorists had mailed those anthrax spores.
The story that’s more likely to be true is that it was an American who mailed the anthrax (which actually doesn’t pose any great threat to the population). Also, the anthrax almost certainly came from a lab funded by American tax payers.
It didn’t really matter where the anthrax came from or who mailed it, all that mattered was that the “gain of function” research into deadly viruses proceeded at warp speed. Scientists researching possible bio-weapons received a blank check. Most significantly, the Science Industrial Complex merged with the Military Industrial Intelligence Complex.
Nobody (except maybe Ron Paul) would have guessed that 20 years later this strain of “disinformation” would lead to the whole world being locked down and then to mandatory mRNA vaccines.
It wasn’t Saddam Hussein who made sure we couldn’t go to church or could no longer go to any job deemed “non-essential.” The dictators issuing those orders worked in our own government … and were issuing orders based on their own disinformation.
The few brave contrarians who tried to warn the population what was really happening were labeled as traitors, the “enemy,” “science deniers” and disinformation spreaders.
Just like it was a coordinated effort to fool everyone into thinking Saddam Hussein was coming after grandma and our children with weapons of mass destruction, so too with the Mother of All Pandemics, which was entirely the product of government-produced disinformation.
In other words, the public shouldn’t need examples of Covid disinformation to realize the government’s been trading in disinformation for longer than most people have been alive.
And the reason the government and its partners trade in disinformation is because … this works.
If more people would just pause and use their brains, they’d probably realize it’s only an entity as powerful as the government (or the government’s shadow rulers) that can use disinformation to control the majority of the population.
Truth be told, a few contrarians on social media probably couldn’t turn the whole giant ship of state or even debunk a few bogus narratives.
However, if the arguments of these contrarians were persuasive enough, these contrarians’ points might spread to the masses.
This scenario no doubt identifies the real fear of our ruling class. To stop this possibility, the contrarians were labeled “disinformation” spreaders … by the very people and organizations who were spreading the real disinformation.
If a few more great communicators could simply point out who actually produces and then disseminates all the key disinformation, the world might have a fighting chance going forward.
What the world needs is some “Most Wanted” type posters that simply include the photos and job titles of the officials who are spreading the world’s important disinformation.
These posters would have to be humongous because they’d include photos of just about every key official in government and every editor and publisher of every mainstream media “news” organization.
The headline on this poster might say, “These are the people and organizations who are really spreading disinformation. These people have the means and the motives to spread dangerous disinformation. The public should quit trusting all of these people.”
I know such a project would be dangerous and wouldn’t even be “allowed” by the Censorship Industrial Complex. Still, somehow we’ve got to identify the real villains, who are the spreaders of the real disinformation.
On Being a “PreBunked Malinformant”
BY JOHN LEAKE | COURAGEOUS DISCOURSE | OCTOBER 31, 2023
In recent years a vast industry has been created for the “detection, management, and correction of disinformation and misinformation.” Dozens of foundations, big tech companies, and government agencies are now disbursing hundreds of millions (in aggregate) to university departments to train young people for a career in misinformation and disinformation management.
Dr. Aaron Kheriaty mentioned this to me in an interview last summer, and a few nights ago, Dr. McCullough asked me to do some research on this new industry. My inquiry has led me into a Bluebeard’s Castle of horrors.
A quick Google search of “misinformation correction” results in countless reports of grant awards in this burgeoning industry. In other words, instead of acquiring a liberal education (based on the central principle of freedom of speech and expression) an army of college students are in training to become professional censors and propagandists.
How do graduates from university censorship programs conceptualize guys like Dr. Peter McCullough and (to a lesser extent) me?
We are, in the Orwellian language of the censorship schools, “Malinformants”— that is, guys who spread “harmful” information. Because we have been designated as such, we are suitable candidates for “PreBunking.” The following video is a sort of “PreBunking” manual. Note that the technique is explicitly and favorably compared to a vaccine.

The telltales that you’ve become a “PreBunked Malinformant” is when you run afoul of internet trolls who display some or all of the following identifiers:
- Express a zealous belief that vaccines are the saviors and redeemers of mankind.
- Display an icon of the Ukrainian flag on their profile.
- Use extremely disparaging, ad hominem, and sanctimonious language.
- Characterize you of being a “grifter.”
So, how does it feel to be a “PreBunked Malinformant”? Setting aside the feeling of vexation that I’m contending with kids who possess none of my education or experience, I’m left with the emotion of total amazement that American universities now have astoundingly well-financed schools of censorship.
How could this have possibly come about in the United States of America?
Place where protests didn’t happen does support Israel
By Yves Engler | October 29, 2023
Apologists for Israeli crimes are constantly gaslighting Palestinians and their supporters. They seek to make those opposing violence and colonialism feel like oppressors.
Last Friday a rally was held in front of Deputy Prime Minister Christya Freeland’s office in Toronto. Freeland recently declared that “Canada stands with Israel” and when she was foreign minister said Canada would act as an “asset for Israel” on the United Nations Security Council.
The poster announcing the rally declared: “PROTEST DEPUTY PRIME MINISTER OF CANADA CHRYSTIA FREELAND OUTSIDE HER TORONTO OFFICE”. During the rally bodies of babies were placed in front of Freeland’s office and at some point a man with an Israeli flag went directly in front of Freeland’s office in a bid to provoke the protesters. There’s video of police intervening and standing in front of the building housing Freeland’s office.
As the rally grew, it reportedly spilled onto the street and intersection directly in front of the Miles Nadal Jewish Community Centre (MNJCC). According to a Canada Files post, someone came out of the community centre to complain and film the Palestine solidarity rally. Footage was later posted to X claiming a Jewish community centre was targeted by protesters. According to multiple comments online, the initial post was deleted after being bombarded with derisive comments about their inability to look at a map. But Canada United for Israel shared the video tweeting, “Targeting a Jewish community center where there is a kindergarten is pure antisemitism. How can the anti-Israel movement justify scaring children?”
Far right Rebel News founder Ezra Levant quote tweeted that statement claiming “Hamas protesters target a Jewish kindergarten” while the head of the ‘progressive’ media watchdog CanadaLand, Jesse Brown, made a similar claim. The incident was referenced by the Toronto Sun, Toronto Star, National Post and other media.
In a transparent bid to enable Israeli violence and colonialism, apartheid apologists regularly fabricate or distort events to claim victimhood. Over two decades I’ve been privy to repeated examples of this. While I no longer consider the tactic noteworthy, an element of the psychological side of it is. In other domains it would be called gaslighting.
In brief, those screaming loudest “it’s just a Jewish institution that has nothing to do with Israel” are generally best placed to know this is untrue. Those who’ve been through the MNJCC – and similar institutions – know they are deeply Zionistic.
MNJCC operates an “Israel Connection” program and promotes the United Jewish Appeal (UJA) Toronto’s annual Walk for Israel. It hosted and cosponsored an Israeli general’s talk, which was held in tandem with the Israeli consulate.
The Thomas & Marjorie Schwartz preschool centre & Junior Kindergarten housed there has three pictures posted on MNJCC’s site. In one the kindergartners are smiling with an Israeli and Canadian flag hanging on the wall. In its “core elements” the kindergarten describes “Israel as a Source and Resource”.
The MNJCC elementary school shows a picture with dozens of Israeli flags. On its Instragram the Paul Penna Downtown Jewish Day School (DJDS) recently posted that “Jewish people have always had and always will have a relationship with Israel. We continue to stand in solidarity with Israel.” Days into that country’s horrific siege and violence in Gaza, DJDS posted on October 13 that “classes created inspirational cards for Israeli soldiers, and sent cards full of well wishes to former classmates now living in Israel.” The MNJCC school’s site notes, “Each year, our school warmly welcomes two young Israelis to the Paul Penna DJDS community. We are delighted to partner with UJA Federation, the Downtown Jewish Community School, and The First Narayever Congregation on this fantastic initiative. These teens have completed high school and have chosen to defer their army service in order to become Israeli ambassadors or ‘shlichim’, spending a year focused on presenting contemporary Israel to our students in passionate, creative ways.”
MNJCC has deep ties to UJA Toronto, which brings young Israeli ‘shlichim’ to live with Toronto families so they can do outreach in schools and community organizations. At the top of UJA’s website, which is prominently linked on the MNJCC site, is an Israel financial appeal and its official advocacy arm is the Centre for Israel and Jewish Affairs.
Alongside a link to UJA Toronto, MNJCC’s site links prominently to the JCC Association of North America. The top of that site notes “JCCs of North America Stand With Israel”.
MNJCC’s namesake funded a major project at the racist Jewish National Fund’s Canada Park, which is built on the remnants of three Palestinian villages in the West Bank. On the board of the JCC, Miles Nidal is a staunch anti-Palestinian.
Even if the target of Friday’s protest had been the JCC it would be altogether legitimate (though considering the political climate, organizers should seek to detail the JCC’s anti-Palestinianism in promotional literature). No organization that promotes and defends Israel the way MNJCC does can then claim, “we are simply Jews, not backing Israel” when it becomes convenient to deny the connection.
It’s highly manipulative for individuals who know the Miles Nadal Jewish Community Centre is part of a network of anti-Palestinian institutions to claim protesting it is antisemitic. Call the complaints what they really are: gaslighting.
Featured Video

Language is a Weapon
or go to
Aletho News Archives – Video-Images
From the Archives
Aaron Siri’s Book: Vaccines, Amen
By Maryanne DemasiMaryanne Demasi | Brownstone Institute | June 15, 2026
For decades, vaccines have been treated as the sacred cow of modern medicine. I was taught that they were the holy grail. To question them was heresy. To raise concerns about safety was to risk professional exile.
Aaron Siri makes it clear in Vaccines, Amen: The Religion of Vaccines that the story we’ve been told about vaccine science rests far more on belief than proof.
“No child should be sacrificed on the altar of the religion of vaccines,” Siri writes, as he turns his focus to America’s overcrowded childhood immunisation schedule.
I assumed little in this book would surprise me. I’ve spent years reporting on drug safety, regulatory capture, and the corruption of science. But Siri showed me how wrong I was.
Siri is not a doctor or a scientist. He is an attorney, and this, he says, is his advantage. In court, rhetoric won’t save you. Evidence does. As he puts it, he doesn’t get to say “trust me” the way many doctors do. “I need to prove claims with real data.”
And he does. … continue
Blog Roll
 Aletho News
Aletho News- The UK Joins the Pirates
- Israeli government plans to fund extremist occupier group in occupied West Bank with $1.89M: Report
- Press TV reporter wounded in Israeli drone strike on southern Lebanon
- Time for Trump to Tell Benjamin Netanyahu to Go Away!
- Israeli officials: ‘Security zones’ to remain in Lebanon, Syria, Gaza
- Israel Fails to Sabotage Islamabad Accord… At Least for Now
- Araghchi: US Responsible for Implementing MoU with Iran
- US must cut military, intelligence assistance to Israel to protect Iran deal: Ex-Trump official
- The 12 Screenings That Manufacture the Patients They Claim to Find
- Iran deputy FM says MoU with US finalized, to be signed in Geneva on Friday
- If Americans Knew
- They Weren’t Convicted of Terrorism, But These Palestine Activists Got Sentenced as Terrorists Anyway
- “Ceasefire” is not in Israel’s vocabulary – Daily Update
- Did Trump just threaten a nuclear attack on Iran? Another merger for Israel-Firster David Ellison –Daily Update
- Israeli Firm Accused of Launching Smear Campaigns During US, European Elections
- As World Cup kicks off, Gaza amputee girls chase football dreams
- Oxfam: More Palestinians killed by Israel across West Bank in last 3 years than previous 17 years combined
- US-Iran ceasefire may be imminent, but will Israel blow it up? – Daily Update
- The Issue of Israel Is Ending Democracy In Michigan
- Israel is stealing homes, livelihoods, and lives in West Bank
- Gaza is not an aberration – Israel planned this genocide decades ago
- No Tricks Zone
- Climate Alarmists Now Using Natural Phenomena To Support Their Claims
- New Study: Significant CO2 Fluxes From Non-Volcanic Sources Are Largely Neglected In Carbon Budgets
- Women Climate Scientists Being Harassed, Insulted By Skeptics, Claims Berkeley Earth Researcher
- Germany’s Longterm Spring Climate Data Show “No Climate Trend”
- New Study: Solar Photovoltaic, Wind Power Fail To Meet Annual Energy Demands 62% Of The Time
- Germany’s Die Welt: “Too Much Is Too Much” … Green Energies Are Cannabalizing Each Other!
- Germany’s Ecological Holocaust… Once Fairy Tale Forests Getting Cleared For Wind Turbines
- A Grand Solar Minimum Has Arrived…Global Cooling Of At Least 1°C Is Expected By The 2030s, 2040s
- European “Expert Commission” Urges COVID-19-Like Global Climate State Of Energency!
- Real-World Observations Do Not Support The Position That Climate Change Is Human-Caused
