Davos Leaders Collude to Force Permanent Global Vaccine Infrastructure
By Jefferey Jaxen | January 19, 2023
What is Davos? The World Economic Forum’s (WEF) annual meeting happens each year in the alpine Swiss ski resort town. Each year global leaders, elected and unelected, gather to collude on policy initiatives and hot button topics concerning humanity overwhelmingly without the consent of the people.
Intel coming out of this year’s meeting has had a more pressing, alarmist nature from the self-proclaimed global elite minders. Don’t worry, the meeting was still filled with the annual hypocrisy we are used to. Squadrons of ‘unsustainable,’ carbon-emitting private jets still flew in at will. Fleets of non-electric cars openly chauffeured the climate alarmist around while they preached about the end of gas vehicles and individual car ownership… for the planet of course. But lets turn to moves by the medical–industrial complex.
Coming off the back of a rushed Covid shot that failed to stop transmission and whose harms and shortcomings are still unraveling in the public conversation, the ‘global leaders’ of Davos used the forum to do what they always do in the uncomfortable spotlight – double down on agendas.
After some of the biggest, concerted global protests in a century against lockdowns and the digital Covid vaccine passports used by governments to enforce them, a call was made to expand such tools of restriction.
Former UK PM Tony Blair of Iraq war criminal fame apparently received his new marching orders speaking passionately at Davos for the implementation of a ‘national digital infrastructure.’
For ‘the vaccines coming down the line [that] will be multiple shots,’ for ‘vaccines [in general]’ and for ‘a pandemic’ Blair stated you need a proper digital infrastructure to know ‘who’s been vaccinated and who hasn’t.’
Founded in Davos by the Gates Foundation, the UK-based Wellcome Trust, the WEF and other governments, the Coalition for Epidemic Preparedness Innovations or CEPI was a central player in global Covid vaccine development efforts.
They now have a new ‘100 day goal’ which has been embraced by the G7 and G20 nations according to a Davos speech attended by Pfizer’s CEO Bourla, Blair and others.
To ‘accelerate vaccine development over and above what was achieved in 2020’ and to be able to deliver vaccines for new threats within 100 days.
So the idea again would be to sidestep proper safety testing to put massive mutation pressure on a new circulating virus or pathogen by vaccinating in a middle of an ongoing pandemic – something Dr. Geert Vanden Bossche has continually warned against.
CEPI’s goal to take Covid’s fast tracking vaccine development precedent and fast track it further has been aided, intentionally or unintentionally, by the newly enacted FDA Modernization Act 2.0 which allows drug and vaccine developers to rely upon computer modeling and testing with virtual patients in their safety assessments of new products to convince regulators they’ve been ‘de-risked.’
While the Davos crowd, along with many others in the public, like Neil DeGrasse Tyson, still believe the official narrative that the rushed Covid shot was a wild, safe and effective success, a growing critical mass continues to expose the truth.
Meanwhile, the FDA still doesn’t have ‘robust’ data from Pfizer or Moderna on their mRNA Covid shot product’s ability to cause potentially deadly heart inflammation.
A 2021 letter by the FDA to Pfizer gave the company until October 2025 to turn in their study looking at that piece which public health leaders and agencies will take, at face value, as the final word on the subject. Despite the foot-dragging by regulators, members of the public and medical community have filled the vacuum with actual data and warnings.
Top UK cardiologist Dr. Aseem Malhotra made history becoming one of the BBC’s most watched segments of the last two years [27.1M view on Twitter] warning about the myocarditis risk live on-air along with its role in the soaring number of excess deaths – the highest in 50 years according to the BBC.
Will the public accept digital restrictions on their life again in the form of vaccine passports?
Will the public accept new, multi-dose vaccines unpinned by even less safety testing and transparency than the mRNA Covid shots?
Are vaccine deaths being disguised as virus deaths?
By Professor Roger Watson and Dr Niall McCrae | TCW Defending Freedom | January 18, 2023
A new Covid-19 variant has appeared: XBB.1.5 (or ‘Kraken’, for the fear factor). This could explain why deaths are surging again, with Japan recording about 400 daily, and Australia (despite being in the height of summer) in the dozens. But are people really dying from the latest strain of coronavirus?
Excess mortality is highest in countries with the highest rates of Covid-19 vaccination. Correlation is not causation, but only the wilfully blind are describing this human toll as ‘baffling’. Ordinary people do not need scientific expertise to join the dots. At the very least, the authorities should be investigating this unprecedented rise in mortality as a possible iatrogenic disaster (ie caused by medical treatment, like thalidomide).
While there is growing public awareness of the lethality of the mRNA injections, the scientific orthodoxy is continuing to suppress the truth. In reports showing an increased incidence of cardiovascular disease after vaccination, researchers always moderate the message by stating that the benefits overwhelmingly outweigh the risks. However, many publications do not even consider the vaccines as a cause of illness or death.
Our editor alerted us to the article Covid Leading Cause of Death Among Law Enforcement for Third Year in Medscape. The data for this study of police officers across the US were taken from an annual report issued by the National Law Enforcement Officers Memorial Fund, titled 2022 End-Of-Year Preliminary Law Enforcement Officers Fatalities Report.
The report claims that in the past year 70 officers died in the line of duty of causes related to Covid-19. The good news is that this is ‘down dramatically from 2021, when 405 officer deaths were attributed to Covid’, but this was still a significant loss of front-line personnel, surpassing the number of deaths from firearms-related incidents.
The authors of the original report attribute the decline in deaths to ‘reduced infection rates and the broad availability and use of vaccinations’. However, this putative triumph of the Covid-19 vaccine needs more scrutiny than afforded by Medscape writer Lisa O’Mary.
In the original report we were keen to know how many law enforcement officers had died of other deadly infections. We anticipated influenza, meningitis, gastroenteritis and septicaemia among other potential killers, but none of these are mentioned in the report despite exposure on duty. We also wondered what the ‘background noise’ was in terms of how many law enforcement officers had died in total during the preceding years whether in the line of duty or not. Sadly, this figure was not reported either.
Covid-19, uniquely amongst infectious diseases, is being recorded as a cause of death in the line of duty but it is not clear why. We do not have any doubts about the bona fides of the National Law Enforcement Officers Memorial Fund and we do not, at face value, question their use of the numbers with which they have been provided. What is clear is that, like most of the public sector in the US (and the UK) they have fallen for the Covid-19 narrative and been willing participants in the ‘fear porn’ that has gripped so many otherwise well-meaning organisations.
We see several problems with the researchers’ claim that low Covid-19 mortality in officers was due to the vaccine. The first problem is the distinction between the definition of deaths ‘with’ as opposed to ‘of’ Covid-19 and the possible attenuation of the Covid-19 virus over time. Then, we are not informed in the report, and data seem unavailable, about the extent to which Covid-19 testing was or is still being carried out. If there was a significant reduction in Covid-19 testing between 2021 and 2022 that would be a significant confounding factor.
A bold claim about the success of the vaccine rollout would need, at least, to show how many law enforcement officers were vaccinated. Even then the outcome would not provide much insight into cause (vaccination) and effect (death from Covid-19).
It is not clear how many US law enforcement officers are vaccinated. There were indications that compulsory vaccination was going to be introduced for law enforcement officers. But there was also evidence that the law enforcement unions ‘pushed back’ against the idea. In fact, uptake of Covid-19 vaccines was so low amongst law enforcement officers that hundreds were reported to be dying and that, according to the Washington Post, they were a danger to the public. Therefore, it seems incongruous that, on the one hand, law enforcement officers are a public hazard due to their low Covid-19 vaccination status, and on the other hand have their own lives saved ‘dramatically’ as a result of the Covid-19 vaccines.
There is a more serious question that the researchers failed to ask themselves. Is it possible that some of the 70 officers dying in 2022, and some of the 405 in the year of the initial vaccine rollout, were victims of the Covid-19 vaccine? Consider, for example, an officer who is hospitalised for breathlessness, and is discovered to have dangerous blood clots. On admission he tests positively on a PCR test, which is notoriously prone to false positives. If this officer were to die, he would be added to the Covid-19 mortality figures. This is not fantasy, but the reality of how the pandemic has been perpetuated over the last three years – with the collusion of the scientific community.
Plain English guide to the pandemic treaty
By Libby Klein | Reclaim Ethical Medicine | January 17, 2023
There are some absolute pearlers buried in the Pandemic treaty:
- Gain of function research is on for young and old – we must not be inhibited by red tape, just get on with it.
- Global sharing of patient data, specimens and pathogens is also the order of the day. Feel free to pick and choose which bits of existing international law to observe.
- We must have a singular focus on vaccines as the answer to everything. We will target the vulnerable in the name of equity, especially in developing nations, with fast tracked, under-tested new drugs – and only give them biased information in favour of taking the treatment.
Oh, and remember these key points:
- The WHO is central to everything.
- The WHO owns the science.
- The WHO controls raw materials, production, allocation, distribution and financing of pandemic products.
- The WHO will decide what restrictions to impose on you to address climate change because climate change might affect your health.
- The WHO decides what medical treatments are allowed, and which are banned.
- The WHO decides what is allowed to be spoken, and stamps out voices of dissent.
I hope you don’t believe me. No sane person would. Read for yourself the ‘Conceptual Zero Draft” of the proposed pandemic treaty. There’s a plain English guide here:
Please read it, then tell at least one person about this stupid treaty every day, until it goes away.
$1,000,000 to forecast Vaccine Misinformation narratives
The Naked Emperor’s Newsletter | January 16, 2023
On 20 October 2022, the CDC published a grant opportunity to develop a public health tool to predict the virality of vaccine misinformation narratives. The application closed a few days ago.

The purpose of the $1,000,000 grant is “to conduct research to develop and pilot a predictive model and tool to aid…in identifying emerging vaccine misinformation about recommended vaccines, including COVID-19 vaccines, that is likely to spread and have a high potential for impacting vaccine confidence”. It will enable public health agencies to identify misinformation before it spreads or impacts people’s health decisions.
According to the proposal, evidence for the negative impact of misinformation continues to grow. Therefore, this proposal has the potential to impact the Healthy People 2030 scheme by ensuring people get vaccinated. Healthy People 2030 sounds and looks suspiciously like something from Agenda 2030 but equally this might just be someone jumping on the bandwagon. However, one of the developmental objectives is to “increase the proportion of immunization information systems that track adult immunizations across their lifespan” which sounds a lot like vaccine passports. Maybe not but unfortunately these things need keeping an eye on these days.
The CDC estimates that “COVID-19 misinformation and disinformation caused $50-$300 million per day in additional medical costs, monetized lives lost and morbidity, and economic costs”. Therefore, they want this new tool to increase vaccination rates and disseminate accurate scientific messages.
There are 3 phases to successfully complete the proposal:
- Phase 1 – Develop a predictive model that identifies misinformation. To do this they will look at old data to find topics (such as vaccine safety and fertility), the types of people sharing this information and the relationship to societal concerns (e.g. personal liberty);
- Phase 2 – Develop a tool that can be used to prioritise the response to misinformation.
- Phase 3 – Pilot and evaluate the tool (that can be used at federal, state, local, tribal and territorial public health agency levels)
Now, I’m all for getting rid of misinformation. In an ideal world I just want to be reading facts, more facts with a few more facts sprinkled on top. However, this isn’t an ideal world and unfortunately, over the last few years, much of the misinformation has come from the CDC itself.
So a ‘Minority Report’ style system that will identify vaccine misinformation pre-crime and eliminate it before it can get out will only add to public distrust.
A Soviet-style public health propaganda set-up is not going to increase vaccine take-up. The only way to do that is to provide transparent data and allow hypotheses to formulate. These can quite easily be shut-down with accurate and open data.
What does increase vaccine hesitancy, is not having a truly independent body to analyse pharmaceutical data and then trying to bury that data for 75 years. Misinforming the public that they are going to die without a vaccine was the most harmful thing they could have done to trust in public health. Along with the suppression of adverse event signals, harms and deaths. However rare they may or may not be, by hiding just one of these causes the public to question what else is being hidden.
So I would like to claim the $1,000,000 to reduce vaccine misinformation with the following steps:
- Firstly produce a product that actually does what it is supposed to do;
- Conduct proper trials that look at short, medium and long term risks;
- Create a truly independent body that not only analyses the data it’s provided with but tests the products themselves;
- Remove propaganda such as ‘95% effective’ or ‘safe and effective’;
- Don’t conduct studies on how to manipulate the population into taking vaccines;
- Don’t force anybody to take a vaccine (by use of the psychological techniques above or through vaccine passports);
- Don’t use fear to convince people they are going to die without being vaccinated;
- Don’t supress safety-signals;
- Don’t gaslight the vaccine injured or families with members killed by vaccines;
- Remove the product from the market as soon as any safety signals, injuries or deaths occur. Explain clearly and openly what has been found and why the product has been removed;
- Don’t label anybody concerned about big pharma corruption or vaccine safety a conspiracy theorist or worse.
There you go. You don’t need any fancy and expensive systems to get people vaccinated. Just follow the steps above. But unfortunately, if your product isn’t up to scratch, you won’t make any money. You can send my $1,000,000 cheque in the post. Thanks.
Did I miss any points? And is it too late anyway? Has the amount of public health misinformation eroded away all trust, never to be regained again?
Campaign funded by Pfizer and Moderna lobbyists sent Twitter weekly lists of tweets to censor
By Tom Parker | Reclaim The Net | January 16, 2023
The Public Good Projects (PGP), a nonprofit that has developed several projects to fight so-called Covid “misinformation,” received $1,275,000 from the Pfizer and Moderna lobbying group, Biotechnology Innovation Organization (BIO), to create a content moderation campaign that influenced Twitter’s Covid misinformation rules. As part of this campaign, PGP sent Twitter lobbyists and content moderators weekly emails containing lists of tweets to censor.
Journalist Lee Fang published one of the weekly emails that Twitter received from PGP as part of the latest release of the Twitter Files — collections of internal Twitter communications that have exposed the censorship relationships Twitter had with government agencies and other powerful groups before Elon Musk took over.
The email shows Todd O’Boyle, a senior manager on Twitter’s Public Policy team, sharing “this week’s misinfo report” from PGP. The February 24, 2022 email included a list of top trends the PGP had seen during the week and two attached lists. According to Fang, one of the lists contained tweets the PGP wanted Twitter to take down and the other list contained tweets that it wanted Twitter to verify.
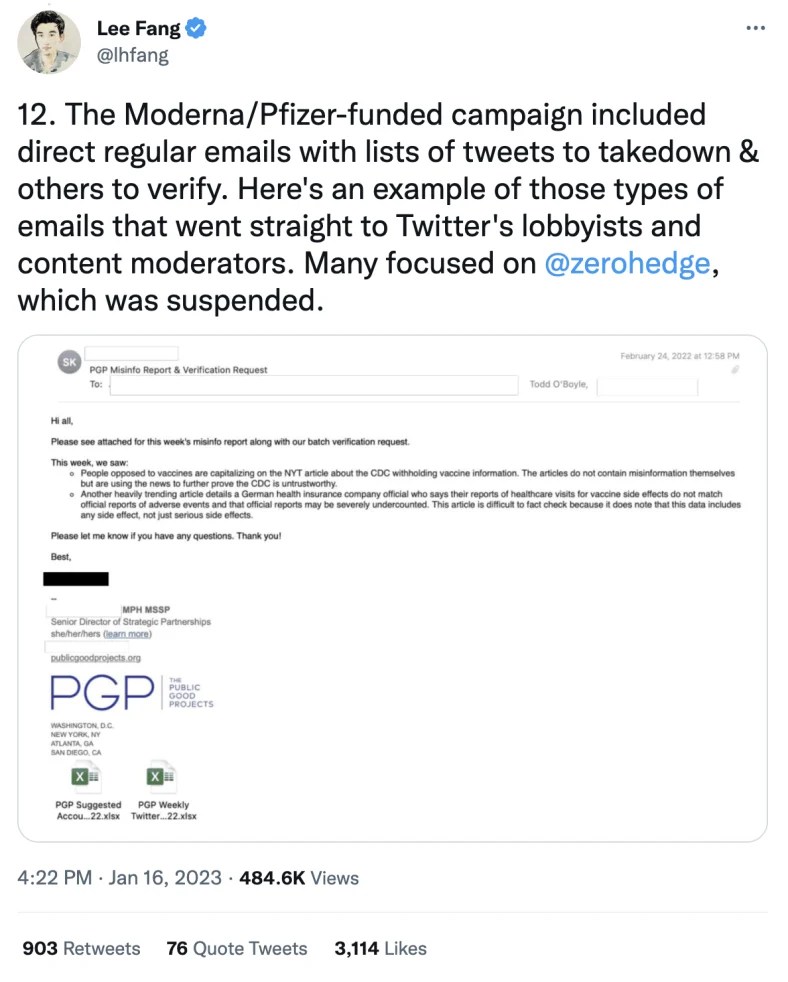
Despite flagging two trends in this weekly misinfo report, the PGP admitted that articles related to the first trend “do not contain misinformation themselves but are using the news to further prove the CDC is untrustworthy.”
The PGP also acknowledged that the second trending article it flagged, which described a German health insurance company official suggesting that reports of healthcare visits for vaccine side effects may be severely undercounted, “is difficult to fact check because it does note that this data includes any side effect, not just serious side effects.”
Fang said many of the PGP’s emails to Twitter focused on independent news outlet ZeroHedge which was banned from Twitter in January 2020 and reinstated in June 2020.
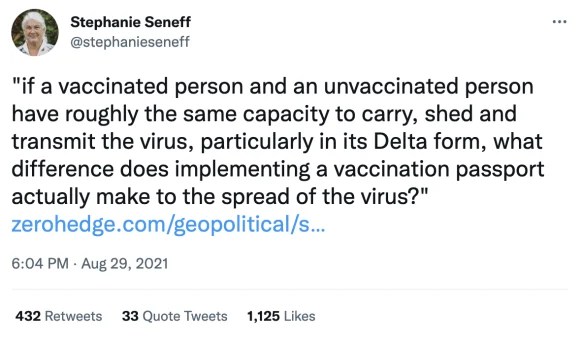
Fang also noted that this campaign flagged a tweet from senior Massachusetts Institute of Technology (MIT) scientist Stephanie Seneff that questioned vaccine passports on the basis that vaccinated and unvaccinated people have “roughly the same capacity to carry, shed and transmit the virus.”
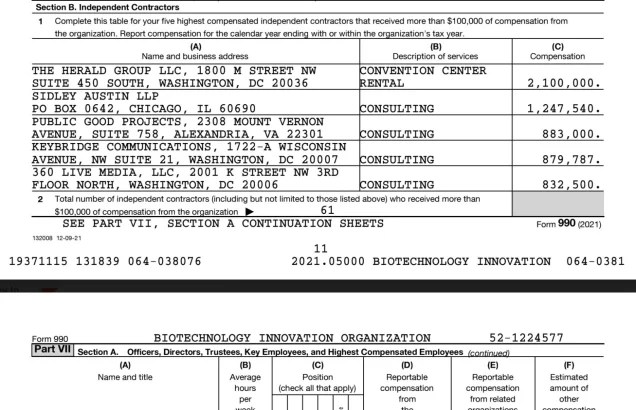
Additionally, Fang shared a screenshot of a BIO tax form that revealed part of the funding ($883,000) it provided to PGP for this campaign.
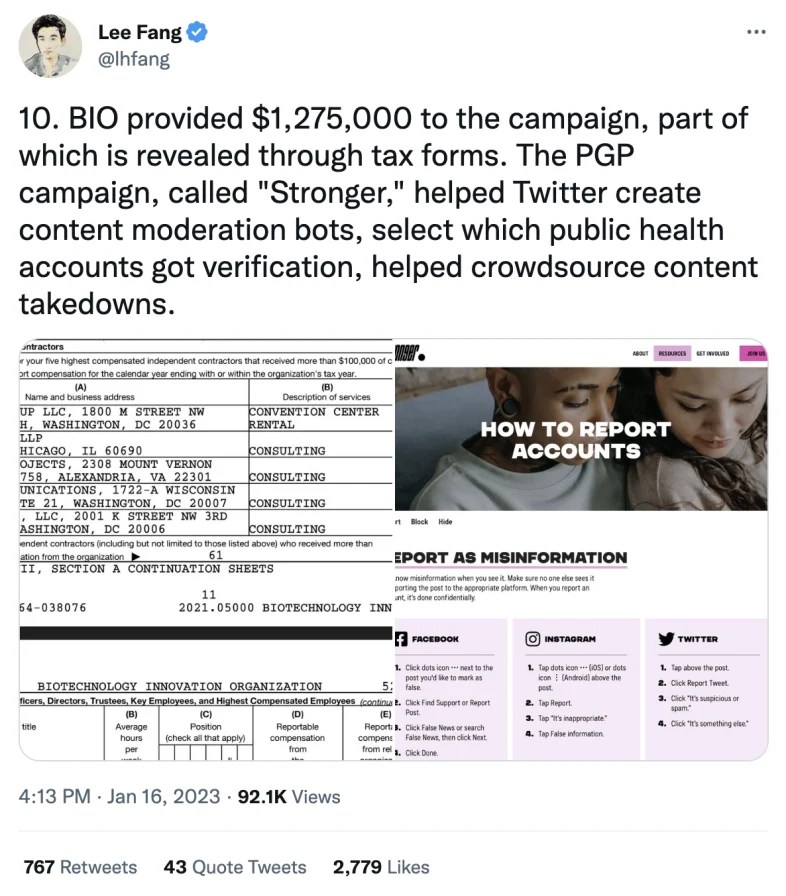
The PGP campaign is called “Stronger” and, according to Fang, it worked with Twitter to craft the platform’s content moderation rules around Covid misinformation, helped Twitter create content moderation bots, and helped Twitter select which public health accounts got verification.
Stronger says its goal is to “stop the spread of misinformation” and its website contains a page that encourages people to flag misinformation to Twitter and other platforms.
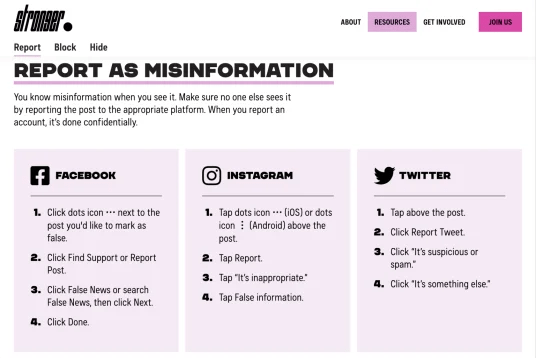
This page also contains a form for users to submit alleged misinformation to Stronger.
“Paste the link to a post, account, or website below, and the Stronger team will report it to the appropriate platform,” the form states.

Previous campaigns from the Public Good Project have involved recruiting pro-vaccine keyboard warriors to mass report anti-vaccine social media posts.
Fang’s revelations are the latest of several examples of those affiliated with Pfizer pushing for the censorship of content that questions or criticizes Covid vaccines.
Pfizer board member Scott Gottlieb complained to Twitter in August 2021 that it was promoting an article from journalist Alex Berenson. A few days after this complaint, Berenson was banned from Twitter. Twitter also censored another tweet after it was flagged by Gottlieb in August 2021.
Meanwhile, Pfizer’s CEO has branded those who share what he deems to be misinformation about vaccines as “criminals.”
WHO Sneak Attack
CHD.TV: “This is the big one. They’re going for broke… I think we may only have potentially until May before one or both of these documents gets voted on” — Meryl Nass, M.D. and James Corbett continue their discussion on the WHO’s proposed International Health Regulation Amendments + potentially legally-binding ‘Zero Draft Treaty’ currently being drawn up in secret meetings behind closed doors. As the WHO touts the solution to worldly problems as possible through their ‘One Health’ approach — one wonders if a world in which humans, animals, agriculture, and weather are dominated by state depicted notions of the highest attainable standard of ‘health’ may secretly be a trojan horse to dominate as much of the sovereign world as possible — usurping power from individual countries and thrusting it into the hands of a mad-with-power agency which seeks to control Earth’s resources, ecosystems, food, animals, and plants.
VIDEO COURTESY Bitchute CHD.TV / RUMBLE
SHOW NOTES:
PREVIOUS TALK: The Weaponization of the WHO on CHD TV
WHO Member States Agree To Develop Zero Draft Of Legally Binding Pandemic Accord In Early 2023
Review Committee Regarding Amendments To The International Health Regulations (2005)
CDC’s One Health Office: What We Do
One Health Joint Plan Of Action Launched And Presented By WHO And The Quadripartite Partners
One Health Joint Plan Of Action Launched And Presented By WHO And The Quadripartite Partners
Please Stop The Ride To A Biotech Food Takeover – Transcript
James Roguski Substack — THE TOP 100 REASONS TO #StopTheTreaty, #StopTheAmendments, And #ExitTheWHO.
The Lancet has become a laughing stock
By Norman Fenton and Martin Neil | Where are the numbers? | January 14, 2023
In summary:
- On 6 May 2021 The Lancet published a blatantly flawed study of the effectiveness of the Pfizer covid vaccine on the population of Israel, claiming it was 95% effective.
- On 17 May 2021 we submitted a rapid response 250 word letter explaining why the study was flawed.
- After an initial response saying they would ask the authors for a response to our letter we heard nothing until 20 months later.
- On 8 January 2023 we got an email out of the blue from The Lancet Senior Editor Josefine Gibson apologising for never having got back to us about the letter, saying that they had asked the lead author Dr Sharon Alroy-Preis (SA-P) to respond to our letter but, because she did not provide any formal response, they have decided not to publish our letter.
- We tweeted The Lancet’s response and within 24 hours it got over one million impressions. We also published a substack article highlighting the fact we were now aware of additional problems with the paper relating to SA-P’s relationship with Pfizer.
- On 10 January 2023 we got an unsolicited email from Josefine Gibson (which we can only assume was a result of the reputation hit they got from our tweet) saying “Thank you for bringing your letter from May 2021 back to our attention. We are looking into next steps and will get back to you as soon as we can.”
- On 11 January 2023 (at 10:58) we sent an email to The Lancet’s Editor-in-Chief Richard Horton directing him to our substack article (which highlighted these new problems relating to SA-P’s relationship with Pfizer) stating that The Lancet was clearly taking a credibility hit surrounding the publication of the Israel-Pfizer study and its response to criticisms of it.
- On 11 January 2023 (at 11:21) we got an email from Josefine Gibson apologising for the ‘sub standard experience’ we had with The Lancet. She said that, after discussing it with Horton, they were now inviting us to publish the original letter or an update to it, suggesting the update ‘reflect more current experience with the vaccine’.
- On 12 January 2023 we submitted our updated letter (of an agreed 350 words).
- On 13 January 2023 we got a response from Josefine Gibson saying they had decided against publishing the letter.
Here is the full narrative and January 2023 correspondence in date order (personal details redacted)… continue
Insider reveals truth about Covid-19 pandemic from within the National Health Service
How the misdiagnosis of deaths occurred and was due to changes from 2016
The Naked Emperor’s Newsletter | January 15, 2023
An ex-director at one of the largest hospital trusts in the UK decided they wanted to reveal what really happened during the pandemic. They have kindly allow me to reproduce their thoughts. The catalyst for this revelation, according to the insider, was Dr. Malhotra speaking out about cardiac problems post vaccination.
This is an interesting take on what happened inside the National Health Service (NHS) and confirms, with more details, what we already knew and suspected.
Introduction (Long but important to understand the rest)
In 2016, the British Government proposed & piloted a change to the process of how deaths were certified across all hospitals in the UK. I have attached a link to this Department of Health (DoH) document.
The DoH document proposed a switch to the “Medical Examiner” (ME) System and was sent to a number of different audiences for feedback and consultation. The ME system was already being piloted at two hospitals up north. The results of the consultation are here.
Prior to the Covid-19 Pandemic, the death certification process involved treating doctors of a patient to attend Bereavement Services/Patient Affairs to discuss the death and either:
a) refer the death to the Coroner or
b) write a Medical Certificate of Cause of Death (MCCD).
The MCCD states the cause of death. Whereby a direct cause (1a) or contributing causes (1b) (1c) (1d) are stated along with co-morbidities (not directly causing the death) being written in (2) on the MCCD. The MCCD is only ever a probable cause of death, it is not definitive.
The only definitive way of determining an accurate and plausible cause of death is to refer the deceased patient to HM Coroner (if certain criteria is met), for HM Coroner to accept and take on the case, resulting in a Post Mortem (PM) being conducted by a Histopathologist. When a death is seen as natural and there is nothing untoward, the MCCD is written by the treating doctor of a deceased patient. Usually this is an F1, F2, SHO or Registrar that attends. It is rare for a treating Consultant to attend, but they will finalise the cause of death.
A strict hospital hierarchy exists within the NHS for doctors. It is as follows – from lowest to highest rank: Foundation Year 1 (FY1), Foundation Year 2 (FY2), Senior House Officer (SHO), Registrar (Reg), Consultant, Clinical Lead, Medical Director. Junior doctors will very rarely speak up or challenge their seniors. A senior decision is seen as final and it will be carried out and executed without any hesitance or questioning. In my 5.5 years of experience in End of Life Care, I have only ever seen one junior doctor disagree with a proposed cause of death and challenge their consultant.
With the number of deaths that occur in a hospital, as you can imagine, there is a great deal of variation with regards to causes of death, as we have numerous different doctors writing an MCCD and coming up with various different potential diseases in different orders.
The proposed ME system would change this, as the government would now hire and pay one Medical Examiner, to sit in every hospital and write all MCCD’s for all deceased patients. This would effectively eliminate any variation in causes of death.
In 2016, when I heard of this proposal, I worked as a Bereavement Officer at a hospital in Central London. My mentor/line manager at the time was a former Chief Nurse who managed Bereavement Services and all hospital deaths would be controlled by her and the department.
We essentially carried a huge amount of power with regards to decision making, as we would go through all patient notes following the death of a patient, and essentially guide and advise doctors on what would need to be written with regards to an MCCD or Coroners Referral.
In my personal opinion, our role was to sit on the fence and act in the best interests of a deceased patient (and their families), but also protect the hospital and our doctors from any potential negligence. As you can imagine many battles were fought over decisions about a cause of death of a patient or a referral to the coroner with a vast amount of doctors over the years.
F2’s and SHO’s were particularly the worst with regards to carrying an arrogance of knowing what should be written on an MCCD or stating that a patient didn’t need to be referred to the Coroner (often stating that their Consultant had given them instructions). It is worth noting that Consultants are also only human and can be incorrect at times too. We have to remember that they are succeeded in hierarchy by a Clinical Lead and beyond that a Medical Director. Who have far more experience and knowledge.
When I asked my mentor in 2016, how the ME system would change things, I was told that Bereavement Services/Patient Affairs would become purely administrative and that the clinical judgement would fall to the Medical Examiner.
The power and decision making with regards to MCCD/Coroners Referrals was being taken away not only from treating doctors but also from Bereavement Services/Patient Affairs/Bereavement Officers/Bereavement Service Managers/Directors of End of Life Care.
This decision making power was being handed solely to the Medical Examiner, who has not been involved in the treatment of a patient during an admission. I took all this information in at the time and acquired as much knowledge as I could from my mentor/line manager.
In 2016, I also happened to make a move and take up an opportunity to manage my own Bereavement Services at one of the largest hospital trusts in the whole of the UK. On average, I would oversee MCCD/Coroner Referrals for approx 1750 deaths on an annual basis. I developed a very close working relationship and friendship with one of the Medical Directors (a doctor with the highest ranking in a hospital). This was especially helpful when having to challenge doctors with regards to MCCDs/Coroners Referrals.
Progressing to Director of End of Life Care, I became involved with the reporting of mortality rates, conducting mortality reviews and writing hospital policies. I had also developed an excellent working relationship with the HM Coroner who oversaw our Trust. HM Coroner holds the power to investigate any hospital or trust with regards to a death or a number of deaths. A slight problem may arise, in that HM Coroner has an allegiance to the Crown and the Government.
When a death is reported to the Coroner. This was previously reported via telephone call by the treating doctor. A discussion was had with the Coroners Office and a direct outcome and instruction would come from the Coroner’s Office, by way of HM Coroner (via a phone call).
There is a fundamental flaw to this system, as there is no documentation of the decision and instruction from the Coroner’s. It comes via word of mouth. There is always room for error without any electronic documentation. Every Hospital/Trust & HM Coroner will have a different system of reporting deaths. I personally made a decision to safeguard my hospital and the trust, by developing an electronic coroners referral form, which I proposed to our Coroner and developed after their agreement. We now had documentation of every death being reported and every outcome.
When reporting a death, the Coroner will look at a proposed cause of death and accept it, or reject the cause of death and take on the case (death of the patient), leading to an Inquest or a PM.
In 2019, our Medical Director, came into my office one morning and stated that the Board of Directors at the Hospital had made a decision to switch to the Medical Examiner System. Hearing the words ME system was a massive case of Déjà vu (conversation with my mentor in 2016). I knew exactly what the ME system was, but I chose instead, to play the fool and enquire what exactly the ME system was and what it meant for our service, my staff and our roles. Everything the Medical Director mentioned to me that day was a carbon copy of what I already knew
I knew that my time in End of Life Care had come to an end. I’d reached the top and there was no more progress for me. Losing all power and decision making to any ME coming into the hospital did not appeal to me. I’d already made up my mind that I needed to leave. Seeking a new challenge and experience, I made a move in 2019 to another major hospital in Central London, this time side tracking into operational management. I was in charge of the operational management of Nephrology, Rheumatology, Dermatology and Diabetes & Endocrinology.
2020 – Covid Arrives
In Jan 2020, I remember hearing about the first case of Covid-19 at our hospital, with a patient arriving from China and walking into our A&E. A&E was shutdown and steam cleaned that day, I recollect the moment I heard about this. In my mind, I saw the reporting of Covid-19 in the media as nothing more than Bird Flu or Ebola, which had caused panic but yet passed. I wasn’t worried in the slightest bit.
Things began to escalate around in Feb 2020, around the time I was going on holiday. Due to the reporting by the media, I bought N95 masks as a precaution for my trip and to give to my parents and younger sister. I was blessed to have had an opportunity to spend a few days in Sri Lanka for a wedding and then nearly a whole month in Australia (March 2020). I watched as the narrative of a deadly infectious disease continued to grow with every day that passed. I made a decision to cut my holiday short by a couple of days so that I could make sure I got back to my family and not end up being stranded in Australia.
Upon returning to the UK in late March 2020. One of the immediate things that struck me was the lack of any temperature monitoring or questioning at Heathrow Airport. This seemed odd for a potentially deadly infectious disease that was spreading around the world. This was especially odd, as Sri Lanka & Australia had questioned me/checked temperatures upon arrival, with even Singapore monitoring temperatures during transit.
My mother had just recovered from Cancer, my father was over 70 and my younger sister was born with Down’s Syndrome alongside having multiple other conditions. I had three high risk individuals to Covid-19 in my family and I was scared/fearful of giving them Covid-19. I asked my hospital to allow me to work from home. They refused. I wasn’t deemed high risk, although I lived with my parents at the time. I needed to help my mum and my sister. The hospital held no regard for the safety of it’s employees. They forced me to come into work. I spent two months isolating in my bedroom, I barely came out of my room, for fear of spreading an infectious disease. Never once did I think about the situation or my prior experience or knowledge, I was just reacting to the media frenzy. I was full of panic and stress.
The first irregularity I noticed, was the government and media stating that Covid-19 was an infectious disease. However just before the first lockdown was implemented, I noted that the government had downgraded the status of Covid-19 stating it was no longer infectious. This made no sense to me. Why would we need to isolate if they downgraded the status? My circle of friends contained many medics and dentists. They were all panicking at the time, saying they had inadequate surgical masks and that they needed N95 masks.
N95 masks were seen as the only way to prevent medical professionals from becoming infected with Covid-19. The public being asked to wear surgical masks made no sense to me. The virus would be able to go straight through. Something didn’t seem right.
I ended up meeting and dating an FY1 doctor (my ex gf) around October 2020. We clicked because she was different from every other doctor, I had previously spoken to about Covid-19. She also had her suspicions and believed it wasn’t as infectious as it was made out to be. We both started to slowly realise that Covid-19 was a real disease (as it was showing up on X-rays in patients) but that it wasn’t infectious at all [NE – I have since confirmed with them that they mean not as infectious as was being made out], despite all the reporting in the media.
I needed to experience working in a Covid-19 hotspot and see all the action for myself. In March 2021, I quit my job at the hospital in Central London and took up an opportunity to manage A&E and AMU (Acute Medical Unit) at a hospital in South London. The 6 months that I spent working in A&E/AMU confirmed all my suspicions and culminated in my decision to end my career in the NHS.
The entire 6 months, I was not tested once with a PCR Test, despite walking into wards full of Covid-19 Positive patients on a daily basis. Yet we were required to test multiple times when visiting another country.
The PCR Test that the NHS was using to test patients, is known to have false-positive results. This is shown in numerous studies which can be found online, an example of which is:
Are you infectious if you have a positive PCR test result for COVID-19? – The Centre for Evidence-Based Medicine.
If a patient tests positive for Covid-19 with a PCR Test, this doesn’t mean they are infected. If tested again, they may well turn out with a negative test. However in the NHS, patients are only tested once and this stays on their record throughout their admission. Hospital policies were changed alongside the implementation of the Medical Examiner System, to ensure that any patient who died within 30 days of positive test, would have to have Covid-19 as their primary cause of death. This was regulated by the Medical Examiner.
The highest cause of death at every hospital per annum pre Covid-19 is Pneumonia. Pneumonia is a Respiratory Disease like Covid-19. Pneumonia can be broken down into 4 different causes of death: Bronchopneumonia, Aspiration Pneumonia, Community Acquired Pneumonia & Hospital Acquired Pneumonia.
These four causes when added together kill the largest number of people on an annual basis prior to the pandemic.
The Medical Examiner (one individual in each hospital), was certifying all these Pneumonia deaths as Covid-19 deaths. When 4 different diseases being grouped and now being called Covid-19, you will inevitably see Covid-19 with a huge death rate.
The mainstream media was reporting on this huge increase in Covid-19 deaths due to the Medical Examiner system being in place. Patients being admitted and dying with very common conditions such as Old Age, Myocardial Infarctions, End Stage Kidney Failure, Haemorrhages, Strokes, COPD & Cancer etc were all now being certified as Covid-19 via the Medical Examiner System.
Hospitals were switching to and from the Medical Examiner system and the Pre Pandemic System as when they pleased. When Covid-19 deaths needed to be increased, the hospital would switch to the Medical Examiner System. Doctors were one week being told they needed to complete an MCCD, to then be told the following week that they weren’t required to fill out an MCCD, as the Medical Examiner was handling this.
Hospitals were incentivised to report Covid-19 deaths over normal deaths, as the government was paying hospitals additional money for every Covid-19 death that was being reported. The Medical Examiner system ensured that Covid-19 was being put down as the cause of death. The government sends out the annual NHS budget to Primary Care Trusts. This is split to fund Hospitals and GP Surgeries. A clinical coding team at each hospital will assign codes to each treatment or death, so that money is paid out to the hospitals.
Any doctor who argued against Covid-19 as a cause of death was bullied and vilified. The General Medical Council maintains a register of all doctors within the UK. This ensures that there is a fear of being struck off for speaking out against an agenda. The GMC effectively controls all doctors in the UK. Even if a doctor realises what is going on and wants to speak out. They will think twice about talking, as they would be risking their entire career and everything that they’ve worked so hard for.
Doctors essentially have their hands tied, many have families, kids, mortgages and mouths to feed. If I was in their situation, I would think twice about speaking out, for fear of being struck off by the GMC and losing everything.
The NHS Track & Trace App, which was introduced to try and control the spread of the virus, did not apply to medical professionals. We were all asked to turn this off, as Doctors and staff isolating for 14 days disrupted patient flow, beds and the discharge of patients.
Any doctor that I spoke to regarding taking the Covid-19 vaccine, were insistent that they were going to wait for a period of time, before taking it themselves, to ensure that it was safe. How is it ethical to give a vaccine to your patients, but not want to take it yourself? In my 12 years of NHS service, never has a doctor pushed or influenced the public to take a vaccine. Yet on social media, I was seeing close friends who were doctors, starting to post on social media that they have taken the vaccine and that the public should. I wouldn’t be surprised if doctors were being forced to promote the vaccine by their superiors or if they were receiving monetary gain in doing so.
I have no doubt in my mind, that the Government has planned the entire pandemic since 2016, when they first proposed the change to medical death certification. Stress leads to disease and illness. Panic leads to people following whatever orders and instructions that are given to them by authority, such as prolonged mask use, which leads to an increase in admissions in to the NHS system due to hypoxia and bacterial pneumonia.
The NHS treatment pathway involved patients being placed onto ventilators. There is a 50% chance of death from this clinical decision alone. How many innocent people have died from the clinical decision to place them onto a ventilator.
During boardrounds (where every admitted patient is discussed), we were seeing patients on a daily basis being admitted due to suffering from adverse affects of taking the vaccine. Patients were blacking out after taking the vaccine or suffering from clots or strokes.
The NHS is all about money and making money. The safety of a patient didn’t seem like the most important thing. It was more about how do we make more beds available so that another patient can be treated. Patients with no next of kin are discharged to nursing homes with care packages. I can’t comment on what happened to these patients in nursing homes, during the pandemic, as I have no experience of their inner workings.
Patients are seen as money, even upon death, hospitals receive money for each death. Is there an actual concern for patient health and safety? I know numerous doctors who are driven primarily by money and monetary gain.
THE REASON WHY I LEFT THE NHS in 2021
56 yr old male, admitted into A&E with end stage kidney failure, has a previous history of regular dialysis treatment for this. No respiratory symptoms on admission and no temperature. However when tested with a PCR Test he unfortunately tests positive. This stays on his record throughout his admission. Our hospital is relatively small in comparison to others I have worked at, we have no dialysis machine as a result. We urgently need to transfer this patient to another hospital otherwise this patient will die. Our treating doctor calls up larger hospitals with a dialysis machine to organise his transfer. All doctors pick up the phone and request the Covid-19 status of the patient. A transfer is declined due to a Covid-19 infection protocol. Our doctors again reiterate the point that this patient will die without dialysis. We are told there is nothing that can be done and that the patient cannot be accepted for transfer.
This gentleman ended up dying without dialysis. Now please tell me what goes on the MCCD….
1a) Covid-19
2) End Stage Kidney Failure
Not written by the treating doctor who disagreed with this cause of death, but by a medical examiner, put in place by the government and the hospital.
When innocent people are being killed by a corrupt organisation and system, for pure monetary gain, I can’t stand by and be part of this anymore. My conscience was clear and I no longer wanted to be a part of this anymore. I am very blessed and lucky that I was in a position to walk away. I’ve been able to speak out, because my hands are not tied and I am not regulated by any organisation or governing body. I believe in speaking the truth and in doing so, I am only just an instrument for God.
I joined the NHS, 12 years ago because I had a desire to help those in need, but the moment I realised that I was not doing this anymore was the time for me to walk away. I apologise to you all if the above thread is confusing with regards to terminology or you cannot understand it’s contents. I’m hoping that at the very least, it can be understood by my fellow medical professionals or by journalists who would like to report the truth.
Turtles All the Way Down: Vaccine Science and Myth
Edited by Zoey O’Toole and Mary Holland
 If you are reading this, you are probably aware of the fierce debate surrounding vaccination and looking for information that will allow you to make the best decisions for yourself and your loved ones. Whether you are a parent or a parent to be, sorting through the many arguments on vaccines can be daunting. Still, you need an answer, a definitive one, to the crucial question: Who has it right in the great vaccine debate – the critics, who claim that vaccines often cause serious harm, or the medical establishment, which tells us that vaccines are safe and effective and the science is settled?
If you are reading this, you are probably aware of the fierce debate surrounding vaccination and looking for information that will allow you to make the best decisions for yourself and your loved ones. Whether you are a parent or a parent to be, sorting through the many arguments on vaccines can be daunting. Still, you need an answer, a definitive one, to the crucial question: Who has it right in the great vaccine debate – the critics, who claim that vaccines often cause serious harm, or the medical establishment, which tells us that vaccines are safe and effective and the science is settled?
Rest assured, you have come to the right place. “Turtles All the Way Down: Vaccine Science and Myth” will resolve the vaccine question for you, once and for all. By the time you finish reading, not only will you see the answer clearly for yourself, you will also have the scientific references and specific quotes at your disposal that prove it — more than 1,200 of them – all from mainstream scientific papers and textbooks, the official publications of relevant government agencies, or manufacturers’ documents.
The book consolidates a great deal of information (accompanied by detailed analysis) that is scattered in hundreds of medical articles, books, and websites. All discussion is presented in clear and easy-to-understand language, so no medical education is required. It presents several original concepts in addition to laying a robust scientific foundation for the more established ones.
Some of the fundamental vaccine safety issues covered in the book are:
- How is safety demonstrated before a new vaccine is licensed? What technique do vaccine manufacturers use in clinical trials to make vaccines appear safer than they actually are?
- What “last ditch” technique is employed when the above one cannot be, and what are its grave (and damning) ethical implications?
- What is the scientific foundation of the safety of vaccination, and what practical tools does this body of science provide physicians to anticipate, diagnose, and treat vaccine injury?
- What fundamental flaws are built into vaccine adverse events reporting systems, and how are these systems used (or misused) by health authorities to support their safety claims?
- What kinds of post-marketing vaccine studies are conducted, and how can they be manipulated by researchers to produce “favorable” outcomes?
- Why would researchers want to skew vaccine research, and how could skewed results be promulgated by the scientific community?
- Why would medical journals publish faulty vaccine science? What is the role of the famed “peer review” in this process?
- What are “the studies that will never be done” by the medical establishment and how long it has resisted doing them? (Hint: more than 100 years!)
- What key CDC-recommended childhood vaccination guidelines were arbitrarily set, without an adequate scientific basis?
In addition, three cornerstones of vaccination lore are covered in depth:
- What is herd immunity, and how does it apply (or not) to the vaccines on the childhood schedule?
- What role did vaccines actually play in the historical decline of infectious disease?
- Was the paralysis associated with polio actually caused by the poliovirus? Is there a better explanation for the great paralysis epidemics of the 20th century? What are the “19 polio mysteries”?
The book is intended for parents overwhelmed by conflicting messaging on this important topic, but it is also an excellent reference for medical researchers and professionals who seek a better understanding of vaccine safety science. Whether you are new to the vaccine debate or a “veteran” seeking a deeper grasp of the science, this book is a must-read. It also serves as an excellent primer on vaccination to share with friends and relatives who may benefit from a deep dive into the subject.
Who designed global guidelines for puberty blockers?
Free West Media | January 13, 2023
Clinics around the world follow guidelines from the Netherlands for gender treatments in children. The basis for this is, among other things, a much-criticized study sponsored by a German hormone manufacturer.
More and more children and young people believe they have to question their gender identity. Some 60 minors were treated in the Netherlands in 2010, but the number has increased to around 1,600 last year. Another 1,800 people under the age of 18 were on the waiting list because gender clinics in the country are full.
Institutions around the world use a standard procedure developed in Amsterdam in the 1990s when it comes to the drug treatment of supposedly transsexual children.
A report by the Dutch newspaper NRC Handelsblad has meanwhile cast doubt on the directive and the independence of gender research at the Amsterdam UMC hospital. As strict as the conditions for treatment may appear, several complications have been overlooked: The terrible side effects of the heavy drug has been brushed off by doctors as being the lesser evil.
Hormone manufacturer sponsored ‘puberty blocker’ study
The approach with puberty inhibitors has since been known internationally as the “Dutch protocol”. The protocol has become the basis for the “gender-affirming standard of care” used throughout the world. Tens of thousands of children are affected worldwide, and in the Netherlands certainly several hundreds, although no precise figures are available.
Scientists investigated whether hormone treatment in transsexuals is more successful if their puberty was initially suppressed with medication. The sponsor of the study was the German hormone manufacturer.
Ferring Pharmaceuticals, the company that markets the drug Triptorelin as a puberty inhibitor had a strong commercial interest in the outcome. Primarily, treatment relies on administering hormones from the opposite sex: men are given oestrogen to become more feminine, women testosterone to become more masculine. But teenagers are additionally administered puberty inhibitors, which prevent boys from developing a low voice and beard growth and girls from developing breasts and other feminine shapes.
There are many criticisms of the study. Questionnaires were inconsistent, there was no control group at all, and the researchers used random samples from the 196 treated children for the results.
Several countries are moving away from ‘puberty blockers’
In the meantime, there is objection in more and more countries to the treatment of children with “puberty blockers”. Not only are they said to impair the physical sexual development of minors, but they can also cause osteoporosis, anorgasmia and infertility. According to the NRC, the drug is said to sometimes even impair the ability to make rational decisions.
Worldwide, there is increasing criticism of the scientific content and non-existent empirical basis of the Dutch protocol developed at the gender clinic of the Free University of Amsterdam. In several countries, health authorities have already decided to treat children mainly psychologically and prescribe puberty inhibitors only exceptionally. In Sweden, they concluded that “the risks currently outweigh the possible benefits” and spoke of possibly the country’s “worst medical scandal”.
In the UK, criticism of the Dutch protocol was so serious that the Tavistock gender clinic, the largest in the world, was closed by the authorities.
Sweden, Finland and Great Britain only want to prescribe the drug in rare, particularly severe cases. Instead, they are increasingly relying on psychological support for patients.
Since February last year, Sweden’s National Board of Health and Welfare has followed the Karolinska Institute’s policy regarding hormonal interventions for gender-dysphoric minors. Karolinska’s pediatric gender services at Astrid Lindgren Children’s Hospital (ALB) has ended the practice of prescribing puberty blockers and cross-sex hormones to gender-dysphoric patients under the age of 18.
Marketing redundant drugs for the wrong condition
In the US, Texas Attorney General Ken Paxton has been investigating two pharmaceutical companies for advertising puberty blockers to children. This is a condition they are not approved to treat.
In December, Paxton announced investigations under the Texas Deceptive Trade Practices Act into Endo Pharmaceuticals and AbbVie Inc., the two companies that sell puberty blockers. The drugs were approved to treat precocious puberty and forms of prostate cancer but were being marketed and prescribed off-label to treat gender dysphoria.
“These drugs were approved for very different purposes and can have detrimental and even irreversible side effects,” Paxton said. “I will not allow pharmaceutical companies to take advantage of Texas children.”
Featured Video

The Source of America’s Wars – Kristol Clear
or go to
Aletho News Archives – Video-Images
From the Archives
Is Israel to blame for the Iraq War?
American Goy | March 10, 2008
I am so tired of this old canard that “Israel had nothing to do with USA’s war with Iraq – in fact, it officially advised America against it”.
Bullshit. … continue
Blog Roll
 Aletho News
Aletho News- Ceasefire for all or for none: Iran shuts Hormuz over Lebanon attacks
- Strait of Hormuz is Iran’s ‘nuclear weapon’ that forced US retreat: Medvedev
- Energy crisis will last for months – Kremlin envoy
- Europe’s quiet role in the war on Iran
- Forty days that shook the Empire: How Iran turned the tables on US and prevailed
- Netanyahu unilaterally declares Lebanon outside of ceasefire deal
- Israeli leaders: ‘Not a single goal’ achieved in war with Iran
- What on earth just happened? Trump, Iran, and the unlikely ceasefire
- Alberta Bill Would Fine Political Deepfakes $10,000 Without Satire Exemptions
- Iran declares ‘historic victory’ over US, says enemy forced to accept its proposal
- If Americans Knew
- NY Times reports how Netanyahu took the US into Iran War
- A sigh of relief over Iran, but Gaza and Lebanon in dire straits – Daily Update
- Thousands dead and neighborhoods razed to the ground: Aid agencies fear southern Lebanon is becoming the new Gaza
- The war the US is fighting for Israel could cost trillions
- ‘Cigarette Burns, Nail Wounds’: Toddler Tortured in Gaza to Coerce Father
- Trump Says US Sent ‘a Lot of Guns’ to Protesters in Iran
- Israeli forces destroy 17 UN peacekeeper cameras in south Lebanon
- US-Israeli strikes ‘completely destroy’ synagogue in Tehran
- Archbishop for US Military Says Iran War Is Unjust Under Catholic Teaching
- Iranian leaders’ Open Letters to the American People
- No Tricks Zone
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
- Devastating Assessment Of Comirnaty Vaccine By Former Senior Pfizer Europe Toxicologist
- New Study: CO2 Is ‘Effectively Negligible’ As An Explanatory Climate Change Factor Since 2000
- Former Pfizer Toxicologist Dr. Helmut Sterz Tells Bundestag Hearing Pfizer Vaccine Should Have Never Been Approved
- Energy Expert: Germany’s Nuclear Phaseout Was A “500 Billion Euro Mistake”
- New Research: South Australia’s Mid-Holocene Sea Surface Temperatures Were 4°C Warmer Than Today
