US children suffer sharp drops in test scores
Samizdat | September 1, 2022
Student test scores in US elementary schools have dropped to levels not seen in decades, marking an historic educational setback that observers have blamed largely on classroom shutdowns during the Covid-19 pandemic.
The latest National Assessment of Educational Progress (NAEP), released on Thursday, showed that reading scores dropped the most since 1990, and math scores fell for the first time in the five-decade history of the study. The declines between 2020 and 2022 wiped out decades of progress in math and reading proficiency.
The report, also known as the “Nation’s Report Card,” marks the first national assessment comparing test results before the pandemic with current performance. It’s based on tests taken by 9-year-olds in early 2022 and early 2020 – just before most of America’s schools were shut due to Covid-19.
Children were deprived of in-person learning for more than a year in some cities. New York City schools, for instance, weren’t fully reopened until 18 months after their first Covid-19 lockdown. In Los Angeles, parents sued the teachers union and schools for “holding children hostage” to their political agenda. Among other demands, the union insisted that police be defunded and new wealth taxes be imposed before they returned to classrooms.
“Actual science didn’t support school closures,” said US Representative Guy Reschenthaler, a Pennsylvania Republican. “Democrats were too busy following political science to care. We lost decades of gains in reading and math scores as a result.”
However, the school closings weren’t the only cause of declines in test scores, said Peggy Carr, commissioner of the National Center for Education Statistics. “Our own data reveal the pandemic’s toll on education in other ways, including increases in students seeking mental health services, absenteeism, school violence and disruption, cyberbullying, and nationwide teacher and staff shortages.”
Children who were already struggling with reading and math suffered the biggest setbacks in proficiency. While the average reading score fell by five points from 2020’s level, the decline was twice as severe for students at the 10th percentile, meaning those who performed worse than 90% of the class. The same trend was evident in math scores, with the overall average falling seven points and the 10th percentile dropping 12 points.
It Was Birx. All Birx.

BY DEBBIE LERMAN | BROWNSTONE INSTITUTE | AUGUST 31, 2022
In two previous articles, I looked into the shady circumstances surrounding Deborah Birx’s appointment to the White House Coronavirus Response Task Force and the laughable lack of actual science behind the claims she used to justify her testing, masking, distancing and lockdown policies.
Considering all that, the questions arise: Who was actually in charge of Deborah Birx and whom was she working with?
But first: Who cares?
Here’s why I think it’s important: If we can show that Birx and the others who imposed totalitarian anti-scientific testing, masking, social distancing, and lockdown policies, knew from the get-go that these policies would not work against an airborne respiratory virus, and nevertheless they imposed them FOR REASONS OTHER THAN PUBLIC HEALTH, then there is no longer acceptable justification for any of those measures.
Furthermore, whatever mountains of post-facto bad science were concocted to rationalize these measures are also completely bunk. Instead of having to go through each ridiculous pseudo-study to demonstrate its scientific worthlessness, we can throw the whole steaming pile in the garbage heap of history, where it belongs, and move on with our lives.
In my admittedly somewhat naive optimism, I also hope that by exposing the non-scientific, anti-public-health origins of the Covid catastrophe, we may lower the chances of it happening again.
And now, back to Birx.
She did not work for or with Trump
We know Birx was definitely not working with President Trump, although she was on a task force ostensibly representing the White House. Trump did not appoint her, nor did the leaders of the Task Force, as Scott Atlas recounts in his revelatory book on White House pandemic lunacy, A Plague Upon Our House. When Atlas asked Task Force members how Birx was appointed, he was surprised to find that “no one seemed to know.” (Atlas, p. 82)
Yet, somehow, Deborah Birx – a former military AIDS researcher and government AIDS ambassador with no training, experience or publications in epidemiology or public health policy – found herself leading a White House Task Force on which she had the power to literally subvert the policy prescriptions of the President of the United States.
As she describes in The Silent Invasion, Birx was shocked when “at the halfway point of our 15 Days to Slow the Spread campaign, President Trump stated that he hoped to lift all restrictions by Easter Sunday.” (Birx, p. 142) She was even more dismayed when “mere days after the president had announced the thirty-day extension of the Slow the Spread campaign to the American public” he became enraged and told her “‘We will never shut down the country again. Never.’” (Birx, p. 152)
Clearly, Trump was not on board with the lockdowns, and every time he was forced to go along with them, he became enraged and lashed out at Birx – the person he believed was forcing him.
Birx laments that “from here on out, everything I worked toward would be harder—in some cases, impossible,” and goes on to say she would basically have to work behind the scenes against the President, having “to adapt to effectively protect the country from the virus that had already silently invaded it.” (Birx, pp. 153-4)
Which brings us back to the question: Where did Birx get the nerve and, more mysteriously, the authority to so blithely act in direct opposition to the President she was supposed to serve, on matters affecting the lives of the entire population of the United States?
Atlas regrets what he thinks was President Trump’s “massive error in judgment.” He argues that Trump acted “against his own gut feeling” and “delegated authority to medical bureaucrats, and then he failed to correct that mistake.” (Atlas, p. 308)
Although I believe massive errors in judgment were not unusual for President Trump, I disagree with Atlas on this one. In the case of the Coronavirus Response Task Force, I actually think there was something much more insidious at play.
Trump had no power over Birx or pandemic response
Dr. Paul Alexander, an epidemiologist and research methodology expert who was recruited to advise the Trump administration on pandemic policy, tells a shocking story in an interview with Jeffrey Tucker, in which bureaucrats at the Department of Health and Human Services (HHS) and lawyers from the Justice Department told him to resign, despite direct orders from President Trump and the White House: “We want you to understand that President Trump has no power,” they reportedly told Alexander. “He cannot tell us what to do.”
Alexander believes these bureaucrats represented the “deep state” which, he was told repeatedly, had decided first not to hire or pay him, and then to get rid of him. Alexander also writes in an upcoming exposé that the entrenched government bureaucracy, particularly at the NIH, CDC, and WHO, used the pandemic response to doom President Trump’s chances for reelection.
Was the entire anti-scientific totalitarian pandemic response, all over the world, a political maneuver to get rid of Trump? It’s possible. I would contend, however, that the politics were only a sideshow to the main event: the engineered virus lab leak and coverup. I believe the “deep state” Alexander repeatedly butted up against was not just the entrenched bureaucracy, but something even deeper and more powerful.
Which brings us back to deep state frontwoman Deborah Birx.
After lamenting Trump’s delegation of authority to “medical bureaucrats,” Scott Atlas also hints at forces beyond Trump’s control. “The Task Force was called ‘the White House Coronavirus Task Force,’” Atlas notes, “but it was not in sync with President Trump. It was directed by Vice President Pence.” (Atlas, p. 306) Yet, whenever Atlas tried to raise questions about Birx’s policies, he was directed to speak with Pence, who then failed to ever address anything with Birx:
“Given that the VP was in charge of the Task Force, shouldn’t the bottom-line advice emanating from it comport with the policies of the administration? But he would never speak with Dr. Birx at all. In fact, (Marc) Short [Pence’s chief of staff], clearly representing the VP’s interests above all else, would do the opposite, telephoning others in the West Wing, imploring friends of mine to tell me to avoid alienating Dr. Birx.” (Atlas, p. 165-6)
Recall that Pence replaced Alex Azar as Task Force director on February 26, 2020 and Birx’s appointment as coordinator, at the instigation of Asst. National Security Advisor Matt Pottinger, came on February 27th. Subsequent to those two appointments, it was Birx who was effectively in charge of United States coronavirus policy.
What was driving that policy, once she took over? As Birx writes, it was the NSC (National Security Council) that appointed her, through Pottinger, and it was her job to “reinforce their warnings” – which, I continue to speculate, were related to the accidental release of an enhanced pandemic potential pathogen from a US-funded lab in Wuhan.
Trump was probably made aware of this, as evidenced not just by his repeated mentions, but by what Time Magazine called his uncharacteristic refusal to explain why he believed it. The magazine quotes Trump saying “I can’t tell you that,” when asked about his belief in the lab leak. And he repeats, “I’m not allowed to tell you that.”
Why in the world was the President of the United States not allowed to override AIDS researcher/diplomat Birx on lockdown policies nor explain to the public why he believed there was a lab leak?
The answer, I believe, is that Trump was uncharacteristically holding back because he was told (by Birx, Pottinger and the military/intelligence/biosecurity interests for whom they worked) that if he did not go along with their policies and proclamations, millions of Americans would die. Why? Because SARS-CoV-2 was not just another zoonotic virus. It was an engineered virus that needed to be contained at all costs.
As Dr. Atlas repeatedly notes with great dismay: “the Task Force doctors were fixated on a single-minded view that all cases of COVID must be stopped or millions of Americans would die.” (Atlas, p. 155-6) [BOLDFACE ADDED]
That was the key message, wielded with great force and success against Trump, his administration, the press, the states, and the public, to suppress any opposition to lockdown policies. Yet the message makes no sense if you believe SARS-CoV-2 is a virus that jumped from a bat to a person in a wet market, severely affecting mostly people who are old and debilitated. It only makes sense if you think, or know, that the virus was engineered to be especially contagious or deadly (even if its behavior in the population at any given moment might not justify that level of alarm).
But, again, before indulging in more speculation, let’s get back to Birx. Who else did she (and her hidden handlers) bulldoze?
She dictated policy to the entire Trump administration
In his book, Atlas observes with puzzlement and consternation that, although Pence was the nominal director of the Task Force, Deborah Birx was the person in charge: “Birx’s policies were enacted throughout the country, in almost every single state, for the entire pandemic—this cannot be denied; it cannot be deflected.” (Atlas, p. 222)
Atlas is “dumbstruck at the lack of leadership in the White House,” in which, “the president was saying one thing while the White House Task Force representative was saying something entirely different, indeed contradictory” and, as he notes, “no one ever set her [Birx] straight on her role.” (Atlas, p. 222-223)
Not only that, but no matter how much Trump, or anyone in the administration, disagreed with Birx, “the White House was held hostage to the anticipated reaction of Dr. Birx” and she “was not to be touched, period.” (Atlas, p. 223)
One explanation for her untouchableness, Atlas suggests, is that Birx and her policies became so popular with the press and public that the administration did not want to “rock the boat” by replacing her before the election. This explanation, however, as Atlas himself realizes, crumbles in the face of what we know about Trump and the media’s hostility towards him:
“They [Trump’s advisors] had convinced him to do exactly the opposite of what he would naturally do in any other circumstance—to disregard his own common sense and allow grossly incorrect policy advice to prevail. … This president, widely known for his signature ‘You’re fired!’ declaration, was misled by his closest political intimates. All for fear of what was inevitable anyway—skewering from an already hostile media.” (Atlas, p. 300-301)
I would suggest, again, the reason for the seemingly inexplicable lack of gumption on Trump’s part to get rid of Birx was not politics, but behind-the-scenes machinations of the (to coin a moniker) lab leak cabal.
Who else was part of this cabal with its hidden agendas and oversized policy influence? Our attention naturally turns to the other members of the Task Force who were presumably co-engineering lockdown policies with Birx. Surprising revelations emerge.
There was no troika. No Birx-Fauci lockdown plan. It was all Birx.
It is universally assumed, by both those in favor and those opposed to the Task Force’s policy prescriptions, that Drs. Deborah Birx, Tony Fauci (head of NIAID at the time) and Bob Redfield (then director of the CDC) worked together to formulate those policies.
The stories told by Birx herself and Task Force infiltrator Scott Atlas suggest otherwise.
Like everyone else, at the onset of his book, Atlas asserts: “The architects of the American lockdown strategy were Dr. Anthony Fauci and Dr. Deborah Birx. With Dr. Robert Redfield… they were the most influential medical members of the White House Coronavirus Task Force.” (Atlas, p. 22)
But as Atlas’s story unfolds, he presents a more nuanced understanding of the power dynamics on the Task Force:
“Fauci’s role surprised me the most. Most of the country, indeed the entire world, assumed that Fauci occupied a directorial role in the Trump administration’s Task Force. I had also thought that from viewing the news,” Atlas admits. However, he continues, “The public presumption of Dr. Fauci’s leadership role on the Task Force itself… could not have been more incorrect. Fauci held massive sway with the public, but he was not in charge of anything specific on the Task Force. He served mainly as a channel for updates on the trials of vaccines and drugs.” (p. 98) [BOLDFACE ADDED]
By the end of the book, Atlas fully revises his initial assessment, strongly emphasizing that, in fact, it was primarily and predominantly Birx who designed and disseminated the lockdown policies:
“Dr. Fauci held court in the public eye on a daily basis, so frequently that many misconstrue his role as being in charge. However, it was really Dr. Birx who articulated Task Force policy. All the advice from the Task Force to the states came from Dr. Birx. All written recommendations about their on-the-ground policies were from Dr. Birx. Dr. Birx conducted almost all the visits to states on behalf of the Task Force.” (Atlas, p. 309-10) [BOLDFACE ADDED]
It may sound jarring and unlikely, given the public perception of Fauci, as Atlas notes. But in Birx’s book the same unexpected picture emerges.
Methinks the lady doth protest too much
As with her bizarrely self-contradictory statements about how she got hired, and her blatantly bogus scientific claims, Birx’s story about her mind-melded closeness with Fauci and Redfield falls apart upon closer examination.
In her book, Birx repeatedly claims she trusts Redfield and Fauci “implicitly to help shape America’s response to the novel coronavirus.” (Birx, p. 31) She says she has “every confidence, based on past performance, that whatever path the virus took, the United States and the CDC would be on top of the situation.” (Birx, p. 32)
Then, almost immediately, she undermines the credibility of those she supposedly trusts, quoting Matt Pottinger as saying she “‘should take over Azar, Fauci, and Redfield’s jobs, because you’re such a better leader than they are.’” (Birx, p. 38-9)
Perhaps she was just giving herself a little pat on the back, one might innocently suggest. But wait. There’s so much more.
Birx claims that in a meeting on January 31 “everything Drs. Fauci and Redfield said about their approach made sense based on the information available to me at that point,” even though “neither of them spoke” about the two issues she was most obsessed with: “asymptomatic silent spread [and] the role testing should play in the response.” (Birx, p. 39)
Then, although she says she “didn’t read too much into this omission,” (p. 39) just two weeks later, “as early as February 13” Birx again mentions “a lack of leadership and direction in the CDC and the White House Coronavirus Task Force.” (p. 54)
So does Debi trust Tony and Bob’s leadership or does she not? The only answer is more self-contradictory obfuscation.
Birx is horrified that nobody is taking the virus as seriously as they should: “then I saw Tony and Bob repeating that the risk to Americans was low,” she reports. “On February 8, Tony said that the chances of contracting the virus were ‘minuscule.’” And, “on February 29, he said, ‘Right now, at this moment, there is no need to change anything you’re doing on a day-to-day basis.’” (Birx, p. 57)
This does not seem like the kind of leader Birx can trust. She half-heartedly tries to excuse Redfield and Fauci, saying “I now believe that Bob and Tony’s words had spoken to the limited data they had access to from the CDC,” and then, in another whiplash moment, “maybe they had data in the United States that I did not.”
Did Tony and Bob provide less dire warnings because they had insufficient data or because they had more data than Birx did? She never clarifies, but regardless, she assures us that she “trusted them” and “felt reassured every day with them on the task force.” (Birx, p. 57)
If I was worried that the virus was not being taken seriously enough, Birx’s reports on Bob and Tony would not be very reassuring, to say the least.
Apparently, Birx herself felt that way too. “I was somewhat disappointed that Bob and Tony weren’t seeing the situation as I was,” she says, when they disagreed with her alarmist assessments of asymptomatic spread. But, she adds, “at least their number supported my belief that this new disease was far more asymptomatic than the flu. I wouldn’t have to push them as far as I needed to push the CDC.” (Birx, p. 78)
Is someone who disagrees with your assessment to the point that you need to push them in your direction also someone you “implicitly trust” to lead the US through the pandemic?
Apparently, not so much.
Although she supposedly trusts Redfield and sleeps well at night knowing he’s on the Task Force, Birx has nothing but disdain and criticism for the CDC – the organization Redfield leads.
“On aggressive testing I planned to have Tom Frieden [CDC director under Obama] help bring the CDC along,” she recounts. “Like me, the CDC wanted to do everything to stop the virus, but the agency needed to align with us on aggressive testing and silent spread.” (p. 122) Which makes one wonder: If she was so closely aligned with Redfield, the head of the CDC, why did Birx need to bring in a former director – in a direct challenge to the sitting one – to “bring the CDC along?” Who is “us” if not Birx, Fauci and Redfield?
Masks were another issue of apparent contention. Birx is frustrated because the CDC, led by her “we’ve-got-each-other’s-back” bestie, Bob Redfield (Birx, p. 31), will not issue strict enough masking guidelines. In fact, she repeatedly throws Bob’s organization under the bus, basically accusing them of causing American deaths: “For many weeks and months to come,” she writes, “I fretted over how many lives could have been saved if the CDC had trusted the public to understand that …masks would do no harm and could potentially do a great deal of good.” (Birx, p. 86)
Apparently, Fauci was not on board with the masking either, as Birx says that “getting the doctors, including Tom [Frieden] and Tony, to be in complete agreement with me about asymptomatic spread was slightly less of a priority. As with masks, I knew I could return to that issue as soon as I got their buy-in on our recommendations.” (Birx, p. 123)
Who is making “our recommendations” if not Birx, Fauci and Redfield?
The myth of the troika
Whether or not she trusted them (and it’s hard to believe, based on her own accounts, that she did), it was apparently very important to Birx that she, Fauci and Redfield appear as a single entity with no disagreements whatsoever.
When Scott Atlas, an outsider not privy to whatever power plays were happening on the Task Force, came in, his presence apparently rattled Birx (Atlas, p. 83-4), and for good reason. Atlas immediately noticed strange goings-on. In his book, he repeatedly uses words like “bizarre,” “odd” and “uncanny” to describe how Fauci, Redfield and Birx behaved. Most notably, they never ever questioned or disagreed with one another in Task Force meetings. Not ever.
“They shared thought processes and views to an uncanny level,” Atlas writes, then reiterates that “there was virtually no disagreement among them.” What he saw “was an amazing consistency, as though there were an agreed-upon complicity” (Atlas, pp. 99-100). They “virtually always agreed, literally never challenging one another.” (p. 101) [BOLDFACE ADDED]
An agreed-upon complicity? Uncanny agreement? Based on all of the disagreements reported by Birx and her repeated questioning and undermining of Bob and Tony’s authority, how can this be explained?
I would contend that in order to obscure the extent to which Birx alone was in charge of Task Force policy, the other doctors were compelled to present a facade of complete agreement. Otherwise, as with any opposition to, or even discussion of, potential harms of lockdown policies, “millions of Amercans would die.”
This assessment is strengthened by Atlas’s ongoing bafflement and distress at how the Task Force – and particularly the doctors/scientists who were presumably formulating policy based on data and research – functioned:
“I never saw them act like scientists, digging into the numbers to verify the very trends that formed the basis of their reactive policy pronouncements. They did not act like researchers, using critical thinking to dissect the published science or differentiate a correlation from a cause. They certainly did not show a physician’s clinical perspective. With their single-minded focus, they did not even act like public health experts.” (Atlas, p. 176)
Atlas was surprised, indeed stunned, that “No one on the Task Force presented any data” to justify lockdowns or to contradict the evidence on lockdown harms that Atlas presented. (Atlas, p. 206) More specifically, no data or research was ever presented (except by Atlas) to contradict or question anything Birx said. “Until I arrived,” Atlas observes, “no one had challenged anything she said during her six months as the Task Force Coordinator.” (Atlas, p. 234) [BOLDFACE ADDED]
Atlas cannot explain what he’s witnessing. “That was all part of the puzzle of the Task Force doctors,” he states. “There was a lack of scientific rigor in meetings I attended. I never saw them question the data. The striking uniformity of opinion by Birx, Redfield, Fauci, and (Brett) Giroir [former Admiral and Task Force “testing czar”] was not anything like what I had seen in my career in academic medicine.” (Atlas, p. 244)
How can we explain the puzzle of this uncanny apparent complicity by the Task Force troika?
Methinks the intelligence agent also doth protest too much
An interesting hint comes from the string of anecdotes comprising Matthew Lawrence’s New Yorker article “The Plague Year.” Lawrence writes that Matt Pottinger (the NSC liaison to Birx) tried to convince Task Force members that masking could stop the virus “‘dead in its tracks’” but his views “stirred up surprisingly rigid responses from the public-health contingent.” Lawrence continues to report that “In Pottinger’s opinion, when Redfield, Fauci, Birx, and (Stephen) Hahn spoke, it could sound like groupthink,” implying that those were the members of the “public-health contingent” who did not agree with Pottinger’s masking ideas.
But wait. We just noted Birx’s frustration, indeed deep regret, that the CDC led by Redfield, as well as Fauci (and even Frieden) did not agree with her ideas on asymptomatic spread and masking. So why does Pottinger imply that she and the “public-health contingent” of the Task Force were group-thinking this issue, against him?
I would suggest that the only way to make sense of these contradictions within Birx’s narrative and between her, Atlas and Pottinger’s stories, is if we understand “align with us” and “our recommendations” to refer not to the perceived Birx-Fauci-Redfield troika, but to the Birx-Pottinger-lab leak cabal that was actually running the show.
In fact, Birx and Pottinger put so much effort into insisting on the solidarity of the troika, even when it contradicts their own statements, that the question inevitably arises: what do they have to gain from it? The benefit of insisting that Birx was allied with Fauci, Redfield and the “public-health contingent” on the Task Force, I would argue, is that this deflects attention from the Birx-Pottinger-cabal non-public-health alliance.
The explanation of Atlas’s perceived “puzzle of the Task Force doctors” that makes the most sense to me is that Deborah Birx, in contrast and often in opposition to the other doctors on the Task Force, represented the interests of what I’m calling the lab leak cabal: those not just in the US but in the international intelligence/biosecurity community who needed to cover up a potentially devastating lab leak and who wanted to impose draconian lockdown measures such as the world had never known.
Who exactly they were and why they needed lockdowns are subjects of ongoing investigations.
In the meantime, once we separate Birx from Trump, from the rest of the administration, and from the others on the Task Force, we can see clearly that her single-minded and scientifically nonsensical emphasis on silent spread and asymptomatic testing was geared toward a single goal: to scare everyone so much that lockdowns would appear to be a sensible policy. This is the same strategy that was, uncannily in my opinion, implemented almost to the letter in nearly every other country around the world. But that’s for the next article.
I’ll close this chapter of the Birx riddle wrapped in a mystery inside an enigma, with Scott Atlas’s report of his parting conversation with President Trump:
“‘You were right about everything, all along the way,’” Trump said to Atlas. “‘And you know what? You were also right about something else. Fauci wasn’t the biggest problem of all of them. It really wasn’t him. You were right about that.’ I found myself nodding as I held the phone in my hand,” Atlas says. “I knew exactly whom he was talking about.” (Atlas, p. 300)
And now, so do we.
Debbie Lerman has a degree in English from Harvard. She is a retired science writer and a practicing artist in Philadelphia, PA.
Why the COVID Jab Should Be Banned for Pregnant Women
By Dr. Joseph Mercola | August 30, 2022
Since the rollout of the experimental COVID shots, U.S. health officials have adamantly claimed the shots are safe for pregnant women, and have been urging all pregnant women to get the jab “to protect themselves and their babies.” To this day, the U.S. Centers for Disease Control and Prevention recommends the COVID shot for:1
“… people who are pregnant, breastfeeding, trying to get pregnant now, or might become pregnant in the future.”
The CDC further recommends:2
“People who are pregnant should stay up to date with their COVID-19 vaccines, including getting a COVID-19 booster when it’s time to get one.”
And claims:3
“Evidence continues to build showing that:
- COVID-19 vaccination during pregnancy is safe and effective.
- There is currently no evidence that any vaccines, including COVID-19 vaccines, cause fertility problems in women or men.”
All the while, they’ve had Pfizer data showing the shots cause shocking rates of miscarriage which, adding insult to injury, have been blatantly miscategorized as a “recovered/resolved” adverse effect.4 Who in their right mind would consider DEATH a resolved side effect unless they had a depopulation agenda in mind all along?
I don’t see how this could be described as anything but a criminal cover-up. The only reason we know any of this is because U.S. District Judge Mark Pittman ordered the U.S. Food and Drug Administration to release Pfizer documents at a rate of 55,000 pages per month. The FDA and Pfizer had asked to release the documents at a pace of 500 pages per month, which meant it would take 75 years to disclose them all.5
Criminal Cover-Up
Dr. Naomi Wolf recently reported that an analysis of Pfizer data revealed 44% of the women in the trial suffered miscarriages.6 That statistic turns out to have been the result of a miscalculation,7 as Pfizer listed the miscarriages in two separate columns, resulting in them being counted twice.
We’ve repeatedly found Pfizer’s data collection and reporting to be all over the place, and seemingly on purpose, to make hazards more difficult to ascertain. Wolf admitted the error and took down the original report. However, while fact checkers are gloating over the perceived victory, there’s plenty of other evidence in the Pfizer material to demonstrate these shots should be banned for all time.
In an August 20, 2022, Substack article, Dr. Pierre Kory addressed other, “absolutely horrifying,” findings on miscarriages found in the Pfizer data dumps:8
“… let’s do a dive on just one page of the many thousands. See below, Section 5.3.6, Page 12 of the document called ‘Cumulative Analysis of Post-Authorization Adverse Event Reports.’

Looking at the first bullet under the header: Pregnancy cases: 274 cases including:
In this paragraph, at first read, it is just a list of adverse events and numbers, detailed in a way that is confusing at best, and obfuscating at worst. I think it is the latter because, if you do some simple arithmetic trying to parse that paragraph, you end up with this:
270 pregnancies were reported in vaccinated women during the first 12 weeks of the vaccine campaign. In 238 of them, ‘no outcome was provided.’ So, they only knew the outcome of 32 pregnancies reported. What happened in those 32 pregnancies they followed up on?
My hands are literally trembling as I write this, but here goes. In these 32 pregnancies, there were:
•23 spontaneous abortions
•2 spontaneous abortions with intra-uterine death
◦So, 25 of the 32 pregnancies with known outcomes resulted in a miscarriage, a rate of 78%. Note that miscarriage normally occurs in only 12-15% of pregnancies
•2 premature births with neonatal death
•1 spontaneous abortion with neonatal death
•1 normal outcome
Note that this only adds up to 29 known outcomes, but then they note that ‘two different outcomes were reported for each twin’ and then they talk about ‘fetus/baby cases as separate from mother cases.’ I have no idea how to interpret this explanation of outcomes, so it may have been one or two less (or more) deaths then.
So, of the 32 pregnancies they knew the outcome of, 87.5% resulted in the death of the fetus or neonate. Burying this data in the way and not alerting the world to what they found, is criminal activity …”
To be perfectly clear, the failure to record and report the outcomes of 238 out of 274 pregnancies during a drug trial is simply unheard of. It’s shockingly unethical. And the fact that both the Food and Drug Administration and the CDC accepted this, and claim there’s “no evidence” of harm to pregnant women and their babies is proof positive of reprehensible maleficence.
There’s no fixing what’s gone wrong at the FDA and CDC. Their credibility with the public is ruined beyond any possible recovery. The CDC can review and reorganize itself all it wants, but it changes nothing. They are, to this day, urging pregnant women to take a shot that they KNOW will cause babies to die. Calling it a dystopia of epic proportions is a profoundly serious understatement.
CDC-Sponsored Study Also Tried to Hide Data
Need more evidence? How about the fact that the CDC-sponsored study9 published in The New England Journal of Medicine (NEJM) in April 2021 — which was widely used to support the U.S. recommendation for pregnant women to get injected — also obfuscated data to hide a shockingly elevated miscarriage rate.
According to this paper, the miscarriage rate within the first 20 weeks of pregnancy was 12.5%, which is only slightly above the normal average of 10%. (Looking at statistical data, the risk of miscarriage drops from an overall, average risk rate of 21.3% for the duration of the pregnancy as a whole, to just 5% between Weeks 6 and 7, all the way down to 1% between Weeks 14 and 20.10)
However, there’s a distinct problem with this calculation, as highlighted by Drs. Ira Bernstein, Sanja Jovanovic and Deann McLeod, HBSc, of Toronto. In a May 28, 2021, letter to the editor, they pointed out that:11
“In table 4, the authors report a rate of spontaneous abortions <20 weeks (SA) of 12.5% (104 abortions/827 completed pregnancies). However, this rate should be based on the number of women who were at risk of an SA due to vaccine receipt and should exclude the 700 women who were vaccinated in their third-trimester (104/127 = 82%).”
In other words, when you exclude women who got the shot in their third trimester (since the third trimester is after week 20 and therefore should not be counted when determining miscarriage rate among those injected before week 20), the miscarriage rate is 82%. (The errors in that NEJM article were also reviewed in a Science, Public Health Policy and the Law paper12 published in November 2021.)
Of those 104 miscarriages, 96 of them occurred before 13 weeks of gestation, which strongly suggests that getting a COVID shot during the first trimester is an absolute recipe for disaster. So, here was yet another attempt to hide the fact that more than 8 in 10 pregnancies may be terminated as a result of the jab.
As of August 12, 2022, the U.S. Vaccine Adverse Event Reporting (VAERS) database listed 4,941 miscarriages post-COVID jab.13 For comparison, the fetal death reports for all other vaccines reported to VAERS in the last 30 years is 2,239.14
Birth Rates Are Suddenly Plummeting Worldwide
In addition to miscarriages, we’re also looking at abruptly plummeting birth rates, suggesting the COVID jabs are having an adverse impact on future fertility as well.
“They are large drops, and they are occurring, almost like clockwork, approximately 9 months after pregnant women around the world started to be vaccinated,” Kory notes.15
For example, Germany recently released data showing a 10% decline in birth rate during the first quarter of 2022.16

The live birth rate graph for Sweden looks much the same, with a 14% drop:17,18 According to Gunnar Anderson, a Swedish professor in demographics at Stockholm University, “We have never seen anything like this before, that the bottom just falls out in just one quarter.”19

Between January and April 2022, Switzerland’s birth rate was 15% lower than expected, the U.K.’s was down by 10% and Taiwan’s was down 23%.20,21,22 In Hungary, MP Dúró Dóra has expressed concern about a 20% drop in birth rate during January 2022, compared to January 2021.23
The U.S. is also showing signs of a drop in live births. Provisional data from North Dakota show a 10% decline in February 2022, 13% reduction in March and an 11% reduction in April, compared to the corresponding months in 2021.24
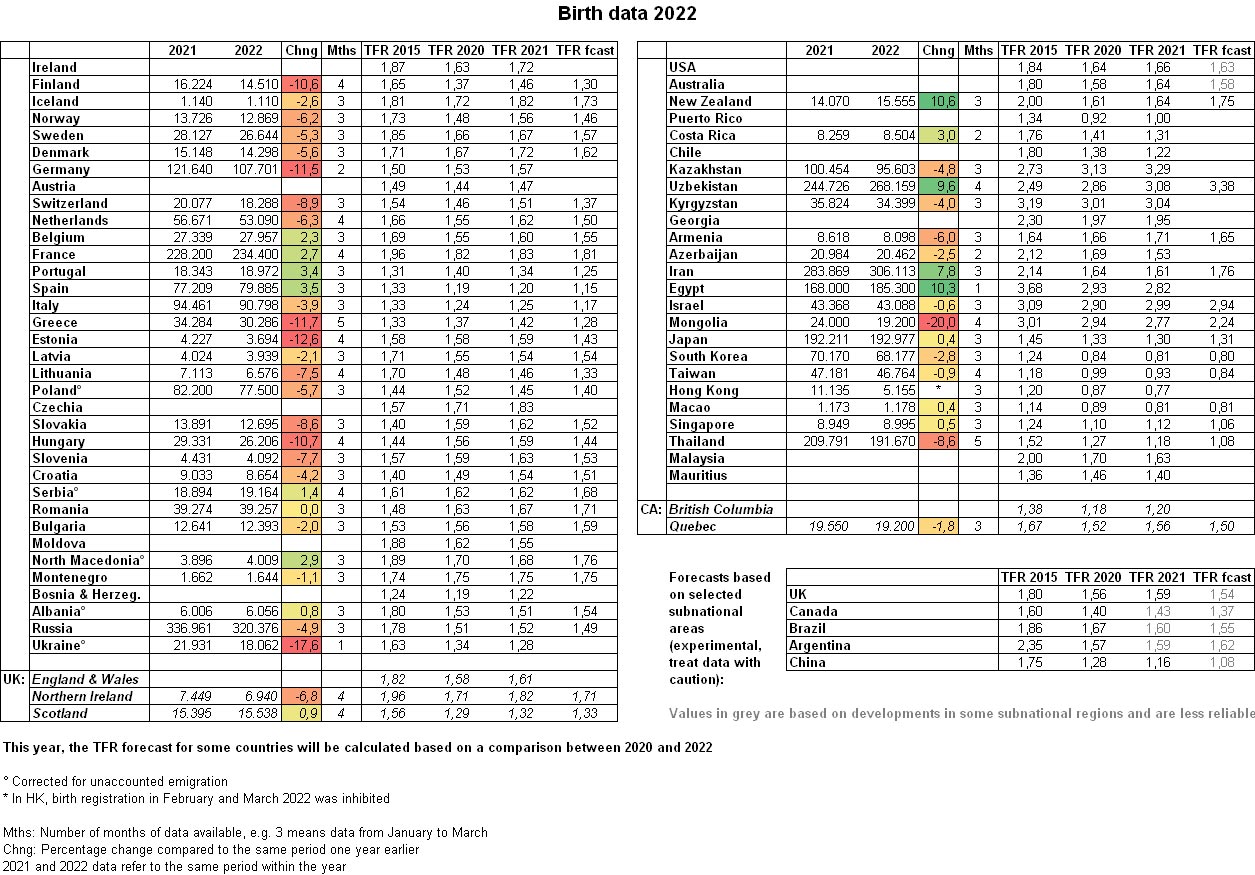
In a July 5, 2022, Counter Signal article, Mike Campbell reported that in the five countries with the highest COVID jab uptake, fertility has dropped by an average of 15.2%, whereas the five countries with the lowest COVID jab uptake have seen an average reduction of just 4.66%. Below is a chart from Birth Gauge25 on Twitter comparing live birth data for 2021 and 2022 in a large number of countries.
Many Women Report Menstrual Irregularities Post-Jab
High rates of menstrual irregularities post-jab are also a warning sign that reproductive capacity may be impacted. As of August 12, 2022, there were 31,443 VAERS reports of menstrual disorders.26
Changes include heavier and more painful periods27 and changes in menses length, as well as unexpected breakthrough bleeding or spotting among women on long-acting contraception or those who are postmenopausal and haven’t had a period in years or even decades.28
Health officials have tried to brush off the reports, but a study published in Obstetrics & Gynecology — funded by the National Institute of Child Health and Human Development (NICHD) and the National Institutes of Health’s Office of Research on Women’s Health — confirmed an association between menstrual cycle length and COVID-19 shots.29
According to the authors, it’s possible that the immune response created by the mRNA shots affect the hypothalamic-pituitary-ovarian axis, which plays a well-known role in the timing of a woman’s cycle:30
“Our findings for individuals who received two doses in a single cycle supports this hypothesis. Given the dosing schedule of the mRNA COVID-19 vaccines in the United States (21 days for Pfizer and 28 days for Moderna), an individual receiving two doses in a single cycle would have received the first dose in the early follicular phase.
Cycle length variability results from events leading to the recruitment and maturation of the dominant follicle during the follicular phase …”
Other Disturbing Evidence
A Japanese biodistribution study for Pfizer’s jab also showed the COVID spike protein from the shots accumulate in female ovaries and male testes,31,32 and there’s credible concern that the COVID jabs will cross-react with syncytin (a retroviral envelope protein) and reproductive genes in sperm, ova and placenta in ways that may impair fertility and reproductive outcomes.
A Pfizer-BioNTech rat study33 revealed the injection more than doubled the incidence of preimplantation loss (i.e., the risk of infertility), and led to mouth/jaw malformations, gastroschisis (a birth defect of the abdominal wall) and abnormalities in the right-sided aortic arch and cervical vertebrae.34,35 As noted by The Exposé :
“With this being the case, how on earth have medicine regulators around the world managed to state in their official guidance that ‘Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy’? And how have they managed to state ‘It is unknown whether the Pfizer vaccine has an impact on fertility’?
The truth of the matter is that they actively chose to cover it up. We know this thanks to a Freedom of Information (FOI) request36 made to the Australian Government Department of Health Therapeutic Goods Administration (TGA).”
You can read more about that in The Exposé’s July 19, 2022, article, “FOIA Reveals Pfizer & Medicine Regulators Hid Dangers of COVID Vaccination During Pregnancy After Study Found It Increases Risk of Birth Defects & Infertility.”37
We’re also seeing a sudden uptick in infant mortality. The Exposé 38 highlighted data from Scotland, showing neonatal deaths were 119% higher above the annual norm in March 2022.
COVID Jab Affects Male Fertility Too
Male fertility is also under attack by these bioweapons. Israeli research39,40 published in the journal Andrology found the Pfizer COVID jab temporarily but significantly impairs male fertility, dropping sperm concentration by 15.4% and total motile count by 22.1%, compared to baseline pre-jab.
Both eventually recovered, some three months after the last jab, but if you destroy a man’s sperm for three months every time he gets a COVID shot, you’re significantly reducing the probability of him fathering a child for a good part of any given year and the stats reviewed above support this.
Remember, the mRNA shots are recommended at three-month intervals for the original series, and boosters are now being recommended at varying intervals thereafter. In the video above, Amy Kelly, project director for the Daily Clout’s Pfizer document analysis team, reviews this study and other post-jab male fertility concerns.41
End the COVID Shots Now, Before It’s Too Late to Recover
In October 2021, when the FDA was voting on whether to authorize the COVID jab for children aged 5 through 11, Dr. Eric Rubin, an FDA advisory panel member, Harvard professor and editor-in-chief of the NEJM, stated:42
“We’re never going to learn about how safe this vaccine is unless we start giving it. That’s just the way it goes … And I do think we should vote to approve it.”
So, in this and other instances, they’ve openly admitted that anyone who takes the jab is part of an experiment. Yet at the same time, the FDA and CDC have insisted that the jabs are perfectly safe — all while in possession of data showing they’re anything but! In conclusion, I agree with Kory, who writes:43
“… when a new medicine or device is introduced, you must first assume any adverse effects or deaths reported to be related to the intervention until proven otherwise. That is what I am doing here.
We must assume the vaccines are impacting fertility unless some other provable or credible explanations for a sudden drop in month to month birth rates. So stop the shots until you can prove they are not …
Too many young people dying,44 too many becoming disabled, too many pregnancies resulting in fetal or neonatal death as above, and now we find out that if we continue with this vaccine obsession, they will not be replaced. This is a humanitarian catastrophe heaped atop the one caused by dangerous gain-of-function research.
When will the world wake up to this rapidly unfolding horror? For those of us who know what is going on, it is hard not to feel helpless as we are forced to watch increasingly apparent and widespread needless death. But we will continue to try to get these truths out despite the massive censorship and propaganda overwhelming the globe.
We have a moral and ethical obligation and take that responsibility seriously no matter what befalls us. Stop the vaccines, now. And if we can’t stop them, we must try to convince everyone we know to no longer agree to get vaccinated. Their lives and our future depend on it.”
Sources and References
- 1, 2, 3 CDC.gov Updated July 14, 2022
- 4, 6 Clark County Today August 18, 2022
- 5 Bloomberg Law January 18, 2022
- 7 Twitter Phil Kerpen August 17, 2022
- 8, 15, 19, 43 Pierre Kory Substack August 20, 2022
- 9 N Engl J Med 2021; 384:2273-2282
- 10 Medical News Today January 12, 2020
- 11 Wayback NEJM Letter to the Editor June 27, 2021
- 12 Science, Public Health Policy, and the Law November 2021; 4: 130-143
- 13, 26 OpenVAERS Reproductive Health Reports as of August 12, 2022
- 14, 35, 38, 44 The Expose August 7, 2022
- 16 Expose News July 18, 2022
- 17, 20, 23 The Counter Signal July 5, 2022
- 18 Twitter Havard Skjaervik June 27, 2022
- 21, 24 Igor Chudov Substack June 25, 2022
- 22 SWPRS June 2022
- 25 Twitter Birth Gauge June 3, 2022
- 27 Boston University September 9, 2021
- 28 NPR August 9, 2021
- 29 Obstetrics & Gynecology: January 5, 2022 – Volume – Issue – 10.1097
- 30 Obstetrics & Gynecology: January 5, 2022 – Volume – Issue – 10.1097, Discussion
- 31 Children’s Health Defense June 3, 2021
- 32 Rights and Freedoms, Confidential Pfizer Research Document
- 33 Reproductive Toxicology August 2021; 103: 28-35
- 34 Science, Public Health Policy, and the Law November 2021; 4:130-143, page 135
- 36, 37 The Expose July 19, 2022
- 39 Andrology June 17, 2022 DOI: 10.111/andr.13209
- 40 Expose June 26, 2022
- 41 Daily Clout August 16, 2022
- 42 Townhall October 26, 2021
UK Agency Says No COVID Shot for Pregnant Women
By Dr. Joseph Mercola | August 29, 2022
United Kingdom vaccine regulatory administrators quietly removed pregnant and breastfeeding women from its recommendations for the COVID-19 shots — almost two weeks ago. Yet, at the same time, a different arm of the U.K. government, National Health Service, is still promoting the shots as safe “at any stage of pregnancy.”
So which is it?
In a blog, Norman Fenton, professor of risk information management in London, points out the contradictions. Below are excerpts from the Gov.UK website of the “Summary of the Public Assessment Report for COVID-19 Vaccine and Pfizer/BioNTech,” dated August 16, 2022, which contradicts the NHS:
“ … It is considered that sufficient reassurance of safe use of the vaccine in pregnant women cannot be provided at the present time … Women who are breastfeeding should also not be vaccinated.”
With women of childbearing “potential,” the agency says “health care professionals are advised to rule out known or suspected pregnancy prior to vaccination.”
It’s safe to have the vaccine during any stage of pregnancy, from the first few weeks up to your expected due date. You do not need to delay vaccination until after you have given birth.
Getting vaccinated against COVID-19 reduces the risk of having a stillbirth.
There’s no evidence COVID-19 vaccination increases the risk of having a miscarriage, pre-term birth or other complications in your pregnancy.
Public Health Agency of Canada is hiring security guards for ‘quarantine facilities’

The Counter Signal | August 31, 2022
The Public Health Agency of Canada (PHAC) has listed openings for security guards for its “quarantine facilities” in Toronto, York and Halton, Ontario.
The posting requires “risk management and security services for Designated Quarantine Facilities in Ontario.”
The job posting was published last week and will close on September 9 at 2 p.m. EST.
During the COVID-19 pandemic, the government of Canada created “Designated Quarantine Facilities” for Canadians unable to quarantine at home after international travel due to proximity with family members. The public became aware of these facilities following reports of Canadians taken from the airport in unmarked vehicles and forcibly placed in a government facility.
In most cases, the facility was a modified hotel. Travellers were typically required to stay in the room for three nights or until they received a negative COVID test.
Quarantine facilities were manned by hotel staff and security guards.
According to the Government of Canada website, “Travellers arriving in Canada who do not have a suitable place to quarantine or isolate may be referred to a designated quarantine facility, upon the direction of a quarantine officer.”
During a stay, travellers are “required to remain in your room until you receive permission and a specific time to leave from a Quarantine Officer at the facility.”
Horror stories frequently emerged from those who stayed at the facilities. Those in forced quarantine were given little to eat and were not allowed to order food. Complaints arose that facilities didn’t comply with specific dietary concerns.
In Quebec, one woman was sexually assaulted during her stay at a facility.
Later in the pandemic, the government required anyone entering Canada by air travel to quarantine at a Designated Quarantine Facilities, costing travellers around $300 per night. Canadians who crossed the border by land were largely exempt from this policy.
The job posting comes as most Canadians have received two doses of a Health Canada-approved COVID-19 vaccine. Federal and provincial governments have dangled COVID-19 vaccination status as a means to return to normal.
Yet, even Canadians with two doses of the vaccine were not exempt from the government’s stringent travel measures during the pandemic, including a stay at a government hotel.
In August, Ottawa announced funding for a “safe voluntary isolation site” in the Windsor-Essex region in Ontario. The government said the isolation site will be used to accommodate foreign agri-workers who can’t find a place to isolate when they enter Canada.
The Historic Suppression of Scientific Debate in COVID
Never before in modern history have entire topics in Medicine been actively prevented from discussion in public forums
By Pierre Kory, MD, MPA | Medical Musings | August 30, 2022
I started reading about the definition, history, and legal background of censorship. The entry on Wikipedia (ugh) was quite revealing:
Censorship is the suppression of speech, public communication, or other information. This may be done on the basis that such material is considered objectionable, harmful, or sensitive. Censorship can be conducted by governments, private institutions and other controlling bodies.
But get this, look at the examples of topics that have traditionally been censored:
General censorship occurs for a variety of claimed reasons including national security, to control obscenity, pornography, and hate speech, to protect children or other vulnerable groups, to promote or restrict political or religious views, and to prevent slander and libel.
Note that “scientific opinion” is not on there. Because scientific data nor interpretations of that data, should ever be considered offensive. You can argue that wrong interpretations of data can be harmful, but debate is how you resolve that, not censorship! Science literally rests on open debate and the sharing of data and exchanging of interpretations amongst not only experts, but the wider public.
Now, also from Wikipedia:
Censorship has been criticized throughout history for being unfair and hindering progress. Censorship is counterproductive as it prevents the censored topic from being discussed. Those who impose censorship must consider what they censor to be true, as individuals believing themselves to be correct would welcome the opportunity to disprove those with opposing views (just ask Steve Kirsch).
But again, science is not on there as a category of discourse to censor. Although history is replete with attempts to censor individuals with scientific views contrary to established orthodoxy, in all the instances I can think of, the person being censored was eventually proven correct! Galileo (earth is round), Seimelwess (importance of handwashing), Scopes (teaching of evolutionary theory) etc.
Yet, in the last 2 years we have undergone a massive censorship of the discussion and sharing of scientific data in public forums. I believe this was the proximate cause of what can now only be viewed as humanitarian catastrophes resulting from 1) the suppression of knowledge of early treatment with effective repurposed drugs and 2) the suppression of data showing the toxicity, lethality, and ineffectiveness of the vaccines.
This period should serve as one of the most damning arguments against censorship.
We were not allowed to openly discuss our data or our interpretations and applications of that scientific data (i.e. scientific opinions) in major media or social media. The journalist Matt Taibbi called me “the ghost of the internet” because whenever I had scientific discussions with folks who are now dear friends and colleagues, their content and podcasts were de-platformed or demonetized (as in the case of my dear friend Dr. Been), and/or they immediately founds their posted videos of those discussions taken down, like immediately (the speed in which I “disappeared” was astonishingly fast at times). All because we had a scientific discussion where I had shared data and interpretations of that data. I was honored with the opportunity to make my case in front of some truly expert and deep thinkers. Folks who could challenge me, ask questions, express concerns or offer alternative interpretations or hypotheses. I would say that the only problem with those discussions is that the data in support of ivermectin was just so overwhelming. It is a drug with proven efficacy in COVID. Note that conclusion is shared by some of the most highly published doctors in the history of our specialty (the FLCCC) as well as by a group of some of the top evidence-based medicine researchers in the world (Tess Lawrie, Andrew Bryant, Edmund Fordham et al. of EBMc2).
And therein lay the problem. The data could not be debated because any other interpretation than ivermectin being effective was pretty much indefensible in the face of a mountain of repeatedly and almost universally supportive data from myriad sources. So, instead, such discussions were banned from wider public view. Strong move. I think the only thing that saved a good portion of humanity was that individual and organizational websites (like the FLCCC’s, AAPS, c19early.com, and others) were largely secure and not taken down or booted off of hosting servers. But I imagine they could have been.
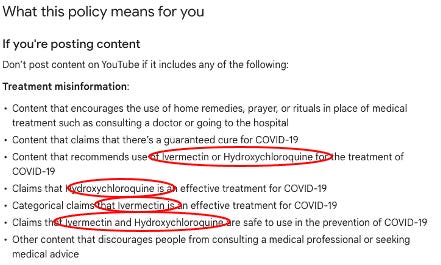
So, in COVID, Big Pharma and Big Government literally got media companies to shut down debate and discussion on certain topics like HCQ and IVM and vaccine toxicity and ineffectiveness. See YouTube’s community guidelines, which are so absurd, I literally turn purple with rage every time I read it. But it is also sort of comical because they literally put it in writing, right out in the open, plain to see, essentially saying “thou shalt not discuss these medicines on our platform.” And they did it while their efficacy was still being debated. In a global pandemic with thousands dying each day. Safe medicines.
Check it out:
Insane. Crazy town. Clown world. Now, keep in mind that these “guidelines” restricting any discussion of the efficacy, even potential efficacy during a global pandemic, were employed by every major media company in the world with few exceptions, like Trial Site News (although massively impactful, not yet “major media”) and maybe on a few occasions Fox News or some conservative radio hosts.
But all was not lost. Independent podcasters and some radio hosts saved the day, contributing to the dissemination of life-saving information to millions of people in this country and world. Folks like Bret Weinstein, Joe Rogan, John Campbell, Dr. Been, Dr. Mercola, Greg Hunter, Vicki McKenna and countless others. But the print and TV media giants did not have that policy written and made public for all to see (and laugh at). It was under the table, understood by all media that ivermectin should instead only be referred to as a horse dewormer. Not subtle. Alex Berenson’s recent sharing of evidence that the White House was behind his Twitter de-platforming shows how high up the censorship was coming from.
So you literally had the government and Pharma pressuring all the media and social media giants (all of them – Facebook, Linked in, Instagram, Twitter etc) to outlaw, yes, outlaw discussion of even the possibility these medications were effective. Never, ever forget this. Note how YouTube wrote that their guidelines were based on WHO recommendations. Control the top, you control everything beneath it. Read my detailed deep dive uncovering the corruption of ivermectin at the WHO here and here.
Now, one of the reasons Paul Marik was such a famous critical care doctor is that he had long been successful at debunking prevailing orthodoxy supporting standard of care practices in our specialty. He did it via lecturing and debating at national conferences and in publications within medical journals. It was how he and I met, when he congratulated me on an editorial I wrote in a major journal, where I argued against using ultrasound to measure the size of the inferior vena cava to estimate central venous pressure (CVP), largely drawing on the science and rationale he had compiled and published.
Talking to Paul this morning, he told me he is most proud of his work (note he accomplished this feat on his own) in teaching a global generation of critical care doctors that measuring the CVP to estimate the fluid needs of a patient was useless outside of a very narrow set of circumstances like hemorrhage (in those circumstances though, you don’t need the CVP to estimate fluid needs as the patients vitals and clinical presentation will tell you all you need to do.
You have to understand that the CVP was used for decades by critical care doctors in ICU patients who were in states of shock (dangerously low blood pressure). It was the standard of care in ICU’s. Paul did a deep dive into the published literature and especially into the complex physiology of the factors which influence CVP and wrote pretty much the coolest and most impactful paper ever called “Does Central Venous Pressure Predict Fluid Responsiveness?: A Systematic Review of the Literature and the Tale of Seven Mares.” The papers most memorable sentence was “the only study we could find demonstrating the utility of CVP in predicting volume status was performed in seven standing, awake mares undergoing controlled hemorrhage.” Brilliant. Funny.
His paper triggered fierce and I mean, fierce debate in critical care… for years. Reversing established orthodoxy in medicine (and anywhere really) is nearly impossible. But Paul singlehandedly pulled it off with his papers and lectures (helped by a lot of folks like me who followed his work closely). I would argue that today, the obsession with using the CVP to guide fluid resuscitation has largely (but never completely) been abandoned. Wow.
But, again, back then, you could have “debates” on controversial topics, in fact, such topics demanded them! I remember when the United Hospital Fund used to put on this terrific conference in Manhattan where they invited experts in the field to debate “controversies” in critical care (like CVP). Each speaker was given ten minutes and were assigned the pro side or the con side of a topic, but the assigned debaters could not choose the side to argue! After both speakers were heard, the audience voted on which conclusion was based on the more compelling data and argument. I was invited several years in a row and sometimes had to argue the side I was not on intellectually. Which made it even more enlightening an exercise – imagine getting Berenson to have to argue in support of ivermectin? It just might happen that he learns something important. Also, it was a “hard” ten minutes they gave you. So much so, I remember one year I got the whole room laughing because I did not shut up when the big timer hit ten minutes and the big red stoplight turned on, so a close colleague of mine ran up to the podium, put me in a headlock and started to drag me away from the podium as I was still yelling my final points. That was fun. Now, not so much.
More trips down the memory lane of debates. One of the first “corruptions” by Pharma that I experienced in my career was when Eli Lilly invented a national campaign called “Surviving Sepsis” in an attempt to create guidelines supporting optimal care practices. They involved all the professional societies in critical care to participate. Leaders in the field all with a seat at the table.
Yep, you guessed it, it turned out to be cover for their efforts in making a $5,000 harmful drug (Xygris) the standard of care in sepsis. Every single one of those committee members got money. The entire campaign and strategy was developed by a PR firm. Recall that Disinformation tactics were first invented by a PR firm in the 1950’s working for the Tobacco Industry at a time when their products were starting to look bad in the scientific literature.
I would argue that Pharma is the most skilled practitioner of Disinformation amongst all industries. I mean 20 years ago already, the entire country’s critical care doctors gave a very expensive, harmful drug to every septic patient for years based on a manipulated trial with the tiniest of mortality benefits amidst a splashy “public health” campaign concocted by a PR firm working for a pharmaceutical company.
When Xygris was eventually shown to be harmful it was abandoned. But that decision occurred on the back of fierce debates and constant re-analysis and discussion of the accumulating data. Hmm, I wonder when that will happen to Remdesivir? Fun fact: during my fellowship training in pulmonary and critical care, my mentors, Dr. Paul Mayo and Dr. Samual Acquah essentially forbade the use of Xygris at a time when every other fellow in training was using it like water. I never once ordered it for any patient.
But there were other controversial aspects of the sepsis guidelines that Paul was a beast in demolishing at national conferences. He was so good, his take on the data so expert and compelling that his lectures were always packed, like standing room only type packed. For a medical lecture.
The most debated aspect of sepsis treatment (and yes, it was debated repeatedly at national conferences) was called “early goal directed therapy” (EGDT) which required that you resuscitate patients using fluids and vasopressors to a target central venous pressure (CVP) and a target central venous oxygen saturation (SCV02), but to monitor the latter continuously, you had to insert a special catheter into the large neck veins to do it. I will not go into the detailed physiology of those parameters but the need to measure them was nonsense.
I knew it (even as a fellow), my mentors knew it, Paul knew it, yet EGDT was widely adopted across the country and world. The protocol was based on a single center study whose Principal Investigator Manny Rivers held the patent on that catheter (unknown by most at the time). Further, information later came out that the data were manipulated. That information was leaked by a whistleblower who was a fellow of Rivers at the time. The fellow was threatened by the hospital with the ending of his career if he were to continue to speak publicly about it. They even apparently threatened to “kill his kids.”
But the point is, the debates were fierce, in the open, and at conferences and hospital auditoriums across the country and world. They were data driven arguments by experts with decades of scientific inquiry and clinical expertise who reviewed the physiology and published literature. And sometimes led to conflicting interpretations. Yes, we all had biases when interpreting the data (all humans do), but we debated. It was not outlawed to say that SCV02 and IVC were unnecessary. Or to say they were critical. And you were not forced to use all aspects of EGDT in the care of patients back then as they were just “guidelines,” not rigid protocols supported by Federal government funded bonuses in every patient you used it in like we have now with Remdesivir.
Interestingly, widespread EGDT adoption actually showed consistent impacts in reducing mortality, but we knew it was not from the targeting of those parameters but instead just from the early recognition and resuscitation of sepsis. Might even be the one instance in history where a corrupt action by Big Pharma actually led to a benefit in public health. Anyway, eventually studies showed that targeting those parameters versus simply using clinical judgement led to the same outcomes and the practice was abandoned. Paul was right again.
Another aspect of the U.S resuscitation guidelines that Paul was absolutely brilliant in debunking was the decision to target a reduction in lactate as a resuscitation endpoint. This was another fiction like the CVP. Again, almost all of emergency and critical care medicine had been indoctrinated with the physiologic concept that lactate is a marker of hypo-perfusion (reduction in blood flow to organs). Now, in certain, specific clinical instances (ischemic bowel etc), a rise in lactate can reflect hypo-perfusion. But in most septic patients it is simply a marker of illness and stress. It is not harmful, in fact, if anything, lactate is better utilized by organs to maintain function and energy. However, doctors were taught to target lactate as a resuscitation endpoint instead of simply interpreting it as a marker of disease severity.
But, in this instance, that practice and belief was not the result of corruption. No-one as far as I can tell was making money off of dumb doctors and nurses being forced to check lactates repeatedly. It simply stemmed from ignorance and established practice, with leading “experts” (dotards) arrogantly teaching that it was important to target (because they were taught that and did not critically think about it). Paul’s research revealed that targeting lactate was the result of a gross misunderstanding of lactic acid physiology. It was again one of the most masterful papers I have read. He marshaled tons of physiologic knowledge and logically presented the concepts and data which defined the cause and purpose of lactic acid production.
Just like with his teachings on CVP, again you had one man arguing against an entire generation of doctors who believed that reducing lactate was important in the general septic patient. I totally agreed with Paul’s papers and conclusions. Which made my life difficult because I tried in vain to disseminate this knowledge among my trainees, trying to stop what I saw as the pervasive “lacto-bolo reflex” they were all exhibiting. Paul actually invented the term, and it was brilliant: “bolo” refers to a bolus of fluids, and the “reflex” was the ordering of an infusion of a half liter or liter of fluids every time a high lactate was measured.
Lacto-bolo reflexes unfortunately led to what he also brilliantly coined as “salt water drowning,” i.e the receipt of excessive amounts of saline fluids by patients. Every time a doctor or nurse received a report of a high lactate… the doc ordered fluids. Lacto-bolo reflex. What is crazy is that the excess fluid administration that resulted paradoxically worsened kidney function and led to more kidney failure despite the fact the doctors were trying to preserve kidney function with fluid infusions! It was insane and I knew it because of Paul’s research and teaching. I also tried for years to fight the lacto-bolo reflex in my trainees and colleagues with little success except for when I was physically present in the ICU. When I went home for the night though, my fellows and residents all continued with their lacto-bolo reflexes. When the cat’s away the mice will play.
However, in this instance, despite Paul’s papers and lectures on the topic, the unthinkable became true. “Experts” (dotards) eventually established the checking of repeated lactate as a national quality of care standard. Those standards are what hospitals are judged on which affects their reimbursement and accreditation.
So, doctors across the country are now literally mandated to repeatedly check and respond to lactates in septic patients. Again, another example of an orthodoxy based on fiction. Despite all of Pauls efforts in teaching, lecturing, and publishing on the topic, this time, he was unsuccessful in changing orthodoxy. He may have been if his career didn’t end but History marches on. I would argue that his efforts in singlehandedly trying to reverse orthodoxies unfounded by “the science” led to a widespread respect, admiration, and reverence for the deep knowledge and scientific acumen he consistently displayed. But not so much anymore it seems.
And that is solely because Paul’s final effort in academic medicine was in trying to reverse the fiction that ivermectin was ineffective in COVID. That effort ended his career because for the first time, unrealized by him at the time, instead of fighting ignorant knowledge of physiology, he was poking The Bear, i.e tackling a subject that threatened Big Pharma. In a big, big way. Thus, that effort ended his career. But let’s be specific about that – his former hospital (SENTARA GENERAL IN NORFOLK, VIRGINA) was the one who actually ended his career.
Now, how they ended it is pretty interesting, as my last job was ended in the same way. They did it by using a process that hospitals have long employed when a physician “doesn’t toe the line.” In COVID, Paul was a clinical leader in a major hospital and was employing a highly effective protocol using a combination of repurposed drugs and not using Remdesivir. And he was vocal about it. And he was teaching the doctors in training about the harms of Remdesivir and all of the data supporting “unapproved therapies.” So, they invoked a process called “sham peer review” to get rid of him. What the heck is “sham peer review?”
From a seminal paper on the topic:
In 1986, the United States Congress enacted the Healthcare Quality Improvement Act (HCQIA). which granted immunity to hospitals and reviewers participating in “good faith” peer review of physicians and dentists. These reviews were envisioned to be vehicles by which it could be determined if any actions or recommendations against a physician should become necessary on the measures of incompetence, unprofessional conduct, or behaviors that impact the doctors’ clinical privileges. However, of late, HCQIA has resulted in many unforeseen consequences, not the least of which is the rise of ‘sham peer reviews’ —and the consignment of guiltless, lifesaving, pre-eminent physicians into obscurity.
What is “Sham” Peer Review?
Sham peer review is an adverse action taken in bad faith by a hospital for purposes other than the furtherance of quality health care. It is a process that is disguised to look like legitimate peer review. But sham peer review is not objectively reasonable, precisely because it is not performed to advance the quality of health care (violation of safe harbor provision).
A sham peer review happens when the hospital invents some pretext on which to attack the physician and acts to disguise the adverse action against the targeted physician by conducting a such a review—where the truth and the facts do not matter, because the process is contrived to be rigged, and the outcome is predetermined.
Over the years, sham peer reviews have unfortunately become fairly well-known. Hospitals in the United States have mounted these proceedings for at least four decades to rid themselves of physicians who “get in their way.” Often, they are doctors who don’t ”follow the party line” and whom they consider “disruptive.” Hospital officials are resistant to physicians who bring patient safety or care quality concerns to their attention. Some hospitals retaliate against these whistleblowers, by instigating these sham peer reviews.
How Sham Peer Review works
Hospitals that use sham peer review bring trumped up, fabricated, and thoroughly false charges against the targeted physician. Although no court of law would permit depriving an accused person of files or records needed to defend himself, as it is fundamentally unfair and in violation of due process, hospitals that employ sham peer review frequently refuse to provide records required to the physician under review. Based on these totally erroneous and phony charges the physician’s hospital privileges are summarily suspended. The physician is usually given 14 days to respond in writing to the sham charges. The charges and the physician’s response are then supposedly shared with the Medical Executive Committee (MEC). The physician then meets with the Medical Executive Committee. The physician is usually denied legal representation (which is unlawful), and the meeting takes the form of a Kangaroo court.
And the above, is EXACTLY what happened to Paul. Like.. to the T. Most importantly, he had no rights during the process. No ability to bring a lawyer in to help defend him. No ability to discover the identity of the complainant or exact documentation of the complaint. That is how they can just make shit up.
I won’t go into the details because the above explains everything that happened to Paul but his was particularly egregious (mine was short and simple). They generated at least 8 anonymous, invented complaints by other providers, nurses and employees inventing things he said or did and characterizing his behavior as “disruptive.” He had never gotten a single complaint from a patient or colleague in his entire career. They even accused him of malpractice for treating a patient for severe COVID who had tested negative for COVID. I saw the patient’s films and labs, heard his history, and presentation. The guy had COVID, period. Plus, the guy was super sick, on a ventilator, and Paul saved him with his protocol. No small feat for a COVID patient on a ventilator. The patient survived yet the hospital used the case as a mark against him. Insane.
Everything was right out of the sham peer review playbook. And it resulted in the ending of his career.
My “sham peer review” was different given that I was working as an independent contractor running an ICU for a hospital in central Wisconsin. The hospital administration had been asking my partners who hired me to get rid of me as soon as they heard I had been hired, likely due to my public profile (ya think?). My partners refused as we got along great and they deeply appreciated my skills, contributions, COVID expertise and protocols. They told the administration “if he goes, we go.” And this was a hospital with a long track record of difficulty recruiting physicians. Yet, my partners were continually harassed by the administration who kept sending them “hit pieces” they found about me in newspapers and magazines.
Six months later, in November 2021, the Chief Medical Officer of the hospital knew I was not vaccinated and that a mandate was about to start. So he called me and asked if I was going to be vaccinated because he had to plan for contingencies. I asked him for a couple of days to think about it. I decided I would just get a vaccine card instead. Not proud of that plan but I knew the vaccines were built on unconscionable lies. He called me two days later, and I told him I would get vaccinated.
The next morning after my shift, my lead partner called and told me “they didn’t need me anymore.” I asked what happened (I knew they needed me, badly). He explained that I had told some ER patient to not get vaccinated and that their practice believed in vaccination so could not be associated with someone who was not. One catch – I had not been in the ER for two weeks. I defended myself, to no avail. My partner knew I was telling the truth, but I knew he was likely under an ultimatum. He apologized and said, “I am so sorry, but there is a war going on and you are unfortunately a casualty of that.” We said pleasant goodbyes and wished each other well. Pretty quick sham peer review because I was not an employee so they had the right to cancel my contract at anytime. Done. Gone.
So, as you can see from the above, COVID is not our first rodeo battling ignorance and corruption in Medicine. But we battled with debate using data, published literature, and deep knowledge of physiology. Now, no more.
Steve Kirsch has been offering 1-2 million dollars for anyone in academia or the agencies to participate in a public or even privately recorded, moderated debate of the evidence to support vaccine safety and efficacy. No-one took him up on it.
An organization in Kansas City asked me, Peter McCullough and two other experts to participate in a debate with the clinical leaders at KU. They refused to show. Their table sat empty on the stage while we debated the public statements they had made with a local TV program instead. They literally told the TV presenter that “we do not debate in public forums, only in journal clubs amongst fellow doctors.” Note he said this on TV then went on to support their policies citing what we know are corrupt and easily disprovable evidence-free narratives. What a farce.
Just as sad as the above is that Paul had long been invited every year by a medical education organization to lecture to anesthesiologists as he was a perennial favorite lecturer. This past year, he gave a masterful lecture on the data supporting the use of ivermectin in COVID. Soon after, he was told that he will never again be invited to give lectures.
He also gave the same lecture to the Anesthesia Department at Mass General (Harvard). The evaluations by attendees all complained that his lecture was full of mis-information. He will never be invited back.
Twitter, which describes itself as a “public square” has de-platformed many of my colleagues (multiple times) for sharing newly emerging data supporting the efficacy of ivermectin. Hey Juan Chamie, how many times have you been Twitterwhacked? One of life’s greatest mysteries (slight overstatement) is how I am still alive on Twitter, although to be accurate, I am only half-alive as they severely shadow ban me on that platform.
I guess we just have to accept the fact that two new commandments have come down from the mountaintop:
- Thou shalt not share favorable ivermectin data in any public media sphere
- Thou shalt not present analyses of the scientific data supporting ivermectin in lectures to physicians
The world has gone mad.
Next post, I will delve more specifically into the tactics Pharma deployed in pulling off their massive Disinformation campaign against ivermectin using propaganda as well as censorship of the FLCCC .
Follow the Science or Follow the Evidence?
Comment on Lord Sumptions’s Times editorial
By Tom Jefferson and Carl Heneghan | Trust the Evidence | August 29, 2022
Throughout restrictions which Lord Sumption called a “catastrophe”, we were exposed to the mantra of “follow the science”. But unfortunately, the only “science” that seems to have been followed in the major decisions is that of modellers and government departments.
Models are akin to opinions. If they are science, the evidence they provide sits on the lowest rung of the ladder. Modellers are accountable to no one; most have never seen a patient in their lives as they have no clinical background, which impedes their understanding of how people behave. Individuals are not herds of buffalos. Some modellers have a consistent track record of getting their predictions dramatically wrong with (again) catastrophic consequences.
Since the start, we have looked at the evidence underpinning the fear-generating narrative pushed by the government, some politicians, the media and many Twitterati, who overnight forgot the principles of scientific investigation, equipoise or uncertainty and the work of many pioneers in respiratory virus epidemiology spanning a century.
The psychotic narrative rests on three legs of what we call the Covid narrative stool.
The first leg is the number of cases. We have shown that misuse of polymerase chain reaction based on a superficial understanding amplified the number of “cases” as many of these were not likely to be infectious at all.
The second leg was the hospital pressure theme. Here using data which should have been available (but is not), we have shown that up to 40% of hospital cases were infected, a phenomenon which shows no sign of abating.
The data from three devolved nations and our interpretation have been serialised on this website.
Finally deaths. A death in epidemiology is the one inevitable outcome you can observe and tally. The question is: what caused it? This is called attribution. Looking at the data from freedom of information requests made by an alert public and the response at times by patronising authorities, we counted 14 different ways of attributing deaths to Covid-19. The first prize for the most bizarre was the Care Quality Commission’s: they left it to the care provider to decide the cause of death. So it is possible that administrators decided what role SARS-CoV-2 played in your grandmother’s death. In one health authority’s case, deaths of people who tested “negative” were rolled into the Covid total.
So the catastrophe described by Lord Sumption was underpinned by very weak evidence; science was nowhere to be seen. Consequently, it remains impossible to separate the impact of SARS-CoV-2 from that of the policies designed to “combat” it.
As the usual sources start gearing up to call for a new round of interventions and restrictions, have these massive cracks in evidence gathering and interpretation been tackled?
Hands up, who’s got the answer?
Brits told to get used to drinking recycled sewage
By Thomas Lambert | The Counter Signal | August 29, 2022
British Environment Agency CEO James Bevan says that Brits should get used to the idea of having to drink recycled sewage in times of water uncertainty.
“We need to treat water as a precious resource, not a free good,” writes Bevan in The Sunday Times. “We will have to be more selective about what we use drinking water for. It makes no sense to use it to clean the car or water the lawn.”
“We will need to be less squeamish about where our drinking water comes from. Part of the solution will be to reprocess the water that results from sewage treatment and turn it back into drinking water — perfectly safe and healthy, but not something many people fancy.”
Bevan continues, explaining that, besides getting Brits to drink recycled sewer water, the government is specifically looking into ways to “help reduce personal water consumption” through measures such as “mandatory water-efficiency labelling for household goods.”
Bevan says that due to droughts and record low rainfall, rivers and reservoirs have fallen to dangerously low levels (not just in the UK but in several European nations), which the government has so far addressed by applying a hosepipe ban on millions along with several other restrictions.
As the UK struggles to keep up with the demand of its growing population — with most growth mainly being a result of immigration — and due to the impact of supposed climate change, he now expects that water security will be one of the government’s chief concerns over the coming years.
“Having enough water is at the heart of the climate emergency and an existential challenge,” Bevan writes. “If we don’t change gears and step up now, we will hit what I’ve called the “Jaws of Death.”
Featured Video

US Middle East Policy: The Growing Propensity for Genocide
or go to
Aletho News Archives – Video-Images
From the Archives
The New Baghdad Pact
By Dr Bouthaina Shaaban | February 23, 2017
A recently declassified CIA document prepared in 1983, and released on 20 January 2017, shows that the United States had at the time encouraged Saddam Hussein to attack Syria, which would have led to a vicious conflict between the two countries, thus draining their resources.
The report, which was then prepared by CIA officer Graham Fuller, indicates that the US tried adamantly to convince Saddam to attack Syria under any pretense available, in order to get the two most powerful countries in the Arab East to destroy each other, turning their attention away from the Arab-Israeli conflict. … continue
Blog Roll
 Aletho News
Aletho News- Hezbollah denies involvement in deadly attack on UNIFIL in south Lebanon
- The prospect of an expanded and far more violent war
- Canada’s Carney Revives Online Censorship Bill
- Israeli soldiers kill UNICEF truck drivers delivering water to Gaza families
- Iran defends limits on Strait of Hormuz passage
- ‘We warned you’: Hormuz Strait back to pervious state amid US blockade
- Iran rejects uranium transfer, warns of response to naval blockade
- US Middle East Policy: The Growing Propensity for Genocide
- Daniel Davis: Iran Reopens the Strait of Hormuz
- Trump taps military-grade flu pandemic architect to lead CDC amid simultaneous gain-of-function and vax development
- If Americans Knew
- Israel relegates another population to life in tents – Daily Update
- Senate again fails to block weapons to Israel
- Think the Iran war is a disaster? Blame these DC think tanks first.
- Number of Palestinian Prisoners Rises By 83% Since October 2023
- With multiple “ceasefires” in place, Israel keeps on killing in Gaza and Lebanon – Daily Update
- Mearsheimer: Israel Owns Trump
- Mark Levin and Jonathan Pollard Push for Nuking Iran
- TCN: America Enables Israel’s Crimes
- Israel’s Next Leader Will Be Just Like Bibi – but Without the Corruption
- Born into war, raised across borders: The story of Gaza’s premature babies separated from their parents amid Israel’s genocide
- No Tricks Zone
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
