They Tried Hard NOT to Find Anything!
My recent post about scientists finding mRNA nanoparticles containing Covid vaccine genetic code, in the breast milk of vaccinated mothers, and mentioning an infant documented to have died thereof, got quite a bit of traction online.

Today, I want to look at a study from a year ago that purported to NOT find mRNA nanoparticles in breast milk. We will see why exactly the team having Bill Gates and CDC-sponsored researchers, could not find what the independent scientists could find a year later!

I decided to compare the two studies (one that found mRNA in breast milk and the other that did not) very closely and compare their methodologies using the “Modern Discontent” method.
Modern Discontent has a great post about his method, but he mostly is saying “pay close attention and understand the whole f… thing”, which is basically what I usually do with something interesting and important anyway. He posted his method three days ago, and I had my substack for a while longer. So, I intuitively used many of his approaches, but he laid them out very systematically and clearly. His article is extremely useful for all people writing about biomedical science, so take a look:
How I Tackle Reading Papers
At first sight, both studies, which I will call the 2022 shedding study (which I discussed two days ago) and the 2021 no-shedding study, superficially appear to be similarly designed. They took several lactating women and tested their milk. One study found shedding, while the other did not. Upon a closer look, the differences between these studies turned out to be extremely important!
Here’s a summary of their differences:

You can see that the study that found mRNA lipid nanoparticle shedding, was done more thoroughly. The shedding study had:
- More participants (11 vs 7)
- More milk samples were taken (131 vs 13!)
- Samples better preserved (frozen immediately)
- Samples were taken at varied moments post-vaccination including within mere hours, and also days
- Looked at very important Extracellular Vesicles
As a result of being more thorough and covering more cases, the shedding study found actual shedding! Surprise!
What if the women in the shedding study, getting the same vaccines, were analyzed using the poorer methodology of the no-shedding study?
I took the chart from the shedding study showing five women with milk samples positive for mRNA nanoparticles. I crossed out samples that WOULD NOT BE DETECTED, if the no-shedding study methodology was applied to the samples of the shedding study:

You can see that if the researchers in the shedding study used the crippled methodology of the no-shedding study, they would detect only two positive samples, instead of seven.
The methodology of the no-shedding study would miss all extracellular vesicle (EV) samples because they did not look at EVs. That is shown in the column on the right that is entirely crossed out.
The no-shedding study would also miss the 1 hour and three-hour samples because they did not take those samples (save for just ONE woman who happened not to be positive).
As a result, had the less thorough no-shedding study methodology been applied to the shedding study, only 2 positive samples, instead of 7, would be detected!
Since the actual no-shedding study collected only 13 samples and not 131 samples and used deficient methodology, no wonder they missed all positive instances!
It is as if the no-shedding study was intentionally designed not to find anything. Hmmm…
Let me give an analogy that many will understand — fishing using fishing nets.
Let’s say that a good fisherman (the shedding study) was asked to do his best job fishing to see if a particular lake has fish (mRNA nanoparticles). A bad fisherman, on the contrary, would be asked to design his fishing expedition to not catch any fish, so as to falsely prove that the lake has no fish. What would they do? This infographic shows the difference:

What’s up with Bill Gates and the CDC?
By pure coincidence, the study that did not find mRNA nanoparticles in breast milk (the no-shedding study), had key scientists sponsored by the Bill and Melinda Gates Foundation. They also received money from the CDC. You can see that Prof. Gaw and Dr. Flaherman were key participants, making the most important decisions and analyses!

Did these sponsorships influence the authors’ approach to designing the experiment? We cannot know this. We can only wonder.
Why would a fisherman try to NOT catch fish?
September 29, 2022
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular | CDC, COVID-19 Vaccine, Gates Foundation |
Leave a comment
One of the best places to raise children is The Netherlands. In several consecutive UNICEF reports the Netherlands ranked first for raising the happiest children among wealthy countries (2008, 2013, 2020). However, in the spring of 2020, The Netherlands became a harsh place for children and young people. The Dutch government adopted a one-size-fits-all policy handling the covid-19 pandemic, which did not spare the youngest and took a great toll on Dutch children. The Nobel Laureate Michael Levitt remarked that the Dutch policies would ‘set the record for worst covid-response ever.’
‘Intelligent Lockdown’
Unable to withstand the rising global panic, the Dutch government on March 16th 2020 announced an “intelligent” lockdown, a phrase coined by Prime Minister Mark Rutte.
Dutch society came to a halt. Offices, shops, restaurants and bars, libraries, sport facilities, as well as daycare centers, schools and universities were closed. The closure of schools was unexpected since the government’s official advisory group, the medics-dominated Outbreak Management Team (OMT), advised against it, for a school closure would have a minimal effect on the spread of the coronavirus.
A reconstruction of events showed that the main reason the Dutch government closed schools was that the educational field started to panic about keeping schools open. Closing schools was a political decision to follow the panic, not a medical decision. Schools supposedly closed for three weeks. Three weeks became three months. Research by The University of Oxford (Engzell, et al. 2021) shows that during the first wave the average Dutch student learned next to nothing during homeschooling. Moreover, students whose parents were not well-educated suffered up to 60% more learning losses.
School Closure ‘No Effect’
According to the Dutch equivalent of Fauci – Jaap van Dissel, chief scientist of the Dutch Health Agency (RIVM) and chairman of the Dutch OMT – the closure of schools in the spring of 2020 had “no effect.” Media, experts and politicians paid no attention to evidence though. Children were portrayed as ‘virus factories’ and schools were depicted as ’unsafe’ environments. Fear had a strong grip on the field of education and teaching unions exaggerated the risks of teachers in schools resulting in a drastic increase in safety demands.
The data was clear that not only did children not run any significant risk, but also that there was ‘no evidence that children play an important role in SARS-CoV-2 transmission.’ Still, a second lockdown would hit children. That second lockdown – now called a ‘hard lockdown’ – was announced on December 15th 2020. Schools closed again, this time advised by the OMT who had increased the number of areas it deemed itself expert on, on the basis of models, of course, proving Martin Kulldorff’s point that lab scientists are no public health scientists.
Dutch minister of Health Hugo de Jonge caused a stir by explaining this intervention was meant to coerce parents to stay at home. The international children’s rights organization KidsRights harshly criticized this policy: “The Netherlands has set a bad example internationally by closing schools during the corona pandemic to keep parents at home.” This children’s rights organization concluded that children were not a priority in Dutch corona policy and warned for the possible consequences.
As new insights on the negative impact of closing schools on children’s lives emerged, governments from countries all over the world decided not to close them again in the future. Undeterred, the Dutch government closed schools again on December 18 2021, just long enough to deny children their traditional Christmas dinner at school with their classmates, a big event in the childhood of Dutch children.
The deteriorating mental health of Dutch children was striking. The Dutch Health Authorities (RIVM) published a disturbing report which stated that more than one in five (22%) teenagers and young adults between the ages of 12 and 25 seriously considered taking their own life between December 2021 and February 2022 during the third lockdown. From happiest in the world to suicidal in a matter of three lockdowns.
Record Low in Sports Participation
Not only were schools closed by diktat. For two years, sports facilities were also repeatedly forced to close. The restrictions were constantly changing, with as a low point banning parents from watching their child play sports outdoors. Once again, there was no scientific evidence that this would help minimize the spread of the virus. The result is a record low in sports participation nationwide. The Dutch Olympic Committee and the Dutch Sports Federation (NOC*NSF) were ‘particularly’ worried by the negative effect on young people’s sports participation.
The Corona Pass
So no school and no sports. Another low point with regard to children was the corona pass (Coronatoegangsbewijs) that was mandatory from September 25th, 2021 for every Dutch citizen above 12. The corona pass was required for most social activities, such as going to the movies, attending a sports game with parents, or entering the canteen at sports club with teammates to drink tea or lemonade after the match.
Unsurprisingly, there was no scientific evidence that this intervention would reduce the spread of covid-19, but the Dutch government enforced it anyway. Crucially, the corona pass required vaccination, recovery from covid-19 or a negative result from a coronavirus test taken less than 24 hours before entry. So essentially, access to social life was used by the government to blackmail Dutch children into invasive medical procedures.
The madness continued, unsupported by evidence. At one point in time, outside playgrounds for children were closed. Parents were not allowed to enter swimming pools to dress their preschoolers before and after swimming lessons. In the winter of 2020-2021 the Dutch government even went as far as trying to regulate snowball fights, by dictating that only those from the same household were allowed to participate, and that their group could not exceed a certain number.
Neither sex nor the sea were exempt from the regulators. Young adults were advised which forms of sex were recommended, bearing the 1.5 m distance rule in mind. Drones were used to prevent people from gathering on the beach. To restrict the movements of young people even further, an evening curfew was introduced. It was not supported by any scientific explanation, just “boerenverstand” (common sense) as the advisory group OMT called it.
Restricting the lives of children and young people during the pandemic should require a great deal of evidence, as well as a risk-benefit evaluation. The Swedish government decided early in January 2020 that the measures in Sweden should be evidence-based. So it kept schools open, a decision supported by the evaluation of the Swedish Corona Commission in 2022. In Norway – where schools only closed briefly – the corona commission concluded in April 2022 that the Norwegian government had not done enough to protect children and that the measures regarding children had been excessive. The Norwegians essentially took the unethical initial decision to harm children without evidence and its authorities recognized that afterwards.
Sweden’s approach to the pandemic contains inconvenient truths for the Dutch, which is why Dutch authorities ignored the evidence from Sweden (and from Norway). As the Swedish journalist and author Johan Anderberg states in the epilogue of his book The Herd:
“From a human perspective, it was easy to understand why so many were reluctant to face the numbers from Sweden. For the inevitable conclusion must be that millions of people had been denied their freedom, and millions of children had had their education disrupted, all for nothing. Who would want to be complicit in that?”
This year, my wife and I decided to spend our summer holidays in Sweden and after two years of often doubtful restrictions in our home country, the Swedish summer and the beaches of Skåne were a breath of fresh air. As a parent and a Special Needs Education Generalist (and former teacher of Physical Education) I am greatly impressed by the path chosen by The Swedish Public Health Agency and the Swedish Government as they remained focused on the health, well-being, and education of children in the process of policy-making. Anders Tegnell and his predecessor Johan Giesecke have tirelessly advocated for not disturbing the lives of children, and they have been proven right.
A very outspoken Giesecke gave his frank opinion on Swedish television: “I am a father and grandfather myself, and I feel if children are given the opportunity to receive a good education and that the risk for me to become infected with covid-19 would increase slightly, it is worth it. Their future is worth more than my future, and it’s not just about my grandchildren, it’s about all the children.”
The successful Swedish approach shows that in many countries government policies met the criteria of child abuse. A key lesson for the future is that schools should not close again in similar circumstances. The Dutch government and the OMT failed the children of their country, a dark and shameful chapter in our history that future historians will surely not look favorably upon.
All expert knowledge and wisdom that has contributed to the health and well-being of Dutch children was thrown out of the window overnight in the spring of 2020. Children and young people were made to carry the burden in order to ‘supposedly’ protect adults.
As Sunetra Gupta and many others have stated, that is the precautionary principle turned upside down. The Danish-American epidemiologist Tracy Beth Høeg rightly condemned such policies, which were also pursued in the US, by calling them: Sacrificing children’s health in the name of Health.
After two years of closing down children’s lives, I firmly believe we owe it to children and their parents to make amends for the wrongs that were done to Dutch children. Above all, Article 3 of the Convention on the Rights of the Child should never be forgotten: “In all measures concerning children, the best interests of the child must come first.” It is mind-boggling how quickly children’s rights have gone out of the window worldwide. With disastrous consequences.
For children and young people a recovery plan should focus on repairing the damage done in education, recovering sports participation, and restoring the trust in the government and institutions that they can traditionally rely on for their health and their well-being. The Netherlands should be a safe haven for children, as it used to be. Pandemic preparedness also includes watching over children’s health and well-being and in this regard the Dutch failed their children and young people. We should do better in the future. Much better.
Dr. Hans Koppies has completed the Academy of Physical Education (ALO). He then studied Pedagogical Sciences at the VU University Amsterdam, specializing in Orthopedagogics: Families in Psychosocial Difficulties. He has worked as a remedial educationalist at various institutions in youth care and special education. He writes about growing up and raising children, parenting and counseling in articles and essays in newspapers and magazines.
September 28, 2022
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Covid-19, Human rights, Netherlands |
Leave a comment
As my beleaguered teaching colleagues and I try to get our school communities into the swing of things once again this new academic year, I find myself to be merely, powerlessly wishing that no more grotesque permutations of the Covid Madness return for a third consecutive winter. ‘Home-learning’ in particular was, of course, disastrous for children in a myriad of ways. On a purely practical level, it was fairly tricky for the teachers too, so I do believe that most of the profession hopes to avoid the insidious perfidy of forced absences or outright closures. Granted, I would prefer my colleagues to be motivated in these desires by an understanding of the abhorrent, casual neglect of children’s fundamental needs over which we were forced to preside for two years. But I’ll have to be content if the Department for Education will just let us stay open.
Belatedly, conventional wisdom has it that Covid doesn’t tend to seriously affect the school-aged population. Perhaps if the undistorted version of that truism was more widely accepted – that Covid doesn’t tend to seriously affect the healthy population – some teachers (and their unions) might find that their selfish and flawed but unending clamour for ‘more to be done’ lost its sympathisers.
It’s been a typically warm and sunny September thus far, but a small number of our students remain curiously attached to their face-coverings, sporting them lesson in, lesson out, as I look on aghast but unable to order their removal. The so-called harmless, cost-free non-pharmaceutical intervention continues to wreak its harms.
For those of us who have, by now, long fought Covid restrictions, it might feel like a further, renewed battle this Autumn to see off the prospect of the Return of the Madness. After all the hammer-blows of Spring 2020, we ordered our thoughts, picked our battles, identified our sacrifices, practised our polemics, marshalled our arguments and, eventually, took to the fray. For many of us with little or no previous experience in politicking, we may even have learnt some tricks about the art of discourse and debate along the way.
I am not referring here to my professional life of course. In my professional life I am – quite rightly – not permitted to express my personal or political ideologies or opinions to students. No good and proper teacher would dream of doing so – unless of course you suddenly, naively found that your beliefs fell in line with the government propaganda of the day. If you happened to support the mantra “Hands, Face, Space”, you could plaster it across every TV screen and vacant stretch of wall in the whole place. If you were minded to promote social distancing, or face coverings, or bubbles, or ‘don’t kill granny’, or healthy 12 year-olds giving their own consent to being tested for Covid before entering the building, or any other similar paean to the dreaded virus – exhort it from the corridors, folks! If you were an Assistant Head, you might even have the surprising chutzpah to lead a series of science-themed assemblies (to 1,200 impressionable young minds) in which you vaingloriously celebrated the disingenuous and risible proposition that Professor Sarah Gilbert’s AstraZeneca vaccine “saved 2 billion lives”.
No – when I refer to my endeavouring anew to muster awareness of the risk of restrictions this winter, I’m talking about in my personal life, away from school.
There is a danger for those of us who have resisted the mainstream Covid narrative for two-and-a-half years that we forget quite how completely and devastatingly uninterested the compliant majority are in our version of events. Many may have shifted their positions slightly, faced with ever more piles of evidence (from their own preferred sources) of the damage needlessly done. Surely, it would be hard to find someone who would embrace it all quite so gleefully all over again.
But the big arguments are not won; the wider population are still just not listening. Family members try to gently talk us down; friends tactlessly avoid the subject altogether or just silently disappear from view; some colleagues regard me warily and with increasing wryness as a bit of a crank. They all seem to manage to tell themselves that none of it really affects them and, with a special kind of inward-looking perspective, I suppose they can make that be true.
So we keep talking and waiting and wondering where the socially palatable prima facie evidence to incontrovertibly back us up and help us definitively put a stop to all this might come from. I continue to posit theories, based on my understanding of basic principles of human decency and common sense. Anecdotes, ideas and experiences should be part of our arguments and, after all, when that single piece of elusive, critical, confirmatory data lands – why should anybody ever believe what any expert says these days anyway?
Some older adults – I overhear them in crowded cafes – are delightedly and obediently getting in line for their fifth (count ‘em!) Covid jab, and some disconcerting individuals in the High Street and park remain devotedly wedded to their face-covering. They don’t seem one bit ashamed or embarrassed by the many peculiar and ridiculous things their Government forced them to do for a good while there. Is that just it for them? Over and Out, Shut Up, Move On. Are these things, this history, these awful, ungodly consequences we’re all living with, just a permanent feature of the rest of their lives, no questions asked?
There are certainly those who seemed to revel in the whole drama of it all, those who still reel performatively, sanctimoniously backwards in doorways when you dare to step near; those who complied without thought and still appear blissfully ignorant of any possibility of error or mishap or downside and who probably watch too much TV; those who spewed the new terminologies of their epoch with uneasy, faltering confidence: ‘flatten the curve’, ‘viral load’, ‘third wave’, and – my personal favourite – ‘asymptomatic’.
Is it possible that this merry, obstinate lot are the very same people who seem in recent times also to be lurching emptily but enthusiastically from one cause to another? ‘Stay Safe everyone!’ ‘Respect this virus!’, bang a kitchen pan and ‘Save the NHS!’, erect a flag and ‘Stand with Ukraine!’, buy some frozen Chicken Kievs, close everything when it’s hot and etcetera and blah, ad infinitum.
Could it be that the common thread which connects all the headline-followers, the unquestioning, the frighteningly readily compliant, is a lack of something raw, true, local, deep and meaningful in their lives? Might there be a link between the modern world’s malaise, the tragic lack of connection and community, and a very public hankering after connection and community? You don’t know your neighbour, you’re not invested in your town, you couldn’t possibly overcome the awkwardness involved in helping the elderly lady down the road – why not get your phone out instead to prove how good you are at Joining In and Helping Out?
If people don’t have a potentially perilous stake in something close, precious and valuable, or anything at all to believe in which reaches them viscerally, it seems as though they might just keep scrambling around, somewhat manically and pathetically, for Another Good Cause to get behind.
And if I’m right about all of that, then the solution to the real Covid problem lies with people and professionals who don’t know they’ve got a problem.
Get a life. Get a community. Get some meaning. And do not force a single school kid to stay at home again this year.
Fraser Krats is a secondary school teacher.
September 28, 2022
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine, UK |
Leave a comment
The Lancet recently released its long-awaited COVID-19 commission report. The report well reflects the current state of public health science and addresses the business needs of the Lancet. It may have been naïve to expect further, but health is an important area and should be taken more seriously.
The level of obfuscation of evidence, misrepresentation of prior knowledge, and disregard for diversity of scientific evidence and opinion does not reflect well on either Lancet or the commission itself.
The Lancet in context
Medicine and public health are particularly dependent on truth and transparency, as the lives and health of people cannot be entrusted to dogma and superstition. Clear and open debate is fundamental to minimizing mistakes, which can kill, and to building the trust that patients and populations need to follow guidance (as they must ultimately be the decision-makers). These two related disciplines are also increasingly lucrative for practitioners and for the companies supplying the wares they employ. These forces inevitably pull in different directions.
Private companies making these wares, such as those in the pharmaceutical industry, have a responsibility to maximize profits for their shareholders. This means encouraging more people to use their tests or drugs, rather than putting people in states of health where they do not need them (either good health, or death).
This is not an extreme position, it is a simple truth – it is how this industry is structured. If there is a wonder drug in a lab somewhere that resolves all metabolic disease with a single dose, and it is easy to manufacture and copy, then the Pharma industry would collapse. Pharma has a duty to build a market, not heal.
Transparency and truth, on the other hand, could mean admitting certain highly profitable drugs are not needed or even dangerous; that an alternative safe and cheap drug, previously available for other purposes, will be more cost-effective and lower risk.
We cannot expect private companies to state this, as it will damage or destroy their income (their business). If they do not try to block a repurposed drug that puts their own investments at risk, they would be betraying their investors. What they should do, for their investors, is overemphasize the advantage of their own product, maximize the desire of people to use them, and run public campaigns to ensure this situation is prolonged as far as possible. This is what any for-profit business does – it is their job. It is not unexpected.
We have long relied on medical journals to act as a conduit for information from researchers to medical practitioners and the public. This is a plausible model if journals are independent and the staff and owners of the journal promote truth above politics or company profit.
This was once the case; the Lancet, a subject of this article, was once family-owned and that could hold to the values of Thomas Wakley and his descendants, standing against medical authorities up to 1921. It has since been owned by other for-profit companies, now a subsidiary of a larger Dutch-based publishing conglomerate, ‘Elsevier.’
Elsevier in turn is owned by RELX group (back in London), a large company with a typical list of major institutional investors including BlackRock (and so its major owner Vanguard), Morgan Stanley and Bank of America – the same list as major pharmaceutical and biotech corporations whose products Lancet publishes on.
The above does not tell us there is intentional wrong or malfeasance, just intrinsic conflicts of interest of the type journals such as Lancet are supposed to guard against. Lancet’s ultimate ownership has a duty to shareholders to use their portfolio of assets to maximize return; on this measure alone Lancet should favor certain pharmaceutical companies. The only thing that could stand in the way is lack of competence by the owners, or a moral code that rates investors below integrity.
In this context, Lancet’s track record over COVID-19 has been checkered. In February 2020 it published a major letter on COVID-19 origins that ignored major conflicts of interest in which nearly all authors were implicated in the alternative lab origin hypothesis. It published clearly fraudulent data on hydroxychloroquine that were significant in halting early treatment studies.
A lack of early effective treatment was necessary to secure Pharma profits for later COVID-19 medications and vaccines. The later exposure of the fraud was subsequently described by The Guardian and was one of the biggest retractions in modern history.
In 2022 Lancet published a weakly-evidenced opinion advocating medical fascism; dividing and restricting people based on compliance with pharmaceutical interventions. Lancet’s top leadership has remained unchanged throughout. This is relevant context for understanding the report of the Lancet ‘commission’ on COVID-19.
The Lancet COVID-19 Commission’s Report
In mid-2020 Lancet recruited people from various aspects of public life to review various aspects of the COVID-19 outbreak. This ‘commission’ (a somewhat grand name for a privately-convened group from a private for-profit business) was headed by economist Jeffrey Sachs, who preceded the recent release of the report by publicly discussing conclusions on the potential source of SARS-CoV-2, highlighting the probability of a laboratory origin as opposed to direct animal-human spread.
This part of the commission’s investigation had been halted early when Sachs discovered that several panel members had undisclosed conflicts of interest amounting to receipt of funding to conduct the very laboratory gain-of-function research widely suspected of promoting rapid human spread. Some had been authors of the earlier Lancet origins letter.
The Executive Summary provides a foretaste of the quality of work to come, noting IHME estimates of “17·2 million estimated deaths from COVID-19,” a “staggering death toll” as the commission notes, particularly staggering as it is higher than the WHO estimates for total excess deaths throughout the pandemic period. These WHO estimates include all deaths caused by lockdowns and those where virus detection was incidental. It is an implausible figure, even ignoring the lack of context here (nearly all in late old age, and with severe comorbidities).
Ironically, the commission reports in its main text over 2.1 million excess deaths from malaria, tuberculosis and HIV arising from the COVID-19 response in 2020 alone. However, this is a misunderstanding by commission members of WHO’s actual estimates – WHO does report significant excess 2020 deaths from these diseases but not this many – though many more will accumulate through subsequent years.
Reflecting the lack of inclusiveness of the commission itself, the report recommends censorship of the alternate approaches, considering “failure to combat systematic disinformation” to be a contributor to severity. The commission then inadvertently provides an example of disinformation in its characterization of the Great Barrington Declaration, misrepresenting it as calling for “uncontrolled spread of the virus.”
This, based on the declaration itself, must be a lie, as the commission must not have read the declaration within the two years they had available. Did they not consider it pertinent to question those who wrote it or (over 900,000) signed it? Whether the declaration was correct or not, it reflected prior WHO evidence-based policy. Ignoring this is simply untenable for a serious inquiry.
The overall findings of the commission are extremely disappointing from the point of view of science, public health, and simple honesty. Its apparent lack of familiarity with prior public health norms and practice, including that of the World Health Organization (WHO), may have been genuine, or may be contrived to emphasize a narrative it was intended to support. Given Lancet’s COVID-19 track record and business imperatives, the latter would not be entirely unexpected, but it is disappointing to see adults in positions of influence producing a document of this nature.
Summary of key findings
The Report helpfully provides a three page ‘Key Findings’ section. While missing aspects of the main body such as the euphemism “prosocial behaviour” to denote social exclusion, and extolling the “logic” of the completely illogical WHO slogan for mass COVID-19 vaccination, “No one is safe until everyone is safe,” it generally captures the main thrust of the whole text. Reading the rest is however recommended to understand how modern public health thinking has so clearly gone off the rails.
The key findings are stepped through here. Anyone with a public health background is encouraged to refute the concerns raised, as many of the commission’s assertions appear to involve common traps that seem inexcusable for public health professionals. They hang heavily on a failure to grasp three fundamentals of COVID-19 and public health:
- Public health interventions are about risk and benefit. Interventions have positive and negative impacts. Recommendations therefore cannot be given without considering the potential harms they may cause in the short and long term, weighing these against perceived benefits.
- COVID-19 mortality is highly skewed towards very old age, and heavily associated with comorbidities. Therefore it is imperative to consider COVID-19 disease burden relative to other diseases in terms of life-years lost, not raw mortality (from or with) COVID-19.
- Prolonged lockdowns, workplace and school closures were not part of prior policy, or were partially recommended only in far more severe outbreaks. This is not implying the interventions were good or bad, it is just a fact that they defied public health norms and prior evidence. They were recommended against due to the harm they potentially cause. This lands most heavily, as WHO notes, on low income people and populations.
Highlights of the commission’s key findings:
“WHO acted too cautiously and too slowly on several important matters: … declare a public health emergency… restrict travel … endorse the use of facemasks…”
The commission seems unaware of the prior WHO pandemic influenza guideline. It is not among their 499 references. WHO specifically warned against restricting travel in this guideline, also noting that evidence on facemasks is “weak.” Travel restrictions can be significantly harmful to economies – cutting tourism income alone in low-income countries can increase mortality through poverty. The report fails to mention costs that extending these response measures would impose. Where lockdown costs are mentioned at all, it is in the context of costs of ‘failure’ to implement earlier or heavier, never in terms of weighing harm avoided against that caused. Ignoring relative costs, including the long-term health costs of increased poverty from longer lockdowns, is anathema to good public health policy.
Metanalyses of randomized control trials of community masking do not show significant benefit, and trials during COVID-19 show similar results. At a minimum, WHO was therefore evidence-based when recommending against community-masking – the organization is yet to provide evidence to back its later endorsement of their widespread use. The Lancet commission appears to be specifically recommending against the use of evidence-based approaches.
“… most governments around the world were too slow to acknowledge its importance and act with urgency in response….”
Most people live in low and middle income countries with low COVID-19 mortality and far higher burdens from other infectious disease, which occur in far younger people. This statement therefore seems strangely Western-centric. If they had known earlier, what would countries have actually done? (if earlier implementation of poverty-inducing responses, then for how long?)
The commission appears unaware of serological evidence of spread prior to January 2020, in some cases backed by PCR. This would negate any benefit from this recommendation, even ignoring the harms.
Citing the Western Pacific Region as an example of ‘lockdowns working’ similarly makes little sense, as comparisons elsewhere (e.g. Europe) did not show significant benefit, while in crowded slum areas they are clearly pointless. Evidence of early wide transmission (e.g Japan) indicates that low mortality was due to other factors.
“Epidemic control was seriously hindered by substantial public opposition to routine public health and social measures, such as the wearing of properly fitting face masks and getting vaccinated.”
This statement is ignorant or disingenuous. If the commission members have experience in public health, they know that quarantine of healthy people, prolonged ‘distancing’ and workplace closures were never used at scale before, and that widespread lockdowns were not ‘routine public health and social measures.’ If they did not know this, they had two years to find out. The world, including Lancet, knew by March 2020 that COVID-19 overwhelmingly targets the elderly and has little impact on healthy working-age adults.
The vaccines do not significantly reduce overall transmission – heavily vaccinated countries continue to show high transmission – so to suggest low vaccination hindered epidemic control is a vacuous statement. It may seem intuitive (e.g. it occurs with some other vaccines) but the commission had 18 months to observe COVID-19 mass vaccination.
“Public policies have also failed to draw upon the behavioural and social sciences.”
This is an extraordinary statement to use regarding COVID-19. Many Western governments have openly employed behavioral psychology in an unprecedented way in the COVID-19 outbreak. No public health campaign has ever gained such media attention or had such uniform suppression of non-official messaging from media outlets. It is strange to see a statement so removed from reality.
“Heavily burdened groups include essential workers, who are already disproportionately concentrated in more vulnerable minority and low-income communities.”
This appears to be a nod to compassion for vulnerable populations. It is true that certain groups did suffer higher rates of severe COVID-19, though these are highly correlated with rates of comorbidities (obesity in Western countries is unfortunately associated with poverty, and poverty with certain ethnic groups).
However, the burden was overwhelmingly on the elderly – to a rate several thousand times that in young people. It is the response that burdened these groups most clearly and the report does mention inequity-driving school closures, but this appears forgotten elsewhere in an apparent blind support for faster and harder lockdowns.
“In low income and middle-income countries (LMICs)… better outcomes were seen when previous experiences with outbreaks and epidemics were built upon, and when community-based resources—notably community health workers—were used to support screening and contact tracing, capacity and trust-building within communities.”
This claim appears false. Sub-Saharan African countries did well irrespective of prior experience, with a relative exception of South Africa where obesity is more prevalent and there is a higher proportion of old people. Tanzania instituted very few COVID-19 specific measures but has similar outcomes. More than half the sub-Saharan population is less than 20 years of age, an age-group with extremely low mortality in the West. Actual spread in Africa, confirmed by WHO, has been very high.
“… the support for vaccine production in LMICs, for use in those countries, has come at a great cost in terms of inequitable access to vaccines.”
Nearly all people in low and middle income countries (except perhaps China) will by now have immunity. Post-infection immunity is equal or more effective to vaccine-induced immunity. Therefore, mass vaccination of a whole population with COVID-19 vaccines that don’t significantly reduce transmission cannot plausibly provide much benefit, whilst resource diversion is harmful. This statement is therefore devoid of public health sense.
“Economic recovery depends on sustaining high rates of vaccination coverage …”
Economic recovery depends on removing impediments to a functioning economy (lockdown measures). Vaccinating immune people with a vaccine that does not stop transmission cannot help to ‘reopen’ an economy. This statement parrots official mass-vaccination messaging elsewhere, but Lancet’s commission had an opportunity to promote logic and evidence-based policy.
“The sustainable development process has been set back by several years, with a deep underfinancing of investments needed to achieve the Sustainable Development Goals.”
This is indeed clear. Poverty is worse, malnutrition is worse, and preventable disease burdens are higher. Women’s rights are greatly reduced across much of the world, and school attendance has been denied to hundreds of millions of children, entrenching future poverty. Acknowledging this is important, but it also calls into question much of the remainder of the report. Recommendations that acknowledge these mass harms which are concentrated on populations with lowest COVID-19 risk, but go on to recommend more of the interventions that caused them, do not seem well considered.
The remainder of the key findings recommend policies of mass vaccination ‘to protect populations,’ more money for the World Health Organization, and more money internationally for supporters of the growing pandemic agenda. This plays to Lancet’s gallery, but does not consider the harms of resource diversion, the actual very low mortality from pandemics over the last 100 years, or the heterogeneity of human populations and of risk to disease.
If vaccines worked in reducing mortality (for all-cause mortality (the Pfizer and Moderna randomized controlled trials have not shown this to date), if vaccination was confined to highly vulnerable groups where benefit is most likely, and if the trillions of dollars spent on lockdown compensation, mass testing and mass vaccination had been spent on chronic and endemic disease burdens and poverty mitigation, does the Commission really believe more people would have died and outcomes been worse?
A travesty of public health and science
The commission members appear convinced that lockdowns and mass vaccination were a net benefit, but It also appears that in two years of consultation they have not considered the alternative. The loss of decades of progress on infectious disease, human rights, and poverty reduction caused by lockdowns has not been given sufficient pause for thought.
A virus that mainly targets people over 75 years of age was addressed with a public health response that targets the children and the economically productive, cementing long-term poverty and inequity. They support this approach, but consider it should have been instituted earlier, and was lifted too soon.
After emphasizing mandatory and restrictive measures throughout, and misrepresenting or ignoring alternative approaches, the report ends on a note that it should perhaps have started with. “We note the timeliness of recommitting to the Universal Declaration of Human Rights, the UN’s moral charter, as we celebrate its 75th anniversary in 2023.”
This declaration includes rights to work, travel, socialize, and express opinions freely including, specifically, through any media. A quick read of the WHO’s charter would also have helped – health includes social and mental well-being (and physical well-being beyond a single disease). The report is void of such thinking – a travesty of both human rights and public health.
The report could well have been written based on slogans from WHO, Gavi and CEPI (whom the Lancet recommends should receive more money), from Pharma companies (on whose support Lancet is heavily directly or indirectly reliant) and from the World Economic Forum (who seem everywhere these days).
Some will have hoped for careful and considered thought, wide consultation, and a strong evidence base. It seems the corporate world may no longer have time for such indulgence. This is, in the end, a rich person’s club, seeking increased taxpayer funding for their favorite project. They are doing this in the name of public health.
It was reasonable to have hoped for better. What would Thomas Wakley have thought?
David Bell, Senior Scholar at Brownstone Institute, is a public health physician and biotech consultant in global health. He is the former Program Head for malaria and febrile diseases at the Foundation for Innovative New Diagnostics (FIND) in Geneva, Switzerland.
September 28, 2022
Posted by aletho |
Corruption, Deception, Science and Pseudo-Science, Timeless or most popular | Covid-19, COVID-19 Vaccine |
Leave a comment
Curing the pandemic of misinformation on COVID-19 mRNA vaccines through real evidence-based medicine

A British doctor, Aseem Malhotra, has just had a two part, peer-reviewed paper published in the Journal of Insulin Resistance. The aim of the paper was to gain a better understanding of the true benefits and potential harms of the mRNA Covid vaccines. You can read Part 1 and Part 2 in full by clicking on the links.
Dr Malhotra. a cardiologist by trade, was originally a strong Covid vaccine advocate. He volunteered in a vaccine centre, was one of the first people to be double dosed and appeared on morning television to encourage everyone to get vaccinated. He was surprised and concerned at vaccine-hesitant patients when they asked about ‘anti-vax’ propaganda.
That was until, sadly, in July 2021, his father suffered a cardiac arrest and died. His father had been the former deputy chair of the British Medical Association (BMA) and honorary vice president. The 73 year old gentleman was extremely fit and active and heart scans from a few years earlier had revealed no significant problems. Dr Malhotra was shocked to read his father’s post mortem which found that two out of three of his major arteries had severe blockages.
Aseem couldn’t explain the post mortem findings and became more concerned in November 2021 after reading a peer-reviewed abstract in Circulation Journal. In the study, the mRNA vaccine was associated with significantly increasing the risk of a coronary event within five years from 11% pre-mRNA vaccine to 25% 2-10 weeks post vaccine.
He began to question his father’s death and wondered whether the Pfizer vaccination he had received six months earlier could have contributed in some way. After six months of critically appraising the data and speaking to eminent scientists, he reluctantly concluded that, contrary to his own dogmatic beliefs, Pfizer’s vaccine was far from being as safe and effective as first thought.
Questioning the data
During his reassessment of the Covid vaccine he recalled a conversation with a cardiologist colleague who decided against vaccination due to his low personal risk and concerns about short and long term harms. His colleague was particularly alarmed that, during the trials, there had been four cardiac arrests in the vaccine group but only one in the placebo group.
Next, Dr Malhotra assessed the 95% efficacy claims. Whilst this relative risk reduction made good sales material, the true value of a treatment can only be established by looking at the absolute individual risk reduction.
This turned out to be 0.84%, in other words, in a trial of 20,000 people (10,000 in the vaccine group and 10,000 in the placebo group), 4 people in the vaccine group and 88 people in the unvaccinated group would end up testing positive for Covid. Another way to express that is that you would need to vaccinate 119 people to prevent one positive test.
This absolute risk reduction figure (0.84%) is extremely important for doctors and patients to know but how many of them were told this when they received the shot? Transparent communication of risk and benefit of any intervention is a core principle of ethical evidence-based medical practice and informed consent.
The trials did not show statistically significant reductions in serious illness or mortality and in fact there were actually more deaths (19) in the vaccine group versus the placebo group (17). Furthermore, there were only nine severe cases of Covid in the placebo group, representing 0.04%. And this was in regions specifically chosen for their high prevalence of infection.
To find protection against death, then the 119 figure above (people vaccinated to prevent one positive test) must be multiplied by the number of infections that would lead to a single death in each age group. So, Dr Malhotra calculates his rate of death from Delta was 1 in 3,000 meaning the absolute risk reduction of the vaccine protecting him from death is (1 x 3000 x 119) 1 in 357,000.
As also pointed out in a recent editorial by John Ioannidis in BMJ evidence-based medicine the inferred efficacy of the vaccine from non-randomised studies may be ‘spurious’, with bias being generated by ‘pre-existing immunity, vaccination misclassification, exposure differences, testing, disease risk factor confounding, hospital admission decision, treatment use differences and death attribution’.
What should be part of the shared decision-making informed consent discussion when any member of the public is considering taking the shot is something along these lines: Depending on your age, several hundreds or thousands of people like you would need to be injected in order to prevent one person from dying from the Delta variant of COVID-19 over a period of around three months. For the over 80s, this figure is at least 230, but it rises the younger you are, reaching at least 2600 for people in their 50s, 10 000 for those in their 40s, and 93 000 for those between 18 and 29 years. For omicron, which has been shown to be 30% – 50% less lethal, meaning significantly more people would need to be vaccinated to prevent one death. How long any protection actually lasts for is unknown; boosters are currently being recommended after as short a period as 4 months in some countries.
But how many people have had a conversation that even approaches an explanation similar to that? This is before we get into the known, unknown and as yet to be fully quantified harms.
Harms
Concerns have been raised about trial participants being limited as to the type of adverse event they could report. Furthermore, hospitalised participants were withdrawn from the trial and not reported in the final results. To make matters even worse, after two months, the FDA allowed the placebo group to be unblinded and get vaccinated, completely removing any control group with which to assess adverse events.
Dr Malhotra sticks with his field of expertise, cardiology and discusses one of the most common vaccine-induced harms, myocarditis. Whilst authorities say that myocarditis is more likely after infection than vaccination, other studies have shown the opposite. There is no evidence of myocarditis until vaccination began in 2021, a full year after millions of youngsters naturally caught Covid.
Although vaccine-induced myocarditis is not often fatal in young adults, MRI scans reveal that, of the ones admitted to hospital, approximately 80% have some degree of myocardial damage. It is like suffering a small heart attack and sustaining some – likely permanent – heart muscle injury. It is uncertain how this will play out in the longer-term, including if, and to what degree, it will increase the risk of poor quality of life or potentially more serious heart rhythm disturbances in the future.
The UK’s Yellow Card reporting system is addressed and determined to be far from adequate to cope with a rapid roll out of a brand new product. 9.7 million doses were administered before the clotting problems with AstraZeneca were detected. In Denmark, they detected the problem after only 150,000 doses.
Since the beginning of the vaccine roll-out, there have been almost 500,000 adverse events reported involving over 150,000 individuals. This shows around 1 in 120 suffer an adverse event that is beyond mild. This number is unprecedented and represents the same as the total number of reports received in the first 40 years of the Yellow Card system being active. The MMR vaccine reports around 1 in 4000 suffer an adverse event.
The paper also looks at VAERS in the US which has recorded over 24,000 deaths, 29% occurring within 48 hours of vaccination and 50% within two weeks. Before 2020 there were approximately 300 deaths recorded per year.
Of most concern is that these reporting systems are actually likely to be underestimates with one paper suggesting that only 1% of serious adverse events are ever reported to the FDA. Another analysis estimated that only 10% of serious adverse events were ever reported on the Yellow Card system.
Moreover, these reporting systems will generally miss medium and long term harms as it is more difficult to attribute to vaccination.
According to ambulance service data, in 2021 there were an extra 20,000 (20% increase) cardiac arrest calls compared to 2019 and 14,000 more than 2020 in the UK.
Similarly, a recent paper in Nature revealed a 25% increase in both acute coronary syndrome and cardiac arrest calls in the 16- to 39-year-old age groups significantly associated with administration with the first and second doses of the mRNA vaccines but no association with COVID-19 infection.
More harm than good?
One has to raise the possibility that the excess cardiac arrests and continuing pressures on hospitals in 2021/2022 from non-COVID-19 admissions may all be signalling a non-COVID-19 health crisis exacerbated by interventions, which would of course also include lockdowns and/or vaccines.
Given these observations, and reappraisal of the randomised controlled trial data of mRNA products, it seems difficult to argue that the vaccine roll-out has been net beneficial in all age groups.
Dr Malhotra concludes the first part by saying that whilst risks from vaccination remain constant, the benefits reduce over time as the virus become less virulent and variants are not targeted by outdated products. He recommends a pause and reappraisal of vaccination policies.
Pandemic of misinformation
In part 2, Dr Malhotra explores the pandemic of misinformed doctors and a misinformed and unwittingly harmed public.
According to one senior doctor in regular contact with England’s Chief Medical Officer, Chris Whitty, most of his colleagues in leadership positions influencing health policy may not have been critically appraising the evidence and were instead relying on media stories on COVID-19 and the vaccines.
He says there are four key drivers and seven sins that are the root of medical misinformation:
- Driver
- Much published medical research is not reliable or is of uncertain reliability, offers no benefit to patients or is not useful for decision makers;
- Most healthcare professionals are not aware of this problem;
- Even if they are aware of this problem, most healthcare professionals lack the skills necessary to evaluate the reliability and usefulness of medical evidence; and
- Patients and families frequently lack relevant, accurate medical evidence and skilled guidance at the time of medical decision making
- Sins
- Biased funding of research (that’s research that’s funded because it’s likely to be profitable, not beneficial for patients)
- Biased reporting in medical journals
- Biased reporting in the media
- Biased patient pamphlets
- Commercial conflicts of interest
- Defensive medicine
- An inability of doctors to understand and communicate health statistics.
There are six components essential to informed decision making: (1) description of the nature of the decision; (2) discussion of alternatives; (3) discussion of risks and benefits (in absolute terms); (4) discussion of related uncertainties; (5) assessment of the patient’s understanding; and (6) elicitation of the patient’s preference.
If the administration of the vaccine did not adhere to these principles (which is likely widespread, consistent with historical evidence), then it is also a significant breach of General Medical Council duties of a doctor to ‘give patients the information they want or need in a way that they can understand’.
The paper continues to look at institutional corruption and erosion of public trust, the failure of regulation, biased reporting in the media and censorship of legitimate scientific debate.
A hard hitting, yet sensible paper which should be read by everyone, especially doctors who lost their critical thinking skills over the last few years. Dr Malhotra is a regular on TV so will this be reported in the MSM… I doubt it.
September 27, 2022
Posted by aletho |
Science and Pseudo-Science, Timeless or most popular | COVID-19 Vaccine |
Leave a comment
During an appearance at the “Goalkeepers 2022” event, investor and philanthropist Bill Gates lamented “misinformation” that was shared about him amid the coronavirus pandemic and complained that so-called misinformation about masks and vaccines reduced compliance with mandates.
“I’d say the biggest tragedy is that it [misinformation] fragmented society where certain sources, if they told you to wear a mask, that was the last thing you were going to do,” Gates said. “Or if they told you, you know, get the vaccine, particularly to protect, reduce transmission to elderly people, they didn’t comply. It is a phenomena that held us back and hurt us in a pretty dramatic way.”
Gates also dismissed “conspiracy theories” about him wanting to track people.
“This whole tracking thing, why would I want to track you?” Gates said. “I don’t know, you know. Do I have time to track all these people?”
While Gates was seemingly referring to vaccines, just one day later, at the “Forbes 400 Philanthropy Summit,” Gates admitted that he has a group dedicated to tracking what people say about him online.
“I have a group that tracks what’s on the web that’s talking about things that connect to me,” Gates said. “Overwhelmingly during the pandemic, 95% was all the conspiracy theory stuff. It is calming down now.”
At the Goalkeepers 2022 event, Gates also complained that conspiracy theories are “cynical” and look for “one bad person who’s doing all this stuff” and welcomed “trusted sources” and “fact-checkers” partnering with social media companies to slow down the spread of content that he deems to be misinformation.
Gates’ nonprofit, The Bill and Melinda Gates Foundation, has provided hundreds of millions of dollars in funding to some of the Facebook fact-checkers whose content is used in warning labels that are appended to Facebook posts. When these warning labels are added to Facebook posts, their click-through rates decline by around 95%.
While Gates framed the debate around so-called misinformation and conspiracy theories as a tragedy that reduced compliance with the advice being pushed by trusted sources, he failed to mention that these so-called trusted sources have issued false or conflicting advice throughout the pandemic.
In the early stages of the pandemic, mainstream media outlets downplayed the severity of Covid and health officials in the US urged people to stop wearing masks, then later reversed their stance.
The theory that the coronavirus leaked from a Wuhan lab was initially dismissed as a conspiracy before so-called trusted sources finally admitted the lab leak theory was a possibility.
And health experts initially suggested that COVID-19 vaccines were up to 90% effective at preventing Covid before ultimately admitting that the vaccines don’t prevent infection.
Those who challenged or questioned the “trusted sources” were accused of spreading misinformation and censored by Big Tech platforms, even though many of their challenges and questions later turned out to be true.
September 27, 2022
Posted by aletho |
Civil Liberties, Full Spectrum Dominance, Science and Pseudo-Science | Covid-19, COVID-19 Vaccine |
Leave a comment
The battle with Big Tech for free speech is heating up! States are passing bills to stop the social media censorship, and legislators are holding investigative hearings, while a recent lawsuit including several State Attorneys General is making headway.
Suddenly, Biden announces the pandemic is over as the narrative is now collapsing from all sides. From boosters to kids shots, the vaccine push is faltering as lawsuits pile up to remove the last covid restrictions.
September 27, 2022
Posted by aletho |
Full Spectrum Dominance, Science and Pseudo-Science, Video | Covid-19, COVID-19 Vaccine, United States |
Leave a comment
Last week, The Epoch Times reported that Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention (CDC), admitted the CDC had stopped monitoring the safety of mRNA COVID-19 vaccines using a method of analysis called proportional reporting ratio (PRR).
Walensky promised to resume the monitoring.
What The Epoch Times missed is that PRR is a fraudulent measure of vaccine harm, designed by the CDC expressly for the new COVID-19 vaccines to disguise the devastation the vaccines are causing.
Why? Because PRR measures the pattern of different vaccine side effects, but it is indifferent to the number of people reporting those side effects.
If some completely new vaccine side effect appears with the introduction of a new vaccine, PRR will catch that.
But the COVID-19 vaccines are associated with huge numbers of people reporting side effects on an unprecedented scale — and, by design, PRR misses this completely.
For example, if one person in a million dies from vaccine A and one person in a thousand dies from vaccine B, then vaccines A and B can have exactly the same PRR score!
PRR is a single number that compares the variety of different side effects for a new vaccine to the variety of side effects from past vaccines.
Of course, there have been many vaccines with different side-effect profiles in the past, and it is difficult to stand out among such a diversity of profiles.
Where the new mRNA vaccines do stand out is the unprecedented number of bad outcomes, including deaths, reported to the Vaccine Adverse Event Reporting System (VAERS).
Of all the reports in the 30-year history of VAERS, two-thirds of them were from the COVID-19 vaccines, introduced in the U.S. in December 2020.
This includes three-fourths of all deaths reported to VAERS and three-fourths of all hospitalizations.
Since the introduction of the COVID-19 vaccines, reports to VAERS have skyrocketed off the charts.

Credit: OpenVAERS
These numbers represent only the reports VAERS has processed and posted. Jessica Rose, Ph.D., has reported that VAERS is months behind in posting these reports because its staff has not increased, while its workload is roughly 50 times greater since the rollout of the COVID-19 vaccines.
The sheer volume of VAERS reports, including deaths, should have set off alarm bells within weeks after the vaccines were introduced.
Reporting only PRR and not the actual count provided a convenient cover for “business as usual.”
I am grateful to Mathew Crawford for pointing this out in an article last year.
Josh Mitteldorf, Ph.D., has a background in theoretical physics. Since the 1990s, he is best known for his contributions to the biology of aging, including many articles and two books.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
September 26, 2022
Posted by aletho |
Deception, Science and Pseudo-Science, Timeless or most popular | CDC, COVID-19 Vaccine, Rochelle Walensky |
Leave a comment
A short collection of key pieces of evidence showing the COVID vaccines are not “safe and effective.” Not even close. They are the most deadly vaccines we’ve ever produced.
Here’s a high level collection of some of the most compelling pieces of evidence I’ve seen to date. This is not an exhaustive list, but just the key pieces of data that are impossible to explain if the vaccines are safe and effective.
I’ve divided the collection into sections and I’ve tried to limit each section to the most compelling data points. So don’t be disappointed if your favorite item isn’t mentioned in this article; I wanted to keep it short enough to be read..
I’ll try to keep this updated over time. It can be found in the Reference section of my Substack.
- The Pfizer trial 6 month report showed absolutely no all-cause morbidity or mortality benefit. There were no all-cause benefits at all. It was all negative. Ask your doctor why you should take a new, unproven medical intervention that is not shown to have an overall benefit. Even if there was a benefit of fewer COVID infections (which is seriously suspect due to the gaming below), the fact that the total all-cause numbers for both mortality and morbidity were negative means the intervention should not be recommended by any doctor.
- The Pfizer trial 6 month report showed that more people died (and were injured) who got the drug than who got the placebo. In other words, the cure was worse than the disease. The drug maker claimed that none of the people in the vaccine group were killed by the vaccine. They do not reveal the tests they did and explain how they were able to make that assessment. Why the secrecy here, especially in light of the study by Bhakdi and Burkhardt showing that trained medical examiners missed the causality link in 93% of the cases they looked at? The Pfizer vaccine had 4X as many cardiac arrests in the treatment group than the placebo (see page 12 of the Supplemental Appendix). This lines up very well with the numerous cardiac-related problems related to the vaccine as documented in the study by Retsef Levi and in the VAERS data which showed that the “cardiac arrest” reports were elevated by a factor of 93X higher than the annual baseline rate (VAERS reports from all vaccines combined in previous years). For some reason, the CDC wasn’t able to detect that signal (it was only 100 times higher than normal so they ignored it for some reason; they won’t let me ask them about it). In short, the claims from the manufacturer that none of the deaths were caused by the vaccine are highly suspect since all the evidence for those claims remains hidden from public view for some reason.
- The Pfizer trial 6 month report showed that at best, the drug saved only 1 COVID life per 22,000 recipients. This means that at best, after vaccinating 220M Americans, we might save 10,000 lives from COVID. But the VAERS reports show an excess death toll of well over 10,000 people and that’s before applying the minimum estimated under-reporting factor of 41. So there isn’t a mortality benefit: it’s actually the reverse. Furthermore, VAERS reports will likely only be filed for deaths in temporal proximity to the shot and is highly unlikely to report those deaths happening 5 months after the shot which appear to be the bulk of the deaths. This makes the comparison even worse. In short, we aren’t anywhere close to saving any lives at all.
- The Classen paper analyzed the clinical trial data for all three US vaccines and confirmed the lack of any overall benefit. There was an increase in morbidity which was highly statistically significant in all three vaccines. It concluded, “Based on this data it is all but a certainty that mass COVID-19 immunization is hurting the health of the population in general. Scientific principles dictate that the mass immunization with COVID-19 vaccines must be halted immediately because we face a looming vaccine induced public health catastrophe.” This is exactly right.
- The paper by Christine Stabell Benn entitled, “Randomised Clinical Trials of COVID-19 Vaccines: Do Adenovirus-Vector Vaccines Have Beneficial Non-Specific Effects?” confirmed that there was no mortality benefit by taking the COVID mRNA vaccines. “Based on the RCTs with the longest possible follow-up, mRNA vaccines had no effect on overall mortality despite protecting against fatal COVID-19.” See this article by Daniel Horowitz for more information. In other words, these vaccines have no death benefit. Period. Full stop. This is exactly what the Canadian analysis below showed.
- Serious adverse reactions, including paralysis, were not reported to the FDA and there were other very serious discrepancies in the trials. For some reason, nobody seems to be interested in exploring or explaining these very serious issues. Some are very clear cut such as the case of Maddie de Garay who was one of 1,000 kids in the clinical trial. She’s paralyzed now and has to eat with a feeding tube. The FDA and Pfizer never investigated, but reported her results as mild abdominal pain in the trial results. This is fraud. Also, there were 5 times as many exclusions in the treatment arm as in the placebo arm of the trial: 311 vs. 60. Do the p-value computation on that one and you’ll find that it could not possibly have happened by chance (1e-40). It means the trial was not blinded. Why didn’t anyone in the medical community ever point this out? Nobody will tell me.
- Pfizer admitted to clinical trial fraud in federal court. Their defense was that the FDA was in on it.
- The VAERS data, which is the official adverse event reporting system used by the US government, shows that an estimated hundreds of thousands have died and millions have been injured. If these weren’t caused by the vaccine, what caused them? Why are there more adverse events reported for these vaccines than for all other vaccines in history combined? Nobody can answer that question. See this tutorial and this recent confirmation and this article on VAERS and causality. Here’s how these numbers were calculated. Here is independent confirmation of the estimates by Dr. Naomi Wolf who used different datasets. No fact checker was interested in contacting me to challenge the facts since I always insist on recording any calls. Also, the causality of events was confirmed by the Israeli safety studies, but nobody wants to look at those.
 Can you spot the unsafe vaccine? People at the CDC don’t see any problem with this mortality chart: all the vaccines look perfectly safe.
Can you spot the unsafe vaccine? People at the CDC don’t see any problem with this mortality chart: all the vaccines look perfectly safe.
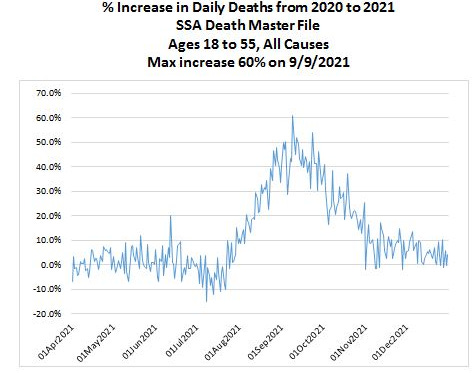
- The US Social Security Death Master File showed a 60% increase in the all-cause death rate in September 2021 vs. September 2020 for ages 18 to 55. According to the insurance companies, it wasn’t COVID. COVID kills only a small fraction of people in this age range so even if the COVID death rate doubled, it would be a minor blip on the all-cause death rate. A five month delay in death vs. vaccination was discovered in multiple countries, not just the US. Different studies found nearly identical delays. Also, I find it very troubling that the insurance companies aren’t asking the family of the policyholders who died whether they were vaccinated with the COVID vaccine and when. They don’t want to collect this information for some odd reason. So let’s be clear that a 60% increase in all-cause death rate makes this intervention extremely dangerous. I’m not aware of anything that comes close to killing people in such massive numbers. The CDC is silent on this. They don’t even want to show the public this chart:
- US disability rose dramatically soon after the vaccines rolled out (Y axis is Z-score). A 3 sigma increase is hard to explain.

- As of Sep 2, 2022, the vaccination rate in Israel is now just 2.4%. They used to be one of the world’s most vaccinated countries. Today, very few people in Israel are considered to be vaccinated. If the vaccines are so beneficial, why has nearly the entire country shifted from extremely pro-vax to extremely anti-vax in such a short period of time?

- The Israeli Ministry of Health revealed in a confidential meeting with scientists that the reason that they never notified the people of Israel about the safety issues from the vaccines was because of budget/staffing issues. Apparently, while they had millions of dollars to promote the vaccines as safe and effective, they forgot to budget for the possibility they were wrong.
- The Israeli vaccine safety data showed very clearly the side-effects are serious, long-lasting, and caused by the vaccines. Secondly, it showed that the Israeli authorities and the worldwide mainstream media are covering it all up. It also showed that US officials were not interested in seeing credible COVID vaccine safety that didn’t go along with the narrative. I tried to find out why, but nobody would talk to me. Harvard Professor Martin Kulldorff, a widely respected authority on vaccines, when asked why these people wouldn’t want to see the data, replied, “I don’t know.” This is the single most damaging report in the history of the COVID vaccines. Nobody wants to talk about it. They are hoping it will die. It won’t. Some people claim Israeli used a broad mix of vaccines, but that’s not true. Over 90% of the reports are from Pfizer, the bulk of the others are from Moderna. See also Israeli Investigators Find COVID-19 Vaccines Cause Side Effects: Leaked Video.
- The Canadian report prepared for the Liberal Party of Canada (Trudeau’s party) showed no benefit for infection, hospitalization, and death for those under 60. “The empirical evidence investigated in this report from PHO and PHAC does not support continuing mass vaccination programs, mandates, passports and travel bans for all age groups.” You can’t have a vaccine that doesn’t work in Canada work in other countries. The authors of the report had to hide their identities for fear of retribution. The statistics analyzed were those from Ontario which is not a small province (15M people). Naturally, the mainstream press ignored the report. Nobody has shown where the experts who wrote this made a mistake. The conclusion of the report is supported by independent analysis done by Mathew Crawford of the data from San Diego County, San Diego County Data Busts a Hole in Vaccine Efficacy Narrative. So apparently, the results are not limited to Ontario.
- The Harvard-Hopkins-UCSF study showed it is unethical to mandate vaccination for college students and anyone younger. The study clearly said, “University booster mandates are unethical.”
- The Thailand study did blood tests before vs. after the jab and determined that nearly 30% of young adults experienced cardiovascular injuries after the jab. How is that safe? And why didn’t anyone in the US ever do such a study? Do we not want to know? This was a simple blood test before and after the vaccine. Why did they not notify parents as soon as the study was published?
- The study by Bhakdi and Burkhardt showing 93% of deaths after vaccination were caused by the vaccine
- The data showing the vaccines cause prion diseases shortly after vaccination. This is impossible if the vaccines are truly safe. See the paper on ScienceOpen.com (after ResearchGate removed it).
- Determinants of COVID-19 Vaccine-Induced Myocarditis Requiring Hospitalization by Jessica Rose and Peter McCullough showing the myocarditis caused by the vaccine have distinct biomarkers.
- The Fraiman-Doshi paper looked at serious adverse event rates and found that the vaccines may not be as safe as has been claimed, but they cannot do a proper analysis because they are not allowed to see the data. “Full transparency of the COVID-19 vaccine clinical trial data is needed to properly evaluate these questions. Unfortunately, as we approach 2 years after release of COVID-19 vaccines, participant level data remain inaccessible.” You have to wonder: if the vaccine is so safe, why are the drug companies hiding the data?
- The Levi cardiac arrest rate elevation paper showed a troubling correlation between vaccine doses and increased cardiac events from January–May 2021. When they tried to get data after May 2021, they were refused access. This begs the question: if the vaccines are perfectly safe, what are they trying to hide?
- There are over 1,250 papers published in the scientific peer-reviewed literature showing the vaccines cause significant adverse events.
- The Walach paper found that the vaccines harm more people than they save.
- This news article published in the BMJ showed that 10 out of 100 deaths in elderly people they examined were “likely” caused by the vaccine. Funny, in America we think the number is 0. They can’t both be right. Someone should investigate why we have different results. This is very important. In fact, with a deeper investigation, over 90% of the deaths thought by medical examiners not to be caused by the vaccine were shown to be caused by the vaccine. This suggests that the US isn’t looking at the deaths.
- My colleagues and I are not misinformation spreaders according to this paper published in a peer-reviewed medical journal.
Are the Covid mRNA Vaccines Safe? was written by Harvard professor Martin Kulldorff who until recently was on vaccine committees of the FDA and CDC. He concluded:
Fraiman and colleagues have produced the best evidence yet regarding the overall safety of the mRNA vaccines. The results are concerning. It is the responsibility of the manufacturers and FDA to ensure that benefits outweigh harms. They have failed to do so.
Canadian court decisions on the constitutionality of Covid measures are invalid due to jurisdictional errors of law reviews court decisions on COVID and emphasizes the courts’ repeated over reliance on government expert testimony. Courts are supposed to find the truth and not rely on government representations or propaganda.
- The Watson et al. “modeling study”: did “COVID vaccinations” really prevent 14 million deaths? The original paper was clearly bogus since the vaccines kill more people than they save. This article examines the paper claiming the vaccines have been ridiculously effective.
There are specialized tests required to diagnose a death from the COVID vaccine.
The CDC has never told any medical examiner in the US about these tests.
So the medical examiners aren’t implicating the vaccine in any of the deaths.
The question is we know what the tests are, we know there is solid evidence from multiple countries that the vaccine causes death, yet we refuse to even consider the possibility that the vaccine caused the deaths. Why?
This paper, A Report on Myocarditis Adverse Events in the U.S. Vaccine Adverse Events Reporting System (VAERS) in Association with COVID-19 Injectable Biological Products, was retracted because the publisher didn’t like the result. So he unilaterally decided to retract the paper. This is unethical.
Here’s the “withdrawn” notice.
Here is the backstory as well as this censorship update.
The publisher hasn’t fixed the problem in over a year despite assurances it would be quickly resolved.
Here is another retracted paper that was correct:
Why are we vaccinating children against COVID-19? by Ron Kostoff
“Compared with the 28,000 deaths the CDC stated were due to COVID-19 and not associated morbidities for the 65+ age range, the inoculation-based deaths are an order-of-magnitude greater than the COVID-19 deaths!”
That is basically what I found: the vaccines kill >10X more people than the number of COVID deaths that they save. The paper passed peer review and was published. The editor of the journal quit after he was overridden by the publisher on the retraction.
The reason cited for the retraction:
- The use of key terminology, specifically the key terms “inoculation” and “vaccination” diverges from common use and are incorrect, indicating clear evidence of bias.
- Publicly available data from the United States Center for Disease Control (U.S. CDC) were concluded by the external reviewers to be misinterpreted to make the erroneous conclusion that the vast majority of reported deaths due to COVID-19 are actually due to other comorbidities. Such an egregious misinterpretation and misrepresentation are unacceptable.
This is completely bogus for two reasons:
- The editor could have easily normalized the terminology to eliminate any perceived “bias.” They simply ask the author to do a quick search and replace.
- The vast majority of COVID-19 deaths were in fact due to other comorbidities. For example, the New Mexico death records where COVID-19 was listed as the cause of death and 5 out 6 were not consistent with a COVID death. If anyone wants to challenge me on that, I have access to the death data. In Massachusetts, only 10% to 20% of the deaths listed as COVID were actually caused by COVID. Most people don’t have access to the death data, but I do. So I wonder if the journal is interested in fixing their error?
Can anyone explain how these anecdotes are possible?
- Why don’t Dr. Paul Offit (FDA vaccine outside committee) and Professor Grace Lee (Chair, CDC vaccine outside committee) want to see the Israeli safety data? They are deliberately avoiding answering the question. Why?
- In Canada, the #1 cause of death is now “unexplained.” See Deaths with unknown causes now Alberta’s top killer: province. If it isn’t the vaccine, what is causing this?
- There is data from over 1,000 vaccine injured people where 10% of the injured report 30 or more symptoms that are unique to the vaccine injured. How is that possible if the vaccine is so safe? Marsha Gee was perfectly healthy before her COVID vaccine. Less than 1 hour after her first Pfizer shot she experienced severe symptoms and experiences 78 of symptoms common with other vaccine injured. If Marsha wasn’t injured by the COVID vaccine, what caused all these symptoms?
- Why is it illegal to analyze the vaccine vials? Why hasn’t a single medical institution done an analysis of the content of the vaccines to see if there are placebos with saline solution and the amount of mRNA degradation, rendering the vaccines useless? Why the secrecy here? If we knew what was in the vaccines would this cause harm? How?
- Why are prominent people risking their careers to obtain fake vaccine cards? We know top people at Mass General Hospital have fake vaccine cards. We’ve heard that people at the highest levels of the DoD can get fake vaccine cards. It is well known that the CEO of a large pharmaceutical company bought a fake vaccine card. Why would he risk spending years in jail if the vaccines are perfectly safe?
- The Died Suddenly group on Facebook was adding users at 20,000 per day making it the fastest growing group in Facebook history. They had to throttle the growth rate due to attempts by the British military to infiltrate the group to cause it to be shut down.
- The average age of the people reported dead in the Died Suddenly group has been trending younger and younger over time. How can you explain that? The only worldwide massive intervention that goes to younger people is the COVID vaccine.
- The embalmer data (such as The Epoch Times article and this interview). These clots are not blood clots, but they are clots embalmers never saw before mid-2021 (since they take 3 months or more to form into large sizes). If the vaccines are not causing these killer clots, what is? They can be found in up to 93% of the embalming cases.
- Insurance company data from insurance companies worldwide:
- Adults Aged 35–44 Died at Twice the Expected Rate Last Summer, Life Insurance Data Suggests
- Millennials Experienced ‘84 Percent Rise of Excess Mortality’ Into Fall 2021: Former BlackRock Portfolio Manager
- Wayne Root’s wedding: 200 guests, half vaxxed, half unvaxxed. Only the vaxxed got injured (26%) or died (7%). I surveyed my readers and collected data from over 600 readers who collectively reported very similar stats. That’s hard to explain if there isn’t a huge effect.
- My neurologist stats: 11 years without needing to do a single VAERS report; this year, she needs to file 1,000 VAERS reports on 20,000 patients in the practice. How can anyone explain that if the vaccine is perfectly safe with mild, short term effects? This is similar to the 4.5% rate of neurological injury reported earlier by the Israeli Ministry of Health.
- The polling results using third party polling firms (so not my followers) consistently show that more people died from the vaccine than from the virus. The mainstream media refuses to do similar surveys and most survey firms refuse to even ask the questions.
- Ten different surveys I did all showed the vaccines are more harmful than helpful.
- Doctors in Canada died at a rate that was more than 10X normal after getting the fourth dose of the vaccine. And those are just the ones we know about.
- The fact that Paul Offit isn’t going to get the latest booster even though the CDC says he should. Why should any of us take the shot if Paul Offit is refusing to take the shot? He’s arguably the world’s most respected authority on vaccines and sits on the FDA outside advisory committee?
- Why are health authorities removing safety data on the latest shots? If they are so safe, why not release the data?
- Google searches show people became interested in topics related to vaccine safety before they became popular on social media
- When I ask data/statistics experts such as Joel Smalley and Professor Norman Fenton whether they’ve seen any credible data proving the vaccines are safe and effective, they are unable to cite a single reference.
- A local news station (WXYZ-TV) asked people to report on unvaxxed loved ones that became sick and died and instead they got hammered with hundreds of thousands of people saying they lost loved ones to the jab. See my video on the WXYZ-TV story and also this video.
- Woman collapses and dies 7 minutes after Booster shot… The stunning thing is the Twitter video documents that the pharmacy workers have been instructed to not bring it up when briefing patients and, if asked, not to comment on the death. Do you think they are looking out for your best interest by withholding adverse events like death 7 minutes after the shot from the public? That should never happen. Have you ever seen a video like this before the COVID vaccines rolled out? The death was ruled as “natural causes” which means it was from internal organ failure as opposed to being hit by a truck. However, the internal organ failure was due to an external event (vaccinated).
- Turbo-cancer is being reported now. It’s impossible to explain. Never been seen before.
- A reader wrote: I work in the financial services industry in Toronto. A co-worker of mine was recently diagnosed with cancer. He has been getting treated at Sunnybrook hospital for it. The doctors there told him they’ve seen a significant spike in cancer cases well above what could be explained by people missing getting screened due to the pandemic. What’s more though is that they catalogue the vaccine status of every cancer diagnosis and the spike in the number of cases is only occurring in those who are vaccinated– apparently they are researching it to try and find out why the vaxed have seen a spike in cancers vs the unvaxed who haven’t- obviously they are not ready to go public with this but they know about it and are researching it fwiw
- Turtles all the way down: Vaccine science and myth shows the vaccines are not nearly as safe as people think. This is the most damaging book ever written showing the safety of the vaccines is highly questionable. There isn’t a single risk-benefit trial on all cause mortality and morbidity vs. placebo for any of the 70 approved vaccines even though they’ve had 60 years to do this. If the vaccines are truly beneficial, why do you think it’s never been done for any vaccine? A team of Israeli scientists wrote this book over 5 years. It was recently translated into English and is available through purchase on Amazon.
- Dissolving Illusions: the history of vaccines shows they did a lot less than people think; probably next to nothing.
- The Real Anthony Fauci: illustrates the corruption in the medical community today. For example, they created a more accurate adverse event reporting system (ESP:VAERS) system and then scrapped it after it showed all the vaccines were unsafe.
- Vaccine Secrets: a 20 minute slide presentation from CHD
- The CCCA presentations:
- Stop the shots,
- More Harm Than Good
- Dispelling the Myth
- My mega-presentations:
- What I learned during the pandemic
- The elephant in the room
- Vaccine Policies
- Vaccine Essentials
- All you need to know
- Things you need to know
- 180 questions they can’t answer
Once I established a policy of always recording calls with “fact checkers,” I’ve not had a single call from them trying to refute anything I’ve written.
None of the drug companies that make these products will refute anything I’ve written or supply a representative to debate me or any of my colleagues in a live debate. They have immunity from liability and they are not willing to be held accountable in the court of public opinion either.
- The COVID lies by Dr. Michael Yeadon
This was a very well done study, but it is of course attacked by the pro narrative people. We’d love to have an open debate about this study, but the other side doesn’t want to talk about it in a neutral forum.
A LITERATURE REVIEW AND META-ANALYSIS OF THE EFFECTS OF LOCKDOWNS ON COVID-19 MORTALITY
Masks don’t work at all. See this article which has plenty of references. If anything, masks are more likely to hurt you than to benefit you.
There is no study at all on the 6 foot distance rule. They just made that one up.
Professor Jeffrey Sachs was tasked by The Lancet to lead an independent investigation into the source of the SARS-CoV-2 virus. After he determined it came from US biotechnology, all of a sudden nobody wanted to pursue the investigation any further.
Tony Fauci gets paid every time you get a Moderna shot. He won’t disclose how much he makes and you can’t get via FOIA (it’s blacked out). If the Republicans get control of the Senate, that will change. Watch this video from Sept 20, 2022 of Rand Paul commenting on this as well as the well founded accusation that Fauci created the virus in the first place and then desperately tried to make it look like it came from nature after top scientists said it was a lab leak (watch the video at 2:00 onwards). Rand Paul called it, quite rightly, “the biggest cover-up in the history of science.”
The question you have to ask yourself is why is Fauci keeping his funding of the gain of function research and also his compensation for each vaccine dose a secret?
Tony Fauci was the primary reason that all early treatments were ignored by the government. It appears he did that because it would cut into his revenue stream.
Early in the pandemic, two physicians, George Fareed and Brian Tyson, developed a treatment protocol using a variety of safe, low cost drugs and supplements with little to no side effects that had a near 100% success track record in preventing hospitalization, death, and long haul COVID if the patient started treatment shortly after realizing they were infected. They’ve treated over 10,000 patients. They wrote a best-selling book about it.
Today, more than two years later, the FDA and the CDC have not returned their calls.
- Why can’t we have open forums where our public health officials can be challenged by experts who disagree? Is there proof that having open debate results in worse outcomes?
- Why doesn’t anyone want to see the Israeli safety data?
- Why isn’t anyone asking for Fauci’s unredacted emails?
- Is there a scientific reason that the CDC is ignoring me and all the experts I work with?
- Questions I’d love to ask Congresswoman Anna Eshoo… that she’ll never answer
- Why hasn’t anyone calculated the minimum VAERS under-reporting factor (URF)?
- Did the propensity to report change in 2021 vs. previous years. What is the new number in 2021 and 2022 compared to previous years? How did you calculate it?
- Why do John Su and Tom Shimabukuro never talk about the URF in the ACIP meetings?
- There were over 14,000 excess deaths reported in VAERS. That’s before the URF is applied. If these weren’t caused by the vaccine, what caused them?
- If these vaccines are so safe, why are there more adverse events reported for these vaccines than for all other vaccines in history combined?
- I found thousands of adverse events that are elevated by these vaccines compared to all other vaccines combined in previous years. How many adverse events did the CDC find?
- There was a dramatic rise in adverse events reported in the VAERS system for the COVID vaccines. How could this not be a serious safety concern? The propensity to report did not increase. If you believe the propensity to report did increase, what data do you have to support that?
- My neurologist has been in practice for 11 years. She has 20,000 patients in her multi-physician practice. In that time, she’s never had to report a single event to VAERS. With the COVID vaccines, she now needs to make 1,000 reports. If the vaccines are safe and effective and most all the symptoms are mild and short term, how do you explain this? Her event rate similar to the 4.5% injury rate that the Israeli MoH found. So her reporting rate is more than 10,000 times higher than for any other vaccine. Couldn’t that be the explanation for the higher rate of VAERS reports? Doesn’t this suggest that the propensity to report is much lower this year because there are so many more events and doctors simply don’t have the time to report them all?
- The NEJM pregnancy paper by Tom Shimabukuro noted that the results on safety for pregnant women was preliminary since many of the women were still pregnant. What was the final result and why wasn’t it published?
- There was an analysis of the VAERS data by Hannah Rosenblum published in the Lancet. It never goes into explaining why there were elevated reporting rates and also the nature of the reported events are not normal background events. Couldn’t the elevated reporting rates be caused by a dangerous vaccine? Does she want to look at the Israeli safety data? If not, why not? The Israeli data directly contradicts the conclusion of the paper. Shouldn’t we figure out which conclusion is correct?
- Why does Carol Crawford not answer my questions about an open discussion with the top vaccine misinformation spreaders to resolve our differences and reduce vaccine hesitancy?
- Why does Martha Sharan ignore my emails and phone messages when I attempted to ask for permission to talk to the authors of the Rosenblum paper? Can’t she reply with the reason questions are not allowed?
Questions I’d love to get the answer to. These were asked, but never answered.
- Why did the CDC never publish the follow up on the NEJM pregnancy paper by Tom Shimabukuro?
- The CEO of Moderna was asked how the 19 nucleotide sequence from a Moderna patent got into the SARS-CoV-2 genome. That sequence is never found in a virus. How did it get in this one? The CEO said he’d look into it, but never reported the explanation. I’d love to know what it was.
- Why hasn’t any Democratic committee chairman asked the NIH for Tony Fauci’s unredacted emails? Don’t we want to know the truth about whether there was a deliberate cover-up? If there was, shouldn’t Fauci be fired?
- Fauci wasn’t supposed to be funding gain of function research but he was. How is he being held accountable?
- How much is Fauci making every time someone gets a Moderna shot? He’s a public official… Why is this a secret?
People who disagree with the mainstream narrative are rewarded with censorship, permanent bans on posting on social media, demonetization of your YouTube account, revocation of your medical license, revocation of your medical certifications, loss of hospital privileges, loss of job, loss of funding, loss of friends, and a Wikipedia entry labeling you a “misinformation spreader” and/or “conspiracy theorist.”
This is a problem. I am not aware of any paper published in the medical literature that shows that such tactics result in better health decisions.
Should we use the same rules at the UN when nations disagree? Do you think that will result in better outcomes?
The way people resolve differences is by confronting the issues and talking through them. But we are not doing this:
- Why can’t we find anyone who will defend the CDC, FDA, and NIH on camera?
- Dr. Byram Bridle and 2 colleagues challenged Canada’s health authorities to a debate
- Vinay Prasad’s most important op-ed
- The head of the CDC’s outside committee on vaccine safety does not want to see the safety data collected by the Israeli Ministry of Health.
This is objective proof of a broken system. It is indefensible. Caught on video camera. There is no reason that anyone in a position of authority on the COVID vaccines would refuse an opportunity to see the most thorough post-vaccine safety study ever done: one that shows causality of serious adverse events.
From Israeli Investigators Find COVID-19 Vaccines Cause Side Effects: Leaked Video:
Rechallenge changes a causal link “from possible to definitive,” Dr. Mati Berkovitch, head of the research team and a pediatric specialist, said at the meeting.
and
Many of the reported adverse events were found to be long-lasting, which researchers said in the meeting was surprising since the brochure handed to vaccine recipients says otherwise. They also said Pfizer officials told them that Pfizer did not know of any long-lasting symptoms.
and
In the official report later issued to the public, the MoH did not detail how researchers were caught off guard by the duration of the events and side effects. The health agency also stated that there were no new events identified.
It concludes:
The choice to omit some of the crucial findings discussed in the meeting from the public report is “a recipe to destroy” the entire vaccine program, according to Levi, an Israeli native and an expert in risk management.
“The more pro-vaccine, the more disturbed you need to be from something like this,” Levi told The Epoch Times. “And the reason is that the two most important enablers for vaccine programs … to be successful is trust and transparency, that you actually communicate to people the real risk-benefits and allow them to make choices about what they want to do. The second thing is that you take care of the people that were harmed by the vaccine because no vaccine has 100 percent safety.”
“I think we have in this example … where we violate these two very important principles,” he added. “This is a recipe to basically destroy all vaccine programs, so the more pro-vaccine you are, you should be more disturbed by this.”
How can you have the chair of a safety committee not interested in seeing important safety data? Professor Grace Lee should be removed from her position by the CDC. Why isn’t she? Does anyone care?
Why does Dr. Paul Offit ignore requests to see the same data?
According to the Epoch Times article, everyone declined to comment on the story: the scientists, the MOH officials, and the CDC’s Immunization Safety Office declined to comment on the Israeli findings.
If the above isn’t enough, there are hundreds more “hard to explain” data points.
- List of over 1,200 papers published in peer-reviewed scientific journals
- The safe and effective narrative is falling apart
- Think we got it wrong?
- How the authorities can INSTANTLY stop the spread of “COVID misinformation”
- Examining COVID Vaccine Efficacy
There is an excellent article written in August 2020 by Norman Doidge entitled “Medicine’s Fundamentalists” which talks about the “all-available-evidence approach.” It should be read by every doctor in America. This is how medical science should work.
The precautionary principle medicine seems to have been thrown under the bus during the pandemic. It says in the face of uncertainty, one should take reasonable measures to avoid threats that are serious and plausible.
For example, the Pfizer clinical trial showed the vaccine saved only one COVID death per 22,000 injected. That means we might only save around 10,000 lives if we inject 200M Americans. So if VAERS, which is at least 41 times under reported, is showing over 12,000 deaths associated with the vaccine, any reasonable person should say that killing more than 41 people to save 1 life is nonsensical… shouldn’t we put a PAUSE on this intervention until we resolve the uncertainty?
In the current system, questioning the CDC or other authorities results in serious retribution as mentioned earlier.
Is that really the right way to handle scientific dissent?
Are the vaccines “safe and effective” as claimed?
To answer this, science requires that we look at all the available data and see whether the data is more consistent with the hypothesis of “safe and effective” or “not safe and effective.”
All the data that I and my colleagues have seen end up being placed in the “not” bucket.
We are open to being shown we got it wrong on the hundreds of pieces of evidence we have examined, but nobody is willing to discuss the data with us to resolve the issue, not even for $1M dollars.
I even went to extraordinary lengths to offer the Israeli safety data to ACIP Chair Grace Lee. Her response: she called the police on me. That pretty much tells you everything you need to know: they simply refuse to look at any data that goes against their currently held beliefs. That’s the way science works.
September 26, 2022
Posted by aletho |
Book Review, Science and Pseudo-Science, Timeless or most popular, War Crimes | Covid-19, COVID-19 Vaccine, United States |
Leave a comment

Twenty years ago, the “Cheney-Bush junta” — as Gore Vidal called it — launched its propaganda campaign to invade Iraq, effectively casting the dye for much of the historic period since.
On Sunday, Sept. 8, 2002, the New York Times ran on its front page the story “U.S. Says Hussein Intensifies Quest for A-Bomb Parts” by Michael Gordon and Judith Miller.
The same day, then Vice President Dick Cheney appeared on Meet the Press with Tim Russert, hyping the New York Times story as evidence that Hussein was attempting to acquire “the kinds of tubes that are necessary to build a centrifuge and the centrifuge is required to take low-grade uranium and enhance it into highly-enriched uranium which is what you have to have in order to build a bomb.” Colin Powell and Condoleezza Rice followed Cheney’s lead on other shows.
In 2005, I confronted Miller about her reporting, asking her at if she would name the anonymous lying source who she allegedly relied on to falsely report “the best technical experts and nuclear scientists at laboratories like Oak Ridge supported” the CIA claim that the tubes were for a nuclear weapons program. In fact, it would later be established, the nuclear scientists did not support such an assessment and were effectively muzzled. When I questioned her, Miller refused to name the source that fed her this false information and Marvin Kalb, the moderator of the event, see video, ran interference, stopping further follow-ups. (See my piece “Should Media Expose Sources Who Lied to Them?”)
Many serious analysts early on deduced that the source was Cheney himself, likely through his chief of staff, Scooter Libby.
Even the mainstream Bob Simon of CBS would later remark to Bill Moyers about Cheney: “You leak a story, and then you quote the story. I mean, that’s a remarkable thing to do.”
Remarkable is actually an understatement. It’s engaging in a de facto conspiracy to deceive the U.S. public into war.
In April of 2020, a journalist asked at the daily White House press briefing: “Mr. President, I wanted to ask Dr. Fauci: Could you address these suggestions or concerns that this virus was somehow manmade, possibly came out of a laboratory in China?”
Anthony Fauci replied: “There was a study recently that we can make available to you, where a group of highly qualified evolutionary virologists looked at the sequences there and the sequences in bats as they evolve. And the mutations that it took to get to the point where it is now is totally consistent with a jump of a species from an animal to a human.”
What Fauci was talking about was the piece “The proximal origin of SARS-CoV-2” in Nature Medicine.
That article was widely accepted by the major media as eviscerating the possibility of lab origin of Covid, shutting down debate at that critical time and continuing to hinder it to this day.
The thing is, Fauci seems to have had a serious role in that article’s appearing.
One of the few people objecting to the piece when it was first published, in the Spring of 2020 was Meryl Nass, who asked: “Why are some of the US’s top scientists making a specious argument about the natural origin of SARS-CoV-2?” She would go on to argue that the signers of the Nature Medicine article were pushed to write it.
In 2021, limited Freedom of Information Act findings showed that Fauci had at minimum effectively coordinated with the named authors of the Nature Medicine article. See Nass’ write-up and subsequent reporting by some mainstream outlets such as USA Today.
Thus, this insidious tactic of helping to plant a story pushing the line you want in a media outlet and then citing it as evidence for your case was employed by both longtime creatures of Washington at historic junctures.
There are other notable parallels. Both Fauci and Cheney have also both been leading beneficiaries of Trumpwashing.
Ashley Rindsberg makes some serious arguments in his piece, “How Dick Cheney created Anthony Fauci,” including about the buildup of US bio“defense” after 9/11 (actually the anthrax attacks) — a trend several observers have noted. Alexis Baden-Mayer traces such arguments back to 1976, when Cheney and Donald Rumsfeld apparently pressured President Ford to order massive inoculations in the Swine Flu scare, which he would be widely mocked for.
While the antiwar forces and “left” criticism of the Iraq WMD propaganda were wholly inadequate, they at least manifested themselves on the national stage to some extent. Covid origins has hardly been recognized as an antiwar issue by most and the “left” at times has actually played a detrimental role, explicitly doing the establishment’s bidding in irrationally denying or minimizing the possibility of lab origin of the pandemic.
One thing that should be kept in mind as one parses through the claims and “exposés” is that some are de facto cover stories.
The Bush administration ramped up their propaganda campaign for the Iraq invasion, as noted at the beginning of this article, in September of 2002.
Why then? Sophisticates at the time would quote Andrew Card: “From a marketing point of view, you don’t introduce new products in August” said Bush’s chief of staff.
With the Bush administration cynically using the one year anniversary of 9/11 as a backdrop to launch their push for invading Iraq, the rationale articulated by Card was actually a remarkably benign motivation, a likely cover, in comparison to the war makers actual thinking.
September 26, 2022
Posted by aletho |
Deception, Fake News, Mainstream Media, Warmongering, Science and Pseudo-Science | Anthony Fauci, Covid-19, United States |
Leave a comment
In the face of incessant media badgering to rush out and take the latest version of experimental coronavirus “vaccine” shot — the “bivalent” booster, the vast majority of Americans are saying “nope” and continuing on with their lives. Three weeks into the all-out push to have every American over 12 years old take the new shot (giving these new booster shots to younger children is up next), it appears that less than two percent of eligible Americans have done so.
The growing resistance to the coronavirus shots pushers’ propaganda gives one hope for America. With each new experimental coronavirus shot Americans are being urged to take, the percentage who acquiesce declines. The line that the shots are needed, safe, and effective has proven a farce on all counts. And the latest shot rushed into distribution has taken the previous shots’ mockery of the process for ensuring safety and efficacy to the next level. The truth is out there; increasingly Americans are seeing past the media hype and finding it.
September 26, 2022
Posted by aletho |
Science and Pseudo-Science | COVID-19 Vaccine, United States |
Leave a comment
Online fact checkers have great authority over what speech gets suppressed on mainstream social media platforms and a fact-check of a post on Facebook can result in that post being suppressed by as much as 95%.
Yet, despite their great power over what people can say, fact checkers are also increasingly frustrated at calls for more transparency about the way they operate and say they are being bombarded with freedom of information act (FOIA) requests and lawsuits.
The fact checkers say these requests and lawsuits are meant to drain the resources of climate change researchers and to discourage them from doing their work which is, in turn, an attempt to shut down their own speech.
“They make a point of going after the fact-checkers because, in addition to stopping regulation, they also want to prevent or discourage climate scientists from doing things that might educate the public,” said Lauren Kurtz, Climate Science Legal Defense Fund’s executive director to Bloomberg.
Kurtz’s organization provides climate researchers with legal assistance. They assist about 40 researchers annually. But this year has been busier, as they have already assisted 35 people.
One of the beneficiaries of the fund is Doug MacMartin, who was sued by Dane Wigington after he fact-checked his documentary “The Dimming,” which, according to MacMartin, is filled with conspiracy theories.
On the science fact-checking website Climate Feedback, used by social media companies to flag what it sees as science misinformation, MacMartin described Wigington’s documentary as “pure fantasy.” The plaintiff sought $75,000 in damages from MacMartin, arguing that the fact-check reduced the visibility of his documentary on Facebook, hurting its revenue.
“I mostly felt disbelief,” MacMartin recalled to Bloomberg. “A bit of shock combined with, ‘I just don’t have time for this.’”
Earlier this month, a federal court dismissed Wigngton’s lawsuit, but he plans to appeal.
Daniel Swain, a climate researcher at University of California, Los Angeles, had to deal with a FOIA request filed by a group called Energy Policy Advocates. Swain is vocal about droughts and fires in Western US. The requests sought text messages, encrypted messages, and emails related to a fact-check written by Swain and others about the book “Unsettled: What Climate Science Tells Us, What It Doesn’t, and Why It Matters,” by Steven Koonin, who worked in the Department of Energy during Obama’s era.
Swain challenged the requests using a university lawyer, arguing that it had the “presumptive intent of disrupting primary research and outreach activities by inundating climate scientists.” The records department said that the motivations of the requester were irrelevant, but was bound by law to provide the information requested.
“I spend nights and weekends compiling and going through thousands and thousands of emails because these requests are extremely broad,” he said. “In some cases they’re essentially open ended: they’re asking about multiple years, multiple keywords and multiple platforms.”
The group filing most of the requests are Government Accountability and Oversight, and Energy Policy Advocates. The two groups go by the acronyms GAO and EPA, the same acronyms used by federal agencies Government Accountability Office and the Environmental Protection Agency.
Climate Feedback and Meta are facing a $2 million lawsuit filed by Libertarian commentator John Stossel who was censored on Facebook as a direct result of a post by the fact-checker.
Climate Feedback flagged Stossel’s video “Government Fueled Fires” about the wildfires in California in 2020. The fact-check resulted in Facebook limiting the visibility of the video and we have more information on that case here.
September 25, 2022
Posted by aletho |
Full Spectrum Dominance, Science and Pseudo-Science | Facebook, United States |
Leave a comment