Brits told to get used to drinking recycled sewage
By Thomas Lambert | The Counter Signal | August 29, 2022
British Environment Agency CEO James Bevan says that Brits should get used to the idea of having to drink recycled sewage in times of water uncertainty.
“We need to treat water as a precious resource, not a free good,” writes Bevan in The Sunday Times. “We will have to be more selective about what we use drinking water for. It makes no sense to use it to clean the car or water the lawn.”
“We will need to be less squeamish about where our drinking water comes from. Part of the solution will be to reprocess the water that results from sewage treatment and turn it back into drinking water — perfectly safe and healthy, but not something many people fancy.”
Bevan continues, explaining that, besides getting Brits to drink recycled sewer water, the government is specifically looking into ways to “help reduce personal water consumption” through measures such as “mandatory water-efficiency labelling for household goods.”
Bevan says that due to droughts and record low rainfall, rivers and reservoirs have fallen to dangerously low levels (not just in the UK but in several European nations), which the government has so far addressed by applying a hosepipe ban on millions along with several other restrictions.
As the UK struggles to keep up with the demand of its growing population — with most growth mainly being a result of immigration — and due to the impact of supposed climate change, he now expects that water security will be one of the government’s chief concerns over the coming years.
“Having enough water is at the heart of the climate emergency and an existential challenge,” Bevan writes. “If we don’t change gears and step up now, we will hit what I’ve called the “Jaws of Death.”
The narrative managers have done their best to memory-hole the Nurenberg Codes

By Helen of desTroy | August 28, 2022
You would be forgiven for not knowing that last Friday was the 75th anniversary of the Doctors’ Trial, one of 13 Nazi war crimes trials conducted at Nuremberg after World War II and the event that birthed the Nuremberg Codes, the most important medical ethics document of the modern era. The Codes set ground rules for requiring informed consent from experimental test subjects; they anchor international agreements like the Helsinki Declaration, the Geneva Convention and the United Nations’ International Covenant on Civil and Political Rights and have been codified into law in the US and other countries.
Sixteen doctors were found guilty at Nuremberg of murder and torture for carrying out a euthanasia program on mentally and physically disabled German citizens deemed “unworthy of life” and experimenting on concentration camp inmates; nine were jailed and seven were executed. Yet the expected flood of commemoratory articles and events marking the anniversary of the Allies’ crowning (if illusory) moment of moral superiority over those Evil Nazis™ has not materialized. It’s downright unnatural for the US and Europe to miss a chance to give the dead Nazi horse a good beating, but any attempts to even discuss the Nuremberg Codes in the last two years have been squelched by militant fact-checkers. Meanwhile, a coterie of corrupt “public health professionals” and the international financial cartels who control them have pulled off perhaps the most shocking and deadly crime against humanity ever committed.
The Big Lie
Mentioning Nuremberg during Covid-19 was asking to be pilloried in the “respectable” press as an anti-science, horse-paste-guzzling right-wing extremist. Fact-checkers came out of the woodwork to reflexively deny that the Nuremberg Codes applied to any aspect of the Covid-19 response, from forced masking to vaccine mandates, sometimes issuing two denials in a single day in their compulsion to keep the claim from spreading. One particularly tenacious fact-check even took issue with the claim “It was the doctors on trial in Nuremberg,” arguing that because the other 12 trials put Nazi Party officials, lawyers, and corporate executives in the dock, the statement “lacked context.”
This display of ideological lockstep was supposed to intimidate anyone who wasn’t already 100% allied with society’s enlightened institutions in defense of The Science™ against the irrational, emotionally-driven forces of ignorance. Those still on the fence about getting their “Warp Speed” car-crash of a shot were shamed by peer pressure psyops like the UK’s “Clap for our carers,” while social media was seeded with controlled but approachable “experts” who carefully crafted the illusion of overwhelming consensus that the measures being taken in the name of “stopping the spread” were not only scientifically but morally beyond reproach.
But this wasn’t an organic moment of unity. These “fact-checkers” have all received big money from the Bill & Melinda Gates Foundation, the eugenics enthusiasts who have rapidly become the most powerful force in global health policymaking and who also control huge chunks of the education, agriculture, and “green” energy spheres. Most fact-checking organizations pay lip service to the rules set by the International Fact-Checking Network, which while it sounds like an upstanding professional association that’s been around a while was actually launched less than a decade ago. The IFCN, which admits it doesn’t follow its own code of principles, has been funded since its 2015 beginnings by the Gates Foundation, the Omidyar Network, George Soros’ Open Society Foundations, Google, Facebook, the US State Department, and CIA cutout the National Endowment for Democracy, among others. It’s hard to think of a worse group of stewards for a gaggle of helpless facts, aside from perhaps the Wikimedia Foundation, about which more later.
The IFCN is run by the Poynter Institute, a “journalism education” nonprofit funded by many of the same entities as its IFCN subsidiary. Loaded down with enough conflicts of interest to make that code of principles swoon, Poynter selects, sponsors, and trains journalists, prioritizing obedience to authority, ideological inflexibility and a total absence of shame. They are then turned loose to mow the internet’s epistemological lawn in military fashion, doxxing some popular opposition voice while merely tagging others for later deplatforming, arrest, or worse. The tactic’s resemblance to the work of Ukrainian vigilante website Mirotvorets, unofficially operated by the country’s Ministry of Information, is unlikely to be an accident, given that Omidyar and Soros both poured billions of dollars into 2014’s Maidan Square color revolution, which was itself choreographed by the State Department’s Victoria Nuland, who knows the value of a well-placed bullet or a warm cookie.
It’s easy to see why Gates just had to buy the industry for himself. If these fact-checkers could reinvent the most corrupt government in Europe, whose military was exposed by dozens of major western media outlets as a hive of neo-Nazi thugs, as a democratic paradise, surely they could spin the vaccine tycoon’s Final Solution as the solution to all humanity’s problems. The Covid-19 experiment saw the closest collaboration yet between the fact-checkers, Big Tech and governments around the world to construct an epistemological roach motel that users could enter easily but would face growing barriers – warning screens, computer failures, personal attacks, deplatforming, financial hardship and a lowered social credit score – if they tried to leave.
It’s no exaggeration to say Poynter’s army of fact-checkers set the narrative of Covid-19 for the public from Day One (or should we call it Year Zero?). The IFCN’s “Coronavirus Alliance” launched in January 2020, before most Americans even knew what a coronavirus was. While the first Twitter users in the western hemisphere were stumbling across bizarre videos of Chinese people dropping to the ground and convulsing, explained in the accompanying broken-English text to be the result of an unknown virus, the fact-checkers were implementing orders from their paymasters. One of the first narrative touchstones, the red and white 3D model of the coronavirus, soon became as ubiquitous as the footage of planes hitting towers on 9/11, triggering intense fear and doubt directed both at the outside world and at the self. After all, they might be an “asymptomatic carrier,” and the only way to be sure was to isolate from their loved ones. As with 9/11, this unfamiliar terror pushed the individual to seek solace in an increasingly totalitarian state that insisted its ‘tough love’ – locking us in our homes, forbidding us from earning money, and keeping us from our families – was for our own good. Frightened and confused, many turned on the TV and sucked down its narcotizing propaganda. Even CNN’s ratings went up that first pandemic year, as Chris Cuomo demanded Americans “sacrifice the me to the we” and compared binge-watching Netflix to landing on the beaches of Normandy while his brother mass-murdered elderly New Yorkers.
The complex choreography of the Covid-19 response could not have unfolded as it did without premeditation. The plot was lifted – not plagiarized, as the authors were the same – from Event 201, the tabletop coronavirus simulation sponsored by the Gates Foundation at Johns Hopkins University’s Center for Public Health Security. This took place just a month after the Global Preparedness Monitoring Board – the product of an unholy marriage between the WHO and the World Bank earlier that year – released a report demanding all UN member countries “conduct at least two system-wide training and simulation exercises” by the following September, “including one for covering the deliberate release of a lethal respiratory pathogen.” Video of Event 201 shows players uninterested in minimizing harm from the virus instead exploring how the “emergency” might be used to stifle undesirable narratives and ram through major changes in society. The “real” pandemic – simulation number two, by the GPMB’s counting – played out months later exactly along the exercise’s script. The WHO, Gates, the World Economic Forum and Big Business took the reins, filling the power vacuum left while individual governments, seemingly baffled by the outbreak despite having repeatedly run their own simulations, ran around in circles.
How to treat an Infodemic
The crisis was planned and then used to crack down on unauthorized views under the reasoning that humanity was in the midst of an infodemic – a surfeit of information encouraging irresponsible beliefs – and careless talk could cost lives. Spreading dissenting opinions could infect friends and loved ones with the virus of doubt, which while perhaps less deadly than the virus itself (with its 99.7% survival rate), could cause society to fracture at a time when all humanity had to unite or be destroyed by the invisible enemy. Reading or hearing “disinformation” about Covid could reduce one’s likelihood of getting vaccinated, putting one’s very life at risk.
Convincing test subjects to discard their self-preservation instincts and their critical capacity and embrace the most absurd statements as gospel truth was the main goal of the first part of the Covid-19 experiment, and given the single-mindedness with which the WHO zeroed in on the “infodemic” before it had even officially declared the real virus to be a pandemic, it’s hard to believe they were making it up as they went along, especially given that the term was allegedly invented during the original SARS outbreak in 2003 (by a Washington Post writer no less) and then apparently put on ice until almost two decades later. Seeking input on how to respond to this new threat, the WHO reached out to professionals of all stripes, with more than a quarter of advisory input coming from academics eager to test out their juiciest hypotheses on real people with no repercussions. Everyone who used social media in 2020 to discuss the Covid-19 pandemic and its aftermath thus became a test subject, “nudged” and prodded for the Public Good, and some of those experiments – particularly those aimed at developing an FBI-style psychological profile of believers in “conspiracy theories” so they can be locked up as domestic terrorists or institutionalized as incurable monsters are very much ongoing.
Those early academic papers describe a chaotic infosphere in which the WHO’s narrative failed to dominate on its merits alone. The academics rose to the challenge, burnishing their half-baked speculations with scientific-looking graphs and charts. Their solutions ranged from Orwellian – deploying “freedom of expression officers” to censor and label rogue content as much as European human rights law would allow; re-education programs for “influencers,” teachers, priests, and other likely “superspreaders,” who could then be suspended from social media entirely if they refused to get their minds right – to the lesser evils of sending in fact-checkers as the equivalent of UN peacekeeping troops to help “inoculate” social media users against the disinformation they were about to see. With distrust in public and private institutions hitting new highs, society didn’t just need a vaccine against the scary new virus, it needed one against “disinformation” as well! But like the Covid vaccines themselves, these digital inoculations didn’t come with an informed consent notice, and the clinical trial results aren’t looking good.
Experiment #1: Shock “therapy”
As the WEF’s Klaus Schwab himself admitted in his pandemic tome The Great Reset, Covid-19 is the least deadly ‘pandemic’ in the last two millennia. But he’s quite open about wanting to use the largely self-inflicted Covid-19 “crisis” to bring about the Fourth Industrial Revolution, a transhumanist “green” dystopia lovingly crafted for “stakeholder capitalists” and inspired by technocratic parasites like Yuval Noah Harari. This is no experiment for the “good of society,” nor are any efforts made to “avoid unnecessary mental and physical suffering,” as Nuremberg demands. If anything, the experiment’s designers deliberately ratcheted up the suffering, believing this was necessary to unfreeze the fixed ideas of western civilization – free will, individuality, rationality, democracy (not to be confused with Our Democracy™) in our minds and replace them with the WEF’s preferred picks: obedience, “equity” (a Newspeak term meaning equality of outcome rather than equality of opportunity), credulity, communitarianism. The group has admitted on its own website that the lockdowns and the rest of the “touchless torture” the Covid response has supposedly required constitute the “world’s biggest psychological experiment.”

The Great Reset is an especially noxious experiment in that it violates the minds and bodies of test subjects on multiple levels, burrowing down into the way we think in its megalomania. It’s the spiritual offspring of CIA-funded Canadian psychiatrist Ewen Cameron, who “de-patterned” his patients’ personalities with high-voltage electroshock, induced coma, and mega-doses of LSD, then attempted to’ ‘build them back better’ by playing their comatose forms 16 hours of tape-recorded messages at a time; and Milton Friedman, the University of Chicago economist and godfather of neoliberalism whose students, the so-called “Chicago Boys,” conducted campaigns of economic “shock therapy” on third-world nations the US worried were too left-wing, assisting far-right leaders in seizing power, further impoverishing the masses with austerity programs, terrorizing what political opposition remained with death squads and disappearances, and privatizing all state-run industries so as to attract foreign investors. Neither Cameron’s patients, most of whom came in with simple problems like anxiety or depression (and one of whom wasn’t even seeking treatment but just looking for a job) and left as husks no longer able to even use the bathroom themselves; nor the inhabitants of Chile, Brazil, Uruguay, Indonesia, Russia, or any of the long list of other countries subject to some variation on Chicago School shock treatment over the years, were ever told they were part of an experiment, let alone asked if they wanted to be.
The Great Reset has not only targeted the entire world with economic shock therapy, triggering a massive depression the current financial system is unlikely to ever shake off (spoiler alert: another experiment coming…) – it funneled unprecedented amounts of fear into populations already thrown off balance by the blinding speed of policy shifts. First scolded for “selfishly” wearing a mask, then attacked for “selfishly” not wearing one; informed their city would be “locking down” at 10pm, when a peek out the window yielded crowds of restive youths hanging out on the corner with nary a cop in sight; told vaccinations were mandatory for school, then told their child could have just “masked up” when little Polly drops dead of a heart attack not 24 hours after her first shot of Moderna; the average person soon lapsed into learned helplessness and became a shut-in, depatterning daily in the glow of the television as they degenerated into an obedient vegetable, capable of “masking up” and socially distancing but little else. Despite leaving a horrific trail of devastation in their wake, the experimental lockdowns were praised by the WEF for the slight dip in carbon emissions they caused, all but guaranteeing phase II of the nonconsensual clinical trials – climate lockdowns – will be rolled out within the year.
Experiment #2: Hackable animals
Given the mountain of evidence against them, it’s perfectly logical that the ruling class would have tried to build up an impenetrable fort of bullshit using their captive fact-checking industry to deflect accusations of war crimes under the Codes. Several patterns pervade the apologist coverage, starting with the idea that these brand new mRNA Covid vaccines, tested on under 100,000 people by Pfizer and Moderna combined (and none who were pregnant or nursing) before receiving their coveted emergency authorization, are somehow not experimental procedures. They use the synonym investigational instead, as ‘experimental’ tends to trigger thoughts of, well, human experimentation, authoritarian regimes, the very Nuremberg Nazis the media establishment is trying its best to keep the average reader away from. But the effect is the same – mRNA vaccines of any kind weren’t tried on the general population until the end of 2020, and the torrent of side effects and death that has been unleashed in the meantime suggests neither Moderna nor Pfizer had informed consent from these gen-pop guinea pigs.
That’s a big deal, because Pfizer knew before it sought emergency authorization that more vaccinated test subjects had died than unvaccinated subjects – it even fudged the numbers for the FDA. Some 1,200 trial participants died in the 90 days following their injection, and Pfizer made sure to vaccinate the placebo group at the end of the trial in order to make sure further comparisons didn’t spoil its story. Indeed, it was so sure its vaccines were going to leave a pile of bodies behind that it refused to even sell them to countries whose governments wouldn’t shield them from liability for the damage caused. One should have expected this from a company with the dubious distinction of paying the largest fine in Justice Department history in 2009 for healthcare fraud, off-label prescribing, misleading marketing and miscellaneous criminality. Nevertheless, they won the “Warp Speed” lottery under Albert Bourla, a veterinarian with a doctorate in the biotechnology of reproduction who was for some reason promoted to CEO of the entire (human-focused) drug company a year before the Covid-19 outbreak. Given that his primary achievement prior to Operation Warp Speed was developing a “vaccine” that chemically castrated boars without ruining the meat, it becomes much more difficult to see the utter disaster the mRNA vaccines have created for both male and female fertility as an accident.
Still questioning authority? The fact-checkers then attempt to distance vaccine mandates – along with health passports, mask mandates, lockdowns and the other psychological aspects of the experiment conducted on the unwitting populace – from the Nuremberg zone by categorizing them as “public health interventions,” not research, or experiments. The Codes simply do not apply. Never mind that public health interventions are supposed to be evidence-based, and no western democracy has ever engaged in anything like the Covid lockdowns before, or that the CDC pulled the six-foot social distancing rule out of its ass, or even that the only “science” backing closing schools to “stop the spread” was a computer model from a 16 year old’s science project. Lockdowns arguably killed more people than Covid-19, and they have cut short many more lives by impoverishing, immiserating, and isolating millions. Arguing public health measures can’t be experimental because they’re public health measures is merely a last-ditch effort to wall the Codes off in a museum, inapplicable to anyone but those nasty Nazis who were – as the narrative managers never tire of reminding us – a unique and special case.
Discouraging cross-time contextualization is very important to the fact-checkers, who aren’t hesitant to shoot the messenger if all else fails. Anyone talking about the Nuremberg Codes in the context of Covid-19 is dismissed as an “alt-righter”, a “covid crazy,” dangerous “extremists,” “anti-vaxxers,” or even actual Nazis who apparently got confused about whose side their team was on back in WW2. In war, dehumanizing the enemy is key to beating him, and this is nothing if not a two-pronged war being fought in our brains and our bloodstreams. “Drawing a link between this final rollout of these vaccines and what the Nazi doctors were doing is morally grotesque,” the British Medical Association’s Dr Julian Sheather told FullFact ; he didn’t explain why, and it’s not apparent why one should not draw parallels between the two cases. According to the Vaccine Adverse Event Reporting System (VAERS), whose own creators admit it contains less than 1% of all adverse events associated with a given vaccine, the Covid shots have already caused nearly 30,000 deaths, over 170,000 hospitalizations, nearly 16,000 heart attacks (a common sight now on sports fields, where 60 times more athletes than normal are flatlining mid-game), and nearly 5,000 miscarriages in the US alone. Using tech entrepreneur Steven Kirsch’s calculations, the numbers are much higher: at least 478,000 Americans have been killed by Covid vaccines, to say nothing of millions permanently disabled, unable to work or function on a basic level. Worldwide, the number of deaths approaches 12 million.
While the number of victims the Nazi doctors left behind is not so meticulously recorded, especially given the high levels of typhus and malnutrition contributing to the mortality rate in the camps, one source has them consigning between 70,000 and 100,000 “unfit” Germans to death between 1939 and 1941 while sterilizing hundreds of thousands more – a detail that once again should send a chill down the spine of anyone who’s noticed the declining birthrates around the world. If the figures aren’t comparable, that’s only because the mRNA vaccine has been so much more efficient in its killing. There’s nothing “morally grotesque” about pointing that out. But since “everybody knows” the Nazis were the pinnacle of Evil™, the realization that Pfizer and Moderna’s death toll might have their doctors beat must be prevented at all costs. Thus even bringing up Nuremberg in relation to Covid-19 is deemed to be “trivializing” the crimes of the Nazis, even when the intention is to draw attention to the seriousness of their modern descendants’ crimes, and efforts are made to further poison the dialogue by suggesting there’s something antisemitic about the whole business.
In Part II: the war on “conspiracy theories,” why Nuremberg is to be memory-holed, infodemic terrorism, and more…
Exhaustive study of German mortality data finds excess deaths tightly correlated with mass vaccination
eugypius | August 27, 2022
Excess mortality in Germany 2020–2022 is a preprint by Christof Kuhbandner (a psychologist at Regensburg) and Matthias Reitzner (a statistician at Osnabrück) that applies sophisticated actuarial analysis to the publicly available all-cause mortality data provided by the German government. It turns out that when you account for historical mortality trends, the virus no longer looks so dangerous, and the vaccines no longer look so great.
From the abstract:
In 2020, the observed number of deaths was close to the expected number with respect to the empirical standard deviation. By contrast, in 2021, the observed number of deaths was two empirical standard deviations above the expected number. The high excess mortality in 2021 was almost entirely due to an increase in deaths in the age groups between 15 and 79 and started to accumulate only from April 2021 onwards. A similar mortality pattern was observed for stillbirths with an increase of about 11 percent in the second quarter of the year 2021.
Something must have happened in April 2021 that led to a sudden and sustained increase in mortality in the age groups below 80 years, although no such effects on mortality had been observed during the COVID-19 pandemic so far.
What happened in April 2021 was the beginning of mass vaccination across Germany.
Here’s an overview of mortality deficit or excess by age bracket:
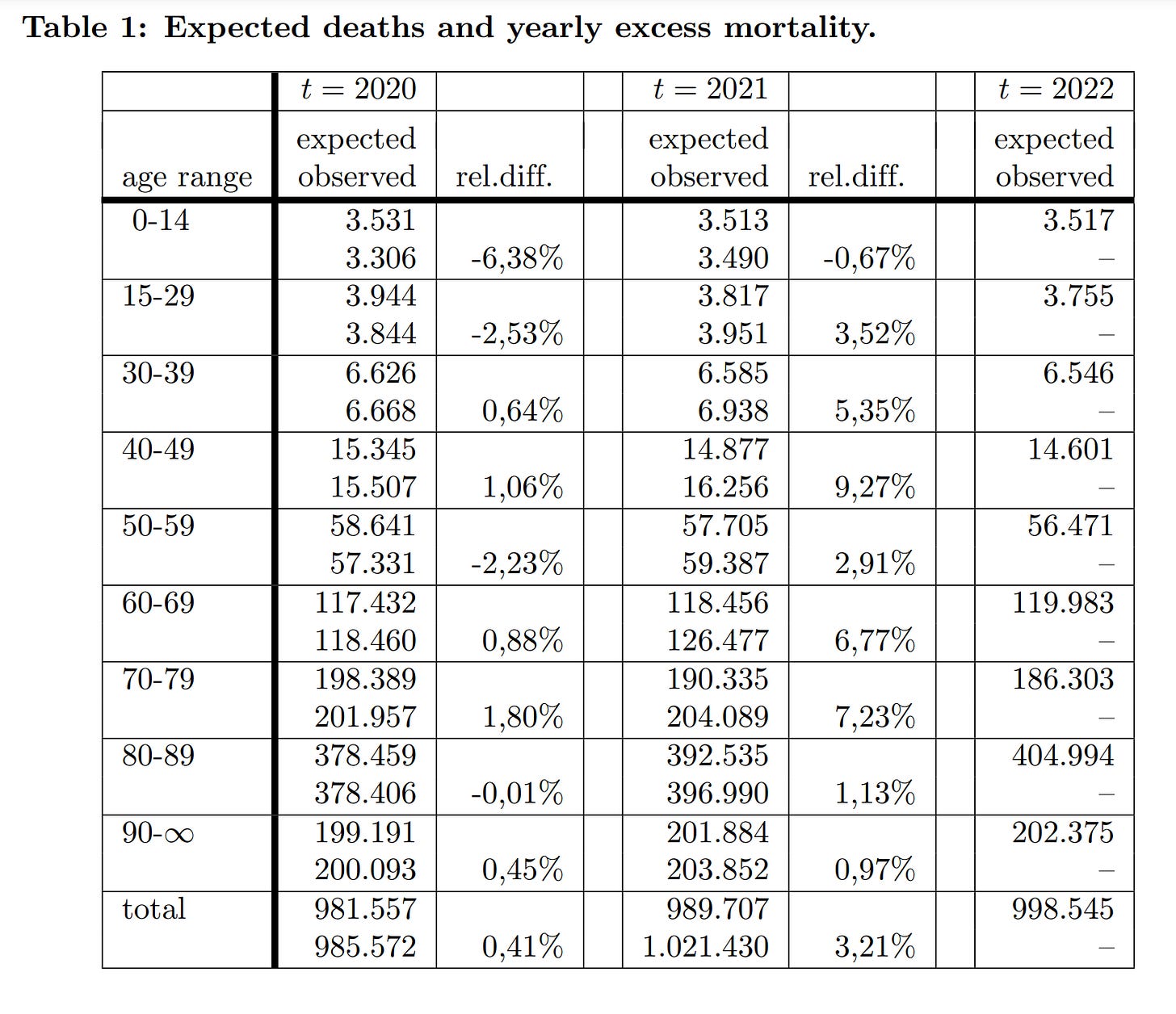
As I’ve said many times, the first year of the German pandemic was a total nothingburger. There was no heightened mortality trend save for among the oldest groups, briefly, in December. In 2021, however, the Year of Maximum Vaccination, the authors estimate almost 32,000 excess deaths. Mortality rose across the board, especially among youngs, with those in their 40s seeing 9% more deaths than expected by their model.
Here are the same figures visualised:
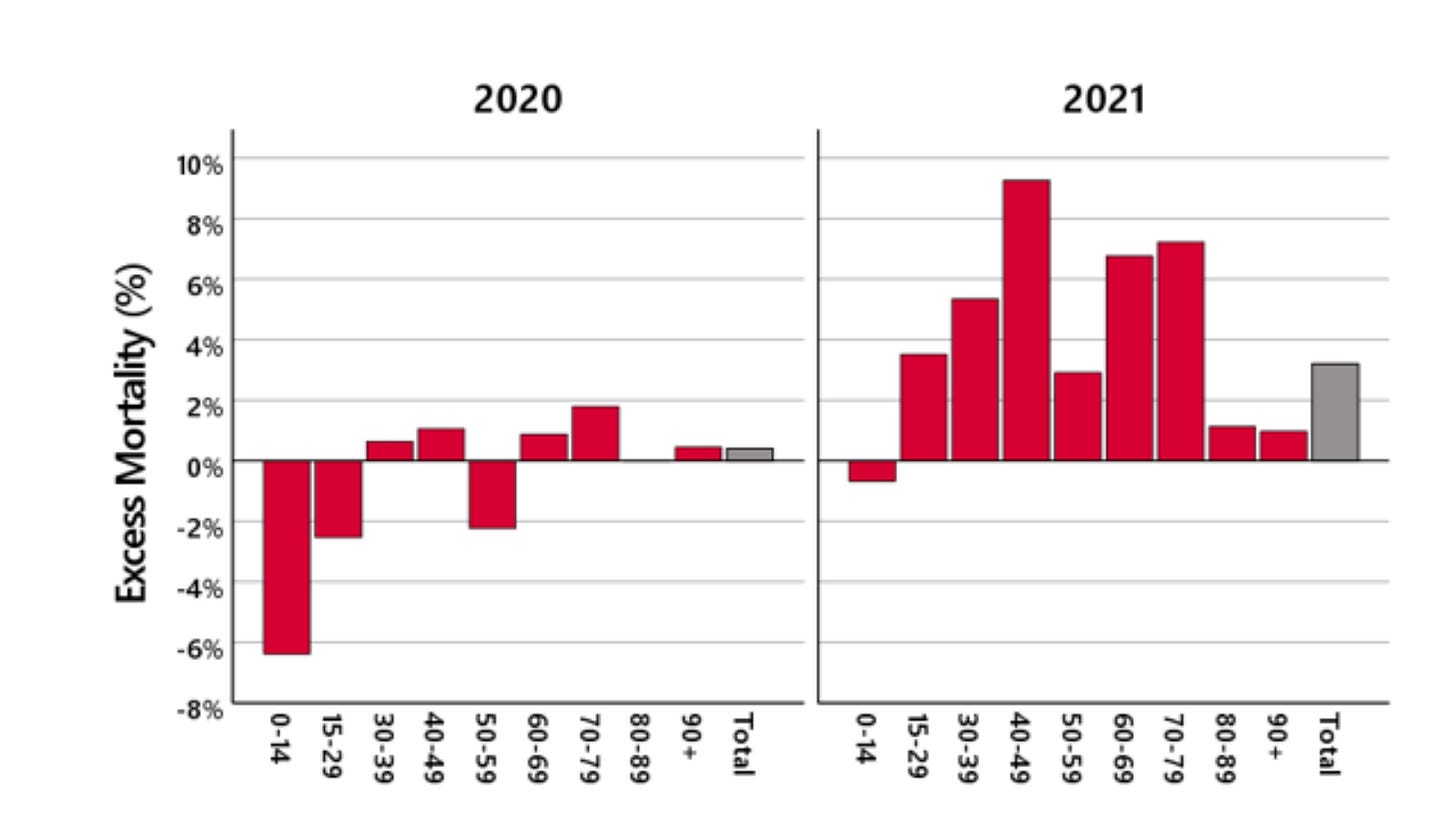
Just looking at that 2021 graph, you can tell there’s something really wrong here. If it’s virus doing all this killing, why is it hardest on people aged 15 to 79? How is it leaving the oldest Germans almost entirely unscathed?
The authors also provide a month-by-month breakdown for the 15-59 age-group:
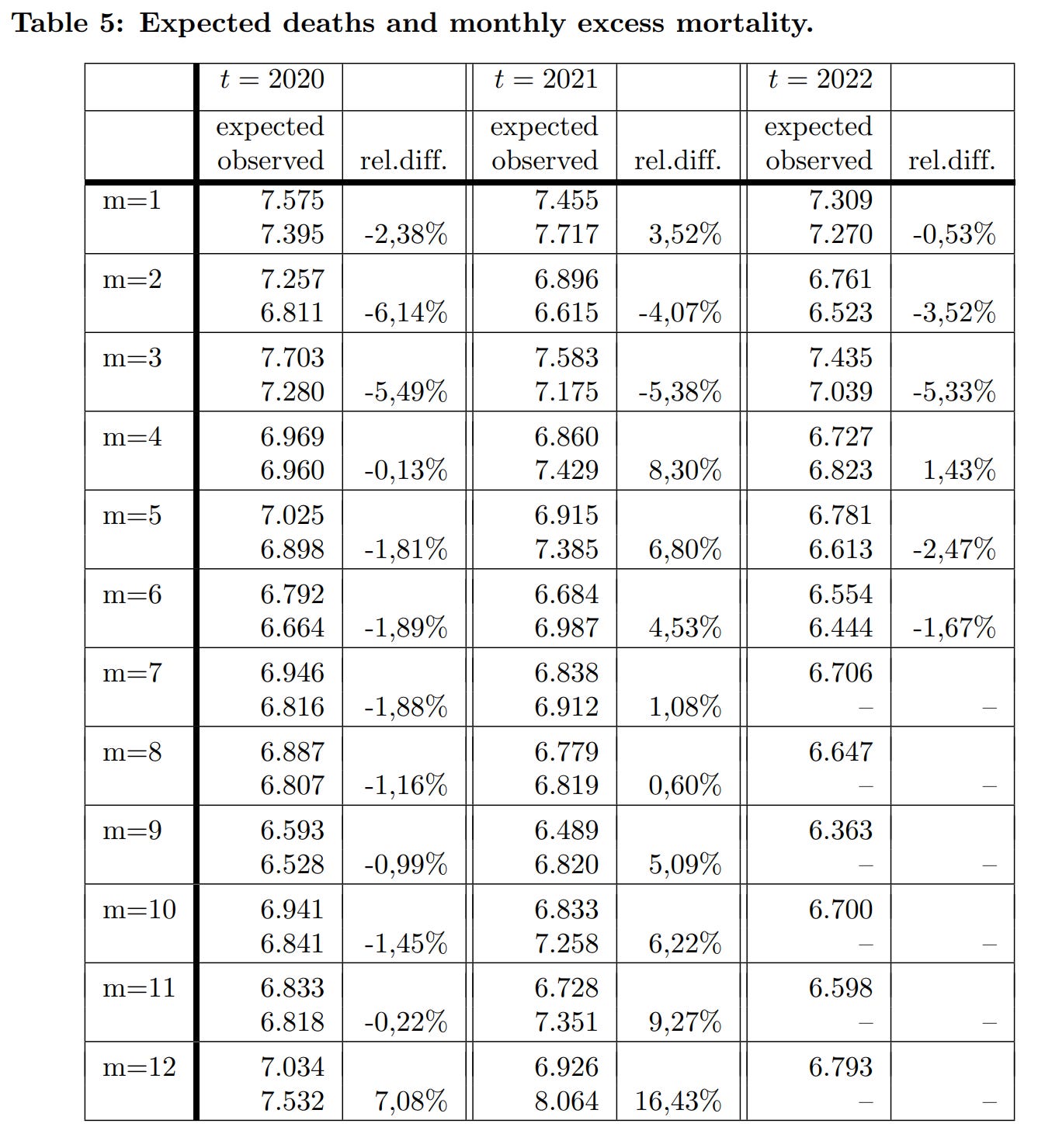
They note that “The significant excess mortality in December 2020 continues slightly in January 2021, and then is mostly compensated until March 2021. That is, by the end of March, the cumulative excess mortality was close to zero.” These are what the funeral industry would call “pull-forward” deaths. In Germany, the virus mainly kills people who are about to die anyway, such that mortality spikes are followed by counterbalancing mortality deficits.
The authors continue:
In April and May 2021, a significant increase in excess mortality is observed, followed by a decrease up to August. However … the increase in excess mortality in April and May is not compensated for. In September there is again a significant excess mortality, which increases in November and is more than doubled in December 2021.
The April increase obviously coincides with the vaccine rollout, while the Fall increase aligns fairly well with the booster campaign. It’s noteworthy that dose 2 doesn’t seem as dangerous as dose 1 or 3; and that the mortality signal is very tightly correlated with the date of vaccination. As soon as you stop vaccinating, excess deaths recede.
As for people 60 and older, there are two distinct trends: Rising mortality coinciding, again, with the mass administration of doses 1 and 3 in the 60-79 bracket, and nothing special in the 80+ bracket:
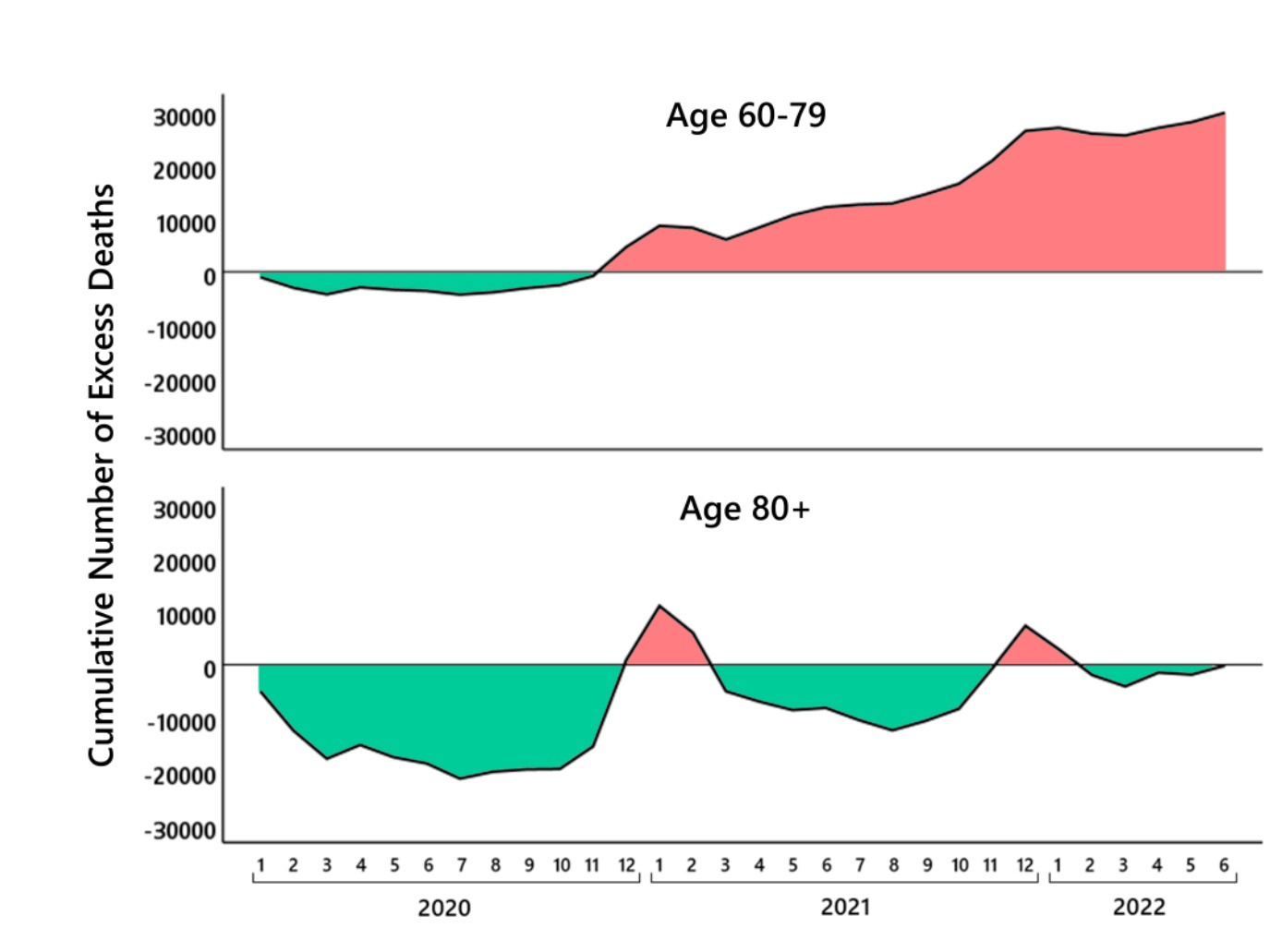
The vaccines obviously do most of their harm by inducing adverse immune reactions, and thus they’re relatively safe in the very elderly, who have weaker immune systems. This makes the oldest Germans a useful control, as they are the most sensitive to virus-associated mortality, and the least sensitive to vaccine-associated mortality. Thus, to anyone who objects that it’s really the April case spike that’s making the vaccines look bad here, or that it’s Delta causing those problems in the Fall, the reply is simple: The olds aren’t dying in April or September 2021, just the youngs. What kills mainly the youngs and spares mainly the olds? The answer is not SARS-2.
As the authors note:
The maybe most surprising fact is that [2021] produces in all age groups a significant mortality increase, which is in sharp contrast to the expectation that the vaccination should decrease the number of COVID-19 deaths. The only exception is the last age group [80+] … However, when interpreting this finding, it has to be taken into account that there wa sa huge mortality deficit in 2019 and until October 2020 which was compensated in November [and] December 2020 and January 2021.
It becomes very hard to doubt that the excess mortality of 2021 is vaccine related, when you compare the relative chronology of deaths and mass vaccination:

There are also more specific mortality correlations by age bracket. Thus the authors note the “further hint” that the vaccines are implicated in these deaths, “is the fact that the age group 0–29 has a peak in the excess mortality in June 2021 instead of April 2021,” precisely when these younger cohorts were lining up for their first dose.
A final intriguing finding relates to the relationship between official Corona death numbers and excess mortality. Nobody will be surprised to learn that the SARS-2 death toll is egregiously inflated, but the age-cohort patterns are worth a look:

The official figures are most accurate for those in their 60s and 70s. For those over 80 years old, they are almost entirely meaningless. This group saw less than 20,000 excess deaths in two-and-a-half years of Corona, while their official death count is approaching 100,000.
It’s no wonder that nothing—not lockdowns, not vaccines, not masks, not all the tests in the world—can drive down all-cause mortality in Germany. Most of the people the virus kills are on the verge of dying anyway, and if you spare them a death from SARS-2, they’ll just die of something else next month.
If It’s Okay for Mice, It’s Good Enough for People, Right?
By Madhava Setty, M.D. | The Defender | August 26, 2022
Its audacity on full display, Pfizer — arguably the most criminal corporation in history — has asked the U.S. Food and Drug Administration (FDA) to greenlight its new bivalent COVID-19 vaccine that targets the Omicron BA.4 and BA.5 subvariants for people 12 and older “to help the country prepare for potential fall and winter surges of the coronavirus,” Pfizer CEO Albert Bourla said in a statement.
Bourla’s good intentions are sadly thwarted by FDA regulations that require an Investigational New Drug (IND) application be submitted and approved before a drug can be tested in humans.
Luckily, the FDA can circumvent the inconvenience of its own regulatory processes by allowing itself the ability “to authorize use of an experimental drug in an emergency situation that does not allow time for submission of an IND in accordance with 21CFR, Sec. 312.23 or Sec. 312.20.”
Section 312.20 of the Code of Federal Regulations specifies that a clinical investigation cannot commence until an IND application has been submitted and approved. Nevertheless, Pfizer on Monday submitted an IND for its new formulation.
Now that the FDA and Pfizer have crossed their Ts and dotted their Is to make sure all the rules are followed, how do we know these products are safe and will work?
This is where the rodents come in — the products seem to work on mice.
As NPR reported, “For the first time, the FDA is planning to base its decision about whether to authorize new boosters on studies involving mice instead of humans.”
Yes, it’s an unprecedented move by the FDA, but Dr. Ofer Levy, professor of pediatrics at Harvard and advisor to the FDA argues that the country has had enough experience with the vaccines at this point to be confident the shots are safe and that there’s not enough time to wait for data from human studies.
He has a point. There were still only 30,479 uninvestigated deaths reported in VAERS after administration of the shots as of Aug. 19.
In any case, why should the FDA be concerned with such things as human studies in the first place?
This maneuver by the FDA may finally unshackle the agency from its overly restrictive responsibility to fulfill its own mission and become more agile in bringing products to market.
Not to be left behind, Moderna also requested the FDA authorize its bivalent vaccine for human beings over the age of 17.
Similar to the Pfizer vaccine, Moderna’s vaccine also, for good measure, will encode for the spike protein for the original ancestral SARS-CoV-2 strain, which for all intents and purposes, does not exist on our planet any longer.
Meryl Nass, M.D., summarized it this way:
“No clinical trials. (You need to obtain an IND before you can start testing the vaccine in humans. Pfizer applied 4 days ago.)”
Taking no chances, the FDA will not convene the Vaccines and Related Biological Products Advisory Committee (just like the first time the FDA authorized boosters) and has announced this today to see how much opposition the agency gets.
Can we dispense with the pretense any of this is about health?
No sane person vaccinates the entire country with an experimental vaccine without trials — particularly since the whole country already has some immunity, the virulence is low and the evidence supports higher all-cause mortality with an increasing number of vaccine doses.
What is in the vaccine that they are desperate to inject us with?
Madhava Setty, M.D. is senior science editor for The Defender.
This article was originally published by The Defender — Children’s Health Defense’s News & Views Website under Creative Commons license CC BY-NC-ND 4.0. Please consider subscribing to The Defender or donating to Children’s Health Defense.
Norwegian Schools Are Disseminating Government-Approved Covid Misinformation

BY KATHRINE JEBSEN MOORE | THE DAILY SCEPTIC | AUGUST 26, 2022
Who needs conspiracy theorists when you’ve got school books teaching children that Covid vaccines are “95% effective”?
This autumn, a new school book was introduced for the ninth grade in Norway. Fabel 10 was revised in 2021/22, but has only now been introduced in schools across Norway. Not only does the book overstate the effectiveness of the novel mRNA vaccines, it decries anyone questioning that as conspiracy theorists.
One excerpt reads:
Since the Covid pandemic broke loose, Covid deniers and vaccine sceptics have spread disinformation about coronavirus through social media. They claimed among other things that COVID-19 was no more deadly than the flu, that the vaccine was dangerous, and that restrictions were unnecessary. On Saturday March 20th 2021, 200 Covid deniers gathered in front of the Parliament. They burnt face masks to show that they thought they were unnecessary.
This short paragraph is easily debunked. Readers of the Daily Sceptic know that Covid now has an infection fatality rate about the same as influenza. We also know that side effects from the Covid vaccines – both the mRNA and the viral vector vaccines such as AstraZeneca’s – are more common than for other tried and tested vaccines. Remember when the Pandemrix vaccine rollout was halted because of a link to rare instances of narcolepsy? Multiple studies show Pfizer and Moderna’s Covid vaccines increase the risk of myocarditis and pericarditis in especially younger males – the demographic who make up precisely half the readership of Fabel 10. The German Government even admits that as many as one in 300 doses of the mRNA jabs produce serious injury. Compared to the danger that Covid poses to most people, does that make vaccines worth having?
And as for restrictions, a new consensus is gaining momentum. Whereas back in 2021, when the book was written, it was mainly agreed that lockdowns and other Covid restrictions were necessary to halt the spread, and countries with low Covid fatalities would credit these non-pharmaceutical interventions for their comparatively low excess mortality, studies later proved them incorrect. Lockdowns and excess mortality were not correlated. Whereas back in the early days of the pandemic, only a few, brave voices spoke up about their concerns, now even Rishi Sunak, who helped implement Britain’s lockdowns, admit they were detrimental to overall health and the economy and did little to stop infection. Yet in Norway, pupils are stuck in the reality curated more than a year ago, a reality that has now been revealed to most as bonkers.
And those 200 “Covid deniers” who burnt face masks deserve praise for being a tiny minority speaking up for science at a time where “the science” became an allegory for anything the authorities wanted us to do without having to prove why.
The book also states that vaccines are “95% effective against COVID-19 infections”. This is clearly nonsense, and doesn’t need further debunking. We all know of multiple-jabbed people getting infected several times over, and that infection rates in highly vaccinated countries went through the roof after the vaccine rollout.
Perhaps the book will serve as a test to pupils old enough to gather information from multiple sources. Some might agree with what they’re presented with, while others will see through this Government-approved misinformation. But that’s not really the sort of education you want in a free, democratic country. The book doesn’t invite 14-15 year-olds to question or discuss – it presents them with all the (wrong) answers. That’s bad enough in itself, but what’s worse is it tells them to ridicule those who don’t agree. The chapter on Covid and conspiracy theories could have been a great opportunity to teach children about academic freedom, online censorship, tolerance, debate, dissent and freedom of speech. Instead, it serves straight-up, Orwellian newspeak to young minds in a way the CCP would be proud of.
DC Mayor: No vaccine passport, no education – even for virtual learners

By Ken Macon | Reclaim The Net | August 26, 2022
The District of Columbia mayor Muriel Bowser said kids who do not have a vaccine passport within the first 20 days when schools resume next week Monday will not be allowed to get educated, even for those doing virtual learning from home.
A press release on the District of Columbia Public School’s website states: “The Coronavirus Immunization of School Students and Early Childhood Workers Amendment Act of 2021, which the Council passed in 2021, requires students ages 12 and older to be vaccinated against COVID-19 in order to attend school.”
The vaccine mandate applies to staff and also private schools.
Asked by The Daily Signal what the plan was for unvaccinated students, Bowser said: “They can go to school on Monday. But they need to get their vaccinations… and their families will be alerted as to the dates.”
The Office of The State Superintendent of Education for the District of Columbia recently announced that “all students must have up-to-date immunization certification on file with the school within the first 20 school days or they will not be allowed to attend school or school activities until the immunization certification is secured by the school.”
“If the student does not come into compliance within a 20-school day period, the school must remove the student from school until the immunization certification is secured by the school,” the office added.
The vaccine mandate will likely affect the education of black students as 47% of black children aged 12-15 in DC have not received the primary vaccination needed to attend school, according to government data. And 42% of black kids aged 16 and 17 are not vaccinated.
CDC Director deflects blame for lockdowns towards predecessors

By Mike Campbell | The Counter Signal | August 25, 2022
CDC Director Rochelle Walensky admitted organizational shortcomings on Fox News while deflecting blame toward predecessors for their lockdown recommendation.
“Many of those lockdowns pre-dated me at the CDC,” she said.
Walensky, who once used ‘Trust the science’ to persuade the public, carried a humbler tone while reflecting on her organization’s decisions.
“There were important decisions that we had to make in imperfect times, with imperfect data, and we always updated those decisions as those data were evolving…”
“So, I don’t really want to re-visit the questions of lockdowns that pre-dated me, but what I will say is, we’ve updated our guidance in the context of new information, and sometimes we have to make a decision before we have all the information that we want…”
Indeed, the CDC updated guidance by removing special quarantine recommendations for unvaccinated persons, effectively admitting that vaccination status is no longer relevant when it comes to infection or spread of the Covid virus.
In fact, on July 23, the CDC deleted a ‘fact’ from their “Facts about mRNA Covid-19 Vaccines”, and they did so without explanation. Last time I checked, facts don’t change — but apparently, they do for the CDC.
Walensky further stated that “[their] science” indicated hybrid immunity was superior to natural immunity. However, we’ve reported on a scientific study that accounted for more than 5.7 million people, which showed that natural immunity is just as effective as hybrid immunity.
To this point, Walensky’s usage of science in the possessive sense — by calling it “our science” — denotes a departure from “the science,” of which they’re either arbitrarily picking from or are completely unaware.
Between Fauci stepping down and Walenski pointing fingers, it appears the blame game has officially started.
Disappearing YouTube Misinformation Prevention Policies on Masks and Social Distancing

The Naked Emperor’s Newsletter | August 23, 2022
Earlier in the year YouTube’s COIVD-19 medical misinformation policy wouldn’t allow you to post content which contradicted the WHO’s or local health authorities’ guidance on various issues including:
- Social distancing;
- Claims that wearing a mask is dangerous or causes negative physical health effects;
- Claims that masks do not play a role in preventing the contraction or transmission of COVID-19

Now, it’s perfectly fine, signalling that those claims are no longer misinformation. Too bad if you previously had your account cancelled for questioning those policies. You should know by now when it is ok to question The Science™ and when it is verboten. Do keep up.

Featured Video

US Middle East Policy: The Growing Propensity for Genocide
or go to
Aletho News Archives – Video-Images
From the Archives
The New Baghdad Pact
By Dr Bouthaina Shaaban | February 23, 2017
A recently declassified CIA document prepared in 1983, and released on 20 January 2017, shows that the United States had at the time encouraged Saddam Hussein to attack Syria, which would have led to a vicious conflict between the two countries, thus draining their resources.
The report, which was then prepared by CIA officer Graham Fuller, indicates that the US tried adamantly to convince Saddam to attack Syria under any pretense available, in order to get the two most powerful countries in the Arab East to destroy each other, turning their attention away from the Arab-Israeli conflict. … continue
Blog Roll
 Aletho News
Aletho News- Hezbollah denies involvement in deadly attack on UNIFIL in south Lebanon
- The prospect of an expanded and far more violent war
- Canada’s Carney Revives Online Censorship Bill
- Israeli soldiers kill UNICEF truck drivers delivering water to Gaza families
- Iran defends limits on Strait of Hormuz passage
- ‘We warned you’: Hormuz Strait back to pervious state amid US blockade
- Iran rejects uranium transfer, warns of response to naval blockade
- US Middle East Policy: The Growing Propensity for Genocide
- Daniel Davis: Iran Reopens the Strait of Hormuz
- Trump taps military-grade flu pandemic architect to lead CDC amid simultaneous gain-of-function and vax development
- If Americans Knew
- Israel relegates another population to life in tents – Daily Update
- Senate again fails to block weapons to Israel
- Think the Iran war is a disaster? Blame these DC think tanks first.
- Number of Palestinian Prisoners Rises By 83% Since October 2023
- With multiple “ceasefires” in place, Israel keeps on killing in Gaza and Lebanon – Daily Update
- Mearsheimer: Israel Owns Trump
- Mark Levin and Jonathan Pollard Push for Nuking Iran
- TCN: America Enables Israel’s Crimes
- Israel’s Next Leader Will Be Just Like Bibi – but Without the Corruption
- Born into war, raised across borders: The story of Gaza’s premature babies separated from their parents amid Israel’s genocide
- No Tricks Zone
- Reality Check: Maldives Have Actually Grown In Size Or Remained Stable Over Recent Decades
- Abrupt Climate Change Also Occurred NATURALLY In The Past …25 Times During Last Ice Age
- Cave Discovery Reveals Today’s Desert Climates Were Recently Far Warmer, Wetter, Teeming With Life
- German Expert: Heat Dome Led To Record Temps In Western USA…Warmer In 1934, 1936
- New Study: No Linear Warming Or Glacier Retreat Along Northern Antarctic Peninsula Since 1980s
- An Inconvenient Tree: Uncovered In Alps… Europe Much Warmer Than Today 6000 Years Ago
- New Study Reports A 60% Slowdown In Greenland’s Ice Loss Rate In The Last Decade
- Low Intensity Tornado Wrecks Major Solar Farm, Creating A Potential Toxic Dump
- New Study Finds Warming Saves Lives…Cold Temperatures 12 Times More Deadly Than Excess Heat
- German Science Blog Accuses PIK Climate Institute Of Hallucinating Climate Tipping Points
